James Hill, father and teacher to two older sons and a younger daughter called Madison Hill, belong to an athletic family. Madison began participating in several sports because she had been a young woman, but she consequently experienced numerous sports injuries. Luckily, James Hill and his daughter Madison Hill went to go to Dr. Alex Jimenez and he has tremendously helped her recover after every injury she experiences. Collectively, they’ve learned to trust in chiropractic care, particularly following Dr. Alex Jimenez’s innovative treatment techniques and procedures. Mr. Hill expresses his gratitude in addition to how far Dr. Alex Jimenez’s understanding in sports injury therapy has greatly enlarged his general comprehension of the human body’s healing process. After Madison suffered a recent ankle sprain, she was instantly reassured by Dr. Alex Jimenez regarding how much faster she’d return-to-play during chiropractic care. James Hill and Madison Hill highly recommend Dr. Alex Jimenez as the non-surgical selection for volleyball sports injuries, among others..
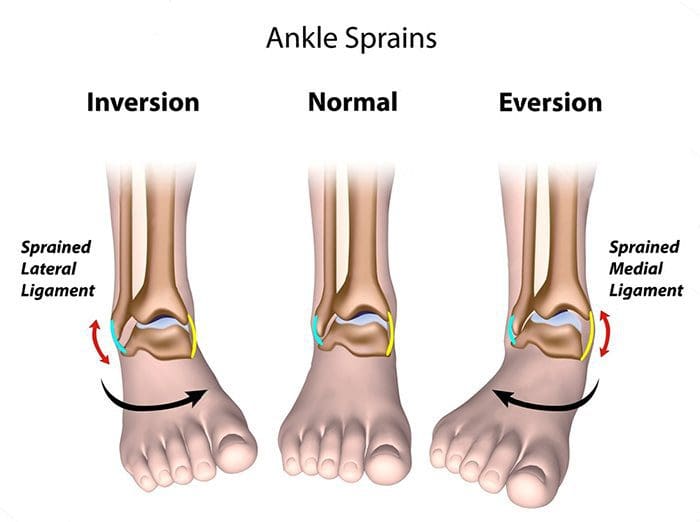
Chiropractor Ankle Sprain Treatment
Every year, millions of young athletes engage in high school sports. However, once an injury occurs, it might develop into an issue that might result in them having to discontinue their particular sport or physical activity if not treated properly. The pressure to continue participating in the sport or physical activity may cause young athletes not to follow proper recovery guidelines, which might subsequently result in more injury with long-term consequences. Sports injuries among young athletes fall into two key categories: overuse injuries and acute injuries. Both kinds include injuries to the soft tissues and bones. Whether an injury is acute or due to overuse, a young athlete who develops a symptom which impacts their athletic performance should be diagnosed appropriately by a health care professional. Sports accidents which are untreated can lead to permanent disability. Many high school sports injuries can be avoided through appropriate instruction and conditioning.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
My treatment with Dr. Alex Jimenez has been helping me by simply making me less tired. I’m not experiencing as many headaches. The headaches are going down dramatically and my back feels much better. I would highly recommend Dr. Alex Jimenez. He’s very friendly, his staff is very friendly and everybody goes well beyond what they can do to help you. –Shane Scott
Neck pain can develop due to a variety of reasons, and it can vary tremendously from mild to severe. Most of the population has suffered from this well-known nagging health issue; however, did you know that headaches can sometimes be caused by neck pain? While these headaches are commonly referred to as cervicogenic headaches, other types, such as cluster headaches and migraines, have also been determined to be caused by neck pain.
Therefore, it’s fundamental to seek a proper diagnosis if you’ve experienced headaches or neck pain to determine the root cause of your symptoms and decide which treatment option will be best for your specific health issue. Healthcare professionals will assess your upper back, or the cervical spine, including your neck, the base of the skull and cranium, and all the surrounding muscles and nerves to find the source of your symptoms. Before seeking help from a doctor, it’s essential to understand how neck pain can cause headaches. Below, we will discuss the anatomy of the cervical spine or neck and demonstrate how neck pain is connected to headaches.
Contents
How Neck Pain Causes Headaches
The muscles between the shoulder blades, the upper portion of the shoulders, and those surrounding the neck, or cervical spine, may all cause neck pain if they become too tight or stiff. This can generally occur due to trauma or damage from an injury, as well as in consequence of bad posture or poor sitting, lifting, or work habits. The tight muscles will make your neck joints feel stiff or compressed, and it can even radiate pain toward your shoulders. Over time, the balance of the neck muscles changes, and those specific muscles that support the neck become weak. They can ultimately begin to make the head feel heavy, increasing the risk of experiencing neck pain as well as headaches.
The trigeminal nerve is the primary sensory nerve that carries messages from the face to your brain. Furthermore, the roots of the upper three cervical spinal nerves, found at C1, C2, and C3, share a pain nucleus, which routes pain signals to the brain and the trigeminal nerve. Because of the shared nerve tracts, pain is misunderstood and thus “felt” by the brain as being located in the head. Fortunately, many healthcare professionals are experienced in assessing and correcting muscular imbalances, which may lead to neck pain and headaches. Moreover, they can help to relieve muscle tension, enhance muscle length and joint mobility, and retrain correct posture.
What Causes Neck Pain and Headaches?
Cervicogenic headaches, otherwise known as “neck headaches,” are caused by painful neck joints, tendons, or other structures surrounding the neck, or cervical spine, which may refer to pain to the bottom of the skull, to your face or head. Researchers believe that neck headaches, or cervicogenic headaches, account for approximately 20 percent of all headaches diagnosed clinically. Cervicogenic headaches and neck pain are closely associated, although other types of headaches can also cause neck pain.
This type of head pain generally starts because of an injury, stiffness, or lack of proper functioning of the joints found at the top of your neck, as well as tight neck muscles or swollen nerves, which could trigger pain signals that the brain then interprets as neck pain. The usual cause of neck headaches is dysfunction in the upper three neck joints, or 0/C1, C1/C2, C2/C3, including added tension in the sub-occipital muscles. Other causes for cervicogenic headaches and neck pain can include:
Cranial tension or trauma
TMJ (JAW) tension or altered bite
Stress
Migraine headaches
Eye strain
The Link Between Migraines and Neck Pain
Neck pain and migraines also have an intricate connection with each other. While in some cases, severe trauma, damage, or injury to the neck can lead to severe headaches like migraines; neck pain might result from a migraine headache in different situations. However, it’s never a good idea to assume that one results from the other. Seeking treatment for neck pain when the reason for your concern is a migraine often will not lead to effective pain management or pain relief. The best thing you can do if you’re experiencing neck pain and headaches is to seek immediate medical attention from specialized healthcare professional to determine your pain’s cause and the symptoms’ root cause.
Unfortunately, neck pain, as well as a variety of headaches, are commonly misdiagnosed or even sometimes go undiagnosed for an extended period. One of the top reasons neck pain may be so challenging to treat primarily because it takes a long time for people to take this health issue seriously and seek a proper diagnosis. When a patient seeks a diagnosis for neck pain, it may already have been a persistent problem. Waiting an extended amount of time to take care of your neck pain, especially after an injury, may lead to acute pain and even make the symptoms more difficult to control, turning them into chronic pain. Also, the most frequent reasons people seek treatment for neck pain, and headaches include the following:
Chronic migraines and headaches
Restricted neck function, including difficulties moving the head
Soreness in the neck, upper back, and shoulders
Stabbing pain and other symptoms, particularly in the neck
Pain radiating from the neck and shoulders to the fingertips
Aside from the symptoms mentioned above, individuals with neck pain and headaches can also experience additional symptoms, including nausea, diminished eyesight, difficulty concentrating, severe fatigue, and even difficulty sleeping. While there are circumstances in which the cause of your headaches or neck pain may be apparent, such as being in a recent automobile accident or suffering from sport-related trauma, damage, or injuries, in several instances, the cause may not be quite as obvious.
Because neck pain and headaches can also develop as a result of bad posture or even nutritional problems, it’s fundamental to find the origin of the pain to increase the success of treatment, in addition to enabling you to prevent the health issue from happening again in the future. It’s common for healthcare professionals to devote their time working with you to ascertain what could have caused the pain in the first place.
A Health Issue You Can’t Ignore
Neck pain is typically not a problem that should be ignored. You may think that you’re only experiencing minor neck discomfort and that it’s irrelevant to any other health issues you may be having. Still, you can’t know for sure more frequently than not until you receive a proper diagnosis for your symptoms. Patients seeking immediate medical attention and treatment for their neck-centered problems are surprised to learn that some of the other health issues they may be experiencing may be correlated, such as neck pain and headaches. Thus, even if you think you can “live with” not being able to turn your neck completely, other health issues can develop, and these problems might be more challenging to deal with.
There are circumstances in which a pinched nerve in the neck is the main reason for chronic tension headaches, where a previous sports injury that was not adequately addressed before is now the cause of the individual’s limited neck mobility and in which a bruised vertebrae at the base of the neck induces throbbing sensations throughout the spine, which radiates through the shoulders into the arms, hands, and fingers. You might also blame your chronic migraines on a hectic schedule and stressful conditions. However, it might be a consequence of poor posture and the hours you spend hunched over a computer screen. Untreated neck pain might lead to problems you never expect, such as balance problems or trouble gripping objects. This is because all the neural roots located on the upper ligaments of the cervical spine or neck are connected to other parts of the human body, from your biceps to each of your tiny fingers.
Working with a healthcare professional to relieve the root cause of your neck pain and headaches may significantly enhance your quality of life. It may be able to eliminate other symptoms from turning into a significant problems. While another health issue or nutritional deficiency generally causes the most common causes of chronic migraines, you might also be amazed to learn how often the outcome may be resolved with concentrated exercises and stretches recommended by a healthcare professional, such as a chiropractor. Additionally, you may understand that the health issues you’ve been having often develop from compressed, pinched, irritated, or inflamed nerves in your upper cervical nerves.
Dr. Alex Jimenez’s Insight
Although it may be difficult to distinguish the various types of headaches, neck pain is generally considered to be a common symptom associated with head pain. Cervicogenic headaches are very similar to migraines, however, the primary difference between these two types of head pain is that a migraine occurs in the brain while a cervicogenic headache occurs in the base of the skull or in the cervical spine, or neck. Furthermore, some headaches may be caused by stress, tiredness, eyestrain and/or trauma or injury along the complex structures of the cervical spine, or neck. If you are experiencing neck pain and headaches, it’s important to seek help from a healthcare professional in order to determine the true cause of your symptoms.
Treatment for Neck Pain and Headaches
Foremost, a healthcare professional must determine the cause of an individual’s symptoms through the use of appropriate diagnostic tools as well as to make sure they have the utmost success in relieving the headache and neck pain without prolonging the duration of the symptoms and extra cost of incorrect therapy. Once an individual’s source of neck pain and headaches has been diagnosed, the kind of treatment a patient receives should depend on the type of headache. As a rule of thumb, treatment starts once the diagnosis has been made. A healthcare professional will work with you to create a treatment plan appropriate for your specific health issues. You’ll be taken through procedures that help build flexibility and strength in your sessions.
Chiropractic care is a well-known alternative treatment option focusing on diagnosing, treating, and preventing various musculoskeletal and nervous system injuries and conditions. A chiropractic doctor or chiropractor can help treat neck pain and headache symptoms by carefully correcting any spinal misalignments, or subluxations, in the cervical spine or neck, through spinal adjustments and manual manipulations, among other therapeutic techniques. Chiropractors and physical therapists may also utilize a combination of gentle Muscle Energy Techniques, muscle building, joint slides, Cranio-sacral therapy, and specific posture and muscle re-education to lower the strain being placed on the structures surrounding the cervical spine. The staff will also help you understand how to better position yourself during your daily life to prevent relapses, like ergonomic and posture tips. Contact a healthcare professional for them to be able to assist you immediately.
In cases where alternative treatment options have been utilized without any results or sometimes used together with other complementary treatment approaches, pain drugs and medications may be contemplated, such as non-steroidal anti-inflammatory drugs (NSAIDs) and anti-seizure agents such as gabapentin, tricyclic anti-depressants, or migraine prescriptions. If pain medications prove ineffective, injections may be contemplated, including peripheral nerve blocks, atlantoaxial joint blocks administered at C1-C2, or aspect joint blocks administered in C2-C3. Surgical interventions may also be other treatment options. However, healthcare professionals suggest attempting all other treatment options before considering surgery. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please ask Dr. Jimenez or contact us at 915-850-0900.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once. The spine is a complex structure of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and aggravated conditions, such as herniated discs, eventually lead to back pain symptoms. Sports or automobile accident injuries are often the most frequent cause of back pain; however, sometimes, the simplest movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through spinal adjustments and manual manipulations, ultimately improving pain relief.
Chiropractic care is a drug-free, nonsurgical treatment for many types of conditions and to help manage pain. As more and more medical professionals are recognizing its effectiveness and viability for treating many issues in the body, chiropractic is gaining popularity and becoming the treatment of choice for many patients with chronic pain, back problems and other issues. In particular, it has been found to be a very effective treatment for spondylolisthesis. It can not only relieve the pain, but often return the patient�s mobility as well.
Contents
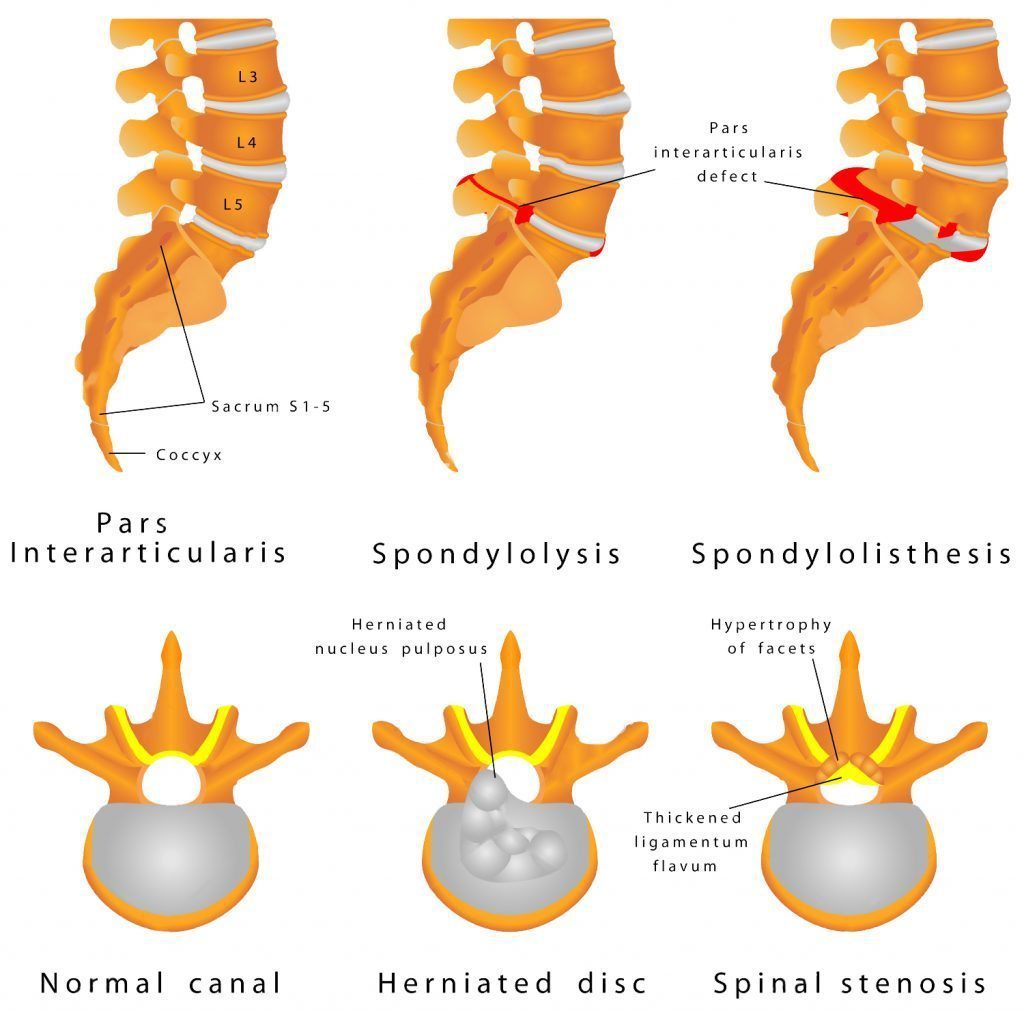
What Is Spondylolisthesis?
Spondylolisthesis is a condition in which one vertebra slides forward over the vertebra that is below it. It is typically confined to the lumbosacral, or lower back area. It can become painful, causing lower back pain and weakness or numbness in one or both legs, when it causes the nerve roots or spinal cord to be squeezed. In severe cases, a patient can lose control of their bowel or bladder function, but this is fairly rare. However, any patient who begins to lose bowel or bladder control should contact their doctor immediately.
In some cases, a person�s vertebra can slip out of place without any symptoms being present. Sometimes the symptoms don�t show up until months or even years later. Symptoms of spondylolisthesis may include:
Low back pain
Pain in the buttock area
Pain that radiates from the lower back down one or both legs
Spondylolisthesis is diagnosed by a doctor or chiropractor who may conduct several diagnostic tests. Typically, the doctor will take X-rays of the patient�s back to rule out certain conditions, especially if they suspect spondylolisthesis.
The X-ray will allow the doctor to see if any of the patient�s vertebrae have slipped out of place, or are cracked or fractured. An MRI or CT scan may also be ordered to better view the spine and see the extent of the damage.
What Are The Treatments For Spondylolisthesis?
The treatment for spondylolisthesis is based on the actual damage identified by the doctor, the pain and mobility problems that the patient is experiencing, and the overall severity of the condition. Rest is the first course of treatment as well as ceasing the physical activities that may have caused the damage in the first place.
Pain may be managed by non-steroidal anti-inflammatory drugs such as naproxen and ibuprofen. Acetaminophen may also be administered for pain.
Other treatments for spondylolisthesis include:
Bracing
Weight loss (if the person is obese or overweight)
Physical therapy to strengthen the core
Epidural steroid injections
Surgery (in severe cases such as damage to the spinal cord or nerve root)
There are several types of surgery that may be used to treat spondylolisthesis. The surgeon may remove tissue or bone in order to relieve pressure on the nerves or spinal cord. Sometimes the doctor may opt for fusing the damaged bones into place so they can no longer slip. In some cases, both procedures are done. This type of treatment is usually a last resort because recovery can be lengthy and the patient will have to wear a back brace or cast while their back is healing.
Is Chiropractic Effective For Treating Spondylolisthesis?
Chiropractic is a drug-free, noninvasive treatment for spondylolisthesis. It is often a preferred treatment because the patient does not have to undergo painful surgery or take medication that could have undesirable side effects. There are three primary spinal manipulation techniques that may be used by the chiropractor:
Spinal manipulation specific to the restricted or impaired joints
Flexion-distraction technique which is a slow, gentle pumping action
Instrument assisted manipulation uses an instrument to apply gentle force to the spine
Chiropractic care has been found to be very effective in treating this condition, but prevention is always the best course of action. Regular exercise, healthy weight management, and regular chiropractic visits can help ward off many spine related conditions including spondylolisthesis.
Shane Scott was involved in an automobile accident when he heard about Dr. Alex Jimenez, chiropractor, from a friend. After experiencing headache, neck and low back pain, several days after the incident, Shane Scott’s quality of life, especially as a new father, was tremendously affected. Thankfully, treatment with Dr. Alex Jimenez has helped Shane Scott return to his regular daily activities. Shane Scott highly recommends Dr. Alex Jimenez as the non-surgical choice for neck pain treatment, encouraging many others to visit him.
Chiropractic Neck Pain Treatment
Neck pain (or cervicalgia) is a frequent problem, where two-thirds of the populace will experience neck pain some time in their lives. Neck pain can be brought on by numerous other spinal issues. Neck pain may arise due to muscle tightness in either the neck and upper spine, or pinching of the nerves emanating from the cervical vertebrae. Joint disturbance in the neck generates pain, as does joint disruption in the top back. The head is supported by the lower neck and upper spine, and it is these places that commonly cause neck pain.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
TMJ dysfunction: The temporomandibular joints, TMJ, are the lower jaw hinges that sit on either side of the head in front of each ear. They are responsible for the lower jaw opening, closing, sliding, and rotating. The TMJs are the most body�s most complex joints. The typical person uses them more than 5,000 times a day by talking, laughing, yawning, chewing, eating, smiling, and swallowing.
Contents
What Is TMJ Dysfunction?
TMJ dysfunction occurs when one or both joints become inflamed or injured causing pain and immobility in the jaw area. Because these joints are used so often and tend to be far more mobile than most other joints in the body, they can be prone to pain.
It is important that both joints work together because if they don�t it could result in more pressure on one joint than the other and this could cause the pain and discomfort that is associated with TMJ dysfunction.
What Are The Symptoms Of TMJ Dysfunction?
There are many symptoms of TMJ dysfunction and they may vary depending on the patient, the extent of inflammation or injury, and the cause of the dysfunction. The symptoms may appear suddenly when there is injury to the joint, or they can gradually develop over a period of months or even years. They may be mild and barely noticeable or they can be severe and debilitating. The most common symptoms of TMJ dysfunction include:
Jaw pain
Jaw pain when moving the joint such as chewing or talking
Popping or clicking of the joint
Pain in the face or side of the neck
Locking jaw
Headaches
Toothache
Earache
Clogged or �stopped up� ear
Ringing in the ears (tinnitus)
TMJ dysfunction can significantly impact a person�s quality of life because the pain prevents them from doing many things they normally do, and often the jaw itself simply no longer functions as it should.
What Causes TMJ Dysfunction?
Damage to the joint is the primary cause of pain associated with TMJ dysfunction. This can be the result of trauma such as:
Subtle movements done repetitively can also cause TMJ dysfunction:
Grinding teeth
Holding a phone between the head and shoulder
Clenching teeth
Nail biting
Gum chewing (excessive)
Eating hard or tough foods
How Can Upper Neck Misalignment Cause TMJ Dysfunction?
When the upper neck sustains trauma such as whiplash it can cause a misalignment. This can also cause TMJ dysfunction in a couple of ways. It can cause one side to work harder or sustain more pressure than the other, or it can put excess pressure on the trigeminal nerve. This causes irritation and inflammation.
When left untreated, the condition can become severe. The misalignment keeps the joints from working as they should because opening and closing the jaw pinches the disc. This results in painful spasms in the shoulder and neck muscles when the patient does simple, everyday activities like talking, smiling, eating, or laughing.
Chiropractic For TMJ Dysfunction
Chiropractic can be a very effective treatment for TMJ dysfunction, especially if it is due to neck misalignment. A chiropractor will perform spinal adjustments in order to realign the spine and neck, bringing the body back into balance. This will allow the jaw to work as it should, minimizing rubbing or friction in the joint.
The patient may also be told to apply heat, massage, and do special exercises for TMJ dysfunction that will help the joints heal and help to minimize the pain.
This condition is not always easy to diagnose so it is wise to talk to your chiropractor and get a diagnosis before attempting any treatment or home remedies for TMJ. Regular chiropractic treatment can not only relieve the pain of TMJ and help to heal it, it can also help prevent it. Your chiropractor can be a great ally in this endeavor.
Injury Medical Clinic: Shoulder Pain Chiropractic Treatment
One of my friends recommended me, over and over, and just extended how good he�(Dr. Alex Jimenez, D.C.) was. So I gave it a shot. I had really bad sciatica and it was killing me, I couldn’t walk, but he has been helping me out, I can walk now… I couldn’t walk more than 25 yards, it (sciatica) was really affecting me. I had to get some help. I can’t say enough about Dr. Jimenez, he’s been helping me out, I can walk.
Contents
Edgar M. Reyes
According to the American Association of Neurological Surgeons, approximately 75 to 85 percent of individuals in the United States alone will experience some form of back pain throughout their lifetime, where 50 percent will suffer more than one episode within a year. Back pain is one of the most common complaints frequently reported among the general population and it is often a symptom which could indicate the presence of another underlying condition. Back pain can be caused by a variety of factors, some due to bad habits, such as improper posture, and others due to injuries from accidents. Other health issues, such as degenerative disc disease, or DDD, and arthritis can also result in back pain.�While the causes can vary, they share the same symptoms.
Bak pain can include upper back pain, middle back pain and lower back pain, often connected to sciatica, or sciatic nerve pain, a condition characterized by the compression or impingement of the sciatic nerve found in the low back. Back pain and sciatica have been closely associated with several common health issues. Often times, sciatica, or sciatic nerve pain, is caused by an underlying health issue along the lumbar spine. The sciatic nerve is the longest nerve in the human body, which connects to nerve roots in the region of the lower back and runs through the buttocks, down along the hips and into the back of each leg. Further sections of this nerve then branch out from the calf to the foot and into the toes. Sciatica can be identified by the following symptoms.
Low back pain which radiates down one or both legs
Leg and/or foot pain along with tingling and burning sensations
Numbness in the leg, feet and/or toes
Persistent pain and discomfort on one or both sides of the buttocks
Intense painful symptoms in the lower extremities
Having difficulties when sitting and while getting up
It’s essential to understand that back pain and sciatica are not generally considered to be a specific health issue themselves but rather, they are usually only considered to be a collection of several symptoms associated with an underlying injury and/or condition. A proper diagnosis of the root cause of your symptoms is additionally important in order to safely and effectively treat back pain and sciatica. As mentioned above, numerous factors can cause back pain and sciatica symptoms. Below, we will discuss some of the most common spine health issues which can cause back pain and sciatica, including degenerative disc disease, lumbar spinal stenosis, lumbar herniated disc and spondylolisthesis. Approximately 90 percent of sciatica cases are due to disc herniations.
Degenerative Disc Disease
The degeneration of the intervertebral discs, found between each vertebrae of the spine, is a natural process which often occurs with age, while for some individuals, however, it can begin to develop earlier than usual. In a healthy spine, the intervertebral discs function as shock absorbers between the bones of the spine, which ultimately provide height and allow the back to remain flexible while resisting forces. As we begin to get older, these rubbery discs begin to shrink and lose integrity. Almost everyone will demonstrate signs of wear-and-tear along their spinal discs over time, but not everyone will experience degenerative disc disease, or DDD. Although not actually a disease, DDD refers to a condition in which pain with the degeneration of the intervertebral discs.
One or more degenerated discs along the length of the spine may irritate a nerve root and cause sciatica. This condition is commonly characterized when a reduced disc becomes exposed. Bone spurs can also develop with disc degeneration and can lead to sciatica. Symptoms of degenerative disc disease, or DDD, frequently occur along the lower back, however, they can also develop in the neck, depending on the location of the degenerated discs. Common symptoms of DDD include, pain and discomfort, particularly when sitting, bending, lifting or twisting, tingling sensations and/or numbness in the extremities, and lessened symptoms when walking and moving, as in with changing positions or lying down. Weakness in the leg muscles or foot drop may be a sign that there is damage to the nerve root.
Lumbar Spinal Stenosis
Another common cause of back pain and sciatica is lumbar spinal stenosis. The natural degeneration of the spine which occurs with age can cause a variety of changes to the spine. Lumbar spinal stenosis is brought on by a gradual narrowing of the spinal canal that is common in the aging process and it generally affects people over the age of 50. When the space around the spinal cord narrows, it can place unnecessary amounts of pressure on the spinal cord and nerve roots. Additionally, it can be the result of a bulging disk, enlarged aspect joints, or an overgrowth of tissue. Only a small number of individuals are born with spine health issues which can develop into lumbar spinal stenosis. This is known as congenital spinal stenosis and it is frequently diagnosed in men.
Arthritis, or the degeneration of any joint in the body, has been attributed to be the most common cause of spinal stenosis. As the intervertebral discs begin to wear-and-tear naturally begin, they can lose water content and eventually dry out, ultimately losing height and even collapsing. This can place pressure on the facet joints, the joints which provide flexibility and movement to the spine, resulting in arthritis. As a result, the ligaments around the structures of the spine can increase in size, lessening the space for the nerves. Also, the human body may respond by growing new bone, additionally narrowing the space for the nerves to pass through. Symptoms of lumbar spinal stenosis may include, pain, tingling or burning sensations, numbness and weakness, as well as less painful symptoms when leaning forward or sitting.
Lumbar Herniated Disc
A herniated disc is a condition which can occur anywhere along the length of the spine, however, it most commonly affects the lower back or lumbar spine. It may also be referred to as a bulging, protruding or ruptured disc. A lumbar herniated disc is considered to be one of the most common causes of back pain in the lower back, as well as sciatica. An intervertebral disc begins to herniate when the soft, jelly-like nucleus, known as the nucleus pulposus, pushes against its outer ring, known as the annulus fibrosus, due to wear-and-tear or a sudden injury. With persistent pressure, the jelly-like nucleus may push through the disc’s outer ring or it may cause the ring to bulge, putting additional pressure on the spinal chord and its surrounding nerve roots.
Moreover, the intervertebral disc material can release chemicals and/or substances which may ultimately irritate the surrounding structures of the spine, contributing to nerve inflammation. When a nerve root becomes irritated, it can potentially lead to symptoms of pain and discomfort, numbness and weakness in one or both legs, otherwise referred to as sciatica, or sciatic nerve pain. An individual may also develop a herniated disc without ever experiencing any symptoms. A lumbar herniated disc is generally caused by the natural degeneration of the spine and discs, however, trauma and/or injury may also result in lumbar disc herniations. Symptoms of a lumbar herniated disc includes sciatica, tingling sensations, numbness, weakness, and loss of bladder or bowel control in severe cases. This last symptoms will require immediate medical attention.
Spondylolisthesis
Spondylolisthesis is another common cause of back pain and sciatica, particularly in young athletes. Repeated stress on the lower back, or lumbar spine, can create a crack or stress fracture in one of the vertebrae. In these cases, however, the stress fracture can often weaken the bone so much, to the point where it is unable to maintain its proper position in the spine, ultimately causing the vertebra to begin to shift or slip out of place. This condition is what is commonly known as spondylolisthesis. In children and adolescents, spondylolisthesis can occur through periods of rapid growth, by way of instance, during an adolescent growth spurt. This condition frequently occurs as a result of overuse, overstretching, or hyperextension, and even due to genetics.
Many healthcare professionals characterize spondylolisthesis as either low grade or high grade, depending on how much the vertebrae have shifted or slipped out of place. A high grade slip is generally identified when more than 50 percent of the width of the fractured vertebra slips forwards onto the vertebra beneath it. Individuals with high grade cases of spondylolisthesis will commonly describe experiencing significant levels of pain and discomfort as well as nerve injury. In the majority of instances, however, individuals with spondylolisthesis will not experience any obvious symptoms, as a matter of fact, most are unaware of the condition till an x-ray is taken for an unrelated injury and/or condition. Individuals with spondylolisthesis may experience back pain and sciatica, including muscle spasms, back stiffness and tight hamstrings.
Dr. Alex Jimenez’s Insight
Back pain is one of the most common reasons why individuals often miss days from work or go to the doctor, as it has also become one of the leading causes of disability worldwide. As a matter of fact, it has been statistically determined that approximately 80 percent of people will or have experienced back pain at least once throughout their life. Fortunately, a variety of treatments are available which can help ease the symptoms of back pain. It’s essential to understand back pain and sciatica, a collection of symptoms commonly associated with spine health issues along the lower back, in order to seek proper diagnosis and continue with an appropriate treatment plan in order to relieve your symptoms of back pain and sciatica.
Treatment for Back Pain and Sciatica
Chiropractic care is a well-known, alternative treatment option commonly utilized to help diagnose, treat and prevent back pain and sciatica. Since there are many factors which can contribute to symptoms of back pain and sciatic nerve pain, a doctor of chiropractic’s, or chiropractor’s, initial step would be to determine the root cause of the patient’s symptoms. Determining a diagnosis involves a thoughtful review of the patient’s health history, and a physical and neurological examination. Diagnostic testing may involve an x-ray, MRI, CT scan and/or electrodiagnostic tests, such as a nerve conduction speed evaluation or an electromyography. These examinations and tests help determine possible contraindications to treatment.
The aim of chiropractic care is to help promote the human body’s potential to heal itself. It is based on the scientific principle that limited spinal motion results in pain and reduced function and performance. Chiropractic care is non-invasive, or non-surgical, and drug-free. The type of chiropractic treatment provided is dependent upon the cause of the individual’s back pain and sciatica. A treatment program may include many distinct treatments and therapies, like ice/cold therapies, ultrasound, TENS, and spinal adjustments or manual manipulations. If the doctor of chiropractic decides that the patient’s spinal health issue requires treatment by a different kind of physician, then the individual may be referred to another healthcare professional.
Physical therapeutics for these conditions is also effective and generally has two components: active and passive. Passive physical therapeutics consist of ultrasound, electric stimulation, heat and ice packs as well as iontophoresis. Active physical therapeutics modalities include stretching exercises, back exercises and low-impact aerobic conditioning. Manual physical therapeutics, such as spinal adjustments and/or manual manipulations, might be integrated in part by a chiropractor. Physical therapists normally recommend 20 minutes of dynamic lumbar stabilization exercises every day. Core muscle strengthening is also important in treating back pain. Low-impact aerobics are also important and include water therapy, biking, and walking.
Physical therapeutics are an important element of treating spinal health issues. If you meet with a physical therapist, there will be a full assessment. Tests will be performed and an individualized treatment plan will be developed based on the patient’s goals. If you’re experiencing back pain or sciatica, don’t wait any longer for relief. Contact a healthcare professional to establish a one-on-one consultation and complete evaluation. Many chiropractors and physical therapists are certified, experienced and dedicated to helping you feel better. They have helped many others recover from spinal health issues and can help you too. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Many headaches that people classify as migraines are actually not migraines at all. Two of the most common headaches confused with migraines are sinus headaches and occipital neuralgia.
The condition can be debilitating but there are treatments, including chiropractic, that are very effective. Understanding occipital neuralgia can help patients better manage it so they can minimize the pain and symptoms of the condition.
Contents
What Is Occipital Neuralgia?
Occipital neuralgia is a neurological condition that affects the occipital nerves which run from the top portion of the spinal cord, through the scalp, transmitting messages to and from the brain. There are two greater occipital nerves, one on each side of the head, from between the vertebrae located in the upper neck through the muscles that are located at the base of the skull and back of the head.
While they do not cover the areas on or near the ears or over the face, they can extend over the scalp as far as the forehead. When those nerves are injured or become inflamed, occipital neuralgia is the result. A person with this condition may experience pain at the base of their skull or the back of their head.
What Are The Symptoms Of Occipital Neuralgia?
Pain is the prevalent symptom of occipital neuralgia. It often mimics the pain of migraine headaches or cluster headaches and is described as throbbing, burning, and aching.
There may also be intermittent shooting or shocking pain. Typically, the pain begins at the base of the skull but may radiate along the side of the scalp or in the back of the head. Other symptoms include:
Pain is experienced on one side (but sometimes both sides)
Pain behind the eye of the side that is affected
Tenderness in the scalp
Sensitivity to light
Pain triggered by neck movement
What Causes Occipital Neuralgia?
Irritation or pressure to the occipital nerves are what actually cause the pain. This may be due to tight muscles in the neck that squeeze or trap the nerves, injury, or inflammation.
However, much of the time doctors are unable to determine the cause. There are several medical conditions linked to occipital neuralgia:
Tight neck muscles
Diabetes
Trauma or injury to the back of the head
Gout
Tension in the neck muscles
Whiplash
Inflammation of the blood vessels in and around the neck
Infection
Neck tumors
Cervical disc disease
Osteoarthritis
What Are The Treatments For Occipital Neuralgia?
Occipital neuralgia treatment focuses on pain relief. It often begins with conservative treatments that include:
In more severe cases the patient may be prescribed a stronger anti-inflammatory medication, muscle relaxants or in some cases an anticonvulsant medication.
If these therapies are not effective or do not bring about the desired level of pain relief, then doctors may recommend percutaneous nerve blocks and steroids. Sometimes surgery is recommended in cases where the pain is severe, chronic, and is unresponsive to more conservative treatments.
Chiropractic For Occipital Neuralgia
Chiropractic was once considered an �alternative� treatment for occipital neuralgia, but now it is often a regular part of recommended patient care. The advantage of chiropractic over medication or surgery is that chiropractic does not come with the side effects of drugs or the risks of surgery.
Another advantage is that chiropractic seeks to correct the root of the problem, not just manage the pain like other treatments.
Chiropractic treatment for occipital neuralgia may include lift adjustments, heat, massage, and traction. This will bring the body back into proper alignment and take the pressure off of the nerves as it loosens the neck muscles.
The patient stands a better chance of staying pain free when taking this treatment route.
Injury Medical Clinic: Doctor Of Chiropractic Near Me
Louie Martinez, business owner, first chose to see Dr. Alex Jimenez, chiropractor, after he suffered several injuries which resulted in lower back pain, among other symptoms. Louie Martinez trusts in Dr. Alex Jimenez’s treatment because it gives him the thorough relief he needs immediately. Before seeing Dr. Alex Jimenez for lower back pain treatment, Louie Martinez experienced pain and limited mobility. However, after initial treatment, his symptoms were tremendously improved. Louie Martinez highly recommends Dr. Alex Jimenez as the non-surgical choice for lower bak pain treatment, among others.
Lower Back Pain Chiropractic Treatment
A lumbar strain is a stretch injury to the ligaments, tendons, and/or muscles of the lower spine. The extending episode ends up in microscopic tears of varying degrees in those cells. A lumbar strain is considered one of the most frequent causes of lower back pain. The injury can occur due to overuse, improper use, or injury. Soft-tissue injury is commonly categorized as “severe” if it has been present for weeks. If the strain lasts longer than three months, it is known as “chronic.” Lumbar strain most often happens in individuals in their 40’s, however, it can occur at any age. The health issue is characterized by localized discomfort in the lower back region.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Did you know that inflammation and low back pain can by caused by a low pH balance? Inflammation is believed to be caused by a variety of factors, including injury and/or an underlying condition, however, recent research studies have found a connection between inflammation, chronic back pain and pH balance. The lower your pH balance is, the more acidic your body is. When the human body is acidic, a condition referred to as acidosis, it can cause inflammation and other symptoms throughout the body, even in the lower back. Whether your pH balance or another health issue is causing your low back pain, it’s important to understand how acidity and low pH levels can affect the structure and function of the human body.
Metabolic acidosis is a condition used to describe when there is too much acid in your body fluids. When there is too much acid in your body, your pH balance reading will be low. In other words, your body will be considered acidic. When the human body is acidic, it neutralizes the acid by leaching calcium, magnesium, potassium and sodium from the bones. Over time, the excess acidity of the body can begin to gradually eat away at the bones, causing the progressive degeneration of the bones and eventually even leading to fractures. While a fracture may seem like a severe cause for back pain, the degeneration of the vertebrae of the spine can also cause disc degeneration disease, or DDD, leading to back pain and low back pain. The purpose of the article below is to demonstrate as well as discuss the relationship between low pH balance in intervertebral discs and low back pain.
Contents
The Relationship Between Low PH in Intervertebral Discs and Low Back Pain: a Systematic Review
Abstract
Introduction: To systematically review the relationship between low pH in intervertebral discs and low back pain.
Material and methods: Electronic database (PubMed, ISI Web of Science, Cochrane Library, CINAHL, AMED, and China National Knowledge Infrastructure) searches and hand searching of conference proceedings were conducted. Two authors independently evaluated the methodological quality and abstracted relevant data according to standard criteria. Then the experimental methods and samples employed in the finally retrieved articles were assessed.
Results: We first retrieved 136 articles regarding pain and pH, and only 16 of them were mainly about low back pain and pH. Finally, 7 articles met our expectation to focus on the pathogenesis of low back pain caused by pH. In these 7 studies the authors held three opinions to explain the pathogenesis of low back pain in relation to low pH. First, low pH caused by lactate stimulates the muscle and increases the muscle tension, which causes low back pain. Second, low pH stimulates the nerve roots and produces the feeling of pain. Third, low pH changes the matrix metabolism, leading to neuronal death and low back pain.
Conclusions: In this systematic review we propose a new hypothesis that low back pain may be caused by low pH based on the previous literature. Further experimental studies are necessary to verify our hypothesis. This hypothesis will promote our understanding of the pathogenesis of low back pain and the development of novel diagnostic and therapeutic approaches for low back pain.
Keywords:low back pain, pH, acidity, intervertebral disc, systematic review
Introduction
Low back pain is one of the most frequent causes of morbidity and disability. Low back pain affects up to 50% to 80% of the population in developed countries and its recurrence rate amounts to 85%, resulting in an economic loss of approximately 50 to 100 billion dollars per year in the US [1, 2].
Currently, effective treatment of low back pain is severely hampered due to the fact that its pathogenesis remains elusive [3, 4]. In recent years, several hypotheses have been proposed to explain the pathogenesis of low back pain and most of them focus on the dysfunction of the spinal column and its components, such as injury and clinical instability [5�7], spinal column degeneration [8], inferior facet-tip impingement on the lamina [9], and Schmorl’s nodes [10] and facet joint injury [11]. Other hypotheses focus on subfailure injury of the spinal muscles and ligaments and propose that spinal ligaments, disc annulus, facet capsules and thoracolumbar fascia may cause chronic back pain due to muscle control dysfunction [12�16]. In addition, the pain adaptation and pain-spasm-pain hypotheses have been proposed [17�19]. However, these hypotheses are largely speculative and need further experimental investigations.
The intervertebral disc (IVD) is composed of the nucleus pulposus (NP), the annulus fibrosus (AF), and the endplates (EP). The corpora vertebrae lie above and below the discs. The healthy disc is avascular, and its nutrition depends on diffusion via the AF and EP [20, 21]. The discs mainly produce ATP via anaerobic glycolysis; consequently lactate is produced and the pH is lower than other tissues. Low back pain is known to be related to intervertebral disc degeneration, and the pH would decrease in degenerated intervertebral discs [22, 23]. Therefore, low pH in the discs may be related to low back pain. Indeed, Hambly and Mooney [24] reported a close relationship between low back pain and low intradiscal pH in rabbits, while Krapf et al. [25] found that low pH could cause muscle spasm which was related to low back pain.
Based on the previous literature we propose a new hypothesis that low pH may cause low back pain. In this systematic review, we have collected and analysed the relevant literature regarding the relationship between low pH and low back pain to address the following questions: (1) What role does low pH play in low back pain? (2) Is the relationship obvious between low pH and low back pain? And (3), why are low pH and low back pain so relevant?
Material and Methods
Electronic databases (PubMed, ISI Web of Science, Cochrane Library, CINAHL, AMED, and China National Knowledge Infrastructure), which were last updated on 26 Nov. 2011, were searched without limit by two independent investigators. The search used terms and Boolean operators as follows: (low back pain OR lower back pain OR low back ache OR low backaches OR lumbago OR recurrent low back pain OR postural low back pain or mechanical low back pain) AND (low pH OR lactate OR lactate OR hydrogen ion concentration). Reference lists of all the selected articles were hand-searched for any additional trials. Conference abstracts of key pain and orthopaedic journals were hand-searched to identify unpublished data. If necessary, we contacted the authors to get additional information.
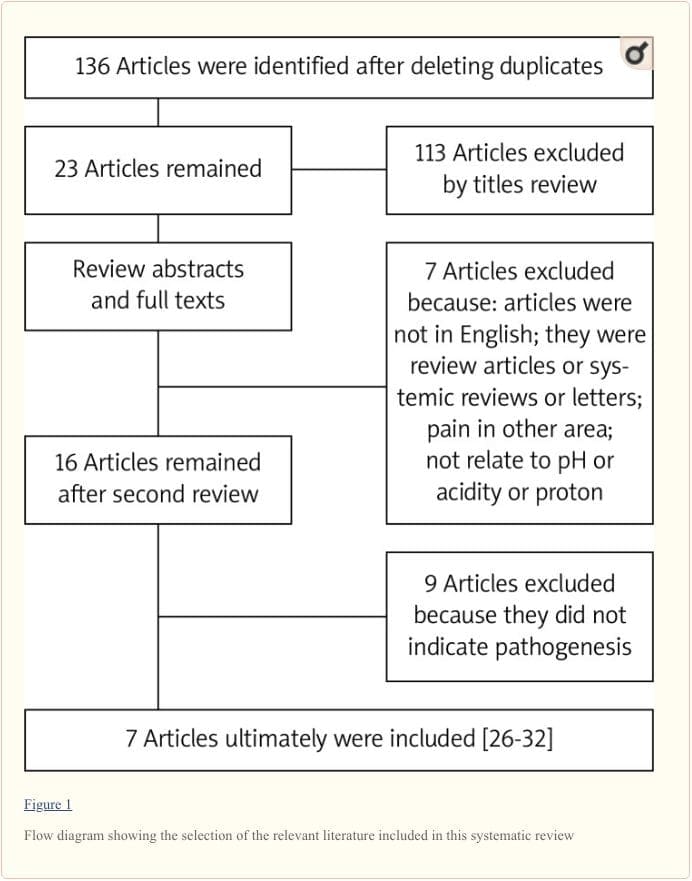
In total 136 articles were initially identified by literature search, and 113 articles were excluded after checking the titles and abstracts, which did not reach our expectation. Next we reviewed the full texts of the remaining articles and excluded the following articles: (1) articles not in English; (2) reviews, systematic reviews or letters; (3) pain in other tissues; (4) not related to pH, acidity or protons. As a result, 16 articles were retrieved and the references of these 16 articles were checked to ensure that other pertinent publications would not be missed. Finally, seven articles met our expectation to focus on the pathogenesis of low back pain caused by pH (Figure 1). The literature search was performed by two of the authors (CZL and HL) independently, and any disagreement was resolved by discussion.
We scrutinized the seven articles with the focus on �the mechanisms by which pH causes low back pain�, and then assessed the experimental methods and samples employed in the seven articles.
Results
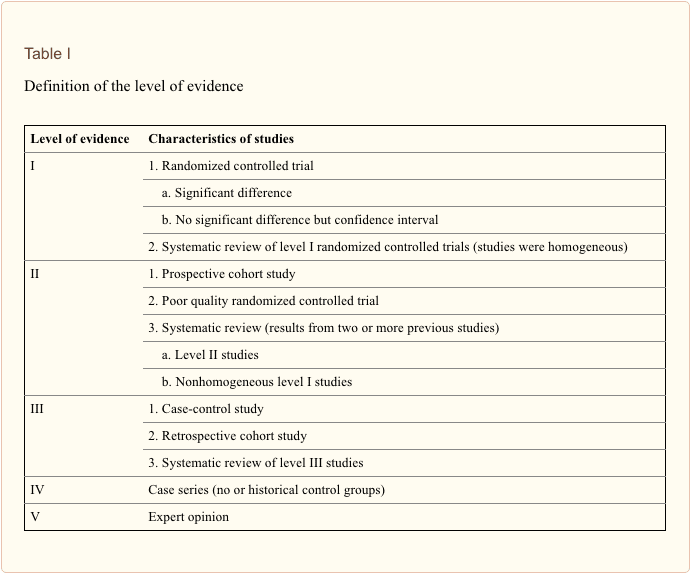
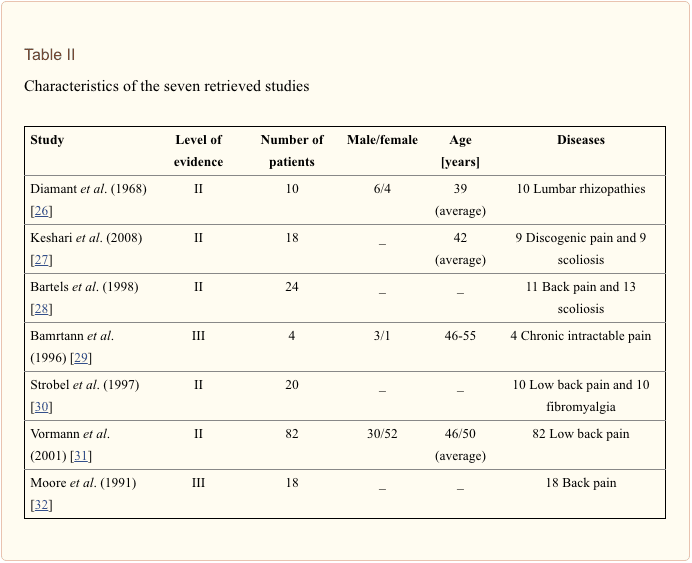
Seven articles met our expectation [26�32]. Then we evaluated the level of evidence for each article, according to the standard listed in Table I [33]. Five of them were level II, and two were level III. The characteristics of the seven studies are listed in Table II.
Nerve Roots
Three studies involving 32 patients [26, 27, 29] suggested that low pH would stimulate the nerve roots and cause low back pain.
Diamant et al. analysed the correlation between lactate level and pH in discs of patients with lumbar rhizopathy and found that low pH was caused by the increased lactate level due to the enhanced anaerobic glycolysis within the NP, which counteracts the decreased nutritional diffusion. The reaction of nerve roots in cases with low pH is related to increased production and leakage of acid metabolism. Sensitive structures such as the nerve roots could be irritated by the leakage of acid metabolites and it was shown that pain will arise in tissues with low pH [26, 34].
Keshari et al. used HR-MAS NMR spectroscopy to analyse snap frozen samples taken from 9 patients who underwent discectomy for painful disc degeneration [27, 35, 36]. They found that proteoglycan, collagen, and lactate may serve as metabolism markers of discogenic back pain. Therefore, they speculated that low pH was caused by increased lactate and increased lactate stimulated nerve fibres in granulation tissue associated with disc healing, which was correlated with discogenic pain [27, 35, 36].
Baumann et al. examined the responses of cultured adult human dorsal root ganglion (hDRG) neurons to low pH [29]. They found that low pH evoked, sustained depolarizations were due to more than one mechanism, and the inhibition of resting membrane conductance contributes to the responses to low pH in some hDRG neurons, which was related to low back pain [29].
Muscle Tension and Swelling of Connective Tissue
A previous study suggested that low pH would increase muscle tension, which could cause low back pain [30]. The authors examined 20 patients with chronic palpable tension of the erector muscles of the spine, and found that the pH decreased because of the enhanced anaerobic glycolysis in NP. The low pH was caused by the accumulation of lactate. Lactate would stimulate the multifidus muscle and increase the muscle tension. Simultaneously, myogelosis is induced, leading to low back pain [30]. Vormann et al. [31] showed that the simple and safe addition of an alkaline multimineral preparate was able to reduce the pain symptoms in these patients with chronic low back pain. These results suggest that a disturbed acid-base balance may contribute to the symptoms of low back pain.
Metabolism
Bartels et al. measured the oxygen and lactate concentrations in 11 patients with back pain and 13 patients with scoliosis, and found that in each case, the oxygen and lactate concentrations were the highest in the interior of the disc and fell toward the outer annulus [28]. Therefore, they speculated that the microcirculation through the endplate and the rate of cellular metabolism would influence the oxygen and lactate concentrations in the disc. For instance, the oxygen concentration would fall as cellular demand increases; consequently the lactate concentration would increase and the pH would decrease. It was observed that in some discs the concentration of oxygen was less than 40 mm Hg and that of lactate was more than 5 mmol/l, which would lead to cell death.
Another study also indicated that decreased pH, decreased PO2 and increased PCO2 may be related to the mechanisms of pain production in patients with back pain [32]. These abnormalities can be identified by magnetic resonance imaging. Further investigation is needed to determine whether therapeutic manipulation of these variables can be effective in relieving axial spinal pain.
Low pH would lead to a change in the matrix metabolism, which could strongly influence the cell activity and even cause cell death. It is well known that acid-sensing ion channels (ASICs) on the cell surface could be stimulated by protons. After cells die, the protons would increase and activate ASICs, which in turn mediate ischaemic neuronal death [37], and eventually cause low back pain [28, 38�40].
Dr. Alex Jimenez’s Insight
When an individual’s bodily fluids contain too much acid, or they’re too acidic,�a common concern known as acidosis, it can lead to a variety of health issues if not properly addressed. Your lungs and kidneys can generally compensate for slight pH imbalances, however, problems with any of these organs or even an improper nutrition consisting of processed foods high in sugar, can result in excess acid accumulating in the human body. Other risk factors which can contribute to an increased chance of developing acidosis include: a high-fat diet that’s low in carbohydrates, kidney failure, obesity, dehydration, aspirin or methanol poisoning, and diabetes. Furthermore, as mentioned in the article, acidosis has also been associated as a cause of inflammation which may lead to chronic back pain and low back pain. Therefore, maintaining pH balance is believed to be able to help treat low back pain, alongside other alternative treatment options, such as chiropractic care.
Discussion
After careful review of the seven articles we retrieved, we obtained a systematic view with regard to the relationship between low pH and low back pain, although the authors of the individual studies had proposed three different opinions.
If low pH directly stimulates the nerve roots, the pH is very important to the healing of low back pain. Lactate would cause low pH, stimulate the nerve roots, cause depolarization at the surface of the nerves, and modulate the nociceptors to let the patients feel pain. However, in order to establish a relationship between discogenic back pain and lactate, a much larger number of patients need to be studied and the changes in proteoglycans (PG)/collagen (col), PG/lactate peak (Lac), and Lac/col ratios should be correlated with visual pain scores or other pain indexes [27, 29].
The second opinion holds that low pH would act on the muscle but not nerve roots. If the oxygen tension falls below 5 mm Hg, the muscle tension would increase, and even result in myogelosis. Muscle contraction depends solely on the chemical energy of ATP. If the oxygen tension decreased, the cells would undergo anaerobic glycolysis and produce much lactate, leading to decreased pH. However, it remains elusive what level of pH would cause pain [30].
The third opinion claims that disc energy and matrix metabolism are crucially involved in low back pain [38�40]. This provides a valuable insight into the pathogenesis of low back pain. Nevertheless, the detailed cellular and molecular mechanisms by which disc energy and matrix metabolism disruption lead to neuronal death and eventually pain development are not completely understood.
This systematic review had several limitations. First, the heterogeneity between individual studies was substantial. Second, there are only small number patients in several prospective cohort studies of selected articles. Third, there may be some selection bias because the retrieved articles were confined to limited databases.
In conclusion, in this systematic review we propose a new hypothesis that low back pain may be caused by low pH based on previous literature, in which three opinions have been proposed by the authors to explain the pathogenesis of low back pain in relation to low pH. First, low pH caused by lactate stimulates the muscle and increases the muscle tension, which would cause low back pain. Second, low pH stimulates the nerve roots and produces the feeling of pain. Third, low pH changes the matrix metabolism, leading to neuronal death and low back pain. These different opinions are not exclusive but may be complementary. Further experimental studies are necessary to verify our hypothesis that low pH causes low back pain. This hypothesis will promote our understanding of the pathogenesis of low back pain and the development of novel diagnostic and therapeutic approaches for low back pain.
Acknowledgments
This study was partly supported by a grant from the National Nature Science Foundation of China (81171756) and the Science and Technology Planning Project of Zhejiang Province (2012C13G2010083).
In conclusion,�a lower pH balance can mean that your blood is more acidic, while a higher pH balance means that your blood is closer to the levels it should be at. While these numbers may only appear to differentiate slightly, these numerical differences can be serious and may ultimately affect your overall health and wellness. In the article above, researchers proposed that low back pain may be caused by low pH levels. Furthermore, the outcome measures of the systematic review will help support the understanding of the pathogenesis of low back pain, promoting more treatment options for chronic back pain. Information referenced from the National Center for Biotechnology Information (NCBI).�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
4.�Ghahreman A, Bogduk N. Predictors of a favorable response to transforaminal injection of steroids in patients with lumbar radicular pain due to disc herniation.�Pain Med.�2011;12:871�9.�[PubMed]
5.�Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis.�J Spinal Disord.�1992;5:390�6.�[PubMed]
6.�Depalma M, Ketchum J, Saullo T, Schofferman J. Structural etiology of chronic low back pain due to motor vehicle collision.�Pain Med.�2011;12:1622�7.�[PubMed]
7.�Raczkowski JW, Daniszewska B, Zolynski K. Functional scoliosis caused by leg length discrepancy.�Arch Med Sci.�2010;6:393�8.�[PMC free article]�[PubMed]
8.�Kirkaldy-Willis WH, Wedge JH, Yong-Hing K, Reilly J. Pathology and pathogenesis of lumbar spondylosis and stenosis.�Spine.�1978;3:319�28.�[PubMed]
9.�Yang KH, King AI. Mechanism of facet load transmission as a hypothesis for low-back pain.�Spine.�1984;9:557�65.�[PubMed]
10.�Lipson SJ, Fox DA, Sosman JL. Symptomatic intravertebral disc herniation (Schmorl’s node) in the cervical spine.�Ann Rheum Dis.�1985;44:857�9.�[PMC free article]�[PubMed]
11.�Farfan HF, Sullivan JD. The relation of facet orientation to intervertebral disc failure.�Can J Surg.�1967;10:179�85.�[PubMed]
12.�Schleip R, Vleeming A, Lehmann-Horn F, Klingler W. Letter to the Editor concerning �A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction� (M. Panjabi)�Eur Spine J.�2007;16:1733�5.�[PMC free article]�[PubMed]
13.�Panjabi MM. A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction.�Eur Spine J.�2006;15:668�76.�[PMC free article]�[PubMed]
14.�DePalma MJ, Ketchum JM, Saullo TR. Etiology of chronic low back pain in patients having undergone lumbar fusion.�Pain Med.�2011;12:732�9.�[PubMed]
15.�Karabekir HS, Yildizhan A, Atar EK, et al. Effect of ligamenta flava hypertrophy on lumbar disc herniation with contralateral symptoms and signs: a clinical and morphometric study.�Arch Med Sci.�2010;6:617�22.�[PMC free article]�[PubMed]
16.�Petronic I, Nikolic D, Cirovic D, et al. Distribution of affected muscles and degree of neurogenic lesion in patients with spina bifida.�Arch Med Sci.�2011;7:1049�54.�[PMC free article]�[PubMed]
17.�van Dieen JH, Selen LP, Cholewicki J. Trunk muscle activation in low-back pain patients, an analysis of the literature.�J Electromyogr Kinesiol.�2003;13:333�51.�[PubMed]
18.�Lund JP, Donga R, Widmer CG, Stohler CS. The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity.�Can J Physiol Pharmacol.�1991;69:683�94.�[PubMed]
19.�Maigne JY, Vautravers P. Mechanism of action of spinal manipulative therapy.�Joint Bone Spine.�2003;70:336�41.�[PubMed]
20.�Roberts S, Evans H, Trivedi J, Menage J. Histology and pathology of the human intervertebral disc.�J Bone Joint Surg Am.�2006;88(Suppl 2):10�4.�[PubMed]
21.�Raj PP. Intervertebral disc: anatomy-physiology-pathophysiology-treatment.�Pain Pract.�2008;8:18�44.[PubMed]
22.�Kitano T, Zerwekh JE, Usui Y, et al. Biochemical changes associated with the symptomatic human intervertebral disk.�Clin Orthop Relat Res.�1993;293:372�7.�[PubMed]
23.�Wuertz K, Godburn K, Iatridis JC. MSC response to pH levels found in degenerating intervertebral discs.�Biochem Biophys Res Commun.�2009;379:824�9.�[PMC free article]�[PubMed]
24.�Hambly MF, Mooney V. Effect of smoking and pulsed electromagnetic fields on intradiscal pH in rabbits.�Spine.�1992;17:S83�5.�[PubMed]
25.�Krapf MW, Muller S, Mennet P, et al. Recording muscle spasm in the musculus erector spinae using in vivo 31P magnetic resonance spectroscopy in patients with chronic lumbalgia and generalized tendomyopathies.�Z Rheumatol.�1992;51:229�37.�[PubMed]
26.�Diamant B, Karlsson J, Nachemson A. Correlation between lactate levels and pH in discs of patients with lumbar rhizopathies.�Experientia.�1968;24:1195�6.�[PubMed]
27.�Keshari KR, Lotz JC, Link TM, et al. Lactic acid and proteoglycans as metabolic markers for discogenic back pain.�Spine.�2008;33:312�7.�[PubMed]
28.�Bartels EM, Fairbank JC, Winlove CP, Urban JP. Oxygen and lactate concentrations measured in vivo in the intervertebral discs of patients with scoliosis and back pain.�Spine.�1998;23:1�7.�[PubMed]
29.�Baumann TK, Burchiel KJ, Ingram SL, Martenson ME. Responses of adult human dorsal root ganglion neurons in culture to capsaicin and low pH.�Pain.�1996;65:31�8.�[PubMed]
30.�Strobel ES, Krapf M, Suckfull M, et al. Tissue oxygen measurement and 31P magnetic resonance spectroscopy in patients with muscle tension and fibromyalgia.�Rheumatol Int.�1997;16:175�80.�[PubMed]
31.�Vormann J, Worlitschek M, Goedecke T, Silver B. Supplementation with alkaline minerals reduces symptoms in patients with chronic low back pain.�J Trace Elem Med Biol.�2001;15:179�83.�[PubMed]
32.�Moore MR, Brown CW, Brugman JL, et al. Relationship between vertebral intraosseous pressure, pH, PO2, pCO2, and magnetic resonance imaging signal inhomogeneity in patients with back pain. An in vivo study.�Spine.�1991;16:S239�42.�[PubMed]
33.�Prommahachai A, Wittayapirot K, Jirarattanaphochai K, Sae-Jung S. Correction with instrumented fusion versus non-corrective surgery for degenerative lumbar scoliosis: a systematic review.�J Med Assoc Thai.�2010;93:920�9.�[PubMed]
34.�Menkin V. Biochemical mechanisms in inflammation.�Br Med J.�1960;1:1521�8.�[PMC free article][PubMed]
35.�Aoki Y, Akeda K, An H, et al. Nerve fiber ingrowth into scar tissue formed following nucleus pulposus extrusion in the rabbit anular-puncture disc degeneration model: effects of depth of puncture.�Spine.�2006;31:E774�80.�[PubMed]
36.�Ozawa T, Ohtori S, Inoue G, et al. The degenerated lumbar intervertebral disc is innervated primarily by peptide-containing sensory nerve fibers in humans.�Spine.�2006;31:2418�22.�[PubMed]
37.�Wang YZ, Xu TL. Acidosis, acid-sensing ion channels, and neuronal cell death.�Mol Neurobiol.�2011;44:350�8.�[PubMed]
38.�Ohshima H, Urban JP. The effect of lactate and pH on proteoglycan and protein synthesis rates in the intervertebral disc.�Spine.�1992;17:1079�82.�[PubMed]
39.�Ishihara H, Urban JP. Effects of low oxygen concentrations and metabolic inhibitors on proteoglycan and protein synthesis rates in the intervertebral disc.�J Orthop Res.�1999;17:829�35.�[PubMed]
40.�Holm S, Maroudas A, Urban JP, Selstam G, Nachemson A. Nutrition of the intervertebral disc: solute transport and metabolism.�Connect Tissue Res.�1981;8:101�19.�[PubMed]
Difficulty making eye contact, gestures and words at the same time
Little imitation of others
No longer uses words they used to use
Uses another person�s hand as a tool
Social Interaction
Difficulty making eye contact
Lack of joyful expression
Lack of responsiveness to name
Does not try to show you things they�re interested in
Repetitive Behaviors & Restricted Interests
Unusual way of moving their hands, fingers or body
Develops rituals, such as lining up objects or repeating things
Focuses on unusual objects
Excessive interest in a particular object or activity which interferes with social interaction
Unusual sensory interests
Under or over reaction to sensory input
ASD Diagnostic Criteria (DSM-5)
Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history (examples are illustrative, not exhaustive; see text):
Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
Deficits in developing, maintaining, and understand relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
ASD Diagnostic Criteria
Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive; see text):
Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypes, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
Hyper – or Hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g. apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
ASD Diagnostic Criteria
Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
ASD Diagnostic Criteria (ICD- 10)
A. Abnormal or impaired development is evident before the age of 3 years in at least one of the following areas:
Receptive or expressive language as used in social communication;
The development of selective social attachments or of reciprocal social interaction;
Functional or symbolic play.
B. A total of at least six symptoms from (1), (2) and (3) must be present, with at least two from (1) and at least one from each of (2) and (3)
1. Qualitative impairment in social interaction are manifest in at least two of the following areas:
a. failure adequately to use eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction;
b. failure to develop (in a manner appropriate to mental age, and despite ample opportunities) peer relationships that involve a mutual sharing of interests, activities and emotions;
c. lack of socio-emotional reciprocity as shown by an impaired or deviant response to other people�s emotions; or lack of modulation of behavior according to
social context; or a weak integration of social, emotional, and communicative behaviors;
d. lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. a lack of showing, bringing, or pointing out to other people objects of interest to the individual).
2. Qualitative abnormalities in communication as manifest in at least one of the following areas:
a. delay in or total lack of, development of spoken language that is not accompanied by an attempt to compensate through the use of gestures or mime as an alternative mode of communication (often preceded by a lack of communicative babbling);
b. relative failure to initiate or sustain conversational interchange (at whatever level of language skill is present), in which there is reciprocal responsiveness to the communications of the other person;
c. stereotyped and repetitive use of language or idiosyncratic use of words or phrases;
d. lack of varied spontaneous make-believe play or (when young) social imitative play
3. Restricted, repetitive, and stereotyped patterns of behavior, interests, and activities are manifested in at least one of the following:
a. An encompassing preoccupation with one or more stereotyped and restricted patterns of interest that are abnormal in content or focus; or one or more interests that are abnormal in their intensity and circumscribed nature though not in their content or focus;
b. Apparently compulsive adherence to specific, nonfunctional routines or rituals;
c. Stereotyped and repetitive motor mannerisms that involve either hand or finger flapping or twisting or complex whole body movements;
d. Preoccupations with part-objects of non-functional elements of play materials (such as their oder, the feel of their surface, or the noise or vibration they
generate).
C. The clinical picture is not attributable to the other varieties of pervasive developmental disorders; specific development disorder of receptive language (F80.2) with secondary socio-emotional problems, reactive attachment disorder (F94.1) or disinhibited attachment disorder (F94.2); mental retardation (F70-F72) with some associated emotional or behavioral disorders; schizophrenia (F20.-) of unusually early onset; and Rett�s Syndrome (F84.12).
Asperger�s Syndrome Diagnostic Criteria (ICD-10)
A. Qualitative impairment in social interaction, as manifested by at least two of the following:
marked impairments in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction.
failure to develop peer relationships appropriate to developmental level.
a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. by a lack of showing, bringing, or pointing out objects of interest to other people).
lack of social or emotional reciprocity.
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus.
apparently inflexible adherence to specific, nonfunctional routines or rituals.
stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements).
persistent preoccupation with parts of objects.
C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning
D. There is no clinically significant general delay in language (e.g., single words used by age 2 years, communicative phrases used by age 3 years).
E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self- help skills, adaptive behavior (other than social interaction), and curiosity about the environment in childhood.
F. Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia.
Attention-Deficit/Hyperactivity Disorder (ADHD)
Inattention – gets off task easily
Hyperactivity – seems to move about constantly
Impulsivity – makes hasty actions that occur in the moment without first thinking about them
ADHD Risk Factors
Genetics
Cigarette smoking, alcohol use, or drug use during pregnancy
Exposure to environmental toxins during pregnancy
Exposure to environmental toxins, such as high levels of lead, at a young age
Somatic signs including sleep disturbances, enuresis or urinary frequency
*The onset of PANS may start with infectious agents other than strep. It also includes onset from environmental triggers or immune dysfunction
Pediatric Autoimmune Disorders Associated With Streptococcus
(PANDAS)
Presence of significant obsessions, compulsions and/or tics
Abrupt onset of symptoms or a relapsing-remitting course of symptom severity
Pre-pubertal onset
Association with streptococcal infection
Association with other neuropsychiatric symptoms (including any of the PANS �accompanying� symptoms)
PANS/PANDAS Tests
Swab/Strep culture
Blood tests for strep
Strep ASO
Anti-DNase B Titer
Streptozyme
Test for other infectious agents
MRI preferred but PET can be used if necessary
EEG
False Negatives
Not all children who have strep have elevated labs
Only 54% of children with strep showed a significant increase in ASO.
Only 45% showed an increase in anti�DNase B.
Only 63% showed an increase in either ASO and/or anti�DNase B.
Treatment Of PANS/PANDAS
Antibiotics
IVIG
Plasmaphoresis
Anti-Inflammatory protocols
Steroid medications
Omega-3’s
NSAIDS
Probiotics
Injury Medical Clinic: Chiropractor (Recommended)
Sources
�Attention Deficit Hyperactivity Disorder.� National Institute of Mental Health, U.S. Department of Health and Human Services, www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml.
Autism Navigator, www.autismnavigator.com/.
�Autism Spectrum Disorder (ASD).� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 29 May 2018, www.cdc.gov/ncbddd/autism/index.html.
�Introduction to Autism.� Interactive Autism Network, iancommunity.org/introduction-autism.
Shet, Anita, et al. �Immune Response to Group A Streptococcal C5a Peptidase in Children: Implications for Vaccine Development.� The Journal of Infectious Diseases, vol. 188, no. 6, 2003, pp. 809�817., doi:10.1086/377700.
�What Is PANDAS?� PANDAS Network, www.pandasnetwork.org/understanding-pandaspans/what-is-pandas/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine