Children walking with their toes pointed in may be pigeon-toed. What are the causes, conditions associated with it, and treatments?
Pigeon-toed Walking
If a child walks with their feet turned inward at the toes, it is usually described as being pigeon-toed. This pointing inward of the feet occasionally occurs as a child learns to walk and may continue through toddlerhood. It is noticed more often in children than adults, but older individuals can experience it. Pigeon-toed walking is rarely a major orthopedic problem and usually disappears without treatment. However, there are times when it may impact a child’s lower extremities and hips. Bracing or surgery may be necessary in these cases to correct the problem. (Paramanandam V. et al., 2019) This condition is common and typically is caused by abnormal birth positions in utero. Sometimes, slight issues may lead to noticeable functional characteristics. Mild changes in bone shape and positioning usually cause pigeon toes. Often, it subsides in a few years as the child continues to develop.
What Does It Mean?
There is usually no need to worry, as this condition is likely not permanent and will go away in a few years. (Paramanandam V. et al., 2019) However, it is recommended that you check in with your healthcare provider to ensure the child is developing normally. Some adults walk with their toes turned in. This may be due to a birth defect, a weakness, or a rare case of pigeon-toed walking as a youth that was left untreated or did not go away.
Causes
There are various reasons for pigeon-toed walking. To determine the cause, a healthcare provider can assess the child’s condition and make a diagnosis, including:
Metatarsus Adductus
A condition where the front part of the foot is turned inward.
The metatarsals are the long bones of the forefoot.
This is when the bones of the foot point inward, leading to pigeon-toed walking.
A clinical examination and X-ray can confirm the metatarsus adducts as a cause of pigeon-toed walking.
Tibial Torsion
A twisted shinbone (tibia) can cause the feet to turn inward in younger children.
The shinbone/tibia in some children may be slightly twisted.
The tibia can either turn outward or inward.
When it twists inward, it may manifest as a pigeon-toed gait.
Tibial torsion may accompany femoral anteversion.
It is diagnosed with an X-ray.
Children with tibial torsion typically grow out of the problem, and the pigeon-toed disappears by age 4. (Uden H., & Kumar S. 2012)
Femoral Anteversion
A common cause, especially in older children, is when the thighbone/femur is twisted inward.
If the femur turns inward and forward unnaturally, where the femoral neck meets the body of the femur, it is called femoral anteversion.
An outward and backward rotation of the femur is called femoral retroversion.
Many children with femoral anteversion appear knock-kneed with a large gap between their feet when standing with knees together, and when they walk, they appear pigeon-toed.
A clinical examination and X-ray diagnose it.
Symptoms
In most cases, the child does not complain of any pain. However, if pain is felt, it can include:
Tightness in the calf muscles
Aching on the outer edges of the feet
Knee pain
Usually, parents will notice pigeon-toes when their child is first learning to walk. Rest assured, the child most likely is not experiencing pain. They have feet and knees that turn inward when they walk and run. (Uden H., & Kumar S., 2012)
A pediatrician or primary care provider can assess the situation and make recommendations. Most pigeon-toed children begin walking and running normally after age 3 or 4, so a watch-and-wait approach is used. Parents may have to take their child to a specialist, like an orthopedic surgeon, if they complain of pain while walking. A specialist may be referred if the child cannot walk due to the inward turn of their feet.
Risk Factors
Pigeon-toed walking is not a preventable condition but rather one that develops during pregnancy. Causes may include: (Scorcelletti M. et al., 2020)
A pregnancy with twins or multiple births
Large fetus
Breech position in utero when the baby is positioned feet first.
Typically, a normal gait will appear by age 3 or 4. Other treatments may include:
Physical Therapy Exercises and Gait Training
Exercises to stretch tight lower extremity muscles and strengthen hip and leg muscles can help improve walking gait.
See a pediatric specialist before starting, as research shows that parental stretching of a newborn with metatarsus adductus offers little benefit. (Eamsobhana P. et al., 2017)
Bracing or Casting
Braces
Serial casting is a procedure that helps children improve their range of movement and may be done to place their lower extremities in an optimum position as they develop. (Uden H., & Kumar S., 2012)
Surgery
For cases in which tibial torsion is the cause, osteotomy surgery, which involves cutting and/or removing bone, may be recommended to correct the structural deformity of the shinbone.
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Foot Pronation
References
Paramanandam, V., Lizarraga, K. J., Soh, D., Algarni, M., Rohani, M., & Fasano, A. (2019). Unusual gait disorders: a phenomenological approach and classification. Expert review of neurotherapeutics, 19(2), 119–132. https://doi.org/10.1080/14737175.2019.1562337
Uden, H., & Kumar, S. (2012). Non-surgical management of a pediatric “intoed” gait pattern – a systematic review of the current best evidence. Journal of Multidisciplinary Healthcare, 5, 27–35. https://doi.org/10.2147/JMDH.S28669
Scorcelletti, M., Reeves, N. D., Rittweger, J., & Ireland, A. (2020). Femoral anteversion: significance and measurement. Journal of Anatomy, 237(5), 811–826. https://doi.org/10.1111/joa.13249
Eamsobhana, P., Rojjananukulpong, K., Ariyawatkul, T., Chotigavanichaya, C., & Kaewpornsawan, K. (2017). Does the parental stretching programs improve metatarsus adductus in newborns?. Journal of Orthopaedic Surgery (Hong Kong), 25(1), 2309499017690320. https://doi.org/10.1177/2309499017690320
Broken bones are common injuries. Because children’s bones grow rapidly, they have increased flexibility. When injuries, specifically fractures, occur, they do not always break cleanly across the bone or into pieces. What type of fracture is this, and how are they treated?
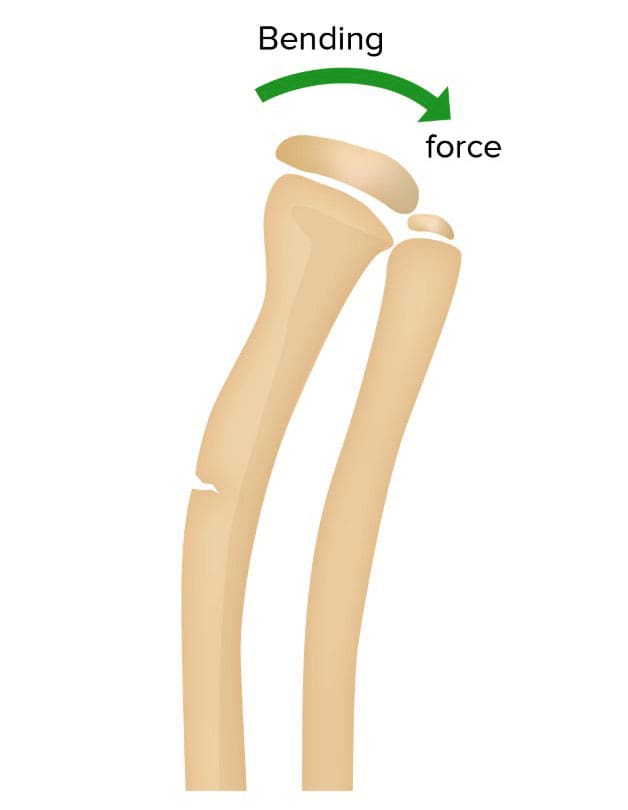
Greenstick Fracture
A greenstick fracture is a partial break in a bone that occurs when a bone bends and cracks instead of breaking into separate pieces. (Wolfe J. A. et al., 2019) The term is based on a young green branch that bends and splinters but does not break into pieces when bent. Only one side of the bone is broken, while the other side gets bent. Many children experience at least one fracture during their growing years. This is one of multiple fracture types seen in children. They can happen in adults but are uncommon.
Causes
Greenstick fractures mostly occur in infants or toddlers, sometimes in children during their early adolescent and pre-adolescent years. They are partial-thickness fractures (a break in a bone that doesn’t completely break it) characterized by a break on one side and a bend on the other. Buckle fractures and bow fractures are different types of partial-thickness fractures. Greenstick fractures commonly occur:
In children under 10 years old
Occurs when a child reaches out to break a fall
During motor vehicle collisions
Sports
Direct impacts
Non-accidental trauma
It is more common in long bones, including:
Radius
Ulna
Humerus
Fibula
Tibia
Clavicle
The fracture pattern often indicates a limb’s bending or contortion.
Deformity, such as the affected body part looking crooked or out of alignment.
Treatment
If the bone is not significantly bent out of alignment, a splint or cast may be all that is necessary to treat the break. If the bone is visibly out of alignment, it must be manually straightened before the limb is put into a cast. If the break is severe, surgery may be required. Fortunately, a growing skeleton can remodel bone, so fractured bones can often realign themselves over time with minimal intervention. Healing depends on various factors, including:
Sometimes, the fracture must be bent back and repositioned in a fracture reduction procedure. An anesthetic may be used as the doctor manually realigns the bone into the correct position. After the reduction, a cast or splint will stabilize the bone and maintain proper alignment. Depending on how quickly the bone heals, a cast may be necessary for a few weeks, months, or longer, depending on the patient and/or underlying conditions.
Healing
Healing involves specialized cells that gradually rebuild and fine-tune the new bone.
The average time for a greenstick fracture to heal completely may take four weeks.
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Building a Stronger Body
References
Wolfe, J. A., Wolfe, H., Banaag, A., Tintle, S., & Perez Koehlmoos, T. (2019). Early Pediatric Fractures in a Universally Insured Population within the United States. BMC pediatrics, 19(1), 343. https://doi.org/10.1186/s12887-019-1725-y
Atanelov, Z., & Bentley, T. P. (2025). Greenstick Fracture. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30020651
Pountos, I., Clegg, J., & Siddiqui, A. (2010). Diagnosis and treatment of greenstick and torus fractures of the distal radius in children: a prospective randomised single-blind study. Journal of children’s orthopaedics, 4(4), 321–326. https://doi.org/10.1007/s11832-010-0269-3
Practicing improper/unhealthy postures throughout the day can severely fatigue the mind and body. Children’s postural health is vital to their overall health and energy levels to perform tasks, school work, and play. An unhealthy posture causes the body to lose its ability to dissipate forces evenly and correctly. Symptoms like soreness, pain, tightness, and irritability can begin to present, which is the body’s way of letting the individual know something is off. When the body is in proper alignment, the spine disperses body weight correctly and efficiently. Chiropractic adjustments can effectively counter the unhealthy posture effects, and simple postural exercises can strengthen the body, increasing healthy posture habits.
Children’s Posture Health
Healthy posture is more than simply sitting and standing up straight. It is how the body is positioned, meaning the head, spine, and shoulders, and how it moves unconsciously like a walking gait. An uneven gait or awkward body position can indicate a problem and cause long-term consequences to a child’s health.
Challenges
Kids and children are constantly hunched, slumped, and slouched over device screens. This constant awkward positioning adds weight to the spine, increasing the pressure, which can cause issues ranging from headaches, mild neck pain, low back pain, and sciatica. Severe health effects from poor posture include:
Shoulder problems.
Chronic pain.
Nerve damage.
Difficulty breathing from prolonged hunching-over.
Spinal joint degeneration.
Vertebral compression fractures.
Poor alignment of the muscles begins to restrict postural muscles from relaxing correctly, making the muscles stay stretched or slightly flexed, causing strain and pain. As a child’s body grows, practicing unhealthy postures can drive continued awkward positioning, abnormal spine growth, and an increased risk for arthritis later in life.
Chiropractic Adjustments
A chiropractor will check for any imbalances, like a hunched back, one shoulder higher than the other, or a pelvic tilt/shift. Through a series of adjustments, chiropractic releases the muscles, relieves pressure on ligaments, allows the postural muscles to relax and realign to their proper position, prevents further muscle overuse, strain, abnormal joint wear, and helps reduce fatigue by conserving/utilizing energy as the muscles are functioning correctly and efficiently.
Exercises
Simple postural exercises can help maintain children’s postural health.
Place hands next to the chest so that they are underneath the shoulders.
Gently press the chest upward.
Keeping the legs on the ground.
Look straight ahead.
They only take a few minutes, but the objective is consistency. Doing the poses for one week won’t immediately change unhealthy posture habits. It is developing consistent healthy postural habits that generate improvement. They should be done at least three times weekly to build strength and endurance.
Kids and Chiropractic
References
Achar, Suraj, and Jarrod Yamanaka. “Back Pain in Children and Adolescents.” American family physician vol. 102,1 (2020): 19-28.
Baroni, Marina Pegoraro, et al. “Factors associated with scoliosis in schoolchildren: a cross-sectional population-based study.” Journal of epidemiology vol. 25,3 (2015): 212-20. doi:10.2188/jea.JE20140061
da Rosa, Bruna Nichele et al. “Back Pain and Body Posture Evaluation Instrument for Children and Adolescents (BackPEI-CA): Expansion, Content Validation, and Reliability.” International journal of environmental research and public health vol. 19,3 1398. 27 Jan. 2022, doi:10.3390/ijerph19031398
King, H A. “Back pain in children.” Pediatric clinics of North America vol. 31,5 (1984): 1083-95. doi:10.1016/s0031-3955(16)34685-5
Poor spinal health in adolescence can lead to chronic pain in adulthood. Teenagers, just like adults, can experience back pain from accidents, sports injuries, a sedentary lifestyle, part-time jobs, chores, etc. However, sitting too long in school along with heavy backpacks can also contribute to compromised spinal health. Chiropractic professionals can help these young individuals address and prevent spinal issues/injuries to maintain a healthy spine.
Teenagers Spine Issues
If discomfort or pain is present, much push through, as they and their spines are young. There are common spinal dysfunctions that teens and parents should be aware of. These include:
Disc injuries
Teenagers can put a serious strain on the spine from various forms of physical activity, jumping, dancing, and playing. This pressure gets transmitted through the spine. During a teenager’s development, this can result in permanent disc damage.
Scoliosis
A spinal deformity or exaggerated curvature of the spine is common and affects young children and teens. It usually happens during the growth spurt just before puberty. This is why it is important to have a teenager’s spine checked regularly and analyzed for signs/symptoms of scoliosis.
Spondylolysis
This condition is often associated with sports injuries. It happens when teenagers overextend/overreach their backs. It’s most common in gymnastics, weight lifting, tennis, football, diving, and other similar sports.
Protection and Prevention
There are several ways that parents and healthcare providers can help teenagers make healthy decisions to achieve and maintain optimal spinal health.
Sitting less, moving more.
Children are taught to sit from a very young age. In school, watching t.v., or doing homework, teenagers spend more time sitting than their bodies should. Teenagers need to stand, walk and move around just like adults to protect their spines from degeneration and injury.
Playing sports is healthy. However, there is a risk associated with teen sports. Although they are taught to play safely, encourage them to continue to educate themselves about sports injuries and know how to address them.
Chiropractic Support
At Injury Medical Chiropractic and Functional Medicine Clinic, we’re committed to helping young adults and adolescents overcome and prevent spinal injuries that could turn into chronic pain conditions. We are continually developing our chiropractic, and physical therapy treatment approaches to achieve optimal results.
Body Composition
Sleep and Growth Hormone In Children
Growth hormones primarily control growth. The hypothalamus and the pituitary gland regulate this hormone. Sleep plays an important role in the proper function of these glands. A review showed that:
Growth hormone levels rise and peak at the onset of deep sleep
Multiple but smaller peaks were seen during other sleep stages
Individuals that have a delay in the onset of deep sleep have delayed peaks in growth hormone levels
For children to grow properly, they need to have adequate levels of growth hormone. This means they need to have a sufficient amount of sleep. The proper amount of sleep is vital for healthy body composition. A study measured the body composition of preschool-aged children. The study found that children who had proper sleep levels had less overall fat mass and reduced body fat. Children and teenagers need to get the proper amounts of sleep for their bodies to grow healthily.
References
Clement, R Carter et al. “What are normal radiographic spine and shoulder balance parameters among adolescent patients?.” Spine deformity vol. 8,4 (2020): 621-627. doi:10.1007/s43390-020-00074-9
Driehuis, Femke et al. “Spinal manual therapy in infants, children and adolescents: A systematic review and meta-analysis on treatment indication, technique, and outcomes.” PloS one vol. 14,6 e0218940. 25 Jun. 2019, doi:10.1371/journal.pone.0218940
Manansala, Christian et al. “Change in young people’s spine pain following chiropractic care at a publicly funded healthcare facility in Canada.” Complementary therapies in clinical practice vol. 35 (2019): 301-307. doi:10.1016/j.ctcp.2019.03.013
Children and adolescents are experiencing back pain. Why it happens, and how parents can help prevent it is the objective. When thinking of back pain the image is typically a man or woman, hunched over grabbing their backs and wincing in pain. However, back pain in children and adolescents is not that uncommon.
According to a 2020 study published in Spine, around thirty-four percent of children report having back pain, with almost nine percentexperiencing severe back pain. By the time they are fifteen, 20 to 70% of children will have experienced back pain at some point. Developing chronic back pain increases with age and is more common in girls.
The study found those that sought out early treatment, physical therapy, and chiropractic being the most prescribed lessened the need for more invasive treatments, like spinal injections, and surgery. Back pain can have a major impact on an adult’s life, and more so on a child. Prevention and treatment are important to help restore overall health and wellness.
Signs and Symptoms
Symptoms can vary, the most common:
Pain increases with movement, like bending or twisting
Increased pain after sitting or standing for an extended period
Sore and tender muscles around the spine
Tight muscles
Muscle spasms
Most back pain in children is mild. However, there are times when the child will require medical attention. A child should see a doctor if back pain persists for more than two or three days, if there is a fever, or if there is any numbness or weakness in the arms and legs.
Common Causes
Like adults, muscle sprains and strains are the most common cause of back pain. Strains are more common in the low back than around the neck or middle back and usually occur from overuse injuries, poor posture, poor body mechanics, and falls. Other common causes include:
Sitting and slouching in front of the computer for too long
Carrying an overloaded backpack
Spinal Conditions
Recreational and sports activities with injuries sustained are the most common causes of developing back pain. However, back pain can be brought on by underlying health and spine-related conditions. About a third of adolescents with low back pain could have a spinal condition. The most common conditions include:
Idiopathic Scoliosis
This is an abnormal curvature of the spine. This is usually not a painful condition. Some curvatures can be severe enough to cause pain and require medical care. Scoliosis can include the middle, low spine, or the entire spine. It is most common in adolescents 11-17 years of age. Symptoms include:
Tilted shoulders
Uneven hip bones
One side of the ribs projects out more than the other
Scheuermann�s kyphosis
This is a growth disorder of the vertebrae. It happens when the front of the spine does not grow as fast as the back of the spine. This can produce a humpback curvature. The spine bends forward but the child cannot stand up straight. Usually, it happens during accelerated growth periods.
Spondylolysis
The vertebrae can break in children and kids that do repetitive exercises involving bending and twisting. Sports like gymnastics and football create a heightened risk for spondylolysis. It usually affects the low back and presents with non-stop low back pain. The most common treatment is rest. Other causes include:
Spinal cord tumors
Sickle cell anemia
Infection
Tumors and infections are highly uncommon in children. They often present with pain and fever. If the nerves are pinched numbness, tingling, and weakness in the extremities can develop.
Common Treatments
Back pain in children is usually a short experience and can be treated with ice, rest, and over-the-counter medications like acetaminophen for children and nonsteroidal anti-inflammatory drugs like ibuprofen. A playing/exercise program can significantly help reduce child back pain.
However, there could be a need to modify the activity, so as to not worsen the injury or create new injury/s. The activities could be made to be lighter or a brace could be utilized. A specialist like a chiropractor/physical therapist can provide treatment, along with exercises, stretches, and lifestyle changes that will help reduce the pain. Complementary therapies like massage and acupuncture can enhance the child�s healing/recovery time and knock out the pain quickly.
Parental Prevention
Proper posture can and will prevent back pain. Children’s and adolescents’ musculoskeletal structures continue to develop at this stage. Therefore, sitting, standing, and lifting properly is paramount to preventing back pain. Along with this is avoiding activities that place repeated strain on the spine. An example is an overexertion while playing sports. Tips for keeping kids back-pain free:
Avoid activities that generate repeated strain on the same muscles
Stretching breaks need to be incorporated when sitting for a long time
As much as possible make the home a stress-free environment
Maintain a healthy weight and diet with balanced meals and snacks
Help promote overall mental and physical health
Children and kids that are stressed out or depressed have a greater risk of developing back pain. Encourage the kids to stay active, get proper sleep, stretch out, and eat foods that are healthy for the spine. If back pain is presenting, a customized treatment plan along with lifestyle changes will get the child back to their favorite activities.
Lower Back Pain Chiropractic Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Chiropractic adjustments for children’s health is nothing new, but it could be something new for parents. Do children really need chiropractic adjustments? Chiropractic physicians, also known as DC’s provide techniques and treatments that pediatricians don’t offer.
Chiropractors offer non-invasive options, before referring an individual to a pain specialist that might only prescribe medication/s and surgery. The body’s central nervous system controls everything. Birth itself can be physically traumatic for some infants. Therefore, receiving an adjustment can improve neurological input and correction, allowing for healthy development. �
�
If involved in sports or some type of physical activity, chiropractic helps recovery from injuries progress faster and is less traumatic than disruptive therapies like pain-meds or surgery. Chiropractic medicine takes into account the entire person when there is an adjustment/correction in one area, it supports and corrects the other areas.
Depending on the chiropractor, other techniques and specialties like acupuncture, craniosacral, nutrition, and more could be incorporated into a patient’s treatment plan. Here are a few ways chiropractic can benefit children’s health.
�
Non-invasive
Chiropractic treatment is holistic and non-invasive. For children’s health, adjustments help with proper growth and development by removing or limiting digestive issues like:
Nursing
Re-flux
Colic
Constipation
Other issues for where pediatric chiropractic care can be utilized include:
Allergies
Asthma
Bed-wetting
Colds
Ear infections
Attention deficit disorder
Attention deficit hyperactivity disorder
Autism
�
However, unlike adults, children, and especially infants, chiropractic medicine focuses on mobilization that places a lower amount of pressure on the area, rather than manipulation associated with chiropractic for adult treatment that places more pressure on the area being adjusted.
�
Nutrition
Parents who are considering chiropractic treatment for their children’s health and wellness should also expect nutritional health coaching for optimal health. Chiropractors go through extensive training in nutrition and are qualified to offer nutritional plans that are part of the treatment.
Proper nutrition is important for everyone�s health. But for children who are growing and developing, it is essential that they get the nutrients they need for optimal spine health and development. Some foods and food additives can cause behavioral issues. These foods include:
Dairy
Artificial colors
Sugar
Preservatives
Other food allergens
Chiropractors can help parents and caregivers by testing and identifying behavioral triggers whose root cause could be nutritional that is improper or deficient for children’s health. �
�
Wellness Philosophy
Educating parents and families about the benefits of proper nutrition and fitness are essential for children’s health and wellness. Families need to follow the principles of:
Eating whole foods
Junk food minimalization
Electronic device limits
Playing/exercising regularly
These are strategies that will reduce childhood obesity that is causing a range of problems for health care like Type 2 diabetes, high cholesterol, and high blood pressure. Excess weight in young children and if it goes on for a long time creates a higher chance of earlier death in adulthood. From a psychological perspective, it is important to understand that during childhood kids can develop a negative body image, leading to low self-esteem, and causing depression. This can lead to serious mental health issues.
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Strength training: The Centers for Disease Control have estimated that around 16% of six to nineteen-year-olds in the US are overweight or obese. This comes from inactivity, no movement, exercise, and poor diet. On the other end, young athletes search for ways to gain an edge, often falling victim to steroids and all of the negative effects they have.
This is where strength training comes in. This could be an answer to getting kids off the couch, moving, and offers a healthy alternative to the young athletes looking for that competitive edge. Fitness experts, doctors, health coaches, and parents say absolutely.
The focus for children in strength training is not to bulk up, as this is not weightlifting, powerlifting, or bodybuilding. Fitness experts agree that these types of training regimens are not healthy or safe for children. The goal is to:
Added benefits of strength training can help young athletes improve performance through increased endurance.
Training Guidelines
It is fundamental to find a program that is safe and successful for children. Parents want a program designed specifically for kidssupervised by a fitness professional with child experience, and most of all, it is fun. For strength training, there is not a minimum age; however, the kids should understand and follow directions.
Before starting a child on any new fitness program, check with their doctor or healthcare provider.
A training program should include:
A session should start with a 5-10 minute warm-up exercise/s like stretching and light aerobics.
Every session should end with a cool-down combined with stretching and relaxation.
Kids should not immediately be using weights until proper form and technique are learned.
Kids should start with their own body weight, bands, or a bar with no weight.
Using 6-8 different exercises that address all the muscle groups, begin with 8-15 repetitions.
Each exercise should be done with a complete follow-through of the full range of motion.
If the repetitions are too much with a specific weight, reduce the weight.
Repetitions and sets should gradually increase over time to maintain the intensity of the training.
Add more weight only when the child displays the proper form and can easily do at least 10 reps.
Workouts should be 20 to 30 minutes long, 2 to 3 times per week, to get the most benefit.
Make sure to rest a day between each workout day.
Safety
Strength training was not always considered an appropriate exercise for kids. Doctors and fitness professionals believed that it was unsafe for a child’s growing body because of the added pressure on growth plates or the cartilage that has not fully turned into solid bone. However, experts now know that kids can safely participate in a strength training program with proper technique and supervision.
As with any exercise/fitness regiment, safety measures need to be in place along with heightened supervision. Unfortunately, most injuries happen when kids are not supervised, not using proper techniques, or from trying to lift too much weight. Here are some safety precautions to remember:
Learning new exercises should be done under the supervision of a trainer/instructor, making sure proper technique and form are used.
Smooth, controlled motions should be the goal.
Controlled breathing and not holding their breath needs to be taught
Proper technique will help avoid injuries
The kids’ progress should be monitored
Have the children record the exercises they have done, how many reps, and the amount of weight/resistance.
If enrolled in a strength training class, a good ratio is one instructor per 10 students. With this ratio, the kids can receive proper instruction and supervision.
Kids should train in a hazard-free, well-lit, and properly ventilated facility.
Make sure the kids drink plenty of water during and after the workout
Fitness trainers/instructors will see to it that there are frequent rest and rehydration breaks
Keep in mind
In a strength training program for children, there should be no competitive drive. Instead, the focus should be on participation, learning the movements, and positive reinforcement. Set realistic goals and expectations for the child to understand that it will take time to learn these new skills.
Remember that kids do not increase muscle size until after puberty. Please make sure the kids enjoy the strength training sessions and that they are having fun. Keep in mind that kids can become easily bored. Therefore, use various exercises and routines, keeping them excited and wanting to learn and do more.
Healthy Habits
Getting kids interested in fitness early on can help establish a life-long habit of wanting to be and stay healthy. This includes a balanced diet, plenty of rest, and regular exercise. When done correctly, strength training can be a fun and highly beneficial activity.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




 Causes
Causes





















