Can individuals dealing with psoriatic arthritis find non-surgical treatments to reduce joint pain and improve skin health?
Introduction
The body is a complex machine with a communal relationship with the joints, organs, bones, muscles, and tissues, each of which has a specific function to ensure the host is alive. The brain is the main control system that gives each body’s systems, organs, muscles and joints a job. When environmental factors or pathogens enter the body, the immune system is the first one to defend the body and eliminate the pathogens to initiate the natural healing process. However, when the immune system is attacking the body constantly, over time, it can lead to autoimmunity and cause overlapping risk profiles in the body. This, in turn, can lead the development of chronic conditions and cause individuals pain and discomfort. In today’s article, we look at an autoimmune disorder known as psoriatic arthritis, its causes and symptoms, and how treatment can help reduce its pain like effects. We discuss with certified medical providers who inform our patients how psoriatic arthritis can affect the joints. While asking informed questions to our associated medical providers, we advise patients to incorporate various non-surgical treatments to reduce psoriatic arthritis symptoms and help manage joint pain that affects a person’s quality of life. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
What Is Psoriatic Arthritis?
Do you experience swelling in your joints that causes pain and discomfort when moving? Do you feel your skin itchier and warmer than usual? Or have you noticed that everyday tasks are more difficult now than before? Many of these pain-like scenarios are associated with joint pain associated with an autoimmune or musculoskeletal condition. Since autoimmunity is developed when environmental factors cause the immune system to attack healthy cells, it can envoke pain and discomfort to the body. When a person is dealing with an autoimmune condition, it can impact not only the individual but also the rest of the body’s system. For instance, if a person is dealing with an autoimmune condition, they could be dealing with skin issues that can cause them to develop scaly, itchy, red skin patches known as psoriasis. If they have joint pain combined with psoriasis, it can develop into psoriatic arthritis. (Skornicki et al., 2021) Now psoriatic arthritis is a heterogeneous autoimmune condition with musculoskeletal involvement that can manifest various symptoms including inflammation and arthritis. (Hackett et al., 2022) This in turn causes many individuals to think they are dealing with rheumatoid factors.
Causes & Symptoms
As a multifactorial pathology, psoriatic arthritis causes care often influenced by a complex interplay of immunological, environmental, and genetic factors that cause its development. (Zalesak et al., 2024) When the immune system starts to attack the healthy cells in the body, the inflammatory cytokines can become haywire and attack the “problem,” causing the development of autoimmunity. Within this integration, some of the causes can include predisposing genetic backgrounds with the presence of environmental factors that can activate the innate immune system precipitate the onset of psoriatic arthritis. (Azuaga et al., 2023) Some of the symptoms can many individuals with psoriatic arthritis can include:
Tendon tenderness
Joint pain
Stiffness
Fatigue
Joint swelling
Skin rash
Musculoskeletal pain
However, there are ways to manage psoriatic arthritis, reduce joint pain from affecting a person, and help them manage the symptoms.
Arthritis Explained-Video
Treatments For Psoriatic Arthritis
When it comes to treating psoriatic arthritis, healthcare professionals need to develop therapeutic options to educate the individual and develop a treatment plan that can include conventional therapies and non-pharmacological therapies that are affordable and customized with the individual’s condition. (Ogdie et al., 2020) Since psoriatic arthritis is a complex inflammatory musculoskeletal condition and skin disease, individuals must try to find ways to reduce the inflammatory effects of causing more joint issues. Non-surgical treatments like chiropractic care, physical therapy, and diet changes can help mitigate the burden of psoriatic arthritis by reducing the complications and the socio-economic impact. (McGonagle et al., 2022)
Another way individuals can reduce the inflammatory effects of psoriatic arthritis is by consuming anti-inflammatory foods to dampen the inflammatory cytokines attacking the joints and going to physical therapy sessions like water aerobics to help stabilize the joints and help people be more mindful about their bodies. Since psoriatic arthritis can be managed through non-surgical therapy, low-weight bearing exercise regimes and incorporating anti-inflammatory foods to reduce inflammation can help people minimize psoriatic arthritis symptoms from impacting their health and wellness journey.
References
Azuaga, A. B., Ramirez, J., & Canete, J. D. (2023). Psoriatic Arthritis: Pathogenesis and Targeted Therapies. Int J Mol Sci, 24(5). https://doi.org/10.3390/ijms24054901
Hackett, S., Ogdie, A., & Coates, L. C. (2022). Psoriatic arthritis: prospects for the future. Ther Adv Musculoskelet Dis, 14, 1759720X221086710. https://doi.org/10.1177/1759720X221086710
McGonagle, D. G., Zabotti, A., Watad, A., Bridgewood, C., De Marco, G., Kerschbaumer, A., & Aletaha, D. (2022). Intercepting psoriatic arthritis in patients with psoriasis: buy one get one free? Ann Rheum Dis, 81(1), 7-10. https://doi.org/10.1136/annrheumdis-2021-221255
Ogdie, A., Coates, L. C., & Gladman, D. D. (2020). Treatment guidelines in psoriatic arthritis. Rheumatology (Oxford), 59(Suppl 1), i37-i46. https://doi.org/10.1093/rheumatology/kez383
Skornicki, M., Prince, P., Suruki, R., Lee, E., & Louder, A. (2021). Clinical Burden of Concomitant Joint Disease in Psoriasis: A US-Linked Claims and Electronic Health Records Database Analysis. Adv Ther, 38(5), 2458-2471. https://doi.org/10.1007/s12325-021-01698-7
Zalesak, M., Danisovic, L., & Harsanyi, S. (2024). Psoriasis and Psoriatic Arthritis-Associated Genes, Cytokines, and Human Leukocyte Antigens. Medicina (Kaunas, Lithuania), 60(5). https://doi.org/10.3390/medicina60050815
For individuals with arthritis, can incorporating acupuncture with other therapies help manage pain and other symptoms?
Acupuncture For Arthritis
Acupuncture has been around for thousands of years and is a form of traditional Chinese medicine that utilizes needles inserted into various parts of the body to relieve pain and inflammation. The practice is based on the concept of life energy that flows throughout the body along pathways called meridians. When the energy flow becomes disrupted, blocked, or injured, pain or illness can present. (Arthritis Foundation. N.D.) Further research is needed to determine how the acupuncture therapeutic mechanisms work and the overall effectiveness. However, there is emerging evidence suggesting that acupuncture can provide symptom relief for individuals with joint pain, especially those with osteoarthritis and rheumatoid arthritis. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Benefits
The actual method that reduces the pain and inflammation is still unclear. Theories include that the needles suppress inflammatory responses, improve blood flow, and relax muscles. Although acupuncture cannot cure or reverse arthritis, it may be useful for managing pain and decreasing associated symptoms, especially in combination with other therapies. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Rheumatoid Arthritis
A systematic review of 43 studies, including humans and animals with rheumatoid arthritis, demonstrated varied results. Several studies showed improvement in symptoms and decreased biological markers of rheumatoid arthritis following one to three sessions of acupuncture for four weeks or more. (Sharon L. Kolasinski et al., 2020) Beneficial outcomes following acupuncture treatment for rheumatoid arthritis include:
Reduced pain
Reduced joint stiffness
Improved physical function
The results of the human and animal studies suggested that acupuncture has the potential to down-regulate:
Levels of interleukins
Levels of tumor necrosis factor
Specific cell signaling proteins/cytokines involved in the inflammatory response, which become elevated in autoimmune conditions like rheumatoid arthritis. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Most of the study subjects were also receiving other forms of treatment, especially medication. Therefore, it is difficult to conclude how beneficial acupuncture is alone or as a supplemental addition to other medical treatments. (Pei-Chi Chou, Heng-Yi Chu. 2018)
Osteoarthritis
Acupuncture for osteoarthritis of the hand, hip, and knee is recommended, according to the American College of Rheumatology and Arthritis Foundation, meaning that it may be worth trying, although more research is needed to confirm its effectiveness. However, since the risk is relatively minor, acupuncture is generally considered a safe alternative treatment option for managing the symptoms. (Sharon L. Kolasinski et al., 2020)
Chronic Pain
As clinical trials suggest that acupuncture may be effective in providing pain relief, it may be a recommended option for individuals suffering from chronic pain. A recent systematic review of 20,827 patients and 39 trials concluded that acupuncture is effective for the treatment of chronic musculoskeletal pain, headache, and osteoarthritis pain. (Andrew J. Vickers et al., 2018)
Triggering the release of endorphins/hormones that help reduce pain.
Safety
Acupuncture is considered a safe procedure by a licensed and certified professional.
To practice acupuncture in the United States, an acupuncturist needs a minimum of a master’s degree from a program accredited by the American Academy of Acupuncture and Oriental Medicine and a license in the state where they received their acupuncture treatment.
Doctors with an MD or DO degree licensed in the United States to practice medicine can also be licensed by the American Academy of Medical Acupuncture after additional training.
Risks
Risks associated with acupuncture are bleeding and bruising, especially for individuals who have a bleeding disorder like hemophilia or take a blood thinning medication. Individuals are recommended to talk to their healthcare provider to determine if acupuncture is a safe option.
Side Effects
Most individuals do not experience any side effects, although possible reactions can include: (Shifen Xu et al., 2013)
Soreness
Bruising
Scarring
Needle shock: a vasovagal response that presents as feeling faint, clammy hands, chills, and slight nausea.
Acupuncture Session
During the initial treatment, individuals will discuss their medical history and what joints and areas of their bodies are presenting with symptoms.
After a physical exam, the individual will lie on a treatment table.
Individuals may be face up or down depending on what areas of the body the acupuncturist needs to access.
It is recommended to wear loose clothing that can be rolled up or moved out of the way to access different areas easily.
Depending on what areas need to be accessed, individuals may be asked to change into a medical gown.
The acupuncturist will use alcohol swabs to disinfect the area before inserting the needles.
The needles are made of stainless steel and are extremely thin.
Individuals may feel a slight pinch in sensitive areas like the hands and feet, but needle insertion should be comfortable and well-tolerated without significant discomfort.
For electroacupuncture, the acupuncturist will pass a mild electric current through the needles, typically 40 to 80 volts.
The needles stay in place for 20 to 30 minutes.
After the treatment is finished, the acupuncturist will remove the needles and dispose of them.
Frequency
The frequency of acupuncture sessions will vary depending on the severity of the symptoms and whether the visits are approved and reimbursed by the health insurance company.
Cost and Insurance
Costs for acupuncture can vary from $75 to $200 per session.
The first session, which involves an initial assessment and evaluation, usually costs more than follow-up visits.
Whether the health insurance will cover some or all of the costs of acupuncture sessions depends on the individual insurance company and the condition being treated.
Medicare currently covers acupuncture services up to 12 visits within a 90-day period for chronic low back pain only.
Medicare will not cover acupuncture for other conditions. (Medicare.gov. N.D.)
Acupuncture is not a cure for arthritis, but it may be a useful tool to help manage pain and other symptoms. Make sure to consult a healthcare provider if acupuncture is safe to try based on medical history.
Chou, P. C., & Chu, H. Y. (2018). Clinical Efficacy of Acupuncture on Rheumatoid Arthritis and Associated Mechanisms: A Systemic Review. Evidence-based complementary and alternative medicine : eCAM, 2018, 8596918. https://doi.org/10.1155/2018/8596918
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W. F., Hawker, G., Herzig, E., Kwoh, C. K., Nelson, A. E., Samuels, J., Scanzello, C., White, D., Wise, B., … Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis care & research, 72(2), 149–162. https://doi.org/10.1002/acr.24131
Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Irnich, D., Witt, C. M., Linde, K., & Acupuncture Trialists’ Collaboration (2018). Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis. The journal of pain, 19(5), 455–474. https://doi.org/10.1016/j.jpain.2017.11.005
Xu, S., Wang, L., Cooper, E., Zhang, M., Manheimer, E., Berman, B., Shen, X., & Lao, L. (2013). Adverse events of acupuncture: a systematic review of case reports. Evidence-based complementary and alternative medicine : eCAM, 2013, 581203. https://doi.org/10.1155/2013/581203
Medicare.gov. (N.D.). Acupuncture. Retrieved from https://www.medicare.gov/coverage/acupuncture
Can individuals with osteoarthritis incorporate spinal decompression therapy to restore spinal mobility and quality of life?
Introduction
As the body ages, so does the spine, as the spinal disc between the joints and the bones starts dehydrating from constant compression through repetitive motions. The many environmental factors contributing to this degenerative disorder can vary within the person and lead to arthritic conditions within the upper and lower extremities. One of the most common types of arthritis is osteoarthritis, and it can affect many people worldwide. Dealing with osteoarthritis in their joints can cause numerous pain-like symptoms that correlate with other body conditions, causing referred pain. However, many treatments can help slow the process of osteoarthritis and relieve the body from the pain-like symptoms of the joints. Today’s article looks at how osteoarthritis affects spinal mobility and how treatments can restore spinal mobility from the effects of osteoarthritis. We talk with certified medical providers who utilize our patients’ information to provide various treatments to reduce the impact of osteoarthritis on the joints. We also inform patients how multiple treatments can help slow down the degenerative process of osteoarthritis. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from osteoarthritis. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
How Does Osteoarthritis Affect Spinal Mobility?
Have you noticed morning stiffness after a good night’s rest? Do you feel tenderness in your joints after some light pressure? Or do you feel limited mobility in your joints, causing a restricted range of motion? Many of these pain-like scenarios are correlated with osteoarthritis, a degenerative joint disorder that has affected many individuals, including older adults. As stated earlier, when the body ages, so do the joints, bones, and spine. Regarding osteoarthritis, the joints will degenerate through natural wear and tear around the cartilage. Osteoarthritis affects multiple joints like the hips and knees, which are the most common, and the spine, and causes numerous sensory-motor dysfunctions. (Yao et al., 2023) When the cartilage around the affected joints starts to deteriorate, the pathogenesis of osteoarthritis causes a disturbed cytokine balance of the proinflammatory cytokines to initiate a vicious cycle that causes cartilage and other intra-articular structure damage around the joint. (Molnar et al., 2021) What this does is that when osteoarthritis starts to affect the joints, it can lead to numerous referred pain-like symptoms.
However, although osteoarthritis can affect the joints, naturally, numerous environmental factors do play a part in the development of osteoarthritis. Physical inactivity, obesity, bone deformities, and joint injuries are some of the causes that can progress the degenerative process. The symptoms that are associated with these environmental factors include:
Pain
Joint stiffness
Tenderness
Inflammation
Swelling
Grating sensation
Bone spurs
Many individuals dealing with pain-like symptoms caused by osteoarthritis will explain to their primary doctors that the pain varies in duration, depth, type of occurrence, impact, and rhythm. This is because the pain from osteoarthritis is complex and multifactorial. (Wood et al., 2022) However, many individuals can look for the help they need to reduce the pain-like issues caused by osteoarthritis through treatments that can slow down the degenerative progress.
An In-depth Look At Spinal Decompression-Video
When it comes to seeking treatment to reduce the effects of osteoarthritis, many individuals seek out treatments that are cost-effective and safe for older individuals. Non-surgical treatments could be the solution many individuals seek to reduce the progress of osteoarthritis. When people experiencing osteoarthritis go to non-surgical treatments, they find out that the pain is decreased, their range of motion is increased, and their physical function has improved. (Alkhawajah & Alshami, 2019) At the same time, non-surgical treatments can be combined with other therapies to the individual’s personalized treatment plan. No-surgical treatments can range from chiropractic care to spinal decompression as they work on gently realigning the spine through traction and help reduce joint and muscle pain. The video above gives an in-depth look at spinal decompression and how it can benefit individuals who are in pain.
Spinal Decompression Restoring Spinal Mobility From Osteoarthritis
Since spinal decompression is a form of non-surgical treatment, it can help slow down the process of osteoarthritis. Spinal decompression incorporates traction to gently pull on the spine, allowing the discs and joints to be lubricated and permitting the natural healing process to occur. This is because the surrounding muscles that protect the joints are being stretched gently and the vertebral disc space is being increased to allow the disc to be rehydrated and the protrusion to recede back to its original position. (Cyriax, 1950) Spinal decompression can help slow down the degenerative process of osteoarthritis, and when combined with physical therapy, the surrounding muscles, tissues, and ligaments are strengthened.
In contrast, joint and spinal mobility and flexibility are increased. Spinal decompression can also help many individuals reduce their chances of surgery, as consecutive sessions can help provide pain relief and functional improvement to the spine. (Choi et al., 2022) When people regain their spinal mobility back to their bodies from spinal decompression, they can make small changes in their daily routine to slow down the degenerative process of osteoarthritis.
References
Alkhawajah, H. A., & Alshami, A. M. (2019). The effect of mobilization with movement on pain and function in patients with knee osteoarthritis: a randomized double-blind controlled trial. BMC Musculoskelet Disord, 20(1), 452. https://doi.org/10.1186/s12891-019-2841-4
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Molnar, V., Matisic, V., Kodvanj, I., Bjelica, R., Jelec, Z., Hudetz, D., Rod, E., Cukelj, F., Vrdoljak, T., Vidovic, D., Staresinic, M., Sabalic, S., Dobricic, B., Petrovic, T., Anticevic, D., Boric, I., Kosir, R., Zmrzljak, U. P., & Primorac, D. (2021). Cytokines and Chemokines Involved in Osteoarthritis Pathogenesis. Int J Mol Sci, 22(17). https://doi.org/10.3390/ijms22179208
Wood, M. J., Miller, R. E., & Malfait, A. M. (2022). The Genesis of Pain in Osteoarthritis: Inflammation as a Mediator of Osteoarthritis Pain. Clin Geriatr Med, 38(2), 221-238. https://doi.org/10.1016/j.cger.2021.11.013
Yao, Q., Wu, X., Tao, C., Gong, W., Chen, M., Qu, M., Zhong, Y., He, T., Chen, S., & Xiao, G. (2023). Osteoarthritis: pathogenic signaling pathways and therapeutic targets. Signal Transduct Target Ther, 8(1), 56. https://doi.org/10.1038/s41392-023-01330-w
As the body ages, individuals want to stay active and maintain a healthy pain free lifestyle. Can regenerative cells for arthritis and cartilage damage be the future of neuromusculoskeletal medicine and joint healing?
Regenerative Cells For Arthritis and Cartilage Damage
Individuals want to continue to do the physical activities they love, which require healthy joints. Scientists are learning how to harness the abilities of regenerative cells to repair and regrow damaged and deteriorated cartilage. Current stem cell treatment of cartilage problems has not been shown to reverse the effects of arthritis and while studies show clinical improvement, further research is necessary. (Bryan M. Saltzman, et al., 2016)
Cartilage and How It Gets Damaged
Cartilage is a type of connective tissue. In the joints, there are a few types of cartilage. The most commonly referred to is the smooth lining known as articular or hyaline cartilage. This type forms a smooth layer of cushion on the end of a bone at the joint. (Rocky S. Tuan, et al., 2013)
The tissue is very strong and has the ability to compress and absorb energy.
It is very smooth allowing a joint to glide effortlessly through a limb’s range of motion.
When joint cartilage is damaged, the cushioning can wear down.
In traumatic injuries, a sudden force can cause the cartilage to break off and/or suffer damage, that exposes the underlying bone.
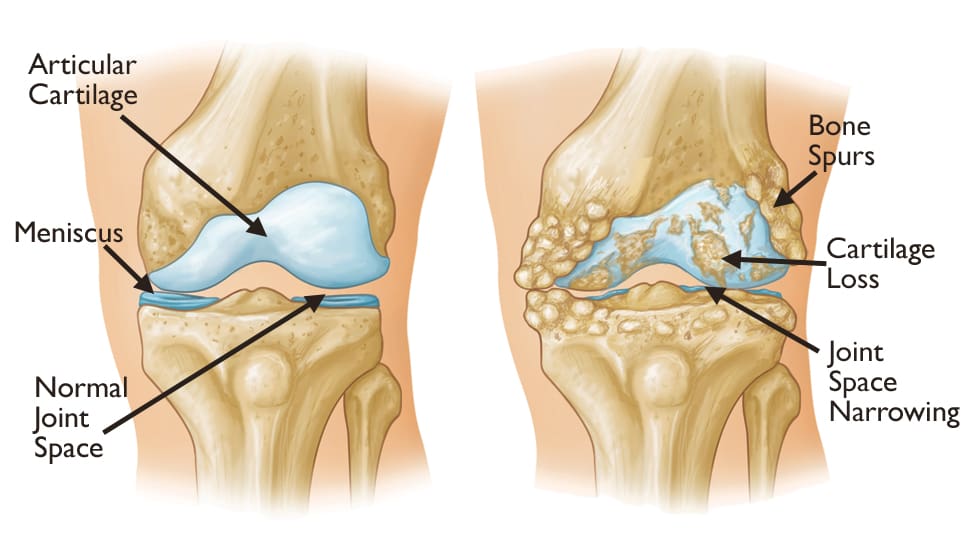
In osteoarthritis – degenerative or wear-and-tear arthritis, the smooth layer can wear down thin and unevenly.
Eventually, the cushion wears away, the joints become inflamed and swollen and movements become stiff and painful.
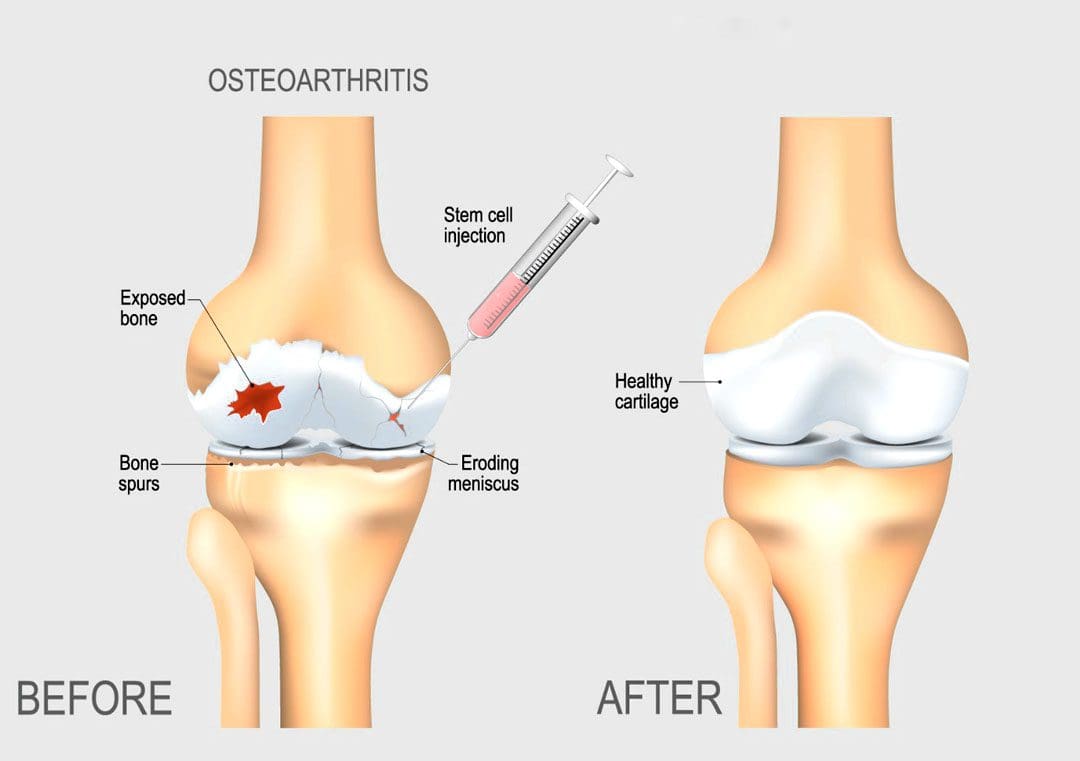
There are treatments for arthritis and cartilage damage, but these treatments are usually focused on relieving symptoms by smoothing down the damaged cartilage or replacing the joint surface with an artificial implant, like knee replacement or hip replacement surgeries. (Robert F. LaPrade, et al., 2016)
Regenerative Cells
Regenerative stem cells are special cells that have the ability to multiply and develop into different types of tissue. In an orthopedic surgery setting for joint problems, stem cells are obtained from adult stem cell primary sources which are bone marrow and fatty tissue. These cells have the ability to develop into cartilage cells, called chondrocytes. (Rocky S. Tuan, et al., 2013)
They also help by stimulating the body to reduce inflammation, stimulate cell repair, and improve blood circulation.
This process is caused by cellular signals and growth factors to stimulate the body to activate the healing processes.
Once stem cells have been obtained, they need to be delivered to the area of cartilage damage.
Cartilage is a complex tissue that is described as a scaffold structure that is composed of collagen, proteoglycans, water, and cells. (Rocky S. Tuan, et al., 2013)
To regenerate cartilage, the complex tissues must also be reconstructed.
There are studies on types of tissue scaffolds engineered to recreate a similar type of cartilage structure.
The stem cells can then be injected into the scaffold, in hopes of restoring a normal type of cartilage.
Non-Surgical Arthritis Treatments
Standard treatments such as cortisone shots or physical therapies work as well and provide benefits that could be utilized in combination with regenerative cells for arthritis and cartilage damage in the near future. Data takes time and therefore how this impacts the long-term health of a joint needs continued research in terms of tissue engineering and cell delivery to determine the best approach to help individuals.
Arthritis
References
LaPrade, R. F., Dragoo, J. L., Koh, J. L., Murray, I. R., Geeslin, A. G., & Chu, C. R. (2016). AAOS Research Symposium Updates and Consensus: Biologic Treatment of Orthopaedic Injuries. The Journal of the American Academy of Orthopaedic Surgeons, 24(7), e62–e78. https://doi.org/10.5435/JAAOS-D-16-00086
Saltzman, B. M., Kuhns, B. D., Weber, A. E., Yanke, A., & Nho, S. J. (2016). Stem Cells in Orthopedics: A Comprehensive Guide for the General Orthopedist. American journal of orthopedics (Belle Mead, N.J.), 45(5), 280–326.
Tuan, R. S., Chen, A. F., & Klatt, B. A. (2013). Cartilage regeneration. The Journal of the American Academy of Orthopaedic Surgeons, 21(5), 303–311. https://doi.org/10.5435/JAAOS-21-05-303
Aging Arthritis: How the body changes as the years go by is determined by an individual’s diet, physical activity/exercise, genetics, stress levels, sleep patterns, and self-care. As the body ages, natural degeneration from everyday wear and tear will present. The focus is on understanding how age-related degeneration can affect the body and what to do to prevent and treat it.
The condition can cause long-term joint damage that can lead to disability.
Aging Arthritis and Chiropractic Care
Chiropractic care is recommended for the treatment of any form of arthritis. Chiropractic care can work with other therapies to reduce swelling and inflammation, alleviate pain, and improve mobility and flexibility.
A chiropractor will utilize body imagery before beginning treatment.
Imaging gives insight into the condition of the joints, and the visual, combined with a self-report from the individual, allows the chiropractor to create a personalized treatment plan.
Once a chiropractor has identified which techniques the body can handle, treatment will commence that can include:
Therapeutic massage
Percussive massage
Ultrasound
Electrotherapy
Low-level cold laser therapy
Infrared heat
A chiropractor’s objective is to rebalance, realign and strengthen the body, relieve pressure or stress at the junction of the joints, and expedite healing and rehabilitation.
LLT Laser Therapy
References
Abyad, A, and J T Boyer. “Arthritis and aging.” Current opinion in rheumatology vol. 4,2 (1992): 153-9. doi:10.1097/00002281-199204000-00004
Chalan, Paulina, et al. “Rheumatoid Arthritis, Immunosenescence and the Hallmarks of Aging.” Current aging science vol. 8,2 (2015): 131-46. doi:10.2174/1874609808666150727110744
Goronzy, Jorg J et al. “Immune aging, and rheumatoid arthritis.” Rheumatic diseases clinics of North America vol. 36,2 (2010): 297-310. doi:10.1016/j.rdc.2010.03.001
Greene, M A, and R F Loeser. “Aging-related inflammation in osteoarthritis.” Osteoarthritis and cartilage vol. 23,11 (2015): 1966-71. doi:10.1016/j.joca.2015.01.008
The body has a defensive response known as the immune system that comes to the rescue when traumatic events or injuries impact certain areas of the body. The immune system releases inflammatory cytokines to the affected area and begins the healing process to repair the damage while also getting rid of the foreign intruders in the body. Inflammation can be potentially beneficial and harmful to the body, depending on how severe the injury has potentially impacted the area. When inflammation begins to cause an impact on the surrounding muscles, ligaments, and joints, it can lead to chronic issues associated with pain. To that point, it causes the body to be dysfunctional while mimicking other symptoms. Today’s article examines how chronic inflammatory responses affect the joints, their associated symptoms, and how to manage chronic joint inflammation. We refer patients to certified providers specializing in anti-inflammatory treatments to help many individuals dealing with chronic inflammation of the joints. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
How Does Chronic Inflammatory Response Affect The Joints?
Have you been experiencing pain in some regions of your body? What about experiencing tenderness in your muscles? Do your joints ache when you are doing everyday activities? If you have been dealing with these issues, it might be due to chronic inflammatory responses affecting your musculoskeletal joints. As stated earlier, inflammation can be both beneficial and harmful to the body, depending on the severity of the impact the body has taken. In its beneficial form, the body activates the immune system and eliminates pathogens from bacteria, viruses, and other environmental triggers to promote healing and tissue repair. This potentially makes the affected area red and inflamed, thus repairing the damaged cells.
However, in its harmful form, studies reveal that chronic inflammatory responses can break down immune tolerance, causing significant alterations to all the tissues, organs, and joints. To that point, the residual effects of high inflammation can cause harm to the joints and cartilage, making them potentially involved with pain and possibly deformity over time. The joints help keep the body moving, surrounded by connective muscle tissue that helps stabilize the body; when chronic inflammatory responses start to affect the joints, they can become a mediator for pain and discomfort while triggering musculoskeletal disorders. Studies reveal that inflammation in the joints can cause damage to the cartilage and result in degenerative changes to the body. This includes functionality loss, joint instability, and other symptoms associated with chronic joint inflammation.
The Symptoms Associated With Chronic Joint Inflammation
When it comes to chronic joint inflammation, it can mimic other chronic conditions that present joint instability while overlapping different chronic disorders. This makes diagnosing difficult, especially if the person is dealing with inflammation on one side of their body, but it affects another part. This is known as referred pain, and studies reveal that most inflammatory forms that affect the joints are sometimes arthritic and have systemic symptoms that may occur in different body areas. Some of the symptoms associated with chronic joint inflammation can include:
Swelling
Stiffness
Grinding sounds
Difficult mobility
Numbness
Joint deformity
The Difference Between Healthy Joints & Inflamed Joints-Video
Have you been dealing with joint pain throughout your life? Do you feel muscle stiffness in certain areas when you move around? Or do you feel muscle tenderness in certain areas? Many of these symptoms are associated with joint inflammation, potentially overlapping with musculoskeletal pain. The video above explains the difference between healthy joints and inflamed joints. Healthy joints are utilized when the surrounding muscles are strong and functional while no pain is inflicted on the body. Inflamed joints may be caused by numerous factors like lifestyle habits, physical inactivity, or previous conditions associated with inflamed joint pain. Studies reveal that inflammatory cytokines may potentially amplify musculoskeletal discomfort that affects the musculoskeletal tissues that surround the joints. To that point, inflammation of the musculoskeletal system may overlap with joint pain, thus directly impacting a person’s quality of life. Fortunately, there are ways to manage chronic joint inflammation and restore a person’s health and wellness.
Managing Chronic Joint Inflammation
Since inflammation is beneficial and harmful to the body, there are different ways to manage chronic inflammatory markers triggering joint pain. Many individuals who want to lower inflammation in their joints will begin to incorporate natural ways to lessen the pain. Eating foods high in fiber may potentially help lower inflammatory markers, including physical activities to improve musculoskeletal and joint stability and utilizing chiropractic care. Studies reveal that chronic joint inflammation associated with pain does affect a person’s ability to sleep and emotional health. To that point, incorporating treatments to manage inflammatory effects may potentially improve a person’s self-efficacy. Now how does chiropractic care help manage chronic joint inflammation? Chiropractic care includes inflammation reduction techniques that help loosen the stiff muscles that surround the inflamed joints. Joint inflammation may also be due to subluxation (spinal misalignment) associated with environmental factors. Utilizing chiropractic care not only alleviates the symptoms caused by joint inflammation but may potentially alleviate the cause of inflammation. Once a person has completed their chiropractic care treatment, they can return to normal activities without the risk of re-injury and re-inflammation.
Conclusion
Inflammation in the body can be beneficial and harmful depending on the impacted area. The body unleashes inflammatory cytokines when a traumatic event or injury has occurred in certain body areas. This is due to the immune system naturally responding to the damaged cells, thus causing the area to be red, hot, and swollen to promote healing. To that point, inflammation can impact the surrounding muscles, ligaments, and joints, which can lead to chronic issues associated with pain. Chronic joint inflammation is residual high inflammatory effects that cause harm to the cartilage and joint structures, thus making them potentially involved with pain and possible deformity. Fortunately, treatments like high fiber and anti-inflammatory foods, getting enough exercise, and chiropractic care may help manage chronic joint inflammation and its associated pain symptoms. This way, many individuals can resume their normal activities.
References
Furman, David, et al. “Chronic Inflammation in the Etiology of Disease across the Life Span.” Nature Medicine, U.S. National Library of Medicine, Dec. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7147972/.
Kim, Yeesuk, et al. “Diagnosis and Treatment of Inflammatory Joint Disease.” Hip & Pelvis, Korean Hip Society, Dec. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5729162/.
Lee, Yvonne C. “Effect and Treatment of Chronic Pain in Inflammatory Arthritis.” Current Rheumatology Reports, U.S. National Library of Medicine, Jan. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3552517/.
The hips in the lower extremities of the body help stabilize the weight of the upper half while providing movement to the lower half. The hips also allow the body to twist, turn, and bend back and forth. The hip joints connect to the inside of the pelvic bone, while the pelvic bone is connected to the sacroiliac joint, which connects to the spine. When natural wear and tear affects the joints as the body ages, issues like hip pain and osteoarthritis associated with low back pain occur, causing various symptoms to arise in the body. Today’s article looks at osteoarthritis, how it impacts the hips, and how to manage hip osteoarthritis. We refer patients to certified providers specializing in musculoskeletal therapies to help those with hip pain and osteoarthritis. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Osteoarthritis?
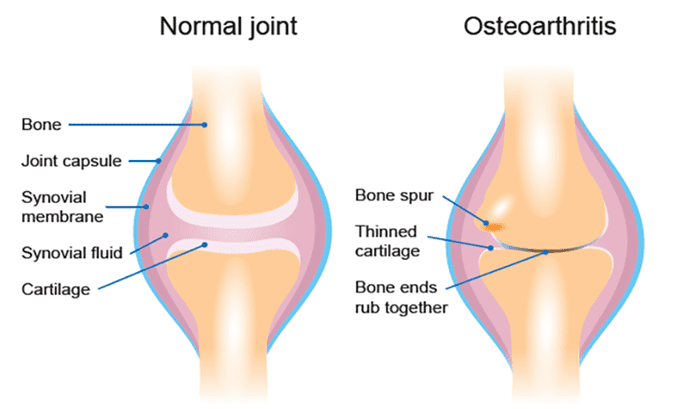
Have you been experiencing pain in your hips or lower back? How about muscle stiffness near the groin? Do symptoms associated with sciatica seem to flare up near your hips and the back of your leg? Many of these symptoms are signs that you could be at risk of developing osteoarthritis near your hips. While arthritis refers to inflammation of the body’s joints, osteoarthritis is a type of arthritis that causes degeneration of the joint cartilage, triggering joint pain and functionality loss. Even though there are several hundred types of arthritis, osteoarthritis is one of the most common types that many people, especially older adults, are affected by. As the body becomes older naturally through age, the repairs from an injury begin to slow down, and the cartilage (the connective tissue that protects the bones from each other) will start to thin out, triggering bone rubbing together, causing inflammation to occur, bone spurs, and inevitable pain. Osteoarthritis is often associated with old age and is multifactorial as factors that can increase the risk of developing osteoarthritis include:
Sex
Age
Obesity
Joint injuries
Genetics
Bone deformities
How Does It Impact The Hips?
Since osteoarthritis affects the joints, how does it cause an impact on the hips? When health issues affect the body, it can cause painful symptoms to gradually worsen and become a risk of developing hip pain. Studies reveal that hip pain is common in all adults and activity levels in the anterior, lateral, or posterior regions near the hips.
Anterior hip pain: Causes referred pain (pain felt in one part of the body but is actually in a different location) associated with internal organ systems.
Lateral hip pain: Causes wear-and-tear pain on the soft muscle tissues on the sides of the hips.
Posterior hip pain: Causes referred pain associated with the lumbar spinal pathology like sciatic nerve entrapment correlating with a deep gluteal syndrome.
All these issues affecting the hips overlap with various issues associated with osteoarthritis. When hip pain originates from osteoarthritis, factors like minimal physical activity or slight movements while resting in bed can worsen due to the hip joints having limited or restricted movement. Studies reveal that hip pain is associated with simple movement impairments that make it difficult to diagnose due to referred pain from the spine, knees, or even the groin area.
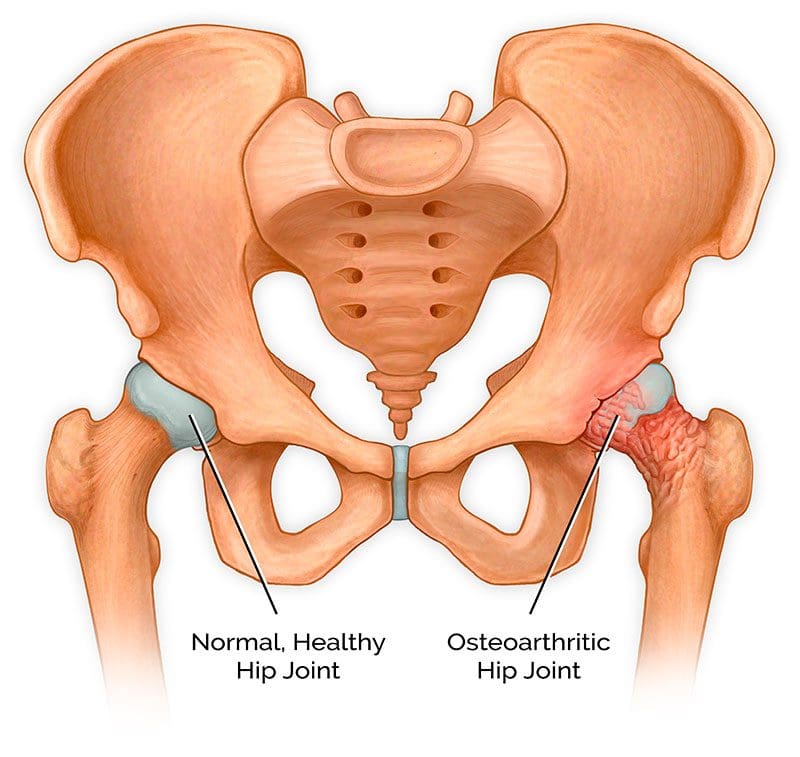
How does hip osteoarthritis correlate with groin pain? Studies reveal that when a person is dealing with hip osteoarthritis, groin and buttock pain are slightly more common. The hip joint is behind the groin muscle, which is why groin pain overlaps with hip pain as the root. Hip and groin pain could also be involved with radiating pain down toward the knees in the body.
Exercises For Hip Osteoarthritis- Video
Are you experiencing bladder issues? How about stiffness near or around your hips and groin area? Do issues like low back and sciatica pain? Experiencing these issues could be signs of hip osteoarthritis affecting your lower body. Studies reveal that hip osteoarthritis is a significant source of morbidity, pain, gait abnormalities, and functional impairments potentially involved with other issues. Fortunately, there are ways to manage hip osteoarthritis, as the video above shows eight great exercises for hip osteoarthritis. Certain exercise moves for individuals with hip osteoarthritis can help strengthen the surrounding muscles around the joints while increasing joint mobility to reduce pain and stiffness. Exercising can also be beneficial to the individual as it can provide:
Increase blood circulation
Maintain weight
Provides energy boost
Improves sleep
Promotes muscle endurance
Other available therapies help manage hip osteoarthritis while alleviating associated symptoms affecting the body.
Managing Hip Osteoarthritis Pain
Many individuals suffering from hip osteoarthritis try to find ways to relieve the pain. While they can’t do anything to prevent wear and tear on the joints completely, there are ways to slow down the process and manage hip osteoarthritis in the body. Small changes like incorporating food can dampen inflammatory effects on the joints while providing nutrients to the body. An exercise regime can help strengthen the weak muscles supporting the joints while increasing mobility and range of motion. Treatments like spinal traction and chiropractic care relieve pain and stiffness from joint disorders like osteoarthritis. Chiropractic care provides spinal manipulation on the back and joints to be adjusted. While spinal traction helps the compressed discs lay off the pressure on the surrounding nerves associated with hip pain. Incorporating any of these can help slow the progression of hip osteoarthritis and bring back mobility to the hips.
Conclusion
The hips provide stability to the upper and lower parts of the body. While supporting the weight of the upper half and movement to the lower half, the hips can succumb to wear and tear in the body. When the hip joints begin to wear and tear slowly, it can lead to the progression of hip osteoarthritis, where the cartilage of the joints begins to cause the bones to rub against each other, triggering inflammation. Hip osteoarthritis makes diagnosing difficult because the referred pain from the spine, knees, or groin area overlaps the symptoms. All is not lost, as there are available treatments to manage hip osteoarthritis that can help slow the progress of this disorder and bring back the mobility of the lower half of the body.
References
Ahuja, Vanita, et al. “Chronic Hip Pain in Adults: Current Knowledge and Future Prospective.” Journal of Anaesthesiology, Clinical Pharmacology, Wolters Kluwer – Medknow, 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022067/.
Chamberlain, Rachel. “Hip Pain in Adults: Evaluation and Differential Diagnosis.” American Family Physician, 15 Jan. 2021, https://www.aafp.org/pubs/afp/issues/2021/0115/p81.html.
Khan, A M, et al. “Hip Osteoarthritis: Where Is the Pain?” Annals of the Royal College of Surgeons of England, U.S. National Library of Medicine, Mar. 2004, https://pubmed.ncbi.nlm.nih.gov/15005931/.
Kim, Chan, et al. “Association of Hip Pain with Radiographic Evidence of Hip Osteoarthritis: Diagnostic Test Study.” BMJ (Clinical Research Ed.), BMJ Publishing Group Ltd., 2 Dec. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4667842/.
Sen, Rouhin, and John A Hurley. “Osteoarthritis – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 1 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK482326/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine