Many individuals have dealt with issues affecting their lives in some way or form. People with autoimmune diseases must learn to manage their immune system from constantly attacking their bodies to function normally. The immune system’s primary function in the body is to attack environmental factors that harm the cells, muscles, and organs. When a person has an autoimmune disease, either from their family history or environmental factors, their immune system will begin to attack the body’s normal cells because it thinks it is a foreign invader to the body. Some common autoimmune disorders that most people have include lupus, ankylosing spondylitis, and rheumatoid arthritis. Most of these common autoimmune disorders correlate to common symptoms that add to other issues that affect the body. Today’s article looks at rheumatoid arthritis, its symptoms, how it relates to fatigue, and how there are available treatments to manage rheumatoid arthritis as well as fatigue. We refer patients to certified providers specializing in musculoskeletal therapies to help those who suffer from rheumatoid arthritis and fatigue. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Rheumatoid Arthritis?
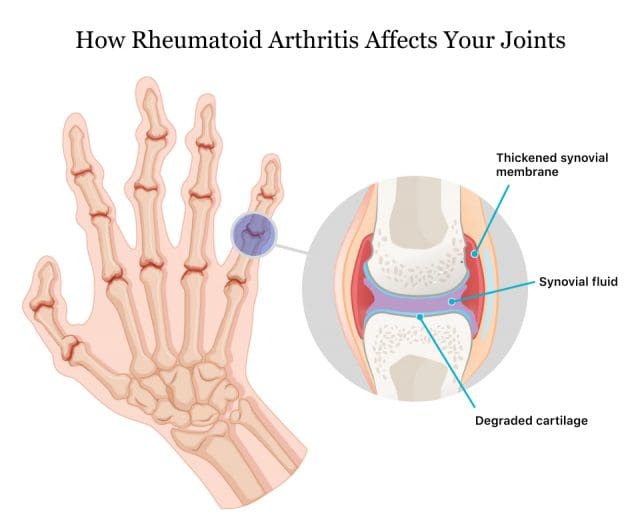
Have you been feeling stiffness and inflammation around your joints? have you experienced gut issues affecting your life? Or do problems of insomnia or fatigue seem to affect your quality of life? Many of these symptoms are associated with rheumatoid arthritis. Rheumatoid arthritis is an autoimmune disease that causes inflammation and swelling in the joints. The video above explains how to manage rheumatoid arthritis and its associated symptoms. Fatigue is one of the symptoms associated with rheumatoid arthritis as the inflammatory cytokines could be a co-morbidity in altering brain function that can lead to an overlap of pain and fatigue in the body, as studies reveal. While there hasn’t been a cure for rheumatoid arthritis, various treatment approaches can help people manage the symptoms of rheumatoid arthritis.
The Symptoms
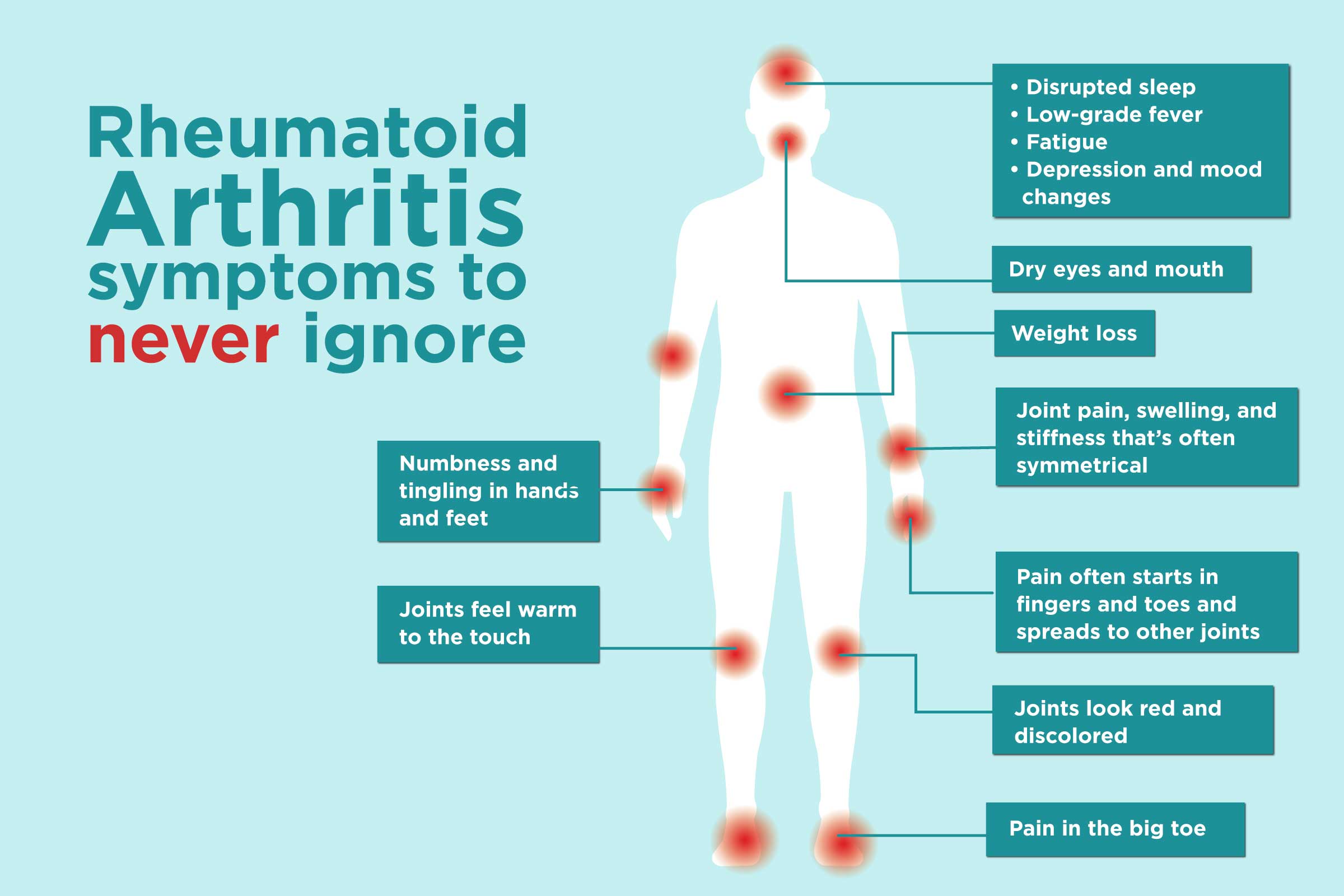
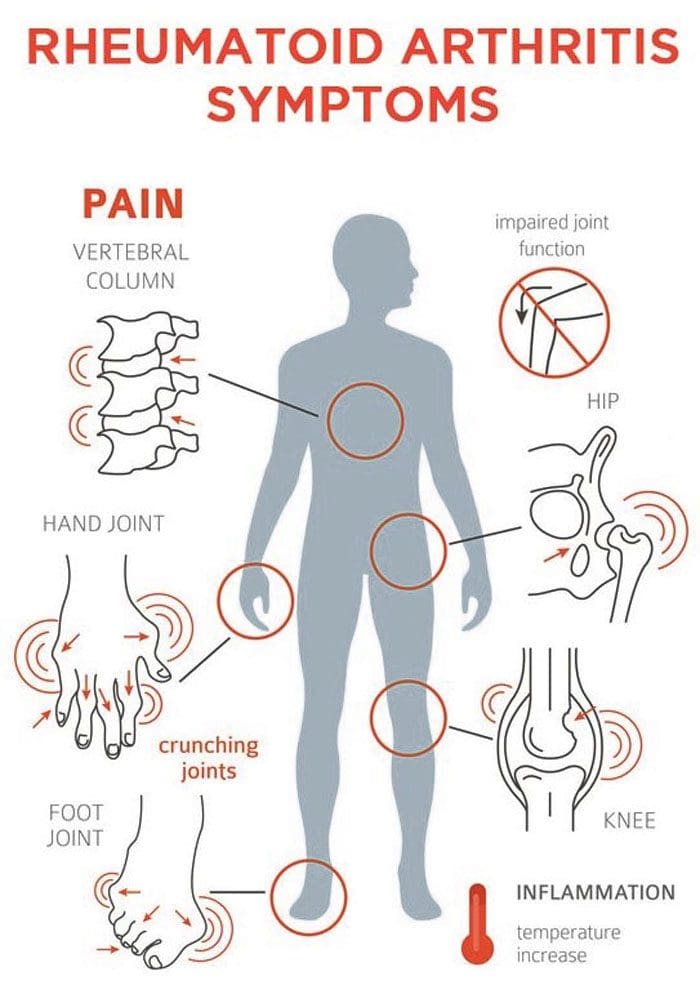
Some of the most commonly rheumatoid arthritis symptoms do to the body include pain, swelling and inflammation of the joints, joint deformity, and stiffness. Unlike wear and tear damage from different types of common inflammatory issues, rheumatoid arthritis symptoms may come and go that can range from mild, moderate, or even severe. When this happens, rheumatoid arthritis may be the result of making it difficult to perform simple tasks and cause joint alterations. Research shows that rheumatoid arthritis associated with inflammation can damage different body parts like the gut. Gastrointestinal problems like leaky gut, IBS, or SIBO could trigger flare-ups in individuals who have rheumatoid arthritis. This is known as somato-visceral pain, where the muscles affect the vital organs, causing problems for the body.
How Does Fatigue Correlate To RA?
Individuals that have rheumatoid arthritis do suffer from various symptoms that are associated with inflammatory issues. When inflammation begins to affect the body, it can overlap the profiles of fatigue and poorer quality of life in the individual. So how does fatigue correlate to rheumatoid arthritis? Studies reveal that fatigue is considered one of the acute symptoms of rheumatoid arthritis that imposes a burden on individuals, thus being associated with reducing their health and wellness. Fatigue has many dimensions that do impact many individuals. Some people will explain to their primary physicians that they are constantly tired, overworked, and repeatedly stressed from everyday life or disorders affecting their bodies. For rheumatoid arthritis individuals, studies reveal that high inflammatory factors associated with fatigue may cause them to feel exhausted. This is related to individuals who have insomnia from other conditions.
Managing Rheumatoid Arthritis-Video
Have you been feeling stiffness and inflammation around your joints? have you experienced gut issues affecting your life? Or do problems of insomnia or fatigue seem to affect your quality of life? Many of these symptoms are associated with rheumatoid arthritis. Rheumatoid arthritis is a chronic autoimmune disease that causes inflammation and swelling in the joints. The video above explains how to manage rheumatoid arthritis and its associated symptoms. Fatigue is one of the symptoms associated with rheumatoid arthritis as the inflammatory cytokines could be a co-morbidity in altering brain function that can lead to an overlap of pain and fatigue in the body, as studies reveal. While there hasn’t been a cure for rheumatoid arthritis, various treatment approaches can help people manage the symptoms of rheumatoid arthritis.
Treatments For RA & Fatigue
Even though there hasn’t been a cure for rheumatoid arthritis, there are ways to manage the associated symptoms of rheumatoid arthritis. Eating anti-inflammatory riched foods could potentially dampen the effect of inflammation on the joints. One way while exercising can help loosen up stiff joints and bring back muscle strength, thus restoring joint motion. Treatments like chiropractic care can also provide pain relief and management for individuals dealing with rheumatoid arthritis. Chiropractic care comprises passive and active treatment modalities for rheumatoid arthritis and fatigue. Chiropractors utilize spinal adjustments and manual manipulation to reduce misalignment or subluxation of the spine. Chiropractic care may also help with many symptoms like fatigue associated with rheumatoid arthritis without invasive treatments or medication. Chiropractic care could potentially improve the function of the bones, joints, and even the nervous system in the body.
Conclusion
Rheumatoid arthritis is a chronic inflammatory disease that causes joint stiffness and swelling. The causes of this autoimmune disease are unknown. Still, factors like stress, gut issues, and obesity are associated with symptoms like fatigue, leaky gut, muscle stiffness, and poorer quality of life could potentially be involved with rheumatoid arthritis. Treatments like eating anti-inflammatory foods, exercising, and chiropractic care could help manage inflammatory issues triggering rheumatoid arthritis and potentially reduce the effects of fatigue from the body, thus slowing down the progression and bringing back a person’s quality of life.
Korte, S Mechiel, and Rainer H Straub. “Fatigue in Inflammatory Rheumatic Disorders: Pathophysiological Mechanisms.” Rheumatology (Oxford, England), Oxford University Press, 1 Nov. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6827268/.
Pope, Janet E. “Management of Fatigue in Rheumatoid Arthritis.” RMD Open, BMJ Publishing Group, May 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7299512/.
Santos, Eduardo J F, et al. “The Impact of Fatigue in Rheumatoid Arthritis and the Challenges of Its Assessment.” Rheumatology (Oxford, England), Oxford University Press, 1 Nov. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6827262/.
Staff, Mayo Clinic. “Rheumatoid Arthritis.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 18 May 2021, https://www.mayoclinic.org/diseases-conditions/rheumatoid-arthritis/symptoms-causes/syc-20353648.
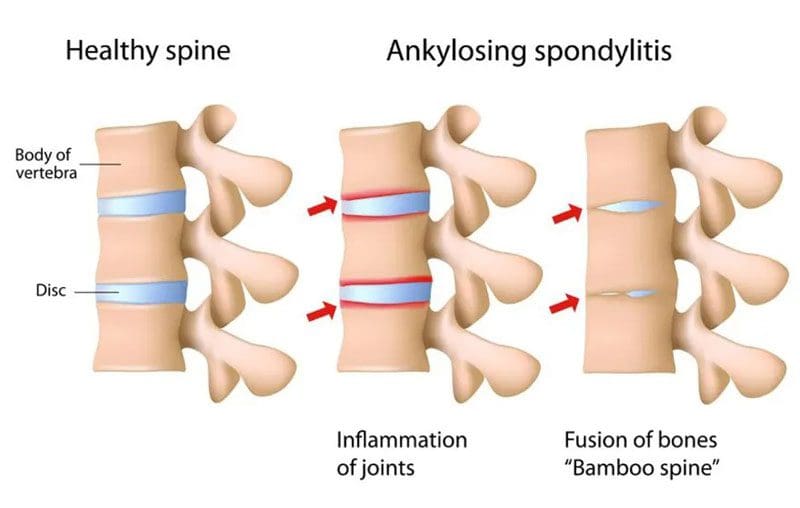
Spondylitis Anti-Inflammation Diet: Individuals who have a chronic back pain condition can be recommended to have two or more vertebrae fused to correct the problem/s and alleviate the pain. However, a form of inflammatory spinal arthritis can cause the vertebrae to fuse by themselves, known as ankylosing spondylitis. One recommended way to bring pain relief is by eating an anti-inflammatory diet. Studies have shown that a low-inflammatory diet can help improve spondylitis symptoms.
Spondylitis Anti-Inflammation Diet
Ankylosing spondylitis is a progressive inflammatory disease that primarily affects the spine; however, individual symptoms vary. Symptoms include stiffness and pain in the neck, hips, low back, and fatigue. There is no definite pattern meaning:
Symptoms can improve.
Symptoms can worsen or flare up.
Symptoms can stop for a period of time.
Women are affected more often than men with no known cause. There is no cure for ankylosing spondylitis, but treatments and self-care can slow down the disease’s progression and help manage symptoms.
Diet and Inflammation
Diet is not the root cause of inflammatory disease, but eating inflammation-causing foods can worsen symptoms. Reducing inflammation can help alleviate pain.
Eliminating foods that cause or increase inflammation is recommended to help the body become stronger and manage symptoms.
Functional medicine practitioners can help guide individuals on maximizing healthy nutrition and using it to reduce pain and symptoms.
If an individual has a genetic predisposition, their diet can be crucial to calm down the symptoms and help turn the autoimmune disease around.
A spondylitis anti-inflammation diet should be rich in vegetables, fruit, whole grains, and omega-3 fatty acids. Evidence shows that a diet low in starches can lead to less ankylosing spondylitis activity. Low-starch can also help limit the presence of Klebsiella pneumoniae, a bacteria that feeds on starch and is a known trigger for the onset and development of ankylosing spondylitis.
Foods To Eat
Leafy greens
These include spinach, kale, Swiss chard, and collard greens containing magnesiumand polyphenols that reduce inflammation.
These can be raw or cooked with garlic and olive oil added to maximize benefits.
Cruciferous vegetables
These contain sulforaphane, anantioxidantthat includes broccoli cauliflower and can be eaten raw or cooked, roasted with olive oil, sauteed, and stir-fried.
Allium Vegetables
These contain sulfuric compounds and quercetin,a flavonoidthat helps reduce inflammation.
These include red and yellow onions, leeks, garlic, and shallots.
They can be eaten raw or cooked in salads, stir-frys, and sandwiches.
Berries
These contain anthocyanin,an antioxidant flavonoid, and other antioxidants and polyphenols that help with inflammation.
These include strawberries, raspberries, blueberries, blackberries and can be eaten raw, in smoothies, in salads, with oatmeal, or mixed in unsweetened yogurt.
Fruits
Certain fruits contain quercetin and polyphenols to help with inflammation.
These include apples, cherries, oranges.
Healthy oils
Contain oleocanthalwhich acts similar to nonsteroidal anti-inflammatory medications and contains various antioxidants.
These include olive oil for low heat cooking and avocado oil for high heat cooking to replace butter and margarine.
It can be served in dressings and drizzled on foods.
Examples include walnuts, almonds, peanuts, pistachios, chia seeds, and ground flaxseeds.
These can be served as snacks, salads, mixed in side dishes, topping, or added to unsweetened yogurt or oatmeal.
Fatty fish
Omega-3 fatty acids help reduce inflammation.
Examples include salmon, cod, rainbow trout, mackerel, and sardines.
These can be baked, sauteed, grilled, mixed into salads, and stir fry.
Avoid These Foods
When making lifestyle adjustments for a spondylitis anti-inflammation diet, focus on reducing or removing processed foods and saturated fats. These include:
Sugars from all sources like soda, sugary drinks, shakes, candy, and desserts.
Trans fats, like those in fried foods like chips and fries.
Individuals may not be symptomatic with certain foods, but that doesn’t mean the foods should be consumed. Gluten, dairy, and eggs can cause potential problems as they compromise the gut and the immune system. These can set back the individual’s healing or remission.
Body Composition
What Happens To The Body When Eating Fruit
Fruit is made up of simple sugar called fructose, providing the body with a carbohydrate energy source. The natural sugar the body gets from a piece of fruit is not the same as processed fructose added to processed products like fructose corn syrup. Processed products are typically filled with empty calories and very little nutrition. When the body has fruit, the liver processes fructose before getting absorbed through the small intestine. Research shows that exposing the gut to more fiber-rich foods like fruit helps the gut achieve an anti-obese condition by increasing the good bacteria and reducing the obese bacteria. Essential nutrients from fruit include:
Folate
Vitamin C
Vitamin B1
The USDA recommends making half of each meal/plate be fruit and vegetables.
References
Harvard Health Publishing. (November 16, 2021) “Foods that Fight Inflammation.” https://www.health.harvard.edu/staying-healthy/foods-that-fight-inflammation
Macfarlane, Tatiana V et al. “Relationship between diet and ankylosing spondylitis: A systematic review.” European journal of rheumatology vol. 5,1 (2018): 45-52. doi:10.5152/eurjrheum.2017.16103
Nielsen, Forrest H. “Magnesium deficiency and increased inflammation: current perspectives.” Journal of inflammation research vol. 11 25-34. January 18 2018, doi:10.2147/JIR.S136742
Rashid T, Wilson C, Ebringer A. The Link between Ankylosing Spondylitis, Crohn’s Disease, Klebsiella, and Starch Consumption. Clin Dev Immunol. 2013;2013:872632. doi: 10.1155/2013/872632.
Sharma, Satya P et al. “Paradoxical Effects of Fruit on Obesity.” Nutrients vol. 8,10 633. 14 Oct. 2016, doi:10.3390/nu8100633
van Buul, Vincent J et al. “Misconceptions about fructose-containing sugars and their role in the obesity epidemic.” Nutrition research reviews vol. 27,1 (2014): 119-30. doi:10.1017/S0954422414000067
Arthritis can be a debilitating disease that interferes with everyday life. There are over 20% of adults aged 65 and older that have arthritis along with all the symptoms like pain, stiffness, swelling, and decreased range of motion. The most commonly affected joints include the shoulders, hands, spine, hips, and knees. Arthritis results from damage to joint cartilage from various factors such as age, wear and tear, injury, being overweight, and disease. While medication and surgery are the most common treatment options, an arthritis chiropractor can offer a conservative, natural, non-invasive option to manage symptoms.
Arthritis Chiropractor Helps By
While arthritis, either caused by wear and tear – Osteoarthritis or disease – Rheumatoid Arthritis cannot be cured. An arthritis chiropractor can help manage symptoms and prevent progression. Chiropractors are trained to use various techniques to help alleviate pain and tension, including arthritis. Chiropractic treatment aims to alleviate pain by adjusting, massaging, and realigning the musculoskeletal system to relieve stress, stretch the muscles, ligaments, tendons, and restore balance within the body. They open the body to allow proper/optimal nerve energy and blood circulation. This is beneficial for arthritic joints to reduce unnecessary strain, translating to reduced wear on the joints and keeping the body active.
Benefits
There are significant benefits that regular chiropractic treatment can offer. These include:
Restored range of motion
Joint pain relief
Inflammation alleviation
Improved nerve function for optimal tissue healing
Regular adjustments will keep the body optimally aligned and functioning smoothly.
Arthritis chiropractors can recognize the most subtle changes.
Lifestyle Adjustments
Healthy lifestyle adjustments help manage arthritis.
Guidance on healthy habits that include:
Anti-inflammatory foods
Weight loss
Proper sleep habits
Exercise training
Stress management
The sooner chiropractic care is sought out, the better to prevent symptoms from worsening. Chiropractic can generate great results with less need for medication/s or surgery.
Body Composition
Identifying The Risk of Sarcopenia and Decreased Mobility
As the body ages, it begins to lose muscle mass, and as more sedentary behavior is adopted, the rate of loss increases along with age-related injury. Identifying these age-related changes in muscle and how they relate to frailty risk can be challenging to identify and track. By accurately measuring fat-free mass in each region of the body, Skeletal Muscle Index – SMI quickly specifies muscle mass and frailty risk. Sarcopenia and frailty specifically affect the elderly population, affecting mortality, cognitive function, and quality of life. Loss of muscle in the arms and legs is associated with:
Reductions in mobility
Increased risk of falls
Frailty
Extended hospital stays
Falls and fractures frequently result in a cycle of muscle deterioration. Analysis tools can help track body composition changes to minimize muscle wasting and the risk of impaired mobility. Assessing skeletal muscle mass in outpatient and hospital settings can decrease debilitating outcomes before they happen. The InBody analysis is quick and easy, providing a calculation for skeletal muscle index and the sum of the lean mass in the arms and legs. The ease of performing the InBody test provides physicians more time to work with and educate individuals on adopting lifestyle changes to help prevent sarcopenia.
References
Aletaha, Daniel. “Precision medicine and management of rheumatoid arthritis.” Journal of autoimmunity vol. 110 (2020): 102405. doi:10.1016/j.jaut.2020.102405
Beasley, Jeanine. “Osteoarthritis and rheumatoid arthritis: conservative therapeutic management.” Journal of hand therapy: official journal of the American Society of Hand Therapists vol. 25,2 (2012): 163-71; quiz 172. doi:10.1016/j.jht.2011.11.001
Demoruelle, M Kristen, and Kevin D Deane. “Treatment strategies in early rheumatoid arthritis and prevention of rheumatoid arthritis.” Current rheumatology reports vol. 14,5 (2012): 472-80. doi:10.1007/s11926-012-0275-1
Kavuncu, Vural, and Deniz Evcik. “Physiotherapy in rheumatoid arthritis.” MedGenMed: Medscape general medicine vol. 6,2 3. 17 May. 2004
Moon, Jeong Jae et al. “New Skeletal Muscle Mass Index in Diagnosis of Sarcopenia.” Journal of bone metabolism vol. 25,1 (2018): 15-21. doi:10.11005/jbm.2018.25.1.15
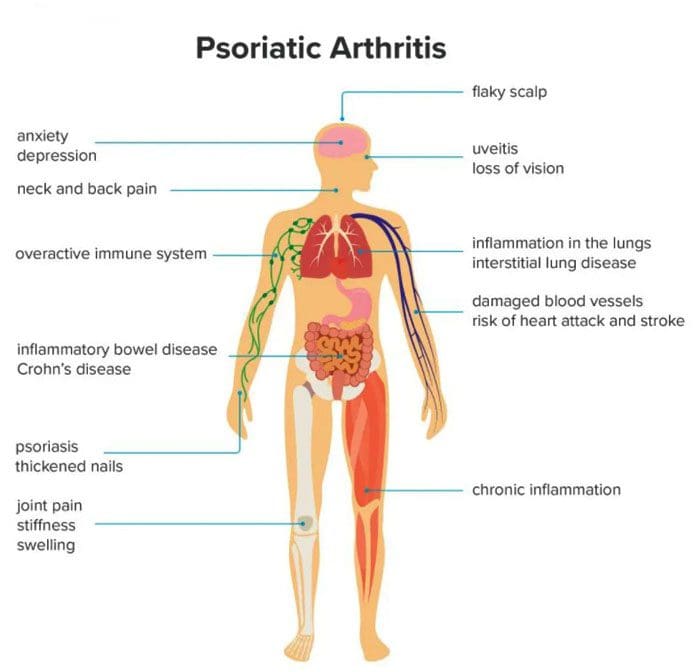
Psoriatic arthritis can develop in individuals who have psoriasis, affecting various joints, especially the knees. Psoriasis is a skin condition that causes skin cells to build up and form patches of itchy, dry skin known as plaques. Psoriatic arthritis is a long-term inflammatory disease that can cause inflammation, stiffness, and pain. Symptoms can progressively worsen over time without treatment. Early diagnosis is vital to minimize damage to the joints and slow the condition’s progress with treatment.
Psoriatic Arthritis
Psoriatic arthritis symptoms like stiffness and swelling can present differently from person to person. For example, some individuals with psoriatic knee arthritis will experience stiffness or pain in one knee, while others experience symptoms in both knees. Psoriatic arthritis in the knee can also cause swelling in the surrounding:
Ligaments
Tendons
Synovial membranes
Symptoms can also present in the:
Elbows
Feet
Hands
Symptoms
Symptoms usually begin between the ages of 30 and 50. Common symptoms include:
Stiffness after resting or sleeping.
Swelling.
Inflammation in the knee and surrounding area.
Warm or hot skin on the knee from the inflammation.
Pain in and around the joints, tendons, or ligaments.
Joint sticking, difficulty moving, or reduced range of motion.
Other symptoms include:
Back pain
Fatigue
Pain and redness in the eyes
Swollen fingers or toes
Difficulty walking from pain in the feet or Achilles tendon.
The severity of psoriasis does not determine psoriatic arthritis symptoms. Symptoms can go through a pattern of relapses and remissions. Individuals can have a sudden attack where symptoms get worse over a short time. After the flare-up, symptoms can improve as the condition goes into remission. Symptoms may not present for a long time until another flare-up. For example, an individual may have severe psoriasis but only mild psoriatic arthritis.
Causes
Psoriatic arthritis develops when the body’s immune system mistakenly attacks healthy cells and tissues. The faulty immune response causes the body to quickly generate new skin cells that stack on top of each other forming plaques. When the condition affects the joints, it leads to inflammation. While there is no apparent cause for psoriatic arthritis, researchers have found connections to genetics and the environment, as well as, individuals with close relatives that have psoriatic arthritis could be more likely to develop the condition. Other factors that could influence the development include:
Severe psoriasis
Traumatic injury/s
Obesity
Nail disease
Smoking
The condition can happen at any age, but according to the National Psoriasis Foundation, most individuals first notice symptoms about ten years after their psoriasis begins. However, only 30% of individuals with psoriasis develop psoriatic arthritis.
Diagnosis
Doctors use imaging tools to diagnose psoriatic arthritis in the knee. They will use:
MRI
X-rays
Ultrasound
To help them check for irregularities or signs of inflammation in the joint and surrounding tissues.
Additional tests are used to rule out other common forms of arthritis like rheumatoid and osteoarthritis.
Blood tests check for inflammation and specific antibodies.
In some cases, a small amount of fluid from the joint is taken to help eliminate the possibility of other underlying conditions like an infection.
Treatment
There is currently no cure for psoriatic arthritis, but treatments are being developed and show promise for long-term management. Current treatments focus on managing symptoms and improving the quality of life for the individual.
Biologics
Biologic medications like tumor necrosis factor or TNF inhibitors are recommended as the first-line therapy for most individuals with a new diagnosis of psoriatic arthritis. These meds help block TNF, which plays a crucial role in inflammation. They have shown to be effective at reducing the severity of symptoms and the frequency of flare-ups. Biologics can cause unwanted side effects, especially in individuals that experience frequent infections and need routine monitoring.
Small Molecule Medications
Individuals that cannot use biologic medications may be recommended a new class of medication called oral small molecules or OSMs. Examples include apremilast – Otezla and tofacitinib – Xeljanz.
Disease-modifying Antirheumatic Drugs
Disease-modifying antirheumatic drugs – DMARDs are a long-term option. They are used to slow the progression of psoriatic arthritis, and examples include methotrexate and cyclosporine. DMARDs work best when an individual begins taking them as early as they can take time to work. However, individuals are encouraged to continue taking them, even if symptoms do not improve right away.
Easing Inflammation
A doctor may prescribe nonsteroidal anti-inflammatory drugs – NSAIDs and corticosteroid injections when knee symptoms flare-up. These are short-term treatments that provide immediate relief, as long-term use can lead to side effects. Individuals can find relief with combined self-care that includes:
Taking over-the-counter NSAIDs like ibuprofen/Advil or naproxen/Aleve.
Applying ice and heat packs.
Gentle exercise to promote a full range of motion.
Gentle stretching or yoga can help relax tight muscles.
However, chiropractic is not the primary treatment for arthritis but is intended to be used in combination to relieve pain, loosen and stretch the muscles and balance the body.
InBody
Strength, Balance, and Improved Body Composition
Functional fitness is the ability to move comfortably every day. The benefits of physical activity also contribute to improved body composition. Working to reach a certain level of functional fitness can help the aging process that has been shown to reduce metabolic rate. Inactivity is why individuals lose Lean Body Mass as they age, leading to increased body fat. Lean Body Mass contributes to the body’s overall Basal Metabolic Rate or BMR, also known as metabolism. This is the number of calories the body needs to support essential functions. Everyone is encouraged to engage in strength training or resistance exercises, but specifically older adults. This can help regain muscle loss which can lead to an increase in lean body mass. The increase in Lean Body Mass increases BMR, which helps prevent fat gain.
References
Chang, K. L., et al. (2015). Chronic pain management: Nonpharmacological therapies for chronic pain [Abstract]. https://www.ncbi.nlm.nih.gov/pubmed/25970869
Chiropractic care for arthritis. (n.d.). arthritis.org/health-wellness/treatment/complementary-therapies/physical-therapies/chiropractic-care-for-arthritis
Managing rheumatoid arthritis is an ongoing balancing act. Flare-ups can still present despite following the rheumatologist’s lifestyle instructions, proper medication use, and a well-maintained RA plan. Monitoring daily activities can help minimize the chances of experiencing episodes.
Rheumatoid Arthritis Flare-Ups
A rheumatoid arthritis flare-up is a short-term escalation of arthritis symptoms. A flare-up can go away within a day or can persist for several weeks or months. A flare-up usually involves joint stiffness and pain but can also present as any symptoms worsening. If the flare-up is severe, it can affect the ability to perform regular everyday activities.
Symptoms
Symptoms can vary, and not every person experiences the same. Most individuals describe flare-ups with a sudden increase in:
Pain
Stiffness
Swelling
Limited joint mobility
Fatigue
Symptoms that feel like the flu.
Frequency and severity can also vary.
Back Pain Symptoms
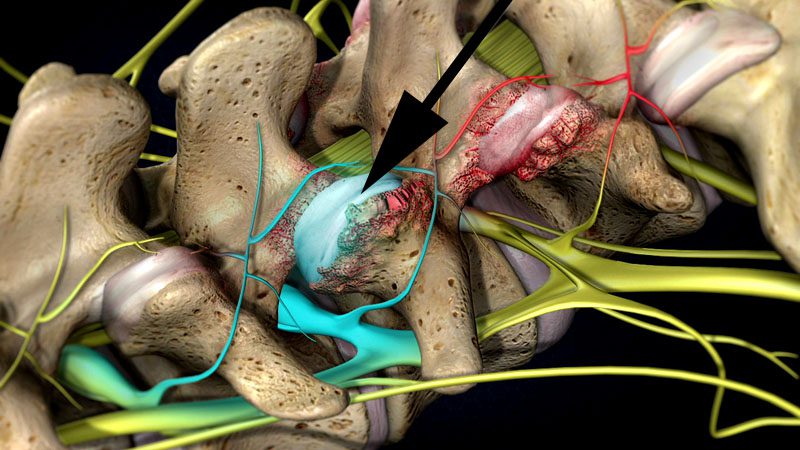
Rheumatoid arthritis can affect many joints. It is the inflammation of a joint’s synovial membrane. These include the facet joints in the spine. The most commonplace in the spine affected by rheumatoid arthritis is the upper neck, around the base of the skull. The joints at the top of the neck get inflamed and can become unstable or form abnormal tissue that sticks out and compress the spinal cord.
Triggers
Several potential flare-up triggers include:
Stress
Not getting enough sleep
Medication changes
Injury
Excessive physical activity and/or exercise
Repetitive overuse injury
Smoking
Spinal infections
Airborne toxins can also be a trigger to a flare-up. Substances include chemicals like household cleaners. Switching to organic and environmentally safe cleaners can help. Airborne toxins are a concern in densely populated cities and areas that experience air pollution and smog. To minimize risks, staying indoors during times of poor air quality is recommended.
However, flare-ups can happen without an identifiable trigger. Certain foods can increase inflammation and could contribute to a flare-up, including:
Avoiding these foods and following a diet that has been developed to prevent symptoms will help significantly. The objective is to learn to identify an RA flare-up to moderate activities accordingly.
Prevention
Managing any chronic medical condition is challenging, especially when trying to predict when a flare-up will happen. There is not a foolproof strategy for prevention, but advice that can help minimize the risks of an RA flare-up.
Understand that the disease can change over time. This means changes in medications and the need for multi-approach treatment. Learning healthy self-care techniques will go a long way in managing symptoms.
Body Composition
Antioxidants protection
Metabolic processes, like energy production, and environmental pollution, can result in free radical production. These are highly reactive molecules that can damage the body’s cells and lead to oxidative stress. This can develop into a disease, including heart disease. The body has natural protective mechanisms to neutralize free radical molecules, including glutathione, which is the body’s top antioxidant. If glutathione becomes depleted because of increased free radicals, the body switches to dietary antioxidants from food as a secondary defense.
Pham-Huy, Lien Ai et al. “Free radicals, antioxidants in disease and health.” International Journal of biomedical science: IJBS vol. 4,2 (2008): 89-96.
Rheumatoid arthritis is said to affect around 1.5 million individuals. Recognized as an autoimmune condition that presents with chronic pain in the body’s joints. It commonly affects regularly used joints like the shoulders, hands, and feet. The condition can begin to present in individuals in their 30s. Concerns that come with a rheumatoid arthritis diagnosis are the condition’s effect on the spinal facet joints. These joints are susceptible to attack from a dysfunctional immune system, leaving them prone to weakness, inflammation, and nerve compression. Chiropractors understand the manifestation of rheumatoid arthritis. They can pinpoint at-risk facet joints and provide corrective relief before more dangerous symptoms begin to present.
Facet joint risks
There are two facet joints that connect each vertebra to the one above and below. Their objective is to stabilize the spine, whether in a neutral position or engaged in flexion/extension movement. When targeted by the body’s immune system, the joints begin to weaken. The body attacks the synovial fluid that lubricates the joints. This creates friction that generates inflammation. Over time the joints break down leading to everything from loss of mobility to bone spurs. When left untreated the facet joints begin to deteriorate, causing nerve compression that can lead to permanent nerve damage. When the joints are not working properly the spine has to work around them.
Subluxations
Disc herniation
Ruptured discs
Sciatica all are possible with facet joint dysfunction.
Treatment
Currently, rheumatoid arthritis cannot be cured but symptoms can go into remission when treatment begins early.Chiropractic is an effective treatment at disrupting the symptoms of joint deterioration that stops the progression.
It has the ability to increase and maintain an individual’s range of motion, from a condition that causes loss of mobility.
It helps to bring rapid pain relief and helps with postural improvements.
It maintains positive spinal health and homeostasis.
Prevents problems with compression and subluxations.
Stretching and strengthening exercises are incorporated to preserve an individual’s spinal integrity.
Diet and nutrition are also adjusted to mitigate the effects, helping with inflammation prevention.
The spinal focus
As rheumatoid arthritis affects the body’s joints, it is vital to protect the facet joints. These joints can experience degenerative damage that can cause long-term problems. Injury Medical Chiropractic and Functional Medicine Clinic provide individuals with the tools necessary to combat rheumatoid arthritis that medications by themselves might not be able to.
Body Composition
Muscle Mass Fitness for Long-Term Health
Muscle building is not just for bodybuilders and athletes. Everyone benefits from building muscle for long-term health. Monitoring the changes in Lean Body Mass can be accomplished by having body composition measured. Body composition analysis can divide an individual’s weight into various components. These include:
Fat Mass
Lean Body Mass
Basal Metabolic Rate will give a clearer picture of overall fitness and health.
Building Lean Body Mass is an investment for maintaining health long-term. The more Lean Body Mass that is built the more is in storage/reserve when the body really needs it. Before adding protein shakes and resistance workouts to the daily regimen, a plan needs to be developed. The first step to building a healthy level of lean body mass is to measure how much there is with a body composition analysis.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Pope JE, Cheng J. Facet (Zygapophyseal) Intraarticular Joint Injections: Cervical, Lumbar, and Thoracic. Injections for Back Pain. 129-135. ClinicalKey.com. Accessed July 16, 2019.
Brummett CM, Cohen SP. Pathogenesis, Diagnosis, and Treatment of Zygapophyseal (Facet) Joint Pain. 816-844. ClinicalKey.com. Accessed July 16, 2019.
Inflammatory spinal arthritis can cause significant joint pain and severely damage sleep quality. Any of the following conditions can cause individuals to experience sleep problems:
Spondylosis (osteoarthritis)
Rheumatoid arthritis
Ankylosing spondylosis
Juvenile idiopathic arthritis
Dr. Jimenez from Injury Medical Chiropractic and Functional Medicine Clinic gives insight into how inflammatory spinal arthritis can disrupt healthy sleep, along with some tips to help individuals with joint pain restore healthy sleep.
Inflammatory Spinal Arthritis and Sleep
First, it is not just the joint pain of arthritis that is causing sleep problems. Research is discovering that more factors could be at play. A study in the journal SLEEP examined how individuals with chronic pain, including osteoarthritis slept. What was revealed was a strong connection between chronic pain and insomnia.
Insomnia can lead to added joint pain because poor sleep can trigger inflammatory pathways that worsen arthritis pain. Plus a poor night of sleep can heighten an individual’s perception of pain the next day. Arthritis pain does not just impact the sleep of adults, but young individuals with juvenile idiopathic arthritis can also struggle with getting healthy sleep. Sleep, pain levels, and mood are strongly related.
Sleep Tips
Achieving quality sleep and a well-rested body can be done. Things to consider to help secure a healthy sleep.
Medication interference/side effects
Corticosteroids could be part of the sleep problem, as corticosteroid treatment has been linked to insomnia. If struggling to fall asleep, talk with a doctor about altering any prescribed medication regimen before sleep like taking aspirin or a nonsteroidal anti-inflammatory NSAID medication in its place.
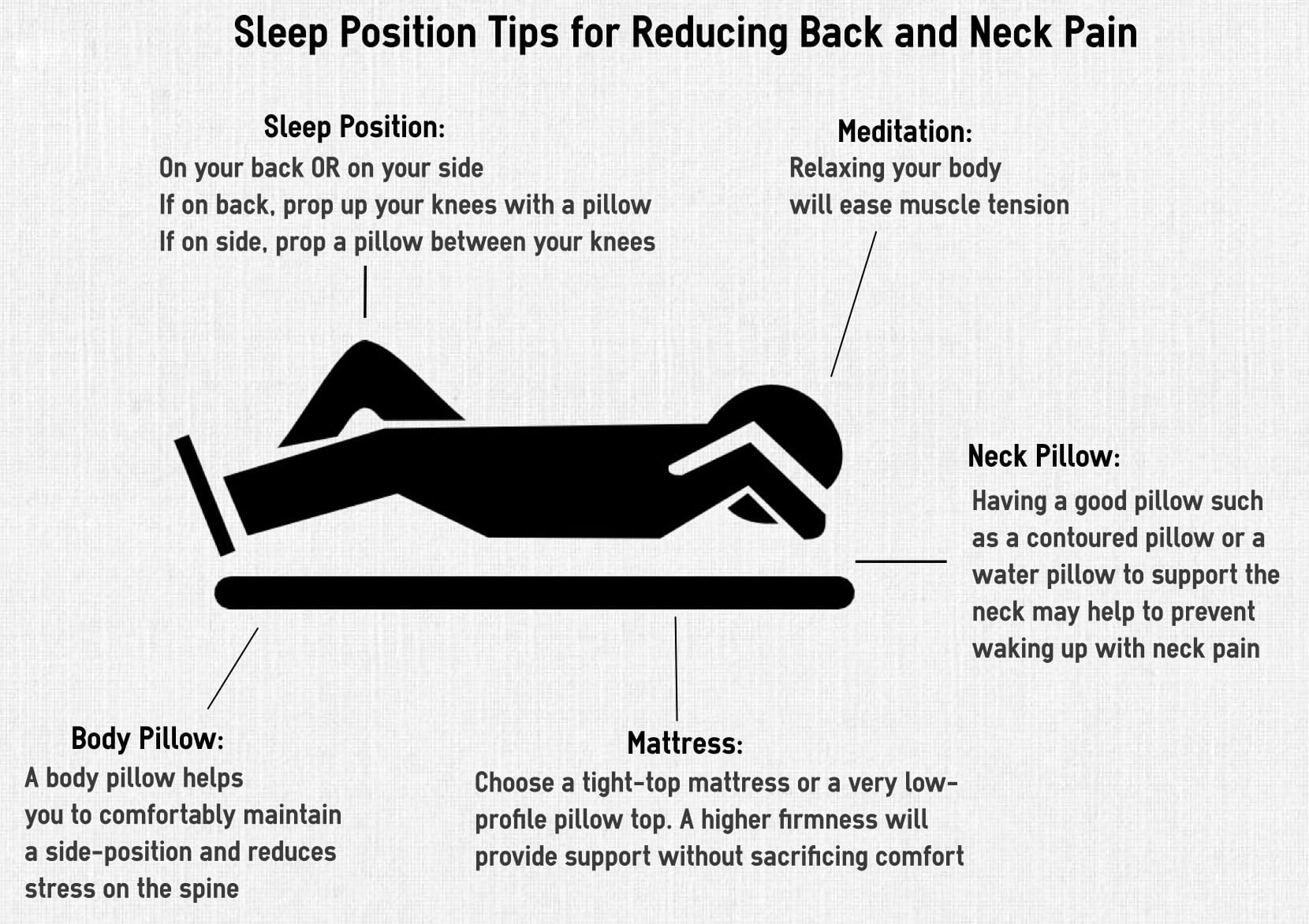
Adjust sleep position to joint pain
If the neck is sore/aching rest the head on a flat pillow so the cervical spine is in a neutral position. For low back joint pain, individuals might find relief by sleeping on their back or side with the knees and hips flexed at a 90-degree angle. For hip joint stiffness, sleeping on the side with a pillow between the legs is recommended.
A firm mattress and support pillow
A firm mattress will support the body and help reduce pain. The right pillow/s are also important for healthy sleep. A lumbar and cervical pillow can help cushion tender areas.
Readjust chores
Joint pain first thing in the morning needs time to adjust. For morning physical chores try to reschedule for later on in the day or if possible the night before. This could be fixing lunches, picking out clothes, preparing breakfast, or packing the work case, tools, etc. The extra time will reduce morning stress and allow the body to gently adjust.
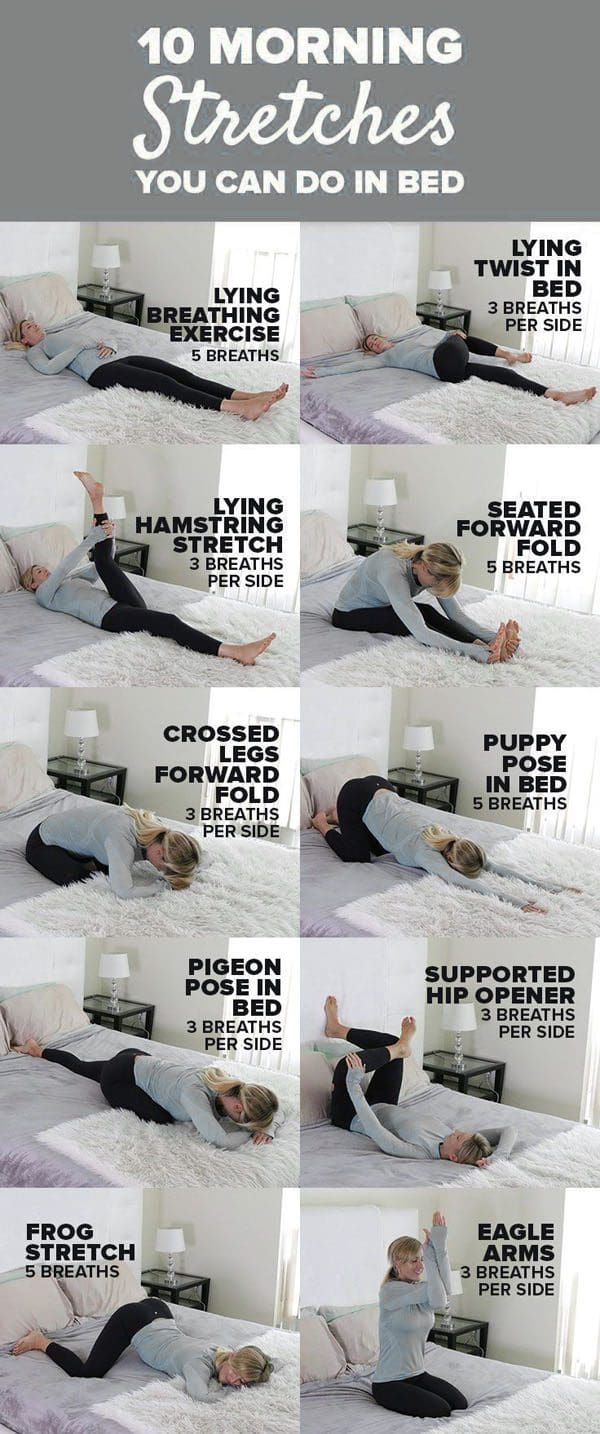
Wake up and stretch
With joint pain in the morning, some gentle stretching can help. Doing some stretches before even getting out of bed will help minimize pain and allow the body to gradually prepare for movement. Follow the stretch session up with a hot shower to loosen stiff joints.
Increase Sleep Quality
Sleep problems can affect anyone even those that don’t have inflammatory spinal arthritis/joint pain. There could be other issues causing sleep problems unrelated to joint pain. If still not getting quality sleep, talk to a rheumatologist about available options.
Body Composition
Osteoarthritis and Exercise
Obesity is a significant risk factor in the development of osteoarthritis. This is not only from the effects of extra weight on the body’s joints but also as a result of the pro-inflammatory effects of adipose tissue. The hips and knees are the weight-bearing joints. Excessive adipose tissue on the midsection and legs have been shown to negatively impact these weight-bearing joints.
Promoting Lean Body Mass and encouraging weight loss can potentially lower the risk of osteoarthritis and improve the quality of life. Gentle exercise is regarded as safe for individuals with osteoarthritis and is a key component to improve body composition, reduce body fat mass, improve lean body mass and maintain a healthy weight. Improving body composition and utilizing exercise in weight management can have a direct and positive effect on joint health.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Myers W. 9 Ways to Rise and Shine With Osteoarthritis. Everyday Health.�http://www.everydayhealth.com/osteoarthritis/ways-to-rise-and-shine-with-osteoarthritis.aspx. Last updated September 25, 2014. Accessed April 18, 2017.
Watson S. Why Osteoarthritis Could Disrupt Your Sleep�and Your Partner�s. Arthritis Foundation. http://www.arthritis.org/living-with-arthritis/comorbidities/sleep-insomnia/osteoarthritis-and-sleep.php. Accessed April 18, 2017.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine