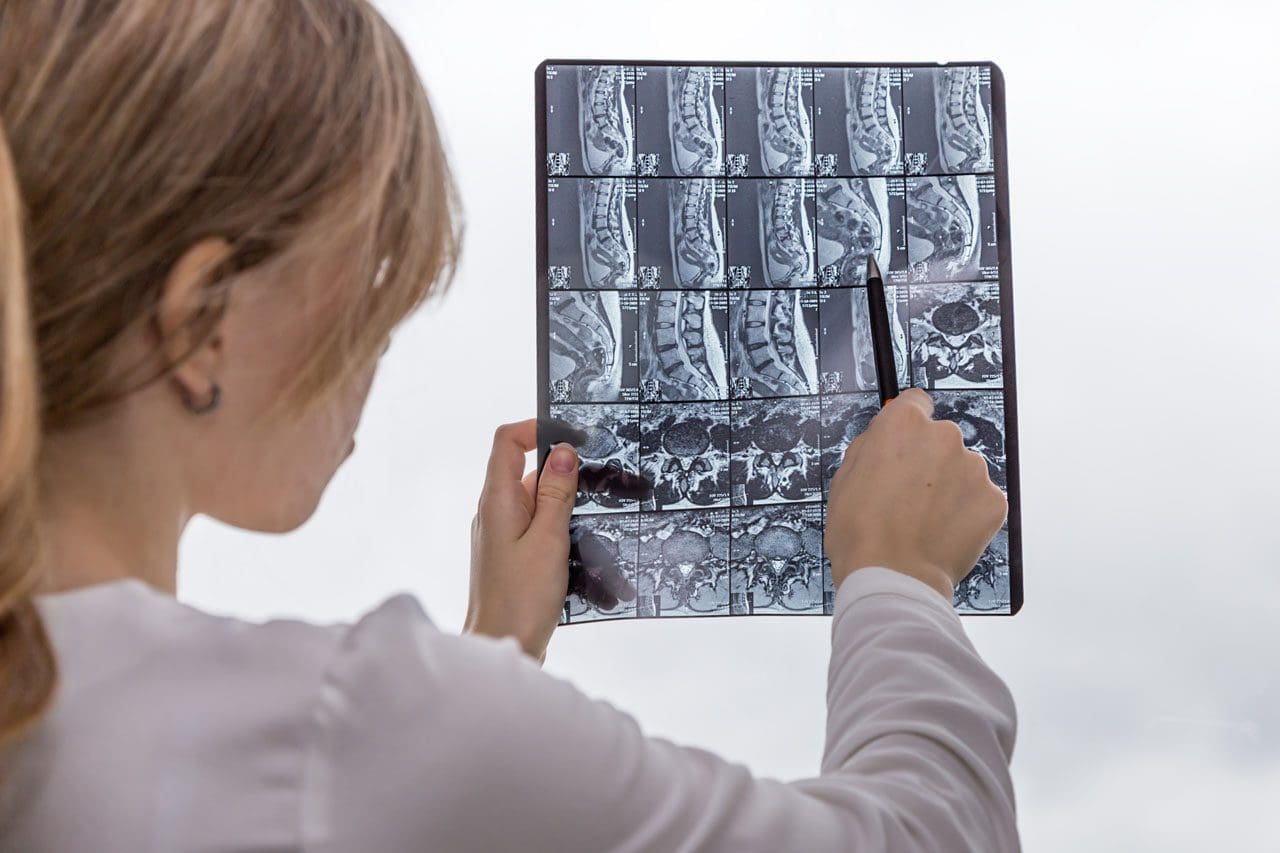
How Telemedicine Can Assist in the Management of Sciatica (with Integrative Chiropractic Care)
A man at home consults a chiropractor via telemedicine for back pain and sciatica.
Sciatica can make even simple tasks—like getting out of bed, sitting at a desk, or driving—feel almost impossible. When pain shoots down your leg or feels like burning, stabbing, or tingling, the idea of driving across town to sit in a waiting room can be overwhelming.
Telemedicine offers a way to get expert help for sciatica without leaving home. Telemedicine can significantly improve the quality of life for many individuals experiencing limited mobility or frequent flare-ups of pain. Spine specialists and integrative chiropractic teams now use secure video visits to evaluate symptoms, design treatment plans, and follow patients through recovery. UT Southwestern Medical Center+1
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a dual-licensed chiropractor and nurse practitioner in El Paso, Texas. His integrative model combines medical decision-making (such as imaging and prescriptions) with chiropractic and functional medicine. This blended approach fits perfectly with telemedicine because it allows him to assess nerve pain, guide movement, and adjust treatment plans over time—even when the patient is at home. El Paso, TX Doctor Of Chiropractic
What Is Sciatica?
Sciatica is not a disease by itself. It is a pattern of symptoms caused by irritation or compression of the sciatic nerve. This nerve starts in the lower back, runs through the hips and buttocks, and travels down each leg.
Common symptoms include:
Sharp or burning pain in the lower back, buttocks, and legs
Numbness, tingling, or “pins and needles” in the leg or foot
Weakness when trying to stand, walk, or lift the leg
Pain that worsens with sitting, coughing, or bending
Sciatica is usually caused by:
Herniated or bulging discs pressing on a nerve root
Spinal stenosis (narrowing of the spinal canal)
Degenerative disc disease
Muscle or joint dysfunction in the pelvis and lower back
Less commonly, tumors, infections, or serious conditions
Because sciatica can have many causes, proper evaluation and treatment planning are very important—this is where telemedicine can help you start sooner and stay on track.
What Is Telemedicine and How Does It Work for Back and Nerve Pain?
Telemedicine (also called telehealth) is health care delivered via secure video or phone rather than an in-person visit. You use a smartphone, tablet, or computer to speak with your provider, similar to a video call with family or friends.
Clinics that treat spine and nerve problems have made telemedicine a core part of their care model. They use it for first visits, follow-ups, second opinions, and surgical planning, especially for conditions like back pain, neck pain, and sciatica. UT Southwestern Medical Center+1
During a typical telemedicine visit for sciatica, your provider can:
Ask detailed questions about your pain pattern
Watch how you move on camera
Guide simple movement and strength tests
Review MRI, X-ray, or CT results
Explain treatment options, including chiropractic, physical therapy, injections, or surgery if needed
Many clinics report that they can accurately diagnose spine issues through video visits and that most telemedicine-based surgical plans do not require major changes after in-person exams. UT Southwestern Medical Center
Why Telemedicine Is Especially Helpful for Sciatica
People with sciatica often have trouble sitting, driving, or walking long distances. Telemedicine meets them where they are—literally.
Key benefits for sciatica patients
Less travel and less pain getting to care
No long car rides or sitting in waiting rooms
Easier for patients who have mobility issues or rely on others for transportation Southeast Texas Spine+1
Faster access to evaluation and treatment
Many clinics can schedule telemedicine visits sooner than in-person visits
You can start treatment earlier instead of waiting weeks to be seen
Better continuity of care
Telemedicine makes it easier to attend follow-ups, especially during long recovery plans
Providers can adjust medications, exercises, and activity limits in real time Southeast Texas Spine+1
Home-based evaluation of your real environment
Your provider can see your work setup, couch, bed, or home office
Straight-leg raise or seated leg raise while on camera
Heel and toe walking to assess nerve strength
Balance and gait observation
Imaging and tests
Your nurse practitioner or physician can order MRI, X-rays, or CT scans when needed
They may also recommend nerve tests (EMG/NCS) through in-person referrals
Spine centers and orthopedic clinics report that telemedicine visits can help determine when conservative care is sufficient and when urgent in-person care or surgery is needed. UT Southwestern Medical Center+1
Integrative Chiropractic Telemedicine for Sciatica
Integrative chiropractic telemedicine combines:
Medical care—history, diagnosis, imaging orders, prescriptions, and referrals
Chiropractic care—movement analysis, spinal and pelvic mechanics, and guided home-based therapies
Dr. Jimenez’s dual-scope role as a chiropractor and nurse practitioner is a strong example of this model. In his practice, he uses telemedicine to:
Review MRI and other imaging results with patients
Coordinate conservative care (chiropractic, physical therapy, massage, acupuncture, and functional medicine)
Monitor nerve symptoms and red flags that require fast in-person intervention
Looks for patterns of dysfunction in the lower back, pelvis, and hips
Guides you through gentle tests and movements
Designs a home exercise and stretching plan
Educates you about ergonomics, sleep positions, and movement habits
Even without hands-on adjustments, chiropractic expertise is used to understand mechanics and guide safe self-care at home. Evolve Chiropractic+2HealthCentral+2
Telemedicine and Medication Management for Sciatica
Telemedicine is also useful for medication oversight and pain management. Virtual pain management services can:
Review current medications and supplements
Start or adjust anti-inflammatory drugs, muscle relaxers, or nerve pain medications when appropriate
Help taper short-term medications to avoid long-term dependence
Coordinate with other therapies like physical therapy and chiropractic care Everlywell+1
This is important because the goal is not just to reduce pain for a few days but to manage it safely while addressing the underlying cause.
Guided Home Exercises and Self-Care for Sciatica via Telemedicine
A large part of sciatica management involves what you do every day at home. Telemedicine allows your integrative provider to coach you in real time.
Types of exercises a provider may guide over video
Always follow your own provider’s instructions. The list below is for education, not a personal prescription.
An integrative chiropractor, such as Dr. Jimenez, will often blend chiropractic reasoning (how joints and muscles are moving) with physical therapy-style exercise progressions to build strength and reduce nerve irritation over time. Integrative Medical of DFW+1
Telemedicine and Physical Therapy for Sciatica
Physical therapy is a key part of long-term sciatica care. Telemedicine makes it easier for your team to coordinate and supervise this care.
An NP–chiropractor team can:
Refer you to in-person physical therapy when you need hands-on manual work
Work with therapists to align goals: pain reduction, nerve mobility, strength, and posture
Review PT progress notes with you by video
Add or modify home exercises between in-person therapy visits
Modern integrative clinics describe physical therapy as treatment focused on your goals, your function, and your time—whether you are recovering from an acute episode of sciatica or managing long-term spine issues. Integrative Medical of DFW+1
Telemedicine for Office Workers and Remote Workers with Sciatica
Many people with sciatica sit for long periods at desks or work remotely at kitchen tables, couches, or beds. Poor ergonomics can worsen nerve pain.
Telemedicine allows providers to see your real work setup and give specific advice.
They may help you:
Adjust chair height, screen level, and keyboard position
Chiropractic-based telemedicine visits for office workers often focus on spinal alignment, hip position, and load sharing between joints — even if the provider cannot physically adjust the spine during the visit, they can teach you how to move better and reduce pressure on the sciatic nerve. tigardchiropracticautoinjury.com+1
How to Prepare for a Telemedicine Visit for Sciatica
Preparing well can make your telemedicine visit smoother and more helpful.
Before your appointment
Check your technology
Test your camera, microphone, and internet connection
Charge your device and have a backup (like a phone) ready
Choose your space
Find a quiet, private room
Make sure you have enough room to stand, walk, and lie down if needed
Gather information
List your current medications and supplements
Have your medical history and imaging reports handy
Dr. Jimenez’s clinical experience shows that when patients feel seen and supported—through regular check-ins, education, and coordinated care—they are more likely to stay consistent with their home program and achieve better long-term outcomes. El Paso, TX Doctor Of Chiropractic+1
Practical Tips for Getting the Most from Telemedicine for Sciatica
Here are some simple strategies to make telemedicine work for you:
Treat the visit like an in-person appointment
Show up on time and minimize distractions
Have a notebook handy for instructions
Be specific about your goals
“I want to sit for 30 minutes without pain”
“I want to walk around the block again”
Clear goals help your provider design better plans
Use photos or videos
Take a short video of how you walk or how you get out of a chair during painful times
Share this with your provider if their platform allows
Stay consistent with home exercises
Put reminders in your phone
Tie exercises to habits (after brushing teeth, after lunch, etc.)
Ask for a written or emailed summary
Many clinics send a visit summary through the patient portal
This can include your diagnosis, exercise plan, and red-flag symptoms
The Future: Telemedicine, Sciatica, and Integrative Care
Telemedicine is no longer just an emergency backup plan—it is a core part of modern spine and pain care. Spine centers, pain clinics, and integrative practices across the country use telemedicine to: UT Southwestern Medical Center+2NJ Spine & Orthopedic+2
Speed up diagnosis and treatment
Improve convenience for patients in pain
Coordinate care between specialists, therapists, and primary providers
Support long-term recovery with flexible follow-ups
For people with sciatica, this means you can:
Get expert guidance without leaving your home
Partner with an integrative chiropractor and nurse practitioner who can see both the nerve problem and the whole person
Combine remote consultations, at-home exercises, and lifestyle changes into a comprehensive plan
Under the care of a dual-licensed provider like Dr. Alexander Jimenez, telemedicine becomes more than a video call. It becomes a bridge between medical science, chiropractic biomechanics, and day-to-day life—helping you move from intense nerve pain toward safer movement, better function, and long-term relief. El Paso, TX Doctor Of Chiropractic+2Evolve Chiropractic+2
Fast Sports Injury Help Online: How Telemedicine Guides Diagnosis, Rehab, and Return to Play
A massage therapist treats the injury of a professional athlete at El Paso Back Clinic
Telemedicine is changing how athletes get help after an injury. When a chiropractor and a nurse practitioner (NP) work together online, they can guide recovery from many sports injuries without the need for an in-office visit. This is especially helpful for athletes who travel, live far from clinics, or are balancing school, work, family, and training.
In this article, we’ll break down how an integrated chiropractor–NP telemedicine team can:
Do virtual exams from a distance
Share treatment plans and coordinate care
Support at-home rehab, nutrition, and mental health
Help with urgent issues like a possible concussion during games
Reduce unnecessary ER visits while still protecting your safety
1. Why telemedicine matters for sports injuries
Telemedicine is more than a video call. It is a structured way to deliver health care at a distance using secure video, phone, apps, and online tools. Johns Hopkins Medicine notes that telemedicine improves comfort, convenience, and access, especially for people who would otherwise struggle to travel or fit visits into a busy schedule. Hopkins Medicine
For athletes, that matters because:
Practices and games already take up time.
Travel teams may compete hours away from home.
Injuries often happen suddenly—during a weekend tournament, camp, or late-night match.
Telehealth physical therapy and sports services now let athletes receive full evaluations and guided rehab sessions from home, with real-time video coaching. SportsMD+1 Research shows telehealth physical therapy is effective for many orthopedic and sports-related conditions, including non-surgical and post-surgical rehab. PMC
At the same time, sports medicine researchers have shown that telehealth can support concussion care, including baseline testing, diagnosis, and follow-up—especially in rural or resource-limited settings. PMC+1
2. What is an integrated chiropractor + NP telemedicine team?
An integrated team means the chiropractor and nurse practitioner work together instead of in separate silos.
The nurse practitioner (NP) focuses on your overall health, medical history, medications, imaging, and underlying conditions (like asthma, diabetes, or heart issues).
The chiropractor focuses on your spine, joints, muscles, and movement patterns, using guided tests, posture checks, and therapeutic exercises delivered remotely.
In Dr. Alexander Jimenez’s clinical model in El Paso, Texas, the same provider is both a board-certified family nurse practitioner and a chiropractor, which allows one clinician to blend medical and musculoskeletal care through telemedicine for neck pain, low back pain, headaches, and sports injuries. El Paso, TX Doctor Of Chiropractic+2El Paso, TX Doctor Of Chiropractic+2
When the chiropractor and NP are separate providers, they can still share:
Notes and findings in the same electronic health record
Imaging reports and lab results
Exercise programs and rehab goals
Messages with athletic trainers, physical therapists, and coaches
This two-pronged approach helps create one unified plan that covers:
Functional goals (return to sport, position-specific demands)
3. How a virtual sports injury exam works
A telemedicine visit is structured and systematic, not just a quick chat.
3.1 Before the visit
You’ll usually:
Complete an online intake form about symptoms, past injuries, and sport.
Upload any previous X-rays, MRIs, or reports, if available.
Test your camera, microphone, and Wi-Fi connection. SportsMD+1
3.2 During the visit: what the NP does
The nurse practitioner can:
Take a detailed medical history:
How the injury happened
Any prior concussions, surgeries, or chronic conditions
Current medications and allergies
Screen for red flags like chest pain, severe shortness of breath, uncontrolled bleeding, or signs of serious head injury. telehealth.hhs.gov+1
Order diagnostic imaging (X-ray, MRI, CT) if needed.
Write or adjust prescriptions, such as:
Pain medications (when appropriate)
Muscle relaxants
Anti-inflammatory medications
Coordinate referrals to orthopedics, neurology, or emergency care if telemedicine alone is unsafe. OrthoLive+1
3.3 During the visit: what the chiropractor does
Over secure video, the chiropractor can:
Observe posture and alignment (standing, sitting, walking).
Guide you through movement tests, for example:
Bending, rotating, or side-bending the spine
Squats, lunges, or single-leg balance
Shoulder or hip range of motion
Identify pain patterns that suggest sprain, strain, tendinopathy, or joint irritation. sportsandexercise.physio+1
Teach safe at-home movements, such as:
Gentle mobility drills
Core stability exercises
Isometrics to protect healing tissue
In his telemedicine work, Dr. Jimenez describes using these virtual exams to track changes in pain, strength, and mobility from week to week, adjusting exercise progressions and ensuring athletes are not overloading injured tissue. El Paso, TX Doctor Of Chiropractic+1
3.4 Typical flow of a telemedicine sports injury visit
NP and chiropractor (or dual-licensed provider) review your history and goals.
Guided movement and functional tests help narrow down the likely diagnosis.
The NP decides whether imaging or labs are needed.
The chiropractor designs initial movement and pain-reduction strategies.
You leave with a clear home plan and follow-up schedule.
4. Building a shared treatment plan online
After the virtual exam, the team builds a plan that blends medical and musculoskeletal care. Telehealth orthopedic and sports practices report four consistent benefits from this style of care: improved access, reduced costs, better quality and safety, and higher patient satisfaction. OrthoLive
Clear guidelines for when to go to urgent care or ER
Chiropractic and movement actions
Joint and spinal stabilization work
Mobility and flexibility progression
Posture and movement training specific to your sport position
Rehab schedule
How often you meet on video
How many daily or weekly exercises
When to retest speed, strength, or sport-specific skills
Telehealth sports physiotherapy services emphasize that virtual care works best when the athlete receives personalized exercise programs, regular online check-ins, and careful progression from injury to return to play. sportsandexercise.physio+1
5. Conditions that respond well to integrated telemedicine care
Research and real-world practice show that many sports injuries can be evaluated and managed, at least partly, through telemedicine. SportsMD+1
5.1 Common injuries suited for telemedicine
Mild to moderate ankle sprains
Knee pain related to overuse (patellofemoral pain, mild tendinopathy)
Back and neck pain from training load, lifting, or collisions
Mild muscle contusions without signs of fracture
Telehealth physical therapy has shown promise in non-operative and post-operative sports rehab, especially when therapists guide exercise, monitor progress, and adjust programs in real time. PMC+1
5.2 How the NP and chiropractor divide roles
The NP can:
Confirm whether the injury is stable enough for home care.
Check for other health issues (asthma, heart conditions, bleeding disorders).
Manage medications and monitor side effects.
The chiropractor can:
Analyze movement patterns that caused or worsened the injury.
Dr. Jimenez’s clinical work often combines telemedicine visits with in-clinic follow-ups, advanced imaging review, and collaboration with physical therapy and sports training teams to keep athletes progressing without re-injury. El Paso, TX Doctor Of Chiropractic+1
6. Telemedicine and concussion: quick decisions from a distance
Concussions and suspected head injuries are a special case. A missed or delayed diagnosis can put an athlete at serious risk.
A systematic review found that telehealth has been used successfully for concussion baseline testing, diagnosis, and management, especially in military and rural settings. PMC+1 Another review focused on sideline telehealth, where sports medicine physicians assist trainers in real time through video connections during games. PMC+1
SportsMD describes “teleconcussion,” where athletes can quickly access concussion specialists via telehealth instead of waiting days or weeks for in-person care. SportsMD
6.1 How telemedicine helps when you suspect a concussion
During or shortly after a game, a telemedicine visit can help:
Review how the head impact occurred (direct hit, whiplash, fall).
Check acute symptoms, such as:
Headache
Dizziness
Nausea or vomiting
Vision changes
Confusion or memory loss
Guide a brief neurological exam and balance checks via video. PMC+1
Decide whether the athlete must leave the game immediately and seek emergency care.
Telemedicine programs in school sports have also been used to minimize risk by providing teams with rapid access to sports medicine expertise, rather than relying solely on coaches to decide whether a player is safe to continue. NFHS+1
6.2 Role of the integrated team
The NP can determine whether emergency imaging or ER evaluation is needed, arrange teleconcussion follow-ups, and manage symptom-relief medications when appropriate.
The chiropractor can later help with neck pain, posture, and vestibular-related issues—such as balance and coordination problems—once the acute phase is stable and medical clearance is given.
7. At-home rehab and return-to-play through telemedicine
Telehealth lets rehab follow you to your home, hotel room, or training camp.
Telehealth physical therapy programs show several key benefits: increased accessibility, reduced travel burden, and the ability to continue personalized plans even when athletes are on the road. SportsMD+2SportsMD+2
7.1 Common tele-rehab tools
An integrated chiropractor–NP team may use:
Video exercise sessions where the provider:
Demonstrates exercises
Watches your form from different angles
Makes real-time corrections
Secure messaging for quick questions about pain flare-ups or modifications. ATI+1
Remote monitoring apps, where you log:
Pain levels
Step counts or training minutes
Completion of home exercises
Progress checks every 1–2 weeks to advance the plan or adjust if pain increases.
7.2 Examples of tele-rehab goals
Acute phase (first days)
Protect the injured area
Control swelling and pain
Maintain gentle mobility where safe
Subacute phase (1–4 weeks)
Restore the normal range of motion
Begin light strengthening and balance work
Fix faulty movement patterns
Return-to-play phase
Add power, agility, and sport-specific drills
Monitor for any return of pain or instability
Clear the athlete for full competition once the criteria are met
Telehealth sports physio services emphasize a “injury to return-to-play” continuum, where the same remote team oversees each phase to avoid gaps in care. sportsandexercise.physio+1
8. Lifestyle, nutrition, and mental health support from afar
Sports injuries are never just physical. Pain, sudden time off from sport, and stress about losing a starting spot can weigh heavily on athletes.
Telemedicine makes it easier to address the whole person, not just the injured body part:
Nutrition – Remote visits can cover:
Protein and calorie needs during healing
Anti-inflammatory food choices
Hydration strategies for training and games SportsMD+1
Sleep and recovery habits – Online coaching about sleep routines, stretching, and scheduling lighter days can support healing. SportsMD
Mental health – some telemedicine platforms connect athletes with sports psychologists or counselors for stress, anxiety, or mood changes after injury. Programs that highlight telemedicine for athlete health care note that virtual visits help athletes stay engaged in care without derailing their training or school schedules. Nully Medical LLC+2Nully Medical LLC+2
In Dr. Jimenez’s integrative model, telemedicine visits often combine pain management, mobility training, nutritional guidance, and coaching on long-term wellness so that athletes return to sport stronger and healthier, not just “cleared.” El Paso, TX Doctor Of Chiropractic+2LinkedIn+2
9. Benefits for remote and traveling athletes
Telemedicine is especially valuable if you:
Live in a rural area with limited access to sports medicine. Hopkins Medicine+1
Travel often for tournaments, camps, or professional seasons. Nully Medical LLC+1
Have trouble arranging rides, time off work, or childcare. Hopkins Medicine+1
Telehealth platforms built for sports and orthopedic care highlight these advantages:
Faster access to specialists who may be in another city or state. OrthoLive+1
Fewer missed practices or school days.
Less time sitting in traffic or waiting rooms.
Continuous oversight of rehab, even during road trips. SportsMD+1
In school and youth sports, telemedicine programs have also been used to minimize risk by providing real-time medical input during events and improving response to injuries. NFHS+1
10. When telemedicine is not enough: red flags
Telemedicine is powerful, but it is not a replacement for emergency or in-person care when certain warning signs are present. National telehealth guidance stresses that some situations require hands-on exams or urgent evaluation. telehealth.hhs.gov+1
If you experience any of the following, seek in-person or emergency care immediately:
Loss of consciousness, seizure, or severe confusion after a hit to the head
Repeated vomiting, severe headache, or worsening neurologic symptoms
Clear deformity of a bone or joint, or inability to bear weight at all
Suspected fracture with severe swelling or visible misalignment
Chest pain, shortness of breath, or signs of allergic reaction
Suspected spinal injury with numbness, weakness, or loss of bowel/bladder control
In these cases, telemedicine can still play a role after emergency care—for follow-up visits, rehab planning, and coordination between specialists, the NP, and the chiropractor. PMC+1
11. Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC
1. Telemedicine speeds up early decisions. Athletes can be evaluated within hours of an injury—sometimes the same day—without waiting for an in-person slot. This helps determine quickly whether an athlete can manage at home, needs imaging, or must seek urgent or emergency care.
2. Dual-scope evaluation reduces gaps. Because Dr. Jimenez is both a chiropractor and an NP, he can:
Interpret imaging and lab results
Address inflammation, pain, and sleep issues medically
Analyze biomechanics, joint function, and movement patterns
Coordinate with attorneys and athletic organizations when injuries occur in organized sports or school settings El Paso, TX Doctor Of Chiropractic+1
3. Telemedicine helps keep athletes compliant. Through secure messaging and remote check-ins, many athletes are more likely to complete their exercises and follow nutrition or recovery plans. This lines up with broader telehealth research showing high patient satisfaction and good adherence when care is accessible and flexible. OrthoLive+1
4. Hybrid care works best. Dr. Jimenez often uses a hybrid model: telemedicine for triage, education, home-based rehab progressions, and imaging review, plus targeted in-clinic visits for hands-on care when necessary. This mirrors national trends where telemedicine is integrated into, not replacing, in-person sports and orthopedic care. El Paso, TX Doctor Of Chiropractic+1
12. Practical tips for athletes using telemedicine for sports injuries
To get the most out of a telemedicine visit with an NP and chiropractor, prepare like you would for a big game.
Before your visit
Write down:
When and how the injury happened
What makes it better or worse
Medications and supplements you take
Set up your space:
Good lighting
Enough room to walk, squat, or lie down
A stable surface for your phone or laptop
Have gear ready:
Resistance bands or light weights (if you have them)
A chair, wall, or countertop for balance work
During your visit
Be honest about your pain level and limitations.
If you are worried about a concussion, clearly describe all symptoms, even if they seem minor. SportsMD+1
Ask about clear return-to-play criteria:
Pain goals
Strength targets
Functional tests (jumping, sprinting, cutting)
After your visit
Follow the home exercise program and track your progress.
Use the patient portal or app to ask questions if pain changes or if you have trouble with a movement. ATI+1
Schedule regular follow-up telehealth visits so your plan can be adjusted as you improve.
13. Putting it all together
An integrated chiropractor and nurse practitioner telemedicine team gives athletes a powerful, flexible way to:
Get fast evaluations after a sports injury
Receive coordinated medical and musculoskeletal care
Follow individualized rehab plans at home
Access nutrition and mental health support
Lower the chance of unnecessary ER visits, while still protecting safety
From major health systems like Johns Hopkins to specialized sports platforms, and from youth leagues to professional levels, the evidence continues to grow that telemedicine—when used wisely—can make sports medicine more accessible, more coordinated, and more athlete-friendly. InjureFree+3Hopkins Medicine+3OrthoLive+3
In real-world practice, clinicians like Dr. Alexander Jimenez show how blending chiropractic care, nurse practitioner expertise, and telemedicine can keep athletes moving forward—even when they are injured, on the road, or far from a clinic. El Paso, TX Doctor Of Chiropractic+2El Paso, TX Doctor Of Chiropractic+2
Kim, B. I., et al. (2022). Telehealth physical therapy for sports medicine and orthopedic care. Journal of Telemedicine and Telecare. (Summary from PMC article). PMC
Integrative Chiropractic Therapy Meets Telemedicine: A Path to Better Pain Relief
A doctor of chiropractic and a nurse practitioner show a patient an X-ray image of the spine post-slip and fall injury
In today’s fast-paced world, many people deal with ongoing pain or injuries that disrupt daily life. Neck aches from desk work, throbbing headaches that won’t quit, or sore muscles from weekend sports can make simple tasks feel overwhelming. That’s where integrative chiropractic therapy steps in, blending hands-on adjustments with modern tools like telemedicine and nurse practitioner support. This approach lets patients get expert care without always leaving home, making treatment easier and more effective.
People often search for ways to manage these issues without relying solely on pills or surgery. Integrative chiropractic therapy combines spinal alignments and muscle work with virtual check-ins and personalized plans from nurse practitioners. Telemedicine adds the convenience of video calls and app-based tracking, allowing real-time tweaks to exercises or lifestyle tips. This mix eases symptoms and builds long-term habits for staying healthy (Mayo Clinic, 2023).
Dr. Alexander Jimenez, a chiropractor and board-certified family nurse practitioner, has seen this firsthand in his practice. With over 30 years of experience, he notes that patients with busy schedules love how virtual sessions keep them on track without missing work. “By linking chiropractic adjustments with remote monitoring, we address the whole person—not just the pain,” Jimenez shares on his professional site (Jimenez, n.d.a).
What Is Integrative Chiropractic Therapy?
Integrative chiropractic therapy goes beyond basic back cracks. It pulls together different health tools to resolve problems at their source. Think of it as a team effort: chiropractors handle spine and joint fixes, nurse practitioners check meds and overall health, and telemedicine keeps everyone connected from afar.
This method shines for everyday woes like stiff necks or lower back twinges. Patients receive in-person tweaks when needed, along with online follow-ups to track progress. Studies show this blend cuts pain faster than solo treatments, thanks to better teamwork among providers (Dallas Accident and Injury Rehab, n.d.).
Key Parts of the Approach
Chiropractic Adjustments: Gentle pushes to realign the spine, easing nerve pressure and boosting movement.
Nurse Practitioner Input: Pros who review symptoms, adjust plans, and spot when extra tests are needed.
Telemedicine Tools: Apps for logging pain levels, video chats for quick advice, and wearables that share data like steps or posture.
One big win? It fits real life. A working parent with chronic neck pain can chat virtually with a nurse while doing home stretches guided by a chiropractor. This setup has grown popular since the pandemic, with more clinics offering hybrid options (National Academy of Medicine, 2023a).
Dr. Jimenez often highlights that his dual role as DC and FNP-BC enables him to spot links between spine issues and factors such as poor sleep or diet. In one case, he used telemedicine to guide a patient through posture fixes after a car accident, blending virtual coaching with occasional office visits (Jimenez, n.d.b).
The Rise of Telemedicine in Health Care
Telemedicine has changed how we think about doctor visits. No more long waits in stuffy rooms—just a quick video link from your couch. For pain and injury care, it’s a game-changer, letting experts review your form during exercises or adjust plans based on daily logs.
This tech isn’t new, but its use exploded during COVID-19. Now, it’s standard for follow-ups, especially when travel is tough. Clinics use secure portals for sharing X-rays or symptom updates, making care feel seamless (Mayo Clinic, 2023).
Benefits for Busy Lives
Saves Time: Skip the drive; log in from anywhere with Wi-Fi.
Better Tracking: Devices send real-time info on pain or activity, helping pros spot patterns early.
Safer Access: Great for those in rural areas or with mobility limitations, cutting infection risks, too.
Research backs this up. A review found that telemedicine boosts patient adherence to pain plans, leading to quicker relief (Alhowimel et al., 2024). Plus, it teams up well with chiropractic work, where virtual sessions reinforce hands-on gains.
In Dr. Jimenez’s view, telemedicine shines for ongoing issues like sports strains. “We can watch a patient’s squat form live and correct it on the spot, preventing re-injury,” he posts on LinkedIn (Jimenez, n.d.c).
How Nurse Practitioners Fit In
Nurse practitioners (NPs) are like bridges in health care. Trained in both nursing and advanced practice, they handle exams, prescribe meds, and team with specialists. In integrative setups, NPs monitor how chiropractic tweaks affect overall health, like checking blood pressure after neck adjustments.
Their role grows as telemedicine expands, with them leading virtual visits. This means faster answers on whether pain signals something bigger, plus tweaks to home routines. NPs also focus on prevention, suggesting diet changes or stress tips alongside spine work (Health Coach Clinic, 2023).
Ways NPs Enhance Care
Full Check-Ups: Review history and symptoms via video, and order tests as needed.
Med Management: Adjust anti-inflammatories or pain relievers based on progress.
Holistic Advice: Link pain to lifestyle, like how poor sleep worsens migraines.
This teamwork cuts errors and boosts results. For instance, an NP might flag inflammation from lab results, while a chiropractor eases the joint strain. Dr. Jimenez, as an FNP-BC, uses this daily: “My nursing background lets me see the full picture, ensuring safe, rounded care” (Jimenez, n.d.a).
Conditions That Thrive with This Integrated Approach
This combination of chiropractic, NPs, and telemedicine directly addresses common pain points. It works best for issues where movement, monitoring, and mindset all play a part. Let’s break down key ones.
Cervical and Lumbar Pain
Neck (cervical) and low back (lumbar) pain hit millions yearly, often from slouching at desks or heavy lifting. Integrative care starts with adjustments to straighten the spine, easing nerve pinches. Telemedicine follows up with posture videos and exercise demos, while NPs track inflammation via apps.
Patients see big wins: less stiffness, better mobility. A study showed that VR-guided exercises via telehealth reduced low back pain by 30% in 4 weeks (Alhowimel et al., 2024). Home setups let folks practice daily, with virtual nudges keeping them motivated.
Dr. Jimenez notes, “For lumbar issues like sciatica, we blend decompression therapy with remote nerve checks—patients report walking easier sooner” (Jimenez, n.d.b).
Quick Tips for Home Relief:
Gentle neck rolls during video calls.
Lumbar stretches tracked via phone apps.
NP-guided heat packs for flare-ups.
Chronic Migraines
Those pounding headaches can sideline anyone. Triggers like tension or poor alignment respond well to chiropractic neck work, which cuts attack frequency by up to 75% in some cases (El Paso Back Clinic, n.d.). Telemedicine adds migraine logs and trigger alerts, with NPs suggesting meds or hydration plans.
Virtual sessions teach relaxation techniques, such as audio-guided breathing exercises. This mix not only douses the fire but also prevents sparks. Research links it to fewer ER trips (Mayo Clinic, 2023).
In practice, Dr. Jimenez uses functional assessments to tie migraines to gut health, adjusting diets remotely: “Telemedicine lets us fine-tune triggers without delay” (Jimenez, n.d.c).
Athletic Injuries
From twisted ankles to pulled hamstrings, sports mishaps need quick, smart fixes. Chiropractors realign joints, NPs handle swelling with meds, and telemedicine coaches rehab moves. Wearables track healing and flag overdoing-it moments.
This approach speeds the return to play. For sudden strains, virtual evals spot issues early and blend with in-person therapy (Health Coach Clinic, 2023). One review praised telerehab for muscle recovery, noting that it matched the results of in-office treatment (Alhowimel et al., 2024).
Dr. Jimenez, working with athletes, says, “Post-game video reviews catch imbalances fast, keeping injuries from lingering” (Jimenez, n.d.a).
Rehab Musts:
Balance drills via app timers.
Strength logs shared with NPs.
Gradual return plans discussed live.
Chronic Pain Management
Lingering aches from old injuries or daily wear demand steady care. Hybrid models combine relief adjustments with telehealth monitoring to detect patterns. NPs weave in non-drug options like mindfulness apps, cutting reliance on opioids (National Academy of Medicine, 2023a).
Outcomes? The results include improved sleep, elevated mood, and enhanced function. Studies show hybrid care halves pain scores over time (National Academy of Medicine, 2023b).
Osteoarthritis Woes
Joint wear, like knee or hip osteoarthritis, stiffens life. Chiropractic eases alignment, physical therapy builds support via virtual guides, and NPs manage flare meds. This trio slows progression, boosting daily ease (Grace Medical Chiro, n.d.).
Dr. Jimenez adds nutrition tweaks: “Anti-inflammatory foods, tracked remotely, pair perfectly with joint work” (Jimenez, n.d.b).
Daily Joint Helpers:
Low-impact walks with step counters.
Heat therapy reminders from apps.
NP check-ins for supplement fits.
Dizziness and Balance Blues
That woozy feeling from neck kinks or inner ear glitches? Adjustments free nerves, exercises via telehealth, steady steps, and NPs rule out other causes. Integrated plans restore confidence fast (Grace Medical Chiro, n.d.).
Real-Life Wins: Patient Stories and Expert Insights
Meet Sarah, a teacher with lumbar pain from hauling books. Traditional visits clashed with her schedule, but switching to hybrid care changed everything. Weekly video tweaks to her stretches, plus NP med reviews, dropped her pain from 8/10 to 3/10 in two months. She describes the experience as having a personal coach at her side.
Or take Mike, an avid runner sidelined by shin splints—an athletic injury classic. Dr. Jimenez’s team used telemedicine for gait analysis, blending chiropractic realigns with home drills. NPs monitored swelling remotely. Back on track in weeks, Mike credits the seamless flow.
These aren’t rare. Clinics report 80% satisfaction with hybrid models, thanks to flexibility (Dallas Accident and Injury Rehab, n.d.). Dr. Jimenez’s observations align: “In my El Paso practice, we’ve treated thousands via this method, seeing faster heals and happier lives” (Jimenez, n.d.a). His LinkedIn shares cases like TBI recovery, where posture videos aid brain rehab (Jimenez, n.d.c).
Challenges and How to Overcome Them
No system is perfect. Tech glitches or spotty internet can be frustrating, especially in rural areas. Plus, not all pains suit screens—some need hands-on feels (National Academy of Medicine, 2023b).
Solutions? Start with simple audio calls for low-bandwidth spots. Training helps patients navigate apps, and hybrid options ensure in-person when key. Policies that promote fair access, such as subsidy programs, level the field (National Academy of Medicine, 2023a).
Dr. Jimenez directly addresses this issue by providing loaner devices and step-by-step guides to ensure that no one is left behind (Jimenez, n.d.b).
Common Hurdles and Fixes
Tech Barriers: Use voice-only options; provide tutorials.
Privacy Worries: Stick to HIPAA-secure platforms.
Equity Gaps: Partner with community groups for device loans.
The Future: Smarter, Wider Reach
Looking ahead, AI could predict flare-ups from app data, while VR amps up the fun of exercise. More states are approving cross-border telehealth, thereby expanding its reach (Alhowimel et al., 2024).
For chronic pain and injuries, this means fewer hospital stays and more empowered patients. Equity pushes, like audio-only coverage, ensure everyone benefits (National Academy of Medicine, 2023a).
Dr. Jimenez envisions: “With functional medicine at the core, we’ll prevent more than we treat, using telehealth to scale wellness” (Jimenez, n.d.c).
Wrapping Up: Your Next Step to Pain-Free Days
Integrative chiropractic therapy with NPs and telemedicine isn’t a fad—it’s a smart, proven path to handling cervical pain, migraines, injuries, osteoarthritis, dizziness, and more. It blends the best of touch and tech for real relief.
Ready to try? Chat with a provider about hybrid options. Small steps, like logging daily aches, can spark significant changes. As Dr. Jimenez puts it, “Healing starts with connection—virtual or not” (Jimenez, n.d.a).
References
Alhowimel, A. S., Alodaibi, F., Shirazi, S. A., Alharthi, S., Alqahtani, B., & Alrawaili, S. (2024). Innovative applications of telemedicine and other digital health solutions in pain management: A literature review. Journal of Pain Research, 17, 2563–2583. https://doi.org/10.2147/JPR.S473619
The Role of Telemedicine in Integrative Injury Care at El Paso Back Clinic: Providing Full Support for Car Accident, Work, and Sports Injuries in El Paso, TX
A doctor of chiropractic and a nurse practitioner review the MRI of a patient following a motorcycle collision.
In El Paso, TX, getting injured in a car crash, at work, or during sports can be tough. But at El Paso Back Clinic®, a top wellness chiropractic care spot, new tools like telemedicine make getting help simpler. Telemedicine uses video calls and online apps to let health experts care for you from home. This article explores how the clinic’s integrative nurse practitioner (NP) and chiropractor team up with telemedicine to provide comprehensive injury care. This covers virtual check-ups, treatment planning, and long-term help. It’s super useful for folks who can’t easily move or get to the clinic. The team also shares tips on eating, working out, and daily habits to speed up healing. They keep everything organized and documented for the best outcomes.
El Paso Back Clinic® focuses on functional medicine and holistic healing. Led by Dr. Alexander Jimenez, who is both a chiropractor (DC) and a family nurse practitioner (FNP-BC), the clinic combines conventional medicine with natural approaches to treat injuries. Telemedicine here means you can get exams, diagnoses, and follow-ups without leaving home. This is great for busy El Paso residents or for those who are hurting too much to travel. The clinic’s approach considers your whole body, with the NP and chiropractor working together to create plans that fit your life.
What Is Integrative Care at El Paso Back Clinic?
At El Paso Back Clinic®, integrative care means a team of doctors, therapists, and nutritionists working together to fully heal you. For car accident injuries like whiplash or back strains, the chiropractor adjusts your spine while the NP manages pain and checks for deeper issues. They make custom plans using evidence-based methods.
Common Injuries Treated: Neck pain from crashes, work lifts causing strains, or sports-related twists leading to sprains.
Why Choose Integrative?: It targets the cause, not just pain, blending adjustments with lifestyle changes.
Telemedicine’s Role: Allows remote care, so you start healing right away from home.
This method helps with lasting health. For sports fans in El Paso, tips on better nutrition can speed up recovery (Dallas Accident and Injury Rehab, n.d.).
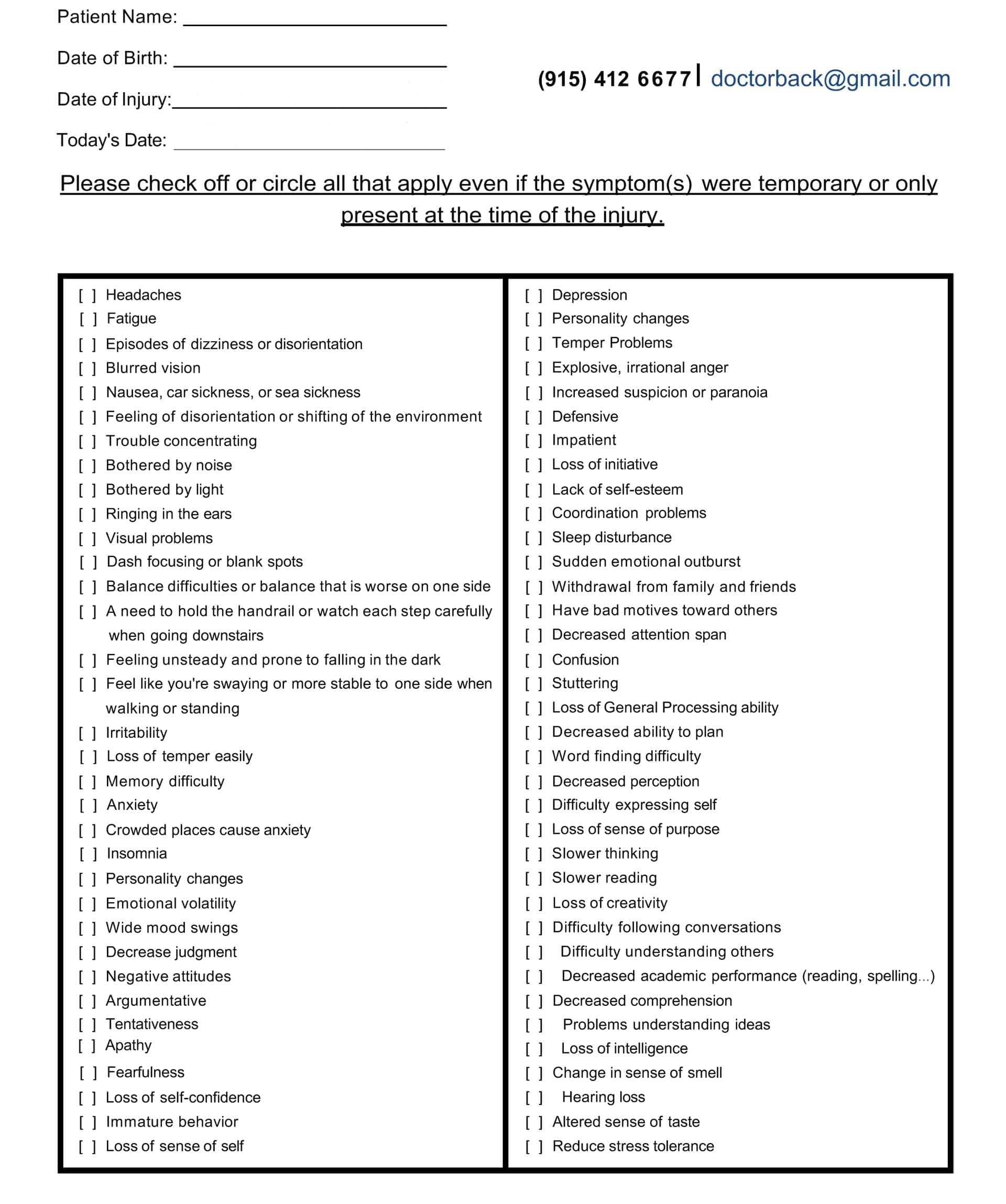
Head Injury/Traumatic Brain Injury Symptom Questionnaire
Virtual Examinations: How El Paso Back Clinic Does It Remotely
Telemedicine at El Paso Back Clinic® starts with virtual exams. You connect via secure video from your phone or computer. Dr. Jimenez or the team talks to you about your injury.
For a car accident, they ask about the crash and pain spots. They watch you move, like bending or walking, to check for swelling or stiffness. Even without hands-on involvement, they spot many problems, such as muscle pulls or nerve issues (Personal Injury Firm, 2025).
Work injuries, like slips, get quick virtual checks to stop things from getting worse. The chiropractor guides home tests, such as balance checks.
Tools in Virtual Exams: Video for movement, apps for sharing photos of injuries, or devices for vital signs.
When It’s Not Enough: Some need in-person touches, so they schedule clinic visits at their El Paso locations.
This remote setup makes getting checked easy, especially in El Paso, where traffic can be a hassle (CK Firm, 2024).
Diagnoses Through Telemedicine at the Clinic
After the exam, the team at El Paso Back Clinic® diagnoses remotely. Common ones from car accidents include whiplash or disc problems. The NP might order X-rays or MRIs, which are performed locally and shared online.
Chiropractors like Dr. Jimenez spot spinal shifts that can cause leg pain, such as sciatica. They explain it clearly on video. The NP assesses whole-body health, including whether swelling worsens.
All sessions are recorded for official documents, insurance keys, or personal injury claims (ChiroMed, n.d.).
Diagnosis Examples: Work-related back pain, sports-related nerve hits, and crash-neck strains.
Team Collaboration: NP handles meds; chiropractor does adjustments.
Tips for Accuracy: Describe pain and show motions well.
This reduces wait times, allowing you to start your El Paso recovery sooner (Complete Care, n.d.).
Managing Treatment Plans Remotely from El Paso Back Clinic
The NP and chiropractor create a treatment plan together, updated via telemedicine. For a sports knee sprain, it might include rest, ice, and shown exercises.
Dr. Jimenez demonstrates stretches on camera. The NP monitors pain and adjusts treatments.
They coordinate to avoid overlaps. For work injuries, plans cover safe job returns. Everything’s online for easy tracking.
Plan Essentials: Pain relief, movement work, and prevention advice.
Integrative Touches: Diet tweaks to cut swelling, like more omega-3 foods.
Telemedicine Updates: Regular video calls to tweak based on progress.
This saves time and money for El Paso patients (Jimenez, n.d.-a).
Ongoing Support and Follow-Up Care at the Clinic
Recovery needs steady help, and El Paso Back Clinic® uses telemedicine for easy follow-ups. Log in to chat about how you’re doing.
For car crash back pain, they check therapy effects and offer encouragement. Support includes mental health tips, as injuries can stress you.
Chiropractors guide home exercises on video. NPs watch for treatment side effects.
Support Types: Mood talks, progress logs, specialist referrals.
How Often: Weekly, early on, then less.
For El Paso Athletes: Safe return-to-play tips, like warm-ups.
This prevents pain from lasting, helping you get back to life fast (Prescient National, n.d.).
Benefits for El Paso Residents with Mobility or Access Issues
Injuries make moving hard, especially in spread-out El Paso. Telemedicine brings care to you.
No travel needed, perfect for remote areas or difficult days. For work injuries, it means less downtime. See pros from home.
Who Gains Most: Those pained by walking, without transport, or packed schedules.
Access Help: Shorter waits than office visits.
Legal Benefits: Docs care for claims without hold-ups.
This makes healing equal for all in El Paso (CK Firm, 2024).
Integrative Advice on Diet, Exercise, and Lifestyle from the Clinic
El Paso Back Clinic® shines with holistic telemedicine tips. They suggest anti-inflammatory foods, such as fruits, to aid healing.
Exercise advice includes easy yoga for pain, demonstrated online. Lifestyle shifts cover better sleep or stress cuts, like apps for calm.
For sports, they teach form to prevent re-injury.
Diet Ideas: Omega-3 for nerves, antioxidants for fixes.
Workout Suggestions: Stretches for range, walks for build-up.
Life Changes: Posture tweaks, drop bad habits.
This addresses root causes for better long-term health (Dallas Accident and Injury Rehab, n.d.).
Coordination and Documentation Between NP and Chiropractor at El Paso Back Clinic
The team shares notes easily on telemedicine platforms. Dr. Jimenez, as both NP and chiropractor, bridges the roles seamlessly.
Records from calls build your file, showing progress for insurance or courts.
Therapies align, like adjustments with rest plans.
Coordination Methods: Shared digital files, joint calls.
Record Value: Shows timely, excellent care.
Your Part: Update honestly for the top plans.
This leads to smooth recoveries in El Paso (Jimenez, n.d.-b).
Insights from Dr. Alexander Jimenez at El Paso Back Clinic
Dr. Alexander Jimenez, DC, APRN, FNP-BC, shares hands-on views from over 30 years at El Paso Back Clinic®. He uses telemedicine for same-day injury exams, like after crashes or sports.
He stresses integrative care for body and mind. For head injuries, he advises sleep, diet, and exercise. His dual license allows him to prescribe medications and adjust spines remotely when possible.
Jimenez highlights tests, such as MRIs, shared online. He combines adjustments in nutrition with other interventions for issues like gut health post-trauma.
Main Observations: Injuries are linked to overall health, like nerves and digestion.
Telemedicine in Practice: Quick virtual help for accidents, with shipped braces.
Tips: Use posture drills and supplements for healing.
His approach shows how the clinic’s NP-chiropractor team excels (Jimenez, n.d.-a; Jimenez, n.d.-b; Jimenez, n.d.-c).
Challenges and Future of Telemedicine at El Paso Back Clinic
Telemedicine has limits, such as the need for touch for some exams. Tech glitches can happen.
But the future is promising. Better apps and AI will improve diagnoses. More insurance covers it.
The clinic trains in remote teamwork.
Fixing Issues: Have in-person backups, help with tech.
Coming Trends: Wearables for live data.
Importance: Makes care more accessible and affordable in El Paso.
Conclusion
At El Paso Back Clinic® in El Paso, TX, telemedicine transforms injury care for car, work, or sports-related injuries. The integrative NP and chiropractor team, led by Dr. Jimenez, offers virtual exams for ongoing support. It includes holistic advice for better living. Ideal for mobility challenges. As Dr. Jimenez proves, this leads to quicker, fuller healing. If injured, reach out to El Paso Back Clinic® for easy, top-notch care at 915-850-0900 or visit their site.
Sports and Activities for TBI Recovery: The Role of Nurse Practitioners and Integrative Chiropractic Care
aquatic rehabilitation class for various injuries, including traumatic brain injuries
Traumatic brain injuries, or TBIs, happen when a sudden bump or blow to the head damages the brain. These injuries can come from car crashes, falls, or even sports accidents. Recovering from a TBI takes time and involves many steps to get back strength, balance, and clear thinking. One great way to help is through sports and activities tailored to a person’s needs. These are called adaptive sports. They can boost physical health and also lift moods by making people feel connected and strong. Along with that, healthcare experts like nurse practitioners and chiropractors play big parts in guiding recovery. Nurse practitioners help manage overall health and meds, while chiropractors focus on fixing spine issues and easing pain. This team approach, often called integrative care, mixes different treatments for better results.
In this article, we’ll look at sports that support TBI recovery, such as adaptive basketball and swimming. We’ll also cover calming activities such as tai chi and hiking. Then, we’ll explain how nurse practitioners and chiropractors fit into the picture, drawing on expert perspectives such as Dr. Alexander Jimenez, who combines chiropractic and nursing skills. By the end, you’ll see how these elements work together to create a comprehensive recovery plan.
Understanding TBIs and the Need for Active Recovery
A TBI can mess with how you move, think, and feel. Mild ones, like concussions, might cause headaches or dizziness. Severe ones can lead to long-term problems with balance or memory. The brain has a cool ability called neuroplasticity, which means it can rewire itself to heal. Activities that get you moving help spark this process by building new connections in the brain.
Doctors say rest is key right after a TBI, but then it’s time to add gentle exercise. Starting slow prevents more harm and builds up skills step by step. For example, light walking can improve blood flow to the brain, helping it heal faster. As you get better, more fun activities like games or outdoor adventures can keep things exciting and motivating.
Why activities matter: They improve strength, coordination, and mood.
Start small: Begin with easy tasks at home, like puzzles or stretching.
Build up: Move to group activities for social support.
Research shows that staying active after a TBI lowers the risk of depression and helps people get back to daily life sooner.
Adaptive Sports for Physical and Mental Healing
Adaptive sports are regular sports modified with special tools or rules so everyone can join, regardless of their limitations. For TBI survivors, these sports target balance, hand-eye skills, and thinking on your feet. They also build confidence by letting you achieve goals in a safe way.
Many groups offer adaptive sports programs, making it easy to find local options. Here’s a look at some top ones for TBI recovery:
Adaptive Basketball: Played in wheelchairs or with lower hoops, this sport boosts coordination and teamwork. It helps with quick decisions and arm strength, which TBIs often weaken. Groups like the National Wheelchair Basketball Association run events where players connect and stay motivated.
Cycling: Use adaptive bikes with extra wheels for stability. Cycling improves leg strength and heart health while being low-impact on joints. It’s great for building endurance without straining the brain too much.
Swimming: Water supports your body, making movements easier. Adaptive swimming uses floats or lanes for safety. It enhances balance and breathing control, plus the calm water reduces stress.
Canoeing: In adaptive versions, boats have seats or handles for support. Paddling builds upper body strength and focus. Being on water also calms the mind, helping with anxiety from TBIs.
These sports aren’t just exercise—they create social bonds. Playing with others fights loneliness, a common issue after brain injuries. Studies note that adaptive sports like these keep people active and linked to their communities. One review found that they improve gait and balance in patients with brain injury.
Other Rehabilitative Activities to Enhance Balance and Well-Being
Not all recovery needs to be high-energy. Slower activities like tai chi or hiking can rebuild skills without overwhelming the brain. These focus on mindful movement, which also supports mental health.
Tai Chi: This gentle martial art uses slow, flowing movements to improve balance and focus. For TBI patients, it reduces falls by strengthening core muscles. Classes often adapt poses for sitting if standing is difficult.
Hiking: Adaptive hiking uses trails with smooth paths or walking sticks. It increases heart rate and provides a refreshing change of scenery. Nature-based activities like this restore energy both physically and emotionally.
Adaptive Water Sports: Beyond swimming, try kayaking or water aerobics. These use buoyancy to reduce pressure on the body while improving coordination. Special gear, like life vests, ensures safety.
Home activities can start the process. Activities like balloon tosses or chair yoga build hand-eye coordination and flexibility. Online videos make it easy to try. As skills grow, add group classes for more challenge. Experts say even simple mobilizing, like walking circuits, aids recovery.
Special tools might be needed based on your strengths. For example, use bigger balls in games or stabilizers in cycling. Always check with a doctor to match activities to your healing stage.
The Role of Nurse Practitioners in Coordinating TBI Care
Nurse practitioners (NPs) are advanced nurses who can diagnose, treat, and manage health issues. In TBI recovery, they act as coordinators, making sure all parts of care fit together smoothly.
NPs monitor your overall health during activities. They check for signs like fatigue or headaches that might mean you’re pushing too hard. They also manage meds for pain or mood, adjusting doses as you improve. For instance, if swimming causes dizziness, an NP might suggest changes or add rest days.
In integrative teams, NPs work with other experts to create safe plans. They ensure activities like canoeing don’t clash with your meds or other treatments. Their focus on whole-person care includes emotional support to help with stress during recovery.
Dr. Alexander Jimenez, a chiropractor and family nurse practitioner, notes that NPs play a key role in linking brain health to daily wellness. His observations show they help with sleep and nutrition, which in turn boost activity benefits. This approach ensures activities are effective and safe.
Integrative Chiropractic Care: Supporting Spine and Pain Management
Chiropractors specialize in spine health, which is crucial after a TBI since head injuries often affect the neck. Integrative chiropractic combines adjustments with other therapies, such as exercises, for full recovery.
Chiropractors realign the spine to ease pressure on nerves, reducing headaches and improving balance. For TBI patients, this can help with dizziness from vestibular issues. They also manage pain without heavy meds, using hands-on techniques.
In recovery plans, chiropractors include exercises such as postural training and balance drills. These complement sports by building a strong base. For example, after an adaptive basketball session, a session might address any spine shifts from play.
Dr. Jimenez’s clinical work highlights how chiropractic aids brain healing. He uses gentle adjustments to improve blood flow and nerve function, key for TBIs. His teams integrate this with nutrition and rehab activities, such as light walking, to prevent reinjury. One method he supports is vestibular rehab, which pairs well with sports for better coordination.
Benefits of integrative chiropractic:
Reduces inflammation and pain.
Improves mobility for activities.
Prevents future issues through education.
Combining chiropractic with NP care creates a strong support system. NPs handle meds and monitoring, while chiropractors focus on physical fixes.
Combining Sports, Activities, and Professional Care for Best Results
The best TBI recovery programs combine adaptive sports, calming activities, and expert guidance. Start with a plan from your healthcare team. For example, begin with tai chi for balance, then add cycling as strength grows.
Community outings, like group hikes, apply skills in real life. These build confidence and social ties. Equine therapy, like therapeutic riding, is another option—horses’ movements aid gait and emotional health.
Dr. Jimenez observes that nutrition supports this, like anti-inflammatory foods for brain repair. His work shows that stress management is key, as it affects outcomes.
Track progress with tools like journals or apps. Adjust as needed with your NP or chiropractor. Over time, this leads to independence and joy in activities.
Challenges and Tips for Success
Recovery isn’t always smooth. Fatigue or setbacks can happen. Tips include:
Listen to your body—rest when needed.
Use adaptive gear for safety.
Join support groups for motivation.
With patience, most people see big gains. Studies show stepwise returns to activity, like in sports protocols, work well.
Conclusion
Recovering from a TBI through sports like adaptive basketball or activities like hiking builds both the body and the mind. Nurse practitioners coordinate safe care, while integrative chiropractic handles pain and alignment. Experts like Dr. Jimenez show how this blend speeds healing. Stay active, seek help, and celebrate small wins to pave the way for a brighter path ahead.
Tests Used for Brain Injuries at El Paso Back Clinic® in El Paso, TX
Doctor of Chiropractic and Nurse Practitioner show the imaging result to the patient post-auto-injury rehabilitation with mild brain injury
Brain injuries can strike without warning, from a simple slip at home to a tough hit during sports or a car crash on El Paso’s busy roads. At El Paso Back Clinic® in El Paso, TX, our team of wellness chiropractic care experts knows how vital it is to spot these issues early. We blend chiropractic skills with modern tools to help patients heal and get back to life. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, our clinic focuses on whole-body wellness, using safe, non-invasive methods to check for head injuries.
This article dives into the tests we use at El Paso Back Clinic® to find brain injuries. We cover hands-on checks, brain function tests, and high-tech scans. Our goal is to give you clear info so you can seek help fast. Early detection means better recovery and fewer long-term problems.
The Importance of Spotting Brain Injuries Early at Our Clinic
Traumatic brain injuries (TBIs) happen when a bump or jolt shakes the brain. Mild ones, like concussions, might cause short-term headaches or dizziness. Serious cases can lead to lasting memory issues or mood changes. At El Paso Back Clinic®, we see many patients from local accidents or sports-related injuries, and we emphasize prompt action.
Our integrative approach mixes chiropractic care with nurse practitioner expertise. Dr. Jimenez uses his dual training to create custom plans. We check the spine, nerves, and brain together because a head injury often affects the neck as well.
Common signs: Headaches, confusion, nausea, or trouble balancing.
Why act fast: Stops swelling or bleeding from getting worse.
Our edge: Our wellness focus means we look at lifestyle and nutrition, too.
Research backs our methods—early tests lead to stronger outcomes (Pickett et al., 2024). At our El Paso, TX clinic, we guide you through every step.
Starting with Neurological Assessments for Head Injuries
At El Paso Back Clinic®, every brain injury check begins with basic neurological tests. These quick exams help us see how the brain responds right away. No need for big machines; it’s all about skilled observation.
We rely on the Glasgow Coma Scale (GCS) to grade injury severity. The Glasgow Coma Scale (GCS), which scores from 3 to 15, assesses eye opening, verbal response, and motor response. High scores mean mild issues; low ones signal urgency. Our team, including Dr. Jimenez, uses GCS to quickly decide on next steps (Bussières et al., 2022).
We also use the Standardized Assessment of Concussion (SAC). This tests memory and focus with simple questions. For athletes, the Sport Concussion Assessment Tool 5 (SCAT5) adds balance and neck checks. Kids receive the Child SCAT5 version.
GCS breakdown:
Eyes: 1 (none) to 4 (spontaneous).
Verbal: 1 (silent) to 5 (oriented).
Motor: 1 (none) to 6 (obeys commands).
SAC quick tips: Asks things like “What month is it?” or repeats word lists.
SCAT5 extras: Includes symptom checklists and coordination drills.
Dr. Jimenez notes that these tests often reveal neck problems linked to head injuries. At our wellness clinic, we adjust spines to ease related pain.
Hands-On Physical Exams to Uncover Hidden Issues
Physical checks are key at El Paso Back Clinic®. We touch and move areas to find pain, weakness, or limits. This builds on your story about how the injury happened.
Reflex tests tap spots, like the knees, to check nerve pathways. Odd responses might point to brain trouble. The Balance Error Scoring System (BESS) tests stability—stand in poses and count errors. It’s useful for detecting dizziness associated with TBIs (Sillevis et al., 2018).
We measure how far you can move your neck or head without pain. Strength tests have you push against our hands. These help link head injuries to spine misalignments.
BESS poses:
These include the double-leg stance, single-leg stance, and tandem pose.
Perform the exercises on both firm ground and foam to increase the challenge.
The errors to avoid include having hands off the hips, keeping eyes open, and falling.
Reflex checks: Hammer taps for quick reactions.
Motion tests: Gentle turns to spot restrictions.
For El Paso locals in car wrecks, these exams guide our chiropractic adjustments. Dr. Jimenez observes that early physical checks prevent chronic issues.
Cognitive Testing to Measure Brain Function
Head injuries can fog thinking. At El Paso Back Clinic®, we use cognitive tests such as ImPACT to assess memory and reaction time. This computer-based tool is perfect for concussion assessment, as it allows you to compare your scores to norms or baselines.
ImPACT includes modules for word recall, symbol matching, and symptom rating. It’s objective and tracks progress over time. We use it for return-to-work or play decisions (ImPACT Applications, Inc., 2023a).
Our nurse practitioners add deeper checks if needed, like repeating stories or drawing shapes. These rule out other causes.
ImPACT features:
Visual memory: Recall designs.
Reaction time: Click on the colors fast.
Symptom scale: Rate 22 items like fatigue.
Baseline testing: Ideal for athletes before seasons.
Retesting: Every 7-10 days to monitor healing.
Dr. Jimenez integrates ImPACT with chiropractic care, noting better results when spine health supports brain recovery.
Advanced Imaging for Clear Views of Injuries
Imaging lets us see inside. At El Paso Back Clinic®, we start with X-rays for bone alignment and fractures. They’re fast and help plan adjustments.
For deeper looks, CT scans catch bleeds quickly. MRIs show soft-tissue damage, such as bruising or tears—no radiation involved. We order these through our network for full pictures (NYU Langone Health, n.d.).
Digital Motion X-ray (DMX) is a favorite here—it films spine movement to spot instability from whiplash.
X-ray basics: Views bones in still shots.
CT strengths: 3D slices for emergencies.
MRI details: Magnets reveal hidden swelling.
DMX unique: Real-time video of neck motion.
Dr. Jimenez uses imaging to confirm diagnoses, ensuring safe, targeted care at our El Paso wellness clinic.
We love tools that avoid invasives at El Paso Back Clinic®. Surface Electromyography (sEMG) measures muscle activity via skin sensors. It identifies imbalances related to nerve issues post-head injury (Injury 2 Wellness Centers, 2023a).
Our INSiGHT scanners combine scans: Thermal for inflammation, Core for posture, Pulse for stress via heart rate. These insights help us create personalized plan maps (CLA Insights, 2023a).
sEMG benefits:
Detects tense muscles around the neck.
Guides gentle adjustments.
INSiGHT scans:
Heat patterns show hot spots.
Muscle scans check symmetry.
No risks: This procedure is safe for individuals of all ages.
These tools reduce the need for pokes or cuts, aligning with our wellness focus (Injury 2 Wellness Centers, 2023b). Dr. Jimenez says they boost patient involvement.
Nurse Practitioners’ Role in Comprehensive Testing
Our nurse practitioners at El Paso Back Clinic® expand options. They order blood tests for markers like inflammation or clotting risks. This rules out serious issues.
They incorporate a comprehensive approach by integrating chiropractic care into their holistic plans. If scans show problems, they coordinate referrals.
Blood work perks:
Checks for hidden infections.
Monitors healing proteins.
Team integration: NPs and chiros share findings.
Patient plans: Include rest, nutrition, and adjustments.
Dr. Jimenez, with his NP background, ensures seamless care.
Chiropractic Perspectives on Brain Injury Diagnosis
Chiropractors at our clinic see the spine-brain connection. Head hits often shift vertebrae, worsening symptoms. We use tools like Sigma for motion analysis (Kawa, n.d.).
Vestibular tests check eyes and balance. Does the patient experience pain during head movements? The source of the pain could be either the inner ear or the brain.
Spine focus:
Palpate for misalignments.
Grade Whiplash: 0-4.
Red flags: Send to ER for severe signs.
Recovery steps: Adjustments plus exercises.
Dr. Jimenez’s observations show that chiropractic care eases concussion symptoms more quickly.
Collaborative Care for Optimal Recovery
At El Paso Back Clinic®, teamwork rules. NPs order MRIs; chiros use them for adjustments. Shared tests like SCAT5 build complete views.
Plans cover therapy, diet, and follow-ups. Patients return stronger.
Benefits:
Full body healing.
Cost-effective.
Customized to you.
Success stories: Less pain, better function.
Dr. Jimenez’s integrative style shines in El Paso cases.
Insights from Daily Practice at the Clinic
We adapt tests to each patient. A work injury requires X-rays and ImPACT. Follow with BESS for balance gains.
Dr. Jimenez shares how INSiGHT scans catch early nerve stress, preventing long-term woes.
Patients love visual reports—they understand and stick to plans.
Overcoming Challenges in Brain Injury Detection
Access and cost can hinder. But our clinic offers affordable options and education.
Future tools, such as blood biomarkers, promise quicker diagnoses. We stay up to date for the best care.
Hurdles:
Rural limits in TX.
Insurance gaps.
Advances: AI for scan reads, more non-invasives.
Dr. Jimenez pushes for community awareness.
Final Thoughts: Seek Care at El Paso Back Clinic®
Brain injuries need prompt attention. At El Paso Back Clinic® in El Paso, TX, we use GCS, ImPACT, scans, and more for wellness-focused recovery.
If you’ve had a head hit, visit us. Our team, led by Dr. Jimenez, is here for you.
References
Bussières, A., et al. (2022). Concussion knowledge among North American chiropractors. Journal of the Canadian Chiropractic Association, 66(1), 17–26. https://pmc.ncbi.nlm.nih.gov/articles/PMC8791549/
Pickett, W., et al. (2024). Expanding concussion care in Canada: The role of chiropractors and policy implications. Journal of the Canadian Chiropractic Association, 68(2), 145–156. https://pmc.ncbi.nlm.nih.gov/articles/PMC11418793/
Sillevis, R., et al. (2018). Survey of chiropractic clinicians on self-reported knowledge and recognition of concussion injuries. Journal of the Canadian Chiropractic Association, 62(2), 84–95. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6000952/
Discover the relationship between somatovisceral disorders, head injuries, and effective management strategies.
Understanding Head Injuries and Their Impact on the Brain-Body Connection: A Comprehensive Guide to Somatovisceral Disorders and Non-Surgical Treatment Approaches
Head injuries represent a significant public health concern affecting millions of individuals worldwide each year. When someone experiences trauma to the head, whether from a sports collision, car accident, or fall, the resulting damage extends far beyond the initial impact site. These injuries create a cascade of physiological changes that disrupt the delicate communication system between the brain and body, leading to what researchers now recognize as somatovisceral disorders. Understanding how head injuries affect this vital brain-body connection and exploring effective non-surgical treatment options can make a meaningful difference in recovery outcomes and quality of life.
What Are Somatovisceral Disorders?
Somatovisceral disorders involve complex interactions between the body’s physical structures (somatic system) and its internal organs (visceral system). This intricate process consists of the transmission of nerve signals from bodily structures to visceral organs, creating specific physiological or pathological reactions. The complexity of somatovisceral response lies not only in its dual-system involvement but also in its capacity for bidirectional communication, allowing information to flow from somatic structures to visceral organs and vice versa. foundationhealth
The relationship between head injuries and somatovisceral disorders has gained increasing attention in medical research. Recent studies have demonstrated that mild traumatic brain injury (mTBI) may be a common precipitant of somatic symptom disorder, with research showing that 15-27% of patients who experienced head trauma met criteria for this condition at six months post-injury. This connection highlights how trauma to the brain can disrupt the normal communication pathways that regulate bodily functions, leading to persistent and often debilitating symptoms throughout the body. neurologyopen.bmj
Somatic symptom disorder occurs when individuals experience distressing physical symptoms combined with excessive thoughts, feelings, or behaviors related to those symptoms. Following a head injury, patients frequently report a wide range of somatic complaints, including pain, weakness, difficulty moving, headaches, dizziness, extreme tiredness, changes in vision or hearing, itching, numbness, abnormal movements, stomach aches, and nausea. These symptoms reflect the disrupted communication between the brain and various body systems, demonstrating how neurological damage can manifest as widespread physical dysfunction. chop+1
The Brain-Body Connection and Head Injury
The human nervous system operates through an intricate network that connects the brain to every organ, muscle, and tissue in the body. This communication highway relies on precise signaling between the central nervous system (brain and spinal cord) and the peripheral nervous system (nerves throughout the body). When head trauma occurs, this delicate communication system can become disrupted at multiple levels, affecting both somatic (voluntary) and autonomic (involuntary) nervous system functions.
According to Dr. Alexander Jimenez, a board-certified Family Practice Nurse Practitioner and Doctor of Chiropractic in El Paso, Texas, the spine houses the spinal cord, which acts as the communication superhighway between the brain and body. Any misalignment in the spine can disrupt the nervous system’s signals, and for traumatic brain injury patients, this connection becomes crucial. Dr. Jimenez explains that misalignment caused by the injury itself or associated whiplash can worsen symptoms like headaches, brain fog, and balance issues, emphasizing the importance of addressing both cranial and spinal components in recovery. northwestfloridaphysiciansgroup
The brain-body disconnect following trauma manifests as disrupted somatic sensory processing, encompassing vestibular (balance) and somatosensory (touch, pressure, temperature) processing. These sensory systems are primarily concerned with survival and safety, given the potential consequences of impaired balance or diminished awareness of physical threats. Following a head injury, trauma-related symptoms are conceptualized to be grounded in brainstem-level somatic sensory processing dysfunction and its cascading influences on physiological arousal modulation, affect regulation, and higher-order capacities. pmc.ncbi.nlm.nih
Research has identified that traumatic conditions may manifest as disrupted vertical integration, in which the balance between lower brain regions and higher cortical areas becomes dysregulated, particularly within the midline neural circuitry responsible for generating a primordial sense of a bodily and affective self as a coherent and stable entity in relation to the environment. This alteration has a cascading impact on the horizontal integration of cortical brain structures, meaning that different regions of the brain may be structurally intact yet lack fluid communication. pmc.ncbi.nlm.nih
Autonomic Dysfunction After Head Injury
One of the most significant yet underappreciated consequences of head injury is autonomic nervous system dysfunction. The autonomic nervous system controls involuntary bodily functions, including heart rate, blood pressure, digestion, breathing, and temperature regulation. Following moderate-to-severe traumatic brain injury, patients often experience significant autonomic dysfunction affecting both sympathetic (fight-or-flight) and parasympathetic (rest-and-digest) branches of this critical system. neurologyopen.bmj
Studies have demonstrated that patients with severe traumatic brain injury can experience sympathetic hyperactivity in the acute stages. More importantly, autonomic dysfunction persists in many patients for months or even years after their initial injury, affecting fully ambulant patients whom many might assume to be fully recovered. This persistent dysfunction occurs through various mechanisms, with the hallmark of moderate-to-severe traumatic brain injury being white matter injury caused by axonal shearing due to injury forces, continuing due to inflammation and delayed axonal degeneration in the chronic period, resulting in network disruption.neurologyopen.bmj
Autonomic dysfunction may occur due to injury to regions of the central autonomic network or their connecting white matter tracts. Brainstem nuclei and white matter connections to and from thalamic and basal ganglia regions may be particularly vulnerable to damage, underlying dysfunction that contributes to cognitive impairment post-traumatic brain injury. Given the importance of brainstem, thalamic, and basal ganglia circuits to autonomic function, injury to these white matter tracts may cause centrally mediated autonomic dysfunction. neurologyopen.bmj
The clinical manifestations of autonomic dysfunction after head injury are diverse and often debilitating. Many classic symptoms following concussion are, at least in part, likely a result of injury to the autonomic nervous system. Cognitive difficulties seen after mild traumatic brain injury may be related to autonomic dysregulation, specifically impaired cerebral blood flow. The presence of autonomic dysfunction has been shown to correlate with increased morbidity and mortality in moderate and severe traumatic brain injury, with perturbations of the autonomic nervous system consisting of either increased sympathetic or reduced vagal activity, potentially resulting in serious cardiac complications. health+1
Dr. Jimenez’s clinical practice emphasizes the importance of recognizing autonomic dysfunction in patients recovering from head injuries. His functional medicine approach includes detailed health assessments evaluating lifestyle, environmental exposures, and psychological factors to understand the root causes of chronic disorders and treat patients holistically. This comprehensive evaluation is particularly important for identifying autonomic dysfunction, which may manifest as dizziness, balance problems, temperature dysregulation, digestive issues, and cardiovascular irregularities.
Environmental Factors Affecting Brain Activity and the Body
Environmental factors play a critical role in shaping brain structure and function, as well as the development of mental and physical health conditions. The macroenvironment encompasses immediate factors such as air, noise, and light pollution; proximal factors, including regional socioeconomic characteristics; and distal factors, such as urbanization, natural spaces, and climate. These environmental exposures are mostly modifiable, presenting opportunities for interventions and strategies to promote the structural and functional integrity of the brain and mitigate the burden of illness following head injury. nature
Air pollution has emerged as a significant concern for brain health, particularly following traumatic brain injury, when the brain is already vulnerable. Studies have demonstrated that air pollution may increase vulnerability to mood dysfunction and potentially inhibit an appropriate stress response. Prolonged exposure to fine particulate matter (PM2.5 and PM10) has been associated with negative stress-related brain activation in the prefrontal cortex, frontoinsular cortex, limbic system, inferior parietal cortex, and cingulate regions. Magnetic resonance imaging studies reveal that increased exposure to PM2.5 is associated with changes in brain structure in older adults, including brain atrophy, that occur before the onset of dementia. environmentalhealth.ucdavis+1
Noise pollution, originating from urban traffic, airports, industries, and construction sites, can evoke negative emotions and disrupt recovery following head injury. Prolonged exposure to disruptive noise induces brain alterations through mechanisms such as sleep disturbances, which create a pro-oxidative environment that predisposes to neuroinflammation and heightened hypothalamic-pituitary-adrenal axis reactivity, contributing to mental and physical health problems. For individuals recovering from head trauma, protecting against excessive noise exposure becomes particularly important as the injured brain requires optimal conditions for healing. nature
Light pollution and exposure to artificial light at night have become increasingly prevalent, especially in urban areas, disrupting natural darkness and circadian rhythms. Light is detected by the retina and transmitted through intrinsically photosensitive retinal ganglion cells to the suprachiasmatic nucleus in the hypothalamus and other brain regions involved in regulating circadian rhythms and sleep-wake cycles. Circadian rhythm disruptions have been linked to elevated risk of mood disorders, bipolar disorders, and heightened mood instability, potentially mediated by oscillations in clock gene expression responsive to light-dark transitions. nature
Following traumatic brain injury, circadian rhythm disruptions become even more pronounced. Research has documented that traumatic brain injury can lead to decreased melatonin release, causing circadian rhythm delays. Studies using animal models have revealed that acute subdural hematoma resulted in dysregulation of circadian gene expression and rhythmic changes in body temperature during the first 48 hours post-injury. The regulation of biological rhythms through changes in core body temperature, pineal gland melatonin secretion, and blood cortisol levels becomes disrupted, affecting the body’s ability to anticipate and adapt to environmental changes. practicalneurology+1
Minor traumatic brain injury contributes to the emergence of circadian rhythm sleep disorders, with research identifying two distinct types: delayed sleep phase syndrome and irregular sleep-wake pattern. These disorders differ in subjective questionnaire scores and have distinct profiles of melatonin and temperature circadian rhythms. The alteration in the circadian timing system partially accounts for the presence of post-traumatic brain injury sleep-wake disturbances, which changes in sleep architecture alone cannot fully explain.pubmed.ncbi.nlm.nih+1
How Head Injuries Affect Daily Tasks and Routines
The impact of head injuries extends far beyond the initial trauma, profoundly affecting an individual’s ability to perform everyday activities and maintain normal routines. The disruption to brain-body communication creates challenges across multiple domains of daily functioning, from basic self-care tasks to complex cognitive and social activities. Understanding these impacts helps patients, families, and healthcare providers develop realistic expectations and appropriate support strategies during recovery.
Cognitive fatigue represents one of the most disabling consequences of traumatic brain injury, affecting 21-73% of patients regardless of injury severity or time since injury. Fatigue has been identified as the main cause of disability after traumatic brain injury, negatively affecting social, physical, and cognitive functions as well as participation in daily activities and social life. At the neural level, patients with fatigue following head injury exhibit significant disruption of global resting-state alpha-band functional connectivity between cortical midline structures and the rest of the brain. Furthermore, individuals with fatigue show reduced overall brain activation during cognitive tasks, without time-on-task effects. academic.oup
Adults with a history of even mild traumatic brain injury report significantly greater fatigue and cognitive impairment than those with no history of head trauma, with symptoms becoming more profound with greater injury severity. This persistent fatigue affects the ability to maintain attention, concentrate on tasks, process information efficiently, and sustain mental effort throughout the day. Patients frequently report that activities requiring cognitive engagement become increasingly difficult as the day progresses, leading to a pattern of morning productivity followed by afternoon exhaustion. pubmed.ncbi.nlm.nih+1
Memory difficulties present another significant challenge affecting daily functioning after a head injury. Patients may struggle with both short-term working memory (holding information in mind while using it) and long-term memory formation (creating new lasting memories). These memory challenges affect practical tasks such as remembering appointments, following multi-step instructions, recalling conversations, and learning new information or skills. The impact extends to occupational functioning, with studies finding a correlation between higher levels of mental fatigue and lower employment status following traumatic brain injury. headway+1
Executive function impairments following head injury affect planning, organization, decision-making, problem-solving, and behavioral regulation. These higher-order cognitive processes are essential for managing daily responsibilities, from planning meals and organizing household tasks to managing finances and making important life decisions. Patients may find themselves struggling with tasks that previously seemed automatic, requiring conscious effort and external supports to maintain daily routines. headway
Sensory processing alterations create additional challenges for daily functioning. The vestibular system, which contributes to balance, spatial processing, arousal modulation, first-person perspective, and social cognition, becomes particularly vulnerable following head trauma. Disturbed temporal binding of sensory information creates perceptual chaos and a lack of coherence, which may lead to bodily disconnection and states of hypervigilance. Patients describe feeling disconnected from their bodies, experiencing the world as if through a fog, or feeling constantly on guard against potential threats. pmc.ncbi.nlm.nih
Balance and coordination problems stemming from vestibular dysfunction affect mobility and safety in daily activities. Simple tasks like walking on uneven surfaces, turning the head while moving, or navigating busy environments become challenging and potentially dangerous. Many patients report increased anxiety about falling, leading to activity restriction and social withdrawal. Over one-third of adults over 40 will experience vestibular dysfunction at some point in their lives, and when it occurs, whether by injury, aging, or disease, individuals can experience vertigo, nauseating dizziness, vision, and balance problems affecting every area of life. neuroinjurycare+1
Dr. Jimenez’s practice in El Paso focuses extensively on helping patients restore function and return to daily activities following head injuries. His integrated approach combines chiropractic care, functional medicine, and rehabilitation therapies to address the multiple systems affected by head trauma. By evaluating the connections between physical, nutritional, and emotional factors, Dr. Jimenez develops personalized care plans that recognize the complex ways head injuries disrupt daily functioning and quality of life.
Overlapping Risk Profiles and Symptoms Associated With Head Injuries
Head injuries create overlapping risk profiles affecting multiple body systems simultaneously, leading to complex symptom presentations that can challenge both patients and healthcare providers. Understanding these interconnected risk factors and symptoms is essential for comprehensive assessment and treatment planning. Individuals who sustain head injuries develop an increased risk for somatic symptom disorder, with early illness beliefs playing a significant predictive role. Specifically, believing that mild traumatic brain injury has serious life consequences and causes distress in the weeks following injury is associated with later development of somatic symptom disorder. Patients with somatic symptom disorder after head injury report more pain and post-concussion symptoms. They are significantly more likely to have comorbid major depressive disorder and anxiety disorders compared to those without this condition. neurologyopen.bmj
The systematic review examining the relationship between somatic symptoms and related disorders and mild traumatic brain injury found that the majority of acceptable evidence supported a relationship between these conditions. Nine studies reported associations between functional seizures and a history of mild traumatic brain injury. In comparison, 31 studies assessed relationships between questionnaires measuring somatic symptom disorder burden and mild traumatic brain injury. Three studies investigated healthcare practitioners’ diagnosis of somatic symptoms and related disorders and post-mild traumatic brain injury symptom burden, collectively demonstrating the strong connection between head trauma and subsequent development of somatic complaints. foundationhealth
Cardiovascular complications represent another significant overlapping risk following head injury. Research demonstrates that individuals with moderate-to-severe traumatic brain injury have increased rates of self-reported hypertension and stroke but lower rates of myocardial infarction and congestive heart failure than uninjured adults. The findings highlight the importance of early screening for and management of cardiovascular risk factors in individuals with chronic traumatic brain injury, particularly those of younger age, who are not typically thought to be at risk for these conditions. ahajournals
The relationship between blood pressure and traumatic brain injury follows a complex U-shaped pattern, with both hypotension and hypertension associated with worse outcomes. Early hypotension has been linked with poor outcomes following severe traumatic brain injury, but recent data suggest that arterial hypertension after injury is also associated with poor outcomes. The initial catecholamine response and resulting systemic hypertension may be protective to a point by maintaining cerebral perfusion pressure in the setting of impaired cerebral autoregulation after injury. Yet, catecholamine-induced hypertension may also cause secondary brain damage by aggravation of vasogenic edema and intracranial hypertension. pmc.ncbi.nlm.nih
Post-traumatic headaches affect approximately 40% of individuals who experience concussions, representing one of the most common and persistent symptoms following head injury. Patients can experience tension headaches, migraine headaches, and cervicogenic headaches (radiating from the neck) all at once, making treatment particularly challenging. Ninety-five percent of people with a concussion experience headache associated with that injury, and among those with headache, about two-thirds have migraine features. Individuals with a family history of migraine or preexisting headache disorders face a higher risk of developing post-traumatic headache. wexnermedical.osu+1
Sleep disturbances cluster with other post-traumatic brain injury symptoms, creating compounding difficulties for recovery. Changes in sleep architecture following injury cannot fully explain the extent and intensity of sleep-wake disturbances reported by patients. The current literature supports cognitive-behavioral therapy and sleep hygiene education, light therapy, and certain pharmacologic interventions for treating sleep disturbances in patients with brain injury, with early screening and individualized approaches prioritized to improve sleep and, consequently, speed recovery. pubmed.ncbi.nlm.nih
Exercise intolerance commonly results from a concussion, often limiting return to activities and quality of life. The reviewed studies support clinical suspicion of autonomic dysfunction as an important component of exercise intolerance, though specific mechanisms of impairment and relationships to symptoms and recovery require additional investigation. Post-concussive exercise intolerance has been linked to a reduction in cerebral blood flow, theoretically prolonging the effects of the metabolic energy crisis associated with injury. pmc.ncbi.nlm.nih
Mental health complications, including anxiety, depression, post-traumatic stress disorder, and behavioral changes, frequently develop following head injury. Brain injuries, no matter how severe, commonly cause emotional and behavioral changes, including emotional lability with extreme mood swings, anxiety disorders, depression, impulsive behaviors, flat affect, a lack of emotional expression, and a lack of empathy and social skills. These psychological changes can cause unnecessary suffering and, in cases of severe depression and anxiety, can even halt physical recovery progress. flintrehab
Understanding Long-Lasting Injuries- Video
Non-Surgical Treatments to Improve Somatovisceral Function
Fortunately, numerous non-surgical treatment approaches have demonstrated effectiveness in improving somatovisceral function and promoting recovery following head injuries. These interventions work through various mechanisms to restore proper communication between the brain and the body, balance the autonomic nervous system, and support the brain’s natural healing processes. Dr. Jimenez’s clinical practice emphasizes comprehensive non-invasive protocols, prioritizing natural recovery and avoiding unnecessary surgeries or medications.
Chiropractic Care and Spinal Adjustments
Chiropractic care focuses on the spine and nervous system, recognizing that the spine houses the spinal cord, which acts as the communication superhighway between the brain and body. For traumatic brain injury patients, proper spinal alignment becomes crucial because misalignment caused by the injury itself or associated whiplash can worsen symptoms like headaches, brain fog, and balance issues. Chiropractic care aims to restore proper alignment, thereby improving nervous system function and supporting the brain’s ability to heal. northwestfloridaphysiciansgroup Chiropractic adjustments help alleviate post-traumatic brain injury symptoms by releasing pressure on irritated nerves and improving joint function. For many patients, this results in improved comfort and reduced reliance on pain medication. Proper spinal alignment promotes better blood flow to the brain. Since the brain requires oxygen-rich blood to heal and function, improved circulation directly supports recovery from traumatic brain injury while reducing dizziness and fatigue. northwestfloridaphysiciansgroup
Research demonstrates that chiropractic intervention can modify proprioceptive input from more functional spinal joints, helping restore this input to the brain’s multisensory integration centers. Studies of patients receiving chiropractic care in neurorehabilitation hospitals have shown that spinal manipulation influences pain through complex mechanisms in the central nervous system. A case study documenting concussion treatment using massage and manipulation techniques showed diminished concussion symptoms. It regained ease in cervical range of motion, highlighting the potential importance of manual therapy in reducing headache, dizziness, and nausea during concussion recovery. pmc.ncbi.nlm.nih+2 Dr. Jimenez explains that by realigning the spine through chiropractic adjustments, treatment reduces nerve interference, optimizing mind-body communication, and enhancing overall function. The adjustments improve cerebral blood flow and reduce inflammation, thereby accelerating recovery from head injury. With enhanced nervous system function comes improved mental clarity, including reduced brain fog, sharper focus, and better memory, while also promoting stress relief and alleviating irritability and emotional strain often linked to head injuries. zakerchiropractic
Vestibular Rehabilitation
Vestibular rehabilitation is a specialized form of physical therapy that focuses on strengthening the connections between the brain, eyes, inner ear, muscles, and nerves. This treatment approach proves particularly valuable for post-concussion patients experiencing dizziness, vertigo, balance problems, and spatial impairment. According to a review in the British Journal of Medicine, vestibular therapy reduced symptoms in patients with sports-related concussions faster, with patients three times as likely to return to play within eight weeks of therapy compared to those who didn’t receive treatment. denverphysicalmedicine+1 Vestibular rehabilitation therapy involves exercises designed to improve the functioning between the inner ear, brain, eyes, muscles, and nerves. These exercises help minimize balance issues and treat dizziness, vertigo, and spatial orientation deficits caused by vestibular impairments that some individuals experience after brain injury. The therapy addresses problems in the inner ear through specific exercises designed to improve balance and coordination. biausa
The Epley Maneuver represents a simple yet effective exercise to treat benign paroxysmal positional vertigo, a very specific form of vertigo quite common after traumatic brain injury. During vestibular rehabilitation, benign paroxysmal positional vertigo generally responds well to the Epley Maneuver, and patients learn to perform the movement at home to alleviate symptoms as they arise. Studies have shown that vestibular rehabilitation is an effective modality for managing dizziness, vertigo, and imbalance following concussion. However, careful consideration of the injury’s acuity and effective management of comorbid conditions will optimize results. pubmed.ncbi.nlm.nih+1 Co-morbidities, including cognitive and behavioral issues, visual-perceptual dysfunction, metabolic dysfunction, and autonomic dysfunction, may hamper the effectiveness of traditional vestibular rehabilitation approaches. Working closely with other disciplines well-versed in treating comorbid conditions helps individuals achieve optimal recovery. Dr. Jimenez’s integrated practice model exemplifies this multidisciplinary approach, bringing together chiropractic care, functional medicine, physical therapy, and other specialties to provide comprehensive treatment for patients with vestibular dysfunction following head injuries. pubmed.ncbi.nlm.nih
Physical Therapy and Exercise Rehabilitation
Physical therapy plays a pivotal role in optimizing recovery and enhancing functional independence after brain injury. Therapeutic approaches include gait training to improve walking patterns, balance activities to enhance stability and prevent falls, strength training to rebuild muscle mass and function, coordination exercises to improve fine and gross motor skills, and range-of-motion exercises to maintain flexibility. In some cases, physical therapists recommend body-weight-supported treadmill training to help patients safely relearn walking patterns. Family and caregiver training proves extremely important and helpful, as loved ones can gain an understanding of how the brain works and the specific nature of the injury, supporting the rehabilitation process. biausa
Available evidence demonstrates the potential of exercise in improving cognitive impairment, mood disorders, and post-concussion syndrome following traumatic brain injury. Exercise rehabilitation has been shown to attenuate cognitive deficits in animal models by stimulating cerebral signaling pathways, with treadmill exercise improving memory by modulating neurotransmitter systems and neurotrophic factors. High-intensity interval training helps regulate the autonomic nervous system while boosting brain-derived neurotrophic factor, thereby promoting neuroplasticity, an essential factor for recovery. sciencedirect+1 However, exercise prescription following head injury requires careful consideration, as exercise intolerance commonly results from concussion and autonomic dysfunction. Graded exercise testing while monitoring symptoms and heart rate helps guide a safe return to physical activity. Current clinical practice involves careful assessment to determine appropriate exercise intensity and duration, gradually progressing as autonomic function improves. pmc.ncbi.nlm.nih
Acupuncture and Neuroplasticity Enhancement
Acupuncture has gained widespread recognition as an effective, low-cost treatment for neurological rehabilitation with minimal adverse effects. Clinical and experimental evidence documents the potential of acupuncture to ameliorate injury-induced neurological deficits, particularly sequelae such as dyskinesia, spasticity, cognitive impairment, and dysphagia. These effects relate to acupuncture’s ability to promote spontaneous neuroplasticity after injury. pmc.ncbi.nlm.nih+1 Specifically, acupuncture can stimulate neurogenesis, activate axonal regeneration and sprouting, and improve the structure and function of synapses. These processes modify the neural network and the function of the damaged brain area, leading to improvements in various skills and adaptability. Astrocytes and microglia may be involved in acupuncture-induced regulation of neuroplasticity, for example, by producing and releasing multiple neurotrophic factors, including brain-derived neurotrophic factor and nerve growth factor. pmc.ncbi.nlm.nih
Studies have shown that acupuncture reduces neuroinflammation after brain injury. A study published in The Journal of Neuroinflammation found that acupuncture significantly reduced neuroinflammation and improved cognitive function in animal models of brain injury. By modulating inflammatory pathways, acupuncture helps reduce the production of pro-inflammatory cytokines, promoting brain healing and reducing symptoms such as headaches and dizziness. betsygordonacupuncture Acupuncture enhances neuroplasticity, which is crucial for recovery after brain injury, facilitating improvements in memory, learning, and overall cognitive function. Research in Neural Regeneration highlighted that acupuncture promotes neuroplasticity, which is essential for rehabilitation. Studies demonstrate that acupuncture improves mental performance and reduces anxiety and depression in patients recovering from brain injuries. betsygordonacupuncture+1 Dr. Jimenez’s functional medicine practice incorporates acupuncture and electro-acupuncture as part of comprehensive care plans for patients recovering from head injuries. His team uses these modalities in combination with other therapies to create customized treatment approaches that promote natural healing, mobility, and long-term wellness.
Nutritional Interventions and Functional Medicine
Nutrition plays a positive role during acute traumatic brain injury recovery, with patient needs being unique and requiring individualized approaches. Following mild traumatic brain injury, patients who consumed enough food to meet calorie and macronutrient (particularly protein) needs specific to their injury severity and sex within 96 hours post-injury had reduced length of hospital stay. Patients receiving nutrients and non-nutrient support within 24-96 hours post-injury had positive recovery outcomes, including omega-3 fatty acids, vitamin D, magnesium oxide, N-acetyl cysteine, and hyperosmolar sodium lactate. frontiersin Traumatic brain injury contributes to extensive dysbiosis of the gastrointestinal system, leading to worsened outcomes, making nutritional support essential. Early nutrition supports preservation of muscle mass, decreases infection complications, promotes cerebral homeostasis, and improves recovery outcomes. The human brain consumes 20% of total resting energy, despite accounting for only 2% of total body mass, underscoring the critical role of adequate nutrition for healing. xiahepublishing
A recent clinical trial demonstrated that dietary changes significantly reduce persistent post-traumatic headaches, a common and debilitating consequence of traumatic brain injury. Researchers found that increasing omega-3 fatty acids (commonly found in fatty fish) while reducing omega-6 fatty acids (abundant in seed oils) led to fewer and less severe headaches. Participants assigned to the intervention diet experienced approximately two fewer headache days per month and a 30% reduction in daily headache pain intensity compared to the control diet group. med.unc Supplementing with omega-3 fatty acids can reduce inflammation and oxidative stress, promote brain-cell survival, and help the brain recover from injury. Vitamins D and E, niacin, zinc, and magnesium have neuroprotective benefits, and supplementing with these vitamins and minerals has been shown to improve recovery, especially in deficient patients. An energy-balanced, anti-inflammatory diet with adequate sources of omega-3 fats and appropriate vitamin D supplementation proves especially important for patients with a history of traumatic brain injury. consultant360
Dr. Jimenez’s practice embraces Functional Integrative Medicine, a patient-focused approach that treats the whole person rather than just symptoms. His team offers detailed health assessments that evaluate genetics, lifestyle, environmental exposures, and psychological factors to create comprehensive health profiles. By combining Institute for Functional Medicine programs with personalized nutrition plans, Dr. Jimenez helps patients address chronic conditions and optimize brain health following head injuries.
Massage Therapy and Manual Techniques
Massage therapy provides valuable support in brain injury rehabilitation, enhancing physical, mental, and emotional well-being. Massage significantly improves blood circulation, ensuring that essential nutrients and oxygen are efficiently delivered to brain cells. By increasing circulation, the brain’s healing process is expedited, promoting cellular regeneration and reducing the risk of secondary complications. Improved blood flow also helps reduce swelling and inflammation, common challenges following brain injury. neuropraxisrehab Post-brain injury pain can be debilitating and hinder recovery, but massage therapy helps alleviate pain by targeting tense muscles and releasing built-up tension. Through gentle manipulation, massage therapists can improve muscle flexibility and joint mobility, relieving discomfort and enhancing overall physical comfort. Brain injuries often lead to muscle stiffness and reduced range of motion, but massage therapy techniques such as stretching and kneading help improve flexibility by breaking down scar tissue and adhesions. neuropraxisrehab
Specific massage modalities show promise for traumatic brain injury recovery. Manual Lymphatic Drainage uses light massage to stimulate the flow of lymphatic fluid, potentially increasing the lymphatic system’s ability to clear waste products from the brain. A case study combining Manual Lymphatic Drainage with craniosacral therapy and glymphatic system techniques resulted in an 87% reduction of concussion symptoms after three months of treatment. concussionalliance A case study documenting massage intervention for post-concussion treatment demonstrated complete return to pre-concussion activities and function with no continued symptoms following a short and specific massage series. The therapy focused on restoring ideal alignment of the atlanto-occipital joint, resulting in reduced pain, muscle hypertonicity, headaches, reduced medication use, and improved balance, posture, cervical range of motion, mental focus, and physical activity. pmc.ncbi.nlm.nih
Dr. Jimenez’s comprehensive approach includes specialized massage and manual therapy techniques, integrated with chiropractic care and other modalities. His team focuses particularly on neck and shoulder areas to reduce effects patients experience after traumatic brain injuries, with goals including improved neck mobility, reduction of headaches and nerve pain, and addressing balance, dizziness, and vertigo issues through specific therapeutic techniques. newapproachescenter
Cognitive Behavioral Therapy and Psychological Support
Cognitive Behavioral Therapy has been demonstrated to be effective by over 1,000 studies involving 10,000 patients, making it one of the most scientifically verified psychotherapy treatments available. CBT has been successfully used on a variety of disorders, including traumatic brain injury patients with post-concussional symptoms and secondary effects such as anxiety and fatigue. The therapy focuses on the relationship between thoughts, feelings, and behaviors, built around three core principles: beliefs create feelings, feelings dictate behavior, and behavior reinforces beliefs.flintrehab A new meta-analysis found substantial evidence for the use of cognitive behavioral therapy in managing anxiety and depression in patients with traumatic brain injury. Researchers identified that CBT interventions had immediate effects of reducing depression and anxiety, with sustained impacts for depression at the three-month follow-up. Effects were greater in groups that received individualized CBT than in those that received group-based CBT. headway
CBT proves particularly valuable for addressing recovery expectations and perceived consequences of traumatic brain injury. Behavioral techniques such as relaxation, behavioral activation, and stress management help patients manage the anxiety, depressive symptoms, and insomnia that can be present following injury. In the acute phase of recovery, brief psychoeducational and cognitive behavioral interventions have consistently been shown to result in improvement in managing cognitive and psychological symptoms for brain injury survivors. abct For patients with cognitive impairment, CBT can be adapted with modifications including simplified concepts, concrete behavioral examples, pictorial handouts and cues, considerable repetition, and booster sessions. Studies found that adapted CBT was able to reduce anxiety and depression in patients who suffered moderate to severe traumatic brain injury. CBT helps patients identify and challenge unhelpful or inaccurate thoughts that can arise or intensify after injury, while focusing on behavioral activation and engaging in meaningful, important activities, which can boost mood and decrease isolation. cbtdenver+1
Mind-Body Therapies and Somatic Approaches
Mind-body therapies have gained recognition for their effectiveness in treating trauma-related symptoms and supporting nervous system regulation. More than 80% of specialized programs to treat post-traumatic stress disorder offer some form of mind-body therapy, including yoga, relaxation, tai chi, guided imagery, and mindfulness practices. These approaches prove particularly valuable for individuals experiencing somatic symptoms following head injuries. research.va Somatic therapy helps individuals reconnect with their bodies through awareness of physical sensations and their relationship to emotional experiences. For patients with head injuries who may feel disconnected from their bodies or experience persistent physical symptoms, somatic approaches provide pathways for healing by working through sensations in safe and supportive environments. Techniques such as grounding exercises, deep breathing, mindful observation of physical sensations, and guided movement empower individuals to explore how trauma manifests physically and provide avenues for release. pacmh
Yoga as a whole significantly reduced post-traumatic stress disorder symptoms in research studies, with a positive impact comparable to that of psychotherapeutic and psychopharmacologic approaches. Yoga may improve the functioning of traumatized people by helping them tolerate physical and sensory experiences associated with fear and helplessness, and increasing emotional awareness and affect tolerance. For individuals recovering from head injuries, gentle yoga practices adapted to their current functional abilities can support both physical and psychological healing. research.va The Polyvagal theory provides a powerful framework for understanding how trauma affects the nervous system and pathways for healing. The theory centers on the autonomic nervous system as a key component in trauma recovery, emphasizing the role of the vagus nerve in regulating physiological and emotional states. Basic somatic exercises can bring the nervous system out of dysfunction, beginning to retrain safety and social cues. This proves particularly helpful for individuals with head injuries who experience autonomic dysregulation and hypervigilance. pyramid-healthcare
Breathing Practices and Vagal Tone Restoration
Voluntary regulated breathing practices offer accessible and effective means to support autonomic nervous system regulation and restore vagal tone. These practices draw on both modern scientific studies and ancient concepts, with applications ranging from clinical anxiety treatment to stress reactivity reduction. Effective breathing interventions support greater parasympathetic tone, which can counterbalance the high sympathetic activity intrinsic to stress and dysfunction following head injury. pmc.ncbi.nlm.nih The physiological sigh is a simple yet powerful breathing technique that involves two nose inhales, followed by a long exhale through the mouth. This technique rapidly reduces stress and calms the nervous system by leveraging the interaction between the sympathetic (arousing) and parasympathetic (calming) branches of the autonomic nervous system to control heart rate and promote calm. Studies have shown that this breathing pattern effectively reduces arousal and returns the body to baseline functioning. hubermanlab+1
Deep, slow breathing benefits vagal outflow, with evidence suggesting particular benefits for older adults in restoring vagal tone. One session of deep and slow breathing can produce measurable improvements in heart rate variability metrics associated with parasympathetic activity. Regular practice of paced breathing at approximately six cycles per minute, significantly lower than the standard respiratory rate of 12 to 20 breaths per minute, can enhance vagal tone and improve overall autonomic regulation. pmc.ncbi.nlm.nih+1 Heart rate variability biofeedback is an innovative, non-invasive, evidence-based technique that enhances vagal nerve activity by combining slow-paced breathing with real-time feedback. The practice proves simple to implement, cost-effective, and carries minimal risk, making it an accessible tool for various health interventions. HRV biofeedback likely modulates neuroplasticity in autonomic control centers, enhancing parasympathetic tone and improving cardiac efficiency, reducing sympathetic overactivation, and lowering systemic inflammation. pmc.ncbi.nlm.nih
Improving Central Nervous System Function and Communication
The comprehensive non-surgical treatments described work synergistically to improve central nervous system function and restore proper communication between the brain and body. These approaches target multiple aspects of neurological health, from cellular-level processes to whole-system integration, supporting the brain’s remarkable capacity for adaptation and healing known as neuroplasticity. Neuroplasticity represents the brain’s ability to reorganize and form new neural connections throughout life, enabling recovery from injury by creating alternative pathways when original circuits become damaged. Following a brain injury, neuroplasticity’s ability to adapt becomes crucial, as these injuries frequently result in severe impairments. Rehabilitation strategies exploit neuroplasticity, leveraging the brain’s plasticity to promote healing through approaches ranging from constraint-induced movement therapy to virtual reality and brain-computer interfaces. pmc.ncbi.nlm.nih
The integration of multiple treatment modalities enhances neuroplastic responses and accelerates recovery. Combining chiropractic care with vestibular rehabilitation, for example, addresses both spinal alignment and sensory integration, creating synergistic effects that amplify benefits beyond what either treatment could achieve alone. Similarly, pairing nutritional interventions with physical therapy provides both the structural building blocks and functional stimulation necessary for optimal neural repair and reorganization. frontiersin+4 Dr. Jimenez’s practice exemplifies this integrated approach, combining specialized chiropractic protocols with wellness programs, functional and integrative nutrition, agility and mobility fitness training, and rehabilitation systems for all ages. The team has taken great pride in providing patients with only clinically proven treatment protocols, using an integrated approach to create personalized care plans that often include functional medicine, acupuncture, electro-acupuncture, and sports medicine principles. The goal is to relieve pain naturally by restoring the body’s health and function through holistic wellness as a lifestyle.
Restoring Vagal Tone and Autonomic Balance
The vagus nerve, as the main neural component of the parasympathetic nervous system, plays a crucial role in maintaining physiological homeostasis. The vagus nerve starts in the brain and ends in the abdomen, and it controls the involuntary functions of the heart, lungs, digestive system, liver, and kidneys. Following a head injury, vagal tone frequently becomes diminished, contributing to autonomic dysfunction and associated symptoms. pmc.ncbi.nlm.nih+3 Heart rate variability is a non-invasive biomarker of vagal tone and autonomic flexibility, with reduced HRV associated with cardiovascular diseases, hypertension, inflammation, and mental health disorders. Non-invasive vagal neuromodulation through HRV biofeedback and similar interventions could potentially serve as rehabilitative strategies to restore autonomic balance, mitigate post-injury fatigue, and improve cardiovascular function. pmc.ncbi.nlm.nih
Practices such as breathwork, cold exposure, exercise, meditation, taking probiotics, laughter, singing, massages, and relaxation exercises help improve vagal tone. These accessible interventions provide multiple pathways for patients to actively participate in their recovery, building resilience and enhancing the body’s natural regulatory capacities. High vagal tone is associated with greater resilience to stress, promoting parasympathetic activation and reducing physiological stress responses, such as increased heart rate and muscle tension. neurodivergentinsights+1 The Safe and Sound Protocol represents another non-invasive approach engaging the ventral vagal complex via auditory-motor pathways, facilitating neuroplasticity and enhancing emotional regulation. This protocol may function by modulating the prefrontal cortex’s influence on autonomic outflow, thereby promoting a shift toward parasympathetic dominance. Combined with heart rate variability biofeedback, these approaches offer promising avenues for restoring vagal tone and autonomic balance following head injury. pmc.ncbi.nlm.nih
A Questionnaire Example of TBI Symptoms
Enhancing Communication Between Brain and Body
Effective treatment of head injuries requires addressing the fundamental disruption in communication between the brain and body that occurs following trauma. The somatovisceral response, characterized by intricate interactions between somatic (bodily) and visceral (organ) systems, depends on intact nerve signal transmission for proper function. When head injuries disrupt these communication pathways, comprehensive interventions targeting multiple levels of the nervous system become necessary. foundationhealth
Chiropractic care directly addresses communication disruption by restoring proper spinal alignment, reducing nerve interference, and optimizing signal transmission between the brain and body. Research demonstrates that chiropractic adjustments can improve brain function by supporting proper cerebrospinal fluid flow and blood circulation, which are crucial for healing after traumatic brain injuries. By facilitating a return to the preferred anatomical form through therapy, function is restored, allowing a complete return to pre-injury activities. hmlfunctionalcare+2
Vestibular rehabilitation specifically targets multisensory integration, recognizing that the vestibular system contributes to multisensory binding, giving rise to a unified multisensory experience that underlies self-representation and bodily self-awareness. By addressing vestibular dysfunction through targeted exercises, therapy helps restore temporal binding of sensory information, reducing perceptual chaos and improving coherence of physical experience.pmc.ncbi.nlm.nih
Acupuncture enhances brain-body communication through multiple mechanisms, including stimulation of neuroplasticity, modulation of neurotransmitter systems, and regulation of inflammatory processes. The effect of acupuncture begins with the stimulation of acupoints, which converts physical or chemical information into electrical activity that sends signals along afferent fibers to the spinal cord and brain. This modulation of neural structure and function supports restoration of proper communication throughout the nervous system. pmc.ncbi.nlm.nih
Functional medicine approaches recognize that optimal brain-body communication requires addressing multiple factors, including nutrition, inflammation, gut health, hormone balance, and detoxification. Dr. Jimenez’s practice uses detailed Institute for Functional Medicine Collaborative Assessment Programs focused on Integrative Treatment Protocols, thoroughly evaluating personal history, current nutrition, activity behaviors, environmental exposures to toxic elements, and psychological and emotional factors. This comprehensive approach addresses the root causes of chronic disorders, treating the person holistically rather than just managing symptoms.
Improving Somatic and Autonomic Systems
The ultimate goal of comprehensive treatment for head injuries is to restore balance and proper function to both the somatic (voluntary) and the autonomic (involuntary) nervous systems. The somatic nervous system connects to most senses. The voluntary nervous system controls voluntary muscle movements, while the autonomic nervous system regulates involuntary bodily functions, including heart rate, blood pressure, digestion, and breathing. clevelandclinic Following a head injury, both systems frequently become dysregulated, leading to wide-ranging symptoms affecting physical function, cognitive abilities, and emotional well-being. Addressing this dysregulation requires integrated approaches that simultaneously target physical alignment, sensory processing, autonomic balance, and neuroplasticity. pmc.ncbi.nlm.nih+1
Physical therapy, including vestibular rehabilitation and gait training, directly addresses somatic system function by retraining movement patterns, improving balance and coordination, and rebuilding strength and endurance. These interventions leverage neuroplasticity to establish new motor programs and compensatory strategies, supporting functional recovery even when some neural damage persists. pmc.ncbi.nlm.nih+1
Autonomic system restoration requires approaches specifically targeting vagal tone and parasympathetic activation. Heart rate variability biofeedback, breathing practices, massage therapy, and acupuncture all support enhanced parasympathetic tone, helping shift the nervous system from states of hyperarousal toward balanced regulation. Dr. Jimenez emphasizes that, by focusing on flexibility, agility, and strength through tailored programs, his practice helps patients of all ages thrive despite health challenges.massgeneral+3
Nutritional interventions support both somatic and autonomic function by providing essential building blocks for neural repair, reducing inflammation, supporting mitochondrial function, and optimizing neurotransmitter production. Omega-3 fatty acids, for example, reduce inflammation and oxidative stress while promoting brain cell survival, supporting both structural repair and functional optimization.xiahepublishing+2
Cognitive-behavioral therapy and mind-body approaches address the psychological and emotional factors that influence both somatic and autonomic function. By helping patients reframe unhelpful thoughts, manage anxiety and depression, and develop healthy coping strategies, these interventions support overall nervous system regulation and functional recovery.pacmh+3
The Path Forward: Integrative Care for Head Injury Recovery
Recovery from head injuries represents a complex journey requiring patience, persistence, and comprehensive support. The disruption to brain-body communication and development of somatovisceral disorders following head trauma creates challenges that cannot be addressed through single-modality treatments. Instead, the most effective approach involves integrated care that simultaneously addresses physical alignment, sensory processing, autonomic regulation, nutrition, psychological well-being, and neuroplasticity enhancement. Dr. Jimenez’s practice in El Paso exemplifies this integrative model, bringing together chiropractic care, functional medicine, physical therapy, acupuncture, and other evidence-based approaches to provide comprehensive treatment tailored to each patient’s unique needs. His philosophy recognizes that the body has an innate healing capacity when provided with proper support, emphasizing natural recovery methods over invasive procedures or addictive medications. The evidence reviewed throughout this article demonstrates that non-surgical treatments can effectively improve somatovisceral function, restore vagal tone, enhance brain-body communication, and support recovery of both somatic and autonomic nervous systems. These approaches work synergistically, creating conditions that support the brain’s remarkable capacity for adaptation and healing through neuroplasticity. pubmed.ncbi.nlm.nih+6
For individuals recovering from head injuries, seeking comprehensive evaluation and integrated treatment early in the recovery process offers the best opportunity for optimal outcomes. Dr. Jimenez emphasizes that early identification of at-risk patients appears feasible, with somatic symptom disorder potentially serving as a useful framework for conceptualizing poor outcomes from mild traumatic brain injury in patients with prominent psychological distress and guiding rehabilitation. neurologyopen.bmj The future of head injury treatment lies in continued refinement of these integrated approaches, with ongoing research exploring optimal combinations of interventions, timing of treatment initiation, and personalization based on individual patient characteristics. As understanding of brain-body connections deepens and evidence for non-surgical treatments continues to accumulate, patients have increasing reason for hope that recovery is possible with the right comprehensive support. frontiersin
Conclusion
Head injuries create profound disruptions to the intricate communication systems connecting brain and body, leading to somatovisceral disorders that affect multiple body systems simultaneously. Understanding how environmental factors influence brain activity, how symptoms overlap and cluster, and how daily functioning becomes impaired provides essential context for developing effective treatment approaches. The comprehensive evidence reviewed demonstrates that non-surgical treatments, including chiropractic care, vestibular rehabilitation, physical therapy, acupuncture, nutritional interventions, massage therapy, cognitive behavioral therapy, and mind-body practices, can effectively restore function following head injuries. These interventions work through multiple mechanisms to improve central nervous system function, restore vagal tone and autonomic balance, and enhance communication between the brain and the body, ultimately supporting the recovery of both somatic and autonomic systems.
Dr. Alexander Jimenez’s clinical observations and integrative treatment approach in El Paso, Texas, exemplify how combining these evidence-based modalities into personalized care plans can help patients achieve optimal recovery. By focusing on the body’s natural healing capacity and addressing root causes rather than just symptoms, this comprehensive approach offers hope for individuals recovering from head injuries and experiencing somatovisceral disorders. The journey of recovery requires patience, persistence, and proper support. Still, with integrated care addressing all aspects of health, individuals can work toward restored function, reduced symptoms, and improved quality of life. As research continues to advance understanding of brain-body connections and treatment effectiveness, the future holds promise for even more refined and effective approaches to supporting recovery following head injuries.
References
Jobin, K., Wilson, A. J., King, R., Eliason, P. H., Galarneau, J., Gilmour, G. S., & Debert, C. T. (2025). Somatic symptom and related disorders and mild traumatic brain injury: A systematic review. Biopsychosocial Science and Medicine. https://doi.org/10.1097/PSY.0000000000001427
Silverberg, N. D., Rioux, M., Mikolić, A., Perez, D. L., Burke, M. J., & Howard, A. (2025). Somatic symptom disorder after mild traumatic brain injury. Journal of Head Trauma Rehabilitation. https://doi.org/10.1097/HTR.0000000000001068
Braun, T., & The ENIGMA Consortium. (2024). How does the macroenvironment influence brain and behaviour—a review. Molecular Psychiatry, 29, 3268–3286. https://doi.org/10.1038/s41380-024-02557-x
Harricharan, S., Nicholson, A. A., Densmore, M., Théberge, J., McKinnon, M. C., Neufeld, R. W., & Lanius, R. A. (2022). The brain-body disconnect: A somatic sensory basis for trauma-related disorders. Frontiers in Neuroscience, 16, Article 1015749. https://doi.org/10.3389/fnins.2022.1015749
Katz, D. I., Cohen, S. I., & Alexander, M. P. (2015). Mild traumatic brain injury. Handbook of Clinical Neurology, 127, 131-156.
Hilz, M. J., Wang, R., Xu, X., & Reichmann, H. (2017). Autonomic dysfunction after mild traumatic brain injury. Frontiers in Neurology, 8, Article 511. https://doi.org/10.3389/fneur.2017.00511
Yuan, J., Liu, W., Liang, Q., Wang, Y., Liu, M., & Zhang, J. (2023). Negative environmental influences on the developing brain. Exploration of Medicine, 4(5), 804-820. https://doi.org/10.37349/emed.2023.00169
Baguley, I. J., Heriseanu, R. E., Cameron, I. D., Nott, M. T., & Slewa-Younan, S. (2008). A critical review of the pathophysiology of dysautonomia following traumatic brain injury. Neurocritical Care, 8(2), 293-300.
Calderón-Garcidueñas, L., Hernández-Luna, J., Mukherjee, P. S., Styner, M., Chávez-Franco, D. A., Luévano-Castro, S. C., … & González-Maciel, A. (2024). Air pollution and brain health. Environmental Health Sciences Center. https://environmentalhealth.ucdavis.edu/air-pollution/brain-health
Poldrack, R. A., Shine, J. M., Shine, R., Ferguson, M. A., Pessoa, L., Lindquist, M. A., & Uddin, L. Q. (2024). A longitudinal single-subject neuroimaging study reveals the effects of daily environmental, physiological, and lifestyle factors on functional brain connectivity. PLOS Biology, 22(10), Article e3002797.
Gianaros, P. J., & Jennings, J. R. (2025). Brain–body states as a link between cardiovascular and mental health. Trends in Neurosciences. https://doi.org/10.1016/j.tins.2025.01.017
Russo, M. A., Santarelli, D. M., & O’Rourke, D. (2021). Benefits from one session of deep and slow breathing on vagal tone and anxiety in young and older adults. Scientific Reports, 11, Article 19267. https://doi.org/10.1038/s41598-021-98736-9
Stude, D., & Mick, G. (2018). Patients receiving chiropractic care in a neurorehabilitation hospital: A retrospective case series. Journal of Chiropractic Medicine, 17(2), 127-136. https://doi.org/10.1016/j.jcm.2017.11.008
Haavik, H., Kumari, N., Holt, K., Niazi, I. K., Amjad, I., Pujari, A. N., … & Murphy, B. (2024). Effect of chiropractic intervention on oculomotor and attentional performance. Brain Sciences, 14(5), Article 423.
Choi, W. J., & Kim, M. J. (2023). Nutritional support following traumatic brain injury. Exploratory Research and Hypothesis in Medicine, 8(4), 389-403. https://doi.org/10.14218/ERHM.2022.00086
Schneider, A. L. C., Lakshminarayan, K., Peterlin, B. L., & Gottesman, R. F. (2013). Vestibular rehabilitation following mild traumatic brain injury. NeuroRehabilitation, 32(3), 519-528.
Chavez, L. M., Huang, S. S., MacDonald, I., Lin, J. G., Lee, Y. C., & Chen, Y. H. (2021). Effect of acupuncture on neuroplasticity of stroke patients with motor dysfunction: A meta-analysis of fMRI studies. Evidence-Based Complementary and Alternative Medicine, 2021, Article 8841720.
Wright, A. D., Smirl, J. D., Bryk, K., & van Donkelaar, P. (2023). Autonomic dysfunction and exercise intolerance in concussion: A narrative review. Journal of Athletic Training, 58(7-8), 539-550. https://doi.org/10.4085/1062-6050-0103.22
Morin, M., & Dumoulin, S. O. (2015). Concussion treatment using massage techniques: A case study. Journal of Bodywork and Movement Therapies, 19(2), 252-258. https://doi.org/10.1016/j.jbmt.2014.04.012
Hassett, L. M., Moseley, A. M., Harmer, A. R., & Mackey, M. G. (2021). The benefits of exercise for outcome improvement following traumatic brain injury: A systematic review. Experimental Neurology, 350, Article 113960.
Gisolfi, A., Wagner, A. K., Rasmussen, S., & Borrasso, A. J. (2025). The acceptability of somatic therapy for PTSD among patients in primary care. Families, Systems, & Health. https://doi.org/10.1037/fsh0001007
Kulkarni, M., Brown, R., Stuart, R., Tahir, H., & Granner, M. A. (2025). Altered autonomic cardiovascular function in adults with persisting post-concussion symptoms and exercise intolerance. Physiological Reports, 13(11), Article e70378.
Davis, D. W., Harris, O. A., & Frim, D. M. (2023). Massage therapy may be safe and reduce pain in critically ill patients with acute neurological injury. Brain Injury, 37(10), 998-1005. https://doi.org/10.1080/02699052.2023.2247990
Lim, J. A., Salles, A., & You, J. S. (2025). Exercise effects on cardiovascular, autonomic, cerebrovascular, and cognitive functions in spinal cord injury. Journal of Neurotrauma. https://doi.org/10.1089/neu.2024.0523
Ćwirlej-Sozańska, A., Sozański, B., Wiśniowska-Szurlej, A., & Wilmowska-Pietruszyńska, A. (2023). Adaptive neuroplasticity in brain injury recovery: Mechanisms, challenges and therapeutic implications. International Journal of Molecular Sciences, 24(18), Article 14210. https://doi.org/10.3390/ijms241814210
Clauw, D. J., & Chrousos, G. P. (2015). Chronic pain: Where the body meets the brain. Transactions of the American Clinical and Climatological Association, 126, 167-183.
Chopra, A., Diwan, A. D., & Cooney, M. (2025). Differentiating complex regional pain syndrome from somatic symptom disorder. PLOS Mental Health, 2(1), Article e0000214.
Khadka, S., Zhou, X., Dhiman, S., Hu, M., & Jiang, H. (2025). A comprehensive review of adaptive plasticity and recovery mechanisms following traumatic brain injury. Neurological Practice and Epidemiology, 7(1), Article 70006.
Modarres, M., Kuzma, N. N., Kretzmer, T., Pack, A. I., & Lim, M. M. (2024). Traumatic brain injury-induced disruption of the circadian clock. Brain, Behavior, & Immunity – Health, 36, Article 100724.
Cantor, J. B., Ashman, T., Gordon, W., Ginsberg, A., Engmann, C., Egan, M., … & Dijkers, M. (2024). Sleep and circadian rhythms after traumatic brain injury: A narrative review. Sleep Medicine Reviews, 81, Article 102065.
Willer, B., & Leddy, J. J. (2012). Medical therapies for concussion. Physical Medicine and Rehabilitation Clinics of North America, 23(2), 467-479.
Morrison, E. H., Cooper, D. B., Kennedy, J. E., Peskind, E. R., Cherman, T. S., & Yurgil, K. A. (2012). Desynchrony as a pathological outcome to traumatic brain injury. Translational Research in TBI, 2, Article 100109.
Cattelani, R., Zettin, M., & Zoccolotti, P. (2019). Psychological intervention in traumatic brain injury patients: An overview. Behavioural Neurology, 2019, Article 4182958. https://doi.org/10.1155/2019/4182958
Rasmussen, L. J. H., Caspi, A., Ambler, A., Broadbent, J. M., Cohen, H. J., d’Arbeloff, T., … & Moffitt, T. E. (2025). Neural correlates of fatigue after traumatic brain injury: Resting state and cognitive task performance. Brain Communications, 7(2), Article fcaf082.
Bose, B., Katznelson, L., & Bose, S. (2013). Hypertension after severe traumatic brain injury: Friend or foe? Journal of Neurosurgical Anesthesiology, 25(4), 455-462.
Mollayeva, T., D’Souza, A., Mollayeva, S., & Colantonio, A. (2024). Prevalence of fatigue and cognitive impairment after traumatic brain injury: An online population study. Archives of Physical Medicine and Rehabilitation, 105(6), 1145-1152.
Faden, A. I., Chan, P. H., & Longar, S. (1987). Treatment of hypertension associated with head injury. Annals of Emergency Medicine, 16(5), 545-549.
Jerath, R., Beveridge, C., & Barnes, V. A. (2023). Breathing practices for stress and anxiety reduction: Conceptual framework of implementation based on a systematic review of the published literature. Brain Sciences, 13(12), Article 1612.
Haarbauer-Krupa, J., Pugh, M. J., Prager, E. M., Harmon, N., Wolfe, J., & Yaffe, K. (2024). Prevalence of cardiovascular conditions after traumatic brain injury: A self-report study. Journal of the American Heart Association, 13(9), Article e033673.
Badjatia, N., Carney, N., Crocco, T. J., Fallat, M. E., Hennes, H. M., Jagoda, A. S., … & Vashi, N. (2024). Hypotension and adverse outcomes in moderate to severe traumatic brain injury: A TRACK-TBI study. JAMA Network Open, 7(11), Article e2447751.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine