If you are pregnant and have back pain, you are not alone. An estimated 50 to 70 percent of women who are pregnant experience back pain, according to the American Pregnancy Association. While pregnancy and childbirth is one of the most incredible experiences a woman can have, it is also very hard on her body. There are many dramatic changes that take place during that 9 to 10 month of gestation so it is understandable that she is going to feel some aches and pains along the way.
There are a number of reasons why a pregnant woman may experience back pain including:
Natural changes to her body such as softening of ligaments and loosening of joints as her body prepares to give birth
A shift in her center of gravity as her girth increases.
Weight gain.
Position of the baby.
Her posture.
Stress, exhaustion, and worry.
Contents
Is Chiropractic Care Safe During Pregnancy?
Chiropractic care has long been held as a viable method for relieving back pain in pregnant women. Historically, midwives and other natural or alternative practitioners were the ones advocating its many benefits. This resulted in minimal data from clinical studies existing on the topic.
However, in the last decade or so, researchers have been looking closer at chiropractic and its many benefits. In one study of pregnant women and chiropractic, 94 percent of the participants experienced dramatic improvement in their pain in just 5 days.
Today many doctors and obstetricians are sending their pregnant patients to chiropractors to help them manage their back and joint pain. It is perfectly safe for both mother and baby � and both can benefit from it.
Benefits Of Chiropractic Care During Pregnancy
While chiropractic care during pregnancy can be used as a safe, non-invasive, and drug free method of pain relief, women may also enjoy other benefits which include:
A healthier, happier pregnancy.
Improved mood and less anxiety.
More mobility.
Decreased morning sickness and nausea.
Easier, faster labor and delivery.
Better flexibility.
In some cases, prevent cesarean delivery.
Improved sleep.
Faster recovery time.
Relief of pain in the back, joints, and neck.
By keeping the body in proper alignment, chiropractic care can help a woman have a healthier, happier pregnancy. She can enjoy the many benefits and experience less pain so that she can better focus on the joy of pregnancy and the wonder of bringing a new life into the world.
Why You Should Have Chiropractic Care During Pregnancy
Pregnancy brings about many changes in a woman�s body. Hormonal changes as well as physiological ones occur at rapid speeds as her body creates and maintains a perfect environment where her baby will develop and grow. These changes can cause the spine or joints to become misaligned. When this occurs, painful conditions can be created, including:
Increased curvature of the back.
Pelvic changes.
Protruding abdomen that puts pressure on the back.
Changes in posture.
Keeping the pelvis and lower back well balanced and aligned is integral to preventing lower back pain during pregnancy. What�s more, when the pelvis and spine are not in alignment, it can limit the amount of room the baby has in the womb. This condition is called intrauterine constraint. This can also inhibit the baby�s ability to get in an optimal position for delivery.
Keeping the body, including the spine, in proper alignment is vital to mobility, flexibility, and overall wellness of the body even when it is not pregnant. However, pregnancy puts specific stress on the body, creating certain needs that chiropractic care can meet. It is safe, it is effective, it is fast, and it works.
Chiropractic Clinic Extra: Stress Management Care & Treatments
Temporomandibular Joint Disorder, or TMJ, is a common condition that affects the jaw. It can be extremely painful and many people are turning to methods other than medication or surgery to relieve that pain. While lifestyle changes such as diet may help, chiropractic care has been cited as a viable treatment for TMJ pain.
At first, this may seem counter-intuitive simply because it is widely believed that chiropractors only treat the spine and neck. This commonly held belief is not entirely accurate. Chiropractors treat all joints, including the spine and neck. A chiropractor may treat ankles, wrists, knees, and, yes, even the jaw. Sometimes the neck and spine can be contributing factors and they can be treated with chiropractic care as well.
Contents
What Is Temporomandibular Joint Disorder?
The joint that connects your jaw to your skull and allows you to open and close your mouth is the temporomandibular joint. When you have problems with the muscles or joint in that area it is called TMJ, or more accurately temporomandibular disorders, or TMD.
This disorder is characterized by pain and stiffness on one or both sides of the jaw. The jaw may also lock or get stuck in either a closed or open position. Patients may also notice a popping, clicking, or grating sound in the jaw when chewing, yawning, or when closing or opening their mouth. They may also have trouble chewing and even experience swelling.
Doctors don�t know what causes TMJ. It seems to be linked to trauma to the neck, such as with whiplash, but it also can be caused by:
Arthritis in the jaw
Grinding the teeth
Stress that causes clenching of the jaw
Movement of the disc, or soft cushion, that lies between the socket and ball of the jaw
Diagnosis & Treatment For Temporomandibular Joint Disorder
Many conditions can mimic the symptoms of TMD. After taking a medical history, your doctor will check the joints in the jaw for popping, clicking, or grating sounds. He will also assess the patient�s pain or tenderness level and check for any stiffness. During the exam, the doctor will assess the job and its ability to function properly. X-rays may also be a part of the examination.
If the doctor can pinpoint the probable cause of the TMJ, he may prescribe certain treatments or make recommendations that will help. Medication is one option, mainly stress or anti-anxiety medication to help the patient relax. A night guard or splint is another option. It helps to put the patient�s teeth in the correct position. A splint is worn all the time and a night guard is worn only at night. Dental work is another option and in come more serious cases, surgery.
Chiropractic Care For Temporomandibular Joint Disorder
Chiropractic for TMJ is not only common, but very effective. The chiropractor may perform neck or spine adjustment as well as adjustments to the jaw. This means that the patient may experience pressure on their skull, jaw, upper spine, or neck as the chiropractor treat the condition. There are also soft tissue treatments that the chiropractor may perform during the course of treatment for TMJ.
The chiropractor will often recommend lifestyle and diet changes to patients. This offers the patient the opportunity to treat the whole body as opposed to just one area. They may apply cold packs or heat packs to the area, recommend supplements, and teach the exercises designed to lessen the pain and encourage healing. Chiropractic is a safe, effective, and non-invasive treatment for TMJ.
So if you or a loved one have been diagnosed with TMD and/or are experiencing TMJ pain, give us a call. Our Doctor of Chiropractic is here to help!
Chiropractic Clinic Extra: Neck Pain Care & Treatments
Chiropractic has been proven to help many health conditions, including those that seem completely unrelated to the spine. Meniere�s Disease is one of those conditions. A disorder of the inner ear, Meniere�s Disease affects somewhere between 3 and 5 million people in the United States alone. The good news is, the majority of patients, as much as 95 percent, are able to control their Meniere�s with medical treatments. Chiropractic has been found to be very effective in relieving patients of their symptoms of Meniere�s.
Contents
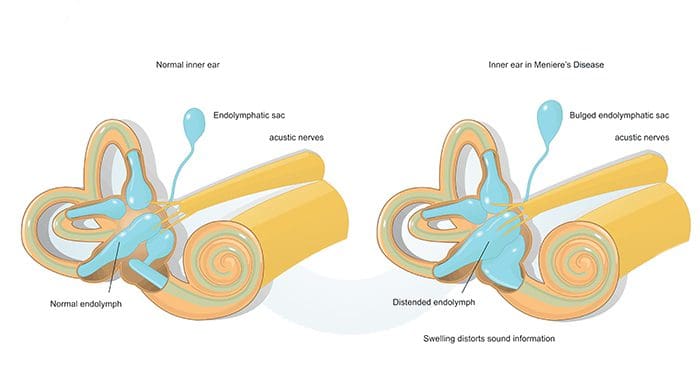
What Is Meniere�s Disease?
Meniere�s Diseaseis a disorder that affects the inner ear, causing ringing of the ears and other uncomfortable symptoms. It affects around 200,000 people every rare, typically adults ranging from 20 to 50 years of age. It does not seem to prefer one gender over the other, affecting both equally.
Symptoms of Meniere�s Disease include:
Dizziness or vertigo. It is not continuous, but instead a dizziness episode may last around 15 to 20 minutes, then stop for a while and begin again. Sometimes the dizziness can last up to 24 hours, but rarely longer. The vertigo can be severe, causing vomiting and nausea.
Tinnitus or ringing in the ear. This may cause a buzzing, hissing, whistling, or roaring sound in the ears.
Loss of hearing. The patient may experience a loss of hearing, only to have it return. However, the majority of people who have Meniere�s Disease do experience permanent hearing loss to some degree.
Full feeling in the ear. The disease can cause feelings of pressure or fullness in the ear that is affected or in the side of the head.
These symptoms usually come and go and the patient may experience one episode but not have another one for a year or more.
Diagnosis & Treatment Of Meniere�s Disease
The doctor who suspects Meniere�s Disease will take the patient�s medical history and conduct a series to tests to determine if the patient has any hearing loss or if their balance is compromised. They will also order a series of blood tests and other lab work in order to rule out other conditions.
While there is not cure for Meniere�s Disease, it can be managed fairly well with drugs like anti-nausea medications and motion sickness medications. There are also other procedures and noninvasive therapies that have proven to be beneficial. Rehabilitation, a Meniett device, and a hearing aid are all effective treatments. Chiropractic care is also proving to be highly effective and a strong treatment option.
Chiropractic Care For Meniere�s Disease
Chiropractic care in the form of spinal manipulation or adjustments of the upper cervical area has proven to be very helpful with many of the symptoms of Meniere�s. There have been several case studies that show in many cases certain chiropractic techniques can relieve patients� pain and symptoms. This is usually due to a subluxation in the upper area of the neck. This restricts movement and throws the body out of alignment.
In many cases, patients who pursue chiropractic services for their Meniere�s Disease are eventually able to stop taking the medications that are prescribed to ease the symptoms. They also find that after the chiropractic treatments, they have more energy, are more flexible, have better mobility, and have a much more positive outlook.
Doctors of Chiropractic advise patients who have been diagnosed with Meniere�s Disease to seek out chiropractic treatments. They typically consist of chiropractic adjustments and the patient can walk out when they are finished. These treatments are effective and safe but drug free and non-invasive. In most cases, it is a preferred way to manage the symptoms and the disease itself.
If you or a loved one suffer from this condition, consider chiropractic. Our Doctor of Chiropractic would love to help. Simply give us a call and we�ll see if chiropractic is the right approach for you.
Back Pain Treatment: Carlos Hermosillo is a small contractor in El Paso, Tx, who’s known Dr. Alex Jimenez for several years. As a result of the physical demands of his job, Mr. Hermosillo often experiences lower back pain and back pain symptoms which tremendously limit his ability to perform his normal physical activities, fortunately, Dr. Alex Jimenez provides him with the chiropractic care he regularly needs to return to work as soon as possible. After being involved in an accident, Carlos Hermosillo once again turned to chiropractic care for relief of his symptoms. Mr. Hermosillo highly recommends Dr. Alex Jimenez as the non surgical choice for back pain treatment.
Back pain can originate from the muscles, nerves, bones, joints or other structures in the spine. Internal structures such as the gallbladder, pancreas, aorta, and kidneys may also cause referred pain in the back. The management goals when treating back pain are to achieve maximal reduction in pain intensity as rapidly as possible, to restore the individual’s ability to function in everyday activities, to help the patient cope with residual pain, to assess for side-effects of therapy, and to facilitate the patient’s passage through the legal and socioeconomic impediments to recovery. For many, the goal is to keep the pain to a manageable level to progress with rehabilitation, which then can lead to long-term pain relief.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
Every El Paso, TX. Resident Involved In A Car Accident Needs Car Accident Specialist
Car Accident Specialist: Did you know that nearly 300,000 car accidents occur in Texas every year? The Texas State police, the Texas Department of Transportation, and the National Highway Traffic Safety Administration estimate that in 2017 there were 286,115 car accidents across the state. Over 60,000 car accidents resulted in someone being injured.
Fortunately, most of these accidents result in only minor injuries. For those who have sustained a car accident, chiropractic treatment should be sought out. In fact, anyone who has been in a moderate or high velocity collision should be evaluated by a car accident specialist/chiropractor.
Effects Of Major Motor Vehicle Accidents On The Spine
Motor vehicle accidents account for nearly half of all spine injuries.1 High velocity car accidents can have devastating effects on the spine. In some cases, the spinal cord could be damaged, causing paralysis. Displacement or fracturing of the spine’s bones (vertebrae) can partially compress the spinal cord, which causes weakness and/or numbness. Spinal cord contusions from a vertebral bone dislocation can injure blood vessels around the spine, that can lead to permanent disability.
Trauma to the spine from a car accident can cause paralysis or long-term disability if not managed properly. If you have been in a major car accident, chiropractic evaluation is critical. Even if there are no immediate symptoms, you should still be evaluated.
Minor Motor Vehicle Accidents Can Affect The Spine
Symptoms from a car accident may not show up for hours or days after the accident. A concussion, for example, may take as many as 24 to 48 hours before symptoms present themselves. Whiplash is the same way. Even if you do not feel a headache or neck pain right after a car accident does not mean that there is no injury. Because symptoms of whiplash may occur hours to days after the auto accident.2
Whiplash is caused by the rapid bending of the neck, often caused by rear end or front end collisions. Half of all people who get whiplash have neck pain symptoms for at least one year after the accident.3
If you have symptoms of whiplash such as neck pain, muscle tightness, muscle spasm, headache that is especially bad in the back of the head, or any difficulty moving your neck or turning your head, you may have whiplash syndrome. It is important to have an evaluation by a spine specialist in El Paso, TX.� or a car accident doctor (i.e., a physician who is experienced in evaluating car accident injuries). Find a chiropractor who is experienced and local.
People Involved In A Car Accident Need An Auto Accident Chiropractor
Spine surgery is not always needed after an auto accident, but until you are evaluated by a spine specialist, you cannot know for sure. Likewise, not every doctor/chiropractor has the experience and qualifications to proper diagnose and treat these types of motor vehicle injuries.
Dr. Jimenez, a car accident specialist at Injury Medical & Chiropractic Clinic, because he has evaluated and treated a substantial number of El Pasoans�who have been injured in auto accidents, over the course of 20+ years of practice. While only a small number of these patients need spine surgery, Dr. Jimenez will provide a comprehensive spine evaluation and will formulate an appropriate, personalized treatment/rehabilitation plan.
Chiropractic Clinic Extra: Back Pain Treatment
References
Carroll LJ, Holm LW, Hogg-Johnson S, et al. Course and prognostic factors for neck pain in whiplash-associated disorders (WAD): results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976). Feb 15 2008;33(4 Suppl):S83-92. doi:10.1097/BRS.0b013e3181643eb8
Kasch H, Bach FW, Stengaard-Pedersen K, Jensen TS. Development in pain and neurologic complaints after whiplash: a 1-year prospective study. Neurology. Mar 11 2003;60(5):743-749.
Spinal Cord Injury Information Network. Understanding Spinal Cord Injury: Part 1�The Body Before and After Injury. 2008;�www.spinalcord.uab.edu
Shoulder Treatment: About two years ago, Denise was involved in an automobile accident which resulted in upper body issues, including shoulder pain. Due to her painful symptoms, Denise was unable to engage in her regular physical activities. While she continued to experience problems with her auto accident injuries, she decided to seek chiropractic shoulder treatment with Dr. Alex Jimenez. Since her first treatment session, Denise noticed tremendous changes to her symptoms and she was once again able to return to her original routines prior to the incident. Denise positively recommends Dr. Alex Jimenez as the non surgical choice for shoulder pain treatment since finding relief.
Upper body issues, such as shoulder pain, are some of the most common reasons for doctor visits. The shoulder is the most mobile joint in the human body, however, because of its increased range of motion, it is also the most unstable joint. This can increase the risk of joint injury, often leading to the degeneration of the soft tissues surrounding the shoulders. Shoulder pain can be categorized as localized or referred, with other health issues causing shoulder pain. The force from the impact of an accident, such as an automobile accident or a sports injury, is a well-known cause for shoulder issues.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
Damaris Foreman started chiropractic care with Dr. Alex Jimenez for her migraine headache pain. When every traditional treatment she received proved ineffective, she turned to spinal adjustments and manual manipulations for relief. Damaris Foreman experienced the benefits of chiropractic care almost immediately after her first visit with Dr. Alex Jimenez and she experienced reduced migraine headache pain symptoms. Furthermore, Damaris Foreman highly recommends chiropractic care with Dr. Alex Jimenez as a non-surgical choice for the effective treatment of migraines.
Globally, approximately 15 percent of people are affected by migraines. It often begins at puberty and is worst through middle age. In many women they become common during menopause. As of 2016, it is among the most common cause of disability. Migraines present with recurrent severe headache associated symptoms. Approximately 15 to 30 percent of people with migraines experience an aura. Those who have migraines with aura also frequently have migraines without aura. The seriousness of the pain, length of the headache, and frequency of the migraine may differ.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Shoulder Pain: The shoulder goes through a lot in a day. It is comprised of an intricate network of ligaments and muscles, with the rotator cuff taking the brunt of much of the movement and exertion.
Not only is the shoulder the most flexible joint in the human body, it is also one of the most unstable. Among athletes, the shoulder injuries are quite common; the shoulder sustains more injuries that almost all other parts of the body.
The shoulder is particularly vulnerable due to its unique construction. Other joints in the body, such as the ankle or elbow, have a somewhat limited range of motion. The shoulder has a wide range of motion as a freely moving joint. This leaves it susceptible to stress, injury, and pain.
The various soft tissues within shoulder, muscles, tendons, and ligaments can be injured from overuse, excessive strain, falls, and improper motion. Treating shoulder pain can be a challenge because it is used so often in the course of daily life. A Doctor of Chiropractic can help relieve shoulder pain and speed healing.
Contents
Causes Of Shoulder Injury & Pain
Shoulder pain can be caused by a number of conditions. Injury to the rotator cuff is one of the most common causes and is commonly seen in athletes, like gymnasts and football players, who use their arms and shoulders frequently and tend to put increased stress on the joint.
Any activity that involved repetitive shoulder movements can also cause injury. Swimmers, tennis players, and baseball players are highly susceptible to injury.
Athletes are not the only ones who experience shoulder pain and injury. People who work in an environment that requires repetitive motion or strenuous upper body work are also at risk. Construction workers commonly experience shoulder injury and pain as do truck drivers.
Prevention Of Shoulder Pain
Preventing shoulder pain and injury is usually quite simple. Athletes and workers whose jobs require repetitive arm work or rotation should take the warm up and cool down before playing, and they should take breaks often.
Pain should be addressed sooner rather than later with ice packs applied immediately and a chiropractic appointment. Ignoring shoulder pain could lead to a more serious injury.
Taking time off to give an injured shoulder rest is always a smart move. The joint needs rest in order to heal and regular activities should not be resumed until the doctor says it is OK. A chiropractor can also recommend exercises specifically geared toward certain types of injuries or conditions � they should be followed to the letter.
The patient will be assessed by the chiropractor at the first visit and the doctor will determine a treatment plan. Ischemic compression techniques have been found to be very effective for certain types of shoulder pain. It is often favored because it is very effective, in not very strenuous for the doctor to perform, is very safe, and is tolerated well by the patient. Other conditions may respond better to different chiropractic techniques.
Chiropractic care is often the treatment of choice for shoulder pain because it is minimally invasive and it works. As is often the case, pain in one part of the body can cause pain in other areas. In the case of shoulder pain, the spine and neck may become inflamed. Chiropractic care addresses all areas of the body to relieve pain without drugs and gets the patient on the road to healing quicker.
Are you or a loved one suffering from shoulder pain? If so, give us a call. Our Doctor of Chiropractic is here to help!
Back Pain Management: Denise was involved in an auto accident which resulted in low back pain. When she realized she couldn’t sit, walk or sleep for extended periods of time without experiencing painful symptoms, Denise found chiropractic care with Dr. Alex Jimenez in El Paso, TX. Once she received treatment for her auto accident injuries, Denise experienced relief from her symptoms and she was able to perform her everyday activities once again. Thanks to the education and care Dr. Alex Jimenez provided, Denise regained her original health and wellness.
Back pain is common, with roughly nine out of ten adults experiencing it at some time in their life, and five from ten working adults developing it every year. Some estimate around 95 percent of Americans will experience back pain at some time in their lifetime. It’s by far the usual cause of chronic pain, as it is also a significant contributor of missed work and disability. In the United States alone, acute cases of lower back pain are the fifth most common reason for physician visits and causes 40 percent of missed days off work. Furthermore, it is the only leading cause of disability globally. Back pain management is possible through chiropractic treatment.�For Answers to any questions you may have please call Dr. Jimenez at 915-850-0900
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
When you walk, more than 200 individual muscles spring into action which includes all of the muscles in your spine and pelvic area. There�s no denying that walking is good for you and very beneficial to overall health. It is also very effective for spinal health. In most cases, walking is an excellent complement to chiropractic care. Here are 5 good reasons for chiropractic patients to get moving.
Contents
Walking Benefits:
Prevents & Relieves Back Pain
The American Chiropractic Association (ACA) recommends walking to help relieve back pain. It is a low impact exercise and very gentle on the back, burning around 265 calories in 30 minutes.
You should avoid walking on uneven terrain or concrete to keep it low impact and avoid injury. Exercise also releases pain relieving endorphins in addition to aiding in other conditions that can relieve pain which includes improving flexibility and mobility, helps rehydrate spinal discs, increases circulation, and aids in weight loss and weight management.
Increases Circulation
Walking increases circulation throughout your body, including your spine. This ensures that you have a continual flow of blood to the muscles and nutrients to the spine. Soft tissues are nourished and enriched while harmful toxins are drained away.
Walking is integral for spinal health. It increases circulation which, in turn, lowers blood pressure. This helps bring the body into balance and increases your stamina. As blood is moved through your body it nourishes all of your muscles, making you stronger and making it easier for you to exercise. Basically, the more you walk, the more you are able to walk.
Improves Flexibility & Mobility
As walking increases circulation, flexibility and mobility are enhanced. When combined with a regimen of light stretching, walking can increase flexibility and a better range of motion. This has the added benefits of reducing the risk of injury and improving posture.
The ACA recommends a series of stretches combined with cardio, including walking, to help with back pain management and good spinal health. It is a very good accompaniment to chiropractic care and is an effective supporting activity which will help your treatment work even better.
Helps Rehydrate Spinal Disks
During the day movement causes compression of your spinal discs, squeezing out the water that fills the discs so they provide a cushion or your vertebrae. The increased circulation that comes from walking also helps to move vital water to the area.
The discs absorb this water, rehydrating them so they can continue to do their job as shock absorbers for the spinal column. This is also a great case for staying well hydrated by drinking lots of water not only while you walk, but also throughout the day.
Aids With Weight Loss & Weight Management
Extra body weight can cause significant stress on the spine. Abdominal fat can create excess weight in the front, causing a swayback effect in the spine. This puts pressure on the lower back, resulting in pain in that area.
The spine is part of the body�s core and the muscles that surround the spine aid in balance and movement. When excess weight is present those muscles become strained as they must work harder to maintain balance. Walking helps with weight management and weight loss eliminating or reducing the effects of excessive weight.
Walking benefits your whole body. It reduces your risk of heart disease, improves blood sugar and blood pressure, reduces your risk of osteoporosis, helps you maintain body weight, improves your mental health, and can even reduce your risk of certain cancers. With your spine at the core of your body, good spinal health plays a part in every one of these conditions. By combining walking with chiropractic care, you are giving your body its best chance at good health and optimal function.
Chiropractic Clinic Extra: Pablo Mena & Son | PUSH-as-Rx ��
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 This disorder is characterized by pain and stiffness on one or both sides of the jaw. The jaw may also lock or get stuck in either a closed or open position. Patients may also notice a popping, clicking, or grating sound in the jaw when chewing, yawning, or when closing or opening their mouth. They may also have trouble chewing and even experience swelling.
This disorder is characterized by pain and stiffness on one or both sides of the jaw. The jaw may also lock or get stuck in either a closed or open position. Patients may also notice a popping, clicking, or grating sound in the jaw when chewing, yawning, or when closing or opening their mouth. They may also have trouble chewing and even experience swelling.


 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
 Minor Motor Vehicle Accidents Can Affect The Spine
Minor Motor Vehicle Accidents Can Affect The Spine
 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You & God Bless.
 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.


 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.







