Chiropractic adjustment has various applications. From the treatment of chronic pain and pre-existing conditions to early or sudden onset pain. Perhaps most frequently cited, sufferers of back and neck pain, sciatica, migraines and more have found relief from chiropractic medicine.
In fact, many medical doctors recommend that their patients seek chiropractic care for a variety of conditions before seeking more invasive measures such as surgery. This sentiment was (echoed by the American Medical Association) as recently as 2013.
Relieving Back & Neck Pain
Roughly 80% of adults have experienced back pain at some point. (In a study by Consumer Reports), �14,000 sufferers were surveyed. None of these individuals had undergone back surgery of any type. By the end of the study, Chiropractic adjustment was rated as the #1 treatment option.
At the conclusion of the twelve-week study, patients who underwent regular chiropractic adjustments were twice as likely to be pain free as those who were treated with medication. (Further research demonstrates) the validity of chiropractic adjustments as easily seen via magnetic resonance imaging (MRI).
Patients with lower back pain often experience limited mobility in the lumbar spine region that produces degeneration as well as adhesions within the joints of the vertebrae. When patients received an MRI scan following a chiropractic adjustment, the imaging showed an increase in spinal gapping. This breaks up the adhesions, allows the joints to move freely, and lead to a reduction in pain.
Headaches and Migraines
Chronic head pain, including migraines is another common condition that chiropractic adjustment can provide relief for. Through manipulation, chiropractic medicine is able to relieve pressure off of the nerves and provide relief. Headache and migraine sufferers may find long-term relief with continued adjustments, resulting in lessening the severity of symptoms or the frequency of onset.
There is also published research showing the validity of these treatment options. In an (Australian study that tracked 127 migraine sufferers), those who received regular chiropractic adjustments reported a decrease in migraine attacks as well as the need to take less medication.
Considering the rising costs of healthcare, specifically prescription medication, mitigating pharmaceutical costs can provide extra benefits.
Foundation for Chiropractic Progress
In Support of Chiropractic Care
Chiropractic care is becoming increasingly more widespread. Support from medical research and organizations such as The American Medical Association, as well as high profile supporters such as Tiger Woods, Jerry Rice, Aaron Rodgers have helped bring the treatments into the mainstream.
Today, Chiropractic medicine is practiced all over the world, and is an increasingly popular as well as effective form of treatment for a variety of conditions, including but not limited to the ones mentioned above.
(Some more statistics)
Utilizing chiropractic adjustments for treatment of back pain may help save Medicare costs by more than $80 million per year.
Back pain sufferers whose first point of treatment included a medical doctor or surgeon, went on to receive surgery 42.7% of the time. For sufferers who sought chiropractic adjustment first, surgery only occurred 1.5% of the time.
Chronic pain sufferers who sought treatment through chiropractic adjustment experienced a 20% reduction in overall care costs.
Is Chiropractic Adjustment Right for You?
The effectiveness of chiropractic adjustment in treating chronic and recent onset conditions is supported through research, scientific study, as well as patients just like you. If you are suffering from pain or discomfort in your neck, back, joints, or elsewhere,�contact a well qualified Chiropractor near you.
About the Author:
Dr. Alec�with Proactive Chiropractic and Rehab Centre extensively studied human anatomy, physiology, radiology, kinesiology and post graduate seminars in topics such as herniated disc, whiplash, functional movement, car accident rehabilitation. With over 10 years of experience, Dr. Alec helps care for patients with back pain, neck pain, headaches, knee pain, shoulder pain, foot pain, whiplash, etc. Treatment services include: spinal decompression therapy, functional rehabilitation, active release technique, gua sha, electro-stimulation, intersegmental traction, hands-on chiropractic adjustment, instrument assisted chiropractic adjustment and rehabilitation. Dr. Alec takes pride in providing individualized treatment for each patient, with lasting results.
Some People don’t believe in Chiropractic Treatment. However, chiropractic care is becoming increasingly widespread through�medical research. And�top supporters, such as Tiger Woods, Jerry Rice, and Aaron Rodgers have helped to bring�chiropractic�treatment into the mainstream.
Dr. Eric Goodman is the creator of Foundation Training, a highly effective protocol. Foundation Training focuses on body weight exercises that integrate as many muscles as possible to strengthen and elongate your core and posterior chain � which includes all the muscles that connect to your pelvis, whether above or below it � thereby alleviating many chronic pain issues.
The protocol has evolved over the years, and I�ve interviewed Goodman twice before, in 2013 and the most recent two years ago in 2014, covering various updates.
Goodman, who is trained as a chiropractor, is a pioneer in the world of structural biomechanics. His program teaches you to optimize your posture, thereby decreasing bodily pain and your risk of exercise injury.
�The idea is really simple. Our body is made to help itself. As long as we can get the muscles to align it properly, our breathing patterns to align properly, our pelvic muscles to be more stabilized, our posture will involuntarily become stronger,� he explains.
�My education is in chiropractic. I�m licensed in Colorado and California, but I only really see patients if they need an adjustment for some reason that they can�t do the poses.�
Contents
Why Foundation Training?
While in chiropractic school, Goodman developed severe low back pain. His doctors suggested surgery, which he wisely rejected. Instead, his own pain set him on the path of discovering a long-term solution, which ultimately resulted in Foundation Training.
�My passive care was good. I was getting chiropractic care. I was being stretched. I was being massaged and worked on. But I wasn�t strengthening my spine myself. That�s the difference that I made,� he explains.
�I don�t think that I will ever negate chiropractic, because I love chiropractic. I love the ability and capacity to align the body, align the nervous system and create a very good environment for different process to occur.
[But] if you�re going to get your neck adjusted, I want your neck to stay long and strong afterwards, because that�s what�s going to stop you from having that same adjustment again a week later.�
While obsessively studying anatomy, alignment and exercise in an effort to resolve his back pain, Goodman began to notice that he, and many other people who were in pain, could not move the way the body was designed to move, and this was causing a degenerative effect � and those who were moving properly were able to regenerate and increase strength, while reducing injury and pain.
�I was in chiropractic school. I really understood the body well. I decided that this is going to become an obsession. I�m going to figure this out. I can�t become a doctor, have patients come to me that are asking for my advice on an injury that I have that I can�t fix. It�s not OK.
So, over the course of about four years, I did that. I became very obsessed. I used my anatomy knowledge. I used my understanding of exercise.
I was a personal trainer actually long before a chiropractor. Foundation Training is what I came up with. It�s what I do for myself every single day, and it�s what I�ve been extraordinarily fortunate to teach to thousands of people at this point.�
The secret to Foundation Training lies in its simplicity: no gyms, no specialized equipment and no complicated stretches. By incorporating a series of powerful movements into your daily routine, you can move better, breathe better and get back to using your body the way nature intended.
Addressing Back Pain
Low back pain is a very common problem, and the most common reason why people seek out Foundation Training. In the video below, Goodman demonstrates a back extension exercise that is particularly helpful for back pain relief.
The premise is simple. By strengthening the muscles in your back, they will keep your spine properly braced through all the movements you do as you go about your day-to-day life.
Overall, about 7 out of 10 people who learn Foundation Training do so to address back pain, 2 out of 10 seek to improve their sports performance and the remaining 10 percent typically seek to address knee pain, neck pain, jaw pain, plantar fasciitis, carpal tunnel and other chronic pain.
How to Get Started With Foundation Training
In addition to their latest book, �True to Form,� Foundation Training offers a variety of ways to get the benefits of their system, including their free videos on their website at www.FoundationTraining.com.
Foundation Training also offers certification for clinicians, practitioners, trainers and instructors who are looking to share this groundbreaking and highly effective protocol with their clients and patients.
�There are probably more people using our free videos to get well than using our DVDs and books,� he says. �That�s awesome. That�s why we have free videos.
Our latest book, �True to Form,� is our illustrative process of bringing Foundation Training into your everyday activities � brushing your teeth, waking up from bed, reaching into the refrigerator, whatever, how to apply very simple movement patterns that make you stronger while you do that.
Then if you want to really get into it, we have DVDs and we have a new streaming website. If you�re really into it � come to our workshop or certification. If you come to our workshop and you decide you want to go through a certification, we take the amount of money you paid on the workshop, 100 percent of it, off the cost of the certification.�
While millions of people have gotten started through the free Foundation Training videos, the optimal way to get the most out of Foundation Training is the comprehensive step-by-step program offered on their website or a certified Foundation Training instructor.
The Importance of Posture for Ease of Movement and Health
As noted by Goodman, �Posture is a beautiful thing, except when it�s messed up.� Indeed, while I see many people walking the beach during my daily walks, poor posture is the norm, with hunching being one of the most prevalent posture problems. Indeed, �standing tall� is so basic yet most have forgotten how to do it. When you stand tall, your muscles actually work more effectively.
�We naturally adapt towards our chosen method of absorbing gravity � �Our muscles absorb force � Whether they�re contracting or expanding, they are absorbing or providing force. If you take the opportunity of gravity � this ever-present weight of your own body � and simply provide 5 percent more energy in absorbing it, 5 percent more conscious effort throughout the day, it�s going to change your life forever. It�s going to have people reacting to you differently. It�s going to have you reacting to things like anxiety differently. You�re going to feel the difference of a closed airway and an open airway.
You�re going to feel the tightness of your jaw from the head traveling to forward, contracting the back of your neck when you�re in a bad posture � You start interacting with people like a confident human being interacts.�
Patience and Practice
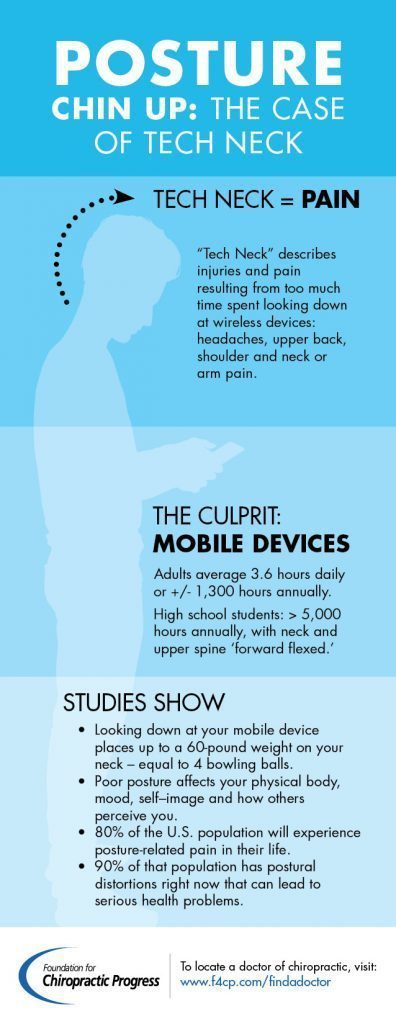
Most people have poor posture these days. Besides chronic peering down on your smartphone or tablet and excessive sitting, which encourages poor posture unless you�re paying careful and active attention to your body at all times, we�ve also been taught certain posture strategies that actually worsen posture rather than improve it.
Pulling your shoulders back to straighten your posture is one example. As noted by Goodman, this is a �compartmentalized correction� at a place that�s not actually causing the problem. More than anything else, the places that cause the problems in posture are the upper and lower ends of your spine.
A very basic explanation is that your upper and lower spine should be pulling away from each other, not compressing or falling toward each other. So the back and top of your head needs to be pulling away from your tailbone, straight up and neither forward nor backward.
As for how long it might take to correct your posture, it clearly depends on your individual and specific circumstances: how long you�ve had poor posture, how much time you dedicate to corrective exercises and the extent of your postural problems.
�It may be a matter of weeks to months. I believe for some people it may be a year [to complete] the whole process. [But] they�re going to be feeling better along the way. They�re going to notice incremental changes. They�re going to see that their body is supporting itself better steadily. They�re thinking about it less. They�re feeling less pain. They�re feeling better posture. That�s when the real changes start to happen. But there�s no set timeline.�
Walking 101
Walking is foundational for optimal health, and walking with good posture can really maximize your benefits. Your choice of footwear can have a significant influence here. When walking in sneakers or heels, your heel is raised higher than your toes. This in turn makes your arch tighter, which completely alters your range of motion. So, to start, walk barefoot or find a pair of zero-drop shoes.
The rationale behind walking barefoot has to do with plantar flexion, the shortening of the muscles on the back of your ankle and the lengthening of the muscles at the front of your ankle and shin. When walking barefoot, you alter the way the back of your body absorbs force for the better.
Dorsiflexing is a tremendously important piece of walking. This is where you�re lifting the top of your foot toward your shin. When you�re walking with plantar flexion (due to wearing heels), you rarely dorsiflex, thereby contracting and shortening the muscles of your shin.
�That�s Step 1, making sure that there is good dorsiflexion in every step,� Goodman says. �Literally lift the top toes away from the ground. Lift the balls of the feet away from the ground and try to spread your feet a little bit. That will allow your hips to follow a much more natural range of motion. As your feet dorsiflex, it triggers these muscles of the inside and outside of your legs.
Those muscles have internal rotation capacity and external rotation capacity. Both of which are very important for walking � The ability of the adductors, the medial hamstring, the muscles of the inner part of the thigh, the inner upper part of the thigh, to contract during a walk, to spin that hip a little bit more neutral towards straight ahead �
Long story short, range of motion of the hips is so significant to walking. That range of motion is limited most frequently in people at the feet with plantar flexion, excessive plantar flexion or excessive external rotation.�
Head Posture While Walking
The other piece of the puzzle is the location of your head. Most people walk as if they�re sniffing their way forward, head leading the rest of the body. A more natural posture is to lift your chest upward, which allows your shoulders to lift and your chin to retract more or less automatically. So think: �Chest up, chin back.� Initially, this may feel and even look a bit awkward, but you�ll notice it�s a significantly more powerful way to walk, allowing you to engage more muscles.
�If you simply focus on chin back, chest up, shoulders big, broad, not backing down but out � if you focus on that � you�re going to be walking very different. You�re going to experience this really rhythmic counterbalance in your walk. When the right foot comes forward, the shoulder comes forward on the opposite side.
It�s just these nice little muscular glutes, hamstrings, calves, adductors across the body to the opposite shoulder and pec � So many muscles involved. It�s the SCMs that are very important as well to keep that chin back, chest up function happen.�
Preventing iPhone Neck and Dowager�s Hump
The chest up, chin back posture will not only make you look better, but proper posture may also help prevent osteoporosis and significantly reduce your risk of developing a dowager�s hump, which tends to be quite common among the elderly, and women in particular.
This forward slumped posture tends to be related to chronic improper posturing that worsens over time, eventually leading to the development of rigid intractable calcifications. The beginning of the progression of the dowager�s hump is typically the loss of thoracic extension.
�I think the lack of movement and stagnation in bone leads to calcification and typical degenerative changes. Degenerative changes along with spine make it less mobile � It supports it because the muscles aren�t, the discs aren�t. It puts very rigid support structures in place.
Now, can you imagine 20, 50 years from now, when it�s 60 or 70 years after cellphones and iPads came around, the dowager�s humps, we can start calling them the iPad hump � The younger you are, the more capacity you have to be plastic, to engage your body�s natural tendency to respond to stimulus in such a fashion that will get better and better at doing the thing you�re asking it to do.
If you�re often asking it to look down at your phone, please often ask it to lift your chest up, to pull your chin back and to just stand very firm on the ground. Just look at your phone while keeping your chin back and chest up.�
According to Goodman, even if you�ve already started to develop a slight hump, chances are you�ll be able to significantly improve your alignment provided your spine has not yet calcified. Exceptions might be if you have ankylosing spondylitis (AS) or diffuse idiopathic skeletal hyperostosis (DISH). Naturally, the younger you are, the more room for improvement there is.
One important aspect of Foundation Training is what Goodman refers to as compression breathing. With his breathing protocol, you literally re-educate the muscles surrounding your axial skeleton, the spine of your rib cage, teaching them to be in a state of expansion rather than contraction. You�ll find a demonstration of this technique in the video above, followed by another founder exercise.
�[This breathing technique] is something that�s always going to set our work aside from everything else. Not better. Not worse. Different. It�s an accessory,� Goodman says.
�Decompression breathing, which can be taken and applied to any movement, any exercise, any activity � will do more for your spine, more for your chest and neck, more for your dowager�s hump � than anything else I can possibly teach you. The unique thing about it is our specific protocol of learning how to engage the diaphragm more appropriately by drastically strengthening the muscles that surround the rib cage.�
Here�s a quick summary of the compression breathing exercise demonstrated above:
Position your feet so that the OUTSIDE of your feet are parallel. This will make it appear as though you�re standing slightly pigeon-toed
Pull your chin back and lift your chest
Place your thumbs at the bottom of your rib cage, and your pinkies on your pelvic bone
With each breath, your aim is to increase the distance between your thumb and pinky fingers, as well as increase the width of your upper back. This occurs as you elongate the back of your rib cage. Each inhalation expands your rib cage, and each exhalation will keep the abdomen extended and tight. So each in-breath fills up your rib cage, and each out-breath maintains the height and width of your rib cage
Repeat five to 10 rounds with three to four breaths per round
More Information
You have many options when it comes to learning Foundation Training. You can start by reading through or listening to my previous interviews with Goodman, �How Foundation Training Can Help You Maximize Strength and Freedom of Movement� and �New and Revised Foundation Training Exercises Add Even Greater Health Benefits.�
For free video demonstrations and tutorials, be sure to check out FoundationTraining.com and the free videos they have available at their site. For even more in-depth information, pick up Goodman�s latest book, �True to Form: How to Use Foundation Training for Sustained Pain Relief and Everyday Fitness.� Join Foundation Training Connect or check out their free resources at FoundationTraining.com/free-resources.
Just remember, the key is to actually DO the exercises. Just reading about them or watching a video will do you no good. The good news is, even if you�re wheel-chair bound, you can perform the compression breathing exercises, which will, at bare minimum, help you breathe better.
�I have a friend that is [in a wheelchair] and we do some of those workouts. He�s a very good guy from Oklahoma City, but had a very tragic accident. I really hope I get to spend some more time with that guy and see what we can do just based on breathing,� Goodman says.
Foundation Training is a�program that teaches you to optimize your posture. By getting the muscles, breathing patterns, and pelvic muscles to be aligned properly and more stabilized, our posture will involuntarily become stronger,� decreasing bodily pain and risk of injury.
While automobile accidents are the most common cause of whiplash, it must be noted, that these aren�t the only possible incidents behind the well-known injury. Any type of accelerated motion which thrusts the head forward and then backwards with extreme force from the entire body can lead to whiplash. Accidents from sports can also cause whiplash-associated injuries but auto accidents are the most prevalent.
The unexpected jolt of the head can damage the complex structures of the cervical spine, leaving the tendons and ligaments within the neck intensely irritated and inflamed. Furthermore, the tendons and ligaments as well as other tissues of the neck may become overly stretched and torn.
A whiplash type injury may be suspected if the individual involved in an automobile accident experiences the following symptoms: neck pain and stiffness; worsening pain with movement; loss of range of motion in the neck; headaches, most often starting at the base of the skull; tenderness or pain in the shoulder, upper back or arms; tingling or numbness in the arms, fatigue and dizziness. Other individual�s may experience: blurred vision; ringing in the ears; sleep disturbances; irritability; difficulty concentrating; memory problems; and even depression. While these are some of the most common symptoms of whiplash, they may also suggest the presence of another type of injury or condition resulting from the automobile accident.
Thus, it�s essential to visit a qualified healthcare professional who can properly identify a whiplash injury and offer the required treatment to eliminate the resulting pain and symptoms.
Apart from assessing the doctor�s experience and qualifications, the victim of an automobile accident must primarily consider their geographical location and the type of insurance they are covered by when deciding on the type of doctor to visit following a whiplash type injury. Other factors that should influence the affected individual�s decision include whether they are represented by an attorney and whether they are living in a state where PIP, or personal injury protection, is mandatory.
Contents
Whiplash Specialists
A large number of people who�ve suffered injuries from auto accidents fail to receive the kind of medical care they require, occurring more frequently in the case of whiplash victims. It has been previously determined that the outcome of the patient�s rehabilitation depends on the type of doctor they receive care from.
Many individuals who�ve been involved in an automobile accident, regardless of the severity of the collision, will generally visit the emergency room, or ER, to have their injuries evaluated. The majority of ERs are designed to take patients out of life threatening situations. First, they immediately assess any visible injuries, such as open wounds and broken bones, treating them effectively on the spot. They may even prescribe medications to temporarily relieve the painful symptoms following a traffic collision. However, many victims are not treated for their whiplash injuries. The trained specialists from the ER, provide first-aid, X-rays and medications to remove individuals from life-threatening situations but they don�t readily treat soft-tissue injuries like whiplash. From there, patients are sent to see their primary care physician, or PCP, to assess the rest of their injuries, yet, they may still face hardships to finally receive the proper care they deserve for their injuries.
Primary Care Physicians and Whiplash
Unfortunately, many primary care physicians are not specifically qualified to treat automobile accident injuries and many of these may even deny patients treatment. For many years, whiplash-associated disorders have been misunderstood in the medical field. Many doctors believe whiplash is not a legitimate injury, however, those whom are suffering from whiplash can account for how painful it could really be.
Other doctors refuse treatment to whiplash patients because they may not accept any kind of 3rd party billing, a paying method where the doctor seeing the car accident victim has to bill the party at fault�s insurance company or utilize PIP or med pay to receive compensation.�This is a commonly well-known reason for denial of treatment as a large number of primary care physicians, or PCPs, still don�t have the required authorizations to accept 3rd party billing.
Besides primary care physicians, medical doctors, orthopedics, chiropractors and physical therapists are several types of qualified healthcare professionals that specialize on treating automobile accident injuries such as whiplash. Among these, chiropractic treatment is the most popular, alternative treatment option for treating various soft tissue injuries or conditions.
Chiropractic Care for Whiplash
A wide number of people belonging to the legal and medical industry will disregard the idea of visiting a chiropractor to treat auto injuries. However, the fact is that a chiropractors are some of the only doctors who offer therapeutic treatments to accident victims. Treatment offered by medical doctors might include the use of drugs, although in many cases, they may also recommend physical therapy. This automatically highlights the importance of chiropractic care for whiplash victims because chiropractic care and physical therapy are very similar forms of treatment.
Whenever an individual who�s been involved in an automobile accident visits a chiropractor and complains of pain in the neck, the medical specialist will carry out a series of tests to determine whether the patient has suffered whiplash. Instead of focusing solely on the specific injury, chiropractors are trained to inspect the affected individual�s entire spine. Aside from soft tissue injuries like whiplash, chiropractic doctors may also check for: disc trauma or injury, tightness or tenderness, restricted mobility, muscle spasms, joint injuries, ligament injuries, posture and spinal alignment. They may also analyze the patient�s gait.
Besides checking for the above, chiropractors might also request X-rays and MRI of the patient�s spine in order to find out whether the spine features any degenerative changes which might have developed before the accident. To offer the best possible treatment, it is extremely important to determine which problems existed prior to the accident and which ones resulted from the accident. In most cases, insurance companies may argue that every single injury in the victim�s body is preexisting. This makes the role of the chiropractor considerably important as they will make sure to document all the previous and new injuries separately to ensure the insurance company pays for the patient�s treatment. In addition, the evaluation performed by the chiropractor also allows them to create the most effective treatment plan for each individual whiplash victim.
Stages of Treatment
The primary concern for chiropractors treating individuals who�ve experienced whiplash-associated disorders involves alleviating the inflammation in the neck, one of the main sources of pain for victims. Chiropractors often recommend ice therapy, or the application of ice pack against the affected area, multiple times a day. This remedy is capable of reducing both pain and inflammation. Once the inflammation subsides, they often carry out a variety of manual therapeutic techniques to restore and increase the individual�s strength, flexibility and mobility.
The kind of chiropractic treatment the individual will require depends largely on the severity of the whiplash encountered. However, it has been previously determined that the majority of individual�s with whiplash find spinal manipulations useful. The most common chiropractic treatment techniques involve, spinal adjustments and manual manipulations, to carefully re-align the structures of the spine and help reduce symptoms. The following spinal techniques are also used to treat whiplash injuries:
Instrument-assisted, this treatment involves the use of handheld instruments to provide a gentle massage by applying force onto the spine without utilizing any kind of thrust. Instrument-assisted chiropractic therapy is used mostly to treat older patients with degenerative joints; flexion-distraction, this technique involves the use of a non-thrusting motions, best described as a slow pumping action; specific spinal manipulation, this therapy involves the use of a mild thrusting technique and is mostly used for restoring motion to the affected joints. Specific spinal manipulation helps stretch the soft tissues, which makes the job of restoring motion to the affected areas of the spine easier; instrument-assisted chiropractic therapy, also known as the Graston Technique, is used during this form of chiropractic therapy to perform repetitive strokes on the injured body part; therapeutic massage, performed to ease muscle tension and stress in the injured region; interferential electrical stimulation, where a patient undergoing this type of therapy will see the chiropractor passing electrical current at a very low frequency through their body. This low frequency current helps stimulate the muscles and reduces inflammation; trigger point therapies, as the name suggests, involves the application of direct pressure onto specific points to alleviating muscle tension; and finally ultrasound therapy, capable of decreasing stiffness, pain, and muscle spasms in the affected areas. When ultrasound is passed through the patient�s muscle tissues, it warms up the treated region and increases blood circulation.
Neck Pain and Auto Injury
Chiropractic Recovery
Ultimately, chiropractors can help victims of whiplash in many ways. These health care providers can ensure that an individual� whiplash and its associated symptoms may subside completely. They always make sure to create a patient-specific treatment plan to make the process of recovery simpler for every individual.
Other than recommending immediate treatment for reducing the acute pain and inflammation, the chiropractor might additionally recommend a series of stretches and exercises, to help speed up the rehabilitation process as well as help increase the individual�s strength, flexibility and mobility.
Whiplash injuries, when left untreated, can cause severe complications. If you or a loved one have been involved in an automobile accident, visit a chiropractor immediately. By being prompt, you can even reduce your recovery time significantly. That�s not all; the chiropractor will also provide the required assistance to your lawyer, proving that the injury resulting from the accident wasn�t a preexisting injury or condition.
When you are injured in a car accident, you must get acquainted with your rights as soon as possible to receive the proper compensation and treatment for your specific situation. There is no such thing as a simple car crash.
Certain injuries or conditions which may have developed following an automobile accident may become chronic or permanent if left untreated. If an individual is experiencing neck stiffness or headaches after a traffic collision, it�s absolutely wrong to assume that this will subside in a few days. A minor discomfort could turn out to be a more serious complication. Often, people injured in auto accidents develop scar tissue that remains with them throughout the rest of their lives and without the necessary treatments or exercises, these can become stiff and greatly limit an individual�s ability to move properly. The above issues generating from a car accident show how important it is for people to seek immediate legal and medical help. Chiropractors are known for their expertise in managing soft tissue injuries and the resulting chronic and traumatic pain; as a result, they are often considered to be the best healthcare professionals to consult after a car accident.
Last nights Super Bowl victory by the New England Patriots was one for the record books! Tom Brady led one of the greatest comebacks in sports history lifting New England from a 25-point hole to the Patriots� fifth NFL championship in the first Super Bowl overtime.
Nothing that Tom Brady has said about chiropractic care will come as a�surprise to Dr. Michael Miller, a graduate of the prestigious Palmer College of Chiropractic, who has been the chiropractic team physician for the Patriots for the past 30 years. He works with anywhere from 30 to 40 Patriots players before each game and is available for specific injuries during the game. He has been to seven Super Bowl games with the team and is the proud possessor of three Super Bowl rings and four championship rings. Miller was the first chiropractor to work for an NFL team 30 years ago, but now every team in the NFL has at least one chiropractor on its full-time staff.
Last evening, Dr. Miller won his fifth Super Bowl ring, along with Tom Brady and the whole Patriots team, making him the only chiropractor in the world with such an extensive collection. It�s another symbol�his role on the team: an important member that contributed to the success of these elite athletes.
Dr. Michael Miller is the Team Chiropractor for the New England Patriots Super Bowl-winning football team. He has served as the Patriots� team chiropractic physician since 1982.
Miller originally went to medical school with plans to become a medical researcher. But during his training, the neurophysicists he worked with suggested that chiropractic might be a better choice�because it focuses on the cause, rather than the symptoms, of disease.
As a chiropractor, Dr. Miller specialized in sports and rehabilitation�and developed a private practice that cares for patients of all kinds, including many professional athletes. �You can be your own boss, have your own practice, and have your own independence,� comments Miller. ��I enjoy that.�
He explains that there is a difference between working with professional athletes and his �regular� patients, but the reward is there either way. �It�s a special feeling when you get recognized by your patients,� says Dr. Miller.
Chiropractic is a natural form of therapy that�s a great fit for elite athletes, who are in a sense like high-performance racing cars. They�re fast, but their bodies are also subjected to tremendous forces when they perform, both during training and competition.These athletes simply can�t rely on drugs to keep playing and most wouldn�t even if they could.
Much of Dr. Miller�s work is done pre-game, making adjustments to players� knees, shoulders, ankles, and backs to help them avoid injury. As he says, �Their job is to get banged and be tackled. They are basically getting beaten up each game. They understand the importance of a chiropractor and see how it allows them to play longer.�
Many athletes in many sports have joined Tom Brady in telling their own stories and offering their endorsements. They recognize that chiropractic care has helped them be more injury-free and kept their bodies performing more optimally, which has made them better at their sport over the course of their careers.
Chiropractors are being utilized all over our beautiful country to advance high performance athletes. Tom Brady has his favorite chiropractor always standing strong to help him when the time is right. What a proud day for those Patriots, what a proud day for chiropractic.
Contents
Additional Topics: Neck Pain and Auto Injury
After being involved in an automobile accident, the tremendous force of the impact can cause damage or injury to the body, primarily to the structures surrounding the spine. Whiplash is a common result of an auto collision, affecting the bones, muscles, tendons, ligaments and other tissues around it, causing symptoms such as neck pain. Neck pain is a common symptom after an automobile accident, which may require immediate medical attention to determine its source and follow up with the appropriate treatment.
Symptoms of neck pain that radiate to the shoulders and down the arms can be caused due to a variety of injuries and conditions, most occurring as the result of complications to the cervical spine and its surrounding structures. A subluxation, or spinal misalignment is one of the most common results of neck and back pain, however, the gradual degeneration of the spine can also create issues over time if not treated accordingly.
A cervical disc herniation is a frequent complication caused by the wear and tear of the tissues around the cervical spine, primarily a degeneration of the discs found cushioning each vertebra of the spine. This condition originates in the upper spine and can generally be referred to as a pinched nerve, ruptured disc or a herniated disc.
Contents
Anatomy of the Cervical Spine
The upper region of the spine is commonly described and identified by healthcare professionals as the cervical spine, which primarily functions to support the weight and movement of the head. The cervical spine is made up of seven vertebrae, from top to bottom, C1 through C7. Each vertebrae in the neck is separated by intervertebral discs which consist of a fibrous tissue, known as the annulus, with a soft nucleus at the center. The annulus and the nucleus that make up each disc function simultaneously to provide each vertebra of the spine to absorb the shock of every movement of the spine as well as help the pressure of these be distributed evenly, separating each vertebrae individually to allow smooth movements.
However, when the annulus of one of these intervertebral discs ruptures, the nucleus can occasionally separate from the center of the disc. If this occurs, the disc is no longer able to properly separate the vertebrae as this process alters the natural shape of the discs, which could often lead to the compression and irritation of the spinal nerves. The symptoms of pain, discomfort and numbness experienced in the neck, shoulders and arms can be closely associated with the compression and irritation of the nerves surrounding the cervical herniated disc.
Causes of Cervical Disc Herniation
The gradual degeneration of the different structures of the body which occurs naturally over time is one of the most common causes of cervical disc herniations, although, these can generally develop until a person is in his 40�s. Other causes for cervical disc herniation includes trauma from improperly lifting heavy objects, equipment or machinery or from other physical activities such as an abrupt, intense twist. Additionally, cervical spine complications may be caused due to damage or injury resulting from an automobile accident or other personal injury accident.
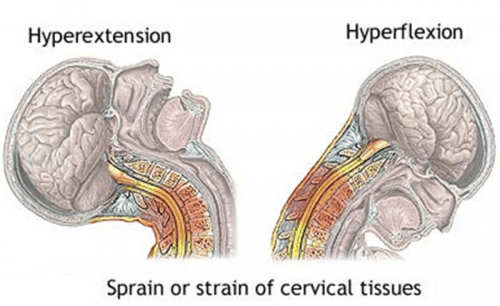
Whiplash is a common injury caused due to the sudden force of an impact, which results in the jolting, back-and-forth motion of the head and neck in any direction, most commonly due to an auto collision. During a whiplash-associated injury, the structures that surround the cervical spine, primarily the tendons, ligaments and nerves, are stretched beyond their natural limit, partially or completely tearing the tissues around the cervical spine. Furthermore, the normal alignment of the spine may be affected, causing a subluxation in the vertebrae of the neck.
As a result, the intervertebral discs found between each vertebrae can become ruptured, leading to the compression or irritation of the spinal nerves, causing symptoms of pain and discomfort, among others, associated with a cervical disc herniation.
Symptoms of Cervical Disc Herniation
Cervical disc herniation could be the cause of an individual�s painful symptoms in their neck, shoulders, and/or arms. The following symptoms could suggest the presence of a cervical disc herniation, however, it�s essential to visit a healthcare professional to receive a proper diagnosis and similar symptoms could suggest the presence of another injury or condition.
Pain, discomfort, or burning sensations originating from the neck and traveling down one or both arms;
Pain with movements of the head or neck;
Pain in the shoulder region;
Tingling or numbness in one or both arms;
Weakness in one or both arms;
Limited mobility or difficulty properly moving the neck, arms or hands;
Difficulty sleeping due to neck, shoulder and/or arm pain.
Diagnosing Cervical Disc Herniation
Your healthcare provider should be able to properly refer you to the best doctors and specialists in the region to properly diagnose your injuries and/or conditions before following through with treatment. Chiropractic care is a common, alternative treatment options that is preferred by many individuals with spine complications. Chiropractic specialized on the diagnosis and treatment of injuries and conditions associated to the musculoskeletal and nervous systems.
Foremost, when visiting a chiropractic office, the chiropractor will perform a thorough physical evaluation to determine the exact cause of the symptoms. In addition, the spine specialist may also take a closer look at the individual�s medical history, including previous test results and prior doctor visits. If necessary, the doctor of chiropractic may issue additional tests if necessary, including X-rays and MRI scans. Once the healthcare professional has concluded the diagnosis and has resolved the source of the symptoms, they will provide the patient with information regarding their injury or condition as well as cover the risks and benefits of each treatment option which may be available to the individual. The chiropractor will determine the individual�s best treatment options according to their specific type of injury or condition and depending on their severity.
Chiropractic Care for Cervical Disc Herniation
Chiropractic treatment utilizes spinal adjustments and manual manipulations to carefully restore the natural alignment of the spine, gradually re-aligning the vertebrae to reduce the pressure being applied against each structure. Chiropractic adjustments and manipulations can ultimately help decrease the compression and irritation of the spinal nerves, relieving the symptoms associated with cervical disc herniation. Subsequently, by reducing the individual�s pain and discomfort, their original strength, flexibility and mobility may also be gradually restores, helping them return to their normal lifestyles in no time.
Additionally, a chiropractor may recommend a series of stretches and exercises to speed up the rehabilitation process. Also, certain lifestyle changes may be implemented to ensure the recovery process proceeds smoothly without further issues. Physical therapy can also be an excellent treatment option to provide the patient with the necessary strength, flexibility and mobility to regain their original way of life.
In conclusion, in the instance that the individual is in need of further treatment through the use of other medical procedures, a chiropractor may refer the individual to other spine specialists that can provide other beneficial treatments and curative methods. In severe cases of cervical disc herniation, a patient may be referred to a spinal surgeon for treatment.
Chiropractic Care and Headaches
Complications affecting the cervical spine, such as a cervical disc herniation, can develop a variety of other symptoms, including headaches. Constant head pain can source from many types of issues along the upper region of the spine, commonly manifesting after an automobile accident or other form or personal injury accident. Fortunately, chiropractic treatment can help restore the original function of the structures surrounding the cervical spine, decreasing the symptoms, including headaches, improving the individual’s lifestyle.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Neck Pain and Auto Injury
After being involved in an automobile accident, the tremendous force of the impact can cause damage or injury to the body, primarily to the structures surrounding the spine. Whiplash is a common result of an auto collision, affecting the bones, muscles, tendons, ligaments and other tissues around it, causing symptoms such as neck pain. Neck pain is a common symptom after an automobile accident, which may require immediate medical attention to determine its source and follow up with the appropriate treatment.
This Sunday over 111 million people will tune into watch the SuperBowl. Behind the scenes both teams and coaches have been fine tuning their game plans as they prepare for the biggest game of their lives. As part of the players preparation there have been a few lucky individuals with direct access to care for these athletes. �Referred to as the �magic workers� by some players these men are the team Chiropractors who serve both the Seattle Seahawks and New England Patriots.
For the last 12 years, Dr. Gerry Ramogida and Dr. Jim Kurtz have had front-row seats to the spectacle of NFL games as chiropractic consultants for the Seattle Seahawks. Attending every game, �Dr. Ramogida was supposed to stay with the team for just a couple of years so he could show the trainers how to use some of his soft-tissue techniques. But as players got used to getting adjusted by him on�game days, a temporary job turned into a permanent one.
�There�s so much behind the scenes that you don�t get a sense for when you�re watching a game. It�s a massive effort. I am just happy to be a part of the preparation as these guys get ready to go out and do what they do best, compete.�
In a interview with Global News�Dr. Ramogida stated, �Over the period of that first season and into the next year, things very quickly became integrated. It�s been a great experience,� he says.
In recent news, The Professional Football Chiropractic Society (PFCS) has taken pride in announcing that all 32 teams in the National Football League offer their players and personnel chiropractic physician services as part of the triage in managing and preventing injuries. According to the Foundation for Chiropractic Progress, this distinction is a benchmark for the profession and documents the important role that chiropractic care plays in optimizing athletic performance.
�The robust need for chiropractic care in the NFL has been deeply driven by the players� desire for peak physical conditioning and not simply for injuries,� states Spencer Baron, D.C., �From the earliest years of full contact football, their bodies are subject to structural stress that doctor of Chiroprctic (DCs) are specially trained to care for. �
Attending this weekend to the New England Patriots is Dr. Mike Miller. �Over twenty five years ago he became the official chiropractor of the New England Patriots. Since that time, he�s treated hundreds of players, watched ownership of the team change hands three times, and seen the Patriots go from one of the worst franchises in the National Football League to a team readying themselves to play in the Superbowl this weekend.
In a interview with Dynamic Chiropractic Dr. Miller states that his position with the Patriots involves him being present during mini-camps, training camp, preseason games, regular-season games (both home and away), and postseason games.
During the games, I see an average of at least 40 players, coaches, and other personnel who are affiliated with the team. I would say just about 90 percent get chiropractic services, because the present coaching staff of the Patriots has almost mandated chiropractic care with the players. The coaches speak about it at team meetings, as the new players and rookies come into the team in the preseason. During mini-camps, they explain the significance of chiropractic, and that we have a chiropractor who has had phenomenal results in dealing with injuries and preventing them from occurring, and that they would like the players to proactively be treated [by] me and begin a chiropractic course of care.
During the season, if there are any injuries, they (the medical staff) will generally send the player to my office to be evaluated. By game time, just about everyone on the roster is adjusted, and you start to learn the idiosyncrasies of each player, because each one wants certain things checked on them. Some are very firm with extremity adjusting; others enjoy use of a specialized technique that we use, called Graston Technique. Basically, it takes me about four hours before the game to go through the entire roster.
The NFL has just released a statement advocating for�all NFL teams as now employing a Chiropractor as part of their medical staff.
If you are interested in learning more about how to be an NFL Chiropractor you can connect with the Professional Football Chiropractic Association�on their website or on their Facebook page.
No matter what the outcome of this weekends game may be, rest assured that both teams will have been well adjusted and their nervous systems tuned on and ready to perform on the biggest stage of all.
Behind the bright lights of the stadium, there is another team that keeps these players and their performance at their optimal level. The healers�if you will, that audiences don’t see, but should know about. These are the Chiropractors!
Super Bowl LI kicks-off with a team of doctors of chiropractic (DC)�to help these professional athletes prevent, manage and care for injuries, as well as, achieve peak performance. The Foundation for Chiropractic Progress� (F4CP), the leading voice of the chiropractic profession, points to the role of DCs with all four play-off teams,and cites data from the Professional Football Chiropractic Society (PFCS) showing on average, a professional football DC performs between 30 to 50 weekly treatments during the regular season � not including training camp or the playoffs.
F4CP� celebrates Super Bowl LI with NFL doctors of chiropractic
New England Patriots Team Chiropractor of 35+ years and proud to attend his ninth Super Bowl, Dr. Michael Miller, states, �During the NFL season, I regularly visit the stadium on my afternoon off from my office, as well as on game days both at home and away. Chiropractic care is emphasized by the head coach, trainers and medical staff as a proactive regimen to prevent injuries, with most of the players receiving adjustments roughly 1-2 times per week.�
He adds that chiropractic care has proven itself over the years in the sports injury arena to be well-accepted as the choice of champions and an integral part of any injury prevention program. �We�ve also earned the respect of other team physicians as a necessary protocol, and are all committed to one goal: keeping the athletes performing at their maximum potential and preventing and managing injuries as they occur.�
He says that chiropractic care provides the athletes with the confidence they need to play without the distraction of pain. �The players are educated about the principles of chiropractic and that it is designed to eliminate the cause of their problem rather than just masking their symptoms.�
Joseph Krzemien, DC, team chiropractor, Atlanta Falcons, says that there is growing evidence and a correlation between football players who receive consistent chiropractic care and a decline in injuries during practice or play:
�During the six seasons I�ve spent with the Atlanta Falcons, my goal has always been to prepare each player�s body to better resist trauma and to speed its natural recovery time,� he says. �This season, the Falcons have been successful for a lot of reasons, but I firmly believe that regular chiropractic care has played an important role in helping us stay healthy and get to Super Bowl LI � I am proud of the role I�ve played in their success.�
For Michael Zoelle, DC, team chiropractor, Green Bay Packers, the trauma experienced by the athletes� bodies during a game is very similar to that of a car accident.
�Ensuring that the joints are functioning properly is critical in the healing process, as well as for injury prevention and optimal performance,� says Dr. Zoelle. �The players recognize that chiropractic care helps them to perform better and heal faster, ultimately leading to better team success.�
DCs receive a minimum of seven years of higher level education, and are qualified to diagnose, treat and manage a broad spectrum of health conditions. They are the primary care professionals for spinal health and well-being. For athletes, chiropractic care helps to reduce the risk of injuries and improve health and performance through enhancements in range of motion, flexibility, balance, muscle strength and other key factors.
On every sideline all over the NFL and NCAA game you will now see chiropractors fixing and maintaining their local teams. In our very own back yard, you will see chiropractors treating El Paso’s finest at most high school games. �UTEP now has Dr. Paul Munoz standing tall ready to help our kids perform better. �The story is getting better each and every year how the public understands joint health as to how it applies to peak performance. �This last Olympics we saw Usain Bolt getting tuned just before his record breaking run. �The day of ushering in alternative care for high performance has for sure landed. �The spine was created to propel the creature faster and to transmit power. �No surprise that most sports have embraced the science and art. �Proud to be a part of the movement…..
Super Bowl 50 showcased the leading players in the NFL along with Joshua Kollmann, DC and Brad Wiest, DC � chiropractors for the Carolina Panthers � and Shawn Caldwell, DC for the Denver Broncos. These doctors of chiropractic helped the players achieve optimal performance.
The Foundation for Chiropractic Progress (F4CP), a not-for-profit organization dedicated to raising awareness about the value of chiropractic care, points out that all 32 NFL teams include the professional services of a doctor of chiropractic (DC) as part of their integrated health care team approach.
Marking their fifth year with the Carolina Panthers, Drs. Kollmann (pic. left) and Wiest (pic. right) highlight the integrative role of chiropractic care: �We are in the stadium training room twice a week � and more often during play-offs � addressing specific sports injuries or providing preventive, maintenance care that the athletes want in order to achieve peak performance. Every player is individually assessed and the treatment plan is communicated and discussed with the training staff. Since the physical nature of the sport really impacts body structure, many players look forward to their pre- and post-game spinal and extremity adjustments as well as other advanced approaches.�
Shawn Caldwell, DC, who has served the Denver Broncos since 2004 and is now preparing for his second Super Bowl, says, �I work hand-in-hand with the athletic trainers and focus on performing chiropractic spine and extremity adjustments that restore joint function. The goal is to enable players to perform optimally or heal from injuries. I am at the facility two-three times weekly or more if necessary. Some players get an adjustment every time I am in the training room, while others when they are symptomatic so they can return to the playing field.�
According to Kyle Prusso, DC, team chiropractor for the Oakland Raiders since 2005 and president of Pro Football Chiropractic Society, an organization of chiropractors who provide the highest quality chiropractic health care to the elite athletes of professional Football: �It�s great to see chiropractic care integrated in all facets of health care, especially in professional and amateur sports. One of the reasons is that athletes are asking for us, with increased player requests driving utilization of chiropractic across all sports. Athletes are very in tune with their bodies and recognize that chiropractic care can boost optimal performance levels.�
All doctors are passionate about their roles as team chiropractors to an NFL Super Bowl contender, as Dr. Kollmann says, �I am humbled by this position and want the world to know that this is a great time to be a chiropractor. It means the world to me to ignite and advance our profession � especially for those who are pursuing a chiropractic education as well as veteran professionals. We are igniting the profession and honor those DCs who pioneered the opportunities that have helped us to become a part of the NFL teams.�
Dr. Caldwell, who is also the chiropractor for the Colorado Rockies Major League Baseball team, sums it up, �Chiropractors are playing an important role in the health care and performance of professional athletes. This is a fantastic experience for us and for the players.�
Doctors of chiropractic receive a minimum of seven years of higher level education, and are qualified to diagnose, treat and manage a broad spectrum of health conditions. They are the primary care professionals for spinal health and well-being. For athletes, chiropractic care helps to reduce the risk of injuries, and improve health and performance through enhancements in range of motion, flexibility, balance, muscle strength and other key factors.
If you are interested in learning more about how to be an NFL Chiropractor you can connect with the Professional Football Chiropractic Association on their website or on their Facebook page.
No matter what the outcome of this weekends game may be, rest assured that both teams will have been well adjusted and their nervous systems tuned on and ready to perform on the biggest stage of all.
Chiropractors swarm the field! Ready for some adjustments to help these players perform their best. The Foundation for Chiropractic Progress (F4CP), a non-profit organization dedicated to raising awareness about the value of chiropractic care share the fact that all 32 NFL teams utilize doctors of chiropractic (DC), as part of their health care programs.
From runners to many other types of athletes, experiencing an accident that results in damage or injury, or developing a previous condition is not uncommon among athletes. Subsequently, a majority of athletes practice preventive measures or they stretch and exercise accordingly before performing in their specific sport or physical activity to avoid any injuries which could remove them from training or competition. Heel pain is among one of the most frequent symptoms athletes report from their sessions, especially since the feet are practically essential in most sports and physical activities.
Plantar heel pain is frequently diagnosed by healthcare professionals, including chiropractors and sports clinicians, often recorded due to mechanical, neurologic, traumatic or other systemic conditions. Without a doubt, plantar fasciitis is the most common pathology among sporting environments. However, other causes of heel pain may be previously considered when evaluating an athlete with heel pain.
Up to 2 million Americans describe symptoms of heel pain every year, accounting for an estimate of up to $400 million in medical bills. Regardless, not much is known about the pathophysiology and etiology of plantar heel pain. By emphasizing on the causes of plantar fasciitis as well as discussing other common mechanical issues behind heel pain, including plantar fascia tears/rupture, heel pain of neural origin, calcaneal stress fractures and atrophy of the heel pad, individuals can learn to understand the diagnostic criteria and possible treatment options of plantar heel pain.
Dr. Alex Jimenez D.C.,C.C.S.T’s insight:
Maintaining an athlete’s overall health and wellness is essential in order to prevent them from missing out on training or competition. However, when an injury or condition affecting the heel occurs, such as plantar fasciitis, chiropractic care can be a safe and effective alternative form of treatment to relieve the symptoms of pain and discomfort the athlete may have. For more information, please feel free to ask Dr. Jimenez or contact us at (915) 850-0900.�
It’s not uncommon for athletes to suffer damage or injury as a result of an accident while on the field, occasionally developing or aggravating a previous condition in the process, which can affect their performance. Sports or physical activities requiring rigorous training and performance during competitive have a higher risk of injury among athletes. Knee injuries are some of the most common complications affecting numerous athletes throughout their career, most frequently hyperextension knee injuries caused during contact sports.
Hyperextension knee injuries can vary from acute to chronic and these are generally painful. The infrapatellar fat pad, abbreviated as IPFP, is one of the most frequently affected structures due to hyperextension knee injuries. In the presence of an acute knee hyperextension injury, for instance, when an athlete is tackled in rugby, the posterior cruciate ligament, or PCL and/or the posterior lateral corner, or PLC, of the knee may suffer injury.
Dr. Alex Jimenez D.C.,C.C.S.T’s insight:
Knee complications can occur due to a variety of factors, such as an accident, however, these types of issues are most commonly the result of sports injuries. During specific sports or physical activities, wear and tear of the tissues is the most common reason knee injuries occur, however, a hyperextension knee injury may also frequently develop. For more information, please feel free to ask Dr. Jimenez or contact us at (915) 850-0900.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Head Posture While Walking
Head Posture While Walking









 he could show the trainers how to use some of his soft-tissue techniques. But as players got used to getting adjusted by him on�game days, a temporary job turned into a permanent one.
he could show the trainers how to use some of his soft-tissue techniques. But as players got used to getting adjusted by him on�game days, a temporary job turned into a permanent one.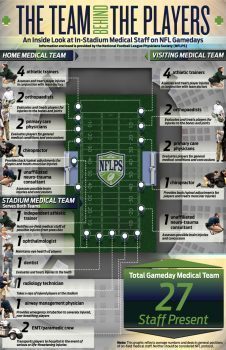
 In a interview with Dynamic Chiropractic Dr. Miller states that his position with the Patriots involves him being present during mini-camps, training camp, preseason games, regular-season games (both home and away), and postseason games.
In a interview with Dynamic Chiropractic Dr. Miller states that his position with the Patriots involves him being present during mini-camps, training camp, preseason games, regular-season games (both home and away), and postseason games.
 Joseph Krzemien, DC, team chiropractor, Atlanta Falcons, says that there is growing evidence and a correlation between football players who receive consistent chiropractic care and a decline in injuries during practice or play:
Joseph Krzemien, DC, team chiropractor, Atlanta Falcons, says that there is growing evidence and a correlation between football players who receive consistent chiropractic care and a decline in injuries during practice or play:
 Marking their fifth year with the Carolina Panthers, Drs. Kollmann (pic. left) and Wiest (pic. right) highlight the integrative role of chiropractic care: �We are in the stadium training room twice a week � and more often during play-offs � addressing specific sports injuries or providing preventive,
Marking their fifth year with the Carolina Panthers, Drs. Kollmann (pic. left) and Wiest (pic. right) highlight the integrative role of chiropractic care: �We are in the stadium training room twice a week � and more often during play-offs � addressing specific sports injuries or providing preventive,  maintenance care that the athletes want in order to achieve peak performance. Every player is individually assessed and the treatment plan is communicated and discussed with the training staff. Since the physical nature of the sport really impacts body structure, many players look forward to their pre- and post-game spinal and extremity adjustments as well as other advanced approaches.�
maintenance care that the athletes want in order to achieve peak performance. Every player is individually assessed and the treatment plan is communicated and discussed with the training staff. Since the physical nature of the sport really impacts body structure, many players look forward to their pre- and post-game spinal and extremity adjustments as well as other advanced approaches.� Shawn Caldwell, DC, who has served the Denver Broncos since 2004 and is now preparing for his second Super Bowl, says, �I work hand-in-hand with the athletic trainers and focus on performing chiropractic spine and extremity adjustments that restore joint function. The goal is to enable players to perform optimally or heal from injuries. I am at the facility two-three times weekly or more if necessary. Some players get an adjustment every time I am in the training room, while others when they are symptomatic so they can return to the playing field.�
Shawn Caldwell, DC, who has served the Denver Broncos since 2004 and is now preparing for his second Super Bowl, says, �I work hand-in-hand with the athletic trainers and focus on performing chiropractic spine and extremity adjustments that restore joint function. The goal is to enable players to perform optimally or heal from injuries. I am at the facility two-three times weekly or more if necessary. Some players get an adjustment every time I am in the training room, while others when they are symptomatic so they can return to the playing field.�