Costochondritis, also called Tietze syndrome, is often misdiagnosed due to the varied symptoms. It involves the ribs and, depending on the area affected, the pain, discomfort, and other symptoms can mislead doctors to underdiagnose or misdiagnose.
Patients may experience pain in the side, back, and chest which means it can mimic several different conditions, including heart attack, gastrointestinal problems, and lung disease. This can lead to anxiety and increased stress. It is also a chronic problem for some people, causing pain that can range from moderate to intense.
What Is Costochondritis?
The body is constructed so that the ribs protect the lungs. The first seven pairs connect to the sternum in the front and at two areas in the back along the spine while the lower five pairs are connected in the front by cartilage and in the back along the spine.
Ribs are meant to protect the organs, including the lungs and they are on hinges so that the lungs have room to expand during respiration. Costochondritis occurs when one of those hinges doesn�t work or the cartilage becomes inflamed. The condition is accompanied by pain and sometimes swelling in the affected area.
Symptoms Of Costochondritis
While swelling may occur in some cases with costochondritis, the primary symptom is pain in the chest area. This pain may become worse when coughing or taking a deep breath and is typically characterized as sharp or aching, although some patients do describe pressure or tightness in the chest area. It often occurs on the left side of the sternum and typically affects several ribs instead of just one. The area is also usually sensitive to touch and pressing on it will increase the pain.
Because the pain occurs in the chest area, many people believe that they are having a heart attack. It is important to note that anyone who experiences chest pain or tightness should seek emergency medical attention immediately in order to rule out heart attack or other life threatening conditions.
How Is Costochondritis Diagnosed?
Usually when a patient seeks treatment for costochondritis, there is no clear cause. However, there are some conditions and activities that have been linked to it and could be the cause or aid in creating the condition. Typical causes of costochondritis include:
Physical strain such as severe coughing, strenuous exercise, and heavy lifting. People with bronchitis and pneumonia sometimes get costochondritis because of the intense coughing. It is also common among body builders, caused when they strain to lift extremely heavy weights.
Injury such as getting hit in the chest.
Joint infection such as bacteria, viruses, and fungi that cause illnesses like aspergillosis, syphilis, and tuberculosis can infect and inflamer the rib joints.
Arthritis such as ankylosing spondylitis, rheumatoid arthritis, and osteoarthritis have all been linked to costochondritis.
Tumors including cancerous as well as noncancerous can cause costochondritis. When cancer moves through the body from the lung, thyroid, or breast it can cause inflammation in the rib joints.
People over 40 years old and women are the high-risk categories for costochondritis. Young adults and teenagers are more prone to the connected condition, Tietze syndrome, which is equally frequent in both women and men.
Chiropractic For Costochondritis
There is no standard treatment for costochondritis other than managing symptoms. However, chiropractic has proven to be exceptional for managing pain. Chiropractic treatment for the condition involves a gentle approach with anterior thoracic chiropractic adjustments along with treatment for the soft tissue around the affected area and extending along the nerve path.
The chiropractor may also recommend alternating heat and cold directly on the painful areas. Light massage may also work and the chiropractor will show them how to do this at home for continuing self-care. With regular chiropractic treatments and diligent self-care at home, patients can lessen the occurrences of costochondritis and greatly reduce or eliminate the pain.
Injury Medical Clinic: New Patient Chiropractic Care Intake Forms
“Clinical decision rules, spinal pain classification and prediction of treatment outcome: A discussion of recent reports in the rehabilitation literature”
Abstract
Clinical decision rules are an increasingly common presence in the biomedical literature and represent one strategy of enhancing clinical-decision making to improve the efficiency and effectiveness of healthcare delivery. In the context of rehabilitation research, clinical decision rules have been predominantly aimed at classifying patients by predicting their treatment response to specific therapies. Traditionally, recommendations for developing clinical decision rules propose a multistep process (derivation, validation, impact analysis) using the defined methodology. Research efforts aimed at developing a diagnosis-based clinical decision rule have departed from this convention. Recent publications in this line of research have used the modified terminology diagnosis-based clinical decision guide. Modifications to terminology and methodology surrounding clinical decision rules can make it more difficult for clinicians to recognize the level of evidence associated with a decision rule and understand how this evidence should be implemented to inform patient care. We provide a brief overview of clinical decision rule development in the context of the rehabilitation literature and two specific papers recently published in Chiropractic and Manual Therapies.
Clinical Prediction Rules
Healthcare has undergone an important paradigm shift toward evidence-based practice. An approach thought to enhance clinical decision-making by integrating the best available evidence with clinical expertise and patients’ preferences.
Ultimately, the goal of evidence-based practice is to improve healthcare delivery. However, the translation of scientific evidence into practice has proven a challenging endeavor.
Clinical decision rules (CDRs), also known as clinical prediction rules, are increasingly common in the rehabilitation literature.
These are tools designed to inform clinical decision-making by identifying potential predictors of diagnostic test outcome, prognosis, or therapeutic response.
In the rehabilitation literature, CDRs are most commonly used to predict a patient’s response to treatment. They have been proposed to identify clinically relevant subgroups of patients presenting with otherwise heterogeneous disorders such as non-specific neck or low back pain, which is the perspective on which we intend to focus.
Clinical Prediction Rules
The ability to classify or subgroup patients with heterogeneous disorders such as spinal pain has been highlighted as a research priority and, consequently, the focus of much research effort. The appeal of such classification approaches is their potential for improved treatment efficiency and effectiveness by matching patients with optimal therapies. In the past, patient classification has relied on implicit approaches founded in tradition or unsystematic observations. The use of CDRs to inform classification is one attempt at a more evidence-driven approach, less dependent on unfounded theory.
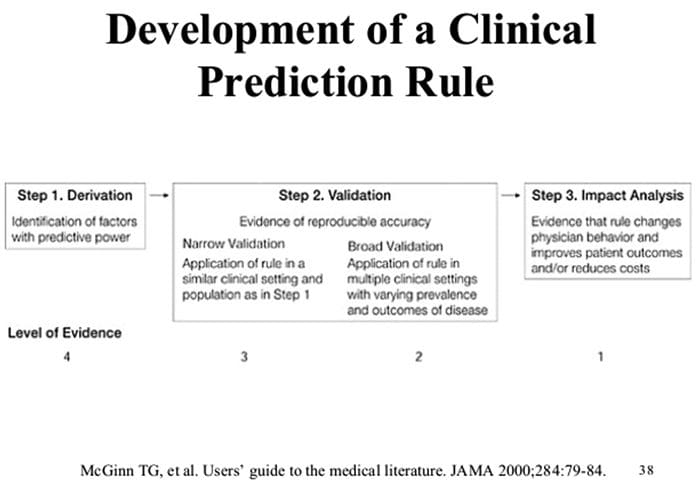
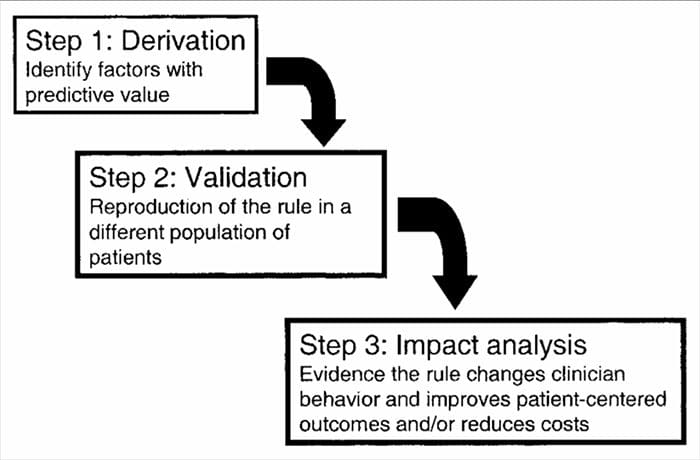
CDRs are developed in a multistep process involving studies of derivation, validation, and analysis of impact, with each having a defined purpose and methodological criteria. As with all forms of evidence used to make decisions about patients, attention to appropriate study methodology is critical to assessing the potential benefits of implementation.
Benefits Of Clinical Prediction Rules
It can accommodate more factors than the human brain can take into account
CDR/CPR model will always give the same result (mathematical equation)
Ultimately, the usefulness of a CDR lies not with its accuracy but with its ability to improve clinical outcomes and enhance the efficiency of care.[15] Even when a CDR demonstrates broad validation, this does not ensure that it will change clinical decision-making or that the changes it produces will result in better care.
The changes it produces will result in better care. McGinn et al.[2] identified three explanations for the failure of a CDR at this stage. First, if clinician judgment is as accurate as a CDR-informed decision, there is no benefit to its use. Second, the application of a CDR may involve cumbersome calculations or procedures which discourage clinicians from utilizing the CDR. Third, using the CDR may not be feasible in all environments or circumstances. In addition, we would include the reality that experimental studies may involve patients that are not entirely representative of those seen in routine care and that this may limit the actual value of a CDR. Therefore, to fully understand the utility of a CDR and its ability to improve healthcare delivery, it is necessary to undertake a pragmatic examination of its feasibility and impact when applied in an environment reflecting real-world practice. This can be undertaken with different study designs such as randomized trials, cluster-randomized trials, or other approaches such as examining the impact of a CDR before and after its implementation.
Prevalence of classification methods for patients with lumbar impairments using the McKenzie syndromes, pain pattern, manipulation, and stabilization clinical prediction rules.
Aims were (1) to determine the proportion of patients with lumbar impairments who could be classified at intake by McKenzie syndromes (McK) and pain pattern classification (PPCs) using Mechanical Diagnosis and Therapy (MDT) assessment methods, manipulation, and stabilization clinical prediction rules (CPRs) and (2) for each Man CPR or Stab CPR category, determine classification prevalence rates using McK and PPC.
CPRs are sophisticated probabilistic and prognostic models where a group of identified patient characteristics and clinical signs and symptoms are statistically associated with meaningful prediction of patient outcomes.
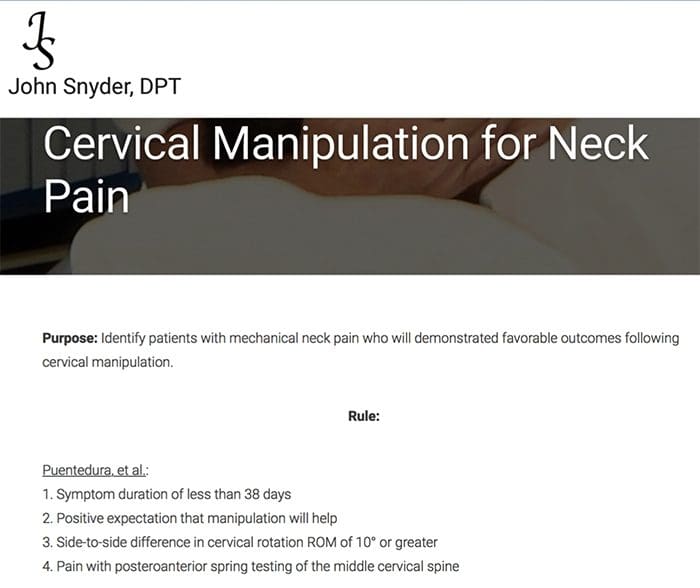
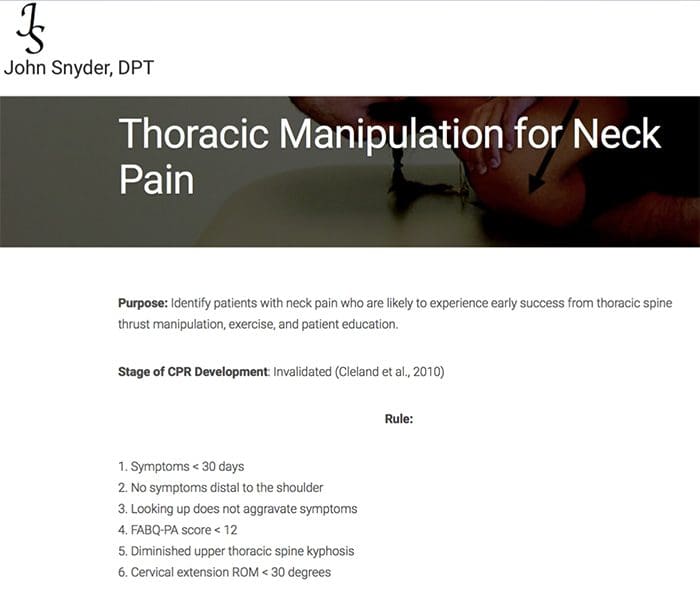
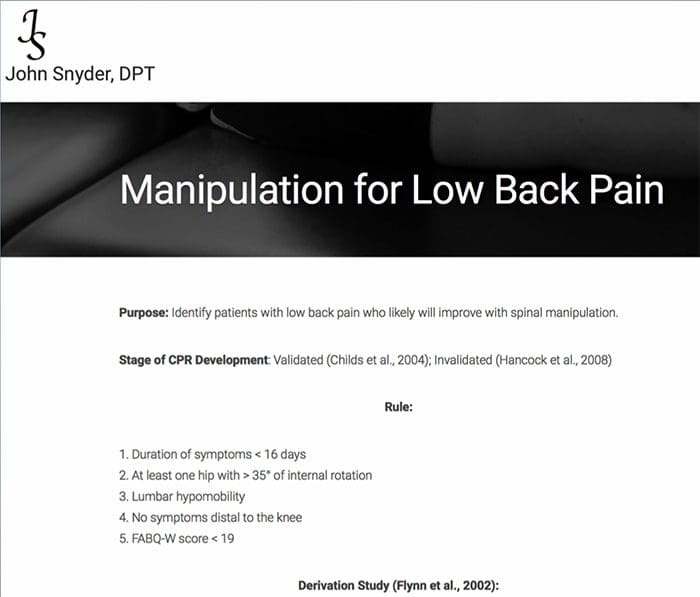
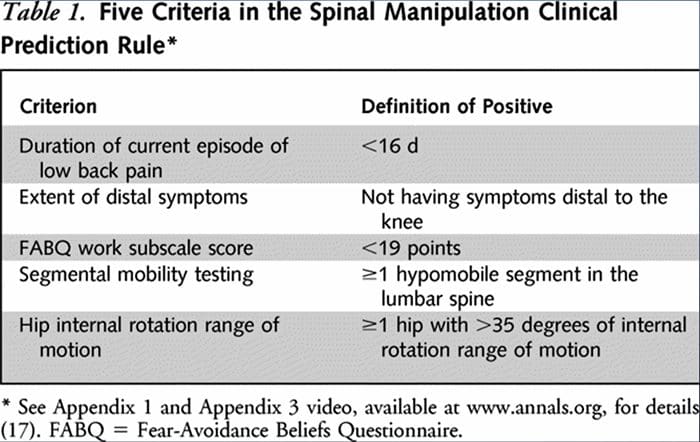
Two separate CPRs were developed by researchers for identifying patients who would respond favorably to manipulation.33,34 Flynn et al. developed the original manipulation CPR using five criteria, i.e., no symptoms below the knee, recent onset of symptoms (<16 days), low fear-avoidance belief questionnaire36 score for work (<19), hypomobility of the lumbar spine, and hip internal rotation ROM (>35 for at least one hip).33
Flynn’s CPR was subsequently modified by Fritz et al. to two criteria, that included no symptoms below the knee and recent onset of symptoms (<16 days), as a pragmatic alternative to reduce clinician burden for identifying patients in primary care most likely to respond to thrust manipulation.34 positively
“Potentia.l Pitfalls Of Clinical Prediction Rules”
What Are Clinical Prediction Rules?
A clinical prediction rule (CPR) is a combination of clinical findings that have statistically demonstrated meaningful predictability in determining a selected condition or prognosis of a patient who has been provided with a specific treatment 1,2. CPRs are created using multi-variate statistical methods, are designed to examine the predictive ability of selected groupings of clinical variables3,4, and are intended to help clinicians make quick decisions that may normally be subject to underlying biases5. The rules are algorithmic in nature and involve condensed information that identifies the smallest number of statistically diagnostic indicators to the targeted condition6.
Clinical prediction rules are generally developed using a 3-step method14. First, CPRs have derived us prospectively-
ing multivariate statistical methods to examine the predictive ability of selected groupings of clinical variables3. The second step involves validating the CPR in a randomized controlled trial to reduce the risk that the predictive factors developed during the derivation phase were selected by chance14. The third step involves conducting an impact analysis to determine how the CPR improves care, reduces costs, and accurately defines the targeted objective14.
Although there is little debate that carefully constructed CPRs can improve clinical practice, to my knowledge, there are no guidelines that specify methodological requirements for CPRs for infusion into all clinical practice environments. Guidelines are created to improve the rigor of study design and reporting. The following editorial outlines potential methodological pitfalls in CPRs that may significantly weaken the transferability of the algorithm. Within the field of rehabilitation, most CPRs have been prescriptive; thus, my comments here are reflective of prescriptive CPRs.
Methodological Pitfalls
CPRs are designed to specify a homogenous set of characteristics from a heterogeneous population of prospectively selected consecutive patients5,15. Typically, the resulting applicable population is a small subset of a larger sample and may only represent a small percentage of the clinician’s actual daily caseload. The setting and location of the larger sample should be generalizable15,16, and subsequent validity studies require assessment of the CPR in different patient groups, in different environments, and with a typical patient group seen by most clinicians16. Because many CPRs are developed based on a very distinct group that may or may not reflect a typical population of patients, the spectrum transportability17 of many current CPR algorithms may be limited.
Clinical prediction rules use outcome measures to determine the effectiveness of the intervention. Outcome measures must have a single operational definition5 and require enough responsiveness to capture appropriate change in the condition14 truly; in addition, these measures should have a well-constructed cut-off score16,18 and be collected by a blinded administrator15. The selection of an appropriate anchor score for measurement of actual change is currently debated19-20. Most outcome measures use a patient recall-based questionnaire such as a global rating of change score (GRoC), which is appropriate when used in the short term but suffers from recall bias when used in long-term analyses19-21.
A potential drawback for CPRs is the failure to maintain the quality of the tests and measures used as predictors in the algorithm. Therefore, the perspective test and measures should be independent of one another during modeling16; each should be performed in a meaningful, acceptable manner4; clinicians or data administrators should be blinded to the patient’s outcomes measures and condition22.
Sources
Potential Pitfalls Of Clinical Prediction Rules; The Journal of Manual & Manipulative Therapy Volume 16 Number Two [69]
Jeffrey J Hebert and Julie M Fritz; Clinical decision rules, spinal pain classification and prediction of treatment outcome: A discussion of recent reports in the rehabilitation literature
The reason I chose Dr. Jimenez is that he’s very thorough. From the get-go, he diagnoses the problem, diagnoses what he needs to do. I’ve had a couple shoulder injuries, I’ve had some wrist and elbow injuries, back injuries, and Dr. Jimenez has been the only one, like I said, he’s very thorough, he’s got great manners, and he’s nursed me back to health immediately. – Louie Martinez
Similar to athletes who suffer sports injuries, employees can also experience work injuries; simply the circumstances are different. And as with athletes with sports injuries, many employees with work injuries can benefit from chiropractic care. If you’ve suffered a work-related accident which resulted in injury and you require treatment for your specific health issues, a worker’s compensation claim can help pay for the expenses of rehabilitation. However, it’s important to understand the various types of work injuries as well as how a worker’s compensation claim should be filed before receiving treatment. Below, we will discuss how a healthcare professional can help you with your work injury.
Strategies for Payment of Work Injury Treatment
To begin with, the appropriate treatment option, such as chiropractic care, needs to be organized by your treating healthcare professional and the patient’s insurance company should offer approval. If you do not get approval for work injury treatment, do not be alarmed, there are a lot of steps you may take to get the treatment accepted. These essential basic guidelines will be described below, including:
Ask the doctor’s office to file a Form WC-205 requesting acceptance
File a Form WC-PMT for treatment approval
Ask for a hearing in front of a judge to get acceptance
Obtain an worker’s compensation lawyer for faster approval
Common Work Injuries
Serious workplace accidents are much too prevalent and there are a variety of common work injuries which can occur across all occupational sectors. People working in different sorts of jobs face a different range of dangers. By way of instance, an office worker would not have the same risk of suffering burns as a chef in a restaurant would.
What we do understand, however, is that about 144 employees were killed at work between 2015 and 2016 and approximately 621,000 estimated non fatal injuries to workers were reported, equating to an astonishing 4.5 million estimated working days being lost.
The workplace can be a very hazardous place and not only is it the employer’s responsibility to guarantee a safe working environment; every worker also has a responsibility to take care of themselves when they’re on the job. But to be forewarned is to be forearmed, as the saying goes. Here are several of the most common work injuries, where we will also discuss various safe and effective ways to prevent future workplace accidents.
Slips, Trips and Falls
Focusing on the most important dangers within your workplace, particularly the ones with the capability to cause harm, can help prevent work injuries. In many cases, simple measures can readily control risks, for example, ensuring spillages are cleaned up immediately so people don’t slip or making sure cabinet drawers are kept closed to make sure people do not trip and fall. For most, these are easy, economical and effective measures to ensure your most precious asset, that your work force is protected.
Muscle Strains
Strained muscles are just another frequent work-related injury, as anyone who frequently lifts hefty things at work will likely know already. Neck and back strains, specifically, are all too often sustained while working. These injuries can be prevented easily, some basic training on proper lifting techniques can make a tremendous difference. The use of specialized equipment as well as safety tools and gear can also help prevent muscle strains.
Being Hit By Falling Objects
Falling or flying objects in the workplace can expose workers to relatively minor injuries, like cuts or abrasions, as well as more severe injuries such as concussions or blindness. Wearing safety gear and equipment in workplace areas where objects can fall or fly out can help prevent these types of injuries. Moreover, ensuring that your own equipment is secured and wont’ fall or fly away can help prevent these type of work injuries in the first place.
Repetitive Strain Injury
Repetitive strain injury, or RSI, is a health issue that’s become increasingly common in the workplace.�RSI may be caused by many different tasks, including strong or repetitive activity, or by poor posture. The condition mostly affects parts of the upper body, such as the�hands, writs, forearm, elbow, neck and shoulders. The cumulative effect of RSI can be severe in some cases, so it is logical to take the necessary precautions and avoid overexertion.
Crashes and Collisions
Accidents leading to crash or impact injuries are rather frequent in workplace settings as well. Whether they involve cars, lorries or smaller vehicles like forklift trucks, they could have serious consequences. It’s therefore up to companies to make sure that seatbelts and other safety precautions are in position and in use where appropriate, to prevent these types of workplace injuries.
Cuts and Lacerations
All kinds of office implements may end up leaving a painful cut. From power generators to paper trimmers, it is easy to get hurt on the job. The most common causes of those lacerations consist of poor training, inadequate security procedures and neglecting to wear the appropriate protection. Employers may help prevent such accidents by providing adequate safety equipment and putting the right procedures, such as training.
Inhaling Toxic Fumes
The air in several workplaces contains toxic substances in the kind of dusts, fumes, mists, gases and vapours. While most of us do not work with toxic chemicals, those of us who do, without the proper safety measures, may be at risk of impairment to breathing, skin or eye reactions as well as possibly more severe injuries. Employers must provide employees with the correct workwear, such as fitted face masks and goggles, to avoid dangerous exposure.
Exposure to Loud Noise
Loud noise on the job can lead to hearing damage that is permanent and disabling. This can be hearing loss that is gradual due to exposure to noise over time, but also damage caused by sudden, extremely loud noises. Industrial deafness may also result in significant compensation payouts farther across the line, and its often considered to be very much in companies’ interest to disregard this health issue. Safety measures like ear protection can help to prevent it.
Walking Into Objects
It is probably safe to say we’ve all done this at any point. Maybe you’re chatting absent-mindedly or perhaps you’re feeling a little under the weather, when you suddenly end up on the sharp end of a doorway, wall, table or cabinet. Obviously, these accidents can cause damage. Fortunately, such mishaps can be avoided by approving employees to be vigilant and transferring unnecessary hazards out of the way so people can’t walk into them.
Fights at Work
Simmering workplace stress can bubble under for weeks or perhaps years before spilling over into physical confrontation, or rather one workmate can take another’s opinion on last weekend’s game the incorrect way. Fights in the workplace can, unsurprisingly, lead to some serious work injuries. Effective procedures for dealing with employee grievances can reduce the probability of them being irritable and causing fights at work.
Oftentimes, accidents aren’t only brought on by a small mistake or a simple mishap from a busy employee. Many workplace accidents are tied to employer or employee negligence. Even though there’s no shortage of ways people can injure themselves in the office, we do know there are various procedures employers can set up to prevent workers from coming to some avoidable harm. Training, signage and accessibility to the essential safety equipment can all be a major assistance, with regular risk assessments becoming a necessity within the office, as well as in other workplace settings, to help avoid unnecessary mishaps and work injuries.
Dr. Alex Jimenez’s Insight
While the workplace is meant to be a safe and professional environment often supplied with protective gear and equipment, work injuries can sometimes occur. A variety of workplace injuries can lead to trauma, damage or injury and can even aggravate a previously existing condition, although some occur more frequently than others. Common work injuries can include, slips, trips and falls, muscle strains, being hit by falling objects, and repetitive strain injury, among others. However, the most important thing for employees to be aware of at any time an accident occurs is that if they are injured on the workplace, they should report the injury immediately to a supervisor.
Chiropractic Care and Workplace Injuries
Individuals who have been injured at work may often have an underlying condition to begin with. Once they’ve suffered a work injury, however, returning to work is a necessity for the individual’s household. A healthcare professional, such as a chiropractor, will produce a treatment plan that is specifically targeted to your own situation. Goals are put up, and your chiropractor can permit you to achieve those aims. This healthcare professional is your trainer in returning to work. Treatment may consist of spinal adjustments and manual manipulations, physical therapeutics, stretching, particular exercises, hot and cold therapy, ultrasound, aquatic therapy and joint mobilization. Chiropractic care is an alternative treatment option which focuses on the treatment of a variety of injuries and conditions associated with the musculoskeletal and nervous system.
When you have been hurt in the workplace, contact a healthcare professional immediately. Chiropractors are skilled and dedicated to your personal restoration. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Gale Grijalva suffered from severe back pain as a result of an automobile accident injury. Where it was once very difficult to go about her regular daily tasks, Gale Grijalva is now able to participate in physical activities she wasn’t able to engage in before thanks to Dr. Alex Jimenez, chiropractor in El Paso, TX. Gale Grijalva describes how patient Dr. Jimenez is and she discusses how thoroughly he’s been able to help her, including answering any concerns she may have. Gale Grijalva also experienced results through rehabilitation.
Chiropractic Severe Back Pain Treatment
Severe chronic back pain is a serious, recurring condition which affects a person’s everyday life. Back pain lasting over three months is considered chronic. The spine is an essential component of the body. Severe chronic back pain might be the backbone’s manner of telling the body that there is an issue. The spine is composed of bony vertebrae, soft spinal discs, facet joints, tendons, ligaments and tendons. Within the bony vertebral artery lies the spinal cord, the delicate but effective nerve pathway of the central nervous system.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
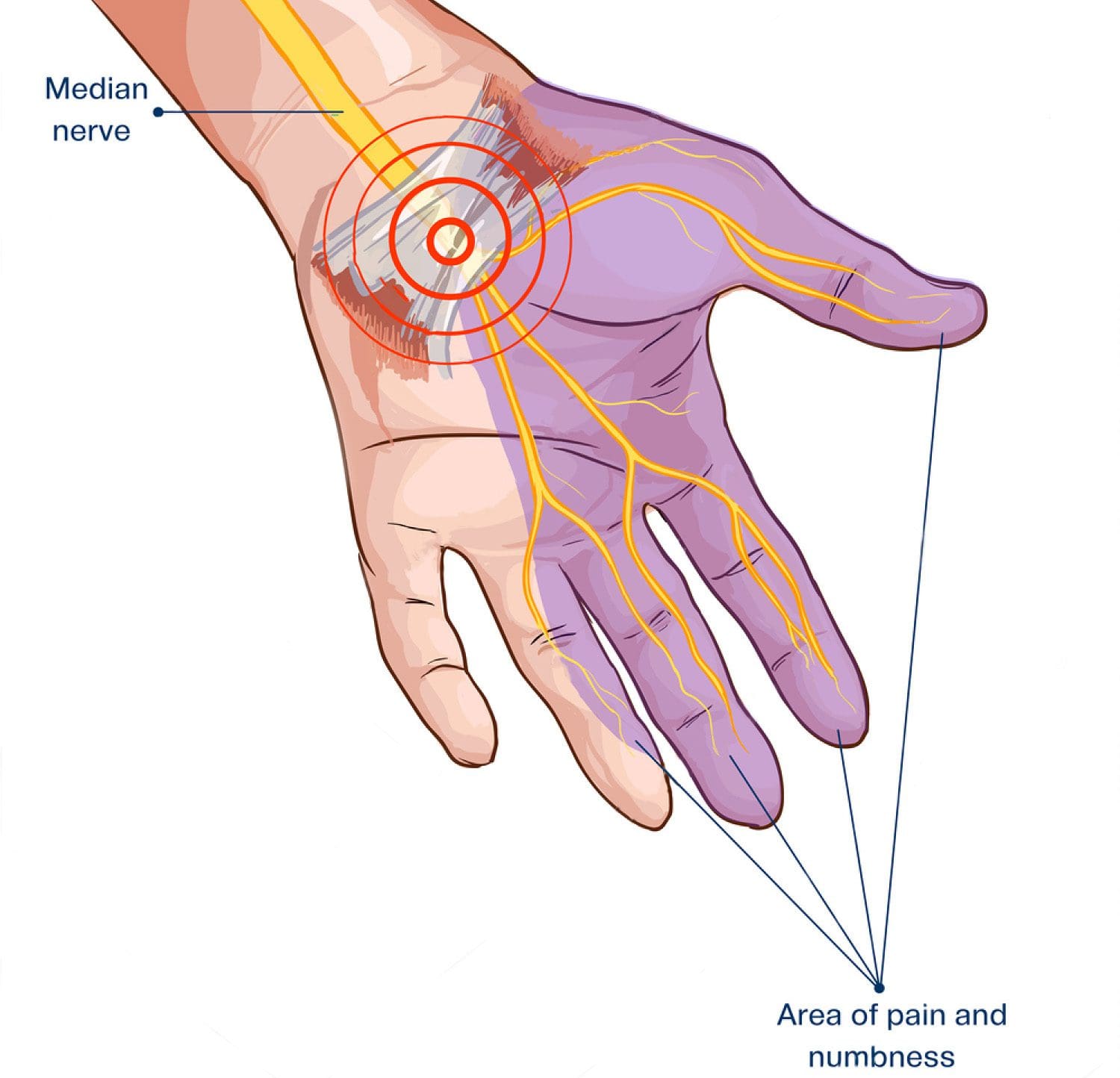
Due to his significant craftsmanship in San Antonio, TX, Ottis Hamlet must largely rely on the use of his best tools: his hands. Unfortunately, Mr. Hamlet developed debilitating symptoms in both of his arms because of carpal tunnel syndrome, which dramatically impacted his capacity to participate in his occupation and therefore affecting his quality of life as a result. Ottis Hamlet was able to find relief for his hand and wrist pain with Dr. Alex Jimenez through a trip to El Paso, TX and he received chiropractic treatment for his carpal tunnel syndrome, preventing the need to undergo any surgical interventions.
Carpal Tunnel Chiropractic Treatment
Carpal tunnel syndrome is a medical condition resulting from the compression of the nerve that travels via the wrist and in the lymph nodes. Typical symptoms include pain, tingling sensations and numbness, at the thumb, index finger, middle finger, and the thumb side of this ring fingers. Symptoms normally begin gradually and may continue throughout the day. Symptoms may stretch throughout the arm and also diminished grip power may also happen. Carpal tunnel syndrome may be diagnosed according to its symptoms.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Once I started treatment with Dr. Jimenez, I started noticing I was able to go back to the gym, I was able to sit longer periods of time, and ever since I’ve been a lot better. – Denise A.
Pain is a fundamental response of the nervous system which functions to help keep the body aware to possible injury. When an injury occurs, pain signals are transmitted from the injured site up through the spinal cord ant into the brain, where the messages are processed accordingly.
As the injury heals, however, the pain will typically become less severe. While it’s normal for everyone to experience occasional aches and pains, chronic pain can become a real health issue which can severely restrict an individual from completing their daily tasks, ultimately affecting their quality of life. Below, we will describe chronic pain and discuss treatment options to help manage chronic pain symptoms.
What is Chronic Pain Syndrome?
Chronic pain is quite different when compared to general types of pain. With chronic pain syndrome, the body will continue to send pain signals to the brain, where symptoms can last for several weeks, months, even years after the initial injury has healed.
Chronic pain is defined as pain which lasts 12 weeks or more. The type of pain is often felt as sharp or dull, causing an aching or burning sensation around the affected regions and it may be steady or intermittent. Chronic pain can develop in almost any section of the human body. Because chronic pain can tremendously restrict an individual’s strength, mobility, flexibility and endurance, these symptoms can make it challenging for anyone to get through their regular tasks and physical activities.
Chronic pain syndrome is usually caused by an initial injury but it’s also believed that symptoms can manifest after nerve damage has occurred.�There are several different types of chronic pain. Also, chronic pain might have a mental and emotional toll in some people in addition to draining your energy and motivation. It’s important to address your chronic pain with a healthcare professional as soon as possible.
Types of Chronic Pain
According to the American Academy of Pain Medicine, more than 1.5 billion people around the world have some type of chronic pain. As a matter of fact, chronic pain syndrome is the most prevalent cause of long-term disability in the United States, affecting approximately 100 million Americans. Chronic pain is generally caused by an initial injury, such as a back sprain or pulled muscle. Sometimes, it can be caused by automobile accident injuries or a different sort of injury. Other times, chronic pain can be caused by previous underlying health issues like medical conditions or even a disease. Chronic pain is usually divided into these categories.
Nociceptive Pain: Nociceptive pain is a medical term used to describe when the pain is located in the muscles and soft tissues. This is also sometimes referred to as somatic pain. Back pain, hip pain, knee pain arthritis, and headaches, can all be considered to be nociceptive pain. Chiropractic care and physical therapeutics can help reduce and eliminate pain and discomfort associated with these health issues.
Neuropathic Pain: This type of pain is associated with actual nerve damage and it is often more intense and may be described as a sharp or stabbing sensation. Phantom limb pain, pain associated with post mastectomy, and diabetic neuropathy, are examples of neuropathic pain. A combination of chiropractic care, physical therapeutics and electrotherapy, is occasionally used in the treatment of neuropathic pain.
Chronic Pain Treatment Options
While pain drugs and/or medications can help ease symptoms associated with chronic pain syndrome, the effects are often only temporary. Fortunately, you can find better treatment options for your chronic pain. Chiropractic care and physical therapy utilize several treatment approaches and techniques to provide pain relief. The objective of these is to increase strength, mobility flexibility and endurance, while reducing overall pain. Several treatment alternatives which may also be used include:
Deep Tissue Massage: A healthcare professional can alleviate tension from the muscles, ligaments, and tendons by applying direct pressure to the affected sites.
Hot and Cold Treatments:�Hot therapies can bring more oxygen and blood to the affected areas whereas cold therapies can decrease muscle spasms and inflammation.
Transcutaneous Electric Nerve Stimulation (TENS): TENS raises the release of natural endorphins to reduce pain throughout the entire body. This therapy may be used to decrease pain associated to several health issues.
Ultrasound: Ultrasound increases blood flow and provides heat deep in joints and muscles. This can facilitate muscle stretching while reducing chronic pain.
Dr. Alex Jimenez’s Insight
Pain is the body’s natural reaction to a possible injury or condition, a warning that something is wrong. Once your body heals, the pain will stop and all bodily functions return to normal, at least, that’s the way it’s supposed to be. For many people, pain can continue long after its cause is gone. Pain that lasts for 3 months or more is medically referred to as chronic pain. Approximately 25 percent of people with chronic pain will develop a condition known as chronic pain syndrome, or CPS. When pain is present day after day, it can take a toll on your physical as well as on your mental and emotional health, where people with CPS will often develop symptoms of anxiety and depression, which can also interfere with their daily lives.
Chiropractic Care and Chronic Pain
Chiropractic care can play an essential role in alleviating and eliminating different kinds of chronic pain symptoms. Among the most fundamental aspects of providing a successful treatment plan for chronic pain is for the chiropractor to develop a specialized treatment plan for each patient. A chiropractor will perform a comprehensive exam to assess the principal cause of the patient’s chronic pain. Using that information, the chiropractor will then customize an individualized treatment plan.
Chiropractic care focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system, including chronic pain. A chiropractor will commonly utilize spinal adjustments and manual manipulations to carefully correct any spinal misalignments, or subluxations, along the length of the spine. By realigning the spine, a chiropractor can restore essential connections between the brain, spinal cord and the rest of the body, which may be responsible for chronic pain symptoms.
Furthermore, a chiropractor can recommend a series of exercises and physical activities, as well as offer nutritional advice, to help promote a speedy recovery. A chiropractor can also teach the patient how they can incorporate ergonomic principles into their everyday life. The healthcare professional will likely assemble a personalized home exercise plan that’ll be a part of the patient’s whole pain management program.
A chiropractor may work closely together with you to establish goals and manage your own personal treatment program. Your chiropractor may also let you work through any challenges you may be experiencing and adapt your treatment as needed. The journey to overcome chronic pain in order to recover maximum freedom. A qualified and experienced chiropractor can allow you to address problems and supply support while providing the best treatment available.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Terry Peoples, relies on her ability to perform her day to day tasks on a regular basis as a beauty adviser in El Paso, TX. However, when she endured a car incident injury, she had no choice but to rely upon others to execute her daily pursuits. That is when Terry Peoples obtained a recommendation to seek chiropractic treatment with Dr. Alex Jimenez. Terry Peoples makes sure to visit Dr. Alex Jimenez’s office as necessary, feeling better and refreshed each time.
Car Accident Chiropractic Pain Treatment
In accordance with the National Highway Traffic Safety Administration (NHTSA), more than three million people are injured each year in car accidents across the country. The several injuries brought on by an auto accident can be as varied as the individual requirements of each episode, but some automobile accidents are more prevalent than the others. The indicators of some automobile collisions may resolve by themselves, but most accidents and/or conditions caused by the effect of a vehicle crash might call for immediate medical care, such as chiropractic treatment, to ultimately help improve the symptoms.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Jesus Rabelo makes a living as an 18 wheeler truck driver at El Paso, TX. After being involved in a crash, Mr. Rabelo suffered from back and shoulder pain that influenced his private life and function, forcing him to need to start all over again. In reference to a highly appreciated recommendation, Jesus Rabelo found Dr. Alex Jimenez, chiropractor in El Paso, TX. Mr. Rabelo describes receiving outstanding service from the team and he highly recommends Dr. Alex Jimenez himself.
18 Wheeler Accident Chiropractic Treatment
In 2013, 54 million individuals sustained injuries from traffic crashes. This led in 1.4 million deaths in 2013, up from 1.1 million deaths in 1990. Automobile accidents can be grouped into various kinds, such as head-on, rear-end, side accidents, and rollovers. Psychological issues may happen because of auto accidents. A variety of injuries and ailments could result in the blunt force injury brought on by a crash, such as whiplash and back pain, among others.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
I got into a car accident, I was rear-ended on Valentine’s Day and things weren’t quite right in my body, the aches and pains started coming. So after I visited another chiropractor and talked to my client, they told me about this place and when I came I was like, okay, I’m not going back to the other place. And that’s how I head about him (Dr. Alex Jimenez) and I’m so grateful. – Terry Peoples
Based on information referenced by the National Highway Traffic Safety Administration, or NHTSA, approximately more than three million individuals are injured annually in automobile accidents throughout the United States alone. While the unique conditions of every car crash can ultimately result in a wide variety of injuries, some types of automobile accident injuries are more common than others.
Fortunately, a majority of automobile accident injuries may resolve on their own without the need for treatment, however, more significant health issues caused by the auto collision may require some amount of treatment and/or rehabilitation and others may unfortunately become permanent if left untreated. It’s fundamental for the victim of an automobile accident to seek immediate medical attention in order for them to receive a proper diagnosis for their motor vehicle injuries before proceeding with the most appropriate treatment option for them.
Prior to following any necessary medical procedure, understanding some of the most common automobile accident injuries can help you become aware of the steps you can take to ensure that you are getting the proper care for your health issues. Furthermore, the type and severity of motor vehicle accidents suffered by the victims involved in a car crash may largely depend on several variables, including:
Was the individual wearing a seat belt?
Did the person’s car get hit from the back, side or front?
Was the occupant facing straight ahead in the seat? Or was the person’s head or body turned in a particular direction?
Was the incident a low-speed collision or a high-speed crash?
Did the car have airbags?
There are two broad categories of automobile accident injuries: impact injuries and penetrating injuries. Impact injuries are generally characterized as those caused when a portion of the individual’s body hits some part of the interior of the car. Frequently, this can be a knee hitting a dashboard or the head hitting the seat rest or the side window during an auto collision. Penetrating injuries are generally characterized as open wounds, cuts and scrapes. Shattering glass or loose items flying inside the car on impact can often cause these types of automobile accident injuries. Below, we will discuss the most common automobile accident injuries and describe them in detail.
Soft Tissue Injuries
Soft tissue injuries are some of the most common types of automobile accident injuries. A soft tissue injury is typically characterized as trauma, damage or injury to the body’s connective tissue, including tendons, ligaments and muscles. Soft tissue injuries can vary depending on the type of connective tissue it affects as well as on the grade and severity of the harm. Because soft tissue injuries do not involve open wounds, it may be challenging to diagnose these type of automobile accident injuries.
A whiplash-associated disorder, most frequently referred to as a whiplash injury to the neck and upper back, is a type of soft tissue injury. In this form of harm, the muscles, tendons and ligaments are stretched beyond their natural range due to the abrupt movements imposed on the neck and head from the force of the impact at the point of collision. These same mechanisms may additionally cause soft tissue injuries in other regions of the body, such as the back. Automobile accidents can also often cause mid-back and low-back muscle sprains, and at times, these may cause severe back injuries and even aggravate underlying conditions due to the sheer force from the impact on the spine.
Cuts and Scrapes from Automobile Accident Injuries
During an auto collision, any loose objects inside the car can immediately become projectiles which can be thrown about the vehicle’s interior. This includes cell phones, coffee glasses, eyeglasses, purses, books, dash-mounted GPS systems, etc.. If one of these objects strikes your body at the time of the incident, they can easily cause cuts and scrapes as well as cause additional trauma, damage or injuries.
Occasionally, these cuts and scrapes are relatively minor and require no immediate medical attention. More severe cases of these type of automobile accident injuries, however, could create a relatively large open wound and may require stitches to prevent blood loss. Cuts or scrapes can also occur when your airbag deploys from the auto collision.
Head Injuries
Head injuries in the form of automobile accident injuries can take a number of forms, where some can be considered comparatively minor and others can virtually be quite severe. The sudden stop or shift in direction by a motor vehicle during an car crash can cause an individual’s head and neck to jolt or jerk abruptly and unnaturally in any direction, overstretching the complex structures of the cervical spine beyond their normal range, leading to muscle strains and whiplash-associated disorders.
The head itself can also be injured during an auto accident. Impact with a side window or with the steering wheel may cause cuts, scrapes and bruises to the head, as well as even deeper lacerations. More severe collision impacts can cause a closed head injury. In that circumstance, the fluid and tissue inside the skull are damaged due to the abrupt movement or impact of the head. Less acute closed head injuries often result in concussions, while the most severe head injuries can cause brain damage.
Chest Injuries
Chest injuries are also common auto accident injuries. These type of injuries are usually identified as contusions or bruises, however, these can also take the form of much more severe injuries, like fractured ribs or internal injuries. Drivers often experience chest injuries due to their position behind the steering wheel, which offers very little space to move before the torso collides with the steering wheel. If an individual’s body is thrown forward during a motor vehicle collision, even if their chest doesn’t impact the steering wheel or dashboard, the torso will experience tremendously high amounts of force, specifically against the shoulder harness or seat belt, which may cause severe bruising.
Arm and Leg Injuries
The very same sheer forces which unexpectedly throw a person’s head and neck back-and-forth during a car crash can behave similarly on arms and legs. If your vehicle experiences a side impact, your arms and legs may be tossed hard against the door. In addition, if you’re a passenger, your legs typically have very little room to move. As a result, automobile accidents often cause an occupant’s knees to strike the dashboard or even chairs in front of them.
Based on the circumstance of the auto collision, automobile accident injuries to your arms and legs may include bruises, scrapes and cuts, however, sprains and even fractures in both the upper and lower extremities can happen. Keep in mind that some injuries aren’t apparent following a car accident. It may take days, weeks, or even months for symptoms to manifest. Therefore, if you’ve been involved in an automobile accident, it is best to seek immediate medical attention.
Dr. Alex Jimenez’s Insight
After being involved in an auto accident, it may sometimes take days, weeks, even months for symptoms to manifest completely. For your own health and wellness, it’s essential to seek immediate medical attention following the car crash. While many types of injuries can occur, there are several common automobile accident injuries which can develop due to the sheer force of the impact, such as whiplash-associated disorders. Whiplash is a prevalent auto accident injury which is characterized as a type of neck injury which happens when the complex structures surrounding the cervical spine are stretched far beyond their natural range of motion. Chiropractic care is a safe and effective treatment option which can treat a variety of auto accident injuries.
Chiropractic Care After an Automobile Accident
Many healthcare professionals are qualified and experienced�in the treatment of a variety of automobile accident injuries, especially chiropractors. Chiropractic care is a well-known, alternative treatment option which focuses on the diagnosis, treatment and prevention of numerous injuries and/or conditions associated with the musculoskeletal and nervous system. If you’ve been involved in an auto collision, chiropractic care can offer substantial benefits towards your current well-being, supporting your recovery process.
After a car collision, you may experience pain and discomfort, decreased range of motion, stiffness or soreness. Remember that these symptoms may not always manifest immediately after a motor vehicle accident. Through the use of spinal adjustments and manual manipulations, chiropractic care will help you manage painful symptoms, as well as help enhance flexibility, increase strength and improve mobility, promoting a faster recovery. In addition, it can prevent long-term symptoms from developing, such as migraines and chronic pain. The sooner you get chiropractic care after a car wreck, the more likely you are to recover fully.
By carefully restoring the original alignment of the spine, chiropractic care helps reduce pain and other painful symptoms. Furthermore, a chiropractor can recommend a series of exercises and physical activities to help pump oxygen, blood and nutrients to the injury site and enhance recovery. A doctor of chiropractic will develop a personalized treatment program targeted to your specific automobile accident injuries. Chiropractic care also makes it possible to avoid the need for surgical interventions. It strengthens ligaments, tendons and muscles, which shield the body’s structures. It’s also a far more cost-effective solution.
Chiropractic care can also restore function in patients with older vehicle collision injuries. You are still able to benefit from chiropractic care even if you had an accident years back. Employing spinal adjustments and manual manipulations, as well as rehabilitation techniques, it helps relieve old pain and improve function. Additionally, it is a non-invasive treatment option, and you won’t end up needing to rely on pain drugs and/or medications for relief of your symptoms.
Chiropractors can even treat vertigo resulting from a car crash. In as little as one treatment, they could fix a dysfunction in the vestibular system. Other types of chiropractic care treatment techniques include massage, ultrasound, ice and cold treatment, specific exercises and physical activities, and even nutritional advice. Chiropractic care is a safe and effective treatment approach which can help treat automobile accident injuries without the need for drugs and/or medications as well as surgery.
If you suffered a car accident injury, don’t delay any longer. Contact a chiropractor and allow them to help you follow the best treatment path. Chiropractors can provide you a consultation to perform a comprehensive evaluation and make a treatment strategy targeted to your injuries.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Vincent Garcia, an athlete training in mixed martial arts, or MMA, suffered a knee injury and developed turf toe, but that has not stopped him from engaging in his normal training regimen. In order to return to as well as enhance his first physical performance, Vincent Garcia found treatment with Dr. Alex Jimenez, doctor of sports chiropractic. Now recovering from his sports injuries, Vincent Garcia looks forward to regaining his strength, flexibility and freedom to go back to sport.
Sports Injury Chiropractic Treatment
Exercising is important for overall health and wellness, but occasionally, an individual can suffer an injury when playing sports or engaging in physical activities. Accidents, poor training methods, or improper equipment can cause them. Some people today get hurt because they aren’t in shape. Not warming up or stretching enough can also lead to injuries. Treatment often begins with the RICE (Rest, Ice, Compression, and Elevation) method to relieve pain, reduce swelling, and speed recovery. Other possible treatments include pain relievers, rehabilitation, and sometimes surgery, if needed.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine