Eric Velasco has a tremendous drive for being competitive, playing sports throughout his life. He was then referred to Push-as-Rx � by a friend and upon entering, he was challenged by the competitive workouts and he quickly fell in love. Eric pushed himself to give it his best, improving as his training progressed day by day alongside the help of the trainers and other groups at Push as Rx.
PUSH-as-Rx � is leading the field with laser focus supporting our youth sport programs.� The�PUSH-as-Rx � System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. �Immediately,�we adjust our methods for our athletes in order to optimize performance.� This highly adaptive system with continual�dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics.��PUSH-as-Rx � offers specialized extreme performance enhancements to our athletes no matter the age.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Ever since coming to Push-as-Rx �, Bill Skov has felt much more capable with his everyday activities and has learned to enjoy life much more. Bill Skov has lost weight and gained strength and stamina. Push as Rx means a lot to Mr. Skov and the relationships he’s had with all the trainers, together with their support, has encouraged him to push through with a healthy lifestyle.
PUSH-as-Rx � is leading the field with laser focus supporting our youth sport programs.� The�PUSH-as-Rx � System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. �Immediately,�we adjust our methods for our athletes in order to optimize performance.� This highly adaptive system with continual�dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics.��PUSH-as-Rx � offers specialized extreme performance enhancements to our athletes no matter the age.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Bryan Filidor, a wrestler for 7 years, strives to continue wrestling in college. Every day, Bryan comes to Push-as-Rx � where he trains hard and pushes himself in order to achieve his goal of becoming an Olympian. At Push as Rx, Bryan makes the best of his work outs and together with the trainer’s care, his endurance has helped him to exceed more than what he has already been accomplished. Bryan Filidor is grateful for coming to Push-as-Rx � because the trainers are there for him, no matter what.
PUSH-as-Rx � is leading the field with laser focus supporting our youth sport programs.� The�PUSH-as-Rx � System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. �Immediately,�we adjust our methods for our athletes in order to optimize performance.� This highly adaptive system with continual�dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics.��PUSH-as-Rx � offers specialized extreme performance enhancements to our athletes no matter the age.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Megan Dominguez, like many, exercised in regular gyms but, when she was talked into trying cross fit at Push-as-Rx �, she knew she wouldn’t be going back to her old routine. Megan described the trainers of Push as Rx as a family and since the beginning, she experienced an atmosphere of instant energy like no other. At Push-as-Rx �, Megan Dominguez was pushed to levels she never thought she could reach.
PUSH-as-Rx � is leading the field with laser focus supporting our youth sport programs.� The�PUSH-as-Rx � System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. �Immediately,�we adjust our methods for our athletes in order to optimize performance.� This highly adaptive system with continual�dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics.��PUSH-as-Rx � offers specialized extreme performance enhancements to our athletes no matter the age.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Chiropractor, Dr. Alexander Jimenez talks about strengthening the body without pain through pilates.
More than 20 years ago in a small walk up studio with hardwood floors that are creaky, several dancers and exercise enthusiasts would join several times for ‘ballet exercise’. In actuality, the motions of Joseph Pilates (Pil-lah-tees) (1880-1967) were in practice. The advantages from his approach removed stress, provided physical and mental balance, and helped to assemble in each individual streamlined and a strong musculature.
Joseph Pilates’ exercise philosophy can help women and men of any age. It’s especially advantageous to individuals who recognize the importance of providing a business support system for the backbone. Its focus is placed by the essence of Pilates on what’s termed the body’s ‘powerhouse.’ Here is the abdominal region, the buttocks, hips and low back – the centre of the body. Pilates works the deep muscles in the body making a powerful centre.
His teachings, “The Art of Contrology” unites mind and body to create a direct connection to the muscles. Each movement that is precise needs mental concentration as well as physical control. The mind and body learn to work together as one harmonious unit. Muscles are stretched and lengthened while building strength through soft, non-impact exercises that, as perfected, are designed to flow in rhythm from one move into the following.
Although, Pilates has been related to odd looking apparatus made up of springs cables and pulleys, or equipment termed the Reformer and also the Cadillac, the foundation is the mat work. Instead of machines and weights, the body uses its own resistance.
The Pilates�Philosophy
The Pilates philosophy incorporates basic principles some of which comprise control and concentration, respiration, and centering.
Concentration and Control includes visualizing the body as movement occurs. Each command that is mental sparks and teaches muscle control that, over time, can become exact. Engram is a medical term used to denote muscle memory, which is stored in the mind ‘s cerebrum. Like learning how to play a musical instrument, diligent practice results in wonderful music. In Pilates, emphasis is positioned on the grade of the motion, not the number of repetitions.
Centering focuses attention on the ‘power station’ – the energy source that flows outward to the extremities of the body. Anatomically, the spinal column is a significant component in the powerhouse. To support the spinal structures, its muscular system (i.e., gluteals, obliques, quadratus, trapezius, scalenes) must be powerful and flexible. Pilates mat work is made to build a strong basis for the entire spinal structure.
Breathing is taking in and expelling air. Breathing properly functions to oxygenate the entire body and cleanse it. Breathing needs complete inhalations and exhalations during the entire length of mat work or exercise when done correctly.
The Advantages Of Pilates
The advantages to be obtained from Pilates are numerous – learn the capability to keep up proper position, which leads to the entire well-being of the body – long, flexible muscles – increased joint range of movement – a flat lean stomach – enhanced circulation and stamina – better dexterity – this and more without pain and soreness often due to conventional forms of exercise.
To realize the numerous benefits Pilates offers does not mean buying clothing or special equipment. All that is needed is a willing disposition to improve the body. The exercises can be performed just about everywhere when completely stretched out the body fits. Many individuals who’ve started Pilates that are in the beginner level state how well they feel after only 8 or 10 sessions.
Check out Brooke Siler’s novel entitled The Pilates Body to find out more about Pilates. This is a superb novel and source for learning the essentials to begin Pilates without attending courses*. The illustrations, photographs and prompts Ms. Siler incorporates make the book easy to use at the mat. The Pilates exercises provided for the beginner, intermediate, and advanced participant are in her novel. Plus, an all-inclusive record of certified Pilates teachers (this is essential!) is provided by the end of her book.
*It is wise to consult with your doctor prior to starting any physical fitness or exercise plan.
Doctor of Chiropractic, Dr. Alexander Jimenez shares some insights about a pain free workday.
#1. Use�Healthy Posture & Movement Patterns
Considering all the emphasis on how little or much we should sit or stand at work, there is almost no discussion of technique in standing and sitting. Inferior technique slumpsitting, archsitting, parking weight is used by many people so on, and poorly on joints.
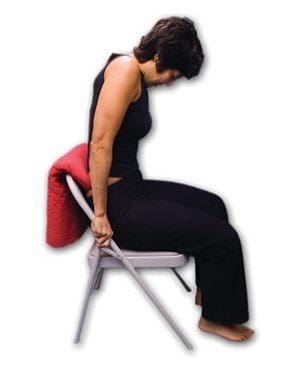
As long as this is actually true, any place is going to stack up badly in the research�we are starting to see it for standing and �ve seen this for sitting. Sitting has been much maligned as �the new smoking�; and now standing as a replacement is being demonstrated to cause increased hospitalization due to varicose veins, atherosclerosis that is increased, etc. A good starting point is stretchsitting, to start the journey back to a pain free workday. Stretchsitting is simple, safe, comfy, and therapeutic.
Work with flannel, a towel, or a Stretchsit pillow so it contacts you at mid-back, below the shoulder blades.
Scoot your bottom all the way back in the seat.
Lean forwards from the hips, like a mini crunch is being done by you, and tip your ribcage forward.
Push downwards on the armrests/side bars/seat pan of your chair to get a soft stretch in your lower back.
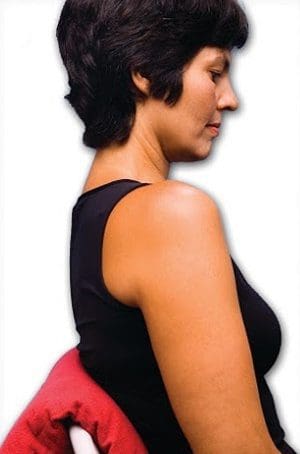
Keeping the stretch, lean back out of your hips and adhere your mid back on to the Stretchsit pillow/towel.
Relax completely, letting the Stretchsit pillow and come from the mini crunch /towel keep you in traction that is light.
Roll each shoulder back and rest your hands close into your own body.
Angle your chin down slightly, letting the back of your neck be long.
(a) Lean forward from the hips, and tilt your ribcage forward, like you are doing a mini-�crunch. (b) Push downwards on the armrests/side bars/seat pan of your chair to get a gentle stretch in your lower back. (c) Keeping the stretch, lean back from your hips and stick your mid-�back on to the Stretch-sit cushion/towel.
(a) Come out of the mini�crunch and relax completely, letting the Stretchsit cushion/towel keep you in mild traction. (b) Roll each shoulder back and rest your hands close into your body.
Angle your chin down slightly, letting the back of your neck be long.
#2. Vary�Your Baseline Posture
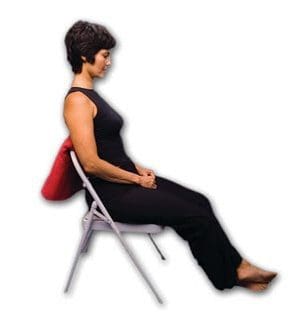
No matter how good your bearing, your body still needs a variety of places. Sitting and standing are the most practical positions for most occupations (example computer occupations)�I recommend switching between them every 20- 30 minutes. If other positions and motions are practical for doing your job (eg, walking when speaking on the phone), that�s an excellent bonus�the more baseline stances and movements, the better. (one sitting against backrest, one stack sitting, standing in a desk, and walking with telephone)
Sitting against the backrest.
Stack sitting
Standing at a desk.
Walking while talking on a cell phone.
#3. Supplement With Rest, Exercise, Movement During & Outside The Workday
Use your breaks in the workday along with your time away from work to supplement your special service line spots. Do you need rest? Exertion? Stretching? Strengthening your abdominal muscles?… There are countless tissues and muscles within your body that have needs just like you are served by a diet that is diverse well, a movement regimen that is varied will also.
#4. Use Well – Designed Tools & Furniture
Experiment and learn with what constitutes furniture that is healthy this is an investment in the way you’ll be spending about half your waking life.
Conventional knowledge wants us to believe that athletes must eat a high carb diet in order to function at optimum levels. While many people believe this, nothing could be further from the truth. Ben Greenfield conducted extensive tests on himself to prove that it is possible to be a fat burning athlete, and that being a high carb athlete should be a thing of the past.
Ben�s analysis was very detailed and impressive: he had blood work, biopsies, urine and stool samples taken before the study began. He then walked on the treadmill for three hours and retook the blood work, biopsies the urine, and the stool samples, then analyzed the data. The study was called The Faster Study, and the data is available via PDF for those interested in looking at his findings and Ben�s write-up on the experience can be found here.
The Faster Study
When I asked Ben why he did the study, he said it was for his own selfish reasons. He said he was training for an Ironman triathlon at the time and wanted to go faster or at least maintain his speed for longer periods without experiencing the deleterious effects that chronically elevated blood sugar�can cause. He also wanted to avoid the potentially unsettling effects that carbohydrates fermenting in your gut can cause.
Ben also had another incentive: he was diagnosed as having a 17% higher than normal risk for Type 2 diabetes. As a result, he needed to figure out a way to complete an Ironman triathlon without going the traditional route of fueling with gels, bars, and energy drinks.
I can attest that his theory works because I tried it myself: while on an 18 hour intermittent fast, I went on a 3 hour bike ride. By the time I got home, it was 22 or 23 hours before I�d eaten one bite of food, and to everyone�s surprise, I didn�t bonk. Everyone on the ride that day was a seasoned athlete and eating constantly. I was the only one not eating, yet had plenty of energy, even after 20 hours without food. Ben proved that in a laboratory and I successfully tested his hypothesis in a real life situation.
The Faster Diet
In preparation for his experiment, Ben followed a diet of 80 to 90% fat and 5 to 10% carbohydrates. His protein intake would vary depending on the day�s activities. For example, protein intake would be approximately 20% on days he�d run or do weight training. On average, the majority of his diet was fat based. He jokingly said he was banned from Italian restaurants during this time.
While on his high fat/low carb diet, Ben did two ironman triathlons that year (Ironman Canada and Ironman Hawaii.) He stresses that that a low carbohydrate diet does not mean a zero carbohydrate diet. Using Ironman triathlon as an example, participants may be out competing for ten or more hours. When passing someone the on the bike, a person may go from their normal race pace of 250 watts up to 400 watts for a few moments. This surge of energy being exerted can cause a pretty significant glycolytic shift, resulting in the body needing to burn through a high amount of carbohydrates.
Ben took in about a quarter of the amount of carbohydrates that he�d normally consume during the actual event, along with ample amounts of easy to digest proteins, amino acids, easy to digest fats, and medium chain triglycerides. After his triathlon season was completed, Ben added exogenous ketones�to his diet in powder form to increase ketone levels. Ben admitted that he finds the ketones extremely beneficial and says he wish he�d known about them while training for previous triathlons. Personally, I have experimented with exogenous ketones in my own fat burning regime, after learning more about how they work during my interview with Dominic D�Agostino (watch the interview here.)
Study Findings
During that triathlon season, Ben conducted quite a few studies, with a few standing out in particular. In this test, a microbiome analysis was conducted to see how the gut differs between someone who follows a high-carbohydrate diet and someone who follows a high-fat diet.
Fat biopsies were taken both before and after exercise to see to see if his actual fat tissue make-up was any different. Tests were also conducted to see if there was any difference in the ability of his muscles to store carbohydrate and how quickly the muscle would burn through carbohydrates. A resting metabolic test was conducted, which is an analysis of how much fat and carbohydrate is burned at rest. And another measurement was taken to determine how many carbohydrates, fats, and calories are burned during exercise.
What makes these tests interesting is even though most physiology textbooks claim that the average person will burn about 1.0 grams of fat per minute during exercise, the athletes who followed a ketogenic or low-carbohydrate diet for close to 12 month were experiencing fat oxidation values of closer to 1.5 to 1.8 grams of fat per minute. This is significantly higher than what experts expected.
Initially, there was some confusion pertaining to this study because it was called � The Faster Study.� Critics would say Ben wasn�t going any faster on the high fat/low carb diet than those on the high carb diet. What they neglected to understand was the purpose of the study wasn�t to go faster than those on high carb diets. Instead, the goal was to maintain similar speeds while limiting (and possibly eliminating) the chronic fluctuations and elevations of blood sugar.
Ben�s thought process behind the study was simple: If he could go just as fast by eliminating sugars, why not do it? If he slowed down or felt his energy levels being depleted, he�d be forced to ask himself the following questions as an endurance athlete:
What kind of balance did he want between health and performance?
How many years of his life was he willing to sacrifice in exchange for going just a little bit faster?
How much pressure was he willing to put on his joints?
As it turns out, Ben could go just as fast on a carbohydrate-limited diet.
Go Just as Fast, Live Longer
While people are focused on getting faster, the ultimate goal should be to go just as fast and live longer doing it. Unfortunately, many high-carb athletes have a wide assortment of health problems, which can range from joint problems to life threatening emergencies such as heart attacks. Many of them are dying prematurely and don�t realize a contributing factor to their ailments is the high carb diet they had been following for years. Ironically, many athletes are thin but show evidence of degenerative disease indicating years of inflammation and oxidative stress�caused by repeated glucose and insulin spikes. We know this damage is oxidative, is harmful to the cells, and causes premature aging.
There are many studies with research illustrating how endurance sports increase oxidation and aging, but I believe as more research is done this belief will change. Studies by Ben and others show that a fat-adapted endurance athlete does not have the same levels of oxidative stress as high carb endurance athletes. At age 50, I have 8% body fat and can exercise for hours without ingesting carbohydrates because, like Ben, I�m very efficient at fat burning.
I firmly believe Ben�s study proves that people who are efficient at fat burning can burn well over one gram of fat per minute of exercise, whereas before it was believed one gram (or less) was a more realistic number. It should be noted that in order to burn that much fat, a person has to be fat adapted. It�s impossible to accomplish this level of fat burning on a high-carbohydrate diet (read more on how to get fat-adapted here: Part 1 and Part 2.)
Fat Adaption: A trick to Accelerate the Process
Becoming an efficient fat burner takes time. Many of the athletes that Ben coaches have been on a high fat diet for twelve months or more. While the greatest benefits aren�t felt for several months, a person can experience lower blood sugar levels and less oxidation within a few short weeks of starting a high fat diet. However, in order to achieve the mitochondrial density necessary for producing a lot of ATP on a high-fat diet while exercising, a person will need to follow a high-fat diet for at least a year.
It can take anywhere from 6 months to 2 years for a person to become fully efficient at burning fat. While some may balk at how long it can take, it�s not long when compared to the time it may take to become proficient in a sport, learning to play a musical instrument, or getting a college degree.
Adjusting to a high fat diet takes time and patience. To accelerate the process, one can choose to eat within a compressed time window, a strategy known as intermittent fasting. Intermittent fasts can range from 14-24 hours with just liquids being consumed. Intermittent fasting can be a challenge for beginners as the body begins to adapt, but becomes easier with each subsequent fast. I intermittent fast daily and must say it�s been the great contributor to my overall cellular health.
Some side effects beginners may experience while intermittent fasting the first few times may include the following
Fatigue
Nausea
Vomiting
Diarrhea
Headaches
Lack of focus
Bad breath
Lethargy
Joint pain
Minor depression
These side effects are normal as the body eliminates various toxins. Drinking pure water�helps to alleviate some side effects and quickly remove them from the body via urination. Staying focused on the long term is key when embarking on these changes.
Occasionally, I will receive emails from my clients or the doctors of my clients, telling me they are keto-adapted, but they�re not burning fat, they don�t notice any significant changes in their bodies, and they haven�t lost any weight. I explain how this is normal, and the body has to adjust. It takes time for the body to realize it is not starving and that it can begin to burn its own fat for energy. Using my wife as an example, it was almost a year before she was able to use her fat storage for energy. Now, she�s an efficient fat burner and finds it much easier to stay lean.
Not All Fat is the Same
An important aspect of being efficient at fat burning is the type of high fat diet you follow. A plant-rich, ketogenic diet not only limits oxidation and free radical production, but it also causes an increase in stable energy sources due to high fiber content. Having high levels of plant-based chlorophylls in the bloodstream also has the potential to increase ATP production beyond what we fully understand in nutrition science.
Ben encounters many people who follow the Bulletproof Coffee type of approach:
Three cups of coffee with grass-fed butter and MCT oil during the day
Coconut milk with some coconut flakes and some chocolate stevia
Fatty grass-fed steak for dinner
Macadamia nuts for a snack
The problem with this type of diet is there�s very little plant matter eaten, and plants are an integral part of a healthy high fat diet.
Ben Greenfield�s Diet
Ben eats an astonishing 20 to 25 servings of plants per day. He has an enormous backyard garden and eats kale, butter lettuce, bok choy, mustard greens, cilantro, parsley, and tomatoes daily. He says these foods do not count towards his total daily carbohydrate intake, and that eating a high-fat diet does not mean that you�re not eating plants. It�s the opposite. �I eat a lot of plants, a lot of fiber, and it makes a night-and-day difference.�
In order to get 20-25 servings Ben eats huge salads and drinks nutrient dense smoothies. He�ll drink one or two large smoothies a day, using a powerful blender that blends everything from the pit of an avocado to an entire bunch of kale. A sample smoothie includes the following ingredients:
Six to eight different plants (both wild plants and herbs)
Lunch. Lunch is a salad in an enormous bowl filled exclusively with vegetables. Ben will spend 30 to 60 minutes chewing each bite 20 to 25 times and �eating lunch like a cow while I go through emails and things like that during lunch.�
Dinner. Another big salad.
Snack. Snacks are normally smaller versions of the smoothie�he had for breakfast.
He stresses that his salads are extremely large and he prefers thicker smoothies: �If you were to see the size of my salads and the size of my smoothies, you would be shocked. You�d think I would be morbidly obese, but if you dig in and you look at it, it�s really just mostly plant volume. That�s generally what I do, salads and smoothies. I make them so thick I need to eat them with a spoon because I really like to chew my food. Yeah, I�m a smoothie and a salad guy.�
He goes on to say �When I look over the blood and bile markers of people following a high-fat diet, a lot of times I see really high triglycerides and really low HDL, which is often what you�ll see in someone who is eating a ton of animal fats without many plants or without much fiber. I�ll see a lot of CO2 and really low chloride levels, an indicator of a net acidic state, and a lot of biomarkers that aren�t necessarily favorable and that can be a result of a high-fat diet done improperly. I think that�s one important thing to bear in mind, too, is that you don�t want to necessarily eschew plant intake and vegetable intake; you just want to ensure that those are accompanied primarily by healthy fats and oils rather than accompanied by high amounts of protein and starches.�
When it comes to good fats, Ben prefers the following:
Animal fats are eaten sparingly. He�ll eat a grass-fed steak and wild fish a couple of times a week. He also likes pemmican, which comes in a tube that he can snack on while flying or if he needs a quick snack on the go.
When Ben was a bodybuilder, he would aim for 200 grams of protein per day but now only consumes between 100 to 120 grams. Currently, he weighs about 180 pounds and consumes between 0.5 and .8 grams of protein per pound of body weight. He feels this is the amount is sufficient to avoid any loss of muscle.
Ben says he has excellent colonic health. Since he started the high fat diet four years ago, he doesn�t have the fermentation, gas, bloating, or constant gas that many endurance athletes have. He also believes the high fat diet offers a lower risk for things like small intestine bacterial overgrowth (SIBO) and fermentation in the gut.
Diet Variation
In addition to eating a variety of plant based foods, an important eating concept that I have written about is something I like to call �diet variation,� which is basically emulating what our ancestors have done: They were forced into different diet variations seasonally, and in some instances, weekly.
When we look at the Hunza people as an example, they were relying mostly on plant food in the summers to survive. During the cold winter months, vegetables and fruits were scarce or nonexistent, and as a result, they were forced to eat higher-fat foods (meats and animal fats). Over time we can see a pattern: there would be long stretches where their diet consisted mostly of vegetables (summer,) then extended periods of time where their diet was mainly meat products (winter.) This type of seasonal eating created a variation in their diet they had little control over. Today, we have the ability to vary our diet at all times, which can work for us and against us.
I go into ketosis every summer and eat more good fats and protein than I do in the winter, when I eat more healthy carbs. Like Ben, I�m very fat adapted, yet still able to stay in ketosis while eating a lot of plants in my diet. I intermittent fast in the morning and by the afternoon I�m burning high ketones.
One of the popular diet trends these days is the Paleo Diet, where a person is instructed to eat large amounts of protein. Quite frankly, I am not a fan of this diet. I have read many studies on high-protein diets and feel they are not healthy. Eating too much protein can cause weight gain, extra body fat, increased stress on the kidneys, dehydration and other health issues.
If you include the dangers of eating grain fed beef instead of the healthier grass fed beef, we can clearly see how the Paleo Diet could be a recipe for disaster. I tell people as a general rule, eating protein that is equivalent to half your body weight (considering that you�re not morbidly obese) is usually safe and practical. Athletes like Ben (and those who do a lot of strenuous physical exercise) can consume more protein than the average person and utilize it safely. These individuals may require 0.7 to 0.8 grams of protein per day, while the average person only needs .55 grams per day.
Fasting
Ben goes on a 24 hour fast once a month, just to �clean things out a little bit.� He will start the fast Saturday at lunchtime end it at lunchtime on Sunday. Or, he�ll skip dinner on Saturday night and won�t eat again until dinner on Sunday. He�ll drink water, coffee�and tea primarily during the fast, and kombucha on occasion. He also goes on a 12-16-hour intermittent fast daily. The majority of the fast is overnight where he�ll finish dinner around 7:00 or 8:00 p.m. and eat breakfast sometime 9 and 10:30 a.m. During the daily fast, Ben will perform a few low-level exercises in the morning: yoga, foam rolling, or mobility work are exercises of choice.
In addition to daily intermittent fasting, Ben believes a likely factor that helps him to stay lean and maintain a low body fat percentage is taking cold showers. He likes to do one of the following daily:
Fast, perform a low intensity exercises then take cold shower or�
Fast, sit in a sauna for a few minutes, followed immediately with a cold shower.
Ben�s Exercise Regimen
Ben is active all day, but in an unconventional way:
�I generally am active all day long. Today, while I�m writing, doing consults, and reading emails, I�ll walk somewhere in the range of three to five miles at a low intensity like I am right now. When I get up in the morning, I�ll generally spend 20 to 30 minutes doing some deep-tissue work and some mobility work, some foam roller, and some band work for traction on my joints. By the time I get to the end of the day, I�ve been mildly physically active for six to eight hours at just very low-level intensity.
�At the end of the day, I�ll throw in 30 to 60 minutes of a hard workout. That might be a tennis match. It might be kickboxing or jujitsu. It might be some kind of an obstacle course workout with sandbags, and kettlebells, and things like that. It might be a swim. It varies quite a bit, but generally it�s 30 to 60 minutes of something hard in the afternoon to the early evening, then up until that point, low-level physical activity all day long. It�s just tough to quantify because I�m always moving. As far as a formal workout, it comes out to about 30 to 60 minutes a day. We�re talking about a workout where the average heart rate is very close to maximum heart rate, so like a puke-fest style workout. That�s pretty draining from an energy standpoint. Generally, for me to do daily�exceeding 16-hour fasts daily�that gets tough.�
What�s Next For Ben?
Ben is an outdoorsman and wants to experiment with living on the land:
�I�d like to look into more of an ancestral application, a more practical application. I would like to look a little bit more into persistence hunting, something closer to where I live where I�d be going after elk or moose or something like that, preferably in the snow where tracking is a little bit easier, but seeing if it�s doable.
�A five to eight day hunt is realistically what you�re looking at with a bow, or with a spear, or with a close-range weapon, and seeing if it�s possible to actually go and get your own food in the absence of food, just to begin to get people thinking about the state that we live in, the culture that we live in where food is just constantly readily available. What would happen if we didn�t have food but we had to figure out a way to feed ourselves?�
Ben also shares the outdoor life with his children: One day week in the summers, they can only eat the plants they find outside in the garden until dinner. As part of their childhood, he wants them to learn how to take care of themselves. They can use the stove and the blender, stuff like that, but they can�t use ingredients from the pantry, or from the refrigerator. It�s all based on plants.
While many people may think this way of thinking and living is extreme, Ben believes more people can benefit from it if they stay open minded and give it a try:
�I would like to get people more aware of that type of practice because it really goes quite handily with the things that we�ve talked about�fasting and ketosis, and denial of modern food sources and starches and instead just learning how to take care of yourself. I think that there�s a lot of lessons to be had from a health and survival standpoint, and so plant foraging, spreading our message, as well as the potential of seeing the persistence hunting in the absence of any significant sources of calories, to be able to take what allows one to, say, do an Ironman Triathlon with very little calorie intake and then turn that into a more practical level like going out and getting your own meat and stuff. Again, without carrying a bunch of power-bars out with you, I think that�d be a cool little adventure to embark upon.�
A Life of Fitness
Ben believes fitness is a lifestyle, and everyone can incorporate fitness into their daily activities:
If you work in a traditional office setting, put a kettlebell underneath your desk.
Get one of these stools that you lean back on rather than sitting down.
Every time that you go to the bathroom have a rule that you�ve got to do 50 air squats.
�Start to work in those little things throughout the day. You�d be surprise at how fit you can stay and how prepared you can be for a big event without necessarily neglecting your family, your friends, hobbies, or work.�
Ben Greenfield is an inspiration. His research on high fat diets is sure to revolutionize the way athletes view diet and endurance exercise as a whole.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine