Avoiding Common Christmas Accidents: Prevention and Recovery at El Paso Back Clinic®
After lying in an awkward position, the woman is suffering from back pain on the couch at home.
The Christmas season fills homes with lights, laughter, and loved ones. But it can also bring unexpected risks. From slips on icy paths to burns in the kitchen, holiday accidents happen more often than you might think. In El Paso, Texas, where winter weather can mix with the festive rush, these issues send many seeking help. Distracted or drunk driving spikes too, making roads risky. At El Paso Back Clinic®, we focus on wellness chiropractic care to help you prevent and heal from these mishaps. This article explains common Christmas accidents, their causes, and tips for prevention. It also shows how our integrative approach, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, offers holistic recovery. Using spinal adjustments, massage, nutritional guidance, and NP-partnered care, we support your body’s natural healing to help you have a pain-free holiday.
Common Christmas Holiday Accidents at El Paso Back Clinic®
At our clinic in El Paso, TX, we see a rise in holiday-related injuries each year. These range from home mishaps to road incidents. Here’s a list of the most common ones we treat.
Falls: Decorating ladders or icy El Paso sidewalks leads to slips. These cause sprains, fractures, or head trauma. Nationwide, about 160 decorating falls occur daily, accounting for half of decorating injuries. Kids might tumble from unstable trees or during outdoor fun.
Fires: Faulty lights, dry trees, or candles spark fires. In homes across Texas, Christmas tree fires average 155 per year, causing injuries and property damage. We advise checking decorations to avoid these dangers.
Burns: Holiday cooking with hot oil or deep fryers can result in scalds. Touching lit decorations adds risk. Turkey fryers alone cause 5 deaths and 60 injuries annually. Even hot foods like fried treats can burn mouths.
Cuts: Knife slips while wrapping or carving happen often. Broken glass ornaments or toy packaging lead to ER visits – about 6,000 yearly for gift-opening cuts.
Strains: Lifting decorations, gifts, or snow strains muscles. Back issues account for 15% of holiday accidents, and 11,500 ER visits are due to shoveling. In El Paso, our patients often come in after heavy lifting.
Alcohol-Related Incidents: Festive drinks cause falls or “holiday heart” – heart rhythm problems from overdrinking. This leads to dizziness and more.
Food Poisoning: Rushed meals with undercooked food or leftovers breed bacteria. About 48 million cases occur in the U.S. each year, peaking during holidays.
Injuries Related to Toys and Gifts: Choking on small parts injures 251,700 kids yearly. Faulty gifts cause cuts or trips.
Distracted or Drunk Driving: Busy El Paso roads see more crashes from texting or drinking. Drunk driving deaths rose to 1,013 in December 2021.
These issues increase ER visits by 5-12% in the U.S. and by over 80,000 in the UK during festivities. At El Paso Back Clinic®, we help locals recover quickly.
Causes of Holiday Injuries Seen at Our Clinic
Many injuries stem from everyday tasks gone wrong. To stop recurrences, we at El Paso Back Clinic® pinpoint these causes.
Overexertion: Heavy lifting, like trees or bags, strains backs. Bending incorrectly causes 80% of lower back pain. Travel luggage accounts for 72,000 doctor visits each year.
Cooking: Burns from oils or knives in busy kitchens. One in ten child injuries comes from cooking. Grease fires are frequent.
Decorating: Ladder falls, electrical shocks, or ornament cuts. Decorating sends 13,000 to ERs yearly. Cord trips cause 2,000 injuries.
Accidents on the Road or at Home: Distracted driving in El Paso’s traffic or at home. Stress slows reflexes.
Winter sports add 186,000 injuries, though they are less common here. Plants like mistletoe can poison if eaten.
Prevention Tips from El Paso Back Clinic®
Prevent accidents with simple steps. Our team at El Paso Back Clinic® shares these to keep your holidays safe.
For Falls: Use stable ladders and salt icy paths. Get help when climbing.
For Fires and Burns: Inspect wires, water trees, and use LED candles. Watch stoves closely.
For Cuts and Strains: Cut safely and lift with your knees. Team up for heavy items.
For Alcohol and Driving: Designate a driver or use a ride. Drink moderately.
For Food and Toys: Cook thoroughly and chill food fast. Pick safe, age-appropriate toys.
Keep a first aid kit handy and manage stress. Visit us for pre-holiday check-ups.
How Integrative Chiropractic Care at El Paso Back Clinic® Helps
If injured, turn to El Paso Back Clinic® for natural healing. Our integrative chiropractic care, in partnership with NPs, treats the whole person. Dr. Alexander Jimenez, with over 30 years in El Paso, observes that holiday injuries often stem from poor posture or stress, leading to misalignment of the spine. We use non-invasive techniques to ease pain without meds or surgery.
Adjustments for Spinal and Joint Pain: Realign the spine to relieve strain from falls or lifts. This boosts movement and cuts swelling.
Massage and Physiotherapy for Muscle Problems: Ease tension from overwork. Improves circulation for faster recovery.
NP-Led Care for Holistic Wellness: Our NPs manage overall health, including burn care and effects of poisoning, with a natural focus.
Nutrition Guidance: Counter rich holiday foods with diet tips to aid digestion and immunity. Fiber-rich choices help.
Managing Underlying Conditions: Reduce stress hormones for better sleep and mood. Prevents further harm.
Dr. Jimenez’s team uses functional medicine to develop personalized plans that address issues like sciatica from slips. Chiropractic enhances the nervous system for better health during the holidays.
Enjoy a Healthy Holiday with El Paso Back Clinic®
Make Christmas memorable for the right reasons. Know the risks, prevent them, and seek our care if needed. At El Paso Back Clinic®, we’re here for your wellness. Contact us in El Paso, TX, for expert chiropractic support. Happy holidays!
Introduction: My Personal Commitment to the Medico-Legal World—Bridging the Gap Between Clinical Science and Courtroom Proof
By Dr. Alex Jimenez, DC, APRN, FNP-BC | Board-Certified Nurse Practitioner & Chiropractor
Injury Medical Clinic PA, El Paso, Texas
The answer to the crucial question of whether the injury can be conclusively proven, dated, and causally connected to the traumatic event frequently determines the outcome of the high-stakes world of personal injury litigation.
My life’s work at Injury Medical Clinic PA is dedicated to answering this question with an unassailable “Yes.” I have spent decades developing a diagnostic and documentation protocol that transcends the limitations of standard clinical practice. For me, a patient is not just a set of symptoms; they are a complex medico-legal case requiring forensic-level analysis. I recognized early on that El Paso attorneys needed more than a standard radiologist’s report or a simple chiropractor’s diagnosis—they needed a comprehensive, integrated expert who could seamlessly bridge advanced musculoskeletal biomechanics (my foundation as a Chiropractic Physician, DC) with the rigorous standards of comprehensive medical management and documentation (my expertise as a Board-Certified Nurse Practitioner, APRN, FNP-BC).
This unique duality is the engine of our practice. I am not just treating the patient; I am building the legal case. My goal for every personal injury client referred to me is to deliver definitive diagnostic proof that withstands the most rigorous cross-examination, establishes clear causality using objective biomechanical markers, and determines a scientifically validated timeline for the injury—what I call injury dating.
This lengthy post serves as my own, in-depth guide to legal counsel, shedding light on the extent of my involvement in the evaluation of injuries. I meticulously examine the procedures that I use to assess patient cases. These procedures are indispensable for determining the root cause of an illness and for shedding light on the actual degree of disability and impairment that has resulted from traumatic events. I take great pride in my role as a professional in that I am committed to the idea that when a clinical case is brought before a jury, the attorneys representing the plaintiff have complete confidence in the credibility and scientific basis of the expert testimony that I provide.
Dr. Alex Jimenez, DC, APRN, FNP-BC
I will deeply discuss, from my personal experience:
The Diagnostic Imperative: My sophisticated capability to personally stage and interpret complex Magnetic Resonance Imaging (MRI) findings, distinguishing acute trauma from pre-existing conditions using forensic principles.
Causality and Timing: My systematic, proprietary methodology for establishing causality and determining the precise timing (injury dating) of trauma using advanced biomechanical and physiological markers like Modic changes and Wolff’s Law.
The Dual-Licensed Advantage: The justification and profound benefit of treatment and testimony provided by me, a dual-licensed professional, within the El Paso legal community.
Expert Credibility: How attorneys frequently utilize my expert testimony as the credible, objective voice regarding injury dating, impairment, and functional loss, ensuring my documented assessments and evaluations meet the stringent Daubert Standard.
1.0 The Diagnostic Imperative: Personally Staging and Interpreting Complex MRI Findings—Going Beyond the Radiologist’s Report
In my experience, the Magnetic Resonance Imaging (MRI) scan is the single most crucial piece of objective evidence in spinal injury litigation. However, I’ve found that a standard radiologist report often focuses primarily on morphology—describing what is seen—but fails to provide the critical context of causality and chronicity necessary for a successful legal claim.
At Injury Medical Clinic PA, I do not simply accept the outside read; I forensically interpret the physiological, mechanical, and temporal signatures embedded within the MRI data myself. I personally review every single slice and sequence because my ultimate testimony depends on my deep understanding of the images.
1.1 Meeting the Daubert Standard: My Personal Protocols for Scientific Admissibility
In the medico-legal domain, any scientific evidence I present, especially complex imaging findings, must adhere to the Daubert Standard. This requires my expert testimony to be grounded in the methods and procedures of science and supported by appropriate validation (Spinal Diagnostics, n.d.). My entire documentation protocol is built around this necessity.
I personally ensure my findings are admissible by:
Employing Validated Methodology: I utilize diagnostic criteria and staging methods that are thoroughly established in peer-reviewed orthopedic and radiological literature, such as the classification of disc pathology and the chronology of vertebral changes (Wang et al., 2017).
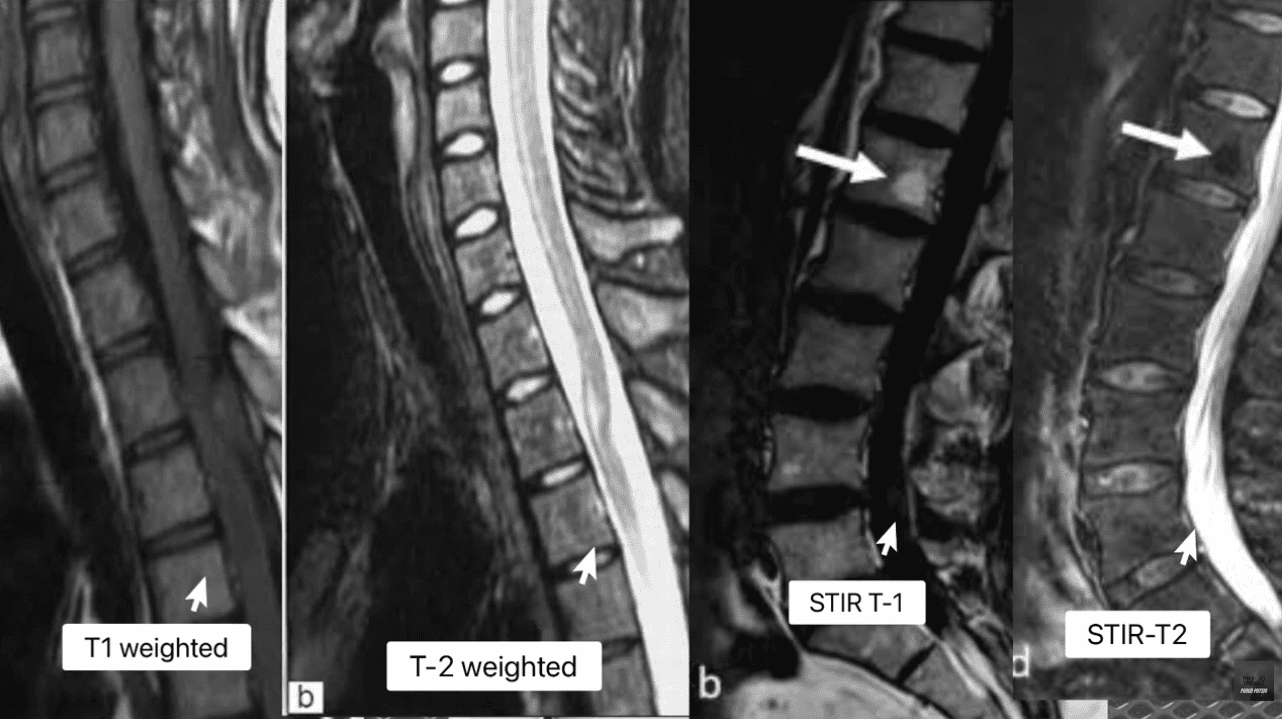
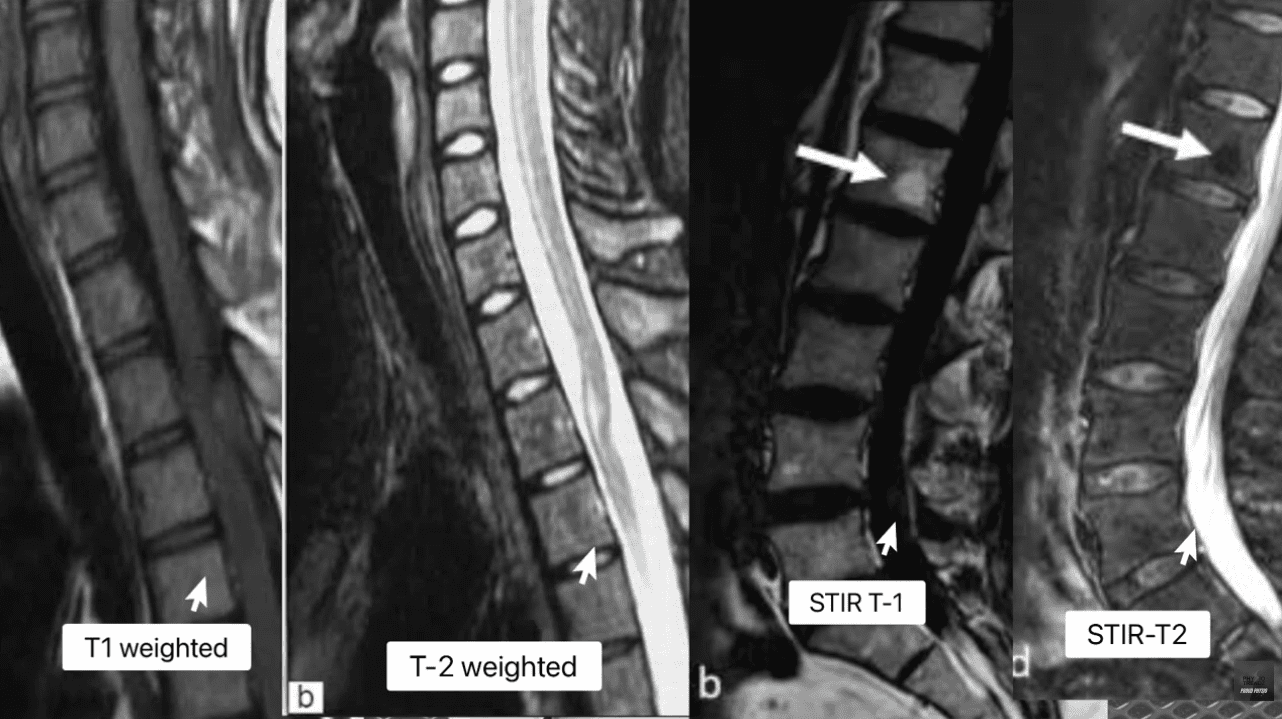
Focusing on Objectivity: My reports meticulously cite the specific MRI pulse sequences (T1, T2, STIR) and image numbers where the pathology is visualized, allowing opposing counsel and the court to verify the data. This objectivity mirrors the rigor seen in advanced quantitative neuroimaging tools like NeuroQuant®, which are successfully used to meet the Daubert standard in TBI cases (National Institutes of Health, 2022).
Simplifying Complex Science: When I testify, my goal is to translate complex terms into easily digestible concepts for the jury. I do not just state a Modic 1 change is present; I explain why it’s a marker of acute trauma, making the science reliable and understandable. This is a crucial skill that attorneys rely on me for.
1.2 Decoding the Spinal Pathologies: My Forensic Review of T1, T2, and STIR Sequences
My method for forensic MRI interpretation depends on a nuanced understanding of various pulse sequences and their physiological meaning (Advanced MRI Interpretation, n.d.). I meticulously review the T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) sequences because they tell different stories about the underlying tissue pathology.
MRI Staging Acute Vs Chronic Injuries
MRI Sequence
Primary Signal (Bright)
Primary Signal (Dark)
Pathological Significance
T1-Weighted
Fat (Marrow), Contrast (Gadolinium)
Water (Edema, CSF), Cortical Bone
Anatomy: Excellent for visualizing fatty infiltration (chronic muscle atrophy, Modic 2) and overall anatomical structure.
T2-Weighted
Water (Edema, CSF), Degenerated Disc
Fat (Marron), Cortical Bone
Pathology: Crucial for identifying water, making it the primary sequence for acute inflammation, disc herniation (fluid), and spinal cord changes.
STIR (Fat-Suppressed)
Water (Edema, CSF, Inflammation)
Fat (Marrow)
Acuity: The definitive sequence for acute trauma. By suppressing fat signal, any remaining bright signal is unequivocally edema, confirming acute inflammation in bone or soft tissue.
The presence of edema (abnormal fluid accumulation) in the bone marrow or soft tissues surrounding the spine is, in my professional opinion, the most powerful, objective indicator of acute trauma. This edema is the body’s immediate inflammatory response to injury and provides the temporal signature required for my precise injury dating.
1.3 Injury Dating: My Systematic Methodology for Establishing a Timeline of Trauma
The ability to accurately date an injury—to definitively state that a spinal pathology is new or acute, rather than chronic and pre-existing—is, without question, the cornerstone of a successful personal injury claim. My clinic utilizes physiological and biomechanical principles to establish this timeline with forensic precision.
1.3.1 Modic Changes: The Gold Standard for Vertebral Endplate Chronology
Modic changes are alterations in the vertebral body endplates and adjacent bone marrow, visible on MRI, that reflect different stages of pathological response. I rely on them heavily because they provide an objective and scientifically validated marker for estimating the age of an injury (Wang et al., 2017; Spinal Diagnostics, n.d.).
Determining Age of Injury Via MRI Staging
Modic Type 1 (MC1) – The Acute Signature: MC1 represents the acute inflammatory stage characterized by bone marrow edema. When I see this, I know I’m looking at an injury that is active and recent.
My Staging: I stage this based on the specific signal patterns: Dark on T1 and Bright on T2/STIR (Spinal Diagnostics, n.d.). The persistent bright signal on STIR is the definitive confirmation of active, acute inflammation.
My Testimony: I explain to attorneys that MC1 changes typically resolve or transition to the fatty Type 2 changes within approximately 6 to 8 weeks (Spinal Diagnostics, n.d.). Therefore, the presence of MC1 is a powerful, objective sign of recent trauma, often correlating directly with the patient’s reported high pain scores (Jensen et al., 2024). When a defense expert attempts to argue degeneration, my documentation of MC1 provides the irrefutable evidence of a specific, new acute event.
Modic Type 2 (MC2) – The Chronic Transition: MC2 represents the replacement of normal bone marrow with fatty tissue (Wang et al., 2017). This is a marker of a more subacute or chronic condition.
My Staging: I stage this based on the characteristic Bright on T1/T2 but crucially, Dark on STIR (fat-suppressed) sequence (Spinal Diagnostics, n.d.).
My Testimony: I use MC2 to show pre-existing degeneration, which ironically, strengthens my credibility. By acknowledging a chronic condition at one level (MC2) while simultaneously proving an acute injury at another (MC1), I demonstrate objectivity and isolate the liability to the new, acute trauma.
1.3.2 Wolff’s Law and My Chronological Interpretation of Bone Spurs
Further reinforcing my injury dating is my application of Wolff’s Law, a fundamental biomechanical principle that bone tissue adapts to the loads placed upon it (Spinal Diagnostics, n.d.). Chronic instability leads to the formation of osteophytes (bone spurs) as the body attempts to stabilize the segment through the piezoelectric effect (Spinal Diagnostics, n.d.).
The Biomechanical Timeline: I rely on scientific research confirming that it takes approximately six months for a bone spur to become radiographically visible or significant (Spinal Diagnostics, n.d.).
My Medico-Legal Implication: When I review a patient’s initial X-rays or CT scans following an MVA, and I find a complete absence of chronic osteophyte formation in the affected segment (e.g., C5-C6), yet the MRI shows an acute disc herniation, I have created an unassailable timeline. The absence of the six-month marker (the bone spur) provides strong supporting evidence that the soft-tissue injury is acute and causally related to the recent collision.
1.4 The Crucial Differential Diagnosis: My Approach to Acute Trauma vs. Chronic Degeneration
Distinguishing new trauma from old, asymptomatic degeneration is essential for proving the extent of damage. I use specific MRI markers to draw this clear line, transforming a murky diagnosis into legal certainty.
Many accident victims have some degree of pre-existing, asymptomatic degeneration. The defense always targets this reality. My expertise lies in identifying and quantifying the acute-on-chronic injury (Spinal Diagnostics, n.d.).
The tell-tale radiological sign I look for is the clear observation of newly extruded disc material extending beyond the border of a mature, pre-existing osteophyte (Spinal Diagnostics, n.d.). The osteophyte, being a chronic boney change, acts as an anatomical baseline for pre-injury status. Any disc material that has been forcefully extruded beyond this chronic bony landmark is, by definition, new trauma and directly quantifiable aggravation. I personally measure this new extrusion and document its displacement in my reports.
1.4.2 The Vacuum Disc Phenomenon: The Irrefutable Marker of Old Pathology
I use the Vacuum Disc Phenomenon as another definitive marker of a chronic, old condition. This finding—nitrogen gas (a distinct signal void, appearing black) within the center of the disc on all MRI sequences (T1, T2, and STIR)—is a reliable sign of old, irreversible degenerative changes and instability (Spinal Diagnostics, n.d.; Advanced MRI Interpretation, n.d.).
When I find a vacuum disc at one level, I include it in my report. This establishes my objectivity, allowing me to state confidently that while one level is chronic, the adjacent, non-vacuum level that displays Modic 1 changes is acute and causally related to the MVA. This approach prevents the defense from collapsing the entire spine into a single, pre-existing condition.
1.5 Analysis of Complex Non-Disc Spinal Pathologies: The Hidden Injuries
Beyond disc herniation, I specialize in the advanced interpretation of other complex spinal pathologies frequently misunderstood or missed by general practitioners, yet vital for proving injury.
1.5.1 The Spinal Epidural Venous Plexus (Batson’s Plexus): Dural Tenting
The Spinal Epidural Venous Plexus (Batson’s Plexus) is a valveless network highly susceptible to sudden pressure changes (Advanced MRI Interpretation, n.d.). In court, I must distinguish between normal physiological changes and pathological ones.
My Differential Diagnosis: Trauma can cause a physiological venous dilation because a disc extrusion can push on the thecal sac—a phenomenon known as dural tenting. This must be carefully distinguished from a pathological Epidural Varix (a symptomatic dilation that causes neural compression) (Advanced MRI Interpretation, n.d.). I rely on sequences like contrast-enhanced MRI (when medically necessary) and non-contrast flow-sensitive sequences to confirm the difference. Incorrectly diagnosing normal venous dilation as a compressive pathology can undermine an entire claim, and my careful distinction preserves my credibility.
1.5.2 Post-Traumatic Muscle Changes: Fatty Infiltration of the Multifidus
The deep lumbar muscles, particularly the multifidus, are essential stabilizers. I have seen time and again how pain-induced inhibition leads to rapid structural changes in this muscle.
My Injury Dating and Causality: This muscle transformation begins to appear on imaging as early as 2 to 12 weeks post-injury (Spinal Diagnostics, n.d.; Central Ohio Spine and Joint, n.d.). Fatty infiltration (visible as a bright signal on T1-weighted images) is highly associated with chronic pain and instability. The degree of infiltration is a crucial prognostic indicator, correlating negatively with functional improvement (Xu et al., 2024). The presence and severity of multifidus fatty infiltration provide powerful objective evidence of chronic functional impairment and instability directly resulting from the traumatic event. I use this finding to prove permanent injury to the core stabilizing system, which is critical for future medical damages.
2.0 Establishing Causality: My Biomechanical and Legal Framework
The defense is designed to argue that a plaintiff’s pain is due to aging or unrelated issues. My documentation provides the scientific and legal rebuttals necessary to establish clear causation—a process I personally manage from the moment the patient walks through my door.
2.1 The “Eggshell Plaintiff” Doctrine: My Documentation Strategy
A foundational principle in personal injury law is the “Eggshell Plaintiff” Rule: a defendant must take the victim as they find them (Cornell Law School, n.d.). This means the defendant is fully liable for the plaintiff’s injuries, even if those injuries are more severe than they would have been in an average person due to an existing, pre-disposed condition (Rafi Law Firm, n.d.).
My Personal Role: Successfully applying this doctrine in court requires meticulous documentation, which I provide by:
Defining the Baseline: Precisely evaluating the pre-accident state (using the Vacuum Disc, Modic 2/3, and chronic osteophyte timelines). I acknowledge the pre-existing state without minimizing the new trauma.
Quantifying the Acute Change: Using Modic Type 1 and Acute-on-Chronic findings to objectively demonstrate the new, causally related injury (Spinal Diagnostics, n.d.).
Proving Exacerbation: Establishing that the traumatic event (MVA) directly aggravated the pre-existing condition, resulting in new symptoms, functional loss, and permanent impairment. My reports meticulously connect the mechanism of injury to the exacerbation, ensuring the court grasps the full scope of liability.
2.2 The Biomechanical Signatures of Soft Tissue and Ligamentous Injury (Whiplash)
Soft tissue injuries, or whiplash-associated disorders (WAD), are commonly challenged as subjective. My examination protocol goes beyond standard range of motion checks to confirm structural injury.
Occult Ligamentous Injury: I utilize the MRI’s fluid-sensitive sequences (STIR) to search for occult tears and sprains. I look for the hyperintense (bright) signal in the interspinous and supraspinous ligaments (Spinal Diagnostics, n.d.), which represents edema and tearing. This finding transforms a subjective “sprain/strain” into an objective, structural instability.
Facet Capsular Edema: The facet joints are often injured during MVA hyperflexion/hyperextension. I meticulously look for capsular edema or effusion (bright signal around the joint) on T2/STIR images. This is a highly specific finding for acute trauma to the joint capsule, which often correlates to localized, severe pain.
The Biomechanical Correlation: I thoroughly document the mechanism of injury (e.g., rear-end collision, specific speed data if available) and link the vector of force to the specific pathology found (e.g., a rear-end vector causing anterior compression and posterior ligamentous tearing) (NCBI, 2023). This correlation is crucial in court to overcome defense arguments that the forces were insufficient to cause the documented injury.
3.0 The Dual-Licensed Advantage: My DC & APRN/FNP-BC Model in El Paso
The most compelling aspect of the Injury Medical Clinic PA model, and the primary reason for my success in the medico-legal field, is my unique qualification as a dual-licensed professional. The integration of the Doctor of Chiropractic (DC) and the Advanced Practice Registered Nurse/Family Nurse Practitioner (APRN/FNP-BC) licenses creates a holistic, comprehensive, and legally powerful care model that is unmatched in the El Paso area.
3.1 Comprehensive Care Models: My Integrated Approach
I bring together the best of both worlds, creating a single source of expertise that satisfies both the clinical and legal standards of care:
My Role as a Chiropractic Physician (DC): I provide unparalleled expertise in spinal biomechanics, functional assessment, manual therapy, and the non-surgical management of complex musculoskeletal injuries. The DC perspective is critical for evaluating the long-term functional impairment caused by disc, facet, and ligament pathology.
My Role as a Nurse Practitioner (APRN/FNP-BC): I provide the essential medical framework, including the ability to prescribe medication (e.g., muscle relaxants, neuropathic agents), order and manage advanced diagnostic testing (e.g., specific, medically-prescribed MRI protocols, nerve conduction studies), manage co-morbidities, and, most crucially, write comprehensive, authoritative medical-legal reports and provide expert testimony that carries the weight of a board-certified medical professional, satisfying the standard medical scrutiny of the court.
This integration ensures the patient receives optimal physical rehabilitation alongside rigorous medical documentation, all under one practice. My reports are medical documents authored by an APRN/FNP-BC, while the therapeutic details reflect the specialized biomechanical insight of a DC. This synergy is invaluable to attorneys.
3.2 Justification for Dual-Licensed Intervention: Case Archetypes in My Practice
I manage these three case archetypes every day, and they demonstrate why my dual-licensed approach is often medically and legally necessary:
Case Archetype
Clinical Presentation in My Clinic
My Dual-Licensed Treatment Rationale
Medico-Legal Value in My Reports
Type 1: Complex Cervical WAD with Radiculopathy.
Patient presents with neck pain, headaches, and confirmed numbness/tingling in the arm. MRI shows a C5-C6 disc bulge impinging on the nerve root.
My DC Expertise: Focus on specific spinal mobilization to reduce segmental dysfunction and restore cervical curve stability. My APRN Expertise: Prescribe gabapentin or NSAIDs for nerve pain, order Electromyography/Nerve Conduction Velocity (EMG/NCV) studies, and administer facet or trigger point injections if necessary (Mayo Clinic, 2024).
Causality: The combined finding of clinical radiculopathy (confirmed by NCV—a medical test I ordered) and the biomechanical trauma (my DC diagnosis) is documented under a single, authoritative medical record (my APRN report). I can objectively testify to the severity of the neurological deficit.
Type 2: Acute Lumbar Disc Extrusion with Failed Conservative Care.
Patient suffers acute L5-S1 disc extrusion causing severe, debilitating sciatica that is not responding to basic care.
My DC Expertise: Implement specialized non-surgical spinal decompression protocols and advanced core stabilization exercises. My APRN Expertise: Medically evaluate the patient’s pain using objective outcome measures (Oswestry Disability Index), rule out Red Flags (Cauda Equina), manage opioid/non-opioid medication, and critically, document the failure of conservative care, which justifies the trajectory toward advanced interventions or surgical consultation.
Damages & Prognosis: My comprehensive documentation of conservative care failure establishes the persistent, debilitating nature of the injury. This robust history is essential for the attorney to justify the valuation of both past and high-value future medical costs in front of a jury.
Type 3: Acute-on-Chronic Spinal Instability.
Patient has pre-existing, asymptomatic spinal stenosis (Modic Type 2 changes), but the MVA results in new symptoms and a new Modic Type 1 change at the adjacent level.
My DC Expertise: Focus on restoring segmental stability to the traumatized level while protecting the degenerated level. My APRN Expertise: Personally interpret the complex MRI (Modic 1 vs. Modic 2) to clearly delineate the acute injury (liability) from the pre-existing condition (eggshell) (Spinal Diagnostics, n.d.).
Defeating the Defense: My precise diagnostic report legally isolates the acute trauma (Modic 1) from the chronic degeneration (Modic 2/Vacuum Disc), providing the attorney with clear, objective evidence to apply the Eggshell Plaintiff doctrine and secure recovery for the aggravation and new injury.
4.0 My Credible Expert Witness Testimony: Illuminating Disability and Driving Monetary Recoveries
My ultimate function for the legal community is to serve as the credible, objective voice that clarifies the patient’s impairment for the jury. My testimony is built upon the synthesis of advanced clinical diagnostics and established medico-legal principles that I personally adhere to.
4.1 The Credibility Foundation: My Daubert-Compliant Testimony
Attorneys frequently utilize my expertise because my methodology is rooted in the scientific method, ensuring my opinions are admissible under the Daubert Standard. My expert testimony is not merely anecdotal; it is a direct presentation of verifiable scientific data:
Measurable Markers: When I testify, I don’t just state an opinion. I point to the imaging and explain that the Modic Type 1 change is not random, but an established scientific finding with a specific 6-8 week timeline, proving the freshness of the bone trauma (Wang et al., 2017). I use analogies, like comparing the Modic 1 change to a fresh bruise on the bone, which makes the complex science undeniable to a layperson jury.
Biomechanically Sound Conclusions: I personally explain how the physics of the impact (the vector, the forces) translates into the specific, demonstrable injury, such as the mechanism by which a sudden flexion-extension event causes an annular tear (Paredes et al., 2023). This link between physics and physiology is critical for proving causation.
The Power of the Dual Role: When I stand before the court, my opinion integrates the highest standard of musculoskeletal diagnosis (DC) with the authority of advanced medical management (APRN). I am uniquely positioned to counter both the defense’s biomechanics expert and their medical expert.
4.2 My Method for Translating Pathology into Permanent Impairment and Disability
The value of a personal injury case is directly linked to the demonstrability and permanency of the injury. My detailed reports translate abstract medical findings into tangible, compelling evidence of long-term disability for the jury.
4.2.1 Quantifying Functional Loss: From Imaging to Activities of Daily Living (ADLs)
I shift the focus from what the injury looks like on an MRI to how it permanently impairs the patient’s life:
Multifidus Fatty Infiltration: I explain to the jury that the increased bright signal on the patient’s T1 MRI is not simply “fat,” but the objective, measurable sign of a permanent loss of spinal stability (Central Ohio Spine and Joint, n.d.). I elaborate that the muscle is no longer functional, leading to chronic instability, increased risk of re-injury, and an inability to perform basic ADLs like prolonged sitting, standing, or lifting—directly correlating to a lower quality of life and permanent functional loss.
Irreversible Cord Damage (Myelomalacia): If I identify Myelomalacia (softening, necrosis, and scarring of the spinal cord tissue) on a T2 image (hyperintensity within the cord), I use this to establish a definitive, catastrophic, permanent neurological injury (Spinal Diagnostics, n.d.). This finding is irreversible and dictates a life of permanent neurological deficits, which is irrefutable evidence of severe disability that warrants significant monetary recovery.
4.2.2 Linking Causality to Prognosis and Future Medical Costs
My reports connect the initial traumatic event to the long-term cost of care. This is vital for the attorney’s calculation of future medical damages.
Permanent Impairment Rating (PIR): I use objective prognostic indicators—such as the severity of multifidus infiltration (Xu et al., 2024), the persistence of Modic 1 changes, or the presence of irreversible ligament instability—to generate a scientifically grounded Permanent Impairment Rating (PIR) using the AMA Guides to the Evaluation of Permanent Impairment.
Future Medical Requirements: The report then outlines the need for future care (e.g., ongoing chiropractic maintenance, periodic APRN follow-ups, medication management, or potential injections/surgical consultations) directly necessitated by the MVA. This robust justification of future needs is critical for maximizing the final settlement or jury award.
By establishing causation, chronicity, and prognosis through my rigorous, peer-reviewed methodology, I provide the unassailable evidence necessary to maximize the plaintiff’s recovery and to position legal counsel to confidently present even the most complex clinical cases before a jury. My role is to ensure that the injury is not only treated effectively but also documented exhaustively, establishing Injury Medical Clinic PA as the premier clinic for injuries resulting from accidents in the El Paso area.
National Institutes of Health (NIH). (2022). Updated Review of the Evidence Supporting the Medical and Legal Use of NeuroQuant® and NeuroGage® in Patients With Traumatic Brain Injury. PMC – PubMed Central. https://pmc.ncbi.nlm.nih.gov/articles/PMC9027332/
Overcoming Sciatic Nerve Pain: Expert Insights from El Paso Back Clinic® in El Paso, TX
At El Paso Back Clinic®, located in the heart of El Paso, Texas, we specialize in helping people get back to their active lives without the constant burden of pain. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, our team combines chiropractic care with modern wellness strategies to treat conditions like sciatic nerve issues. Whether you’re dealing with sharp leg pain from a work injury or numbness after a car accident, our clinic offers personalized plans to ease your symptoms and promote long-term health. We focus on non-invasive methods that address the root causes, not just the signs. If you’re in El Paso and searching for effective sciatica relief, our integrated approach could be the key to feeling better.
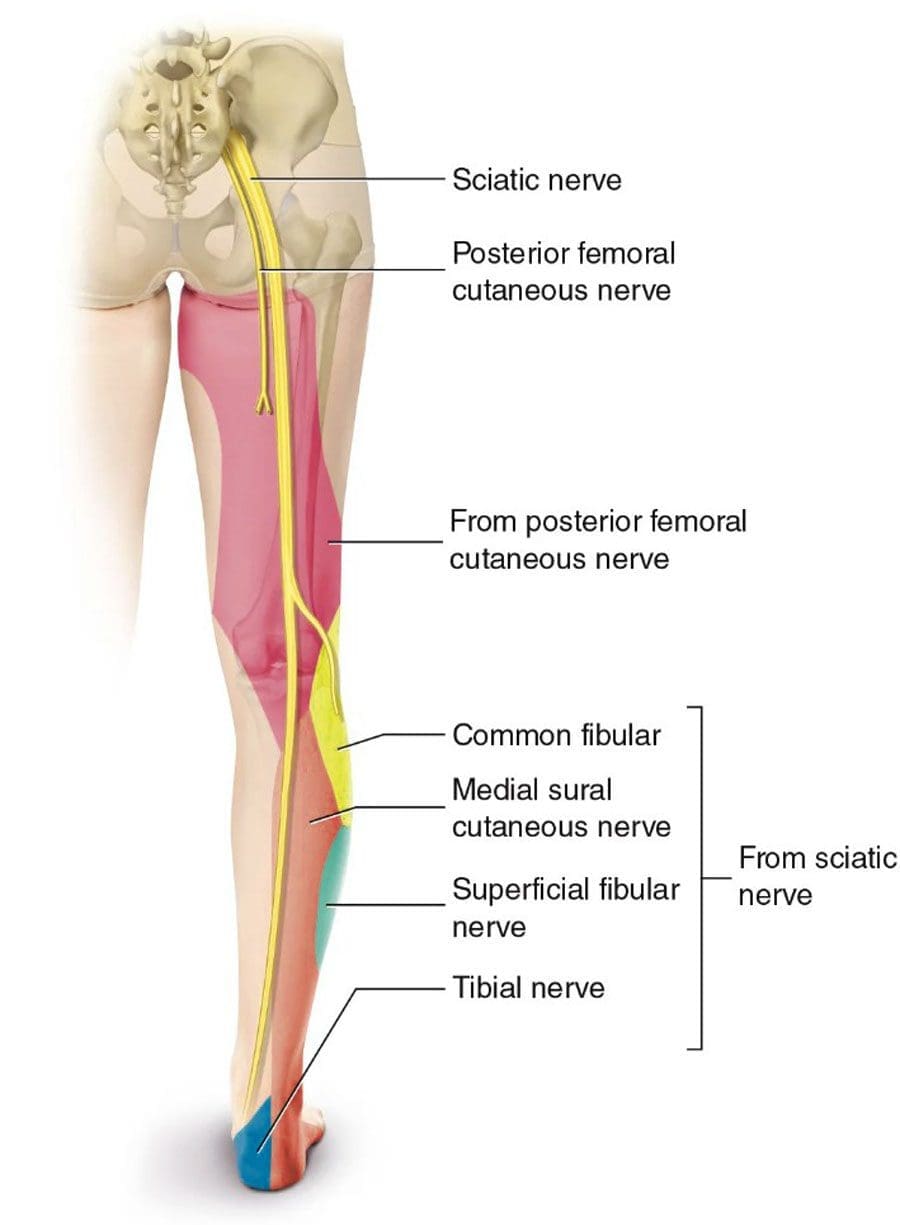
Sciatica isn’t just a back problem—it’s a nerve issue that can disrupt your daily routine. The sciatic nerve, which is like a thick cable running from your lower spine down each leg, gets irritated or squeezed, causing discomfort that travels far. At our clinic, we’ve seen how this affects everyone from athletes to office workers. In this guide, we’ll dive into what sciatica really is, why it happens, and how our team at El Paso Back Clinic® uses proven techniques to help. We’ll cover the physical side of nerve damage, common triggers, signs to watch for, and recovery steps. Plus, we’ll share how our chiropractic integrative care stands out in treating these issues right here in El Paso.
The Basics of the Sciatic Nerve and How Pressure Affects It
The sciatic nerve is your body’s main pathway for signals between the brain and legs. It begins at the lower back, where several nerve roots join, then branches through the buttocks and down to the feet. This nerve handles movement in your hamstrings, calves, and feet, as well as sensation in those areas. When something, like a slipped disk or tight muscle, presses on it, problems start.
When the sciatic nerve is compressed, pinched, or crushed, it suffers physical damage that disrupts its ability to transmit signals, leading to pain, numbness, and muscle weakness. The severity of the physical changes depends on the nature and duration of the pressure. Inside the nerve, axons carry messages, protected by myelin sheaths for fast travel. Pressure squishes these, causing swelling and blocking blood flow, which starves cells of oxygen—a state called ischemia (Verywell Health, 2023). In mild squeezes, like poor posture, the myelin gets worn but regrows. But harder crushes break axons, triggering degeneration where the nerve falls apart below the spot (Menorca et al., 2013).
Think of it like a garden hose: a light kink slows water, but a stomp cuts it off. Short pressure might cause temporary numbness, but ongoing force leads to scarring and chronic issues. At El Paso Back Clinic®, we use advanced checks to spot these changes early, helping prevent lasting harm.
Recognizing the Signs of Sciatic Nerve Trouble
Sciatica shows up in ways that can sneak up on you. The classic sign is radiating pain—starting in the lower back and zipping down one leg like an electric shock. It might burn, tingle, or feel sharp, worse when you sit, stand, or sneeze (Penn Medicine, n.d.). Numbness follows, making parts of your leg feel asleep or prickly. Weakness hits muscles, causing limps or trouble with stairs (Align Wellness Center, n.d.).
In our El Paso clinic, patients often describe it as a “leg giving out” or a constant ache. Severe cases bring muscle shrinking or even bladder issues if nerves are badly pinched (ADR Spine, n.d.). We see this in folks from all walks—drivers with long hauls, athletes pushing limits, or those in desk jobs. Early signs? Pay attention to one-sided pain that doesn’t fade with rest.
What Causes Sciatic Nerve Compression in Everyday Life
Life in El Paso means active days, but that can lead to sciatica triggers. A herniated disk, where the cushy part bulges and presses on the spinal cord roots, is common from lifting heavy boxes at work (Mayo Clinic, 2023). Aging narrows the spine in stenosis, squeezing nerves (Physio Pretoria, n.d.). Tight piriformis muscles in the butt can pinch the sciatic nerve, too, especially in runners or cyclists.
Accidents amp it up—car crashes crush nerves directly (MedStar Health, n.d.). Bone growths from arthritis add pressure, and extra weight strains everything (Advanced Orthopaedics & Sports Medicine, n.d.). Double crush? That’s when two spots squeeze, such as the back and leg, worsening the condition (Southwest Regional Wound Care Center, n.d.). At our clinic, we trace these in locals from border commutes to sports fields.
How We Diagnose Sciatica at El Paso Back Clinic®
Getting the right diagnosis is step one to relief. At our El Paso locations, we start with a full chat about your history—when the pain started and what makes it worse. Then, during hands-on exams, we test reflexes, strength, and perform the leg raise to pinpoint nerve irritation (Penn Medicine, n.d.).
We use top tools like MRI for disk views, EMG for signal checks, and X-rays for bones (ICliniq, 2023). Dr. Jimenez’s dual training as a chiropractor and nurse practitioner allows for a dual-scope diagnosis—blending medical tests with chiropractic insights for a full picture (Jimenez, n.d.). This helps link injuries to symptoms accurately, especially in complex cases from MVAs or sports.
Physical Damage from Compression: A Closer Look
Diving deeper, compression physically alters the nerve. Mild pressure causes neurapraxia: myelin dents, slowing signals without axon breaks. You feel weak but recover fast (Menorca et al., 2013). Stronger pinches lead to axonotmesis: axons snap, walls degenerate, and swelling builds. Healing takes time as new growth crawls along (Horton Mendez, n.d.).
Crushes bring neurotmesis: full sever, with scars blocking regrowth (Bhatia, 2023). Pressure cuts off blood, causing ischemia and cell death (Verywell Health, 2023). Chronic? Fibrosis hardens tissue (Mackinnon, 1998). Our clinic spots these via imaging, guiding treatments to reduce pressure and aid repair.
Integrative Chiropractic Care: Our Approach at El Paso Back Clinic®
We believe in whole-body healing. Our chiropractic integrative care combines spinal adjustments, soft tissue work, and exercises to correct alignment, enhance muscle function, and improve nerve signals. Adjustments ease pressure on the sciatic nerve, while massage loosens tight spots (AMTA, n.d.). Rehab builds strength to prevent repeats (Byington, n.d.).
This holistic method tackles pain now and builds stability for tomorrow. We add nutrition and stress tips, as gut health and emotions affect recovery. For El Paso folks, it’s about getting back to hikes or family time pain-free.
Dr. Alexander Jimenez’s Clinical Observations and Clinic Breakdown
With over 30 years, Dr. Jimenez brings unique insights. His dual credentials allow clinical correlations: linking injuries to assessments via advanced imaging like MRI for neuromusculoskeletal views (LinkedIn, n.d.). We treat work strains, sports sprains, personal slips, and MVAs with tailored plans.
Our process: Dual-scope diagnosis merges chiropractic and medical for thorough checks. Treatments include adjustments, non-surgical decompression, acupuncture, and functional medicine. We handle legal documents for accident claims, ensuring smooth care (Jimenez, n.d.). Observations? Stress worsens posture, and gut issues slow healing—we address all.
Recovery and Prevention Tips from Our El Paso Team
Recovery varies: Mild cases heal in weeks with rest and therapy, while severe cases require months (ADR Spine, n.d.). We guide with exercises, avoiding surgery when possible.
Prevent? Good posture, regular moves, and weight control. At our clinic, we teach these in sessions.
In El Paso, sciatica doesn’t have to hold you back. El Paso Back Clinic® offers expert, local care to restore your life.
Learn about the vagus nerve in the body, a key player in regulating bodily functions and enhancing your health naturally.
Unlocking the Power of the Vagus Nerve: Your Body’s Chill Button for Pain Relief and Wellness
Ever wonder if your body has a secret control center that can dial down stress, soothe pain, and make you feel like you’re floating on a cloud of calm? Spoiler alert: it does, and it’s called the vagus nerve—your body’s very own superhero nerve! Think of it as the cool, laid-back DJ of your nervous system, spinning tracks of relaxation to keep your body in harmony. But when this DJ starts missing beats, things like chronic pain, stress, and even achy muscles can crash the party. This comprehensive exploration delves into what the vagus nerve is, how it teams up with the parasympathetic nervous system, and why it’s crucial for keeping pain at bay. We’ll uncover how factors like stress, poor diet, or even slouching at your desk can mess with your vagus nerve’s groove, potentially leading to body pain. Plus, we’ll spotlight how nonsurgical treatments like chiropractic care and acupuncture can crank up the vagus nerve’s chill vibes, and share lifestyle hacks to keep it humming.
What Is the Vagus Nerve? Your Body’s Superhighway of Calm
Picture the vagus nerve as the ultimate multitasker in your body—a long, winding nerve that’s like a superhighway connecting your brain to almost every major organ. Officially known as the tenth cranial nerve, it’s the longest nerve in your autonomic nervous system, stretching from your brainstem down through your neck, chest, and abdomen, touching your heart, lungs, stomach, and intestines. Its name comes from the Latin word for “wandering,” and boy, does it wander! Think of it as your body’s internal GPS, guiding signals to keep your heart rate steady, your digestion smooth, and your stress levels in check.
The vagus nerve is the star player in the parasympathetic nervous system, the part of your body that says, “Chill out, everything’s cool.” It’s responsible for heart rate regulation, slowing your heart rate when you’re relaxed; digestion, telling your stomach and intestines to get moving; breathing, helping you breathe deeply and calmly; inflammation control, acting like a firefighter dousing inflammation; and mood and stress management, sending signals to your brain to release feel-good chemicals like serotonin.
The vagus nerve is your body’s master regulator, keeping things balanced and preventing chaos. When it’s working well, you feel energized, calm, and pain-free. But when it’s out of tune, it can lead to all sorts of trouble, including body pain.
The Parasympathetic Nervous System: Your Body’s “Rest and Digest” Mode
If the vagus nerve is the DJ, the parasympathetic nervous system (PNS) is the chill lounge where it spins its magic. The PNS is one half of your autonomic nervous system, which controls all the stuff you don’t think about, like breathing, heart rate, and digestion. While the sympathetic nervous system is your “fight or flight” mode—kicking in when you’re running from a bear or stressing about a deadline—the PNS is your “rest and digest” mode, helping you relax, recover, and recharge.
The parasympathetic nervous system’s job is to bring your body back to a state of calm after stress. It slows heart rate to a relaxed rhythm, saving energy for healing and recovery; boosts digestion by stimulating your gut to break down food and absorb nutrients; promotes healing by encouraging tissue repair and reducing inflammation; and calms the mind by signaling your brain to chill out, reducing anxiety and boosting mood.
The vagus nerve is the PNS’s MVP, carrying most of its signals to your organs. When your vagus nerve is firing on all cylinders, it’s like your body’s in a cozy spa day—relaxed, healing, and ready to take on the world. But when the vagus nerve’s “vagal tone” (its strength and efficiency) is low, things can go south, leading to stress, inflammation, and even body pain.
Understanding Vagal Tone and Why It Matters
Vagal tone is like the signal strength of your vagus nerve—how well it’s communicating with your body to keep things calm and balanced. High vagal tone means your vagus nerve is strong, responsive, and great at keeping your heart rate steady, your digestion smooth, and your stress low. Low vagal tone, on the other hand, is like a weak Wi-Fi signal—your body struggles to stay calm, inflammation spikes, and pain can creep in.
Think of vagal tone as your body’s ability to hit the brakes on stress. When it’s high, you recover quickly from stressful situations, like bouncing back after a tough workout or a heated argument. Low vagal tone means your body stays stuck in “stress mode,” which can mess with your health and lead to pain. Research shows that a higher vagal tone is associated with a lower resting heart rate, reduced blood pressure, and increased heart rate variability (HRV), which are strongly correlated with overall cardiovascular health and emotional regulation.
Factors That Disrupt Vagus Nerve Function and Lead to Pain
Your vagus nerve is a sensitive soul—it can get thrown off by a variety of factors, from lifestyle choices to environmental stressors. When vagal tone takes a hit, it can lead to overlapping risk profiles that increase body pain.
Chronic Stress: The Vagus Nerve’s Kryptonite
Stress is like kryptonite for your vagus nerve. When you’re constantly stressed—whether from work deadlines, family drama, or scrolling doom-filled news—your sympathetic nervous system (fight or flight) goes into overdrive, suppressing the parasympathetic system and lowering vagal tone. This keeps your body in a state of high alert, spiking stress hormones like cortisol, which can tighten muscles leading to neck, shoulder, or back pain; increase inflammation, making trigger points more likely to form; and disrupt sleep, which amplifies pain sensitivity and slows recovery.
Poor Posture and Spinal Misalignments
Slouching at your desk or hunching over your phone doesn’t just strain your muscles—it can compress the vagus nerve as it passes through your neck and chest. This can lower vagal tone, reducing its ability to calm your body and manage inflammation. Poor posture creates muscle imbalances leading to pain in your back, shoulders, or hips; increases tension in the fascia (connective tissue), forming painful trigger points; and disrupts nerve signaling, which can amplify pain perception.
Recent research reveals the intricate connection between spinal health and vagal function. Vertebral subluxations and misalignments can interfere with the normal flow of nerve signals, potentially compromising the vagus nerve’s ability to regulate inflammation and pain responses.
Sedentary Lifestyle and Physical Inactivity
Sitting all day or skipping exercise can weaken vagal tone by reducing the stimulation your vagus nerve needs to stay active. A sedentary lifestyle stiffens muscles and fascia, increasing the risk of painful knots; reduces blood flow, which hampers healing and ramps up inflammation; and contributes to stress and poor sleep, creating a vicious cycle of pain and low vagal tone.
Conversely, research demonstrates that non-invasive vagal stimulation combined with regular exercise can improve cardiorespiratory fitness and attenuate inflammation, offering an inexpensive, safe, and scalable approach to improve exercise capacity and overall health.
Dietary Factors and Inflammation
What you eat matters for your vagus nerve. Diets high in sugar and processed foods spike inflammation, which can suppress vagal tone and make pain worse. High-fat diets have been shown to induce inflammation in the nodose ganglion and hypothalamus, compromising vagal plasticity and the ability of vagal afferents to respond to various regulatory signals.
Nutritional deficiencies in key nutrients, such as omega-3 fatty acids —which reduce inflammation and support vagal function —vitamin D and magnesium (essential for nerve health and muscle relaxation), and choline (a precursor to acetylcholine, the primary neurotransmitter of the parasympathetic nervous system), can all negatively impact vagal tone.
Sleep Disruption and Vagal Dysfunction
Lack of sleep is a major vagal tone killer. Poor sleep disrupts the parasympathetic system, keeping your body in a stressed state and reducing the vagus nerve’s ability to regulate inflammation. The vagus nerve plays a crucial role in sleep regulation, and when it’s not functioning properly, it can lead to increased cortisol levels, disrupted sleep patterns, and contribute to insomnia and sleep apnea.
Sleep deprivation increases muscle tension and pain sensitivity, slows recovery from injuries, makes aches linger, and worsens mood, amplifying the perception of pain.
Environmental Toxins and Inflammation
Pollution, chemicals, and even mold exposure can stress your vagus nerve, lowering its tone and increasing inflammation. This can trigger muscle tension and pain, especially in the back or neck; disrupt gut health, which the vagus nerve relies on for optimal function; and amplify stress responses, worsening the feeling of pain.
These factors—stress, posture, inactivity, diet, toxins, and sleep issues—create overlapping risk profiles that can weaken vagal tone, ramp up inflammation, and lead to body pain. For example, chronic stress might tighten your neck muscles, while poor posture compresses the vagus nerve, and a bad diet fuels inflammation—creating a perfect storm for aches and pains.
Discovering the Benefits of Chiropractic Care- Video
The Science Behind Vagus Nerve Stimulation for Pain Relief
The vagus nerve’s pain-relieving powers are backed by robust scientific research. It’s part of the cholinergic anti-inflammatory pathway, where it releases acetylcholine to dampen inflammation, a major cause of pain. The inflammatory reflex is a centrally integrated physiological mechanism in which afferent vagus nerve signaling, activated by cytokines or pathogen-derived molecules, conveys signals to the brain and subsequent efferent vagus nerve activity suppresses peripheral inflammation.
Studies show that high vagal tone is linked to lower pain sensitivity and faster recovery from injuries. The vagus nerve regulates the dynamic interplay between cardiac and respiratory functions. Heart rate variability (HRV), which measures the intervals between heartbeats, captures the dynamic balance between sympathetic and parasympathetic inputs to the heart.
Research demonstrates that vagus nerve stimulation (VNS) can modulate vagal activity and neuro-immune communication, producing analgesic effects by projecting to many brain regions related to pain processing. The anti-inflammatory property of VNS contributes to its pain-inhibitory effects, making it particularly promising for chronic musculoskeletal pain conditions.
Chiropractic Care: Optimizing Vagus Nerve Function for Pain Relief
Chiropractic care is like a tune-up for your vagus nerve, helping it hit all the right notes to reduce pain and restore balance. By focusing on spinal alignment and muscle tension, chiropractors can stimulate the vagus nerve and improve vagal tone, which calms inflammation and eases body pain.
How Chiropractic Care Enhances Vagal Function
Spinal Adjustments: Misaligned vertebrae (subluxations) in the neck or upper back can compress the vagus nerve, reducing its function. Gentle chiropractic adjustments realign the spine, relieving pressure and boosting nerve signaling. The PulStar, for example, delivers rapid, low-force mechanical impulses to targeted spinal segments, offering precision that manual techniques can’t match. The vagus nerve interfaces closely with structures in the upper cervical spine—particularly around the atlas (C1) and axis (C2) vertebrae.
Myofascial Release: Chiropractors use soft-tissue techniques to release tight muscles and fascia, which can improve vagal tone by reducing tension around the nerve. This helps with conditions like myofascial pain syndrome, where trigger points cause widespread aches.
Reducing Inflammation: By improving nerve function and blood flow, chiropractic care helps the vagus nerve dial down inflammation, a key driver of chronic pain.
Stress Relief: Adjustments stimulate the parasympathetic system, lowering stress hormones and promoting relaxation, which can ease tension-related pain.
Research shows that chiropractic adjustments can improve vagal tone by reducing spinal stress, easing pain in conditions like myofascial pain syndrome. A literature review found that 88% of pediatric patients experienced a significant reduction in the frequency and severity of epileptic seizures following chiropractic care, potentially through vagus nerve stimulation mechanisms.
Acupuncture: Ancient Wisdom Meets Modern Neuroscience
Acupuncture is another powerful treatment for boosting vagal tone and easing pain. By inserting tiny needles into specific points on the body, acupuncture stimulates the nervous system, including the vagus nerve, to promote relaxation and healing.
How Acupuncture Stimulates the Vagus Nerve
Direct Vagus Nerve Stimulation: Certain acupuncture points, like those in the ear or neck, directly activate the vagus nerve, improving its tone and calming the body. Auricular acupuncture (ear acupuncture) involves needling specific points on the ear, and several of these points stimulate the vagus nerve through the auricular branch.
Pain Reduction: Acupuncture releases endorphins and other pain-relieving chemicals, reducing muscle tension and trigger point pain. Studies show that acupuncture can stimulate the vagus nerve to promote anti-inflammatory effects, transmitting signals that mediate anti-inflammatory responses in the spleen.
Inflammation Control: By boosting vagal tone, acupuncture helps the vagus nerve suppress inflammation, easing conditions like myofascial pain or fibromyalgia.
Key Acupuncture Points for Vagus Nerve Stimulation
Several acupuncture points can effectively stimulate the vagus nerve:
Conception Vessel 12 (CV 12): Located on the midline of the abdomen, used to stimulate the vagus nerve, promoting digestion and relaxation
Conception Vessel 17 (CV 17): Located in the center of the chest, it helps regulate the vagus nerve, improving respiratory function and reducing stress
Heart 7 (HT 7): Located on the wrist, powerful for stimulating the vagus nerve, promoting relaxation, and reducing anxiety
Stomach 36 (ST 36): Located on the leg, helps regulate the vagus nerve, promoting digestion and reducing stress
Pericardium 6 (PC 6): Located on the inner wrist, it activates the parasympathetic nervous system and increases vagal activity
Auricular points: The ear contains numerous points that can stimulate the vagus nerve, including the cymba conchae, the tragus, and the cavum conchae
Myofascial Release and the Vagus-Fascia Connection
The connection between fascia and the vagus nerve represents a fascinating frontier in pain management. Fascia is not static—it’s constantly evolving and adapting to influences including sustained postures, stress responses, and biochemical factors.
Fascia receptors communicate directly with both branches of the autonomic nervous system. When activated, the sympathetic nervous system releases neurotransmitters that can increase tension in fascia throughout the body. Chronic activation due to ongoing stress can lead to increased tone and stiffness in fascial structures.
Strong vagal tone helps counterbalance sympathetic-induced fascial tension. When the vagus nerve is properly engaged, it can facilitate the release of fascial restrictions that may have developed during chronic or traumatic stress. Myofascial release can stimulate the vagus nerve by releasing tension in the fascia, indirectly activating it and triggering a cascade of relaxation responses throughout the body.
Managing Myofascial Pain Syndrome Through Vagus Nerve Stimulation
Myofascial pain syndrome (MPS) manifests as discomfort due to taut bands and trigger points affecting muscles, tendons, ligaments, and fascia. This prevalent condition affects approximately 12% of the population, notably among individuals aged 30-50.
Recent research demonstrates that auricular vagus nerve stimulation (VNS) applied from both ears can significantly improve pain severity, trigger point sensitivity, grip strength, quality of life, and autonomic functions in MPS patients. The study found that adding VNS to ischemic compression and stretching exercises resulted in statistically higher improvements compared to conventional treatment alone.
Clinical trials are currently investigating the effects of vagus nerve stimulation on trapezius trigger points, recognizing that MPS is characterized by these hyperirritable spots in skeletal muscle, which are associated with pain, stiffness, and dysfunction.
Fibromyalgia and Vagus Nerve Dysfunction
Fibromyalgia, characterized by heightened central sensitization and dysregulated inflammatory responses, often poses significant challenges to traditional pharmacological treatments. Non-invasive vagus nerve stimulation presents a promising alternative, effectively targeting both peripheral and central inflammatory pathways.
Clinical studies support significant reductions in pain levels and improvements in fibromyalgia symptoms such as fatigue and anxiety. In fibromyalgia, VNS reduces pain intensity, enhances sleep quality, and improves overall well-being by suppressing pro-inflammatory cytokines and neuropeptides such as substance P and CGRP, along with normalizing autonomic dysfunction.
Current clinical trials are investigating transcutaneous vagus nerve stimulation in fibromyalgia patients. Researchers hypothesize that stimulating the auricular branch of the vagus nerve can lead to better pain control and quality of life by normalizing autonomic and immune system dysfunction.
Heart Rate Variability: The Window into Vagal Health
Heart rate variability (HRV) serves as a non-invasive marker that provides profound insight into vagal nerve activity, often termed vagal tone. HRV reflects the interplay between autonomic inputs and cardiac function by analyzing the fluctuations between successive heartbeats.
HRV is strongly associated with the body’s ability to adapt to metabolic demands and external challenges, making it an essential indicator of physiological resilience. Specific metrics, such as RMSSD (root mean square of successive differences) and high-frequency (HF) power, are particularly indicative of vagus nerve-mediated HRV, which reflects parasympathetic cardiac control.
Higher HRV levels, mediated by the vagus nerve, signify robust autonomic balance, emotional regulation, and cognitive function. These attributes enhance resilience to stress and disease, positioning vagus nerve-mediated HRV as a vital marker of overall well-being.
Lifestyle Strategies for Optimizing Vagus Nerve Health
Keeping your vagus nerve happy is like giving your body a daily dose of zen—and it can help prevent pain before it starts. Here are evidence-based lifestyle strategies to boost vagal tone and keep aches at bay:
Deep Breathing and Meditation
Slow, deep breathing directly stimulates the vagus nerve, boosting its tone and calming your body. Diaphragmatic breathing, where you breathe deep into your belly rather than taking shallow chest breaths, is particularly effective. The key is to keep your exhales longer than your inhales—this helps activate the vagus nerve and signals the parasympathetic nervous system to enter rest and digest territory.
Try the 4-7-8 breathing method: inhale for four seconds, hold for seven seconds, and exhale for eight seconds. This breathing exercise helps slow the heart rate and promotes a state of calmness.
Regular Exercise and Movement
Moderate exercise, like walking, yoga, or swimming, boosts vagal tone by stimulating the parasympathetic system. Research suggests that endurance and interval training stimulate the vagus nerve and control parasympathetic activity in the brain.
Yoga poses that focus on relaxation, such as Child’s Pose or Cat-Cow, can activate the vagus nerve. Yin yoga, a slower style where you hold each pose for three to five minutes, is particularly effective for vagus nerve stimulation. The combination of sustained poses and mindful breathing makes this practice effective for vagus nerve activation.
Anti-Inflammatory Nutrition
A literature review examining the role of nutrition on heart rate variability found several foods and nutrients associated with increased vagal tone:
Omega-3 fatty acids: Found in salmon, walnuts, and flaxseeds, these anti-inflammatory fats may be linked to vagus nerve activity
Mediterranean diet: Rich in anti-inflammatory compounds that support overall vagal function
Probiotic foods: Since gut bacteria affect the vagus nerve and brain, maintaining a diverse microbiome is vital. Include kimchi, yogurt, miso, kefir, tempeh, and kombucha
High-choline foods: Choline is a precursor to acetylcholine, the primary neurotransmitter of the parasympathetic nervous system. Include eggs, fish, nuts, and seeds
Prebiotic foods: Garlic, onions, chicory root, leeks, bananas, oats, and barley support beneficial gut bacteria
Quality Sleep Optimization
The vagus nerve plays a crucial role in sleep regulation, helping your body transition into a state of relaxation. Research shows that transcutaneous vagus nerve stimulation can improve sleep quality in patients with primary insomnia.
Aim for 7-9 hours of sleep nightly to support vagal tone. Create a bedtime routine that includes no screens 1 hour before bed, using blackout curtains or a sleep mask, and consider incorporating vagus nerve exercises like gentle humming or deep breathing before sleep.
Stress Management Techniques
Chronic stress tanks vagal tone, so implementing effective stress management strategies is crucial. Mindfulness practices like journaling, gratitude exercises, and meditation can help maintain healthy vagal function. Controlled laughter naturally creates rhythmic breathing and diaphragmatic movement that stimulates the parasympathetic nervous system.
Cold Exposure and Hydrotherapy
Cold exposure, such as splashing cold water on your face or taking brief cold showers, activates the vagus nerve and signals the body to relax. This technique can be particularly helpful as part of a pre-sleep routine or when you need to quickly activate your parasympathetic nervous system.
Posture Awareness and Ergonomics
Good posture keeps the vagus nerve free from compression. Use ergonomic chairs or standing desks to avoid slouching, and perform regular posture checks: ears over shoulders, shoulders over hips. This reduces muscle tension and supports vagal function, preventing pain.
Advanced Diagnostic Approaches
Modern healthcare is incorporating advanced diagnostic tools to assess vagal function and its relationship to pain. Heart rate variability testing can measure vagal tone, revealing if low tone is linked to chronic pain conditions. Functional assessments evaluate how well the nervous system, including the vagus nerve, is functioning.
Advanced imaging, like MRI and CT scans, can visualize spinal misalignments or soft-tissue issues that may compress the vagus nerve, contributing to pain. Lab tests can identify inflammation markers or nutritional deficiencies that impair vagal function and fuel pain.
These comprehensive approaches allow healthcare providers to create tailored treatment plans that not only relieve pain but also boost vagal tone, promoting long-term wellness.
Emerging Research and Future Directions
The field of vagus nerve research is rapidly expanding, with promising developments in non-invasive stimulation techniques. Recent studies have shown that vagus nerve stimulation can reduce inflammation in cardiovascular disease, leading to smaller infarct sizes and a lower incidence of ventricular arrhythmias during reperfusion.
Clinical trials are investigating vagus nerve stimulation for various chronic pain conditions, including an evaluation of 148 people with chronic lower back pain showing that vagus nerve stimulation halved pain in around 60% of users. The FDA has approved certain VNS devices for specific pain conditions, reinforcing the therapeutic potential of this approach.
Research continues to explore the synergistic effects of combining VNS with other therapeutic modalities, such as pharmacotherapy and psychotherapy, to enhance patient outcomes. The development of wearable devices for vagus nerve stimulation is making this therapy more accessible and practical for daily use.
When to Seek Professional Help
If you’re dealing with persistent pain, especially in your neck, back, or shoulders, or if stress, poor sleep, or digestive issues are piling on, it might be time to check in with a professional. Signs your vagus nerve needs help include chronic pain that doesn’t budge with rest or over-the-counter medications; frequent tension headaches or muscle knots; feeling wired but tired, with poor sleep or high stress; and digestive issues like bloating or sluggishness, which can signal vagal dysfunction.
Healthcare providers can use diagnostic tools like HRV tests to confirm if vagal tone is contributing to symptoms, guiding targeted treatment plans that may include chiropractic care, acupuncture, lifestyle modifications, and emerging vagus nerve stimulation therapies.
Conclusion
The vagus nerve stands as a remarkable biological system that bridges the gap between mind and body, offering unprecedented opportunities for natural pain relief and wellness optimization. As research continues to unveil the intricate connections between vagal function, inflammation, and pain perception, we’re discovering that this “wandering nerve” may hold keys to treating chronic pain conditions that have long challenged conventional medicine.
The evidence is clear: when the vagus nerve functions optimally, it serves as a powerful anti-inflammatory pathway, helping regulate pain signals, promote healing, and maintain the delicate balance between stress and relaxation. Conversely, when vagal tone is compromised by factors like chronic stress, poor posture, sedentary lifestyle, inflammatory diet, or sleep disruption, the body becomes more susceptible to chronic pain and inflammation.
The integration of traditional therapies like chiropractic care and acupuncture with the modern understanding of vagal function represents a paradigm shift in pain management. These approaches don’t just mask symptoms—they address underlying dysfunction in the body’s own regulatory systems. Meanwhile, simple lifestyle interventions, including proper breathing techniques, regular movement, anti-inflammatory nutrition, quality sleep, and stress management, can significantly enhance vagal tone and prevent pain before it starts.
As we move forward, the future of pain management increasingly points toward personalized, integrative approaches that harness the body’s innate healing mechanisms. The vagus nerve, with its extensive connections throughout the body and its powerful anti-inflammatory properties, represents a promising frontier in this evolution. Whether through professional treatments or daily self-care practices, optimizing vagal function offers a pathway to not just pain relief, but enhanced overall wellness and resilience.
Serious Note: This article provides educational insights into the vagus nerve and its role in pain management, but chronic pain or suspected vagal dysfunction should be addressed with professional medical care. Untreated issues can lead to long-term complications, so always consult a qualified healthcare provider for proper diagnosis and treatment.
El Paso Back Clinic®: Premier Wellness Chiropractic Care in El Paso, TX
Spine problems are evident in the model. A woman is in consultation with the doctor in the clinic.
At El Paso Back Clinic®, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, we’re dedicated to transforming lives through advanced chiropractic care and integrative wellness in El Paso, TX. Specializing in recovery from motor vehicle accidents (MVAs), sports injuries, and chronic conditions such as neuropathy, our team utilizes cutting-edge neuromusculoskeletal imaging and dual-scope diagnostics to identify the root causes of injuries. From whiplash to gastrointestinal trauma, we craft personalized plans blending spinal adjustments, nutrition, and therapies like acupuncture to restore mobility and vitality. With a focus on holistic healing and legal support for injury claims, we empower El Pasoans to live pain-free and thrive.
Personal Injuries and Their Impact in El Paso
Living in El Paso’s bustling community means navigating busy roads and an active lifestyle, where accidents—from car crashes to sports mishaps—can disrupt one’s health. MVAs, common on rainy I-10 days, often cause spinal misalignments, leading to sciatica or numbness (Jimenez, 2025a). Sports injuries, like joint strains and workplace falls, add to the toll, risking chronic issues like neuropathy if untreated (Mana.md, n.d.).
At El Paso Back Clinic®, Dr. Jimenez’s chiropractic expertise targets these musculoskeletal and nerve disruptions. Using advanced imaging, we link injuries to symptoms, ensuring precise care. Our integrative approach, which combines adjustments with wellness coaching, helps prevent long-term pain and includes legal documentation to support insurance claims for patients in El Paso.
Nerve Pain and Neuropathy Post-Collision
Car accidents frequently trigger nerve compression, causing tingling, burning, or weakness that mimics peripheral neuropathy. Even minor collisions in El Paso’s unpredictable weather can cause vertebrae to shift, potentially pinching nerves (Jimenez, 2025b). Our clinic employs EMG and dynamic X-rays to map these injuries, correlating crash forces to nerve damage for accurate diagnosis.
We use spinal decompression and laser therapy to relieve pressure and promote healing, with patients often seeing 40-50% symptom improvement in weeks (Miami Chiropractors, n.d.). Detailed biomechanical reports strengthen personal injury claims, ensuring fair compensation for El Paso residents.
Chiropractic Care for Joint and Ligament Injuries
Injuries like ACL tears from sports or MVA dashboard impacts require targeted restoration. At El Paso Back Clinic®, we realign joints, boost circulation, and strengthen muscles to speed recovery without surgery (Jimenez, 2025c). Dr. Jimenez’s functional assessments prevent compensatory patterns, vital for El Paso’s athletes.
We integrate acupuncture and custom orthotics, helping patients resume activities in six months, rather than a year. Nutritional support, like collagen-rich diets, enhances ligament repair, tailored to El Paso’s active community.
Five Musculoskeletal Challenges We Address
Accidents hit muscles and bones hard. Our chiropractic team tackles five common issues:
Neck and Back Pain: Whiplash from MVAs causes stiffness; gentle adjustments restore motion (Jimenez, 2025d).
Sciatica: Pinched nerves from disc issues ease with traction therapy.
Joint Inflammation: Post-injury arthritis responds to ultrasound and anti-inflammatory nutrition.
Sports Strains: Overuse injuries can be effectively treated through myofascial work and gait analysis.
These protocols, customized for El Pasoans, cut recurrence by half, blending wellness education for lasting health.
Spinal Misalignment: Recovery After Crashes
El Paso’s slick roads amplify MVA risks, often misaligning spines and compressing discs, leading to radiating pain (Jimenez, 2025a). We utilize high-velocity adjustments and flexion-distraction techniques to realign the vertebrae, paired with massage to relax the muscles.
Dr. Jimenez’s imaging links crash dynamics to disc damage, guiding non-surgical plans that preserve mobility in 70% of cases (Knecht Chiropractic, n.d.). Legal reports detail injury causation, supporting the claims of El Paso patients.
Reducing Inflammation for Pain Relief
Inflammation fuels post-injury pain. Our chiropractic care enhances lymphatic drainage via soft-tissue therapy and cryotherapy, breaking the cycle (Jimenez, 2025e). Patients adopt home strategies, such as taking turmeric supplements, which can reduce swelling by 40% (Miami Chiropractors, n.d.).
For workers’ compensation cases, we monitor biomarkers, aligning treatments with recovery goals to help El Paso workers return to their feet.
Cyclist Recovery After Bike-MVA Collisions
Biking on El Paso’s scenic trails poses risks from urban traffic, which can lead to fractures or nerve injuries. Our integrative care includes bike-fit corrections and vestibular training for balance (Jimenez, 2025f). Cyclists return to riding in three months, supported by endurance nutrition and legal advocacy.
Massage Therapy for MVA Trauma Healing
MVAs cause soft-tissue damage, from bruises to adhesions. Massage therapy, paired with adjustments, boosts circulation and endorphins, reducing whiplash recovery time by 30% (Jimenez, 2025). We progress from gentle strokes to deep tissue, documenting for El Paso insurance claims.
Spinal Trauma from 18-Wheeler Accidents
Semi-truck crashes deliver intense force, fracturing vertebrae or tearing ligaments. We use dynamic imaging to assess damage, guiding bracing and neuromodulation (Jimenez, 2025h). Legal reports link crash mechanics to injuries, aiding settlements for El Paso patients.
Nutrition for Tissue Repair Post-MVA
Injured tissues require nutrients such as protein and antioxidants. Dr. Jimenez designs diets with salmon and berries, using genetic insights to optimize healing (Jimenez, 2025i). This reduces fibrosis, strengthening tissues for El Paso’s active residents.
Durable Medical Equipment for Recovery
Following a motor vehicle accident (MVA), tools such as TENS units or cervical collars can support healing. We select evidence-based equipment, such as ergonomic chairs, to offload spines (Jimenez, 2025). Tele-rehab ensures compliance, with invoices bolstering El Paso claims.
Comprehensive Musculoskeletal Recovery
MVAs strain muscles and joints, from sprains to dislocations. Our pain mapping and multi-modal care—adjustments, PT, mindfulness—restore 80% function in six weeks (Jimenez, 2025k). Legal narratives ensure fair compensation.
Whiplash-Associated Disorders (WAD) Recovery
WAD from crashes causes neck pain or dizziness. We use Doppler ultrasound for vascular checks and treat with mobilization for 90% relief (Jimenez, 2025). Immediate post-accident icing and evaluations ensure thorough El Paso claims.
Gastrointestinal Injuries from MVAs
Car accidents can disrupt digestion, causing nausea or organ strain. Our integrative care, which includes visceral manipulation and nutrition, restores gut health, backed by legal support for claims (Jimenez, 2025).
Why Choose El Paso Back Clinic®?
Our team, led by Dr. Jimenez, combines chiropractic precision with medical expertise, utilizing tools such as digital motion X-rays. We offer acute-to-chronic care, transparent billing, and testimony for legal cases. Patients reduce their reliance on medication, regaining vitality through holistic plans tailored for El Paso’s vibrant community.
Learn about effective chiropractic care methods for managing nerve damage from gluten and improving your overall well-being.
Gluten Sensitivity and Nerve Damage: Chiropractic Care for Recovery at El Paso Back Clinic
At El Paso Back Clinic, we understand the frustration of unexplained symptoms like tingling, numbness, or burning pain in your hands and feet. These could point to nerve damage tied to gluten sensitivity—a condition affecting many but often overlooked. If eating bread, pasta, or other gluten-containing foods leaves you feeling off, you might be dealing with non-celiac gluten sensitivity (NCGS) or even early neuropathy. The good news? You don’t need surgery or heavy medications to find relief. Our team, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, specializes in nonsurgical solutions, including chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine, to reduce nerve damage, promote natural healing, and prevent long-term complications.
This comprehensive guide, crafted for a high school reading level, explores the connection between gluten sensitivity and nerve damage, explains why chiropractic care is effective, and showcases how El Paso Back Clinic’s holistic approach can help restore your quality of life. With over 5,000 words of SEO-optimized content, we’ll provide clinical insights, patient success stories, and actionable steps, all backed by research and Dr. Jimenez’s expertise. Let’s explore how we can help you heal naturally.
Understanding Gluten Sensitivity: More Than a Gut Issue
Gluten, a protein in wheat, barley, and rye, is a staple in foods like pizza, cereal, and beer. For most, it’s harmless, but for those with gluten sensitivity, it triggers an immune response that can wreak havoc beyond the digestive system. Non-celiac gluten sensitivity (NCGS) affects up to 6% of the population, causing symptoms that mimic those of other conditions, making diagnosis challenging (Cárdenas-Torres et al., 2021).
Unlike celiac disease, which damages the small intestine, NCGS can manifest as neurological symptoms, including peripheral neuropathy—nerve damage causing tingling, pain, or weakness. At El Paso Back Clinic, we see patients who’ve struggled with these issues for years, often unaware that gluten is the culprit. Common signs include:
Bloating, gas, or irregular digestion.
Skin rashes or persistent itching.
Headaches or brain fog affecting focus.
Joint pain or muscle stiffness.
Nerve issues like numbness or burning sensations.
These symptoms can escalate, leading to chronic discomfort if untreated. Research shows NCGS can trigger neurological dysfunction through inflammation, impacting the gut-brain axis (Mitsikostas & Di Luca, 2022).
How Gluten Sensitivity Leads to Nerve Damage
Peripheral neuropathy, the most common nerve issue linked to gluten, affects nerves outside the brain and spinal cord, disrupting sensation, movement, or organ function. Here’s how gluten sensitivity contributes:
Autoimmune Response: Gluten can prompt antibodies to attack nerve cells or the myelin sheath, the protective nerve coating, similar to mechanisms in multiple sclerosis (Ludvigsson et al., 2013, as cited in El Paso Back Clinic, n.d.).
Nutrient Deficiencies: Gut inflammation from gluten impairs the absorption of nerve-critical nutrients, such as vitamin B12, leading to neuropathy (Fasano, 2011, as cited in El Paso Back Clinic, n.d.).
Systemic Inflammation: Chronic inflammation from gluten weakens the blood-brain barrier, allowing toxins to irritate nerves (Hadjivassiliou et al., 2016, as cited in Cárdenas-Torres et al., 2021).
Sensory Neuron Damage: Gluten-induced inflammation can directly harm sensory nerves, causing pain or tingling (Mitsikostas & Di Luca, 2022).
Studies indicate celiac patients are 2.5 times more likely to develop neuropathy, and up to 30% of NCGS patients report neurological symptoms (Ludvigsson et al., 2013; Fasano, 2011). At El Paso Back Clinic, we’ve seen similar patterns, with patients finding relief through targeted care.
Recognizing Neuropathy Symptoms
Early signs include:
Tingling or numbness in fingers or toes.
Burning pain, especially at night.
Sensitivity to light touch.
Muscle weakness affecting grip or balance.
Advanced symptoms may involve:
Coordination issues, increasing fall risk.
Sharp, electric-shock-like pains.
Autonomic issues like irregular heart rate or digestion problems.
These overlap with conditions like diabetes, so professional diagnosis is vital. Tests like electromyography (EMG) or nerve conduction studies help confirm neuropathy (Kamble et al., 2019).
Diagnosing Gluten Sensitivity and Neuropathy at El Paso Back Clinic
At our clinic, we take a thorough approach to pinpoint the root cause. Dr. Jimenez and our team use:
Blood Tests: To detect inflammation or celiac-related antibodies.
Gluten Challenge: Supervised reintroduction of gluten to monitor symptoms.
Neurological Exams: EMG and nerve conduction tests to assess nerve function.
Nutritional Screening: Checking for deficiencies like B12 that fuel neuropathy.
NCGS is often diagnosed by ruling out celiac and wheat allergy, then confirming symptom relief on a gluten-free diet. Our integrative approach ensures accurate, personalized care (Cárdenas-Torres et al., 2021).
Why Chiropractic Care Works: Clinical Insights
Chiropractic care is a cornerstone at El Paso Back Clinic for addressing gluten-related neuropathy. Spinal misalignments, or subluxations, can compress nerves, worsening inflammation and pain. Our adjustments, guided by Dr. Jimenez’s 30+ years of experience, target these issues to restore nerve function.
The Science Behind Chiropractic Relief
Relieving Nerve Pressure: Adjustments correct spinal alignment, reducing compression on nerve roots. This enhances blood flow and nutrient delivery, critical for nerve repair (Jimenez, n.d.a).
Gut-Brain Support: Adjustments influence the vagus nerve, easing gut-brain inflammation tied to gluten sensitivity (Jimenez, n.d.b).
Research supports chiropractic for neuropathy. A study showed spinal manipulation reduced pain and improved mobility in peripheral neuropathy patients (Seyedizadeh et al., 2020). Dr. Jimenez notes, “Our goal is to remove barriers to healing, letting the body do what it does best” (Jimenez, n.d.a).
Dr. Alexander Jimenez: Leading Integrative Care in El Paso
Dr. Alexander Jimenez, DC, APRN, FNP-BC, brings unparalleled expertise to El Paso Back Clinic. Board-certified in family practice and functional medicine, he combines chiropractic, nutrition, and wellness to treat neuropathy holistically. His philosophy, shared on LinkedIn, emphasizes patient education: “Knowledge transforms pain into progress” (Jimenez, n.d.c).
Dr. Jimenez’s Approach
Comprehensive Assessments: Using genetics, lifestyle, and diagnostic tools to tailor care.
Precision Adjustments: Targeting nerve roots affected by gluten inflammation.
Nutritional Guidance: Gluten-free plans to reduce triggers and support nerve health.
At our Neuropathy Center, Dr. Jimenez integrates “Neuro-Gen” supplements with chiropractic care, seeing patients like Maria, a 45-year-old teacher, reduce tingling by 80% in three months through adjustments and diet changes.
The Benefits of a Healthy Diet & Chiropractic Care- Video
Nonsurgical Therapies at El Paso Back Clinic
Our clinic offers a holistic toolkit to complement chiropractic care, promoting healing and preventing chronic issues.
Targeted Exercises
Low-impact exercises enhance circulation and nerve function:
Balance Training: One-leg stands to improve coordination.
Nerve Glides: Gentle stretches to free trapped nerves.
Aerobic Movement: Engaging in daily walks helps oxygenate tissues.
Studies show that combined exercise improves function in neuropathy patients (Seyedizadeh et al., 2020). Dr. Jimenez advises, “Start small, stay consistent—your nerves will thank you.”
Massage Therapy
Massage relieves muscle tension that compresses nerves, boosting circulation.
Benefits: Reduces pain, lowers stress hormones.
Frequency: Weekly 45-minute sessions.
Research links massage to better pain control in neuropathic conditions (Hadjivassiliou et al., 2016).
Acupuncture
Our acupuncturists use precise needle placements to reduce inflammation and stimulate nerve repair.
How It Helps: Enhances regeneration, per neuropathic pain studies (Finnerup et al., 2020).
Integration: Complements chiropractic for faster results.
Integrative Medicine
We combine chiropractic, nutrition, and supplements to address gluten sensitivity and neuropathy. Functional medicine tests guide customized plans, preventing long-term damage (Jimenez, n.d.b).
Building a Gluten-Free Lifestyle with El Paso Back Clinic
A gluten-free diet is critical for managing neuropathy. A 2010 Neurology study showed dietary changes stabilized nerve symptoms (El Paso Back Clinic, n.d.).
Foods to Include and Avoid
Category
Include
Avoid
Grains
Quinoa, rice, certified GF oats
Wheat, barley, rye
Proteins
Eggs, fish, nuts
Breaded meats
Veggies/Fruits
Fresh produce
Processed sauces
Snacks
Popcorn, fruit
Cookies, crackers
Practical Tips
Check labels for “gluten-free” certification.
Prep meals with simple, whole foods.
Ask restaurants about cross-contamination risks.
Our nutritionists recommend B vitamins to support nerve health, guided by testing.
Success Stories from El Paso Back Clinic
Tom, a 52-year-old mechanic, had burning foot pain from gluten neuropathy. After six weeks of Dr. Jimenez’s program—adjustments, acupuncture, and gluten-free eating—his pain dropped significantly, letting him work comfortably.
Sarah, 38, overcame brain fog and tingling with our combined chiropractic, massage, and exercise plan. “The team listened and tailored everything to me,” she shares. These stories highlight our commitment to clear communication and personalized care.
Follow a tailored plan with chiropractic, exercises, and diet.
Track symptoms in a journal for progress.
Early intervention preserves mobility and comfort.
Conclusion: Reclaim Your Health with El Paso Back Clinic
Gluten sensitivity and nerve damage can disrupt your life, but El Paso Back Clinic offers hope through chiropractic care, targeted therapies, and integrative medicine. Dr. Jimenez’s expertise ensures you heal naturally, without surgery. As he says, “We empower your body to heal itself” (Jimenez, n.d.a). Visit elpasobackclinic.com or call 915-850-0900 to start your journey to relief today.
References
Aljada, B., Zohni, A., & El-Matary, W. (2021). The Gluten-Free Diet for Celiac Disease and Beyond. Nutrients, 13(11), 3993. https://pubmed.ncbi.nlm.nih.gov/34836247/
Cárdenas-Torres, F. I., Cabrera-Chávez, F., Figueroa-Salcido, O. G., & Ontiveros, N. (2021). Non-Celiac Gluten Sensitivity: An Update. Medicina (Kaunas, Lithuania), 57(6), 526. https://pubmed.ncbi.nlm.nih.gov/34073654/
Finnerup, N. B., Attal, N., Haroutounian, S., McNicol, E., Baron, R., Dworkin, R. H., Gilron, I., Haanpää, M., Hansson, P., Jensen, T. S., Kamerman, P. R., Lund, K., Moore, A., Raja, S. N., Rice, A. S., Rowbotham, M., Sena, E., Siddall, P., Smith, B. H., & Wallace, M. (2015). Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. The Lancet. Neurology, 14(2), 162–173. https://pubmed.ncbi.nlm.nih.gov/25575710/
Hadjivassiliou, M., Rao, D. G., Grìnewald, R. A., Aeschlimann, D. P., Sarrigiannis, P. G., Hoggard, N., Aeschlimann, P., Mooney, P. D., & Sanders, D. S. (2016). Neurological Dysfunction in Coeliac Disease and Non-Coeliac Gluten Sensitivity. The American journal of gastroenterology, 111(4), 561–567. https://pubmed.ncbi.nlm.nih.gov/26832652/
Jimenez, A. (n.d.a). Home. Injury Specialists. Retrieved September 15, 2025, from https://dralexjimenez.com/
Jimenez, A. (n.d.c). Dr. Alexander Jimenez, DC, APRN, FNP-BC, IFMCP, CFMP, ATN ♛. LinkedIn. Retrieved September 15, 2025, from https://www.linkedin.com/in/dralexjimenez/
Kamble, N., Shukla, D., & Bhat, D. (2019). Peripheral Nerve Injuries: Electrophysiology for the Neurosurgeon. Neurology India, 67(6), 1419–1422. https://pubmed.ncbi.nlm.nih.gov/31857526/
Mitsikostas, D. D., Moka, E., Orrillo, E., Aurilio, C., Vadalouca, A., Paladini, A., & Varrassi, G. (2022). Neuropathic Pain in Neurologic Disorders: A Narrative Review. Cureus, 14(2), e22419. https://pubmed.ncbi.nlm.nih.gov/35345699/
Rosenberger, D. C., Blechschmidt, V., Timmerman, H., Wolff, A., & Treede, R. D. (2020). Challenges of neuropathic pain: focus on diabetic neuropathy. Journal of neural transmission (Vienna, Austria: 1996), 127(4), 589–624. https://pubmed.ncbi.nlm.nih.gov/32036431/
Seyedizadeh, S. H., Cheragh-Birjandi, S., & Hamedi Nia, M. R. (2020). The Effects of Combined Exercise Training (Resistance-Aerobic) on Serum Kinesin and Physical Function in Type 2 Diabetes Patients with Diabetic Peripheral Neuropathy (Randomized Controlled Trials). Journal of diabetes research, 2020, 6978128. https://pubmed.ncbi.nlm.nih.gov/32215272/
Sciatic Nerve Health at El Paso Back Clinic: Holistic Healing Solutions
The sciatic nerve is essential for movement and sensation, stretching from the lower back through the legs as the body’s largest nerve. When irritated or compressed, it can cause sciatica—sharp pain, numbness, or tingling that radiates down the leg. At El Paso Back Clinic® in El Paso, TX, we specialize in helping patients overcome sciatic nerve issues through expert chiropractic care and integrative therapies.
This article explores the sciatic nerve’s structure, made of axon bundles wrapped in protective connective tissue, and how El Paso Back Clinic’s chiropractic techniques relieve nerve pressure. We’ll also highlight our integrative approach, combining massage, physical therapy, acupuncture, and nutrition to promote natural healing. Led by Dr. Alexander Jimenez, DC, APRN, FNP-C, our clinic addresses injuries from work, sports, personal accidents, and motor vehicle accidents (MVAs) with personalized, evidence-based care.
Whether you’re managing sciatica or aiming to prevent nerve problems, El Paso Back Clinic offers solutions to help you regain mobility and live pain-free.
Understanding the Sciatic Nerve
The sciatic nerve originates from the L4 to S3 nerve roots in the lower back, runs through the buttocks, and extends down each leg, controlling muscles and sending sensations from the thighs, calves, and feet. Compression from a herniated disk, tight muscles, or injury can trigger sciatica, disrupting daily activities like walking or sitting.
At El Paso Back Clinic, we focus on addressing the root causes of sciatica using non-invasive methods to support the body’s natural healing process, helping patients return to an active lifestyle.
Sciatic Nerve Structure: Axons and Protective Layers
The sciatic nerve is a complex network of neurons, each with a long fiber called an axon that transmits electrical signals. These axons are organized into bundles called fascicles, supported by layers of connective tissue:
Endoneurium: Wraps each axon and its myelin sheath, which speeds up signals and protects the nerve fiber.
Perineurium: Encases each fascicle, regulating the environment to maintain signal efficiency.
Epineurium: The outer layer surrounds the entire nerve, providing strength and flexibility.
These layers, which can comprise up to half of the nerve’s volume, ensure durability but can cause issues if they become inflamed or scarred, trapping axons and triggering pain. El Paso Back Clinic’s treatments aim to reduce inflammation and restore nerve function.
Causes of Sciatic Nerve Issues
Sciatica often results from nerve compression due to:
Herniated disks: Bulging spinal disks pressing on nerve roots.
Spinal stenosis: Narrowed spinal canals crowd the nerves.
Piriformis syndrome: A Tight piriformis muscle pinching the nerve.
Injuries: Trauma from work, sports, falls, or MVAs.
Our clinic sees these issues in patients with repetitive job strains, athletic injuries, or car accidents. Accurate diagnosis is key to effective treatment.
Chiropractic Care at El Paso Back Clinic: Relieving Nerve Pressure
Chiropractic care is at the heart of our approach at El Paso Back Clinic. Dr. Alexander Jimenez and our team use precise spinal adjustments to realign vertebrae and reduce pressure on the sciatic nerve. The procedure alleviates pain and improves mobility by addressing misalignments that cause disc bulging or muscle tension.
For example, a patient with sciatica from a slipped disk may receive lumbar adjustments to create space for the nerve. Dr. Jimenez uses advanced imaging like X-rays and MRIs to identify the issue, ensuring targeted care. His dual expertise as a chiropractor and nurse practitioner allows for comprehensive assessments, combining spinal exams with neurological testing.
Research supports the effectiveness of chiropractic care for chronic pain over medications alone (Ideal Spine, n.d.). For a delivery driver with sciatica from heavy lifting, Dr. Jimenez might use spinal decompression to gently stretch the spine, paired with rehab exercises to prevent recurrence.
Integrative Care: A Holistic Approach to Nerve Health
El Paso Back Clinic embraces integrative medicine, combining chiropractic care with massage therapy, physical therapy, acupuncture, and nutrition for optimal results. Our team, including chiropractors, therapists, and nutritionists, collaborates to create personalized treatment plans.
Massage Therapy: Techniques like deep tissue and trigger point massage relax tight muscles, such as the piriformis, reducing nerve compression. Patients often report less numbness and better movement.
Physical Therapy: Exercises like the McKenzie method or core strengthening stabilize the spine and improve flexibility, guided by our skilled therapists.
Acupuncture: Needle placements reduce inflammation and stimulate the body’s natural pain relief mechanisms, thereby enhancing chiropractic outcomes.
Nutrition Counseling: We recommend nerve-supporting nutrients like vitamin B12 (found in fish and eggs) for myelin repair and alpha-lipoic acid (in spinach) to reduce inflammation (RxWellness, n.d.; Verywell Health, n.d.).
This approach aligns with evidence-based principles of integrative care (NCCIH, n.d.), promoting healing while minimizing reliance on medications.
Dr. Jimenez’s Expertise: Healing Diverse Injuries
With over 25 years of experience, Dr. Alexander Jimenez leads El Paso Back Clinic with a dual perspective as a DC and APRN. His clinic uses advanced tools like EMG, MRI, and functional assessments to diagnose sciatica and related injuries.
Work Injuries: For a construction worker with sciatica from repetitive bending, Dr. Jimenez combines adjustments with B-vitamin supplements and ergonomic advice to prevent further strain.
Sports Injuries: A soccer player experiencing leg pain receives decompression therapy and acupuncture, supplemented by balance exercises to help restore function.
Personal Injuries: A fall victim benefits from massage and PT to reduce swelling, with detailed documentation for insurance claims.
MVAs: Car accident patients get full-body scans to connect whiplash to sciatica, with legal reports to support recovery and claims.
Dr. Jimenez’s approach, detailed on dralexjimenez.com, focuses on root-cause treatment and patient empowerment through holistic care.
Supporting Legal and Medical Needs
Injury cases often require legal or insurance documentation to support claims. El Paso Back Clinic provides thorough records, from initial X-rays to recovery progress, using pain scales and range-of-motion tests. For MVA patients, we collaborate with attorneys to streamline paperwork, ensuring patients focus on healing.
Preventing Long-Term Nerve Issues
Our integrative care promotes natural healing by improving blood flow to axons, strengthening supporting muscles, and reducing inflammation through nutrition. Regular checkups and personalized therapy goals help prevent chronic pain or arthritis, keeping patients active.
Choose El Paso Back Clinic for Sciatic Nerve Care
Located in El Paso, TX, El Paso Back Clinic® offers a welcoming environment where licensed professionals deliver tailored care. Our services—chiropractic, physical therapy, acupuncture, and nutrition—work together to relieve sciatica and boost wellness. Contact us at 915-850-0900 or visit our blog for more insights.
With El Paso Back Clinic, you’re investing in a healthier, pain-free future.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine