Our diet can significantly affect inflammation in our bodies. Several foods can increase inflammation while other foods can reduce inflammation. According to healthcare professionals, a diet that is high in sugar may be associated with chronic inflammation. A systematic review in 2018 demonstrated that eating excess sugar can ultimately cause inflammation and a variety of other health issues, such as diabetes. Another 2014 research study showed that people who decreased their consumption of sugary or sweetened drinks had reduced inflammation. These research findings support the theory that eating excess sugar can cause chronic inflammation and various other diseases, including diabetes.
How Sugar Can Cause Inflammation
Healthcare professionals have tried to understand how eating excess sugar can cause chronic inflammation. Sugar triggers the production of free fatty acids in the liver. When the human body digests these free fatty acids, the resulting compounds can trigger inflammation. Different types of sugar may also cause more inflammation. By way of instance, one research study found that fructose can cause more inflammation than glucose. However, a systematic review found that fructose didn’t cause more inflammation than glucose. Therefore, further research studies are still required to determine which types of sugar may cause more inflammation. Symptoms associated with chronic inflammation can include:
pain and fatigue
sleeping problems or insomnia
anxiety, depression, and other mood disorders
digestive problems like acid reflux, constipation, and/or diarrhea
weight gain or obesity
constant infections
People with chronic inflammation may also have an increased risk of developing a variety of other health issues, including diabetes and dementia. Chronic inflammation in older adults may also be associated with an increased risk of death.
Health Issues Caused by Chronic Inflammation
Observational research studies in humans have associated diets with high added sugar and refined carbohydrates to the increased risk of developing a variety of health issues, including diabetes, IBD, liver disease, dementia, and arthritis.
Diabetes
Research studies showed a connection between the increased consumption of added sugar and type 2 diabetes. A large analysis that included over 38,000 participants found that simply consuming one serving of sweetened drinks or beverages on a regular basis was associated with an 18 percent increased risk of developing type 2 diabetes. Another research study found that increasing the consumption of high-fructose corn syrup was also associated with diabetes.
Other Diseases
Increased consumption of added sugar and refined carbohydrates has also been associated with the development of other diseases, such as arthritis, inflammatory bowel disease, liver disease, and dementia. Furthermore, excess fructose consumption has been associated with non-alcoholic fatty liver disease. Healthcare professionals believe this may be due to a combination of ongoing low-grade inflammation, increased gut permeability, and bacterial overgrowth in the gut.
Other Foods That Can Cause Inflammation
sugary foods like pastries, desserts, and chocolate
saturated fats from processed meats and dairy products
trans fats found in fast, fried, foods
vegetable and seed oils
refined carbohydrates
excessive alcohol
MSG in prepared Asian foods and deli meats
For information regarding how excess sugar can cause chronic inflammation and various other health issues like diabetes, please review this article:
Diet can affect inflammation in our bodies. Several foods can increase inflammation while other foods can reduce inflammation. A diet that is high in sugar may be associated with inflammation. Numerous research studies have demonstrated that eating excess sugar can ultimately cause chronic inflammation and various other diseases, including diabetes. Because sugar triggers the production of free fatty acids in the liver, it can also trigger inflammation. Excess sugar can cause chronic inflammation. Different types of sugar may also cause different amounts of inflammation. There are many symptoms associated with chronic inflammation, including pain, fatigue, obesity, anxiety, and depression, among others. Inflammation can lead to a variety of health issues, such as diabetes and arthritis. Although excess sugar is associated with chronic inflammation, other foods like saturated fats and refined carbohydrates can also cause health issues. In the following article, we discuss how sugar can cause inflammation and a variety of other health issues, such as diabetes, in the human body. – Dr. Alex Jimenez D.C., C.C.S.T. Insights
Sea Green Smoothie
Servings: 1 Cook time: 5-10 minutes
� 1/2 cup cantaloupe, cubed
� 1/2 banana
� 1 handful of kale or spinach
� 1 handful of Swiss chard
� 1/4 avocado
� 2 teaspoons spirulina powder
� 1 cup of water
� 3 or more ice cubes
Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Leafy Greens Hold the Key to Gut Health
A unique type of sugar found in leafy greens can help feed our beneficial gut bacteria. Sulfoquinovose (SQ) is the only known sugar molecule to be made up of sulfur, an extremely essential mineral in the human body. The human body uses sulfur to produce enzymes, proteins, and a variety of hormones as well as antibodies for our cells. A fast and easy way to get leafy greens into your diet is to toss a couple of handfuls of them into a delicious smoothie!
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas*& New Mexico*�
Curated by Dr. Alex Jimenez D.C., C.C.S.T.
References:
Spritzler, Franziska. �6 Foods That Cause Inflammation.� Healthline, Healthline Media, 12 Nov. 2019, www.healthline.com/nutrition/6-foods-that-cause-inflammation#1.
Caporuscio, Jessica. �Does Sugar Cause Inflammation? What the Research Says.� Medical News Today, MediLexicon International, 19 Sept. 2019, www.medicalnewstoday.com/articles/326386.
Brown, Mary Jane. �Does Sugar Cause Inflammation in the Body?� Healthline, Healthline Media, 12 Nov. 2017, www.healthline.com/nutrition/sugar-and-inflammation.
Reducing stress is important for emotional well being and physical health. Rheumatoid arthritis is a complex condition with no cure and can cause intense chronic pain. Stress only exacerbates the symptoms, affects pain perception, and weakens the body. Stress management is highly important for reducing pain. In a weakened state, an individual is more vulnerable to arthritis symptoms, like flare-ups, weakness, and fatigue.�Chiropractic can help.
There are non-surgical treatments for arthritis, like medications, physical, and massage therapy that address the physical nature of the condition. By eliminating stressful triggers and making healthy behavioral/lifestyle changes a better sense of well being can be achieved.
Different emotions can run rampant:
Confusion
Frustration
Anger
Sadness
Helplessness
And all of these feelings can generate intense stress on an individual. Chiropractic excels in wellness and is becoming more common for individuals to visit chiropractic clinics for treating a variety of different kinds of pain symptoms and conditions. Chiropractic adjustments provide countless benefits to those with arthritis. We�ll explore how chiropractic can help those with arthritis and give additional information along with suggestions on how to alleviate the pain.
What Chiropractic Does
A doctor of chiropractic is a health professional that focuses on wellness and optimal health instead of ailment/sickness symptoms. Their specialty aims at adjusting the spine to correct misalignments that could be pressing down on nerves and causing major disruption in the body. Regular chiropractic not only restores health throughout the body but helps alleviate back pain and any other symptoms associated with an out of alignment spine.
They also work in setting up exercise programs specific to the condition being treated along with the proper diet to utilize in assisting with the management of inflammation and pain.
Arthritis
Arthritis is inflammation in the body’s joints which results in pain, stiffness and limited range of movement. There are over 200 different varieties of arthritis. Generally associated with age, it can affect young people. It can strike pretty much any area of the body. Arthritis can cause damage to soft tissues and muscles.
Osteoarthritis also known as degenerative joint disease, is the most common type. It comes from repeated trauma to the joints and occurs more often in the elderly.
Other forms include:
Rheumatoid arthritis is the second common type in which the body�s immune system attacks the joint/s.
Psoriatic arthritis, an autoimmune form of arthritis.
Ankylosing spondylitis is a type of arthritis where the body attacks itself.
Septic arthritis is caused by a viral or bacterial infection of the joint/s.
Diagnosis
Diagnosing arthritis involves a thorough physical examination. Rheumatologists often need help with these cases, and so a medical work-up can be done and a chiropractor could be recommended. This includes X-rays or MRIs, urine, blood analysis, and physical examinations. Having the condition properly diagnosed will help to more effectively treat the symptoms.
Chiropractic
The most common treatment is medication, which takes down the inflammation, the swelling and reduces pain. Chiropractors can be of great help in managing arthritis. Medications work but as we’ve seen they can have long-term health risks like impaired healing, damage to the stomach lining and internal bleeding.
A chiropractor can reduce stress, and reliance on medications, all the while managing the pain and symptoms in a natural way. Chiropractic can:
Improve range of motion
Keeps the spine properly aligned
Improve endurance
Improve flexibility
Increase strength
Increase muscle tone
Develop a dietary and nutritional plan to reduce inflammation
Recommend an exercise regimen conducive to arthritis symptoms
According to the American Chiropractic Association, this is vital in managing arthritis symptoms.
Treatment
Understand that chiropractic cannot cure arthritis. They can help alleviate symptoms, slow the progression and help to reduce stress levels. They will use adjustments in combination with other treatments. This can include:
Hot and cold treatments
Ultrasound treatments
Massage
Electronic muscle stimulation
Physical rehabilitation
Magnet therapy
Reduce Stress
Exercise
Water aerobics or make walking around the park/neighborhood part of a daily routine, as it promotes a healthy mind by reducing stress and anxiety. Gentle exercises like aerobic exercise are perfect because it improves mobility and helps shed a few pounds taking pressure off the joints. Exercise creates endorphins, which reduces pain and uplifts the mood.
Support groups
With any type of painful condition, it’s easy to feel alone. Joining a support group can connect you with people who understand what’s going on and the emotions you’re experiencing. The community helps diminish the sense of isolation.
Relaxation therapy
This focuses on calming the body and mind by making a conscious effort to relax. Even for only a few moments, you might find this technique effective at controlling the stress response. Begin by focusing on one part of the body like the hands, feet, etc.
Concentrate until the area you’re focusing on is completely free of stress or tension. Then imagine weightlessness flow through the body. Close your eyes, lie down, turn off the lights, and think of something soothing. There are no strict guidelines for relaxation. Whatever puts you in a relaxed frame of mind is the way to do it.
Warm bath
Warm moist heat from a shower, bath, or steam room can decrease the secretion of stress hormones and raise levels of endorphins, as aforementioned the body’s natural pain killers.
Take time for yourself
When it comes to reducing stress, balance is key. Staying active, and regular rest/sleep is vital to successful treatment. A balance needs to be in everything you do. Therefore, make time for the things you want to do.
Results
Inflammatory diseases like arthritis have shown the best results are achieved from combating it from all angles. Working with a chiropractor and rheumatologist to combine treatments can make all the difference. A healthy diet and active exercise program will get you in the right direction toward a healthy active lifestyle. If you or a loved one are suffering from arthritis, don�t hesitate to call. We�re here to help in any way possible!
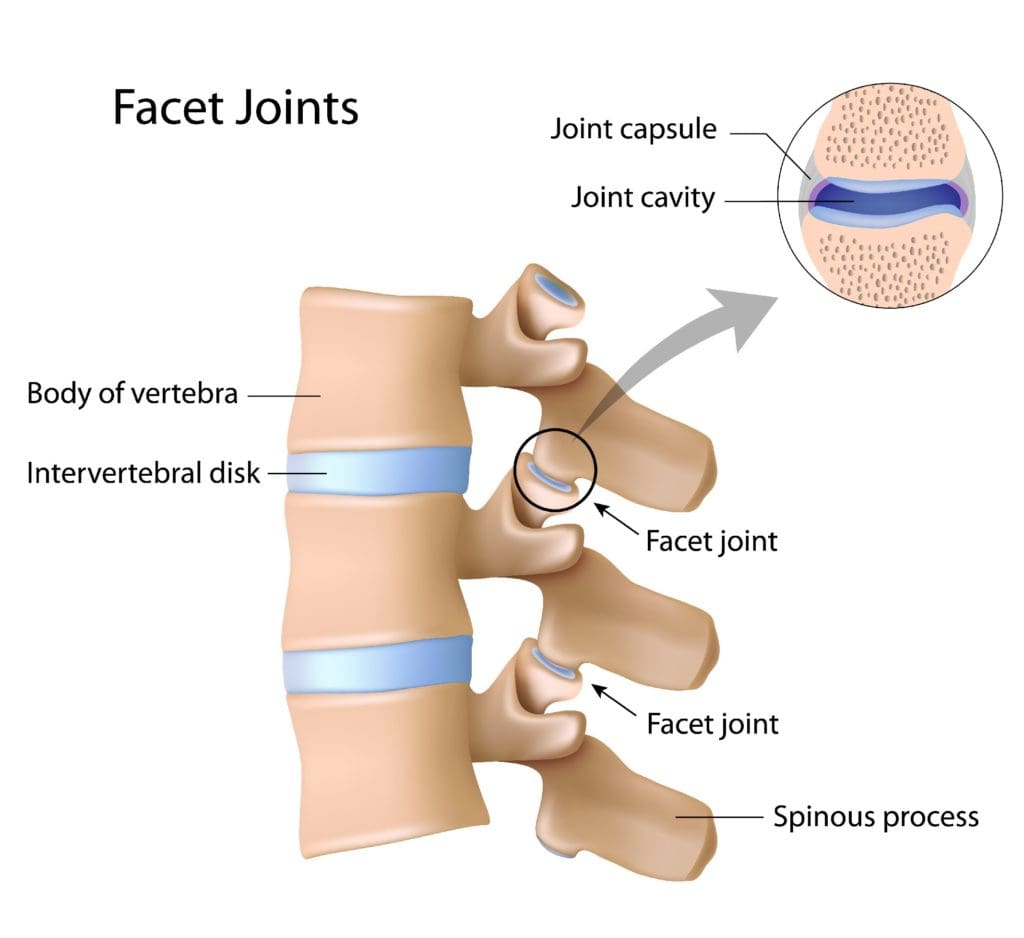
The most�common type of arthritis in children and adolescents is Juvenile idiopathic arthritis aka (JIA) a type of inflammatory arthritis that affects kids 16 years and younger. It is a rare condition, that affects around 1 in every 1,000 children. It can cause�joint�pain and stiffness throughout the body, especially the facet joints/spinal joints.
Types of Arthritis that Fall Under JIA
Juvenile Idiopathic arthritis was known as juvenile rheumatoid arthritis, but it is not a child/teenage version of adult rheumatoid arthritis. Juvenile Idiopathic arthritis falls into a group of several types of arthritis. When a doctor diagnoses JIA, they will determine the type.
To better understand how this arthritis affects the spine, it helps to know some of the terminology.
Enthesitis: Inflammation of the entheses is the area where tendons and ligaments connect to bone/s.
Spondyloarthritis: Arthritis that attacks the entheses of the spine. Ankylosing spondylitis is an example of spondyloarthritis.
The neck joints are the most common to be attacked by JIA. Whereas, spondyloarthritis causes pain and stiffness in the low back.
Typical Symptoms
Juvenile idiopathic arthritis happens in children aged 16 years and younger. Symptoms include:
Joint pain
Swelling
Stiffness
Tenderness
Mild heat or a warmness that has been present for at least 6 weeks.
Other symptoms can include muscles and soft tissues becoming tight, erosion of the bone,�joint misalignment, and abnormal growth patterns.
Diagnosis Can Be A Challenge
Diagnosis is not always straightforward, and there are criteria for diagnosing juvenile idiopathic arthritis. The doctor will perform a physical exam and order tests. They will monitor the child�s symptoms for at least 6 weeks initially, and then for 6 months after the onset of the disease. During this time, figuring the number of joints involved helps determine the diagnosis. As joint involvement can vary by the type of arthritis, and symptoms can and do change regularly.
This arthritis attacks the joints of the spine, specifically in the neck. However, with certain types of spondyloarthropathy, the lower back can become the target.
Diagnosing arthritis involves a complete and thorough examination. If a chiropractor has been brought in to help with the case, a medical work-up by a rheumatologist could be recommended. This includes radiology/X-rays or an MRI, urine, blood analysis and physical examinations.
Treatment
A doctor may recommend a multi-disciplinary approach to treat JIA. They may prescribe various types of therapies/treatments focused on stopping the disease’s progression. The treatment plan will include teaching healthy habits to prevent future back pain.
Medication/s
Treatment usually starts with nonsteroidal anti-inflammatory’s. A doctor can also prescribe a corticosteroid to control the inflammation. Most respond well to anti-inflammatory medication, however, these medicines do not treat the underlying disease or the root cause.
Inflammatory arthritis and its progression can be controlled with certain medications. There are disease-modifying antirheumatic medications that can slow the disease�s progression. There are also TNF-blocking medications that can help block a specific protein known as tumor necrosis factor that causes inflammation. Etanercept known on the market as Enbrel and adalimumab aka Humira are examples of TNF-blockers that can prevent the disease from progressing.
Chiropractic
Understand that chiropractic medicine cannot cure arthritis, but it can help alleviate the symptoms and slow the progression. They will use spinal adjustments in conjunction with other treatments. These can include:
Hot and cold treatments
Ultrasound
Massage
Electronic muscle stimulation
Magnet therapy
Physical rehabilitation
Physical Therapy Exercise
Focuses on:
Proper posture
Joint mobility
Deep breathing
Exercises
Healthy lifestyle education
Patients can develop a forward posture that can lead to a hunched back and neck pain. Postural training and back extension exercises are helpful. Stretching and range of motion exercises keep the facet and rib joints functioning and mobile. Deep breathing expands the chest which expands the rib joints and aids lung function. Depending on the type and severity, a doctor might try other approaches like spine surgery.
Optimal Results
If you or someone has been diagnosed with juvenile idiopathic arthritis in the spine,�learn as much as possible about the disease and the ways to combat it. Being informed about this or any disease encourages empowerment and engagement throughout the treatment process.
The best results are achieved by attacking it from all angles. Working with a chiropractor and rheumatologist in combination. A chiropractor will train the individual on how to maintain a healthy diet and maintain an active exercise program to help with movement. This is geared toward a healthy outcome.
Rheumatoid arthritis (RA) is a condition that causes considerable discomfort if diagnosed with this autoimmune disease. This is when your immune system starts attacking your joints, instead of foreign invaders, which then causes inflammation.
The worse the RA, the more severe the symptoms become. If things get bad enough you can lose mobility altogether, which is why it is so important to get treatment. Fortunately, chiropractic is excellent for reducing inflammation and improving mobility. Chiropractic treatment can do a lot to ease your pain and get you back to moving the way you are supposed to.
RA and Chiropractic
Chiropractic is an effective RA treatment for a number of reasons. Chiropractic treatment:
Individual Treatment
The image many people have of a chiropractic adjustment is one of popping backs and hard, jerking motions. While adjustments can certainly include these things, they do not have to. According to the Arthritis Foundation, chiropractors have more than 150 techniques they can use to adjust your body.
They strive to give treatments specific to the needs of each patient, which means adjusting the body as gently as necessary to produce the desired result. If your joints are swollen and painful the chiropractor will carefully work to realign the joint�which reduces inflammation and improves movement�while minimizing any pain or discomfort you feel from the adjustment.
Reduced Inflammation
With RA typically the worst symptoms are the result of inflammation. Chiropractic treatment may not be able to change the way your immune system is malfunctioning, but it can do a lot to help the painful areas become less inflamed.
The treatment you get from your chiropractor will ensure that your joints are moving as properly as possible given your condition. By putting the body back in alignment, chiropractic improves the way the nervous system operates and lessens inflammation.
Improved Mobility
One of the most difficult things for many with RA is the loss of mobility that comes when their joints swell. When the pain becomes more substantial it is normal for RA sufferers to avoid movement because it hurts.
But it is important to remember that movement, even when it hurts, is necessary to maintain joint mobility. The longer you avoid moving a joint the more likely it is that you will lose function.
A useful aspect of chiropractic is that you can get help with moving, so you are not all alone with the daunting prospect of moving your joints so they start working better. Your chiropractor is your partner in movement, helping to guide your body so that it moves as well as possible. Results are different for everyone based on their unique situations, but you can be sure that chiropractic will serve as a powerful tool to keep your body working as well as possible.
Hand Deformed From Rheumatoid Arthritis
Drug-Free and Non-invasive
In chiropractic, the focus is to help the body heal itself, which means avoiding surgery and prescription medications as much as possible. Surgery and medication often have unwanted side-effects�sometimes worse than the problem they were intended to solve. With chiropractic negative side-effects are unlikely. You can get a lot of relief from gentle, effective treatments that will not make you feel worse than when you started.
Please contact our office to schedule an appointment. We look forward to speaking with you!
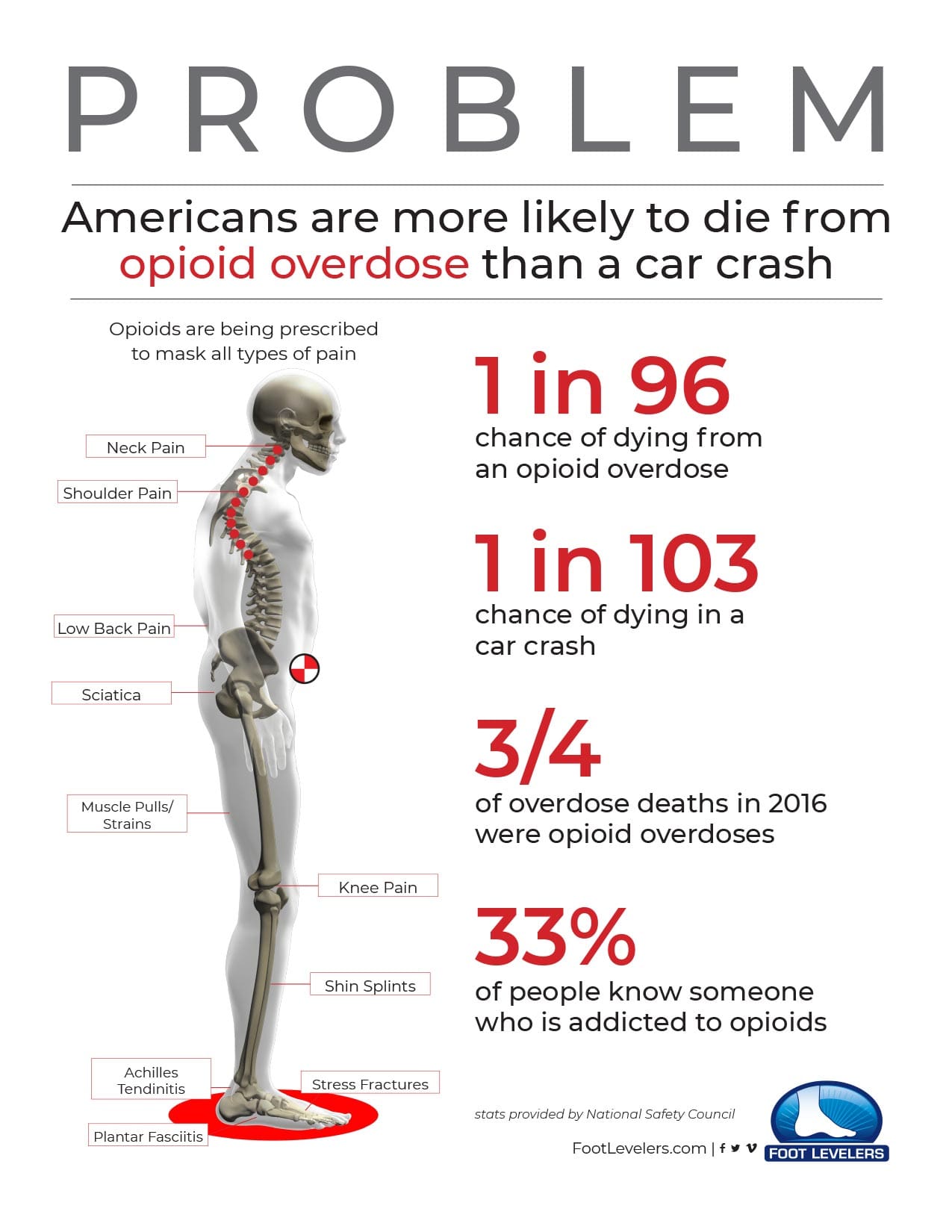
Opioid Addiction Alternative
Opioids (such as hydrocodone, oxycodone, codeine, and morphine) mask symptoms and do nothing to address the cause of pain.
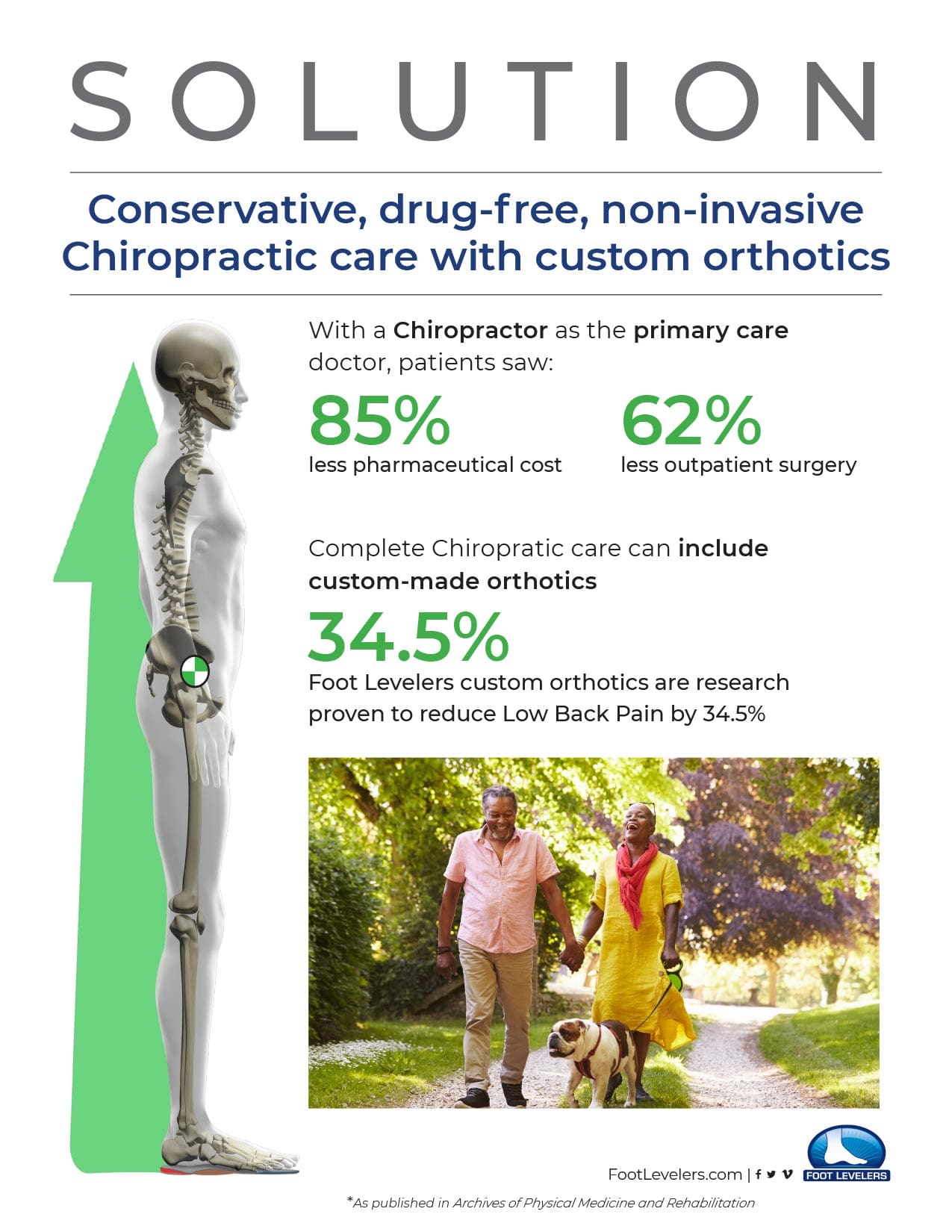
There is an opioid crisis raging.� A sensible and safe alternative to opioids: Custom-made orthotics help relieve low back pain as well as hip and neck pain by removing imbalances in the musculoskeletal system, which originate in the feet.
Before considering taking an opioid for pain control, give Chiropractic care and foot orthotics a try. The combination of Chiropractic and orthotics is proven in clinical studies.
In 2015, about 2 million Americans had substance abuse disorders related to opioid medications.
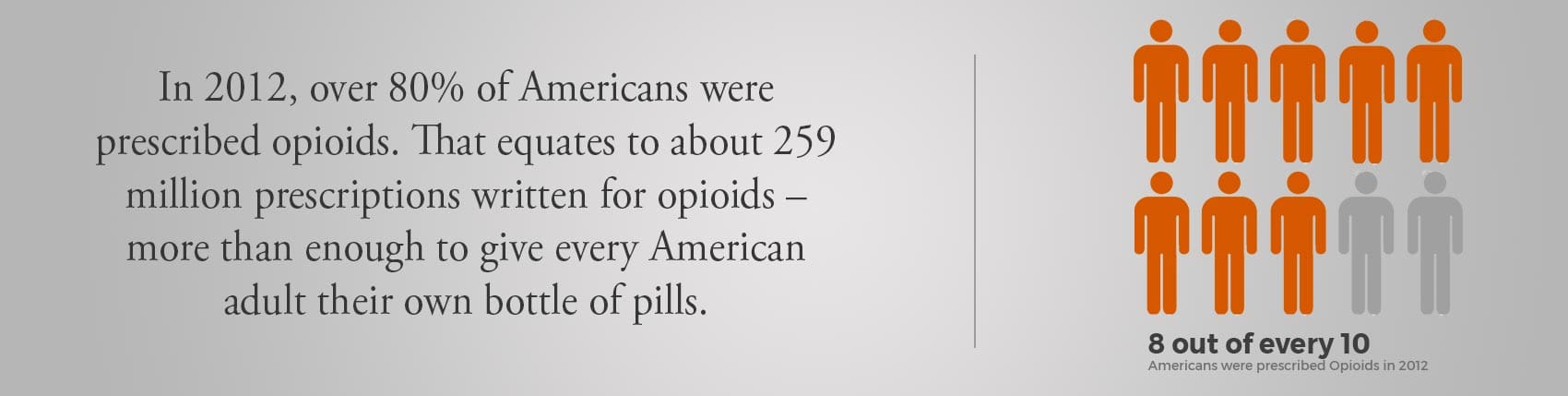
In 2012, 80 out of 100 Americans were prescribed opioids. That’s about 259 million prescriptions � more than enough to give every American adult their own bottle of pills.
Less Pain & More Comfort
Custom orthotics help more than your feet! Stabilizing orthotics bring health and healing to the whole body by balancing the musculoskeletal system.
El Paso Back Clinic
Here are some videos that discuss how chiropractic care can help with arthritis, fibromyalgia, seniors and whole body wellness.
NCBI Resources
Here are some articles to check out for extended information on arthropathies.
About 1.5 million people in the United States have rheumatoid arthritis. Rheumatoid arthritis, or RA, is a chronic, autoimmune disease characterized by pain and inflammation of the joints. With RA, the immune system, which protects our well-being by attacking foreign substances like bacteria and viruses, mistakenly attacks the joints. Rheumatoid arthritis most commonly affects the joints of the hands, feet, wrists, elbows, knees and ankles. Many healthcare professionals recommend early diagnosis and treatment of RA.
Abstract
Rheumatoid arthritis is the most commonly diagnosed systemic inflammatory arthritis. Women, smokers, and those with a family history of the disease are most often affected. Criteria for diagnosis include having at least one joint with definite swelling that is not explained by another disease. The likelihood of a rheumatoid arthritis diagnosis increases with the number of small joints involved. In a patient with inflammatory arthritis, the presence of a rheumatoid factor or anti-citrullinated protein antibody, or elevated C-reactive protein level or erythrocyte sedimentation rate suggests a diagnosis of rheumatoid arthritis. Initial laboratory evaluation should also include complete blood count with dif- ferential and assessment of renal and hepatic function. Patients taking biologic agents should be tested for hepatitis B, hepatitis C, and tuberculosis. Earlier diagnosis of rheumatoid arthritis allows for earlier treatment with disease-modifying antirheumatic agents. Combinations of medications are often used to control the disease. Methotrexate is typically the first-line drug for rheumatoid arthritis. Biologic agents, such as tumor necrosis factor inhibitors, are generally considered second-line agents or can be added for dual therapy. The goals of treatment include minimiza- tion of joint pain and swelling, prevention of radiographic damage and visible deformity, and continuation of work and personal activities. Joint replacement is indicated for patients with severe joint damage whose symptoms are poorly controlled by medical management. (Am Fam Physician. 2011;84(11):1245-1252. Copyright � 2011 American Academy of Family Physicians.)
Rheumatoid arthritis (RA) is the most common inflammatory arthritis, with a lifetime prevalence of up to 1 percent worldwide.1 Onset can occur at any age, but peaks between 30 and 50 years.2 Disability is common and significant. In a large U.S. cohort, 35 percent of patients with RA had work disability after 10 years.3
Etiology and Pathophysiology
Like many autoimmune diseases, the etiology of RA is multifactorial. Genetic susceptibility is evident in familial clustering and monozygotic twin studies, with 50 percent of RA risk attributable to genetic factors.4 Genetic associations for RA include human leukocyte antigen-DR45 and -DRB1, and a variety of alleles called the shared epitope.6,7 Genome-wide association studies have identified additional genetic signatures that increase the risk of RA and other autoimmune diseases, including STAT4 gene and CD40 locus.5 Smoking is the major environmental trigger for RA, especially in those with a genetic predisposition.8 Although infections may unmask an autoimmune response, no particular pathogen has been proven to cause RA.9
RA is characterized by inflammatory pathways that lead to proliferation of synovial cells in joints. Subsequent pannus formation may lead to underlying cartilage destruction and bony erosions. Overproduction of pro-inflammatory cytokines, including tumor necrosis factor (TNF) and interleukin-6, drives the destructive process.10
Risk Factors
Older age, a family history of the disease, and female sex are associated with increased risk of RA, although the sex differential is less prominent in older patients.1 Both current and prior cigarette smoking increases the risk of RA (relative risk [RR] = 1.4, up to 2.2 for more than 40-pack-year smokers).11
Pregnancy often causes RA remission, likely because of immunologic tolerance.12 Parity may have long-lasting impact; RA is less likely to be diagnosed in parous women than in nulliparous women (RR = 0.61).13,14 Breastfeeding decreases the risk of RA (RR = 0.5 in women who breastfeed for at least 24 months), whereas early menarche�(RR = 1.3 for those with menarche at 10 years of age or younger) and very irregular menstrual periods (RR = 1.5) increase risk.14 Use of oral contraceptive pills or vitamin E does not affect RA risk.15
Diagnosis
Typical Presentation
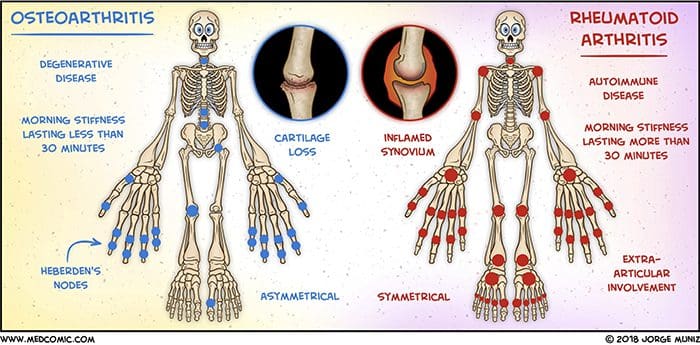
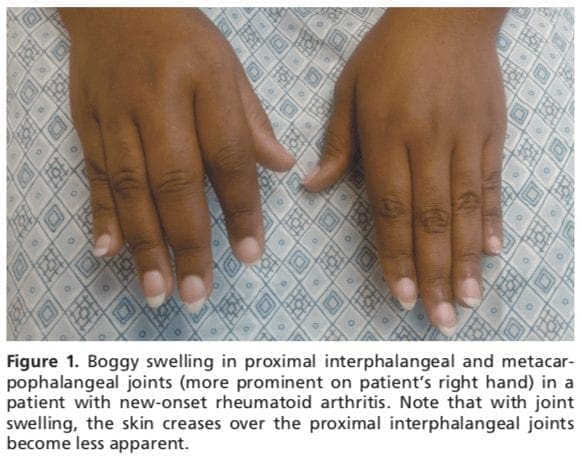
Patients with RA typically present with pain and stiffness in multiple joints. The wrists, proximal interphalangeal joints, and metacarpophalangeal joints are most commonly involved. Morning stiffness lasting more than one hour suggests an inflammatory etiology. Boggy swelling due to synovitis may be visible (Figure 1), or subtle synovial thickening may be palpable on joint examination. Patients may also present with more indolent arthralgias before the onset of clinically apparent joint swelling. Systemic symptoms of fatigue, weight loss, and low-grade fever may occur with active disease.
Diagnostic Criteria
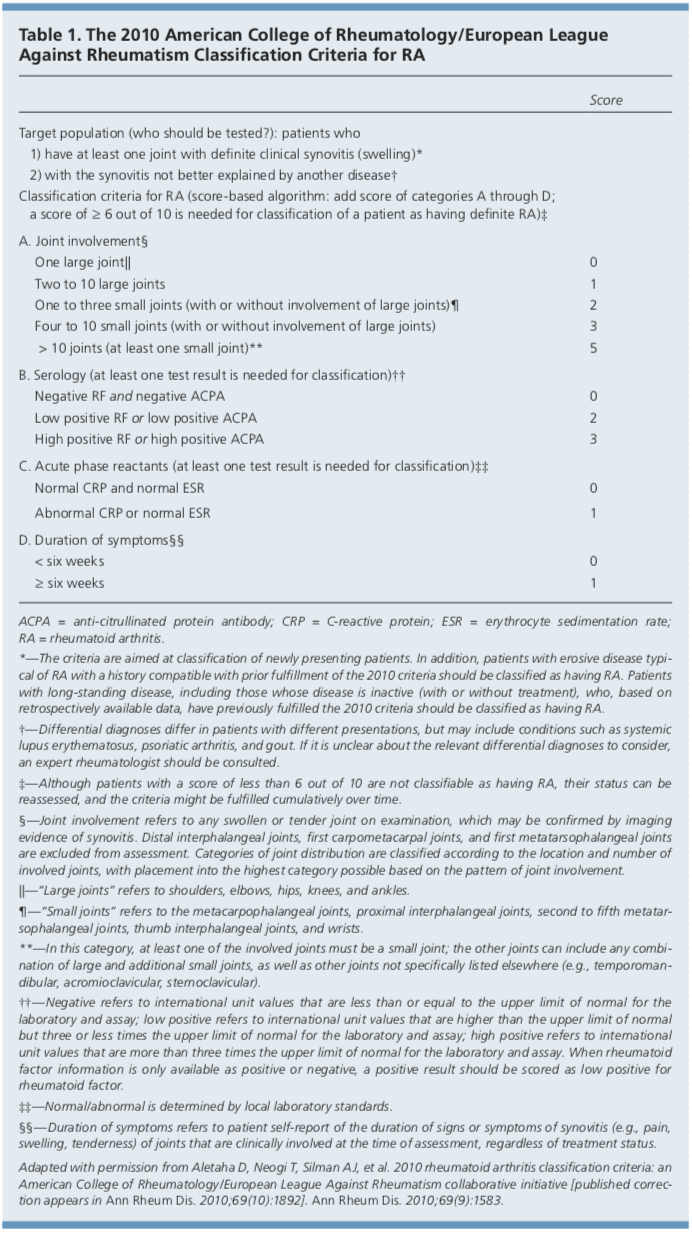
In 2010, the American College of Rheumatology and European League Against Rheumatism collaborated to create new classification criteria for RA (Table 1).16 The new criteria are an effort to diagnose RA earlier in patients who may not meet the 1987 American College of Rheumatology classification criteria. The 2010 criteria do not include presence of rheumatoid nodules or radiographic erosive changes, both of which are less likely in early RA. Symmetric arthri- tis is also not required in the 2010 criteria, allowing for early asymmetric presentation.
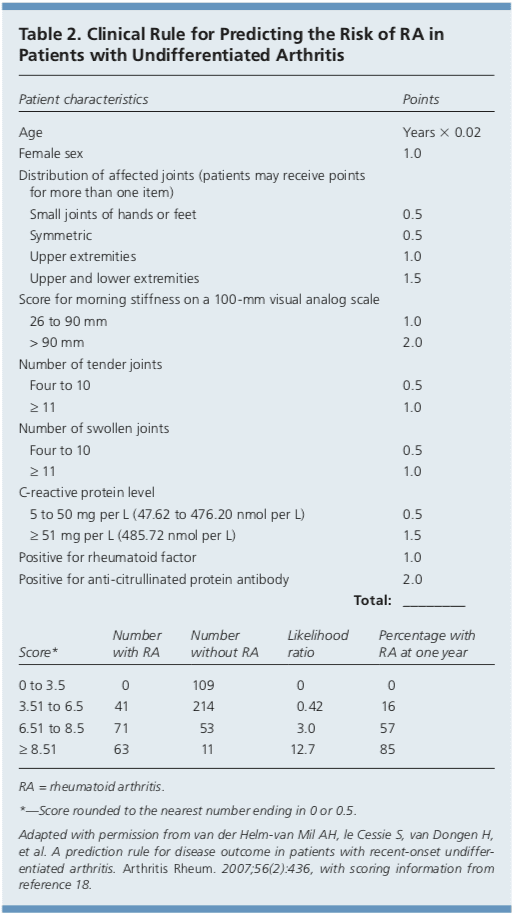
In addition, Dutch researchers have developed and validated a clinical prediction rule for RA (Table 2).17,18 The purpose of this rule is to help identify patients with undifferentiated arthritis that is most likely to progress to RA, and to guide follow-up and referral.
Diagnostic Tests
Autoimmune diseases such as RA are often characterized by the presence of autoanti- bodies. Rheumatoid factor is not specific for RA and may be present in patients with other diseases, such as hepatitis C, and in healthy older persons. Anti-citrullinated protein antibody is more specific for RA and may play a role in disease pathogenesis.6 Approxi- mately 50 to 80 percent of persons with RA have rheumatoid factor, anti-citrullinated protein antibody, or both.10 Patients with RA may have a positive antinuclear antibody test result, and the test is of prognostic impor- tance in juvenile forms of this disease.19 C-reactive protein levels and erythrocyte sedimentation rate are often increased with active RA, and these acute phase reactants are part of the new RA classification criteria.16 C-reactive protein levels and erythrocyte sedimentation rate may also be used to follow disease activity and response to medication.
Baseline complete blood count with differential and assessment of renal and hepatic function are helpful because the results may influence treatment options (e.g., a patient with renal insufficiency or significant thrombocytopenia likely would not be prescribed a nonsteroidal anti-inflammatory drug [NSAID]). Mild anemia of chronic disease occurs in 33 to 60 percent of all patients with RA,20 although gastrointestinal blood loss should also be considered in patients taking corticosteroids or NSAIDs. Methotrexate is contraindicated in patients with hepatic disease, such as hepatitis C, and in patients with significant renal impairment.21 Biologic therapy, such as a TNF inhibitor, requires a negative tuberculin test or treatment for latent tuberculosis. Hepatitis B reactivation can also occur with TNF inhibitor use.22 Radiography of hands and feet should be performed to evaluate for characteristic periarticular erosive changes,�which may be indicative of a more aggressive RA subtype.10
Differential Diagnosis
Skin findings suggest systemic lupus erythematosus, systemic sclerosis, or psoriatic arthritis. Polymyalgia rheumatica should be considered in an older patient with symptoms primarily in the shoulder and hip, and the patient should be asked questions related to associated temporal arteritis.
Chest radiography is helpful to evaluate for sarcoidosis as an etiology of arthritis.�Patients with inflammatory back symptoms, a history of inflammatory bowel disease, or inflammatory eye disease may have spondyloarthropathy. Persons with less than six weeks of symptoms may have a viral process, such as parvovirus. Recurrent self-limited episodes of acute joint swelling suggest crystal arthropathy, and arthrocentesis should be performed to evaluate for monosodium urate monohydrate or calcium pyrophosphate dihydrate crystals. The presence of numerous myofascial trigger points and somatic symptoms may suggest fibromyalgia, which can coexist with RA. To help guide diagnosis and determine treatment strategy, patients with inflammatory arthritis should be promptly referred to a rheumatology subspecialist.16,17
Rheumatoid arthritis, or RA, is the most common type of arthritis. RA is an autoimmune disease, caused when the immune system, the human body’s defense system, attacks its own cells and tissues, particularly the joints. Rheumatoid arthritis is frequently identified by symptoms of pain and inflammation, often affecting the small joints of the hands, wrists and feet. According to many healthcare professionals, early diagnosis and treatment of RA is essential to prevent further joint damage and decrease painful symptoms. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Treatment
After RA has been diagnosed and an initial evaluation performed, treatment should begin. Recent guidelines have addressed the management of RA,21,22 but patient preference also plays an important role. There are special considerations for women of childbearing age because many medications have deleterious effects on pregnancy. Goals of therapy include minimizing joint pain and swelling, preventing deformity (such as ulnar deviation) and radiographic damage (such as erosions), maintaining quality of life (personal and work), and controlling extra-articular manifestations. Disease-modifying antirheumatic drugs (DMARDs) are the mainstay of RA therapy.
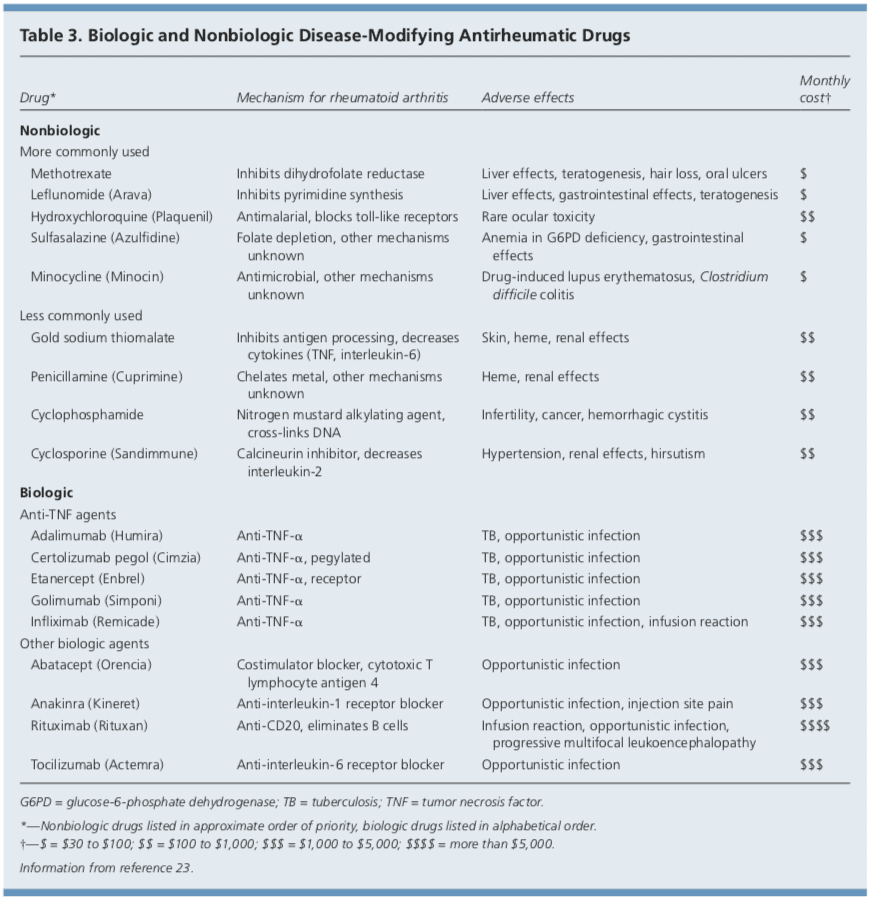
DMARDs
DMARDs can be biologic or nonbiologic (Table 3).23 Biologic agents include monoclonal antibodies and recombinant receptors to block cytokines that promote the inflammatory cascade responsible for RA symptoms. Methotrexate is recommended as the first- line treatment in patients with active RA, unless contraindicated or not tolerated.21 Leflunomide (Arava) may be used as an alternative to methotrexate, although gastrointestinal adverse effects are more common. Sulfasalazine (Azulfidine) or hydroxychloroquine (Plaquenil) pro-inflammatory as monotherapy in patients with low disease�activity or without poor prognostic features (e.g., seronegative, non-erosive RA).21,22
Combination therapy with two or more DMARDs is more effective than monotherapy; however, adverse effects may also be greater.24 If RA is not well controlled with a nonbiologic DMARD, a biologic DMARD should be initiated.21,22 TNF inhibitors are the first-line biologic therapy and are the most studied of these agents. If TNF inhibitors are ineffective, additional biologic therapies can be considered. Simultaneous use of more than one biologic therapy (e.g., adalimumab [Humira] with abatacept [Orencia]) is not�recommended because of an unacceptable rate of adverse effects.21
NSAIDs and Corticosteroids
Drug therapy for RA may involve NSAIDs and oral, intramuscular, or intra-articular corticosteroids for controlling pain and inflammation. Ideally, NSAIDs and corticosteroids are used only for short-term management. DMARDs are the preferred therapy.21,22
Complementary Therapies
Dietary interventions, including vegetarian and Mediterranean diets, have been�studied in the treatment of RA without convincing evidence of benefit.25,26 Despite some favorable outcomes, there is a lack of evidence for the effectiveness of acupuncture in placebo-controlled trials of patients with RA.27,28 In addition, thermotherapy and therapeutic ultrasound for RA have not been studied adequately.29,30 A Cochrane review of herbal treatments for RA concluded that gamma-linolenic acid (from evening primrose or black currant seed oil) and Tripterygium wilfordii (thunder god vine) have potential benefits.31 It is important to inform patients that serious adverse effects have been reported with use of herbal therapy.31
Exercise and Physical Therapy
Results of randomized controlled trials sup- port physical exercise to improve quality of life and muscle strength in patients with RA.32,33 Exercise training programs have not been shown to have deleterious effects on RA disease activity, pain scores, or radiographic joint damage.34 Tai chi has been shown to improve ankle range of motion in persons with RA, although randomized trials are limited.35 Randomized controlled trials of Iyengar yoga in young adults with RA are underway.36
Duration of Treatment
Remission is obtainable in 10 to 50 percent of patients with RA, depending on how remission is defined and the intensity of therapy.10 Remission is more likely in males, nonsmokers, persons younger than 40 years, and in those with late-onset disease (patients older than 65 years), with shorter duration of disease, with milder disease activity, without elevated acute phase reactants, and without positive rheumatoid factor or anti-citrullinated protein antibody findings.37
After the disease is controlled, medication dosages may be cautiously decreased to the minimum amount necessary. Patients will require frequent monitoring to ensure stable symptoms, and prompt increase in medication is recommended with disease flare-ups.22
Joint Replacement
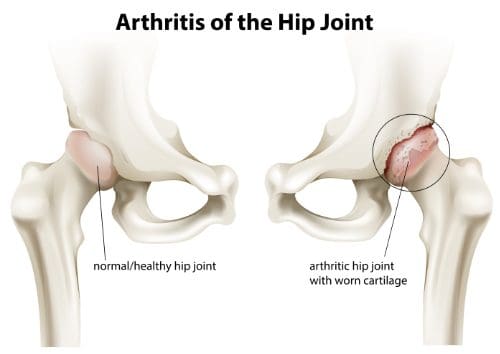
Joint replacement is indicated when there is severe joint damage and unsatisfactory control of symptoms with medical management. Long-term outcomes are support, with only 4 to 13 percent of large joint replacements requiring revision within 10 years.38 The hip and knee are the most commonly replaced joints.
Long-Term Monitoring
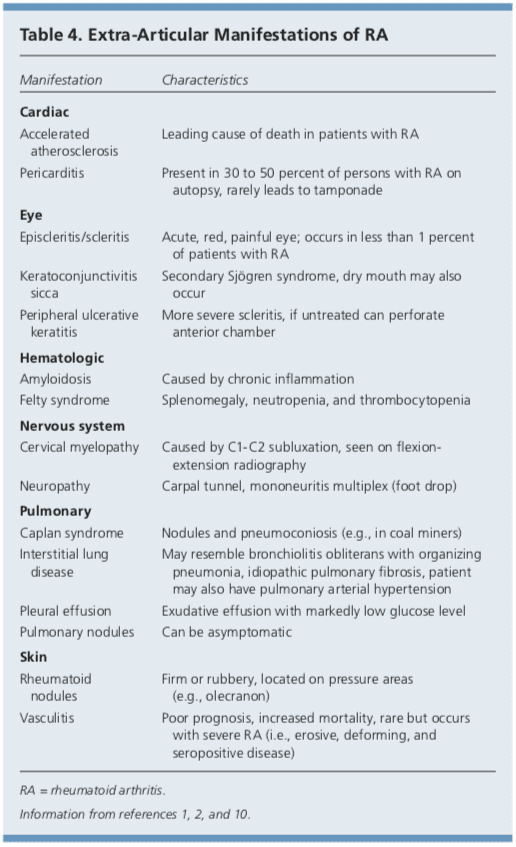
Although RA is considered a disease of the joints, it is also a systemic disease capable of involving multiple organ systems. Extra-articular manifestations of RA are included in Table 4.1,2,10
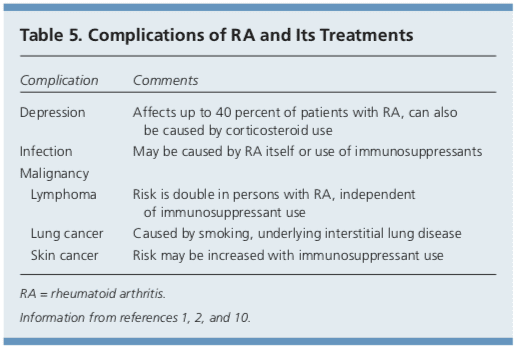
Patients with RA have a twofold increased risk of lymphoma, which is thought to be caused by the underlying inflammatory�process, and not a consequence of medical treatment.39 Patients with RA are also at an increased risk of coronary artery disease, and physicians should work with patients to modify risk factors, such as smoking, high blood pressure, and high cholesterol.40,41 Class III or IV congestive heart failure (CHF) is a contraindication for using TNF inhibitors, which can worsen CHF outcomes.21 In patients with RA and malignancy, caution is needed with continued use of DMARDs, especially TNF inhibitors. Biologic DMARDs, methotrexate, and leflunomide should not be initiated in patients with active herpes zoster, significant fungal infection, or bacterial infection requiring antibiotics.21 Complications of RA and its treatments are listed in Table 5.1,2,10
Prognosis
Patients with RA live three to 12 years less than the general population.40 Increased mortality in these patients is mainly due to accelerated cardiovascular disease, especially in those with high disease activity and chronic inflammation. The relatively new biologic therapies may reverse progression of atherosclerosis and extend life in those with RA.41
Data Sources: A PubMed search was completed in Clinical Queries using the key terms rheumatoid arthritis, extra-articular manifestations, and disease-modifying antirheumatic agents. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. Also searched were the Agency for Healthcare Research and Quality evidence reports, Clinical Evidence, the Cochrane database, Essential Evidence, and UpToDate. Search date: September 20, 2010.
Author disclosure: No relevant financial affiliations to disclose.
In conclusion, rheumatoid arthritis is a chronic, autoimmune disease which causes painful symptoms, such as pain and discomfort, inflammation and swelling of the joints, among others. The joint damage characterized as RA is symmetrical, meaning it generally affects both sides of the body. Early�diagnosis is essential for treatment of RA. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Etiology and pathogenesis of rheumatoid arthritis. In: Firestein GS, Kelley WN, eds. Kelley�s Textbook of Rheu- matology. 8th ed. Philadelphia, Pa.: Saunders/Elsevier; 2009:1035-1086. 2. Bathon J, Tehlirian C. Rheumatoid arthritis clinical and laboratory manifestations. In: Klippel JH, Stone JH, Crofford LJ, et al., eds. Primer on the Rheumatic Dis- eases. 13th ed. New York, NY: Springer; 2008:114-121. 3. Allaire S, Wolfe F, Niu J, et al. Current risk factors for work disability associated with rheumatoid arthritis. Arthritis Rheum. 2009;61(3):321-328. 4. MacGregor AJ, Snieder H, Rigby AS, et al. Characteriz- ing the quantitative genetic contribution to rheumatoid arthritis using data from twins. Arthritis Rheum. 2000; 43(1):30-37. 5. Orozco G, Barton A. Update on the genetic risk fac- tors for rheumatoid arthritis. Expert Rev Clin Immunol. 2010;6(1):61-75. 6. Balsa A, Cabezo?n A, Orozco G, et al. Influence of HLA DRB1 alleles in the susceptibility of rheumatoid arthritis and the regulation of antibodies against citrullinated proteins and rheumatoid factor. Arthritis Res Ther. 2010;12(2):R62. 7. McClure A, Lunt M, Eyre S, et al. Investigating the via- bility of genetic screening/testing for RA susceptibility using combinations of five confirmed risk loci. Rheuma- tology (Oxford). 2009;48(11):1369-1374. 8. Bang SY, Lee KH, Cho SK, et al. Smoking increases rheu- matoid arthritis susceptibility in individuals carrying the HLA-DRB1 shared epitope, regardless of rheumatoid factor or anti-cyclic citrullinated peptide antibody sta- tus. Arthritis Rheum. 2010;62(2):369-377. 9. Wilder RL, Crofford LJ. Do infectious agents cause rheu- matoid arthritis? Clin Orthop Relat Res. 1991;(265): 36-41. 10. Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376(9746):1094-1108. 11. Costenbader KH, Feskanich D, Mandl LA, et al. Smoking intensity, duration, and cessation, and the risk of rheu- matoid arthritis in women. Am J Med. 2006;119(6): 503.e1-e9. 12. Kaaja RJ, Greer IA. Manifestations of chronic disease during pregnancy. JAMA. 2005;294(21):2751-2757. 13. Guthrie KA, Dugowson CE, Voigt LF, et al. Does preg- nancy provide vaccine-like protection against rheuma- toid arthritis? Arthritis Rheum. 2010;62(7):1842-1848. 14. Karlson EW, Mandl LA, Hankinson SE, et al. Do breast- feeding and other reproductive factors influence future risk of rheumatoid arthritis? Results from the Nurses� Health Study. Arthritis Rheum. 2004;50(11):3458-3467. 15. Karlson EW, Shadick NA, Cook NR, et al. Vitamin E in the primary prevention of rheumatoid arthritis: the Women�s Health Study. Arthritis Rheum. 2008;59(11): 1589-1595. 16. Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative [published correction appears in Ann Rheum Dis. 2010;69(10):1892]. Ann Rheum Dis. 2010;69(9):1580-1588. 17. van der Helm-van Mil AH, le Cessie S, van Dongen H, et al. A prediction rule for disease outcome in patients with recent-onset undifferentiated arthritis. Arthritis Rheum. 2007;56(2):433-440. 18. Mochan E, Ebell MH. Predicting rheumatoid arthritis risk in adults with undifferentiated arthritis. Am Fam Physi- cian. 2008;77(10):1451-1453. 19. Ravelli A, Felici E, Magni-Manzoni S, et al. Patients with antinuclear antibody-positive juvenile idiopathic arthri- tis constitute a homogeneous subgroup irrespective of the course of joint disease. Arthritis Rheum. 2005; 52(3):826-832. 20. Wilson A, Yu HT, Goodnough LT, et al. Prevalence and outcomes of anemia in rheumatoid arthritis. Am J Med. 2004;116(suppl 7A):50S-57S. 21. Saag KG, Teng GG, Patkar NM, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheu- matic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59(6):762-784. 22. Deighton C, O�Mahony R, Tosh J, et al.; Guideline Devel- opment Group. Management of rheumatoid arthritis: summary of NICE guidance. BMJ. 2009;338:b702. 23. AHRQ. Choosing medications for rheumatoid arthritis. April 9, 2008. http://www.effectivehealthcare.ahrq.gov/ ehc/products/14/85/RheumArthritisClinicianGuide.pdf. Accessed June 23, 2011. 24. Choy EH, Smith C, Dore? CJ, et al. A meta-analysis of the efficacy and toxicity of combining disease-modify- ing anti-rheumatic drugs in rheumatoid arthritis based on patient withdrawal. Rheumatology (Oxford). 2005; 4 4 (11) :1414 -1421. 25. Smedslund G, Byfuglien MG, Olsen SU, et al. Effective- ness and safety of dietary interventions for rheumatoid arthritis. J Am Diet Assoc. 2010;110(5):727-735. 26. Hagen KB, Byfuglien MG, Falzon L, et al. Dietary inter- ventions for rheumatoid arthritis. Cochrane Database Syst Rev. 2009;21(1):CD006400. 27. Wang C, de Pablo P, Chen X, et al. Acupuncture for pain relief in patients with rheumatoid arthritis: a systematic review. Arthritis Rheum. 2008;59(9):1249-1256. 28. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484. 29. Robinson V, Brosseau L, Casimiro L, et al. Thermother- apy for treating rheumatoid arthritis. Cochrane Data- base Syst Rev. 2002;2(2):CD002826. 30. Casimiro L, Brosseau L, Robinson V, et al. Therapeutic ultrasound for the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. 2002;3(3):CD003787. 31. Cameron M, Gagnier JJ, Chrubasik S. Herbal therapy for treating rheumatoid arthritis. Cochrane Database Syst Rev. 2011;(2):CD002948. 32. Brodin N, Eurenius E, Jensen I, et al. Coaching patients with early rheumatoid arthritis to healthy physical activ- ity. Arthritis Rheum. 2008;59(3):325-331. 33. Baillet A, Payraud E, Niderprim VA, et al. A dynamic exercise programme to improve patients� disability in rheumatoid arthritis: a prospective randomized con- trolled trial. Rheumatology (Oxford). 2009;48(4): 410-415. 34. Hurkmans E, van der Giesen FJ, Vliet Vlieland TP, et al. Dynamic Exercise programs (aerobic capacity and/or mus- cle strength training) in patients with rheumatoid arthri- tis. Cochrane Database Syst Rev. 2009;(4):CD006853. 35. Han A, Robinson V, Judd M, et al. Tai chi for treat- ing rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD004849. 36. Evans S, Cousins L, Tsao JC, et al. A randomized con- trolled trial examining Iyengar yoga for young adults with rheumatoid arthritis. Trials. 2011;12:19. 37. Katchamart W, Johnson S, Lin HJ, et al. Predictors for remis- sion in rheumatoid arthritis patients: a systematic review. Arthritis Care Res (Hoboken). 2010;62(8):1128-1143. 38. Wolfe F, Zwillich SH. The long-term outcomes of rheu- matoid arthritis: a 23-year prospective, longitudinal study of total joint replacement and its predictors in 1,600 patients with rheumatoid arthritis. Arthritis Rheum. 1998;41(6):1072-1082. 39. Baecklund E, Iliadou A, Askling J, et al. Association of chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis Rheum. 2006;54(3):692-701. 40. Friedewald VE, Ganz P, Kremer JM, et al. AJC editor�s consensus: rheumatoid arthritis and atherosclerotic cardiovascular disease. Am J Cardiol. 2010;106(3): 442-447. 41. Atzeni F, Turiel M, Caporali R, et al. The effect of phar- macological therapy on the cardiovascular system of patients with systemic rheumatic diseases. Autoimmun Rev. 2010;9(12):835-839.
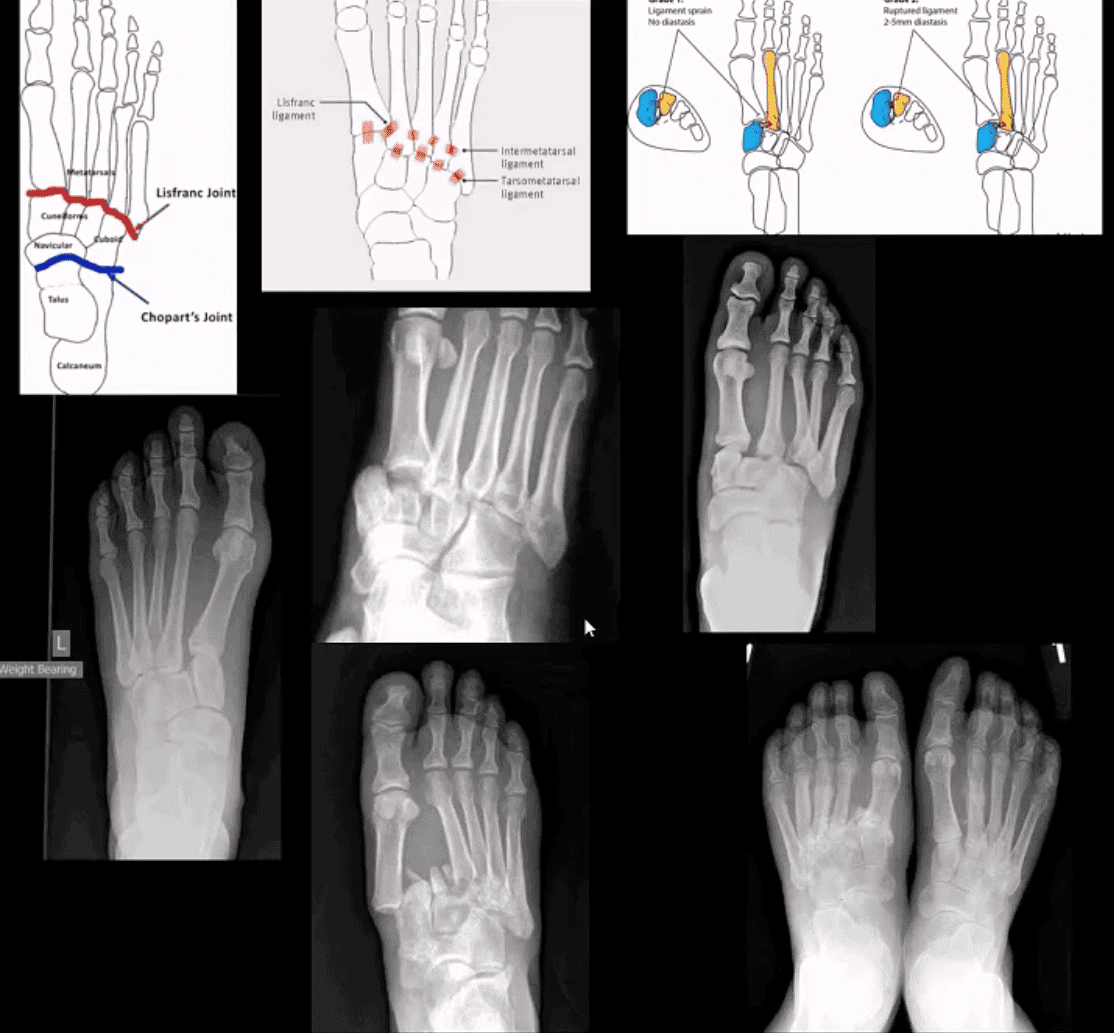
M/C dislocation of the foot at tarsal-metatarsal articulation (Lisfranc joint). Direct impact or landing and plantar or dorsal flexing the foot. Lisfranc ligament holding 2nd MT base and 1st Cu is torn. Manifests with or w/o fracture-avulsion.
Imaging: 1st step: foot radiography in most cases sufficient to Dx. MSK US may help: show disrupted Cu1-Cu2. Ligament and widened space > 2.5mm. MRI may help but not essential. Weight-bearing view aids Dx.
2-types: homolateral (1st MTP joint in contact) and divergent (2-5 MT displaced laterally and 1st MT medially)
Management: operative fixation is crucial
N.B. Atraumatic Lisfranc dislocation is a frequent complication of a diabetic Charcot foot
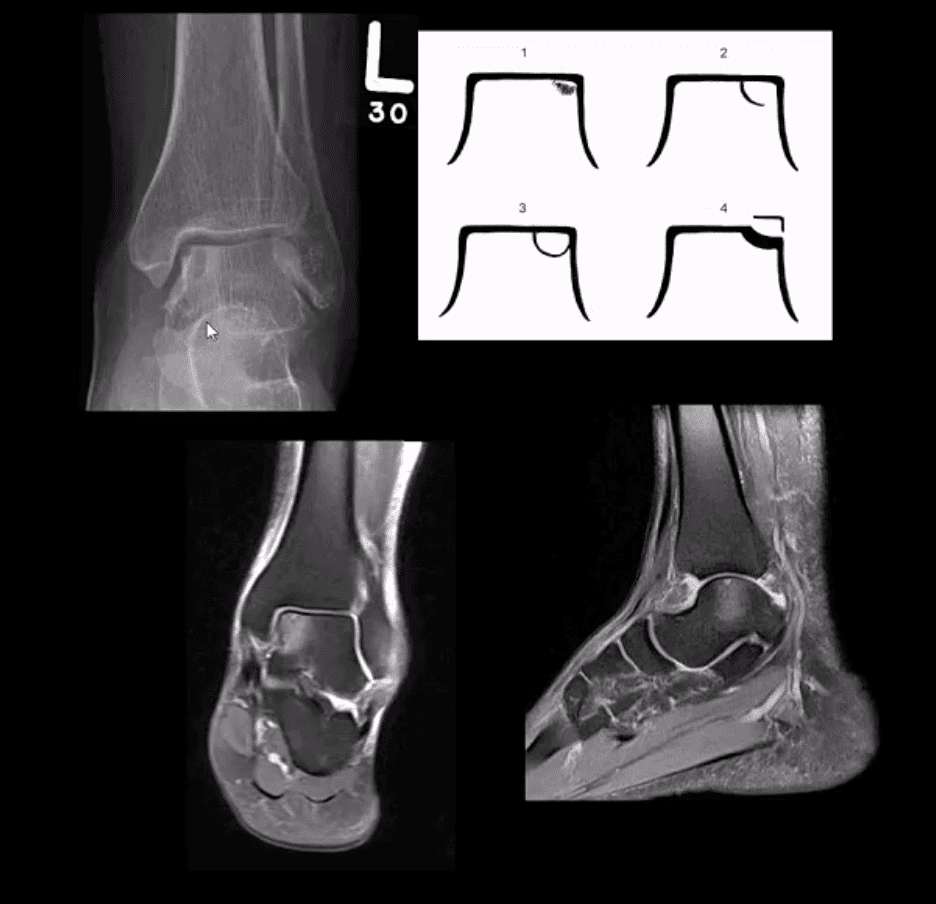
Osteochondral Injury of the Talus (OCD)
Common. Non-traumatic found in superior-medial talar dome. Traumatic may affect supero-lateral dome.
Clinically: pain/effusion/locking. Imaging is crucial.
1st step: radiography may reveal focal radiolucent concavity/halo, fragment.
MRI helpful esp. if OCD is cartilaginous and to demonstrate bone edema.
Jones Fx: extra-articular Fx of proximal metaphysis of the 5th MT. Prone to non-union. Often fixed operatively.
Pseudo-Jones: intra-articular avulsion of 5th MT styloid/base by eccentric contraction of Peroneus Brevis M. Managed conservatively: boot-cast immobilization. Both Jones & Pseudo-Jones Dx by foot series radiography.
Stress Fx. Calcaneus, 2nd, 3rd, 5th MTs. Repeated loading (running) or “March foot” 2nd/3rd MT. Clinically: pain on activity, reduced by rest. Dx: x-rays often unrewarding earlier. MRI or MSK US may help. Managed: Conservatively. Complications; progress into complete Fx
Turf toe: common athletic hyperextension of 1st MTP-sesamoid/plantar plate complex is tearing. 1st MTP unstable/loose. Managed operatively.
Arthritis of the Foot & Ankle
DJD of the ankle: uncommon a primary OA. Typically develops as 2nd to trauma/AVN, RA, CPPD, Hemophilic arthropathy, Juvenile Idiopathic Arthritis, etc. manifests as DJD: osteophytes, JSL, subchondral cysts all seen on x-rays
Inflammatory Arthritis: RA may develop in the ankle or any synovial joint. Will typically presents with symmetrical Hands/feet RA initially (2nd, 3rd MCP, wrists, MTPs in feet) usually with erosion, uniform JSL, juxta-articular osteopenia, and delayed subluxations.
HLA-B27 spondyloarthropathies: commonly affect lower extremity: heel, ankle esp in Reactive (Reiter). Erosive-productive bone proliferation is a crucial Dx.
Gouty Arthritis: common in the lower extremity. Ankle, mid-foot foot esp 1st MTPs. Initial onset: acute gouty arthritis with ST effusion and no erosions/tophi. Chronic tophaceous gout: peri-articular, intra-osseous punched-out erosions with over-hanging edges, no initial JSL/osteopenia, ST. Tophi may be seen.
Miscellaneous arthropathy: PVNS. Not common. Affects 3-4th decades of life. The result of synovial proliferation with Macrophages and multi-nucleated Giant Cells filled with hemosiderin and fatty accumulation may lead to inflammation, cartilage damage, extrinsic bone erosions. Dx: x-rays are insensity, MRI modality of choice. Synovial biopsy. Management: operative, can be difficult.
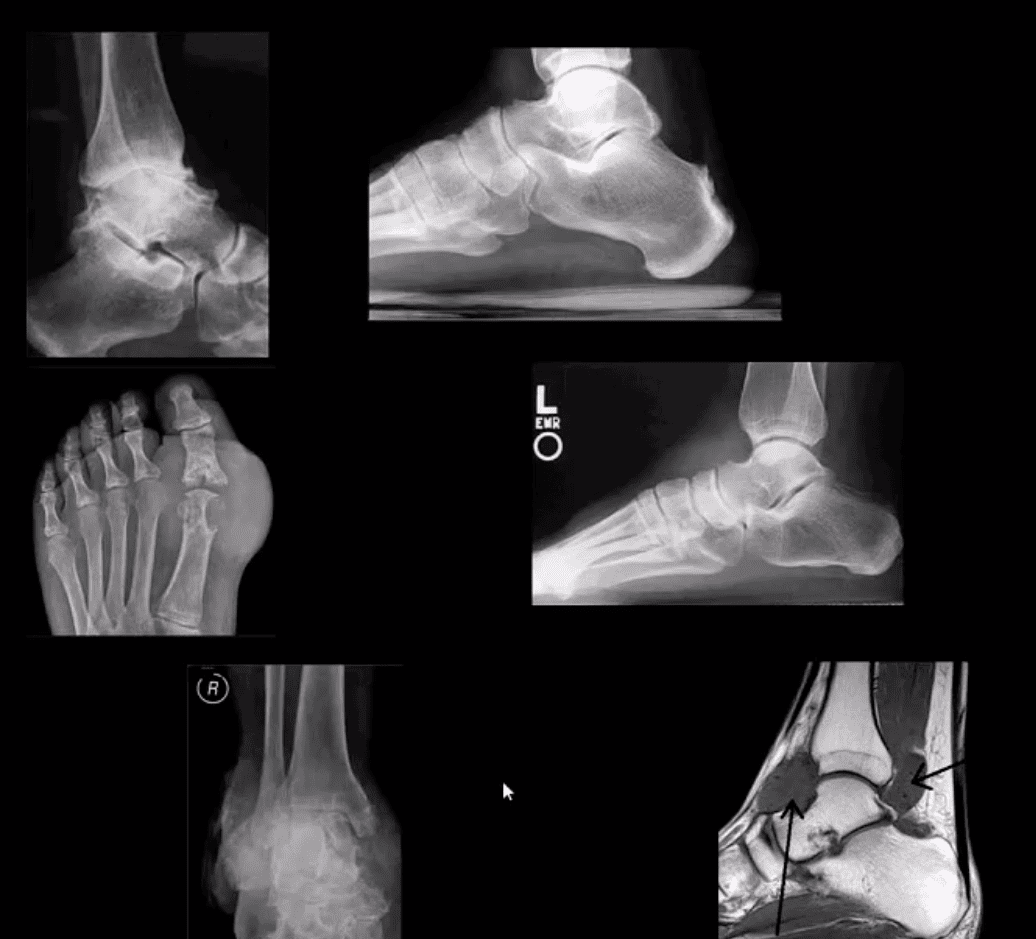
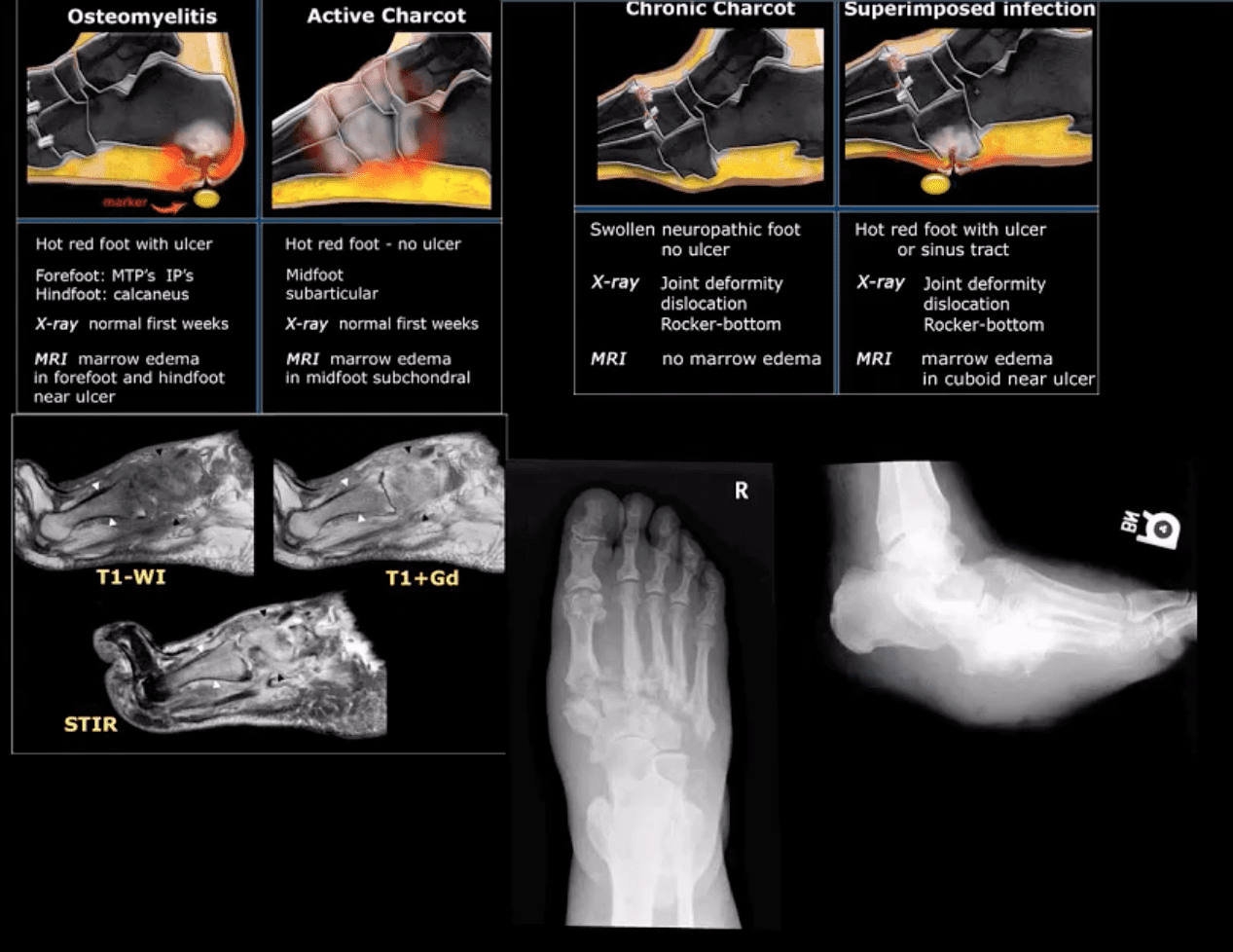
Neuropathic Osteoarthropathy
(Charcot’s joint) Common and on the rise d/t epidemic in type 2 DM. May present with pain initially (50% of cases) and painless destructive arthropathy as a late manifestation. Early Dx: delayed. Imaging is crucial: x-rays: initially unrewarding, some SF effusion is seen. MRI helps with early Dx and extremity off-loading. Late Dx: irreversible dislocations, collapse, disability. Note: Lisfrance dislocation in Charcot joint
M/C mid-foot (TM joint) in 40% of cases, ankle 15%. Progression: Rocker-bottom foot, ulcerations, infections, increased morbidity, and mortality.
Early Dx: by MRI is crucial. Suspect it in patients with type 2 DM especially if early non-traumatic foot/ankle pain reported.
Arthritis is characterized as the inflammation of one or multiple joints. The most common symptoms of arthritis include pain and discomfort, swelling, inflammation, and stiffness, among others. Arthritis may affect�any joint in the human body, however, it commonly develops in the knee. � Knee arthritis can make everyday�physical activities difficult. The most prevalent types of arthritis are osteoarthritis and rheumatoid arthritis, although there are well over 100 distinct forms of arthritis, affecting children and adults alike. While there is no cure for arthritis, many treatment approaches can help treat the symptoms of knee arthritis.
Anatomy of the Knee
� The knee is the largest and strongest joint in the human body. It is made up of the lower end of the thigh bone,�or femur, the top end of the shin bone, or tibia, and the kneecap, or patella. The ends of the three bones are covered with articular cartilage, a smooth, slippery structure which protects and cushions the bones when bending and straightening the knee.
� Two wedge-shaped parts of cartilage, known as the meniscus, function as shock absorbers between the bones of the knee to help cushion the joint and provide stability. The knee joint is also surrounded by a thin lining known as the synovial membrane. This membrane releases a fluid which lubricates the cartilage and also helps reduce friction in the knee. The significant kinds of arthritis that affect the knee�include osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis.
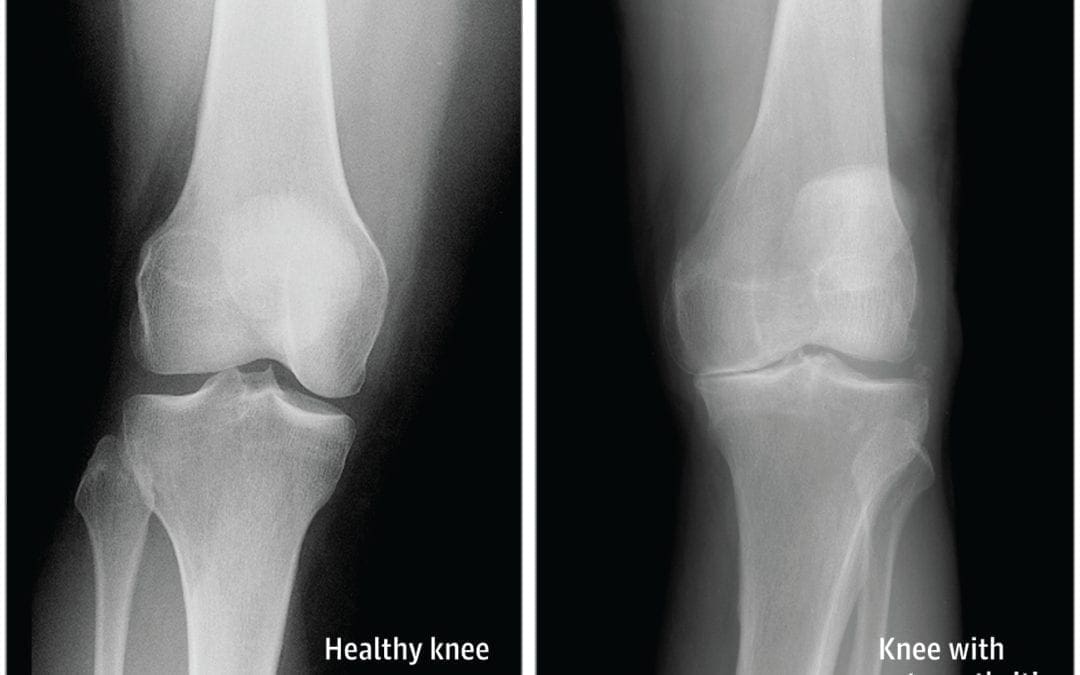
Osteoarthritis
� Osteoarthritis is the most common type of arthritis which affects the knee joint. This form of arthritis is a degenerative, wear-and-tear health issue which occurs most commonly in people 50 years of age and older, however, it may also develop in younger people.
� In osteoarthritis, the cartilage in the knee joint gradually wears away. As the cartilage wears away, the distance between the bones decreases. This can result in bone rubbing and it can�create painful bone spurs. Osteoarthritis generally develops slowly but the pain may worsen over time.
Rheumatoid Arthritis
� Rheumatoid arthritis is a chronic health issue which affects multiple joints throughout the body, especially the knee joint. RA is also symmetrical, meaning it often affects the same joint on each side of the human body.
� In rheumatoid arthritis, the synovial membrane that covers the knee joint becomes inflamed and swollen, causing knee pain, discomfort, and stiffness. RA is an autoimmune disease, which means that the immune system attacks its own soft tissues. The immune system attacks healthy tissue,�including tendons, ligaments and cartilage, as well as softens the bone.
Post-traumatic Arthritis
� Posttraumatic arthritis is a form of arthritis that develops after damage or injury to the knee. By way of instance, the knee joint may be harmed by a broken bone, or fracture, and result in post-traumatic arthritis years after the initial injury. Meniscal tears and ligament injuries can cause additional wear-and-tear on the knee joint, which over time can lead to arthritis and other problems.
Symptoms of Knee Arthritis
� The most common symptoms of knee arthritis include pain and discomfort, inflammation, swelling, and stiffness. Although sudden onset is probable, the painful symptoms generally�develop gradually over time. Additional symptoms of knee arthritis can be recognized as follows:
The joint may become stiff and swollen, making it difficult to bend and straighten the knee.
Swelling and inflammation may be worse in the morning, or when sitting or resting.
Vigorous activity might cause the pain to flare up.
Loose fragments of cartilage and other soft tissue may interfere with the smooth motion of the joints, causing the knee to lock or stick through motion. It could also creak, click, snap or make a grinding sound, known as crepitus.
Pain can cause a sense of fatigue or buckling from the knee.
Many individuals with arthritis may also describe increased joint pain with rainy weather and climate changes.
Diagnosis for Knee Arthritis
� During the patient’s appointment for diagnosis of knee arthritis, the healthcare professional will talk about the symptoms and medical history, as well as conduct a physical examination. The doctor may also order imaging diagnostic tests, such as X-rays, MRI or blood tests for further diagnosis. During the physical examination, the doctor will search for:
Joint inflammation, swelling, warmth, or redness
Tenderness around the knee joint
Assortment of passive and active movement
Instability of the knee joint
Crepitus, the grating sensation inside the joint, with motion
Pain when weight is placed on the knee
Issues with gait, or manner of walking
Any signs of damage or injury to the muscles, tendons, and ligaments surrounding the knee joint
Involvement of additional joints (an indicator of rheumatoid arthritis)
Imaging Diagnostic Tests
X-rays. These imaging diagnostic tests produce images of compact structures, such as bones. They can help distinguish among various forms of arthritis. X-rays for knee arthritis may demonstrate a portion of the joint distance, changes in the bone as well as the formation of bone spurs, known as osteophytes.
Additional tests. Sometimes, magnetic resonance imaging, or MRI, scans, computed tomography, or CT,�scans, or bone scans are required to ascertain the condition of the bone and soft tissues of the knee.
Blood Tests
� Your doctor may also recommend blood tests to determine which type of arthritis you have. With some kinds of arthritis, such as rheumatoid arthritis, blood tests can help with the proper identification of the disease.
Although the knee joint is one of the strongest and largest joints in the human body, it is often prone to suffering damage or injury, resulting in a variety of conditions. In addition, however, other health issues, such as arthritis, can affect the knee joint. In network for most insurances of El Paso, TX, chiropractic care can help ease painful symptoms associated with knee arthritis, among other health issues. Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Treatment for Knee Arthritis
Non-surgical Treatment
� Non-surgical treatment approaches are often recommended before considering surgical treatment for knee arthritis. Healthcare professionals may recommend a variety of treatment options, including chiropractic care, physical therapy, and lifestyle modifications, among others.
� Lifestyle modifications. Some lifestyle modifications can help protect the knee joint and impede the progress of arthritis. Minimizing physical activities which aggravate the condition, will put less strain on the knee. Losing weight may also help lessen stress and pressure on the knee joint, resulting in less painful symptoms and increased function.
� Chiropractic care and physical therapy.�Chiropractic care utilizes full body chiropractic adjustments to carefully restore any spinal misalignments, or subluxations, which may�be causing symptoms, including arthritis. The doctor may also recommend physical therapy to create an individualized exercise and physical activity program for each patient’s needs.�Specific exercises will help increase range of motion and endurance, as well as help strengthen the muscles in the lower extremities.
� Assistive devices. Using assistive devices, such as a cane, shock-absorbing shoes or inserts, or a brace or knee sleeve, can decrease painful symptoms. A brace helps with function and stability, and may be particularly useful if the arthritis is based on one side of the knee. There are two types of braces that are often used for knee arthritis: A “unloader” brace shifts weight from the affected section of the knee, while a “support” brace helps support the entire knee load.
� Drugs and/or medications. Several types of medications are useful in treating arthritis of the knee. Since individuals respond differently to medications, your doctor will work closely with you to determine the medications and dosages which are safe and effective for you.
Surgical Treatment
� The healthcare professional may recommend surgical treatment if the patient’s knee arthritis causes severe disability and only if the problem isn’t relieved with non-surgical treatment. Like all surgeries, there are a few risks and complications with surgical treatment for knee arthritis. The�doctor will discuss the possible problems with the patient.
� Arthroscopy. During arthroscopy, physicians use instruments and small incisions to diagnose and treat knee joint problems. Arthroscopic surgery isn’t frequently used in the treatment of arthritis of the knee. In cases where osteoarthritis is accompanied with a degenerative meniscal tear, arthroscopic surgery may be wise to treat the torn meniscus.
� Cartilage grafting. Normal cartilage tissue may be taken from a tissue bank or through a different part of the knee to fill out a hole in the articular cartilage. This process is typically considered only for younger patients.
� Synovectomy. The lining damaged by rheumatoid arthritis is eliminated to reduce swelling and pain.
� Osteotomy. In a knee osteotomy, either the tibia (shinbone) or femur (thighbone) is cut then reshaped to relieve stress and pressure on the knee joint. Knee�osteotomy is utilized when early-stage osteoarthritis has damaged one facet of the knee joint. By changing the weight distribution, this can relieve and enhance the function of the knee.
� Total or partial knee replacement (arthroplasty).�The�doctor will remove the damaged bone and cartilage, then place new plastic or metal surfaces to restore the function of the knee�and its surrounding structures.
� Following any type of surgery for knee�arthritis will involve a period of recovery. Recovery time and rehabilitation will depend on the type of surgery performed. It’s essential to talk with your healthcare professional to determine the best treatment option for your�knee arthritis. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
� Curated by Dr. Alex Jimenez �
�
Additional Topic Discussion: Relieving Knee Pain without Surgery
� Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine