A trigger point is a knot or bundle of stiff spine muscle tissue that you can’t move or relax, and when touched pain spreads to the neck, shoulders, and upper back.
Pretty much everyone can relate to this type of pain in the neck or what is known as myofascial pain syndrome when several of these trigger points are grouped.
How to ease the pain and prevent it
Trigger points can form in muscles all over the body. Myofascial pain syndrome in the neck happens when trigger points develop in the muscles of the shoulders, upper back, and neck.
A Trigger Point
Trigger points have a unique connection to America. They were first identified in the 1940s by Janet Travell, MD, who was John F. Kennedy’s doctor. JFK had severe chronic back pain and had trigger point injections to ease the pain.
A trigger point is a sensitive area within the muscles. They are typically described as knots and feel like a bundle of tense, contracted muscles that twitch and spread pain when touched. The spreading pain is known as referred pain. Example: Trigger points in the shoulder send pain into the neck.
Trigger points cause muscles to stress and to contract. This results in:
Muscle weakness
Numbness
Limited muscle movement
Formation of Points in The Neck
They are usually caused by mechanical factors (factors that strain or stress the muscles).� Spinal trauma, like whiplash from an automobile accident or sports-related injury, can create trigger points.
They also develop through repetitive actions and routine everyday chores that can hurt the spine over time.
Straining the neck muscles from poor posture for extended times like craning the neck while working on a computer, carrying a heavy bag that stresses the muscles of the neck, upper back, and shoulders.
Trigger Points vs Fibromyalgia Tender Points
Trigger points do get confused with tender points of fibromyalgia. Trigger points and tender points are both defined as local areas of pain but are not the same.
Tender points do not cause referred pain the way trigger points do.
Tender points are symmetrical meaning that they are on both sides of the body. Whereas trigger points do not follow a symmetrical pattern.
But it can become complicated because individuals with fibromyalgia can have both tender points and trigger points. People with fibromyalgia can also have myofascial pain syndrome.
Trigger Point Diagnosis
Trigger points are a regular cause of different types of spine pain, that can range from neck pain to low back pain. However, doctors are still trying to understand how trigger points produce referred pain. This is why diagnosing trigger points can be difficult for doctors.
They are complex because they are easy to pinpoint but difficult to diagnose. As they can directly cause muscle pain but they can mimic other pain making conditions exactly the way Myofascial pain and fibromyalgia get confused.
Jaw pain
Earaches
Toothaches
These types of pain that do not go away could be caused by trigger point/s in the neck.
Individuals with chronic neck pain that don’t seem to have a cause, could be trigger points. A doctor will refer you to a physical therapist, chiropractor or another spine specialist to conduct an examination for trigger points.
Treatment
Treatment can range from home remedies, chiropractic care, physical therapy and if severe muscle injections. There is no one treatment that works, as everyone and their injuries are different, meaning that various treatment options need to be looked into.
Home
Before starting any home therapy, discuss it with a trained professional like a doctor, chiropractor, massage therapist, or physical therapist to identify the location of the trigger point to effectively treat it.
Treated with massaging the area but can be tough with hard-to-reach places in the upper back. If unable to reach the point slowly and gently roll over a foam roller, golf or tennis ball for quick relief.
Massage
Massage therapists are trained in relieving muscle pain. Deep tissue massage can relieve an irritated area. Regular massage sessions can reduce pain and prevent the points from reemerging.
Physical therapy
Physical therapy treats trigger points in different ways, this includes:
Massage
Heat
Electrical stimulation
Ultrasound
A cooling spray is applied followed with stretches to relax and relieve the contracted muscle/s
Medications
Muscle relaxants can be used to reduce the symptoms and relieve pain. However, these meds can have all kinds of side effects, and become habit-forming, so use should be limited and in conjunction with a proper chiropractic/physical therapy treatment plan.
Injections
If the pain continues despite the non-surgical treatments or worsens, then your doctor could recommend trigger point injections. Injections are late-stage therapy. Doctors want to avoid patients becoming dependant on injections and will prescribe injections with an exercise, chiropractic/physical therapy program for maximum relief and effectiveness.
Overall Health
The majority of people have felt tight muscles around the neck. Utilizing proper posture and healthy spinal mechanics can prevent trigger points and myofascial pain syndrome.
Our services are specialized and focused on injuries and the complete recovery process.�Our areas of practice include�Wellness & Nutrition, Chronic Pain,�Personal Injury,�Auto Accident Care, Work Injuries, Back Injury, Low�Back Pain, Neck Pain, Migraine Headaches, Sports Injuries,�Severe Sciatica, Scoliosis, Complex Herniated Discs,�Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, and Functional Medicine Treatments.
�Neck Pain and Chiropractic Treatment El Paso, Texas
NCIB Resources
Many people who have trigger points or myofascial pain syndrome in their spine have knots and tightness throughout their back and neck. To prevent myofascial pain syndrome one needs to practice a healthy lifestyle that promotes good spine health. Stretching and exercising regularly can help keep stress under control and prevent tension from building up, which makes it harder for trigger points to activate and cause pain.
Q: My neck pain comes and goes, depending on the weather, and has for a few years. I have found certain exercises that help and others that make the pain worse. A co-worker told me about Mechanical diagnosis therapy. What is it and can it help? � El Paso, TX.
A: Mechanical Diagnosis Therapy also known as the McKenzie Method is a spinal technique that teaches how to safely and effectively reduce neck pain and improve neck function.
The goal of mechanical diagnosis therapy is to:
Assess
Treat
Prevent back and neck pain
This puts you in a position to control the pain. This technique can also help with joint problems that cause
Shoulder
Hip
Knee pain
Exercises that help reduce neck pain are highly beneficial, especially combined with chiropractic, physical therapy, rehabilitation treatment plan. But, mechanical diagnosis therapy definitely would be worth trying out for relief and prevention of neck pain. This method finds a key exercise that you can do to control the pain, which can be more effective than other exercises.
This is known as the directional preference of movement�and can hold the key to reducing pain.
The best results have been demonstrated with patients who work with chiropractors and physical therapists who have completed training and passed a standardized examination by the McKenzie Institute.
Chiropractic/Physical Therapy session that incorporates Mechanical Diagnosis Therapy:
A physical therapist or chiropractor will perform a detailed assessment. Your health history, neck pain, and other symptoms.
The therapist instructs the patient on how to perform specific, structured exercises.
This helps determine what movements or positions cause the neck pain and which positions and movements are more comfortable, and help reduce symptoms.
Patients often show signs of centralization. This is when the original�pain in the neck is felt in other parts of the body like the arm or hand and radiates toward the spine from specific positions or movements.
The chiropractor/therapist will create a customized exercise plan that the patient will do at work/home to reduce neck pain and other symptoms.
Every patient’s plan is different and completely individualized to treat your specific neck pain.
After the first appointment, the patient will perform the exercises themselves. But depending on the treatment plan, chiropractic exams could be implemented for 3 to 4 weeks to monitor progress. As these appointments are fulfilled the chiropractor could add or alter the exercises as the pain and symptoms reduce and range of motion increases.
Doing these exercises regularly will help reduce neck pain and prevent it from worsening.
The exercises can be performed quickly and easily so they become a part of the patient’s regular routine. A chiropractor/therapist will work with the patient to design a simple but effective exercise plan that fits into their schedule. The chiropractor will also teach ways to prevent aggravating neck pain by avoiding positions and other activities not thought about.
Mechanical Diagnosis Therapy can create tools to help reduce and prevent neck pain along with other symptoms. Most of the time, a few sessions are all that is needed to see benefits. Results happen rather quickly, especially as the patients are managing their neck pain between visits with their chiropractor.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Clinic,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
El Paso, TX Chiropractic Neck Pain Treatment
Shane Scott was involved in an automobile accident when he heard about Dr. Alex Jimenez from a friend. After experiencing headache, neck and low back pain, several days after the incident, Shane’s quality of life, was tremendously affected. Thankfully, treatment with Dr. Jimenez helped Shane return to his normal life. Shane recommends Dr. Jimenez as the non-surgical choice for neck pain treatment.
Neck pain (or cervicalgia) is a common problem, where two-thirds of individuals will experience neck pain some time in their lives. Neck pain can be brought on by numerous other spinal issues. It can arise from muscle tightness in either the neck and upper spine or pinching of the nerves in the cervical vertebrae.
NCBI Resources
A chiropractor evaluates the spine as a whole because other regions of the�neck (cervical), mid-back (thoracic) and low back (lumbar) can be affected as well. Along with treating the spine as a whole, chiropractic treatment is geared toward the entire body and not just symptom/s. Chiropractors will also educate on nutrition, stress management, and lifestyle goals in addition to treating neck pain.
How often do you feel you have something that must be done? How often do you have difficulty concentrating before eating? Do you suffer from headaches and/or migraines? Head pain is commonly characterized by a variety of symptoms, including pain and discomfort, photophobia or light sensitivity, dizziness, lethargy, and mood changes. However, one of the most common symptoms of head pain is brain fog, which also causes its own variety of symptoms. In the following article, we will discuss brain fog associated with head pain and pressure as well as the common cause of brain fog and headache/migraine. �
�
�
Many patients will commonly visit healthcare professionals reporting mild or moderate head pain and pressure as well as a variety of other symptoms, such as brain fog, fatigue, and even vision problems, among others.� The patients frequently experience a “constant cloud” over their brain and they generally never have a clear head or mental clarity. Many patients will commonly report numerous other symptoms, including poor short-term memory, detachment from reality, sharp pain and discomfort in the head, and ringing in the ears. Many others report anxiety, caused or worsened by the symptoms. �
�
�
Brain Fog and Head Pain
The first approach towards characterizing brain fog associated with head pain is to make sure it’s not caused by a secondary headache or a headache with an identifiable cause. Several types of head pain are more severe than others, such as giant cell arteritis or inflammation of the arteries that run along the temples, raised blood pressure or hypertension,�brain hemorrhage, brain infections like encephalitis, increased pressure in the fluid of the brain or raised intracranial pressure, and brain tumors. Less severe types of head pain include�carbon monoxide poisoning, taking too many painkillers or medication-overuse headache, disorders of the joints of the jaw or temporomandibular joint disorders, dental problems, and sinus infections or sinusitis. Below, we will discuss several of the most common causes of brain fog associated with head pain.
�
Causes of Brain Fog and Head Pain
Researchers and healthcare professionals have offered their own hypotheses for why brain fog occurs with head pain, based on their own knowledge and experiences. They believe that brain fog and head pain occur due to epilepsy, overactive parathyroid glands or hyperparathyroidism, overactive thyroid gland or thyrotoxicosis, and brain circulation problems. Researchers and healthcare professionals also suggest it could be due to a vitamin B12 deficiency. Fortunately, the utilization of CT and MRI brain scans, heart tracing, EEG and blood tests, can be utilized to rule out many of these health issues.
Moreover, several health issues require specific tests and evaluations. These include tests for lupus or an inflammatory disorder, magnesium deficiency, zinc deficiency,�Lyme disease or an infection resulting from a tick bite, and postural tachycardia syndrome or an increase in heart rate on standing. Many researchers and healthcare professionals also recommend a detailed examination and investigation of a misalignment or subluxation of the neck or cervical spine. �
If all these tests and evaluations return as normal, then the next approach towards characterizing brain fog associated with head pain is to make sure it’s not caused by a primary headache or a headache without an underlying secondary cause. Primary headaches are diagnosed in 9 out of 10 cases of head pain and pressure. The most common types of primary headaches include tension-type headache,�migraine, and daily persistent headache. Diagnosis depends on the pattern of symptoms as well as examinations and investigations to rule out underlying causes. Although there are specific treatment options for several primary headaches like migraines, in many instances, treatment is frequently a matter of trial and error. �
Furthermore, despite the best efforts of researchers and healthcare professionals as well as comprehensive examinations and investigations, many people who suffer from brain fog associated with head pain and pressure are still left without any explanation for their symptoms. Researchers and healthcare professionals have a name even for this type of brain fog-related head pain known as medically unexplained symptoms or MUS. This ultimately means exactly what reads as: no one is denying that the person has the symptoms, but doctors have been unable to find a medical condition to explain them. �
Several people with MUS undoubtedly do have stress, anxiety, and even depression whether as a result of the symptoms or as a cause of the symptoms. Researchers and healthcare professionals recommend continuing to pursue psychological support if you have brain fog and head pain, as this may help to relieve a potential cause as well as helping to cope with the symptoms. Cognitive-behavioral therapy�would be ideal for this purpose, as would�mindful awareness, a technique that would arm people with a way of deflecting their mind away from their troubling symptoms, improving overall well-being. �
Brain fog can make people feel as if they’re not able to focus or concentrate accordingly and it’s commonly accompanied by head pain, fatigue and even vision problems. While brain fog is a symptom rather than a single health issue, it can be a cause or be caused by other underlying health issues. Head pain and pressure can have a variety of symptoms on its own but head pain-related brain fog has a whole different variety of symptoms. Understanding brain fog associated with head pain and pressure as well as what you can do about the symptoms can help manage brain fog symptoms and promote overall brain health and wellness. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
How often do you feel you have something that must be done? How often do you have difficulty concentrating before eating? Do you suffer from headaches and/or migraines? Head pain is commonly characterized by a variety of symptoms, including pain and discomfort, photophobia or light sensitivity, dizziness, lethargy, and mood changes. However, one of the most common symptoms of head pain is brain fog, which also causes its own variety of symptoms. In the following article, we will discuss brain fog associated with head pain and pressure as well as the common cause of brain fog and headache/migraine. �
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Often referred to as C1-C7, with the “C” indicating cervical, and the numbers 1-7 indicate the level.
C1 is closest to the skull
C7 is closest to the thoracic chest/rib cage area
The cervical spine is particularly susceptible to degenerative problems because:
Highly mobile with a broad range of motion
Supports the skull
Neck anatomy is complex
Many degenerative problems, including osteophytes or bone spurs, can develop.
Neck Pain Symptoms
Several symptoms can occur and indicate the presence of a degenerative condition:
Neck pain
Pain around the back of the shoulder area
Arm pain, numbness, or weakness
Difficulty with hand dexterity or walking
Conditions That Affect the Neck
The degenerative process begins in any of the joints in the spine, but over time it can cause changes in the other joints.
An example is an intervertebral disc�where:
The disc narrows and the normal movement becomes altered, and the adjacent joints are subjected to force and pressure, which can lead to degenerative arthritis joint inflammation.
Spondylosis or spinal osteoarthritis causing pain in the neck is common. The pain can radiate, or spread, into the shoulder/s or down the arm/s. Arm pain or weakness caused by a bone spur compressing a spinal nerve root can also occur.
Diagnosing Cervical Spine Conditions
Once examined one or more symptoms are likely to be present.
The doctor will ask the patient questions to learn the history of the patient.
A thorough evaluation of the patient will be conducted, including tests to identify the cause of pain and symptoms.
A neurologic examination is performed to rule out neurological disorders
Shoulder examination will also be done to ensure that the symptoms originate from the neck
Diagnostic tests
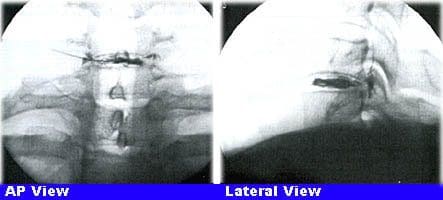
X-rays for:
Narrow intervertebral disc space
Anterior osteophytes or bone spurs
Spondylosis (ie, arthritis) of the facet joints
Osteophytes created from the uncovertebral joints
CT Scans or computed tomography can show bone changes associated with degenerative spondylosis. Osteophytes can be observed and evaluated.
CT does not provide an optimal evaluation but can sometimes show disc herniations.
MRI magnetic resonance imaging is a powerful tool for cervical spondylosis.
MRI can help doctors identify:
Disc herniation
Osteophytes
Joint arthrosis a type of osteoarthritis
MRI is best for soft disc herniation/s.
Myelogram/CT can be utilized in complex cases that involve multi-level spinal diseases.
It is very useful in delineating bone spurs from safe disc herniations.
Discography is used diagnostically when viewing the lumbar/low back and thoracic/mid-back spine, but using it in cervical spine imagery is debated among doctors.
Treatment Options
After the tests have been performed, a custom treatment plan is created.
Nonsurgical Neck Pain Treatment
Nonsurgical treatment of cervical degenerative disease has been proven to provide excellent results in over 85% of patients.
A multi-disciplinary approach:
Immobilization of the neck�to reduce motion can be beneficial during acute episodes of pain.
Physical therapy (PT) and Chiropracticcan be useful to decrease muscle spasms and return motion.
Non-surgical treatment provides positive long-term pain and symptom relief.
Surgery
A surgeon is likely to consider surgery for a disorder if one or more of the following criteria are met:
Nonsurgical care has been tried and has not worked
Spinal cord dysfunction
Arm pain or weakness (neurological symptoms) that do not go away
Depending on the diagnosis, surgical procedures can vary:
One type of surgery is the removal of the bone spur(s)
Cervical spinal fusion that joins two or more vertebrae
But the surgical procedure is based on the way you the patient wants to go, the diagnosis, general health, and what the spine surgeon recommends.
The surgeon will explain the recommended procedure to you clearly.
Most of the time the preferred approach is anterior or from the front interbody fusion.
A cervical plate could be placed over the interbody device or graft to stabilize the neck. This can avoid the need for a brace after.
A posterior approach from the back of the spine is considered when a disc has herniated laterally or to the side.
Things You Can Do
Cervical spine disorders can be diagnosed�and treated more accurately with today’s advancing technology.
With the guidance and treatment of an expert medical team, patients can expect to see a definite improvement in their condition and symptoms.
El Paso, TX Neck Pain Chiropractic Treatment
Sandra Rubio discusses the symptoms, causes, and treatments of neck pain. Headaches, migraines, dizziness, confusion, and weakness in the upper extremities are a few of the typical symptoms. Trauma from an accident, such as that from an automobile accident or a sports injury, or an aggravated illness because of improper posture can commonly cause neck pain and other ailments. Dr. Alex Jimenez uses spinal alterations and manual manipulations, one of other chiropractic treatment techniques like deep-tissue massage, to reestablish the alignment of the cervical spine and improve neck pain. Chiropractic care with Dr. Alex Jimenez is your non-surgical choice for restoring general patient well-being.
Neck pain is a frequent health issue, with roughly two-thirds of the people being influenced by neck pain at any time throughout their lifetimes. Numerous other health issues can cause pain arising in the upper back, or the spine. Neck pain can result emanating from the vertebrae, or because of muscular tightness in both the neck and the upper back. Joint disruption in the neck causes migraines, and headache, as does joint disturbance at the trunk, or can generate a variety of other symptoms. Neck pain affects about 5 percent of the worldwide population as of 2010, based on figures.
NCBI Resources
A chiropractor evaluates the spine as a whole because other regions of the�neck (cervical), mid-back (thoracic) and low back (lumbar)�can be affected as well. Along with treating the spine as a whole, chiropractic medicine treats the entire person and not just a specific symptom/s. Chiropractors may�educate on nutrition, stress management, and lifestyle goals in addition to treating neck pain.
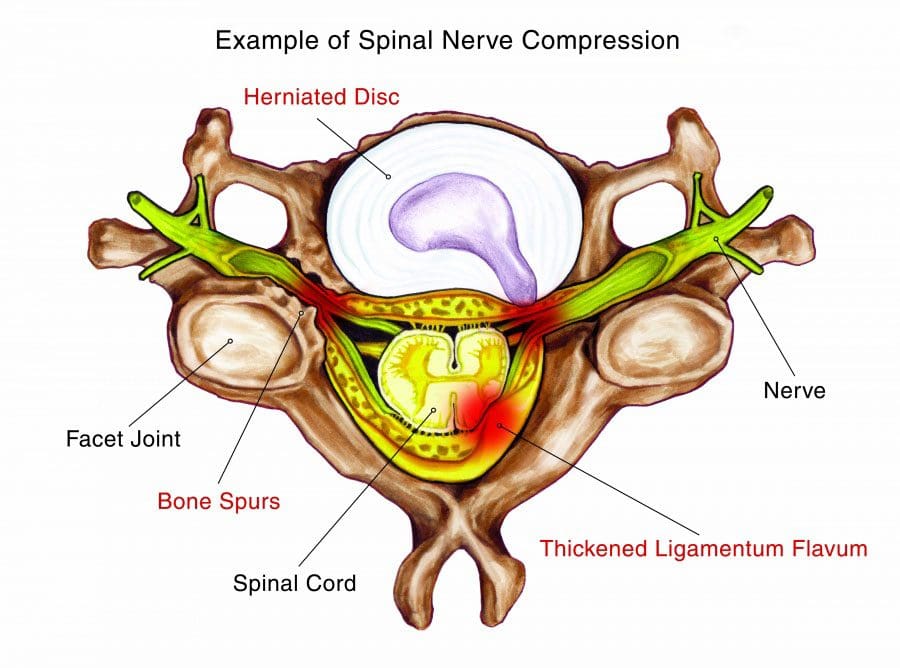
Cervical radiculopathy happens when a pinched nerve in the neck (cervical spine) causes pain.
Radicular pain can extend beyond the neck and radiate down:
The shoulders
Arms
Fingers
This type of nerve compression also causes:
Weakness
Numbness
Tingling
Reflex problems
The neck consists of 8 pairs of nerves that control several motor (strength) and sensory (feel) functions.
The cervical nerve roots at the top send movement and feeling signals to the head and neck, and the nerves at the bottom enable motor and sensory function to the arms and hands.
If one or more of the spinal nerves in the neck gets pinched, it can disturb its ability to function correctly.
This results in radiating pain in the neck and other areas of the body.
This condition can affect anyone but usually affects middle-aged adults.
Men also tend to develop cervical radiculopathy more than women.
Causes
The natural aging process on the spine is what usually causes cervical radiculopathy.
The spine goes through the aging process just like the rest of the body and even more as it is the basis of our structure.
This process can lead to several degenerative spinal disorders, that include:
Cervical spondylosis (osteoarthritis)
Spinal stenosis
Herniated discs
When nerve passageways begin to narrow, intervertebral discs begin to protrude,� and bone spurs, caused by these disorders can put pressure on the nerves in the neck.
The condition can also be caused by a traumatic injury to the neck like whiplash or sports injury.
Rarely is it caused by an infection or spinal tumor.
Symptoms
The primary symptom is pain radiating from the neck down to the:
Shoulders
Arms
Hands
Fingers
The above is an example of sensory function, which is related to feeling.
In addition to sensory symptoms, radiculopathy can also cause motor dysfunction.
Motor dysfunction relates to muscles and movement.
Reflex changes in the neck and upper body and weakness are examples of motor dysfunction.
Diagnosis
A spine specialist/chiropractor has several tools to diagnose cervical radiculopathy.
First and foremost your medical history will be reviewed and then will be:
Asked to describe symptoms
A physical exam will be conducted�to recreate the pain in a controlled manner in the:
Neck
Shoulder
Arms
Example: Spurling�s maneuver, which gently rotates the head, while applying gentle pressure.
Once the information from the medical history and physical exam are done,��imaging tests such as an MRI�may be ordered so they can pinpoint the location of the nerve compression.
MRI scans show the soft tissues in the spine, including the nerves.
The doctor may request a pair of diagnostic tests called electromyogram (EMG) and nerve conduction exam if there are significant upper nerve arm and neck pain.
These tests help understand if there is nerve damage, the cause of the damage and if the symptoms are related to the nerve damage.
EMG and nerve conduction tests are usually performed together to help in the diagnosis.
Emergency Symptoms
Once the spine specialist confirms the diagnosis, they will develop a treatment plan to relieve the nerve compression or prevent it from getting worse.
Most cases are taken care of with non-surgical treatment, however, if the following occurs you should contact your doctor:
Neck pain does not improve with treatment in the time your doctor expects.
Pain worsens regardless of treatment
Or you develop new:
Numbness
Weakness in the
Neck
Arms
Upper body
Develop fever
If you experience symptoms in the lower body like:
Weakness in the leg
Difficulty walking
Lack of bowel/bladder function, then seek medical attention immediately.
These symptoms may indicate cervical myelopathy, a more severe condition.
Cervical myelopathy is the compression of the spinal cord.
When the spinal cord gets compressed, it can generate widespread spine issues and usually requires surgery.
Treatment Cervical Radiculopathy
Like most types of spine pain, a doctor will recommend trying one or more conservative treatments first.
Conservative treatments are nonsurgical means.
It�s important to understand that just because a treatment is considered conservative does not mean it is ineffective.
In fact, it�s quite the opposite. Most people with nerve compression in their neck respond well to conservative therapies.
Though research on the efficacy of conservative treatments for cervical radiculopathy has produced mixed results, findings show that these therapies help eliminate pain and other nerve-related symptoms (like numbness and muscle weakness) in 40-80% of people.
The following are the most common conservative treatments:
Over-the-counter medications, like acetaminophen (Tylenol) or nonsteroidal anti-inflammatory medications(ibuprofen, Motrin)
Prescription medications, like steroids (prednisone), neuropathic agents (gabapentin, pregabalin), and muscle relaxants (baclofen, cyclobenzaprine)
Cervical spinal traction, that can be performed during physical therapy
Avoiding strenuous activity, but don’t avoid all activity, as too much rest can exacerbate the injury and extend the recovery time
These conservative treatments can go on for 6 to 8 weeks. If there is no improvement or it gets worse, then a doctor may want to step you up to the next level.
This may include steroid injections.
Spinal Injections
Cervical epidural steroid injections are considered a second-line treatment for radiculopathy that is not responding to conservative therapy. These injections send a dose of anti-inflammatory medicine into a specific nerve root�s that can relieve pain.
The number of injections differs from patient to patient. A doctor will make recommendations based on the condition and response to the first injection.
If the first injection reduces the pain and symptoms, a second or third injection might not be necessary unless symptoms recur.
If more than one is needed, they are given 3 weeks between each injection.
Injections can help manage pain and inflammation, but cannot strengthen or improve the flexibility of the cervical muscles.
Because of this, a doctor may prescribe physical therapy, chiropractic or an exercise program to condition the neck muscles.
Surgery Considered
When surgery is needed it is considered a last resort option. This is not a guaranteed solution and there are risks and complications.
Different types of surgical approaches are available. These procedures can be performed minimally invasively in a hospital setting or an outpatient surgery center.
Discussing options with a doctor and whether you are a candidate for minimally invasive surgery or not, along with other types of surgery e.g. artificial disc, is a discussion that is different for everybody, as some patients have existing medical conditions that can increase risks and complications.
Anterior cervical discectomy and fusion (ACDF)
This approach is the most widely used surgical approach.
The surgeon makes an incision through the front of the neck and removes the damaged intervertebral disc, fills the empty space with spacers to restore the height and attaches spinal instrumentation (plate, screws) for stabilization.
A bone graft is then packed into and around the body spacers for bone ingrowth and healing.
Posterior cervical foraminotomy
Here, the surgeon accesses one or more levels of the cervical spine with an incision in the back of the neck.
Foraminotomy decompresses the nerve root by removing whatever is compressing the nerve like a bone or soft tissue.
The procedure opens/widens the neural foramen or the nerve passageway where the nerve exits the spinal canal.
Cervical artificial disc replacement (C-ADR)
Here an artificial disc device is implanted in the empty disc space.
C-ADR is like a shock absorber and enables healthy movement the way that an actual disc does.
Conclusion
A compressed nerve in your neck can lead to radiating pain. This pain can make it almost unbearable to do simple tasks, even moving the neck from side to side or just opening a jar. Conservative treatment like chiropractic and exercise can ease the pain of this condition and restore function. Fortunately, surgery is rarely necessary.
El Paso, TX Neck Pain Chiropractic Treatment
Alfonso J. Ramirez now retired, found follow-up treatment with Dr. Alex Jimenez for his neck pain. Mr. Ramirez experienced chronic pain and headaches, but after receiving chiropractic care, he found relief from his symptoms. Ever since that time, Alfonso Ramirez has continued to maintain the alignment of his backbone with Dr. Jimenez. Mr. Ramirez is grateful for the chiropractic care he’s received for his neck pain and for his knee and shoulder pain. Alfonso J. Ramirez recommends Dr. Alex Jimenez as the non-invasive pick for neck pain.
NCBI Resources
Approximately two-thirds of the population being affected by neck pain at any time throughout their lives. Pain that originates in the cervical spine, or upper spine, can be caused by numerous other spinal health issues. Joint disruption in the neck can generate a variety of other common symptoms, which include headaches, head pain, and migraines. Neck pain affects about 5 percent of the global population, according to statistics.
Weighing an average of 10 pounds, the human head is heavier than most people think. The head can put a great deal of pressure on the neck when it is placed in different positions for prolonged periods � especially regularly looking down at your phone.
The damage caused to the neck from time spent staring at mobile screens has been given the name �Text Neck�, and it is a growing problem among not only teens but for everyone.
Regularly Looking Down at Your Phone Is Cause For Neck Injury
Your body is well-designed to bear the weight of your head when you maintain good posture � but tilting your head down to look at your phone is not good posture. In fact, for every inch you move angle your head downward, you double the pressure on your spine.
Looking at your phone can put an extra ten or twenty pounds of pressure on your neck. That would be worth noting even if you only did it occasionally, but most people spend hours looking at their phones throughout the day. That amounts to hours of excessive pressure on the soft tissues that make up your neck � pressure that will inevitably lead to inflammation and discomfort if left unchecked.
According to this article featured in the Washington Post, the pressure you put on your neck by bending and staring at your phone is much like bending your finger back as far as it will go, and then keeping it in that position for approximately an hour. Day after day, such stress is bound to lead to complications.
Resulting Injuries from Text Neck
The strain put on the neck by text neck is enough to cause mild to severe injuries, including:
Sore muscles
Inflamed Tissues
Pinched nerves
Herniated discs
Elimination of the natural curve of the neck
These injuries can cause considerable pain and discomfort and may lead to further health complications. They can lead to neck and back pain that can last for years.
Tips to Avoid Text Neck
Smartphones offer numerous benefits and opportunities for enjoyment, so it is unlikely that most people will stop using them. Luckily, there are things you can do to protect yourself, including:
Work Your Eyes, Not Your Neck
One of the simplest ways to avoid text neck is to look down with your eyes instead of tilting your head down. While it may not be practical to always use this technique, it is certainly useful in many circumstances. Your eyes can tilt down with little effort and can allow you to lessen the tilt of your neck as you use your phone.
Strength Train your Neck & Shoulder Muscles
You will inevitably do some head tilting as you use your phone throughout the day. Strengthening the muscles that support your head is one way to protect your delicate neck tissues and maintain mobility. Simple exercises like turning your head each way repeatedly and using your hands to provide resistance can make your neck much stronger. Your shoulders also provide a lot of support for your neck. Shoulder exercises can increase the stability of your neck as well.
Have an Awareness of Your Head Position
Just maintaining awareness of how your head is tilted as you use your phone can help you avoid excessive tilting. Practice looking at your smartphone with your head upright to remind yourself of what good posture feels like, and pay attention during the times you deviate from good posture.
Chiropractic Treatment
If you are experiencing neck pain from text neck, or from any other type of injury, chiropractic can help. Please contact us now to schedule your appointment and get some relief!
Text neck is a very real condition that is caused by staying in a prolonged �texting� position � hunched shoulders and neck tilted forward. As a result, the back, neck, and shoulder muscles become overworked and your spinal structure is actually changed. Many people who spend a lot of time on their mobile devices such as smartphones and tablets, develop this condition (and others including �cellphone elbow� and tendinitis of the wrist and hand) and it can be very painful, even causing mobility problems. More than 95% of Americans have a smartphone or mobile device and most people spend a great deal of time on their devices � it is easy to see how this is a common problem.
What Exactly is Text Neck?
A normal human neck has a slight curve to it that travels along the spine. It is part of the intricate system that supports the head and body. However, a person with text neck will have a straight cervical spine. Their neck will not have that slight curve and that is a problem.
The cause of the absence of the curve is because of the position that the head stays in for such long periods of time. The average adult human head weighs between 10 and 12 pounds. When the head is upright, the neck supports it and the slight curve gives it the stability that it needs.
When you keep your head tilted forward, such as when you are hunched over your smartphone or mobile device, your head is thrust forward instead of sitting over the balanced curve of the cervical spine. The gravitational pull is greatly increased and the neck is already in an unnatural position. This combination places unnatural and damaging stress on your neck. It is like carrying around an additional 60 pounds on your neck.
Symptoms of Text Neck
In the early stages of text neck, a person may feel some tightness in their shoulders, neck, and upper back. This may progress to discomfort in those areas and eventually pain. If left untreated, you can develop pinched nerves and herniated discs.
Your central nervous system begins at the base of your skull, so it extends down your neck and upper back. When you put unnatural pressure on your neck, you are also affecting your nervous system, causing it to malfunction. This can lead to pain throughout your body, stiffness, headaches, low back pain, and problems with your hands and arms.
How to Prevent Text Neck
Text neck is surprisingly easy to prevent. Your first step is awareness. Over two or three days, take some time to be very aware of your body�s position. Carefully examine your posture while you go about all of your daily activities. It is important to remember that text neck is not strictly confined to texting. You can get it any time you have your head bent down for an extended period of time, such as when looking at a laptop screen or even writing for a long time.
The best way to avoid the problem is to keep your devices at eye level. If you have a handheld device, hold it up at the level of your eyes instead of bending your neck to look down. The same goes for your laptop; arrange it so that your screen is at eye level.
Chiropractic for Text Neck
If you are already suffering from the effects of text neck, your chiropractor can help reverse the condition if it hasn�t progressed to disc degeneration (even then he or she can help with associated pain). Regular chiropractic treatments, along with following expert recommendations for screen heights, can help reduce the pain and discomfort. It is smart to address these issues before they become a bigger problem. Your chiropractor can help.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine