Dr. Alex Jimenez, a chiropractor in El Paso, TX, Kenna Vaughn, Truide Torres, and Astrid Ornelas discuss what it is that they do and why they do it. Chiropractic care is a safe and effective, alternative treatment option that focuses on the diagnosis, treatment, and prevention of a variety of health issues associated with the musculoskeletal and nervous system, including neck pain, back pain, low back pain, and sciatica, among other health issues within the scope of chiropractic care. Dr. Alex Jimenez utilizes spinal adjustments and manual manipulations, among other well-known chiropractic care treatment methods and techniques, to help provide pain relief and promote overall health and wellness. Dr. Alex Jimenez, Kenna Vaughn, Truide Torres, and Astrid Ornelas discuss how they patients, from chiropractic care to educating them on diet and lifestyle changes, to help patients achieve their nutrition and fitness goals. According to Dr. Alex Jimenez, Kenna Vaughn, Truide Torres, and Astrid Ornelas, chiropractic care and functional medicine are treatment options that can naturally support well-being. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Reducing stress is important for emotional well being and physical health. Rheumatoid arthritis is a complex condition with no cure and can cause intense chronic pain. Stress only exacerbates the symptoms, affects pain perception, and weakens the body. Stress management is highly important for reducing pain. In a weakened state, an individual is more vulnerable to arthritis symptoms, like flare-ups, weakness, and fatigue.�Chiropractic can help.
There are non-surgical treatments for arthritis, like medications, physical, and massage therapy that address the physical nature of the condition. By eliminating stressful triggers and making healthy behavioral/lifestyle changes a better sense of well being can be achieved.
Different emotions can run rampant:
Confusion
Frustration
Anger
Sadness
Helplessness
And all of these feelings can generate intense stress on an individual. Chiropractic excels in wellness and is becoming more common for individuals to visit chiropractic clinics for treating a variety of different kinds of pain symptoms and conditions. Chiropractic adjustments provide countless benefits to those with arthritis. We�ll explore how chiropractic can help those with arthritis and give additional information along with suggestions on how to alleviate the pain.
What Chiropractic Does
A doctor of chiropractic is a health professional that focuses on wellness and optimal health instead of ailment/sickness symptoms. Their specialty aims at adjusting the spine to correct misalignments that could be pressing down on nerves and causing major disruption in the body. Regular chiropractic not only restores health throughout the body but helps alleviate back pain and any other symptoms associated with an out of alignment spine.
They also work in setting up exercise programs specific to the condition being treated along with the proper diet to utilize in assisting with the management of inflammation and pain.
Arthritis
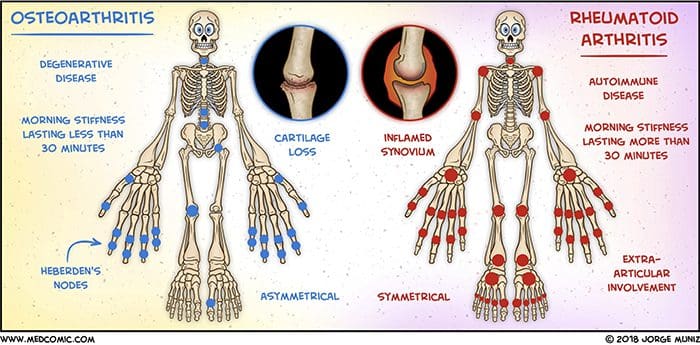
Arthritis is inflammation in the body’s joints which results in pain, stiffness and limited range of movement. There are over 200 different varieties of arthritis. Generally associated with age, it can affect young people. It can strike pretty much any area of the body. Arthritis can cause damage to soft tissues and muscles.
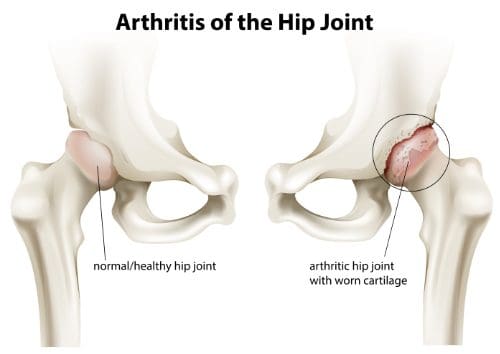
Osteoarthritis also known as degenerative joint disease, is the most common type. It comes from repeated trauma to the joints and occurs more often in the elderly.
Other forms include:
Rheumatoid arthritis is the second common type in which the body�s immune system attacks the joint/s.
Psoriatic arthritis, an autoimmune form of arthritis.
Ankylosing spondylitis is a type of arthritis where the body attacks itself.
Septic arthritis is caused by a viral or bacterial infection of the joint/s.
Diagnosis
Diagnosing arthritis involves a thorough physical examination. Rheumatologists often need help with these cases, and so a medical work-up can be done and a chiropractor could be recommended. This includes X-rays or MRIs, urine, blood analysis, and physical examinations. Having the condition properly diagnosed will help to more effectively treat the symptoms.
Chiropractic
The most common treatment is medication, which takes down the inflammation, the swelling and reduces pain. Chiropractors can be of great help in managing arthritis. Medications work but as we’ve seen they can have long-term health risks like impaired healing, damage to the stomach lining and internal bleeding.
A chiropractor can reduce stress, and reliance on medications, all the while managing the pain and symptoms in a natural way. Chiropractic can:
Improve range of motion
Keeps the spine properly aligned
Improve endurance
Improve flexibility
Increase strength
Increase muscle tone
Develop a dietary and nutritional plan to reduce inflammation
Recommend an exercise regimen conducive to arthritis symptoms
According to the American Chiropractic Association, this is vital in managing arthritis symptoms.
Treatment
Understand that chiropractic cannot cure arthritis. They can help alleviate symptoms, slow the progression and help to reduce stress levels. They will use adjustments in combination with other treatments. This can include:
Hot and cold treatments
Ultrasound treatments
Massage
Electronic muscle stimulation
Physical rehabilitation
Magnet therapy
Reduce Stress
Exercise
Water aerobics or make walking around the park/neighborhood part of a daily routine, as it promotes a healthy mind by reducing stress and anxiety. Gentle exercises like aerobic exercise are perfect because it improves mobility and helps shed a few pounds taking pressure off the joints. Exercise creates endorphins, which reduces pain and uplifts the mood.
Support groups
With any type of painful condition, it’s easy to feel alone. Joining a support group can connect you with people who understand what’s going on and the emotions you’re experiencing. The community helps diminish the sense of isolation.
Relaxation therapy
This focuses on calming the body and mind by making a conscious effort to relax. Even for only a few moments, you might find this technique effective at controlling the stress response. Begin by focusing on one part of the body like the hands, feet, etc.
Concentrate until the area you’re focusing on is completely free of stress or tension. Then imagine weightlessness flow through the body. Close your eyes, lie down, turn off the lights, and think of something soothing. There are no strict guidelines for relaxation. Whatever puts you in a relaxed frame of mind is the way to do it.
Warm bath
Warm moist heat from a shower, bath, or steam room can decrease the secretion of stress hormones and raise levels of endorphins, as aforementioned the body’s natural pain killers.
Take time for yourself
When it comes to reducing stress, balance is key. Staying active, and regular rest/sleep is vital to successful treatment. A balance needs to be in everything you do. Therefore, make time for the things you want to do.
Results
Inflammatory diseases like arthritis have shown the best results are achieved from combating it from all angles. Working with a chiropractor and rheumatologist to combine treatments can make all the difference. A healthy diet and active exercise program will get you in the right direction toward a healthy active lifestyle. If you or a loved one are suffering from arthritis, don�t hesitate to call. We�re here to help in any way possible!
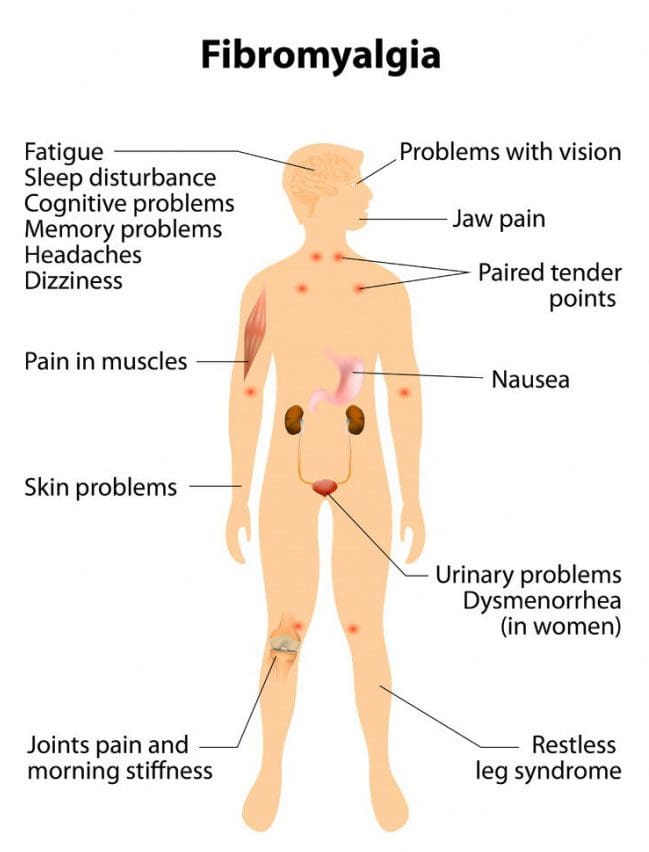
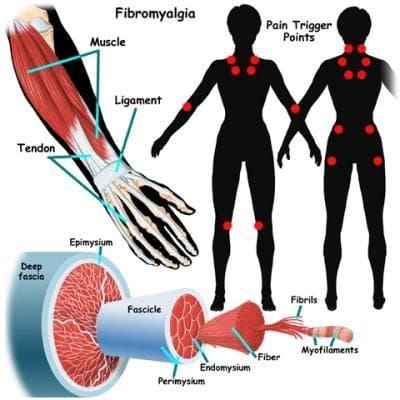
Fibromyalgia is a chronic pain disorder affecting millions and mostly women. It is physically and emotionally distressing. Those with the condition experience widespread chronic muscle pain. Research has shown that individuals with fibromyalgia could have a lower threshold for pain. This can come from injury, emotional distress, or abnormal levels of substances/chemicals in the brain and spine linked to pain sensitivity. One of the most common treatments is chiropractic medicine.
Common symptoms/conditions individuals report:
Chronic fatigue syndrome
Irritable bladder
Irritable bowel syndrome
Migraines
Sleep disorders
Restless legs syndrome
TMJ or Temporomandibular joint disorder
Raynaud’s Syndrome�-�a�rare blood vessel disorder causing the toes and hands to feel cold or numb.
Doctors are still trying to figure out the relationship between these conditions and fibromyalgia.
Causes
Doctors have yet to determine the exact cause, however, research is ongoing and beginning to shed light on the condition. Some possible causes include:
Abnormalities in the endocrine system
Abnormalities in the autonomic nervous system
Genetics
Muscle tissue abnormalities
Abnormal blood flow
As research has discovered many conditions/disorders do not have one cause but rather, several factors that impact the probability of developing the condition.
Questions
It has become one of the most common chronic pain conditions. 1 in 50 Americans are dealing with fibromyalgia. The condition can be difficult to diagnose, and, because of its chronic nature, it can linger for months and even years. Typically it causes pain throughout the body and creates areas that become tender to the slightest touch. There are both traditional and alternative treatments available.
Traditional approaches to manage the pain:
Anti-inflammatory’s
Over-the-counter pain relievers
Sleep medications
Muscle relaxants
Fibromyalgia medications include:
Lyrica – pregabalin, which is a nerve pain medication
Cymbalta – duloxetine hydrochloride, which is an antidepressant that can also help manage pain
Savella – milnacipran HCI, which is an antidepressant and nerve pain medicine
The type of treatment depends on the symptoms. For example, a doctor could prescribe an antidepressant to reduce pain and depression. If stress, anxiety, and trouble sleeping are presenting,�a therapeutic exercise program could be the answer. Individuals prefer natural remedies/therapies instead of more medications like vitamin therapy, acupuncture, and meditation.
Other treatment options include alternative treatments like:
The most common issue is constant and consistent pain, which can affect the entire body for weeks and even months. Individuals realize that chiropractic helps restore overall health and aids the body to heal itself. Adjustments to the spine bring alignment and balance back to the body. Also incorporated is soft tissue work that can relieve and reduce painful pressure/trigger points and decrease pain in tender spots.
Range of motion is increased
Chiropractic medicine also adjusts the body’s joints and helps loosen them up. This increases the range of motion and allows the individual to move more freely and easily. Depending on how long the individual has been dealing with the condition, it can take a few treatments to achieve optimal results, so it does take a commitment from the individual patient. However, in the long run, it is well worth the time.
Sleep is improved
The pain associated with fibromyalgia often affects an individual’s ability to sleep well. Being unable to sleep normally will leave you exhausted, foggy, unable to accomplish things and irritable to downright angry. A chiropractor’s ability to loosen the body’s joints, massage tender points, and kickstart the body’s self-healing mechanisms means individuals with this condition can enjoy deep sleep, and stay asleep.
Complements other therapies
Medicines/treatments/therapies can counteract with each other, or get mixed up and cause side effects. Chiropractic medicine can be utilized in combination with medications/treatments, either traditional or natural. Individuals diagnosed with this condition should speak to their chiropractor about the different treatments available. Customized treatment programs are created case-by-case and are tailored to the specific needs of that individual. Remember there is not a one-stop solution.
Empowers the individual
Individuals that have to deal with painful, chronic conditions can exhaust themselves with the varying treatment options and can feel as if they have no control over the situation. This causes stress, anxiety, and depression, which works against achieving overall wellness. With chiropractic, individuals are more in charge of their treatment plan, which leads to an optimistic outlook in their recovery.�
Chiropractic medicine treats not only the symptoms of fibromyalgia but attempts to get to the root cause to alleviate the condition or to activate the body’s self-healing response. Patients that commit will see the benefits along with reduced pain, better mobility, and sound sleep.
The best benefit is being able to take control of the circumstances and playing a vital role in the managing of an individual’s well-being. Understand that there are options available for fibromyalgia pain management. If you or a loved one has been diagnosed with fibromyalgia, don�t go it alone. Dr. Alex Jimenez is passionate about helping those who are injured or struggling with a condition get relief. Contact us today to schedule an appointment.
We are familiar with neck stiffness or a crick. This can prevent us from comfortably moving the head all around. A crick can cause the spine, and shoulders to feel rigid and stressed from not being able to turn around and could cause an upper or low-back strain from having to turn the whole body to look back or even just to the side. Chiropractic treatment is available and will help, along with some self-care therapies that can be done at home.
Crick in the Neck vs. Neck Stiffness
A crick in the neck is the same as a stiff neck. It develops when the neck muscles, tendons, and ligaments become strained/sprained. Most strains and sprains are minor but do cause inflammation/swelling of the neck�s soft tissues, which results in stiffness and, at times muscle spasms.
The symptoms
Cricks in the neck are uncomfortable, but not necessarily painful. If there is a pre-existing neck condition or injuries like whiplash the crick and stiffness could increase the uncomfortableness and generate pain.
The most common symptoms include:
Neck stiffness
Muscle stiffness
Reduced mobility affecting the neck�s range of motion
A popping sensation when trying to turn or tilt the head
Causes of a stiff neck or crick
There are different causes of neck stiffness. It can be a combination of things you can control and some you can�t.
Possible causes that you can control:
Poor posture working either sitting or standing for several hours without breaks or stretching.
Sleeping in a position that puts the neck in an awkward position or using a pillow that does not support the neck when sleeping.
Constantly looking down at a cell phone or tablet.
Stress and emotional tension can cause involuntarily tightening of the neck muscles and shoulders.
Heavy labor along with incorrect lifting techniques.
Reaching or having to look up/overhead for several hours like when painting a ceiling.
Possible causes that are out of your control:
Whiplash injury
Sports-injuries like a football stinger
Aging muscles and bones
Around 13% of cases the stiffness, and pain are caused by separate cervical spinal conditions, like:
Cold therapy reduces the swelling of soft tissues, like muscles and ligaments, while heat soothes the tightness by boosting blood circulation to the affected area. There are different products available that can deliver cold or heat to the neck and upper back.
Apply ice for 15 minutes each hour.
Apply heat therapy like a heating pad for 15 minutes every 2 or 3 hours.
Over-the-counter anti-inflammation medicines
Non-steroidal anti-inflammatory medications like ibuprofen and naproxen can help relieve inflammation and pain.
Because neck stiffness can be linked to lifestyle choices, individuals may find that they occur repeatedly. Simple neck stretches, chiropractic treatment, using a supportive pillow, and taking frequent breaks at your job can help prevent neck stiffness and keep you moving. These professionals have undergone extensive training in their field and are capable of treating neck pain effectively. So if you or a loved one are experiencing neck pain, give us a call. We�re ready to help!
In the following podcast video article, Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Dr. Mario Ruja, another chiropractor in El Paso, TX, discuss chiropractic care and why it works. Chiropractic care is a safe and effective, alternative treatment option that focuses on the diagnosis, treatment, and prevention, of injuries and underlying conditions associated with the musculoskeletal and nervous system. Chiropractic care is a healthcare profession that has existed for many years throughout many civilizations and it focuses on the use of spinal adjustments and manual manipulations to carefully restore the original alignment of the spine and the human body as a whole. Dr. Alex Jimenez and Dr. Mario Ruja describe how they were first interested in becoming chiropractors, or doctors of chiropractic, as they also describe how they feel when they are able to provide pain relief to their patients. Dr. Jimenez and Dr. Ruja will focus on discussing why chiropractic care works and how it is different from other healthcare professions in the way it helps treat a variety of health issues associated with the spine, from neck pain to low back pain and sciatica. Chiropractic care can help promote overall health and wellness. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Dr. Alex Jimenez and Dr. Mario Ruja discuss basal metabolic rate, BMI, and BIA. Body mass and body fat can be measured in a variety of ways, however, several measurement tools may ultimately be inaccurate for many athletes. According to Dr. Alex Jimenez and Dr. Mario Ruja, calculating an individual�s body mass and body fat utilizing various tools is essential to determine overall health and wellness. BMI uses a person�s height divided by twice their weight. The results may be inaccurate for athletes because their body mass and body fat is different, in terms of weight, compared to the average person. Dr. Alex Jimenez and Dr. Mario Ruja demonstrate that BIA, or bioelectrical impedance analysis, and various other tools, such as the DEXA test, the Tanita scale, and the InBody, among others, can help more accurately determine an athlete�s body mass and body fat. Basal metabolic rate, BMI, and BIA is essential for parents that have young athletes as well as for the general population. Healthcare professionals that have these tools available can ultimately help provide individuals with the results they may need to maintain overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Dr. Alex Jimenez, a chiropractor in El Paso, TX, and his staff, health coach Kenna Vaughn, and chief editor Astrid Ornelas, discuss the role of inflammation in metabolic syndrome. The following podcast offers a deeper look at understanding how inflammation can ultimately cause metabolic syndrome. Metabolic syndrome is a collection of risk factors that can increase the risk of developing a variety of health issues, including diabetes, stroke, and heart disease. The risk factors associated with metabolic syndrome can also include, waist fat, high blood pressure, high blood sugar or glucose, high triglycerides, and low HDL or good cholesterol levels. Inflammation is the immune system’s natural response against injury, infection, and environmental toxins. Although inflammation is necessary, too much of it can ultimately cause a variety of health issues, including metabolic syndrome. Dr. Alex Jimenez, Kenna Vaughn, and Astrid Ornelas discuss how nutrition, diet, and fitness, as well as getting good sleep, can help regulate inflammation to prevent further health issues. Smoothies are also a good way to add extra nutrients. Dr. Alex Jimenez, Kenna Vaughn, Astrid Ornelas, discuss what type of foods, nutraceuticals, and supplements, you can eat, drink, and take to regulate inflammation and promote overall health and wellness to prevent health issues like metabolic syndrome, among others. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine