Gluteus Tendinopathy and Sciatica Symptoms in Fibromyalgia
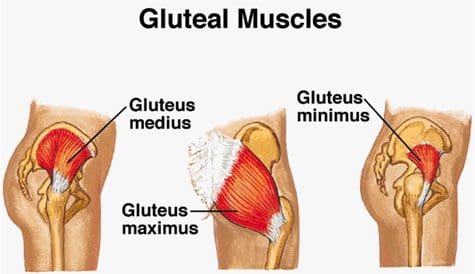
Gluteus medius tendinopathy (GMT), also known as dead butt syndrome (DBS), is a painful health issue caused by the inflammation of the tendons in the gluteus medius muscle. The gluteus medius (GM) is one of the smallest, less-known muscles of the buttocks which ultimately functions by providing stability and support to the structures of the hip and pelvis, especially throughout weight-bearing physical activities. Although GMT most commonly affects athletes, it can also affect people starting a new exercise program, during an intense workout routine or due to an underlying health issue. �
Healthcare professionals have reported an increased number of GMT cases over the past several years. While many doctors and functional medicine practitioners believe that this may perhaps be due to how many people participate and engage in exercise or physical activities after sitting down for extended periods of time, many GMT cases may actually be due to a well-known health issue called fibromyalgia. In the following article, we will discuss gluteus medius tendinopathy (GMT), or dead butt syndrome (DBS), fibromyalgia and how these two conditions can also be associated with sciatica symptoms. �
�
Sciatica and Gluteus Medius Tendinopathy Causes in Fibromyalgia
The common symptoms associated with gluteus medius tendinopathy, or GMT, include pain and discomfort, stiffness, and weakness in the hip or buttocks region. The painful symptoms can generally worsen throughout weight-bearing exercises, such as walking, running, and/or climbing. For many people, the pain and discomfort associated with dead butt syndrome, or DBS, can radiate down the hips, buttocks, and legs or thighs, similar to sciatica and hamstring tendinopathy. Sciatica is a collection of symptoms characterized by pain and discomfort, tingling sensations, and numbness along the sciatic nerve. �
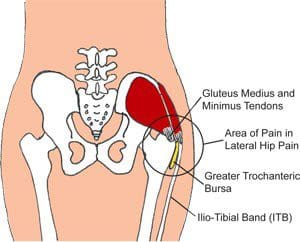
Many patients diagnosed with GMT also report experiencing painful symptoms when lying in bed on the affected hip or buttocks region as well as pain, discomfort, stiffness, and weakness throughout the night and upon rising in the morning. Moreover, if DBS progresses past the initial stage, the hip bursa may become inflamed, another health issue known as trochanteric bursitis, which may also cause swelling, tenderness, redness or warmth in the hip. In people with fibromyalgia, the widespread pain and discomfort caused by the inflammation of the condition may also ultimately cause GMT symptoms. �
The role of the gluteus medius muscle is to contract the weight-bearing hip throughout walking and running. When this small, lesser-known muscle triggers, the hip flexors release and vice versa. However, when the tendon becomes inflamed due to an injury or an aggravated underlying condition, such as fibromyalgia, the gluteus medius can fail to trigger appropriately, hence why the “dead butt” term is utilized as an alternate name for this health issue. People sitting down for extended periods of time may cause their hip flexors to become tight and failure to stretch before physical activities can cause DBS. �
Furthermore, poor gluteal or buttocks and hip muscle control cause excess stress on the gluteal medius tendon and/or muscle. Several athletes, especially runners, generally avoid utilizing cross-training and weight-lifting in order to help strengthen the larger muscles which support the pelvis when running, however, the hip’s and buttock’s smaller tendons and muscles may take on the excess pressure. If left untreated, gluteus medius tendinopathy (GMT), or dead butt syndrome (DBS) may lead to complications,�including trochanteric bursitis, IT band syndrome, and plantar fasciitis, among other health issues.
Differential Diagnosis of Hip Pain and Discomfort
� �
Fibromyalgia is widespread pain and discomfort throughout the human body. People with this painful condition can experience a variety of symptoms, including sciatica or sciatic nerve pain. Doctors and functional medicine practitioners believe that fibromyalgia can aggravate how the human body feels painful sensations by affecting how the human brain processes pain signals. Fibromyalgia and sciatica are two well-known conditions which can commonly coexist together. However, many fibromyalgia sufferers have also reported experiencing gluteal medius tendinopathy (GMT), or dead butt syndrome (DBS), a painful health issue caused by the inflammation of the tendons in the gluteus medius muscle. Because fibromyalgia is often associated with increased inflammation and painful symptoms, GMT or DBS and sciatica can commonly develop together. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
People with fibromyalgia experience widespread pain and discomfort as a result of their medical condition, however, healthcare professionals have demonstrated that fibromyalgia may also cause other symptoms and health issues to manifest, such as sciatica, or sciatic nerve pain, and gluteal tendinopathy. The purpose of the article above was to demonstrate and compare fibromyalgia, sciatica and gluteal tendinopathy symptoms. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
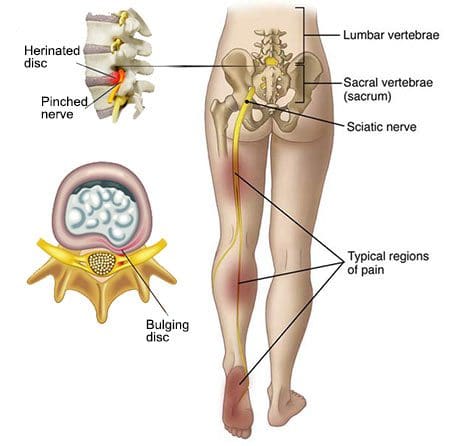
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Carpal tunnel syndrome, or CTS, is a condition where the nerve that runs from the forearm into the hand gets compressed. Carpal tunnel can cause significant pain and result in numbness that makes using your hand practically impossible.
Carpal tunnel affects�approximately 3% of the population. Carpal tunnel sufferers, fortunately, there are effective treatments that do not require surgery. Chiropractic care can help relieve the pain of carpal tunnel, and can often improve mobility and range of motion in the process.
Contents
What is it?
The term �carpal tunnel� refers to an actual tunnel created by ligaments and bones in the wrist. Tendons and median nerves travel from the forearm through the carpal tunnel in the wrist and into the hand. When the median nerve becomes compressed inside the carpal tunnel�usually due to injury or inflammation�it can lead to the symptoms associated with CTS.
The Causes
The exact cause of CTS is not always easy to identify, but there are many factors that can play a role. A family history of CTS makes it more likely that you will develop the condition. Repetitive work, such as a job on an assembly line, is known to increase the risk of CTS. Wrist injuries can also cause carpal tunnel. There are other contributing factors that are not as obvious, such as pregnancy, menopause, and dialysis.
Symptoms
The first signs of carpal tunnel often include a feeling of pins and needles in the wrist, hands, and fingers. You may notice some numbness from time to time, especially after using the wrist in a way that causes compression�like performing a task over and over at work.
Over time, the symptoms can become more severe. Eventually, carpal tunnel can lead to a loss of coordination with the thumb, then other digits. Pain may not be significant at first, but tends to get worse and the condition progresses.
Chiropractic Can Help
Standard medical treatments for carpal tunnel include using anti-inflammatory drugs, refraining from using the wrist/hand, wearing a splint and eventually surgery. While these treatments can sometimes be effective, the risks associated with surgery are significant. Carpal tunnel surgery may or may not fix the problem, and as with any surgery, can sometimes cause more issues than it helps.
Learning to Protect Yourself
Chiropractic care offers a safe alternative to standard medical care, one that is non-invasive and minimizes the need for medications and their potential side effects. Chiropractic treatments for carpal tunnel can help to reduce inflammation and minimize pain. But chiropractic goes further than just treating the symptoms�it can also help you avoid aggravating the condition so that it can heal.
Chiropractors are trained in proper movement and ergonomics. Your chiropractor can help you understand what you are doing that is causing the carpal tunnel to begin with. He or she can also advise you on ways to adjust your movements to protect your wrists moving forward. You may be able to learn new ways of doing things that will allow you to achieve your goals without risking injury.
Getting Stronger
One of the fundamentals of chiropractic care is improving strength and mobility to aid in healing and protect from further injury. Your chiropractor can guide you through exercises to make you stronger. Once you know how to do the exercises, you can do them at home to continue to gain strength.
Schedule An Appointment
Carpal tunnel sufferers, don’t wait any longer and contact us to schedule an appointment. We will get you the relief you need!
Fibromyalgia and sciatica are two well-known health issues which can commonly occur at seemingly the same time in people, however, these may also frequently require different treatment approaches to help manage their painful symptoms. Fibromyalgia is characterized by widespread pain throughout numerous regions of the human body. As complex as the diagnosis and treatment for fibromyalgia might be, it’s ultimately fundamental for patients to be aware of any other conditions which may subsequently develop due to the painful symptoms of these well-known health issues. �
Sciatica, also known as sciatic nerve pain, is a collection of symptoms rather than a single condition and it is one of the most common health issues to coexist together with fibromyalgia. In this instance, one condition doesn’t necessarily cause the other, however, they can basically be present together. Fibromyalgia�patients should understand how sciatica and its characteristic symptoms can affect their overall health and wellness. Many people with fibromyalgia may subsequently develop other health issues when these painful symptoms overlap with other conditions, such as piriformis syndrome. �
Contents
Piriformis Syndrome vs Sciatica and Fibromyalgia
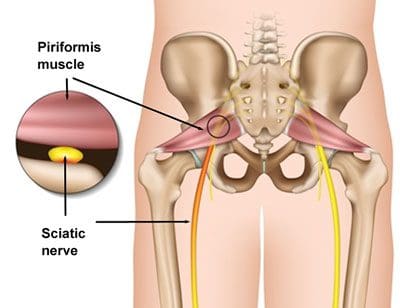
People with sciatic nerve pain, or sciatica, will often report experiencing pain and discomfort, tingling sensations, and numbness anywhere along the length of the sciatic nerve. The sciatic nerve is the longest and largest nerve in the human body, which travels from the lower back into the hip and buttocks, down into the thighs, knees, legs, and feet. Healthcare professionals may perform a variety of evaluations and tests to determine the source of a patient’s symptoms. People with fibromyalgia and sciatica may also experience another common health issue known as piriformis syndrome. �
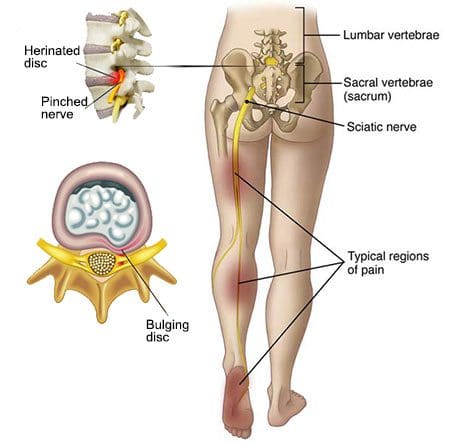
Sciatica is caused by the compression or impingement of the sciatic nerve, frequently due to a herniated disc. Piriformis syndrome can cause sciatica when a piriformis muscle spasm irritates the sciatic nerve. The piriformis is a muscle which extends from the front of the sacrum, or the triangle-shaped bone between the two hipbones in the pelvis, across the sciatic nerve and into the top of the femur, or the large bone in the upper leg.� The piriformis muscle is fundamental because it allows the thighs to move from side to side. When an injury or underlying condition causes the piriformis muscle to compress or impinge the sciatic nerve due to irritation and/or inflammation, the end result is typically piriformis syndrome. �
�
Sciatica is the most common symptom associated with piriformis syndrome. Other common symptoms associated with piriformis syndrome include tingling sensations and numbness, muscle tenderness, pain and discomfort while sitting or engaging in physical activities, and difficulty sitting comfortably. Because fibromyalgia causes widespread pain and inflammation, it’s also fundamental for people with fibromyalgia to seek immediate medical attention to diagnose all of their symptoms and rule out the possibility of their sciatica symptoms being due to piriformis syndrome or any other health issue. �
As previously mentioned above, sciatica, or sciatic nerve pain, is a medical condition or rather a collection of symptoms which causes pain and discomfort anywhere along the entire length of the sciatic nerve. For both fibromyalgia sufferers and people with the health issue alone, the pain and discomfort will generally manifest on one or both sides of the hips, buttocks, and thighs, where it will then radiate down the back of the leg, knees, and feet. In some instances, other common symptoms may manifest along the lower extremities, including tingling sensations, burning sensations, numbness, and weakness.
Sciatic nerve pain is most frequently caused by a slipped disc, a bulging disc, a herniated disc, or any other health issue which ultimately causes nerve pain and discomfort, such as fibromyalgia. When sciatica due to piriformis syndrome and/or another medical condition is experienced by fibromyalgia sufferers, it may be difficult for healthcare professionals to find the true source of their painful symptoms. Also, the symptoms associated with sciatic nerve pain and piriformis syndrome are generally the same for fibromyalgia sufferers, however, the most common causes may not be responsible for the symptoms.
Differential Diagnosis in Hip Pain
�
Fibromyalgia is characterized as widespread pain and discomfort throughout the human body. People with this painful health issue can experience a variety of symptoms, including sciatic nerve pain, or sciatica. Healthcare professionals believe that fibromyalgia can increase the way the human body experiences painful sensations by affecting the way the brain processes pain signals. Fibromyalgia and sciatica are two well-known conditions which can commonly coexist together. However, many fibromyalgia sufferers have reported piriformis syndrome, a condition caused when the piriformis muscle irritates the sciatic nerve. Because fibromyalgia can often be associated with increased pain and inflammation, these painful symptoms and health issues can ultimately occur. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
�
�
People with fibromyalgia experience widespread pain and discomfort as a result of their medical condition, however, healthcare professionals have demonstrated that fibromyalgia may also cause other symptoms and health issues to manifest, such as sciatica, or sciatic nerve pain, and piriformis syndrome. The purpose of the article above was to demonstrate and compare fibromyalgia and sciatica symptoms versus piriformis syndrome. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
*All of the above XYMOGEN policies remain strictly in force. �
An ankle sprain is always inconvenient, and often painful. But not all ankle sprains are equal in their severity. When diagnosing an ankle sprain, your doctor or chiropractor will classify the injury in one of three ways�first degree, second degree, and third degree. Knowing what each classification means can help you understand the nature of your injury and how careful you need to be with it. For you and your chiropractor, the classification of the ankle sprain degrees will help to direct the best treatment options.
Contents
Ankle Sprain Degrees and What They Mean
A sprain is an injury involving the stretching and/or tearing of your ligaments. With the ankle, it is possible to suffer an injury to either side of the joint, the interior or the exterior. You may have an inversion sprain or an eversion sprain. Whichever type you suffer from, it will fall into one of three categories:
Grades of ankle sprains
First Degree
A first-degree sprain is one where the ligaments have not torn, only stretched further than normal. Symptoms of a first-degree sprain include discomfort when jumping, jogging or sometimes walking. Pain is usually mild and swelling is minimal. The joint may be a little stiff and slightly less stable than normal.
Second Degree
A second-degree sprain is the most common type of sprain people seek medical care for. The ligament is partially torn, which can lead to several uncomfortable symptoms. The sprain will make walking difficult, be moderately painful and make it hard to use the ankle. The injury will result in noticeable swelling and often bruising.
Third Degree
A third-degree sprain is the most severe and involves a full tear of the ligament. Pain is often severe and swelling is significant. The torn ligament makes the joint unstable, so it is not only painful but also very hard to use.
How Chiropractic Can Help
Whether you are walking, running, jumping or just standing, the ankle plays a vital role in how you move and use your body. That is why it can be so frustrating when you find yourself with an ankle injury. Fortunately, ankle sprains do heal with enough rest and the right treatment.
Your chiropractor can help you recover from an ankle injury, both reducing pain and speeding up recovery time. There is research to support the use of chiropractic for ankle sprains.�One study showed that patients with ankle sprains experienced less pain when chiropractic was added to their treatment program. Chiropractic also focuses on improving mobility and range of motion, which can be quite beneficial when trying to recover from a sprain and get back to your normal life.
Some of the most common chiropractic treatments for ankle sprains include:
Adjustments
Adjustments can be made to more than just the spine. The bones, ligaments, and tendons in the ankle are designed to work in a certain way. A sprain can knock the ankle out of alignment, something that most traditional doctors and rehabs do not consider. An ankle adjustment will work to put things back into their proper places.
Strengthen Exercises
There are a variety of useful exercises that your chiropractor can take you through to improve strength and mobility in the ankle. Things like a wobble board, where you stabilize yourself on a wobbly platform and drawing on a board with a market held in your toes can be surprisingly effective at strengthening your ankle.
Call Us Today
Please contact us today to schedule an appointment with a chiropractor for your sprained ankle. Let us help you get stronger and heal faster!
April Hermosillo achieves overall health and wellness every day by following proper nutrition and engaging in exercises or physical activities. As a regular fitness participant, however, April Hermosillo can experience back and low back pain which ultimately affects even her most basic daily tasks.
April Hermosillo struggled with spine health issues and sciatica before she received chiropractic care. Dr. Alex Jimenez is a chiropractor in El Paso, TX who has helped April Hermosillo achieve pain relief so she can return to her everyday fitness routines. April Hermosillo describes how Dr. Alex Jimenez has tremendously helped improve her overall symptoms. April Hermosillo highly recommends Dr. Alex Jimenez as the non-surgical choice for personalized spine and sciatica treatment and rehabilitation.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
Our services are specialized and focused on injuries and the complete recovery process. Our areas of practice includeWellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Treatment, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Stress Management, and Complex Injuries.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
A variety of health issues can cause common symptoms which may make it difficult for people to determine the source of their pain and discomfort. Because sciatica is a collection of symptoms rather than a single condition, sciatic nerve pain can often be a frequent symptom for many health issues. The purpose of the following article is to demonstrate the differences between true sciatica and painful symptoms associated with other health issues, such as ischiofemoral impingement. �
Contents
What is Sciatica?
Sciatica is characterized as pain, tingling sensations, and numbness, due to compression or impingement anywhere along the length of the sciatic nerve. The sciatic nerve is the largest nerve in the human body and it stretches from the lower back through the hips and buttocks, down into the legs and feet. Sciatica can affect one or both sides of the human body. �
�
Symptoms
The characteristic symptoms of sciatica can range from mild to severe where the sciatic nerve pain is described as a dull ache to pain or as a sharp, searing, or electric-like pain. Symptoms differ from one person to another. By way of instance, some people may experience shooting pain while some people may only experience tingling sensations and/or numbness. � The common symptoms of sciatica, also known as sciatic nerve pain, include: �
Radiating pain along the length of the sciatic nerve
Discomfort, tingling sensations, and numbness
Muscle weakness in the lower back, hips, legs, and feet
A combination of pain, discomfort, tingling sensations and numbness
Painful sensations on one or both sides of the human body
Causes
Sciatica commonly occurs when an underlying health issue results in the compression or impingement of the sciatic nerve in the lower back. A bulging or herniated disk is one of the most common causes of sciatica. However, a variety of other underlying health issues can cause sciatica and determining what causes sciatica is necessary for proper treatment. � The most common causes of sciatic nerve pain, or sciatica, include: �
Bulging disk
Herniated disk
Degenerative disk disease
Bone spur osteophytes, or bone spurs
Spinal stenosis
Piriformis Syndrome
Arthritis
Treatments
Sciatica will often resolve on its own over several weeks. Healthcare professionals recommend the use of over-the-counter drugs and/or medications, ice or heat packs on the affected areas, stretches, and exercise, among other alternative treatment options to help reduce sciatica. If symptoms worsen or do not resolve on their own, seek immediate medical attention. � People with mild or moderate sciatica may find relief from any of the following treatments, including: �
Ice or heat therapy
Stretches and exercises
Physical therapy
Chiropractic care
Acupuncture
Alexander technique or Feldenkrais method
Yoga
Drugs and/or medications
If these approaches do not help reduce sciatica, the patient may need to take one or more imaging tests, such as an X-ray or magnetic resonance imaging (MRI), to diagnose the source of their symptoms. It’s important to note that sciatica is a collection of symptoms rather than a single condition. Sciatica may be caused by a variety of underlying health issues. �
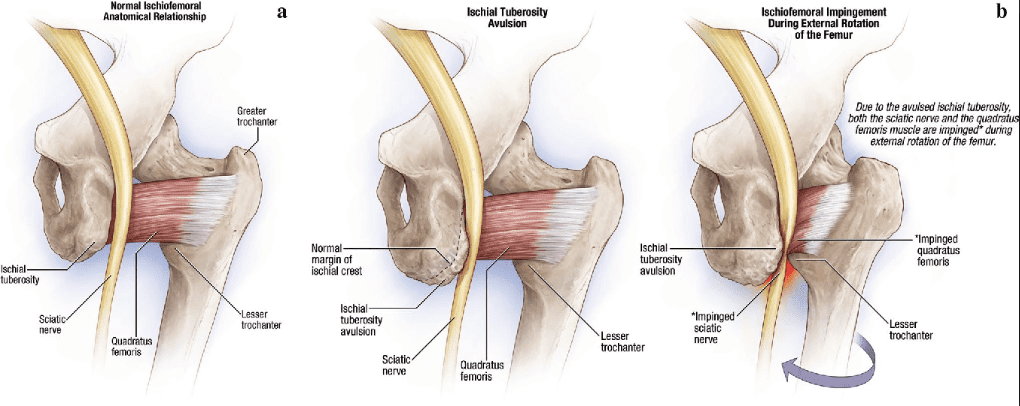
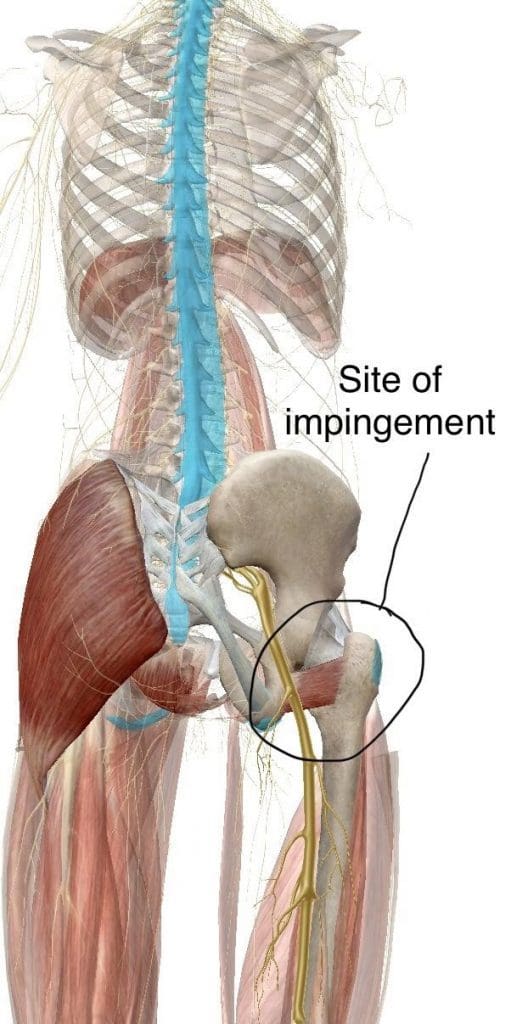
What is Ischiofemoral Impingement?
Ischiofemoral impingement syndrome is a condition which occurs when the ischium and the head of the femur experience excessive amounts of pressure, generally due to trauma, overuse, or surgery. The trauma, overuse, or surgery, can also cause bone spurs to grow along the ischium. This gives the bones an abnormal shape which makes them no longer fit together. �
Because these don�t fit properly together anymore, the bones may then start to rub against each other during movement causing friction which can damage the joint and cause painful symptoms. As friction worsens, the pain may also increase and restrict movements. The symptoms for ischiofemoral impingement may vary and treatment can also depend on symptoms. �
Symptoms
The main symptom of ischiofemoral impingement syndrome is hip pain. The pain from this underlying health issue may start off as mild, however, it can often worsen as the rubbing of the bones causes more damage and inflammation. Ischiofemoral impingement syndrome can feel similar to a pulled hamstring but the pain is generally closer to the buttocks. �
Causes
Ischiofemoral impingement occurs due to excess friction between the top of the thighbone, or the femur, and the hip bone, or the ischium. These two bones generally touch in a way which allows them to move without causing pain, however, trauma, overuse, and surgery can ultimately damage the bone. Moreover, if the damage causes a bone spur to grow on the hip or femur, as described above, the extra piece of bone�can cause more damage and make the condition worse. �
People who experience pain in the hips, buttocks, or groin that does not go away, should seek immediate medical attention to determine the underlying cause of their symptoms. Several of the symptoms associated with ischiofemoral impingement syndrome may be similar to other health issues, including sciatica, muscle, ligament and tendon tears, or fractures. A healthcare professional can perform a diagnosis to rule out ischiofemoral impingement as well as these other conditions. �
Diagnosis
To diagnose an ischiofemoral impingement, the healthcare professional may perform a physical exam. During the evaluation, doctor may feel specific areas in the hips to determine the presence of an ischiofemoral impingement. If the healthcare professional suspects you may have ischiofemoral impingement syndrome, they may request additional imaging tests, such as an X-ray or MRI, to confirm the diagnosis. Treatment will depend on the diagnosis of the source of the symptoms. �
Ischiofemoral Impingement Syndrome is quite an uncommon diagnosis for hip and groin pain � thus it is important that more common conditions like those listed below, are ruled out by a qualified Medical Professional, Chiropractor or� Physiotherapist before considering it as a diagnosis: �
Lumbar disc disease
Spinal stenosis
Bursitis
Osteoarthritis
Rheumatoid arthritis
Cancer
Inguinal hernias
Inguinal lymphadenopathy
Menstrual conditions
Urinary tract problems
Pelvic inflammatory diseases
Femoroacetabular impingement/piriformis syndromes
Treatments
There is no single treatment which can be utilized to help improve ischiofemoral impingement syndrome. The healthcare professional might recommend a variety of alternative conservative treatment options. By way of instance, they may restrict physical activities or they may recommend rest as well as prescribe drugs and/or medications to help ease the symptoms. There are many dynamic treatment protocols that can assist in these diagnoses. If alternative treatment options do not help improve the ischiofemoral impingement, the healthcare professional may also recommend the utilization of injections which contain pain medicine and/or steroids to help control the pain. If neither of these treatment approaches helps relieve the symptoms, the healthcare professional may also recommend surgery. Due to the rarity of Ischiofemoral Impingement, treatment for the condition has varied on a case by case basis. However, conservative treatment is broadly recommended as a first line approach to resolving the condition. Current conservative treatment strategies in the literature for Ischiofemoral Impingement Syndrome include: �
Nonsteroidal anti-inflammatory drugs and Gabapentin for pain associated with quadratus femoris muscle and sciatic nerve irritation
Heat, Ultrasound, and Interferential current therapies applied around the hip area.
Deep Specialized Myofascial protocols can be used.
An individually prescribed exercise program by a Physiotherapist or joint specialist targeting muscles like the quadriceps femoris, piriformis in order to adequately reduce pain and increase the range of motion in the hip joint.
CT-guided steroid and local anesthetic injection around the QFM may provide pain relief
Surgical intervention in order to correct/decompress anatomical pathology such as that first described by Johnson in 1977 is reserved for cases that do not respond to conservative therapy. Potential surgical interventions include excision of the lesser trochanter (in those experiencing pain post hip surgery), and more recent/popular peri-articular endoscopic decompression around the hip 2,7. Further research is required to better understand Ischiofemoral Impingement Syndrome � its causes, at-risk populations, and optimal management strategies- both conservative and surgical. As this condition is not yet widely recognized and understood. �
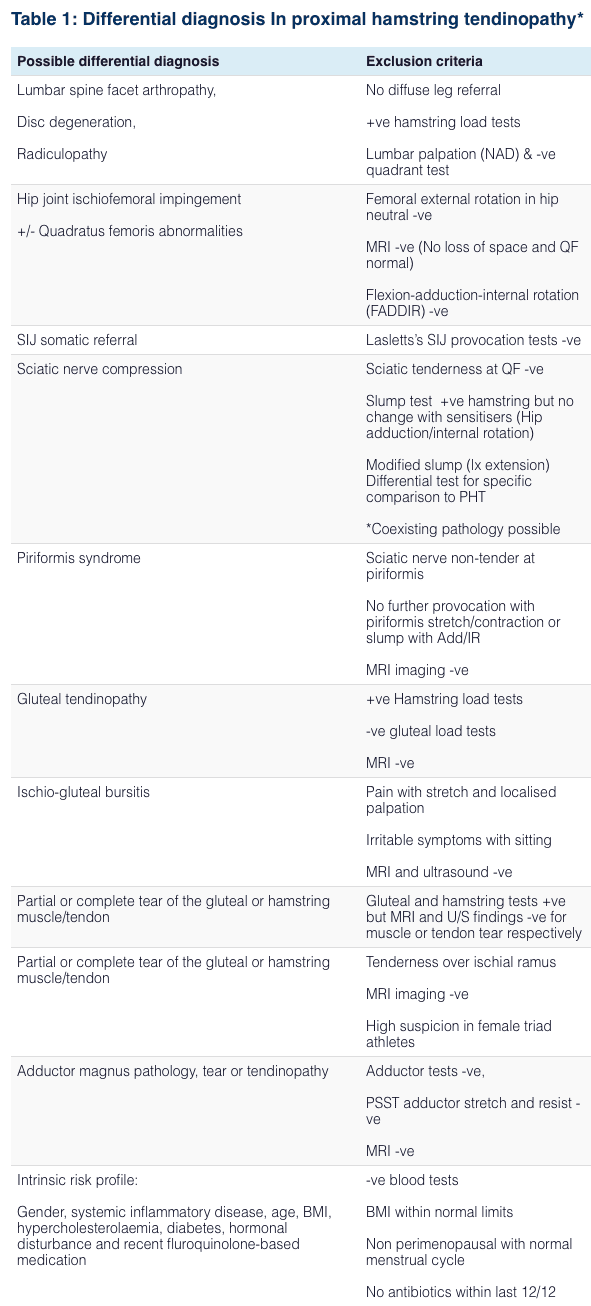
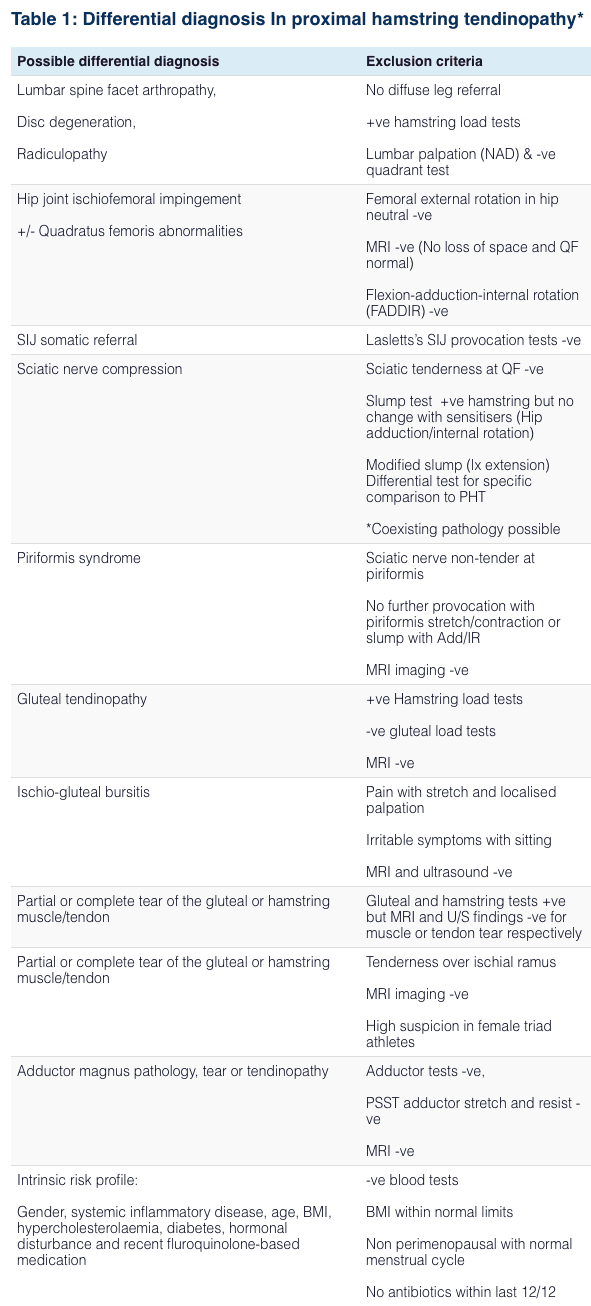
Differential Diagnosis In Proximal Hip Pain Syndroms
� �
Sciatica, or sciatic nerve pain, commonly characterized by pain and discomfort, tingling sensations, and numbness, can be a common symptom for a variety of underlying health issues, such as ischiofemoral impingement. Because sciatica is well-known as a collection of symptoms, rather than a single condition or disorder, patients with sciatic nerve pain should seek immediate medical attention to determine if their painful symptoms are caused by another underlying health issue. Treatment for both sciatica and ischiofemoral impingement will depend on the symptoms and diagnosis. There are many treatment options for these complex cases – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Non-Invasive Treatments for Chronic Low Back Pain
�
�
The article above demonstrates the differences between true sciatica and painful symptoms associated with other health issues, such as ischiofemoral impingement, to help provide a diagnosis and treatment. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
� For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
� �
References Singer, Adam D., Ty K. Subhawong, Jean Jose, Jonathan Tresley, and Paul D. Clifford. �Ischiofemoral impingement syndrome: a meta-analysis.� Skeletal radiology 44, no. 6 (2015): 831-837 Johnson, K. A. �Impingement of the lesser trochanter on the ischial ramus after total hip arthroplasty. Report of three cases.� JBJS 59, no. 2 (1977): 268-269 Spencer-Gardner, Luke, Asheesh Bedi, Michael J. Stuart, Christopher M. Larson, Bryan T. Kelly, and Aaron J. Krych. �Ischiofemoral impingement and hamstring dysfunction as a potential pain generator after ischial tuberosity apophyseal fracture non-union/malunion.� Knee Surgery, Sports Traumatology, Arthroscopy 25, no. 1 (2017): 55-61 Lee, Soyoung, Inhwan Kim, Sung Moon Lee, and Jieun Lee. �Ischiofemoral impingement syndrome.� Annals of rehabilitation medicine 37, no. 1 (2013): 143
Backpacks allow us to carry everything we need wherever we go. But as great as backpacks are, the fact is they can cause real damage if they are not carried correctly. It is possible to carry more weight than you should and in ways that are not healthy. From children to the elderly, everyone should know how to properly carry a backpack.
Contents
How Not Carrying Properly Can Hurt Your Back
A recent article on NBC News discussed the health concerns that backpacks present, discussing the various studies that have shown the damage they can cause. As the article noted, most everyone uses a backpack at one time or another. They are simply too useful to do otherwise. But research has demonstrated that they can hurt the back significantly, especially in children.
The back injuries that a backpack can cause include:
Disc Injuries
The spine is made up of vertebrae separated by spinal discs. The discs provide cushioning and flexibility in the spine. But the discs in your spine are only capable of carrying so much weight. When a backpack is too heavy, it can lead to disc compression and possibly tearing of the disc.
Carrying a backpack over one shoulder day after day will eventually cause your body to alter its alignment and your muscles to become imbalanced. Muscle imbalances can cause a cascade of problems, including altering the way you walk and increasing wear on your spine.
How to Carry Properly
Backpacks can be used safely, you just need to take the proper steps. These include:
1. Do Not Carry too much weight.
The recommended percentage of your body weight when using a backpack ranges from 10% – 15%. Someone that weighs 100 lbs should carry a backpack weighing no more than 15 lbs. Ideally, you should keep it around 10%. The more you go over the recommended weight, the more risk of injury to your back.
2. Utilize both straps.
Backpacks are designed to be carried using a strap over each shoulder. Using both straps distributes the weight evenly across your shoulders, minimizing the risk of excessive wear or injury.
3. Adjust the straps.
The straps of your backpack should be pulled snug, but not too tight. If your backpack includes a belt or additional straps, use them � especially if you are carrying a lot of weight.
4. Carry only what is needed.
It is easy to accumulate items in your backpack without realizing how much you have. Try to examine what is in your pack on a regular basis to ensure you are only taking what you need.
5. Use roll bags for heavy loads.
If you really need to carry more weight, invest in a bag with wheels. Rolling backpacks or other rolling bags can allow you to carry significantly more weight in comfort and safety.
6. Apply all of the above to your child�s backpack.
If you have one or more children, it is important to train them on how to use backpacks safely � and to check them from time to time.
Enjoy Back Pain Relief
Our chiropractic team is ready to help you get relief from your back pain. If you are suffering from back pain, please contact us to schedule an appointment with an experienced chiropractor.
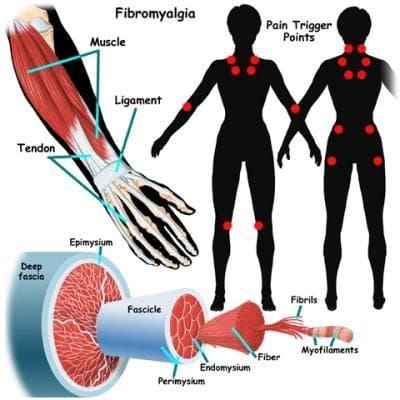
Fibromyalgia is a disorder characterized by widespread musculoskeletal pain which is also generally accompanied by fatigue, sleep, memory, and mood health issues. The most common symptoms associated with fibromyalgia include muscle pain and tenderness, however, many people with this painful condition also experience sciatica, a collection of symptoms characterized by pain, discomfort, tingling sensations, and numbness along the length of the sciatic nerve in the lower back. �
Because fibromyalgia can cause painful symptoms throughout several regions of the human body, many people with fibromyalgia may also be diagnosed with other health issues which may overlap with their present symptoms, such as sciatica. It’s essential for patients to seek immediate medical attention from a healthcare professional to receive a proper diagnosis of all of their symptoms as these other health issues may generally require different treatment approaches. �
Sciatica is one of the most common health issues to coexist with fibromyalgia. Fibromyalgia doesn’t necessarily cause sciatica or sciatic nerve pain, however, these can ultimately exist together. It’s also essential for people with fibromyalgia to understand what sciatica is and how these painful symptoms can affect their health and wellness. Healthcare professionals believe that fibromyalgia amplifies painful sensations by affecting the way the human brain processes pain signals. Moreover, fibromyalgia can affect a variety of other structures and functions in the human body, such as the gastrointestinal tract. �
Fibromyalgia and Digestion Problems
Along with muscle pain and tenderness, patients with this painful disorder also experience digestive health issues. About 70 percent of people with fibromyalgia suffer from irritable bowel syndrome symptoms, including gas, bloating, constipation, and diarrhea. Although the causes of digestion health issues and fibromyalgia are unknown, healthcare professionals have demonstrated that there is an undeniable connection between fibromyalgia and digestive health issues. �
The gastrointestinal, or GI, system consists of several fundamental parts including, the esophagus, the stomach, the small intestine, and the bowel. When digestion slows down or a food intolerance, described in further detail below, disrupts the natural process of digestion, a chain of events can cause pain and discomfort, among other symptoms, throughout the entire gastrointestinal, or GI, tract. Patients with fibromyalgia commonly report frustrating digestive problems, such as: �
Acid reflux. When the gastric juices are not being utilized in the stomach, they can often travel back up through the esophagus, causing heartburn or a painful sensation in the chest, known as acid reflux.
Cramping and constipation. When the process of peristalsis, or the smooth muscle contractions which move food through the gastrointestinal tract, becomes affected due to the irritation of the intestines, it can begin to cramp and prevent the movement of waste through the bowel, causing cramping and constipation.
Diarrhea. When the digestive process slows down or stops, undigested food can move from the stomach and into the intestine, where it can irritate the lining of the colon and produce IBS symptoms, such as diarrhea.
Gas. The longer food stays in your stomach and intestines, the longer the natural GI bacteria has to break down the compounds and the more methane gas is produced from bacteria metabolism, resulting in gas.
Research studies have utilized brain scans to demonstrate the physiological responses of patients with irritable bowel syndrome, or IBS, and patients with fibromyalgia. According to the research studies, both groups of patients demonstrated higher neurological responses to pain. Patients with IBS and fibromyalgia also demonstrated higher pain awareness. Due to the similar brain activity to pain stimulus, researchers suspect that the two health issues may share underlying causes. �
Many people with fibromyalgia frequently report that certain types of foods irritate their stomach or exacerbate their fibromyalgia symptoms. Dairy and gluten, among other foods, can worsen fibromyalgia. Many people have food intolerances which can be challenging to diagnose. Another common explanation for the digestion problems of patients with fibromyalgia involves the autonomic nervous system, which is in charge of regulating the structure and function of internal organs. �
This autonomic nervous system is made up of two subsystems: the sympathetic nervous system and the parasympathetic nervous system, which rarely work together simultaneously. In patients with fibromyalgia, the sympathetic nervous system, which is largely responsible for increasing blood pressure, heart rate and adrenaline, is almost always active, causes the parasympathetic system, which is largely responsible for relaxation and digestion, to become inactive. Fortunately, patients with fibromyalgia and its associated symptoms like sciatica and digestive problems, can find relief through treatment.
�
Patients with fibromyalgia commonly experience widespread pain and discomfort, however, research studies have demonstrated a connection between other symptoms and health issues, such as sciatica and digestive problems. The purpose of the following article is to educate as well as discuss how fibromyalgia may be connected to other symptoms like sciatica and irritable bowel syndrome, among other digestive problems. By understanding how these symptoms and health issues are associated with fibromyalgia, patients and doctors can safely and effectively treat this painful condition and its symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Non-Invasive Treatments for Chronic Low Back Pain
�
Fibromyalgia is a disorder characterized by widespread musculoskeletal pain accompanied by a variety of symptoms. Many people with this painful condition also experience sciatica and digestive problems. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
� For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Individuals dealing with chronic pain talk about their symptoms and how they have affected their overall health. After getting chiropractic treatment, patients describe how local chiropractor Dr. Alex Jimenez helped them get back to their normal lives.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities. �
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
We Can Get You Back On Track!
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us. �
The human body can absorb toxins in a variety of ways, from the type of foods we eat to the external and environmental factors we’re exposed to on a regular basis. Fortunately, the human body can also eliminate toxins in a variety of ways. Healthcare professionals have recognized that the accumulation of toxins in the human body can cause numerous health issues, including inflammation which may lead to back pain and sciatica. A good detox plan can help improve your overall health and wellness from the inside. Detoxing is also a fundamental process which can help relieve sciatica and back pain.
Contents
Back Pain and Sciatica
Back pain is one of the most common health issues reported among the general population. Although back pain affects approximately 80 percent of people at least once throughout their lifetime, sciatica continues to be one of the most frequently misunderstood health issues across the world. Also known as sciatic nerve pain, sciatica is characterized by irritation or inflammation due to the compression or impingement of the sciatic nerve, the longest and largest nerve in the human body. The sciatic nerve travels from the lower back, down the hips and buttocks, into the legs and feet. �
A variety of alternative treatment options, such as chiropractic care, can help safely and effectively treat sciatica symptoms without the side-effects of drugs and/or medications. Many healthcare professionals may recommend the use of drugs and/or medications to help offer sciatic nerve pain relief, however, these are only managing the symptoms rather than treating the health issue at the source. Research studies demonstrated that 76 percent of patients with sciatica reported complete relief of their symptoms without any toxic side-effects after following a detox plan for 45 days. �
Detox for Sciatica and Back Pain
For those people who may not be sure how or where to start with a detox plan, it’s fundamental for you to know that you can detox the human body on a variety of levels. First, you can start off with a simple foot detox. Healthcare professionals have demonstrated that a detox foot bath is a good way to cleanse the human body. Best known as the BioElectric Field Enhancement Unit, this helps generate positive and negative ions which creates the pH balance in the human body. As a result, the human body’s negative ions decrease while the human body’s positive ions increased to provide pain relief. �
To perform a detox foot bath, soak your feet for 30 minutes in warm salt water together with the foot coil. This process can help give muscles the strength and endurance they need to deal with back pain and sciatica symptoms. Moreover, a detox foot bath can also help eliminate free radicals which enhance range of motion. A detox foot bath also supports circulation. A good detox plan to help improve sciatica and back pain can also include following proper nutrition. Healthcare professionals can recommend a diet food plan which can help detox the human body from the inside with other treatment approaches. �
As previously mentioned, nutrition and lifestyle modifications below can help cleanse and detox the human body, including: �
Drinking more water, at least a minimum of two liters a day.
Drinking freshly squeezed juices without adding sugar, several times a day.
Replacing one meal with fresh smoothies, preferably breakfast.
Eating a healthy diet without processed foods, red meat, sugar, and dairy products.
According to healthcare professionals, it is a healthy practice to follow a detox plan once every 3 to 4 months. Do you remember when was the last time you had a detox? Or do you at least remember ever having a moment where you considered detoxification? Whether you followed a detox plan a few months ago, a year ago, several years ago, many years ago or simply never, it doesn�t matter. There is no better time then to start now. A detox plan cleanses the bloodstream, improves gut health, channels energy levels and strengthens muscles. Detox helps improve sciatica from its source. �
Sciatica is a collection of symptoms which can manifest due to a variety of underlying health issues. However, numerous research studies have demonstrated that following a detox plan can help tremendously reduce irritation and inflammation associated with sciatic nerve pain. Following a proper nutrition and lifestyle modifications together with a detox plan can ultimately help improve overall health and wellness, including sciatica and back pain. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Non-Invasive Treatments for Chronic Low Back Pain
Following a detox plan may help pain and inflammation associated with sciatica. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
� For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
 �
� 
 �
�



 �
�
 �
�




 If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Recommend: Dr. Alex Jimenez – RN, DC, MSACP, CCST
Health Grades:
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Recommend: Dr. Alex Jimenez – RN, DC, MSACP, CCST
Health Grades: 
 �
�