Music therapy, combined with standard medical treatment�has been found to reduce the perception of pain in individuals recovering from spinal surgeries, according to a study published in the American Journal of Orthopedics. Spine surgery recovery can take a long time and take a tremendous toll on the individual and family. Research has found that music therapy can help reduce pain post-surgery.
The study has shown solid findings that this therapy, when combined with standard treatment, positively impacts pain. Individuals report an increase in comfort during the recovery time. Utilizing music in a therapeutic setting can benefit a patient’s treatment plan, as it addresses the whole individual, including mind, body, and spirit. This is the same approach that chiropractic uses.
Combining Standard Treatment with Music Therapy
The study took place at the Spine Institute of New York with the music therapy set-up through the hospital�s Louis Armstrong Center for Music and Medicine. There were 60 patients thirty-five females and twenty-five males ranging in age from 40 to 55. They underwent anterior, posterior, or anterior-posterior spinal fusion surgery. The groups were equally split up. The experimental group had music therapy included with their standard medical care, and the control group only received standard medical treatment.
The experimental group would undergo a 30-minute music therapy session over an 8-hour period within 72 hours after the procedure. The music options included:
Patient-preferred music
Singing
Rhythmic drumming that encourages relaxation
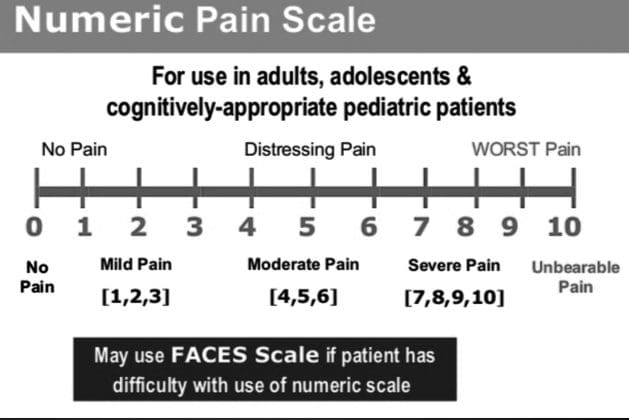
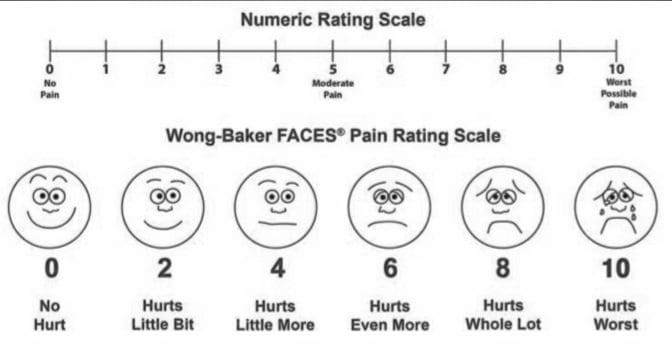
The sessions focused on personal treatment, where the individuals were encouraged to express emotions. A pain scale was used before and after the interventions to measure the results. What was found, was that pain levels would go up slightly in the control group, and in the experimental group, the pain dropped.
Spine Surgery Recovery
With standard care medications are typically the first-line treatment post-spine surgery pain. With all of the negative side effects that come with pain meds/opioids, music therapy is worth considering when looking for non-drug therapies. If anything music is an excellent distraction tool. So long as the music is enjoyable to the individual.
For the most part, many individuals that underwent spine surgery already listen to their music pre and post-operation. It helped them to relax before the surgery and allowed them to focus on something else after. Much like athletes that have their headphones/earbuds when they get to the venue to focus and block out everything going on around them. This therapy works the same way. But now we want to encourage anyone undergoing some spinal procedure to go ahead and jam out.
Calcium is vital to bone health, and as long as you are getting enough supplements are not necessary. Calcium is a primary building block for strong, healthy bones, especially the bones of the spine. A diet rich in Cacan help prevent spinal problems/issues/conditions like spinal fractures and osteoporosis.
The best and easiest way to get the proper amount of calcium is by eating plenty of Ca-rich foods. However, calcium supplements could be utilized to ensure the proper amount is taken every day. To determine if you may need a calcium supplement talk with your doctor to make sure it�s the best option for you.
Calcium Supplements
Calcium supplements can help individuals reach the daily recommended amount, but they are not intended to replace real Ca-rich foods. If there is enough Ca in your diet, a supplement won’t be necessary, unless there is an underlying condition that doesn’t allow the individual to eat certain Ca-rich foods. However, if there is only a lack of sufficient calcium intake then supplements could help. Otherwise, if there is a continued lack of Ca it could be detrimental to bones and overall health.
Proper Amount Every Day
Before considering a supplement, it�s essential to know how much calcium you should be getting each day. Daily recommendations vary by age and sex but largely depend on age:
Men and women age 19-50, including pregnant women, require 1,000 mg a day
Men 51-70 require 1,000 mg a day
Women 51-70 require 1,200 mg a day
The elderly 71 and over require 1,200 mg a day
Your Diet
Once you know how much Ca you need, the next step is to evaluate how much to get. The American Bone Health advocacy group recommends using the Calcium Rule of 300 to determine if a supplement is necessary.
The way it works:
Begin with the number of dairy or juices with added calcium and the amount that is consumed daily.
Multiply that number by 300.
Add 300 if a nutritious and balanced diet is being observed
The total is the proper dietary intake of calcium
If the total does not meet the recommended number consult a doctor or health coach about a calcium supplement.
Supplement Tips
If you decide to take a supplement, check out these tips:
Make sure your doctor/pharmacist know all medications and supplements being taken, this includes over-the-counter products. The reason for this is your doctor wants so be sure they will not interfere with each other or have some kind of negative side effect. An example of this is calcium and iron supplements can prevent each other from properly�absorbing into the body when taken together.
Buy supplements that have the USP Verified symbol, which shows that the supplement has been independently evaluated and certified.
Rather than taking one high-dose calcium supplement, which could be more than 500-600 mg. Smaller-doses of supplements can be taken 2-3 times throughout the day.
The body cannot absorb more than 500-600 mg of calcium supplement at once
Don�t take the supplement with a high-fiber meal or laxative. This fiber can prevent the body from fully absorbing the calcium
There are all kinds of nutrients that contribute to the development and maintenance of healthy bones, but calcium is backed by a strong body of evidence that presents a clear connection to bone health. A simple and straight-forward focus on eating foods rich in calcium can help keep the bones of the spine, and entire body for that matter�strong and supportive for life-long healthy movement.
A February 2020 study explored the relationship between low back pain and menopause. Hormones and vitamin D play a role. Vitamin D deficiency is related to increased lower back pain and degenerative disc disease in postmenopausal women. Decreasing estrogen levels can also drop levels of vitamin D, which can be downright painful if left unaddressed.
Menopause:
Hot flashes
Mood swings
Sleep issues
Libido changes
A drop in�estrogen levels can cause these symptoms.
Degenerative Disc Disease
In between the vertebra are fibrous discs that are the shock absorbers for the spine. These discs also support and stabilize the spine, which allows you to move freely pain-free. The health of the spine is a vital part of well-being and provides the ability to bend, lift, twist, and perform normal activities without pain.
With the passage of time, the discs start to dry out and lose their flexibility and elasticity. When the discs dry out, known as desiccation is a natural process that happens as we age and does not always cause pain symptoms. The discs become thinner and less able to absorb shock that can lead to pain and stiff movement. The loss of elasticity and height in the discs is known as degenerative disc disease.
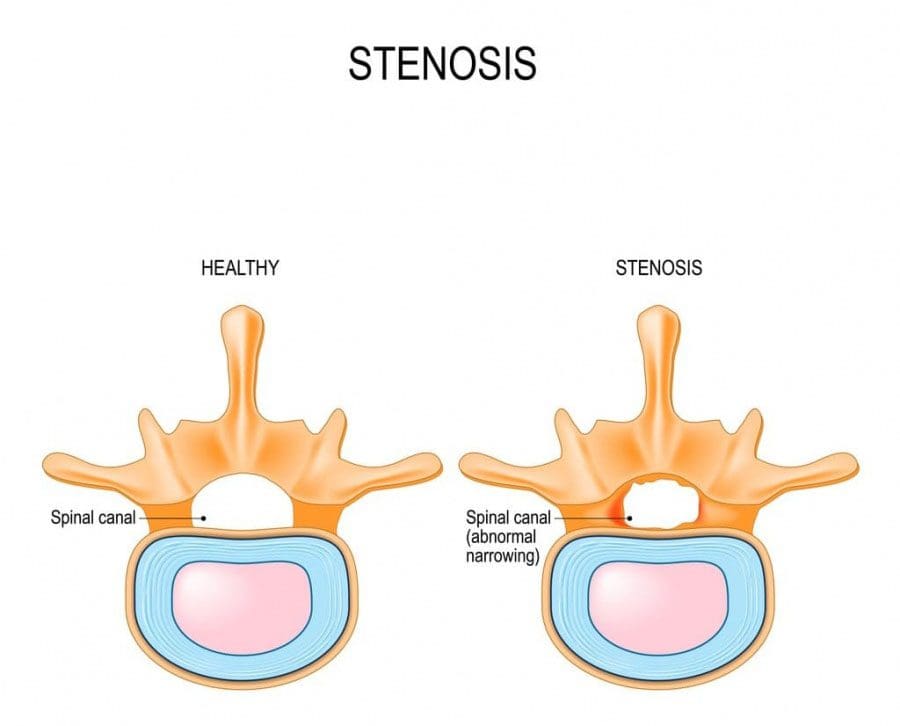
Stenosis/Compression
With degenerative disc disease, sometimes the body tries to compensate for the loss of stability by producing more bone to stabilize the spine.
This causes bone growth/s, called bone spurs or osteophytes. These can crowd the spinal canal, which is a condition called stenosis.
Stenosis places pressure on the nerve roots that branch off the spinal cord.
The symptoms of this compression can present with:
Pins and needles sensations
Muscle spasms
Decreased sensation to touch
Weakness and pain in the back or that radiate down the arms or legs.
Treatments for degenerative disc disease include physical therapies and surgery. Most cases are treatable without surgery by utilizing physical therapy, occupational therapy, strength/flexibility exercises, injections, and supplements. Surgery could be considered to make more room in the spinal canal, relieve nerve compression, and reduce pain.
Vitamin D and Bone Health
Vitamin D has multiple functions in the body. It’s produced by the body when exposed to sunlight and is also found in certain foods and supplements. One function of vitamin D involves bone health support. The body needs vitamin D to absorb calcium and phosphorus, which are essential for bone production. Calcium is stored inside the bones.
When there is a deficiency in calcium, the body breaks down the bone/s and takes/pulls the calcium back into the blood. Inadequate vitamin D means the body is not able to absorb enough calcium and cannot prevent the bones from being broken down. Vitamin D deficiency at an early age can cause low bone density along with diseases like rickets, osteopenia, and osteoporosis. Osteoporosis is a condition where the bone gradually weakens and breaks easily.
It can cause vertebral compression fractures, where the vertebrae crack because the bone tissue is not strong enough to support the body�s weight and resist gravity.
Two causes of osteoporosis are nutritional deficiencies and hormonal imbalances, like low estrogen production after menopause. Proper vitamin D/calcium intake is essential for preventing and reducing bone loss that can lead to these conditions and increased lower back pain.
Estrogen and Bone/Spine Health
Estrogen plays a role in male and female bone health. Cells called osteoblasts help in the production of bone are highly active. Estrogen helps slow the breakdown of bones and promotes bone growth. A drop in estrogen over time compromises the health of bones. Individuals with chronic hormone imbalances and postmenopausal women are frequently affected by bone disease/s and the loss of bone density over time.�Studies reveal the risk of developing osteoporosis is higher in postmenopausal women.
Estrogen helps maintain tissues that contain collagen, which is found in intervertebral discs. Lower estrogen levels following menopause have shown to lead to more severe lumbar disc degeneration and increased lower back pain in women when compared to men. This demonstrates the importance of monitoring changes in lower back pain for women after menopause.
Vitamin D and the Spinal Discs
The relationship between increased low back pain in postmenopausal women and vitamin D deficiency is real. Supplements can help correct these deficiencies, can help reduce low back pain and promote bone health.
Postmenopausal women are especially at risk for vitamin D deficiency. Vitamin D and calcium supplements can be used in combination.The bone/s breakdown is stopped, while the bone tissue is strengthened thus reducing back pain. Low back pain brought on by degenerative disc disease is pretty much present in patients over age 65.
These health concerns can be helped through:
Vitamin supplementation
Exercise
Healthy diet
Slowing down bone loss can be achieved with strategies that range from diet change to prescription medication.
A doctor could recommend alternative treatments, as part of aplan for neck pain like acupuncture, herbal compounds, and yoga. You may want to try them out yourself. Many have reported that these have really helped. Please consult a doctor before trying any alternative therapies. These are safe but should be set-up by a professional to make sure they are done safely. For example, there could be negative interactions between herbs, supplements, and other medications being used.
Acupuncture
This is an eastern approach to healing. Acupuncture focuses on the body’s energy force known as Qi or Chi. When the energy is blocked from flowing this is when physical illnesses develop. Acupuncture restores the healthy energy flow. It isn’t better or worse it is just different.
Herbal Medicine
There are herbal compounds that have proven to be useful for neck pain.
Capsaicin Cream
Capsaicin is a chili pepper extract and can help relieve neck pain. It temporarily reduces pain. Capsaicin cream can help with osteoarthritis and muscle pain, which both cause neck pain.
Devil’s Claw
Devil’s claw comes from southern Africa, where it has been used for centuries to treat fever, arthritis, and gastrointestinal problems. It is used for conditions that cause inflammation and pain, like cervical osteoarthritis.
White Willow Bark
White willow bark is how aspirin in Europe was developed. Synthetic versions like aspirin can irritate the stomach, which is why the natural white willow bark is used instead. It helps with conditions that cause pain and inflammation like osteoarthritis.
Massage
Neck pain can be caused by stress, overuse, and misuse. Misuse means like sitting hunched over a computer for too long every day will take its toll. Massage helps to release tension, relieve muscle inflammation, and pain. Regular massages could help as a preventative measure.
Yoga/Pilates
Yoga and Pilates can increase core strength, improve balance, posture, and reduce stress. These can all help deal with neck pain/ prevent neck pain when done correctly and safely. Neck pain relief can be found with these treatments. Treatments that focus on relieving tension or stress can prove especially helpful if the pain is related to tight muscles and the physical effects of stress.
These alternative treatments could work at their optimal in combination with other therapies. This is to fully address the underlying spinal condition/root cause, along with any other neck-related symptoms.
Companies are doing what they can to keep operations moving and workers employed. Those that are able to work-from-home are doing so. But working from home is new to many and creates new challenges of converting an area in the house, apartment, etc, to become the workspace.
Back pain is common whether at the office or at the house. Everyday activities like the way you sit or lift can cause back pain if you�re not careful. At the house, it can be easy to lose track of time working. However, sitting with the wrong chair, at an improper height is not great for the body and overall health.
Working from Home and Back Pain
You probably thought you�d be comfortable working while lounging in bed or slouching on the sofa. However, after a few hours,�you would have a sore back, neck, or shoulders muscles. Working on a laptop for hours daily�at the kitchen counter or hunched over a coffee table and not sitting at a table or desk with a proper chair can lead to pain.�The best way to reduce and avoid back/neck pain is to make a few changes to the workstation.
Setting Up The Workspace
A comfortable workspace will increase productivity and physically help you feel good.
Working comfortably for hours, maintaining proper posture, it would be wise to invest in practical office appliances that can support physical well-being. Proper office ergonomics include:
The correct chair height
Footrest
Working desk posture that keeps muscles and joints comfortable
Choosing the ergonomic office chair is important, considering you will be using it for back support. Office chairs are not a one size fits all. The choice could be the difference between having continuing back pain or improving comfort, health, and overall productivity.
Ergonomic Back Support
Despite the adjustable ergonomic chair, you might still have back pain while working. Consider the following because it might not be the chair that�s not working.
Keep Moving Around
Step counts could take a dive when working from home. Exercise and stretching at regular intervals are extremely important to protecting the spine throughout the day. Remembering to do this at home can be harder than working in an office environment. Use an automatic reminder on the phone. Our bodies need regular low-impact aerobic activity. It provides the tissues with vital blood flow and helps minimize back pain.
Be Sure To Check Your Posture
The spine is not fixed in abnormal positions. Sitting and slouching forward for a long time will contribute to back pain. The advantages of sitting straight:
Keeps the Joints Aligned
Keeps the Bones Aligned
Supports the Muscles
Supports the Ligaments
Prevents Muscle Fatigue
Sit all the way back in your chair and take full advantage of the lower back support. The knees should be bent at a 90-degree angle with the feet flat on the floor or on a footrest.
Proper Screen Height
The height of the computer screen should not be too high or too low. Your eyes should aim at the center of the screen without having to crane your neck up or down. It should be directly in front to avoid tilting or turning your head. A laptop should be raised anywhere from 5 to 10 inches to provide the proper height.
Speaker Setting
Don’t go for the multitask when it comes to the phone. Having the phone between your neck/shoulder and working at the same time can lead to stressing your back and hurting/injuring the muscles. Turn on the speaker or use a headset to avoid the awkward neck position.
Breathe Deep
Proper breathing keeps the body and the muscles in the mid and lower back nicely relaxed. Improper breathing can make the nervous system react, causing pain or discomfort. Breathing exercises can be a way to target lower back pain/s. No special equipment is needed and can be done anywhere, anytime. Concentration is the key. Inhale and bring the navel towards the spine and then exhale. This exercise will engage the core muscles and will support the upper body.
With so much at stake, our bodies have developed a complex self-defense system to protect the spinal cord and its critical two-way�sensory information flow. As the body�s nerve center the spinal cord controls almost all voluntary and involuntary movements throughout the torso, arms, and legs.�It also receives sensory input from the torso and limbs. The�spinal cord plays a critical role and needs to be defended. The most prominent protection for the brain is the skull, for the spinal cord, it is more complicated.
Self Defense
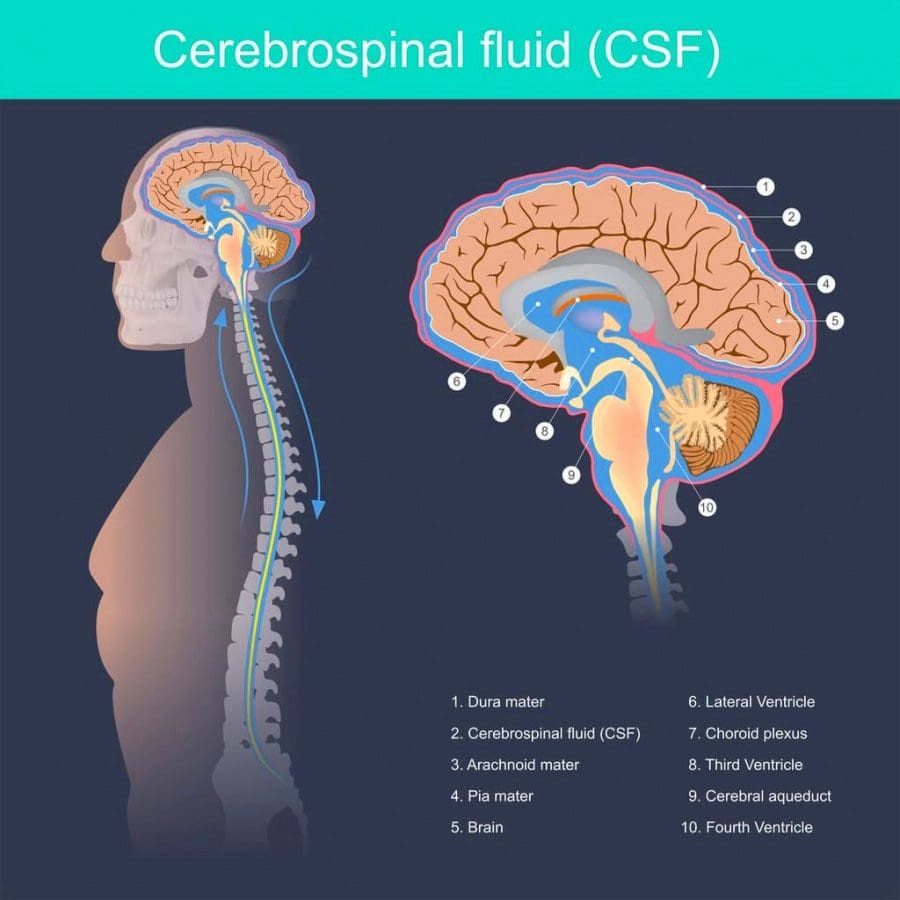
The spinal cord consists of a bunch of nerves. One of the self-defenses is the cerebrospinal fluid (CSF) that cushions and nourishes them. On the outside, the spinal cord is protected by the tube structure known as the meninges. Three-layered membranes make up the meninges, each with its own protective role:
Pia mater
Arachnoid mater
Dura mater
Self-defenses do not stop there. Another self-defense includes the vertebrae or the backbones themselves, intervertebral discs, and various muscles and ligaments.
Meninges
The meninges are three layers of membranes that encapsulate the spinal cord at the brainstem from the top to the bottom of the spine. The innermost layer is the pia mater and is attached directly to the spinal cord. It is made up of mostly collagen that has an elasticity that allows the cord to maintain its shape. Next comes the arachnoid mater and is the middle layer.
Its primary role is to maintain the cerebrospinal fluid that fills the subarachnoid space between the pia and the arachnoid. A common condition known as arachnoiditis involves the arachnoid mater. It is a painful inflammation of the membrane that requires medical treatment. It can lead to disability if it is progressive.
Dura Mater
The outer layer is the dura mater and is the toughest. The dura rests on the arachnoid with a small amount of fluid in-between. The epidural space separates this membrane from the wall of the vertebral canal. Although it is tough, tears can occur. Tears can result from:
Injury
Epidural injections
Lumbar punctures
Complications from spine surgery
Some individuals can even develop tears spontaneously, sometimes as a result of a connective tissue disorder. When the dura tears cerebrospinal fluid leaks out of the space, leaving the brain and spine with less cushion and support.
Postural headaches are worse standing than sitting or laying down and can be severe are the most common symptom of spinal fluid leaks. But these tears typically heal quickly with bed rest.
Cerebrospinal Fluid
Cerebrospinal fluid is the clear liquid that fills the space between the pia and the arachnoid. It is made in the brain�s ventricles with its primary function to protect and nourish the spinal cord and brain. The fluid also removes waste products from the brain. The fluid also plays a role in helping doctors diagnose disease/s.
If a doctor suspects a severe infection or disorder of the central nervous system, they perform a lumbar puncture or spinal tap. The fluid can also contain evidence of inflammation or infection from waste products that the central nervous system discarded into the fluid. A doctor inserts a needle between two vertebrae in the lower back to remove a small amount of cerebrospinal fluid. The fluid is sent to the lab and analyzed. Lumbar punctures can be used to diagnose conditions like:
Infectious brain and spinal diseases like meningitis and encephalitis
To see how the fluid is moving diagnostic images are done by injecting dye know as myelography or radioactive substances known as cisternography into the subarachnoid space before imaging. Lumbar punctures can also be used to measure the pressure of the cerebrospinal fluid.
Vertebrae
There are 33 bones that make up the spine that forms a framework shaping the body and protecting the spine.�In a healthy spine, the neck vertebrae curve slightly inward called lordosis, while the middle vertebrae curves outward called kyphosis before meeting the low vertebrae curved inward. This makes the spinal cord flexible and balanced.
Each vertebra has a complex shape with a precise configuration determined by the location in the spine. Many conditions of the vertebrae involve nerves that get pinched/compressed as they exit the spine. Pinched nerves usually result from bone spurs on the vertebrae that crowd the canal and from herniated discs.
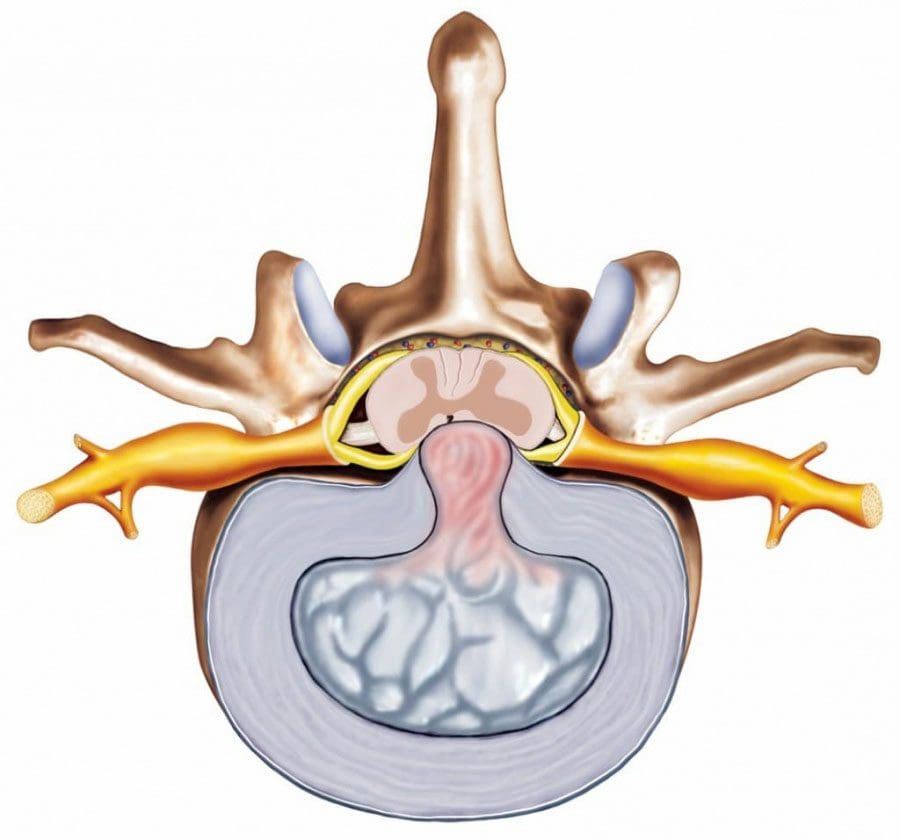
Intervertebral Discs
The intervertebral discs are the spine�s shock absorbers. They fill the space between two vertebrae with no direct contact. The endplates of each are coated with protective cartilage which anchors the discs in place. The gel substance part of each disc is called the nucleus pulposus. The tough cover known as the annulus fibrosus wraps around each disc to protect and shape it. There are no blood vessels in the discs and are nourished by the endplates of the vertebrae.
Herniated discs are the most common disc-related condition. When a disc herniates, the annulus fibrosus tears. The tear leaks out the protective gel to bulge out into the spinal canal. With no room in the canal for anything but the spinal cord and spinal fluid, the gel puts pressure on the surrounding nerve/s and the spinal cord itself. This is called myelopathy when the spinal cord gets compressed. Non-surgical treatments are quite successful in healing herniated disc/s.
The spine�s self-defense is elaborate, effective, and complicated. Consult an experienced spine specialist/chiropractor who can produce the best results and benefits.
Dr. Alexander Jimenez takes a look at how to keep your back healthy while doing yard work and gardening. We�re looking for ways to find mental and physical engagement without socializing. Many individuals are breaking up isolation and monotony by doing some home projects out in the yard and garden.
Doctors may tell patients that yard work and gardening should be avoided if they have a bad back. Individuals with a history of back pain/issues or have had spinal surgery might think that gardening is out of the question.�None of this is true. Yard work and gardening can be therapeutic physically and mentally for individuals with compromised backs as long as they follow some common-sense safety concepts.
Gardening with an ergonomic approach can make yard work and gardening very back/spine-friendly. If possible try to get tools for gardeners with neck and back problems or modify your own. Modified tools can highly reduce the chances of injuring your back. Try to set up the yard or garden in a way where there is minimal bending and reaching.
If this cannot be achieved set up the work to be done in an order where any bending/reaching tasks are spaced out so as not to be doing them all at once. Here are some ways for back-preservation when doing yard work and gardening. They will make your work more productive and reduce fatigue, discomfort, and minimize the risk of exacerbating any back injuries/problems.
Environment
Working in the right environment is an important step for those with a bad back. If possible garden on a raised platform or a raised garden that is at a comfortable height to be able to stand and garden without bending and reaching. Structures can be purchased, or make them yourself with old broken used furniture like tables, shelves, etc. Garden beds can be worked using the square foot technique to minimize bending, reaching and squatting.
The Square Foot gardening technique was invented in 1976 by Mel Bartholomew, a civil engineer, and efficiency expert that took up gardening after retiring. These types of gardens are made to be waist level using old furniture, self-made or store-bought frames that are back-friendly. Gardening like this means less time weeding, bending and reaching with more time enjoying the therapeutic benefits.
Preparation with the Spine in Mind
Here are some tips on modifying your methods and tools for safe yard work and gardening. One example is using a golf bag with wheels for carrying and select long tools. Also using a two-wheeled garden cart/wheel-barrow. It is more balanced than a standard wheelbarrow and is better for the spine.
Practice Safe Posture/Position
Never use the back muscles to lift. Lift with the legs. Bend the knees, hinge at your hips and keep the back straight. If needed practice bending in front of a mirror to see your form and make sure the technique is being done properly. Check out this YouTube video on raking and hoeing. Plant containers while standing using a potting bench, or an old table. Have a stool, chair or heavy-duty bucket to sit down easily when a break is needed.
Containers
One back-friendly gardening technique is to plant in containers. Plant them where they will sit, which minimizes having to lift or carrying to a location. Styrofoam peanuts can be placed at the bottom third of the container instead of gravel to make the containers lighter. If using large containers, invest in a wheeled pot dolly to move the containers easily.
Focus on the Time and Not the Task
With big projects, break them down into smaller more manageable tasks. Dividing the bed/s into halves or thirds makes the work more pleasant. Underestimating how long a project might take can be a major set back. So set time limits and follow through. When recovering from surgery or a back injury, set a limit of 15 minutes of work and see how it feels.If your back is not irritated or sore then expand to 30 minutes and so on.
Work smarter not harder. Under no circumstances should you shovel or pull up heavy, deep-rooted plant/s. This type of movement could put an end to yard work and gardening for some time. Do not forget that pain is our body’s way of telling us to stop. Be sure to talk with a spine specialist or chiropractor before starting yard work or gardening.
Gardening Benefits
Activity and fresh air can make us feel healthy and happy. Gardening can provide this along with healthy exercise. Therapeutic benefits of yard work and gardening have been well documented. Gardeners that did daily work were found to experience significant reductions in stress and improvement in overall health and quality of life compared to non-gardeners.
Gardening can significantly raise levels of energy, optimism, zest for life, self-esteem, openness and other factors relevant to self-image. Even a little gardening goes a long way. Just being outside and the physicality of yard work and gardening contributes to stress reduction. Another benefit from gardening is if planting herbs, and veggies you can cook even healthier. Much like a farm to table restaurant.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine