PODCAST: Ryan Welage and Alexander Jimenez, both medical students at the National University of Health Sciences, discuss the several new approaches that they developed in order to help people continue to engage and participate in exercise from the comfort of their own homes. Using their advanced understanding of functional medicine, biomechanics, and nutrition, they undertake explaining simple methods and techniques for complex movement protocols. Moreover, Alexander Jimenez and Ryan Welage discuss how diet can be an essential element in overall health and wellness. Dr. Alex Jimenez offers additional guidelines with the Functional Fitness Fellas, among further advice. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
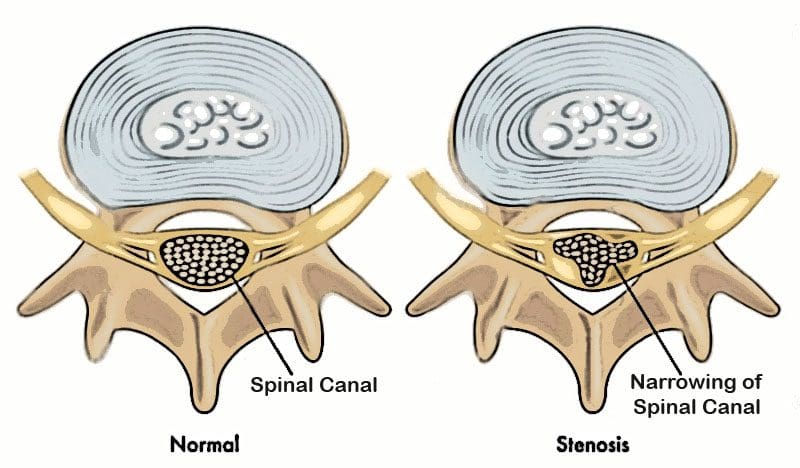
Recognizing and understanding common and not so common neck and lower back spinal Stenosis symptoms can help in getting an early diagnosis and beginning a preventative treatment plan. Symptoms develop when the spinal canal begins to narrow. The nerve roots become compressed/pinched causing:
Neural irritation
Inflammation
Pain
The low back and neck are commonly affected by this age-related and progressivedisorder. Symptoms can inhibit the ability to move without discomfort, pain, and neurological issues like tingling sensations and numbness that spreads out or radiates into other parts of the body.
Low Back Spinal Stenosis Symptoms
The most common symptom of spinal Stenosis is pain in the:
Low back
Buttock area
Back of the thigh that gets worse when standing and walking
These symptoms are called neurogenic claudication. Some individuals with low back spinal stenosis experience symptoms only when standing or moving/walking around. Discomfort usually eases up when bent forward and goes away when the individual sits down. Example: Grocery shopping feels a lot better when leaning forward on the handle of the cart, with pain reduced. This is common for people with spinal stenosis in the low back. Pain that goes away and reduces when bending forward, sitting down, or lying down is common of low back spinal Stenosis.
Understanding that claudication is not neurogenic or pseudo claudication is important. The symptoms of claudication are similar to pseudo claudication, however, the cause is different. Claudication is caused by the blood not circulating properly in the leg muscles. Other symptoms are low back pain and low back spreading pain or radiculopathy.
Better known as sciatica, lumbar radiculopathy involves:
Pain
Numbness
Weakness
Tingling/numbing sensations that travel down from the low back into the buttock/s and leg/s.
Some individuals experience pain in both legs, with one leg having worse pain than the other.
Bowel/Bladder emergency:
There can be severe cases of lumbar spinal Stenosis where the nerves that control the bladder or bowel can get compressed, leading to partial or complete incontinence. If there are problems controlling the bladder or bowel seek immediate medical attention.
Neck Spinal Stenosis Symptoms
Spinal Stenosis symptomsin the neck can cause cervical radiculopathy. This can include pain along with:
Tingling sensations
Numbness
Weakness
These symptoms may radiate downward from your neck into one or both shoulders, arms, and/or hands. The pain caused by cervical spinal Stenosis has been described as:
Acute
Episodic
Occasional
Chronic
The intensity can go from mild to severe along with other symptoms that include:
Headache/s
Balance issues with a higher risk of falling
Fine Motor skills like writing, buttoning up a shirt/blouse, computer keyboarding skills can become affected
With severe cervical spinal stenosis, symptoms can be associated with cervical myelopathy. Cervical myelopathy happens when the spinal canal narrows so much that it compresses the spinal cord in the neck. Pinched nerves in the neck can affect the shoulders, arms, and hands. Myelopathy can affect both the arms and legs.
Symptoms of cervical myelopathy can include:
Neck pain
Stiffness
Tingling sensations
Numbness
Weakness
Clumsiness
Balance issues
Difficulty walking
Bowel and Bladder problems
Sexual dysfunction
Symptoms Don’t Always Present
Imaging studies like MRI and CT scans can detect a spinal disorder from an individual that has no symptoms. This is why imaging tests are performed to confirm a diagnosis. This is supported by results from the physical/ neurological exams, medical history, and symptoms.
Those who have undergone an x-ray or other imaging test for a non-spinal related issue could have discovered they have spondylosis, osteophytes, and a herniated disc. However, they never knew it because they showed no symptoms. Spinal Stenosis of the spine is usually an age-related and gradual process of physical change. It can take time for symptoms to show themselves. If you have neck or low back pain symptoms that are becoming worse, speak with your doctor.
Bertolotti syndrome is something has not been heard of when it comes to lower back pain, but diagnostic work has uncovered a common congenital condition. Back pain is experienced at some point by all of us. Around two-thirds of the population will develop low back pain in their life, and more than half will develop chronic low back pain or pain that has lasted more than six months. Low back pain can be challenging in finding the root cause. Diagnostic work is required through� X-rays and MRIs. These tests can identify a lesser-known cause of mechanical low back pain called Bertolotti syndrome.
Bertolotti Syndrome
This congenital condition’s name comes from Italian physician Mario Bertolotti. It is in 10 to 20 percent of the population, �with or with no lower back pain. Bertolotti syndrome happens when the last lumbar vertebra, known as the lumbosacral transitional vertebra/LSTV. This vertebra and the sacrum become fused together or create a false joint due to an enlarged transverse process.
This can be bony bumps on the vertebrae where muscles and ligaments attach to the lumbosacral transitional vertebra. When the LSTV and sacrum fuse together, known as sacralization or pseudo-joint, it does not generate pain. It�s just the way that an individual’s anatomy has been since birth. Only when it causes lower back pain that it is called Bertolotti syndrome.
Causes
Low back pain that leads to inflammation and reactive muscle spasms brought on from Bertolotti syndrome can be caused by:
Asymmetrical structures of the lumbar vertebrae. If the LSTV is fused to the sacrum and iliac bone, these are the wings of the pelvis, which can place unwanted stress on the sacroiliac joint, which can cause pain that is felt above the buttocks.
A�pseudo-joint does not have the cushion or lubrication between the bones like real joints to absorb shock. This causes bone-on-bone grinding, which can be quite painful and can lead to osteoarthritis. This can also generate added stress on the discs of the pseudo-joint.
Sacralization fusion can decrease the spine�s mobility. This can speed up the wear and tear of the vertebrae and shock-absorbers of the intravertebral discs.
Added non-equal force/s on the muscle tissues that surround the lower back. This can be caused by the spine not being properly�aligned causing muscle imbalance/s and fatigue. Both sides of the back can be affected, but when tightness and muscle spasms in the low back and pelvis present, it’s usually only on one side.
Symptoms
Most individuals usually never know they have a sacralization or pseudo-joint. These are often found accidentally from an X-ray for something unrelated. But when symptoms present they can vary from person to person and usually appear in adulthood�in the 20s or 30s.
These include:
Low back pain that is localized and does not spread/radiate down the legs
Pain or discomfort in or around the sacroiliac joint
Stiffness that comes out of nowhere or difficulty moving a certain way with pain present
Symptoms improve once the individual sits or lays down
Diagnosis
Bertolotti syndrome can be diagnosed based on medical history, physical exam, and X-rays. A physical exam can include a recreation of the movement/s that triggered the pain/discomfort. An X-ray of the low back and pelvis will reveal any bony abnormalities.
Treatment
Bertolotti syndrome can be effectively managed with non-invasive treatments. These� include:
Improperly and overdoing repetitive rotation/s and extension/s through work or just movements that have become second nature are injuries just waiting to happen. Lifestyle changes and re-learning how to move properly will ease the strain on the affected area.
Over the counter pain medication/s like�Advil, Aleve, or Tylenol.
Chiropractic/Physical therapy can help build low back areas and increase mobility.
Local anesthetic and spaced out intervals of corticosteroid injections to the affected nerve/s to reduce inflammation.
Platelet-rich plasma (PRP) uses the body�s platelets to reduce pain, inflammation, and healing the damaged joints through an injection.
Prolotherapy treatment uses concentrated local anesthetic and dextrose injected into the low back area to enhance the body�s natural healing.
Radiofrequency ablation uses heat to numb the affected nerves around a pseudo-joint so that pain reduces.
Surgery is the last resort and is usually done to eliminate a pseudo-joint. It can also consist of reducing or removing an elongated transverse process�and can be performed as a same-day or outpatient procedure.
If you or someone you know is dealing with some form of idiopathic low back pain and doctors can’t seem to pinpoint the cause. Bertolotti syndrome could be a suspect, therefore it’s best to seek a spine specialist near you that can help.
PODCAST: Dr. Alex Jimenez, chiropractor in El Paso, TX, and Victoria Hahn discuss the fasting-mimicking diet and the ProLon Fasting Mimicking Diet program developed by Dr. Valter D. Longo. The ProLon Fasting Mimicking Diet is a high-fat, low-calorie intermittent fasting diet that may promote fat loss and reduce blood sugar, inflammation, and cholesterol, similar to other fasting methods. Valter D. Longo is an Italian-American biogerontologist and cell biologist known for his research studies on the role of fasting and nutrient response genes on cellular protection aging and diseases as well as for proposing that longevity is regulated by similar genes and mechanisms in many eukaryotes. Only a few research studies have been carried out to date regarding the fasting-mimicking diet and more research is needed to validate its benefits. �- Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
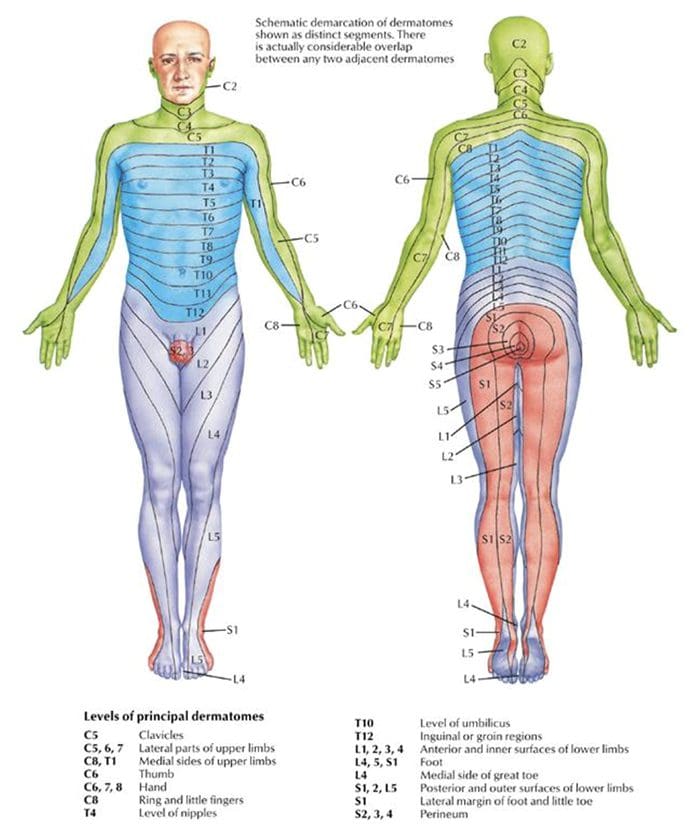
Burning, numbness, tingling, and pain can be felt in the back, lower back, legs, and feet. A lot of times these symptoms spread out/radiate from one part of the body into another area. Sciatica is an example of pain that radiates into an extremity, in this case, the back of the leg. Nerves originate from the spine and are divided/separated into sensory and motor nerves. The sensory nerve/s give the sensation to the skin known as dermatomes. Dermatomal patterns act as a map on the body.
Example: Dermatomes on the torso of the body react to the thoracic spinal nerve roots, the arms react to the cervical spine nerve roots, and the legs react to the lumbar spinal nerve roots.
Dermatome Location – Corresponding Spine Level
Shoulders – C4, C5
Inner/Outer Forearms – C6, and T1
Thumbs and Little Fingers – C6, C7, C8
Front of Thighs – L2
Middle, Sides of Both Calves – L4, L5
Little Toes – S1
A physician might use a piece of cotton, a swab, pin, or paperclip to test the symmetrical feelings in the arms and legs. Abnormal responses could be a sign of a nerve root problem.
Tendon Reflexes
Most individuals have experienced a physician tapping the knees with a rubber hammer. The normal response is a kick. This is a reflex, which is an involuntary muscular response generated by the hammer tapping the tendon. When the reflex responses do not present, this could mean that the spinal cord, nerve root, peripheral nerve, or muscle has been injured/damaged in some way. Absent reflexes are also clues to other conditions/injuries. An abnormal reflex response could also be caused by a disruption of the sensory (feeling) or motor (movement) nerves and sometimes both. Determining where the neural problem might be, a physician will test reflexes in various parts of the body.
Reflex Tested Areas – Corresponding Spine Level
Upper Arm Biceps – C5-C6 Cervical Spine
Forearm Distal Radius – C6-C7
Elbow Triceps – C7
Abdominal – T8, T9, T10, T11, T12, Thoracic
Knees/Thighs Patellar, Quadriceps – L3, L4 Lumbar
Ankles – S1 Sacral
Neurological Exams for Neck/Back Pain
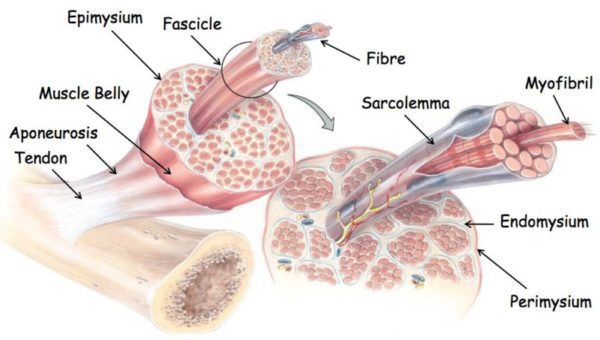
Muscle Strength/Tone
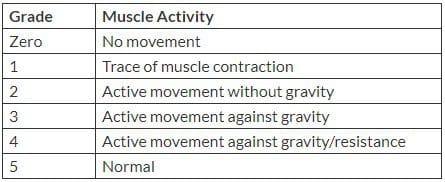
Muscle strength and tone measurements are another way to diagnose nerve deficits. Depending on the symptoms/condition/injury/s there are different ways to evaluate muscle strength:
Stepping on a stool
Standing on the heels
Standing on the toes
Hopping in place
Performing knee bends
Gripping an item in each hand
Muscle strength is graded and recorded in the patient’s chart.
A physician will test the body’s muscle tone by passively flexing and extending the arms and legs. Normal muscle tone will respond with a slight resistance to passive motion. Other movements test for proximal (trunk/torso) and distal (distant) weakness. Muscle symmetry is also taken into account.
Neurological Tests
If necessary a spine specialist might order neurological studies like a Nerve Conduction Study (NCS) or Electromyogram (EMG), to measure nerve performance.
Imaging Studies
MRI and/or CT scans of the spine can be ordered to help the spine specialist/chiropractor make a correct diagnosis, as well as help in creating a plan of treatment.
Conclusion
A neurological exam, along with a mechanical examination consisting of movement of the arms, legs, and torso, can significantly help doctors in making the correct diagnosis. Examination results are then correlated with the patient�s history, illness, and diagnostic studies. Once the diagnosis is made an appropriate treatment plan is discussed. This will begin with non-surgical strategies but if those fail, then surgical intervention could be considered.
Research has found that vertebrogenic chronic low back pain could be caused by a lumbar vertebral endplatechange that involves the basivertebral nerveand is not disc-related. The underlying cause of chronic low back pain can be very difficult to diagnose. The intervertebral discs are a common suspect, but when disc-related treatments don�t ease the pain, the root problem could be something else. Researchers are exploring an overlooked area with the vertebral endplates being the cause of vertebrogenic low back pain.
Research has found that there are more nerves in the vertebral endplates than in the spinal discs. More nerves can mean higher potential/increase in pain. And like the other areas of the spine such as the discs and joints, vertebral endplates can also degenerate, also increasing the risk for pain.
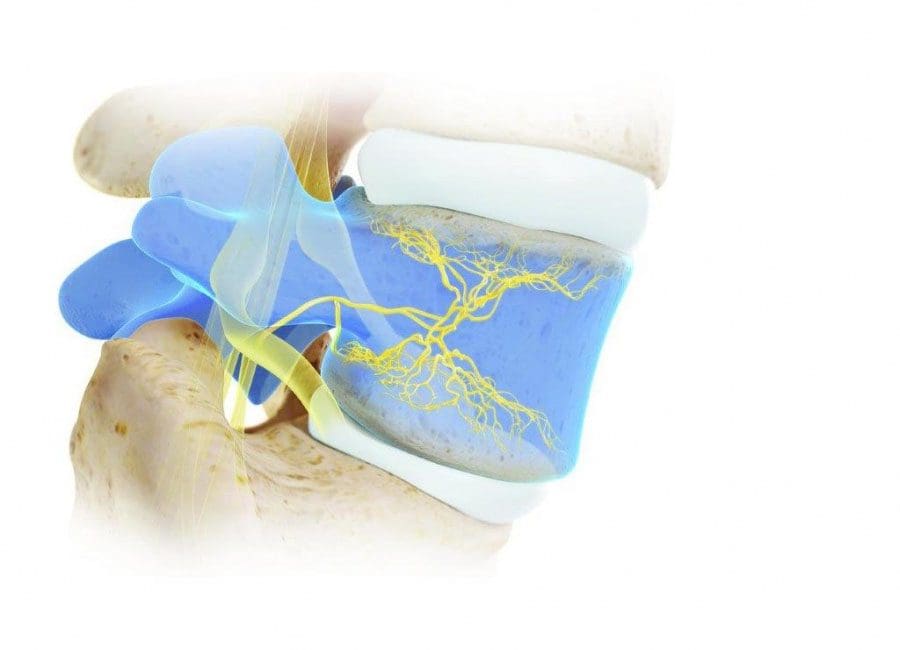
Vertebral Endplates and Basivertebral Nerve
The vertebral endplates line the top and bottom of each vertebral body. These are the round, thick, weight-bearing bones in the spine. The vertebral endplates are made of cancellous or spongy bone and function as the barrier between each disc and the vertebrae.
The low back/lumbar spine takes the most weight. That can be a significant amount of pressure on the structures in the low back. The endplates are situated between a cushioned disc/s and the hard, bony vertebral body making them vulnerable to degeneration and nerve damage contributing to chronic low back pain. The endplates and vertebral bodies consist of a network of intraosseous nerves.
Intraosseous nerves live within the bone.
The basivertebral nerve� BVN is an intraosseous nerve that winds through the vertebral bodies. This nerve feeds into each spinal bone through the back of the vertebral body and then branches out with nerves going towards the top and bottom vertebral endplates. Research has shown that although these nerves are inside the bone they can send pain signals from a damaged vertebral endplate that could result in vertebrogenic low back pain. This is why it has been�recently linked it as a possible cause of chronic low back pain.
Nerve pain in the spine has been linked with discs that have degenerated. A doctor, chiropractor/spine specialist refers to this as discogenic pain. But with new research, an understanding of the function the vertebral endplates and BVN play in the sensation of pain has been realized and this is where the term vertebrogenic pain comes from. If a doctor discovers that the endplates could be the source of your chronic low back pain, they might use this term.
Vertebral Endplate Pain Diagnosis
Like most back pain conditions diagnosing vertebral endplate pain can be just as challenging. This is because diagnostic imaging scans typically don�t pick up mild to moderate endplate damage. A classification scale known as Modic changes helps doctors identify vertebrogenic pain.
Modic changes or MC are areas that show up on an MRI showing bone marrow damage that has been linked to low back pain. The name comes from the doctor that classified them in 1988, Dr. Michael Modic. Modic changes help doctors and spine specialists see and understand the connection between endplate damage and chronic low back pain.
2 types were identified that show a connection between vertebral endplate damage and chronic low back pain:
Type 1
This type shows a�development� in the vessels of the vertebral body, that includes:
Inflammation
Edema, which is a collection of excess fluid
Endplate changes like a split or crack/s in the endplate
Type 2
This type reveals changes in the bone marrow like fatty deposits that have taken the place of bone marrow.
If the lumbar MRI shows Type 1 or Type 2 MC, a doctor could recommend a conservative treatment plan that could include:
These could be utilized in conjunction with spine specialist care in addressing symptoms and pain. However, if the pain does not ease or reduce with conservative treatment, a doctor could suggest an outpatient procedure.
Candidates for this procedure usually qualify meeting the following:
The individual has struggled with chronic low back pain for at least 6 months
The pain has not reduced/eased up with at least 6 months of conservative care
MRI shows Type 1 or Type 2 Modic changes�that correlate symptoms of vertebrogenic low back pain
The procedure uses fluoroscopy or an x-ray video. A thin tube called a cannula is inserted into a vertebral pedicle. A pedicle is a structure that sticks out from the back of the vertebra. The cannula tunnels its way to the basivertebral nerve. The doctor then runs the Intracept Radiofrequency generator into the path of the nerve and ablates destroys/removes any obstructions in the nerve with the help of the frequency generator. Since it�s a minimally invasive procedure, it can be performed in an outpatient clinic, allowing the patient to go home the same day.
The device/tool used in the procedure is not implanted in the spine. It is removed once the procedure is done.
Expectations as to how long the pain relief will last depends on:
The severity of the condition
Post-physical therapy
Type of work
Diet
Exercise
One study showed the benefits to last up to two years.
If�nonsurgical treatment has not worked for at least six months talk to your doctor about basivertebral nerve ablation for vertebrogenic chronic low back pain. There are risks and benefits both of which should be discussed in depth.
Endplate or Disc and the Root Cause
The intervertebral discs are often the more common cause of low back pain. But they might not be the root cause of spine pain. More research is going on with the role the vertebral endplates play in spine health. As more patients are being diagnosed earlier then better long-term outcomes will follow.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine