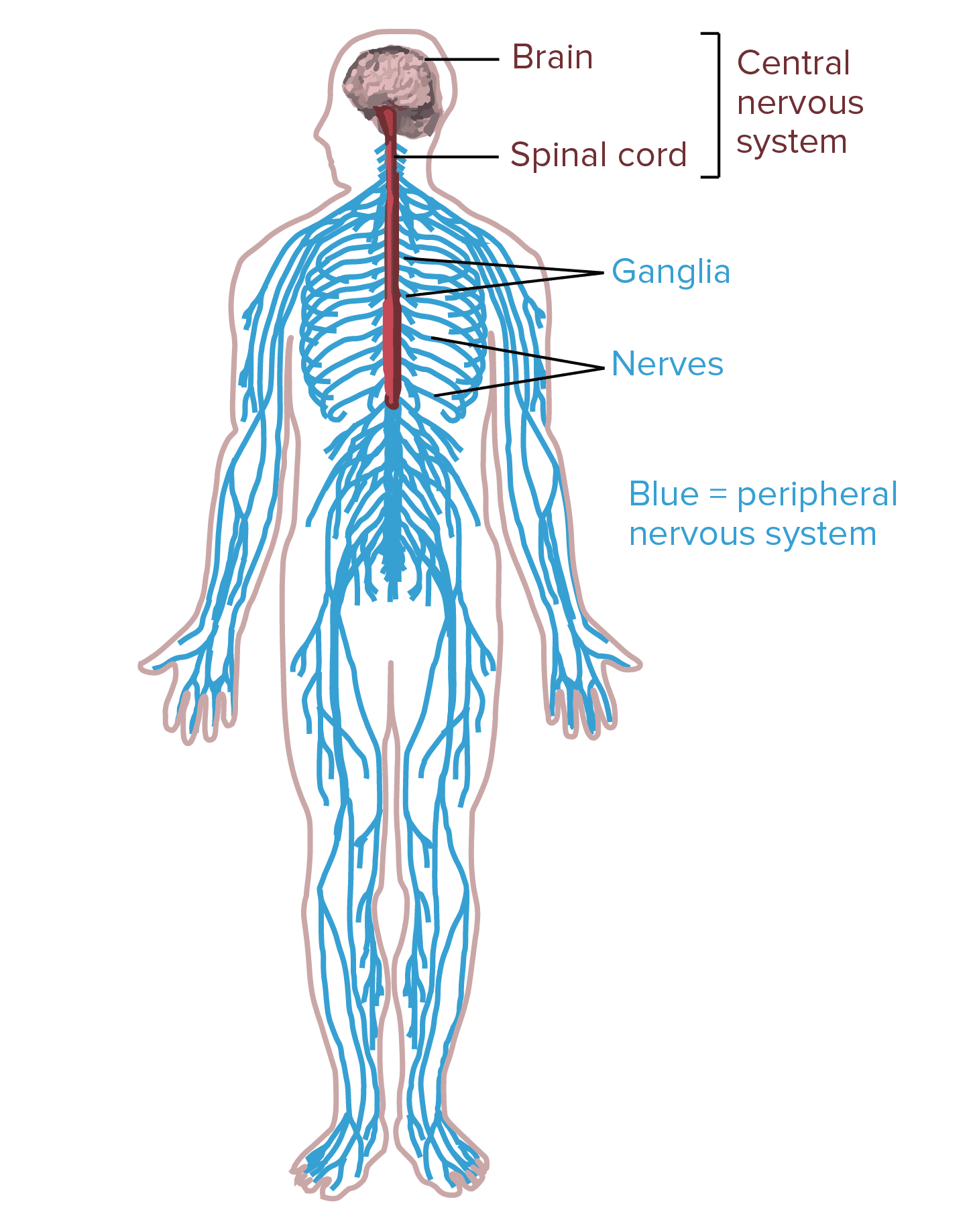
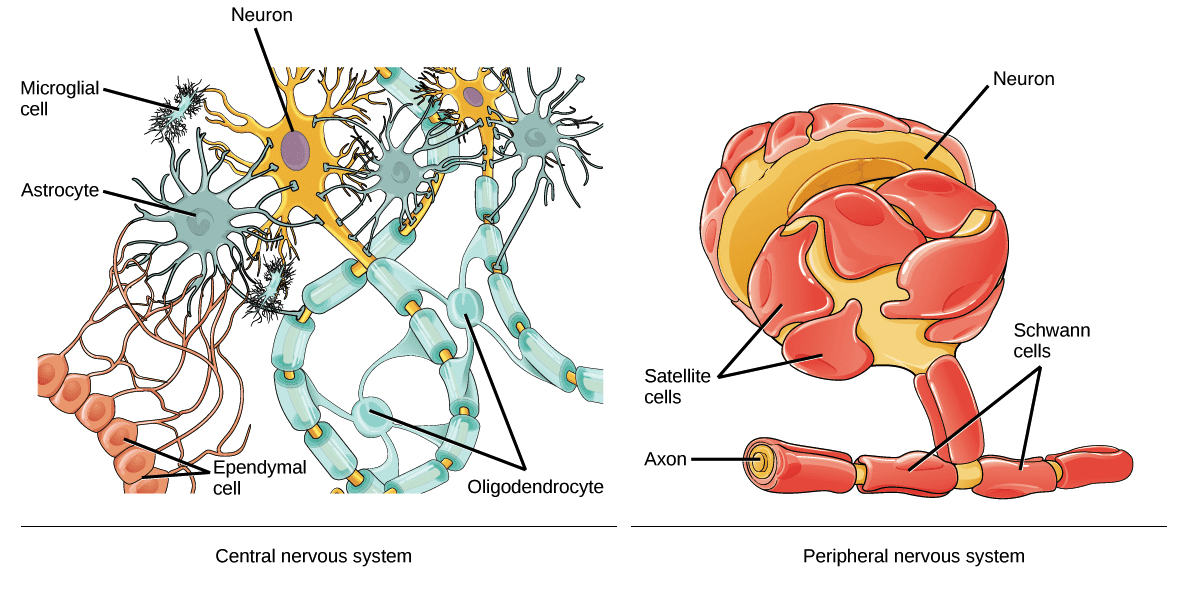
In humans, the nervous system consists of the central nervous system and the peripheral nervous system. The central nervous system, or CNS, consists of the brain and the spinal cord. It is in the CNS where the review of information occurs. The peripheral nervous system, or PNS, consists of the neurons and parts of neurons outside the CNS, including sensory neurons and motor neurons. Sensory neurons bring signals into the CNS, and motor neurons carry signals out of the CNS. �
The cell bodies of PNS neurons, such as the motor neurons which control skeletal muscles, are found in the CNS. These motor neurons have long extensions, known as axons, which run from the CNS all the way to the muscles with which they connect with or innervate. The cell bodies of additional PNS neurons, such as the sensory neurons which provide information on touch, pain, position, and temperature, are found outside the CNS, in which they are found in clusters known as ganglia. The axons of peripheral nerves which run through a common pathway are bundled together to form nerves. �
Types of Neurons
According to their roles, the neurons within the human nervous system can be separated into three different categories, including the sensory neurons, the motor neurons, and the interneurons. Below, we will describe the types of neurons. �
Sensory Neurons
The sensory neurons get information about what’s going on inside and outside the human body and they bring that information into the CNS where it could become processed. By way of instance, if you pick up a hot coal, the sensory neurons with nerve endings in your fingertips would communicate the information to your CNS that the hot coal is really hot. �
Motor Neurons
The motor neurons get information from other neurons and they communicate commands to your muscles, organs, and glands. In the previous circumstance where you picked up a hot coal, the motor neurons innervating the structures on your fingers would cause your hand to let go of the hot coal. This is only one example of the role of motor neurons. �
Interneurons
The interneurons, which can only be found in the CNS, connect one neuron to another. They get information from other neurons and communicate information to other neurons. When picking up a hot coal, the signals from the sensory neurons in your palms communicate to the interneurons on the spinal cord. Several of these interneurons communicate to the motor neurons controlling your finger muscles and cause your hand to let go of the hot coal. The motor neurons may communicate the signals to the interneurons in the spinal cord where it would ultimately create the perception of pain in the brain. �
Interneurons are the most numerous types of neurons and they are involved in processing information, both through basic neural circuits, such as those triggered by picking up a hot coal, as well as in much more complicated circuits in the brain. Different combinations of interneurons in the brain and spinal cord allow you to draw the conclusion that objects which look similar to a lump of hot coal shouldn’t be picked up and they will also help keep that information for future reference. �
Anatomy of a Neuron
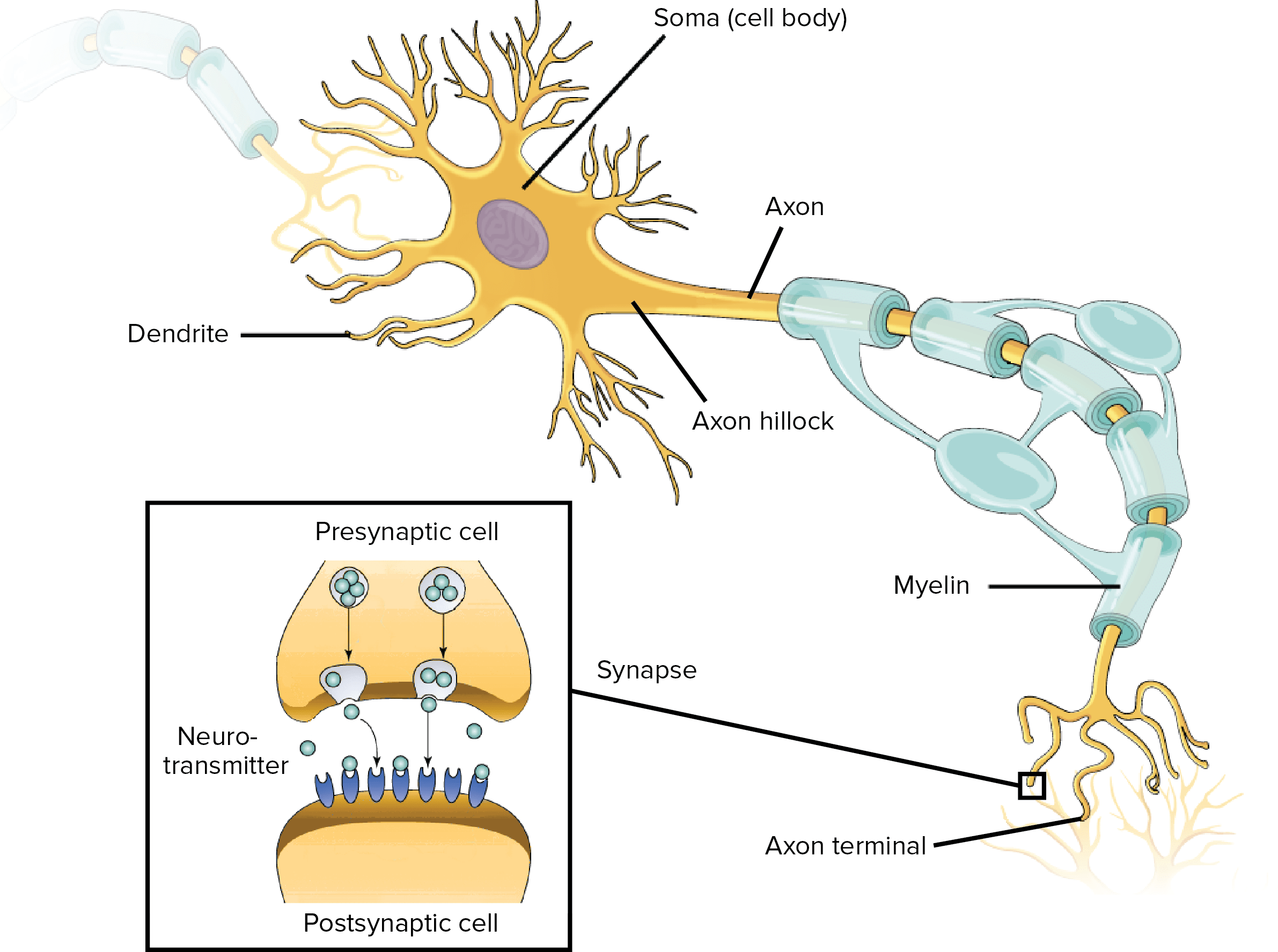
Neurons, similar to other cells, consist of a cell body known as the soma. The nucleus of the neuron is found in the soma. Neurons need to create proteins and most neuronal proteins are synthesized in the soma. Various processes, known as appendages or protrusions, run from the cell body. These include many small, branching processes, known as dendrites, and another process which is generally longer than the dendrites, known as the axon. It is possible to generalize that most neurons have three standard functions. These neuronal functions are mirrored in the anatomy of the neuron, including: �
Communicating information or signals.
Combining incoming signals to determine whether or not the information should be passed along.
Communicate information or signals to target cells, including muscles, glands, or other neurons.
Dendrites
The first two functions of the neuron, receive and process incoming signals or information, generally occur in the dendrites and cell body. Incoming signals can be either excitatory, which means that they tend to make the neuron generate an electrical impulse, or even inhibitory, which means that they tend to keep the neuron from generating an electrical impulse. �
Most neurons receive many incoming signals or information throughout the dendrites. A single neuron can have more than one pair of dendrites and they may receive thousands of incoming information or signals. Whether or not a neuron is excited into firing an electrical impulse is dependent on the amount of each of the excitatory and inhibitory signals, or information, it receives. If the neuron does end up firing an electrical impulse, the action potential or nerve impulse runs down the axon. �
Axons
The axon separates into many branches and develops bulbous swellings known as axon terminals or neural terminals. These axon terminals communicate with target cells. Axons are different from dendrites in several ways, as demonstrated below. �
The dendrites generally taper and are frequently covered with little bumps known as spines. The axon generally stays the same diameter for most of its length and doesn’t have spines.
The axon exits from the cell body through a special region known as the axon hillock.
Last but not least, many axons are covered with a special insulating compound known as the myelin, which helps them communicate the nerve impulse quickly. The myelin is never found on dendrites.
Synapses
Neuron-to-neuron communications are created on the dendrites and cell bodies of other neurons. These connections, known as synapses, are regions where information is taken from the first neuron, or the presynaptic neuron, to the target neuron, or the postsynaptic neuron. The synaptic connections between neurons and skeletal muscles are known as neuromuscular junctions and the connections between neurons and smooth muscle cells or glands are known as neuroeffector junctions. �
Signals communicate through chemical messengers known as neurotransmitters. When an action potential runs down an axon and reaches the axon terminal, it triggers the release of neurotransmitters from the presynaptic cell. Neurotransmitters run through the synapse and connect to membrane receptors on the postsynaptic cell, communicating excitatory or inhibitory information. The first two basic functions of the neuron are important for the third basic function of the neuron. �
The third function of the neuron, communicating signals to target cells, is also completed through the function of the axon and the axon terminals. Just as one neuron may communicate through many presynaptic neurons, it may also ultimately communicate through synaptic connections on numerous postsynaptic neurons throughout different axon terminals. �
Glial Cells
The glia, or glial cells, are fundamental to the nervous system. There are more glial cells in the brain than there are neurons. There are four types of glial cells in the adult human nervous system. Three of these, the astrocytes, the oligodendrocytes, and the microglia, are only found in the central nervous system or the CNS. The fourth, the Schwann cells, are only found in the peripheral nervous system or the PNS. Below, we will discuss the four types of glial cells, or glia, and their functions. �
Astrocytes are the most numerous types of glial cell. There are also many different types of astrocytes and they each have a variety of different functions, such as regulating blood flow in the brain, maintaining the composition of the fluid which surrounds the neurons, and maintaining communications between nerves in the synapse. During development, astrocytes help neurons find their way and add to the development of the blood-brain barrier, which also helps protect the brain. � Microglia are associated to the macrophages of the immune system and act as scavengers to remove dead cells and debris. �
The oligodendrocytes of the CNS and the Schwann cells of the PNS share a similar function. Both types of glia, or glial cells, create myelin, or the insulating compound which develops a sheath around the axons of many neurons. Myelin increases the speed with which an action potential runs down the axon and it plays a fundamental role in nervous system function. �
Additional types of glial cells, along with the four main types of glia, include satellite glial cells and ependymal cells. �
Satellite glial cells cover the cell bodies of neurons in PNS ganglia. Satellite glial cells are believed to support the role of the nerves and function as a protective barrier, however, their role is still misunderstood. Ependymal cells, which line the ventricles of the brain and the central canal of the spinal cord, have hairlike cilia which help improve the flow of the cerebrospinal fluid found within the ventricles and spinal tract. The human nervous system is necessary for our function. �
Neurons are special cells found within the nervous system which communicate with other neurons in unique ways. The neuron is the basic working unit of the brain and it is designed to communicate information, or signals, to muscles, organs, gland, and other nerve cells. Most neurons consist of a cell body, an axon, and dendrites. The cell body contains the nucleus and the cytoplasm. Understanding the structure and function of the neuron is fundamental for overall health and wellness. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to discuss the purpose of functional neurology in the treatment of neurological disease. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Leg Length Discrepancy (LLD) has profound effects on the body’s biomechanics, which can result in back pain and a number of other debilitating conditions.
Overview
Also known as Leg length inequality leg length discrepancy affects as many as 60 to 90% of the population.
It is categorized as functional or structural, but both have profound effects on the body’s biomechanics and result in back pain.
Other conditions include:
Arthritis of the knee
Psoasitis
Arthritis of the hip
Patellar tendinitis
Patellofemoral pain syndrome
Plantar fasciitis
Medial tibial stress syndrome
Iliotibial band syndrome
Lateral knee pain
Trochanteric bursitis
Sacroiliac discomfort
Achilles tendinitis
Cuboid syndrome
Functional Short Leg: Alignment�difference of the supporting structures between the ground and the top of the femur or thigh bone.
This is caused by excessive pronation or the natural rolling in of the foot as someone walks.
Anatomical Short Leg: A difference in the size or length of the thigh bone (femur).
This is most often caused by growth asymmetry that can be inherited/genetic condition�but can sometimes come from a fracture or surgery.
Our body can work with leg inequality for short a period but over time, biomechanical problems throughout the body can begin to happen.
Our body’s ability to adapt to abnormal stress eventually takes its toll and the surrounding soft tissues can’t take it anymore.
Even the simplest movements begin to require much more muscular effort and energy, which reduces endurance.
Excessive stress gets transmitted to the ligaments, which then creates:
The first goal of treatment is to improve alignment and restore symmetry.
This can be accomplished with:
Spinal adjustments focus on providing better spinal column alignment
Exercises to help the affected muscles
Proper orthotics with a pronation wedge under the heel for long-term correction
Sometimes LLI causes a profound gait (walk) disfunction, which means physical therapy might be necessary.
Prevention
Keep your bones and tissues strong and healthy with exercise and diet can help.
Avoid tobacco and excessive alcohol use, which weaken bones and can cause problems with the blood supply in the legs.
Reduce your risk of injury by adhering to safety measures (like wearing a seatbelt).
Custom orthotics provide support, stability, and shock absorption.
Recovery
The body�s foundation can be made level with custom orthotics, but it does take some time to adjust to proper and healthier alignment/posture.
Talk to your doctor or chiropractor to learn more.
Symptoms:
Back pain
Leg pain
Pelvic obliquity
Scoliotic deviations of the lumbar spine
Increased risk of injury, especially in athletes
Chiropractic care does wonders for helping individuals regain their spinal alignment and loosen the joints and muscles affected by leg length inequality, and the orthotic heel lifts balance out the legs, which balances the hips and pelvis.
Reduce *PLANTAR FASCIITIS PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Foot problems can affect the overall well-being of the human body. Many health issues which affect the foot can result in poor posture, low back pain, and sciatica. These imbalances can ultimately result in a variety of other health issues. Custom-made foot orthotics can help promote and support overall well-being by relieving foot problems. The following video discusses how many health issues which affect the foot can cause a variety of foot problems, including poor posture, low back pain, and sciatica. Dr. Alex Jimenez is the non-surgical choice for foot problems and other health issues. Dr. Alex Jimenez can help promote and support overall well-being with the use of custom-made foot orthotics and other treatments approaches.
What’s Afoot
According to the�American Chiropractic Association, a study found 75% of subjects who suffered from lower back pain had legs that were slightly different lengths (5 millimeters or more). This condition is called�Short Leg Syndrome�and causes a variety of issues for its sufferers. The symptoms can be quite severe, depending on the degree of difference in the leg length.
NCBI Resources
The premise of this condition is that the leg length inequality disrupts the�body�s entire balance, possibly resulting in issues in the knees, hips, and back. The spinal system is designed to bear weight evenly, and, when one leg is shorter than the other, this places additional weight and stress on one side. According to�The Back Pain Authority, common causes of Short Leg Syndrome are a past history of fractures, hip or knee issues, or the individual was simply born that way.
Functional neurology primarily focuses on the fundamentals of neuron health and it is mainly based on neuroplasticity theories. It’s believed that the brain and the nervous system are capable of changing, and can become malleable, due to a reaction to certain stimulation. The brain can be shaped by sensory, motor, cognitive, or emotional experiences. �
The creation of synapses in the nervous system depends on the stimulation they receive. Neurons which receive too much stimulation are the ones which become stronger and those which don’t receive stimulation become weaker and eventually diminish. It is believed that it is possible to create new neurons even after there has been damage to the nervous system. �
The Role of Functional Neurology
Functional neurology evaluates changes in the nervous system before these become severe health issues. The practice of functional neurology has been adopted by several modalities of practice, such as chiropractic, psychology, occupational therapy and even by conventional healthcare professionals. Functional neurology is commonly practiced by chiropractors. �
The practice of neurology involves applying neuroscience research from laboratory studies to determine how it can be practically applied in health care. The brain is protected by supporting the nervous system. The ultimate goal of functional neurology is to treat brain and nervous system health issues without the utilization of drugs or together with conventional treatment approaches. Functional neurologists can help treat a wide variety of neurological health issues, including: �
Neurodegenerative disorders: Alzheimer�s disease, Parkinson�s disease, dementia, and multiple system atrophy.
Demyelinating conditions: Multiple sclerosis, transverse myelitis, and leukodystrophies.
Trauma and brain injuries: Concussions and whiplash-associated disorders.
Vestibular conditions: Motion sickness, dizziness/disequilibrium, labyrinthitis, vertigo, and Meniere’s disease.
Movement disorders: Tics, restless leg syndrome, myoclonus, and dystonia.
Neuro-developmental conditions: Autism spectrum disorders, ADHD, Asperger’s syndrome, Tourette syndrome, dyslexia, processing disorders, and global developmental delay.
Headaches and pain syndromes: Cluster headaches, complex regional pain syndrome, migraines, and fibromyalgia
Functional neurological disorders which are best referred to as a group of physical, sensory and cognitive symptoms which do not seem to have an identifiable organic etiology.
Functional Neurology Treatment
The primary goal of functional neurology is to promote, support, and restore the optimal function of the brain and the nervous system, as opposed to the absence of pathology. Sometimes it’s not always possible to determine the natural source of a person’s neurological disease and its symptoms. Functional neurology can be particularly beneficial in these instances. �
The patient’s medical history and a non-invasive evaluation are required for diagnosis. Treatment is determined based on the patient’s current and targeted well-being. Any blood tests, x-rays, MRIs and/or other tests are also evaluated. During the evaluation, the healthcare professional will observe all aspects of the patient, including eye movements and posture, which can demonstrate the function of the brain and the nervous system. Blood pressure, pulse, and reflexes are also evaluated. �
Neuro-developmental conditions and behavioral disorders are generally treated with functional neurology. Anxiety is commonly increased in patients with these type of health issues, therefore, it is recommended that the non-invasive evaluation is performed in a way which does not trigger anxiety in the patient. Functional neurology treatment is individualized and every part of the treatment approach is customized to the individual’s treatment requirements. �
Functional neurology emphasizes on encouraging patients to practice self-care so that face-to-face treatment with a healthcare professional does not continue for months or years without end. Home exercise programs are developed to treat the associated health issues, meaning that functional neurology treatment is incorporated into the patient’s daily activities. �
Biochemistry and Nutrition in Functional Neurology
Functional neurology treatment focuses on retraining the brain. Neurons need energy and stimulation to survive and thrive, therefore, functional neurology treatment may involve exercises, such as eye exercises, cognitive activities, balancing activities, and joint adjustments. Different stimulation can affect different regions and pathways in the human brain. �
Moreover, functional neurology treatment may also involve a nutritional and biochemical approach by eliminating several factors which may potentially affect neurons. These can ultimately include toxins, chemicals, and infection, among other factors. Dietary modifications and supplementation may also be included to provide optimal energy for neurons. �
An individualized treatment approach is applied to each individual otherwise there exists the risk of over-stimulating and exceeding the capacity of a patient’s nervous system. The goal of functional neurology treatment is to improve brain and nervous system health, neural processing, communication, and all signaling involving the brain and the entire human body. �
Functional neurology focuses on the diagnosis and treatment of the human brain and the nervous system utilizing sensory and cognitive based treatment methods and techniques to promote, support, and restore neuroplasticity, integrity, and functional optimization. Functional neurology can be utilized to help improve a variety of neurological diseases and health issues, including Alzheimer’s disease. Functional neurology is frequently practiced by chiropractors. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to discuss the purpose of functional neurology in the treatment of neurological disease. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Over-the-counter or (OTC) orthotic insoles are foot supports that can be made from various materials which include:
Foam
Leather
Plastic
OTC insoles are designed to fit inside your shoe.
These have become popularized through T.V. commercials, fancy packaging and can be bought at pretty much any grocery/pharmacy store.
OTC’s can be marketed to:
Provide comfort�
Bring pain relief from common conditions:
Bunions
Plantar fasciitis
Arch support problems
OTC insoles are also available to fit in a variety of shoes:
High heels
Athletic shoes
Boots
That work with every individual’s lifestyle.
OTC insoles are dangerous and can cause more harm than help.
Many people do not realize their feet could be the cause of:
Knee
Hip
Back pain
This is why Chiropractors treat issues, such as plantar fasciitis by performing lower back adjustments and look to the feet when diagnosing and treating patients.
Patients must be cautioned against self-diagnosing and using OTC orthotics.
Custom made orthotic insoles are a great solution.
Here are the three bad things that OTC insoles can do to your body.
1. OTC Insoles Do Not Provide Support
Every person�s body is unique.
We are all different:
Heights
Weights
Have different body compositions
This also means that our feet are unique, with some of us even having two feet that completely different from one another. Because of our unique body composition, there is really no one-size-fits-all cure. When it comes to the feet, customization is the key. Ineffective support can lead to increased pain and discomfort.
The way to avoid ineffective support is to seek professional advice first.
You see the scanners inside the stores to help you find which insole is right for you, however, these are designed to sell, sell, sell.
Getting a foot scan by a medical professional that can assess your body and feet in person is the way to go.
They will talk with you, personally about treatment options and will help you find the best solution.
2. Make Physical Discomfort Worse & Cost You More Money because now you need Treatment
OTC insoles are typically made of inexpensive materials.
OTC insoles wear down faster and require constant replacement.
You could purchase the wrong type of OTC insole, which can create more pain and discomfort.� When experiencing pain or discomfort, our bodies are under stress. Stress also increases from financial burdens or seeking medical treatment which can be time-consuming and uncertain.
Self-diagnosing your issues while standing in a store can be dangerous, instead relieve your stress by seeking expert help.
Custom orthotics are also covered by some insurance providers.
3. The function of Your Foot/Ankle Worsens
Body function goes down when insoles are not properly prescribed or fitted.
The wrong insole can make a well-fitting shoe too tight for example.
Wrong insoles can redistribute body weight the wrong way to think that the foot pain is alleviated but then the ankles get sore or we can’t bend our feet.
Bad insoles can also make it difficult to run or walk.
Wearing the wrong insole can create new injuries.
Orthotics alter the way our bodies move and affect how we walk, stand, and absorb shock.
Selecting the right orthotic is essential to how our body functions every day.
Custom orthotics are designed specifically for an individual�s body:
Stabilize joints
Reduce pain
Prevent deformity
Create proper posture�
Improve foot function
Remember that it’s not possible to purchase� OTC insoles designed specifically for an individual.
But you can get custom fit orthotics to:
Relieve discomfort
Help your body operate properly
Save you stress and money
Proven Reduced Back Pain with *FOOT ORTHOTICS* | El Paso, Tx
Kent S. Greenawalt, President, and CEO of Foot Levelers discuss how custom foot orthotics can help reduce back pain, low back pain, and sciatica. In a recent research study published by the American Congress of Rehabilitation Medicine (ACRM), researchers demonstrated that Foot Levelers custom foot orthotics help considerably reduce back pain and several of its associated health issues. The research study also demonstrated that Foot Levelers custom foot orthotics and chiropractic care help tremendously reduce low back pain and sciatica. Foot Levelers custom foot orthotics and chiropractic care helped improve the patient’s overall health and wellness. Dr. Alex Jimenez is a chiropractor in El Paso, TX who can help provide these benefits through the utilization of chiropractic care and Foot Levelers custom foot orthotics, among other treatments.
What’s Afoot
If you have low back pain�or have had it, you are not alone. Experts estimate that around�80% of people�will experience some type of back problem at some point in their lives.�The Global Burden of Disease 2010�lists low back pain as the number one cause of disability worldwide. The good news is the majority of back pain is mechanical in origin or is not organic. This means that infection, cancer, fracture, inflammatory arthritis, and other serious conditions are not the cause. In fact, you may benefit by looking to your feet, knees,�and hips as the culprits.
NCBI Resources
Experienced chiropractors understand there are some other treatments in addition to chiropractic care that help aid pain management, increase mobility, and decrease healing time. Depending on the condition, individuals may experience a wide array of benefits from blending these treatments into their chiropractic treatment. One such treatment is orthotics or inserts. If life were a sandbox, chiropractic care and orthotics would be the best of friends. They treat muscle and skeletal conditions, as does chiropractic treatment.
Chiropractic along with Other? Natural Treatments Can Help Reduce the Opioid Epidemic
As of now, there are over 2 million Americans dependent on opioids. For most of these individuals, the addiction comes from seeking pain management for an injury or chronic condition. The opioid crisis has become a national emergency causing overdose remedies to be sold over-the-counter.
Seeking chiropractic care can provide patients with relief, and aid in reducing any negative effects of the opioid epidemic.
The most commonly abused opioids are:
Fentanyl
Oxycodone
Tramadol
Opioids are often given to people battling cancer but are also prescribed following surgery and for people with chronic pain.
Taking opioids over a long period of time is the most dangerous because the effects can trick your brain to thinking the drugs are necessary to live.
Opioids are a convenient and fast remedy for pain, but only provide pain relief, and do not treat the actual issues.
That is why opioids should be a last resort.
A chiropractor can assess your body from head to toe and provide pain relief through:
Adjustments
Massage
Acupuncture
Electromagnetic therapy
Chiropractic is a drug-free approach to pain relief and pain management.
The American College of Physicians (ACP) recommends the use of non-invasive, drug-free treatments such as Chiropractic care, first for chronic and acute lower back pain.
Lower back pain is one of the primary causes of opioid dependency.
Lower back pain can be difficult to treat, due to identifying and the cause.
Many doctors prescribe pain killers to provide comfort, while the actual problem goes untreated.
Chiropractors can identify the root cause of the pain.
Lower back pain can be caused by issues with the feet, ankles, knees, or hips.
Chronic back pain is due to some form of musculoskeletal weakness or imbalance.
An imbalance in one or both of the feet can cause problems throughout the entire body, especially placing stress on the lower back. Chiropractors are trained to examine the feet when a patient complains of back pain. Once the cause is identified, they can treat an individual without any prescription drugs.
Treatments for chronic pain typically include:
Chiropractic adjustments
Custom orthotics to help maintain the effectiveness of the adjustments
You can be examined for custom orthotics in less than five minutes and have them sent directly to you or pick them up.
Custom orthotics help us stand for extended periods, and with walking/working out.
Custom orthotics help you function without pain, and prescription-free.
�Treat pain without the use of surgery and addictive drugs.
Control *FOOT MOTION & POSTURE* with Functional Foot Orthotics | El Paso, Tx (2019)
If you have low back pain�or have had it, you are not alone. Experts estimate that around�80% of people�will experience some type of back problem at some point in their lives.�The Global Burden of Disease 2010 lists low back pain as the number one cause of disability worldwide. The good news is the majority of back pain is mechanical in origin or is not organic. This means that infection, cancer, fracture, inflammatory arthritis, and other serious conditions are not the cause. In fact, you may benefit by looking to your feet, knees,�and hips as the culprits.
What’s Afoot
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot�line up which extends through the tibia, or shin bone.
NCBI Resources
The most commonly prescribed opioids are hydrocodone products. They are used to treat pain from injuries, dental work, and typically moderate pain. Milder pain is often treated with codeine but it is also used to treat coughing as well as severe diarrhea. Overall, opioids are used to treat everything from cancer pain to post-op pain to osteoarthritis.
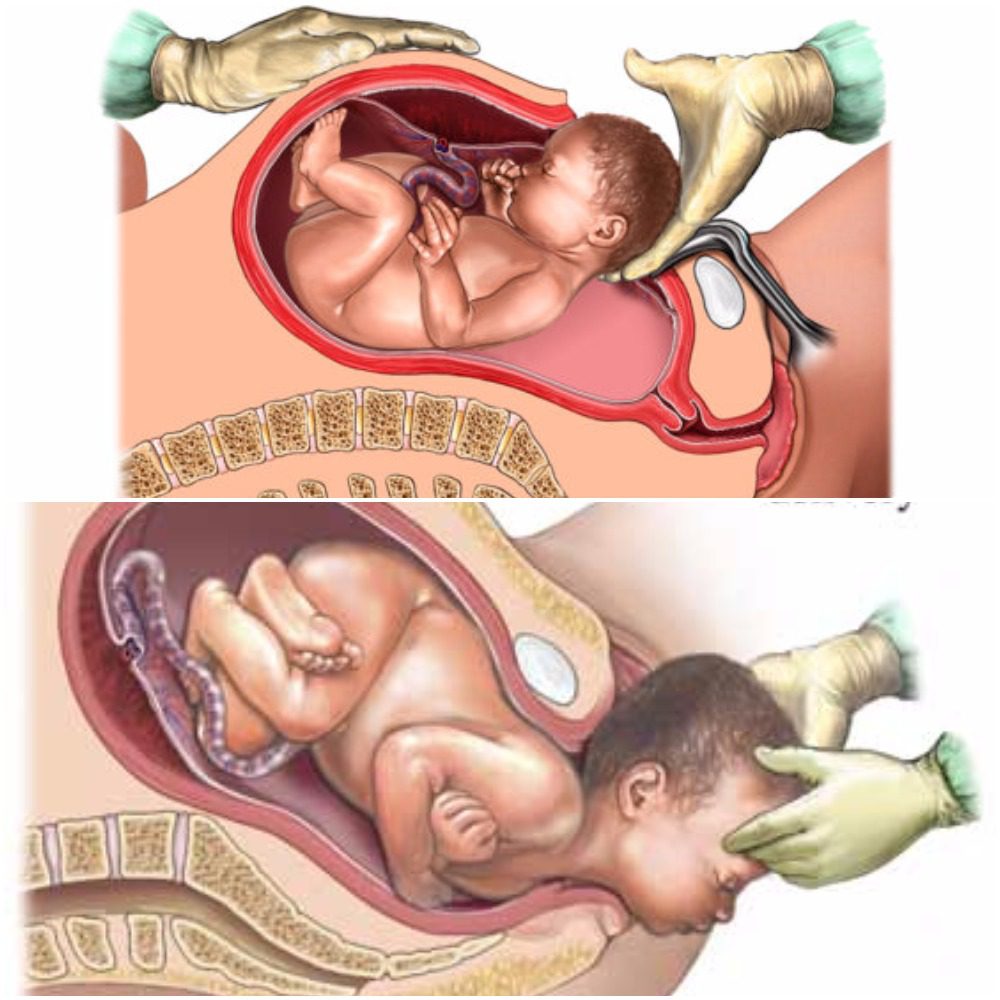
As humans, we depend on microbiomes to stay alive. Microbiomes are essential in fighting off germs and maintaining health. The development of microbiomes begins in utero where the microbes have been isolated to the placenta, fetal membranes, amniotic fluid, and umbilical cord blood, but are mainly transferred from mother to child during birth in a process referred to as “seeding” (1,2). “Seeding”� occurs as the child passes through the mothers vaginal canal and becomes coated in her microbiome. In addition to this, small amounts of microbiomes get transferred to the child as the mother breastfeeds. This early introduction from mother to infant serves as an inoculation process with long term health outcomes for the newborn (2). With the number of cesarean births being higher this decade than in the past, you may find yourself asking, “How does a cesarean birth affect my child’s microbiomes?”
Vaginal
With vaginal births still being the most common way of delivery (68%), these children are seen to have overall better health throughout their lifetime than those born via cesarian (2). Vaginal birth is the most effective way to spread the microbiomes to the child’s skin, but studies have found that microbiomes do differ between ethnic groups. Microbiomes are made up of multiple bacterias and specifically, women with a higher pH have a smaller community of protective biomes. It has also been seen that the gut microbiota in pregnant women with gestational diabetes, tend to have an increased abundance of disease-associated microbes (2). That being said, the pH and mothers gut microbes play a significant role in the types of microbiomes that get transferred to their child.
Cesarean
There are generally two ways a child ends up being born via cesarean, labor ending in a cesarean, or a planned cesarean with no labor attempted. Children who are born via cesarean with labor attempted first, have a slightly higher number of microbiomes due to the vaginal fluids exposed to them during labor than that born elective cesarean. The most effective way a mother can transfer microbiomes to their newborn via cesarean is to “incubate” a cloth for 1 hour in their vaginal canal. When the infant is born,� the doctors rub the child’s mouth, eyes, and skin with the cloth that was previously incubated within minutes after birth (2). This process ensures that the child will have microbiomes more closely related to those born vaginally. Children born elective cesarean without using the incubation method, show fewer gut microbiomes related to their mother, but rather have more skin and oral microbes, and bacteria due to the operating room (2).
Children who are born via cesarean, whether labor was attempted first or not, are more likely to develop immune-related disorders such as asthma, allergies,� inflammatory bowel disease, and obesity (2). This is directly linked to not being “seeded” by the mother. Furthermore, adults who were born via cesarean contain a fecal microbiota that is drastically different than adults who were born vaginally (2).
The purpose of the female reproductive system is to reproduce and birth. Therefore, the best route will always be vaginal if it is safe for baby and mom. This being said, a cesarean is not a bad way to bring a child into the world. The child will just face more skin irritability and have a greater risk of developing health issues due to not receiving the same microbiomes as a child born vaginally. – Kenna Vaughn, Health Coach Insight
References:
(1) Aagaard, Kjersti, et al. �The Placenta Harbors a Unique Microbiome.� Science Translational Medicine, U.S. National Library of Medicine, 21 May 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4929217.
(2) Dunn, Alexis B, et al. �The Maternal Infant Microbiome: Considerations for Labor and Birth.� MCN. The American Journal of Maternal Child Nursing, U.S. National Library of Medicine, 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5648605/.
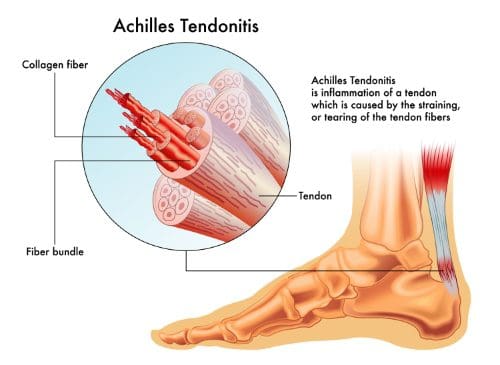
If you are suffering from Achilles tendonitis, you are definitely not alone. Plantar fasciitis and Achilles tendonitis are the two most common causes of pain in the heel. Athletes and active individuals, in particular, find themselves developing pain in the heel from Achilles tendonitis, but it is possible to develop the condition even if you are not an athlete.
Fortunately, chiropractic and associated therapies can do a lot to relieve your heel pain. With a combination of chiropractic care and Active Release therapy, you can get back on your feet and back to doing what you love as soon as possible.
Heel Pain Connected to the Achilles Tendon
Most people know how to point out the Achilles tendon. It is the large, thick tendon that travels up from the base of the heel and into the calf muscle. In fact, it connects the calf muscle and heel. It allows your body to transfer power from the calf muscle to the feet so that you can walk, run and jump. The Achilles tendon is strong and durable, but it is possible to overwork it and cause enough repetitive strain to develop tendonitis in the tendon.
Pain Causes in the Achilles Tendon
There are several stages to the process of developing pain in the Achilles tendon. These include:
Micro-tears
Heavy use of the tendon can lead to small tears. The micro-tears that develop in the Achilles tendon are known as tendinosis. They may not be noticeable at first and you may not feel much pain or any pain at all. However, over time and with increased tearing, the condition can become chronic.
Tendonitis
When you start to feel pain in your Achilles tendon that keeps occurring or lasts for a few days, you are likely experiencing tendonitis. The pain and inflammation of tendonitis need to be treated to avoid developing a chronic condition.
Tendinosis
If the pain becomes chronic�meaning it never or rarely goes away�then you have developed tendinosis. Instead of being inflamed, tendinosis is characterized by a lack of inflammation and the development of scar tissue. The scar tissue makes the tendon stiff and is usually quite painful. The stiffness of the tendon makes it more prone to tearing.
Rupture
If the tendinosis is not treated properly the tendon can eventually tear. A torn tendon is referred to as a rupture and usually requires surgery.
Symptoms
Pain and stiffness around the lower leg, right above the back of the heel
Begins as a mild ache and worsens throughout the day
Jumping,� running, stair climbing, and sprinting can spark intense pain
Tenderness or stiffness especially in the morning, but improves with movement/activity
Achilles Tendonitis Treatment
When you start to feel constant pain in your Achilles tendon it is time to go see your chiropractor. It is important to start treatment as soon as possible to avoid developing more advanced issues like tendinosis or even a ruptured tendon.
Your chiropractor will recommend several different types of treatment, including:
Active Release Therapy (ART)
ART is extremely effective for breaking up scar tissue and improving issues with soft tissues. Treatment can do a lot to improve the health of your tendon and the surrounding tissues to avoid further complications. It will also do a lot to help relieve the pain you are experiencing.
Chiropractic
Many times, the issues with your Achilles tendon are the result of misalignment in other parts of your body. When your joints are misaligned it tends to put extra stress on your feet and Achilles tendons. To minimize the stress on your joints, your chiropractor will adjust your spine and other joints to ensure proper alignment.
Get Help for Your Achilles Tendonitis
If you are experiencing heel pain, please get in touch with our chiropractic team. We can help to alleviate your pain and help you avoid experiencing further problems with your Achilles tendon.
Reduce *PLANTAR FASCIITIS PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Foot pronation is the natural movement which occurs during foot landing while walking or running. Foot pronation also occurs while standing, and in this instance, it is the amount in which the foot rolls inward toward the arch. Foot pronation is normal, however, excessive foot pronation can cause a variety of health issues, including bad posture. The following video describes the 5 red flags of excessive foot pronation, which can ultimately affect a person’s overall health and wellness. Dr. Alex Jimenez can help diagnose and treat excessive foot pronation. Patients recommend Dr. Alex Jimenez and his staff as the non-surgical choice for excessive foot pronation health issues.
Orthotics
If you are considering custom orthotics, a health care professional such as Doctor Jimenez and Injury Medical Chiropractic Clinic can perform a foot scan to show you what imbalances in the feet can lead to. The foot scan will show how the orthotics can help. Following the foot scan, a report will provide the caregiver a�Pronation/Stability Index, Foot Assessment, and Body Assessment.
What’s Afoot
Foot pain can commonly occur from various injuries. In the United States alone, about 2 million acute ankle sprains occur every year, one of the most prevalent causes of ankle pain. Chiropractic care is a popular alternative treatment option which can help treat a variety of health issues, including foot and ankle pain.
NCBI Resources
Tendonitis often recurs in many people. This is due, at least in part to improper or incomplete healing. Many people will resume normal activities as soon as the pain subsides when they should continue caring for the injury so that it can heal completely. This leads to inflammation of the area again as the original injury is aggravated, but it can also lead to re-injury in that same area. Chiropractic care can help tendonitis heal completely and help prevent re-injury to the area.
Glutamate is the main excitatory neurotransmitter in the central nervous system, or CNS, of mammals and it primarily interacts with both metabotropic and ionotropic receptors to activate and regulate postsynaptic responses. Both AMPA and NMDA receptors are fundamental mediators of synaptic plasticity, the ability of synapses to strengthen or weaken, where dysregulation of those receptors leads to neurodegeneration in a variety of disorders, including Alzheimer’s disease. �
The main difference between AMPA and NMDA receptors is that sodium and potassium increases in AMPA receptors where calcium increases along with sodium and potassium influx in NMDA receptors. Moreover, AMPA receptors do not have a magnesium ion block while NMDA receptors do have a calcium ion block. AMPA and NMDA are two types of ionotropic, glutamate receptors. They are non-selective, ligand-gated ion channels, which mainly enable the passage of sodium and potassium ions. Furthermore, glutamate is a neurotransmitter which creates excitatory postsynaptic signals in the CNS. �
�
What are AMPA Receptors?
AMPA, also known as ?-amino-3-hydroxy-5-methyl-4-isoxazole-propionate, receptors are glutamate receptors which are in charge of maintaining the rapid, synaptic transmission in the central nervous system. AMPA receptors have four subunits, GluA1-4. Moreover, the GluA2 subunit is not permeable to calcium ions because it contains arginine from the TMII region. �
Furthermore, AMPA receptors are involved in the transmission of the majority of the rapid, excitatory synaptic signals. The increase of the post-synaptic response depends on the amount of receptors in the post-synaptic surface. The type of agonist which activates the AMPA receptors is ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid. The activation of the AMPA receptors leads to the non-selective transportation of cations, such as sodium and potassium ions, into the cell. This generates an action potential in the postsynaptic membrane. Figure 1 below demonstrates a diagram of AMPA receptors. �
What are NMDA Receptors?
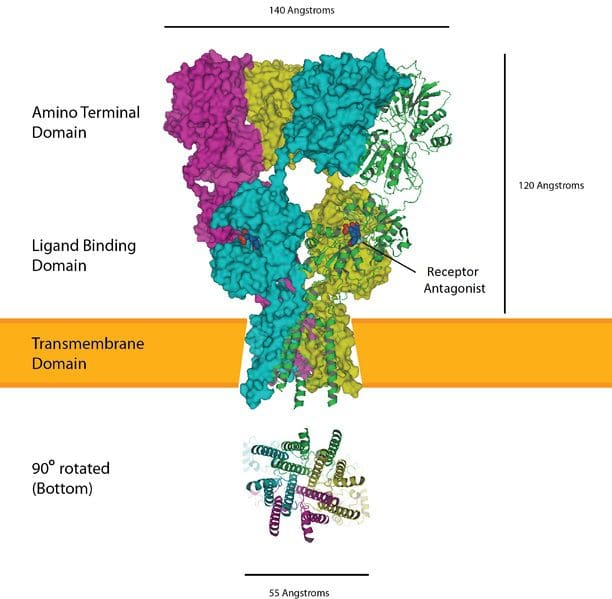
NMDA, also known as N-methyl-d-aspartate, receptors are glutamate receptors which are found in the postsynaptic membrane. The NMDA receptors are made up of two varieties of subunits: GluN1 and GluN2. The GluN1 subunit is fundamental for the role of the receptor. This subunit can associate with one of the four types of GluN2 subunits, GluN2A-D. �
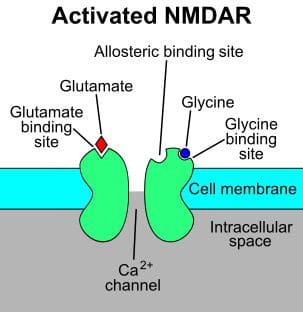
Furthermore, the main utilization of the NMDA receptors is to maintain the synaptic response. In the resting membrane potential, these receptors are inactive due to the creation of a magnesium block. The agonist of the NMDA receptor is N-methyl-d-aspartic acid. L-glutamate, including glycine, can connect to the receptor to activate it. Upon stimulation, NMDA receptors activate the calcium influx along with the potassium and sodium influx. Figure 2 demonstrates NMDA receptors. �
Similarities Between AMPA and NMDA Receptors
AMPA, NMDA, and kainate receptors are the three main types of glutamate receptors.
These are ligand-gated ion channels which activate and regulate sodium and potassium ions.
These are known due to the type of agonist which activates the receptor.
Moreover, the activation of these receptors produces excitatory postsynaptic responses or ESPSs.
Furthermore, several protein subunits connect together to form these receptors.
Difference Between AMPA and NMDA Receptors
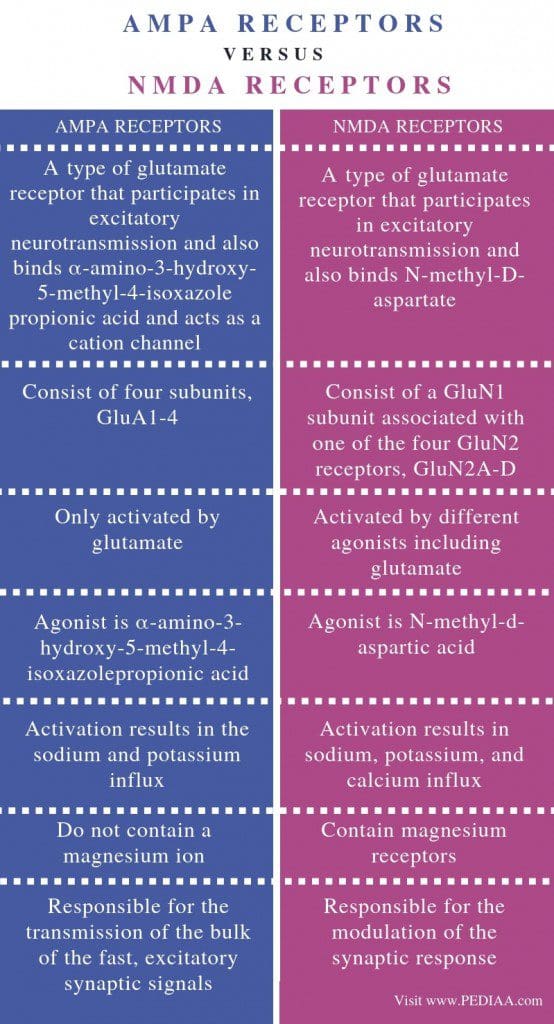
AMPA receptors are best known as a type of glutamate receptor which activates in excitatory neurotransmission and connects ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid which additionally works as a cation channel. Where the NMDA receptors are best known as a type of glutamate receptor which helps in excitatory neurotransmission and also connects N-methyl-D-aspartate. This is the most fundamental difference between AMPA and NMDA receptors. �
AMPA receptors have four subunits, GluA1-4 while NMDA receptors have a GluN1 subunit associated with one of the four GluN2 receptors, GluN2A-D. Activation can also be a difference between AMPA and NMDA receptors. AMPA receptors are only activated by glutamate while NMDA receptors are activated by different agonists. The agonist for AMPA receptors is ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid where the agonist for NMDA receptors is N-methyl-d-aspartic acid. �
Ion influx is a fundamental difference between AMPA and NMDA receptors. Activation of AMPA receptors results in the sodium and potassium influx while the activation of NMDA receptors leads to an increase in potassium, sodium, and calcium. Another distinction between AMPA and NMDA receptors is that AMPA receptors do not contain a calcium ion where NMDA receptors contain magnesium receptors. Also, AMPA receptors are responsible for the transmission of the majority of the rapid, excitatory synaptic signals while NMDA receptors are responsible for the modulation of the synaptic response. �
AMPA receptors are glutamate receptors which lead to the influx of sodium and potassium ions. NMDA receptors are another type of glutamate receptors which result in the influx of calcium ions with potassium and sodium ions. The main difference between AMPA and NMDA receptors is the type of ion influx associated with their activation and regulation. �
Several varieties of ionotropic glutamate receptors have been demonstrated in the following article. Three of these main excitatory neurotransmitter in the central nervous system, or CNS, are ligand-gated ion channels best known as AMPA receptors, NMDA receptors, and kainate receptors. These ionotropic glutamate receptors are best referred to after the agonists which activate and regulate them: AMPA or ?-amino-3-hydroxy-5-methyl-4-isoxazole-propionate, NMDA or N-methyl-d-aspartate, and kainic acid. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to demonstrate the difference between AMPA and NMDA receptors for brain health. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
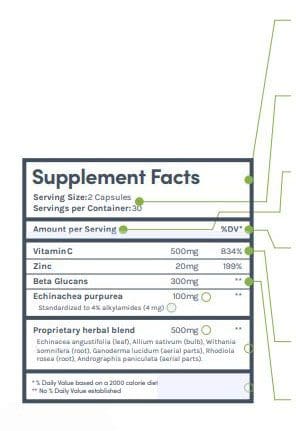
Supplemental Facts title indicates that the product is marketed for sale in the USA and is FDA standard.
Serving size, and the number of servings per container will be included to help you compare between products.
Make sure the serving sizes match when comparing supplements to get an accurate comparison.
Vitaminsand minerals always show the dose in weight and % percentage daily value to help you understand your dietary requirements.
Supplements often will have doses that exceed the recommended daily value.
Dietary supplement ingredients that are not vitamins or minerals will not have the % percentage daily value because they are not essential ingredients in the diet.
Dietary supplements are regulated by the FDA, and all labels must follow a consistent format to make it easier for consumers to understand. Understanding dietary supplement labels well require some attention to the following points when you�re evaluating supplements.
Herbs sometimes have additional information listed in the supplement panel. You might see ratio numbers (example 4:1) that show how much raw material of the herb (fresh or dried herb) is in the supplement version.
Herbs might have a standardization amount that shows how much of an active ingredient is present. The dose of the active ingredient is often listed, but sometimes it is not.
Proprietary blends are common. Only the total amount of the blend in a serving needs to be listed, which means that you don�t get all of the information about every ingredient.
Proprietary blend ingredients are listed in order from most to least. Similar to how food ingredients are listed on prepared foods nutrition facts panels.�
The daily value percent is established against a 2000 calorie diet. This is the standard calorie amount, however, it�s always important to determine your calorie requirements that you need for your health goals.
How To Identify Organic Foods
In the United States, a food or product that is labeled as organic is required to be certified by the�U.S. Department of Agriculture (USDA). The USDA has a certification program for natural growers and it has a set of very stringent standards that the product or food must meet.
There are some exemptions. For instance, a producer who does not sell more than $5,000 annually just in organic foods is not required to get the certification although they do have to adhere to the USDA�s stringent requirements for organic foods.
When a food carries the USDA Organic label, it means that it meets the requirements. While natural producers are not required to put the label on their products, many do.
The labeling varies, depending on the type of food. Single-ingredient foods like eggs, vegetables, and fruits�are considered to be 100 percent natural and are allowed to carry the USDA seal.
Foods that contain two or more ingredients, like breakfast cereal, are still allowed to use the USDA seal, but also must include the following information:
Organic � The product must be 95 percent organic or greater in order to be able to use this term
100 percent organic � The product must be completely organic or all of its ingredients must be natural
Made with organic ingredients � The product contains no less than 70 percent natural ingredients
If the product has less than 70 percent natural ingredients, they are not allowed to use the word �organic� anywhere on their product labels.
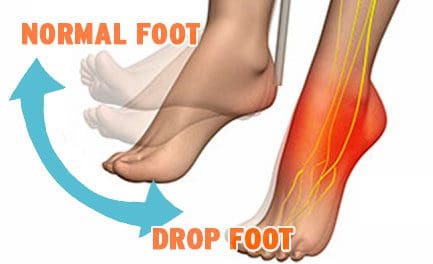
Drop Foot
Drop Foot is a symptom associated with an underlying neurological, muscular or anatomical problem that is often treated with a combination of non-invasive techniques and procedures.
Overview
Drop foot/foot drop is a general term that means lifting the forefoot (front part of the foot) is difficult to do.
Drop foot is not a diagnosis but a symptom associated with an underlying condition such as:
Neurological
Muscular
Anatomical problem
Nerve or muscle injury
Brain/spinal cord disorder, including
Herniated disc
Spinal Stenosis
Spondylolisthesis
Vertebral Fractures
Walking can be difficult, so the foot tends to drag on the floor.
Those suffering from drop foot sometimes raise the thigh up in an exaggerated fashion, such as when climbing stairs.
Stepping high is the most common symptom.
Symptoms of Drop Foot
High steppage gait
Foot drop may be experienced in one or both feet.
It is typically experienced in one foot if the drop foot is caused by:
Braces can provide additional support, stability, and shock absorption
Specific exercises to help the affected muscles
Physical therapy
Prevention
Prevention includes keeping your bones and tissues strong and healthy through diet and�exercise.
Avoid tobacco and excessive alcohol use creates weak bones and problems with the blood supply
Reduce the risk of injury by following safety measures on the job and beyond (i.e. wear a seatbelt).
Custom orthotics can provide additional support, stability, and shock absorption.
Kneeling for extended periods, such as on the job (certain construction functions laying tile, yard work).
Recovery
Some cases of drop foot are temporary; however, others can become permanent.
The recovery time and process depend on the cause.
Reduce *PLANTAR FASCIITIS PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Foot problems can affect the overall well-being of the human body. Many health issues which affect the foot can result in poor posture, low back pain, and sciatica. These imbalances can ultimately result in a variety of other health issues. Custom-made foot orthotics can help promote and support overall well-being by relieving foot problems.
Dr. Alex Jimenez is the non-surgical choice for foot problems and other health issues. Dr. Alex Jimenez can help promote and support overall well-being with the use of custom-made foot orthotics and other treatments approaches.
What’s Afoot
Foot Dysfunction can very easily cause a domino effect that extends all the way to the back. The feet are the foundation of the body and when there is a problem with the way they function it can cause the entire body to shift out of alignment. Overpronation and oversupination, for example, can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees, hips, and back as well.
NCBI Resources
If you have further questions or concerns about your particular�diet, please ask us! Our Doctor of Chiropractic can help guide you toward a more healthy life, including the foods you consume. It comes down to two major areas: safety and�nutrition. That is what consumers need to understand when they are trying to make a decision on whether to purchase foods that have been conventionally farmed or foods that are natural.
Until only several decades ago, neuroscientists believed that the brain stopped creating new neural connections, meaning that your memory starts to become irreversibly worse when the human body stopped developing, which is generally in your early 20s.� Neuroscientists also understood that neurons weaken and die as we age. The loss of brain function due to neural breakdown was believed to be a normal part of aging until recent research studies demonstrated the opposite of this belief. �
Over the last several years, it has become evident to neuroscientists that you can, as a matter of fact, create new neurons and develop new neural connections starting in your early 20s and continuing well into your old age. As the older regions of the brain start to wear out, you can ultimately rewire your brain and improve your overall brain health. But, how can you improve brain health? In the following article, we will discuss 5 ways you can improve your brain health and promote your well-being. �
Eat Healthy Foods
You are what you eat, or at least, your brain can be affected by the types of foods you eat. Eating junk food can have a tremendous impact on your brain health because trans fats and saturated fats, frequently found in processed foods, can negatively alter the brain’s synapses. Synapses connect the brains neurons and are fundamental for memory and learning. But, a balanced diet rich in omega-3 fatty acids, which are found in salmon, walnuts, and kiwi, can provide the synapses with a boost which can ultimately help fight against neurological diseases, including depression, dementia, and Alzheimer’s disease. �
Participate in Exercise
Participating in exercise and physical activity can also help boost your memory and help you think more clearly, reducing the risk of developing neurological diseases. Because exercise and some physical activity is a moderate stressor to the body, which uses energy needed by the brain, it triggers the release of substances, known as growth factors, which make the brain’s neurons fitter and stronger. Participating in 30 minutes of exercise or physical activity every other day can help improve brain health, and don’t forget to stretch. Stretching can help reduce anxiety, which can affect overall brain health. �
Mental Stimulation
Make sure to also give your brain a workout with brainteasers, crossword puzzles, and memory games. Research studies have demonstrated that using these tools to remain mentally active can help reduce the risks of developing dementia and other neurological diseases by building and maintaining a reserve of stimulation on your brain. Mental stimulation can help boost the regions of your brain which control and regulate learning and attention, which are hard-wired into the brain. �
Memory Training
Maintaining information stored in your memory banks and retaining that memory with age may also be a simple matter of mind control. By way of instance, confidence in your cognitive abilities might actually influence how well your memory works, especially for the elderly. Because many older adults tend to blame memory lapses on age, regardless of whether or not that is the reason, they may often be keeping themselves out of even trying to remember. Prediction can also enhance memory. If you have an idea of the information you have to remember afterward, you’re more likely to remember it. �
Get Enough Sleep
Getting enough sleep can help improve your overall well-being, especially your brain health. Sleep gives your brain an opportunity to match the memories of the day and combine them for long-term storage. One research study demonstrated that the brain can perform its reviewing much quicker when you are asleep than when you’re wide awake. A 90-minute mid-afternoon nap can help store long-term memories, such as events or skills you are attempting to master. Research studies have demonstrated that developing Alzheimer’s disease and other types of dementia are generally due to genetics. �
One research study, presented in July at the Alzheimer’s Association’s International Conference on Alzheimer’s Disease, demonstrated a connection between moms who develop Alzheimer’s disease and the chances that their children will develop the health issue in older age. Another research study suggests that a pattern of proteins is a risk factor for neurological disease. But, no one can predict who will develop dementia. While neuroscientists discover better treatments for these health issues, following ways to improve brain health is probably the best you can do to promote your overall well-being. �
Many neuroscientists once believed that the brain stopped developing new neurons and new neural connections as soon as you reached adulthood. However, recent research studies have demonstrated that we can create new neurons and new neural connection which can continue well into your old age.�In the following article, we discuss 5 ways you can improve your brain health and promote your well-being. From eating healthy foods to getting enough sleep, maintaining your overall well-being can help improve your brain health. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to demonstrate 5 ways which can ultimately help improve your overall brain health. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine










 �
�

 Herbs sometimes have additional information listed in the supplement panel. You might see ratio numbers (example 4:1) that show how much raw material of the herb (fresh or dried herb) is in the supplement version.
Herbs sometimes have additional information listed in the supplement panel. You might see ratio numbers (example 4:1) that show how much raw material of the herb (fresh or dried herb) is in the supplement version.