The spine is made of bones called vertebrae, with the spinal cord running through the spinal canal in the center. The cord is made up of nerves. These nerve roots split from the cord and travel between the vertebrae into various areas of the body. When these nerve roots become pinched or damaged, the symptoms that follow are known as, radiculopathy. El Paso, TX. Chiropractor, Dr. Alexander Jimenez breaks down�radiculopathies,�along with their causes, symptoms and treatment.
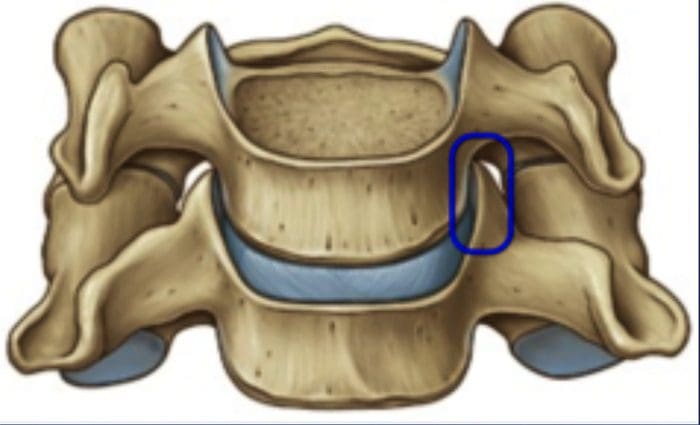
The entire length of the spine, at each level, nerves exit through holes in the bone of the spine (foramen) on each side of the spinal column. These nerves are called nerve roots, or radicular nerves and�branch out from the spine and supply different parts of the body.
Nerves exiting the cervical spine travel down through the arms, hands, and fingers. This is where neck problems affecting a cervical nerve root can cause pain, as well as, other symptoms through the arms and hands, one form of (radiculopathy). Another is low back problems that affect a lumbar nerve root. This can radiate through the leg and into the foot, another form of (radiculopathy, or sciatica), which creates leg pain and/or foot pain.
The spinal cord does not go into the lumbar spine and because the spinal canal has space in the lower back, problems in the lumbosacral region often cause nerve root problems and not a spinal cord injury. Serious conditions i.e. disc herniation or fracture in the lower back are also not likely to cause permanent loss of motor function in the legs.
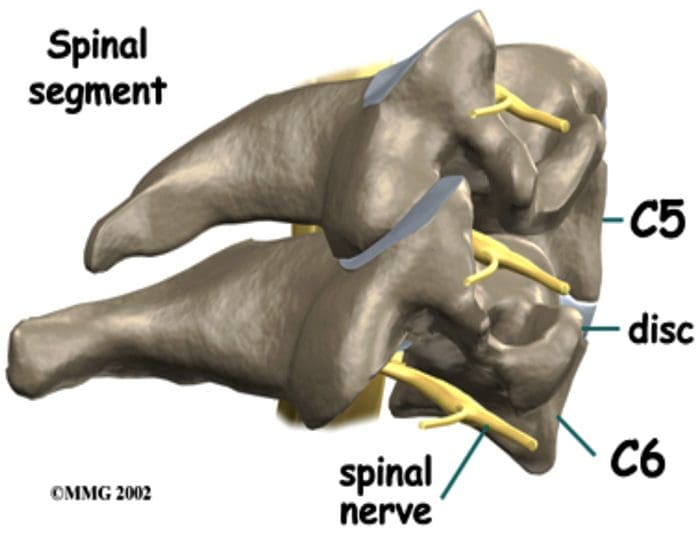
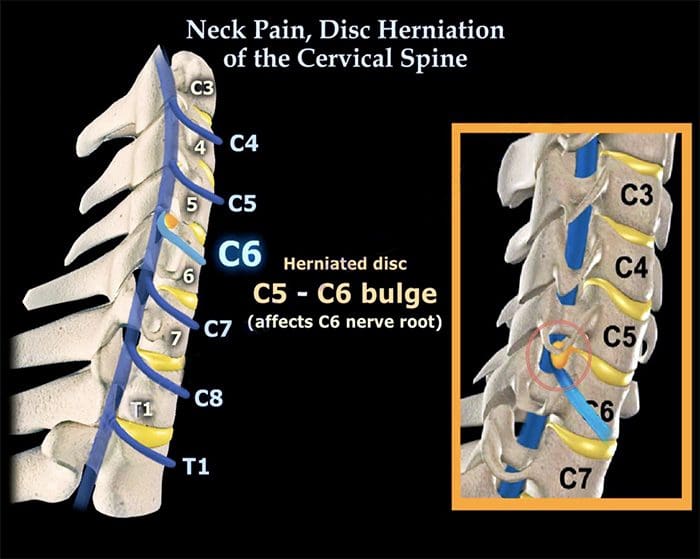
Cervical Spine – This nerve root is named according to the Lower spinal segment that the nerve root runs between.�
Example – The nerve at C5-C6 level is called the C6 nerve root.
It’s named like this because as it exits the spine, it passes Over the C6 pedicle (a piece of bone part of the spinal segment).
Lumbar Spine – These nerve roots are named according to the Upper spinal segment that the nerve runs between.
Example – The nerve at L4-L5 level is called the L4 nerve root.
The nerve root is named this way because as it exits the spine it passes Under the L4 pedicle.
Contents
Two Nerve Roots
Two nerves cross each disc level
Only one exits�the spine (through the foramen) at that level.
Exiting Nerve Root –�This is the nerve root exiting the spine at a certain level.
Example: L4 nerve root exits the spine at L4-L5 level.
Traversing Nerve Root –�This nerve root goes across the disc and exits the spine at the level below.
Example: L5 nerve is the traversing nerve root at L4-L5 level, and is the exiting nerve root at L5-S1 level.
There is some confusion when a nerve root is compressed by disc herniation or other cause to refer both to the intervertebral level (where the disc is) and to the nerve root that is affected. This depends on where the disc herniation or protrusion is happening. It could impinge upon either the exiting nerve�or the traversing nerve.
If The Traversing Nerve Is Affected
Lumbar Radiculopathy
In the lumbar spine, there is a weak area in the disc space right in front of the traversing nerve root, so lumbar discs tend to herniate or leak out and impinge on the traversing nerve.
If The Exiting Nerve Is Affected
Cervical Radiculopathy
The opposite is true in the neck. In the cervical spine, the disc tends to herniate to the side, rather than toward the back and the side. If the disc material herniates to the side, it will compress or impinge the exiting nerve root.
Radiculopathy & Sciatica
Nerve root goes by another name Radicular Nerve, and when a herniated or prolapsed disc presses on a radicular nerve, this is referred to as a radiculopathy. A medical physician might say there is herniated disc at L4-L5, which creates an L5 radiculopathy or an L4 radiculopathy. It all depends on where the disc herniation occurs (the side or the back of the disc) and which nerve is affected. And the term for radiculopathy in the low back is the ever famous Sciatica.
Radiculopathy
A pinched nerve can occur at different areas of the spine (cervical, thoracic or lumbar).
Common causes are narrowing of the hole where the� nerve roots exit, which can result from stenosis, bone spurs, disc herniation and other conditions.
Symptoms vary but often include pain, weakness, numbness and tingling.
Symptoms can be managed with nonsurgical treatment, but minimal surgery can also help.
Prevalence & Pathogenesis
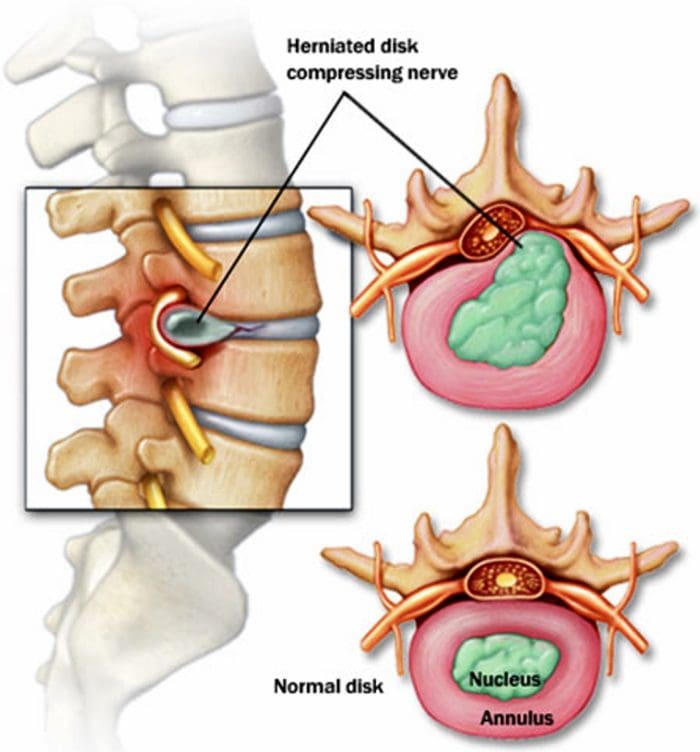
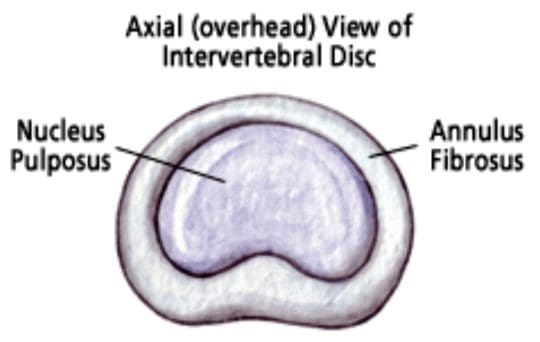
A herniated disc can be defined as herniation of the nucleus pulposus through the fibers of the annulus fibrosus.
Most disc ruptures occur during the third and fourth decades of life while the nucleus pulposus is still gelatinous.
The most likely time of day associated with increased force on the disc is the morning.
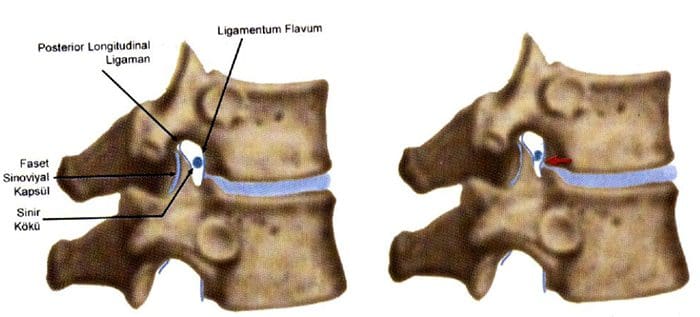
In the lumbar region, perforations usually arise through a defect just lateral to the posterior midline, where the posterior longitudinal ligament is weakest.
Epidemology
Lumbar Spine:
Symptomatic lumbar disc herniation occurs during the lifetime of approximately 2% of the general population.
Approximately 80% of the population will experience significant back pain during the course of a herniated disc.
The groups at greatest risk for herniation of intervertebral discs are younger individuals (mean age of 35 years)
True sciatica actually develops in only 35% of patients with disc herniation.
Not infrequently, sciatica develops 6 to 10 years after the onset of low back pain.
The period of localized back pain may correspond to repeated damage to annular fibers that irritates the sinuvertebral nerve but does not result in disc herniation.
Epidemology
Cervical Spine:
The average annual incidence of cervical radiculopathies is less than 0.1 per 1000 individuals.
Pure soft disc herniations are less common than hard disc abnormalities (spondylosis) as a cause of radicular arm pain.
In a study of 395 patients with nerve root abnormalities, radiculopathies occurred in the cervical and lumbar spine in 93 (24%) and 302 (76%), respectively.
Pathogenesis
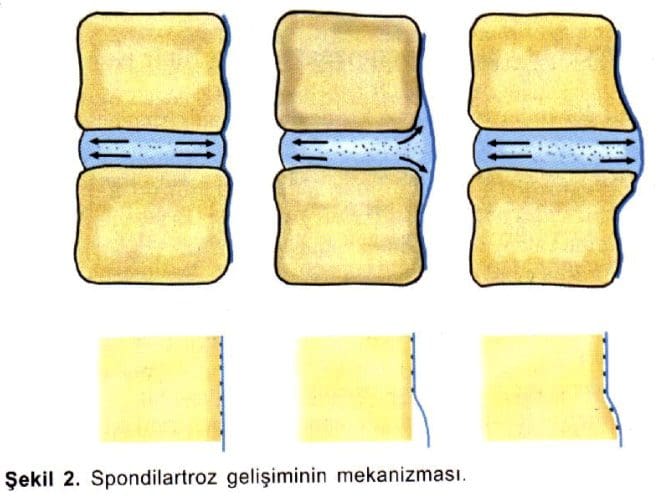
Alterations in intervertebral disc biomechanics and biochemistry over time have a detrimental effect on disc function.
The disc is less able to work as a spacer between vertebral bodies or as a universal joint.
Pathogenesis – LUMBAR SPINE
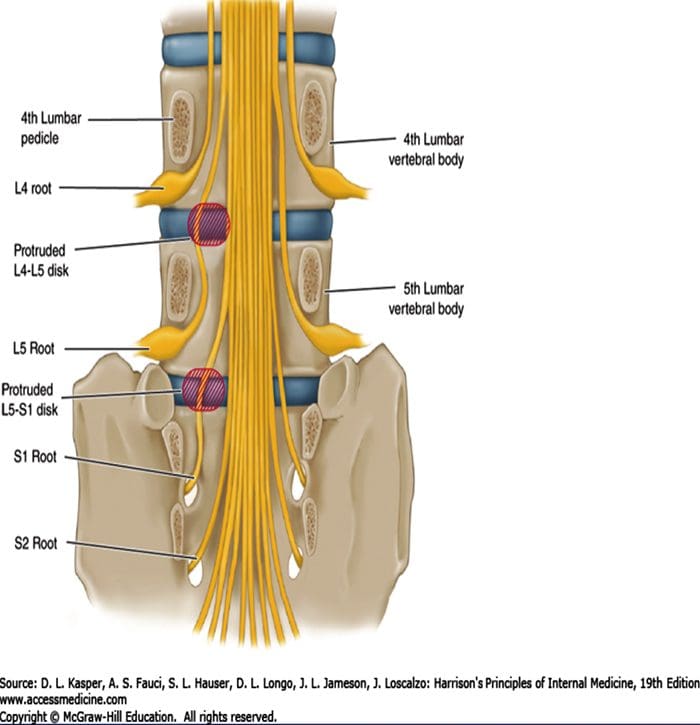
The two most common levels for disc herniation are L4-L5 and L5-S1, which account for 98% of lesions; pathology can occur at L2-L3 and L3-L4 but is relatively uncommon.
Overall, 90% of disc herniations are at the L4-L5 and L5-S1 levels.
Disc herniations at L5-S1 will usually compromise the first sacral nerve root, a lesion at the L4-L5 level will most often compress the fifth lumbar root, and herniation at L3-L4 more frequently involves the fourth lumbar root.
Disc herniation may also develop in older patients.
Disc tissue that causes compression in elderly patients is composed of the annulus fibrosus and and portions of the cartilaginous endplate (hard disc.)
The cartilage is avulsed from the vertebral body.
Resolution of some of the compressive effects on neural structures requires resorption of the nucleus pulposus.
Disc resorption is part of the natural healing process associated with disc herniation.
The enhanced ability to resorb discs has the potential for resolving clinical symptoms more rapidly.
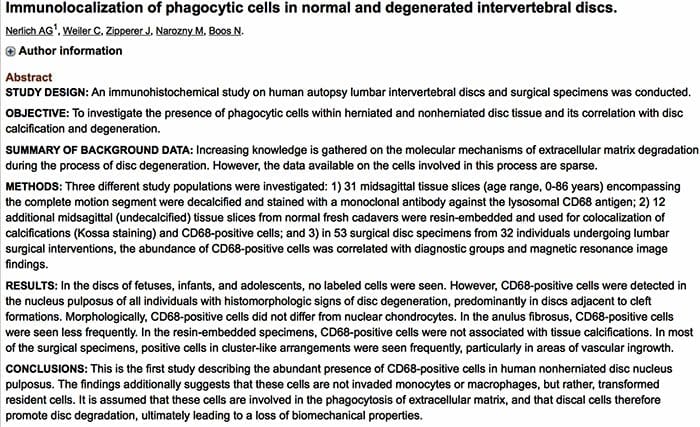
Resorption of herniated disc material is associated with a marked increase in infiltrating macrophages and the production of matrix metalloproteinases (MMPs) 3 and 7.
Nerlich and associates identified the origins of phagocytic cells in degenerated intervertebral discs.
The investigation identified cells that are transformed local cells rather than invaded macrophages.
Degenerative discs contain the cells that add to their continued dissolution.
Pathogenesis – CERVICAL SPINE
In the early 1940s, a number of reports appeared in which cervical intervertebral disc herniation with radiculopathies was described.
There is a direct correlation between the anatomy of the cervical spine and the location and pathophysiology of disc lesion.
The eight cervical nerve roots exit via intervertebral foramina that are bordered anteromedially by the intervertebral disc and posterolaterally by the zygapophyseal joint.
The foramina are largest at C2-C3 and decrease in size until C6-C7.
The nerve root occupies 25% to 33% of the volume of the foramen.
The C1 root exits between the occiput and the atlas (C1)
All lower roots exit above their corresponding cervical vertebrae (the C6 root at the C5-C6 interspace), except C8, which exits between C7 and T1.
A differential growth rate affects the relationship of the spinal cord and nerve roots and the cervical spine.
Most acute disc herniations occur posterolaterally and in patients around the forth decade of life, when the nucleus is still gelatinous.
The most common areas of disc herniations are C6-C7 and C5-C6.
C7-T1 and C3-C4 disc herniations are infrequent ( less than 15 %).
Disc herniation of C2-C3 is rare.
Patients with upper cervical disc protrusions in the C2-C3 region have symptoms that include suboccipital pain, loss of hand dexterity, and paresthesias over the face and unilateral arm.
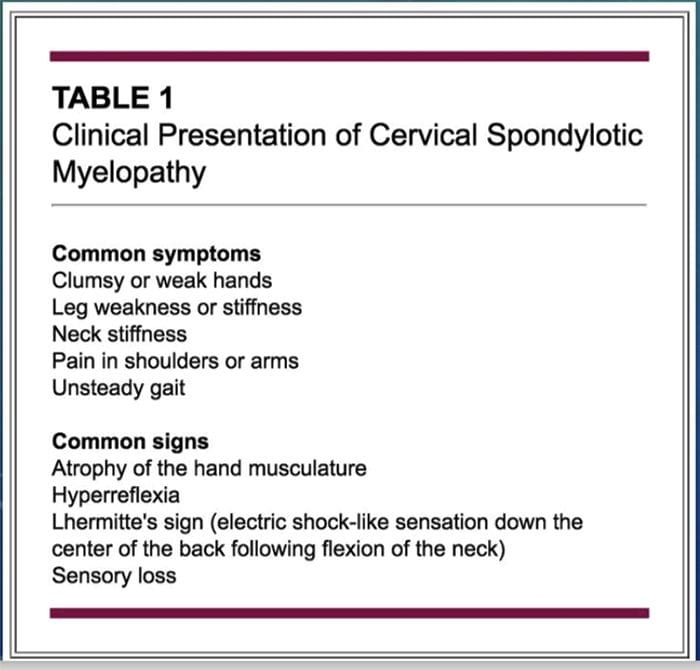
Unlike lumbar herniated discs, cervical herniated discs may cause myelopathy in addition to radicular pain because of the anatomy of the spinal cord in the cervical region.
The uncovertebral prominences play a role in the location of ruptured discs material.
The uncovertebral joint tends to guide extruded disc material medially, where cord compression may also occur.
Disc herniations usually affect the nerve root numbered most caudally for the given disc level; for example, the C3 � C4 disc affects the fourth cervical nerve root; C4- C5, the fifth cervical nerve root; C5 � C6, the sixth cervical nerve root; C6 � C7, the seventh cervical nerve root; and C7 � T1, the eighth cervical nerve root.
Not every herniated disc is symptomatic.
The development of symptoms depends on the reserve capacity of the spinal canal, the presence of inflammation, the size of the herniation, and the presence of concomitant disease such as osteophyte formation.
In disc rupture, protrusion of nuclear material results in tension on the annular fibers and compress?on of the dura or nerve root causing pain.
Also important is the smaller size of the sagittal diameter, the bony cervical spinal canal.
Individuals in whom a cervical herniated disc causes motor dysfunction have a complication of cervical disc herniation if the spinal canal is stenotic.
Clinical History – LUMBAR SPINE
Clinically, the patient�s major complaint is a sharp, lancinating pain.
In many cases there may be a previous history of intermittent episodes of localized low back pain.
The pain not only in the back but also radiates down the leg in the anatomic distribution of the affected nerve root.
It will usually be described as deep and sharp and progressing from above downward in the involved leg.
Its onset may be insidious or sudden and associated with a tearing or snapping sensations of the spine.
Occasionally, when sciatica develops, the back pain may resolve because once the annulus has ruptured, it may no longer be under tension.
Disc herniation occurs with sudden physical effort when the trunk is flexed or rotated.
On occasion, patients with L4-L5 disc herniation have groin pain. In a study of 512 lumbar disc patients, 4.1% had groin pain.
Finally, the sciatica may vary in intensity; it may be so severe that patients will be unable to ambulate and they will feel that their back is “locked”.
On the other hand, the pain may be limited to a dull ache that increases in intensity with ambulation.
Pain is worsened in the flexed position and relieved by extension of the lumbar spine.
Characteristically, patients with herniated discs have increased pain with sitting, driving, walking, couching, sneezing, or straining.
Clinical History – CERVICAL SPINE
Arm pain, not neck pain, is the patient� s major complaint.
The pain is often perceived as starting in the neck area and then radiating from this point down to shoulder, arm and forearm and usually into the hand.
The onset of the radicular pain is often gradual, although it can be sudden and occur in association with a tearing or snapping sensation.
As time passes, the magnitude of the arm pain clearly exceeds that of the neck or shoulder pain.
The arm pain may also be variable in intensity and preclude any use of the arm; it may range from severe pain to a dull, cramping ache in the arm muscles.
The pain is usually severe enough to awaken the patient at night.
Additionally, a patient may complain of associated headaches as well as muscle spasm, which can radiate from the cervical spine to below the scapulae.
The pain may also radiate to the chest and mimic angina (pseudoangina) or to the breast.
Symptoms such as back pain, leg pain, leg weakness, gait disturbance, or incontinence suggest compression of the spinal cord (Myelopathy).
Physical Examination – LUMBAR SPINE
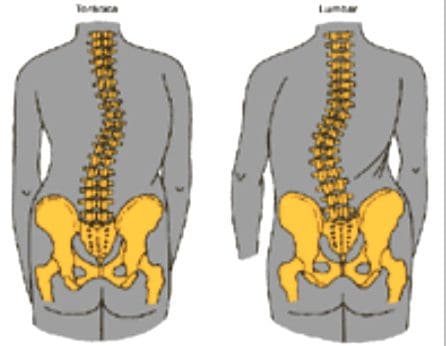
Physical examination will demonstrated a decrease in range of motion of the lumbosacral spine, and patients may list to one side as they try to bend forward.
The side of the disc herniation typically corresponds to the location of the scoliotic list.
However, the specific level or degree of herniation does not correlate with the degree of list.
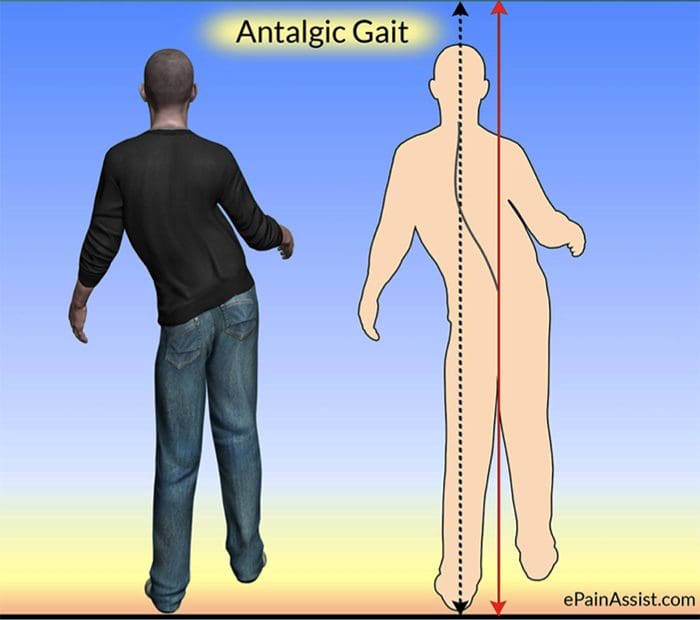
On ambulation, patients walk with an antalgic gait in which they hold the involved leg flexed so that they put as little weight as possible on the extremity.
Neurologic Examination:
The neurologic examination is very important and may yield objective evidence of nerve root compression (We should evaluate of reflex testing, muscle power, and sensation examination of the patient).
In addition, a nerve deficit may have little temporal relevance because it may be related to a previous attack at a different level.
Compression of individual spinal nerve roots results in alterations in motor, sensory, and reflex function.
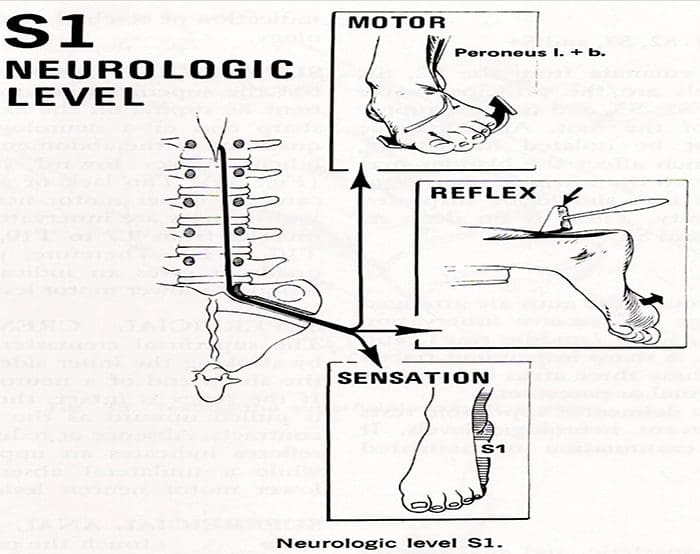
When the first sacral root is compressed, the patient may have gastrocnemius-soleus weakness and be unable to repeatedly raise up on the toes of that foot.
Atrophy of the calf may be apperent, and the ankle (Achilles) reflex is often diminished or absent.
Sensory loss, if present, is usually confined to the posterior aspect of the calf and the lateral side of the foot.
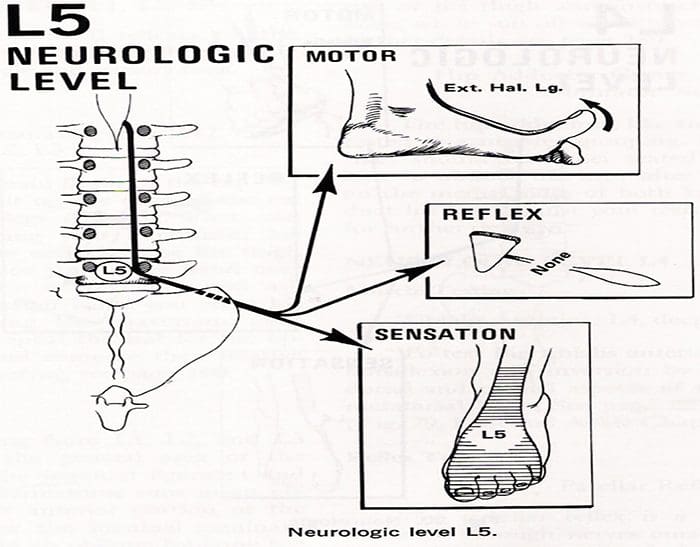
Involvement of the fifth lumbar nerve root can lead to weakness in extension of the great toe and, in a few cases, weakness of the everters and dorsiflexors of the foot.
A sensory deficit can appear over the anterior of the leg and the dorsomedial aspect of the foot down to the big toe
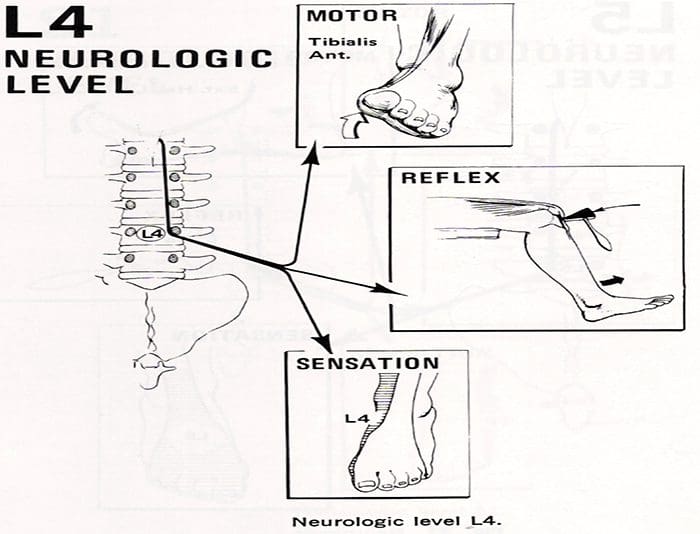
With compression of the fourth lumbar nerve root, the quadriceps muscle is affected; the patient may note weakness in knee extension, which is often associated with instability.
Atrophy of the thigh musculature can be marked. Sensory loss may be apparent over the anteromedial aspect of the thigh, and the patellar tendon reflex can be diminished.
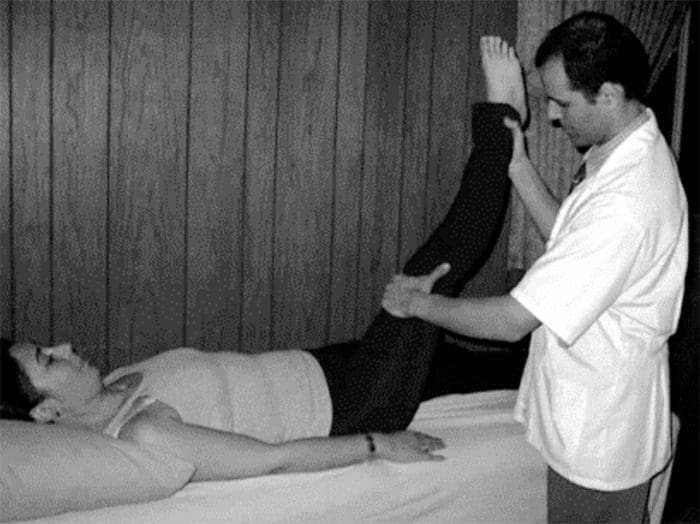
Nerve root sensitivity can be elicited by any method that creates tension.
The straight leg-raising (SLR)test is the one most commonly used.
This test is performed with the patient supine.
Physical Examination – CERVICAL SPINE
Neurologic Examination:
A neurologic examination that shows abnormalities is the most helpful aspect of the diagnostic work-up, although the examination may remain normal despite a chronic radicular pattern.
The presence of atrophy helps document the location of the lesion, as well as its chronicity.
The presence of subjective sensory changes is often difficult to interpret and requires a coherent and cooperative patient to be of clinical value.
When the third cervical root is compressed, no reflex change and motor weakness can be identified.
The pain radiates to the back of the neck and toward the mastoid process and pinna of the ear.
Involvement of the fourth cervical nerve root leads to no readily detectable reflex changes or motor weakness.
The pain radiates to the back of the neck and superior aspect of the scapula.
Occasionally, the pain radiates to the anterior chest wall.
The pain is often exacerbated by neck extension.
Unlike the third and the fourth cervical nerve roots, the fifth through eighth cervical nerve roots have motor functions.
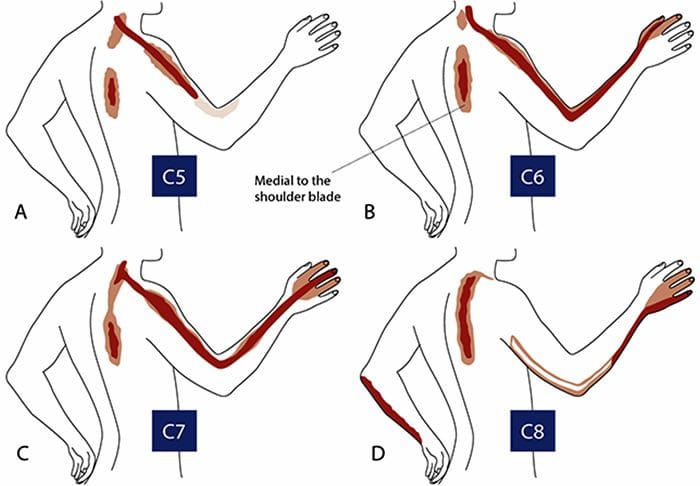
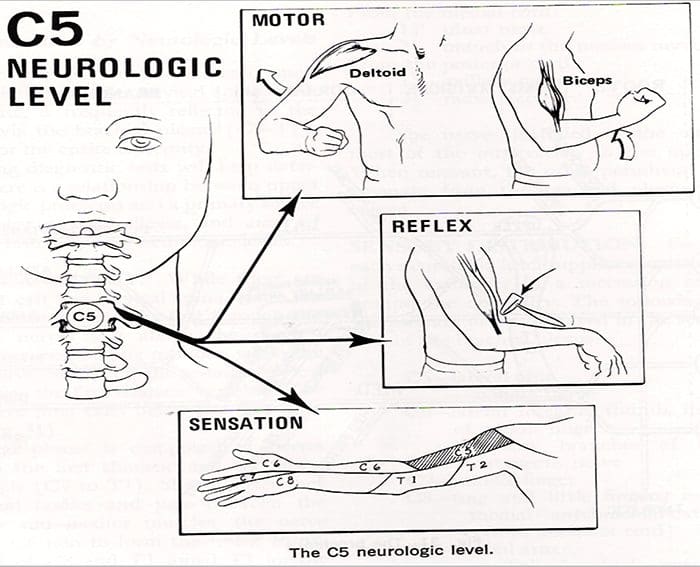
Compression of the fifth cervical nerve root is characterized by weakness of shoulder abduction, usually above 90 degree, and weakness of shoulder extension.
The biceps reflexes are often depressed and the pain radiates from the side of the neck to the top of the shoulder.
Decreased sensation is often noted in the lateral aspect of the deltoid, which represents the autonomous area of the axillary nerve.
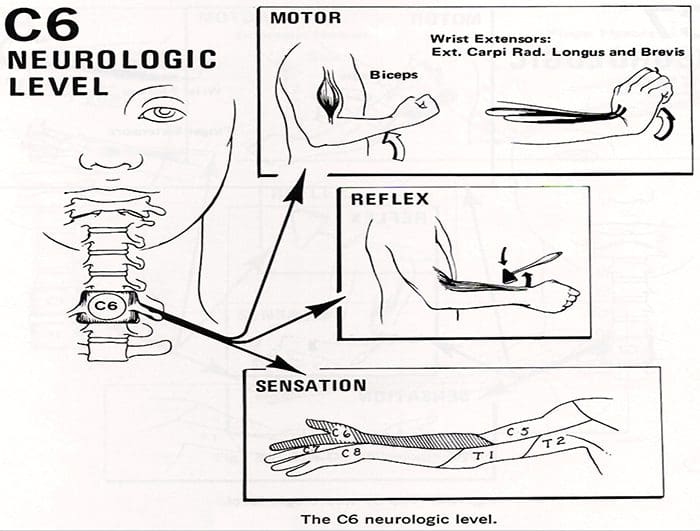
Involvement of the sixth cervical nerve root produces biceps muscles weakness as well as diminished brachioradial reflex.
The pain again radiates from the neck down the lateral aspect of the arm and forearm to the radial side of hand (index finger, long finger, and thumb).
Numbness occurs occasionally in the tip of the index finger, the autonomous area of the sixth cervical nerve root.
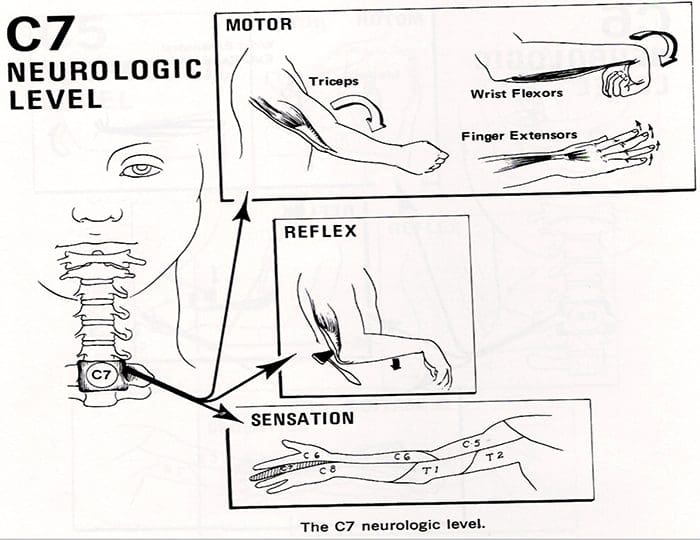
Compression of the seventh cervical nerve root produces reflex changes in the triceps jerk test with associated loss of strength in the triceps muscles, which extend the elbow.
The pain from this lesion radiates from the lateral aspect of the neck down the middle of the area to the middle finger.
Sensory changes occur often in the tip of the middle finger, the autonomous area for the seventh nerve.
Patients should also be tested for scapular winging, which may occur with C6 or C7 radiculopathies.
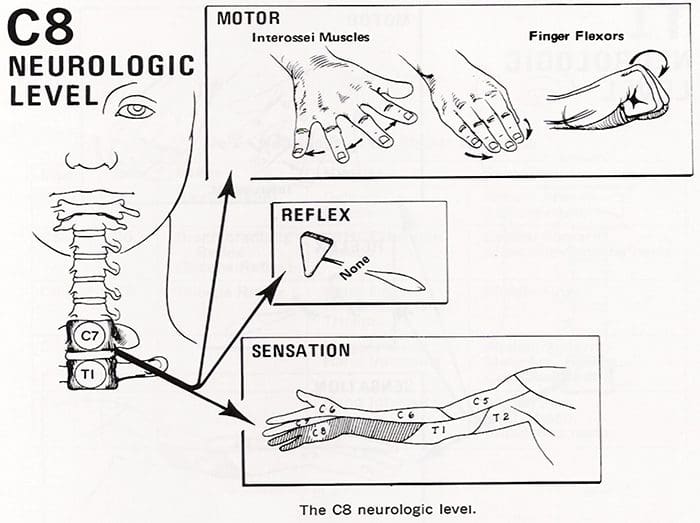
Finally, involvement of the eighth cervical nerve root by a herniated C7-T1 disc produces significant weakness of the intrinsic musculature of the hand.
Such involvement can lead to rapid atrophy of the interosseous muscles because of the small size of these muscles.
Loss of the interossei leads to significant loss of fine hand motion.
No reflexes are easily found, although the flexor carpi ulnaris reflex may be decreased.
The radicular pain from the eighth cervical nerve root radiates to the ulnar border the hand and the ring and little fingers.
The tip of the little finger often demonstrates diminished sensation.
Radicular pain secondary to a herniated cervical disc may be relieved by abduction of the affected arm.
Although these signs are helpful when present, their absence alone does not rule out a nerve root lesion.
Laboratory Data
Medical screening laboratory test (blood counts, chemistry panels erythrocyte sedimentation rate [ESR]) are normal in patients with a herniated disc.
Electro diagnostic Testing
Electromyography(EMG)is an electronic extension of the physical examination.
The primary use of EMG is to diagnose radiculopathies in cases of questionable neurologic origin.
EMG findings may be positive in patients with nerve root impingement.
Radiographic Evaluation – LUMBAR SPINE
Plain x-rays may be entirely normal in a patient with signs and symptoms of nerve root impingement.
Computed Tomography
Radigraphic evaluation by CT scan may demonstrate disc bulging but may not correlate with the level of nerve damage.
Magnetic Resonance Imaging
MR imaging also allows visualization of soft tissues, including discs in the lumbar spine.
Herniated discs are easily detected with MR evaluation.
MR imaging is a sensitive technique for the detection of far lateral and anterior disc herniations.
Radiographic Evaluation – CERVICAL SPINE
X-rays
Plain x-rays may be entirely normal in patients wit han acute herniated cervical disc.
Conversely,�70% of asymptomatic women and 95% of asymptomatic men between the ages of 60 and 65 years have evidence of degenerative disc disease on plain roentgenograms.
Views to be obtained include anteroposterior, lateral, flexion, and extension.
Computed Tomography
CT permits direct visualization of compression of neural structures and is therefore more precise than myelography.
Advantages of CT over myelography include better visualization of lateral abnormalities such as foraminal stenosis and abnormalities caudal to the myelographic block, less radiation exposure, and no hospitalization.
Magnetic Resonance
MRI allows excellent visualization of soft tissues, including herniated discs in the cervical spine.
The test is noninvasive.
In a study of 34 patients with cervical lesions, MRI predicted 88% of the surgically proven lesions versus 81% for myelography-CT, 58% for myelography, and 50% for CT alone.
Differential Diagnosis – LUMBAR SPINE
The initial diagnosis of a herniated disc is ordinarily made on the basis of the history and physical examination.
Plain radiographs of the lumbosacral spine will rarely add to the diagnosis but should be obtained to help rule out other causes of pain such as infection or tumor.
Other tests such as MR, CT, and myelography are confirmatory by nature and can be misleading when used as screening tests.
Spinal Stenosis
Patient with spinal stenosis may also suffer from back pain that radiates to the lower extremities.
Patients with spinal stenosis tend to be older than those in whom herniated discs develop.
Characteristically, patients with spinal stenosis experience lower extremity pain (pseudoclaudication=neurogenic claudication) after walking for an unspecified distance.
They also complain of pain that is exacerbated by standing or extending the spine.
Radiographic evaluation is usually helpful in differentiating individuals with disc herniation from those with bony hypertrophy associated with spinal stenosis.
In a study of 1,293 patients, lateral spinal stenosis and herniated intervertebral discs coexisted in 17.7% of individuals.
Radicular pain may be caused by more than one pathologic process in an individual.
Facet Syndrome
Facet syndrome is another cause of low back pain that may be associated with radiation of pain to structures outside the confines of the lumbosacral spine.
Degeneration of articular structures in the facet joint causes pain to develop.
In most circumstances, the pain is localized over the area of the affected joint and is aggravated by extension of the spine (standing).
A deep , ill-defined, aching discomfort may also be noted in the sacroiliac joint, the buttocks, and the legs.
The areas of sclerotome affected show the same embryonic origin as the degenerated facet joint.
Patients with pain secondary to facet joint disease may have relief of symptoms with apophyseal injection of a long-acting local anesthetic.
The true role of facet joint disease in the production of back and leg pain remains to be determined.
Other mechanical causes of sciatica include congentenial abnormalites of the lumbar nerve roots, external compression of the sciatic nerve (wallet in a back pants pocket), and muscular compression of the nerve (piriformis syndrome).
In rare circumstances, cervical or thoracic lesion should be considered if the lumbar spine is clear of abnormalities.
Medical causes of sciatica (neural tumors or infections, for example) are usually associated with systemic symptoms in addition to nerve pain in a sciatic distribution.
Differential Diagnosis – CERVICAL SPINE
No diagnostic criteria exist for the clinical diagnosis of a herniated cervical disc.
The provisional diagnosis of a herniated cervical disc is made by the history and physical examination.
The plain x-ray is usually nondiagnostic, although occasionally disc space narrowing at the suspected interspace or foraminal narrowing on oblique films is seen.
The value of x-rays is to exclude other causes of neck and arm pain, such as infection and tumor.
MR imaging and CT-myelography are the best confirmatory examinations for disc herniation.
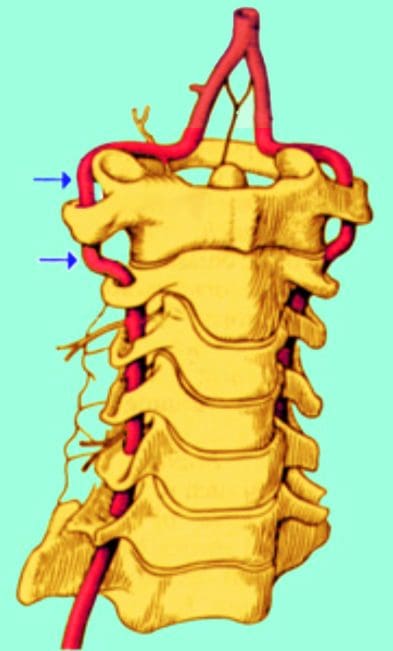
Cervical disc herniations may affect structures other than nerve roots.
Disc herniation may cause vessel compression (vertebral artery) associated with vertebrobasilar artery insufficiency and be manifested as blurred vision and dizziness.
Other mechanical causes of arm pain should be excluded.
The most common is some form of compression on a peripheral nerve.
Such compression can occur at the elbow, forearm, or wrist. An example is compression of the median nerve by the carpal ligament leading to carpal tunnel syndrome.
The best diagnostic test to rule out these peripheral neuropathies is EMG.
Excessive traction on the arm secondary to heavy weights may cause radicular pain without disc compression of nerve roots.
Spinal cord abnormalities must be considered if signs of myelopathy are present in conjunction with radiculopathies.
Spinal cord lesions such as syringomyelia are identified by MRI, and motor neuron disease is identified by EMG.
Multiple sclerosis should be considered in a patient with radiculopathies if the physical signs indicate lesions above the foramen magnum (optic neuritis).
In very rare circumstances, lesions of the parietal lobe corresponding to the arm can mimic the findings of cervical radiculopathies.
For people struggling to control their blood glucose levels, the most common concern is, how can you regulate blood sugar levels? Maintaining healthy blood sugar levels can be complicated and unyielding. Along with food and beverages, our blood sugar levels fluctuate in response to a huge variety of unique factors. Exercise, psychological stress, the previous night’s rest, and genetics all play a role in the human body’s effort to closely regulate the degree of glucose circulating in the blood. Additionally, no matter whether or not somebody has a blood glucose dysregulation problem or full-blown diabetes, that morning meal we call breakfast actually sets the stage for your day.
What is often known as the “Dawn Phenomenon” occurs between 4:00 AM to 8:00 AM when the human body produces sufficient amounts of glucagon, cortisol and epinephrine to boost blood glucose as a natural procedure before waking up in the morning. And science supports those people who prefer to eat a hearty breakfast as soon as they wake up. One study that monitored the sugar profiles of healthy people during the day saw that the largest increase in blood glucose occurs right after breakfast. Just about every nutritionist, dietitian and endocrinologist recommends eating a high-protein breakfast so as to restrain the naturally-occurring spike in sugar during the daytime. As mentioned previously, these meals, as well as other variables, will dictate the difference in blood glucose levels throughout the day, which directly impacts the way the human body works and an individual’s overall awareness of their health and wellness.
Contents
When Maintaining Healthy Blood Sugar Levels is Difficult
A consistently higher blood sugar level has a deleterious impact on organ function. Risks for diabetes, further heart disease, stroke, kidney disorders, vision impairment and cardiovascular issues that can result in infections and amputation of recurrence increase when blood sugar is uncontrolled. Intense oscillations in blood sugar may stem from many hormonal imbalances, specifically where there is a lack of insulin manufacturing, as in the case of type I diabetes, or an inability to use insulin correctly, commonly referred to as insulin resistance. Either type of diabetes is recognized and monitored with many evaluations, but the most prevalent one is the HbA1C. As a mark of longer-term glucose levels, the HbA1C suggests the average proportion of the particular hemoglobin subtype A1C that has glucose bound to it, glycated or glycosylated, producing a glycoprotein. Since hemoglobin cells normally die off after 120 days, this process firmly reflects the typical plasma glucose level over in the past 90 days. This diagnostic tool proves more helpful than a diagram of blood sugar, which shows great vacillations through the day. Individuals with diabetes or more lengths of hyperglycemia, as noticed in patients diagnosed with metabolic syndrome, have increased HbA1C levels. It’s projected that in 2015 over 7 million cases of diabetes and insulin resistance went undiagnosed. The famed incidence of those conditions is alarming as the trend is nearing 10 percent of the populace.
Regulating Blood Glucose Levels with Nutrition
Though genetics�are not something people can control, nutrition, diet and other lifestyle variables are within your reach. Eating a balanced diet of low-glycemic, high fiber, and also low-saturated fat meals is recommended for individuals with glycemic control health issues. Combining foods which contain all three macronutrients, such as proteins, fats, and carbohydrates, can also be valuable in regulating blood glucose levels. This list of foods provides a wonderful start to a healthy diet and a platform for preventing those wild swings in sugar throughout the day:
All colors and varieties of fresh fruits and vegetables
Legumes, such as kidney beans, black beans, chickpeas, and lentils
Whole grains, such as brown rice, quinoa, barley, and millet
Olive oil
Tomatoes
Fermented, organic and raw dairy
Cold-water wild fish, such as salmon, mackerel and sardines
Tempeh, tofu and natto
Cage-free, organic eggs
Green and black tea
Supplemental nutrients and botanicals to help encourage wholesome glucose levels and supply a hypoglycemic effect are currently being studied and comprise of:
Magnesium
Chromium, as chromium picolinate
Vanadium
Alpha lipoic acid
Gymnema sylvestre
Fenugreek
Bitter melon
Cinnamon
Berberine
Berberine functions on multiple fronts. It was found to substantially improve glucose levels by an average of 9.5 percent down to 7.5 percent, as effective as metformin from 9.15 percent down to 7.7 percent, in a research study to find out its effectiveness and safety in type 2 diabetes patients. Furthermore, it had the effect of enhancing both entire cholesterol and low-density lipoprotein cholesterol in the evaluation and analysis.
Dr. Alex Jimenez’s Insight
Diabetes has become one of the fastest growing diseases in the United States, where it is prevalent among both children and adults. With the increase in cases each year, the numbers of individuals seeking treatment and a potential cure are also rising. Fortunately, research studies have found that maintaining healthy blood sugar levels can help stabilize a case of diabetes. Proper nutrition, as well as natural remedies and botanicals, including alternative treatment options, such as chiropractic care, have been determined to help regulate healthy blood glucose levels, improving an individual’s quality of life.
While there are many other ways in which healthy blood sugar levels can be achieved, recent research studies have also determined that chiropractic care may be able to control blood sugar levels, potentially regulating type 2 diabetes. According to these, the key to managing blood glucose levels can be found in the connection between the central nervous system and blood sugar levels in the human body. Chiropractic care focuses on the use of spinal adjustments and manual manipulations to correct spinal misalignments, or subluxations. It has been demonstrated that spinal misalignments, or subluxations, can interfere with important communications signals from the brain to the spinal chords as well as the rest of the body. By carefully restoring the natural integrity of the spine, chiropractors can help regulate healthy blood sugar levels and improve overall health and wellness.
Sleep disorders, such as obstructive sleep apnea, commonly related to obesity and metabolic syndrome, can hinder good quality sleep, and also have been considered as a risk factor for diabetes. Although there isn’t any clearly defined correlation between sleep and glucose control, there are multiple pathways involved together with a cascade of metabolic functions which could result in metabolic derangements when disturbed.
To remain steady on what could be a roller coaster ride of blood sugars, a high priority should be given to a well-balanced diet plan, replete with proper nutrition and supplementation, and the close observation of lifestyle and genetic aspects. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Research has found about 35% of Americans experience symptoms of a warning stroke. However, only 3% seek out immediate medical attention. A stroke occurs when the blood supply to part of the brain is blocked or reduced, which deprives brain tissue of oxygen and nutrients. Within minutes, brain cells start to die.
Adults who have had a sign of a�temporary blockage aka, a Transient Ischemic Attack (TIA)waited/rested until symptoms had subsided instead of calling 911. This is according to the research from the American Heart Association/American Stroke Association (AHA/ASA).
Only a formal medical diagnosis with brain imaging can determine whether someone is having a TIA or stroke. If you or someone experiences warning signs that come on suddenly or go away,�CALL 911 IMMEDIATELY!
Contents
Stroke: Early Signs
Ischemic strokes occur when a clot blocks blood flow to the brain.
This type may be treated immediately with a special clot-busting drug
A device called a stent retriever may also be used to remove the clot and help prevent long-term disability.
TIA precedes about 15% of strokes
People who have had TIA are at greater risk for stroke within three months
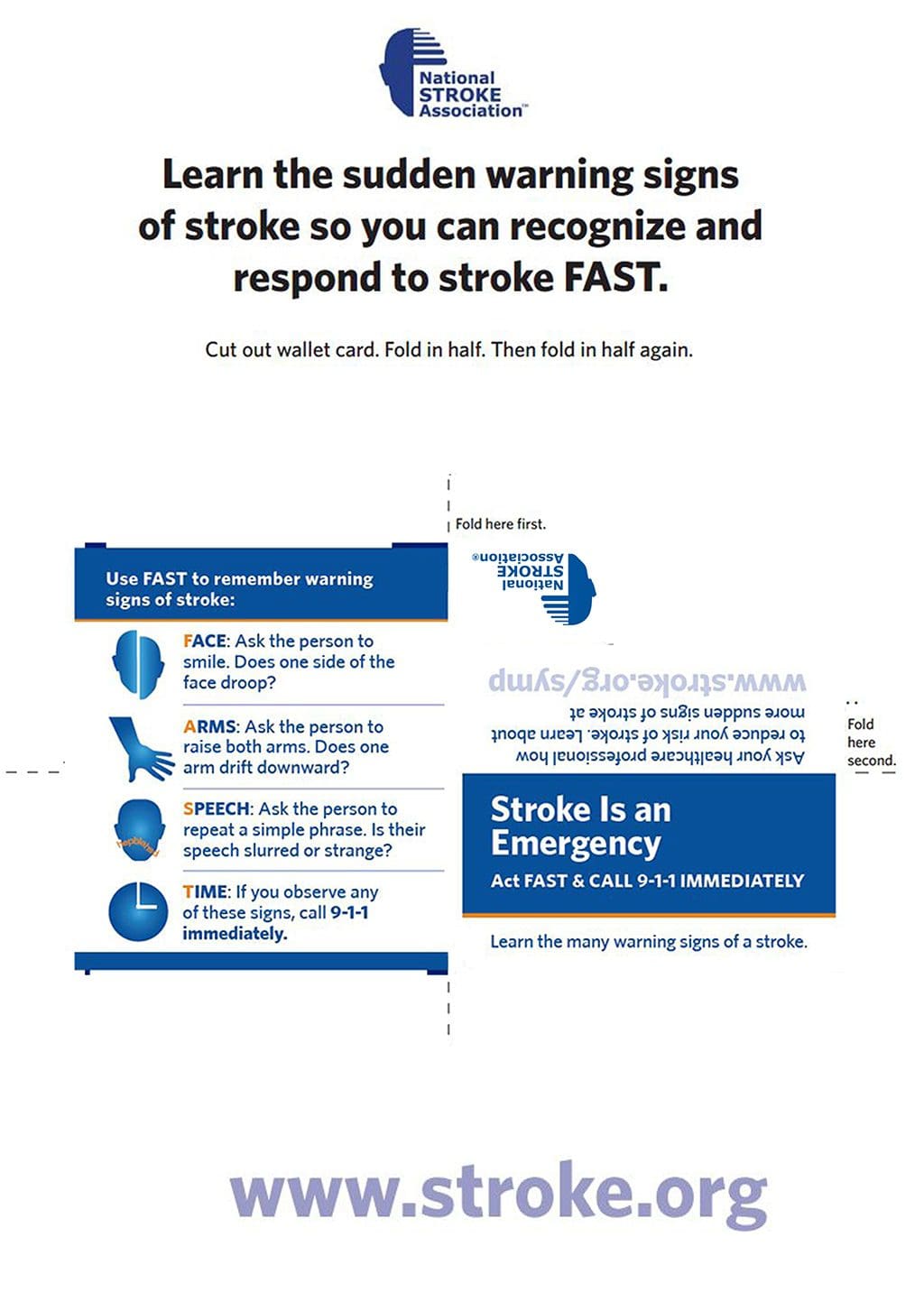
Use The Acronym F.A.S.T. To Help Remember Common Signs:
�
Face Drooping
Arm Weakness
Speech Difficulty
Time To Call 911
Other Warnings Signs:
Confusion
Dizziness
Loss Of Balance/Coordination
Numbness Or Weakness Of Face, Arm or Leg, Particularly On One Side Of The Body
Trouble Speaking Or Understanding
Trouble Walking
Unexplained Severe Headache
Vision Loss In One Or Both Eyes
Injury Medical Clinic: Stress Management Care & Treatments
How important is nutrition for our brain health? In the current work force, we are continuously stressed, often forced to finish tasks faster in order to meet ever so demanding deadlines. In addition, we are expected to maintain our optimal mental health, as this can be an essential�part towards delivering quality work. When our mental health is being affected by our hectic lifestyles, however, several practices which can help you start thinking more clearly can include sleeping properly, controlling stress, and even taking nutritional supplements for your brain health.
One nutritional supplement which has been widely recognized for its ability to boost brain health is curcumin, the active ingredient found in turmeric. Well-known for its antioxidant properties and its capacity to control inflammation in the human body, this powerful herb can also promote good mood and cognition. Another specific group which has reported significant benefits with the increased use of curcumin, is the elderly population. Below, we will discuss how curcumin can help boost brain health as well as demonstrate additional benefits this golden gem can have on our overall health and wellness.
Contents
Curcumin: a Golden Gem for Brain Health
In accordance with the Journal of Pharmacology, curcumin is made-up of a variety of substances which can encourage biological mechanisms that counteract age-related cognitive decline, dementia, or mood disorders. One randomized, double-blind, placebo-controlled trial analyzed the acute, of approximately 1 and 3 hours following a single dose, chronic, of approximately 4 weeks, and acute-on-chronic, of approximately 1 and 3 hours after one dose subsequently after chronic treatment, consequences of a curcumin formulation on cognitive function, mood, and blood biomarkers in 60 healthy adults ranging from the 60 to 85 years of age. After about one hour of application, the curcumin had considerably enhanced the participant’s functionality on attention and working memory tasks, in comparison with the placebo. Working memory and mood, which included general fatigue, change in calmness, contentedness and fatigue triggered by emotional strain were fundamentally improved following chronic therapy.
Curcumin boosts BDNF (brain-derived neurotrophic factor), the brain hormone which helps boost the development of new neurons that are in charge of improving memory and learning as well as supplying a substantial option for countering the aging brain. Additionally, this powerful ingredient increases blood circulation to the brain, also providing a much better attention span for greater work productivity.
Appreciating its anxiolytic effects can be one of the greatest benefits of carrying curcumin. According to the Journal of Clinical Psychopharmacology, a randomized double-blinded and double-blind trial with 60 subjects experiencing stress-related symptoms, including exhaustion, were to get routine curcumin nutritional supplements, and placebo for 30 days. The results indicated a greater quality of life, and diminished stress and fatigue for those receiving regular curcumin intakes. This progressive compound is believed to be able to help alleviate depression by altering the release of dopamine and serotonin, two powerful hormones which help keep the human mind and body at ease. Curcumin also promotes the optima health and wellness of inflammation pathways from the brain, which ultimately will help improve energy, mood, and production levels.
Curcumin may additionally promote cognition via its powerful antioxidant action which improves the bioavailability of DHA, the potent omega-3 fatty acid demonstrated to boost brain health. A research study in the American Journal of Geriatric Psychiatry revealed that curcumin really does protect the brain from neurodegeneration. The evaluation and analysis included 40 participants ranging from the ages of 51 to 84 years of age. Each individual subject consumed 90mg of curcumin twice per day or placebo for 18 weeks. The results indicated enhanced long-term healing, visual memory, and focus. With its tremendous medicinal properties, curcumin can also support neuroplasticity, which empowers the brain to change and fortify itself even through the natural degeneration with aging.
Curcumin can also promote anti-seizure action. With its antioxidant properties, this golden gem can help slow down reactive astrocyte expression, which helps cells survive within the mind. According to the Neuropharmacology Laboratory, Department of Pharmacology, the antioxidant properties of curcumin helped alleviate migraines, cognitive impairment, and cognitive stress in rats. A dental pre-treatment of curcumin was given to male rats which were additionally treated together with Pentylenetrazole, or PZT, every other day. The study demonstrated that curcumin enhanced the seizure score and indicated a diminished amount of myoclonic jerks. Furthermore, the outcome measures of the research study demonstrated that curcumin restructures seizures, oxidative stress, and brain function. Moreover, it helps protect memory function which may also be jeopardized by seizure activity.
Using its capability to strengthen fatty acids in the mind, curcumin helps athletes achieve better physical performance by boosting critical thinking, improving problem solving, and developing improved choices. The neuroprotective properties in curcumin also help regenerate tissues. In reality, based on Stem Cell Research and Therapy, a research study was conducted between the effects of curcumin on endogenous stem cells which were impartial. The study demonstrated that curcumin played an essential role in the healing of cells from combating the activation of microglia cells. Scientists in the Institute of Neuroscience and Medicine in Julich, Germany, observed the effects of impartial stem cell generation. During a 72-hour period, the evaluation and analysis demonstrated and indicated that the turmeric curcumin improved cellular generation by up to 80 percent. This shows how powerful curcumin could be for successful brain health function.
Dr. Alex Jimenez’s Insight
Nutrition is a fundamental factor in overall health and wellness. In today’s stressful world, however, it can often become difficult to eat a proper meal, let alone making sure we are taking in all the necessary nutrients we require on a regular basis. That, plus the added pressure of the workforce can have detrimental effects on our brain health. Dietary supplements, such as curcumin, have been demonstrated to have tremendous benefits on brain health. Although we may not always have the “free time” to sit down and have a properly balanced meal, taking nutritional supplements like curcumin, among others, can help improve the human body’s general well-being.
While many research studies have found that natural remedies and botanicals, such as dietary supplements apart from vitamins and minerals, continue to be the most common complementary health approach in the United States today, more and more alternative treatment options, such as chiropractic care, have started to incorporate these into their practices. As a matter of fact, a majority of chiropractors give nutritional advice, as well as recommendations for other lifestyle recommendations, as a general part of their treatment plan. Because chiropractic care is based on the notion of naturally treating the human body as a whole, enhancing it’s own healing properties without the use of drugs and/or medications as well as other invasive procedures, this healthcare profession relies on offering the necessary health maintenance components for optimal health and wellness. These components can include nutrition, water, rest, exercise, and clean air. Many chiropractors also offer curcumin supplements to help promote recovery.
This exceptional nutritional supplement, curcumin, helps improve mental clarity, improve cognition, improve endurance, and supplies anxiolytic benefits. Whether it’s more work fabricating, or a much better disposition, curcumin is a hidden golden gem for health.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Are you the type of person who drinks a cup of coffee with breakfast every morning? Or perhaps you need that cup of coffee first thing in the morning in order to be able to go about your day? And if so, how many cups of coffee do you drink? With more and more people stopping by coffee shops before work on a regular basis, the debate on whether coffee is good or bad for your health is one that has become increasingly important to researchers and consumers alike.
Several research studies have demonstrated coffee’s remarkable benefits towards lowering the risk of cardiovascular disease, type 2 diabetes, and Parkinson’s Disease, while several have associated high coffee consumption with an 8 to 15 percent decrease in risk of death, others have warned how coffee can be harmful towards your health. The World Health organization and the Dietary Guidelines Advisory Committee have changed their idea from coffee being detrimental to coffee being a health food, going so far as advocating the consumption of 3 to 5 cups every day for achieving overall health and wellness.
Contents
The Coffee Debate
As many coffee aficionados would do anything to defend this dark elixir to the end, science is helping shed some light on the true advantages and disadvantages of drinking coffee on a regular basis. Whilst coffee on its own is full of a variety of beneficial antioxidants, caffeine being the active ingredient of this popular beverage is also at the center of the entire debate.
Aside from avoiding any of the symptoms listed by the DSM-V, there are other reasons why you should decrease or stop your consumption of caffeine and prevent caffeine intoxication. Caffeine has also been reported to display adverse effects on individuals with hypertension, nervousness, adrenal fatigue, and GERD. Its intake can aggravate symptoms of circulation diseases like Raynaud’s Phenomenon. We also shouldn’t ignore the fact that many healthcare professionals regularly indicate removing caffeine through a structured detox program to rest the liver.
But quitting the consumption of coffee is simpler said than done. The average amount of caffeine found in a normal coffee shop beverage easily exceeds the quantity indicated for overdose. By way of instance, a 20-ounce Blonde Roast coffee from Starbucks is roughly 475 mg. The same size of a Dunkin Donuts coffee with a turbo shot is almost 400 mg and a 16-ounce light-roast from Panera Bread is 300 mg. Even if we avoid drinking coffee altogether, caffeine can also be found in teas, chocolate and soda. As a result, a lot of us are walking around every single day overdosing on caffeine. According to a review, nearly 90 percent of people in the United States consume well over 250 milligrams of caffeine daily.
While the debate on whether coffee is good or bad for your health continues, an important thought to consider is that “one size does not fit all” when it comes to the consumption of caffeine. Personalized treatments have gained plenty of popularity because of this. While some individuals may get the jitters from drinking caffeine, not everybody will report experiencing the same symptoms needed to determine the diagnosis of an overdose. The main cause of this is simple, the liver’s capacity to metabolize caffeine will often differ from person to person. Concentrations of CYP450 enzymes required for stage I liver detox causes some people to be “fast-clearers” of caffeine, or people who may have a double espresso and drift dreamily to bed within the hour, and lots of others may be slow-to-impossible clearers, or people who can be considered as no more than nervous wrecks when given the tiniest sip of hot chocolate.
Alternatively, the effects of caffeine can be utilized to treat certain symptoms associated with headaches or asthma, and provide attention and focus, as well as energize the muscles of a training athlete. However, caffeine’s addictive quality, and its capability to tax the liver and nervous system, shouldn’t be ignored. When confronted with a reason to decrease or eliminate caffeine from their diet, conventional coffee lovers may be challenged by withdrawal symptoms, such as headache, agitation, muscle strain, and even anxiety, as well as altering psycho-social behaviours, such as a societal coffee-culture or an afternoon chocolate pick-me-up.
If you are on the path to attempt to detox from your coffee drinking habits, then here are a few tips that can help make the process easier for you:
Drink additional water
Eat a minimally-processed diet rich in minerals and vitamins
Get plenty of exercise and/or physical activity
Sleep properly
Find other choices to decaffeinated coffee, from several chicory and dandelion mixtures, to herbal teas
Supplement using a full-spectrum multivitamin, magnesium, L-theanine and L-DOPA
Persistent caffeine consumption can also deplete calcium, leading to muscle tension and headaches. Restoring healthy magnesium levels will help alleviate these symptoms. In addition, L-theanine is considered to have a calming effect. One research study from 2012 revealed that L-theanine reduced stress and inhibited increases in blood pressure from participants who were confronted with stressful tasks on a computer. L-DOPA, or Dopamine, otherwise referred to as the “happy chemical”, is accountable for controlling the joy and reward centers of the brain, the very same regions aroused by addictive substances like sugar and caffeine. A recent double blind, randomized controlled crossover trial compared the pharmaceutical levodopa used to treat Parkinson’s sufferers to Mucuna pruriens, a natural supply of L-Dopa, and found them similar in clinical efficacy, with Mucuna pruriens being considered more tolerable.
The right answer for when to drink coffee or not is as private as a Starbucks custom coffee order. If you’d love to kick the caffeine habit, however, here’s a simple, no-nonsense approach to slowly getting away from caffeine:
Days 1 to 2: Combine 25 percentage decaf, 75 percent caffeinated
Days 3 to 4: Combine 50 percent decaf, 50 percent caffeinated
Days 5 to 6: Combine 75 percent decaf, 25 percent caffeinated
Day 7: Try entirely decaf.
Dr. Alex Jimenez’s Insight
The advantages and disadvantages of drinking coffee have become highly dependent on the amount of evidence provided over the numerous of research studies conducted to solve the health mysteries of this popular dark beverage. While some studies describe coffee to be good for your health and others urge that coffee is bad for your health, the answer to this debate is simple, it’s a little bit of both. Too much coffee can cause a variety of undesirable symptoms, however, a moderate amount of coffee can provide a wide array of benefits, including lowering the risk of developing many health issues like type 2 diabetes. Whether you choose to believe if coffee is good or bad for your health, alternative treatment options, such as chiropractic care, can help provide you with a variety of health benefits in order to help improve and maintain your overall well-being.
As mentioned above, with the increasing number of coffee lovers found around the world today, the debate regarding whether coffee is good or bad for your health has peaked the interest of many healthcare professionals as well. While research studies and scientific evidence continues to amount to both of these options, you can find alternative treatment options which can help improve and maintain overall well-being. Chiropractic care is a healthcare profession which focuses on the diagnosis, treatment and prevention of a variety of injuries and conditions associated with the musculoskeletal and nervous systems. A chiropractor, will utilize spinal adjustments and manual manipulations to correct spinal misalignments, or subluxations, to restore the natural integrity of the human body. When a spinal misalignment is interrupting the signals being sent from the brain, to the spinal chord and the rest of the body, many important structures and functions can suffer.
Like the favorable effects expected from coffee and caffeine by consumers, chiropractic care can help increase strength, mobility and flexibility. Furthermore, chiropractic care can promote proper circulation and reduce inflammation associated with stress and tension. By reducing pressure around the complex structures of the spine, spinal adjustments and manual manipulations can also help reduce pain and discomfort, increasing many fundamental functions. In addition, a doctor of chiropractic, or DC, can offer exercise and nutritional advice, which may be important to those individuals who wish to cut back on their coffee intake. With the additional benefits you experience from chiropractic care, even the most avid coffee aficionado can benefit from the advantages of chiropractic care.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
A majority of individuals today are aware about the gut-brain connection and how approximately 90 percent of their body’s serotonin is really generated in the gastrointestinal, or GI, tract as well as the way the gut-brain axis is associated with depression. Overall gut health involving a healthy population of gut microbiota can affect many facets of our well-being, therefore, it’s no mystery that the connection between the gut and chronic health issues, such as cardiovascular disease, diabetes and neurodegenerative diseases, are also significantly strong.
Berberine, an ancient mixture frequently utilized in a variety of medicinal herbs throughout several traditional treatments has been demonstrated to benefit as well as link the gut and the heart. Berberine is an isoquinoline derivative alkaloid found in numerous herbs. Although these berberine-containing herbs aren’t traditionally utilized in food preparations, the active ingredient has been identified and may be isolated from a variety of plant sources, such as Coptis chinensis, or Coptis or Goldthread, Hydrastis canadensis, or goldenseal, Berberis aquifolium, or Oregon grape, Berberis aristata, or Tree Turmeric, Berberis vulgaris, or Barberry, and Arcangelisia flava.
Berberine is most favorably known for its function in gut health, demonstrating activity which can help support gut microbial balance. In fact, scientists have shown a growing interest in many plant-derived compounds which affect bacterial direction and berberine is a pioneer in the group. Additionally, its a botanical proven to influence blood glucose, blood lipids and also the immune system. Researchers today have learned how berberine can provide these tremendous benefits.
Contents
Gut Health Equals Heart Health
According to evidence from a 2016 research study, the gut’s immune system is fundamental towards preventing a variety of diseases and it may often contribute to metabolic disorders. However, it might also help provide a treatment goal when observing systemic inflammation in insulin resistance. Moreover, modified gut immunity has been linked with changes to the gut microbiota, intestinal barrier function, gut-residing immune cells, and resistance to antigens which enter the gastrointestinal, or GI, system. Although this has been previously believed to raise the danger of esophageal ailments including, pathogenic infections and chronic inflammation, which may ultimately lead to chronic health issues.
In our currently hectic and stressful world, a growth in the numbers of chronic disease has begun to negatively affect our overall health health. The best instance of this increase in chronic illness is type 2 diabetes, abbreviated in this article as T2DM, which often coexists with hypertension and causes individuals to pursue nutritional advice in order to achieve healthy blood sugar levels. The information viewing T2DM alone are shocking. As of 2015, the Center for Disease Control and Prevention reported that over 30 million people in the United States had diabetes, where approximately three times as many had pre-diabetes. According to statistics, 70 percent of individuals with pre-diabetes will develop type 2 diabetes.
Natural remedies and botanicals utilized as herbal treatments which have been previously used to promote healthy blood sugar levels have been strongly evaluated in order to determine their safety and effectiveness. Numerous berberine research studies are being conducted, though these are mostly in vitro, or in cell cultures. A majority of in vivo research studies have used animals for the analysis. Despite the quality and size of those research studies, virtually all of the outcome measures throughout the last two decades are positive. One research study from 2012 looked at in vitro results to thoroughly assess the assumed mechanism of action by which berberine affects fat storage. The outcome measures using clinical therapeutics of berberine to observe participants with metabolic syndrome appeared promising.
Another research study evaluated and analyzed the use of berberine in human cell cultures to ascertain how it influenced preadipocyte, a precursor to fat cells, comparison and fat hormone as well as cell activity in patients with metabolic disease. The researchers demonstrated that preadipocyte differentiation was restricted by berberine, while leptin, adiponectin, PPAR?2, or the nuclear receptor known as the master regulator of fat cell biology and target of many diabetes drugs and/or medications, and C/EBP?, a protein necessary for fat cell differentiation, diminished. After several months, participants demonstrated a drop in their BMI and leptin/adiponectin ratio, showing that berberine could boost insulin sensitivity by limiting fat storage, which may also have beneficial effects in the regulation of blood lipid levels.
Concerning how berberine affects cardiovascular biomarkers, many assessments can be found in the literature. The administration of berberine in one analysis generated a substantial decrease in total cholesterol, triglycerides, and low-density lipoprotein cholesterol levels, with a marked rise in high-density lipoprotein. Furthermore, a meta-analysis of this anti-diabetic, hypolipidemic and anti-inflammatory effects of berberine were reviewed in twenty-seven randomized controlled clinical trials. The researchers have concluded that berberine is safe and effective due to its support of the cardiovascular system and the maintenance of healthy blood sugar levels, without any severe adverse reactions found in some of the other research studies. Berberine has also been demonstrated to restrict complex I of the mitochondrial respiratory chain, leading to a growth of 5′ adenosine monophosphate, or AMP and 5′ adenosine monophosphate-activated protein kinase, or AMPK activation. This seems to have a direct impact on energy metabolism as well as that in other structures and functions.
The neurological health effects of berberine have also been considered, particularly from the modulation of the dopaminergic system. Berberine has also demonstrated a possibility in the successful management of seizures, diabetes-induced memory malfunction and hyperexcitability. One animal research study investigating obsessive-compulsive disease found that berberine can promote anti-compulsive and/or anxiolytic effects because of its ability to boost brain monoamine levels. Another review from 2016 demonstrated berberine’s ability to reduce oxidative stress and supply neuroprotective benefits. The review further cites research studies which examine the botanical’s function in the evolution of amyloid plaques and intracellular neurofibrillary tangles. Berberine has found its function in the gastrointestinal, cardiovascular as well as brain worlds. Truly offering a wholesome dose of gut-heart-brain link, berberine is definitely one to consider.
Dr. Alex Jimenez’s Insight
Research studies have found that the relationship between a healthy gut, brain and heart is fundamental towards overall well-being. Natural remedies and botanicals, such as berberine, can help promote as well as support this gut-brain-heart connection, while other alternative treatment options, such as chiropractic care, can restore balance and encourage the human body’s natural healing abilities by correcting spinal misalignments of the spine. Furthermore, by establishing the proper relationship between the brain, the spinal chord and the rest of the body, chiropractic care can help regulate the proper structure and function of each system in the human body.
With the increasing number of gut health issues, it’s become a priority to find safe and effective treatment options to properly address these common problems. More and more research studies have found a connection between the gut, brain and heart. As previously mentioned, by both supporting and promoting the well-being of the gastrointestinal, or GI, system, the structure and function of a variety of other systems can be sustained. Natural remedies and botanicals, such as berberine, have been utilized for centuries as herbal treatments, however, other alternative treatment options can also be used to help improve gut health. Chiropractic care is a well-known, alternative treatment option which has been demonstrated to help promote the natural healing of the human body through the use of spinal adjustments and manual manipulations as well as other therapeutic techniques to correct spinal misalignments, or subluxations. Moreover, a doctor of chiropractic, or chiropractor, can recommend a series of lifestyle modifications, including exercise and nutritional advice, in order to help further improve the overall health and wellness of the human body. Maintaining the well-being of the gut can help boost brain and heart health as well.
Berberine Warnings
In large doses, berberine may lead to gastrointestinal irritation. Thus, it’s typically administered in divided doses and taken with a meal. In addition, researchers have revealed that berberine can limit particular cytochrome enzymes that also target a lot of different kinds of drugs and/or medications, including certain antibiotics. Inhibiting cytochrome enzymes influences the liver’s detoxification system, which will be required to metabolize and, finally, clear drugs and/or medications. For this reason, it’s essential to carefully monitor those patients that are using berberine if other medicines are used concomitantly. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Before erectile dysfunction started to become a more well-known health issue among the population of men across the United States, male reproductive and endocrine problems were rarely a topic of discussion. In the modern world, however, and with the increasing availability of information from the internet, many individuals have become surprisingly interested in understanding the consequences that diminishing testosterone levels can have on overall health and wellness.
Much like female hormone production, male hormone production can also gradually decrease with age. The period of time in which the male human body experiences a hormonal decline is most commonly known as andropause. Other terms which have been used interchangeably to refer to this structural and functional change with age includes: hypogonadism, late-onset hypogonadism, male menopause, male climacteric, androclise, androgen decline in aging male and aging man syndrome.
For women, menopause is characterized by a halt in menses, indicating the start of a new phase past their childbearing years. In Greek, “andras” means individual men, and “pause” means cessation. Therefore, andropause literally means “human male cessation”. Decreased levels of testosterone in men have been connected with a variety of symptoms, such as night sweats, decreased libido, dry skin and hair, difficulty concentrating, muscle loss, sleeplessness or insomnia, stress, anxiety and/or irritability, decreased bone integrity and insulin resistance. These symptoms have all been commonly associated with “human male cessation” and can often indicate diminishing testosterone levels in the body.
Contents
Function of Testosterone in the Human Body
Similar to the mechanisms of actions of estrogen and other androgens/sex hormones, testosterone functions as three unique hormones or cellular messengers within the human body. It can attach directly to androgen receptors; it engages in a variety of important processes on the peripheral cells of the prostate and hair glands in which 5-alpha-reductase is often found, producing dihydrotestosterone which also attaches to androgen receptors; and finally, it can ultimately be converted into estradiol, which develops on estrogen receptors in bone and in abdominal fat or connective tissue. These functions are fundamental towards preserving fertility, libido, weight management, bone health, and basic overall health and wellness.
Symptoms of low testosterone, which will be abbreviated in this article as Low-T, are generally hardly noticeable, as a result, these may only gradually become more severe health issues, aside from altering complete well-being. In addition, hypogonadism has also been reported to develop in younger men, although rarely, together which amounts to an incidence of approximately 3.1 to 7.0 percent in males 30 to 69 years of age, and about 18.4 percent in older men. From these numbers, 5.6 percent of males 30 to 79 years of age will experience symptomatic androgen deficiency. Besides it signaling a natural aging process in human males, very low testosterone levels may also serve as a biomarker signaling the presence of an underlying health issue. By way of instance, metabolic syndrome and testosterone deficiency have been reported by healthcare professionals to have a close association with each other. Various research studies have demonstrated that reduced testosterone levels may also be connected with obesity, insulin resistance and dyslipidemia in men. In the same manner, men with metabolic syndrome and type 2 diabetes have been reported to have a greater incidence of hypogonadism.
Is Andropause Similar to Menopause?
In comparison to menopause, where women’s estrogen levels decrease abruptly, total testosterone levels in men decrease at an average rate of 1.6 percent annually once a human male reaches the age of 40, while free and bioavailable levels generally decline by 2 to 3 percent each year. Even though the decline is normally continuous and gradual, about 50 percent of men over the age of 80 still report having total serum testosterone within normal standard quantities. Additionally, fertility is not affected in men exactly the same way as post-menopausal women.
According to the British Medical Journal, or BMJ, the estimate of the prevalence of Low-T was recorded from the European Male Aging Study. Measuring a combination of sexual symptoms and testosterone levels, it was discovered that just about 0.1 percent of men in their 40’s, 0.6 percent of men in their 50’s, 3.2 percent of men in their 60’s, and 5.1 percent of men in their 70’s, would meet the criteria for a Low-T evaluation and analysis.
Pros and Cons of Hormone Therapy
Despite information suggesting that Low-T may be as widespread as we all believe, at least we know that the search to increase testosterone levels is. Testosterone replacement therapy, or TRT, has been a widely considered yet controversial treatment utilized by endocrinologists and urologists when hypogonadism is found. A variety of research studies have discovered that it may be a viable choice, while others shed light on an assortment of concerns and contraindications. An observational research study conducted in 2012 compared the mortality of men over 40 years of age with reduced testosterone levels that had been treated with TRT to men who were not treated with TRT. The research study demonstrated that the mortality rate of those men not treated with testosterone replacement therapy was greater, approximately 20.7 percent compared to 10.3 percent. Although the research study outcome measures seemed to favor TRT, it was not a gold-standard, placebo controlled randomized clinical trial and it also did not account for confounders.
Moreover, TRT has been demonstrated to enhance insulin resistance, dyslipidemia and sexual dysfunction in males with Low-T, although there have been no long-term research studies to assess its overall impact on mortality. In patients with breast or prostate cancer, TRT, or testosterone replacement therapy, often comes with risks. As a matter of fact, guidelines in the Endocrine Society suggest not utilizing TRT when a patient has been diagnosed with prostate cancer, a palpable prostate nodule, or even after a raised prostate-specific antigen, or PSA, test with results over 4 ng/ml has been determined. Even men with a family history of prostate cancer have been steered away from utilizing this kind of treatment option.
Dr. Alex Jimenez’s Insight
The spine is primarily in charge of protecting the spinal chord, one of the main channels between the communication of the brain to the rest of the body, such as that of the endocrine system, which helps in the production and regulation of hormones. When there is a spinal misalignment, or subluxation, however, these signals may be interrupted, ultimately affecting your overall health and wellness. Through the use of spinal adjustments and manual manipulations, a doctor of chiropractic, or DC, can help carefully restore the integrity of the spine, correcting these fundamental connections and their relation to the rest of the human body’s structures and functions. The balance of the spine can help delay the decrease of testosterone levels associated with human male cessation or andropause, reducing symptoms and boosting essential energy and vitality.
Delaying Low-Testosterone Levels
Though decreasing testosterone levels are commonly associated as a part of the normal aging process, many men dread andropause or “human male cessation”. The loss of muscular mass itself generally motivates men to search for solutions to delay this natural process. Steroids help build muscle by raising testosterone, but they can also ultimately affect the liver, prostate, heart and even the sexual organs. Selective androgen receptor modulators, or SARMs, are encouraged to athletes and active individuals as an alternative to anabolic steroids, but these can also include their own risks and concerns. Many of these alternative treatment options can actually decrease natural testosterone production since they change the chemical structure of testosterone alone.
Thus, some lifestyle modifications worth exploring which can help delay the decrease of testosterone levels include health, diet, stress reduction and supplementation. A prerequisite for healthy testosterone levels include maintaining regular weight and encouraging overall endocrine function. In addition to deciding upon an entirely whole foods-based diet teeming with healthful fats which serve as a hormone precursor and fiber, a few research studies have found that intermittent fasting, characterized by remaining anywhere from 12-16 hours every day, by way of instance, sleeping hours, without eating food, as a way to help maintain weight and testosterone levels during the rebalancing of hormones. Intermittent fasting was additionally found to increase the adrenal hormone, or LH, by 67 percent, overall testosterone by 180 percent and improve the growth hormone secretion in men. Intermittent fasting also helps to improve leptin levels, which ultimately benefits testosterone levels since the clinical condition most closely associated with reduced cholesterol is obesity, and normalizing leptin levels is vital for maintaining healthy weight. In terms of fluids, significant water consumption, while reducing caffeine and alcohol consumption helps bring hydration into the epidermis and hair in addition to reducing fatigue associated with “human male cessation”. Physical activity for at least 30 minutes per day boosts energy and fundamental vitality.
Supplement suggestions for Low-T include vitamin D, Ginseng, Ginkgo biloba, Ashwagandha, Damiana, Velvet Deer Antler, Maca or combinations thereof. Anecdotal evidence abounds concerning supplementation, with more and more clinical evidence coming forward. Recently, one research study measured the cross-sectional association of plasma 25(OH)D levels and total and free testosterone in 1,362 male participants, which also found 25(OH)D to be positively associated with total and free testosterone levels.
Moreover, other alternative treatment options, such as chiropractic care, can be beneficial towards delaying the decrease of testosterone levels in men. Many people believe that chiropractic care only works for spinal health issues, however, an individual’s overall health and wellness also depends largely on the proper alignment of the spine. Spinal misalignments, or subluxations, can interrupt the communications which travel from the brain to the spinal chord and the rest of the human body, ultimately affecting a variety of other essential structures and functions. By carefully restoring the balance of the musculoskeletal and nervous system, a chiropractor can influence positive effects throughout other areas of the body. One of the many benefits of chiropractic care includes the maintenance of hormone imbalances. Through the use of spinal adjustments and manual manipulations, along with guidance and advice on specific lifestyle modifications, such as exercise and nutrition, chiropractic care can help regulate hormones.
Overall, Low-T might feel as the conclusion of manhood, but the conversation about it is just starting. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Envision yourself waking up entirely rested, prepared to deal with any obstacle and adopt all the joys of the world with gratitude. The majority of us know what a good night’s sleep resembles, but are we really getting the proper rest we should be getting? Within this stressful universe, it’s tough to achieve the sleep schedule that our brains and bodies require to operate to its fullest potential.
Proper sleep hygiene and the application of organic herbs and botanicals can help promote a healthy amount of sleep. The outcome could result in a wide array of benefits, including an improvement in problem solving and work performance, weight management, and even promote the prevention of chronic health issues, such as diabetes, cardiovascular disease and mood disorders like depression. You may find numerous products and information regarding how to manage proper sleep. A research study from 2016 indicated that individuals in the United States alone spent over $41 billion on sleeping treatments, where it is expected to rise up to $52 billion by the year 2020.
What Natural Remedies or Botanicals Can Help Promote Sleep?
The�German Commission E, globally recognized for its understanding information on the role of medicinal herbs, additionally recommends the frequent utilization of certain botanicals, such as valerian, lavender, lemon balm, and hops, to promote the right level of relaxation and support proper sleep. There are several other well-known options which have sedative qualities, such as passion flower, chamomile, and kava kava. Nearly all of those relaxant natural remedies and botanicals are available commonly in teas, but they are also found in supplement form. Nearly always found in specialized mixes, these herbs have various mechanisms of action, and, therefore, behave synergistically when mixed together.
Lavender (Lavandula angustifolia) is a very popular floral herb utilized in fundamental oil form, teas, extracts and in other botanical combinations to promote relaxation as well as to relieve stress and anxiety. Recent research studies have identified that lavender works by antagonizing NMDA-receptors and serotonin transporters. Doses of about 80 milligrams every day of lavender from gel cap type for up to ten weeks were utilized in a research study where participants had previously been diagnosed with an unspecified type anxiety disorder. Both quality and length of sleep seemed to have been enhanced in those subjects without them experiencing the sedative side-effects as demonstrated in pharmaceutical sleep treatments. Other uses of lavender include 1 to 2 tsp in hot water as a tea every day, or its key oil diluted in a carrier oil used for massage or in a hot bath. Lavender is generally considered safe, however it’s also believed to be toxic if ingested orally in large quantities.
Hops (Humulus lupulus), aside from its frequently enjoyable pronunciation and serving as the main ingredient in a variety of beers, this is one of the herbs which is most commonly mixed in teas or supplements to achieve as well as maintain an overall calming effect. Researchers haven’t completely discovered how hops causes this effect, however, it’s been demonstrated to bind to serotonin and melatonin receptors. Valerian-hops blend products have also become the most widely researched in placebo-controlled, double-blind randomized controlled trials comparing them to benzodiazepine-class sleep drugs and/or medications with varying results. Like lemon balm, signs for its use as a herbal treatment for relaxation or insomnia includes an extended background in history.
Passionflower (Passiflora incarnata) is basically another botanical utilized to remedy stress, anxiety and insomnia. Researchers have discovered that passionflower works by increasing levels of GABA, achieving a comforting effect. In a Japanese research study from 2017, scientists discovered that passionflower extract modulates the amounts of the receptors as well as the genetic expression of the related enzymes in vivo and in vitro. This ultimately resulted in favorable effects on circadian rhythms.
Dr. Alex Jimenez’s Insight
Natural remedies and botanicals are a natural option for promoting sleep. While various herbs taken in numerous forms can help provide a good night’s rest, other alternative treatment options can also be considered to get you through a full night of rest. Chiropractic care can help promote sleep by carefully correcting spinal misalignments, or subluxations, through spinal adjustments and manual manipulations, among other techniques. Spinal misalignments, or subluxations, can cause tension and stress along the back, causing pain and discomfort which can contribute to poor sleep. Regular chiropractic care can solve a variety of health issues which may be causing you sleepless nights, thus helping you sleep better and improving quality of life.
Proper Sleep Hygiene Advice
Dr. Michael Polsky, a board-certified sleep physician, recommends contemplating proper sleep hygiene for improving sleep. Sleep hygiene is a phrase utilized to refer to how we prepare our bodies and minds for sleep, beginning hours before we actually have to sleep. In fact, the window of 2 to 3 hours before sleeping proves to be significantly the most essential when attempting to get a good night’s rest. Below, are several notes of advice for achieving and maintaining proper sleep hygiene:
At least 2-3 hours before bedtime, have a light, balanced meal and also reduce fluids
Make a strategy to avoid the use of electronic devices 1 to 2 hours before bed
Do a little mild activity, like walking or yoga; avoid a hard workout or some other action which is too stimulating
Reduce or eliminate caffeine, commonly from coffee, tea, or chocolate, drink no more than 1 to 2 cups of coffee or tea before lunch
Keep a regular sleep schedule, even on weekends
A Simple Tea Recipe
Blend a batch of 2 parts peppermint leaf, 1 piece lemon balm, 1 part passionflower, and 1 part lavender. Steep one heaping teaspoon in a teacup of hot water for 5 minutes and enjoy only as a relaxing drink.
Sleep deprivation is one of the most common behaviors which can lead to a variety of health issues. While the natural remedies and botanicals mentioned above can be utilized to help promote sleep, other alternative treatment options, such as chiropractic care, have been reported to help provide a better good night’s rest. Chiropractic care focuses on the diagnosis, treatment and prevention of a variety of musculoskeletal and nervous system injuries and/or conditions, through the use of spinal adjustments and manual manipulations. A spinal misalignment, or subluxation, can cause pain and discomfort when trying to get proper sleep. Through chiropractic care, a chiropractor can help promote sleep by carefully correcting any spinal misalignment which may be causing painful symptoms. By treating symptoms of pain and discomfort, chiropractic care can help promote sleep, naturally, without the need for drugs and/or medications as well as surgical interventions.
In conclusion, proper sleep and rest are essential elements towards achieving and maintaining overall health and wellness. Through the use of natural remedies and botanicals, by practicing good sleep hygiene tips, and by receiving chiropractic care, the average American can begin to experience the benefits of proper sleep. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Antibiotics have long been used to treat infection and illness. While they can be effective, there is a down side. Antibiotics can have some unpleasant side effects. What�s more, bacteria can become resistant. The more you take the less effective they can be, making the healing process much more difficult. It isn�t smart to depend on antibiotic for ultimate health. The better route is to take a more holistic approach by incorporating chiropractic, nutrition, exercise, and healthy lifestyle changes.
Contents
What Are Antibiotics?
Since the discovery of penicillin in the 1920s, antibiotics have been used to treat illness and infection. They have become a major component in American medicine. However, few people know exactly what they are or how they work.
They are medications that are used in the prevention and treatment of infections such as pneumonia, kidney infection, or an abscessed tooth. They are a type of antimicrobial drug and are not effective against viruses like the flu or a cold. As medicine has made significant advances in treating some of the worst and even deadly illnesses in the world, more are being developed to better target specific bacteria.
How Do Antibiotics Work?
Different antibiotics work in different ways on the cells that they seek out. Cells in the human body have some similarities to bacteria. Antibiotics affect those properties in bacteria that are different from human cells.
For instance, many strains of bacteria have cell walls while human cells do not. Penicillin prevents the bacteria it attacks from building those cell walls. Other antibiotics use other differences such as how they copy DNA or build proteins or dissolve bacteria cell membranes. The effects that antibiotics have on bacteria are intended to keep it from replicating and kill it.
Do Antibiotics Only Affect The �Bad� Bacteria?
Unfortunately, antibiotics can�t always distinguish between �bad� and �good� bacteria. This means that while they attack the harmful bacteria that is making you sick, they also attack the resident, helpful bacteria.
The �good� bacteria, or friendly bacteria, keeps you healthy in a variety of ways. It protects you from certain illnesses and keeps your body functioning at an optimal level. When you no longer have that friendly bacteria in your body, you lose out on the health boosting benefits that they offer. What�s more, when you lose the friendly bacteria it leaves room for certain other harmful bacteria to come in.
How Do Bacteria Become Resistant To Antibiotics?
When these medications are misused it can result in the emergence of bacteria that is resistant to antibiotics. There are several ways that they can be used inappropriately. They are only meant to be taken for a limited time, usually five or ten days. When they are taken longer than that or when several rounds are taken back to back, that qualifies as misuse. It can also occur when antibiotics are taken for viruses or other purposes for which they are not intended.
What Happens When Bacteria Become Resistant To Antibiotics?
Bacteria has a very strong ability to adapt to environments in order to survive. It can evolve and change as their environment becomes uninhabitable, such as with increasingly higher antibiotic doses. As bacteria is exposed to antibiotics it will make adjustments, adapting to them, even thriving.
The bottom line here is that while these medications may be beneficial in certain situations, they should be used as rarely as possible and usually as a last resort. There are many lifestyle changes that a person can make that can help them stay healthy and prevent illness so that they have no need for these medications.
A healthy diet, regular exercise, proper food handling and preparation, adequate sleep, regular chiropractic treatments, and eliminating unhealthy activities like smoking and alcohol consumption can all lead to better health and fewer illnesses. It is much easier and less expensive to prevent illness than it is to treat it.
Irrespective of a continuous surge in interest regarding the ketogenic diet, exactly why is it that individuals have been utilizing this dietary pendulum swing from the�nutritional worries that have been spreading across the world? Many people appear to be�obsessed with the latest diet fads and trends associated with achieving and maintaining a balanced weight and supporting overall health and wellness. Research studies have demonstrated evidence outcomes regarding the benefits of dieting.
The National Weight Control Registry has stored data about these types of ongoing research studies. More than half of subjects involved in these varieties of tests and evaluations had revealed that they were following some sort of diet or intended to become involved in programs or routines for weight loss. You often see annual reports listing the very best diets, including: the Top 5 Diets to Try in 2018, According to Experts, published by Time magazine. Moreover, the report claims that healthcare professionals have ranked the DASH Diet as the number one diet, followed by the Mediterranean Diet, Weight Watchers, the MIND diet, the TLC Diet and Volumetrics, as the top diets to try this year. The article, however, additionally discusses the ketogenic diet and ranks it as being among one of the lowest-ranked diets to try this year. No further details are given about this diet and the consensus appeared to be that it is challenging to follow.
However, the ketogenic diet is actually one of the most popular diets people generally talk about, subtly out-ranking paleolithic diet in most conversations. As a matter of fact, you may have already read or heard about the ketogenic diet from a variety of sources or perhaps you may even known a friend or a family member who has been trying it out themselves. A frequent concern about popular or fad diets, though, is that there doesn’t seem to be an exact guide on how to properly follow them, what kinds of problems they may cause, and/or even for whom these might be most appropriate. With eating habits like those described in the ketogenic diet, there are frequently risks or disadvantages, often involving nutrient deficiencies or lack of efficacy, especially if they’re truly hard to follow. But, how can this common issue regarding the proper diet be solved? Foremostly, it’s essential for individuals to weigh the advantages and disadvantages when choosing to attempt the ketogenic diet.
Contents
What is the Ketogenic Diet?
Let’s start with some history of what, where and when the ketogenic diet begain. There are various diets out there today which may have a lot in common with this well-known diet. Simply take a peek at a newstand, a bodybuilding website, or maybe the blogs of practicing healthcare professionals. First developed in 1921 by Dr. Russell Wilder of the Mayo Clinic as an alternative for children with intractable epilepsy, a classical ketogenic diet is supposed to alter the human body’s natural inclination to metabolize carbohydrates for energy. This can be achieved by adjusting an individual’s nutritional daily value to a particular macronutrient intake ratio of 4:1 fat-to-carbohydrates and protein diet. In this arrangement, fat comprises approximately 90 percent of daily calories, together with 7 percent of proteins and 3 percent of carbohydrates. Some alternatives for the ketogenic diet include a Medium Chain Triglyceride Diet consisting of 70 percent of fats, 10 percent of proteins and 20 percent of carbohydrates, or a Modified Atkins Diet with much more protein including 70 percent of fats, 25 percent of proteins, and 5 percent of carbohydrates, and a Low-Glycemic Index Treatment consisting of 45 percent of fats, 28 percent of proteins and 27 percent of carbohydrates.
The consequence of eating in this manner mimics what occurs when engaging in physical activities or exercise as well as what happens when fasting, a process referred to as ketosis. In ketosis, there is a depletion of glycogen reserves in the muscles and in the liver, which ultimately causes the liver to produce ketone bodies that can be used as fuel instead. Some healthcare professionals advise using either ketone strips or a sugar ketone meter to test the levels of ketosis in urine or blood. There is also a breath ketone analyzer available for purchase on Amazon. Don’t confuse ketosis with ketoacidosis, or the potentially deadly condition common to Type 1 diabetics when there are incredibly substantial levels of blood glucose and ketones.
Proof the Ketogenic Diet Works
It goes without saying, when a new dietary routine is useful for weight loss, nutrition experts understand they may also be used therapeutically for the treatment of many different diseases and ailments, among other health issues. The ketogenic diet has been used for decades to help with the treatment of epilepsy, and it has gained recent traction in its use for the treatment of obesity, type 2 diabetes, cardiovascular disease and neurological disorders. It has even been demonstrated to positively affect the gut microbiota.
Research studies regarding the use of a very-low carbohydrate, high fat diet for obesity, however, is in its initial stages. One research study, retrospectively in comparison to a non-carb/ketogenic-style diet, utilized a classic low-carb diet in bariatric patients, focusing on weight loss. The researchers found comparable weight-loss between both diets by 12 months post-intervention. Nonetheless, the ketogenic dieters that obtained follow-up guidance on a restricted carbohydrate routine had the best success following 24 months, indicating importance of care regarding an individual’s specific dietary habits.
One masterpiece post from 2008 clearly outlines the benefits of restricting carbohydrates to cause a unique metabolic state that favorably impacts atherogenic dyslipidemia, fatty acid partitioning and metabolic syndrome. The report clearly demonstrates that ketone bodies represent an efficient fuel for the body, about 25 percent more efficient at producing ATP than glucose or fatty acid, with curative potential towards numerous health issues. Following a carbohydrate-restrictive diet might also lead to a decrease in the release of pro-inflammatory chemicals, substances and compounds, which ultimately has positive implications for cardiovascular health.
On the reverse side, another research study found that the information on the effects of ketogenic diets on cardiovascular disease appeared to be contradictory in animal and human studies to produce an astounding recommendation. Recently presented in the 2018 American Diabetes Association seminar, a research study consisting of a 2-year randomized controlled trial, compared a high-carbohydrate diet to some very-low carbohydrate, like the ketogenic diet, with a reduced saturated fat diet in type 2 diabetic subjects. Both diets provided similar weight loss and reductions in HbA1c, whereas the very-low carbohydrate diet enabled participants to reduce their use of drugs/medications and improved their diurnal blood glucose equilibrium and blood lipids.
Missing Link in Keto Diet
One challenge that many healthcare professionals often face, however, is that sometimes, the ketogenic diet can make you feel sick. There is even a term for this: the Keto Flu. This is mostly because of a change in electrolyte conditioning together decreased insulin levels, resulting in a greater need for potassium, magnesium and sodium. If not properly managed, it can lead to nutrient deficiencies of those electrolytes, among different micronutrients, that may have consequences not completely elucidated as a result of the paucity of research on the long-term use of the ketogenic diet. Sodium is generally over-consumed in a typical diet, and a lot of high-sodium foods make their way into ketogenic diet cured meats, cheeses, and other foods that are processed. But most individuals in Western cultures today do not get enough potassium or magnesium, found mainly in fruits and vegetables, which may play a fundamental role in the pathology of chronic diseases like stroke and kidney stones.
A 2007 research study emphasized the risk factors for kidney stones after following the ketogenic diet. Approximately 6.7percent of the children who have been prescribed the ketogenic diet for intractable epilepsy were reported to have developed kidney stones. In these cases, utilizing potassium citrate significantly diminished the incidence of kidney stones and increased the expression time on the ketogenic diet. Potassium citrate solubilizes calcium, thus decreasing concentrations of free calcium readily available to crystallize. Additionally, it will also help to improve urine pH, helping to dissolve uric acid crystals. The research study concluded that “oral potassium citrate in clinical and prospective studies, using this treatment empirically was justified.”
Dr. Alex Jimenez’s Insight
The ketogenic diet, or the keto diet for short, is a low-carb, high-fat diet which has been previously described to offer many heath benefits. As a matter of fact, numerous research studies have demonstrated how this type of diet can help with weight loss as well as help improve overall health and wellness. The ketogenic diet may often be described as a “difficult to follow” diet because it involves drastically reducing carbohydrate intake to replace it with fat. However, its this reduction in carbs which allows the human body to enter a metabolic state known as ketosis. Once the human body enters ketosis, it becomes tremendously efficient in burning fat and turning it into energy, additionally turning fats into ketones in the liver, supplying energy directly to the brain. This, along with reductions in blood sugar and insulin levels, can have a variety of health benefits, making the ketogenic diet suitable for individuals with specific health issues.
Advice on the Keto Diet
If you would like to try the ketogenic diet or feel like it would benefit you in any sort of way, first make sure to check with your healthcare professional. There are a number of resources online and in texts that aren’t all peer-reviewed. Use the information with care and listen to your own body. Remember: this kind of diet requires additional understanding of biochemical processes, it may behard to follow due to its limitations and possible lack of palatability, and it has to be limited in length. Also, based on one’s genetics, the keto diet can yield quite different outcomes.
Nutrition is a fundamental part of overall health and wellness. Proper nutrition can ultimately affect the way an individual’s bodily system’s functions and without it, a variety of structures and functions can be affected. If you are seeking treatment for a specific health issue, nutrition becomes even more important. Chiropractic care focuses on the natural treatment of the spine, through the use of spinal adjustments and manual manipulations, as well as through the implementation of lifestyle modifications, to provide the human body with all the necessary components it needs to heal itself, without the use of drugs/medications and/or surgery. Many chiropractors often recommend the ketogenic diet, alongside chiropractic care, to improve well-being. Be sure to talk to your doctor of chiropractic, or DC, regarding any nutrition plan you want to follow and they can discuss the best options for your specific health issues and basic treatment needs.
That made clear, there are some smart recipes available on the marketplace to rival those which have observed from the fantastic Paleo popularity. One standout origin for the ketogenic diet is the Charlie Foundation website, which was put up to give dietary advice for caregivers of young children with uncontrolled epilepsy. Check out their site for ideas to feed your keto. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

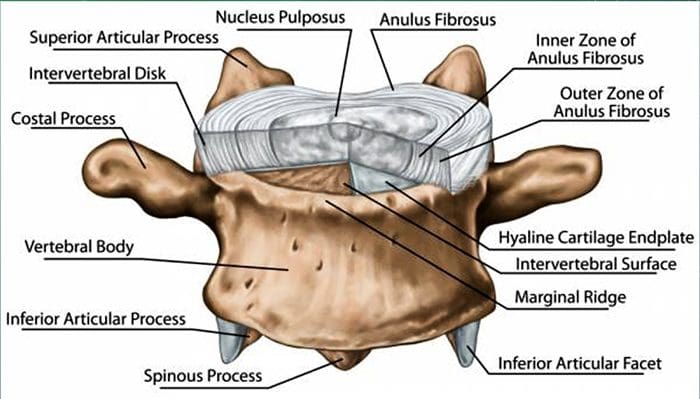
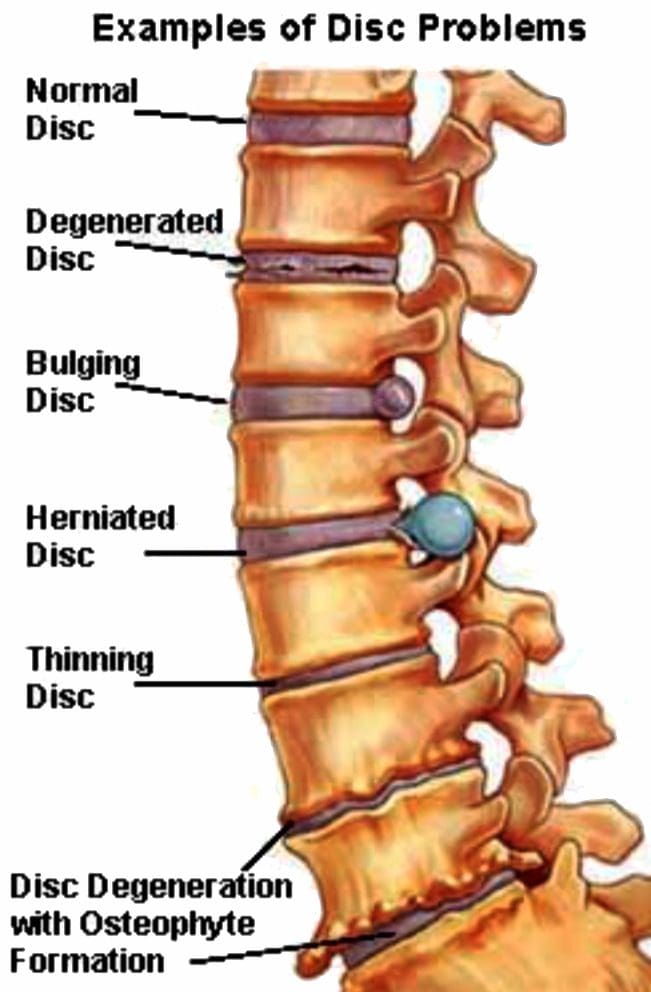 Lumbar Spine:
Lumbar Spine: