Can physical therapy help individuals with a pinched nerve in the neck?
Pinched Nerve In The Neck
A pinched nerve in the neck can cause pain, numbness, and weakness that extends through the neck, shoulder, and arm. (American Academy of Orthopaedic Surgeons, 2024) Over-the-counter pain medications, resting the muscles, and gentle stretching can help. However, if you’re still in pain after a few days, see a healthcare provider. Common treatments include:
Rest
Over-the-counter (OTC) pain meds
Physical therapy
Steroid injections
Wearing a neck collar
Surgery is rarely needed, but it can provide relief if other treatments don’t help. Most of the time, a pinched nerve resolves within days or weeks.
Sharp pain that extends into the shoulder and arm.
The pain worsens, or there is a shooting sensation when turning the head.
Tingling or feeling of pins-and-needles in the fingers or hand.
Weakness in the arm, shoulder, or hand.
Numbness or loss of feeling.
Often, these symptoms occur only on one side. Some find their pain less when they lift their hand onto their head, which can relieve pressure on the nerve.
Causes
The cervical spine is the spinal cord area around the neck. It’s made up of seven vertebrae. Nerves branch off the spinal cords in the spaces between the vertebrae. Nerve compression occurs when the space between two vertebrae is reduced, putting pressure on the nerve, pinching it, and causing pain. Pinched nerves develop from age because the spinal discs between the vertebrae become compressed over time. Age causes about 70% to 80% of nerve compression. Other factors that cause pinched nerves include: (Harvard Health Publishing, 2021)
Degenerative disc disease
A herniated disc
Injuries like car accidents falls, or other trauma to the spine
Find a comfortable position and try to allow the muscles in your neck to relax and rest.
Heat or Ice
Warmth and coolness can relieve pain and inflammation.
Use a warm or cool compress for 15 minutes at a time.
Over-The-Counter Pain Medications
Pain medications, including nonsteroidal anti-inflammatory drugs (NSAIDs), can help bring relief.
Treatment for Severe Symptoms
If pain doesn’t resolve within a few days, or if it is so bad that you can’t go about daily activities, it’s recommended to see a healthcare provider. They can diagnose a pinched nerve after a physical exam and may also recommend imaging, including an X-ray, CT scan, MRI, or EMG, to reveal what’s causing the symptoms. After diagnosing the condition, the healthcare provider will develop a personalized treatment plan, which may include the following (Harvard Health Publishing, 2021)
Physical Therapy
Physical therapy can help build strength and flexibility in the neck.
This is especially important if there is frequent nerve pain in the same spot.
Cervical Collar
A soft cervical collar is a brace that fits around the neck.
It supports your head so the neck muscles can relax, facilitating healing.
The collar can also keep the head from turning in painful ways.
Oral Corticosteroids
Oral steroids like prednisone can help reduce inflammation.
If inflammation or swelling in the neck puts more pressure on the nerve, they can help.
Steroid Injections
Steroid shots right into the painful tissue reduce inflammation right away.
Muscle Relaxers
These medications keep the muscles in the neck from seizing up.
As the muscles relax, this brings pain relief.
Narcotic Pain Medications
Narcotic pain medications can be used short-term by individuals who have severe pain.
A healthcare provider will inform the patient of the benefits and drawbacks of these medications, which include opiates.
Hold for 20 seconds, then return to a neutral position.
Do this five times.
Eyes to Sky
Lean your head back and look toward the sky.
Hold for 20 seconds, then return to your starting position.
Do this five times.
Side to Side
Turn your head to the right as far as possible, bringing your chin in line with your shoulder.
Hold for 20 seconds, then turn as far as possible toward the left.
Repeat four times.
Ear to Shoulder
Bring your ear down toward your shoulder.
Hold for 20 seconds, then repeat the exercise on the other side.
Alternate between the right and left, stretching each side five times.
While it’s normal for exercises to hurt from stretching the muscles, they should never hurt more than a five on a pain scale of 1 to 10. If they do, stop exercising (National Health Service, 2025)
Healing Time
Healing and recovery depend on the severity of the injury. Some individuals find that the pain from a pinched nerve goes away in days, while for others, it can last for weeks. The pain goes away and then returns. If pain doesn’t go away with the conservative treatments or lasts more than a few days, talk with a healthcare provider or return for a second visit. Rarely do individuals need surgery to bring pain relief. The healthcare provider will discuss whether surgery is the best option and what to expect regarding pain relief. (American Academy of Orthopaedic Surgeons, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Revitalize and Rebuild with Chiropractic
References
American Academy of Orthopaedic Surgeons. OrthoInfo. (2024). Cervical radiculopathy (pinched nerve). https://orthoinfo.aaos.org/en/diseases–conditions/cervical-radiculopathy-pinched-nerve/
Harvard Health Publishing. Publishing, H. H. (2021). Treating a pinched nerve. https://www.health.harvard.edu/pain/treating-a-pinched-nerve
National Institute of Neurological Disorders and Stroke. (2025). Pinched Nerve Definition. Retrieved from https://www.ninds.nih.gov/health-information/disorders/glossary-neurological-terms#-P-
National Health Service. Service, N. H. (2025). Exercises for neck problems. https://www.nhsinform.scot/illnesses-and-conditions/muscle-bone-and-joints/neck-and-back-problems-and-conditions/exercises-for-neck-problems
Could individuals who are having headaches with neck pain need emergency treatment or need to get started with sustained physical therapy?
Headaches and Neck Pain
Headaches and neck pain are two very common symptoms. They often occur together and signal common health issues, including fatigue, sinus headaches, and migraines. The combination can also occur due to serious health issues such as a concussion or meningitis. Causes of headaches with neck pain range from various causes, such as not getting enough sleep, having the neck in an awkward position, or having a hangover, to life-threatening issues like fluid buildup in the brain. It is recommended that individuals see a healthcare provider as soon as possible to rule out any life-threatening issues. Discuss the symptoms of neck pain with headache, what can cause these symptoms, and discuss treatment and prevention.
Symptoms
Symptoms are similar to what they feel like when they occur alone. Headache can present as:
A feeling of fullness in the head
Head soreness
Sharp head pain
Throbbing head pain
Pounding head pain
Neck pain can present as:
Pain in the back of the neck
Pain and/or aching of the upper back and/or shoulders
Associated Symptoms
Additional symptoms are common. Symptoms associated with headaches and neck pain include:
Neck stiffness
Trouble concentrating
Exhaustion or sleepiness
Aching throughout the body
Nausea
Dizziness
Vertigo – feeling like the room is spinning.
Photophobia – discomfort when looking at bright lights.
A feeling of numbness or tingling down the arm
Generally, associated symptoms suggest a more severe cause and can help a healthcare provider make a diagnosis.
Emergency Help
New symptoms of headache or neck pain can indicate a serious condition. If you develop these symptoms together, get prompt medical attention.
Causes
There are a variety of medical conditions that can cause headaches and neck pain. Both of these conditions are caused by irritation of sensory nerve fibers. Sometimes, head or neck pain can spread to other areas because the sensory nerves of these structures are so close together. (Côté P. et al., 2019) Additionally, a medical condition like an infection can affect the other due to proximity. Causes of headaches with neck pain include:
Headaches
Sinus headaches, tension headaches, and cervicogenic headaches are usually associated with head pain, but they can also involve neck pain. (Côté P. et al., 2019)
Migraine
Migraines are commonly associated with headaches and often cause neck pain as well.
In addition, they can cause nausea and body aches.
Fatigue
Being tired commonly leads to temporary headaches and neck pain until thorough rest is achieved.
Alcohol Consumption and/or a Hangover
For many, drinking can trigger a headache.
This is a common migraine trigger, but it can also trigger headaches for those who don’t have migraines.
Muscle Strain
Prolonged or recurrent positions that strain the neck muscles, like lifting or sitting at a desk, can cause aching or pain that involves both the head and neck. (Houle M. et al., 2021)
Injuries
Trauma such as whiplash or falling can cause soreness in the head and neck.
Bruises or other injuries may be present.
Severe injuries can cause damage to the skull, brain, spine, spinal nerves, or spinal cord.
Concussion
A concussion often causes trouble concentrating, persistent headaches, and neck pain.
Usually, these symptoms improve within a few weeks after a mild concussion.
Meningitis
Inflammation or infection of the lining around the brain and spinal cord causes pain or tenderness in the head, back, and neck.
Neck stiffness and fever are commonly associated symptoms.
Pinched Nerve
Arthritis is a common cause of pressure on spinal nerves.
A pinched nerve in the upper spine can cause pain in the head and neck and tingling down the arm.
Herniated Disc
Degenerative arthritis or trauma can cause a spinal disc to press on a nerve and possibly on the spinal cord.
This may cause loss of sensation or weakness of the arm.
Subarachnoid Hemorrhage
This is a serious condition caused by bleeding of a blood vessel in the brain.
Irritation and inflammation can cause severe head and neck pain, possibly with seizures and loss of consciousness.
Hydrocephalus
Fluid can accumulate around the brain, causing pain-inducing pressure.
Causes include obstruction of cerebrospinal fluid flow due to brain tumors, brain infections, or congenital malformations. (Langner S. et al., 2017)
Increased Intracranial Pressure
Pressure on the brain and the brain’s blood vessels can cause pain.
Causes of pressure within the skull include hydrocephalus, head trauma, brain tumors, or swelling from a stroke.
Severe cases can cause lethargy or loss of consciousness.
Brain or Spine cancer
Cancer of the brain or within the spine can cause pain affecting the head and neck, often with other symptoms, like loss of vision.
Treatment
Talk to a healthcare provider about the following treatments. Treating headaches with neck pain includes methods that address symptoms and methods that treat the underlying cause. The medications used for headaches with neck pain often reduce both symptoms, but this depends on the cause. Treatments that can relieve both headaches and neck pain when they occur together include:
Getting proper sleep to alleviate fatigue.
Rest and rehabilitation after a concussion or another injury.
Physical therapy to keep muscles flexible and relaxed.
Fluids for meningitis treatment and antibiotics for bacterial meningitis.
Surgical procedures for a tumor or subarachnoid hemorrhage.
A surgical procedure to relieve hydrocephalus.
Headache Treatment
You can do a few things to relieve your headaches, and although they won’t directly take away your neck pain, your headache relief might also decrease your neck pain. These include:
Avoiding loud noises
Cranial massage
Applying gentle cranial pressure
Avoiding bright lights as much as possible
Using specialized migraine sunglasses
Neck Pain Treatment
Some treatments that can specifically treat neck pain include:
Injury Medical Chiropractic and Functional Medicine Clinic
Knowing whether a serious problem is causing headaches and neck pain can be difficult. The more dangerous conditions don’t necessarily cause more severe pain. This is why getting medical attention is crucial if you have these symptoms together. If you frequently have both headaches and neck pain, it can have a substantial impact on your quality of life. There are ways to manage the symptoms, including preventative measures such as physical therapy, exercises, and avoiding triggers. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Tension Headaches
References
Côté, P., Yu, H., Shearer, H. M., Randhawa, K., Wong, J. J., Mior, S., Ameis, A., Carroll, L. J., Nordin, M., Varatharajan, S., Sutton, D., Southerst, D., Jacobs, C., Stupar, M., Taylor-Vaisey, A., Gross, D. P., Brison, R. J., Paulden, M., Ammendolia, C., Cassidy, J. D., … Lacerte, M. (2019). Non-pharmacological management of persistent headaches associated with neck pain: A clinical practice guideline from the Ontario protocol for traffic injury management (OPTIMa) collaboration. European journal of pain (London, England), 23(6), 1051–1070. https://doi.org/10.1002/ejp.1374
Houle, M., Lessard, A., Marineau-Bélanger, É., Lardon, A., Marchand, A. A., Descarreaux, M., & Abboud, J. (2021). Factors associated with headache and neck pain among telecommuters – a five days follow-up. BMC Public Health, 21(1), 1086. https://doi.org/10.1186/s12889-021-11144-6
Langner, S., Fleck, S., Baldauf, J., Mensel, B., Kühn, J. P., & Kirsch, M. (2017). Diagnosis and Differential Diagnosis of Hydrocephalus in Adults. Diagnostik und Differenzialdiagnostik des Hydrozephalus beim Erwachsenen. RoFo : Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin, 189(8), 728–739. https://doi.org/10.1055/s-0043-108550
Petersen, S. M., Jull, G. A., & Learman, K. E. (2019). Self-reported sinus headaches are associated with neck pain and cervical musculoskeletal dysfunction: a preliminary observational case-control study. The Journal of manual & manipulative therapy, 27(4), 245–252. https://doi.org/10.1080/10669817.2019.1572987
Can choosing the right pillow help many individuals with neck pain get a full night’s sleep and reduce pain-like symptoms?
The Effects Of Neck Pain
How often do you feel stiffness in your neck and shoulders after being hunched for an extended period? Does it hurt when turning your neck from side to side? Or have you been suffering from constant headaches or migraines that are making you have a hard time falling asleep? As the second most common musculoskeletal condition, neck pain is a multifactorial disease developed through various risk factors that can impact a person. (Kazeminasab et al., 2022) The multiple muscles surrounding the neck are constantly overstretched and tight, which can cause pain and discomfort to the upper extremities due to environmental factors. Some environmental factors can range from improper posture to injuries that can affect the neck. When many people are experiencing neck pain associated with environmental factors, it can cause considerable personal pain and discomfort, disability, impaired quality of life, and, for adults, loss of time from work. (Ben Ayed et al., 2019) At the same time, when people experience neck pain, they can develop disruptive sleeping habits. We associate with certified medical providers who inform our patients of the effects of neck pain and how it can disrupt their sleeping habits. While asking important questions to our associated medical providers, we advise patients to incorporate various techniques to reduce neck pain and find ways to stay asleep longer. Dr. Alex Jimenez, D.C., envisions this information as an academic service. Disclaimer.
How Neck Pain Disrupts Sleep
Now, many people wonder how neck pain is associated with sleep. Environmental stressors like chronic stress from the workplace or natural disasters can cause a person to have tense neck muscles and can increase sleep disturbances. (Yabe et al., 2022) When environmental stressors impact the body, the musculoskeletal system becomes tight and tense in different body areas. In the neck, the muscles that surround the cervical can become tense and develop trigger points in muscle tissue, causing referred pain and discomfort. When neck pain causes disruptive sleep problems, it can cause impairment to the multifunctional protective role of sleep via physiological homeostasis and restoration. (Van Looveren et al., 2021) At the same time, some of the pain-like symptoms that can be increased with neck pain associated with disruptive sleep include: (Chin et al., 2021)
Soreness
Pain
Numbness
Difficulty in movement
However, there are ways to reduce the effects of neck pain and get a full night’s sleep, starting with the bedroom.
Low Back & Neck Pain Rehabilitation-Video
Choosing The Right Pillow For Neck Pain
Now, when it comes to getting a full night’s sleep, it is important to find the right mattress to stay asleep as well as feel refreshed. However, as important as it is to sleep in the right mattress when dealing with neck pain, finding the right pillow can do wonders for the neck and help people get enough sleep. When it comes to finding the right pillow, the individual needs to find a pillow with an appropriate height that can provide adequate support for the head and neck to reduce cervical spinal stress and relax the surrounding neck and shoulder muscles. (Lei et al., 2021) This is because when it comes to quality sleep, many people prefer sleeping positions, pillows, and mattresses aimed at comfort. Many pillows have a variety of materials that can help aid in comfort and help reduce neck pain. Some of the types of pillows include:
Memory foam
Polyfilled pillows
Down Pillow
Latex
Combo style
Finding the right pillow for neck pain allows the individual to have their neck fully supported while having the pillow in a lateral position to reduce neck fatigue and improve sleep quality (Son et al., 2020). By doing so, many people can finally get a good night’s sleep and wake up feeling better. By choosing the right pillow, many people will begin to be more mindful of their bodies and make small changes to their routine while getting the sleep they deserve.
References
Ben Ayed, H., Yaich, S., Trigui, M., Ben Hmida, M., Ben Jemaa, M., Ammar, A., Jedidi, J., Karray, R., Feki, H., Mejdoub, Y., Kassis, M., & Damak, J. (2019). Prevalence, Risk Factors and Outcomes of Neck, Shoulders and Low-Back Pain in Secondary-School Children. J Res Health Sci, 19(1), e00440. https://www.ncbi.nlm.nih.gov/pubmed/31133629
Chin, W. S., Chen, Y. C., Lin, T. T., Guo, Y. L., & Shiao, J. S. C. (2021). Short sleep and chronic neck and shoulder discomfort in nurses. J Occup Health, 63(1), e12236. https://doi.org/10.1002/1348-9585.12236
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Lei, J. X., Yang, P. F., Yang, A. L., Gong, Y. F., Shang, P., & Yuan, X. C. (2021). Ergonomic Consideration in Pillow Height Determinants and Evaluation. Healthcare (Basel), 9(10). https://doi.org/10.3390/healthcare9101333
Son, J., Jung, S., Song, H., Kim, J., Bang, S., & Bahn, S. (2020). A Survey of Koreans on Sleep Habits and Sleeping Symptoms Relating to Pillow Comfort and Support. Int J Environ Res Public Health, 17(1). https://doi.org/10.3390/ijerph17010302
Van Looveren, E., Bilterys, T., Munneke, W., Cagnie, B., Ickmans, K., Mairesse, O., Malfliet, A., De Baets, L., Nijs, J., Goubert, D., Danneels, L., Moens, M., & Meeus, M. (2021). The Association between Sleep and Chronic Spinal Pain: A Systematic Review from the Last Decade. J Clin Med, 10(17). https://doi.org/10.3390/jcm10173836
Yabe, Y., Hagiwara, Y., Sekiguchi, T., Sugawara, Y., Tsuchiya, M., Yoshida, S., & Tsuji, I. (2022). Sleep disturbance is associated with neck pain: a 3-year longitudinal study after the Great East Japan Earthquake. BMC Musculoskelet Disord, 23(1), 459. https://doi.org/10.1186/s12891-022-05410-w
Can cervical retraction be a good addition to a home exercise program for individuals with neck pain, spinal arthritis, or needing to strengthen their neck muscles?
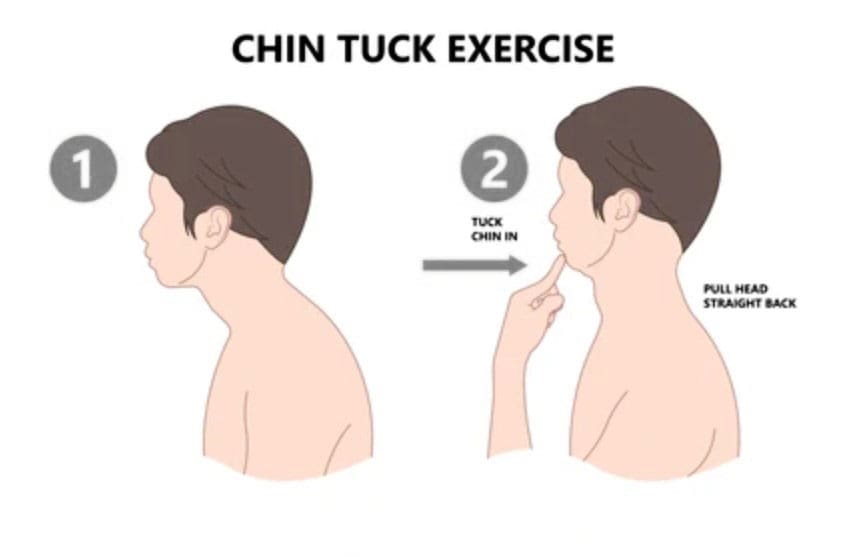
Cervical Retraction
Cervical retraction is a neck exercise that involves gently sliding the head backward while keeping the chin tucked. It can help with:
Neck pain
Stretching and loosening the muscles at the back of the neck.
Headaches
Tightness
Improve posture
Improve flexibility and mobility
Preparation
Basic steps for performing a cervical retraction exercise:
Sit upright with good posture.
Tuck your chin as far as you can comfortably.
Look up while keeping your chin tucked.
Rotate the neck 1-2 inches to each side.
Return to the starting position.
Stop the exercise if you experience pain.
You want to get good at this without loading the joints while learning the movement. Gently and accurately moving your head in alignment with the neck will help you find the correct head action as it moves. Then, it can be performed as a full exercise. Performing the movement correctly requires focus. This is why cervical retraction is done while sitting in a chair with proper posture. Individuals can also stand, but it is more complicated for the body to coordinate than sitting, but it can be done once the individual has practiced.
Sitting or Standing
Gently tuck your chin down toward your neck.
The focus is alignment.
Keeping your chin where it is, press your head back.
There will be soreness, especially for those with pain symptoms, but the neck should feel better.
Be mindful of any intense or severe pain resulting from cervical retraction.
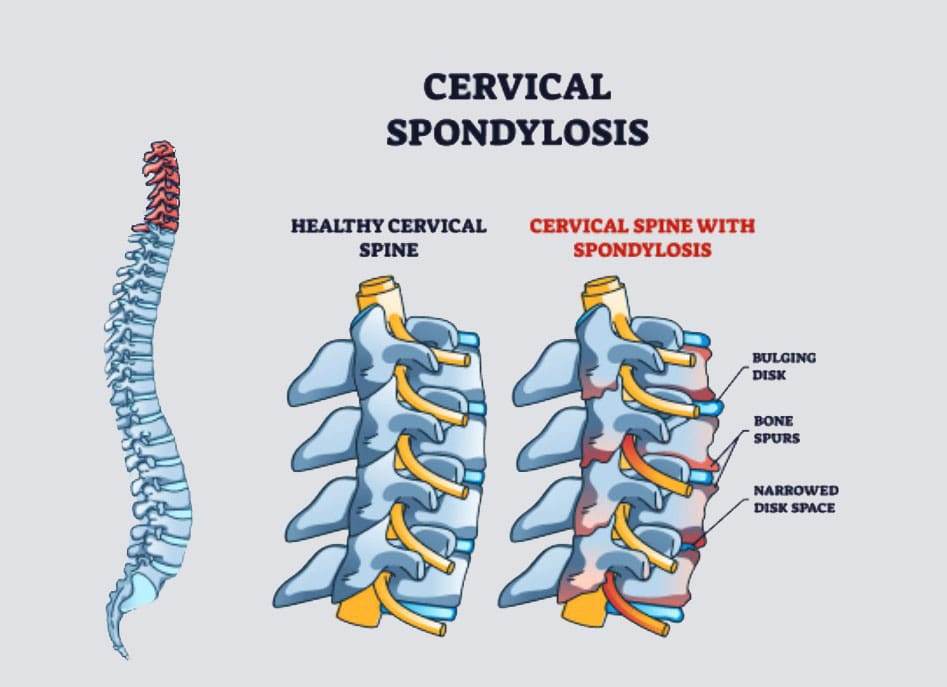
Individuals with cervical spondylosis (neck arthritis) stop if pain presents. (Cleveland Clinic, 2023)
Other Neck Exercises
Another good neck-strengthening exercise is the isometric neck press. In this exercise, you move your head forward, backward, and to each side while your hand provides resistance. This develops flexibility and is recommended for those with arthritis in this area. (Sadeghi, A. et al., 2022) Other exercises include: (Pain Consultants of West Florida, 2019)
Neck extensions: Backward bending can help relieve nerve compression and ease the strain on the cervical spine.
Side rotation: This exercise can improve neck mobility.
Shoulder rolls: This exercise can help keep the neck and shoulder joints fluid.
Injury Medical Chiropractic and Functional Medicine Clinic
If you have a neck condition or radiculopathy that causes pain or other symptoms going down the arm or are unsure how to do it, check with a healthcare provider or physical therapist before trying the exercise. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Neck Injuries
References
North American Spine Society. (2012). Cervical exercise: The Backbone of Spine Treatment. https://www.spine.org/KnowYourBack/Prevention/Exercise/Cervical-Exercise
Cleveland Clinic. (2023). Could your neck pain actually be neck arthritis? https://my.clevelandclinic.org/health/diseases/17685-cervical-spondylosis
Pain Consultants of West Florida. (2019). Chronic Neck Pain: How Core Exercises Can Help. Our Blog. https://pcwfl.com/chronic-neck-pain-how-core-exercises-can-help/
Sadeghi, A., Rostami, M., Ameri, S., Karimi Moghaddam, A., Karimi Moghaddam, Z., & Zeraatchi, A. (2022). Effectiveness of isometric exercises on disability and pain of cervical spondylosis: a randomized controlled trial. BMC sports science, medicine & rehabilitation, 14(1), 108. https://doi.org/10.1186/s13102-022-00500-7
For individuals with cervical arthritis, can physical therapies help manage symptoms and bring pain relief?
Cervical Arthritis
Cervical spondylosis, more commonly known as cervical arthritis or arthritis of the neck, refers to the wearing down of neck bones, discs, tendons, ligaments, and joints. The primary symptoms are neck pain and stiffness. However, it is also possible to have cervical spondylosis and not have any symptoms. The condition affects over 85% of individuals over age 65. (American Academy of Orthopaedic Surgeons, 2021) Treatment can consist of conservative therapies and includes physical therapies, alternative medicine therapies, at-home self care, and over-the-counter and prescription medications. Severe cases of cervical spondylosis are treated with surgery to repair damaged parts of the spine.
Symptoms
Neck pain and headaches at the back of the head are usually the first symptoms. (Kazeminasab S. et al., 2022) The neck can also feel stiff, with worse morning symptoms that improve throughout the day. (Johns Hopkins Medicine, 2024) Symptoms can range from mild discomfort to severe pain. As cervical spondylosis progresses, individuals can experience:
Inability to turn the head or bend the neck.
A clicking or grinding noise when turning the neck.
Tenderness with pressure on the neck.
Pain that radiates to the shoulders or shoulder blades.
Pain and symptoms that disrupt sleep, sometimes causing waking up throughout the night.
Symptoms that decrease with rest.
More severe symptoms include:
Cervical Bone Spurs – Osteophytes
Some with cervical spondylosis have bony growths that can place pressure on the spinal nerves (a pinched nerve) (Bon Secours, 2024). Compression of spinal nerve roots produces cervical radiculopathy, which leads to pain, tingling, and weakness that radiates into the shoulders, arms, and hands.
Cervical Myelopathy
This refers to spinal impingement that leads to spinal cord dysfunction. (Spinal cord dysfunction is a nervous system disorder with interruptions in the spinal cord’s motor, sensory, and autonomic functions.) Symptoms include pain, tingling, numbness, muscle spasms, and weakness in areas below the neck. Spinal cord dysfunction can affect mobility, hand use, and bladder or bowel function control.
Causes
Where degenerative changes are commonly associated with cervical spondylosis, other conditions, and factors can lead to it and include:
Autoimmune Diseases
Rheumatoid arthritis and psoriatic arthritis can cause chronic inflammation in the cervical spine.
Trauma
Neck trauma, including injury and repetitive stress on the neck.
Cervical spondylosis is commonly seen in occupations that involve neck-stressing activities, such as sports.
Age
Wearing down of the spinal discs cartilage between the vertebrae.
Genetic components have been identified in connection with cervical spondylosis, meaning that some types of arthritis that lead to spinal damage are hereditary. (Kazeminasab S. et al., 2022)
Treatment
Treatment begins conservatively, using protocols to preserve function and avoid surgery. Nonsurgical treatments include medications, physical therapy, at-home exercises, and alternative medicine. The treatment method a healthcare provider chooses will depend on how severe the spondylosis is and other factors like age, how much pain is being experienced, the cause, and overall health. The main objectives are to relieve pain, prevent long-term damage to the spinal cord and nerves, and help maintain performing daily activities. (Bon Secours, 2024)
Medications
Medicines used to treat cervical spondylosis include:
Nonsteroidal Anti-inflammatory Drugs NSAIDs
NSAIDs, including ibuprofen and naproxen sodium, are available without a prescription to relieve pain and inflammation.
A healthcare provider can prescribe a more powerful NSAID to help manage severe symptoms.
Corticosteroids
A corticosteroid injection or a short course of an oral corticosteroid, like prednisone, can ease pain and reduce inflammation.
Muscle Relaxants
If cervical spondylosis causes muscle spasms, a healthcare provider can prescribe cyclobenzaprine, a muscle relaxant, to manage symptoms.
Antidepressants
Some types of antidepressants can ease neck pain from cervical spondylosis.
Anti-seizure Meds
Some anti-seizure drugs can cause nerve pain resulting from damaged nerves.
Physical Therapies
Physical therapy will help manage pain and stiffness and keep muscles loose and relaxed.
A physical therapist will teach the patient exercises to stretch and strengthen neck and shoulder muscles.
At-Home Self Care
At-home exercises can help relieve pain, stiffness, and swelling. Some can include:
Reducing inflammation and stress on the neck through posture training.
At-home targeted stretches and exercises will help bring pain relief.
Ice treatment reduces swelling.
Heat will increase circulation.
A neck brace may be recommended briefly to avoid muscle weakness and stiffness.
Alternative Medicine
Chiropractic adjustments and massage therapy are alternative treatments that will help manage cervical spondylosis.
Acupuncture can also be beneficial in reducing neck pain and increasing energy circulation. (Gu C. L. et al., 2019)
Various therapeutic massage therapies will help relieve neck pain and stiffness. Talk to a healthcare provider before starting treatment so they can advise on whether neck massages are safe.
Surgery
A healthcare provider may recommend surgical treatment when all other treatments have failed, if neurological symptoms are severe, or if neck arthritis causes extreme pain or disability. Surgery to treat cervical spondylosis can involve removing bone spurs, part of the cervical vertebra, or a herniated disc. The removed portions of the cervical spine are fused with hardware and bone grafts.
Injury Medical Chiropractic and Functional Medicine Clinic
Chiropractic therapy is among the more conservative treatment options and may be tried first before proceeding with surgery. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution.
Arthritis Explained
References
American Academy of Orthopaedic Surgeons. (2021). Cervical spondylosis (arthritis of the neck). https://orthoinfo.aaos.org/en/diseases–conditions/cervical-spondylosis-arthritis-of-the-neck/
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC musculoskeletal disorders, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Johns Hopkins Medicine. (2024). Spinal arthritis (arthritis in the back or neck). https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-arthritis
Bon Secours. (2024). Cervical osteoarthritis (arthritis in the neck). https://www.bonsecours.com/health-care-services/spine-care/conditions/cervical-osteoarthritis
American Chiropractic Association. (2024). Neck pain. https://www.acatoday.org/patients/neck-pain-and-chiropractic/
Jenkins, H. J., Downie, A. S., Moore, C. S., & French, S. D. (2018). Current evidence for spinal X-ray use in the chiropractic profession: a narrative review. Chiropractic & manual therapies, 26, 48. https://doi.org/10.1186/s12998-018-0217-8
Gu, C. L., Yan, Y., Zhang, D., & Li, P. (2019). An evaluation of the effectiveness of acupuncture with seven acupoint-penetrating needles on cervical spondylosis. Journal of pain research, 12, 1441–1445. https://doi.org/10.2147/JPR.S199798
Can incorporating various yoga poses help reduce neck tension and provide pain relief for individuals dealing with neck pain?
Introduction
Within the hustling and bustling of modern life, it is common for many individuals to carry stress in their bodies. When the body deals with everyday stressors, tension, discomfort, and pain can often manifest in the upper and lower portions of the body. When the body’s upper and lower portions deal with these issues, they can cause overlapping risk profiles in the musculoskeletal system. One of the most common musculoskeletal issues is neck pain. It can cause many problems to the cervical portion of the spine and cause the surrounding muscles to become tense and in pain from the stress of everyday responsibilities. Luckily, there are numerous ways to reduce stress from the neck and help relax the affected muscles from discomfort, including yoga. In today’s article, we will look at how neck pain affects the upper body, the benefits of yoga for neck pain, and various yoga poses to reduce the overlapping effects of neck pain. We discuss with certified medical providers who consolidate our patients’ information to assess how neck pain is correlated with everyday stressors that affect the upper body. We also inform and guide patients on how yoga and the various poses can benefit the body and provide pain relief to the surrounding muscles. We also encourage our patients to ask their associated medical providers many intricate and important questions about incorporating yoga into their daily routine to reduce muscle tension and provide clarity to their bodies. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Does Neck Pain Affect The Upper Body?
Do you feel discomfort or pain in your neck and shoulders after a long, hard workday? Do you notice you hunched more than usual when doing your daily routine? Or do you see yourself developing a hunched posture from looking at the computer screen or phone for an extended period? Many of these normal motions are often correlated with the upper body, especially in the neck and shoulder regions, which causes neck pain. As one of the most common problems affecting many people worldwide, neck pain is a multifactorial disease with numerous risk factors contributing to its development. (Kazeminasab et al., 2022) Like back pain, neck pain can have acute and chronic stages depending on the severity and environmental factors leading to its development. The various muscles, ligaments, and tissues surrounding the neck and shoulders keep the neck stable and mobile. When many individuals overuse these muscles in the neck and shoulders repetitively, it can increase neck pain in the upper body in adulthood. (Ben Ayed et al., 2019)
When acute neck pain turns chronic, it can cause the individual to be in constant discomfort, pain, and misery, so they start to look for various solutions to reduce the correlating symptoms when speaking to their primary doctors. When many individuals begin to explain to their doctors what their daily routine looks like, many doctors will start to assess and formulate a plan that focuses on any specific description of any injuries, including potential mechanisms, inciting and relieving factors, and pain patterns they have encountered throughout the day to come up with a personalized treatment plan to not only reduce neck pain but also provide relief to tension and discomfort to the body. (Childress & Stuek, 2020)
The Science of Motion- Video
The Benefits Of Yoga For Neck Pain
Many primary doctors will work with associated medical providers to develop a personalized plan to relieve neck pain and its associated symptoms in many individuals. Many of these customized treatment plans include spinal manipulation, acupuncture, massage, decompression therapy, and therapeutic exercises. One of the therapeutic exercises that many individuals have utilized is yoga. Yoga is a holistic practice encompassing breathing control, meditation, and various poses to stretch and strengthen the affected upper muscles. Yoga is excellent for reducing neck pain and helping with upper cervical spine mobility, stretching the neck musculature to help the individual improve mobility and flexibility. (Raja et al., 2021) Additionally, the effects of yoga and its many poses can reduce tension, give clarity to the mind, and allow the nutrients and oxygen to the musculo-articular system to naturally heal the body itself. (Gandolfi et al., 2023)
Yoga Poses For Neck Pain
At the same time, many individuals with sedentary jobs that correlate to neck pain have implemented yoga as part of their routine. Yoga improves their range of joint motion and cognitive function and helps relieve musculoskeletal discomfort in the neck and shoulder regions. (Thanasilungkoon et al., 2023) Below are some of the various yoga poses that can help reduce the pain-like symptoms of neck pain and ease the surrounding muscles.
Seated Neck Stretches
For seated neck stretches, this yoga pose helps stretch and release the neck muscles that carry tension and stress in the cervical region of the body.
In a seated upright position, turn the head to the right and gently lift the chin.
You should feel a stretch along the left side of the neck and shoulders.
Hold the position for three to five breaths and repeat on the left side.
Camel Pose
For the camel pose, this yoga pose helps strengthen the front neck muscles while easing tension on the shoulders and back of the neck.
You can kneel on a yoga mat by keeping your knees and feet hip-distance apart while keeping the pelvis neutral.
Lift the chest while arching your back and pressing the pelvis slightly forward.
Bring the fingertips to the heels or yoga blocks beside the ankles.
Focus on drawing the chin close to the neck while pressing the feet to the mat.
Hold the position for three to five breaths before releasing and lifting the sternum to rise back up.
Sphinx Pose
The sphinx pose allows you to lengthen and strengthen the spine while stretching the shoulders and releasing tension.
On a yoga mat, lie on your stomach with the elbows under the shoulders.
Press your palms and forearms on the mat and tighten the lower half to support you as you lift your upper torso and head.
Keep looking straight ahead as you are being mindful of lengthening the spine.
Hold this position for three to five breaths.
Thread The Needle Pose
The thread-the-needle pose helps release tension stored in the neck, shoulders, and back.
On a yoga mat, start in an all-fours position with the wrist under the shoulders and the knees under the hips.
Lift the right hand and move it to the left along the floor with the palm facing up.
Hold the position for three to five breaths for thirty seconds and release.
Return to the all-fours position and repeat to the left side.
Conclusion
Overall, incorporating yoga as part of a daily routine can provide beneficial results in reducing neck pain and its associated comorbidities. Yoga does not require hours of practice or even contorting into various poses, as just a few minutes of gentle stretching and mindful breathing each day can provide positive results. When people start to utilize yoga as part of their daily activities, they will notice their posture improving, their minds clearer than ever, and live a happier, healthier life without dealing with neck pain.
References
Ben Ayed, H., Yaich, S., Trigui, M., Ben Hmida, M., Ben Jemaa, M., Ammar, A., Jedidi, J., Karray, R., Feki, H., Mejdoub, Y., Kassis, M., & Damak, J. (2019). Prevalence, Risk Factors and Outcomes of Neck, Shoulders and Low-Back Pain in Secondary-School Children. J Res Health Sci, 19(1), e00440. https://www.ncbi.nlm.nih.gov/pubmed/31133629
Gandolfi, M. G., Zamparini, F., Spinelli, A., & Prati, C. (2023). Asana for Neck, Shoulders, and Wrists to Prevent Musculoskeletal Disorders among Dental Professionals: In-Office Yoga Protocol. J Funct Morphol Kinesiol, 8(1). https://doi.org/10.3390/jfmk8010026
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Raja, G. P., Bhat, N. S., Fernandez-de-Las-Penas, C., Gangavelli, R., Davis, F., Shankar, R., & Prabhu, A. (2021). Effectiveness of deep cervical fascial manipulation and yoga postures on pain, function, and oculomotor control in patients with mechanical neck pain: study protocol of a pragmatic, parallel-group, randomized, controlled trial. Trials, 22(1), 574. https://doi.org/10.1186/s13063-021-05533-w
Thanasilungkoon, B., Niempoog, S., Sriyakul, K., Tungsukruthai, P., Kamalashiran, C., & Kietinun, S. (2023). The Efficacy of Ruesi Dadton and Yoga on Reducing Neck and Shoulder Pain in Office Workers. Int J Exerc Sci, 16(7), 1113-1130. https://www.ncbi.nlm.nih.gov/pubmed/38287934
Can individuals with thoracic outlet syndrome incorporate electroacupuncture to reduce neck pain and restore proper posture?
Introduction
More times throughout the world, many individuals have experienced pain around their necks, which can lead to pain and discomfort. Many environmental factors, like being in a hunched position while looking at the computer or phone, traumatic injuries, poor posture, or spinal issues, can cause pain-like symptoms and complications to the body. Since neck pain is a common complaint many people suffer, symptoms like tingling, numbness, or muscle weakness in the upper extremities can lead to comorbidities. When this happens, it can lead to the development of a complex condition known as thoracic outlet syndrome or TOS. Today’s article looks at the link between thoracic outlet syndrome and neck pain, how to manage TOS while alleviating neck pain, and how electroacupuncture can help with TOS. We talk with certified medical providers who consolidate our patients’ information to assess how to minimize the effects of TOS while reducing neck pain. We also inform and guide patients on how electroacupuncture can help manage TOS. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating electroacupuncture to alleviate TOS associated with the neck. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
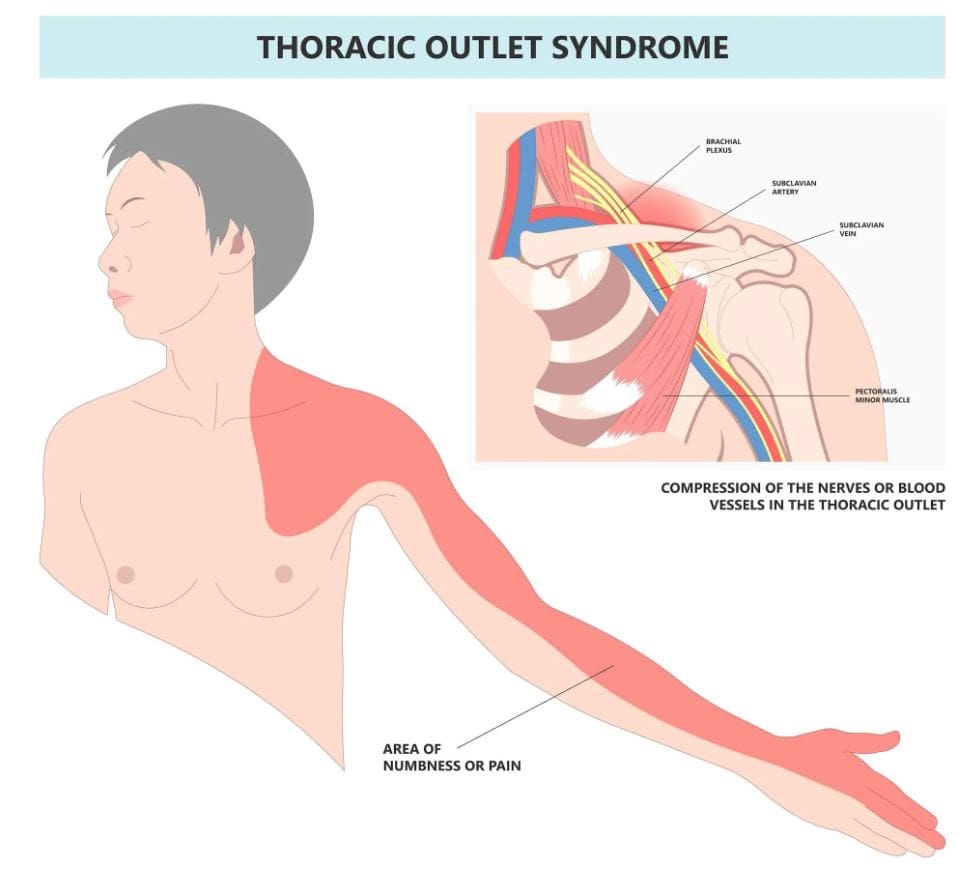
The Link Between Thoracic Outlet Syndrome & Neck Pain
Have you been noticing how you are hunched over more than usual? Do you experience symptoms of tingling or numbness down from your arms to your hands? Or do you feel muscle tension in your neck? Thoracic outlet syndrome, or TOS, is a challenging condition resulting in the compression of neurovascular structures between the clavicle and the first rib. (Masocatto et al., 2019) These neurovascular structures are near the neck and shoulders. When environmental structures affect the upper extremities, it can lead to referred neck pain, which can cause overlapping risk profiles. Some of the factors that TOS can contribute to neck pain include:
Atomical variations
Poor posture
Repetitive motions
Traumatic injuries
At the same time, people with neck pain can develop TOS, as neck pain is a multifactorial musculoskeletal condition that can be associated with overlapping risk profiles that contribute to TOS. (Kazeminasab et al., 2022) As stated earlier, factors like poor posture can overstretch the neck muscles and the neurovascular structures, leading to neuropathic pain symptoms that can cause deep aching referred pain to the neck and muscle weakness. (Childress & Stuek, 2020) When this happens, many people will begin to feel miserable and start to seek treatment to not only reduce TOS but also alleviate neck pain.
What Is Thoracic Outlet Syndrome- Video
Managing TOS & Alleviating Neck Pain
When it comes to treating TOS, especially when neck pain is a significant component, many individuals will try to seek out non-surgical treatments to reduce the symptoms. Many individuals may try physical therapy to stretch and strengthen their shoulder, chest, and neck muscles to relieve compression. Others might try a manual treatment that is joint-oriented for the neck while neural-tissue-oriented for TOS to improve mobilization on the upper extremities and even improve poor posture. (Kuligowski et al., 2021) Additionally, non-surgical treatments can be combined with other therapies to reduce the chances of TOS from returning as they can further increase sensory-motor function back to the neck and upper extremities. (Borrella-Andres et al., 2021)
How Electroacupuncture Can Help With TOS
Electroacupuncture is a modern form of traditional acupuncture that is part of the non-surgical treatments that can help manage TOS while alleviating neck pain. Electroacupuncture is a modification of inserting needles into the body’s acupoints while incorporating electric stimulation to deliver a pulsed electrical current to the affected area gently. (Zhang et al., 2022) Some of the beneficial properties that electrostimulation can provide for TOS include:
Pain reduction by stimulating the release of endorphins to decrease inflammation.
Help relax the affected muscles in the chest and neck to alleviate the pressure on the nerves of the thoracic outlet.
Help enhance the blood flow to reduce vascular compression of TOS.
Help stimulate the nerve pathway to promote healthy nerve function and reduce pain-like symptoms.
By incorporating electroacupuncture and non-surgical treatments to reduce TOS, many individuals can make modifications to their lifestyle habits and prevent issues from affecting their upper body extremities. By utilizing these treatments, many people can listen to their bodies and focus on their health and well-being by addressing the pain-like symptoms they are experiencing from TOS correlating with neck pain. At the same time, they have a positive relationship with their primary doctors to develop a personalized treatment plan that can manage their TOS symptoms to the best outcomes.
References
Borrella-Andres, S., Marques-Garcia, I., Lucha-Lopez, M. O., Fanlo-Mazas, P., Hernandez-Secorun, M., Perez-Bellmunt, A., Tricas-Moreno, J. M., & Hidalgo-Garcia, C. (2021). Manual Therapy as a Management of Cervical Radiculopathy: A Systematic Review. Biomed Res Int, 2021, 9936981. https://doi.org/10.1155/2021/9936981
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Kuligowski, T., Skrzek, A., & Cieslik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health, 18(11). https://doi.org/10.3390/ijerph18116176
Masocatto, N. O., Da-Matta, T., Prozzo, T. G., Couto, W. J., & Porfirio, G. (2019). Thoracic outlet syndrome: a narrative review. Rev Col Bras Cir, 46(5), e20192243. https://doi.org/10.1590/0100-6991e-20192243 (Sindrome do desfiladeiro toracico: uma revisao narrativa.)
Zhang, B., Shi, H., Cao, S., Xie, L., Ren, P., Wang, J., & Shi, B. (2022). Revealing the magic of acupuncture based on biological mechanisms: A literature review. Biosci Trends, 16(1), 73-90. https://doi.org/10.5582/bst.2022.01039
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine