Even if you have never stepped foot onto a court before, you may end up with tennis elbow. Occurring along the muscle that allows extension of the wrist, it is a painful condition that can linger for weeks or months.
Previously, tennis elbow primarily showed up in athletes. Due to the increased interest in physical fitness, tennis elbow is being found in everyday exercisers, as well as people who perform work-related repetitive motion.
Tennis elbow presents several symptoms. Pain will occur on the outside of the elbow an inch or so down from the bony part.
There may also be pain when the individual tries to extend the hand and fingers against resistance. Extreme weakness in the wrist is another symptom.
I Have Been Diagnosed With Tennis Elbow. Now What?
Tennis elbow is often difficult to diagnose, which can delay treatment. A correct diagnosis of tennis elbow is the first step towards being able to treat the condition and rehab the afflicted area. From there, a variety of treatments for tennis elbow are available.
Passive remedies like rest, ice, and arm braces are critical components to healing tennis elbow. Take measures to reduce the movements that aggravate the pain, and use ice at regular intervals to help minimize pain and inflammation.
An arm brace supports and stabilizes the area to promote healing. These remedies assist greatly in treating the condition, especially in the beginning.
Active remedies consist of stretching and strengthening exercises, and are vital aspects of improving the condition. Individuals suffering from tennis elbow should begin an exercise regimen as soon as the pain allows.
An individual dealing with tennis elbow may utilize a variety of medicinal remedies to manage pain and inflammation. Over-the-counter pain relievers and steroid injections are commonly used to treat the condition. Following doctor’s orders when taking medications is strongly recommended.
Untraditional remedies also provide vast improvements in tennis elbow, and these treatments have gained favor in the last few years due to their effectiveness. Regimens of massage therapy and acupuncture work on small areas contributing to the condition, and make significant strides in pain reduction and promote the body’s restorative healing process.
Another remedy that offers strong benefits to treating tennis elbow is chiropractic care. A chiropractor assesses the condition, then lays out a plan to promote healing.
Treatment often includes working to align the bones and treating the surrounding joints so they function at maximum capacity, and can “take up the slack” of the injured area while it heals. Chiropractic care serves the dual purpose of treating the condition directly, and healing the areas around the injury so that the body continues to strengthen and renew.
In a very small number of cases, the only remedy for tennis elbow is surgery. This is considered as the last straw, once all other forms of treatment have been exhausted.
The best way to treat tennis elbow is to avoid it in the first place. Be sure to stretch before exercising, consistently perform strengthening exercises, employ correct techniques and proper equipment during physical activity, and don’t overexert your arms (this goes for your entire body, by the way) during physical activity.
If you are diagnosed with tennis elbow, it’s essential to understand the variety of treatment options available. The best course is often a blend of more than one remedy. Chiropractic care should be part of your healing process, as it helps decrease pain, reduce healing time, and offers a non-medicinal approach to treating the body as a whole.
The Risks Of College Sports
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Running is one of the most popular forms of exercise, and offers many benefits. It can be done anywhere, it tones the lower body, and it burns a ton of calories. Pounding the pavement over time, however, can result in injuries to the knees, ankles, and hips.
Whether you run a few miles a week to keep the extra pounds off, or hoof it in several marathons a year, there is unfortunately a good chance you will get hurt at some point.
The first step to recovery if you injure yourself running is to give your body time to heal. A visit to the doctor, ice packs, and over the counter pain medication are all ways to treat an injury. However, one of the best ways runners can treat their injuries is by visiting a chiropractor.
If you are dealing with a running injury and think a chiropractor may be able to help you get back on your feet with less pain, you are most likely correct. Here are four important things to know about chiropractors and how runners can benefit from chiropractic care:
Runners: Chiropractors Work On More Than Necks And Backs
It’s a common misconception that a chiropractor’s sole purpose is to adjust their patients’ necks and backs. The entire body can benefit from a chiropractic manipulation. For example, the American Chiropractic Association (ACA) states that knee pain is the most common running injury.
Chiropractors are often able to work with an injured knee and bring about a positive outcome. Strains, sprains, and other trauma to your body’s joints can be treated by a chiropractor. Soft tissue around the joints benefit from chiropractic treatment, which can greatly ease an injury to the ankle, knee, or hip.
Chiropractic Promotes Quicker Healing Of The Injured Area
From increasing blood flow to the hurt area to breaking up restrictions with manual manipulation, chiropractic treatment helps the body heal itself. Chiropractors view the body in its entirety, and may use manipulations and adjustments on other parts of the body to stimulate healing of the afflicted area.
Chiropractors Assist In Pain Management
Running injuries can often cause great pain that lasts for weeks. Visiting a chiropractor can help reduce the severity of the pain and shorten the amount of time you experience pain. This is an especially attractive benefit for those who avoid taking medicine. Chiropractic care helps manage the discomfort and soreness associated with the injury, allowing the patient to rely less on drugs.
Chiropractic Reduces The Risk Of Getting Re-Injured
A common reason runners end up hurt is their bodies had something “out of whack” in the first place. Since chiropractors take the wellness of the body as a whole into consideration, they often work with runners to minimize the chance of re-injuring themselves or suffering a different injury. By making certain an individual’s body is in alignment and functioning properly, a chiropractor can help the runner feel comfortable moving back into the routine of running.
Running is a great form of exercise and stress relief, and many people run for years without incident. However, it�s vital to take steps up front to minimize the chances of getting hurt, including choosing proper shoes, stretching beforehand, and avoiding overexertion.
Stephanie Rothstein-Bruce: Professional Marathoner
If, however, you feel a twist, pop, or crack as you are out for your morning run or finishing your half marathon, know there are chiropractic treatment options available to you that will decrease pain, healing time, and the risk of re-injury. Just pick up the phone and give us a call. We�re here to help!
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Asthma is a chronic lung disease that has afflicted more people in the last 20 years than ever. Some doctors attribute the increase to the pollutants in the air, the changes in the modern diet, and lack of adequate ventilation in homes.
According to the Mayo Clinic, asthma symptoms vary by individuals and may be mild, severe, or somewhere in between. Shortness of breath and tightness in the chest, along with a wheezing sound when exhaling are common asthma symptoms. Common treatments include inhalers and other medications.
With the millions of asthma sufferers seeking relief, non-traditional treatments have emerged in addition to the everyday remedies. One of the alternatives that has shown positive results is chiropractic care.
A person who suffers from asthma can enjoy multiple benefits from chiropractic. Four of the top benefits chiropractic care can bring to asthma patients are the following:
Reducing The Frequency Of Attacks
Over time, spinal adjustments can help some asthma sufferers decrease the number of attacks. When a spine is in alignment, energy flows through the nerves to the person’s organs. A nonaligned spine can cause the energy to fail to flow through the nerve endings as effectively, and a host of issues can arise.
The lungs can suffer when the spine is not aligned. Chiropractors are able to treat the spine so that, over time, it aligns. In some cases, this helps lung function and decreases the number of asthma attacks.
Stimulating Air Flow
The lungs are obviously vital for breathing, but the airway and diaphragm also play a part. Both of these can be hindered by a spine that is not aligned.
When a chiropractor works with a patient to align the spine, the airways and diaphragm can move more freely, allowing better airflow. While this is not a cure for asthma, in many cases stimulating a body’s airflow can help decrease the suffering the chronic condition causes.
Boosting The Immune System
A significant number of asthma attacks are brought on and exacerbated by an individual’s low immune system. Chiropractic care helps increase the effectiveness of the immune system.
Think of it this way: The autonomic nervous system is connected to the body’s immune system by way of the endocrine system. When the spine is out of line, it can affect the immune system.
If a person suffers from chronic asthma attacks, this could be the time when he or she has an episode. A chiropractor who can align the spine can create a positive domino effect. The nervous system improves, the immune system improves, and the asthma attacks decrease.
Working In Conjunction With Traditional Asthma Medication
People with asthma commonly use inhalers and steroids to manage their symptoms. Chiropractic care is non-invasive and works with these treatments to lessen the instances and severity of attacks.
A study by Michigan Chiropractic Council showed that asthma sufferers who went through 30 days of chiropractic treatments reported a 70% reduction in medication.
Patients who commit to chiropractic can sometimes manage the symptoms more naturally, and lessen their dependence on medications. (It’s important to note that patients should never go off medications on their own. Always speak to a doctor before changing medications).
Patients fortunately have a variety of treatment options. For those who don’t respond to traditional medication, or who wish to decrease their dosage, non-traditional choices like chiropractic may be the answer.
Tips For Preventing Dehydration
It’s advisable to speak to both your medical doctor and Doctor of Chiropractic about your asthma symptoms. By having both disciplines co-manage your case, you�ll work toward a healthier outcome, possibly even without the use of drugs. Give us a call to learn more.
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
While back pain is a known and widely-studied issue in adults, its prevalence in school-aged children has received comparatively little scientific attention. Elementary, middle, and high school students must often carry backpacks that weigh enough to cause chronic back pain, poor posture, and even decreased lung volume. Recently, several studies reveal the truths behind childhood back pain and ways to mitigate it.
Are Backpacks Too Heavy for Kids?
Recent research supports that children carrying backpack loads of more than ten percent of their bodyweight have a greater risk of developing back pain and related issues. An international study found that an alarmingly large proportion of school-aged children in Australia, France, Italy, and the United States regularly carried backpacks weighing more than the ten percent threshold.
In another study involving a sample of 1540 metropolitan school-aged children, over a third of the children surveyed reported back pain. In addition to carrying heavy backpacks, female students and those diagnosed with scoliosis had a greater association with back pain. Children with access to lockers reported less pain.
The number of straps on the backpack had little impact on the respondents’ answers. Children also reported limited physical activity due to back pain, and some took medication to relieve the pain.
Girls who carried purses in addition to wearing a backpack reported significantly greater back pain. Adolescents with back pain spent more time watching television than their peers. Over 80 percent of those surveyed believed that carrying a heavy backpack caused their back pain.
Proper Backpack Carrying Techniques
The studies revealed several factors that may help reduce back pain in school-aged children. The best way to prevent back pain is to avoid carrying heavy loads.
Children should take advantage of locker breaks and only carry items necessary for a couple of classes at a time. When lifting a backpack, children should crouch down and bend their knees rather than curve the spine.
Children should avoid carrying over 10 percent of their bodyweight in their backpack. For example, an 8th-grader weighing 120 pounds should carry no more than 12 pounds.
Place the heaviest objects at the back of the pack.
Make sure the items fit as snugly as possible to minimize back pain due to shifting weight.
Adjust the shoulder straps so they fit snugly over your child’s shoulders and the backpack doesn’t drag your child backward. The bottom of the pack should be less than four inches below your child’s waist.
Children should avoid carrying backpacks slung over one shoulder, as it can cause spinal pain and general discomfort.
Encourage your child to carry only necessary items in their backpack. Additional items can be carried in hand.
Look for backpacks with helpful features such as multiple compartments for even weight distribution, padded straps to protect the shoulders and neck, and waist belt.
If your child’s school allows, consider a rollerpack, which rolls across the floor like a suitcase.
If problems continue, talk to your child’s teacher or principal about implementing paperback textbooks, lighter materials, or digital versions.
Chiropractic Care Can Help
If your child continues to experience back pain, contact your local chiropractor. Chiropractic care benefits many adults with spinal discomfort, and licensed practitioners can provide tailored treatments for children.
Chiropractors can also recommend safe exercises to improve back strength, and additional advice on proper nutrition to build strong bones and joints, healthy posture, and more. If your child is experiencing back pain from carrying a backpack, gives us a call. We�re here to help!
Backpack Safety
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
When you suffer from joint or muscle pain, it is important to work on maintaining as much flexibility as possible. The more flexible you are, the less likely you will be to further injure yourself. One of the best ways to improve your flexibility is by stretching before you are active.
However, you need to warm up your muscles before you stretch. If you stretch first, you can actually injure yourself by pushing your joints too far. Spend a few minutes doing some light activity before you stretch. This can be as simple as a brisk walk or some basic calisthenics.
If you have been seeing a chiropractor, he or she may be able to recommend some stretches for you. Otherwise, you can use some of these basic techniques. There are two basic forms of stretching, static and dynamic.
Static Stretching vs. Dynamic Stretching
Static stretches involve holding a position for a certain period of time to loosen up your muscles. These tend to be what most people think of when they think about stretching. However, dynamic stretches are also important. With these, you move parts of your body to work on your flexibility.
Many of the most effective stretches for back pain can be done right at home. For example, lie on your back with your knees bent. Grasp one knee in both hands and pull it up towards your chest. Hold this position for 30 seconds and then lower the knee to the starting pose. Repeat with the other knee. You can also do both knees at the same time.
A similar stretch begins in the same position as the previous one. However, instead of lifting your knee to your chest, roll both legs to one side so that your knees are as close to the floor as possible. Hold this position for 10 seconds, and then roll to the other side.
Another common stretch recommended by many chiropractors comes from yoga, where it is known as the “cat pose.” Get down on the floor on your hands and knees, with your hands underneath your shoulders. First, let your abdomen drop down towards the floor. Then, reverse this movement by arching your back. Repeat this cycle three to five times.
More dynamic stretches can also be good for your muscle pain. Try doing handwalks to stretch your shoulders and abdominal muscles. Stand up straight and slowly lower your hands towards the floor. Walk your hands out in front of you until you are as far down as you can go. Then walk your hands back to the starting position.
A final stretch that can help your back muscles is known as the “scorpion.” Lie face-down and stretch your arms out to the sides. First, slowly move your right foot towards your left arm. Then, move your left foot towards your right arm. Make sure to move in a slow and controlled fashion.
When you are suffering from muscle or joint pain, it is a good idea to stretch both in the morning and the evening. By incorporating these exercises into your daily routine, you can avoid many common injuries.
If you need further instruction regarding stretches, please give us a call so that you can schedule an appointment with our Doctor of Chiropractic.
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Chiropractic care is designed to alleviate pain and restore the body to its natural balance. For chiropractors, injury prevention is key for a healthy body. Good practices combined with solid exercises creates toned muscles that protect the body and spine from harm. While each patient receives exercise instructions for their specific condition, the following exercise tips for chiropractic patients apply to everyone.
Take Time To Warm Up Before You Exercise
Before starting any exercises, it’s important to warm up. A series of dynamic moves will boost your heart rate and heat up the muscles that you will be using during your work out.
Select whole body movements such as leg lunges paired with arm motion or walk in place while raising and lowering your arms. Once you’ve warmed up, you can safely stretch without risk of injury.
Introduce Ergonomics Into Your Home And Work Space
One of the most important exercise tips for chiropractic patients is to take steps to keep your body in alignment as you move through your day. In the workplace, check with an ergonomics consultant to ensure proper positioning, especially if you spend most of the day seated or doing repetitive tasks.
A comfortable chair reduces muscle strain and prevents injury. Make sure that your feet sit firmly on the floor and that lumbar support is in place. At home, you should have a good mattress and supportive furniture.
Choose The Right Shoes
Before you buy your next pair of shoes, check for stability, flexibility, and comfort. During your test drive, make sure that the shoes feel firmly in place as you move through your entire range of motion for a stable gait during wear.
Footwear should be flexible enough to give easily at the base of the toe for a smooth gait, and there should be cushioning at all the right places with plenty of room for the toes to move. Shoes that properly fit your feet means that your walk will be more natural and healthy during exercise and in daily motion.
Sit And Stand With Posture In Mind
Perhaps the biggest reason that these exercise tips for chiropractic patients are so important is that strong and flexible muscles will help you have good posture. Be mindful of the following as you move through your day:
When sitting, your feet should be on the floor, your shoulders should be relaxed, and your forearms should remain parallel with the ground.
If you will be standing for a time, make sure that you maintain posture by tucking your stomach muscles in.
When standing for an especially long period of time, be sure to shift your weight from one foot to the other and from the heels to the toes and back again.
These simple tips for maintaining good posture will passively work your muscles and result in a healthier spine.
Passive Stretches For Large Muscles
Finally, it is important to target large muscle groups with passive exercises. Use your weight to slowly stretch your hamstrings, your piriformis, and your entire back. Passive stretching is gentle and relieves stress points that cause back pain. These gentle exercises provide a great deal of relief and are easily adjusted to suit your current ability.
Your chiropractor will work with you to design an exercise program that is optimal for you. Be sure to follow through with the plan and include these tips in your regular work out to experience the joy of healing from chiropractic care.
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?
Albert Einstein, in his infinite wisdom, discovered that the total energy of an object is equal to the mass of the object multiplied by the square of the speed of light. His formula for atomic energy, E = mc2, has become the most recognized mathematical formula in the world. According to his equation, any change in the energy of an object causes a change in the mass of that object. The change in energy can come in many forms, including mechanical, thermal, electromagnetic, chemical, electrical or nuclear. Energy is all around us. The lights in your home, a microwave, a telephone, the sun; all transmit energy. Even though the solar energy that heats the earth is quite different from the energy used to run up a hill, energy, as the first law of thermodynamics tells us, can be neither created nor destroyed. It is simply changed from one form to another.
ATP Re-Synthesis
The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP.
Like many other animals, humans produce ATP through three metabolic pathways that consist of many enzyme-catalyzed chemical reactions: the phosphagen system, glycolysis and the aerobic system. Which pathway your clients use for the primary production of ATP depends on how quickly they need it and how much of it they need. Lifting heavy weights, for instance, requires energy much more quickly than jogging on the treadmill, necessitating the reliance on different energy systems. However, the production of ATP is never achieved by the exclusive use of one energy system, but rather by the coordinated response of all energy systems contributing to different degrees.
1. Phosphagen System
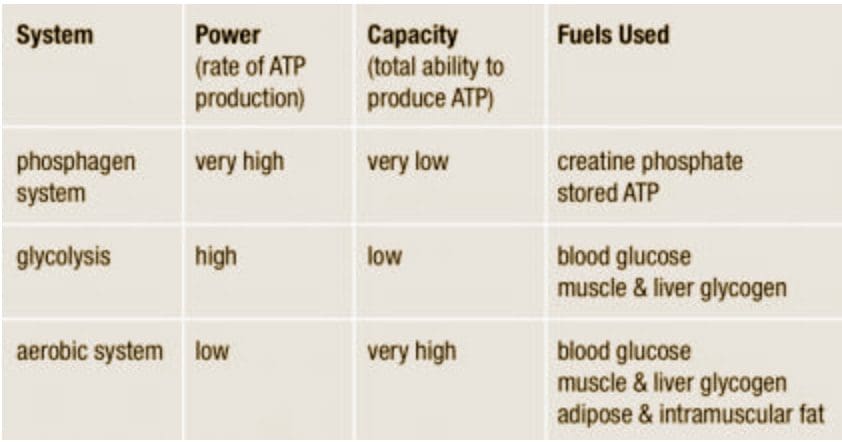
During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.
2. Glycolysis
Glycolysis is the predominant energy system used for all-out exercise lasting from 30 seconds to about 2 minutes and is the second-fastest way to resynthesize ATP. During glycolysis, carbohydrate�in the form of either blood glucose (sugar) or muscle glycogen (the stored form of glucose)�is broken down through a series of chemical reactions to form pyruvate (glycogen is first broken down into glucose through a process called�glycogenolysis). For every molecule of glucose broken down to pyruvate through glycolysis, two molecules of usable ATP are produced (Brooks et al. 2000). Thus, very little energy is produced through this pathway, but the trade-off is that you get the energy quickly. Once pyruvate is formed, it has two fates: conversion to lactate or conversion to a metabolic intermediary molecule called acetyl coenzyme A (acetyl-CoA), which enters the mitochondria for oxidation and the production of more ATP (Robergs & Roberts 1997). Conversion to lactate occurs when the demand for oxygen is greater than the supply (i.e., during anaerobic exercise). Conversely, when there is enough oxygen available to meet the muscles� needs (i.e., during aerobic exercise), pyruvate (via acetyl-CoA) enters the mitochondria and goes through aerobic metabolism.
When oxygen is not supplied fast enough to meet the muscles� needs (anaerobic glycolysis), there is an increase in hydrogen ions (which causes the muscle pH to decrease; a condition called acidosis) and other metabolites (ADP, Pi�and potassium ions). Acidosis and the accumulation of these other metabolites cause a number of problems inside the muscles, including inhibition of specific enzymes involved in metabolism and muscle contraction, inhibition of the release of calcium (the trigger for muscle contraction) from its storage site in muscles, and interference with the muscles� electrical charges (Enoka & Stuart 1992; Glaister 2005; McLester 1997). As a result of these changes, muscles lose their ability to contract effectively, and muscle force production and exercise intensity ultimately decrease.
3. Aerobic System
Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�
The aerobic system�which includes the�Krebs cycle�(also called the�citric acid cycle or TCA cycle) and the�electron transport chain�uses blood glucose, glycogen and fat as fuels to resynthesize ATP in the mitochondria of muscle cells (see the sidebar �Energy System Characteristics�). Given its location, the aerobic system is also called�mitochondrial respiration.�When using carbohydrate, glucose and glycogen are first metabolized through glycolysis, with the resulting pyruvate used to form acetyl-CoA, which enters the Krebs cycle. The electrons produced in the Krebs cycle are then transported through the electron transport chain, where ATP and water are produced (a process called�oxidative phosphorylation) (Robergs & Roberts 1997). Complete oxidation of glucose via glycolysis, the Krebs cycle and the electron transport chain produces 36 molecules of ATP for every molecule of glucose broken down (Robergs & Roberts 1997). Thus, the aerobic system produces 18 times more ATP than does anaerobic glycolysis from each glucose molecule.
Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).
Following acetyl-CoA formation, fat metabolism is identical to carbohydrate metabolism, with acetyl-CoA entering the Krebs cycle and the electrons being transported to the electron transport chain to form ATP and water. The oxidation of free fatty acids yields many more ATP molecules than the oxidation of glucose or glycogen. For example, the oxidation of the fatty acid palmitate produces 129 molecules of ATP (Brooks et al. 2000). No wonder clients can sustain an aerobic activity longer than an anaerobic one!
Understanding how energy is produced for physical activity is important when it comes to programming exercise at the proper intensity and duration for your clients. So the next time your clients get done with a workout and think, �I have a lot of energy,� you�ll know exactly where they got it.
Energy System Characteristics
Energy System Workouts
Have clients warm up and cool down before and after each workout.
Phosphagen System
An effective workout for this system is short, very fast sprints on the treadmill or bike lasting 5�15 seconds with 3�5 minutes of rest between each. The long rest periods allow for complete replenishment of creatine phosphate in the muscles so it can be reused for the next interval.
2 sets of 8 x 5 seconds at close to top speed with 3:00 passive rest and 5:00 rest between sets
5 x 10 seconds at close to top speed with 3:00�4:00 passive rest
Glycolysis
This system can be trained using fast intervals lasting 30 seconds to 2 minutes with an active-recovery period twice as long as the work period (1:2 work-to-rest ratio).
8�10 x 30 seconds fast with 1:00 active recovery
4 x 1:30 fast with 3:00 active recovery
Aerobic System
While the phosphagen system and glycolysis are best trained with intervals, because those metabolic systems are emphasized only during high-intensity activities, the aerobic system can be trained with both continuous exercise and intervals.
60 minutes at 70%�75% maximum heart rate
15- to 20-minute tempo workout at lactate threshold intensity (about 80%�85% maximum heart rate)
5 x 3:00 at 95%�100% maximum heart rate with 3:00 active recovery
Brooks, G.A., et al. 2000.�Exercise Physiology: Human Bioenergetics and Its Applications.Mountain View, CA: Mayfield.
Enoka, R.M., & Stuart, D.G. 1992. Neurobiology of muscle fatigue.�Journal of Applied Physiology, 72�(5), 1631�48.
Glaister, M. 2005. Multiple sprint work: Physiological responses, mechanisms of fatigue and the influence of aerobic fitness.�Sports Medicine, 35�(9), 757�77.
Hochachka, P.W., Gunga, H.C., & Kirsch, K. 1998. Our ancestral physiological phenotype: An adaptation for hypoxia tolerance and for endurance performance?�Proceedings of the National Academy of Sciences, 95,�1915�20.
Hochachka, P.W., & Monge, C. 2000. Evolution of human hypoxia tolerance physiology.�Advances in Experimental and Medical Biology, 475,�25�43.
McLester, J.R. 1997. Muscle contraction and fatigue: The role of adenosine 5′-diphosphate and inorganic phosphate.�Sports Medicine, 23�(5), 287�305.
Robergs, R.A. & Roberts, S.O. 1997.�Exercise Physiology: Exercise, Performance, and Clinical Applications.�Boston: William C. Brown.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Boosting The Immune System
Boosting The Immune System





 We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?
We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?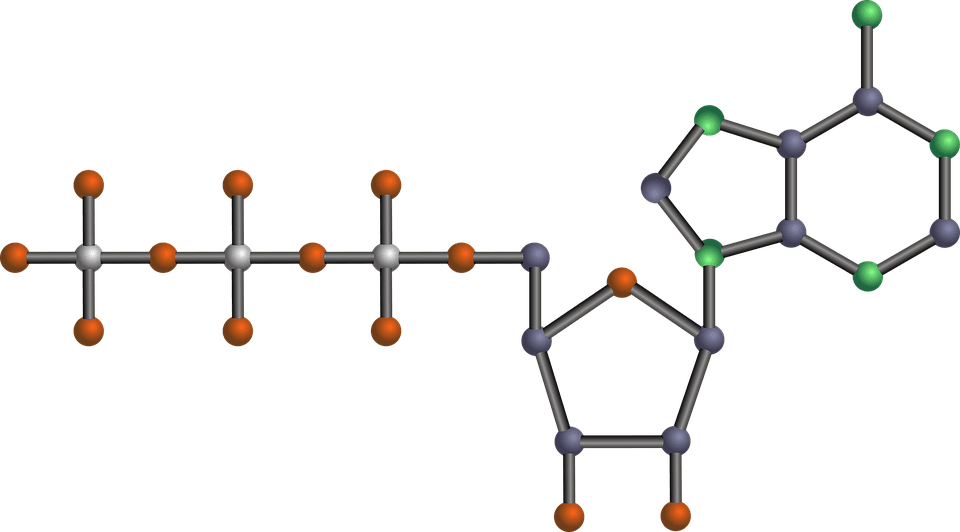 The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP.
The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP. During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.
During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.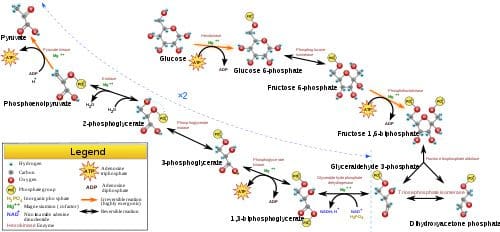 Glycolysis is the predominant energy system used for all-out
Glycolysis is the predominant energy system used for all-out  Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�
Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�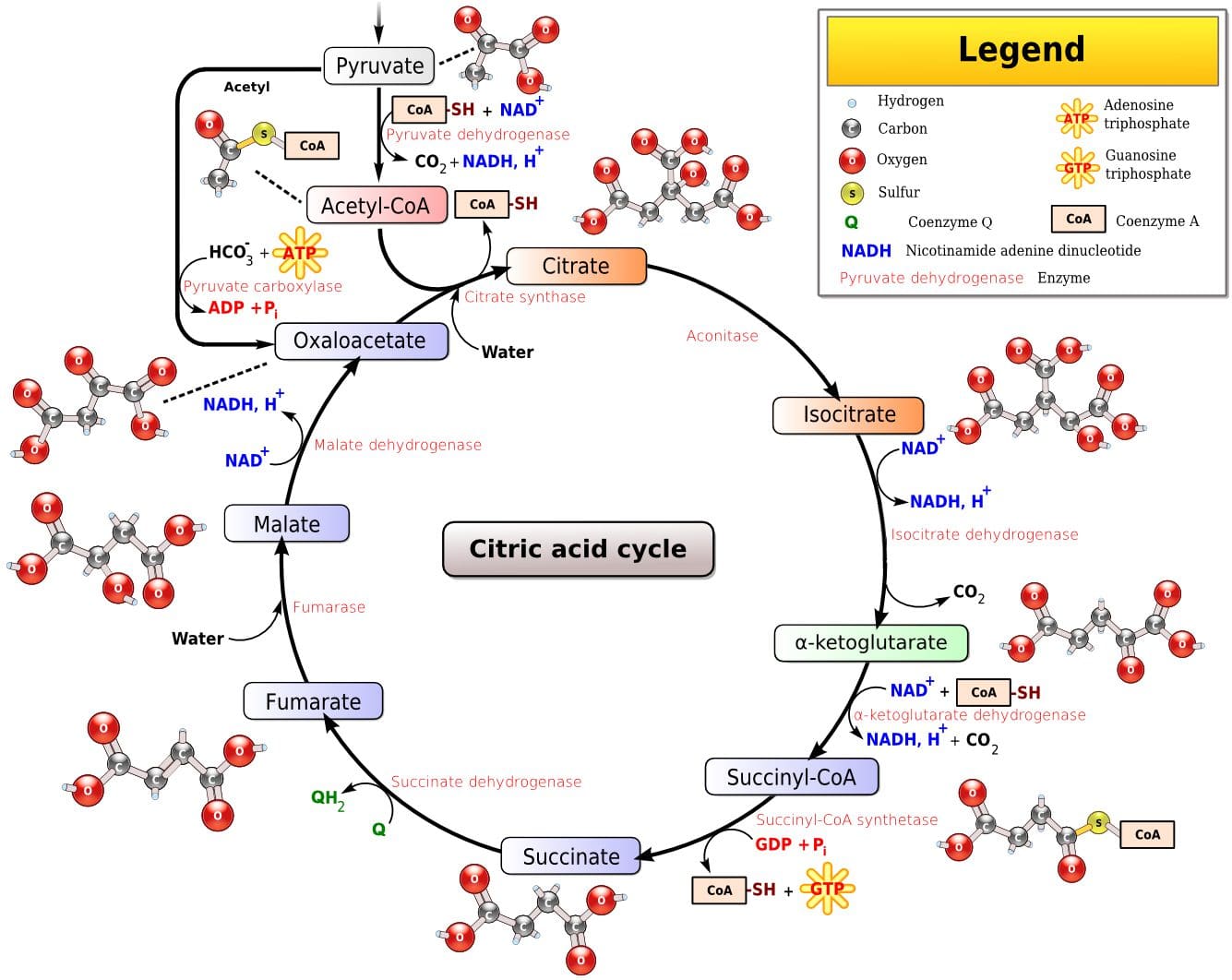 Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).
Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).