Many people experience pain daily at some point in their lives. The causes of pain can vary from person to person and can be due to environmental factors or normal wear and tear on the body. When the spine is under unwanted pressure, spinal discs can become compressed and musculoskeletal disorders can cause vertebrae to wear down, leading to chronic pain and disability. Fortunately, many treatments are available to alleviate pain and help the body restore itself naturally. This article focuses on a non-surgical treatment called spinal decompression, which can reduce the effects of musculoskeletal pain and help with the back and spine’s cervical, thoracic, and lumbar areas. We utilize and incorporate valuable information about our patients to certified medical providers using non-surgical therapies like spinal decompression to alleviate pain-like symptoms associated with environmental factors. We encourage referring patients to associated medical providers based on their findings while supporting that education is a remarkable tool to ask our providers essential questions at the patient’s request. Dr. Jimenez, D.C., comprises this information as an educational service. Disclaimer
What Is Spinal Decompression?
Do you feel stiffness in your upper or lower body? Are you experiencing any discomfort in your back, neck, or shoulders? Or are you feeling pain during simple movements? If these issues persist, consider spinal decompression therapy to alleviate your pain. Research studies reveal that many people experience pain at least a few times due to compression of the intervertebral discs caused by everyday wear-and-tear injuries and poor posture. This happens when the vertebral bones compress the spinal cord and discs, creating a risk of further complications. Luckily, spinal decompression is a non-surgical treatment option that is safe, gentle, and proven successful. It gently stretches the spine, relieving pressure on the spinal disc. Some of the physical benefits of spinal decompression therapy include:
Pain level decrease
Spine mobility improves
Postural integrity enhances
Develops core strength
Joint flexibility increases
Decrease stress levels
The immune system is boosted
Prevents new injuries from occurring
Chiropractic Care for Disc Herniation-Video
Do you feel pain or stiffness in certain body areas, especially when stretching or bending? These symptoms are often caused by spinal disc compression. Fortunately, many non-surgical treatments are available to help reduce the effects of spinal disc compression and promote natural healing. One such treatment is spinal decompression, as studies reveal that it uses negative pressure to stretch the muscles around the spine and reduce stress. Spinal decompression can be combined with other non-surgical treatments like chiropractic care to relieve pressure from the spine and reduce pain. Chiropractic care involves realigning the spine and reducing referred neck, shoulder, or back pain. Both therapies are non-invasive and can be combined with physical and nutritional treatment for optimal results. The video above explains how non-surgical treatments can help with disc herniation and associated symptoms.
Spinal Decompression For Musculoskeletal Pain
If you experience axial load on your spine from various factors, it could lead to musculoskeletal pain. Research shows that musculoskeletal pain is somatic by nature and can be associated with other pain syndromes related to the spine. Spinal decompression therapy can help alleviate this referred pain by using gentle traction to stretch the spine. Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C.’s book, “The Ultimate Spinal Decompression,” stated that this therapy creates space between the vertebrae, allowing herniated or bulging discs to return to their positions in the spine. This reduces pressure on nerves and soft tissues and increases the circulation of oxygenated blood, fluids, and nutrients to the spinal disc. This helps stimulate the body’s natural healing mechanism and reduce musculoskeletal pain in the cervical, thoracic, and lumbar regions. Therefore, spinal decompression therapy can alleviate pain symptoms associated with those areas.
Conclusion
If you’re experiencing musculoskeletal pain in your neck, upper back, or lower back, it could be due to unwanted pressure on your spine. A variety of environmental factors can cause this pressure. Spinal decompression is a non-surgical treatment that can help alleviate this pressure using gentle traction on the spine. Spinal decompression can create negative pressure, increasing disc height and stretching the surrounding muscles. This can help reduce pain and prevent new injuries from occurring. Combining spinal decompression with other therapies can help individuals become more mindful of their bodies and avoid adding unwanted pressure to their spine.
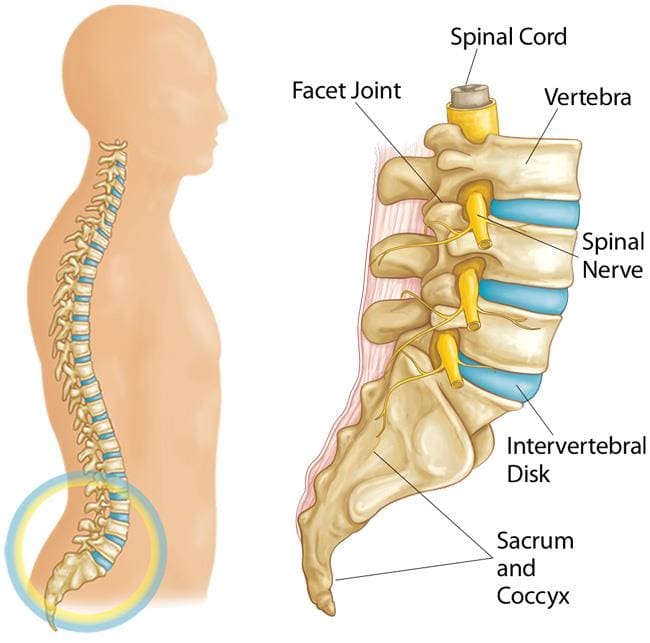
The human body has muscles surrounding and protecting the spine to prevent pain and disability. The spine is divided into three sections in the body: cervical, thoracic, and lumbar, which form an S-shape curve to promote stability and good posture. The spine has several discs, facet joints, and spinal nerves that work with the surrounding muscles, making the body mobile. However, various factors can pressure the spine, compressing the spinal discs and invoking referred pain to the surrounding muscles and tissues in different locations, leading to overlapping risk profiles if left untreated. This article focuses on the lumbar spine, explaining what vertebral pain syndrome is and how non-surgical treatments such as spinal decompression can restore mobility to the lumbar spine. We utilize and incorporate valuable information about our patients to certified medical providers using non-surgical therapies like spinal decompression to alleviate vertebral pain syndrome associated with the lumbar spine. We encourage while referring patients to associated medical providers based on their findings while supporting that education is a remarkable tool to ask our providers the essential questions at the patient’s request. Dr. Jimenez, D.C., comprises this information as an educational service. Disclaimer
An Overview Of the Lumbar Spine
We will concentrate on the lumbar spine, one of the three spine sections. The lumbar spine or low back begins at the T12 (the last thoracic vertebra) and ends at the S1 (the sacrum). It comprises five vertebrae with a common structure supporting the low back. These vertebrae are as follows:
The body
Pedicles
Laminae
Transverse processes
Spinous process
Superior/inferior articular processes
The lumbar spine has bigger and stronger bones that provide stability to the upper and lower parts of the body. Research studies reveal that the lumbar spine performs three essential functions that enable the body to function properly:
It supports the upper body.
It absorbs axial forces that move from the head to the trunk. This allows the muscles in the trunk to move without causing pain.
The lumbar spine forms a canal that safeguards the spinal cord and nerves.
The Structures Of the Lumbar Spine
The spine comprises several structures, including the vertebrae, spinal cord, spinal nerves, facet joints, and intervertebral discs. Each structure plays a unique role in keeping our bodies functioning properly. The vertebrae protect the spinal cord and nerves from injury, while the facet joints guide the motion of the vertebrae and help maintain stability. The spinal cord and nerves work with the central nervous system to send signals from the brain to the body for coordinating reflex actions. Intervertebral discs act as shock absorbers, allowing the spine to be flexible. Muscles, tissues, and ligaments protect the entire lumbar spine structure from pain. However, traumatic injuries or unwanted pressures can cause misalignment and low back pain. Low back pain is a common musculoskeletal complaint, and several factors can contribute to its development, often confused with vertebral pain syndrome associated with the lumbar spine, as research studies reveal.
Move Better, Live Better- Video
Do you have stiffness in your lower back or experience constant aches in certain regions? These may be signs of low back pain related to vertebral pain syndrome. Research shows that pathologic degeneration in the lumbar spine can cause low back pain, affecting all components. Several mechanical, traumatic, nutritional, and genetic factors contribute to spinal degeneration. However, non-surgical treatments can help reduce muscle pain and alleviate unwanted pressure on spinal discs. Chiropractic care and spinal decompression are two treatments that enhance mobility and function in the spine, relieving pain. The video above talks more about these treatments.
What Is Vertebral Pain Syndrome?
Experiencing pressure on the lumbar spine can result in various issues that can worsen low back pain. One of these issues is called vertebral pain syndrome. In “The Ultimate Spinal Decompression,” Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., explain that this syndrome occurs when environmental factors start affecting the lumbar spine. It can be caused by visceral pain in the lower back that disrupts neuron signals in the lumbar spine. This can irritate spinal nerves, leading to referred pain in the lower body. The book also mentions that vertebral pain syndrome can happen when the vertebrae end plates on spinal discs wear thin, causing pressure to move with the disc. This can inflame the spine, causing chronic low back pain.
How Spinal Decompression Alleviate Vertebral Pain Syndrome
How can non-surgical spinal decompression treatments help alleviate vertebral pain syndrome in the lumbar spine? Research studies revealed that spinal decompression could reduce pressure on the spinal disc and gently stretch the spine, restoring disc height. This treatment can relieve many people from low back pain and its associated symptoms. Moreover, it can rehydrate spinal discs by promoting the flow of blood and nutrients, which aids in the healing process to reduce the effects of vertebral pain syndrome.
Conclusion
Taking care of your spine is crucial as everyday factors can put pressure on it, causing damage to the spinal discs. This can lead to vertebral pain syndrome, which can cause lumbar back pain and referred pain linked to visceral problems. Luckily, spinal decompression therapy can ease the effects of this syndrome by gently stretching the spine and restoring hydration to the discs. Incorporating spinal decompression into your routine allows you to enjoy a pain-free life without worrying about lower back pain.
Kang, J.-I., Jeong, D.-K., & Choi, H. (2016). Effect of spinal decompression on the lumbar muscle activity and disk height in patients with herniated intervertebral disk. Journal of Physical Therapy Science, 28(11), 3125–3130. https://doi.org/10.1589/jpts.28.3125
Kaplan, E. & Bard, P. (2023). The Ultimate Spinal Decompression. JETLAUNCH.
The spine is essential for maintaining our upright posture and allowing us to move without pain. The cervical, thoracic, and lumbar sections support different body areas. However, environmental factors and pathogens can cause musculoskeletal pain, leading to spine misalignment and stress on the surrounding muscles and nerve roots. Non-surgical treatments like IDD therapy can help realign the spine and relieve pain. We utilize and incorporate valuable information about our patients to certified medical providers using non-surgical treatments like IDD therapy to alleviate pain associated with musculoskeletal pain along the spine. We encourage and refer patients to associated medical providers based on their findings while supporting that education is a remarkable and fantastic way to ask our providers the essential questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., comprises this information as an educational service. Disclaimer
The Pathological Effects Of Musculoskeletal Pain On The Spine
Are you experiencing muscle pain in various parts of your body? Do you feel stiffness in your back, neck, hips, or shoulders? Or are you experiencing localized pain in a specific area? These are common symptoms of musculoskeletal pain, which affects the spine. Unfortunately, research studies reveal that musculoskeletal pain is a leading cause of long-term suffering, disability, and decreased productivity. This type of pain can strain the surrounding muscles in the upper and lower body, affect joints, and cause overlapping risk factors that make diagnosis challenging. Research studies also suggest that musculoskeletal pain can arise from different structures, leading to local or central sensitization and correlating pain intensity and duration.
Did you know that musculoskeletal pain can have pathological effects on the spine? Research studies revealed that the musculoskeletal system significantly impacts the central nervous system regarding pain. This means that when pain occurs in a certain area, neuron signals are sent to the brain, increasing sensitivity markers to that location. In the case of a traumatic spinal cord injury, these signals can become chaotic, leading to additional risk factors for the muscles surrounding the spine. This can result in musculoskeletal pain, which may cause referred pain in other body parts. Additionally, research has indicated that severe pathologies associated with the central nervous system can also lead to musculoskeletal pain. This is because the brain’s neuron signals alert the immune system that something is wrong and needs immediate attention.
The Science Of Motion-Video
Have you been experiencing stiffness or pain in different parts of your body? Do you feel discomfort lifting heavy objects or feel a pinched nerve in your lower back or legs? These daily issues could be caused by musculoskeletal pain affecting your spinal cord. Traumatic or non-specific issues can lead to overlapping risk profiles and the development of musculoskeletal pain associated with the spine. If the spinal column is affected, it can cause neuron signals to become hypersensitive, resulting in a misalignment of the body. Fortunately, non-surgical treatments can help realign and heal the body naturally, reducing the effects on affected muscles while allowing necessary nutrients and blood to flow back to the spine. The video above explains how non-surgical treatments like chiropractic care can harness the body’s ability to heal and restore stability through manual manipulation. Chiropractic care can also be combined with decompression therapy to stretch and alleviate pressure off the spine gently.
What Is IDD Therapy?
The musculoskeletal system depends on nerves, bones, and muscles for body structure and function. When affected by unwanted pathogens, it can cause pain in various areas and make a person feel miserable. Fortunately, non-surgical treatments like IDD therapy or intervertebral differential dynamic therapy can help reduce musculoskeletal pain affecting the spine. IDD therapy is decompression therapy that can help reduce pain by mobilizing and lengthening compressed spinal discs with special treatment forces. In “The Ultimate Spinal Decompression,” Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., states IDD therapy effectively alleviates spinal pain associated with the musculoskeletal system. The book also mentions that this therapy helps free the spinal discs and nerve roots as the compressed pressure is dropped. To that point, it allows the oxygen-riched blood and nutrients back to the spinal discs to begin the healing process, as research studies revealed.
Conclusion
When the spine experiences traumatic forces or injuries, it can result in musculoskeletal pain that can be constant and miserable for the individual. However, no one should have to endure such pain. The spine supports the upper and lower sections of the body and needs to be mobile to perform this task. Non-surgical treatments, such as IDD therapy, can help alleviate unwanted pressure off the spinal discs and nerve roots that have become hyper-sensitive due to trauma or injury. This decompression therapy can help restore mobility to the spine and rehydrate the spinal discs to begin the healing process. With IDD therapy, individuals can relieve pain and experience freedom of movement.
References
Arendt-Nielsen, L., Fernández-de-Las-Peñas, C., & Graven-Nielsen, T. (2011). Basic aspects of musculoskeletal pain: from acute to chronic pain. The Journal of manual & manipulative therapy, 19(4), 186–193. https://doi.org/10.1179/106698111X13129729551903
Bang, A. A., Bhojraj, S. Y., & Bang, A. T. (2021). Back pain and musculoskeletal pain as public health problems: Rural communities await solution. Journal of global health, 11, 01007. https://doi.org/10.7189/jogh.11.01007
George, S. Z., & Bishop, M. D. (2018). Chronic Musculoskeletal Pain is a Nervous System Disorder… Now What?. Physical therapy, 98(4), 209–213. https://doi.org/10.1093/ptj/pzy002
Kaplan, E. & Bard, P. (2023). The Ultimate Spinal Decompression. JETLAUNCH.
Puntillo, F., Giglio, M., Paladini, A., Perchiazzi, G., Viswanath, O., Urits, I., Sabbà, C., Varrassi, G., & Brienza, N. (2021). Pathophysiology of musculoskeletal pain: a narrative review. Therapeutic advances in musculoskeletal disease, 13, 1759720X21995067. https://doi.org/10.1177/1759720X21995067
Schimmel, J. J., de Kleuver, M., Horsting, P. P., Spruit, M., Jacobs, W. C., & van Limbeek, J. (2009). No effect of traction in patients with low back pain: a single centre, single blind, randomized controlled trial of Intervertebral Differential Dynamics Therapy. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 18(12), 1843–1850. https://doi.org/10.1007/s00586-009-1044-3
One of the most prevalent types of pain worldwide is lumbar back pain, which affects many people and can be costly. This type of pain can be triggered by several environmental factors, which can overlap and cause referred pain throughout the body. Some factors linked to low back pain include those that impact people working for a living.
Age
Physical inactivity
Excess weight
Improper lifting
Excessive sitting
Stress
Wear and tear on the spinal discs
When environmental factors cause spine misalignment, the surrounding muscles become weak, tense, and strained. This can result in the body shifting its weight to alleviate pain. However, many non-surgical treatments are available to relieve low back pain and realign the spine. In this article, we will discuss how lumbar back pain affects the body and how non-surgical therapies such as vertebral axial decompression can help to reduce it. We utilize and incorporate valuable information about our patients to certified medical providers using non-surgical treatments like vertebral axial decompression to relieve pain associated with the lumbar spine. We encourage and refer patients to associated medical providers based on their findings while supporting that education is a remarkable and fantastic way to ask our providers the essential questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., comprises this information as an educational service. Disclaimer
What Is Lumbar Back Pain?
Research studies suggest that lumbar back pain is commonly experienced as a symptom in the midline or sacral region of the body. This pain can develop gradually due to unwanted pressure and weight on the spinal discs, which compresses the nerve roots surrounding the spinal cord. Based on additional studies, lumbar back pain is often categorized into two types for diagnosis.
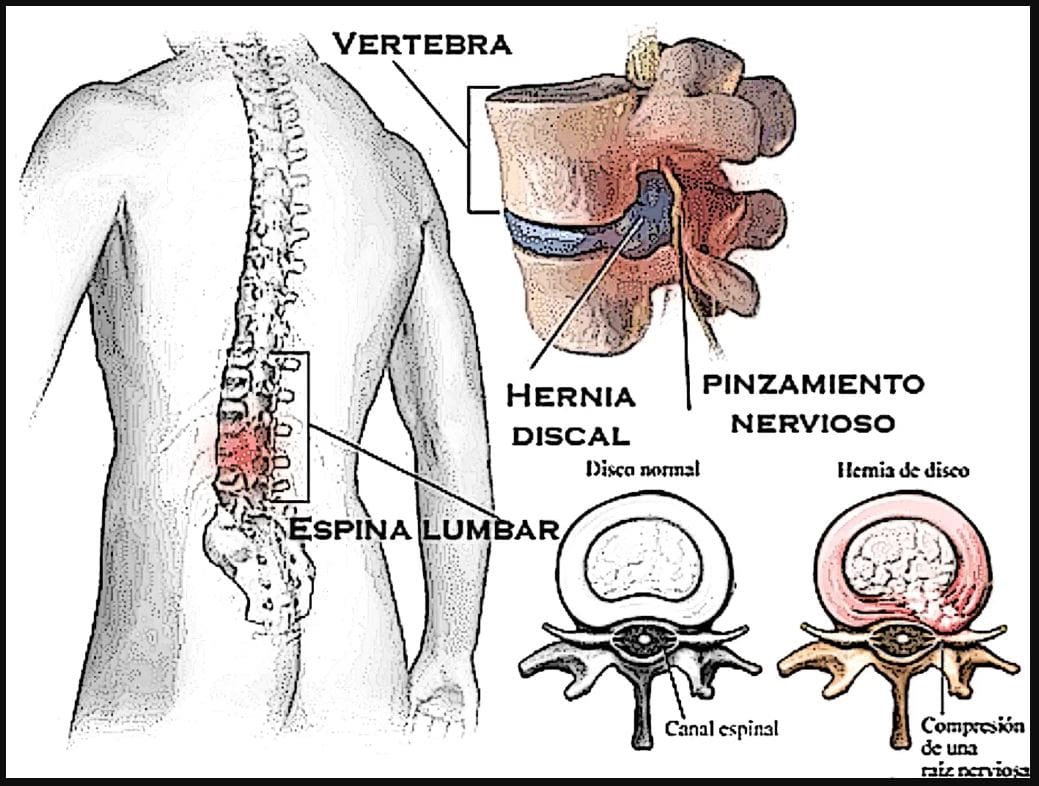
Specific low back pain: overlapping symptoms are caused by pathological mechanisms like, herniated discs, infections, musculoskeletal disorders, fractures, or disc degeneration.
Non-specific low back pain: where overlapping symptoms are causing pain in the lumbar region without a specific cause. This form of low back pain causes referred pain to different locations.
Many individuals commonly suffer from non-specific lower back pain, which can be triggered by environmental factors and affect their daily function. However, there are methods to alleviate lumbar back pain without surgery.
From Injury to Recovery with Chiropractic Care-Video
Nobody must suffer from lumbar back pain, as many effective treatments are available to help realign the body back to normal. Non-surgical treatments like chiropractic care and decompression therapy can reduce the effects of lumbar back pain and realign the spine. These treatments can restore blood flow and nutrients to spinal discs, relieve the affected muscles, and be personalized to an individual’s health and wellness plan. This may include physical therapy to strengthen weak muscles surrounding the lumbar, nutritional advice to incorporate healthy whole foods to feed the body, and mindfulness practices to reduce the effects of stress on the body. Check out the video above to learn how to identify the root cause of health issues related to lumbar back pain and take steps toward your health and wellness journey.
What Is Vertebral Axial Decompression?
If you’re experiencing lumbar back pain, there are a variety of non-surgical and non-invasive treatments that can help alleviate the discomfort. One such treatment is decompression therapy, which involves gently pulling the spine to reduce pain and rehydrate the spinal disc. In this article, we’ll discuss vertebral axial decompression, a specific type of therapy. According to Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C.’s book, “The Ultimate Spinal Decompression,” vertebral axial decompression can effectively reduce lumbar pain. Vertebral axial decompression (VAX-D) was developed by Dr. Allen Dyer, M.D., Ph.D. The book also explains that VAX-D uses a logarithmic time force curve to apply tension to the spinal column, bypassing muscle guarding reflexes in the lumbar spine and reducing disc pressure. Overall, vertebral axial decompression can be a useful treatment option for those with lumbar back pain.
How Does It Reduce Lumbar Back Pain?
Many individuals who suffer from lumbar back pain experience associated pain symptoms that affect their legs and feet. This is referred to as sciatica or leg pain associated with pressure on the spinal discs. Vertebral axial decompression is one effective solution to reduce this pressure and alleviate nerve root aggravation. Research studies have shown that this treatment can improve mobility, reduce pain in the lumbar spine, and minimize the effects of lumbar back pain. By lowering intradiscal pressure, vertebral axial decompression allows for better blood flow and nutrient absorption to rehydrate spinal discs.
Conclusion
Lumbar back pain is a common and costly issue that causes misalignment in the body by putting pressure on the spinal disc, resulting in referred pain in various body parts. Environmental factors can contribute to the development of this condition, causing muscles and nerves to become tense, weak, or strained. Fortunately, many treatments are available to alleviate lumbar spine pain and relieve pressure from the spinal discs. Decompression therapy is effective in restoring mobility and reducing pain. Vertebral axial decompression is a non-surgical option that gently stretches the spine and rehydrates the spinal disc, revitalizing the body.
References
Casser, Hans-Raimund, et al. “Acute Lumbar Back Pain.” Deutsches Arzteblatt International, 1 Apr. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4857557/.
Goose, E E, et al. “Vertebral Axial Decompression Therapy for Pain Associated with Herniated or Degenerated Discs or Facet Syndrome: An Outcome Study.” Neurological Research, Apr. 1998, pubmed.ncbi.nlm.nih.gov/9583577/.
Kaplan, Eric, and Perry Bard. The Ultimate Spinal Decompression. JETLAUNCH, 2023.
Koes, B W, et al. “Diagnosis and Treatment of Low Back Pain.” BMJ (Clinical Research Ed.), 17 June 2006, www.ncbi.nlm.nih.gov/pmc/articles/PMC1479671/.
When it comes to our muscles, many of us often don’t stretch each muscle group at least two to three times per week. From waking up in the morning, we stretch our arms, legs, and back to relieve any stiffness or soreness from the previous day. However, many individuals deal with musculoskeletal issues that can affect not only the back and the neck but also the upper and lower extremities of the body, causing pain-like symptoms that can worsen throughout the entire day if not treated right away. When this happens, musculoskeletal pain can lead to overlapping risk problems that can cause the body to be misaligned and dysfunctional. Hence why numerous therapies help reduce the effects of musculoskeletal pain and help restore the body naturally. Today’s article looks at how musculoskeletal pain affects the body and how treatments like MET can be used as self-help methods to reduce musculoskeletal pain. We utilize valuable information about our patients to certified medical providers using MET therapy to relieve musculoskeletal pain by incorporating various exercises and stretches. We encourage and refer patients to associated medical providers based on their diagnosis while supporting that education is a remarkable and fantastic way to ask our providers the essential questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., comprises this information as an educational service. Disclaimer
Musculoskeletal Pain Affecting The Body
Are you experiencing muscle stiffness or weakness in your back, neck, or shoulders? Do you feel pain when stretching or hunched over due to discomfort? Musculoskeletal pain is a common issue that can interfere with daily activities. Research studies show that this type of pain can cause symptoms that overlap with neuropathic or visceral pain. This means that problems with one muscle or organ in the body can lead to pain in other areas, causing significant discomfort.
Further research has shown that musculoskeletal pain can originate in the muscle tissues and persist for over three months, affecting many individuals’ social and emotional skills, work productivity, and independence. Several environmental factors like obesity, stress, poor sleep, inadequate nutrition, and lack of physical activity can overwork the muscles and joints, leading to trigger points and muscle strain in the musculoskeletal system, resulting in bodily misalignment.
Improving Athletic Performance Through Chiropractic- Video
Are you experiencing pain in specific areas of your body? Does the pain worsen when you are active or when you stretch? These pains are often associated with musculoskeletal issues, which can greatly affect your daily life. Research studies have revealed that musculoskeletal pain can significantly reduce a person’s productivity and job performance. Fortunately, several treatments are available to alleviate musculoskeletal pain and its symptoms. Many people seek chiropractic care or MET therapy to help realign their spine, stretch their muscles, and improve joint mobility. The video above demonstrates how chiropractic care uses manual manipulation to relieve musculoskeletal pain by stretching the muscles and realigning the spine.
MET Self-Help Methods For Musculoskeletal Pain
According to a book called “Clinical Applications of Neuromuscular Techniques” by Dr. Leon Chaitow, N.D., D.O., and Dr. Judith Walker DeLany, L.M.T., musculoskeletal pain can cause the soft tissues in the body to shorten and lead to disability. To alleviate the effects of musculoskeletal pain, people often seek the help of pain specialists such as chiropractors or massage therapists. These specialists often use muscle energy techniques (MET) to stretch the soft tissues and muscles and provide relief. Below are some exercises and techniques that are commonly used in MET therapy.
MET Neck Relaxation Techniques
The neck comprises soft tissues and is part of the musculoskeletal system. Two relaxation techniques can stretch out the shortened muscles to relieve soreness and stiffness in the scalene muscles. These techniques can help release tightness and improve the neck’s range of motion.
Phase 1:
Sit close to the table with the elbows and hands resting on the table surface on each side of the face.
Turn your head to the right or left as far as you can comfortably in one direction while letting your hands move with your face until you reach a pain-free rotation limit.
Afterward, use your left hand as resistance when turning your head to the left while using 25% or less of your strength to build up a force to match the resistance and start turning your head slowly.
Hold this push for 7-1o seconds and slowly stop turning your head to the left or right.
Return to a neutral position and turn to the right or left again to see how far you can stretch without pain.
You should notice the neck stretch is farther than it was previously.
This is known as post-isometric relaxation in MET therapy, as it allows the tight muscles to relax and stretch farther without pain than before.
Phase 2:
While lying on the table, the hands and elbows should be on the sides of the face.
Turn your head to the right to stretch as far as you can comfortably in one direction.
Use your right hand as resistance to attempt to turn without pain by using only 25% or less of your strength.
Slowly turn your head and maintain the turn and resistance for 7-10 seconds.
Slowly stop the resistance effort to see how far your neck can turn without pain. If you are experiencing pain, you use too much strength and reduce the contraction level where no pain is experienced.
This is known as reciprocal inhibition in MET therapy, as it achieves a different release for tight neck muscles.
Flexion Exercises Using MET
Flexion exercises in MET therapy help stretch the postural muscles and legs, feeling stiff. This allows spine flexibility while stretching out and reducing mechanical stresses in the surrounding muscles.
While sitting on the floor, your legs should be straight out, and your toes pointed towards the ceiling.
Bend comfortably as far as you can and grasp one leg with each hand.
Hold the position for 30 seconds and do four deep breathing cycles while allowing your head to hang down and relax into the stretch. *You will feel the stretch on your lower back and the back of your legs.
As you release during the fourth breathing cycle, ease yourself further down the legs and hold for another 30 seconds.
After 30 seconds, slowly return to an upright position by lightly pushing upwards from the hands.
Alternatively, you can bend one leg and do the same sequence on each leg to stretch out any leg muscles that are cramping or stiff. This flexion exercise help reduces pain and prevents trigger points from re-forming in the muscle fibers.
Extension Exercises Using MET
The extension exercises in MET therapy help the muscles and joints in the body group to increase movement without pain. This allows the body to be mobile and reduces the effects of musculoskeletal pain.
Lie on your stomach on a carpeted floor with a pillow to support your head and neck while your legs are together.
Bend your knees as comfortably as possible, and bring your heels towards your backside.
Now slowly grasp your legs and gently bend backward as far as possible without pain. Your back should be slightly arched.
Lift your head and shoulders gently to increase the arch in your back slowly and without pain.
Hold the position for four slow deep breaths, and hold your breath for 15 seconds on the last breathing cycle.
As you release, bring your body down slowly, from the legs to the stomach and finally, the shoulders and neck to rest.
This extension exercise, known as the boat position, helps lengthen and stretch the back and leg muscles while reducing pain and restoring mobility in the spine.
Conclusion
It is crucial to be aware of musculoskeletal pain in your body, whether in the morning or during work. This type of pain can lead to discomfort in other areas and even impair your ability to function. Fortunately, MET therapy can alleviate musculoskeletal pain by stretching the muscles and tissues and providing immediate relief. By utilizing stretching and physical therapy, you can help your body heal naturally and be more mindful of what triggers pain. Stretching can also prevent future injuries and promote a pain-free lifestyle.
References
Buck, Rhiannon, et al. “Working with Musculoskeletal Pain.” Reviews in Pain, June 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC4590039/.
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
El-Tallawy, Salah N, et al. “Management of Musculoskeletal Pain: An Update with Emphasis on Chronic Musculoskeletal Pain.” Pain and Therapy, June 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC8119532/.
Puntillo, Filomena, et al. “Pathophysiology of Musculoskeletal Pain: A Narrative Review.” Therapeutic Advances in Musculoskeletal Disease, 26 Feb. 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC7934019/.
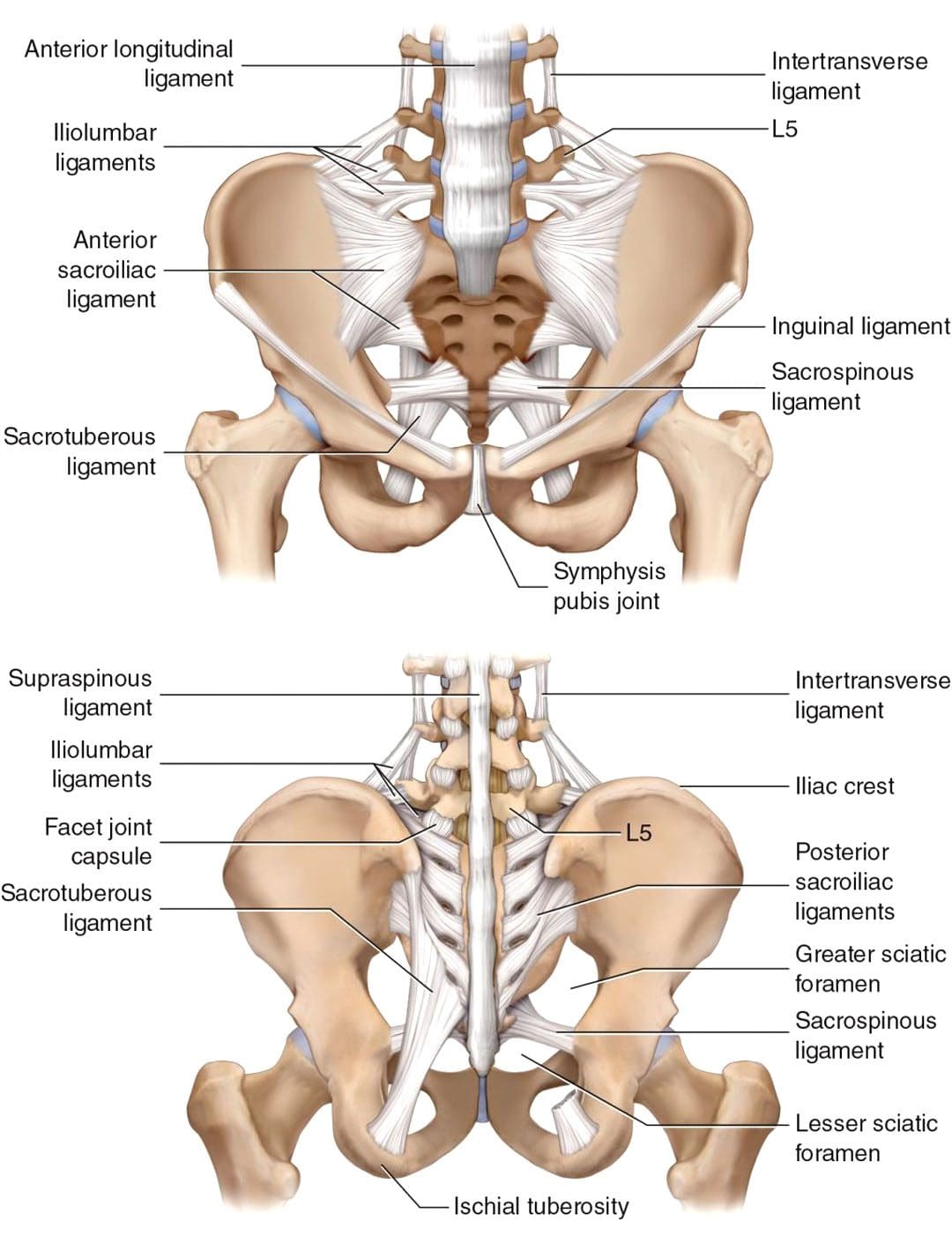
A joint is where two bones meet. The two sacroiliac or SI joints connect the spine, pelvis, and hips. This strong joint balances and transmits stress from the upper body to the pelvis and legs. The joints can suffer a sprain causing pain and discomfort symptoms. There can also be the feeling of tightness wrapping around the waist and dull aching across the low back as the surrounding muscles tighten up as a form of protection, also known as muscle guarding. A correct diagnosis is vital to avoid any potentially serious complications. Chiropractors are experts on neuromusculoskeletal problems and can treat, heal, and strengthen the body through various MET, mobilization, and manipulation techniques.
Sacroiliac Sprain
The main function is to balance the upper and lower body forces. The sacroiliac joints are surrounded by muscle, connective tissue, nerves designed to withstand large stresses and a complex system of ligaments, further strengthening the joints.
Injury Causes
Sacroiliac sprains can be caused by direct trauma to the pelvis from a fall or automobile collision or jobs and sports that involve a lot of bending and twisting. However, sometimes there is no distinct cause. Common causes include:
Repetitive microtrauma is excessive/repetitive movements like prolonged twisting, bending, or lifting at work, home, physical activities, and sports.
The joint can be pushed out of alignment.
Muscular imbalance or weakness in the muscles surrounding the sacroiliac joints can cause problems to develop over time, presenting little or no symptoms.
The tissues around a sacroiliac joint also can be stretched or torn.
Trauma such as a fall or road traffic accidents
Problems with the hips, knees, and feet can generate increased pressure on the joint, which can become painful over time due to repetitive strain.
Pregnancy hormones released to promote pelvis relaxation can increase the risk of SI sprain injury.
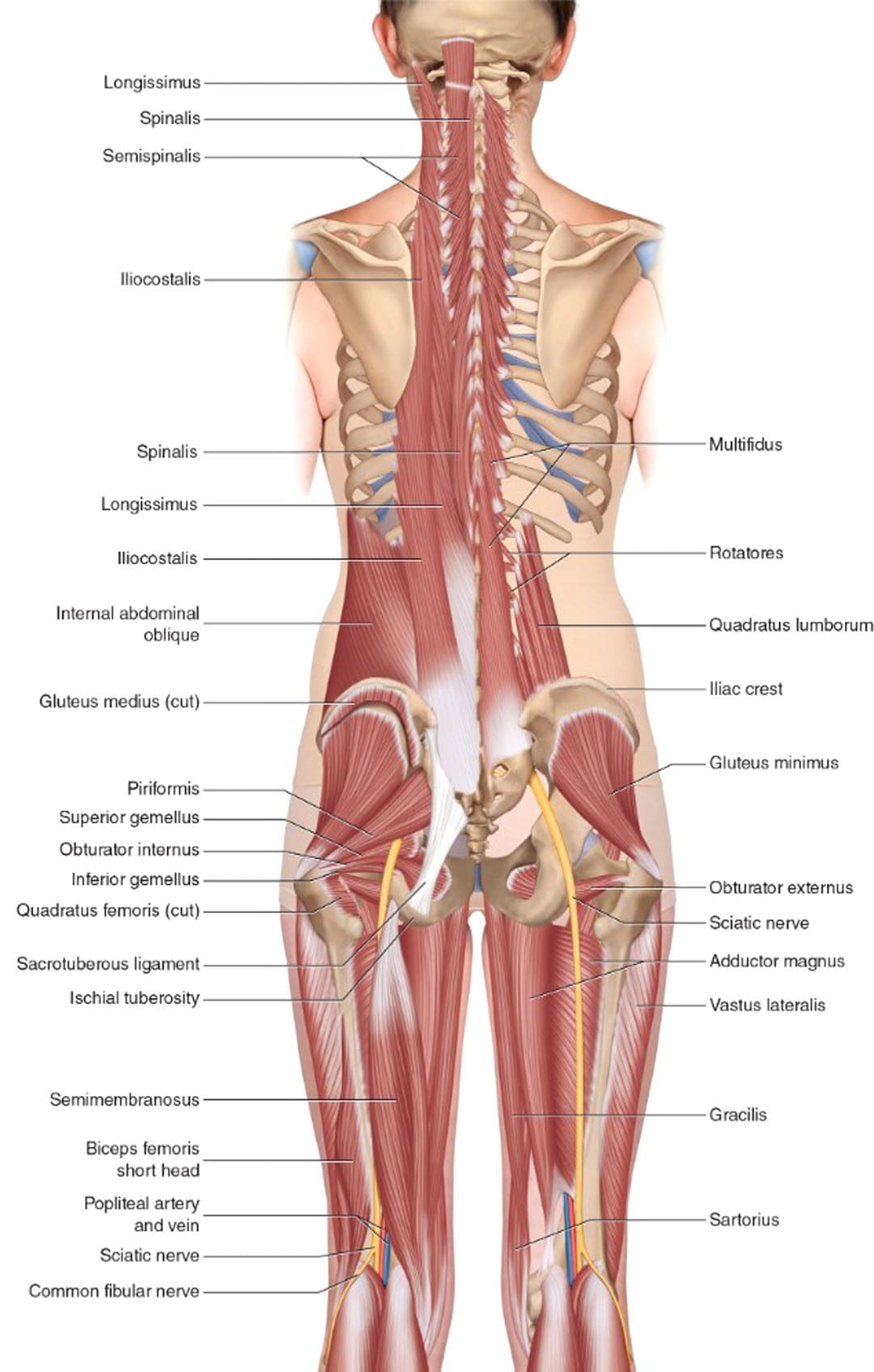
Excessive stress on the joint can cause microscopic damage to the ligaments surrounding the joint. The joint then becomes inflamed and presents with pain and sensations of discomfort. The body responds by contracting the muscles to prevent further damage. However, the muscle spasms may not stop, resulting in more pain. Referred pain is common from the muscles that go into spasm, with the most affected being the piriformis, gluteal/buttock, and psoas muscles.
Signs and Symptoms
Tenderness over the affected joint and area.
Pain symptoms on one or both sides above the joints and into the buttocks.
Standing or working with increased weight on one leg increases pain symptoms.
Pain after lifting or twisting that develops a little while later.
Pain travels to the back of the leg, front of the thigh, and the groin.
Pain gets worse when sitting and bending forward.
Lying down eases the symptoms.
Most cases report no loss of strength, tingling, or numbing sensations.
Chiropractic Treatment
Chiropractic treatment will relieve the pain symptoms, but there are stages of treatment, each with specific goals before moving to the next.
The objective of the initial stage is to decrease pain and inflammation.
The second stage is stabilizing and restoring proper musculoskeletal function.
Rehabilitation and targeted stretches and exercises will be introduced as the treatment continues.
In the maintenance stage, there should be no pain, and the individual should be able to perform normal daily activities and return to normal life.
Recovery time for a sacroiliac sprain can be 4-6 weeks but can take months to heal completely.
Chiropractic Approach for Pain Relief
References
BIDWELL, A M. “Treatment of sacroiliac sprain by manipulation.” The Medical World vol. 65,1 (1947): 14-6.
Evans, P. “Sacroiliac sprain.” American family physician vol. 48,8 (1993): 1388; author replies 1390.
LeBlanc, K E. “Sacroiliac sprain: an overlooked cause of back pain.” American family physician vol. 46,5 (1992): 1459-63.
Sun, Chao, et al. “Cost and outcome analyses on the timing of first independent medical evaluation in patients with a work-related lumbosacral sprain.” Journal of Occupational and environmental medicine vol. 49,11 (2007): 1264-8. doi:10.1097/JOM.0b013e318156ecdb
The lumbar/low back muscles support the upper body’s weight and are involved in moving, twisting, bending, pushing, pulling, and reaching. These repetitive actions can result in a lumbar strain, which is muscle damage or injury to the tendons or muscles of the lower back, causing spasms, soreness, and pain. A lumbar strain can be the source of severe pain symptoms; it can be debilitating and, if left untreated, can lead to chronic conditions. Injury Medical Chiropractic and Functional Medicine Clinic can relieve symptoms, realign the body, relax, rehabilitate, strengthen muscles, and restore function.
Lumbar Strain
The lumbar vertebra makes up the region of the spine in the lower back. Sudden injuries or overuse injuries can damage the tendons and muscles. Lumbar muscle strain is caused when the muscle fibers are abnormally stretched or torn. Lumbar strain can be acute/sudden or chronic/lingering. A strain that has been present for days or weeks is referred to as acute. It is considered chronic if it has persisted for over three months. It can occur at any age but is most common in individuals in their forties. Increased risk factors can include:
Weakened back or abdominal muscles can cause
Tight hamstrings can pull the low back muscles down.
Excessive lower back curvature.
Forward-tilted pelvis.
Symptoms
Lumbar strain can have varied signs and symptoms depending on the location, damage, and cause of injury. The damage can range from simple overstretching injuries to partial or complete tears of varying degrees. The tears cause inflammation in the surrounding area, resulting in back spasms and difficulty moving. A muscle spasm is a cramp caused by a sudden and involuntary contraction or twitch and can be one of the symptoms of a lumbar strain. Other symptoms can include:
Muscle spasms either with activity or when resting.
Stiffness in the low back.
Difficulty standing or walking, with slight relief when resting.
Trouble doing simple tasks like bending or climbing stairs.
Low back pain can radiate into the buttocks without affecting the legs.
The lower back may be tender and sore to the touch.
Decreased muscle strength.
Restricted or limited range of motion.
Inability to maintain healthy posture because of stiffness and/or pain.
Discomfort symptoms that persist.
Discomfort ranges from mild aches to sharp, debilitating pain.
Intermittent flare-ups.
Causes
There are often multiple underlying risk factors contributing to the injury or damage. A few of the most common causes:
Depending on the severity, a doctor or health care provider could recommend chiropractic treatment and physical therapy. The chiropractor will perform an evaluation, combined with the doctor’s diagnosis, to develop a customized/personalized treatment plan. Treatment may include:
Ice and heat therapy
Massage to stimulate blood circulation
Percussive muscle stimulation
Pelvic traction
Ultrasound
Stretching exercises
Exercises to do at home for long-term relief.
It is a safe option to loosen tight back muscles, relieve pain, and promote lower back healing.
Spine Injuries In Sports
References
Ball, Jacob R et al. “Lumbar Spine Injuries in Sports: Review of the Literature and Current Treatment Recommendations.” Sports medicine – open vol. 5,1 26. 24 Jun. 2019, doi:10.1186/s40798-019-0199-7
Domljan, Z et al. “Lumbalni strain-sindromi” [Lumbar strain syndromes]. Reumatizam vol. 38,5-6 (1991): 33-4.
Li, H et al. “Rehabilitation effect of exercise with soft tissue manipulation in patients with a lumbar muscle strain.” Nigerian journal of clinical practice vol. 20,5 (2017): 629-633. doi:10.4103/njcp.njcp_126_16
Williams, Whitney, and Noelle M Selkow. “Self-Myofascial Release of the Superficial Back Line Improves Sit-and-Reach Distance.” Journal of sport rehabilitation vol. 29,4 400-404. 18 Oct. 2019, doi:10.1123/jsr.2018-0306
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine