The body is a functional machine that consists of muscles, organs, and skeletal joints that play different parts in making the body healthy as possible. Each section has a casual relationship as they work together and do their jobs separately. The muscles provide protection and movement from daily activities. The organs supply hormones, oxygen, and nutrients, so the body’s internal functions work correctly. And finally, the skeletal joints help with mobility and stabilization for the body to stay upright. When environmental factors or traumatic injuries affect the body, many issues over time may cause damage, and the body may develop pain-related symptoms. Today’s article examines how the musculoskeletal system works in the body, how trigger points affect the musculoskeletal system, and how chiropractic care can help alleviate trigger point pain. We refer patients to certified providers specializing in musculoskeletal treatments to aid individuals suffering from muscle pain associated with trigger points. We also guide our patients by referring them to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
How Does The Musculoskeletal System Works?
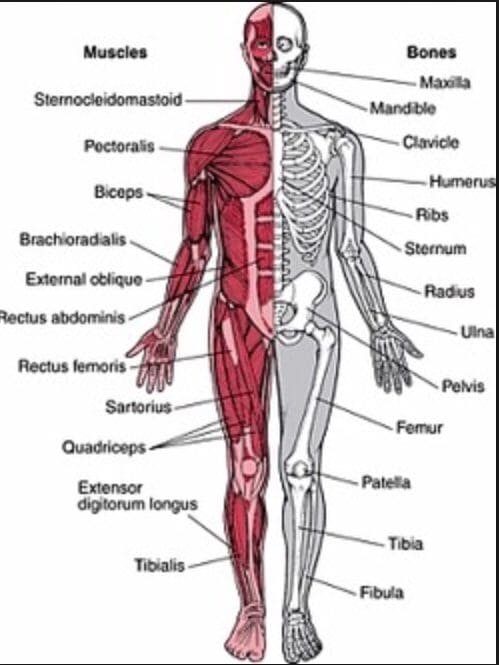
Have you been experiencing muscle stiffness in specific areas located in your body? Do you feel tenderness in your neck, shoulders, or back? Or do you feel knots along your muscles that are causing you pain? Some of these symptoms are associated with muscle pain in the musculoskeletal system. The musculoskeletal system in the body has muscles, ligaments, and connective tissues surrounding the skeletal joints. Studies reveal that the structure of the musculoskeletal system shows how the surrounding muscles protect the joints and help provide the body functionality. The various muscles in the body offer a range of motion, sensory-motor functions, reflexes, and strength when functioning normally. However, when environmental factors begin to affect the body over time, it can lead to musculoskeletal disorders associated with pain. Studies reveal that when the body succumbs to pain related to musculoskeletal disorders. Musculoskeletal disorders are a common issue that has affected many individuals worldwide and causes various disabilities and symptoms that affect the body. Some of the musculoskeletal disorder symptoms that affect the body include:
Burning sensations
Muscle twitches
Fatigue
Stiffness and aching
Myofascial trigger pain
How Do Trigger Points Affect The Body?
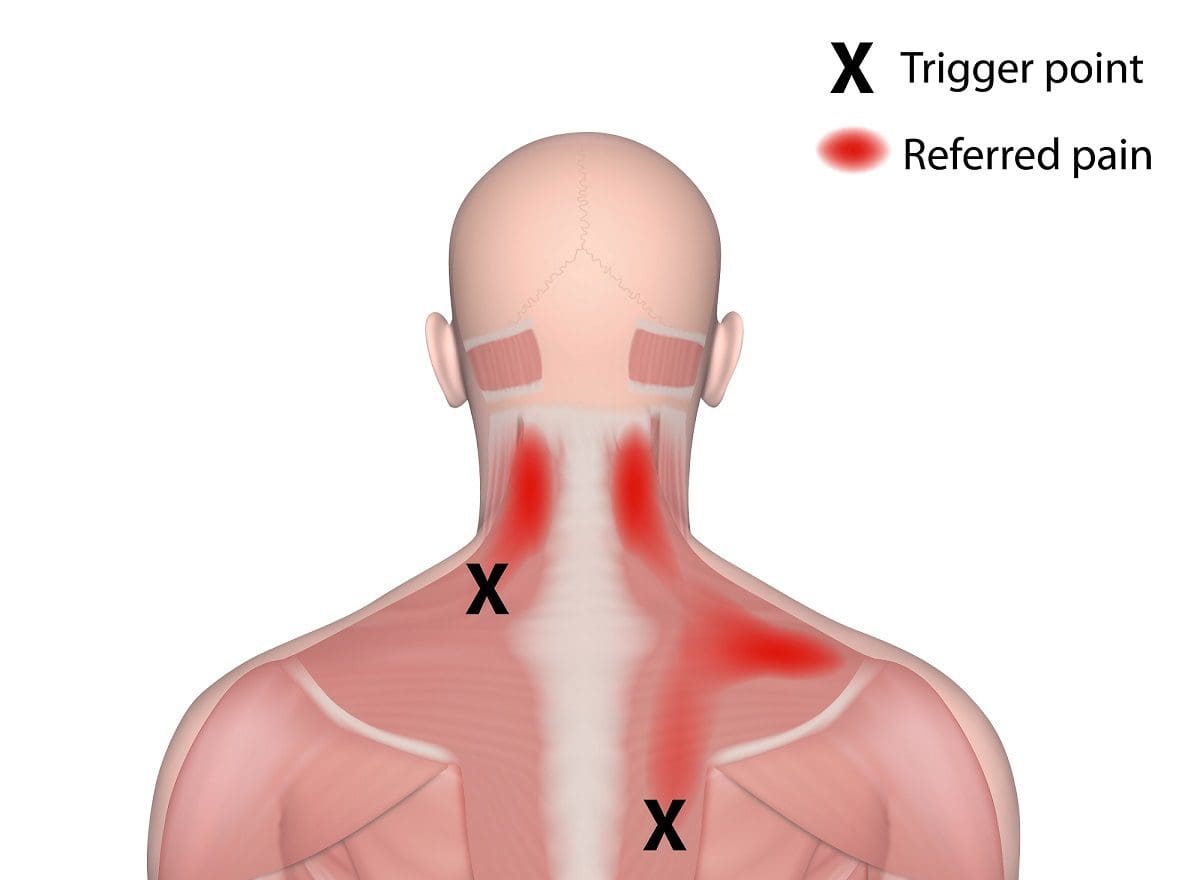
One of the musculoskeletal symptoms associated with muscle pain is trigger points or myofascial pain. Myofascial pain is a common condition involving the muscles and surrounding connective tissues that may be acute or chronic depending on where the pain is located. While trigger points refer to hard palpable nodules in the taut bands of the skeletal muscle that can be active (causes spontaneous pain or abnormal sensory symptoms) or latent (causes no spontaneous pain but shows operational myofascial trigger points characteristics). Studies reveal that myofascial pain can be associated with muscle dysfunction, weakness, and limited range of motion that affects the body. A knot in the muscle in certain body areas can make the muscle hyperirritable, causing painful compression while invoking characteristic referred pain and autonomic phenomena in the body. To that point, it can be difficult for doctors to diagnose since trigger points are caused by traumatic events in the body and can occur in different spots in different people. Trigger points can form all over the body, including:
Neck
Mid-back
Low back
One common characteristic when trigger points affect the body is that they can travel or even spread to the surrounding muscles.
Myofascial Pain Syndrome & Trigger Points- Video
Have you been feeling pain located in your neck, back, or particular areas in your body? What about feeling pain in a different location of your body? Or have you experienced muscle stiffness or tenderness in certain areas of your body? If you have been experiencing these symptoms associated with muscle pain, you could be dealing with trigger point pain or myofascial pain in your musculoskeletal system. The video above explains myofascial pain and trigger points and how they affect the body. Studies reveal that myofascial pain is caused by myofascial trigger points that produce exquisitely tender spots in the taut bands of hardened muscles. To that point, it stimulates local and referred pain amongst other sensory, motor, and autonomic symptoms. Myofascial trigger points can cause stiffness and weakness in the involved muscle, making it difficult to diagnose since it can cause pain in different body areas. Fortunately, there are ways to alleviate trigger point pain associated with myofascial pain syndrome from the body.
How Chiropractic Care Alleviates Trigger Point Pain
Since myofascial trigger point pain can be challenging to diagnose, it can range from neck to low back pain in different locations and mimic other pain conditions that affect the body. It can affect the body to become hypersensitive and hyperirritable while decreasing a person’s overall sense of well-being. Luckily, treatments like chiropractic care can help alleviate trigger point pain and help manage myofascial pain syndrome. Chiropractic care is not just for the skeletal system but can help relieve muscle pain associated with myofascial pain. Since the muscles are layered and interwoven around the joints, they play an integral part in supporting the body. Studies reveal that chiropractors are great at finding trigger points and utilize specific exercises and physical modalities to treat myofascial pain syndrome symptoms. Some of the benefits chiropractic care use include:
Breaking up scar tissue
Applying pressure on the trigger point
Aligning the spine to reduce the spinal subluxation
Ease muscle pain
Conclusion
The body consists of muscles, organs, and joints in a casual relationship that helps function and stabilizes the host. The musculoskeletal system has muscles, tissues, and ligaments that are interwoven and layered, surrounding the skeletal joints to prevent injuries or traumatic events from affecting the body. When the body does suffer from damages caused by traumatic events, it can lead to a musculoskeletal disorder known as myofascial pain or trigger pain. Trigger pain is when the muscles have knots along taut bands of the muscle that can cause muscle stiffness and pain. Trigger point pain can be challenging to diagnose since the pain can travel from one location to another section of the body. This is referred pain, and myofascial trigger pain can mimic other chronic musculoskeletal symptoms. Treatments like chiropractic care can help alleviate myofascial trigger pain through spinal manipulation and trigger point therapy, thus relieving the stiff muscle causing pain. Incorporating treatments like chiropractic care can help loosen stiff muscles, increase joint range of motion and bring a person’s wellness back.
References
Bron, Carel, and Jan D Dommerholt. “Etiology of Myofascial Trigger Points.” Current Pain and Headache Reports, Current Science Inc., Oct. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3440564/.
Murphy, Andrew C, et al. “Structure, Function, and Control of the Human Musculoskeletal Network.” PLoS Biology, Public Library of Science, 18 Jan. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5773011/.
Shah, Jay P, et al. “Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective.” PM & R : the Journal of Injury, Function, and Rehabilitation, U.S. National Library of Medicine, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4508225/.
The body is exposed to various environmental factors daily. Whether it is the environment that a person is living, the foods being consumed, or the level of physical activities a person has plays a part in the body. Many individuals that want to live a healthier lifestyle will start small by incorporating nutritious foods they can add, sticking to an exercise regime they might enjoy, and finding time to meditate. Those who don’t want to change their lifestyle habits will continue eating foods that are high in fats, not exercising enough, or have problems sleeping. Over time, the body will be at risk of developing autoimmune disorders associated with musculoskeletal symptoms when exposed to environmental factors that impact a person’s lifestyle. Today’s article looks at an autoimmune disorder that causes inflammatory effects on the joints, known as polymyalgia rheumatica, the symptoms associated with this disorder, and how chiropractic care can help manage the symptoms of polymyalgia rheumatica. We refer patients to certified providers specializing in autoimmune treatments to help many individuals with autoimmune diseases associated with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Polymyalgia Rheumatica?
Have you been experiencing pain along your shoulders, neck, hips, or thighs? Does your body feel stiff in the morning and better throughout the day? Or have you been experiencing a limited range of motion in certain areas of your body? Many of these symptoms are signs that you might be at risk of developing polymyalgia rheumatica in your joints. Polymyalgia rheumatica is defined as a rheumatic disorder that is common in elderly adults over the age of 50. Polymyalgia rheumatica is an inflammatory musculoskeletal disorder that induces muscle pain and stiffness around the joints, especially in the morning. Studies reveal that polymyalgia rheumatica is often characterized by aching muscle pain in the shoulders, pelvis, and neck; it can mimic other rheumatic diseases like RA (rheumatoid arthritis), SLE (systemic lupus erythematosus), and polymyositis. When the body is dealing with the inflammatory effects of polymyalgia rheumatica, many people believe they are dealing with a different disorder affecting their bodies. To that point, diagnosing polymyalgia rheumatica is difficult.
The Symptoms Associated With Polymyalgia Rheumatica
Since polymyalgia rheumatica can mimic other rheumatic diseases, some of the symptoms associated with this inflammatory musculoskeletal disorder are similar to other chronic common diseases in the body. Studies reveal that the cause of polymyalgia is unknown, but environmental and genetic factors contribute to this inflammatory disease. Another disease that shares similar symptoms with polymyalgia is a disease known as giant cell arteritis. Giant cell arteritis causes inflammatory effects along the lining of the arteries, and individuals with this disease may have polymyalgia rheumatica. Some of the symptoms associated with polymyalgia rheumatica include:
Shoulder pain
Pelvic pain
Limited range of motion
Muscle stiffness
Joint pain
Inflammation
Neck pain
An Overview Of Polymyalgia Rheumatica- Video
Have you been experiencing pain in some regions of your body, like the shoulders, pelvis, and neck? Do you feel muscle stiffness every morning, but does it get better throughout the day? Have you been dealing with joint inflammation? If you have been experiencing these musculoskeletal symptoms, you might be at risk of developing polymyalgia rheumatica. The video above gives an insightful overview of what polymyalgia is and the symptoms associated with this inflammatory musculoskeletal disorder. Polymyalgia rheumatica is an auto-inflammatory musculoskeletal disorder that affects many adults over 50 and causes muscle stiffness in the body’s neck, shoulder, and pelvic regions. This inflammatory musculoskeletal disorder does mimic other rheumatic disorders like RA (rheumatoid arthritis) and lupus. The symptoms associated with polymyalgia rheumatica are generally similar to other common chronic disorders, making diagnosis challenging to pinpoint. Luckily there are ways to manage polymyalgia rheumatica and its associated musculoskeletal symptoms.
Managing Polymyalgia Rheumatica With Chiropractic Care
Since the body is dealing with symptoms from polymyalgia rheumatica is challenging to diagnose since it mimics other rheumatic disorders and their associated symptoms. When the body is suffering from joint pain associated with polymyalgia rheumatica, the surrounding muscles, and ligaments that help stabilize the joints become inflamed and cause discomfort to the body. Fortunately, treatments like chiropractic care are available to help manage the joint inflammation associated with polymyalgia rheumatica. Chiropractic care utilizes spinal manipulation of the body by manipulating spinal subluxation or misalignment of the joints. Spinal manipulation helps the body relax and incorporates healing properties into the inflamed joints. Chiropractic care helps loosen up the stiff muscles and ligaments surrounding the joints to reduce pressure on the nerves and help bring the range of motion back to the joints. Many individuals who incorporate chiropractic care to help manage musculoskeletal symptoms associated with rheumatic disorders like polymyalgia rheumatica will be pain-free on their wellness journey.
Conclusion
Polymyalgia rheumatica is an inflammatory musculoskeletal disorder common in elderly adults that induces muscle pain and stiffness around the joints. This inflammatory musculoskeletal disorder affects the shoulder, neck, and pelvic region while mimicking other rheumatic disorders like RA (rheumatoid arthritis) and lupus. Since the body is exposed to various environmental daily, over time may be at risk of developing autoimmune diseases associated with musculoskeletal symptoms that can impact the individual. To that point, making it difficult to diagnose. Fortunately, treatments like chiropractic care can help manage the musculoskeletal symptoms associated with polymyalgia rheumatica. Chiropractic care can help reduce stiff joint inflammation by manipulating the body, causing the aching muscles to relax and increase their range of motion. Utilizing chiropractic care can help a person get back to their health and wellness journey.
References
Acharya, Saurav, and Rina Musa. “Polymyalgia Rheumatica – StatPearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 21 June 2022, https://www.ncbi.nlm.nih.gov/books/NBK537274/.
Al-Kaabi, Juma, et al. “Non-Hodgkin Lymphoma Mimicking Polymyalgia Rheumatica in a Young Patient.” Oman Medical Journal, OMJ, July 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3282323/.
Michet, Clement J, and Eric L Matteson. “Polymyalgia Rheumatica.” BMJ (Clinical Research Ed.), BMJ Publishing Group Ltd., 5 Apr. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2287267/.
Milchert, Marcin, and Marek Brzosko. “Diagnosis of Polymyalgia Rheumatica Usually Means a Favourable Outcome for Your Patient.” The Indian Journal of Medical Research, Medknow Publications & Media Pvt Ltd, May 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5644293/.
The muscles, tissues, and ligaments help stabilize the joints and structure of the spine so that the body can function. These muscles are layered and interwoven in the spine and joints that help facilitate movement. When the body suffers from injuries or traumatic events, the muscles, tissues, and ligaments become affected, causing muscle pain and discomfort. This causes the muscles to be tender to the touch and sensitive. This is known as myofascial pain syndrome. Today’s article looks at myofascial pain syndrome, how it is linked with central sensitization, and ways to manage myofascial pain syndrome. We refer patients to certified providers specializing in musculoskeletal treatments to help many individuals with myofascial pain syndrome associated with central sensitization. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Myofascial Pain Syndrome?
Have you been experiencing muscle tightness in different areas of your body? Have you felt your muscles tender to the touch? Or have you been having trouble sleeping? Many of these overlapping risk factors are signs that you might have myofascial pain syndrome. The term “myofascial” is split into two parts. “Myo” refers to the muscles, while “fascia” refers to the connective tissues found throughout the body. So myofascial pain syndrome is where there is muscle pain in various forms, which includes the muscle tissues, connective tissues, or both. Studies reveal that myofascial pain syndrome originates from trigger points in the skeletal muscle, causing the affected muscle to be in pain. The trigger points in the body’s skeletal muscles are the “knots” people feel when their muscles feel tight. These trigger points are challenging to identify because they occur in different areas causing referred pain (pain in one place but in another body area).
How Central Sensitization Link To Myofascial Pain Syndrome?
Studies reveal that central sensitization in the body is represented as an enhancement in neuron function and circuits in the nociceptive pathways that increases membrane excitability and synaptic efficacy. To that point, it reduces inhibition and manifests the remarkable plasticity of the somatosensory nervous system. The nociceptor inputs can trigger and manifest central sensitization as pain hypersensitivity when the body suffers from an injury. So how is central sensitization linked to myofascial pain syndrome? Let’s use fibromyalgia as an example. Many individuals dealing with myofascial pain may be potentially involved with fibromyalgia. This is due to fibromyalgia being a chronic condition that features widespread pain, and this causes the body to be more sensitive to pain. Central sensitization linked to myofascial pain syndrome can mimic fibromyalgia symptoms in the body, causing muscle pain and discomfort.
An Overview Of Myofascial Pain Syndrome-Video
Are you experiencing muscle weakness or soreness in some regions of your body? Have you dealt with chronic fatigue or poor sleep quality? Or have you been dealing with headaches constantly throughout the entire day? Many of these symptoms are signs that you might be at risk of developing myofascial pain syndrome. The video above explains myofascial pain syndrome, the symptoms, and the causes that affect the body. Studies reveal that myofascial pain has two types of trigger points:
Active trigger points associated with muscle pain without movement
Latent trigger points associated with muscle pain with movement
Myofascial pain syndrome can vary in acute or chronic forms and can range from mild to severe while being in different locations, making it very difficult to pinpoint where the pain is localized. Fortunately, there are ways to manage myofascial pain syndrome in the body that can help with the pain.
Ways To Manage Myofascial Pain Syndrome
When managing myofascial pain syndrome, many individuals dealing with muscle pain will take pain medication to alleviate it; however, that only minimizes the pain for a short period. One way to manage myofascial pain syndrome is by utilizing chiropractic care as part of treatment. Chiropractic care is non-invasive and often the preferred treatment for individuals with myofascial pain syndrome due to its effectiveness and drug-free approach. Chiropractors are not only good at finding the trigger points, but they are good when it comes to treating them using various techniques. Studies reveal that chiropractors use direct pressure on the trigger points to relieve the pain with their hands or specific tools. Incorporating chiropractic care provides the body with an increase in muscle strength, flexibility, and range of motion. Since chiropractic care is a whole-body approach, it allows many people with myofascial pain syndrome to have a better quality of life and learn healthy habits, which include diet, exercise, and mental health, while living with less or no pain at all.
Conclusion
The body has muscles, tissues, and ligaments that help stabilize the joints and structure of the body, so there is functionality. These muscles help facilitate movement since the muscles are interwoven in the spine and joints. When the body suffers from a traumatic event or an injury, the muscles, tissues, and ligaments become affected. This causes muscle pain and discomfort, known as myofascial pain, where the trigger points cause pain in the body and can occur in different areas. Myofascial pain can be challenging to diagnose since it can be on one side of the body but affects a different section, known as referred pain. Fortunately, treatments like chiropractic care can help manage myofascial pain by treating the pain and using direct pressure to alleviate the pain. Incorporating chiropractic care to manage myofascial pain can help many individuals be pain-free on their health and wellness journey.
References
Bordoni, Bruno, et al. “Myofascial Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 18 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK535344/.
Desai, Mehul J, et al. “Myofascial Pain Syndrome: A Treatment Review.” Pain and Therapy, Springer Healthcare, June 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4107879/.
Latremoliere, Alban, and Clifford J Woolf. “Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity.” The Journal of Pain, U.S. National Library of Medicine, Sept. 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2750819/.
When many individuals look for ways to relax after a stressful event in their daily lives, many people have an exercise regime that allows them to take their minds off of their hectic lives. When finding the proper exercise, it is best to consider that everybody is different and has different fitness levels. Many individuals could be dealing with chronic issues that affect them drastically and with so much pain in their bodies. When these chronic issues overlap with muscle and joint pain, it can make the body dysfunctional while potentially being involved in environmental factors. Yoga is a low-impact exercise that helps tone muscles, relax tension in the body, and focus on deep breathing. Today’s article looks at the benefits of yoga for the body, how chiropractic care works together with yoga, and different yoga poses can help manage various chronic issues. We refer patients to certified providers specializing in musculoskeletal treatments to help many individuals with musculoskeletal problems affecting their bodies. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Benefits of Yoga For The Body
Have you been dealing with chronic stress affecting your quality of life? Have you been dealing with bladder or gut issues constantly? What about feeling muscle stiffness in your back, neck, shoulders, or pelvic regions? Some of these symptoms are signs that you could risk developing musculoskeletal problems associated with pain. Dealing with musculoskeletal issues related to pain can make a person feel miserable and have stress affecting their bodies. Yoga is a low-impact exercise that doesn’t put pressure on the joints and will provide a full-body workout through strengthening and stretching weak muscles. Yoga has many benefits for many individuals that are dealing with the following:
Studies reveal that environmental factors are involved in non-specified chronic pain in the spine, overlapping musculoskeletal disorders causing many individuals to try to find relief. Many individuals incorporate yoga because it is a safe and effective way to alleviate various forms of back, neck, or pelvic pain causing issues to the body. Yoga utilizes gentle stretching and strengthening of weak, injured muscles while increasing blood circulation to promote healing in the body.
Chiropractic Care & Yoga
When people are dealing with health conditions or injuries that have affected their bodies, it can make them feel frustrated and think their injuries are taking forever to heal. Many individuals don’t realize that incorporating yoga practices provides impressive health benefits while mirroring the similar foundations of chiropractic care. Both chiropractic care and yoga provide many beneficial results to an aching body that needs a good stretch and ready the body to heal itself naturally. Chiropractic care includes spinal manipulation to the spinal joints while reducing inflammation and strengthening weak muscles. Yoga allows the body to increase its flexibility and stamina, reduces stress and blood pressure, and provides a better sense of breathing and balance.
Yoga For Chronic Pain-Video
Have you felt muscle stiffness in your neck, back, or body? Have you felt sluggish or overly stressed from your day-to-day lives? Do you want to improve your balance? If you have been experiencing these issues affecting your quality of life, why not incorporate yoga as part of your exercise regime? The video above shows that yoga poses for chronic pain affect the body, including the neck, back, and pelvic regions. Studies reveal that yoga can help relieve intense neck pain while improving pain-related function disability. Yoga allows the muscles to not only relax but strengthen them as well. Yoga can also help improve the body’s range of motion through deep breathing and give more awareness of how the body holds tension in places a person hasn’t realized they were holding onto.
Yoga Poses For Different Issues
When a person does yoga, they will go through various poses and repeat them constantly as their body begins to get used to the movements. This allows the body to challenge itself and helps the individual focus more on deep breathing. A good example would be an individual taking a yoga class due to experiencing pelvic pain. By going through each yoga pose, many individuals suffering from pelvic pain will reduce the pain intensity while improving their quality of life. Below are some yoga poses that anyone can do to reduce pain associated with their back, neck, or pelvis.
Bridge Pose
Lie on your back
Bend both knees while placing the feet on the floor at hip-width apart
Arm on the sides with palms facing down
Press feet to the floor and lift the hips as you inhale
Engage the legs and buttock
Hold 4-8 breaths and exhale to lower the hips back to the ground slowly
Cobra Pose
Lie on your stomach with hands near the chest just under the shoulders and fingers facing forward
Keep elbows close to sides
Press hands on the floor and slowly lift your head, chest, and shoulders while slightly bending the elbows by inhaling
Exhale to go back down slow and rest your head
Cat-Cow
Be on all fours, hands under the shoulders and knees under hips (Think like a table)
Inhale to lower your core to the floor as your head looks up to the sky
Exhale slowly to lower your chin to the chest as you round your back
Continue fluid motion for a minute
Forward Bend
Be in a standing position, and feet are at a hip distance apart
Lengthen the body as you lean forward while keeping the knees slightly bended
Place hands on either legs, yoga block, or the floor (Whichever makes you comfortable)
Tuck the chin into the chest, letting the neck and head relax
Gently rock your head side to side to relieve tension in the neck and shoulders
Slowly roll up to a standing position allowing the arms and head to be the last to rise
Supine Spinal Twist
Lie on your back while your knees bent and feet flat on the floor
Extend arms out of the side and place palms down on the floor
As you inhale, breathe into the gut and lower limbs
Exhale to lower knees on the left side (Look at the opposite way to slowly stretch the neck and shoulder muscles)
Pay attention to the stretches for 5 breathes as well as the lengthening sensations on the ribs
Return the knees to the middle and repeat on the right side
Child’s Pose
Sit back on the heels with the knees together (For added support, you can use a rolled-up blanket under your knees)
Bend forward and walk hands in front of you
Gently rest your forehead on the floor
Keep arms extended in the front while focusing on relieving tension in the back as the upper body falls to the knees
Stay in that pose for 5 minutes
Conclusion
Incorporating yoga as part of an exercise regime allows the individual to focus on deep breathing while calming the mind. Yoga is a low-impact exercise that helps strengthen weak muscles associated with pain and inflammation. Yoga provides a full-body workout that benefits many people dealing with chronic pain. Utilizing yoga as part of a daily practice might help individuals learn to be calm and practice mindfulness.
Crow, Edith Meszaros, et al. “Effectiveness of Iyengar Yoga in Treating Spinal (Back and Neck) Pain: A Systematic Review.” International Journal of Yoga, Medknow Publications & Media Pvt Ltd, Jan. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4278133/.
Li, Yunxia, et al. “Effects of Yoga on Patients with Chronic Nonspecific Neck Pain: A Prisma Systematic Review and Meta-Analysis.” Medicine, Wolters Kluwer Health, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6407933/.
Saxena, Rahul, et al. “Effects of Yogic Intervention on Pain Scores and Quality of Life in Females with Chronic Pelvic Pain.” International Journal of Yoga, Medknow Publications & Media Pvt Ltd, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5225749/.
Everyone has headaches at some point throughout their lives, which can be excruciating, depending on the severity. Whether it is a heavy workload that causes a person to have severe tension on their foreheads, allergies that cause immense pressure in between the sinus cavity in the middle of the face, or common factors that seem to cause a pounding sensation in the head, headaches are no joke. Often, headaches seem to go away when it’s in their acute form but can become chronic when the pain doesn’t go away, causing issues to the eyes and muscles. Today’s article looks at how headaches affect the body and how they can become a somatovisceral problem for many individuals. We refer patients to certified, skilled providers specializing in neurological treatments that help those individuals that are suffering from headaches. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
How Headaches Affect The Body
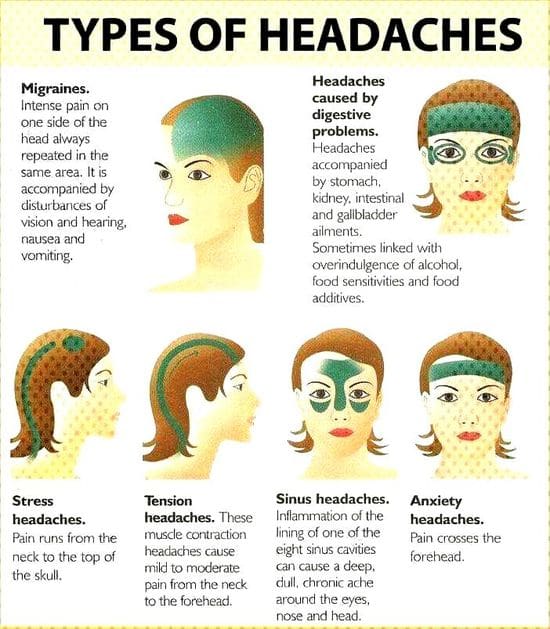
Do you feel a pounding sensation in your forehead? Do your eyes seem to become dilated and sensitive to light? Do both arms or hands seem to lock up and have a pins-and-needles sensation that feels uncomfortable? These signs and symptoms are various forms of headaches affecting the head. The head helps protect the brain from damage as the neuron signals from the central nervous system are connected to the cervical regions of the spine. When factors like lifestyle habits, dietary food intake, and stress affect the central nervous system, they begin to co-mingle to form various forms of headaches. Each form of headache continuously shifts in many suffering individuals to never sit still for their clinicians to capture their specific profile. Some of the multiple headaches include:
Tension headaches
Migraines
Stress headaches
Sinus pressure
Clustered headaches
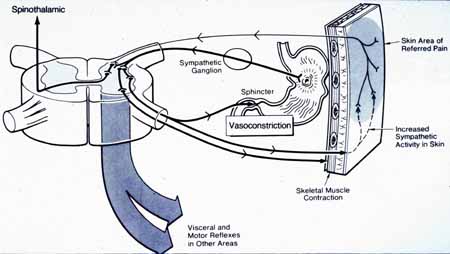
When headaches begin to affect the neck and head, research shows that these headaches cause a convergence between the cervical sections of the spine and the skull base. This becomes a mediator for the neck and head to develop referred pain. Referred pain is known as pain that occurs in one section of the body than where it is located. For example, say someone has been through a traumatic injury that causes them to have whiplash in their neck; that pain in their neck muscles can mimic a headache affecting one side of their head. Additional information has mentioned that migraine headaches can cause chronic inflammatory issues in the gut-brain axis, causing dysfunctional autonomic and enteric nervous systems and affecting the body.
How The Body Deals With Migraines-Video
Have you experienced throbbing in various sections of your face? Do you feel your muscles tense up around your neck or shoulders? Or does your body feel exhausted that noise seems to cause immense pain? The various forms of headaches can cause many problems not only in the neck but in the body as well. The video above shows what happens to the body when a person is suffering from a migraine. Research studies have noticed that individuals suffering from migraines will develop associated somatic comorbid symptoms like anxiety and depression, making migraine headaches more frequent. At the same time, being the top three of the most common forms of headaches, migraines may share a common underlying mechanism involving the overlapping profiles of the cerebrovascular system that is equivalent to a repetitive stress disorder affecting the central nervous system.
How Headaches Are A Somatovisceral Problem
Research studies have found that the severity of the headache in a person, especially in women, causes a synergetic relationship that causes somatic symptoms and depression to be so high. This is due to the overlapping risk profiles that affect the mechanisms of the sympathetic nervous system, causing the production of cervicogenic headaches and chronic migraines to form. This is because the junction of the brain stem and the spinal cord is called the trigeminocervical nucleus and overlaps the nociceptive cells. When this happens, The close anatomic pain fibers from the cervical spine and the trigeminal system start to be aggravated; it creates pain impulses from the neck to the head, causing headaches to be interpreted.
Conclusion
Overall, headaches are no joke when they start to affect the body and cause mimic pain in different parts of the body. When various factors begin to cause somatic issues that tense the muscles but also affect the surrounding nerves, it can cause headaches to form and become excruciating. Different forms of headaches can affect other regions of the face and can go away for a short period in their acute form. However, in its chronic condition, it can cause the body to be in so much pain. Finding ways to prevent headaches from progressing further can benefit the individual.
References
Castien, René, and Willem De Hertogh. “A Neuroscience Perspective of Physical Treatment of Headache and Neck Pain.” Frontiers in Neurology, Frontiers Media S.A., 26 Mar. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6443880/.
Cámara-Lemarroy, Carlos R, et al. “Gastrointestinal Disorders Associated with Migraine: A Comprehensive Review.” World Journal of Gastroenterology, Baishideng Publishing Group Inc, 28 Sept. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5037083/.
Maizels, Morris, and Raoul Burchette. “Somatic Symptoms in Headache Patients: The Influence of Headache Diagnosis, Frequency, and Comorbidity.” Headache, U.S. National Library of Medicine, 2004, https://pubmed.ncbi.nlm.nih.gov/15546261/.
Tietjen;Brandes JL;Digre KB;Baggaley S;Martin V;Recober A;Geweke LO;Hafeez F;Aurora SK;Herial NA;Utley C;Khuder SA;, G E. “High Prevalence of Somatic Symptoms and Depression in Women with Disabling Chronic Headache.” Neurology, U.S. National Library of Medicine, 9 Jan. 2007, https://pubmed.ncbi.nlm.nih.gov/17210894/.
The neck can make sure that the head doesn’t flop around by letting the muscles, ligaments, and the spine hold the head upright. The neck is responsible for twisting and turning the head in all directions without the feeling of discomfort. However, the neck also has soft tissues, and nerve roots spread out from the cervical area of the spine that helps control the shoulders, arms, and hands. When a person suffers from a neck injury, it can cause unwanted pain and discomfort to the neck muscles and disrupt the motor functions in the upper body. Luckily, some treatments help alleviate the pain and restore motor function to the neck. Today’s article post will examine how cervical stenosis affects the neck and the cervical spine and how traction therapy can help alleviate cervical stenosis for many suffering individuals. Patients are referred to qualified, skilled providers who specialize in spinal decompression therapy. We go hand in hand with our patients by referring them to our associated medical providers based on their examination when it’s appropriate. We find that education is valuable for asking crucial questions to our providers. Dr. Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
How Does Cervical Stenosis Affect The Neck?
Has your neck been feeling stiff lately? Do you suffer from any pain in your neck after stretching from side to side? How about feeling discomfort after being hunched over for an extended period? All these issues are due to neck pain, and if a traumatic event or injury affects the neck even more, it can lead to the development of cervical stenosis. Like the lower back, the neck can also be injured as the soft tissues, and nerve roots spread out from the cervical area are compressed and aggravated. Research studies have found that cervical stenosis develops when the spinal column in the cervical spine becomes narrow due to either degenerative spinal changes or traumatic incidents. When the spinal canal becomes more limited, it can cause unwanted neck issues like cervical herniation and neck pain. If the nerve roots are aggravated due to being compressed, it can disrupt the sensory-motor function of the shoulders and arms, and hands. Additional information has shown that the symptoms of cervical stenosis symptoms develop gradually over time as there is no pain in the early stages. However, as cervical stenosis begins to progress in compressing the spinal canal and provoking the nerve roots, motor functions in the hands will start to lose their function in writing or grasping items. This can become a problem for many individuals if cervical stenosis is not treated immediately.
What Other Causes Does It Do To The Cervical Spine?
Since cervical stenosis progresses gradually without any pain symptoms in the early stages and becomes worse in the advanced settings, other causes can start affecting the neck and cervical spine. One of them is cervical myelopathy. Research studies have shown that it is a condition where the spinal cord becomes compressed and causes a disturbance in the upper extremity portions. When the upper part of the body begins to feel sharp electric sensations radiating from the neck down to the hands, it can cause muscle weakness and numbness in each section of the upper body. Other causes like natural degenerative issues can also result from cervical stenosis occurring in the cervical spine. Other research studies have shown that degenerative causes associated with cervical stenosis can activate pro-inflammatory factors in the spinal joints and cause excruciating swelling and pain-like symptoms along the spine. However, there are treatments to help reduce the pro-inflammatory markers and alleviate spinal cord compression along the cervical spine.
Traction Therapy For Cervical Stenosis-Video
Do you have neck pain? Do your shoulders feel tight and tense? Have you lost the sensation in your hands? Traction therapy alleviates spinal stenosis in the cervical area and has given many beneficial factors for people who need neck pain relief. Experiencing cervical stenosis can dampen a person’s day and progressively worsen if it is not treated right away; traction therapy can help alleviate cervical stenosis. The video above shows how traction therapy works using the cervical mechanics from the Chatanooga decompression table. Cervical traction helps loosen up the tight muscle tissues and resets the cervical spine by setting it back in its proper alignment. This allows the spinal cord and nerve roots to feel relief from the pressure they’ve been under. Cervical traction also helps rehydrate the dry spinal discs with the nutrients beneficial to the body. This link will explain what traction has to offer and the impressive results for many individuals who suffer from cervical spinal stenosis or other issues that occur in the neck.
Traction Therapy To Alleviate Cervical Stenosis
Many treatments associated with neck pain do have beneficial results when people are trying to relieve the pain. Some people use ice/hot packs to ease tense neck muscles, while others take over-the-counter medicine to stop the pain for the remainder of the day. Traction therapy is one treatment that seems to alleviate the pain and help restore the cervical spine. Research studies have mentioned that cervical traction is a non-surgical procedure that uses a tension pull on the cervical spine to increase the height of the spinal disc and take the pressure off the spinal cord and surrounding nerve roots. Traction on the cervical spine helps relax the neck muscles while also providing much-needed relief to the cervical spine. Additional research mentioned the beneficial properties that cervical traction offers to help separate the vertebral bodies while providing movement on the facet joints and gently stretching the soft tissues.
Conclusion
The neck makes sure that the head stays upright and can make everyday motions without feeling pain or discomfort. When traumatic events or injuries affect the sensory-motor functions of the neck, it can narrow the spinal canal in the cervical spine and cause many unwanted symptoms like cervical stenosis. Cervical stenosis can develop over time and can progressively become worse if it is not treated right away. Some of the symptoms can induce muscle weakness, numbness, and pain along the neck, shoulders, arms, and hands in the body’s upper portion. Traction therapy for the cervical spine can help ease the painful symptoms by taking the pressure off the spinal canal and help reset the spine back in alignment. Incorporating cervical traction for neck pain can help many suffering individuals become pain-free on their health and wellness journey.
References
Abi-Aad, Karl R, and Armen Derian. “Cervical Traction – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 1 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK470412/.
Bjerke, Benjamin. “Cervical Stenosis with Myelopathy.” Spine, Spine-Health, 10 July 2017, https://www.spine-health.com/conditions/spinal-stenosis/cervical-stenosis-myelopathy.
Burns, Stephen P, et al. “Cervical Stenosis in Spinal Cord Injury and Disorders.” The Journal of Spinal Cord Medicine, Taylor & Francis, July 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5102300/.
Donnally III, Chester J, et al. “Cervical Myelopathy.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 Mar. 2022, https://www.ncbi.nlm.nih.gov/books/NBK482312/.
Meyer, Frerk, et al. “Degenerative Cervical Spinal Stenosis: Current Strategies in Diagnosis and Treatment.” Deutsches Arzteblatt International, Deutscher Arzte Verlag, May 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2696878/.
Rulleau, Thomas, et al. “Effect of an Intensive Cervical Traction Protocol on Mid-Term Disability and Pain in Patients with Cervical Radiculopathy: An Exploratory, Prospective, Observational Pilot Study.” PloS One, Public Library of Science, 11 Aug. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8357129/.
The neck has two functions that allow the body to make sure that it holds the head up. The motor functions enable the neck to be mobile with the head as it can turn, twist and rotate without any discomfort or pain affecting it. For the sensory functions, the neck can feel when it has been stretched or adjusted or feel pain when it is injured. These two functions ensure that the neck is working correctly, but when injuries or unwanted events occur and affect the neck, it can cause unwanted problems. Neck injuries have a wide range of painful symptoms that can affect the spine’s head, neck, and cervical region. Today’s article will focus on myelopathy neck pain, its causes and symptoms, and how decompression therapy can help alleviate myelopathy neck pain for many individuals. Referring patients to qualified and skilled providers who specialize in spinal decompression therapy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Myelopathy Pain?
Have you been experiencing upper back or neck pain? Do you feel a tingling sensation running from your neck down to your hands? Or have you experienced difficulty in simple tasks like writing or putting on clothes? Experiencing these symptoms might show that you are suffering from myelopathy pain in the neck and cervical area of the spine. Research studies have defined myelopathy pain as when the neck suffers from a traumatic injury that causes severe compression on the spinal cord in the cervical area. The spinal cord in the spine has nerve roots that are branched out in the cervical region and allow the signals to be transported from the brain to the rest of the body. When traumatic injuries cause an impact on the spine, the blunt force will compress the spinal cord causing unwanted symptoms that affects either the cervical or lumbar portions of the spine. When the spinal cord becomes compressed, it can cause issues to the cervical part of the spine’s sensory and motor neck functions.
The Symptoms & Causes
When a person is suffering from myelopathy pain in the cervical regions of their spine, research studies have shown that the symptoms that myelopathy pain causes are motor dysfunction, where a person is having difficulty doing ordinary activities like getting ready for the day. Other symptoms that cervical myelopathy can cause to the neck are sensory dysfunctions, where the arms and hands feel numb to the touch. This tingling sensation gives off a pins and needles feeling to the body, and it can become uncomfortable for many individuals experiencing this sensation. This could be due to the cervical nerves and the spinal cord nerves being in pain. Additional research has mentioned that cervical myelopathy is caused when osteoarthritic changes in the spinal column that causes the spinal canal to be reduced. Myelopathy cervical pain can also be caused by cervical herniation in the neck, where the spinal discs aggravate the nerve roots. Other causes for the development of myelopathy are:
Feeling a tingling sensation running down from your shoulders to your hands? How about muscle stiffness from your neck turning it side to side? Is it difficult to do simple tasks like brushing your hair or buttoning up a shirt? Perhaps you are experiencing cervical myelopathy in the neck that is causing these symptoms, and decompression/traction treatments could be the relief you need. The video above shows how to assemble the Chatanooga decompression machine for cervical decompression/traction treatments. This treatment allows the individual to lay their head on the traction table and be secured. The device enables moderate pulling to release the pinched nerves from causing more pain to the neck and upper half of the body. Cervical decompression/traction can also help with neck and spinal issues like cervical herniation, radicular pain, and muscle stiffness. Cervical decompression/traction therapy has many beneficial factors in a person’s wellness treatment. This link will explainhow cervical decompression offers impressive relief for many people who suffer from neck pain and cervical myelopathy.
How Decompression Therapy Helps Alleviate Myelopathy Neck Pain
With myelopathy, neck pain causing not only neck pain but also upper body pain that hinders a person’s ability to do simple tasks. Research studies have shown that decompression surgery can help alleviate myelopathy neck pain by restoring the neurological motor function back in the spinal cord and providing relief to the cervical nerve roots. Other research studies have found that decompression treatments for myelopathy neck pain can help improve neck functionality, reduce neck disability, and even help restore a person’s quality of life by bringing back their motor function for the upper extremities that are associated with the neck.
Conclusion
Overall, having myelopathy neck pain can cause a person to lose their motor and sensory functions in their upper body. The factors like herniation, spinal spondylolysis, and spinal injuries are some of the causes of the development of myelopathy. It can make a person deal with constant neck pain without finding relief. Decompression treatments help many suffering individuals dealing with myelopathy neck pain by relieving the tension from the cervical nerve root that is causing the pain signals in the cervical area. By reducing the inflamed cervical nerve, people can feel the relief they desire when incorporating decompression treatments into their wellness journey.
References
Cheung, W Y, et al. “Neurological Recovery after Surgical Decompression in Patients with Cervical Spondylotic Myelopathy – a Prospective Study.” International Orthopaedics, Springer-Verlag, Apr. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2269013/.
Donnally, Chester J, et al. “Cervical Myelopathy.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 Mar. 2022, https://www.ncbi.nlm.nih.gov/books/NBK482312/.
Fehlings;Wilson JR;Kopjar B;Yoon ST;Arnold PM;Massicotte EM;Vaccaro AR;Brodke DS;Shaffrey CI;Smith JS;Woodard EJ;Banco RJ;Chapman JR;Janssen ME;Bono CM;Sasso RC;Dekutoski MB;Gokaslan ZL;, Michael G. “Efficacy and Safety of Surgical Decompression in Patients with Cervical Spondylotic Myelopathy: Results of the Aospine North America Prospective Multi-Center Study.” The Journal of Bone and Joint Surgery. American Volume, U.S. National Library of Medicine, 18 Sept. 2013, https://pubmed.ncbi.nlm.nih.gov/24048552/.
Medical Professionals, Cleveland Clinic. “Myelopathy: Symptoms, Causes and Treatments.” Cleveland Clinic, 2 Oct. 2021, https://my.clevelandclinic.org/health/diseases/21966-myelopathy.
Milligan, James, et al. “Degenerative Cervical Myelopathy: Diagnosis and Management in Primary Care.” Canadian Family Physician Medecin De Famille Canadien, College of Family Physicians of Canada, Sept. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6741789/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine