Individuals experiencing radiculopathy in and around the neck notice it immediately often driving them to the medicine cabinet. This condition presents with:
Acute pain
Numbness
Muscle spasms
However, medication will only help relieve the pain temporarily but it won’t alleviate what is causing the radiculopathy. This is because pain medication/s can exacerbate the condition by blocking the pain signals with the root nerve issue never being resolved. Chiropractic is a complete solution that specifically mobilizes the cervical joints where nerve impingement is happening. The objective is to help individuals understand the underlying cause of the acute pain induced by radiculopathy and provide long-term pain relief through cervical joint mobilization.
Radiculopathy Pain
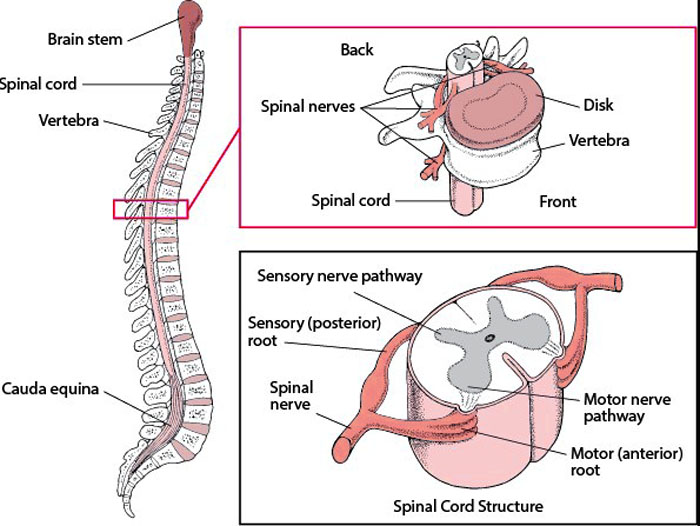
To determine what cervical nerve bundles are being affected by a subluxation or vertebral compression a chiropractor needs to isolate the pain. This is accomplished through a description of symptoms, radiological imaging to provide visual confirmation, and an examination of the affected area. Isolating the pain allows the chiropractor to determine the extent of misalignment and how much the nerve is being compressed. This will help in the development of a customized treatment plan. A chiropractor will be able to see and feel the degree of pressure being placed on the nerve or bundle of nerves.
Mobilizing The Cervical Joints
Chiropractors approach this directly based on the individual and the severity of the case. The most common joint mobilizations include:
Low-impact adjusting will shift the misaligned vertebrae back into place
Adjustments to the opposite non-painful area will help counterbalance stress in the spine
Radiculopathy improvement consists of:
The cervical spine is stabilized through bracing and posture supports
Isometric exercises will recondition the neck, shoulders, and upper back
Range of motion exercises will prevent any subtle compression/s
Corrective restoration of the cervical spine’s curve
The spine returns to normal during cervical joint mobilization and alleviates radiculopathy immediately and long term.
Proper chiropractic care will correct the affected nerve bundle, and stabilize the cervical spine to prevent/resist:
Compression
Translation
Subluxation
Other shifts that can occur
Chiropractic Mobilization Long Term Relief
A pinched nerve should not be treated with over-the-counter medications for long-term health. Corrective chiropractic mobilization is a recommended course of action for alleviating this and other musculoskeletal conditions. Chiropractic understands the nature and severity of radiculopathy as well as developing the proper customized treatment plan that will bring optimal results.
Body Composition
DASH Diet Example
Breakfast
3/4 cup bran flakes cereal with 1 banana and 1 cup low-fat milk
1 slice whole-wheat bread with 1 tsp. unsalted butter
1 orange
1 cup coffee
Lunch
Sandwich 2 slices of whole-wheat bread
3 oz. grilled thin chicken breast
2 slices low-fat cheese
1 tbsp. mustard
Salad
1/2 cup chopped/diced cucumbers
1/2 cup chopped/diced tomatoes
1 tablespoon sunflower seeds
1 teaspoon low-calorie non-cream dressing
1/2 cup fruit cocktail with no sugar
Snack
1/3 cup unsalted almonds
Dinner
3 oz. lean beef with 2 tbsp. fat-free, low sodium gravy
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
Evid Based Complement Alternat Med. 2015. Complementary and Alternative Medicine for the Management of Cervical Radiculopathy: An Overview of Systematic Reviews. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4541004/
Eating healthy and spinal health are interconnected. Eating healthier will help to lose weight, and provide a healthier body mass index. This means more muscle mass, especially when integrated with more protein. The spine sustains and supports the whole torso and upper body. When weight increases in these areas it can cause an array of issues like subluxations, curvature problems, sciatica, and more. The extra muscle mass takes the added stress from any extra weight off of the spine. Strong muscles can carry the weight of the body, taking the pressure off the spine and keeping it healthy and operating in top form.
Making Healthy Adjustments
No matter where an individual is on their healthy eating plan, there are common practices that work for many and helps improve their diet. This involves integrating healthy food groups into the diet in different ways, and not giving up when mistakes are made, but learning from them. When developing new healthy habits it takes time, diligence, practice, and research to eat the right foods.
Fruits and Veggies
It is easier and tastier to forget the nutritious foods and go for the carbs, fats, etc. Rather than trying to add more vegetables, or eating fruit as a snack every day can be tough. An easier, and better way to integrate fruits and vegetables into one’s diet is to substitute the carbs and fats for fruits and veggies in the main meals every day.
This could be spiralized zucchini, squash, or no-carb spaghetti instead of pasta spaghetti.
Instead of ice cream try real fruit sorbet.
Mashed cauliflower instead of white rice or mashed potatoes.
There are plenty of substitutes that are healthier and just as tasty and as the real thing.
Healthy recipes out there that can give you ideas on how to do this.
The benefit of substituting fruits and vegetables, rather than just adding them to a diet is individuals increase their health by reducing unhealthy dietary elements and adding healthy new ones at the same time. However, this does not mean doing it all at once. The goal is to gradually substitute these nutritious foods into everyday dishes for maximum health benefits.
More Fiber and Protein
It is important that the body gets enough fiber and protein as a healthy energy source. Many individuals can become dependent on:
Ingesting unhealthy foods all day every day takes a significant toll on the body. This includes:
Blood sugar
Weight
Energy
Mood
Fiber and protein are important because the two regulate the body’s systems to promote healthy bodily functions.Fiber helps the digestive system and regulates carbohydrate breakdown. This means the energy obtained from any carb will last longer and will not increase blood sugar when integrated with fiber. Most individuals know that protein builds muscle. But it also makes the body feel full much longer than carbs or sugars do. This allows for natural regulation of how much is eaten during the day so an individual does not eat more than the body needs. Carbs and sugars are not filling and can become addictive. This means that they can be eaten all day long without feeling full and just load up with empty calories. A few ways to integrate fiber and protein into a diet:
Breakfast
Eggs
Turkey bacon
Whole wheat/multigrain toast
Lunch
Whole wheat wrap or sandwich
Dinner
Brown rice and beans are loaded with protein and fiber.
A great substitution for vegetarians/vegans for more protein or fiber
Reduce Sugar Intake
Reducing sugar intake or switching to balanced sugars from fruits, yogurt, etc. A diet high in sugar can wreck the body, causing:
Weight gain
Mood swings
Overeating
Other unhealthy effects
Sugar is fine when practiced in moderation. But when it becomes a daily habit, that’s when it can start affecting the body. The objective is to drink more water, and use substitutions when cravings present. Try:
Yogurt instead of ice cream
Healthy fruit drinks instead of soda
Tea instead of wine
Keep the indulgences to once or twice a week if possible.
Eating Healthy Benefits
A few of the benefits from eating healthy that will improve quality of life:
Improved digestive health
Weight loss
Reduced to no back pain
Reduced to no foot pain
Healthy sleep patterns
Less fatigue
Improved focus
Improved brain health
Clear skin
Reduced to no irritability
Body Composition
New Health Issues
Steady weight gain throughout life can lead to adult diabetes. This is brought on by more body fat and muscle loss. Loss of skeletal muscle mass is linked to insulin resistance. The less muscle is available, the less insulin sensitive the body becomes. Loss of muscle can cause other problems with age. One damaging condition, especially for women, is osteoporosis. This happens when old bone is reabsorbed rather than new bone being created. Both men and women can have decreased muscle mass with thinner, weaker bones. This increases the risk of osteoporosis and the risk of serious injury from falls. Prevention includes
Eat sufficient protein throughout the day. It is often best to space out protein intake across meals and not consume all at once to ensure the proper amount is being met daily. Regular body composition monitoring can help. The goal is to minimize muscle mass loss and fat mass gain as the body ages.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Cena, Hellas, and Philip C Calder. “Defining a Healthy Diet: Evidence for The Role of Contemporary Dietary Patterns in Health and Disease.” Nutrients vol. 12,2 334. 27 Jan. 2020, doi:10.3390/nu12020334
Locke, Amy et al. “Diets for Health: Goals and Guidelines.” American family physician vol. 97,11 (2018): 721-728.
Warensjö Lemming, Eva, and Liisa Byberg. “Is a Healthy Diet Also Suitable for the Prevention of Fragility Fractures?.” Nutrients vol. 12,9 2642. 30 Aug. 2020, doi:10.3390/nu12092642
Brain fog, memory problems, concentration, and the inability to form clear thoughts is an issue that many will face at some point. The progression of losing the ability to focus or think clearly can lead to decreased productivity with normal daily tasks, work, or taking care of a household. It can be a short-term issue experience caused by sleep deprivation or stress. However, if these issues are allowed to continue it can negatively change an individual’s quality of life.
Affected Productivity Factors
Causes that can lead to poor productivity include:
The underlying issue/s associated with brain function and the ability to focus are connected to the spine being out of alignment. Individuals often have poor spinal alignment without even realizing it is happening. It affects the body’s blood and nerve transmitting abilities to complete normal daily tasks. Chiropractic treatment is an expert-based approach that focuses on restoring spinal alignment to increase an individual’s health and brain function. Proper spinal alignment allows the nerves to relay messages clearly and optimally through the spinal cord to the brain. This allows for:
Clear thinking
Improved memory
Better decision making
Staying focused on tasks
Chiropractic Optimal Nerve Flow
When the central nervous system/brain/spinal cord is not transmitting properly it can lead to significant issues with concentration and productivity. When nerve energy and brain function is optimized productivity is improved. Research has shown that chiropractic can help:
Reduce the risk of disease
Prevent injuries
Prevent pain conditions
Improved quality of life
Chiropractic medicine can increase the ability to focus, optimize brain health, and more.
Body Composition
Tracing the sources of fatigue
There is a difference between being tired periodically from a long day and being tired daily. Being tired daily is also known as Chronic Fatigue Syndrome. This is a fatigue condition that has lasted longer than 6 months. It is typical to experience many of the symptoms of fatigue that disrupt the ability to achieve health goals like:
Weight loss
Muscle gain
Maintaining body weight
Symptoms include:
Constantly tired
Reduced appetite
Moodiness
Reaction time slows down
Memory Loss
Dizziness
The nature of hectic daily schedules can allow sources of fatigue to pile up. The objective is to find a balance between home, work, physical activity, diet, etc. Chiropractic medicine and health coaching can help develop an optimal plan to get healthy.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Craniocervical Junction Disorder. USC Spine Center Web site. http://spine.keckmedicine.org/treatments-services/craniocervical-junction-disorder/. Accessed August 25, 2017.
Anderson, Brian, and Adam Pitsinger. “Improvement in chronic muscle fasciculations with dietary change: a suspected case of gluten neuropathy.” Journal of chiropractic medicine vol. 13,3 (2014): 188-91. doi:10.1016/j.jcm.2014.01.002
Ross, Amanda J, et al. “What is brain fog? An evaluation of the symptom in postural tachycardia syndrome.” Clinical autonomic research: official journal of the Clinical Autonomic Research Society vol. 23,6 (2013): 305-11. doi:10.1007/s10286-013-0212-z
When a machine isn’t working correctly because the mechanism’s parts have slipped, shifted, become loose, and are on the verge of breaking down, an expert/professional is called in to repair the damaged parts. The same can be said of the spine. From all the movement at home, work, shopping, activities the spine also compresses and falls out of place becoming misaligned. That’s when individuals need to call a chiropractor to repair/realign the spine. The spine is an integral component of the body’s functionality and health. This includes:
For the spine to operate at its best proper alignment is necessary. The spine is impacted by everyday activities that shift, jolt, bounce, and stress the spine. Exacerbating the regular wear and tear includes:
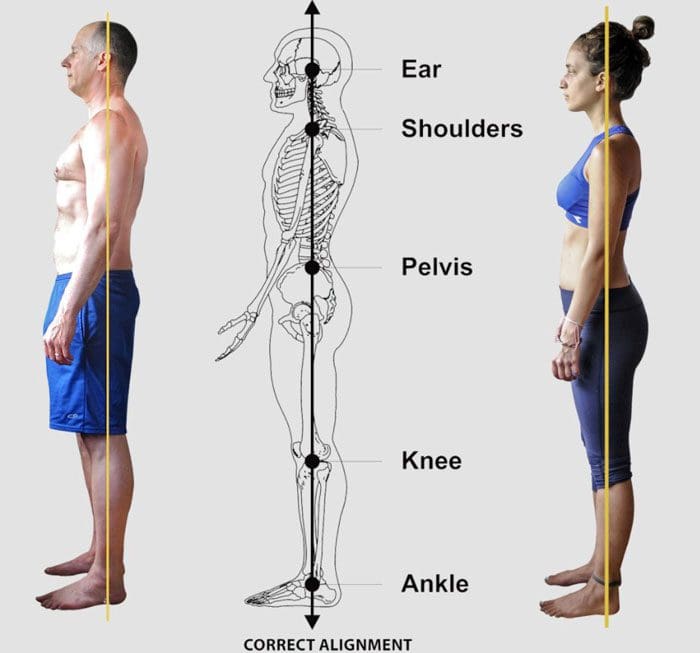
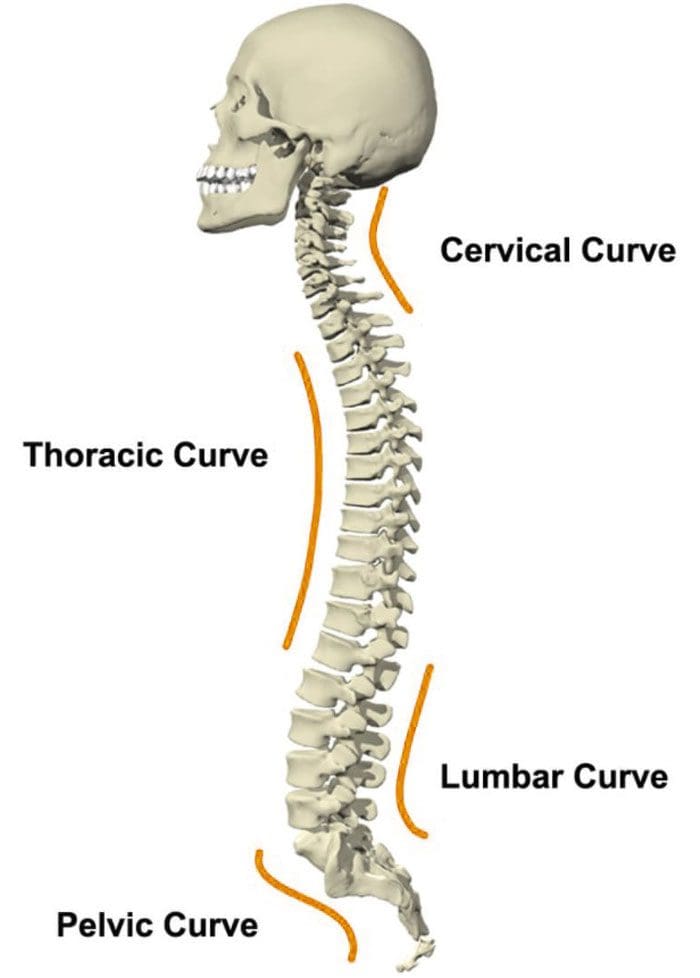
The head, shoulders, and spinal curves align from the side in general creating an S shape
Every individual’s spine varies significantly. This is why a professional chiropractic examination, diagnosis, and customized treatment plan will maximize spinal alignment and overall health.
Chiropractors are the Expert Repair Specialists
Chiropractors are specially trained at spotting spinal misalignment/s and repair. This is done non-invasively through manual adjustments and mobilization techniques. When the spine is in optimal alignment it will prevent and activate the body’s natural healing abilities. Once spinal alignment is achieved the chiropractor can help maintain proper alignment with exercise, health coaching, lifestyle adjustments, and nutrition to maximize individual health.
Body Composition
A partner, spouse, friend, co-worker, professional for maintaining health
Finding someone to share the highs and lows during an individual’s health journey will significantly help relieve stress and continue to be motivated. It can be a spouse, best friend, coworker, or licensed professional. When an individual vocalizes their thoughts and feelings, they gain confidence in their ability to handle whatever comes their way. This is an individual that will help navigate the negative emotions by listening and providing advice and encouragement.Take some time every week to share successes, failures, goals, etc. Whatever comes to mind to just get it out there so it can be evaluated and broken down into manageable parts. The great thing about sharing is that it can inspire positive changes.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Diebo, Bassel G et al. “Sagittal alignment of the spine: What do you need to know?.” Clinical neurology and neurosurgery vol. 139 (2015): 295-301. doi:10.1016/j.clineuro.2015.10.024
Caprara, Sebastiano et al. “Spinal sagittal alignment goals based on statistical modeling and musculoskeletal simulations.” Journal of biomechanics vol. 102 (2020): 109621. doi:10.1016/j.jbiomech.2020.109621
Senzon, Simon A. “The Chiropractic Vertebral Subluxation Part 10: Integrative and Critical Literature From 1996 and 1997.” Journal of chiropractic humanities vol. 25 146-168. 6 Apr. 2019, doi:10.1016/j.echu.2018.10.008
Rheumatoid arthritis is said to affect around 1.5 million individuals. Recognized as an autoimmune condition that presents with chronic pain in the body’s joints. It commonly affects regularly used joints like the shoulders, hands, and feet. The condition can begin to present in individuals in their 30s. Concerns that come with a rheumatoid arthritis diagnosis are the condition’s effect on the spinal facet joints. These joints are susceptible to attack from a dysfunctional immune system, leaving them prone to weakness, inflammation, and nerve compression. Chiropractors understand the manifestation of rheumatoid arthritis. They can pinpoint at-risk facet joints and provide corrective relief before more dangerous symptoms begin to present.
Facet joint risks
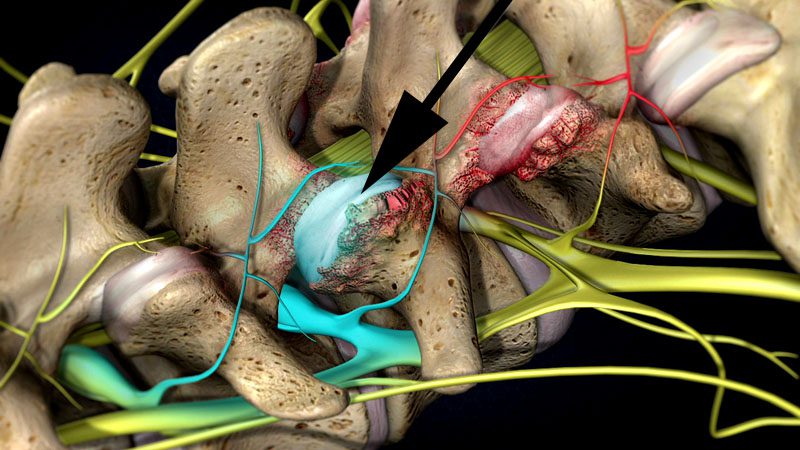
There are two facet joints that connect each vertebra to the one above and below. Their objective is to stabilize the spine, whether in a neutral position or engaged in flexion/extension movement. When targeted by the body’s immune system, the joints begin to weaken. The body attacks the synovial fluid that lubricates the joints. This creates friction that generates inflammation. Over time the joints break down leading to everything from loss of mobility to bone spurs. When left untreated the facet joints begin to deteriorate, causing nerve compression that can lead to permanent nerve damage. When the joints are not working properly the spine has to work around them.
Subluxations
Disc herniation
Ruptured discs
Sciatica all are possible with facet joint dysfunction.
Treatment
Currently, rheumatoid arthritis cannot be cured but symptoms can go into remission when treatment begins early.Chiropractic is an effective treatment at disrupting the symptoms of joint deterioration that stops the progression.
It has the ability to increase and maintain an individual’s range of motion, from a condition that causes loss of mobility.
It helps to bring rapid pain relief and helps with postural improvements.
It maintains positive spinal health and homeostasis.
Prevents problems with compression and subluxations.
Stretching and strengthening exercises are incorporated to preserve an individual’s spinal integrity.
Diet and nutrition are also adjusted to mitigate the effects, helping with inflammation prevention.
The spinal focus
As rheumatoid arthritis affects the body’s joints, it is vital to protect the facet joints. These joints can experience degenerative damage that can cause long-term problems. Injury Medical Chiropractic and Functional Medicine Clinic provide individuals with the tools necessary to combat rheumatoid arthritis that medications by themselves might not be able to.
Body Composition
Muscle Mass Fitness for Long-Term Health
Muscle building is not just for bodybuilders and athletes. Everyone benefits from building muscle for long-term health. Monitoring the changes in Lean Body Mass can be accomplished by having body composition measured. Body composition analysis can divide an individual’s weight into various components. These include:
Fat Mass
Lean Body Mass
Basal Metabolic Rate will give a clearer picture of overall fitness and health.
Building Lean Body Mass is an investment for maintaining health long-term. The more Lean Body Mass that is built the more is in storage/reserve when the body really needs it. Before adding protein shakes and resistance workouts to the daily regimen, a plan needs to be developed. The first step to building a healthy level of lean body mass is to measure how much there is with a body composition analysis.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Pope JE, Cheng J. Facet (Zygapophyseal) Intraarticular Joint Injections: Cervical, Lumbar, and Thoracic. Injections for Back Pain. 129-135. ClinicalKey.com. Accessed July 16, 2019.
Brummett CM, Cohen SP. Pathogenesis, Diagnosis, and Treatment of Zygapophyseal (Facet) Joint Pain. 816-844. ClinicalKey.com. Accessed July 16, 2019.
Chiropractic treatment and physical therapy are treatment methods/approaches that are conservative, non-invasive, and are both practical options. Both address health concerns, like various types of pain, automobile, work, sports, and personal injuries. Both are focused on helping individuals achieve long-term results and maintain health.
Chiropractic and physical therapy are usually done in combination, as they complement one another. There are benefits and similarities between the two treatment options. Here are some general guidelines to decide which treatment option is best for your needs.
Primary symptoms
Chiropractors are known for the ability to provide quick relief to individuals dealing with pain and stiffness in the joints, particularly the spine. They are experts in spinal realignment and proper posture. If flexibility is limited or the joints are locking up, a chiropractor is the recommended choice.
Physical therapists or PTs are the experts in body biomechanics and soft tissue injuries. If an individual finds themselves moving differently because of pain or injury, training and exercise will help movement and maximum recovery.
Treatment style
Chiropractors follow a meticulous expert-based protocol for achieving the best results. They provide a hands-on approach to treatment that requires regular follow-ups and maintenance. This is an approach that some individuals prefer. Physical therapy treatment/rehabilitation programs are typically short-term. The average treatment usually lasts only 12 weeks. A physical therapist’s primary objective is to provide a fundamental understanding of how to move properly and self-manage symptoms for the long term. This usually includes a balanced exercise program.
Insurance coverage
Insurance plans vary in what is covered. The first step is to see what an individual’s insurance will cover. Benefits can be found online or by calling a representative to see how to get the care/treatment needed. Most plans cover some form of physical therapy. Chiropractic is also usually covered by insurance providers. Skipping the insurance can also be done with chiropractic clinics providing affordable options.
Options
There is no clear-cut answer as to which to see. A physical therapist or chiropractor. Individuals should follow a doctor’s recommendations as to which treatment type would benefit them. If no recommendations have been given then take a look at a clinic’s website to see what they are about. Fortunately, many chiropractic clinics include physical therapists as part of their medical team. Both chiropractic and physical therapists provide dynamic benefits for increasing and maintaining overall health.
Body Composition
Hydration Guidelines
Drink according to thirst
The body knows when it needs water. Therefore drink when you are thirsty, not before. An adequate fluid intake should be timed according to feelings of thirst.
Estimate hourly sweat loss
Those that exercise or engage in regular physical activities for prolonged periods should weigh themselves before engaging in the exercise/activity. Then drink according to thirst as the event goes on, then weigh yourself after the activity. The goal is to maintain the same weight or be slightly less. If an individual weighs more than what they drank, then they drank too much.
Excess water consumption
If an individual is not thirsty, the recommendation is to not drink water in excess. Nausea and even vomiting could ensue. A simple indicator to determine if enough water is being consumed is to check urine color. If it is colorless or slightly yellow then an individual is drinking enough water.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
American Association of Physical Therapists. www.apta.org
Cherkin, D C et al. “A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain.” The New England journal of medicine vol. 339,15 (1998): 1021-9. doi:10.1056/NEJM199810083391502
Fritz, Julie M. “Physical therapy in a value-based healthcare world.” The Journal of orthopaedic and sports physical therapy vol. 42,1 (2012): 1-2. doi:10.2519/jospt.2012.0101
Shrier I. Does stretching help prevent injuries? Evidence-based Sports Medicine. Williston, VT: BMJ Books; 2002.
Individuals tend to think of chiropractic treatment for pain relief, injury recovery, and help with poor posture. This is correct, but regular chiropractic spinal adjustments can provide numerous benefits to feel your absolute best and improve an individual’s quality of life. Doctors of chiropractic/DCs perform a thorough physical and neurological evaluation of the individual to diagnose the root cause of spine pain. The proper diagnosis is essential to the individual’s customized treatment plan.
Benefits of Regular Chiropractic Spinal Adjustments
Chiropractic spinal adjustments address a variety of health-related issues. A chiropractor will work with the individual to determine the most beneficial treatment possible. This includes posture training, exercise, stretching, massage therapy, and more. Below are a few of the benefits of chiropractic spinal adjustments:
Better joint health and mobility
Enhances physical and athletic abilities
Restores muscle balance which is secondary to alignment and loosens/releases tight muscles and resets loose/misaligned muscles
Risk of spine and other conditions is reduced
The body’s natural healing potential is increased along with blood and nerve circulation
Organ function is improved
Sense of well-being increases through:
Symptom management of depression, anxiety, and hyperactivity symptoms
Overall Energy is increased
Sleep improves from the realignment and tension release
Brain fog clears up along with improved concentration
Body’s immune response increases
From the reset blood and nerve circulation, the immune system’s response time improves
This helps prevents the onset of disease and illness
Symptoms of pain are alleviated
Chronic pain conditions are avoided
Highly beneficial for prenatal care
Reduces body discomfort
Helps maintain a healthy posture
Prepares the body for labor
Doctors of Chiropractic
Chiropractors are trained in musculoskeletal treatment and dedicated to providing the best possible. Spinal misalignment is often at the root of body dysfunction and poor health. Contact Injury Medical Chiropractic and Functional Medicine Clinic today with your health goals and see how we can help achieve them.
Body Composition
Complex Carbs Help Build Muscle
Carbs help regulate muscle glycogen repletion. Glycogen is a form of glucose that gets stored for later use. When the body needs energy, the glycogen activates and is ready as a fuel source. Carbohydrates are stored as glycogen. When the body’s carbohydrates are low, glycogen stores are low. When carbohydrates are taken in the glycogen stores are refilled. Because glycogen is used for energy the replenishment of those stores is important. This is why it is recommended to take in carbs immediately after exercising/physical activity. This replenishes glycogen stores for later.
Carbohydrates prevent muscle degradation
Low-carb diets and muscle loss. A study compared a low-carb diet to other diets and found the restriction of carbs resulted in protein loss. Restricting carbohydrates causes an increase in the amount of nitrogen that gets excreted. Nitrogen is a component of amino acids that forms muscle proteins. Loss of nitrogen indicates the muscles are breaking down.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Dubinsky RM, Miyasaki J.Assessment: Efficacy of transcutaneous electric nerve stimulation in the treatment of pain in neurologic disorders (an evidence-based review). Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2010;74:173-176.
Fritz JM, Lindsay W, Matheson JW, Brennan GP, Hunter SJ, Moffit SD, et al. Is there a subgroup of patients with low back pain likely to benefit from mechanical traction? Results of a randomized clinical trial and subgrouping analysis. Spine. 2007 Dec 15;32(26):E793-800.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine