Self-care for secondary type headaches. Different types of headaches range from mild to excruciating, and the frequency of occurrence also varies from person to person. Headaches are classified into three types that are primary, secondary, and nerve pain headaches. Primary are tension, migraine, and cluster headaches. Nerve pain headaches are also called cranial neuralgia headaches. This is when one or more cranial nerves that run down the neck from the brain become inflamed, causing pain and discomfort. Secondary headaches are a symptom of a bodily reaction or an injury. These types of headaches can be caused by:
Sinus problems
Allergies
Physical exertion
Dehydration
Caffeine
Hormones
Medications
Alcohol consumption
Concussion
Trauma
Sinus Headaches
These can be caused by a sinus infection. If pain presents in the upper teeth, a fever, and yellow or green nasal discharge, this could mean an infection. A doctor can help with some antibiotics. For individuals that regularly get sinus headaches from changes in air pressure or other causes, here are a few self-care techniques:
Hot Shower
Steam can help drain the sinuses. Take a hot shower or hold your head over a pot of steaming water.
Nasal Irrigation and Neti Pots
This ancient remedy comes from India. The concept is simple; the teapot has a long spout that goes inside one nostril. The water/saline solution will go through the sinuses and come out the other nostril draining the nose and relieving the pressure.
Hot and Cold Compresses
Individuals can find relief by alternating between hot and cold compresses placed on the forehead. This reduces swelling and allows the sinuses to drain.
Eucalyptus Oil
This powerful oil from Eucalyptus leaves helps clear up sinuses. It can be done by smelling a few drops placed on a cloth for 10 minutes or placing a drop or two in hot water and breathe in the steam.
Allergy Headaches
Allergies are a common cause of headaches. Self-care can include:
Nitrates and Nitrites Avoidance
These are common food preservatives in processed types of meat like bacon, hot dogs, and sausages. It is a preservative, but many individuals can have an allergic reaction that causes headaches instead of hives.
Avoid Powerful Smells and Odors
This can be difficult with all the smells wafting around but try to pay attention to the surrounding smells as any could cause an allergic reaction. Strong odors can include:
Cleaning products
Nail polish
Perfume
Hair spray
Paint
Cigarette smoke
Elimination Diet
Food allergies often result in digestive problems, hives, and swollen airways but can also cause headaches. Even individuals that are not allergic to the food itself could be sensitive to other items like artificial colors or preservatives. The most common food items that cause headaches include:
Cheese
Chocolate
Citrus fruit
Coffee
Alcohol
Consulting with a health coach and/or nutritionist can help to create a customized meal plan.
Exertion Headaches
Exertion headaches can be produced by physical activity/exercise or strain. They usually begin with throbbing pain on both sides of the head and cause a red face or complexion. They can be caused by:
Prolonged physical activities, exercise.
Strenuous activity at work lifting objects or weights.
Self-care for stopping an exertion headache includes:
Cooling Down
An exertion headache is the body’s way of saying that it has overextended its ability.
Drinking some cool water
Take a break for 20-30 minutes.
Avoid Headache Triggers
Try to stay aware when these headaches present and pay attention to see if there is a trigger.
This can be caused by dehydration
Not enough sleep.
Chiropractic and Physical Therapy
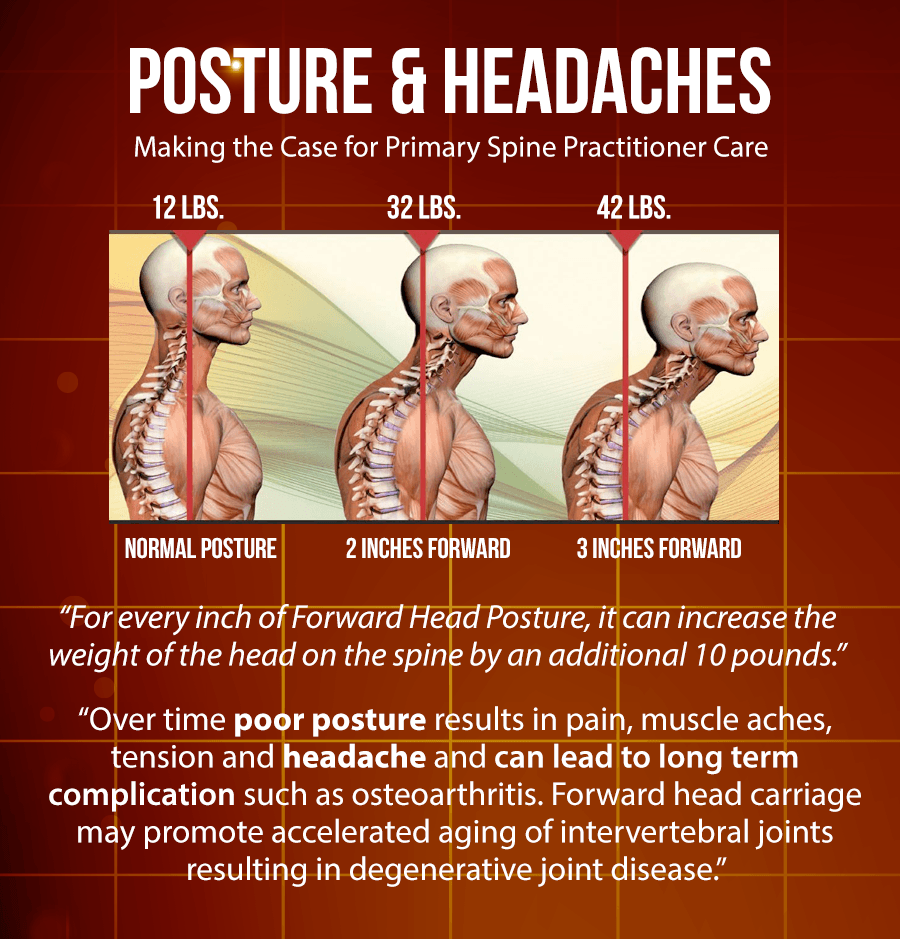
These types of headaches can also be caused by incorrect posture when working or exercising.
Lifting heavy weights or running with the head too far forward or back limits blood flow, causing muscle tension.
A chiropractor adjusts the spine and whole-body
Educate on core strengthening exercises and proper form.
Caffeine Headache
Caffeine narrows the blood vessels that surround the brain. When an individual stops consumption, the blood vessels enlarge. This causes an increase in blood flow and pressures on the brain’s surrounding nerves. This can trigger a caffeine withdrawal headache. Self-care includes:
Peppermint or Lavender Oil
Massaging a drop of oil into the temples can open up the blood vessels and relieve the pressure.
Ice Packs
Applying an ice pack to the back of the neck can stop a caffeine headache.
Taking a Nap
Lying down and taking a nap for 30-60 minutes can help bring relief.
Alternate decaf coffee with regular coffee.
Hormone Headache
Estrogen levels can affect various areas of a woman’s body, including headaches. Headaches experienced just before or in the first days of a menstrual cycle are known as menstrual migraines. Headaches that start when ovulating are called hormone headaches. Self-care can include:
Yoga
Practicing yoga can help prevent headaches from occurring.
Sleep
7-9 hours of sleep are recommended every night to allow the body to flush out old hormones and create new ones.
This can help prevent a hormone overload.
Massage
Stress leads to headaches.
Massage therapy is highly recommended to reduce stress and keep the body loose and relaxed.
Changing Birth Control Pills
Certain types of birth control pills can have more side effects than others, including headaches.
Ask a doctor about switching to another type to see if it helps.
Body Composition
Master Cleanse Diet
The Master Cleanse Diet is a prescriptive program that focuses on a specific food or drink regimen. This diet is intended to last around two weeks and relies on:
Bryans, Roland et al. “Evidence-based guidelines for the chiropractic treatment of adults with headache.” Journal of manipulative and physiological therapeutics vol. 34,5 (2011): 274-89. doi:10.1016/j.jmpt.2011.04.008
Chaibi, Aleksander, and Michael Bjørn Russell. “Manual therapies for primary chronic headaches: a systematic review of randomized controlled trials.” The journal of headache and pain vol. 15,1 67. 2 Oct. 2014, doi:10.1186/1129-2377-15-67
Green, Mark W. “Secondary headaches.” Continuum (Minneapolis, Minn.) vol. 18,4 (2012): 783-95. doi:10.1212/01.CON.0000418642.53146.17
Individuals that experience frequent headaches can have sensitive headache trigger points. Every case is different and requires a thorough examination before a proper and personalized chiropractic treatment plan can begin. Headaches can be brought on from a variety of causes. This could be:
Drug reactions
Temporomandibular joint dysfunction (TMJ)
Tightness in the neck muscles
Low blood sugar
High blood pressure
Stress
Fatigue
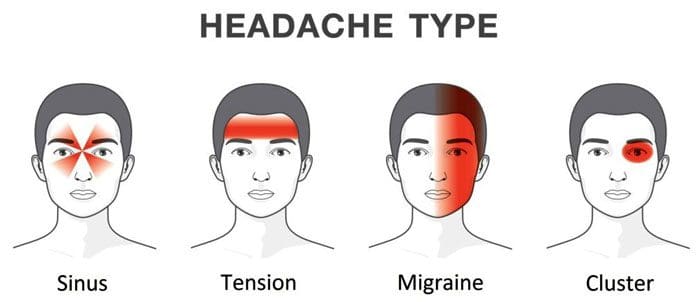
The majority of recurrent headaches fall into three types:
Tension headaches, also known as cervicogenic headaches
Tension headaches are the most common and affect around 77% of individuals experiencing chronic headaches. Most individuals describe a tension headache as a consistent dull ache on one side of the head and sometimes both sides. They are often described as having a tight band/belt around the head or behind the eyes. These headaches usually start slowly, gradually and can last for a few minutes or days. They tend to start in the middle of the day or before the end of the day.
These headaches can be the result of stress and/or poor posture. The most common cause is subluxations in the upper back and neck, usually combined with active headache trigger points. This stresses the spinal muscles in the upper back and neck. A tension headache or stress headache can last 30 minutes to a few days. Chronic tension headaches can last for months. The pain can be severe; however, these headaches are typically not associated with symptoms like throbbing, nausea, or vomiting.
If the top cervical vertebrae shift out of their position and lose their normal motion, a small muscle called the rectus capitis posterior minor/RCPM begins to spasm. This small muscle has a tendon that slips between the upper neck and the base of the skull. It attaches to a thin, sensitive tissue called the dura mater that covers the brain. The dura mater is very pain-sensitive. When the RCPM muscle goes into spasm, the tendon pulls the dura mater causing a headache. Individuals that work at a desk station for long hours tend to experience headaches from this cause. Another cause comes from referred pain caused by headache trigger points in the Sternocleidomastoid/SCM or levator muscle on the side of the neck. This cause tends to happen more to individuals that have suffered a whiplash injury with muscle damage in the neck region.
Migraine Headaches
Migraines are intense and throbbing headaches that are associated with nausea and sensitivity to light or noise. They can last for a few hours to a few days. Many experience visual symptoms known as an aura just before they come on. This is described as seeing flashing lights or when things take on a dream-like appearance. However, even in individuals that don’t experience the aura, most can tell that a migraine is getting ready to present. Individuals usually have their first attack before age 30. They tend to run in families supporting a genetic component. Some have attacks several times a month, while others can have less than one a year. Most individuals find that migraines happen less and become less severe as they get older.
These headaches are caused by the constriction of blood vessels in the brain. During the constriction period, there is a decrease in blood circulation. This is followed by dilation/enlargening of the blood vessels. This is what leads to the visual symptoms. Then the blood vessels dilate, generating a rapid increase in blood pressure inside the head. This increased pressure is what leads to a pounding headache. Every time the heart beats, it sends another shock wave through the carotid arteries in the neck into the brain. There are different theories as to why the blood vessels constrict, but they are still unknown. What is known is that several factors can trigger a migraine. This includes:
Lack of sleep
Stress
Flickering lights
Strong smells
Changing weather
Foods that are high in an amino acid known as tyramine
Cluster
Cluster headaches are very short excruciating headaches. They are usually felt on one side of the head behind the eyes. These headaches affect about 1 million individuals and are more common in men. This type of headache tends to happen at night. They are called cluster headaches because they tend to happen one to four times a day over several days. After one cluster is over, it could be months or even years before they present again. Like migraines, cluster headaches cause the dilation of the blood vessels in the brain, increasing the pressure.
Trigger Points
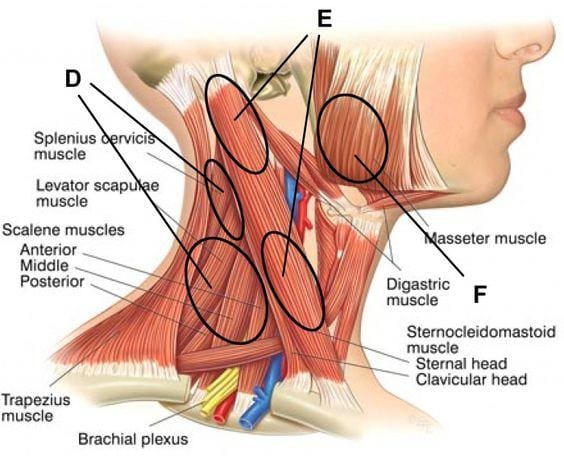
Headache trigger point therapy involves four muscles. These are the:
The Splenius muscles involve two individual muscles, the Splenius Capitis and the Splenius Cervicis. These muscles run along the upper back to the skull base or the upper cervical/neck vertebrae. Trigger points in the Splenius muscles are a common contributor to pain that travels through the head to the back of the eye and top of the head.
The Suboccipitals are a group of four small muscles that maintain proper movement and positioning between the first cervical vertebra and the skull base. Trigger points in these muscles can cause pain that feels like it’s happening inside the head, from the back to the eye and forehead. Individuals report that the whole side of the head hurts. This is a pain pattern similar to a migraine.
The Sternocleidomastoid muscle runs along the base of the skull, behind the ear, down the side of the neck. It attaches to the top of the sternum/breastbone. Although most are not aware of this muscle’s trigger points, the effects are evident. This includes:
Referred pain
Balance issues
Visual symptoms
Referred pain tends to be eye pain, headaches over the eye, and can even cause earaches. An unusual characteristic of SCM headache trigger points is that they can cause dizziness, nausea, and balance problems.
The trapezius muscle is the large, flat muscle in the upper and middle back. Pain can be felt in the temple and back of the head. A common trigger point is located at the top of the muscle. This particular point can activate secondary trigger pointsin the temple or jaw muscles, leading to jaw or tooth pain.
Headache Triggers
Stress can be a trigger.
Depression, anxiety, frustration, and even pleasant excitement can be associated with headache development.
A headache diary can help determine whether factors like food, weather, and/or mood correlate with headache patterns.
Repeated exposure to nitrite compounds can result in a dull headache accompanied by a flushed face. Nitrite dilates blood vessels and is found in products like heart medications, and is also used as a chemical to preserve meat. Processed meats containing sodium nitrite can contribute to headaches.
Foods prepared with monosodium glutamate or MSG can result in headaches. Soy sauce, meat tenderizers, and various packaged foods contain this chemical as a flavor enhancer.
Exposure to poisons, even household varieties like insecticides, carbon tetrachloride, and lead, can contribute.
Contact with lead batteries or lead-glazed pottery.
Foods that are high in the amino acid tyramine should be avoided. This could be ripened cheeses like cheddar, brie, chocolate, and pickled or fermented food.
Bio-Chiropractic
Chiropractic adjustments are highly effective for treating tension headaches, especially those that originate in the neck. Research has found that spinal manipulation resulted in almost immediate improvement and had fewer side effects and longer-lasting relief than taking common medications. There is a significant improvement by manipulating the upper two cervical vertebrae, combined with adjustments to the area between the cervical and thoracic spine.
Body Composition Testing
Vibration Exercise
Vibration exercise is believed to stimulate the muscle fibers without going to a gym or stressing the bones. One study broke up postmenopausal women into three groups: resistance training, vibration training combined with resistance training, or no exercise/training. Their body composition was measured before starting the study. After the study was completed, the findings included:
Both the resistance group and the resistance group with vibration training increased lean tissue mass.
The control group did not show an increase in lean tissue and, in fact, gained body fat.
The combination group, using vibration training with resistance training, showed a drop in body fat.
Another study placed male athletes in a training program that included vibration training. The first group had lower-limb strength training combined with vibration training, and the other had lower-limb strength training without vibration training. The researchers found that the athletes in the vibration training group improved leg extension strength by five percent. In addition, the vibration training groups balancing ability and vertical lift/jumping test improved as well.
References
Bryans, Roland et al. “Evidence-based guidelines for the chiropractic treatment of adults with headache.” Journal of manipulative and physiological therapeutics vol. 34,5 (2011): 274-89. doi:10.1016/j.jmpt.2011.04.008
Chaibi, Aleksander et al. “Chiropractic spinal manipulative therapy for cervicogenic headache: a single-blinded, placebo, randomized controlled trial.” BMC research notes vol. 10,1 310. 24 Jul. 2017, doi:10.1186/s13104-017-2651-4
Bryans R, Descarreaux M, Duranleau M, et al. Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J Manipulative Physiol Ther 2014; 37: 42-63.
Bryans R, Descarreaux M, Duranleau M, et al. Evidence-based guidelines for the chiropractic treatment of adults with headache. J Manipulative Physiol Ther 2011; 34: 274-89.
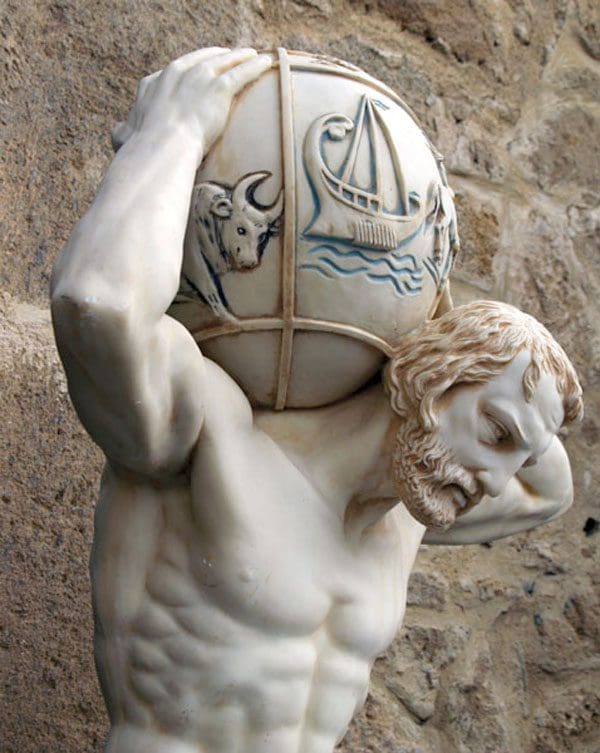
The Atlas vertebra is named for the mythological figure who held the world on their back/neck. The vertebrae are located at the top of the spine, where the cranium and spine connect. More than just a foundation for support, the vertebrae could be the most important vertebrae of the body. It consists of a complex bundle of nerves, vertebral arteries, and is the point where the entire weight of the cranium makes contact.
The myth requires Atlas to be careful while holding the world carefully and confidently at all times, otherwise it will come crashing down. The key is being able to balance it perfectly. The vertebra has the same job to hold the head up properly and maintain posture. If not problems with balance and alignment will begin to develop, and affect the entire spine.
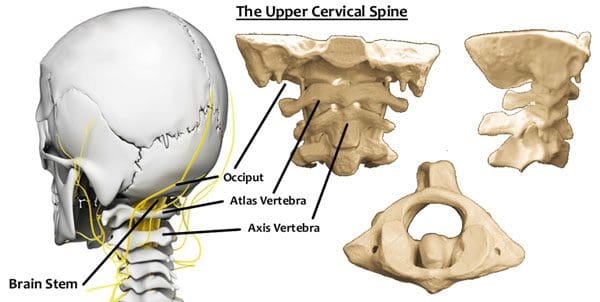
The Atlas Vertebra
Balance
The Atlas vertebrae’s role in maintaining balance is based on its ability to adjust to the weight of the head. The actual vertebra is wider than the other cervical vertebrae. This creates a center of gravity that is reinforced through proper posture. It distributes the weight of the head (10-12lb) evenly to centralize the weight and is supported by the natural curvature of the spine.
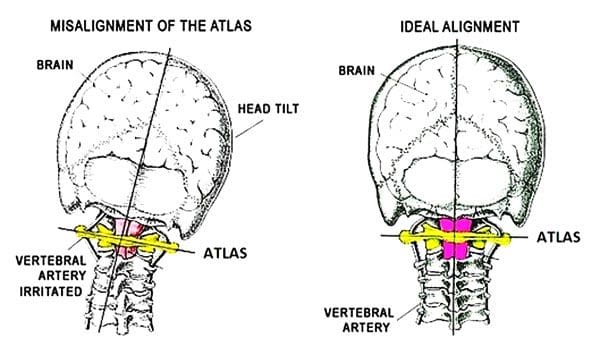
If the center of gravity shifts, the Atlas vertebra will tilt in that direction as well. This creates instability in the cervical spine and can increase the amount of weight the spine is taking and trying to redistribute. This creates spinal issues and leads to everything from poor posture, overcompensation that leads to injury.
Shifting Causes
Disruption to the vertebra and its ability to balance can come from a variety of causes and can occur as a result of chronic and acute conditions. Some include:
Auto accidents, sports, work injuries can cause cervical soft tissue damage
Dislocation of cervical vertebrae below the Atlas results in instability
Poor posture/s make individuals overcompensate to one side of the body straining muscles, ligaments, tendons causing pain and other issues
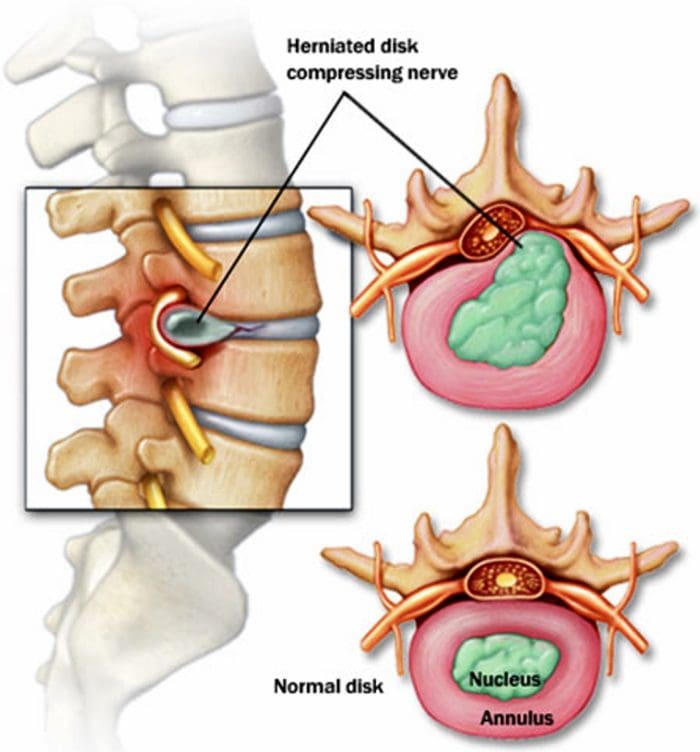
Herniated, bulging, and slipped discs
Unbalanced effects
Spinal issues range from simple neck pain and soreness to full-on chronic pain. Because the Atlas can alter the balance of the entire spine, combined with cranium support, issues can be localized and referred creating further complications. Addressing the root problems requires a comprehensive chiropractic approach. Chiropractic will assess the position of the spine and determine the degree to which Atlas has shifted out of place. An adjustment treatment plan makes it possible to undo the widespread damage.
Body Composition
Muscle Loss
Individuals do not realize that muscle loss occurs throughout their lifetime. This is because muscles, like other tissues in the body, must go through cell turnover and protein synthesis. This means that the body is constantly breaking down protein in the muscles and rebuilding them.
Skeletal muscle can be developed with proper nutrition and includes consuming a proper amount of protein to provide the necessary amino acids and from physical activity. The reverse is also true, if an individual becomes less physically active and/or their diet no longer supports the development of increased muscle tissue, the body enters a catabolic/tissue-reducing state known as muscle atrophy.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Woodfield, H Charles 3rd et al. �Craniocervical chiropractic procedures – a pr�cis of upper cervical chiropractic.��The Journal of the Canadian Chiropractic Association�vol. 59,2 (2015): 173-92.
Headaches can be detrimental to a high quality of life.� Especially, migraine and tension headaches.�Some deal with them on a weekly, or even daily, basis.�They can range from minor to life-changing afflictions. There are various causes, symptoms, and treatment options. The first step in treating headaches is understanding the type of headache it is.
Some people think they have a migraine, when in fact, they are suffering from a tension headache. Tension headaches are more common. But the Migraine Research Foundation found that 1 in 4 U.S. households include someone that suffers from migraines. Determining what type of headache can take some research.
Here are some things to think about to determine if the headache is a migraine or a tension headache.
Headache/s origin
According to the Mayo Clinic, migraines often begin in adolescence or early adulthood. Tension headaches can start at any time in an individual’s life.� An adult just beginning to have recurring headaches means that they are most likely tension headaches.
Where is the pain located
Migraines usually happen on one side of the head. Tension headaches can affect both sides of the head and can produce intense pressure on the forehead. The location of the pain can be a key indicator of the type of headache.
Describe the pain
If it is a dull pain, with pressure, and tenderness around the scalp, this could mean a tension headache. If the pain is throbbing or pulsing pain, it could be a migraine. Both headaches can present intense pain, just different types of pain.
Other symptoms
Migraines often come with symptoms beyond head pain.
Nausea
Light sensitivity
Sound sensitivity
Seeing bright flashing/sparkling lights
A sensation of Pins and needles in one or both arms
Dizziness
Individuals not experiencing any of these symptoms are more than likely dealing with a tension headache.
Functionality
Those with tension headaches can still perform jobs, drive, read, and operate through daily life even though it can be painful and frustrating. Migraines are very different. Lying down in a dark, quiet room with an eye mask on until the headache passes is how many handle their migraines. If the headache disrupts your life it is more than likely a migraine.
Over the counter pain killers
Tension headaches can usually be relieved with over-the-counter pain meds. However,�this type of treatment does not work for migraines. When a migraine shifts into full force, the individual has to go through it. Headaches that respond well to nonprescription pain killers means it’s a tension headache. The majority will at some point deal with a headache.
Although tension headaches are more common that doesn’t rule out the possibility of the headache being a migraine. Just a little insight as to the type of headache that is presenting, and some proactive treatments. No matter the type of headache, if the pain is severe, or starts up after a head injury, seek medical treatment.
There are different kinds of head and upper cervical disorders that are also known as:
Upper neck disorders
Craniovertebral junction – CVJ – abnormality
Craniocervical disorders
Some are present at birth while others are developed later in life. Whether congenital or acquired, they share many of the same symptoms.
Neck Pain/Headache
Where your skull and spine meet is where upper cervical disorders take place. Neck pain along with headaches along the back of the head are the most common symptoms. People with craniocervical disorders often experience neck pain and headache in combination and symptoms worsen with head and neck movement. Even just a sneeze or cough can cause pain. Neck pain can also spread to the arms if spinal nerves are compressed.
Spinal Cord Compression
The more complex upper cervical disorders involve spinal cord compression. When the spinal cord gets compressed, nerve problems can happen that make daily function a challenge.
With spinal cord compression, neurological symptoms can present like:
Weakness in the arms, legs or both
Loss of sensation and awareness of the limbs called positional sense
There can be an electrical/shooting pain or tingling running down the spine and into the legs when pitching the neck forward called Lhermitte sign
Hot and cold sensational loss in hands, feet or both
All of these can cause malformation and physical changes in the neck. The neck may appear short, webbed, or twisted. There can also be a limited ability to move the neck.
Symptoms can also be caused by brain and cranial nerve pressure
Conditions like platybasia, basilar invagination, and craniocervical tumors can place pressure on the brain stem and the cranial nerves around it. If this happens the following symptoms can occur:
Eye issues like abnormal eye movements and double vision
Throat and speech problems like hoarseness, slurred speech, and swallowing problems
Loss of coordination
Sleep problems like sleep apnea
Vertigo Faint Feeling
Some individuals could experience a set of symptoms that don’t occur too often called vertebrobasilar ischemia.
This happens when the head position changes placing pressure on the cranial arteries and cutting off the blood supply.
The result is:
Weakness
Confusion
Light-headedness
Feeling faint
Vertigo or a dizzy spinning sensation
Syringomyelia
Syringomyelia is a fluid-filled cyst known as a syrinx that forms inside the spinal cord. If the cyst grows, it can damage the spinal cord causing painful neurological symptoms throughout the body that include weakness, and numbness. In extreme cases loss of ability to feel heat or cold in the neck, hands, and possibly throughout the spine. The hand muscles can become paralyzed.
Quality of Life with Upper Cervical Disorder
While some individuals have no symptoms associated with a craniocervical disorder, others experience intense pain and neurological dysfunction. There are treatment options that can help you successfully manage and eliminate symptoms.
Chiropractic
When headaches present it usually means there is a misalignment in the cervical spine. This is often combined with tight muscles in the neck, shoulders, and surrounding area. Pressure on the nerves can cause sharp shooting pain along with a continual dull throbbing sensation.
A chiropractor will assess the area and then move forward with an adjustment to relieve the pressure and pain. Chiropractic medicine does not just focus on relieving symptoms but finding the root cause and correcting the problem. In addition, the chiropractor will take the time to educate you on the importance of diet, exercise, stretching, and making healthy lifestyle choices.
Whiplash Massage Therapy
NCBI
The effectiveness of chiropractic care for headaches has been proven by many research studies. Chiropractic is not only excellent for treating headaches, but is gentle, non-invasive, does not require medications, and is known for being free of side effects.
Metabolic Syndrome affects many people. In fact, more than a quarter of the United States has it! Metabolic Syndrome is not a disease, but instead a cluster of disorders. These disorders on their own are not necessarily alarming but when you have more than one, the body starts to feel the repercussions.
Symptoms
Those with metabolic syndrome often suffer from frequent headaches, inflammation, nausea, fatigue, joint pain, and many more. On top of these symptoms, metabolic syndrome can put individuals at a higher risk for Type 2 Diabetes, Heart Disease, Stroke, Obesity, Sleep Apnea, and Kidney Disease.
Risk Factors
Individuals who have an “apple or pear” body shape, are at an increased risk for developing metabolic syndrome. There are no “obvious” signs of metabolic syndrome, but rather one with metabolic syndrome has 3/5 of these risk factors.
A fasting blood glucose level of 100 mg/DL
High Blood Pressure, measuring 130/85
High Triglycerides
Low HDL (Good Cholesterol)� measuring <40mg/DL Men & <50mg/DL Women
Excess Waist Fat (>40in Men & >35in Women)
What Can You Do About It?
Of course, no one wants to be left feeling sick and stranded. There are ways to help prevent metabolic syndrome at home. Below there are five tips for each risk factor and how to prevent/reduce your symptoms.
A Fasting Blood Glucose Level Of 100 mg/DL
Ketogenic Diet
Increase Fiber
Control Portions
Set “Carb Goals”
Choose complex carbs over simple carbs
High Blood Pressure, measuring 130/85
Reduce Sodium
Lower caffeine
DASH diet (Dietary Approaches to Stop Hypertension)
Boost Potassium
Read Food labels
High Triglycerides
Limit sugar intake
Increase fiber
Establish a regular eating pattern
Eat more “tree nuts” ( almonds, cashews, pecans)
Switch to unsaturated fats
Low HDL ( Good Cholesterol) measuring <40mg/DL Men & <50mg/DL Women
Reduce Alcohol
Do not smoke
Choose better fats
Purple Produce (antioxidants to help inflammation)
Increase fish consumption
Excess Waist Fat >40 in Men & >35 in Women
Ketogenic Diet
Exercise Daily
Walk after dinner
Grocery Shop without Aisles
Increase in Water Consumption
Solutions
Aside from doing these tricks and tips at home, a doctor or health coach will be able to further assist one in healing. The main goal is to take these symptoms and disorders and correct them before they become a full-blown diagnosis.
Rather than just running a basic blood panel, they now have tests that allow us to see multiple different levels and numbers. these elaborate blood tests provide great insight to allow us to see the full picture. By completing these labs, it allows the doctor to evaluate the patients better and provide a more specific treatment plan.
In addition to detailed lab work, there are all-natural supplements that have been shown to help improve these symptoms along with proper diet and exercise. Some of these supplements include Vitamin D, Berberine, and Ashwagandha.
On top of these things, there is also an app that is available to download. This app is called, “Dr. J Today”. This app connects you directly to our clinic and allows us to monitor your diet, supplements, activity, BMI, water weight, muscle mass, and more! This app also gives you a direct portal to message Dr.Jimenez or myself.
As stated before, our main goal is to help you decrease your symptoms before they turn into a full-blown diagnosis. One thing we want to surround our patients with is knowledge and a team atmosphere. With the right team, anything is possible and better health is more attainable than you think!
Having Type 1 Diabetes, I have experienced metabolic syndrome before. It is one of my least favorite feelings that exist. I want our patients to know that they do not have to feel that way and there are treatment plans that can help! I will help to create a personalized plan that is tailed to you, so success is the only option. – Kenna Vaughn, Senior Health Coach�
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Detailed lab testing is becoming more and more essential as integrative medicine is on the rise. Detailed lab testing goes more in-depth than the traditional blood levels usually taken. This allows physicians to understand more of the underlying issues that are causing the patients headaches, inflammation, pain, or overall discomfort.
There are multiple lab companies that utilize top of the line technology in order to obtain the best results for the patient. By running a detailed test, it allows more data to be collected and the physician to get a deeper look at what the patient might be lacking.
SpectraCell
One test that is extremely detailed and allows an abundance of information is the Micronutrient test from SpectraCell. Micronutrients are essential for the body to function properly. The body requires macronutrients and micronutrients. Macronutrients are those obtained through the diet, such as protein, carbohydrates, and fat. Micronutrients are vitamins and minerals that the body needs to achieve proper nutrition.
The Micronutrient test came from Dr. William Shive who was a biochemist that realized many serum (blood tests) do not adequately show the number of vitamins and minerals in an individual. In turn, the labs are not a true number of the patients health.
The Micronutrient test from Spectracell is unique because it is the only test on the market that obtains a history of 4-6 months from inside the cells. Thus, allowing practitioners and patients to see if their cells are truly healthy and what they are lacking in.
Who Should Be Tested?
Micronutrients are needed to perform almost all metabolic processes in the body. When these essential vitamins and minerals are lacking, the body is more prone to degenerative processes like arthritis.
Getting tested can provide an inside look at what is actually happening in your body. This can shine some light and possibly even explain some health symptoms you’ve been struggling with. Due to the fact that micronutrients are needed in the body and not having them does affect your health, getting tested could help prevent a compromised immune system.
Applications
As mentioned earlier, this test measures micronutrients, which are essential vitamins and minerals in the body. But, what else can this test really tell an individual besides the fact that they’re lacking in vitamin D?� This test can help provide measures for:
Diabetes
Alzheimer’s
Mood Disorders
Osteoporosis
Fatigue
Sports Performance Optimization
SpectraCell is all about giving their patients high-end results that lead to real solutions. By creating a test that captures the functional level and the actual capability of the nutrients present in the white blood cells, it allows physicians to see a patient’s metabolism from a different standpoint. Getting tested could be the first step towards a healthier future.
SpectraCell is an amazing company, which is why we use them! This test is very detailed and provides us with a great deal of information. The science behind this test not only allows our patients to feel better by getting on the correct vitamin regimen for their body but also by allowing us to treat patients on an individualized level without the guesswork. – Kenna Vaughn, Senior Health Coach
*All information for this article was found onSpectraCell.com and is properly cited below
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request.�
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine