Most of us have heard the adage connected with physicians’ medical advice: “Take two aspirin and call me in the morning.” Imagine a scenario in which, instead of offering a fast cure, the doctor sat down with you and inquired about the elements of your lifestyle. That’s what physicians who exercise functional medicine do. They are also medical doctors. What they have in common is that they take a holistic approach to your well-being.
What is Patient-Centered Healthcare?
The term “patient-centered healthcare” is becoming popular in the last decade. You might ask yourself, shouldn’t healthcare always center on the individual? This concept, which is an integral value in functional medicine, means physicians focus on the entire person rather than on a disease or disease. Rather than finding the way to eradicate symptoms, the functional medicine doctor searches for the origin of the individual’s problem. These doctors recognize each patient’s identity rather than taking a one-size-fits-all strategy.
Mind, Body and Spirit in Functional Medicine
Functional medicine physicians probe deeper than just finding out what is going on physically with their own patients. They can ask you about your spiritual and emotional health, and want to learn about your relationships with loved ones and partners. They aim to make the most of your overall health and wellness.
Cost Effective Disease Prevention
Preventing a disorder is significantly more cost effective than treating one. By minimizing damage done by poor nutrition, stress and exposure to environmental toxins and preserving your well-being, functional medicine doctors can save you money altogether. In all this, where does chiropractic fit in?
Chiropractic care is one aspect of comprehensive functional medicine, since it helps patients achieve optimum health. Furthermore, concepts of medication fit into chiropractors’ clinics, since they optimize their tools to treat patients.
Some chiropractors chiefly focus on conventional spinal adjustments and manipulations. However, others have included these elements to the chiropractic practice that they offer, in accordance with the fundamentals of medicine. These may include counseling and lifestyle interventions. This integrated approach is especially popular with complex but common disorders, such as fibromyalgia and chronic fatigue syndrome.
Functional medicine chiropractors work together with other practitioners to maximize patients’ health. For instance, a chiropractor may refer a patient to an acupuncturist for additional help. The acupuncturist may send the chiropractor their patients. They work with each other, focusing on the patient’s best interests.
?
Things to Expect From a Functional Medicine Chiropractor
Patients are often surprised by how long a practical medicine chiropractor spends with them. Expect a much longer visit than you’d get from your typical MD. The staff will probably ask you to complete questionnaires about your diet history, exposure to symptoms, past illnesses and toxins. Your functional medicine doctor might order lab tests too.
The individual has an active role in functional medicine. You may work with your physician to boost your health, frequently by altering your diet and lifestyle, rather than passively taking medications to relieve existing symptoms.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
A chiropractic adjustment, also commonly referred to as spinal manipulation, manual manipulation, or chiropractic manipulation, is a curative treatment frequently utilized for chronic pain, such as lower back pain.
What is a chiropractic adjustment?
A chiropractor applying manipulation into the vertebrae that fail to function or have abnormal movement patterns is referred to as a chiropractic adjustment. The goal of this chiropractic treatment is to decrease the subluxation, or misalignment, with the focus of increasing range of movement, reducing nerve wracking and improving function.
Chiropractic Adjustment Description
A chiropractic adjustment typically involves:
A high velocity, short lever arm thrust applied to a vertebra
An accompanying, perceptible discharge of gas (joint cavitation) that is brought on by the release of oxygen, nitrogen and carbon dioxide, that releases joint pressure (cavitation).
An alleviating sensation the majority of the time, though minor distress has been reported (that generally lasts for a brief time period) if the surrounding muscles are in spasm or the patient tenses up during the adjustment.
It ought to be known that joint cavitation or cracking doesn’t happen at times, typically as a result of significant muscle splinting or the individual not being adequately relaxed during the chiropractic manipulation. At times such as this, it is sometimes best for your chiropractor to apply ice, have the patient break, or perform electrical stimulation and massage prior to trying the adjustment, to ensure the treatment modality is effective.
Chiropractic Adjustment Techniques
There are several different manipulative methods that can be utilized in chiropractic care, and there’s a specific ability level and “art” involved in high velocity, low amplitude modification or manipulation. It’s perhaps more important for the chiropractor to determine when to not apply the adjustment.
Chiropractic Adjustment Side Effects
The most frequent response to a chiropractic adjustment is soreness or aching in the spinal joints or muscles. If this soreness or aching happens, it does not last longer than 24 hours and is typically within the first few hours post-treatment. The symptoms are frequently reduced by application of an ice pack.
Other Chiropractic Services Beyond Adjustments
The focus on spinal adjustment is the thing that makes doctors of chiropractic unique in their approach to treating patients with spinal complaints. The adjustment, however, may not be the only procedure a chiropractor uses.. For example, chiropractic care has utilized drugless therapeutics (natural remedies) since as early as 1912.
Natural agents like heat, cold, water, massage, light, and exercise are a few of the physiological curative steps which are frequently utilized by chiropractors. When controlled, other and these components can aid a number of common lower back pain problems and exert a beneficial influence on body functions.
Common Alternatives of Chiropractic Care
Some physiological therapeutic measures Which Are often used in chiropractic care include:
Cold and Heat. Chiropractors may alternate between heat and ice therapy to help patients treat back pain. Ice packs can be used to numb the back to get a 10 to 15 minute period and then switched using hot water bottle, heat wrap or a heating pad promote faster recovery and to restore blood flow.
Exercise. Chiropractors can provide patients with directions for an exercise program focusing on strengthening and extending the back, to improve overall health and function alongside other treatments.
Massage. Chiropractors may massage the tissues to improve circulation, reduce inflammation and swelling associated with the pain, and encourage recovery.
Dietary management. Chiropractors will supply patients with tips on how an improved diet may help with their pain, and some could recommend dietary supplements after manipulation.
Ultrasound. With ultrasound, sound waves create heat treatment that is applied to the soft tissues and joints. Basically micro-massaging the delicate tissues and joints, ultrasound therapy doesn’t only help reduce back stiffness, pain, and migraines, but increase blood circulation and accelerate the healing process.
Diathermy. A form of shortwave therapy that passes the softer tissues and provides warmth to denser tissues, hastens the healing process by increasing circulation, decreases muscle spasms, and diathermy relaxes the muscles and connective tissues. In chiropractic therapy using diathermy, the treated area will feel pleasantly warm.
Hydrotherapy. Using water and changing its own temperature and pressure through saunas, whirlpools, baths or wraps, and hydrotherapy concentrates on the human body’s recovery response for back pain. In chiropractic, hydrotherapy may be used to reduce the sensitivity of pain through stimulation that soothes the pain and using hot stimuli to promote recovery and blood circulation.
Electrical muscle stimulation. During this chiropractic therapy, electrodes are placed on the skin which send mild pulses to different regions of the body with the purpose of curtailing muscle spasms, decreasing inflammation and relieving pain back.
Transcutaneous electric nerve stimulators (TENS). The most common form of electrical stimulation, TENS units contain electrodes that are placed using the power to control the intensity of stimulation. It is believed that TENS help prevent the transmission of pain signals and also discharge endorphins, the body’s natural painkillers.
Traction. A chiropractic traction massage could include the patient lying face upward about the back, all of the while stretching and massaging the muscles in the back as a method of rollers maneuver. Chiropractors may use other traction devices that stretch the backbone, decompress the disks and reduce the strain on the nerve roots (a procedure called non-surgical spinal decompression).
Infrared radiation. In chiropractic, a camera may be utilized to image colors indicating the blood circulation in the back. From the body images, reddish shades would indicate IR radiation and blood circulation for instance. Radiation may be used by chiropractors to evaluate conditions which are causing pain back and to distinguish temperature fluctuations from abnormal differences.
Cold laser therapy. After penetrating the skin surface, with cold laser therapy, particles of energy are carried at a laser and absorbed by the photograph receptors of the cell membrane. Tissues and the cells then convert this light energy inducing a biological process that’s thought to decrease swelling, reduce back pain and inflammation, and enhance circulation.
Ergonomics. During the course of care, the chiropractor may recommend some modification like a work station change that is applied at home and/or on the job. The failure or success of obtaining satisfying that is patient outcome may be related to employing an alteration or a hobby-related bothersome activity.
Pelvic stabilization. When deficiency feet and/or subtalar instability are present, the nurse may place a little heel lift in the shoe on the short leg side or urge arch supports to help stabilize the pelvis.
Patient education. A chiropractor can advise a number of lifestyle modifications, including nutritional and diet programs, self-care and working strategies, to the individual experiencing back pain.
These methods may or may not be utilized by the therapist at the duration of a patient’s situation management depending upon their particular needs.
Chiropractic Manipulation and Therapies
Utilizing specific manipulations (chiropractic adjustments) together with one or a combination of the aforementioned, the physician’s aim is to get rid of structural or nervous system discomfort which could possibly be a major contributing element in a patient’s lower back pain, improving the patient’s overall well-being.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Chiropractic is a healthcare profession devoted to the nonsurgical treatment of ailments of the nervous system and/or musculoskeletal system. Chiropractors keep a focus on therapy and manipulation of surrounding structures.
What can chiropractic care treat?
Many studies have concluded that massage therapies widely used by chiropractors are effective for treating lower back pain, in addition to for therapy of lumbar herniated disk for radiculopathy and neck pain, among other ailments.
In fact, when patients using non-specific chronic low back pain have been treated by physicians, the long-term result is enhanced by obtaining maintenance spinal manipulation following the initial intensive manipulative treatment.
Core Chiropractic Treatment Plan
The center of chiropractic usually involves treatment of common lower back pain conditions through manual therapy:
Spinal manipulation and manual manipulation. This type of manual manipulation identifies a short lever arm push that is applied to vertebra. It is also commonly called “chiropractic adjustment”.
There is firm literature support for chiropractic treatment of lower back pain. Many of the guidelines that are published urge manipulation to be contained in the therapy strategy in the maintenance of back pain.
Mobilization. Mobilization describes velocity manipulation, motion and stretching of the muscles and joints, with the goal of increasing the assortment of movement.
What Does a Chiropractic Treatment Plan Consist Of?
Most chiropractors start treatment throughout the patient’s first visit, although some might wait until the next appointment of the practice. Chiropractic therapy goals and recommendations can include some or all of the following:
Adjustments to key joint dysfunctions
Modalities to enhance soft tissue healing and pain management, such as ultrasound, electric stimulation, and grip
Strengthening and/or stretching exercises to improve muscle balance, strength, and coordination
Patient instruction to improve posture and motor controller, as well as potentially reduce anxiety
Other treatments like massage, heat/cold application, and education on ergonomics and nourishment.
Goals of Chiropractic Care
The chiropractor will establish Certain goals for a patient’s individual plan for therapy:
Short-term goals typically include reducing pain and restoring normal joint function and muscle balance
Long-term targets include assigning functional independence and tolerance to normal activities of daily living.
To accomplish these goals, a particular number of chiropractic visits will be recommended.
For most kinds of lower back pain, a treatment recommendation of 1 to 3 chiropractic visits per week for 2 to 4 weeks will be prescribed, followed closely by a re-examination from the chiropractor.
Chiropractic Evaluation of the Treatment
In the re-evaluation, the chiropractic physician will Assess the response to treatment and decide whether to:
Continue chiropractic treatment, if appropriate
Release the Individual from chiropractic care, if treatment goals have been met
Refer the patient to another health care specialist if treatment goals have not been fulfilled.
Chiropractic adjustment (also referred to as spinal manipulation) is a popular and recognized pain relief therapy for many types of lower back pain, sciatica, and neck pain. Knowing what to anticipate from the first visit might help an individual get the maximal benefit from treatment.
Since this profession has an unusually large selection of practice philosophies and chiropractic methods, people should feel comfortable asking all of the questions necessary to comprehend the chiropractic examination, diagnosis, and therapy plan.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The manipulation of the cervical spine or neck is a common technique utilized by doctors of chiropractic for individuals complaining of upper back, neck, and shoulder/arm pain, in addition to headaches.
What is the benefit of cervical spinal manipulation?
Similar to the treatment for many injuries and/or conditions which affect the thoracic and lumbar spine, or back, chiropractic treatment is thought of as a first line of therapy for a range of cervical spine conditions.
Chiropractic treatment aiming for cervical spine pain management include (but aren’t limited to) a mix of:
Reducing pain
Improving movement
Restoring function into the head and neck region
Patients must be advised that the treatment will start after a complete patient history, physical examination, review of past, family histories, and review of systems are completed. Tests might include X-ray, CT, MRI, EMG/NCV, urine analysis and lab blood, referral to a professional, more, depending on each individual case demonstration.
Different Types of Chiropractic Manipulation
There are two general manipulation approaches for spine ailments:
Cervical spinal manipulation – frequently thought of as the conventional chiropractic adjustment, or even a high-velocity, low-amplitude (HVLA) technique
Cervical spinal mobilization – which can be a more gentle/less forceful modification, or even a low-velocity, low-amplitude (LVLA) technique moving the joint through a tolerable range of movement.
The combination of the many approaches varies from patient to patient depending on the healthcare professional’s preferred tactics and tastes, the patient’s comfort and tastes, and the patient’s response to the treatment, in addition to both previous experience and observations made during the course of therapy.
Chiropractors may also use therapy to treat other cervical spine complaints. Adjunctive therapies may include therapeutic heat program, massage exercises, and more. Chiropractic manipulation can handle numerous causes of neck pain. It’s not a cure for every single type of neck problem. Two causes of pain which originate in the neck and may be treated by manipulation comprise of mechanical neck pain and disc problems.
Mechanical Neck Pain
Mechanical neck pain comprises of pain associated with the tendons, joint capsules, ligaments and/or the fascia. This type of issue is a frequent cause of neck pain and stiffness.� Facet joint issues are a well-known case of mechanical neck pain. The facets are located in the back of the neck. If a facet joint is hurt or sprained, pain may be localized or may radiate along other upper extremities. The pain pattern depends upon the specific level and is unique.
Cervical Disc Issues
Tears may develop in the cervical disc and/or the inside of the disc (the nucleus) may herniate through the outer area (the annulus) and trap or pinch the nerve root as it leaves the spine.
Cervical nerve root irritation can frequently refer pain down the arm and into the hand, typically affecting particular areas like the 4th and 5th digits, the palms side thumb to 3rd fingers and/or the back of the hands on the thumb, index finger side of the hand, depending on which nerve root is irritated.
On rare occasions, if the nucleus of the disc herniates straight backward, it can compress the spinal cord and create symptoms in the legs and also impact the function of the bowels and/or bladder. On such occasions, the patient needs to be referred to a spine surgeon to get prompt care.
These are two examples of types of cervical spine conditions which may be treated with spinal manipulation. The patient needs to receive a whole exam prior to receiving any kind of manipulation.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
From acute pain, to chronic pain and neuropathic pain, when painful symptoms begin to affect you or a loved one, it becomes a priority to seek medical attention immediately to diagnose the source of the pain and begin treatment. But with so many types of injuries and/or conditions, it may often be difficult to know the exact cause without properly understanding the different types of pain and why they could affect you or a loved one.
What are the different types of pain?
Knowing how pain is defined can be beneficial in learning how to control it even better. For the purposes of study and medical clinic, pain is usually divided into three categories:
Acute Pain is Often Temporary
Pain related to tissue damage, or pain that lasts less than 3 to 6 weeks, is known as acute pain. This is the type of pain caused by a needle prick or by a paper cut. Other cases of acute pain can include:
Touching a hot stove or iron. This pain can cause an instant, intense pain with a virtually simultaneous withdrawal of the entire body part. More of the annoyance, a few moments after the initial withdrawal and pain, another kind of pain, is very likely to be experienced.
Smashing one’s finger with a hammer. This pain is similar to that of touching a hot stove in that there’s immediate pain, withdrawal, and then a “slower” aching pain.
Labor pains. The pain during childbirth is acute and the cause is identifiable.
When pain persists, it becomes even more affected by other influences, which may increase the individual’s risk of developing chronic pain. These impacts include such things as the pain signal continuing to get to the central nervous system after the tissue has healed, lack of exercise (physical deconditioning), a person’s thoughts regarding the pain, as well as psychological conditions, such as depression and anxiety.
Chronic Pain Continues After Tissue Heals
The term “chronic pain” is normally used to describe pain that lasts over three to six months, or beyond the stage of tissue recovery. This kind of pain might also be termed “chronic benign pain” or “chronic non-cancer pain,” based on the circumstance. (Chronic pain due to cancer is more of an acute or acute-recurrent kind of pain since there’s continuing and identifiable tissue damage. There’s also chronic pain because of an identifiable cause, which will be discussed subsequently). For the purposes of the discussion, the term “chronic pain” will be used.
Chronic pain is usually less directly linked to recognizable tissue structural and structural problems. Chronic back pain without a clearly ascertained cause, failed back surgery syndrome (continued pain after the surgery has fully healed), and fibromyalgia are all cases of chronic pain. Pain is a lot less well understood than acute pain.
Chronic pain can take many forms, but is often put in one of two of these main types of its own:
Pain with an identifiable cause, such as an injury. Structural spine conditions, such as spondylolisthesis, spinal stenosis, and degenerative disc disease, may lead to ongoing pain until they are successfully treated. These conditions are the result of a diagnosable problem. Spine surgery may be regarded as a treatment alternative, if the pain caused by these types of ailments has not subsided after a couple weeks or months of nonsurgical remedies. This pain may often be considered as long-term acute pain, rather than chronic pain.
Persistent pain with no identifiable cause. When pain persists after the tissue has healed and there isn’t any obvious cause of the pain which may be identified, it is often termed “chronic benign pain.”
It appears that pain can establish a pathway in the nervous system in some cases, getting the problem in and of itself. To put it differently, the nervous system may be sending a pain signal although there is no tissue damage. The system misfires and generates the pain. The pain is the disease rather than a symptom of an injury.
Neuropathic Pain Differences
In a third type of chronic pain, neuropathic pain, no signs of the initial injury remain along with the pain and may even be unrelated to an observable injury or illness. Certain nerves continue to send pain messages to the brain even though there’s no ongoing tissue damage or condition which could be causing the symptoms.
Neuropathic pain could be placed in the chronic pain group, but it has a different feel than chronic pain. The pain is referred to as severe, sharp, lightning-like, stabbing, burning, or even cold. The individual may also experience numbness, tingling, or weakness. Pain may be felt from the spine, down to the arms/hands or even legs/feet.
It is thought that harm to the motor or sensory nerves in the peripheral nervous system can possibly cause neuropathy. If the cause can be discovered and reversed, treatment may enable the nerves to heal, relieving the pain. But the pain can be harder to manage, and require more aggressive therapy, if medical care for the pain is postponed.
Treatment for neuropathic pain varies significantly in the procedures used for different kinds of back pain. Opioids (such as morphine) and NSAIDs (like ibuprofen or COX-2 inhibitors) are usually not effective in relieving neuropathic pain.
Drugs made for epilepsy or depression (anticonvulsants or antidepressants) often lessen the symptoms, and topical medications are sometimes valuable. If other approaches and medications do not offer sufficient aid, spinal cord stimulation, nerve block injections, and pain pumps might be considered for pain.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Editors Note: The information provided here was forwarded to Planet Chiropractic by a chiropractor in Texas. Far too many people (including chiropractors) are not aware of historical events that took place during the 1917 � 1918 Spanish Flu years, which involved chiropractors caring for thousands that suffered influenza infection during those times. With such a firestorm of media coverage and fear surrounding the Swine Flu Pandemic, it would be irresponsible not to attempt seeking knowledge regarding influenza events of the past.
The Official History of Chiropractic in Texas By Walter R. Rhodes, DC
Published by the Texas Chiropractic Association � 1978
CHAPTER VI: THE THREE GREAT SURVIVAL FACTORS [Excerpts by Dan Murphy, DC]
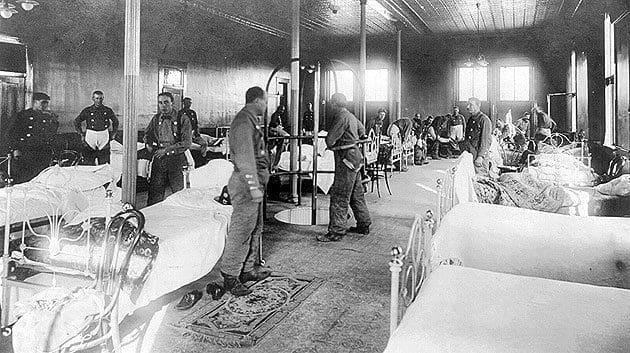
�The 1917 � 1918 influenza epidemic swept silently across the world bringing death and fear to homes in every land. Disease and pestilence, especially the epidemics, are little understood even now and many of the factors that spread them are still mysterious shadows, but in 1917-1918 almost nothing was known about prevention, protection, treatment or cure of influenza. The whole world stood at its mercy, or lack of it.�
�But out of that particular epidemic, the young science of chiropractic grew into a new measure of safety. While many struggles would lie ahead this successful passage of the profession into early maturity assured its immediate survival and made the eventual outcome of chiropractic a matter for optimism. If there had been any lack of enthusiasm among the doctors of chiropractic, or a depleting of the sources of students then the epidemic took care of them too. These chiropractic survivors of the flu epidemic were sure, assured, determined, and ready to fight any battle that came up. The effect of the epidemic becomes evident in interviews made with old-timers practicing in those years. The refrain comes repeatedly,�
�I was about to go out of business when the flu epidemic came � but when it was over, I was firmly established in practice.�
�Why? The answer is reasonably simple. Chiropractors got fantastic results from influenza patients while those under medical care died like flies all around.� �Statistics reflect a most amazing, almost miraculous state of affairs. The medical profession was practically helpless with the flu victims but chiropractors seemed able to do no wrong.�
�In Davenport, Iowa, 50 medical doctors treated 4,953 cases, with 274 deaths. In the same city, 150 chiropractors including students and faculty of the Palmer School of Chiropractic, treated 1,635 cases with only one death.�
�In the state of Iowa, medical doctors treated 93,590 patients, with 6,116 deaths � a loss of one patient out of every 15. In the same state, excluding Davenport, 4,735 patients were treated by chiropractors with a loss of only 6 cases � a loss of one patient out of every 789.�
II.
�National figures show that 1,142 chiropractors treated 46,394 patients for influenza during 1918, with a loss of 54 patients � one out of every 886.�
�Reports show that in New York City, during the influenza epidemic of 1918, out of every 10,000 cases medically treated, 950 died; and in every 10,000 pneumonia cases medically treated 6,400 died. These figures are exact, for in that city these are reportable diseases.�
�In the same epidemic, under drugless methods, only 25 patients died of influenza out of every 10,000 cases; and only 100 patients died of pneumonia out of every 10,000 cases. This comparison is made more striking by the following table:�
Influenza Cases Deaths � Under medical methods � Under drugless methods �In the same epidemic reports show that chiropractors in Oklahoma treated 3,490 cases of influenza with only 7 deaths. But the best part of this is, in Oklahoma there is a clear record showing that chiropractors were called in 233 cases where medical doctors had cared for the patients, and finally gave them up as lost. The chiropractors saved all these lost cases but 25.�
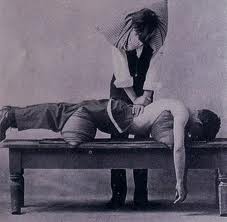
�Statistics alone, however, don�t put in that little human element needed to spark the material properly. Dr. S. T. McMurrain [DC] had a makeshift table installed in the influenza ward in Base Hospital No. 84 unit stationed in Perigau, in Southwestern France, about 85 kilometers from Bordeaux [during WWI]. The medical officer in charge sent all influenza patients in for chiropractic adjustments from Dr. McMurrain [DC] for the several months the epidemic raged in that area. Lt. Col. McNaughton, the detachment commander, was so impressed he requested to have Dr. McMurrain [DC] commissioned in the Sanitary Corps.�
III.
�Dr. Paul Myers [DC] of Wichita Falls was pressed into service by the County Health Officer and authorized to write prescriptions for the duration of the epidemic there � but Dr. Myers [DC] said he never wrote any, getting better results without medication.�
Dr. Helen B. Mason [DC], whose �son, when only a year old, became very ill with bronchitis. My husband and I took him to several medical specialists without any worthwhile results. We called a chiropractor, as a last resort, and were amazed at the rapidity of his recovery. We discussed this amazing cure at length and came to the decision that if chiropractic could do as much for the health of other individuals as it had done for our son we wanted to become chiropractors.�
Dr. M. L. Stanphill [DC] recounts his experiences: �I had quite a bit of practice in 1918 when the flu broke out. I stayed (in Van Alstyne) until the flu was over and had the greatest success, taking many cases that had been given up and restoring them back to health. During the flu we didn�t have the automobile. I went horseback and drove a buggy day and night. I stayed overnight when the patients were real bad. When the rain and snow came I just stayed it out. There wasn�t a member of my family that had the flu.�
When he came to Denison he said: �I had a lot of trouble with pneumonia when I first came. Once again took all the cases that had been given up. C. R. Crabetree, who lived about 18 miles west of Denison, had double pneumonia and I went and stayed all night with him and until he came to the next morning. He is still living today. That gave me a boost on the west side of town.�
�And when interviews of the old timers are made it is evident that each still vividly remembers the 1917-1918 influenza epidemic. We now know about 20 million persons [recent estimates are as high as 100 million deaths] around the world died of the flu with about 500,000 Americans among that number. But most chiropractors and their patients were miraculously spared and we repeatedly hear about those decisions to become a chiropractor after a remarkable recovery or when a close family member given up for dead suddenly came back to vibrant health.�
�Some of these men and women were to become the major characters thrust upon the profession�s stage in the 20�s and 30�s and they had the courage, the background and the conviction to withstand all that would shortly be thrown against them� [including being thrown in jail for practicing medicine without a license].
�The publicity and reputation of such effectiveness in handling flu cases also brought new patients and much acclaim from people who knew nothing of chiropractic before 1918.�
IV.
�The first survival factor for chiropractic: they were the legal and legislative salvation. But the fabulous success of chiropractic in combating the 1917-1918 influenza outbreak was the public relations breakthrough that can certainly be called the second great survival factor. Better acceptance by the public followed and more patients meant financial safety for practicing chiropractors. Dedicated chiropractors came into the profession in increasing numbers and they had a sure sense of certainty, heady conviction, and a great willingness to fight for the cause.�
Other Texas Chiropractic History (view more at chirotexas.com)
1916 � Texas State Chiropractic Association Formed
1916 � First TSCA annual convention held at the St. Anthony Hotel in San Antonio
1917 � First chiropractic bill introduced into Texas Legislature
1923 � Second chiropractic bill introduced into Texas Legislature
A range of factors can play an essential part in the experience of chronic pain. Pain is the body’s normal reaction to an injury or illness, But for many people, pain can be a constant.
When pain lasts for 3 to 6 months or more, it�s called chronic pain. If you hurt day after day, it can take a toll on your emotional and physical health. And, if your emotional and physical health are affected, a variety of fundamental microorganisms can be affected as well. In order to maintain overall health and wellness, following a biocentric approach can often help best understand the impact of maintaining the health of every part which makes the human body. It may be beneficial to view this model to conceptualize the complex nature of this frequent condition.
Tissue Damage
This is damage or injury to the tissue which often generally can be the start of pain. The tissue damage causes input to the nervous system, commonly identified as the pain signal. This is also termed as “nociceptive input.” Each cell in the body comes together to form a variety of complex tissues, which independently come together to form organs and other important structures, each in charge of performing essential functions for the body.
Biocentrism,�the view or belief that the rights and needs of humans alone are not more important than those of other living things, explains how taking care of every single structure in the body, such as the cells which form tissues, even including microorganisms, can ensure the well-being of the body as a whole. Damaged tissues can often be a sign of a deeper issue within the human body. Tissue damage can be additionally caused by a variety of other issues.
Pain Sensation
In the simplest terms of this model, pain sensation is the actual perception that occurs in the brain following the nerve signals, due to nociception, which travel from the periphery into the central nervous system. Whilst nociception occurs at the site of injury, pain sensation is experienced in the brain. The human body is not simply a single organism, it is comprised of a wide variety of microorganisms, many of which help maintain the well-being of the nervous system.
Thoughts
Cognitions or ideas occur and are an assessment of the pain sensation signal coming into the nervous system as well as events surrounding it. These thoughts can be unconscious or conscious and will influence the way pain signals are perceived. For example, general body aches and stiffness are traditionally considered to be “good pain” when those happen after a vigorous exercise session, whereas they’re perceived as bad pain when related to a health illness, such as fibromyalgia,�a chronic disorder characterized by widespread musculoskeletal pain, fatigue, and tenderness.
Emotions
The psychological component of pain is a person’s response to thoughts about the pain. If you believe (thoughts) that the pain is a serious danger (e.g. a tumor), subsequently emotional responses will incorporate fear, depression, and anxiety, amongst others. If you believe the pain isn’t a threat, then the psychological response will probably be negligible. Chronic pain has been a misunderstood condition and it’s effects have been reported to cause an array of emotional as well as mental disorders, due to the difficult ability to assess such conditions.
Suffering
The term “suffering” is often employed as a synonym for “pain” even though they’re theoretically and conceptually distinct. For example, a broken bone might cause pain without discomfort (since the individual knows the pain isn’t deadly and the bone will heal). By comparison, bone pain due to a tumor might cause the identical pain for a break but the distress will be much greater because of the “meaning” behind the pain (that tumor could be life-threatening). Suffering is connected to the psychological component of pain. For certain conditions which cause chronic pain, often seen in patients with fibromyalgia, a condition believed to have no cure, the fact alone that the individual’s symptoms of discomfort will never “go away” can implement a great deal of suffering.
Pain Behaviors
Pain behaviors are defined as things people do if they are in pain or suffer. These are behaviors that others observe as indicating pain, like limping, grimacing, talking about the pain, moving and taking pain medication. Pain behaviors are in reaction to all the other facets in the pain system model (tissue damage, pain feeling, thoughts, emotions, and distress). Life experiences, expectations, and ethnic influences also affect pain behaviors of the way the pain is expressed in terms. Interestingly, pain behaviors are also influenced by the environment, like how others react.
According to biocentrism, taking care of the environment, including taking care of all forms of life, such as its plants and animals, among others, is ultimately important towards the health and wellness of every organism. For example, if the food we eat is being properly taken care of, its full benefits can be properly absorbed. Nutrition is an important contributing factor for people with chronic pain. A balanced nutrition, consisting of healthy products, can help.
Additionally,�the�psychosocial environment includes each of the environments where an individual resides, works, and plays. Studies have consistently proven that these surroundings influence how an individual will reveal pain behaviors.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine