Since its establishment five months ago, the new in-house fraud unit at the Division of Workers� Compensation has opened more than 40 investigations and hired additional fraud investigators to extend its reach.
�It�s a huge benefit to have a fraud unit that is 100 percent dedicated to workers� compensation,� said Commissioner of Workers� Compensation Ryan Brannan. �In-house investigators are more exposed to workers� compensation issues, so they are aware of the latest schemes.�
Teresa Carney, DWC�s Director of System Monitoring and Oversight, said that in an effort to coordinate anti-fraud efforts, the unit reaches out to insurance carriers, district attorneys, fraud prevention groups, and DWC employees.
�We can�t do it alone,� she said. �Workers� compensation fraud impacts all Texans, and we want to work with people who want to help stop workers� compensation fraud. Many complaints come from injured employees or insurance carriers, but we can also be proactive by reviewing the claim or medical billing data already on hand or tap people in our Hearings Division or maybe a field office, who help in the workers� compensation system every day.�
The fraud team was set up in May and has already issued warning and education letters as well as referred a case for prosecution. In one recent case, a Houston health clinic owner entered a guilty plea and was sentenced to seven years deferred adjudication and ordered to pay $88,000 in restitution.
Carney says that while the fraud unit does catch and punish bad actors, it�s important to remember there�s a lot of good in the workers� compensation system as well.
�When you are looking for fraud, you only see a small part of the workers� compensation system,� she said. �We know there�s also lots of good stuff happening�when people get their workers compensation benefits on time, they get back to work, everyone is happy. We like to think our work helps the system work better and that leads to more of the good stories.�
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Additional Topics: What is Chiropractic?
Chiropractic care is an well-known, alternative treatment option utilized to prevent, diagnose and treat a variety of injuries and conditions associated with the spine, primarily subluxations or spinal misalignments. Chiropractic focuses on restoring and maintaining the overall health and wellness of the musculoskeletal and nervous systems. Through the use of spinal adjustments and manual manipulations, a chiropractor, or doctor of chiropractic, can carefully re-align the spine, improving a patient�s strength, mobility and flexibility.
A research study published in the Journal of the American Medical Association in September 2015 demonstrated that nearly 50 percent of adults in the United States may have pre-diabetes or diabetes.
Approximately 9 out of 10 people may have undiagnosed pre-diabetes while 1 out of every 4 people may have undiagnosed diabetes. Statistics from the Center for Disease Control also revealed that about 30 percent of all individuals with pre-diabetes will develop type 2 diabetes within 5 years.
While these statistics have become dangerously alarming in the United States, the increasing issue of pre-diabetes and diabetes cases in adults has been growing throughout the world. Over the last decade, for instance, Great Britain has seen a drastic rise in both pre-diabetes and diabetes cases as well. According to a BBC News report, approximately more than one-third of British adults have been diagnosed with pre-diabetes, as compared to a 2003 report, where only 11.6 percent of British adults had been diagnosed with pre-diabetes. By 2011, the amount of individuals diagnosed with the conditions had almost tripled to about 35.3 percent.
Pre-diabetes is medically characterized as having a fasting blood sugar of 100-125 mg/dl or a hemoglobin A1C of 5.7-6.4 percent. Researchers medically defined diabetes as having a fasting blood sugar greater than 126 mg/dl or a hemoglobin A1C > 6.5 percent, a measure of long term glucose control.
Contents
Health Complications Related to Diabetes
A majority of the complications associated with pre-diabetes and diabetes can develop gradually over time. Individual�s who�ve had the condition for an extended period of time, and who also maintain less control of their blood sugar levels, may have a higher risk of suffering other complications commonly associated with type 2 diabetes. If these issues are not treated accordingly, they could eventually lead to disabling or even life-threatening complications.
Common complications associated with pre-diabetes and diabetes include:
Skin and tissue infections: Damage to blood vessels and nerves can affect the proper circulation and blood flow to the skin. This can result in the death of skin cells which may lead to a variety of changes in the skin as well as in other important structures of the body.
Foot damage: The Improper blood flow and circulation as well as damage to the nerves in the feet can increase the risk of experiencing a variety of foot issues. If left untreated, these foot complications, such as cuts and blisters, can develop into serious infections which can often heal poorly. Severe infections may ultimately require toe, foot or leg amputations.
Eye damage or retinopathy: Diabetes can damage the blood vessels of the retina which can potentially lead to blindness. This complication of the condition also increases the risk of other serious vision conditions, such as the development of cataracts and glaucoma.
Kidney damage or nephropathy: The kidneys are made up of millions of tiny blood vessel clusters, known as glomeruli, which function by filtering waste from the blood. Type 2 diabetes can damage these blood vessel clusters, affecting their normal function to properly filter the blood. Severe damage to the glomeruli can lead to kidney disease or kidney failure which may require dialysis or a kidney transplant.
Peripheral neuropathy or nerve damage: Increased blood sugar levels can injure the walls of the capillaries, tiny blood vessels which nourish the nerves, particularly those found in the legs. Peripheral neuropathy can cause pain, tingling and burning sensations and numbness along the upper and lower extremities. If this type of nerve damage is left untreated, the symptoms mentioned above may worsen, resulting in loss of strength and balance as well as the complete loss of feeling in the affected limbs. A majority of people with advanced stages of peripheral neuropathy experience chronic symptoms of pain and they may be unable to walk without the help of a cane or walker. Some people may need to use a wheelchair. Nerve damage can also affect the nerves of the digestive system, causing nausea, vomiting, diarrhea or constipation. For men, peripheral neuropathy may lead to erectile dysfunction.
Cardiovascular disease: Pre-diabetes and diabetes also dramatically increases the risk of developing a variety of cardiovascular problems, including coronary artery disease with chest pain or angina, heart attack, stroke and narrowing of arteries, or atherosclerosis. Individuals with diabetes are more likely to experience heart disease or stroke.
Hearing impairment: Individuals with diabetes have double the risk of experiencing hearing loss and other auditory complications than adults without the condition.
Alzheimer�s disease: According to various research studies, type 2 diabetes has been linked to the development of Vascular Dementia and Alzheimer�s disease.
Risk Factors Leading to Diabetes
Pre-diabetes and type 2 diabetes can develop due to a variety of risk factors. Knowing these factors can help individuals be more aware of their chances of developing the condition in order to help them take the necessary precautions to prevent diabetes from developing.
Several risk factors contributing to pre-diabetes and diabetes include:
Weight: Excess weight and obesity can cause the development of insulin resistance, one of the most common reasons behind pre-diabetes and diabetes in adults.
Inactivity: Sedentary individuals who engage in less exercise and physical activity can be at greater risk of developing the condition. Physical activity and exercise helps control weight, utilizes glucose as energy and improves insulin sensitivity.
Family history: A person�s risk of developing pre-diabetes or diabetes can increase if a parent or sibling has the condition. Although Type 2 Diabetes is not hereditary, it can develop due to lifestyle habits. Your family history can help predict the probability of developing diabetes.
Race: Research published in JAMA revealed that African-Americans, Hispanics, American Indians and Asian-Americans are at higher risk for developing Type 2 Diabetes.
Age: The risk of developing pre-diabetes and diabetes does increase with age. This is generally believed to be due to inactivity associated with aging, loss of muscle mass and weight gain. However, pre-diabetes and diabetes has also dramatically increased among children, adolescents and younger adults over the past several years.
Gestational diabetes: A woman who developed gestational diabetes while pregnant, may have an increased risk of developing pre-diabetes and type 2 diabetes. If you gave birth to a baby weighing more than 9 pounds, 4 kilograms, you may also be at risk of developing diabetes.
Polycystic ovary syndrome or PCOS: For women, having polycystic ovary syndrome, a common condition characterized by irregular menstrual periods, excess hair growth and obesity, can also increase the risk of developing diabetes.
High blood pressure: Having blood pressure of over 140/90 mm Hg, or millimeters of mercury, has been associated to an increased risk of type 2 diabetes.
High cholesterol and triglyceride levels: Individuals with low levels of high-density lipoprotein, HDL or good cholesterol, their risk of developing pre-diabetes or diabetes is generally higher. Triglycerides are another type of fat carried in the blood. People with high levels of triglycerides can be at risk of developing type 2 diabetes. Consulting a doctor at this point is important as they can inform you on what your cholesterol and triglyceride levels are.
Preventing Diabetes
Diabetes has become one of the most common diseases of the 21st century, most of which can lead to peripheral neuropathy. Although there are many factors behind this type of nerve damage, such as the use of medications and drugs, approximately 66 percent of all people with diabetes will develop peripheral neuropathy over time.
Fortunately, you can avoid developing pre-diabetes, diabetes and ultimately, peripheral neuropathy, by making some simple lifestyle changes. While changing the regular diet you are used to can be challenging, taking such a task slowly can help ease the daunting change. For instance, you can try changing one thing about your diet today. Whether it involves giving up soda or skipping sweets after dinner, this small change can be effortless for many. Now try doing this for 30 days. It will be difficult at first but it will get progressively easier.
For people who already developed diabetes as well as some of the common complications associated with the condition, keep in mind that both type 2 diabetes and peripheral neuropathy can be reversed with the right lifestyle changes as well. By addressing your diet and other lifestyle habits, such as the amount of exercise you participate in and how much sleep you get, the condition and its complications can be tremendously improved. In one 10-year long study of 70,000 diabetes-free women, researchers found that women who either slept less than five hours a night or more than nine hours each night were 34 percent more likely to develop diabetes than women who slept seven to eight hours each night.
In addition, getting the appropriate amount of vitamin D on a daily basis can also help improve diabetes. Evidence demonstrated that vitamin D can be extremely beneficial for both type 1 and type 2 diabetes. Taking vitamin D supplements if you�re not spending the necessary amount of time out in the sun can in turn help provide the required nutrients and minerals.
In conclusion, diabetes is considered to be one of the most prevalent conditions today, where nearly up to 50 percent of people have been diagnosed with type 2 diabetes. Many factors can often increase the risk of developing the condition but diabetes can be prevented as well as reversed. If you�ve been diagnosed with diabetes or you suspect you may have the condition, make sure to seek professional care to receive proper diagnosis and treatment.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: What is Chiropractic?
Chiropractic care is an well-known, alternative treatment option utilized to prevent, diagnose and treat a variety of injuries and conditions associated with the spine, primarily subluxations or spinal misalignments. Chiropractic focuses on restoring and maintaining the overall health and wellness of the musculoskeletal and nervous systems. Through the use of spinal adjustments and manual manipulations, a chiropractor, or doctor of chiropractic, can carefully re-align the spine, improving a patient’s strength, mobility and flexibility.
Sweet foods were a rare delicacy for our ancient ancestors.� Today, we have an unlimited supply of sugary foods and beverages at our disposal.� Natural sweeteners can be used effectively in moderation to provide the sweetness that most people crave.� Here are the best natural sweeteners ranked in order based on low glycemic index and additional health benefits.
Every living creature is designed to run off of a simple sugar called glucose.� It is the primary unit in the study of metabolism.� However, there are certainly dangers involved with consuming too much glucose. Those dangers mostly involve elevated blood sugar and insulin which trigger fat accumulation, cellular inflammation and insulin resistance.
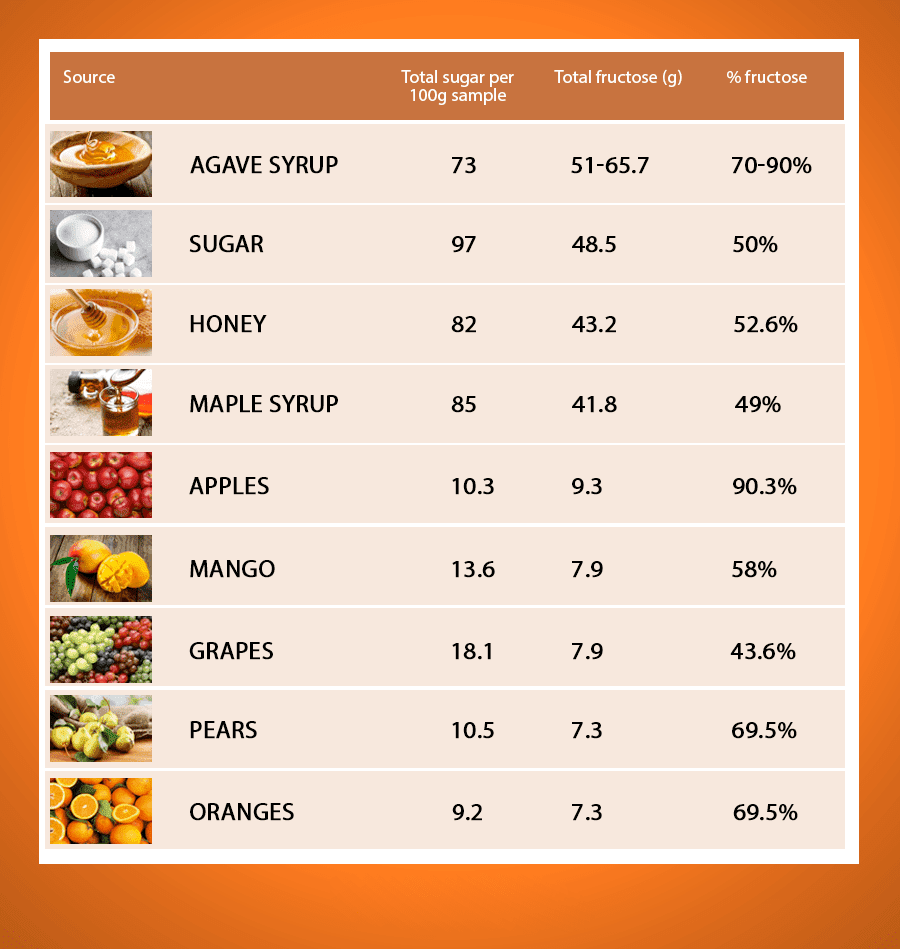
Fructose is another simple sugar that is found in nature within fruits, honey and plant/tree nectar.� This is metabolized differently than glucose and can cause even more hazardous effects when consumed in excess.� Most plant based sweeteners such as agave nectar are extremely high in fructose.� Agave was thought to be a good sweetener until health researchers found out the dangers of it�s nearly 80% fructose content.
Contents
1. Stevia:
Processed from the leaf of the stevia plant which is native to South America.� This herb derivative has no effect on blood sugar, insulin signaling and triglyceride formation.�� It develops most of its sweetness from glycosides called stevioside and rebaudioside.� �These compounds are 250-300 times sweeter than sucrose and they have the ability to withstand heat and have a long shelf life (1, 2).
Studies have even shown the stevia leaf to have beneficial effects at improving cellular insulin sensitivity and reduce the risk of type II diabetes and high blood pressure (3, 4). �My favorite stevia to use personally is Sweet Leaf stevia in the liquid dropper here� I like this brand because it is pure stevia, without any sugar alcohols or other sweeteners added. � Most people also like the flavor better as it has less of an aftertaste.
You can find it in a variety of flavors including vanilla, chocolate, hazelnut, cinnamon, English toffee, grape�and lemon. �If you are noticing an unpleasant aftertaste with the Sweet Leaf brand, than try adding a little bit of sea salt or pink salt (to taste � not too salty) to your recipe using the stevia and this can help remove the after taste. �I have seen a lot of people who once �hated� stevia, completely change their opinion after adding the salt.
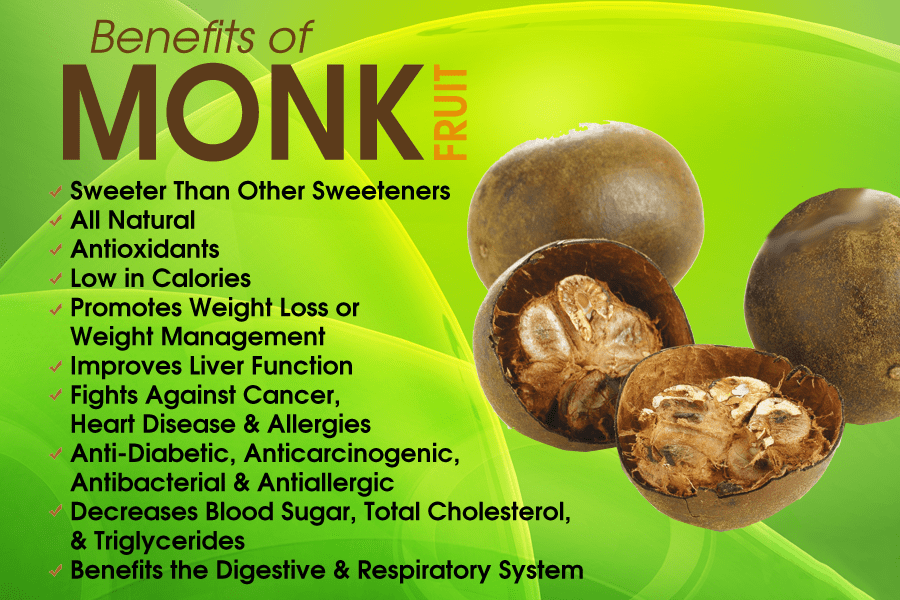
2. �Monk Fruit or Lo Han Extract:
Lo Han Extract is also called monk fruit. �The monk fruit plant grows native in Southern China/Northern Thailand.� Lo Han has a very low glycemic index and low sugar content.� It gets the majority of its sweetness from a glycoside nutrient called mogrosides.
These mogrosides are 300 times sweeter than sugar and act as anti-oxidants that have shown abilities to inhibit cancer cell formation (5, 6).� This is a wonderful sweetener but it can be hard to find and expensive. �I like Pure Monk Fruit from Julian Bakery because it is the only one I found without other sweeteners such as erythritol.
3. �Yacon Syrup:
Yacon syrup is extracted from the roots of the Yacon plant which�grows throughout the Andes mountains in South America. �This plant has a long history as a powerful food that has been eaten and used for medicinal purposes in South America.
Yacon syrup is rich in prebiotic fibers (roughly 40-50%) called inulin and fructooligosacchardes (FOS) which are undigestable by the body but feed healthy gut bacteria (7). � Yacon does contain a small amount of sugar through fructose, glucose and sucrose but the rich fiber within it makes it a very low-glycemic sweetener. � The use of Yacon syrup has been shown to reduce obesity and insulin resistance (8).
This is a very low glycemic liquid sweetener derived from the liquid sap of the coconut blossoms. �It is also called coconut sugar. �The glycemic index is 35 making it one of the lowest of natural sweeteners.
Also, the fructose levels are very low at 10% and it contains a wide variety of anti-oxidants, minerals and other nutrients that enhance blood sugar stability.� It can be found in health food stores but is somewhat pricey. �Although I really don�t use coconut nectar or coconut sugar, one of the better brands is Coconut Secret here
5. �Organic, Raw Honey:
This superfood does have an effect on blood sugar and contains approximately 53% fructose so one should only consume this in moderation.� Honey contains a wide array of trace minerals such as calcium, iron, zinc, potassium, phosphorous, magnesium, copper, chromium, manganese and selenium.� These nutrients are critical for healthy cellular insulin sensitivity and blood sugar balance.
Raw honey is also extremely rich in anti-oxidants and natural enzymes.�� Honey contains flavonoid anti-oxidants such as pinocembrin and pinostrobin that help reduce oxidative stress in the body and promote better enzyme activity (9). �Finding local raw honey is the best as it contains small amounts of local flower pollen which enhances our bodies ability to adapt to this potential allergen.
It is best to find a local producer so you can get the best locally developed raw honey. �If you cannot find a honey producer in your area, than I would use HoneyTrees here
6. �Organic Blackstrap Molasses:
Molasses is a byproduct of the processing of sugar.� It does have an effect on glycemic index and must only be consumed in moderation.� Blackstrap molasses is a very rich source of iron, copper, manganese, potassium, magnesium and selenium.
This syrup is a dark sap from the xylem of maple trees.� It does contain sucrose, glucose & fructose and therefore has an effect on blood sugar and insulin levels.� Please use in moderation.� Maple syrup contains significant amounts of zinc, calcium, manganese and anti-oxidant phenol vanillin.
One of the better brands on the market is Crown Maple organic maple syrup here
8. Sugar Alcohols:
These include xylitol, glycerol, sorbitol, maltitol, mannitol, and erythritol.� Sugar alcohol is supposed to just pass through the body unrecognized and metabolized. �This causes no blood sugar imbalances and is considered a safe sweetener.� However, many individuals have reported significant gastrointestinal distress that includes cramping, bloating, gas & diarrhea (10).
There are many blends of stevia-erythritol and monk fruit with erythritol. �If you are noticing unpleasant digestive symptoms with these�it is more than likely the sugar alcohols that are causing it. �So be on the lookout.
If you are purchasing erythritol, look for one labeled non-GMO, since this is a corn derived product. �If you have a corn sensitivity, be sure to avoid it. �A good brand is NOW Foods erythritol here�and Xylitol
Sugar Detox Free PDF
What Does Dr Jockers Do:
I personally use stevia as my main sweetener. �I prefer the SweetLeaf brand�here�or the Pure Monk fruit.� I am not against using these other sweeteners as we have many of them in our recipes on DrJockers.com, but I would caution to use them in moderation.
We all love a sweet taste but overconsuming them can lead to increased sugar cravings and blood sugar dysregulation. �Be sure to follow the strategies I discuss in this article�on buffering blood sugar naturally. �I also have a complete program designed to help you overcome sugar cravings, lose weight and improve your energy and mental clarity. �It is called the Sugar Detox Program and you can check it out here
Call Today!
Sources for this Article Include:
W�lwer-Rieck U. The leaves of Stevia rebaudiana (Bertoni), their constituents and the analyses thereof: a review. J Agric Food Chem. 2012 Feb 1;60(4):886-95. PMID: 22250765
Brahmachari G, Mandal LC, Roy R, Mondal S, Brahmachari AK. Stevioside and related compounds � molecules of pharmaceutical promise: a critical overview. Arch Pharm (Weinheim). 2011 Jan;344(1):5-19. PMID: 21213347
Shivanna N, Naika M, Khanum F, Kaul VK. Antioxidant, anti-diabetic and renal protective properties of Stevia rebaudiana. J Diabetes Complications. 2013 Mar-Apr;27(2):103-13. PMID: 23140911
Ferri LA, Alves-Do-Prado W, Yamada SS, Gazola S, Batista MR, Bazotte RB. Investigation of the antihypertensive effect of oral crude stevioside in patients with mild essential hypertension. Phytother Res. 2006 Sep;20(9):732-6. PMID: 16775813
Xu Q, Chen SY, Deng LD, Feng LP, Huang LZ, Yu RR.Antioxidant effect of mogrosides against oxidative stress induced by palmitic acid in mouse insulinoma NIT-1 cells. Braz J Med Biol Res. 2013 Nov 18;46(11):949-955. PMID: 24270904
Takasaki M, Konoshima T, Murata Y, Sugiura M, Nishino H, Tokuda H, Matsumoto K, Kasai R, Yamasaki K. Anticarcinogenic activity of natural sweeteners, cucurbitane glycosides, from Momordica grosvenori. Cancer Lett. 2003 Jul 30;198(1):37-42. PMID: 12893428
Restaurants are the number-one place to sabotage your diet, according to new research that will surprise no one who�s ever tried to lose weight while eating out.
The year-long study, which was presented at a recent meeting of the American Heart Association, offers insight into tempting foods and the behaviors they trigger. By using a smartphone app, researchers followed 150 overweight people who were trying to stick to a weight-loss plan throughout their daily lives. The people in the study, most of whom were women, checked in up to five times a day and reported where they were, who they were with and whether they had strayed from their eating plan (or were tempted to do so.)
The dieters were also asked to log in anytime they ate (or considered eating) foods or portion sizes they knew were inconsistent with their plan.
Some clear patterns emerged from this deluge of data. People reported the most temptations when they were in a restaurant or bar, or when they were in the presence of other people eating. They noted fewer desires to overeat at home or work, and even fewer when they were in their car or in other people�s homes.
People had about a 60% chance of succumbing to those temptations at restaurants and when they were around others who were eating. Their odds of lapsing at work or in the car were lower, about 40% and 30%, respectively.
�You might think that everybody knows they�re at higher risk when they go into a restaurant, but people go out into these toxic environments and they forget,� says lead author Lora Burke, professor of nursing at the University of Pittsburgh.
People may also see eating out as an excuse to take a break from their diet, she adds. �We remind people that it�s not a diet they can go on and off; it�s a lifestyle,� she says. �It�s okay if they want to go out Friday night and eat wings, but then they need to cut back on Thursday and Saturday.�
Eating at home was a safer bet, though not a foolproof one. People reported fewer food temptations in their homes and those of their friends than they did in restaurants. But when those temptations appeared, people gave in nearly 65% of the time. Even when they were completely alone, people were still likely to lapse about half the time.
Burke says there aren�t yet any commercially available smartphone apps that collect and analyze this type of data for the general public. But such a tool could be valuable for helping people learn and adapt to their diet-related weaknesses, she adds.
�We can go to an individual and say, �These are the high-risk situations you�re vulnerable to, so you need to keep your guard up and practice strategies for sticking with your plan,�� she says. �We could even intervene by sending a message right back to them when they need it, reminding them of why they may need to work really hard.�
Measuring diet in the moment may also provide researchers with data that�s more detailed and accurate. �When we ask people to recall what they ate and how they felt, there are a lot of biases and problems remembering,� says Burke. �This way, we can be there as people are going through weight-loss challenges and find out exactly what they�re feeling, and when.�
To get better balance, power and agility, kickboxing is king among workouts. Experts who have studied the sport say nearly everyone—even older people who might shy away from such things—can benefit from throwing a punch.
Unlike most other types of exercise, kickboxing emphasizes powerful movements. Power is different from strength, and for older adults, it’s an even better predictor of mobility and their risk for falls, says Kurt Jackson, an associate professor of neurology and rehab science at the University of Dayton in Ohio. “Pure strength is what a weightlifter uses, but producing power is about both force and speed,” he says.
Kickboxing training tends to involve shorts bouts, two to three minutes long, of intense, repetitive movement—like hitting a punching bag over and over again and kicking and kneeing a pad someone else is holding. “If you look at the research on high-intensity interval training [HIIT], you see these short, intense periods of activity can have big benefits,” he says. Some research shows that even very brief stretches—just 60 seconds—of HIIT can offer the same gains in heart and lung health as 45 minutes of less-intense exercise.
Kickboxing has been shown to improve fitness, power, flexibility and agility, according to a study of healthy men in their twenties who trained three days a week for five weeks. The men in the study improved their upper and lower body power by about 7%, while shaving off more than a second from their time in a 50-meter dash.
It also torches a lot of calories. One study from the American Council on Exercise (ACE) found that the kind of punching-and-kicking combinations used in Tae Bo or “cardio kickboxing” classes burn more than eight calories per minute—about the same amount you’d burn while swimming.
The sport can also improve coordination, even in the most extreme cases. Jackson studies the neuromuscular benefits of kickboxing training for people with multiple sclerosis (MS), a condition in which poor communication between the brain and muscles can lead to falls or problems with activities that rely on multitasking, like walking and talking. Kickboxing helps strengthen neuromuscular control in people with the disease in ways that improve balance, mobility and dual-tasking activities, he found.
The benefits likely apply to older adults as well. Kickboxing improves both types of balance that the body requires—anticipatory and reactive—and better balance reduces risk of falls or muscle weakness. “Anticipatory balance is something you use when you can see a need coming, like when you’re stabilizing yourself to reach up into a cupboard,” Jackson says. Reactive balance is the type of mind-muscle coordination you need to catch your balance when you trip, or when life throws some unexpected object your way.
Those skills are useful before you hit old age. If your workout routine relies on lifting weights, running or yoga, your neuromuscular system may not be tuned to handle the kind of dynamic motion required for sports—even the ones you do just a few times a year, like skiing or pickup basketball. “You see these people step or twist wrong and suffer major tears,” Jackson says. “Kickboxing training is a great way to avoid those types of injuries.”
However, the swift whole-body movements required in kickboxing could also cause injuries. Back, knee, hip and shoulder strains are all common among kickboxers, found a study in the Journal of Strength and Conditioning Research.
As with most other forms of vigorous exercise, if you’re a newbie, it’s important to ease into kickboxing gradually. “If you have a bad knee or some other limitation, it’s important to have a coach or physical therapist who knows how to adapt a kickboxing program to your needs, and who will introduce it in a controlled, systematic manner,” Jackson says. Start slow, and you’ll get the most benefits in the end.
The UTEP track and field team will head to Austin, Texas, for the 90th edition of the Clyde Littlefield Texas Relays held at the Mike A. Myers Stadium.
More than 7,700 athletes from around the world will compete in the four-day meet that begins Wednesday and concludes Saturday. The meet will have 14 hours of coverage on the Longhorn Network (schedule listed below).
Junior Lucia Mokrasova returns to the state capital where she scored 5,615 points last year to set the school record, previously held by Jallycia Pearson (2014). She will be in action Wednesday and Thursday.
Tobi Amusan will compete in the 100m hurdles and the 4x100m relay. Amusan set the nation’s fastest time (12.63) this year and ninth best in NCAA history at the UTEP Springtime on March 25. The two time All-American will take to the track on Friday for the 100m hurdles at 8:35 a.m. MT and again in the 4x100m relay shortly after. Israel Ramsay, Florence Uwakwe, and Madison Gibson complete the relay team.
Yanique Bennett will also run in two events, the 400m Friday (6 p.m. MT Friday) and the mile relay Saturday at 3:05 p.m. MT. Completing the 4x400m relay will be Uwakwe, Gibson and Ada Benjamin.
The distance contingent of Linda Cheruiyot, Gladys Jerotich and Winny Koech will compete Thursday evening in the 5,000m run. Lilian Koech will race in the 1,500m run.
Fayon Gonzales will take the field Thursday in the hammer throw starting at 10 a.m. MT. Samantha Hall will throw the discus on Saturday at 12:10 p.m. MT.
On the men’s side, All-American Michael Saruni will compete in the 800m Thursday evening at 6 p.m. MT. That will be followed by Cosmas Boit (1,500m), Jonah Koech (mile), Daniel Cheruiyot (3,000m steeplechase) and Antony Kosgei (5,000m).
Freshman Karol Koncos will compete in the hammer throw set to start at 1 p.m. MT Thursday.
For live updates, follow @UTEPTrack on Twitter. This year’s meet will be available online at espn3.com and via the WatchESPN app for smartphones and tablets.
T.V. Schedule
Wednesday March 29: 5-6:30 p.m. MT (tape delay of heptathlon) Thursday March 30: 3:30 – 5 p.m. MT (tape delay of multi-events) 5-7 p.m. MT (LIVE) Friday March 31: 8:30 a.m. – 11:30 a.m. MT (LIVE); 6-8 p.m. MT (LIVE) Saturday April 1: 12:30- 4:30 p.m. MT (LIVE)
Via the embedded player, fans can follow their favorite team via any web-enabled device – even from the in-dash entertainment centers in newer vehicles.
Users need only log on, click on the story, bookmark it and hit play!
As part of the partnership with 600ESPN El Paso, the coverage will feature Chris Babcock calling all the action, along with different members of 600ESPN’s Football Friday Night Crew throughout the season.
The partnership between Herald-Post and 600ESPN El Paso allows for the most complete, live coverage of high school football in the El Paso area.
****
Thursday, October 27 REPLAY Franklin vs Coronado @ Sun Bowl
A variation of the traditional push-up, the pike push-up zeroes in on your arms and shoulders. You won’t have to worry about what’s your best angle in your wedding photos—your arms will look sexy from every angle.
How to do it: Begin in push-up position with hands in a wide diamond (fingers pointing toward each other).
Bend at waist, lifting hips up and coming onto toes (walk them in a bit if needed) so body forms upside-down “V”. Bend elbows to lower head toward hands.
Press back up; do 10 reps. For even more of a challenge, do 10 reps with right leg raised, then repeat with left leg raised.
Nothing says summer like sleeveless tops and strapless dresses. But the idea of showing so much skin can be daunting. Our solution? Get started early with these six sculpting exercises from Nike trainer Lauren Williams. They will sculpt your upper body stat, so you’ll feel good at your next wedding or outdoor social event. Watch this video and try Lauren’s best get-fit moves for awesome arms, strong shoulders, and a beautiful back.
1. Wide hand walkout: Start in a plank position with your hands directly underneath your shoulders. From here, walk your hands out to a wide push-up position. Return to plank and repeat.
2. Tricep drops: Start in a plank position with your hands slightly in front of your shoulders. Gently drop your elbows to the ground. Return to high plank and repeat.
3. Front and side dumbbell arm raises: Stand tall with a dumbbell in each hand. Raise both to chest level to create a 90-degree angle with your torso, then lower back down. Next, raise both arms out straight to each side on the diagonal, stopping at shoulder level to create an open T shape with the arms, palms facing each other. Lower back down and continue to repeat this combination, moving the arms up and down as they extend in front of you and to the sides.
4. Bent-over tricep kickbacks: From standing, lean your upper body forward so you’re slightly bent over with a dumbbell in each hand. Bend arms at the elbows until dumbbells reach chest, then straighten arms back out as the weights reach back behind the upper body. Repeat.
5. Bent-over alternating rows: From standing, lean your upper body forward so you’re slightly bent over with a dumbbell in each hand. First raise your right arm up so your elbow bends deeply and the weight is next to your chest. Return arm down to center, then repeat the row movement on the left arm. Continue alternating arms.
6. Inverted push-up: From a downward dog, bend the elbows out wide to create a 90-degree angle, keeping the hips raised high toward the ceiling. Extend arms to return to starting position and repeat push-up.
The birth of my twins 13 years ago coincided with the death of any semblance of privacy or personal space.
First there was the nursing, which kept at least one of them dangling off my body for a good part of the day and night. Then, once they could crawl, I was afraid to shut the bathroom door for fear they’d bring a bookshelf down on their heads or eat the refrigerator magnets and get stuck to one another at the belly.
I was a nervous mom to begin with, and the two of them, constantly in motion and mischief, made me anxious and hypervigilant. Unfortunately, my open-door policy with my toddlers led to their begging to sit on my lap, even when I was peeing. I said no, but I was too ridden with working-mom guilt (bad mommy, earning money to support your children!) to boot them out and too exhausted to deal with the ensuing meltdowns if I tried.
I’d gotten myself into a bad pattern in which the kids felt entitled to a 24-hour all-access mommy pass, and I didn’t know how to break it. I loved them to the moon, but I was depleted and not exactly a joy to be around.
That’s when I started saying, “Mommy has to go to the gym.” I’m not sure whether my husband was more thrilled to afford me the free time or to just be rid of me, but it didn’t really matter. For a full hour, I’d go downstairs to our building’s gym and do… whatever. At first, I’d simply sit in the ladies’ room and marvel at what it was like to not have to rush out—pants open, hands unwashed—to avert some impending crisis. I’d noodle around on the bike and then head back upstairs, a saner person for it. Sometimes I made uninterrupted phone calls, and occasionally I cried from the stress of it all.
But eventually I began to use my time efficiently, doing 40 minutes of cardio and either stretching or using the weight machines. I’d been a regular before I had my kids, so getting back in shape wasn’t hard. And just going to a place where I could have myself all to myself was amazing.
Now my children are teenagers, and when I text them through the closed door of their bedroom to say, “Mommy’s going to the gym,” I’m lucky if I get a thumbs-up emoji in reply. But it’s all good, and the gym is still my sanctuary, a place I will forever associate with blissful escape.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine