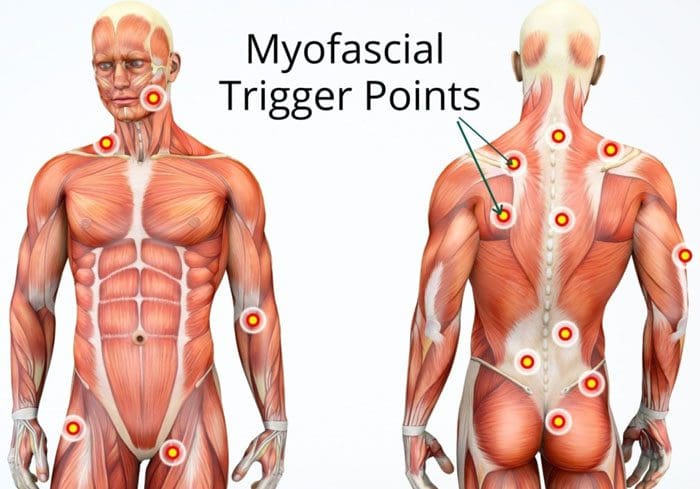
Muscle knots are common and can occur anywhere on the body. They can cause aching and pain in the muscles and joints. When examining a muscle knot also known as myofascial trigger points, it can feel swollen, tense, or like a bump. A particular area where these knots present is in the low back. This happens from excessive wear-and-tear on the lower spine from work, school, daily tasks, and chores. This causes the muscle fibers to tear, and with restricted or no time to rest the area and let it heal properly leads to the fibers bunching/clumping together forming a painful knot.
Muscle Knots In The Lower Back
A muscle knot in the lower back causes aching, soreness, and full-on pain. They tighten and contract even when the muscle is resting. The affected area often becomes inflamed or swollen causing pain and aches to radiate/spread to the gluteal muscles, as well.
Development
These knots develop when the tissue fibers pull apart and bunch up together. They start to stick together and with time the area becomes thicker. This results in the muscle knot. They can be caused by:
Stress
Tension
Poor posture
Muscle overuse
Muscle strain
Sedentary habits
Body dehydration and an unhealthy diet can also contribute to muscle knots. They look like a small bump under the skin. The bump can be red and is usually tender/sore when touched. However, not all muscle knots are visible, but when touched there is soreness and/or pain.
Do They Go Away?
They can go away on their own, but this comes from proper rest and recovery time. However, muscle knots should not be ignored, as even the smallest knot can compress surrounding nerves and muscle tissues. This can cause irritation and weakness. Larger muscle knots could cause movement/mobility issues.
Therapies
Stretching
Stretching will help stretch out and release tight muscle knots. Stretching loosens the muscle fibers and prevents them from becoming attached. Stretches to release a muscle knot include:
Start with these simple stretches/exercises and slowly work up to more vigorous ones.
Chiropractic Care
Chiropractic care can break down muscle knots through various adjustments. They are experts on the musculoskeletal system and understand where the problem is occurring along with the connected muscles.
A chiropractor will palpate the spot where the most pain presents and the surrounding area.
They will begin with a soft massage. This warms up the area getting the blood circulating. The blood circulation helps prevent pain making the adjustment/s far more effective.
Then pressing on nearby joints that the muscle knot is connected to breaks up the tight fibers.
Then the section/area is stretched out. This extends the fibers and prevents them from winding back into a knot.
They will recommend stretches and exercises
Therapeutic Massage
A massage helps to release tension and encourages muscle knots to loosen up and break down. A massage therapist will perform a deep tissue massage or a Swedish massage. Massage helps to release endorphins, which are the body’s natural painkiller. These calm the body and reduce pain. They will also recommend simple massages at home. These can include:
Rolling a massage ball/roller on the muscle knot
Self-massage using the fingers in circular motions on the affected area
Heat and Ice
Hot and cold therapy can calm and prevent inflammation. Heating pads are best if the area has stiffness or is painful. The heat relaxes tight muscles and increases blood flow. Cold therapy stops the swelling. If the muscle knot gets bigger or begins turning red, icing the area is recommended. Alternating between the two can eliminate symptoms and assist with quicker healing.
Body Composition
Building Functional Strength
There are exercises to improve functional strength. Functional training targets specific areas:
Then lift the outside leg up as high as possible and hold for 10 seconds
Repeat on the other side
Do 6-10 repetitions on each side
This exercise builds shoulder, arm, and hip strength. It engages the core and abdominal muscles and improves flexibility in the shoulders, back, and hips.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Cramer, Holger et al. “Postural awareness and its relation to pain: validation of an innovative instrument measuring awareness of body posture in patients with chronic pain.” BMC musculoskeletal disorders vol. 19,1 109. 6 Apr. 2018, doi:10.1186/s12891-018-2031-9
Malanga, Gerard A et al. “Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury.” Postgraduate medicine vol. 127,1 (2015): 57-65. doi:10.1080/00325481.2015.992719
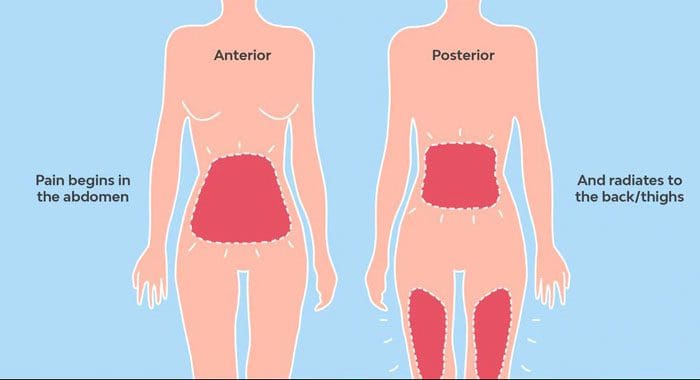
Women are familiar with abdominal cramps, Pre Menstrual Syndrome, and headaches that accompany their menstrual cycle. However not as many are aware of backache to throbbing back pain sometimes before and/or after a monthly cycle. Many women go to over-the-counter pain medication like ibuprofen. In a study, the regular use of NSAIDs found that it can lead to:
Stomach problems
Bleeding ulcers
Fluid retention
High blood pressure
Kidney
Heart problems
Why Back Pain Presents During Menstrual Cycle
When the uterus is in a contracting state, the nerves around the pelvis feel the sensations. The uterus only contracts for a few seconds, but repeatedly for hours. Sometimes, the uterus compresses blood vessels in the region. This can limit or completely block the blood vessels supplying the muscles around the pelvis. This is a major contributor to back pain during a period. This is known as referred pain, which means the body feels the pain in one area, in this case, the lower back. But the pain is caused by another area of the body, the uterus. This can cause cramping and low back pain before, during, and after a period. If cramps and back pain become debilitating or worsen over time, it could indicate:
If fever is present along with back pain seek professional help as soon as possible.
Here are a few ways that can help bring relief from back pain during the monthly cycle.
Heat Therapy
Heat generates increased blood circulation, specifically where it is applied. Therefore any blood vessels that are blocked by the uterus will have improved circulation to the muscles surrounding the uterus, allowing them to relax. This could be the use of:
Heating pads
Hot water bottle
Warm bath or shower
If at work, many pharmacy stores and regular stores sell heat patches that are applied with adhesive tape. These can be used on the lower abdomen or lower back, providing soothing heat.
Light Exercises
Most doctors refer to exercise throughout the month, just not during the period. As staying in shape will maintain the body’s proper circulation and keep the muscles strong. However, some women can perform light exercises like yoga or swimming. This helps decrease back pain even on the first or second day of a menstrual cycle which for many women is the heaviest and most painful.
Meditate
Meditation can help gain control and insight from feelings about life situations. It takes practice, but once an individual gets the hang of it they are amazed at how much pain can be reduced with a 15-minute meditation session.
Supplemental Support
Taking omega 3’s and magnesium supplements can help with the pain. Omega 3s reduce blood clotting and improve circulation. They are natural anti-inflammatories that decrease prostaglandin, which is associated with backaches and cramps. Magnesium supplements, especially those that contain vitamin B6, can help relieve back pain before and after a period. Magnesium can also be found in:
Beans
Beets
Salmon
Shrimp
Chiropractic Care
The uterus, like every organ in the body, sends and receives nerve signals, from the brain to the uterus. The menstrual cycle has a close relationship with the spine because of its location. Regular chiropractic adjustments can maintain proper communication between the brain and uterus. Chiropractic realigns the entire spine back to its proper position. This relieves the pressure on the nerves of the reproductive organs. Seeing a chiropractor is the right step towards stopping the pain and healing the body naturally.
Positive body composition changes can be seen with higher load volume and less explosive tempo that is combined with shorter rest periods when weight or strength training.
When lifting weights or resistance training, it could be difficult to gain muscle mass if on birth control, near the perimenopausal stage, or officially on menopause.
One of the benefits of weight and strength training is that it can help an individual feel better about themselves. Weight training is associated with significant improvements in:
Body image
Quality of life
Physical activity behaviors
Overall satisfaction
Well being
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Brynhildsen, J O et al. “Does the menstrual cycle and use of oral contraceptives influence the risk of low back pain? A prospective study among female soccer players.” Scandinavian journal of medicine & science in sports vol. 7,6 (1997): 348-53. doi:10.1111/j.1600-0838.1997.tb00165.x
Forozeshfard, Mohammad et al. “Short term effects of Kinesio taping on pain and functional disability in young females with menstrual low back pain: A randomized control trial study.” Journal of back and musculoskeletal rehabilitation vol. 29,4 (2016): 709-715. doi:10.3233/BMR-160673
Seguin, Rebecca A et al. “Strength Training Improves Body Image and Physical Activity Behaviors Among Midlife and Older Rural Women.” Journal of extension vol. 51,4 (2013): 4FEA2.
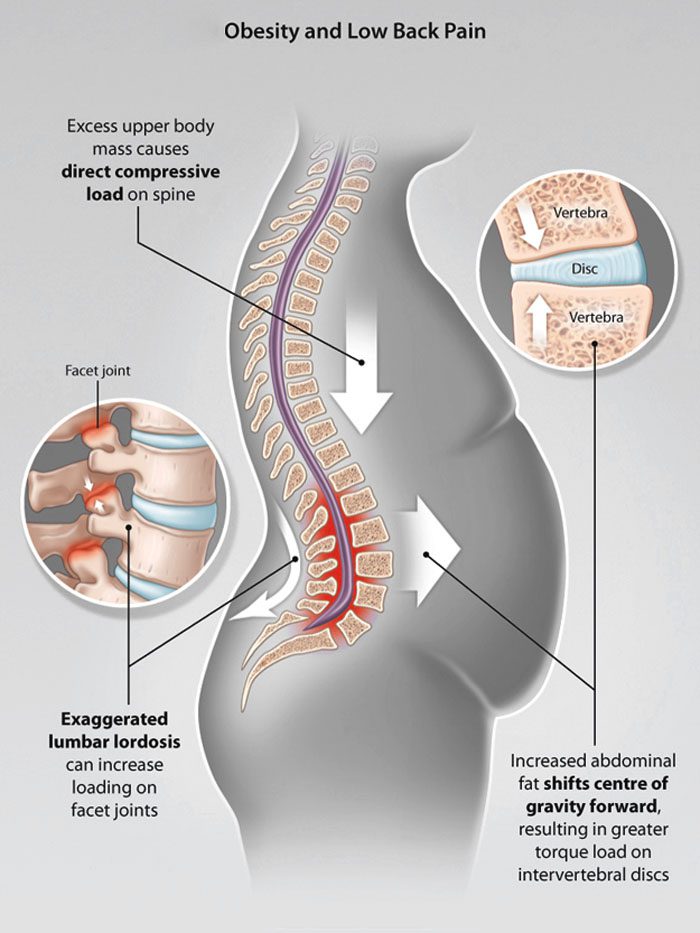
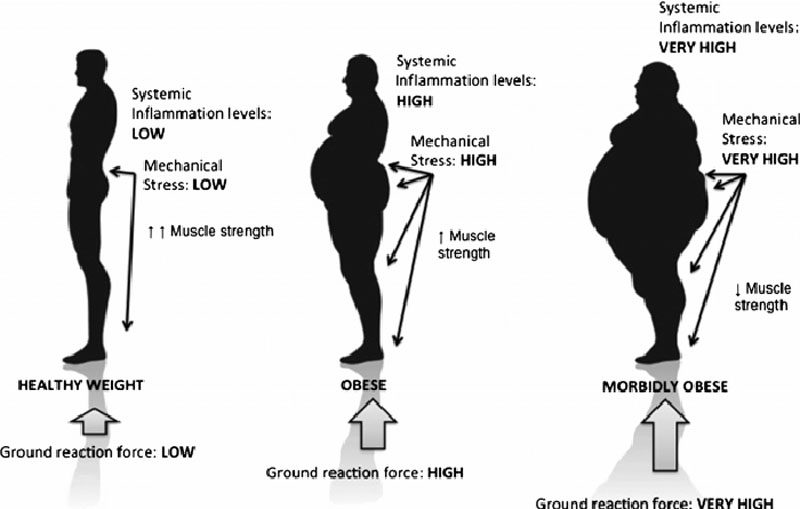
Belly fat is a gateway to back pain/spinal issues that can lead to various health problems. The bulging belly population has grown a bit since the beginning of the COVID-19 pandemic. 37% of individuals have gained weight since it began, according to a global Ipsos survey. If back pain is presenting and there is excess weight around the abdomen known as abdominal obesity, this could be a contributing factor.
Belly fat and posture
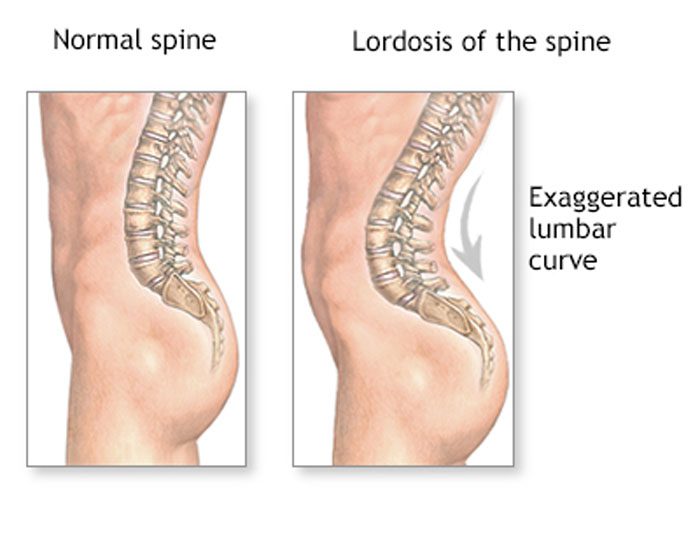
When the natural curves of the spine are normal, the core is stable and well-supported. Excessive weight, including a large abdomen, shifts these curves out of correct alignment. Excessive abdominal fat has been associated with lordosis, which is an excessive inward curve of the spine toward the lower back. One study found that severely obese individuals had pain and changes in posture. This was especially visible in the spine, knees, and feet.
Front-loading shift
The back pain felt from a bulging belly can be caused by a shift in posture and body mechanics. Studies show these can have a negative impact on back pain and body positioning. All or most of the weight is placed on the lower back.
Overloaded discs
Abdominal obesity can damage/injure the discs/shock absorbers of the spine. This leads to:
And a bulging belly can flatten the height of the intervertebral discs.
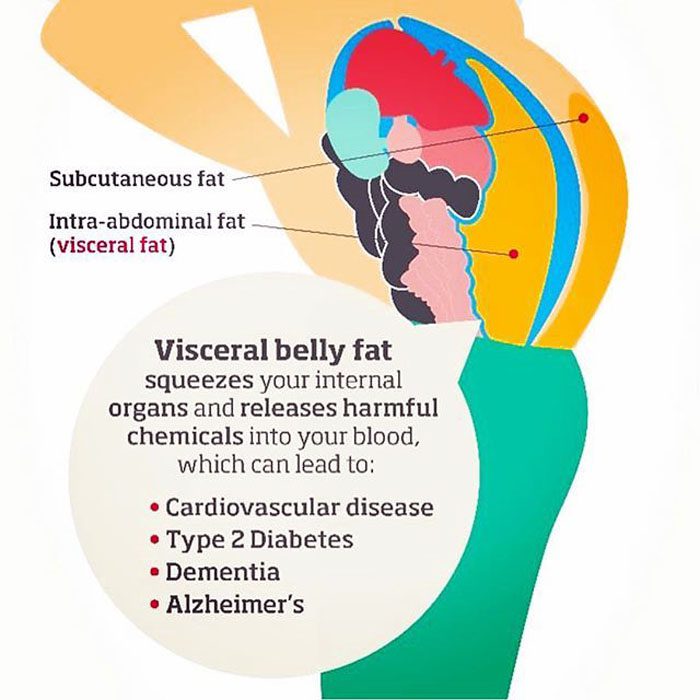
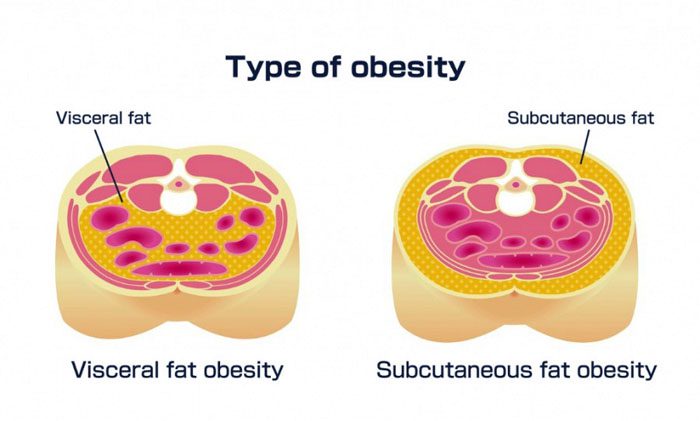
Fat pollutants in the blood
Fat can accumulate and secrete toxins that contribute to swelling and inflammation that can be painful. Over time, these toxins wear down components of the skeletal system.A study found potential links between obesity and degenerative disc disease. Scientists found a connection in obese men, but not obese women. This is believed to be because men tend to store fat in their bellies, and women tend to store fat in the buttocks and thighs.
Damage to the musculoskeletal system
The bones constantly renew themselves, but when there is excess body fat it can interfere with the process. This has the potential to turn into osteoporosis over time. Studies associate visceral fat with lower bone mineral density, and an increase in the risk of fractures.
Ankylosing spondylitis treatment and fat interference
Ankylosing spondylitis is an inflammatory disease that causes chronic back pain and can cause the vertebrae to fuse. The back can be extremely stiff, and the condition can lead to a permanently hunched posture. There are medications to improve symptoms and slow the disease. However, being overweight reduces the drugs’ effectiveness. This is because belly fat can cause medication absorption problems.
Rare spinal condition linked to obesity
Obesity along with a high Body Mass Index increases the risk of a rare condition called spinal epidural lipomatosis or SEL. This is an overgrowth of body fat in the spinal canal. Spinal epidural lipomatosis can cause various types of back pain. This is why it is recommended to have a doctor examine and evaluate any aches or pains.
Body Composition
Kombucha beneficial for gut bacteria
Kombucha contains a wide variety of bacteria and fungi that helps ferment the sugar in kombucha drinks. It is able to affect the existing microbes in the gut by inhibiting the growth of various gut-dwelling pathogens. These include:
It is a probiotic drink made from fermenting green or black tea
It is made up of healthy bacteria that produce acetic acid that is beneficial for blood sugar, insulin levels, and body composition
It helps the body process food by lowering insulin levels after a meal
It contains polyphenols that reduce oxidative stress, to help fight disease risks
It destroys unhealthy bacteria in the gut
It helps increase healthy bacteria
Kombucha can be thought of as a natural antibiotic. However, it does not come with the weight-gain side effect. Improving the health of the gut through fermented foods like kombucha help reduce the risk for weight gain/obesity, as well as restore gut health for those trying to lose weight by creating a healthy gut environment.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
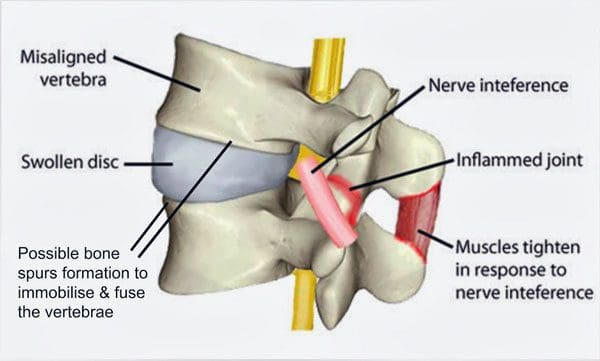
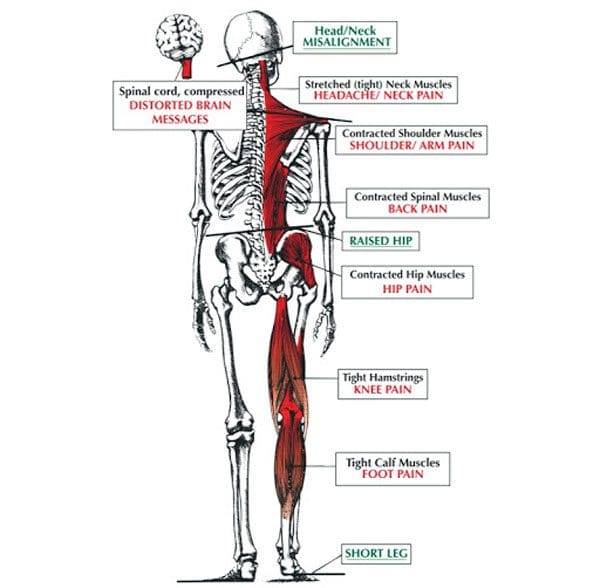
When spinal misalignments happen the body experiences soreness, inability to rotate the neck, or after sitting/standing in one position for too long hip and leg discomfort/pain. This is why spinal alignment is so crucial to healthy living. These examples help to illustrate the delicate balance required in the spine to maintain optimal health, stay pain-free, prevent injury, and the ability to conduct everyday chores/responsibilities without the fear and anxiety of setting off pain symptoms.
Understanding how pain is processed
Pain is a complex sensation. Neural pain receptors, also known as nociceptors detect harmful stimulation/s in the form of:
Body Temperature changes
Mechanical forces and pressure on the body
Chemical changes in the body brought on by inflammation or cell damage
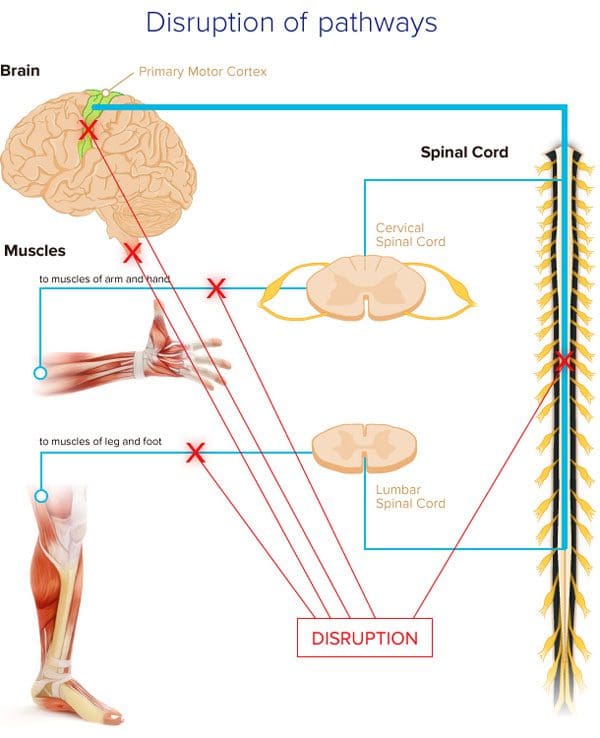
How the signal transmits from the stimulated nerve and how it is perceived depends on the upper levels of neural activity in the body. Specifically, the spinal cord, brainstem, and the brain. Examples of pain perceptions:
Previous pain generating experiences – auto accident, work injury, etc.
Spinal Misalignments and Balance
Pain is essential for alerting the body when engaged in activities, and body positions that can cause damage to the tissues like poor postures, work/sports/personal injuries, inflammatory foods, etc. The nerves’ pain pathways can experience overstimulation when the system is overloaded.
Excessive stimulation can be brought on by chronic inflammation, mood disorders, and poor health. One overlooked issue with the perception of pain is the health/effectiveness of the actual neural pathways. The nerve’s energy is affected by spinal misalignments. Proper nerve health and circulation are crucial for the body to transmit proper pain signals. Spinal misalignments can be brought on by:
Can lead to major dysfunction of the nerves pathways
The longer the pain and discomfort go on the more intense/severe the issues can become. This is when pain and discomfort become chronic leaving individuals feeling hopeless, frustrated.
Symptoms
The spine does more than provide stability. Any type of spinal misalignments will affect the rest of the body as well. Possible symptoms that the spine is out of alignment includes:
Chronic headaches
Frequent illnesses
Fatigue
Lower back pain
Neck pain
Hip pain
Knee pain
Numbness/tingling in the hands or feet
Walking gait abnormalities causing one shoe to wear out quicker than the other
Chiropractic Management
Many treatments focus on masking the pain rather than addressing the underlying root cause. This can lead to a chronic pain cycle and dependence on pain medications and invasive treatment. Chiropractic is a science-based approach that focuses on getting to the root issue. Chiropractic utilizes gentle and effective techniques like:
Manipulation
Exercise regimen
Stretching regimen
Body mechanics training
Health nutritional education
When the body is aligned and the spinal nerves are healthy, an individual’s pain perception will be changed for optimal functionality.
The first step is to reduce caloric intake by changing/adjusting dietary nutritional habits. Individuals can experiment with various types of diets and regular exercise regimens, and getting into the habit of getting the proper amount of sleep. Depending on an individual’s existing muscle mass, gaining Lean Body Mass first could be an option. An individual may be able to lose fat and gain muscle because:
Increased muscle mass will increase the Basal Metabolic Rate/metabolism, and if no extra calories are added body fat can be shed while building muscle.
Lifting weights can increase Total Daily Energy Expenditure, causing the body to burn more calories.
Circuit training is one option for improving changes in body composition while not affecting changes in overall body weight. This means muscle gain and fat loss is happening at the same time.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Dubinsky RM, Miyasaki J.Assessment: Efficacy of transcutaneous electric nerve stimulation in the treatment of pain in neurologic disorders (an evidence-based review). Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology.�Neurology. 2010;74:173-176.
Shrier I. Does stretching help prevent injuries?�Evidence-based Sports Medicine. Williston, VT: BMJ Books; 2002.
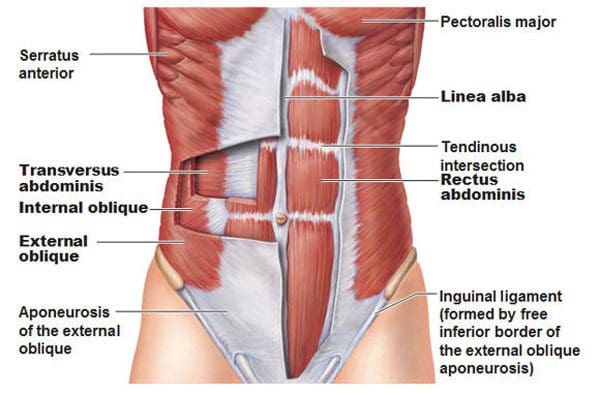
The core and the muscles involved are a group of muscles that wrap around the body’s torso. The front, back, and sides. Strengthening these muscles will improve and ultimately alleviate lower back pain. One of the main muscles that are overlooked is the transverse abdominis muscle. It is vital to a healthy core, especially if back pain is presenting. It’s known as the seatbelt muscle as it is deep in the abdomen and wraps around the waist. It has everything to do with long-term core strength and function. A properly developed transverse abdominus functions like a lumbar support belt that protects the spine. When the transverse abdominus is strong the muscle contracts to generate the correct amount of support and stability when in motion. �
�
For example, individuals that do not have low back pain engage the transverse abdominus around 30 milliseconds before moving the shoulder, while individuals that have low back pain have a delayed contraction of the transverse abdominus muscles that makes them take on awkward postures, and move in an awkward fashion contributing to back pain and continuing to weaken the core muscles. Individuals that regularly do transverse abdominus strengthening exercises greatly reduce the risk of experiencing low back pain for the first time and reduce the recurrence of those already with back pain. �
Core Muscle Anatomy
The first step to strengthening is understanding the moves and how to do them correctly with basic anatomy. Think of the core as a muscle box where the:
The body flexes and extends whenever bending forward and standing up
The body does a lateral side bend when bending the trunk to one side
The body rotates the trunk when twisting the torso
�
Muscle Weakness
The transverse abdominus tends to suffer from neglect which is one reason why it becomes weakened. This increases the risk of developing back pain. Another reason is that individuals have a weak muscle is they exercise in one-plane of movement. Not working out the core muscles in all planes of motion can contribute to back pain. For example, if an individual performs pelvic tilts, they are only moving in one plane when tilting the hips forward and back, known as flexion and extension. To achieve optimal/functional strength, the core workout needs to include side bending and twisting movements. �
Strengthening The Transverse Abdominus
Pigeon Pose
Many individuals sit for extended amounts of time and are excessively tight along the sides and hips. The first step should be to increase the hip’s mobility before strengthening the core. If the hip muscle’s fibers become shortened, it can affect hip joint function and efficiency during core movement. The Pigeon Pose is a hip opener. How to do it:
Get on the floor with the knees and palms on the ground.
Slide the left leg back so the hip is extended, then externally rotate the right hip/turn the right leg out from the hip. Focus on positioning the right shin perpendicular to the body.
Extend the trunk so the body is upright, lifting the chest, arching the back, and looking toward the ceiling, while resting the fingertips on the floor a little forward of the hips.
Hold the pose for 30 seconds and switch sides.
This stretches the hip flexor muscles in the extended leg and the rotator and outer hip muscles in the flexed leg.
�
Pay Attention To The Engaged Muscles
Individuals can train the transverse muscles to activate faster and more effectively throughout the day by slowing down and paying attention to moving with more intent. Place the hands around the waist and engage the core to feel the muscles contracting. This will help get a feel for the movement. Once comfortable remember to engage these abdominal musclesbefore and while reaching, twisting, or lifting items. �
Pelvic Tilt
This exercise is vital for building the smaller muscles that support a healthy core. How to do it:
Lie on back with knees bent and feet on the floor.
Engage the transverse muscles and gently tilt the pelvis upward.
Return the pelvis to a neutral position.
Repeat.
Start with 3 sets of 10-12 reps.
When this is no longer challenging and can be completed without increasing back pain, advance to more challenging exercises like the bird dog, planks, or plank variations.
�
Standing Exercises
Translating core strength into functional strength and pain-free movement progresses to standing exercises that require rotation. One example is a standing lunge with rotation. How to do it:
Get into a lunge stance with the front leg flexed 90 degrees at the hip, knee, and ankle. The rear leg should be extended at the hip with the knee touching or almost touching the floor.
Twist from the waist. When comfortable doing this movement, hold weight like a dumbbell, medicine ball, or gallon jug of water in both hands, and gradually increase the weight as the muscles get stronger.
When in the process of strengthening the core, consistency is the key. Commit to a short workout every day instead of one massive workout once or twice a week. Ten minutes a day is enough to build strength, improve function, and decrease back pain. �
Improved Body Composition
Functional fitness and the ability to move about comfortably not only benefit physical wellness but also improves body composition. The aging process reduces the metabolic rate, which leads to increased body fat. Lean Body Mass gets lost from age and inactivity. Lean Body Mass contributes to the overall Basal Metabolic Rate, also known as the body’s metabolism. It is the number of calories the body needs to support essential functions. Engaging in strength training or resistance exercises will help regain the muscle loss from aging/inactivity, and can lead to an increase in lean body mass.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
People who regularly engaged in TVA-strengthening exercises were less likely to experience a recurrence of low back pain:�Australian Journal of Physiotherapy�(2002), �Specific spinal exercise substantially reduces the risk of low back pain recurrence��https://www.sciencedirect.com/science/article/pii/S000495141460283X?via%3Dihub
Participating in any sports or physical activities strengthens the mind and body. But working out and engaging in these types of activities too much or without rest periods wears down the body. There is the feeling of a good workout with some sore muscles and achiness that lets you know the activity is working positively.
However, soreness can quickly lead to pain and further injury if ignored. The lower back is a common area of soreness after working out playing sports, and where muscle spasms, pulls, and pinches occur. Being able to distinguish between workout soreness and pain is critical for maintaining a healthy spine.
A constant-sore back or feelings of sharp pains is not normal. If there is a feeling of low back pain during or after a physical routine, stop and take a moment to examine the tingling, discomfort, or pain being experienced. If unsure if the soreness or pain is a cause for concern call or video conference with a chiropractor to discuss what is going on.
Physical activity and pain
Individuals participating in physical/sports activities have an increased risk of low back pain because of the consistent running, twisting, and jumping. Any of these movements place pressure on the spine along with the surrounding ligaments and muscles, which can lead to injury.
Repetitive twisting and turning, stresses the muscles around the spine, which can cause frequent muscle sprains. Running and jumping also wears down the vertebrae and discs. Impact activities can also cause injuries to the spine, nerve roots, and surrounding tissues. The most common back problems include:
Muscle sprains
Osteoarthritis
Bulging discs
Herniated discs
Sciatica
Fractures are less common but still pose a risk
Individuals should watch for achiness or stiffness that lasts longer than a few days and does not alleviate with ice or anti-inflammatory over the counter medication, or sharp pain that happens with specific movement/s, along with any pain, numbness, tingling that runs down the leg/s or to other areas should consult a medical professional.
Treatment and prevention
Maintaining the body’s health is critical. If the lower back begins to present discomfort or hurts, do not ignore it. Many will play through the pain when they should be taking a break. And ignoring any back pain could create new injuries or worsen the condition. Continued pressure on the back will worsen any strains or fractures and will hinder the body from healing properly.
Individuals tend to take on awkward/uncomfortable postures and move in awkward ways to avoid or compensate for the pain. This places added pressure in the wrong places and can cause/worsen an injury or condition. Pay attention to the pain. Try ice and heat therapy at home to see if it eases up. Using a foam roller or self-massage device can help if the back pain is muscular. However, if the pain is sharp, shooting, or does not go away, visit a chiropractor for diagnosis and treatment.
A chiropractor will conduct imaging tests and physical exams to identify the root cause. Once a diagnosis has been reached a treatment plan will be implemented through:
Massage
Stretches
Therapeutic exercises
Spinal adjustments
Health coaching
Visiting a chiropractic professional will improve the condition and strengthen the spine.
Fit Body Composition
Muscle recovery
When engaging in physical activity there is microscopic damage to the muscle cells. The stress and fatigue the body goes through during physical activity cause hormone and enzyme levels to fluctuate, increasing inflammation. This leads to:
Fat loss
Increased metabolism
Increased strength
Muscle growth
However, it happens through proper recovery. There are different types of recovery: immediate, short-term, and training.
Immediate recovery is the short time between movements. For example, when jogging, immediate recovery is the time between each stride.
Short-term is the time between sets of exercises. For example, the rest periods between exercise intervals.
Training recovery is the period between one workout session ending and the next beginning.
Research has shown that rest time is not a one size fits all. Everyone is different and therefore should consult a fitness trainer, or sports chiropractor and experiment with what feels right. For some individuals, 24 hours works. For others, it can be 48 or 72 hours to feel fully recovered. It depends on age, fitness level, physical activity intensity, diet, sleep, and more.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Smith, Jo Armour et al. �Risk Factors Associated With Low Back Pain in Golfers: A Systematic Review and Meta-analysis.��Sports health�vol. 10,6 (2018): 538-546. doi:10.1177/1941738118795425
Remote working and learning have changed the way we operate, but too much sitting and no physical activity is the perfect set up for back pain. Here are a few tips for spine friendly remote working and learning. Spine-health is just as important working or learning remotely, if not more so because it is easy to fall into bad posture habits that will affect the spine. Poor home working/learning habits can cause upper and lower back pain that could become chronic.
Individuals become too comfortable making the home working environment a damaging experience on spinal health. For chiropractors, the pandemic brought an influx of individuals of all ages with upper, middle, and lower back pain. This was caused by poor posture when video conferencing on the couch, slouching at the table and sitting for way too long, and never getting up and moving around.
Children tend to present with pain and aches on the side of the spine versus pain directly centered. This is from side slouching, often when staring at the computer monitor. Adults, especially over 40 complained of pain and stiffness in the upper and lower back. Herniated discs, degenerative disc disease, and sciatica risks increase as bad habits continue and do not improve. However, this can all be helped with a little exercise, work/school space optimization, and forming healthy work and schooling from home habits.
Stretching Out
When working/schooling remotely, there�s a tendency to be more sedentary. Individuals need to learn to take time to stretch out and keep the body limber. It is easy to use breaks to scroll through social media or binge on movies, videos, etc. This can still be accomplished, but stretch out and move around while taking breaks. An exercise program of stretching daily during the workday and endurance training twice a week will help reduce back pain and increase flexion. Results vary for everyone and the type of stretching exercises they are performing.
Core Exercises
Core exercises are a perfect way to work out muscle stress and back pain resulting from poor posture. Slumped over a computer can place significant stress on the trapezius muscle causing the muscle to knot up and tighten. The trapezius muscle is crucial to neck and shoulder movement and helps stabilize the shoulder blades.
Trapezius stretch with band
Holding an elastic band between the hands, place the band at the back of the skull.
Slowly tilt the head back to its full range of motion as the resistance is felt.
Return the head back to the neutral position maintaining alignment with the spine.
Choose 2 items of equal weight such as 2 books, 2 quarts of water, or 2 hand weights, and hold one item in each hand.
Position keeping hands near your sides
Slowly raise up and shrug your shoulders for several seconds
Gently release shoulder shrug and bring back arms to neutral
Repeat for 10 reps
Posture
Proper posture is a learned process that requires practice. Using a mirror to check posture can help maintain proper posture while seated when working/schooling. Self-assessing posture correctly is important and viewing oneself in a mirror is an easy way to figure out what adjustments are needed. Questions to ask oneself while self-assessing include:
Is the head far too forward?
Is there slouching?
Are the shoulders curling/rounding around the body?
Posture tips when seated:
Keep the feet flat on the floor or on a footrest
If in the habit of crossing ankles and knees change position often
Position the back against the chair. If the spine does not align with the chair use a cushion or backrest
Position knees at hip height or a little lower
Maintain some space between the back of the knees and the chair�s edge
Look straight ahead but make sure the neck is comfortable
Position forearms parallel to the floor
Maintain relaxed shoulders
Adjust the Light
When lighting is not optimal there can be a tendency to strain forward in various positions. This can cause excessive stress and inflammation to the upper spine area. Natural ambient lighting is recommended. In general, the lighting set-up should be adjusted to easily see the screen without causing glare or any type of discomfort to the eyes.
Take a Walk
A daily routine that will support spine health is to take walk breaks every half hour for a few minutes. If every half hour is not doable then take a 5 or 10-minute break to walk around and stretch every hour. It is important not to remain seated for too long. Remember the body was meant to move and be active.
Optimization Work Station
Using ergonomic office furniture for home use can help prevent the development of unhealthy posture along with the development of further musculoskeletal issues. Laptops are great for their portability and ability to work-from-anywhere. However, actually placing them on your lap and working on them for too long will cause back and neck strain. It is difficult to position the keyboard and screen for maintaining a proper line of sight and hand position.
The most spine-healthy way to work on a laptop is to position the screen at eye level with the keyboard level with slightly extended hands. A recommended long-term solution is using a screen and keyboard that can be adjusted. One type of computer set up is an iPad positioned at eye-level with a stand and a wireless external keyboard/mouse on a table or desk.
A lot of money does not have to be spent on the setup. Books or boxes laying around the house can be used to prop up the screen to the proper height. The goal is when working/schooling remotely is to ensure the body is not hunched over, bent, or straining forward and to maintain proper posture with optimal spinal alignment.
There are unique spinal health challenges when working/learning remotely. However, they can be avoided with a little planning and small adjustments.Taking time to stretch, do a little exercise, walk around the house, have adequate lighting, and making some ergonomic desk, chair, and computer changes that will help maintain a healthy spine.
Back Pain Rehabilitation
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Moretti A, Menna F, Aulicino M, Paoletta M, Liguori S, Iolascon G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis.�Int J Environ Res Public Health. 2020;17(17):6284. Published 2020 Aug 28. doi:10.3390/ijerph17176284
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine