Dr. Alex Jimenez is excellent, he’s patient, he gets right to the point of the situation, and then helps you with your stretching and therapy to make sure that it doesn’t continue. I recommend him for everybody in El Paso, the whole state of Texas. He should be in every town, move to San Antonio. -�Ottis Hamlet
Are you aware of how dependent you are on the use of your hands for everyday tasks? As humans, we rely tremendously on the proper function of our hands, wrists and elbows to perform many physical activities. Many people may not understand how essential this can be until they encounter an injury or condition which impedes them from using their hands.
Hand, wrist and elbow pain can cause a wide variety of problems, preventing you from being able to take part in even some of the simplest, ordinary chores without experiencing painful symptoms. Based on the severity of the pain, health issues affecting your hands, wrists or elbows can prevent people from driving, utilizing a computer or other electronic devices, cooking dinner and it can even make working difficult.
To make matters worse, the condition of your hands can ultimately affect the entire condition of your upper extremities. An injury or aggravated condition along a single part of the hand, such as a finger, could cause pain to radiate through the wrist and elbow, into the arm and shoulder. Below, we will discuss the common causes of hand pain and their treatment.
Common Causes of Hand Pain
While many instances of hand pain, wrist pain and elbow pain may resolve on their own, a minor inconvenience can quickly become a much bigger health issue if left untreated. Painful symptoms can slow us down as we’re attempting to go about our day and chances are that the need to finish a job will continue to aggravate the pain and cause discomfort. If you experience chronic hand pain symptoms, you may want to visit a doctor immediately.
Because our arms and hands are interconnected, an injury or condition to any part of the upper extremities can end up causing anything from tingling sensations and numbness in the fingers to pain and discomfort in the arms. A qualified and experienced healthcare professional, such as a chiropractor, can help you understand the source of your hand pain as well as determine the best treatment option for your specific health issue.��
There are many health issues which might lead to pain and discomfort in the hands, elbows and wrists. Common causes of hand pain include:
Joint pain
Arthritis
Tendonitis
Tennis/Golf Elbow
Fractures
Sprains
Carpal tunnel syndrome
Carpal Tunnel Syndrome
One of the most common causes of hand pain is the result of a chronic condition called carpal tunnel syndrome. Carpal tunnel syndrome, or CTS, is a painful syndrome caused by a pinched nerve in the wrist which causes pain, tingling sensations and numbness in the hand and arm. The pain usually feels like a�profound and intense hand cramp although cramping is not a common symptom associated with carpal tunnel syndrome.
Carpal tunnel syndrome develops due to heightened stress and pressure on the median nerve, frequently due to highly repetitive movements with the hand and wrist. Some of the most common tasks in today’s society,�such as writing, typing on a keyboard, playing with video games, gardening, and anything else which requires repetitive alternative or lifting hand motions, have become one of the leading causes of carpal tunnel syndrome.
As mentioned above, several common symptoms of carpal tunnel syndrome, or CTS, may cause�severe pain in the hand, wrist and elbow, as well as result in tingling sensations and numbness which may radiate from the fingers up to the arm. Research studies have also found that patients who may be experiencing hormone fluctuations are at an increased risk of developing the condition. However, people who are most at risk of developing CTS have been found to be those who work in a position that requires them to engage in repetitive motions with their hands.
Many healthcare professionals recommend surgical interventions to treat carpal tunnel syndrome but many patients have experienced relief from their hand pain through the use of alternative treatment options, such as chiropractic care,. Moreover, wearing a brace, working to counteract repetitive motions and taking steps to decrease stress and pressure on the hand can help improve pain associated with carpal tunnel syndrome.
While a number of these treatment techniques and methods can be performed at home by the patient, it’s essential to seek immediate medical attention from a qualified and experienced healthcare professional to avoid further damage. A chiropractor can help treat hand pain. Below, we will describe how chiropractic care may improve chronic hand pain symptoms.
Because we depend tremendously on the use of our hands, injuries and/or conditions which result in hand pain, such as carpal tunnel syndrome, can be very debilitating, ultimately affecting every aspect of an individual’s quality of life. Chiropractic care is a safe and effective, alternative treatment option which can help treat hand pain. Through a series of exercise and physical activity programs, chiropractic care can help restore normal hand function and reduce hand pain. -�Dr. Alex Jimenez D.C., C.C.S.T.
Chiropractic Care for Hand Pain
Chiropractic care is a healthcare profession which utilizes spinal adjustments and manual manipulations to treat a variety of injuries and conditions associated with the musculoskeletal and nervous system. For a doctor of chiropractic, or chiropractor, the first step for managing hand, wrist or elbow pain is to evaluate the source of the symptoms.�
After the diagnosis, the chiropractor’s next priority is to use a series of alternative treatment options to relieve the patient’s hand pain as soon as possible. A chiropractor may use spinal adjustments and manual manipulations to carefully correct any spinal misalignments, or subluxations, which may be causing referred hand pain.
After that, a chiropractor may recommend a series of lifestyle modifications, including exercise and physical activity programs, in order to promote recovery and begin focusing on building the patient’s assortment of motion, particularly flexibility maneuvers. Stretches and exercises for building strength will be included following the patient’s treatment plan, in order to ensure no additional damage occurs.
When you’re ready to start, contact a chiropractor to set up an appointment to get yourself on the road to relieving your hand, wrist and/or elbow pain.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
On my first visit, I automatically felt better but along came with soreness. I did continue treatment, I saw him (Dr. Alex Jimenez) maybe two or three times out of the week. Shortly after that I started noticing change.�
Denise
The shoulder consists of a number of joints which merge together with other complex structures, including muscles, tendons and ligaments, to provide a wide range of movement in the arm, like scratching your back.
This increased range of motion, however, can cause a variety of health issues. It might lead to problems with impingement or it might even result in instability on the bony structures or the soft tissues of the shoulder. Shoulder pain might be felt continuously or it might occur through movements of the shoulder. Moreover, shoulder pain can be temporary or it might become chronic and require proper diagnosis and treatment.
The article below describes a few of the common causes of shoulder pain and discusses various treatment approaches to help improve shoulder pain. A qualified and experienced healthcare professional may be able to provide you with more information regarding your shoulder pain.
Anatomy of the Shoulder
The shoulder is a complex structure which is made up of three bones: the upper arm bone, also known as the humerus, the shoulder blade, also known as the scapula, along the collarbone, also known as the clavicle.
The head of the upper arm bone fits into a round socket on the shoulder blade, called the glenoid. A variety of ligaments, tendons and muscles then function by holding the upper arm bone. These collection of soft tissues are referred to as the rotator cuff. The main function of the rotator cuff is to both attach and cover the head of the upper arm bone in the shoulder.
Causes of Shoulder Pain
Most health issues that cause shoulder pain fall into four big categories:
Tendon inflammation, bursitis and tendinitis, or a tendon tear
Instability
Arthritis
Fracture or broken bone
Other much less common causes of shoulder pain can include factors such as tumors, disease or aggravated conditions, and nerve-related problems. Below, we will discuss the common causes of shoulder pain in detail.
Bursitis
The bursae are small, fluid-filled sacs which are found between joints throughout the entire body, including the shoulder. These function by decreasing friction between the bone and the muscles as well as act as cushions between the soft tissues and the bones.
Occasionally, excessive utilization of the shoulder can contribute to the swelling and inflammation of the bursa between the rotator cuff and a part of the shoulder blade called the acromion. The outcome measure of this health issue is a condition known as bursitis.
Bursitis often occurs in association with rotator cuff tendinitis, discussed below. The soft tissues in the shoulder can then become painful and inflamed. As a result, daily tasks, such as cleaning or brushing your hair and getting dressed, can become challenging to perform.
Tendinitis
A tendon is a cord which connects the muscles to the bones at different sites. Tendinitis is a consequence of inflammation in this soft tissue.
Ordinarily, tendinitis is frequently categorized as one of two types:
Acute. Overhead physical activities or ball projecting during a sport game or work may result in acute tendinitis.
Chronic. Degenerative diseases like arthritis or degenerative wear and tear as a result of age, may lead to chronic tendinitis.
The joints in the shoulder most commonly affected with tendinitis include the four rotator cuff tendons, particularly the shoulder tendons. The rotator cuff consists of four muscles and their respective tendons which keep the shoulder stable and protect the head of the upper arm bone. The rotator cuff provides equilibrium and shoulder movement.
Tendon Tears
The splitting and tearing of the tendons may by caused by severe damage or trauma from an injury as well as from degenerative changes in the joints due to the normal aging process, long-term overuse and the general wear-and-tear of the joints. These tears may divide the tendon completely out of its attachment or they may only be partial. Normally of tears, the tendon is entirely separated from the bone. Rotator cuff and biceps tendon injuries are among the most common types of tendon tears.
Impingement
Shoulder impingement happens when the cap of the shoulder blade, known as the acromion, places pressure on the underlying soft tissues once the arm is raised away from the torso. When the arm is raised, the acromion rubs, or “impinges” on, the rotator cuff tendons and bursa. This may result in tendinitis and bursitis, restricting motion and causing pain.
Instability
Shoulder instability occurs when the head of the upper arm bone is forced out from the shoulder socket. This can occur as a consequence of a sudden injury or even due to the excessive use of the shoulder.
Shoulder dislocations may only be partial, where only a part of the head of the upper arm may come out partially from the socket. This is also referred to as a subluxation. A complete dislocation usually means that the ball of the upper arm at the shoulder comes out all of the way from the socket.
When the ligaments, tendons, and muscles around the shoulder become torn or loose, dislocations can happen differently. Dislocations, which might be complete or partial, cause unsteadiness and pain when the arm is moved or lifted. Episodes of dislocations or subluxations result in an increased chance of developing arthritis in the shoulder joint, among others.
Arthritis
Health issues resulting in shoulder pain may also lead to arthritis. There are various kinds of arthritis. The most common kind of arthritis in the shoulder is osteroarthritis, also called the “wear-and-tear” arthritis. Osteoarthritis symptoms can include pain, stiffness and swelling which may begin during the day and may worsen throughout the day.
Osteoarthritis might also be associated with work or sports accidents as well as chronic wear-and-tear problems. Other kinds of arthritis could be linked to rotator cuff tears or an inflammation of the joint lining.
Many times, individuals who already have arthritis in the shoulder joints will attempt to prevent moving their shoulder in an effort to reduce arthritis pain and discomfort, However,�this often contributes to the stiffening or the tightening of the soft tissues surrounding the shoulder joints, leading to a painful restriction of movement.
Fracture
Fractures are frequently referred to as broken bones. Shoulder fractures commonly involve the clavicle, or the collarbone, the humerus, or the upper arm bone, and the scapula, or the shoulder blade.
Shoulder fractures in elderly patients are frequently the consequence of a fall from standing height. In the average person, harm from a motor vehicle accident or a sports accident often causes shoulder fractures.
Fractures frequently cause acute pain, swelling, and bruising concerning the shoulder. If a shoulder fracture is suspected, it’s important for the person to seek immediate medical attention by a healthcare professional.
Diagnosis for Shoulder Pain
In the instance of any of the health issues mentioned above resulting in extreme shoulder pain, seek medical attention as soon as possible to receive a proper diagnosis. While many cases of shoulder pain may resolve on their own, make sure to see a doctor if symptoms persist or worsen.
A healthcare professional will conduct a comprehensive evaluation so as to ascertain the cause of the patient’s shoulder pain before providing them with the appropriate treatment options for their health issues.
Medical History
The first step for diagnosis is a comprehensive look at the patient’s medical history. The doctor will ask how the problem has been previously treated and how the pain began, if they are aware of that information. Moreover, additional questions will help determine the causes of the patient’s shoulder pain. Since certain actions may improve or worsen symptoms, a record may be an important tool in discovering the origin of shoulder pain.
Physical Evaluation
A thorough examination will help to discover the source of a patient’s shoulder pain. A doctor will assess for tender places and will try to find physical abnormalities, swelling, deformity or muscular fatigue. They will also observe the shoulder’s strength, flexibility and movement.
Tests
The healthcare professional may additionally order certain tests to help identify the reason for the patient’s shoulder pain and help determine if the symptoms are due to other health issues. The following list demonstrates the variety of tests which can help determine the diagnosis.
X-rays. These images will reveal bone injuries.
Magnetic resonance imaging, or MRI and ultrasound. These imaging studies produce images of soft tissues. MRI can help your doctor identify injuries to the ligaments and tendons.
Computed tomography, or CT, scan. This instrument joins computer technologies and x-rays to make a better, much detailed image of the bones located in the shoulder region.
Electrical studies. The doctor may order an evaluation, including an EMG, or electromyogram, to assess neural function.
Arthrogram. In this study, dye is injected to show the joint and its surrounding soft tissues. It might be used together with an MRI.
Arthroscopy. During this procedure, a doctor looks inside the joint using a camera. Arthroscopy may reveal soft tissue injuries that aren’t apparent in evaluations along with the exam. Arthroscopy can be used to fix the problem and help find the reason for symptoms.
Dr. Alex Jimenez’s Insight
As the most mobile joint in the human body, the shoulder joint is often vulnerable to experience a variety of problems which can result in shoulder pain. Shoulder pain can tremendously affect an individual’s ability to perform everyday tasks and, if lest untreated, it can progress into neck and back pain as well as cause other severe symptoms. Understanding the cause of a patient’s shoulder pain can help diagnose their problem in order to recommend the best treatment option.
Treatment for Shoulder Pain
Chiropractic Care
Chiropractic care is a safe and effective, alternative treatment option which can help manage shoulder pain by relieving discomfort and swelling, among other painful symptoms. A chiropractor will utilize chiropractic adjustments and manual manipulations to reduce joint restrictions and correct spinal misalignments, in an effort to improve function.
Lifestyle Modifications
Furthermore, a doctor of chiropractic, or chiropractor, will recommend a series of lifestyle modifications to help promote a faster recovery process. Changing a patient’s actions through a balance of rest and physical therapeutics can help improve shoulder endurance. Avoiding overexertion can also help prevent further harm and shoulder pain.�
Drugs & Medications
A doctor may also prescribe drugs and/or medications to decrease shoulder pain and inflammation. It needs to be taken only as directed, however, if medicine is prescribed to ease pain. A physician can also recommend shots of numbing steroids to alleviate pain.
Surgery
Surgical interventions can be used to help treat the causes attributing to shoulder pain, however, it should only be considered as a last resort. A majority of patients will react positively to alternative treatment options like chiropractic care and through lifestyle modifications.�
For certain types of shoulder problems, like recurring dislocations and a few rotator cuff tears, alternative treatment options may not be recommended and surgery may be considered, in this instance.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Epigenetic: A fine interplay exists between sensory experience and innate genetic programs leading to the sculpting of neuronal circuits during early brain development. Recent evidence suggests that the dynamic regulation of gene expression through epigenetic mechanisms is at the interface between environmental stimuli and long lasting molecular, cellular and complex behavioral phenotypes acquired during periods of developmental plasticity. Understanding these mechanisms may give insight into the formation of critical periods and provide new strategies for increasing plasticity and adaptive change in adulthood.
Introduction
During early development, neuronal circuits are created and connections between neurons undergo remodeling as they develop their adult functional properties in response to the surrounding environment. The adult brain loses this extraordinary plasticity. Recent findings support a key role of epigenetic factors in mediating the effects of sensory experience on site-specific gene expression, synaptic transmission, and behavioral phenotypes. Here we review recent evidence implicating multiple epigenetic mechanisms in experience-dependent changes during development and discuss their role in critical period expression in the developing and adult brain.
Epigenetics: Molecular Mechanisms Of Gene Regulation
The term �epigenetic� refers to chromatin modifications which alter gene expression without affecting DNA sequence. The factors that contribute to the epigenetic regulation of transcriptional activity are numerous and include microRNA [1], DNA methylation [2,3] and post- translational modifications of nucleosomal histones [2,4]. DNA methylation refers to a chemical modification to DNA whereby cytosine is converted to 5-methylcytosine with the consequence of reduced accessibility of the DNA to transcription factors (Figure 1a�d). These modi- fications can be stable and heritable and provide a critical mechanism in cellular differentiation [3]. The process of methylation is dependent on the presence of methyl donors (provided by nutrients such as folic acid, meth- ionine and choline) and methyltransferases which med- iate either maintenance (i.e. DNMT1) or de novo DNA methylation (i.e. DNMT3). Transcriptional repression associated with DNA methylation is further sustained through methyl-binding proteins such as MeCP2 [5]. Epigenetic control of gene expression is also mediated through multiple post-translational modifications of histone proteins, including methylation, acetylation and ubiquination, which can alter the accessibility of DNA and the density of chromatin structure (Figure 1e,f). In particular, histone acetylation is associated with increased transcriptional activity whereas histone deacetylation is associated with transcriptional repression. The acetylation state of these nucleosomal proteins is controlled by the presence of histone acetyltransferases (HATs), histone deacetylases (HDACs), which are recruited by methyl-binding proteins, and by HDAC inhibitors, which effectively increase gene expression through shifting histones to an acetylated state [2,6]. The timing and degree of gene expression are controlled through these complex mechanisms, thus providing a link between single genotypes and multiple phenotypes.
Epigenetic Factors & The Influence Of Early Life Experiences
In mammalian development, the prenatal and postnatal periods are characterized by rapid changes in neuronal organization, thus providing a critical window of opportunity during which environmental experiences can lead to long-term influences on brain and behavior. There is increasing evidence for the role of epigenetic factors in mediating the relationship between these experiences and long-term outcomes. Mueller and Bale [7] have recently demonstrated decreased DNA methylation of the corticotrophin-releasing-factor (CRF) gene promotor and increased methylation of the glucocorticoid receptor (GR) exon 17 promotor region in hypothalamic tissue of adult male mice born to gestationally stressed females. These epigenetic modifications are associated with exposure to stress during the early stages of prenatal development and may involve dysregulation of placental gene expression. The nutritional environment during fetal development has likewise been demonstrated to influence growth, metabolism and brain development and there is increasing evidence that dietary levels of methyl-donors can epigenetically alter gene expression in offspring [8,9]. In rats, Lillycrop et al. [10] illustrate that GR 110 and PPARa (peroxisome proliferator-activated receptor alpha) gene promotor methylation is reduced in the hepatic tissue of offspring born to protein restricted dams whereas methylation is increased in offspring of dams whose diet is supplemented with methyl donors [10,11]. These effects may be related to DNMT1 expression, which is likewise decreased with dietary protein restriction [11]. Prenatal nutritional regulation of DNA methylation has similarly been observed in brain tissue associated with levels of DNMT1 expression [12], suggesting that in the rapid period of cell division ocurring during fetal development, the level of methyl donors can have a significant impact on transcriptional activity that is maintained into adulthood.
The role of epigenetic modification in sustaining the effects of environmental experience has also been demonstrated in the context of postnatal mother�infant interactions. Individual variations in maternal care during the immediate postpartum period in rats are associated with changes in offspring hypothalamic-pituitary-adrenal (HPA) activity, neuroendocrine systems involved in reproduction and hippocampal plasticity [13]. Analyses of levels of promotor methylation within the hippocampal GR 17 and hypothalamic ERa genes in offspring of rat dams that provide high vs. low levels of maternal care indicate that high levels of care are associated with decreased promotor methylation and thus increased gene expression [14,15]. Though the route through which these epigenetic changes are mediated is not yet clear, there is evidence for increased binding of nerve growth factor-inducible protein A (NGFI-A) to the GR exon 17 promoter amongst offspring who receive high levels of care in infancy [15] and in vitro models suggest that NGFI-A up-regulation is associated with histone acetylation, DNA demethylation, and activation of the exon 17 GR promoter [16]. The relevance of these effects in humans has recently been demonstrated by Oberlander et al. [17] in the analysis of methylation status of the GR promotor at NGFI-A binding sites in cord blood mononuclear cells of infants exposed to third trimester maternal depressed or anxious mood. Maternal depression was found to be associated with increased GR 1F promotor methylation in fetal blood samples and these methylation patterns predicted HPA reactivity in infants at 3 months of age [17]. Analysis of hippocampal tissue from suicide victims with a history of childhood abuse similarly indicates lower GR expression and higher GR 1F promotor methylation associated with disruptions of the early environment and confirms the findings from rodent studies that differential NGFI-A binding is a functional consequence of these epigenetic effects [18]. However, the impact of perinatal mother� infant interactions is not limited to GR regulation as illustrated by Roth et al. [19] examining the effects of postnatal abuse on offspring brain derived neurotrophic factor (BDNF) methylation [19]. In rats, an increase in methylation of exon IV of the BDNF promotor and consequent decrease in BDNF mRNA in the prefrontal cortex was found in association with exposure to periods of abusive maternal care (dragging, rough handling, etc.). As was the case with the effects of individual differences in maternal care, these effects emerged in infancy and were sustained into adulthood. Moreover, these effects on BDNF exon IV methylation are perpetuated to the F1 generation suggesting a role for epigenetic mechanisms in transgenerational effects [20].
Development Across The Lifespan: Epigenetics & Experience Dependent Plasticity
The previous section highlights the stable effects of early life experiences and how these events become encoded at a molecular level. Another approach to the study of epigenetics and development comes from studies of synaptic plasticity during the expression of long-term potentiation (LTP) and memory consolidation. High levels of maternal care and exposure to juvenile environ- mental enrichment (EE) have been demonstrated to improve capacity for learning and memory associated with LTP enhancement [21,22]. Moreover, recent evidence suggests that EE modulates NMDAr/p38/LTP signaling pathways in the hippocampus and improves contextual fear memory formation across generations such that offspring of enriched mothers likewise show enhanced LTP even when cross-fostered at birth to non- enriched mothers [23]. Environmental enrichment has been associated with increased histone acetylation in the hippocampus and improved spatial memory [24,25]. Pharmacological targeting of the epigenome has been used to demonstrate the role of histone acetylation and DNA methylation in the consolidation of long-term memory [26]. Treatment with zebularine (an inhibitor or DNA methyltransferases) has been shown to block memory formation and reduce histone acetylation following con- textual fear conditioning in adult rats [27] whereas treatment with the HDAC inhibitor sodium butyrate lead to enhanced formation of contextual fear memories [28]. The particular HDAC target of these inhibitors may be HDAC2 as recent evidence has emerged illustrating decreased synaptic plasticity and memory formation in mice over-expressing HDAC2 but not HDAC1; with the converse effect in HDAC2-deficient mice [29]. These studies illustrate a possible relationship between synaptic activity and histone acetylation/DNA methylation in mature neurons, suggesting that there is continued plasticity in these epigenetic systems beyond the prenatal and postnatal periods of development.
Epigenetic Mechanism & The Regulation Of Synaptic Transmission
Activity-dependent changes in gene expression within neuronal pathways during development may serve as a critical pathway linking experience of the external environment and epigenetic modifications within the cell nucleus. In a recent study, Monteggia and colleagues elegantly demonstrated that spontaneous synaptic trans- mission in hippocampal neurons is regulated by alterations in DNA methylation that occur in response to synaptic activity [30]. Treatment with a DNMT inhibitor lead to a significant decrease in frequency of miniature excitatory post-synaptic currents (mEPSCs) and rate of spontaneous synaptic vesicle fusion correlated with a decrease in BDNF promoter I methylation and increased BDNF expression. This effect was blocked with inhibition of synaptic activity and reductions in mEPSCs were prevented in the absence of MeCP2. These results strongly suggest a role for DNA methylation/MeCP2 pathways in the control of synaptic function. Activity- dependent phosphorylation of MeCP2 via Ca2+-calmodulindependent kinase II has been shown to cause MeCP2 dissociation from target genes and relieve transcriptional repression [31]. Consequently, genes such as BDNF are increased in expression leading to normal dendritic patterning and dendritic spine development [32]. These findings suggest an epigenetic mechanism through which neurons can monitor alterations in activity level and adjust neurotransmitter output via altered gene expression with consequences for network excitability and circuit refinement. Impairments in these MeCP2 pathways may lead to several neurodevelopmental abnormalities including Rett syndrome, infantile autism, mental retardation, and schizophrenia [33] and targeted deletion of MeCP2 in the amygdala has recently been demonstrated to impair learning and memory and lead to increased anxiety-like behavior in mice [34].
Epigenetic Control Of Critical Period Plasticity
Though epigenetic mechanisms have certainly been implicated in mediating the high levels of plasticity in early development, it is also possible to view the decreased plasticity and sensitivity that occurs later in development from an epigenetic perspective. Neocortical circuits are extremely sensitive to manipulations of the sensory environment during restricted temporal windows of postnatal development called �critical periods�. For example, an imbalance in binocular vision during child- hood affects perception leading to amblyopia or �lazy eye�. Monocular deprivation (MD) reproduces this classical paradigm of experience-dependent plasticity [35]. The striking physiological effect of MD is a shift in visual cortical neuron response in favor of the non-deprived eye; an example of ocular dominance (OD) plasticity. The critical period during which this OD plasticity occurs is defined by the activation and subsequent inhibition of specific molecular pathways involving signaling molecules such as aCaMKII, calcineurin, PKA, ERK, and CREB [36]. Recently, Pizzorusso and colleagues identified rapid increases in ERK-dependent phosphorylation of histones associated with activation of the juvenile visual cortex and a developmental downregulation of this effect in older mice [37]. In adult mice, the reduced OD plasticity can be reinstated through treatment with the HDAC inhibitor trichostatin A (TSA). Multiple cellular mechanisms might contribute to experience-dependent plasticity expression [38]. Further work is necessary to understand if epigenetic mechanisms are generally acting in all cellular substrates or only within a specific subset.
Myelin maturation has also been proposed as one of the major factors contributing to decreased neuronal plasticity. During the onset of critical period plasticity, oligodendrocytes start to express specific myelin structural proteins, including myelin basic protein (MBP), myelin-associated glycoprotein (MAG), myelin oligodendrocyte glycoprotein (OMgp) and myelin-associated oligodendrocyte basic protein (MOBP) [39]. As myelination reaches adult levels, OD plasticity is strongly reduced or absent. MAG and OMgp may contribute to critical period closure through activation of Nogo receptors. Indeed, mice lacking Nogo receptors exhibit OD plasticity even in adulthood [40]. Manipulation of epigenetic status of oligodendrocytes may also be an effective strategy for modulating plasticity. Casaccia-Bonnefil and colleagues have shown that histone modifications are involved in oligodendrocyte precursor cell (OPC) differentiation during development and in recovery from injury [41� 43]. Administration of the HDAC inhibitor valproic acid during the critical period of myelination onset was found to prevent the OPC maturation into myelinating cells. These results suggest that HDAC activity during a specific temporal window of postnatal development is required for OPC differentiation and myelination. At later developmental stages, histone deacetylation subsides and is replaced by repressive histone methylation and the establishment of a compact chromatin structure, characteristic of the differentiated oligodendrocyte phenotype [43]. Shen et al. [44] found that in response to damage of oligodendrocytes, robust remyelination occurred in juvenile but not in older animals with the new myelin synthesis preceded by down regulation of oligodendrocyte differentiation inhibitors and neural stem cell markers and the recruitment of HDACs to promoter regions. This HDAC recruitment is inefficient in older brains, allowing for the accumulation of transcriptional inhibitors and prevention of myelin gene expression. This age-depend- ent effect can be induced in young mice treated with HDAC inhibitors during the period when damage to oligodentrocytes is occurring. Thus, there are epigenetic changes that are characteristic of periods of developmental plasticity that could provide a target for therapeutic intervention in the event of CNS damage. The use of HDAC inhibitors to increase plasticity in the brain may be a promising therapeutic approach as there is conver- ging evidence from rodent models that treatment with these compounds (1) can lead to dramatic shifts in gene expression and behavior in adult offspring who have received low levels of maternal care [15] and (2) mimic the effects of EE on reversal of neurodevelopmental abnormalities [24]. Rather than producing a generalized increase in transcription, these compounds lead to acti- vation of a specific subset of genes [45�47], suggesting possible targeted intervention to reinstate plasticity in adult brain.
Conclusions
There is converging evidence for the role of epigenetic modifications such as histone acetylation and DNA meth- ylation in both the stability and plasticity of developing neuronal circuits. The persistent effects on gene expression that can be achieved through these mechanisms provide a biological route through which environmental experiences can become embedded, leading to long-term changes in neurobiology and behavior. Enhancing plasticity in the adult brain is an exciting prospect and there is certainly evidence emerging that suggest the possible use of epigenetic factors to induce a �younger� brain. The challenge of future studies is to establish the pathways through which site-specific and gene-specific transcriptional modifications can be achieved and to better understand the route through which experiences across the lifespan induce this molecular plasticity.
Michela Fagiolini 1, Catherine L Jensen 2 and Frances A Champagne 2
Current Opinion in Neurobiology 2009, 19:1�6
This review comes from a themed issue on Development
Edited by Takao Hensch and Andrea Brand
0959-4388/$ � see front matter Published by Elsevier Ltd.
DOI 10.1016/j.conb.2009.05.009
4. Fukuda S, Taga T: Cell fate determination regulated by a
transcriptional signal network in the developing mouse brain.
Anat Sci Int 2005, 80:12-18.
5. Fan G, Hutnick L: Methyl-CpG binding proteins in the nervous
system. Cell Res 2005, 15:255-261.
6. Strathdee G, Brown R: Aberrant DNA methylation in cancer:
potential clinical interventions. Expert Rev Mol Med 2002,
2002:1-17.
7. Mueller BR, Bale TL: Sex-specific programming of offspring
emotionality after stress early in pregnancy. J Neurosci 2008,
28:9055-9065.
Rodent study illustrating alterations in DNA methylation of placental and
brain tissue following exposure to gestational stress, providing a possible
mechanism mediating the long-term neurobiological effects of prenatal
exposure to elevated maternal HPA activity
8. Hoet JJ, Hanson MA: Intrauterine nutrition: its importance
during critical periods for cardiovascular and endocrine
development. J Physiol 1999, 514(Pt 3):617-627.
9. Zeisel SH: Importance of methyl donors during reproduction.
Am J Clin Nutr 2009, 89:673S-677S.
10. Lillycrop KA, Phillips ES, Torrens C, Hanson MA, Jackson AA,
Burdge GC: Feeding pregnant rats a protein-restricted diet
persistently alters the methylation of specific cytosines in the
hepatic PPAR alpha promoter of the offspring. Br J Nutr 2008,
100:278-282.
11. Lillycrop KA, Slater-Jefferies JL, Hanson MA, Godfrey KM,
Jackson AA, Burdge GC: Induction of altered epigenetic
regulation of the hepatic glucocorticoid receptor in the
offspring of rats fed a protein-restricted diet during pregnancy
suggests that reduced DNA methyltransferase-1 expression is
involved in impaired DNA methylation and changes in histone
modifications. Br J Nutr 2007, 97:1064-1073.
Illustrates the impact of methyl donors in the maternal diet on offspring
DNA methylation and histone acetylation patterns, providing an important
link between nutrition and gene regulation
12. Kovacheva VP, Mellott TJ, Davison JM, Wagner N, LopezCoviella
I, Schnitzler AC, Blusztajn JK: Gestational choline
deficiency causes global- and Igf2 gene- DNA
hypermethylation by upregulation of Dnmt1 expression. J Biol
Chem 2007, 282:31777-31788.
13. Meaney MJ: Maternal care, gene expression, and the
transmission of individual differences in stress reactivity
across generations. Annu Rev Neurosci 2001, 24:1161-1192.
14. Champagne FA, Weaver IC, Diorio J, Dymov S, Szyf M,
Meaney MJ: Maternal care associated with methylation of the
estrogen receptor-alpha1b promoter and estrogen receptoralpha
expression in the medial preoptic area of female
offspring. Endocrinology 2006, 147:2909-2915.
15. Weaver IC, Cervoni N, Champagne FA, D�Alessio AC, Sharma S,
Seckl JR, Dymov S, Szyf M, Meaney MJ: Epigenetic programming
by maternal behavior. Nat Neurosci 2004, 7:847-854.
16. Weaver IC, D�Alessio AC, Brown SE, Hellstrom IC, Dymov S,
Sharma S, Szyf M, Meaney MJ: The transcription factor nerve
growth factor-inducible protein a mediates epigenetic
programming: altering epigenetic marks by immediate-early
genes. J Neurosci 2007, 27:1756-1768.
17. Oberlander TF, Weinberg J, Papsdorf M, Grunau R, Misri S,
Devlin AM: Prenatal exposure to maternal depression,
neonatal methylation of human glucocorticoid receptor gene
(NR3C1) and infant cortisol stress responses. Epigenetics
2008, 3:97-106.
Provides evidence for the relevance of epigenetic mechanisms in mediating
the effects of maternal mood on infant development. Illustrates the
translation of experimental approaches conducted in animal models to
the study of clinically relevant issues in humans
18. McGowan PO, Sasaki A, D�Alessio AC, Dymov S, Labonte B,
Szyf M, Turecki G, Meaney MJ: Epigenetic regulation of the
glucocorticoid receptor in human brain associates with
childhood abuse. Nat Neurosci 2009, 12:342-348.
Provides compelling evidence for the presence of differential methylation
of GR with consequences for gene expression in the human hippocampus
as a function of early childhood abuse using brain tissue obtained
from suicide victims
19. Roth TL, Lubin FD, Funk AJ, Sweatt JD: Lasting epigenetic
influence of early-life adversity on the BDNF gene. Biol
Psychiatry 2009, 65:760-769.
Rodent study of the transgenerational impact of exposure to maternal
abuse in infancy and the role of differential methylation of BDNF in the
prefrontal cortex in mediating these effects
20. Champagne FA: Epigenetic mechanisms and the
transgenerational effects of maternal care. Front
Neuroendocrinol 2008, 29:386-397.
21. Bruel-Jungerman E, Laroche S, Rampon C: New neurons in the
dentate gyrus are involved in the expression of enhanced
long-term memory following environmental enrichment.
Eur J Neurosci 2005, 21:513-521.
22. Champagne DL, Bagot RC, van Hasselt F, Ramakers G,
Meaney MJ, de Kloet ER, Joels M, Krugers H: Maternal care and
hippocampal plasticity: evidence for experience-dependent
structural plasticity, altered synaptic functioning, and
differential responsiveness to glucocorticoids and stress.
J Neurosci 2008, 28:6037-6045.
23. Arai JA, Li S, Hartley DM, Feig LA: Transgenerational rescue of a
genetic defect in long-term potentiation and memory
formation by juvenile enrichment. J Neurosci 2009, 29:1496-
1502.
Rodent study illustrating the transgenerational impact of environmental
enrichment on LTP suggesting that genetically induced deficits can be
overcome through environmental conditions experienced by a previous
generation
24. Fischer A, Sananbenesi F, Wang X, Dobbin M, Tsai LH: Recovery
of learning and memory is associated with chromatin
remodelling. Nature 2007, 447:178-182.
Rodent study showing that environmental enrichment increases histone
acetylation in the hippocampus. HDAC inhibitors induce increased spatial
memory in a neurodegenerative disorder mouse model
25. Williams BM, Luo Y, Ward C, Redd K, Gibson R, Kuczaj SA,
McCoy JG: Environmental enrichment: effects on spatial
memory and hippocampal CREB immunoreactivity. Physiol
Behav 2001, 73:649-658.
26. Sweatt JD: Experience-dependent epigenetic modifications in
the central nervous system. Biol Psychiatry 2009, 65:191-197.
27. Lubin FD, Roth TL, Sweatt JD: Epigenetic regulation of BDNF
gene transcription in the consolidation of fear memory.
J Neurosci 2008, 28:10576-10586.
Recent paper from a series of investigations by the Sweatt lab illustrating
the dynamic changes to DNA methylation which occur during the process
of learning and the critical role of these modifications in the consolidation
of memory
28. Levenson JM, Roth TL, Lubin FD, Miller CA, Huang IC, Desai P,
Malone LM, Sweatt JD: Evidence that DNA (cytosine-5)
methyltransferase regulates synaptic plasticity in the
hippocampus. J Biol Chem 2006, 281:15763-15773.
29. Guan JS, Haggarty SJ, Giacometti E, Dannenberg JH, Joseph N,
Gao J, Nieland TJ, Zhou Y, Wang X, Mazitschek R et al.: HDAC2
negatively regulates memory formation and synaptic
plasticity. Nature 2009, 459:55-60.
Study in mice examining the particular HDAC target through which HDAC
inhibitors exert enhancements in synaptic plasticity and memory. Using
targeted up- and downregulation of HDAC2 the authors illustrate the
importance of levels of this enzyme in mediating cognitive enhancement
30. Nelson ED, Kavalali ET, Monteggia LM: Activity-dependent
suppression of miniature neurotransmission through the
regulation of DNA methylation. J Neurosci 2008, 28:395-406.
This paper focuses on the regulation of DNA methylation by NMDA
receptor-mediated synaptic activity within mature neurons and how
epigenetic alterations affect basal synaptic function. These findings
suggest a synaptic basis for neurological symptoms associated with
neurodevelopmental disorders such as Rett syndrome
31. Chen WG, Chang Q, Lin Y, Meissner A, West AE, Griffith EC,
Jaenisch R, Greenberg ME: Derepression of BDNF transcription
involves calcium-dependent phosphorylation of MeCP2.
Science 2003, 302:885-889.
32. Zhou Z, Hong EJ, Cohen S, Zhao WN, Ho HY, Schmidt L,
Chen WG, Lin Y, Savner E, Griffith EC et al.: Brain-specific
phosphorylation of MeCP2 regulates activity-dependent Bdnf
transcription, dendritic growth, and spine maturation. Neuron
2006, 52:255-269.
33. Moretti P, Zoghbi HY: MeCP2 dysfunction in Rett syndrome and
related disorders. Curr Opin Genet Dev 2006, 16:276-281.
34. Adachi M, Autry AE, Covington HE 3rd, Monteggia LM: MeCP2-
mediated transcription repression in the basolateral amygdala
may underlie heightened anxiety in a mouse model of Rett
syndrome. J Neurosci 2009, 29:4218-4227.
35. Tropea D, Van Wart A, Sur M: Molecular mechanisms of
experience-dependent plasticity in visual cortex. Philos Trans
R Soc Lond B Biol Sci 2009, 364:341-355.
36. Medini P, Pizzorusso T: Visual experience and plasticity of the
visual cortex: a role for epigenetic mechanisms. Front Biosci
2008, 13:3000-3007.
37. Putignano E, Lonetti G, Cancedda L, Ratto G, Costa M, Maffei L,
Pizzorusso T: Developmental downregulation of histone
posttranslational modifications regulates visual cortical
plasticity. Neuron 2007, 53:747-759.
The authors identify ERK/MAPK-dependent regulation of histone modifications
as a new mechanism underlying the expression of ocular
dominance plasticity
38. Hensch TK: Critical period mechanisms in developing visual
cortex. Curr Top Dev Biol 2005, 69:215-237.
39. Quarles RH: Myelin sheaths: glycoproteins involved in their
formation, maintenance and degeneration. Cell Mol Life Sci
2002, 59:1851-1871.
40. McGee AW, Yang Y, Fischer QS, Daw NW, Strittmatter SM:
Experience-driven plasticity of visual cortex limited by myelin
and Nogo receptor. Science 2005, 309:2222-2226.
41. He Y, Dupree J, Wang J, Sandoval J, Li J, Liu H, Shi Y, Nave KA,
Casaccia-Bonnefil P: The transcription factor Yin Yang 1 is
essential for oligodendrocyte progenitor differentiation.
Neuron 2007, 55:217-230.
42. Shen S, Casaccia-Bonnefil P: Post-translational modifications
of nucleosomal histones in oligodendrocyte lineage
cells in development and disease. J Mol Neurosci 2008,
35:13-22.
43. Shen S, Li J, Casaccia-Bonnefil P: Histone modifications
affect timing of oligodendrocyte progenitor differentiation
in the developing rat brain. J Cell Biol 2005, 169:
577-589.
44. Shen S, Sandoval J, Swiss VA, Li J, Dupree J, Franklin RJ,
Casaccia-Bonnefil P: Age-dependent epigenetic control of
differentiation inhibitors is critical for remyelination efficiency.
Nat Neurosci 2008, 11:1024-1034.
This paper provides mechanistic insight into how oligodendrocytes precursors
cell differentiation is epigenetically regulated during remyelination
and how these mechanisms change with aging.
45. Fass DM, Butler JE, Goodman RH: Deacetylase activity is
required for cAMP activation of a subset of CREB target
genes. J Biol Chem 2003, 278:43014-43019.
46. Vecsey CG, Hawk JD, Lattal KM, Stein JM, Fabian SA, Attner MA,
Cabrera SM, McDonough CB, Brindle PK, Abel T et al.: Histone
deacetylase inhibitors enhance memory and synaptic
plasticity via CREB:CBP-dependent transcriptional activation.
J Neurosci 2007, 27:6128-6140.
47. Weaver IC, Meaney MJ, Szyf M: Maternal care effects on the
hippocampal transcriptome and anxiety-mediated behaviors
in the offspring that are reversible in adulthood. Proc Natl Acad
Sci U S A 2006, 103:3480-3485.
[/accordion]
[/accordions]
Low back pain represents one of the most common complaints in healthcare settings. While various injuries and conditions associated with the musculoskeletal and nervous system can cause low back pain, many healthcare professionals believe that work injury may have a prevalent connection to low back pain. For instance, improper posture and repetitive movements may often cause work-related injuries. In other cases, environmental accidents at work may cause work injuries. In any case, diagnosing the source of a patient’s low back pain to correctly determine which would be the best treatment method to restore the individual’s original health and wellness is generally challenging.
First and foremost, getting the right doctors for your specific source of low back pain is essential for finding relief from your symptoms. Many healthcare professionals are qualified and experienced in treating work-related low back pain, including doctors of chiropractic or chiropractors. As a result, several work injury treatment guidelines have been established to manage low back pain in healthcare settings. Chiropractic care focuses on diagnosing, treating, and preventing various injuries and conditions, such as LBP, associated with the musculoskeletal and nervous system. By carefully correcting the misalignment of the spine, chiropractic care can help improve symptoms of low back pain, among other symptoms. The purpose of the following article is to discuss occupational health guidelines for the management of low back pain.
Occupational Health Guidelines for the Management of Low Back Pain: an International Comparison
Abstract
Background: The enormous socioeconomic burden of low back pain emphasizes the need to manage this problem, especially in an occupational context effectively. To address this, occupational guidelines have been issued in various countries.
Aims: To compare available international guidelines for managing low back pain in an occupational health care setting.
Methods: The guidelines were compared regarding generally accepted quality criteria using the AGREE instrument and also summarised regarding the guideline committee, the presentation, the target group, and assessment and management recommendations (that is, advice, return to work strategy, and treatment).
Results and Conclusions: The results show that the guidelines variously met the quality criteria. Common flaws concerned the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the extent to which editors and developers were independent. There was general agreement on numerous issues fundamental to occupational health management of back pain. The assessment recommendations included diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery. The guidelines also agreed on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Dr. Alex Jimenez’s Insight
Low back pain is one of the most prevalent health issues treated in chiropractic offices. Although the following article describes low back pain as a self limiting condition, the cause of an individual’s LBP can also trigger debilitating and severe pain and discomfort of left untreated. It’s important for an individual with symptoms of low back pain to seek proper treatment with a chiropractor to properly diagnose and treat their health issues as well as prevent them from returning in the future. Patients who experience low back pain for more than 3 months are less than 3 percent likely to return to work. Chiropractic care is a safe and effective alternative treatment option which can help restore the original function of the spine. Furthermore, a doctor of chiropractic, or chiropractor, can provide lifestyle modifications, such as nutritional and fitness advice, to speed up the patient’s recovery process. Healing through movement is essential for LBP recovery.
Low back pain (LBP) is one of the industrial countries’ most common health problems. Despite its benign nature and sound course, LBP is commonly associated with incapacity, productivity loss due to sick leave, and high societal costs.[1]
Because of that impact, there is an obvious need for effective management strategies based on scientific evidence derived from studies of sound methodological quality. Usually, these are randomized controlled trials (RCTs) on the effectiveness of therapeutic interventions, diagnostic studies, or prospective observational studies on risk factors or side effects. The scientific evidence, summarised in systematic reviews and meta-analyses, provides a solid basis for guidelines on managing LBP. In a previous paper, Koes et al. compared various existing clinical guidelines for managing LBP targeted at primary healthcare professionals, showing a considerable commonality.[2]
The problems in occupational health care are different. Management focuses mainly on counseling the worker with LBP and addressing the issues of assisting them to continue working or return to work (RTW) after sick listing. However, LBP is also an important issue in occupational health care because of the associated incapacity for work, productivity loss, and sick leave. Several guidelines, or sections of guidelines, have now been published dealing with the specific issues of management in an occupational health care setting. Since the evidence is international, it would be expected that the recommendations of different occupational guidelines for LBP would be more or less similar. However, it is not clear whether the guidelines meet currently accepted quality criteria.
This paper critically appraises available occupational guidelines on managing LBP and compares their assessment and management recommendations.
Main Messages
In various countries, occupational health guidelines are issued to improve the management of low back pain in an occupational context.
Common flaws of these guidelines concern the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the independence of editors and developers.
In general, the assessment recommendations in the guidelines consisted of diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery.
There is general agreement on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Methods
Guidelines on the occupational health management of LBP were retrieved from the authors’ personal files. Retrieval was checked by a Medline search using the keywords low back pain, guidelines, and occupational up to October 2001, and personal communication with experts in the field. Policies had to meet the following inclusion criteria:
Guidelines aimed at managing workers with LBP (in occupational health care settings or addressing occupational issues) or separate sections of policies that dealt with these topics.
Guidelines are available in English or Dutch (or translated into these languages).
The exclusion criteria were:
Guidelines on primary prevention (that is, prevention before the onset of the symptoms) of work-related LBP (for example, lifting instructions for workers).
Clinical guidelines for the management of LBP in primary care.[2]
The quality of the included guidelines was appraised using the AGREE instrument, a generic tool designed primarily to help guideline developers and users assess the methodological quality of clinical practice guidelines.[3]
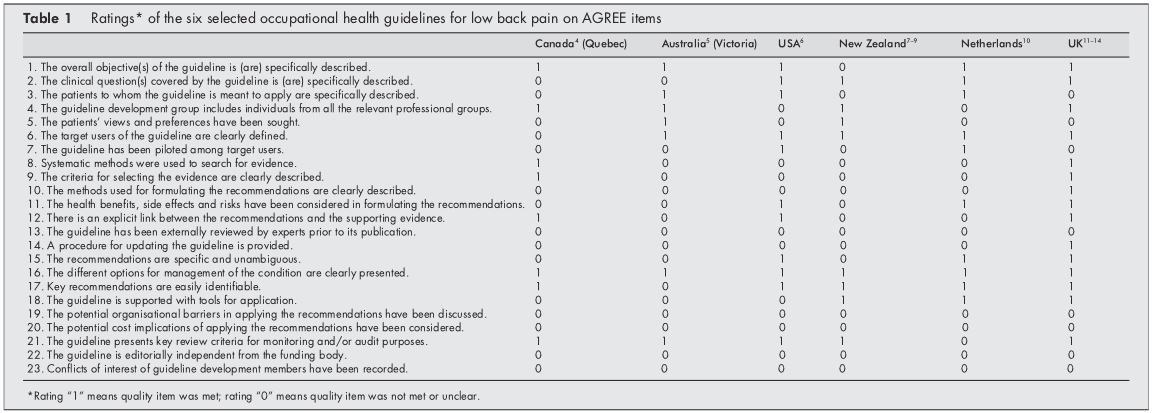
The AGREE instrument provides a framework for assessing the quality on 24 items (table 1), each rated on a four-point scale. The full operationalization is available on www.agreecollaboration.org.
Two reviewers (BS and HH) independently rated the quality of the guidelines and then met to discuss disagreements and to reach a consensus on the ratings. When they could not agree, a third reviewer (MvT) reconciled the remaining differences and decided on the ratings. To facilitate analysis in this review, ratings were transformed into dichotomous variables of whether each quality item was or was not met.
The assessment recommendations were summarised and compared to recommendations on advice, treatment, and return to work strategies. The selected guidelines were further characterized and reached regarding the guideline committee, the presentation of the procedure, the target group, and the extent to which the recommendations were based on available scientific evidence. All of this information was extracted directly from the published guidelines.
Policy Implications
The management of low back pain in occupational health care should follow evidence-based guidelines.
Future occupational guidelines for managing low back pain and updates of those guidelines should consider the criteria for proper development, implementation, and evaluation of approaches as suggested by the AGREE collaboration.
Results
Selection of Studies
Our search found ten guidelines, but four were excluded because they dealt with the management of LBP in primary care,[15] were aimed at the guidance of sick-listed employees in general (not specifically LBP),[16] were intended for the primary prevention of LBP at work,[17] or were not available in English or Dutch.[18] The final selection, therefore, consisted of the following six guidelines, listed by date of issue:
(1) Canada (Quebec). A scientific approach to the assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Quebec Canada (1987).[4]
(2) Australia (Victoria). Guidelines for the management of employees with compensable low back pain. Victorian WorkCover Authority, Australia (1996).[5] (This is a revised version of guidelines developed by the South Australian WorkCover Corporation in October 1993.)
(3) the USA. Occupational Medicine Practice Guidelines. American College of Occupational and Environmental Medicine. USA (1997).[6]
(4) New Zealand
(a)Active and working! Managing acute low back pain in the workplace. Accident Compensation Corporation and National Health Committee. New Zealand (2000).[7]
(b)Patient guide to acute low back pain management. Accident Compensation Corporation and National Health Committee. New Zealand (1998).[8]
(c) Assess psychosocial yellow flags in acute low back pain. Accident Compensation Corporation and National Health Committee. New Zealand (1997).[9]
(5) the Netherlands. Dutch guideline for managing occupational physicians of employees with low back pain. Dutch Association of Occupational Medicine (NVAB). Netherlands (1999).[10]
(6) the UK
(a)Occupational health guidelines for managing low back pain at work principal recommendations. Faculty of Occupational Medicine. UK (2000).[11]
(b)Occupational health guidelines for managing low back pain at work leaflet for practitioners. Faculty of Occupational Medicine. UK (2000).[12]
(c)Occupational health guidelines for managing low back pain at work evidence review. Faculty of Occupational Medicine. UK (2000).[13]
(d)The Back Book, The Stationery Office. UK (1996).[14]
Two guidelines (4 and 6) could not be evaluated independently from additional documents to which they refer (4bc, 6bd), so these documents were also included in the review.
Appraisal of the Quality of the Guidelines
Initially, there was an agreement between the two reviewers regarding 106 (77%) of the 138 item ratings. After two meetings, the consensus was reached for all but four items, which required adjudication by the third reviewer. Table 1 presents the final ratings.
All included guidelines presented the different options for managing LBP in occupational health. In five of the six policies, the overall objectives of the procedure were explicitly described,[46, 1014] the target users of the system were clearly defined,[514] easily identifiable key recommendations were included,[4, 614] or critical review criteria were presented for monitoring and audit purposes.[49, 1114]
The results of the AGREE appraisal showed that none of the guidelines paid sufficient attention to potential organizational barriers and cost implications in implementing the recommendations. It was also unclear for all included guidelines whether or not they were editorially independent of the funding body and whether or not there were conflicts of interest for the members of the guideline development committees. Furthermore, it was unclear for all guidelines whether experts had externally reviewed the policies before publication. Only the UK guideline clearly described the method used to formulate the recommendations and provided for updating the approach.[11]
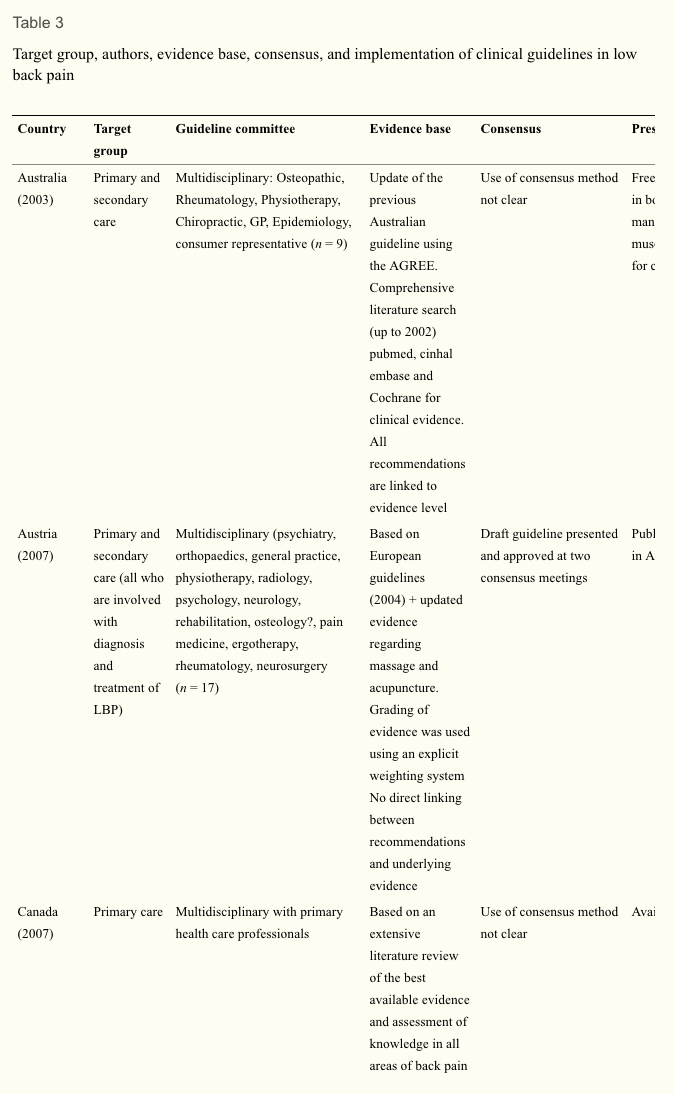
Development of the Guidelines
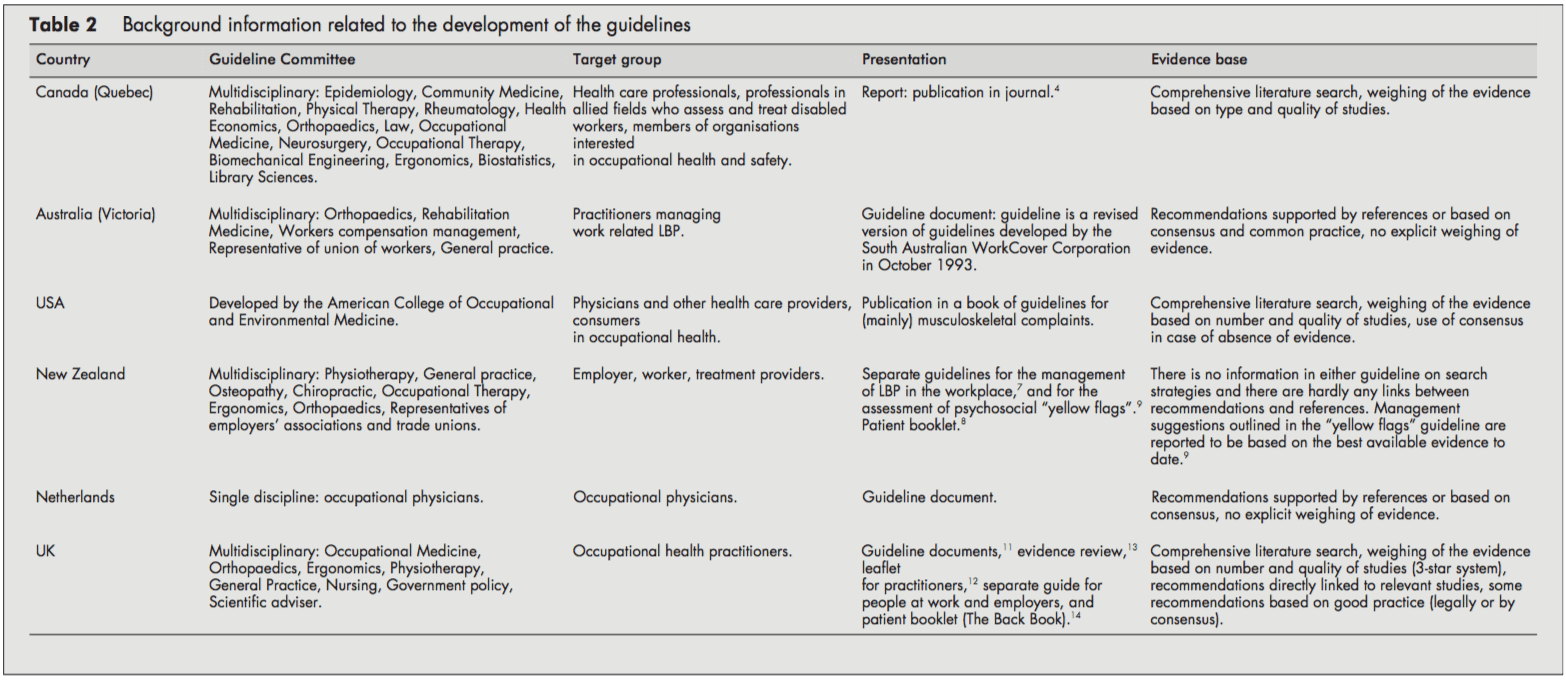
Table 2 presents background information on the development process of the guidelines.
The target users for the guidelines were physicians and other healthcare providers in the field of occupational healthcare. Several policies were also directed at informing employers, workers [68, 11, 14], or members of organizations interested in occupational health.[4] The Dutch guideline was only targeted at the occupational health physician.[10]
The guideline committees responsible for developing the guidelines were generally multidisciplinary, including disciplines like epidemiology, ergonomics, physiotherapy, general practice, occupational medicine, occupational therapy, orthopedics, and representatives of employers’ associations and trade unions. Chiropractic and osteopathic representatives were in the guideline committee of the New Zealand guidelines.[79] The Quebec task force (Canada) also included representatives of rehabilitation medicine, rheumatology, health economics, law, neurosurgery, biomechanical engineering, and library sciences. In contrast, the guideline committee of the Dutch guideline consisted only of occupational physicians.[10]
The guidelines were issued as a separate document,[4, 5, 10] as a chapter in a textbook,[6] or as several interrelated documents.[79, 1114]
The UK,[13] the USA,[6] and Canadian[4] guidelines provided information on the search strategy applied to the identification of relevant literature and the weighing of the evidence. On the other hand, the Dutch[10] and the Australian[5] guidelines supported their recommendations only by references. The New Zealand guidelines showed no direct links between suggestions and concerns [79]. The reader was referred to other literature for background information.
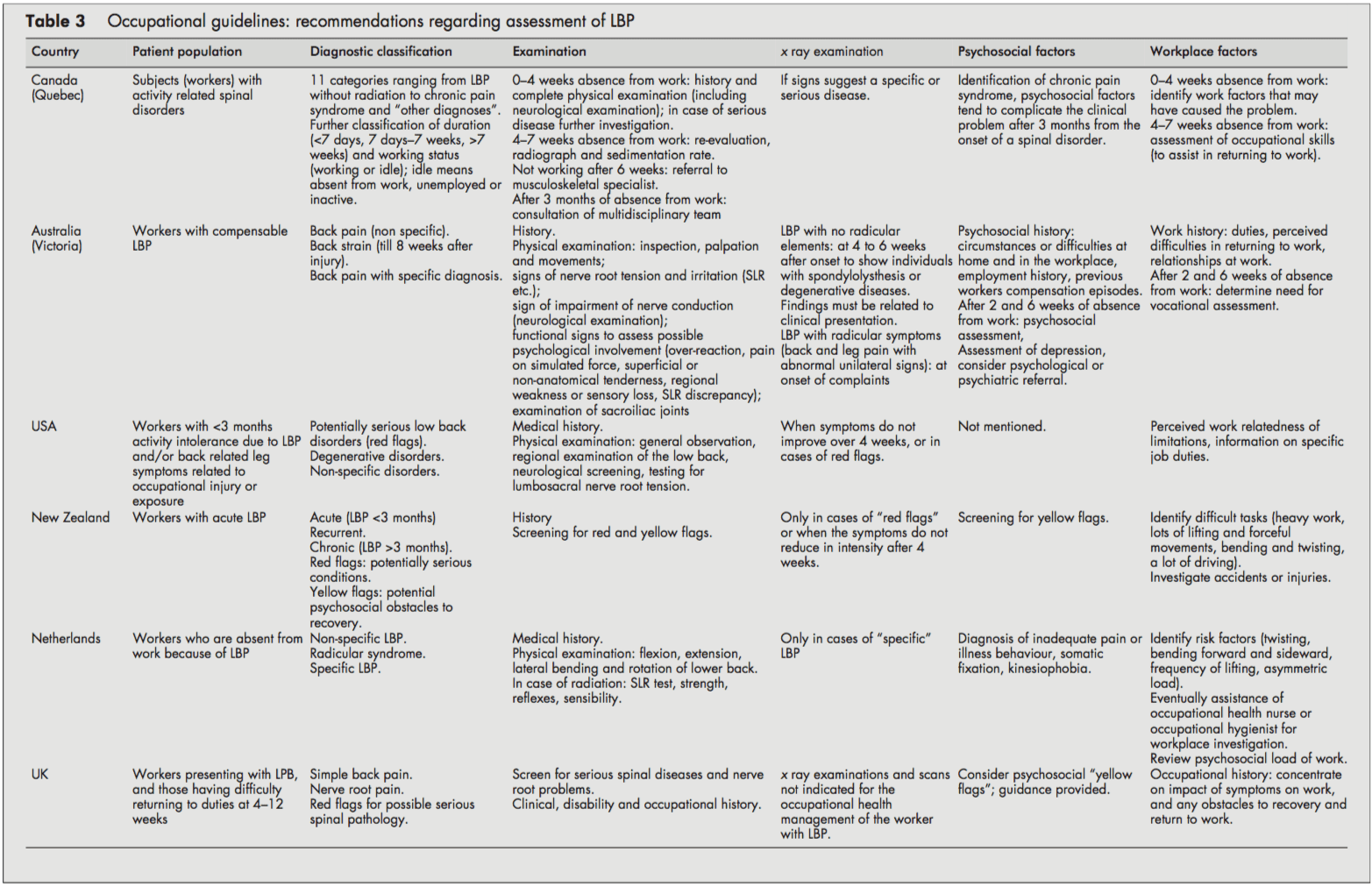
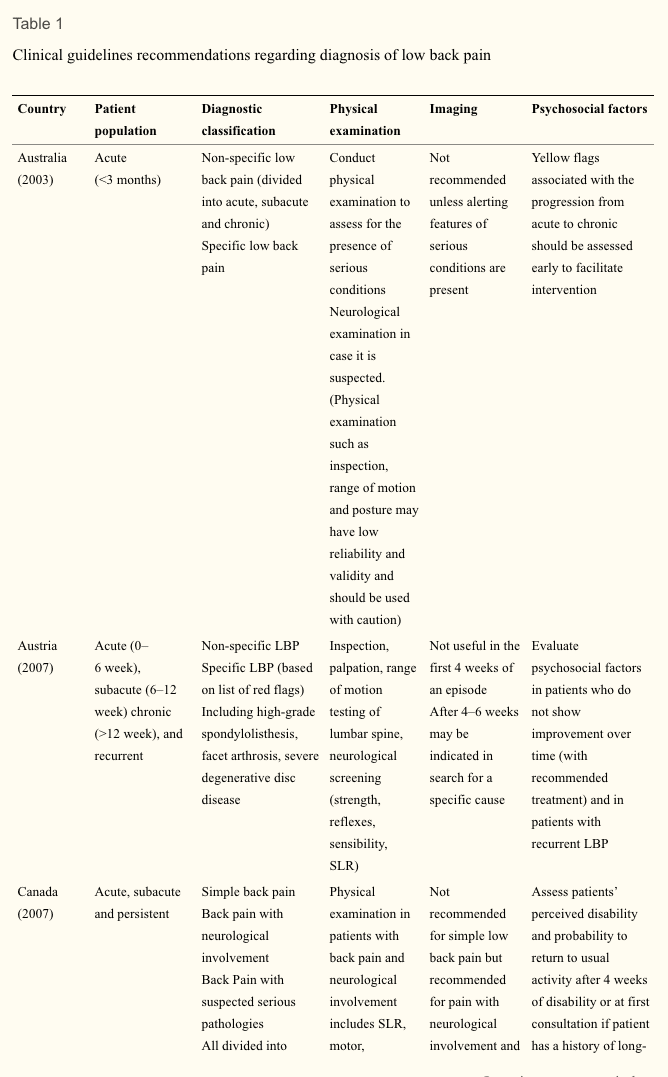
Patient Population and Diagnostic Recommendations
Although all guidelines focused on workers with LBP, it was often unclear whether they dealt with acute or chronic LBP or both. Acute and chronic LBP were often not defined, and cut-off points were given (for example, <3 months). It was usually unclear whether these referred to the onset of symptoms or absence from work. However, the Canadian guideline introduced a classification system (acute/subacute/ chronic) based on the distribution of claims of spinal disorders by time since absence from work.[4]
All guidelines distinguished specific and non-specific LBP. Specific LBP concerns the potentially serious red flag conditions like fractures, tumors, or infections, and the Dutch and UK guidelines also distinguish the radicular syndrome or nerve root pain.[1013] All procedures were consistent in their recommendations to take a clinical history and to carry out a physical examination, including neurological screening. In cases of suspected specific pathology (red flags), x-ray examinations were recommended by most guidelines. In addition, New Zealand and the US guideline also recommended an x-ray examination when symptoms did not improve after four weeks.[6, 9] The UK guideline stated that x-ray examinations are not indicated and do not assist occupational health management of the patient with LBP (distinct from any clinical indications).[1113]
Most guidelines considered psychosocial factors as yellow flags as obstacles to recovery that healthcare providers should address. The New Zealand[9] and UK guidelines [11, 12] explicitly listed factors and suggested questions to identify those psychosocial yellow flags.
All guidelines addressed the importance of the clinical history identifying physical and psychosocial workplace factors relevant to LBP, including physical demands of work (manual handling, lifting, bending, twisting, and exposure to whole-body vibration), accidents or injuries, and perceived difficulties in returning to work or relationships at work. The Dutch and the Canadian guidelines contained recommendations to carry out a workplace investigation[10] or an assessment of occupational skills when necessary.[4]
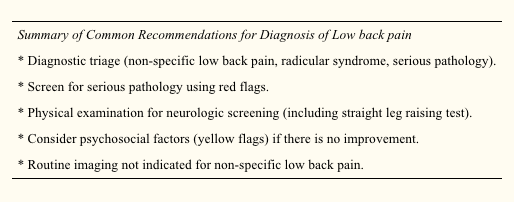
Summary of Recommendations for the Assessment of LBP
Diagnostic triage (non-specific LBP, radicular syndrome, specific LBP).
Exclude red flags and neurological screening.
Identify psychosocial factors and potential obstacles to recovery.
Identify workplace factors (physical and psychosocial) that may be related to the LBP problem and return to work.
X-Ray examinations are restricted to suspected cases of specific pathology.
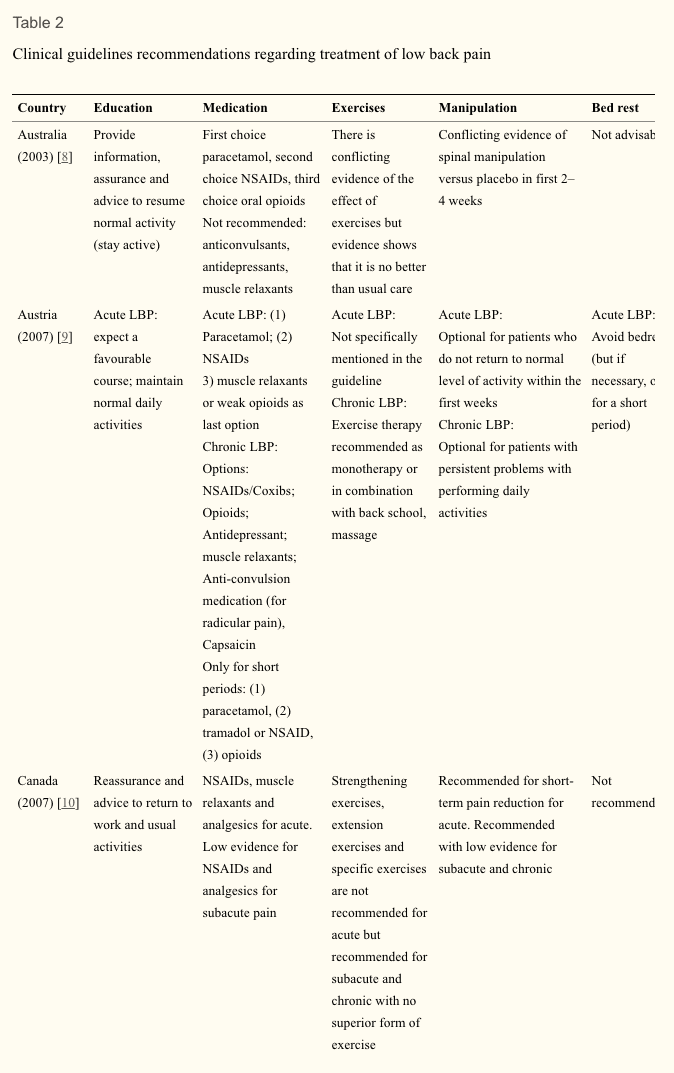
Recommendations Regarding Information and Advice, Treatment, and Return to Work Strategies
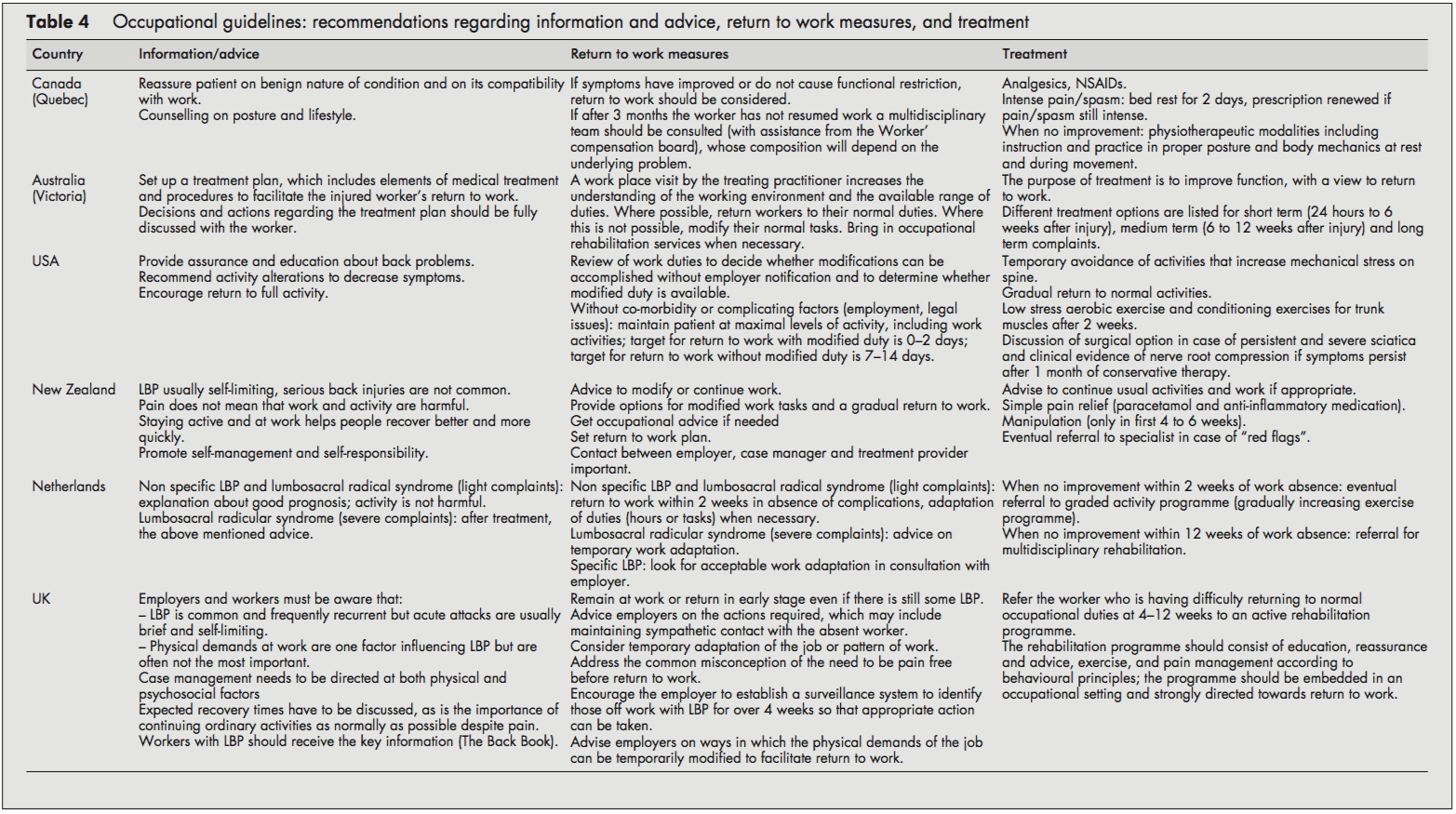
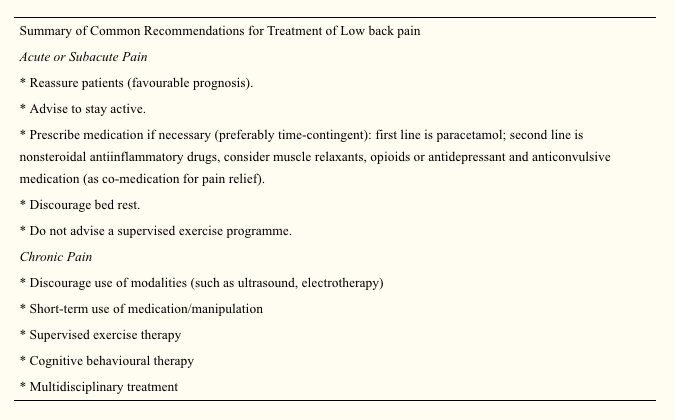
Most guidelines recommended reassuring the employee and providing information about LBP’s self-limiting nature and good prognosis. Encouragement of return to ordinary activity as generally as possible was frequently advised.
In line with the recommendation to return to regular activity, all guidelines also stressed the importance of returning to work as rapidly as possible, even if there is still some LBP and, if necessary, starting with modified duties in more severe cases. Work duties could then be increased gradually (hours and tasks) until total return to work was reached. The US and Dutch guidelines provided detailed time schedules for return to work. The Dutch approach proposed a return to work within two weeks with an adaptation of duties when necessary.[10] The Dutch system also stressed the importance of time-contingent management about a return to work.[10] The US guideline proposed every attempt to maintain the patient at maximal levels of activity, including work activities; targets for disability duration in terms of return to work were given as 02 days with modified duties and 714 days if modified duties are not used/available.[6] In contrast to the others, the Canadian guideline advised return to work only when symptoms and functional restrictions had improved.[4]
The most frequently recommended treatment options in all the included guidelines were: medication for pain relief,[5, 7, 8] gradually progressive exercise programs,[6, 10] and multidisciplinary rehabilitation.[1013] The US guideline recommended referral within two weeks to an exercise program consisting of aerobic exercises, conditioning exercises for trunk muscles, and exercise quota.[6] The Dutch guideline recommended that if there is no progress within two weeks of work absence, workers should be referred to a graded activity program (gradually increasing exercises) and, if there is no improvement by four weeks, to a multidisciplinary rehabilitation program.[10] The UK guideline recommended that workers who have difficulty returning to regular occupational duties by 412 weeks should be referred to an active rehabilitation program. This rehabilitation program should include education, reassurance and advice, a progressive vigorous exercise and fitness program, and pain management according to behavioral principles; it should be embedded in an occupational setting and directed firmly toward a return to work.[11-13] Extensive lists of possible treatment options were presented in the guidelines of Canada and Australia [4, 5], although most of these were not based on scientific evidence.
Summary of Recommendations Regarding Information, Advice, Return to Work Measures, and Treatment in Workers with LBP
Reassure the worker and provide adequate information about LBP’s self-limiting nature and good prognosis.
Advise the worker to continue ordinary activities or to return to regular exercise and work as soon as possible, even if there is still some pain.
Most workers with LBP return to more or less regular duties quite rapidly. Consider temporary adaptations of work duties (hours/tasks) only when necessary.
When a worker fails to return to work within 212 weeks (there is considerable variation in the time scale in different guidelines), refer them to a gradually increasing exercise program, or multidisciplinary rehabilitation (exercises, education, reassurance, and pain management following behavioral principles). These rehabilitation programs should be embedded in an occupational setting.
Discussion
The management of LBP in an occupational health setting must address the relation between low back complaints and work and develop strategies aimed at a safe return to work. This review compared available occupational health guidelines from various countries. Policies are rarely indexed in Medline, so when searching for guidelines, we had to rely primarily on personal files and personal communication.
Quality Aspects and Development Process of the Guidelines
The assessment by the AGREE instrument[3] showed some differences in the quality of the guidelines reviewed, which may partly reflect the variation in the dates of development and publication of the guidelines. The Canadian guideline, for example, was published in 1987 and the Australian guideline in 1996.[4, 5] The other guidelines were more recent and incorporated a more extensive evidence base and more up to date guideline methodology.
Several common flaws related to the development process of the guidelines were shown by the assessment by the AGREE instrument. Firstly, it is important to make clear whether a guideline is editorially independent from the funding body, and whether there are conflicts of interest for the members of the guideline committee. None of the included guidelines clearly reported these issues. Further, reported external review of the guideline by clinical and methodological experts prior to publication was also lacking in all guidelines included in this review.
Several guidelines provided comprehensive information on the way relevant literature was searched and translated into recommendations.[4, 6, 11, 13] Other guidelines supported their recommendations by references,[5, 7, 9, 10] but this does not permit assessment of the robustness of the guidelines or their recommendations.
Guidelines depend on the scientific evidence, which changes over time, and it is striking that only one guideline provided for future update.[11, 12] Possibly there are updates planned for the other guidelines but they are not explicitly stated (and conversely stating there will be future update does not mean it will actually occur). This lack of reporting may also hold true for other AGREE criteria that we rated negatively. The use of the AGREE framework as a guide for both the development and the reporting of guidelines should help to improve the quality of future guidelines.
Assessment and Management of LBP
The diagnostic procedures recommended in the occupational health guidelines were largely similar to the recommendations of clinical guidelines,[2] and, logically, the main difference was the emphasis on addressing occupational issues. The reported methods for addressing workplace factors in the assessment of LBP of the individual worker concerned the identification of difficult tasks, risk factors, and obstacles for return to work by occupational histories. Obviously, these obstacles for return to work not only concern physical load factors, but also work related psychosocial problems regarding responsibilities, cooperation with co-workers, and the social atmosphere at the workplace.[10] Screening for work related psychosocial yellow flags may help to identify those workers who are at risk for chronic pain and disability.[1113]
A potentially important feature of the guidelines is that they were consistent regarding their recommendations to reassure the employee with LBP, and to encourage and support return to work even with some persisting symptoms. There is general consensus that most workers do not have to wait until they are completely free of pain before returning to work. The lists of treatment options provided by the Canadian and Australian guidelines may reflect the lack of evidence at that time,[4, 5] leaving users of the guidelines to choose for themselves. It is, however, questionable whether such lists really contribute to improved care, and in our view guideline recommendations should be based on sound scientific evidence.
The US, Dutch, and UK occupational guidelines[6, 1013] recommend that active multidisciplinary treatment is the most promising intervention for return to work, and this is supported by strong evidence from RCTs.[19, 20] However, more research is still needed to identify the optimum content and intensity of those treatment packages.[13, 21]
Despite some evidence for a contribution of workplace factors in the aetiology of LBP,[22] systematic approaches for workplace adaptations are lacking, and are not offered as recommendations in the guidelines. Perhaps this represents a lack of confidence in the evidence on the overall impact of workplace factors, a difficulty of translation into practical guidance, or because these issues are confounded with local legislation (which was hinted at in the UK guideline[11]). It may be that the participatory ergonomics intervention, which proposes consultations with the worker, the employer, and an ergonomist, will turn out to be a useful return to work intervention.[23, 24] The potential value of getting all the players onside[25] was stressed in the Dutch and the UK guidelines,[1113] but further evaluation of this approach and its implementation is required.
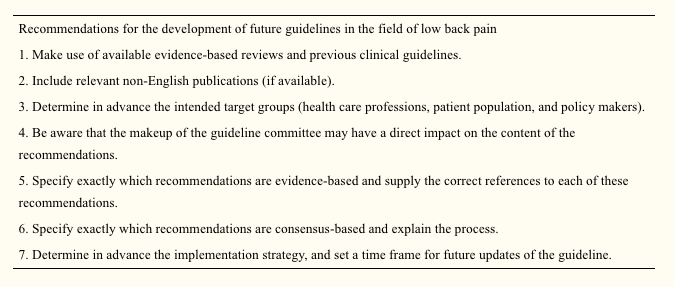
Development of Future Guidelines in Occupational Health Care
The purpose of this review was to give both an overview and a critical appraisal of occupational guidelines for the management of LBP. The critical appraisal of the guidelines is meant to help direct future development and planned updates of guide- lines. In the still emerging field of guideline methodology we consider all past initiatives as laudable; we recognise the need for clinical guidance, and appreciate that guidelines developers cannot wait for research to provide all the methodology and evidence required. However, there is room for improvement and future guidelines and updates should consider the criteria for proper development, implementation, and evaluation of guidelines as suggested by the AGREE collaboration.
The implementation of the guidelines is beyond the scope of this review, but it was noted that none of the guideline documents specifically described implementation strategies, so it is uncertain to what extent the target groups may have been reached, and what effects that may have had. This may be a fruitful area for further research.
The very existence of these occupational health guidelines shows that existing primary care clinical guidelines for LBP2 are considered inappropriate or insufficient for occupational health care. There is a clear perception internationally that the needs of the worker experiencing back pain are intrinsically linked to a variety of occupational issues not covered by usual primary care guidance and, consequently, practice. What emerges is that, despite the methodological flaws, considerable agreement is evident on a range of fundamental occupational health strategies for managing the worker with back pain, some of which are innovative and challenge previously held views. There is agreement on the fundamental message that prolonged work loss is detrimental, and that early work return should be encouraged and facilitated; there is no need to wait for complete symptom resolution. Although the recommended strategies vary somewhat, there is considerable agreement on the value of positive reassurance and advice, availability of (temporary) modified work, addressing workplace factors (getting all the players onside), and rehabilitation for workers having difficulty returning to work.
Acknowledgements
This study was supported by the Dutch Health Care Insurance Council (CVZ), grant DPZ no. 169/0, Amstelveen, Netherlands. J B Staal is currently working at the Department of Epidemiology, Maastricht University, PO Box 616 6200 MD Maastricht, Netherlands. W van Mechelen is also part of the Research Centre on Physical Activity, Work and Health, Body@work TNO-VUmc.
In conclusion, symptoms of low back pain are one of the most common health issues associated with work injuries. Because of it, several occupational health guidelines have been established for the management of low back pain. Chiropractic care, among other treatment methods, may be utilized in order to help the patient find relief from their LBP. Furthermore, the article above demonstrated the safety and effectiveness of a variety of traditional as well as alternative treatment options in the diagnosis, treatment and prevention of a variety of low back pain cases. However, further research studies are required in order to properly determine the efficiency of each individual treatment method. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. Van Tulder MW, Koes BW, Bouter LM. A cost-of-illness study of back pain in the Netherlands. Pain 1995;62:233�40.
2. Koes BW, van Tulder MW, Ostelo R, et al. Clinical guidelines for the management of low back pain in primary care: an international
comparison. Spine 2001;26:2504�14.
3. The AGREE Collaboration. Appraisal of Guidelines Research &
Evaluation Instrument, www.agreecollaboration.org.
4. Spitzer WO, Leblanc FE, Dupuis M. Scientific approach to the
assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Spine 1987;12(suppl 7S):1�59.
5. Victorian WorkCover Authority. Guidelines for the management of employees with compensable low back pain. Melbourne: Victorian WorkCover Authority, 1996.
6. Harris JS. Occupational medicine practice guidelines. Beverly, MA: OEM Press, 1997.
7. Accident Compensation Corporation and National Health Committee. Active and working! Managing acute low back pain in the workplace. Wellington, New Zealand, 2000.
8. Accident Compensation Corporation and National Health Committee, Ministry of Health. Patient guide to acute low back pain management. Wellington, New Zealand, 1998.
9. Kendall, Linton SJ, Main CJ. Guide to assessing psychosocial yellow flags in acute low back pain. Risk factors for long-term disability and work loss. Wellington, New Zealand, Accident Rehabilitation & Compensation Insurance Corporation of New Zealand and the National Health Committee, 1997.
10. Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (Dutch Association of Occupational Medicine, NVAB). Handelen van de bedrijfsarts bij werknemers met lage-rugklachten. Richtlijnen voor Bedrijfsartsen. [Dutch guideline for the management of occupational physicians of employees with low back pain]. April 1999.
11. Carter JT, Birell LN. Occupational health guidelines for the management of low back pain at work�principal recommendations. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
12. Occupational health guidelines for the management of low back pain at work�leaflet for practitioners. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
13. Waddell G, Burton AK. Occupational health guidelines for the management of low back pain at work�evidence review. Occup Med 2001;51:124�35.
14. Roland M, et al. The back book. Norwich: The Stationery Office, 1996.
15. ICSI. Health care guideline. Adult low back pain. Institute for Clinical Systems Integration, 1998 (www.icsi.org/guide/).
16. Kazimirski JC. CMA policy summary: The physician�s role in helping patients return to work after an illness or injury. CMAJ 1997;156:680A�680C.
17. Yamamoto S. Guidelines on worksite prevention of low back pain. Labour standards bureau notification, No. 57. Industrial Health 1997;35:143�72.
18. INSERM. Les Lombalgies en milieu professionel: quel facteurs de risque et quelle prevention? [Low back pain at the workplace: risk factors and prevention]. Paris: les editions INSERM, Synthese bibliographique realise a la demande de la CANAM, 2000.
19. Lindstro?m I, Ohlund C, Eek C, et al. The effect of graded activity on patients with subacute low back pain: a randomised prospective clinical study with an operant-conditioning behavioural approach. Physical Therapy 1992;72:279�93.
20. Karjalainen K, Malmivaara A, van Tulder M, et al. Multidisciplinary biopsychosocial rehabilitation for subacute low back pain in working-age adults: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 2001;26:262�9.
21. Staal JB, Hlobil H, van Tulder MW, et al. Return-to-work interventions for low back pain: a descriptive review of contents and concepts of working mechanisms. Sports Med 2002;32:251�67.
22. Hoogendoorn WE, van Poppel MN, Bongers PM, et al. Physical load during work and leisure time as risk factors for back pain. Scand J Work Environ Health 1999;25:387�403.
23. Loisel P, Gosselin L, Durand P, et al. A population-based, randomised clinical trial on back pain management. Spine 1997;22:2911�18.
24. Loisel P, Gosselin L, Durand P, et al. Implementation of a participatory ergonomics program in the rehabilitation of workers suffering from subacute back pain. Appl Ergon 2001;32:53�60.
25. Frank J, Sinclair S, Hogg-Johnson S, et al. Preventing disability from work-related low-back pain. New evidence gives new hope�if we can just get all the players onside. CMAJ 1998;158:1625�31.
According to the American Chiropractic Association, approximately 31 million people in the United States experience low back pain throughout their lifetime. Low back pain can occur due to a variety of injuries and/or conditions and it can range in severity. Trauma from an injury or an aggravated condition can cause symptoms ranging from mild and annoying to intense and debilitating. The most common type of low back pain is described as a dull, achy, burning or spasming sensation.
Diagnosing the source of a patient’s low back pain can be challenging, however, several healthcare professionals are qualified and experienced in the treatment of spinal health issues, including chiropractors and physical therapists. As a matter of fact, new guidelines from the American Medical Association, or the AMA, have suggested that people affected with low back pain should seek chiropractic care before seeking treatment from conventional medical doctors because chiropractors primarily focus on the diagnosis, treatment and prevention of injuries and/or conditions affecting the musculoskeletal and nervous system.
Chiropractic care is a well-known alternative treatment option commonly utilized to treat injuries and/or conditions causing low back pain. Regular chiropractic care can provide safe and effective, non-invasive treatment without the need to utilize drugs and/or medications. A chiropractor, or doctor of chiropractic, will commonly use spinal adjustments and manual manipulations to carefully correct any spinal misalignment, or subluxation, along the lumbar spine which may be causing symptoms of low back pain. Other treatment methods commonly utilized in chiropractic care include, hot or cold compresses, massage and physical therapy modalities like interferential therapy or transcutaneous electrical nerve stimulations, or TENS and spinal decompression therapy. A chiropractor may also offer nutritional advice and fitness plans to speed up the patient’s recovery process.
By restoring the original alignment of the spine, a chiropractor can help improve the function of the spine by reducing pain and discomfort, decreasing inflammation, and improving range of motion and flexibility as well as increasing strength. Chiropractic care allows the human body to naturally heal itself in order to better be able to manage symptoms associated with low back pain. Based on the diagnosis of a patient, a doctor of chiropractic may also refer patients to other healthcare professionals for further treatment. The purpose of the following article is to demonstrate an overview of updated clinical treatment guidelines for the proper management of non-specific low back pain in a primary care setting.
An Updated Overview of Clinical Guidelines for the Management of Non-Specific Low Back Pain in Primary Care
Abstract
The aim of this study was to present and compare the content of (inter)national clinical guidelines for the management of low back pain. To rationalise the management of low back pain, evidence-based clinical guidelines have been issued in many countries. Given that the available scientific evidence is the same, irrespective of the country, one would expect these guidelines to include more or less similar recommendations regarding diagnosis and treatment. We updated a previous review that included clinical guidelines published up to and including the year 2000. Guidelines were included that met the following criteria: the target group consisted mainly of primary health care professionals, and the guideline was published in English, German, Finnish, Spanish, Norwegian, or Dutch. Only one guideline per country was included: the one most recently published. This updated review includes national clinical guidelines from 13 countries and 2 international clinical guidelines from Europe published from 2000 until 2008. The content of the guidelines appeared to be quite similar regarding the diagnostic classification (diagnostic triage) and the use of diagnostic and therapeutic interventions. Consistent features for acute low back pain were the early and gradual activation of patients, the discouragement of prescribed bed rest and the recognition of psychosocial factors as risk factors for chronicity. For chronic low back pain, consistent features included supervised exercises, cognitive behavioural therapy and multidisciplinary treatment. However, there are some discrepancies for recommendations regarding spinal manipulation and drug treatment for acute and chronic low back pain. The comparison of international clinical guidelines for the management of low back pain showed that diagnostic and therapeutic recommendations are generally similar. There are also some differences which may be due to a lack of strong evidence regarding these topics or due to differences in local health care systems. The implementation of these clinical guidelines remains a challenge for clinical practice and research.
Keywords:Low back pain, Clinical guidelines, Review, Diagnosis, Treatment
Dr. Alex Jimenez’s Insight
Low back pain is one of the most common reasons for doctor office visits each year. In fact, about 80 percent of the population in the United States will suffer from back pain at least once throughout their lifetime. Regular chiropractic care can help prevent, treat and manage low back pain symptoms. Chiropractic care can provide many other benefits as well. Patient’s who have received chiropractic care for injuries and/or conditions affecting the musculoskeletal and nervous systems have experienced improvements to their digestive health and have reported better and deeper sleep after a visit to a chiropractor office. Furthermore, research studies have demonstrated that chiropractic care can help build your immune system. Chiropractic care has even been associated with stress management, reducing depression and anxiety levels. Chiropractic care can provide low back pain relief and improve overall health and wellness.
Introduction
Low back pain remains a condition with a relatively high incidence and prevalence. Following a new episode, the pain typically improves substantially but does not resolve completely during the first 4�6 weeks. In most people the pain and associated disability persist for months; however, only a small proportion remains severely disabled [1]. For those whose pain does resolve completely, recurrence during the next 12 months is not uncommon [2, 3].
There is a wide acceptance that the management of low back pain should begin in primary care. The challenge for primary care clinicians is that back pain is but one of many conditions that they manage. For example while back pain, in absolute numbers, is the eighth most common condition managed by Australian GPs, it only accounts for 1.8% of their case load [4]. To assist primary care practitioners to provide care that is aligned with the best evidence, clinical practice guidelines have been produced in many countries around the world.
The first low back pain guideline was published in 1987 by the Quebec Task Force with authors pointing to the absence of high-quality evidence to guide decision making [5]. Since that time there has been a strong growth in research addressing diagnosis and prognosis but especially research on therapy. As an example of this growth, at the time of the Spitzer guideline [5] there were only 108 randomised controlled trials evaluating physiotherapy treatments for low back pain but as at April 2009 there were 958.1 The Cochrane database (Central) currently lists more than 2500 controlled trials evaluating treatment for back and neck pain. The evidence from these trials for most interventions is summarised in systematic reviews and meta-analysis. The Cochrane Back Review Group, for example, has now published 32 systematic reviews of randomised controlled trials evaluating interventions for low back pain. In the near future, systematic reviews of studies evaluating diagnostic intervention for low back pain will also be included in the Cochrane Library.
This dramatic growth in research would be a comfort to those who were members of the original Quebec Task Force but perhaps a challenge to those who served on committees for later guidelines. With a large and ever increasing research base to inform guidelines two potential problems arise. The first and most obvious is that the recommendations in the guidelines may become out of date. The second is that with a wealth of information to consider, the various committees producing guidelines may produce quite different treatment recommendations. At the same time one can argue that if more precise and valid information becomes available recommendations will become more similar. A previous systematic review of clinical practice guidelines was conducted in 2001 [6]. In that review we assessed the available clinical guidelines from 11 countries and concluded that the guidelines provided generally similar recommendations regarding the diagnostic classification (diagnostic triage) and the use of diagnostic and therapeutic interventions. Consistent features were the early and gradual activation of patients, the discouragement of prescribed bed rest, and the recognition of psychosocial factors as risk factors for chronicity. However, there were discrepancies for recommendations regarding exercise therapy, spinal manipulation, muscle relaxants, and patient information.
Bouwmeester et al. [7] concluded recently that the quality of mono- and multidisciplinary clinical guidelines for the management of low back pain, as measured with the AGREE instrument has improved over time. The present article focuses on the actual content of national clinical guidelines on low back pain which have been issued since 2001. These guidelines are compared regarding the content of their recommendations, the target group, the guideline committee and its procedures, and the extent to which the recommendations were based on the available literature (the scientific evidence). We also highlight any changes in recommendations that have occurred over time in comparison with our previous review [6].
Methods
Clinical guidelines were searched using electronic databases covering the period 2000�2008: Medline (key words: low back pain, clinical guidelines), PEDro (key words: low back pain, practice guidelines, combined with AND), National Guideline Clearinghouse (www.guideline.gov; key word: low back pain), and National Institute for Health and Clinical Excellence (NICE) (www.nice.org.uk; key word: low back pain). Guidelines used in the previous review were checked for updates. We also checked the content and reference list of relevant reviews on guidelines, included a search on the Web of Science citation index for articles citing the previous review and asked experts in the field. To be included in this review, the guidelines had to meet the following criteria: (1) the guideline concerned the diagnosis and clinical management of low back pain, (2) the guideline was targeted at a multidisciplinary audience in the primary care setting, and (3) the guideline was available in English, German, Finnish, Spanish, Norwegian or Dutch because documents in these languages could be read by the reviewers. Only one guideline was included per country unless there were separate guidelines for acute and chronic low back pain. Where more than one eligible guideline was available for a country, we included the most recent guideline issued by a national body. Guidelines from the following countries/regions and agencies (year of publication) were included:
Australia, National Health and Medical Research Council (2003) [8];
Austria, Center for Excellence for Orthopaedic Pain Management Speising (2007) [9];
Canada, Clinic on Low back Pain in Interdisciplinary Practice (2007) [10];
Europe, COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care (2004) [11];
Europe, COST B13 Working Group on Guidelines for the Management of Chronic Low Back Pain in Primary Care (2004) [12];
Finland, Working group by the Finnish Medical Society Duodecim and the Societas Medicinae Physicalis et Rehabilitationis Fenniae. Duodecim (2008) [13];
France, Agence Nationale d�Accreditation et d�Evaluation en Sante (2000) [14];
Germany, Drug Committee of the German Medical Society (2007) [15];
Italy, Italian Scientific Spine Institute (2006) [16];
New Zealand, New Zealand Guidelines Group (2004) [17];
Norway, Formi & Sosial- og helsedirectorated (2007) [18];
Spain, the Spanish Back Pain Research Network (2005) [19];
The Netherlands, The Dutch Institute for Healthcare Improvement (CBO) (2003) [20];
United Kingdom, National Health Service (2008) [21]; and
United States, American College of Physicians and the American Pain Society (2007) [22].
Data regarding the diagnostic and therapeutic recommendations as well as background information of the guideline process were extracted from the guidelines by four of the authors, each assessing 3�4 guidelines. The Finnish and Norwegian guidelines were assessed by colleagues with relevant language skills from The Netherlands and Finland. The focus was on the process of guideline development and the recommendations for diagnosis and treatment. We used the same data categories as in the previous review to facilitate comparisons (see Tables 1, ?,2,2, ?,33).
Results
Patient Population
Each of the guidelines considered the duration of symptoms but they vary in their scope and definitions. For example, the guidelines from Australia and New Zealand focus on acute low back pain whereas the guidelines from Austria and Germany consider acute, subacute, chronic and recurrent low back pain. The cut-off for chronic is not always specified but when it was, 12 weeks was used. Sometimes the word persistent rather than chronic was used. Two guidelines (Austrian and German) provide recommendations for recurrent low back pain but do not explicitly define �recurrent�.
Diagnostic Recommendations
Table 1 compares the diagnostic classification and the recommendations on diagnostic procedures in the various guidelines. All guidelines recommend a diagnostic triage where patients are classified as having (2) non-specific low back pain, (2) suspected or confirmed serious pathology (�red flag� conditions such as tumour, infection or fracture) and (3) radicular syndrome. Some guidelines, e.g. the Australian and New Zealand guidelines, do not distinguish between non-specific low back pain and radicular syndrome. The German guideline also classifies a group of patients who are at risk for chronicity, based on �yellow flags�.
All guidelines are consistent in their recommendations that diagnostic procedures should focus on the identification of red flags and the exclusion of specific diseases (sometimes including radicular syndrome). Red flags include, for example, age at onset (<20 or >55 years), significant trauma, unexplained weight loss and widespread neurologic changes. The types of physical examination and physical tests that are recommended show some variation. Some, such as the European guideline, limit the examination to a neurological screen whereas others advocate a more comprehensive musculoskeletal (including inspection, range of motion/spinal mobility, palpation, and functional limitation) and neurological examination. The components of the neurologic screening are not always explicit but where they are, comprise testing of strength, reflexes, sensation and straight leg raising.
None of the guidelines recommend routine use of imaging, with imaging recommended at the initial visit only for cases of suspected serious pathology (e.g. Australian, European) or where the proposed treatment (e.g. manipulation) requires the exclusion of a specific cause of low back pain (French). Imaging is sometimes recommended where sufficient progress is not being made but the time cut-off varies from 4 to 7 weeks. Guidelines often recommend MRI in cases with red flags (e.g. European, Finland, Germany).
All guidelines mention psychosocial factors associated with poor prognosis with some describing them as �yellow flags�. There is, however, considerable variation in the amount of details given about how to assess �yellow flags� or the optimal timing of the assessment. The Canadian and the New Zealand guidelines provide specific tools for identifying yellow flags and clear guidelines for what should be done once yellow flags are identified.
Therapeutic Recommendations
Table 2 compares therapeutic recommendations given in the various guidelines. Patient advice and information is recommended in all guidelines. The common message is that patients should be reassured that they do not have a serious disease, that they should stay as active as possible and progressively increase their activity levels. Compared with the previous review, the current guidelines increasingly mention early return to work (despite having low back pain) in their list of recommendations.
Recommendations for the prescription of medication are generally consistent. Paracetamol/acetaminophen is usually recommended as a first choice because of the lower incidence of gastrointestinal side effects. Nonsteroidal anti-inflammatory drugs are the second choice in cases where paracetamol is not sufficient. There is some variation between guidelines with regard to recommendations for opioids, muscle relaxants, steroids, antidepressant and anticonvulsive medication as co-medication for pain relief. Where the mode of consumption of analgesics is described, time-contingent rather than pain-contingent use, is advocated.
There is now broad consensus that bed rest should be discouraged as a treatment for low back pain. Some guidelines state that if bed rest is indicated because of severity of pain, then it should not be advised for more than 2 days (e.g., Germany, New Zealand, Spain, Norway). The Italian guideline advises 2�4 days of bed rest for major sciatica but does clearly describe how major sciatica differs from sciatica where bed rest is contraindicated.
There is also consensus that a supervised exercise programme (as distinct from encouraging resumption of normal activity) is not indicated for acute low back pain. Those guidelines that consider subacute and chronic low back pain recommend exercise but note that there is no evidence that one form of exercise is superior to another. The European guideline advises against exercise that requires expensive training and machines. The one area of therapy that is contentious is the use of spinal manipulation. Some guidelines do not recommend the treatment (e.g. Spanish, Australian), some advise that it is optional (e.g. Austrian, Italian) and some suggest a short course for those who do not respond to the first line of treatment (e.g. US, the Netherlands). For some it is optional only in the first weeks of an episode in acute low back pain (e.g. Canada, Finland, Norway, Germany, New Zealand). The French guideline advises that there is no evidence to recommend one form of manual therapy over another.
Setting. Table 3 shows some background variables related to the development of the guidelines in the various countries. Most of the guidelines focus on primary care though some also include secondary care. The Spanish guideline is written for health professions that treat low back pain.
Guideline committee. The various committees responsible for the development and publication of guidelines appear to be different in size and in the professional disciplines involved. Most committees are characterised by their multidisciplinary membership. These usually included primary care physicians, physical and manual therapists, orthopaedic surgeons, rheumatologists, radiologists, occupational and rehabilitation physicians. The number of members varied from 7 to 31. Only three committees included consumer representation (Australia, New Zealand, the Netherlands).
Evidence-based review. All guidelines are more or less based on a comprehensive literature search, including Cochrane Library, Medline, Embase. Some committees (Austria, Germany, Spain) based their recommendations, entirely or in part, on the European guidelines. Most guidelines use an explicit weighting of the strength of the evidence.
The Dutch, UK, European, Finnish, German, Norwegian and Australian guidelines give direct links between the actual recommendations and the evidence (via specific references) on which the recommendations are based. Other guidelines do not present a direct link but state that for recommendation there is at least moderate or fair evidence (New Zealand, US). Most committees use consensus methods, mostly by group discussions when the evidence was not convincing or not available.
Presentation and implementation. The activities related to the publication and dissemination of the various guidelines show some differences and some similarities. In most cases, the guidelines are accompanied by easily accessible summaries for practitioners and booklets for patients. Systematic implementation activities are rare. In most cases, the printed versions of the guidelines are published in national journals and/or disseminated through professional organisations to the target practitioners. Most guidelines are available on the websites of participating organisation. In many countries, regular updates of the guidelines are planned with time horizons of 3�5 years.
Discussion
In the past decade many countries have issued (updated) clinical guidelines for the management of low back pain. In general these guidelines provide similar advice on the management of low back pain. Common recommendations are the diagnostic triage of patients with low back pain, restricted use of radiographs, advice on early and progressive activation of patients, and the related discouragement of bed rest. The recognition of psychosocial factors as a risk factor for chronicity is also consistent across all guidelines, though with varying emphasis and detail. There are also differences in the recommendations provided by the guidelines, but these are few and probably less than could expected for different health care systems and cultures. One of the reasons for the similarity of the guidelines might be that guideline committees are usually aware of the content of other guidelines and are motivated to produce similar recommendations that are deemed sensible and relevant. In some instances the guidelines are a national adaptation (e.g. in Spain) of the European guidelines.
We do not present an exhaustive overview of all clinical guidelines available, but focused on national multidisciplinary guidelines. This enables a reasonable comparison of recommended approaches across countries. A limitation is thus that not all available guidelines, including mono-disciplinary guidelines, are included.
Use of Available Evidence
Most reviews are based on extensive literature reviews. Cochrane reviews are frequently used, comprehensive searches in databases such as Medline, Embase and PEDro. Increasingly the literature reviews of other and previous guidelines are used as starting point for the (additional) searches. Most committees also use some kind of weighting system and rating of the evidence. There is some variation in the way the recommendations are presented. In some guidelines all the recommendations are directly linked with references to the supporting evidence, and in others a general remark is made that for all recommendations that there is at least moderate evidence available.
Differences in Recommendations
Recommendations about the prescription of analgesic medication remain fairly consistent. Most guidelines recommend paracetamol as the first option and nonsteroidal anti-inflammatory preparations as the second option. Further recommendations about other drugs like opioids, muscle relaxants and benzodiazepines and antidepressants vary quite considerably. Part of these variations might reflect the setting and custom in different countries. Since all the guidelines were issued within a relative short time frame, the availability of underlying evidence did not vary much.
The recommendations regarding spinal manipulation continue to show some variation. In some guidelines manipulation is recommended, or presented as a therapeutic option, usually for short-term benefit, but others do not recommend it. This holds true for acute as well as chronic low back pain. The reasons for these differences remain speculative. Probably the underlying evidence is not strong enough to result in similar recommendations regarding manipulation across all guidelines, leaving the committees some more room for interpretation, but also local or political reasons may be involved.
There is now relatively large consensus across the various guidelines that specific back exercises (as opposed to the advice to stay active, including for example walking, cycling) are not recommended for patients with acute low back pain. At the same time back exercises are recommended in chronic low back pain. Most guidelines do not recommend a particular type of exercises for chronic low back pain, but some state that they should be intense.
Recommendations in guidelines are based not only on scientific evidence but also on consensus and discussion in the guideline committees. Usually it is stated that consensus was based on group discussion, but the details of these discussions are seldom reported. It is also generally unclear which recommendations are based mainly on scientific evidence and which are based on (mainly) consensus.
There is little information on whether cost-effectiveness played an important role as a basis for the recommendation in a guideline. Of course, there are not yet many cost-effectiveness studies available [23], but it is not fully clear to what extent the published studies were used.
Most guidelines state that the prognosis of an episode of low back pain is good. This holds especially true for patients with acute episodes of low back pain. For patients presenting with a longer duration with low back pain or with recurrent low back pain the prognosis may be less favourable. More individualised and precise estimates of the prognosis of an episode of low back pain may be desirable in the future.
Few Changes in Management Recommendations Over Time
This update showed that overall the recommendations in the current guidelines regarding diagnosis and treatment of low back pain did not change substantially compared to the guidelines issued about a decade ago. This may well illustrate the lack of new evidence showing better results with new diagnostic and therapeutic approaches and/or new evidence showing the inefficacy of existing interventions. A less nihilistic view could be that already a decade ago the most valid recommendations for the management of low back pain were identified. Some may argue that this is indeed the case, and that much more effort should now be given to implementation of guidelines (see below).
Some recommendations did change over time. We now see diagnostic recommendations appearing concerning the value of MRI and CT scans (i.e. in relation to exclusion and further diagnosis of red flags and serious spinal disorders). However, these recommendations are not yet strong, possibly because there are not many diagnostic studies available evaluating the value of MRI in patients with low back pain. Also, the recommendations regarding the assessment of psychosocial risk factors for chronicity are more firm in the current guidelines than that a decade ago. This reflects the insight of the importance of these risk factors for the development of chronicity and future disability. At the same time we must conclude that we are not yet very successful in effective screening of the patients at risk and subsequent therapeutic management of them [24].
Most apparent changes regarding therapeutic interventions include the advice to continue work (despite having low back pain) and or return to work as soon as possible. There are now more recommendations of second line medications such as antidepressants, opioids, benzodiazepines and compound medications. But these recommendations are not consistent across countries, potentially because of weak underlying evidence. There are now also more firm recommendations in favour of exercise therapy in patients with subacute and chronic low back pain. The latter is partly due to the fact that currently more guidelines include recommendation for the management of chronic low back pain as compared to a decade ago. Finally, the reasons and options for referral within primary care and secondary care are now more explicitly presented. It appears that the global approach regarding the management of low back pain remained largely unchanged in the past decade, although some refinements have been suggested.
Implementation
The extent to which currently available guidelines are used and followed in the various countries remains largely unknown. A few studies evaluating various implementation strategies for low back pain guidelines show that changing clinical practice is not an easy task [25, 26]. The publication and dissemination of guidelines alone is usually not enough to change the behaviour of health care providers [27]. The development of effective implementation strategies in this area remains a challenge.
Future Developments in Research and Guideline Development
The present study was primary aimed at presenting an update of the current clinical guidelines for the management of low back pain in primary care. Clinical guidelines focused at secondary care settings, occupational care settings, or specific subgroups of patients with lumbosacral radicular syndrome were not considered. Separate studies need to be undertaken to present an overview for these settings.
We assessed various aspects of the guideline development in Table 3. A formal assessment of the quality, e.g. with the AGREE instrument was not included. This was the topic of a separate paper which concluded that the quality of the guidelines indeed has improved over time [7].
The development of future guidelines in this field may benefit from previous experiences, evidence-based reviews, and various (inter) national guidelines as presented in this overview. The previous review of clinical guidelines listed the following recommendations (slightly modified) for the development of future guidelines in this field. Similar to a recent review on the quality of guidelines [7], this review shows that the quality of guidelines has improved over time and some of the recommendations have been followed. This includes recommendations 1, 3, and 4 (see below). For others, there still is room for improvement Recommendation 2 is not consistently applied. Recommendations 5 and 6 have improved over time, but not all recommendations in the guidelines are directly linked to the underlying evidence, and the process of the consensus methods used is not well described. Finally, the implementation strategies and the time frame of future updates are not well presented.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Footnotes
Based upon search of PEDro database April 29, 2009.
In conclusion,�low back pain is a prevalent medical complaint which affects million of people in the United States alone. Although it may seem difficult to diagnose low back pain because of its many possible causes, a chiropractor, or doctor of chiropractic, can properly diagnose the source of a patient’s low back pain to treat as well as prevent a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractic care utilizes spinal adjustments and manual manipulations, among other treatment methods, to carefully restore the original alignment of the spine, allowing the human body to naturally heal itself. The purpose of the article above is to present updated treatment guidelines fot the management of low back pain in a primary care setting.� Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Koes BW, Tulder MW, Thomas S. Diagnosis and treatment of low back pain.�BMJ.�2006;332(7555):1430�1434. doi: 10.1136/bmj.332.7555.1430.�[PMC free article]�[PubMed]�[Cross Ref]
2.�Pengel L, Herbert R, Maher CG, Refshauge K. Acute low back pain: systematic review of its prognosis.�BMJ.�2003;327:323�327. doi: 10.1136/bmj.327.7410.323.�[PMC free article]�[PubMed]�[Cross Ref]
3.�Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J, York J, Das A, McAuley JH. Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study.�BMJ.�2008;337:171. doi: 10.1136/bmj.a171.�[PMC free article]�[PubMed]�[Cross Ref]
4.�Australian Institute of Health and Welfare (2004) Australia�s Health 2004. AIHW, Canberra
5.�Spitzer W. Scientific approach to the assessment and management of activity-related spinal disorders.�Spine.�1987;12:1�58. doi: 10.1097/00007632-198701000-00001.�[PubMed]�[Cross Ref]
6.�Koes BW, Tulder MW, Ostelo R, et al. Clinical guidelines for the management of low back pain in primary care: an international comparison.�Spine.�2001;26:2504�2513. doi: 10.1097/00007632-200111150-00022.�[PubMed]�[Cross Ref]
7.�Bouwmeester W, Enst A, Tulder MW. Quality of low back pain guidelines improved.�Spine.�2009;34:2562�2567. doi: 10.1097/BRS.0b013e3181b4d50d.�[PubMed]�[Cross Ref]
8.�Evidence-based management of acute musculoskeletal pain.�Bowen Hills: Australian Academic Press; 2003.
9.�Friedrich M, Likar R. Evidenz- und konsensusbasierte �sterreichische Leitlinien f�r das Management akuter und chronischer unspezifischer Kreuzschmerzen.�Wien Klin Wochenschr.�2007;119(5�6):189�197. doi: 10.1007/s00508-006-0754-3.�[PubMed]�[Cross Ref]
11.�Tulder MW, Becker A, Bekkering T, et al. European guidelines for the management of acute low back pain in primary care.�Eur Spine J.�2006;15(Suppl 2):S169�S191. doi: 10.1007/s00586-006-1071-2.[PMC free article]�[PubMed]�[Cross Ref]
12.�Airaksinen O, Brox JI, Cedraschi C, et al. European guidelines for the management of chronic non-specific low back pain.�Eur Spine J.�2006;15(2):S192�S300. doi: 10.1007/s00586-006-1072-1.[PMC free article]�[PubMed]�[Cross Ref]
13.�Malmivaara A, Erkintalo M, Jousimaa J, Kumpulainen T, Kuukkanen T, Pohjolainen T, Seitsalo S, �sterman H (2008) Aikuisten alaselk�sairaudet. (Low back pain among adults. An update within the Finnish Current Care guidelines). Working group by the Finnish Medical Society Duodecim and the Societas Medicinae Physicalis et Rehabilitationis, Fenniae. Duodecim 124:2237�2239
14.�Agence Nationale d�Accreditation et d�Evaluation en Sante (2000) Guidelines department, diagnosis and management of acute low back pain (<3�months) with or without sciatica & diagnosis, management and follow-up of patients with chronic low back pain, Paris.�www.anaes.fr�or�www.sante.fr
15.�Drug Committee of the German Medical Society (2007) Recommendations for treatment of low back pain [in German]. K�ln, Germany
16.�Negrini S, Giovannoni S, Minozzi S, et al. Diagnostic therapeutic flow-charts for low back pain patients: the Italian clinical guidelines.�Euro Medicophys.�2006;42(2):151�170.�[PubMed]
17.�National Health Committee (2004) National Advisory Committee on Health and Disability, Accident Rehabilitation and Compensation Insurance Corporation. New Zealand Acute Low back pain Guide. Wellington, New Zealand
18.�Laerum E, Storheim K, Brox JI. New clinical guidelines for low back pain.�Tidsskr Nor Laegeforen.�2007;127(20):2706.�[PubMed]
19.�Spain, the Spanish Back Pain Research Network (2005) Guia de practica clinica. Lumbalgia Inespecifica. Version espnola de la Guia de Practica Clinica del Programa Europeo COST B13
20.�The Dutch Institute for Healthcare Improvement (CBO) (2003) Clinical guideline for non-specific low back pain [in Dutch]
22.�Chou R, Qaseem A, Snow V, et al. Clinical Efficacy Assessment Subcommittee of the American College of Physicians American College of Physicians American Pain Society Low back pain Guidelines Panel Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society.�Ann Intern Med.�2007;147(7):478�491.�[PubMed]
23.�Roer N, Goossens ME, Evers SM, Tulder MW. What is the most cost-effective treatment for patients with low back pain? A systematic review.�Best Pract Res Clin Rheumatol.�2005;19(4):671�684. doi: 10.1016/j.berh.2005.03.007.�[PubMed]�[Cross Ref]
24.�Jellema P, Windt DA, Horst HE, Blankenstein AH, Bouter LM, Stalman WA. Why is a treatment aimed at psychosocial factors not effective in patients with (sub)acute low back pain?�Pain.�2005;118(3):350�359. doi: 10.1016/j.pain.2005.09.002.�[PubMed]�[Cross Ref]
25.�Bekkering GE, Tulder MW, Hendriks EJM, Koopmanschap MA, Knol DL, Bouter LM, Oostendorp RAB. Implementation of clinical guidelines on physical therapy for patients with low back pain: randomized trial comparing patient outcomes after a standard and active implementation strategy.�Phys Ther.�2005;85(6):544�555.�[PubMed]
26.�Engers AJ, Wensing M, Tulder MW, Timmermans A, Oostendorp RA, Koes BW, Grol R. Implementation of the Dutch low back pain guideline for general practitioners: a cluster randomized controlled trial.�Spine.�2005;30(6):595�600. doi: 10.1097/01.brs.0000155406.79479.3a.�[PubMed][Cross Ref]
27.�Becker A, Leonhardt C, Kochen MM, Keller S, Wegscheider K, Baum E, Donner-Banzhoff N, Pfingsten M, Hildebrandt J, Basler HD, Chenot JF. Effects of two guideline implementation strategies on patient outcomes in primary care: a cluster randomized controlled trial.�Spine.�2008;33(5):473�480. doi: 10.1097/BRS.0b013e3181657e0d.�[PubMed]�[Cross Ref]
Chiropractic care is a well-known alternative treatment option commonly utilized to treat symptoms of sciatica. Sciatica is characterized as radiating pain that originates in the lower back which then travels down the buttocks and hips into the leg and foot as a result of the compression of the sciatic nerve. Symptoms generally develop on a single side of the body, however, sciatica may occur on both sides of the human body. Sciatic nerve pain can vary in frequency and intensity from person to person and it’s commonly described as a dull, sharp, pins and needles sensation similar to electric shocks.
Other symptoms include, burning, numbness and tingling sensations. Common disorders known to cause sciatic nerve pain include, piriformis syndrome or compression caused by the inflammation of the piriformis muscle, subluxations or misalignments of the lumbar spine, bulging or herniated discs, pregnancy, tumors and non-spinal disorders like diabetes and constipation. Because many disorders can cause sciatica, the proper diagnosis of the source of the symptoms of each individual is essential towards every patient’s treatment requirements. Diagnostic testing for sciatic nerve pain includes x-ray, MRI, CT scan and/or electrodiagnostic tests. These examinations can help determine possible contraindications to chiropractic care.
Chiropractic care focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions affecting the musculoskeletal and nervous system by carefully restoring the original alignment of the spine through the use of spinal adjustments and manual manipulations, among other types of treatment methods. The purpose of chiropractic care is to naturally increase the human body’s ability to heal itself without the need for drugs/medication and/or surgery. A chiropractor can provide a variety of treatment methods depending on the source of a patient’s sciatic nerve pain. A common treatment plan for sciatic nerve pain performed by a chiropractor may include spinal adjustments and manual manipulations, ice/cold therapies to reduce inflammation, ultrasound for increasing circulation, TENS or transcutaneous electrical nerve stimulation and lifestyle modifications, such as nutritional advice, fitness recommendations and sleep scheduling. Other treatment methods commonly utilized by a chiropractor to treat sciatica include, flexion-distraction therapy, spinal decompression therapy and the McKenzie therapy.
Flexion-distraction therapy is a gentle procedure utilized for neck and back pain that increases the intervertebral disc height, allowing each disc to assume its central position in order to decrease tension, relieve irritation of the spinal nerve and improve circulation. Flexion-distraction therapy can restore body functions as well as relieve pain. Spinal decompression therapy involves intermittent stretching of the spine in a controlled manner utilizing a traction table or similar motorized device to create a negative intradiscal pressure in order to relieve back pain and/or radiating pain by promoting the passage of healing nutrients into the disc and providing a better healing environment for bulging or herniated discs. And finally, the McKenzie therapy is a standardized approach to both the assessment and treatment of sciatica. The treatment method requires a patient to participate in a series of physical activities in order to evaluate the patient’s pain response and determine the health issue. The McKenzie therapy then utilizes that information to develop a fitness routine with a focus on alleviating painful symptoms.
Although chiropractic care is a safe and effective alternative treatment option commonly utilized to treat symptoms of sciatica, sciatica can be caused by disorders beyond the limit of chiropractic care. If a doctor of chiropractic, or chiropractor, determines that a patient’s disorder requires treatment from another type of specialist, they may refer the individual to another healthcare professional for further treatment. In several cases, the referring chiropractor may continue chiropractic care while co-managing the patient’s treatment with the other specialist. Furthermore, the purpose of the following article is to demonstrate a variety of treatment guidelines on the diagnosis and treatment of sciatica. However, because the information regarding the prevalence of the source of sciatica and its response to specific treatment methods is lacking, further research studies are still required to determine the efficiency of the treatment guidelines mentioned below.
Diagnosis and Treatment of Sciatica
Sciatica affects many people. The most important symptoms are radiating leg pain and related disabilities. Patients are commonly treated in primary care but a small proportion is referred to secondary care and may eventually have surgery. Many synonyms for sciatica appear in the literature, such as lumbosacral radicular syndrome, ischias, nerve root pain, and nerve root entrapment.
Summary Points
Most patients with acute sciatica have a favourable prognosis but about 20%-30% have persisting problems after one or two years
The diagnosis is based on history taking and physical examination
Imaging is indicated only in patients with �red flag� conditions or in whom disc surgery is considered
Passive (bed rest) treatments have been replaced with more active treatments
Consensus is that initial treatment is conservative for about 6-8 weeks
Disc surgery may provide quicker relief of leg pain than conservative care but no clear differences have been found after one or two years
In about 90% of cases sciatica is caused by a herniated disc with nerve root compression, but lumbar stenoses and (less often) tumours are possible causes. The diagnosis of sciatica and its management varies considerably within and between countries�for example, the surgery rates for lumbar discectomy vary widely between countries.[w1] A recent publication confirmed this large variation in disc surgery, even within countries.[1] This may in part be caused by a paucity of evidence on the value of diagnostic and therapeutic interventions and a lack of clear clinical guidelines or reflect differences in healthcare and insurance systems. This review presents the current state of science for the diagnosis and treatment of sciatica.
Sources and Selection Criteria
We identified systematic reviews in the Cochrane Library evaluating the effectiveness of conservative and surgical interventions for sciatica. Medline searches up to December 2006 were carried out to find other relevant systematic reviews on the diagnosis and treatment of low back pain. Keywords were sciatica, hernia nuclei pulposi, ischias, nerve root entrapment, systematic review, meta-analysis, diagnosis, and treatment. In addition we used our personal files for other references, including publications of recent randomised clinical trials. Finally we checked the availability of clinical guidelines.
Dr. Alex Jimenez’s Insight
Sciatica is medically defined as a collective group of symptoms, rather than a single injury and/or condition, commonly characterized by radiating pain along the sciatic nerve in the lower back, which runs down the buttocks and into both legs and feet. Sciatica generally occurs along a single side of the body although it can rarely affect both sides of the human body. Sciatic nerve pain can manifest as a result of a variety of injuries and/or conditions, such as a bulging or herniated disc, which can often make it difficult for healthcare professionals to properly treat it. The role of a chiropractor is to determine the source of a patient’s sciatica in order to utilize the best treatment method for their specific health issue. A chiropractor, or doctor of chiropractic, will commonly use spinal adjustments and manual manipulations, among other treatment methods, to carefully restore the original integrity of the spine and improve symptoms of sciatica. Chiropractic care can increase the human body’s potential to naturally heal itself.
Who Gets Sciatica?
Exact data on the incidence and prevalence of sciatica are lacking. In general an estimated 5%-10% of patients with low back pain have sciatica, whereas the reported lifetime prevalence of low back pain ranges from 49% to 70%.[w2] The annual prevalence of disc related sciatica in the general population is estimated at 2.2%.[2] A few personal and occupational risk factors for sciatica have been reported, including age, height, mental stress, cigarette smoking, and exposure to vibration from vehicles.[2, 3, w2] Evidence for an association between sciatica and sex or physical fitness is conflicting.[2, 3, w2]
Risk Factors for Acute Sciatica[3, w2]
Personal Factors
Age (peak 45-64 years)
Increasing risk with height
Smoking
Mental stress
Occupational Factors
Strenuous physical activity�for example, frequent lifting, especially while bending and twisting
Driving, including vibration of whole body
How is Sciatica Diagnosed?
Sciatica is mainly diagnosed by history taking and physical examination. By definition patients mention radiating pain in the leg. They may be asked to report the distribution of the pain and whether it radiates below the knee and drawings may be used to evaluate the distribution. Sciatica is characterised by radiating pain that follows a dermatomal pattern. Patients may also report sensory symptoms.
Physical examination largely depends on neurological testing. The most applied investigation is the straight leg raising test or Las�gue’s sign. Patients with sciatica may also have low back pain but this is usually less severe than the leg pain. The diagnostic value of history and physical examination has not been well studied.[4] No history items or physical examination tests have both high sensitivity and high specificity. The pooled sensitivity of the straight leg raising test is estimated to be 91%, with a corresponding pooled specificity of 26%.[5] The only test with a high specificity is the crossed straight leg raising test, with a pooled specificity of 88% but sensitivity of only 29%.[5] Overall, if a patient reports the typical radiating pain in one leg combined with a positive result on one or more neurological tests indicating nerve root tension or neurological deficit the diagnosis of sciatica seems justified. Below shows the signs and symptoms that help to distinguish between sciatica and non-specific low back pain.
Indicators for Sciatica[w5]
Unilateral leg pain greater than low back pain
Pain radiating to foot or toes
Numbness and paraesthesia in the same distribution
Straight leg raising test induces more leg pain
Localised neurology�that is, limited to one nerve root
What is the Value of Imaging?
Diagnostic imaging is only useful if the results influence further management. In acute sciatica the diagnosis is based on history taking and physical examination and treatment is conservative (non-surgical). Imaging may be indicated at this stage only if there are indications or �red flags� that the sciatica may be caused by underlying disease (infections, malignancies) rather than disc herniation.
Diagnostic imaging may also be indicated in patients with severe symptoms who fail to respond to conservative care for 6-8 weeks. In these cases surgery might be considered and imaging used to identify if a herniated disc with nerve root compression is present and its location and extent. It is important as part of the decision to operate that the clinical findings and symptoms correspond well with the scan findings. This is especially relevant because disc herniations identified by computed tomography or magnetic resonance imaging are highly prevalent (20%-36%) in people without symptoms who do not have sciatica.[6, w3] In many people with clinical symptoms of sciatica no lumbar disc herniations are present on scans.[7, 8] At present no one type of imaging method shows a clear advantage over others. Although some authors favour magnetic resonance imaging above other imaging techniques because computed tomography has a higher radiation dose or because soft tissues are better visualised,[9, 10] evidence shows that both are equally accurate at diagnosing lumbar disc herniation.[11] Radiography for the diagnosis of lumbar disc herniation is not recommended because discs cannot be visualised by x rays.[11]
What is the Prognosis?
In general the clinical course of acute sciatica is favourable and most pain and related disability resolves within two weeks. For example, in a randomised trial that compared non-steroidal anti-inflammatory drugs with placebo for acute sciatica in primary care 60% of the patients recovered within three months and 70% within 12 months.[12] About 50% of patients with acute sciatica included in placebo groups in randomised trials of non-surgical interventions reported improvement within 10 days and about 75% reported improvement after four weeks.[13] In most patients therefore the prognosis is good, but at the same time a substantial proportion (up to 30%) continues to have pain for one year or longer.[12, 13]
What is the Efficacy of Conservative Treatments for Sciatica?
Conservative treatment for sciatica is primarily aimed at pain reduction, either by analgesics or by reducing pressure on the nerve root. A recent systematic review found that conservative treatments do not clearly improve the natural course of sciatica in most patients or reduce symptoms.[14] Adequately informing patients about the causes and expected prognosis may be an important part of the management strategy. However, educating patients about sciatica has not been specifically investigated in randomised controlled trials.
The information below summarises the evidence of effectiveness for commonly available conservative treatments for sciatica, including injection therapy. Strong evidence of effectiveness is lacking for most of the available interventions. Little difference in effect on pain and functional status has been shown between bed rest and advice on staying active.[15] As a result of this finding, bed rest�for a long time the mainstay of treatment for sciatica�is no longer widely recommended.[w2, w4] Analgesics, non-steroidal anti-inflammatory drugs, and muscle relaxants do not seem to be more effective than placebo in reducing symptoms. Evidence for opioids and various compound drugs is lacking. A systematic review reported that no evidence exists for traction, non-steroidal anti-inflammatory drugs, intramuscular steroids, or tizanidine being superior to placebo.[13] This review suggested that epidural injections of steroid might be effective in patients with acute sciatica.[13] However a more recent systematic review of a larger number of randomised trials reported that there was no evidence of positive short term effects of corticosteroid injections and that the long term effects were unknown.[14] The same systematic review reported that active physical therapy (exercises) seemed not to be better than inactive (bed rest) treatment and other conservative treatments, such as traction, manipulation, hot packs, or corsets).[14]
Levels of Evidence for Conservative Treatments for Sciatica
Bed rest (trade-off)
Staying active, in contrast to bed rest (likely to be beneficial)
Surgical intervention for sciatica focuses on removal of disc herniation and eventually part of the disc or on foraminal stenosis, with the purpose of eliminating the suspected cause of the sciatica. Treatment is aimed at easing the leg pain and corresponding symptoms and not at reducing the back pain. Consensus is that a cauda equina syndrome is an absolute indication for immediate surgery. Elective surgery is the choice for unilateral sciatica. Until recently only one relatively old randomised trial was available that compared surgical intervention with conservative treatment for patients with sciatica.[16] This study showed that surgical intervention had better results after one year, whereas after four and 10 years of follow-up no significant differences were found.[16]
A Cochrane review summarised the available randomised clinical trials evaluating disc surgery and chemonucleolysis.[17] In chemonucleolysis the enzyme chymopapain is injected in the discus with the purpose of shrinking the nucleus pulposus. The review reported better results with disc surgery than with chemonucleolysis in patients with severe sciatica of relatively long duration varying from more than four weeks to more than four months. Chemonucleolysis was more effective than placebo. Indirectly therefore the review suggested that disc surgery is more effective than placebo. On the basis of data from three trials the authors concluded that evidence is considerable that surgical discectomy provides effective clinical relief for carefully selected patients with sciatica as a result of lumbar disc prolapse that fails to resolve with conservative care. A recent review came to the same conclusion.[18] The Cochrane review further concluded that the long term effects of surgical intervention are unclear and that evidence on the optimal timing of surgery is also lacking.[17]
Randomised Controlled Trials not yet Included in Systematic Reviews
Two additional randomised controlled trials have been published comparing disc surgery with conservative treatment. One trial (n=56) compared microdiscectomy with conservative treatment in patients who had had sciatica for six to 12 weeks.[19] Overall, no significant differences were found for leg pain, back pain, and subjective disability over two years of follow-up. Leg pain, however, seemed to initially improve more rapidly in patients in the discectomy group. The large spine patient outcomes research trial (a randomised trial) and related observational cohort study was carried out in the United States.[20, 21] Patients with sciatica for at least six weeks and confirmed disc herniation were invited to participate in either a randomised trial or an observational cohort study. Patients in the trial were randomised to disc surgery or to conservative care. Patients in the cohort study received disc surgery or conservative care based on their preference. In the randomised trial (n=501) both treatment groups improved substantially over two years for all primary and secondary outcome measures. Small differences were found in favour of the surgery group, but these were not statistically significant for the primary outcome measures. Only 50% of the patients randomised to surgery received surgery within three months of inclusion compared with 30% randomised to conservative care. After two years of follow-up 45% of patients in the conservative care group underwent surgery compared with 60% in the surgery group.[20]
The observational cohort included 743 patients. Both groups improved substantially over time, but the surgery group showed significantly better results for pain and function compared with the conservative group. The authors did mention caution in interpreting the findings because of potential confounding by indication and because outcome measures were self reported.[21]
The results indicate that both conservative care and disc surgery are relevant treatment options for patients with sciatica of at least six weeks’ duration. Surgical intervention may provide quicker relief of symptoms compared with conservative care, but no large differences have been found in success rate after one or two years of follow-up. Patients and doctors may thus weigh the benefits and harms of both options to make individual choices. This is especially relevant because patients’ preference for treatment may have a direct positive influence on the magnitude of the treatment effect.
What are the Recommendations in Clinical Guidelines?
Although in many countries clinical guidelines are available for the management of non-specific low back pain this is not the case for sciatica.[22] Below shows the recommendations for sciatica (lumbosacral radicular syndrome) in clinical guidelines recently issued by the Dutch College of General Practice.[w4] After excluding specific diseases on the basis of red flags, sciatica is diagnosed on the basis of history taking and physical examination. Initial treatment is conservative, with a strong focus on patient education, advice to stay active, continuing daily activities, and adequate treatment for pain. In this phase imaging has no role. Referral to a medical specialist�for example, neurologist, rheumatologist, spine surgeon�is indicated in patients whose symptoms do not improve after conservative treatment for at least 6-8 weeks. In these referred cases surgery may be considered. Immediate referral is indicated in cases with a cauda equina syndrome. Acute severe paresis or progressive paresis are also reasons for referral (within a few days).
Clinical Guideline for Diagnosis and Treatment of Sciatica from Dutch College of General Practice[w4]
Diagnosis
Check for red flag conditions, such as malignancies, osteoporotic fractures, radiculitis, and cauda equina syndrome
Take a history to determine localisation; severity; loss of strength; sensibility disorders; duration; course; influence of coughing, rest, or movement; and consequences for daily activities
Carry out a physical examination, including neurological testing�for example, straight leg raising test (Las�gue’s sign)
Carry out the following tests in cases with a dermatomal pattern, or positive result on straight leg raising test, or loss of strength or sensibility disorders: reflexes (Achilles or knee tendon), sensibility of lateral and medial sides of feet and toes, strength of big toe during extension, walking on toes and heel (left-right differences), crossed Las�gue’s sign
Imaging or laboratory diagnostic tests are only indicated in red flag conditions but are not useful in cases of suspected disc herniation
Treatment
Explain cause of the symptoms and reassure patients that symptoms usually diminish over time without specific measures
Advise to stay active and continue daily activities; a few hours of bed rest may provide some symptomatic relief but does not result in faster recovery
Prescribe drugs, if necessary, according to four steps: (1) paracetamol; (2) non-steroidal anti-inflammatory drugs; (3) tramadol, paracetamol, or non-steroidal anti-inflammatory drug in combination with codeine; and (4) morphine
Refer to neurosurgeon immediately in cases of cauda equina syndrome or acute severe paresis or progressive paresis (within a few days)
Refer to neurologist, neurosurgeon, or orthopaedic surgeon for consideration of surgery in cases of intractable radicular pain (not responding to morphine) or if pain does not diminish after 6-8 weeks of conservative care
Promising Developments
More evidence based information has become available on the efficacy of surgical care compared with conservative care for patients with sciatica. Although evidence is limited, initial findings suggest no important differences in long term (one or two years) effect between these two approaches. This finding may be partly explained by patients who initially received conservative care later undergoing disc surgery. In all available studies it seems that a substantial proportion of patients improve over time. This holds true for patients undergoing surgery or receiving conservative care. Patients undergoing disc surgery are more likely to get quicker relief of leg symptoms than patients receiving conservative care. If symptoms do not improve after 6-8 weeks patients may opt for disc surgery. Those who are hesitant about surgery and can cope with their symptoms may opt for continued conservative care. Patient preference is therefore an important feature in the decision process.
Since the mid-1990s a switch has occurred in the management of sciatica from passive treatments, such as bed rest, to a more active approach, with patients being advised to continue their daily activities as much as possible.
Future Research
More information is needed on the importance of clinical signs and symptoms for the prognosis of sciatica and the response to treatment. This includes the value of size and location of the disc herniation, visible nerve root compression, sequestration, and the results of history taking and physical and neurological examinations. Subgroup analysis in a Finnish trial showed that discectomy was superior to conservative treatment in patients with disc herniation at L4-5.[23] No strong evidence exists for or against the efficacy of many of the available conservative treatments. Much progress can be achieved here. Questions remain about the efficacy of analgesics for sciatica and the value of physical therapy and of patient education and counselling. No trial has yet evaluated the effectiveness of behavioural treatment and multidisciplinary treatment programmes.
Tumour necrosis factor ? has been identified in animal and human studies as one factor in the development of sciatica.[23, 24] The first randomised trial evaluating a tumour necrosis factor ? antagonist in patients with sciatica did not find a positive result.[25]
Additional Educational Resources
BMJ Clinical Evidence (www.clinicalevidence.org)�Up to date evidence for clinicians on the benefits and harms of treatments for a variety of disorders
Cochrane Back Review Group (www.cochrane.iwh.on.ca)�Activities of review group responsible for writing systematic Cochrane reviews on the efficacy of treatments for low back pain and sciatica
Low back pain: guidelines for its management (www.backpaineurope.org)�Recently issued guidelines for the management of low back pain and sciatica from the European Commission Research Directorate General
A Patient’s Perspective (A)
After an episode of lumbago during a vacation I continuously had low back pain and tingling feet for about nine months. Then suddenly my right foot started to hurt badly and after a while the pain became so severe that I was unable to leave my house. The specialist ordered an MRI (magnetic resonance imaging) scan and it revealed a large lumbar disc herniation. Since it only got worse after that I decided to have surgery.
After the operation I recovered quickly and the back pain and leg pain were completely gone. I soon was able to go back to work and rebuild my social life. Unfortunately after a couple of months the low back pain and the other symptoms returned, although not as severe as before surgery. A new MRI scan now revealed two small disc herniations and two bad intervertebral discs. The specialist told me that it was too early for a second operation.
Now it is unclear to me what the doctor can do about it and I don’t even know which measures I can take myself. The constant back and leg pain are greatly interfering with my work and my social life. I sometimes feel like an elderly person because of my physical limitations. I try to stay positive, but it is hard to cope with the uncertainty.
C Penning, aged 32, Rotterdam
A Patient’s Perspective (B)
My complaints started about four months ago with pain in the lower back. Soon after the pain radiated into my legs, for which I went to my general practitioner. His analysis was no herniated disc. A muscle relaxant in combination with referral to a physiotherapist would reduce the symptoms. Three weeks of physiotherapy followed by several treatments by a chiropractor did not provide any symptom relief. In fact the symptoms became worse�especially during walking and standing. Lying down and cycling were much better tolerated. Additional complaints were reduced strength in the left leg, not being able to stand on the heel or toes, a cold feeling in the lower leg at the end of the day, while in the morning it felt like standing in a bunch of needles.
About one month ago a neurologist diagnosed a herniated disc on the right side based on an MRI scan that was taken. However, this could not explain the symptoms in the left leg. The symptoms in the left leg could be due to spinal stenosis. The complaints were not severe enough to recommend surgery and the neurologist told me that a substantial improvement was to be expected within a period of 3-4 months. His advice was to continue normal daily activities as much as possible. At present (one month later) I feel some improvement of my symptoms.
Contributors: BWK wrote the first draft. MWvT and WCP critically appraised and improved the manuscript. BWK is guarantor.
Competing interests: None declared.
Provenance and peer review: Commissioned; peer reviewed.
In conclusion,�chiropractic care is a popular alternative treatment option commonly utilized to treat sciatica symptoms. While sciatic nerve pain can occur due to a variety of injuries and/or conditions, the purpose of chiropractic care is to determine the source of a patient’s sciatica in order to properly treat their symptoms using a variety of treatment methods. The article above demonstrates several treatment guidelines for sciatica, however, further research studies are required. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Weinstein JN, Lurie JD, Olson PR, Bronner KK, Fisher ES. United States’ trends and regional variations in lumbar spine surgery: 1992-2003.�Spine�2006;31:2707-14.�[PMC free article]�[PubMed]
2.�Younes M, Bejia I, Aguir Z, Letaief M, Hassen-Zroer S, Touzi M, et al. Prevalence and risk factors of disc-related sciatica in an urban population in Tunisia.�Joint Bone Spine�2006;73:538-42.�[PubMed]
3.�Miranda H, Viikari-Juntera E, Martikainen R, Takala E, Riihimaki H. Individual factors, occupational loading, and physical exercise as predictors of sciatic pain.�Spine�2002;27:1102-9.�[PubMed]
4.�Vroomen PCAJ, Krom MCTFM de, Knottnerus JA. Diagnostic value of history and physical examination in patients suspected of sciatica due to disc herniation: a systematic review.�J Neurol1999;246:899-906.�[PubMed]
5.�Deville WLJM, Windt DAWM, van der Dzaferagic A, Bezemer PD, Bouter LM. The test of Lasegue: systematic review of the accuracy in diagnosing herniated discs.�Spine�2000;25:1140-7.�[PubMed]
6.�Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain.�N Engl J Med�1994;331:69-73.[PubMed]
7.�Modic MT, Ross JS, Obuchowski NA, Browning KH, Cianflocco AJ, Mazanec DJ. Contrast-enhanced MR imaging in acute lumbar radiculopathy: a pilot study of the natural history.�Radiology�1995;195:429-35.�[PubMed]
8.�Modic MT, Obuchowski NA, Ross J, Brant-Zawadzki MN, Grooff PN, Mazanec DJ, et al. Acute low back pain and radiculopathy: MR imaging findings and their prognostic role and effect on outcome.�Radiology�2005;237:597-604.�[PubMed]
9.�Govind J. Lumbar radicular pain.�Aus Fam Phys�2004;33:409-12.�[PubMed]
10.�Awad JN, Moskovich R. Lumbar disc herniations: surgical versus nonsurgical treatment.�Clin Orthop Relat Res�2006;443:183-97.�[PubMed]
11.�Jarvik JG, Deyo RA. Diagnostic evaluation of low back pain with emphasis on imaging.�Ann Intern Med�2002. 137:586-97.�[PubMed]
12.�Weber H, Holme I, Amlie E. The natural course of acute sciatica with nerve root symptoms in a double blind placebo-controlled trial of evaluating the effect of piroxicam (NSAID).�Spine�1993;18:1433-8.[PubMed]
13.�Vroomen PCAJ, Krom MCTFM de, Slofstra PD, Knottnerus JA. Conservative treatment of sciatica: a systematic review.�J Spinal Dis�2000;13:463-9.�[PubMed]
14.�Luijsterburg PAJ, Verhagen AP, Ostelo RWJG, Os TAG van, Peul WC, Koes BW. Effectiveness of conservative treatments for the lumbosacral radicular syndrome: a systematic review.�Eur Spine J�2007. Apr 6;(Epub ahead of print).�[PMC free article]�[PubMed]
15.�Hagen KB, Jamtvedt G, Hilde G, Winnem MF. The updated Cochrane review of bedrest for low back pain and sciatica.�Spine�2005;30:542-6.�[PubMed]
16.�Weber H. Lumbar disc herniation. A controlled prospective study with ten years of observation.�Spine1983;8:131-40.�[PubMed]
17.�Gibson JN, Waddell G. Surgical interventions for lumbar disc prolapse.�Cochrane Database Syst Rev2007. Jan 24;(1):CD001350.�[PubMed]
18.�Van Tulder MW, Koes B, Seitsalo S, Malmivaara A. Outcome of invasive treatment modalities on back pain and sciatica: an evidence-based review.�Eur Spine J�2006;15:S82-92.�[PMC free article]�[PubMed]
19.�Osterman H, Seitsalo S, Karppinen J, Malmivaara A. Effectiveness of microdiscectomy for lumbar disc herniation.�Spine�2006;31:2409-14.�[PubMed]
20.�Weinstein JN, Tosteson TD, Lurie JD, Tosteson ANA, Hanscom B, Skinner JS, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the spine patient outcomes research trial (SPORT): a randomized trial.�JAMA�2006;296:2441-50.�[PMC free article]�[PubMed]
21.�Weinstein JN, Lurie JD, Tosteson TD, Skinner JS, Hanscom B, Tosteson ANA, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the spine patient outcomes research trial (SPORT) observational cohort.�JAMA�2006;296:2451-9.�[PMC free article]�[PubMed]
22.�Koes BW, Tulder MW van, Ostelo R, Burton AK, Waddell G. Clinical guidelines for the management of low back pain in primary care: an international comparison.�Spine�2001;26:2504-13.�[PubMed]
23.�Mulleman D, Mammou S, Griffoul I, Watier H, Goupille P. Pathophysiology of disc-related sciatica. I. Evidence supporting a chemical component.�Joint Bone Spine�2006;73:151-8.�[PubMed]
24.�Mulleman D, Mammou S, Griffoul I, Watier H, Goupille P. Pathophysiology of disc-related low back pain and sciatica. II. Evidence supporting treatment with TNF-alfa antagonists.�Joint Bone Spine2006;73:270-7.�[PubMed]
25.�Korhonen T, Karppinen J, Paimela L, Malmivaara A, Lindgren KA, Bowman C, et al. The treatment of disc herniation-induced sciatica with infliximab: one-year follow-up results of FIRST II, a randomized controlled trial.�Spine�2006;31:2759-66.�[PubMed]
Whiplash is one of the most prevalent types of injuries resulting from an automobile accident, most commonly during rear-end auto collisions. However, whiplash-associated disorders can develop due to a variety of other circumstances, including sports injuries, amusement park rides or physical abuse. Whiplash occurs when the soft tissues of the neck, such as the muscles, tendons and ligaments, extend beyond their natural range of motion because of a sudden back-and-forth movement of the head. Furthermore, the sheer force of an impact can stretch and even tear the complex structures surrounding the cervical spine.
The symptoms of whiplash-associated disorders may take days, weeks or even months to manifest, which is why it’s important for individuals who’ve been involved in an automobile accident to seek immediate medical attention. There are many different types of treatment options which can safely and effectively help treat whiplash. The purpose of the following article is to demonstrate the treatment guidelines of neck pain-associated disorders and whiplash-associated disorders.
The Treatment of Neck Pain-Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline
Abstract
Objective: The objective was to develop a clinical practice guideline on the management of neck pain�associated disorders (NADs) and whiplash-associated disorders (WADs). This guideline replaces 2 prior chiropractic guidelines on NADs and WADs.
Methods: Pertinent systematic reviews on 6 topic areas (education, multimodal care, exercise, work disability, manual therapy, passive modalities) were assessed using A Measurement Tool to Assess Systematic Reviews (AMSTAR) and data extracted from admissible randomized controlled trials. We incorporated risk of bias scores in the Grading of Recommendations Assessment, Development, and Evaluation. Evidence profiles were used to summarize judgments of the evidence quality, detail relative and absolute effects, and link recommendations to the supporting evidence. The guideline panel considered the balance of desirable and undesirable consequences. Consensus was achieved using a modified Delphi. The guideline was peer reviewed by a 10-member multidisciplinary (medical and chiropractic) external committee.
Results: For recent-onset (0-3 months) neck pain, we suggest offering multimodal care; manipulation or mobilization; range-of-motion home exercise, or multimodal manual therapy (for grades I-II NAD); supervised graded strengthening exercise (grade III NAD); and multimodal care (grade III WAD). For persistent (N3 months) neck pain, we suggest offering multimodal care or stress self-management; manipulation with soft tissue therapy; high-dose massage; supervised group exercise; supervised yoga; supervised strengthening exercises or home exercises (grades I-II NAD); multimodal care or practitioner�s advice (grades I-III NAD); and supervised exercise with advice or advice alone (grades I-II WAD). For workers with persistent neck and shoulder pain, evidence supports mixed supervised and unsupervised high-intensity strength training or advice alone (grades I-III NAD).
Conclusions: A multimodal approach including manual therapy, self-management advice, and exercise is an effective treatment strategy for both recent-onset and persistent neck pain. (J Manipulative Physiol Ther 2016;39:523-44.e20) Key
Whiplash occurs when the sheer force of an impact causes the head and neck to jolt abruptly back-and-forth in any direction, stretching the complex structures surrounding the cervical spine beyond their normal range. Neck pain, headache and radiating pain resulting from whiplash are common complaints frequently reported by individuals after being involved in an automobile accident. However, whiplash can also result from a variety of other circumstances. Whiplash-associated disorders are a prevalent source of disability and a common reason many auto accident victims seek medical attention from chiropractors, physical therapists and primary care physicians. Fortunately, many treatment guidelines exist to safely and effectively improve as well as manage the symptoms of whiplash. Chiropractic care is a well-known alternative treatment option for whiplash-associated disorders. Spinal adjustments and manual manipulations can safely and effectively restore the original alignment of the spine, reducing symptoms and alleviating whiplash complications.
Introduction
Neck pain and its associated disorders (NAD), including headache and radiating pain into the arm and upper back, are common and result in significant social, psychological, and economic burden.1-4 Neck pain, whether attributed to work, injury, or other activities,5 is a prevalent source of disability and a common reason for consulting primary health care providers, including chiropractors, physical therapists, and primary care physicians.6 The estimated annual incidence of neck pain measured in 4 studies ranged between 10.4% and 21.3%, with a higher incidence noted in office and computer workers.7 Although some studies report that between 33% and 65% of people have recovered from an episode of neck pain at 1 year, most cases follow an episodic course over a person�s lifetime, and thus, relapses are common.7 Neck pain is a leading cause of morbidity and chronic disability worldwide.5,8 In 2008 the Bone and Joint Decade Task Force on Neck Pain and Its Associated Disorders reported that 50% to 75% of individuals with neck pain also report pain 1 to 5 years later.4 Several modifiable and nonmodifiable environmental and personal factors influence the course of neck pain, including age, previous neck injury, high pain intensity, self-perceived poor general health, and fear avoidance.7
Neck pain related to whiplash-associated disorders (WADs) most commonly results from motor vehicle accidents.9,10�Whiplash-associated disorders disrupt the daily lives of adults around the world and are associated with considerable pain, suffering, disability, and costs.3,11 Whiplash-associated disorders are defined as an injury to the neck that occurs with sudden acceleration or deceler- ation of the head and neck relative to other parts of the body, typically occurring during motor vehicle collisions.10,12 The majority of adults with traffic injuries report pain in the neck and upper limb pain. Other common symptoms of WADs include headache, stiffness, shoulder and back pain, numbness, dizziness, sleeping difficulties, fatigue, and cognitive deficits.9,10 The global yearly incidence rate of emergency department visits as a result of acute whiplash injuries after road traffic crashes is between 235 and 300 per 100,000.3,13,14 In 2010, there were 3.9 million nonfatal traffic injuries in the United States.11 The economic costs of motor vehicle crashes that year totaled USD$242 billion, including $23.4 billion in medical costs and $77.4 billion in lost productivity (both market and household).11 In Ontario, traffic collisions are a leading cause of disability and health care use and�expenditures, resulting in the automobile insurance system paying nearly CND$4.5 billion in accident benefits in 2010.15
More than 85% of patients experience neck pain after a motor vehicle accident, often associated with sprains and strains to the back and extremities, headache, psychological symptomatology, and mild traumatic brain injury.10 Whiplash injuries have an effect on general health, with recovery in the short term reported by 29% to 40% of individuals with WAD in Western countries that have compensation schemes for whiplash injuries. 16,17 The median time to first reported recovery is estimated at 101 days (95% confidence interval: 99-104) and about 23% are still not recovered after 1 year.13
The 2000-2010 Bone and Joint Decade Task Force on Neck Pain and its Associated Disorders recommended that all types of neck pain, including WADs,18 be included under the classification of NAD.19 NAD can be classified into 4 grades, distinguished by the severity of symptoms, signs, and impact on activities of daily life (Table 1).
The clinical management of musculoskeletal disorders, and neck pain in particular, can be complex and often involves combining multiple interventions (multimodal care) to address its symptoms and consequences.19�In this guideline, multimodal care refers to treatment involving at least 2 distinct therapeutic methods, provided by 1 or more health care disciplines.20 Manual therapy (including spinal manipulation), medication, and home exercise with advice are commonly used multimodal treatments for recent- onset and persistent neck pain.21,22 Thus, there is a need to determine which treatments or combinations of treatments are more effective for managing NAD and WAD.
Rationale for Developing This Guideline
The Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration20 recently updated the systematic reviews from the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders (Neck Pain Task Force).23 Consequently, it was deemed timely to update the recommendations of 2 chiropractic guidelines on NAD (2014)24 and WAD (2010)25 produced by the Canadian Chiropractic Association and the Canadian Federation of Chiropractic Regulatory and Educational Accrediting Boards (the �Federation�) into a single guideline.
Scope and Purpose
The aim of this clinical practice guideline (CPG) was to synthesize and disseminate the best available evidence on the management of adults and elderly patients with recent onset (0-3 months) and persistent (N3 months) neck pain and its associated disorders, with the goal of improving clinical decision making and the delivery of care for patients with NAD and WAD grades I to III. Guidelines are �Statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.�26
The target users of this guideline are chiropractors and other primary care health care providers delivering conservative care to patients with NADs and WADs, as well as policymakers. We define conservative care as treatment designed to avoid invasive medical therapeutic measures or operative procedures.
OPTIMa published a closely related guideline in the European Spine Journal.27 Although we reached similar results, OPTIMa developed recommendations using the modified Ontario Health Technology Advisory Committee (OHTAC) framework.28 In contrast, our guideline used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach. GRADE provides a common, sensible, and transparent approach to grading quality (or certainty) of evidence and strength of recom- mendations (www.gradeworkinggroup.org). GRADE was the highest scoring instrument among 60 evidence grading systems29 and has been determined to be reproducible among trained raters.30 GRADE is now considered a standard in guideline development and has been adopted by many international guideline organizations and journals.31 The Canadian Chiropractic Guideline Initiative (CCGI) guideline panel considered available high-quality systematic reviews, updated the search of the peer-reviewed published reports up to December 2015, and then used the GRADE approach to formulate recommen- dations for the management of neck pain and associated disorders.
Framework
To inform its work, the CCGI considered recent advances in methods to conduct knowledge synthesis,32 derive evidence-based recommendations, 31,33 adapt high- quality guidelines, 34 and develop 35 and increase the uptake of CPGs.36,37 An overview of CCGI structure and methods is provided in Appendix 1.
Methods
Ethics
Because no novel human participant intervention was required and secondary analyses were considered, the research presented in this guideline is exempt from institutional ethics review board approval.
Selection of Guideline Development Panelists
The CCGI project lead (A.B.) appointed 2 co-chairs (J.O. and G.S.) for the guideline development group and nominated the project executive committee and the remaining guideline panelists. J.O. served as the lead methodologist on the guideline panel. G.S. helped ensure geographic representation of the panel and advised on specific duties of panel members, time commitment, and decision-making process for reaching consensus (develop- ment of key questions and of recommendations). To ensure a broad representation, the guideline panel included clinicians (P.D., J.W.), clinician researchers (F.A., M.D., C.H., S.P., I.P., J.S.) methodologists (J.O., A.B., M.S., J.H.), a professional leader/decision maker (G.S.), and 1 patient advocate (B.H.) to ensure that patient values and preferences were considered. One observer (J.R.) moni- tored the 3 face-to-face meetings of the guideline panel held in Toronto (June and September 2015 and April 2016).
All CCGI members, including guideline panelists and peer reviewers, were required to disclose any potential conflict of interest by topic before participation and during the guideline development process. There was no self- declaration of conflicts of interest among the panel or the reviewers.
Key Question Development
Six topic areas (exercise, multimodal care, education, work disability, manual therapy, passive modalities) on the conservative management of NAD and WAD grades I to III were covered in 5 recent systematic reviews by the OPTIMa Collaboration,38-42 among a total of 40 reviews on the management of musculoskeletal disorders.20 The panel met over 2 days in June 2015 to brainstorm about potential key questions.
Search Update and Study Selection
The panel assessed the quality of eligible systematic reviews using the AMSTAR tool43 and its 11 criteria (amstar.ca/Amstar_Checklist.php).
Because the last search dates of included systematic reviews were 2012,40,41 2013,38,39,42 and 2014,42 the panel updated the literature searches in Medline and Cochrane Central databases on December 24, 2015 using the published search strategies. We used a 2-phase screening process to select additional eligible studies. In phase 1, 2 independent reviewers screened titles and abstracts to determine the relevance and eligibility of studies. In phase 2, the same pairs of independent reviewers screened full-text articles to make a final determination of eligibility. Reviewers met to resolve disagreements and reach consensus on the eligibility of studies in both phases, with arbitration by a third reviewer if needed. Studies were included if they1 met the PICO (population, intervention, comparator, outcome) criteria and2 were randomized controlled trials (RCTs) with an inception cohort of at least 30 participants per treatment arm with the specified condition, because this sample size is considered the minimum needed for non-normal distributions to approx- imate the normal distribution.44
Data Abstraction and Quality Assessment
Data were extracted from the included studies identified in each systematic review, including study design, participants, intervention, control, outcomes, and funding.
The internal validity of included studies was assessed by the OPTIMa collaboration using the Scottish Intercollegiate Guidelines Network (SIGN) criteria.45
For articles retrieved from the updated search, pairs of independent reviewers critically appraised the internal validity of eligible studies using the SIGN criteria,46 similar to the OPTIMa collaboration reviews. Reviewers reached consensus through discussion. A third reviewer was used to resolve disagreements if consensus could not be reached. A quantitative score or a cutoff point to determine the internal validity of studies was not used. Instead, the SIGN criteria were used to assist reviewers in making an informed overall judgment on the risk of bias of included studies. 47
Synthesis of Results
J.O. extracted data from scientifically admissible studies into evidence tables. A second reviewer (A.B.) indepen- dently checked the extracted data. We performed a qualitative synthesis of findings and stratified results based on the type and duration of the disorder (ie, recent [symptoms lasting b3 months] vs persistent [symptoms lasting N3 months]).
Recommendation Development
We used the Guideline Development Tool (http:// www.guidelinedevelopment.org), and assessed the quality of the body of evidence for our outcomes of interest by�applying the GRADE approach.48 We used the evidence profiles to summarize the evidence.49 The quality of evidence rating (high, moderate, low, or very low) reflects our confidence in the estimate of the effect to support a recommendation and considers the strengths and limitations of the body of evidence stemming from risk of bias, imprecision, inconsistency, indirectness of results, and publication bias.50 Assessment of quality of evidence was carried out in the context of its relevance to the primary care setting.
Using the Evidence to Decisions (EtD) Framework (www.decide-collaboration.eu/etd-evidence- decision-framework), the panel formally met in September 2015 and April 2016 to consider the balance of desirable and undesirable consequences to determine the strength of each recommendation, using informed judgment on the quality of evidence and effect sizes, resource use, equity, acceptability, and feasibility. To make a recommendation, the panel needed to express an average judgment that was beyond neutral with respect to the balance between desirable and undesirable consequences of an intervention, as outlined in the EtD. We defined the strength rating of a recommendation (strong or weak) as the extent to which the desirable consequences of an intervention outweigh its undesirable consequences. A strong recommendation can be made when the desirable consequences clearly outweigh the undesirable consequences. In contrast, a weak recommendation is made when, on the balance of probabilities, the desirable consequences likely outweigh the undesirable consequences. 49,51
The panel provided recommendations based on the evidence if statistically and clinically significant differ- ences were found. The panel followed a 2-step process in making a recommendation. We first agreed that there should be evidence of clinically meaningful changes occurring over time in the study population and that a single consensus threshold of clinical effectiveness should be applied consistently. We reached a consensus decision that a 20% change in the outcome of interest within any study group was required to make a recommendation. The decision to use a 20% threshold was informed by current published reports and relevant available minimal clinically important differences (MCIDs).52-55
However, MCIDs can vary across populations, settings, and conditions and depending on whether within-group or between-group differences are being assessed. Therefore, the panel considered MCID values for the most relevant outcomes (ie, 10% for visual analog scale [VAS] or Neck Disability Index [NDI; 5/50 on the NDI], 20% for numerical rating scale [NRS]) and chose the more conservative of these values as the threshold when evaluating between group differences.52,54
Second, the results from relevant studies were used to formulate a recommendation where appropriate. A treat- ment determined to be effective (with statistically significant differences between baseline and follow-up scores and�clinical significance based on the MCID applied in the study) was recommended by our panel. If a study found 2 or more treatments to be equally effective based on our threshold, then the panel recommended all equivalently effective treatments.
The EtD Frameworks were completed and recommen- dations were drafted over a series of conference calls with panel members after making judgments about 4 decision domains: quality of evidence (confidence in estimates of effect); balance of desirable (eg, reduced pain and disability) and undesirable outcomes (eg, adverse reactions); confidence about the values and preferences for the target population; and resource implications (costs).56,57 A synthe- sis of our judgments about the domains determined the direction (ie, for or against a management approach) and the strength of recommendations (the extent to which one can be confident that the desirable conse- quences of an intervention outweigh the undesirable consequences). A specific format was followed to formulate recommendations using patient description and the treatment comparator.56 Remarks were added for clarification if needed. If the desirable and undesirable consequences were judged to be evenly balanced and the evidence was not compelling, the panel decided not to write any recommendation.
A modified Delphi technique was used at an in-person meeting to achieve consensus on each recommendation.58 Using an online tool (www.polleverywhere.com), panelists�voted their level of agreement with each recommendation (including quality of evidence and strength of recom- mendation) based on a 3-point scale (yes, no, neutral). Before voting, panelists were encouraged to discuss and provide feedback on each recommendation in terms of suggested wording edits or general remarks. To achieve consensus and be included in the final manuscript, each recommendation had to have at least 80% agreement with a response rate of at least 75% of eligible panel members. All recommendations achieved consensus in the first round.
Peer Review
A 10-member external committee composed of stake- holders, end-users, and researchers from Canada, the United States, and Lebanon (Appendix 2) independently reviewed the draft manuscript, recommendations, and supporting evidence. The AGREE II instrument was used to assess the methodological quality of the guideline.35 Feedback received was collected and considered in a revised draft for a second round of review. Chairs of the guideline panel provided a detailed response to reviewers� comments. For a glossary of terms, please see Appendix 3.
Results
Key Question Development
Thirty-two standardized key questions were developed in line with the PICO (population, intervention, comparator, outcome) format. The panel recognized overlap in content and relevance among some key questions. After combining 3 questions, we ultimately addressed a total of 29 key questions (Table 2).
Study Selection and Quality Assessment: OPTIMa Reviews
OPTIMa searches yield 26 335 articles screened.38-42 After removal of duplicates and screening, 26 273 articles did not meet selection criteria, leaving 109 articles eligible for critical appraisal. Fifty-nine studies (62 articles) published from 2007 to 2013 were deemed scientifically admissible and included in the synthesis (Appendix 4). Each review used was rated as either moderate or high quality (AMSTAR score 8-11).59
Search Update and Study Selection
Our updated search yielded 7784 articles. We removed 1411 duplicates and screened 6373 articles for eligibility (Figs. 1-5). After screening, 6321 articles did not meet our selection criteria (phase 1), leaving 52 articles for full-text review (phase 2) and critical appraisal (studies on the topic of multimodal care (n = 12), structured patient education (n = 3),�exercise (n = 8), work disability interventions (n = 13), manual therapy (n = 4), soft tissues (n = 2), and passive modalities (n = 6). Of the 52 RCTs, 4 scientifically admissible studies were included in our synthesis. The remaining articles failed to address the key question (n = 1); selected population (n = 2), outcomes (n = 13), or intervention (n = 11); had no between estimates (n = 19); or were duplicates (n = 1) or a secondary analysis of an included study (n = 1) (Appendix 5).
Quality Assessment and Synthesis of Results
The GRADE evidence profile and risk of bias within included studies are presented in Tables 3-15 and Appendix 6, respectively.
Recommendations
We present recommendations as follows:
Recent-onset (0-3 months) grades I to III NAD
Recent-onset (0-3 months) grades I to III WAD
Persistent (N3 months) grades I to III NAD
Persistent (N3 months) grades I to III WAD
Recommendations for Recent-Onset (0-3 Months) Grades I to III NAD
Manual Therapy
Key Question 1:Should neck manipulation vs neck mobilization be used for recent-onset (0-3 months) grades I to II NAD?
Summary of Evidence. One RCT by Leaver et al. 60 evaluated the effectiveness of neck manipulation or neck mobilization delivered by physiotherapists, chiropractors, or osteopaths for recent-onset grades I to II neck pain (?2 NRS). All patients received advice, reassurance, or a continued exercise program as indicated for 4 treatments over 2 weeks unless recovery was achieved or a serious adverse event occurred. There was no statistically significant difference in Kaplan-Meier recovery curves between groups for recovery from neck pain and recovery of normal activity, and no statistically significant differences between groups for pain, disability, or other outcomes (function, global perceived effect, or health-related quality of life) at any follow-up point (Table 3).
One other RCT by Dunning et al.61 evaluated the effectiveness of a single high-velocity, low-amplitude (thrust) manipulation (n = 56) directed to the upper cervical spine (C1-C2) and upper thoracic spine (T1-T2) compared with a (nonthrust) mobilization (n = 51) directed to the same anatomical regions for 30 seconds for patients with neck pain. Findings indicated a greater reduction in pain (NPRS) and disability (NDI) in the thrust manipulation group compared with the mobilization at 48 hours. No serious adverse events were reported. Minor adverse events were not collected. This study did not inform our recommendation because1 patient complaints were not recent onset (mean�duration N337 days in both groups), and2 outcomes were measured at 48 hours only. The Guideline Development Group (GDG) considered this an important study limitation because one cannot assume these benefits would have carried on for a longer period. The panel acknowledged, however, that some patients may value obtaining fast pain relief even if temporary.
The panel determined that the overall certainty in the evidence was low, with large desirable relative to undesirable effects. The relative small cost of providing the option would make it more acceptable to stakeholders and feasible to implement. Although the panel decided the desirable and undesirable consequences were closely balanced, the following statement was provided:
Recommendation: For patients with recent (0-3 months) grades I to II NAD, we suggest manipulation or mobilization based on patient preference. (Weak recommendation, low-quality evidence)
Exercise
Key Question 2:Should integrated neuromuscular inhibition technique be used for recent-onset (0-3 months) grades I to II NAD?
Summary of Evidence. Nagrale et al.62 reported non� clinically significant differences for neck pain and disability outcomes at 4 weeks. This study suggested that a soft tissue therapy intervention to the upper trapezius, combining ischemic compression, strain-counterstrain, and muscle energy technique, provides similar clinical benefit compared with muscle energy technique alone. Participants were required to have neck pain of less than 3 months� duration.
The panel determined moderate certainty in the evidence, with small desirable and undesirable effects and no serious adverse events. Low costs are required for the intervention and no specific equipment is needed, with the exception of training to provide the technique. Because the intervention is widely practiced and taught, it is acceptable and feasible to implement. However, its effects on health equities cannot be determined. Overall, the panel decided the balance between the desirable and undesirable consequences was uncertain, and more evidence is needed before a recommendation can be made.
Multimodal Care
Key Question 3:Should multimodal care vs intramuscular ketorolac be used for recent (0-3 months) grades I to III NAD?
Summary of Evidence. McReynolds et al. 63 presented short-term outcomes of pain intensity and concluded that sessions of multimodal care (manipulation, soft tissue techniques) provided equivalent outcomes to an intramuscular injection of ketorolac. However, the follow-up time of 1 hour is generally atypical and the dosing was determined to be incomplete for multimodal care as reported. Furthermore, the study was limited to an emergency setting only.
The panel determined low certainty in the clinical evidence, with small desirable and undesirable effects. There is relatively low risk for multimodal care, considering the reported outcomes were equal. From a clinician standpoint, resources required are small assuming no additional staff are needed. However, one practitioner gave most multimodal therapies. Expenses may vary depending on the definition of multimodal care. This option should not create health inequities, except for those who cannot access clinicians or choose to pay out of pocket, and would be feasible to implement. Professional associ- ations would generally support the option, yet extended multimodal therapies can incur additional costs, which can be unfavorable to both payors and patients. Overall, the balance between the desirable and undesirable conse- quences is uncertain and more research is needed in this area before any recommendation can be made.
Exercise
Key Question 4:Should multimodal care vs home exercises vs medication be used for recent-onset (0-3 months) grades I to II NAD?
Summary of Evidence. One RCT by Bronfort et al.22 evaluated the efficacy of multimodal care over 12 weeks compared with a 12-week home exercise and advice program or medication on neck pain (11-box NRS) and disability (NDI) in 181 adult patients with acute and subacute neck pain (2-12 weeks� duration and a score of ?3 on a 10-point scale). Multimodal care by a chiropractor (mean of 15.3 visits, range 2-23) included manipulation and mobilization, soft tissue massage, assisted stretching, hot and cold packs, and advice to stay active or modify activity as needed. Daily home exercise was to be done up to 6 to 8 times per day (individualized program including self- mobilization exercise of the neck and shoulder joints) with advice by a physical therapist (two 1-hour sessions, 1-2 weeks apart on posture and activity of daily living). Medication prescribed by a physician included nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, opioid analgesic, or muscle relaxants (dosage was not reported). The results displayed in Table 4 indicated that multimodal care and home exercises and advice were as effective as medication in reducing pain and disability at short term (26 weeks). However, medication was associated with a higher risk for adverse events (mostly gastrointestinal symptoms and drowsiness in 60% of participants) than home exercises. The choice of medications was based on the participant�s history and response to treatment. Clinicians and patients should be aware that current evidence is insufficient to determine the effectiveness of long-term opioid therapy for improving chronic pain and function. Importantly, evidence supports a dose-dependent risk for serious harms, including increased risk for overdose, dependence, and myocardial infarction.64
Recommendation: For patients with recent (0-3 months) neck pain grades I to II, we suggest either range-of-motion home exercises, medication, or multimodal manual therapy for reduction in pain and disability. (Weak recommendation, moderate- quality evidence)
Remark: Home exercises included education self-care advice, exercises, and instruction on activities of daily living. Medication included NSAIDs, acetaminophen, muscle relaxant, or a combination of these. Multimodal manual therapy included manipulation and mobilization with limited light soft tissue massage, assisted stretching, hot and cold packs, and advice to stay active or modify activity as needed.
Key Question 5:Should supervised graded strengthening exercises vs advice be used for recent-onset (0-3 months) grade III NAD?
Summary of Evidence. One RCT by Kuijper et al.65 evaluated the effectiveness of supervised strengthening exercises compared with advice to stay active for recent-onset grade III neck pain. This RCT reported that strengthening exercises (n = 70) were more effective than advice to stay active (n = 66).65 Trial participants were followed at 3 weeks, 6 weeks, and 6 months. Based on panel consensus, outcomes determined to be important in the assessment of effectiveness in this RCT included neck and arm pain (VAS) and disability (NDI). These outcomes were both statistically and clinically significant (Table 5).
In this RCT, the strengthening exercise program was delivered by physiotherapists 2 times per week for 6 weeks.65 It included supervised graded strengthening exercises for the shoulder and daily home exercises to strengthen the superficial and deep neck muscles (mobility, stability, and muscle strengthening). Participants in the comparison group were advised to continue daily activities. Both groups were allowed to use painkillers. See Key Question 6 for a recommendation on cervical collar.
Recommendation: For patients with recent (0-3 months) grade III neck and arm pain, we suggest supervised graded strengthening exercises* rather than advice alone.� (Weak recommendation, moderate-quality evidence)
Remark: *Supervised graded strengthening exercises con- sisted of strengthening and stability exercises twice a week for 6 weeks with daily home exercises (which included mobility, stability, and muscle strengthening). �Advice alone consisted of maintaining activity of daily living without specific treatment.
Passive Physical Modalities
Key Question 6:Should cervical collar vs graded strengthening exercise program be used for recent-onset (0-3 months) grade III NAD?
Summary of Evidence. One RCT by Kuijper et al.65 randomly assigned 205 patients with recent-onset neck�cervical radiculopathy (NAD grade III) to 1 of 3 groups 1 : Rest and semi-hard cervical collar for 3 weeks, then weaned off during weeks 3-6 2 ; physiotherapy (mobilizing and stabilizing the cervical spine, standardized graded neck strengthening exercises twice per week for 6 weeks, and education to do daily home exercises); or3 a control group (wait and see with advice to continue daily activities). All patients received written and oral reassurance about the usually benign course of the symptoms and were allowed painkillers.
Wearing a semi-hard cervical collar or receiving standardized graded strengthening exercise program and home exercises for 6 weeks provided similar improvements in arm pain (VAS), neck pain (VAS), or disability (NDI) compared with a wait-and-see policy at 6 weeks. There were no between-group differences at 6 months.
Because of uncertainty about potential for iatrogenic disability associated with the prolonged use of cervical collar,27,42 one recommendation made in the current guideline favoring strengthening exercise programs over advice, and the lack of consensus among the guideline panel, the GDG decided not to make a recommendation against the use of cervical collar (first vote on the proposed recommendation with direct results from the study [11% agree, 11% neutral, 78% disagree, 1 abstained]). A second vote favored also removing the remark from the recommendation (27% agree, 9% neutral, 64% disagree, 1 did not vote). Choice should be based on patient�s preference and management changed if recovery is slow.66
Key Question 7:Should low-level laser therapy be used for recent-onset (0-3 months) grade III NAD?
Summary of Evidence. One RCT by Konstantinovic et al.67 evaluated the effectiveness of low-level laser therapy (LLLT) delivered 5 times per week for 3 weeks compared with placebo (inactive laser treatment) for recent-onset grade III neck pain. LLLT leads to statistically but not clinically significant improvements in neck pain and disability at 3 weeks compared with placebo. Transitional worsening in pain (20%) and persistent nausea (3.33%) were observed in the LLLT group, whereas no adverse events were reported in the placebo group.
The panel determined the overall certainty of the evidence was moderate, with small desirable effects and minor adverse events. LLLT can be expensive. If practitioners choose not to purchase, it may negatively affect health equities. However, the option is acceptable to stakeholders and is relatively easy to implement. The panel was uncertain about the balance between desirable and undesirable consequences and voted against making a recommendation because of a lack of clear evidence (LLLT was no better than placebo but both groups demonstrated within-group change over time).
Work Disability Prevention Interventions
Key Questions 8 and 9:Should work disability prevention interventions vs fitness and strengthening exercise program be used for recent-onset nonspecific work-related upper limb disorders?�Should work disability prevention interventions be used for recent-onset work-related neck and upper limb complaints?
In reviewing the evidence on work disability prevention interventions,41 the GDG concluded that the balance between desirable and undesirable consequences was �closely balanced or uncertain.� As a result, the guideline panel was unable to formulate recommendations for these key questions, yet future research is very likely to either positively or negatively support the various types of work disability prevention interventions.
Although some benefits were reported favoring computer-prompted and instructed exercise interventions,68 the incremental self-reported improvement was insufficient to formulate a recommendation considering1 a follow-up period of 8 weeks in reviewed studies is too short to estimate long-term sustained benefits; and2 the potential costs related to programming and worker instruction may be significant.
Overall, it appears that adding computer-prompted exercises (with workplace breaks), or workplace breaks alone, to a program of ergonomic modification and education improves self-perceived recovery and symptomatic benefits in computer workers with neck and upper back complaints.41 However, it is unclear whether the addition of computer- prompted exercises to the various established workplace interventions alters perceived or objective health outcomes. Future research may identify added benefits in order for stakeholders to consider the extra cost as being surmountable.
Recommendations for Recent-Onset (0-3 Months) Grades I to III WAD
Multimodal Care
Key Question 10:Should multimodal care vs education be used for recent (0-3 months) grades I to III WAD?
Summary of Evidence. A 2-part RCT by Lamb et al.69 evaluated the effectiveness of oral advice compared with written material for improving pain (self-rated neck pain) and disability (NDI) in patients with recent-onset grades I to III WAD. Lamb et al.69 included a total of 3851 participants with a history of WAD grades I to III of less than 6 weeks� duration who sought treatment at an emergency department. A total of 2253 participants received active management advice in the emergency department incorporating oral advice and the Whiplash Book, which included reassurance, exercises, encouragement to return to normal activities, and advice against using a collar;�1598 participants received usual care advice, including verbal and written advice along with anti-inflammatory medication, physiotherapy, and analgesics. No between-group difference was observed in self-rated neck pain and disability at 12-month follow-up and no difference in workdays lost was observed at 4-month follow-up (Table 6).
Lamb et al.69 included 599 participants with WAD grades I to III that persisted for 3 weeks after attending emergency departments. Three hundred participants were treated by a physiotherapist (maximum 6 sessions over 8 weeks) including psychological strategies (goal setting or pacing, coping, reassurance, relaxation, pain and recov- ery), self-management advice (posture and positioning), exercises (shoulder complex mobilization and range of motion [ROM]; cervical and scapular stability and proprioception), and cervical and thoracic spine Maitland mobilization and manipulation; a total of 299 received single-session reinforcement advice from a physiothera- pist during their previous visit to emergency department. No difference in self-rated disability was identified at 4-month follow-up; however, greater reductions in workdays lost after 8-month follow-up were determined with self-management advice over single-session rein- forcement. Similar findings were found in an earlier study.70
Recommendation: For adult patients with recent (0-3 months) WAD grades I to III, we suggest multimodal care over education alone. (Weak recommendation, moderate-quality evidence)
Remark: Multimodal care may consist of manual therapy (joint mobilization, other soft tissue techniques), education, and exercises.
Structured Education
Key Question 11:Should structured patient education vs education reinforcement be used for recent-onset (0-3 months) WAD?
Summary of Evidence. Lamb et al.69 reported outcomes at 4 months for self-rated disability, identifying no clinically significant differences between groups. The study sug- gested that oral advice and an educational pamphlet provide similar benefits.
The panel determined moderate quality in the clinical evidence, yet uncertain desirable effects with small, minor, and transient adverse events. Relatively few resources would be required for the intervention, and wide dissemination of educational materials through electronic tools can help reduce inequities. The option is acceptable to stakeholders and feasible to implement. Overall, the desirable consequences probably outweigh the undesirable consequences. The panel determined this topic and its evidence has substantial overlap with Key Question 10. Therefore, one recommendation was made, addressing both topics.
Recommendations for Persistent (N3 Months) Grades I to III NAD
Exercise
Key Question 12:Should supervised exercise (ie, qigong exercise) vs no treatment (wait listing) be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. Two RCTs (Table 7) evaluated the effectiveness of supervised qigong compared with super- vised exercise therapy and no treatment on neck pain (101-point VAS), disability (NDI), and Neck Pain and Disability Scale in a total of 240 patients with chronic neck pain (N6 months). 71,72 Rendant et al. 72 reported that, in adults with chronic neck pain, supervised qigong is more effective than no treatment and as effective as exercise therapy in reducing neck pain and disability at 3 and 6 months. Conclusions regarding the effectiveness of these 2 interventions compared with no treatment in patients aged older than 55 years cannot be drawn from the included studies.
In their study of these interventions for neck pain in elderly patients, von Trott et al.71 observed a reduction in pain and disability in both intervention groups at 3 and 6 months (although not statistically significant). The quality of the evidence was downgraded to low based on the SIGN criteria (concealment method not reported). In the von Trott et al. study, the interventions consisted of two 45-minute sessions per week for 3 months (a total of 24 sessions),71 whereas in the Rendant et al. study, interventions consisted of 12 treatments in the first 3 months and 6 treatments in the following 3 months (total of 18 sessions).72 Exercise therapy in both studies included repeated active cervical rotations and strengthening and flexibility exercises in the form of Dantian qigong71 or Neiyanggong qigong.72 Similar minor transient side effects were reported in both the intervention and comparison groups.
Recommendation: For adult patients with persistent (N6 months) neck pain grades I to II, we suggest supervised group exercises* to reduce neck pain and disability. (Weak recommendation, moderate-quality evidence)
Remark: Patients received 18 to 24 group sessions during a period of 4 to 6 months. Patients considered had a rating of 40/100 on a pain scale (VAS). The intervention group reached suggested MCID level of 10% difference for pain and functional outcomes. *Exercises included qigong or ROM, flexibility, and strengthening exercises. No evidence of significant effect in the elderly population.
Key Question 13:Should supervised yoga vs education be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. Yoga is an ancient Indian practice involving postural exercises, breathing control, and med-
itation. 20 One RCT by Michalsen et al. 73 evaluated the effectiveness of Iyengar yoga compared with a self-care/exercise program on neck pain (VAS) and disability (NDI) in 76 patients with chronic neck pain (pain for at least 3 months and a score of more than 40 mm on a 100-mm VAS). Yoga consisted of a weekly 90-minute session for 9 weeks of a wide range of postures aimed to enhance flexibility, alignment, stability, and mobility. The self-care/ exercise group had to practice for 10 to 15 minutes at least 3 times a week a series of 12 exercises focusing on muscle stretching and strengthening and joint mobility. The results indicated that yoga is more effective for reducing neck pain and disability at short term (4 and 10 weeks) than self-care/ exercise (Table 8). No serious adverse events were reported in either group. In this study, the quality of evidence was downgraded to low because blinding was �poorly ad- dressed.�45
One RCT by Jeitler et al.74 evaluated the effectiveness of Jyoti meditation compared with exercise on neck pain (VAS). The results showed that Jyoti meditation (sitting motionless, repeating a mantra, and visual concentration while keeping the eyes closed) is more effective than exercise (established and previously used self-care manual for specific exercise and education for chronic neck pain).74 Because Jyoti meditation only includes 1 of the 3 components of yoga (ie, meditation), Jeitler et al.74 was not considered in developing the following recommendation.
Recommendation: For patients with persistent (N3 months) grades I to II neck pain and disability, we suggest supervised yoga over education and home exercises for short- term improvement in neck pain and disability. (Weak recommendation, low-quality evidence)
Remark: Baseline intensity of pain was more than 40/100 and duration was at least 3 months. Yoga was specific to the Iyengar type, with a maximum of 9 sessions over 9 weeks.
Key Question 14:Should supervised strengthening exercises vs home ROM or stretching exercises be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. Three RCTs evaluated the effectiveness of supervised strengthening exercises compared with home exercises for grades I to II neck pain and disability.38 Two RCTs (Hakkinen et al.75 and Salo et al.76) reported no significant between group differences at 1 year for primary or secondary outcomes. One RCT (N = 170) reported that supervised strengthening exercises were more effective than home ROM exercises.77 Two smaller RCTs (N = 107) found that both treatments are equally effective.75,76 All 3 trials had a follow-up of 1 year. Based on our panel�s consensus, outcomes determined to be important in the assessment of effectiveness for these RCTs included pain (NRS) and disability (NDI).
In the RCT by Evans et al.77 the strengthening exercise program (delivered by exercise therapists) was determined to be more effective than home exercises. The program�included 20 supervised sessions over a period of 12 weeks and consisted of neck and upper body dynamic resistance strengthening program with and without spinal manipula- tive therapy.77 Conversely, the home exercises included an individualized program of neck and shoulder self- mobilization with initial advice regarding posture and daily activities (Table 9). In the 2 RCTs demonstrating equivalence, the strengthening program included 10 supervised sessions over 6 weeks of isometric exercises for the neck flexors and extensors, dynamic shoulder and upper extremity exercises, abdominal and back exercises, and squats.43,44
A fourth RCT by Maiers et al.78 assessed the effectiveness of supervised rehabilitative exercises in combination with and compared with home exercises alone for persistent neck pain in individuals aged 65 years or older. All participants in the study received 12 weeks of care. One group received 20 supervised 1-hour exercise sessions in addition to home exercises. Home exercises consisted of four 45- to 60-minute sessions to improve flexibility, balance, and coordination and enhance trunk strength and endurance. Participants also received instruc- tions on pain management, practical demonstrations of body mechanics (lifting, pushing, pulling, and rising from a lying position), and massaging to stay active. Results favored supervised rehabilitative exercises combined with home exercises over home exercise for pain (NRS) and disability (NDI) at 12 weeks. However, between-group differences did not reach statistical significance.
Recommendation: For patients with persistent (N3 months) grades I to II neck pain, we suggest supervised strengthening exercises or home exercises. (Weak recommendation, low-quality evidence)
Remark: For reduction in pain, supervised strength- ening exercises, provided along with ROM exercises and advice, were evaluated at 12 weeks within 20 sessions. Home exercises include stretching or self-mobilization.
Key Question 15:Should strengthening exercises vs general strengthening exercises be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. Griffiths et al.79 presented non� clinically significant outcomes for neck pain and disability among patients with persistent neck pain and concluded there is no added benefit of incorporating specific isometric exercise to a general exercise program. Dosages were up to 4 sessions per 6-week period, with advice for 5 to 10 times at home. The general exercise program consisted of postural exercise, active ROM, 5 to 10 times daily with reinforcement.
The panel determined there is low certainty in the clinical evidence and uncertainty in the desirable effects of the intervention. Isometric exercises have little anticipated adverse effects, require minimal resources, and are generally acceptable to stakeholders and feasible to�implement. Yet uncertainty remains regarding their effects on health equity and the overall balance between desirable and undesirable consequences. More research is needed in this area before a recommendation can be made.
Key Question 16:Should combined supervised strengthening, ROM, and flexibility exercises vs no treatment (wait listing) be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. von Trott et al. 71 and Rendant et al. 72 presented significant outcomes for reduction in neck pain and disability that favor combined strengthening, ROM, and flexibility exercises. Both studies address different popula- tions and lead to similar outcomes (von Trott et al.71 addressed elderly populations).
The panel determined there was moderate certainty in the clinical evidence, with large desirable and small undesirable anticipated effects. Yet there may be differences in adverse events for strengthening vs ROM and flexibility exercises, along with the chal- lenges of such adverse events being self-reported. For example, strengthening exercises likely coincide with short-term pain after the intervention. Further, signifi- cant space may be required for exercises, which may incur large costs that need to be considered up front. As a result, there is uncertainty about the feasibility to implement and whether this could widely affect health inequalities. However, the option would be acceptable to stakeholders. Overall, the desirable consequences would probably outweigh the undesirable consequences. The panel determined this topic and its evidence has substantial overlap with Key Question 12 (qigong was considered exercise). Therefore, 1 recommendation was made, addressing both topics.
Manual Therapy
Key Question 17:Should multimodal care vs self-management be used for persistent (N3 months) grades I-II NAD?
Summary of Evidence. One RCT by Gustavsson et al.80 evaluated the effectiveness of self-management of persis- tent musculoskeletal tension type neck pain for grades I to II neck pain. They compared treatment effects of a multicom- ponent pain and stress self-management group intervention (n = 77) to individually administered multimodal physical therapy (n = 79). Measures of pain (NRS) and disability (NDI) were collected at baseline and at 10 and 20 weeks. Both groups had within-group differences for decreased pain intensity and disability. At the 20-week follow-up after an average of 7 sessions, based on the measures used, the multicomponent pain and stress self-management group intervention had a greater treatment effect on coping with pain and patients� self-reported pain control and disability than the multimodal care group. The initial treatment effects were largely maintained over a 2-year follow-up period (Table 10).81
Recommendation: For patients with persistent (N3 months) neck pain and associated disorders grades I to II, we suggest multimodal care* or stress self-management� based on patient preference, prior response to care, and resources available. (Weak recommendation, low-quality evidence)
Remark: *Individualized multimodal care may include manual therapy (manipulation, mobilization, massage, trac- tion), acupuncture, heat, transcutaneous electrical nerve stimulation, exercise, and/or ultrasound. �Stress self-manage- ment may include relaxation, balance and body awareness exercises, pain and stress self-management lectures, and discussion. The multimodal care group received an average of 7 (range 4-8) sessions, compared with 11 (range 1-52) sessions for the stress self-management group over 20 weeks.
Education
Key Question 18:Should structured patient education vs massage therapy be used for persistent (N3 months) NAD?
Summary of Evidence. Sherman et al.82 reported non� clinically significant outcomes at 4 weeks for disability. This study suggests a mailed self-care book and a course in massage therapy provide similar clinical benefits for
patients with persistent neck pain.
The panel determined the overall certainty of the evidence was low, with relatively large anticipated effects and no serious adverse events noted from intervention (some headaches possibly). There is uncertainty in the costs required, including necessary staff, equipment, and mate- rials. Yet this option is feasible to implement in most settings and has strong implications for reducing health inequities. As a preventive strategy, the intervention is acceptable to stakeholders, including the chiropractic practitioners, patients, and policymakers. The panel was uncertain about the balance between the desirable and undesirable consequences. Additional high-quality studies are needed in this area before any recommendation can be made.
Manual Therapy
Key Question 19:Should manipulation be used for persistent grades I to II NAD?
Summary of Evidence. Evans et al.77 compared spinal manipulation in addition to 20 weeks of supervised exercise therapy (20 sessions) to supervised exercise therapy alone in adults with persistent grades I to II neck pain, whereas Maiers et al.78 compared spinal manipulation in addition to home exercises (20 sessions maximum) to home exercise alone in seniors with persistent grades I to II neck pain. Pain and disability outcomes at 12 and 52 weeks did not reach statistical significance in between-group differences, except for pain level at 12 weeks in the Maiers study.78 A third RCT by Lin et al.83 allocated 63 persistent neck pain patients (NAD I-II) to the experimental group (n = 33) treated with�cervical spine manipulation and traditional Chinese massage (TCM) compared with TCM alone (n = 30) over 3 weeks. Results favored cervical manipulation with TCM over TCM alone for pain (NPS) and disability (Northwick Park Neck Disability Questionnaire) at 3 months (Table 11).
The panel concluded low certainty in the evidence, with small desirable and undesirable effects of the intervention. Few resources are required for the intervention, and it is probably acceptable to stakeholders and feasible to implement. Although the panel decided the desirable and undesirable consequences were closely balanced, the following statement was provided.
Recommendation: For patients with persistent grades I to II NAD, we suggest manipulation in conjunction with soft tissue therapy. (Weak recommendation, low-quality evidence)
Remark: Evaluated after eight 20-minute sessions (over a 3-week period). Does not include manipulation as a standalone treatment.
Manual Therapy
Key Question 20:Should massage vs no treatment (wait listing) be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. Sherman et al.82 and Lauche et al.84 reported non�clinically significant differences in outcomes for disability at 4 and 12 weeks, respectively. Sherman et al.82 suggested Swedish and/or clinical massage with verbal self- care advice provides similar clinical benefit to a self-care book for disability outcomes. Lauche et al.84 suggested cupping massage and progressive muscle relaxation lead to similar changes in disability. Sherman et al.85 reported outcomes for neck pain and disability at 4 weeks and suggested that higher doses of massage provide superior clinical benefit (Table 12).
The panel determined low certainty in the evidence, with small desirable and undesirable effects. Additional costs may be needed to get clinical benefit. Sherman et al.85 suggested a minimum of 14 hours of staff time needed. Because of the costs associated with high-dose massage, it may not be entirely acceptable to patients or payors. However, this option is feasible and relatively easy to implement in educated and affluent populations similar to subjects primarily studied.85 Overall, the panel decided the desired consequences probably outweigh the undesirable consequences and suggest offering this option.
Recommendation: For patients with persistent (N3 months) grades I to II NAD, we suggest high-dose massage over no treatment (wait listing) based on patient preferences and resources available. (Weak recommendation, low-quality evidence)
Remark: Interventions were given 3 times for 60 minutes a week for 4 weeks. Lower dosages and duration did not have therapeutic benefit, and we cannot suggest offering as an option.
Passive Physical Modalities
Key Question 21:Should LLLT be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. After full-text screening and review, no studies addressing between-group differences among outcomes of pain or disability were included to inform this key question. The lack of evidence and uncertainty in the overall balance between desirable and undesirable consequences led the panel to decide not to write a recommendation for this topic at this time. More high-quality studies are needed in this area before certainty in judgments or recommendations can be made.
Key Question 22:Should transcutaneous electrical nerve stimulation vs multimodal soft tissue therapy program be used for persistent (N3 months) grades I to II NAD?
Summary of Evidence. After full-text screening and review, no studies addressing between-group differences among outcomes of pain or disability were included to inform this key question. The lack of evidence and uncertainty in the overall balance between desirable and undesirable consequences led the panel to decide not to write a recommendation for this topic at this time. More high quality studies are needed in this area before certainty in judgments or recommendations can be made.
Key Question 23:Should cervical traction be used for grade III NAD (variable duration)?
Summary of Evidence. After full-text screening and review, no studies addressing between-group differences among outcomes of pain or disability were included to inform this key question. The lack of evidence and uncertainty in the overall balance between desirable and undesirable consequences led the panel to decide not to write a recommendation for this topic at this time. More high-quality studies are needed in this area before certainty in judgments or recommendations can be made.
Multimodal Care
Key Question 24:Should multimodal care vs continued practitioner care be used for persistent grades I to III NAD?
Summary of Evidence. One RCT by Walker et al.86 evaluated the effectiveness of multimodal care for neck pain with or without unilateral upper extremity symptoms (grades I-III). They compared treatment effects of combined multimodal care and home exercises (n = 47) to multimodal minimal intervention (n = 47). Both intervention groups received on average of 2 sessions per week for 3 weeks. No interventions were rendered after 6 weeks. Baseline self- reported questionnaires included neck and arm pain (VAS) and disability (NDI). All measures were repeated at 3, 6, and 52 weeks. Patients in the multimodal care and home exercise group had significantly greater reduction in short-term neck pain and in short-term and long-term disability compared with the multimodal minimal interven- tion group (Table 13). A secondary analysis of the Walker et al. study87 determined that patients receiving both�cervical thrust and nonthrust manipulations did no better than the group receiving cervical nonthrust manipulations only. This underpowered secondary analysis prohibits any definitive statement regarding the presence or absence of a treatment advantage of one approach over the other. The reduction in pain reported by Walker�s multimodal care and exercise group compared favorably to the change scores reported by other studies, including Hoving et al.88,89
In an RCT, Monticone et al.90 evaluated the effective- ness of multimodal care for persistent neck pain. They compared treatment effect of multimodal care alone (n = 40) to multimodal care in conjunction with cognitive behavioral treatment (n = 40). Both groups had a reduction in pain (NRS) and disability (NPDS), but there were no clinically significant differences between the groups at 52 weeks. The addition of a cognitive behavioral treatment did not provide greater outcomes than multimodal care alone.
Recommendation: For patients presenting with persistent neck pain grades I to III, we suggest clinicians offer multimodal care* and/ or practitioner advice based on patient preference. (Weak recommendation, low-quality evidence)
Remark: *Multimodal care and exercises may consist of thrust/nonthrust joint manipulation, muscle energy, stretching, and home exercises (cervical retraction, deep neck flexor strengthening, cervical rotation ROM). �Multimodal minimal intervention may consist of postural advice, encouragement to maintain neck motion and daily activities, cervical rotation ROM exercise, instructions to continue prescribed medication, and therapeutic pulsed (10%) ultrasound at 0.1 W/cm2 for 10 minutes applied to the neck and cervical ROM exercises.
Exercise
Key Question 25:Should group exercises vs education or advice be used for workers with persistent neck and shoulder pain?
Summary of Evidence. We have combined the key questions for �Should structured patient education vs exercise programs be used for persistent neck pain and associated disorders in workers?� and �Should workplace-based exercises vs advice be used for neck pain in workers?� One large cluster RCT (n = 537) by Zebis et al.91 evaluated the effectiveness of strength training in the workplace compared with receiving advice to stay physically active on nonspecific neck and shoulder pain intensity. The findings indicated a similar reduction in neck and shoulder pain intensity at 20 weeks for the exercise program compared with advice (Table 14). The intervention consisted of 3 sessions per week, each lasting 20 minutes, for up to 20 weeks (total of 60 sessions).
The workplace exercise program consisted of high- intensity strength training relying on principles of progres- sive overload and involved local neck and shoulder muscles strengthening with 4 different dumbbell exercises and 1 exercise for the wrist extensor muscles. More than 15% of�workers assigned to the workplace exercise group reported minor and transient complaints. The comparison group reported no adverse events.
A subgroup analysis92 of the primary Zebis et al. study91 included 131 women with a baseline neck pain rating of at least 30 mm VAS from the 537 male and female participants. Results favored specific resistance training over advice to stay active for pain (VAS) at 4 weeks. This study was not included because findings were already considered in the primary study.
Recommendation: For workers with persistent neck and shoulder pain, we suggest mixed supervised and unsupervised high- intensity strength training or advice alone. (Weak recommendation, moderate-quality evidence)
Remark: For reduction in pain intensity, 3 sessions per week, each lasting 20 minutes, over a 20-week period. Exercise includes strengthening. Extra resources are likely required for complete exercise intervention implementation.
Structured Patient Education
Key Question 26:Should structured patient education vs exercise programs be used for persistent (N3 months) NAD in workers?
Summary of Evidence. Andersen et al.93 reported non� clinically significant outcomes at 10 weeks for neck and shoulder pain, suggesting weekly e-mailed information on general health behaviors and shoulder abduction exercise programs provide similar clinical benefit. Yet implementa- tion of high-intensity strength training exercises in industrial workplaces (implementation of exercise into day-to-day life and to increase active leisure time) is generally supported.94,95 In another RCT, pain reduction was significantly greater than in the group receiving advice alone. 91 Findings from Zebis et al. 91 are also included in the exercise intervention section of this guideline.
The panel determined moderate certainty in the clinical evidence, with small desirable and undesirable effects of the intervention. The resources required are relatively small, assuming the practitioner presents the education to the patient. Health inequities would be positively affected, and the intervention would be acceptable to stakeholders and feasible to implement. The panel decided not to repeat these findings in the current section. The panel felt that the benefits of increasing the frequency and intensity of exercise regimes was not restricted to those working in an industrial environment or to any specific population subgroup with the exception of older adults.
Work Disability Prevention Interventions
Key Questions 27-29:Should work-based hardening vs clinic-based hardening be used for persistent (N3 months) work-related rotator cuff tendinitis? Should work disability prevention interventions be used for persistent neck and shoulder pain?�Should work disability prevention interventions be used for persistent (N3 months) upper extremity symptoms?
Summary of Evidence. In reviewing the evidence on work disability prevention interventions,41 the GDG concluded that the balance between desirable and undesirable consequences was �closely balanced or uncertain� for Key Questions 27-29. As a result, the guideline panel was unable to formulate recommendations for these key questions, yet future research is very likely to either positively or negatively support the various types of work disability prevention interventions.
Recommendations for Persistent (N3 Months) Grades I to III WAD Exercise
Key Question 30:Should supervised general exercise and advice vs advice alone be used for persistent (N3 months) grades I to II WAD?
Summary of Evidence. In an RCT, Stewart et al. (2007)96 evaluated the effectiveness of 3 advice sessions alone compared with 3 advice sessions combined with 12 exercise sessions over 6 weeks on neck pain (NRS) and disability�(NDI) among 134 patients with persistent grades I to II WAD. The results, presented in Table 15, indicated that supervised exercises with advice are as effective as advice alone at long term (12 months). Advice included standardized education, reassurance, and encouragement to resume light activity and consisted of 1 consultation and 2 follow-up phone contacts. However, the quality of the evidence was downgraded to low based on SIGN criteria (randomization and outcome measurement were �poorly addressed�) and the low number of participants and events.45
A pragmatic trial assigned 172 patients with persistent WAD grades I to II to receive a comprehensive 12-week exercise program (20 sessions including manual therapy technique the first week [no manipulation] and cognitive behavioral therapy delivered by physiotherapists) or advice (1 session and telephone support).97 The comprehensive exercise program was not more effective than advice alone for pain reduction or disability, although findings favored a comprehensive physiotherapy exercise program over advice.
The panel determined low certainty in the evidence, with small desirable and undesirable effects and no serious adverse events (5 patients who received the comprehensive exercise program and 4 who received advice had minor transient adverse events). Overall, the panel decided the balance between the desirable and undesirable conse- quences such as costs was uncertain, and more evidence is needed before a recommendation can be made.
In a 20-week cluster RCT, Gram et al. (2014)98 randomly assigned 351 office workers to 2 training groups receiving the same total amount of planned exercises 3 times per week, with 1 group supervised throughout the intervention period and the other receiving minimal supervision only initially, and a reference group (without exercise). Although results indicated that supervised training at the workplace reduced neck pain, results were not clinically significant and both training groups improved independently of the extent of supervision. The panel decided not to consider this study in formulating a recommendation because exercise was not directly com- pared with advice and an important loss to follow-up occurred across groups. Although supervised exercise appears to be beneficial, costs can be high. This could possibly be mitigated, however, by offering group treat- ment, which may increase compliance and accountability with a supervised group.
Recommendation: For patients with persistent (N3 months) grades I to II WAD, we suggest supervised exercises with advice or advice alone based on patient preference and resources available. (Weak recommendation, low-quality evidence)
Remark: Extra resources may be required for supervised exercises.
Multimodal Care
Key Question 31:Should multimodal care vs self- management program be used for persistent (N3 months) grade II WAD?
Summary of Evidence. Jull et al.99 reported no clinically or statistically significant outcomes for pain and disability at 10 weeks. They suggested that multimodal care (exercises, mobilization, education, and ergonomic advice) provided similar outcomes to a self-management program based on an educational booklet (mechanism of whiplash, reassur- ance of recovery, stay active, ergonomic advice, exercise). Care did not include high-velocity manipulation. Although this study is specific to physiotherapists, it is well within the scope of chiropractors (manual therapists).
One other RCT by Jull et al.100 evaluated the effectiveness of multidisciplinary individualized treat- ments for patients with acute whiplash (b4 weeks postinjury). Patients randomly assigned to pragmatic intervention (n = 49) could receive medication including opioid analgesia, multimodal physiotherapy, and psy- chology for post-traumatic stress over 10 weeks. No significant differences in frequency of recovery (NDI ? 8%) between pragmatic and usual care groups was found at 6 or 12 months. There was no improvement in current nonrecovery rates at 6 months (63.6%, pragmatic care; 48.8%, usual care), indicating no advantage of the early multiprofessional intervention.
The panel determined low certainty in the clinical evidence, with small desirable and undesirable effects reported. Yet there were relatively small costs and resources required to implement the intervention. Electronic dissem- ination of the educational component of multimodal care may reduce health inequities. The option may be acceptable to clinicians (assuming collaborative care approaches), policymakers, and patients and is likely feasible to implement in usual care settings. Overall, the balance between the desirable and undesirable consequences is uncertain, and no recommendation is given at this time. Further studies need to be conducted in this area and should involve multimodal care including high-velocity proce- dures or manipulation.
Education
Key Question 32:Should structured patient education vs advice be used for persistent (N3 months) WAD?
Summary of Evidence. Stewart et al. (2007)96 reported non�clinically significant between differences for pain and disability outcomes at 6 weeks. This study suggested that adding a physiotherapy-based graded exercise program to a structured advice intervention provided similar clinical benefit as structured education alone.
The panel determined low certainty of the evidence, with low desirable and undesirable anticipated effects. The main complaints were muscle pain, knee pain, and spinal pain with mild headaches.96 The small resources required for the intervention may reduce health inequities, and the option is acceptable to stakeholders and feasible to implement in most settings.
The panel determined that this key question had substantial overlap with Key Question 5 and decided to make 1 recommendation addressing both topics.
Discussion
This evidence-based guideline establishes the best practice for the management of NAD and WAD resulting from or aggravated by a motor vehicle collision and updates 2 previous guidelines on similar topics.24,25 This guideline covers recent-onset (0-3 months) and persistent (N3 months) NADs and WADs grades I to III. It does not cover the management of musculoskeletal thoracic spine or chest wall pain.
The primary outcomes reported in the selected studies were neck pain intensity and disability. Although all recommendations included in this guideline are based on low risk of bias RCTs, the overall quality of evidence is generally low considering other factors considered by GRADE such as imprecision, and thus the strength of recommendations is weak at this time. Weak recommen- dations mean that clinicians need to devote more time to the process of shared decision making and ensure that the informed choice reflects patient values and preferences.56 Interventions not described in this guideline cannot be recommended for the management of patients with NAD or WAD because of a lack of evidence about their effective- ness and safety (Table 16).
A recent systematic review and meta-analysis by Wiangkham (2015)101 on the effectiveness of conservative management for acute WAD grade II included 15 RCTs, all assessed as high risk of bias (n = 1676 participants), across 9 countries. Authors concluded that conservative interven- tions (noninvasive treatment), including active mobilization exercises, manual techniques, physical agents, multimodal therapy, behavioral approaches, and education, are gener- ally effective for recent-onset WAD grade II to reduce pain in the medium and long term and to improve cervical ROM in the short term compared with standard or control intervention.101 Although findings from the Wiangkham review are generally in line with those from the systematic reviews we included in this guideline,24,25 the pooling of high risk of bias and of clinically heterogeneous trials seriously challenges the validity of this more recent review.
Similarities and Differences With Recommendations by the OPTIMa Collaboration
First, the recommendations for the management of minor injuries of the neck were recently released by the Ministry�of Finance of Ontario in collaboration with the OPTIMa Collaboration 20 and published as a separate guideline. 27 They considered the risks of bias of included RCTs using the SIGN criteria45 and the guideline recommendations developed using the modified OHTAC framework,28 based on 3 decision determinants1: overall clinical benefit (evidence of effectiveness and safety) 2 ; value for money (evidence of cost-effectiveness where available); and3 consistency with expected societal and ethical values. In the current guideline, we used the GRADE approach, which, in addition to considering risk of bias of included RCTs, takes into account 4 other factors (imprecision, inconsistency, indirectness, publication bias) to rate the confidence in effect estimates (quality of evidence) for each outcome.102 As a result of imprecision of estimates in several RCTs, the overall quality of admissible studies was deemed low. GRADE considers similar decision determi- nants as the modified OHTAC to develop recommendations when subsequently making an overall rating of confidence in effect estimates across all outcomes based on those outcomes considered critical to a particular recommenda- tion.56 Accordingly, the guideline panel was asked to consider this low quality of evidence when judging the �desirable� consequences. When the benefits of important outcomes slightly outweighed undesirable effects of the intervention, a weak recommendation was made (ie, suggestions for care). This is likely to involve ensuring patients understand the implications of the choices they are making, possibly using a formal decision aid.56 However, if the judgment was �closely balanced or uncertain,� no recommendation could be made.
Second, OPTIMa 20 recommended that interventions should only be provided in accordance with published evidence for effectiveness, including parameters of dosage, duration, and frequency, and within the most appropriate phase. The emphasis during the early phase (0-3 months) should be on education, advice, reassurance, activity, and encouragement. Health care professionals should be encouraged to consider watchful waiting and clinical monitoring as evidence-based therapeutic options during the acute phase. For injured persons requiring therapy, time-limited and evidence-based interventions should be implemented on a shared decision-making basis, an approach that equally applies to patients in the persistent phase (4-6 months). Despite using slightly different methods to derive recommendations, the 2 processes generally led to similar guidance.
Third, OPTIMa20 reported that the following interven- tions are not recommended for recent-onset NAD: struc- tured patient education alone (either verbal or written); strain-counterstrain or relaxation massage; cervical collar; electroacupuncture (electrical stimulation of acupuncture points with acupuncture needles or electrotherapy applied to the skin), a topic not covered in our guideline; electric muscle stimulation; heat (clinic based). Similarly for�persistent NAD, programs solely of clinic-based supervised high-dose strengthening exercises, strain-counterstrain or relaxation massage, relaxation therapy for pain or disability outcomes, transcutaneous electrical nerve stimulation (TENS), electric muscle stimulation, pulsed shortwave diathermy, heat (clinic based), electroacupuncture, and botulinum toxin injec- tions are not recommended. In contrast, based on the RCT by Zebis et al.91 the current guideline suggests offering multimodal care and/or patient education for industrial workers presenting with neck pain grades I to III. Although structured patient education used alone cannot be expected to yield large benefits for patients with neck pain, this strategy may be of benefit during the recovery of patients with persistent WAD when used as an adjunct therapy.40 For persistent neck pain (grades I-II), Gustavsson et al.80 reported that multimodal care combining manual therapy (spinal manipulation, mobilization, massage, traction) and passive modalities (heat, TENS, exercise, and/or ultrasound) reduced neck disability. It should be noted, however, that past reviews were unable to make any definitive conclusions about the effectiveness of TENS as an isolated treatment for acute pain 103 or chronic pain 104 in adults, nor about the effectiveness of heat therapy.105,106
A comparison of the recommendations with 2 previous chiropractic guidelines 24,25 reveals that a multimodal approach including manual therapy, advice, and exercise remains the overall recommended strategy of choice for the treatment of neck pain. However, treatment modalities included in recommended multimodal care differed accord- ing to the quality of the evidence available at the time. The 2010 guideline on the management of WAD developed treatment recommendations based on low-quality evidence from 8 available RCTs and 3 cohort studies.25 Overall, recommendations for recent and persistent WAD are similar (multimodal care, and supervised exercise and multidisciplinary care, respectively). The 2014 guideline on neck pain24 developed 11 treatment recommendations from 41 RCTs. The current guideline developed 13 recommenda- tions from 26 low risk of bias RCTs. In line with the 2014 guideline24 for recent-onset neck pain, the current recom- mendations suggest offering multimodal care including mobilization, advice, and exercises. The current guideline recommendations also suggest offering supervised graded strengthening and stability exercises. Similar to the 2014 guideline for persistent neck pain (grades I-II),24 the current recommendations suggest offering multimodal care consisting of manual therapy (spinal manipulation therapy or mobilization) and exercises. Details on specific exercise modalities are now provided, including suggestions for supervised and unsuper- vised exercises, strength training, and supervised group exercises such as workplace exercise programs and supervised yoga.
Adverse Events
This guideline did not specifically review the evidence on adverse events from treatments. However, in the review�by Wong et al.42 on manual therapy and passive modalities, 22 of the low risk of bias RCTs addressed the risk of harm from conservative care. Most adverse events were mild to moderate and transient (mostly increased stiffness and pain at the site of treatment, with a mean rate of about 30%). No serious neurovascular adverse events were reported. Another review of published RCTs and prospective cohort studies confirmed that around half of people treated with manual therapy can expect minor to moderate adverse events after treatment, but that the risk of major adverse events is small.107 The pooling of data from RCTs of manual therapy on the incidence of adverse events indicated that the relative risk of minor or moderate adverse events was similar for manual therapy and exercise treatments, and for sham/passive/control interventions.
A patient-centered holistic and collaborative view of the needs of the patient with pain and disability is encouraged. 108,109 Although chiropractors are not responsible for pharmacologic management, they should have sufficient knowledge about pharmacologic agents and their adverse events. One eligible RCT22 found home exercises and advice to be as effective as medication (acetaminophen, NSAIDs, muscle relaxant, and opioid analgesic) in reducing pain and disability at short term for patients with acute or subacute neck pain grades I to II. However, medication was associated with a higher risk for adverse events. Of interest, recent evidence suggests that acetaminophen is not effective for managing low back pain,110,111 and the effectiveness of long-term opioid therapy for improving chronic pain and function is uncertain.64 However, a dose-dependent risk for serious harms is associated with long-term use of opioid (increased risk for overdose, opioid abuse and dependence, fractures, myocardial infarction, and use of medications to treat sexual dysfunction).64 Risk of unintentional opioid overdose injury appears to be particularly important in the first 2 weeks after initiation of long-acting agents.112,113
Recommendations
I. Stakeholders
Choosing a Care Provider. A range of health care providers (chiropractors, general medical practitioners, physiothera- pists, registered massage therapists, and osteopaths) deliver care for NADs and WADs.108,114 Considering the level of skills required to deliver manual therapy, including spinal manipulative therapy and other forms of therapies (eg, prescription of specific exercise) and based on individual patient preference, cervical spine manipulation as part of multimodal care should be delivered by properly trained licensed professionals. 115
II. Practitioners
Best Practice Recommendations-Initial Assessment and Monitoring.
This guideline specifically addresses the treatment of NAD and WAD grades I to III. Importantly, our panel supports�the following 5 best practice recommendations on patients care outlined in the OPTIMa guideline27: Clinicians should1 rule out major structural or other pathologic conditions as the cause of neck pain�associated disorders before classifying as grade I, II, or III2; assess prognostic factors for delayed recovery3; educate and reassure patients about the benign and self-limited nature of the typical course of NAD grades I to III and the importance of maintaining�activity and movement4; refer patients with worsening symptoms and those who develop new physical or psychological symptoms for further evaluation at any time during their care; and5 reassess the patient at every visit to determine whether additional care is necessary, the condition is worsening, or the patient has recovered. Patients reporting significant recovery should be discharged. Similar recommendations were formulated by the Neck Pain Task Force116 and in prior practitioner guides on the management of WAD and NAD by chiropractors.24,25
Benefits of Physical Activity and Self-management. Educating patients about the benefits of being physically active and participating in their care has become the standard of care internationally. Despite the benefits of therapeutic exercise for managing chronic neck pain and the strong evidence favoring regular physical activity to reduce related comorbidities, care providers fail to routinely prescribe these to patients.117-120 When prescribed, the amount of supervision and types of exercises do not follow practice guidelines and are not linked to the degree of patient impairment.118,121 On the patient side, adherence to prescribed exercise programs is often low. 122
The promotion of physical activity, including exercise, is a first-line treatment considered important in the prevention and treatment of musculoskeletal pain and its related comorbidities (eg, coronary heart disease, type 2 diabetes, and depression).123-126 For a minority of patients with chronic spine pain, clinician-delivered interventions and pharmacologic treatments are appropriate; and in fewer cases, multidisciplinary pain management or surgery may be indicated. 118
People with musculoskeletal pain will often adopt an inactive lifestyle. Unfortunately, physical inactivity is associated with important adverse health effects, including increased risks of coronary heart disease, type 2 diabetes, and breast and colon cancers, and shorter life expectancy in general.127 The World Health Organization128 provided clear guidance on physical activity for health for children, adults, and elders. In addition, recent research suggests that WAD patients with high levels of passive coping�strategies have slower pain and disability recovery.129 Self-management support (SMS) strategies aimed at increasing physical activity and active coping strategies are key to effectively managing spinal pain and related comorbidities. 124,125,130-134 The CCGI developed a theory-based knowledge translation (KT) intervention targeting identified barriers to professional behavior change to increase the uptake of SMS strategies among Canadian chiropractors.135 Interviews of clinicians identified 9 theoretical domains as likely relevant (ie, factors perceived to influence the use of multimodal care to manage nonspecific neck pain).135 The intervention, comprising a webinar and a learning module on Brief Action Planning, is a highly structured SMS strategy that allows patient- centered goals136 and is being pilot-tested among Canadian chiropractors (ongoing pilot trial).137 Care providers are encouraged to perform periodic clinical revaluations and to monitor patient progression of self-management strategies while discouraging dependence on passive treatment.
III. Research
Overall, the quality of the research on conservative management of NADs and WADs remains low, partly explaining that only weak recommendations could be formulated for clinical practice. Further, the reporting of RCTs remains suboptimal. 138 Past recommendations for improving the quality of the research still apply.24,25 Future research should aim to clarify the role of spinal manipulation therapy alone or as part of multimodal care for the management of recent neck pain and have adequate frequency and length of follow-up. For instance, a large number of patient visits to the emergency departments each year are for acute neck and arm pain resulting from WADs.14,139 A small RCT suggested that cervical spine manipulation is a reasonable alternative to intramuscular NSAID for immediate pain relief in these patients.63 However, the small sample size, comparison of a single session of spinal manipulation to an NSAID injection, and a 1-day follow-up was not representative of clinical practice.
Few recent adequately controlled high-quality research studies of chiropractic care for NADs have been published. In addition, studies included in the reviews did not estimate the maximum therapeutic benefits (ie, best dosage for treatment under evaluation). Well-designed clinical trials with sufficient numbers of participants, longer-term treatments, and follow-up periods are needed to increase the confidence in the recommendations and to advance our understanding of effective and cost-effective conservative care, and spinal manipulation, for the management of patients with NADs and WADs.
Dissemination and Implementation Plan. Evidence-based practice aims to improve clinical decision making and patient care.140,141 When followed, CPGs have the potential to improve health outcomes and the efficiency of the health care system.142-144 However, low adherence to CPGs has been noted across health care sectors145 and in the management of musculoskeletal conditions, including NADs and WADs.77,101,102 Such gaps contribute to wide geographic variations in the use and quality of health care services. 146
Efforts to bridge the �research-practice gap� have led to a growing interest in KT.145,147 Knowledge translation is defined as the exchange, synthesis, and ethically sound application of knowledge to improve health and provide more effective health services. 148 Knowledge translation aims to bridge the research-practice gap and improve patient outcomes by promoting the integration and exchange of research and evidence-based knowledge into clinical practice.
To prepare for guideline implementation, we considered the Guideline Implementation Planning Checklist 149 and�available strategies and supporting evidence141,150 to increase guideline uptake. Although effects of KT inter- ventions tend to be modest, they are likely important at a population health level.37
To raise awareness, chiropractic professional organiza- tions are encouraged to inform their members of new CCGI guidelines and tools easily accessible on our website (www. chiroguidelines.org). The guideline implementation tools framework was used to clarify the objectives of the tools; identify end users and the context and setting where tools will be used; provide instructions for use; and describe methods to develop the tools and related evidence and to evaluate the tools.151 Implementation tools designed to increase guideline uptake include practitioner and patients� handouts (Fig. 8, Appendix 7); algorithms (Figs. 6 and 7), webinars, videos, and learning modules (www.cmcc. ca/CE); point-of-care checklists; and health status reminders.152-154 The CCGI has established a network of opinion leaders across Canada (www.chiroguidelines.org). Based on successful efforts to implement a WAD guideline in Australia using opinion leaders among regulated physiotherapists, chiropractors, and osteopaths, 155 the CCGI is planning a series of implementation studies among Canadian chiropractors.137 We will also pilot within chiropractic practice-based research networks.156 Monitor- ing guideline use in chiropractic is challenging because the use of electronic health records to routinely collect clinical practice information is not common in Canada and those using electronic health records often collect different indicators. 157 Nonetheless, the frequency of downloads (posting of the open access guideline on the CCGI website) and number of registering participants and completion of educational online material (webinar, video, and learning module) will be monitored monthly as proxy measures of guideline uptake.
Guideline Update
The methods for updating the guideline will be as follows: 1) Monitoring changes in evidence, available interventions, importance and value of outcomes, resources available or relevance of the recommendations to clinicians (limited systematic literature searches each year for 3-5 years and survey to experts in the field annually): 2) assessing the need to update (relevance of the new evidence or other changes, type and scope of the update); and 3) communi- cating the process, resources, and timeline to the Guideline Advisory Committee of the CCGI, who will submit a recommendation to the Guideline Steering Committee to make a decision to update and schedule the process.158-163
Strengths and Limitations
Shortcomings for this guideline include the low quantity and quality of supporting evidence found during the searches. Most of the downgrading of evidence supporting the outcomes occurred because of imprecision. In addition, our updated search of the published reports included 2 databases (Medline and Cochrane Central Register of Controlled Trials) but was limited to the English published reports, which possibly excluded some relevant studies. This, however, is an unlikely source of bias.164,165 Qualitative studies that explored the lived experience of patients were not included. Thus, this review cannot comment on how patients valued and experi- enced their exposure to manual therapies or passive physical modalities. Although the composition of the guideline panel was diverse, with experienced methodologists, expert clini- cians, and stakeholder and patient representatives, only 1 member was from another health discipline (physiotherapist). The scope of this guideline focused on selected outcomes such as pain and disability, although included studies assessed several additional outcomes.
Conclusion
This CPG supersedes the original (2005) and revised (2014) neck pain guideline as well as the 2010 whiplash-associated guidelines produced by the Canadian Chiropractic Association (CCA); Canadian Federation of Chiropractic Regulatory and Educational Accrediting Boards (CFCREAB).
People should receive care based on evidence-based therapeutic options. Based on patient preference and resources available, a mixed multimodal approach includ- ing manual therapy and advice about self-management and exercise (supervised/unsupervised or at home) may be an effective treatment strategy for recent-onset and persistent NAD and WAD grades I to III. Progress should be regularly monitored for evidence of benefit, in particular on the basis of pain alleviation and reduction of disability.
Funding Sources and Conflicts of Interest
Funds provided by the Canadian Chiropractic Research Foundation. The views of the funding body have not influenced the content of the guideline. No conflicts of interest were reported for this study.
Guideline Disclaimer
The evidence-based practice guidelines published by the CCGI include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.21 Guidelines are intended to inform clinical decision making, are not prescriptive in nature, and do not replace professional chiropractic care or advice, which always should be sought for any specific condition. Furthermore, guidelines may not be complete or�accurate because new studies that have been published too late in the process of guideline development or after publication are not incorporated into any particular guideline before it is disseminated. CCGI and its working group members, executive committee, and stakeholders (the �CCGI Parties�) disclaim all liability for the accuracy or completeness of a guideline, and disclaim all warranties, expressed or implied. Guideline users are urged to seek out newer information that might impact the diagnostic and/or treatment recommendations contained within a guideline. The CCGI Parties further disclaim all liability for any damages whatsoever (including, without limitation, direct, indirect, incidental, punitive, or consequential damages) arising out of the use, inability to use, or the results of use of a guideline, any references used in a guideline, or the materials, information, or procedures contained in a guideline, based on any legal theory whatsoever and whether or not there was advice of the possibility of such damages.
Through a comprehensive and systematic literature review, CCGI evidence-based CPGs incorporate data from the existing peer-reviewed literature. This literature meets the prespecified inclusion criteria for the clinical research question, which CCGI considers, at the time of publication, to be the best evidence available for general clinical information purposes. This evidence is of varying quality from original studies of varying methodological rigor. CCGI recommends that performance measures for quality improvement, performance-based reimbursement, and public reporting purposes should be based on rigorously developed guideline recommendations.
A multimodal approach including manual therapy, self-management advice, and exercise can be an effective treatment strategy for recent-onset and persistent neck pain and whiplash-associated disorders.
Acknowledgements
We thank the following people for their contributions to this paper: Dr. John Riva, DC, observer; Heather Owens, Research Coordinator, proofreading; Cameron McAlpine (Director of Communication & Marketing, Ontario Chiro- practic Association), for assistance in producing the companion document intended for patients with NAD; members of the guideline panel who served on the Delphi consensus panel, who made this project possible by generously donating their expertise and clinical judgment.
In conclusion, whiplash-associated disorders can cause damage to the complex structures of the cervical spine, or neck, because the sheer force of an impact can extend the soft tissues beyond their natural range of motion. Many healthcare professionals can safely and effectively treat whiplash as well as other automobile accident injuries. The results of the article above demonstrate that a multimodal approach, including manual therapy, self-management advice and exercise can be an efficient treatment strategy for both recent-onset and persistent neck pain caused by whiplash-associated disorders.�Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. Ferrari R, Russell A. Regional musculoskeletal conditions: neck pain. Best Pract Res Clin Rheumatol. 2003;17(1):57-70.
2. Hogg-Johnson S, van der Velde G, Carroll LJ, et al. The burden and determinants of neck pain in the general population: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine.
2008;33(4 Suppl):S39-S51.
3. Holm L, Carroll L, Cassidy JD, et al. The burden and
determinants of neck pain in whiplash-associated disorders after traffic collisions: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine. 2008;33(4 Suppl):S52-S59.
4. Co?te? P, van der Velde G, Cassidy JD, et al. The burden and determinants of neck pain in workers: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine. 2008;33(4 Suppl): S60-S74.
5. Vos T, Flaxman A, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859): 2163-2196.
6. Co?te? P, Cassidy JD, Carroll L. The treatment of neck and low back pain: who seeks care? Who goes where? Med Care. 2001;39(9):956-967.
7. Hoy DG, Protani M, De R, Buchbinder R. The epidemi- ology of neck pain. Best Pract Res Clin Rheumatol. 2010; 24(6):783-792.
8. Murray C, Abraham J, Ali M, et al. The state of us health, 1990-2010: burden of diseases, injuries, and risk factors. JAMA. 2013;310(6):591-606.
9. Manchikanti L, Singh V, Datta S, Cohen S, Hirsch J. Physicians. ASoIP. Comprehensive review of epidemiolo- gy, scope, and impact of spinal pain. Pain Physician. 2009; 12(4):E35-E70.
10. Hincapie? C, Cassidy J, Co?te? P, Carroll L, Guzma?n J. Whiplash injury is more than neck pain: a population-based study of pain localization after traffic injury. J Occup Environ Med. 2010;52(4):434-440.
11. Blincoe L, Miller T, Zaloshnja E, Lawrence B. The Economic and Societal Impact of Motor Vehicle Crashes, 2010. (Revised) (Report No. DOT HS 812 013). Washington, DC: National Highway Traffic Safety Administration; 2015.
12. Bannister G, Amirfeyz R, Kelley S, Gargan M. Whiplash injury. J Bone Joint Surg. 2009;91-B(7):845-850.
13. Johansson M, Boyle E, Hartvigsen J, Carroll L, Cassidy J. A population-based, incidence cohort study of mid-back pain after traffic collisions: factors associated with global recovery. EuroJ Pain. 2015;19(10):186-195.
14. Styrke J, Stalnacke B, Bylund P, Sojka P. A 10-year incidence of acute whiplash injuries after road traffic crashes in a defined population in northern Sweden. PM R. 2012;4(10):739-747.
15. Ontario MoFo. Ontario Auto Insurance Anti-Fraud Task Force Interim Report. Available at: www.fin.gov.on. ca/en/autoinsurance/interim-report.pdf Accessed May 7, 2016.
16. Karlsborg M, Smed A, Jespersen H, et al. A prospective study of 39 patients with whiplash injury. Acta Neurol Scand. 1997;95(2):65-72.
17. Sterling M, Jull G, Vicenzino B, Kenardy J, Darnell R. Development of motor system dysfunction following whiplash injury. Pain. 2003;103(1-2):65-73.
18. Guzman J, Hurwitz EL, Carroll LJ, et al. A new conceptual model of neck pain: linking onset, course, and care: the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine. 2008;33(4 Suppl): S14-S23.
19. Leaver A, Maher C, McAuley J, Jull G, Refshauge K. Characteristics of a new episode of neck pain. Man Ther. 2013;18(3):254-257.
20. Co?te? P, Shearer H, Ameis A, et al. Enabling recovery from common traffic injuries: a focus on the injured person. UOIT-CMCC Centre for the Study of Disability Prevention and Rehabilitation; 2015.
21. Clar C, Tsertsvadze A, Court R, Hundt G, Clarke A, Sutcliffe P. Clinical effectiveness of manual therapy for the management of musculoskeletal and non-musculoskeletal conditions: systematic review and update of UK evidence report. Chiropract Man Ther. 2014;22(1):12.
22. Bronfort G, Evans R, Anderson A, Svendsen K, Bracha Y, Grimm R. Spinal manipulation, medication, or home exercise with advice for acute and subacute neck pain. Ann Intern Med. 2012;156(1 Part 1):1-10.
23. Hurwitz EL, Carragee EJ, van der Velde G, et al. Treatment of neck pain: noninvasive interventions. Results of the Bone and Joint Decade 2000�2010 Task Force on Neck Pain and its Associated Disorders. Spine. 2008;33(4S):S123-S152.
24. Bryans R, Decina P, Descarreaux M, et al. Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J Manip Physiol Therap. 2014;37(1):42-63.
25. Shaw L, Descarreaux M, Bryans R, et al. A systematic review of chiropractic management of adults with whiplash- associated disorders: recommendations for advancing evidence-based practice and research. Work. 2010;35(3): 369-394.
26. Graham G, Mancher M, Miller Wolman D, Greenfield S, Steinberg E, editors. Clinical Practice Guidelines We Can Trust. Institute of Medicine, Shaping the Future for Health.
Washington, DC: National Academies Press; 2011.
27. Co?te? P, Wong JJ, Sutton D, et al. Management of neck pain and associated disorders: a clinical practice guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Euro Spine J. 2016;25(7): 2000-2022.
28. Johnson AP, Sikich NJ, Evans G, et al. Health technology assessment: a comprehensive framework for evidence- based recommendations in ontario. Int J Technol Assess Health Care. 2009;25(2):141-150.
29. Shukla V, Bai A, Milne S, Wells G. Systematic review of the evidence grading system for grading level of evidence. German J Evid Qual Health Care. 2008; 102:43.
30. Mustafa RA, Santesso N, Brozek J, et al. The GRADE approach is reproducible in assessing the quality of evidence of quantitative evidence syntheses. J Clin Epidemiol. 2013;66(7):736-742.e5.
31. Woolf S, Schunemann H, Eccles M, Grimshaw J, Shekelle P. Developing clinical practice guidelines: types of evidence and outcomes; values and economics, synthesis, grading, and presentation and deriving recommendations. lImplementation Sci. 2012;7(1):61.
32. Tricco A, Tetzlaff J, Moher D. The art and science of knowledge synthesis. J Clin Epidemiol. 2011;64(1):11-20.
33. Guyatt G, Eikelboom JW, Akl EA, et al. A guide to GRADE
guidelines for the readers of JTH. J Thromb Haemost. 2013;
11(8):1603-1608.
34. Adaptation. The ADAPTE Manual and Resource
Toolkit V2. G-I-N Adaptation Working Group. Available at: www.g-i-n.net/working-groups/adaptation Accessed May 16, 2016.
35. Brouwers M, Kho M, Browman G, et al. AGREE II: advancing guideline development, reporting and evalua- tion in health care. J Clin Epidemiol. 2010;63(12): 1308-1311.
36. Flottorp S, Oxman AD, Cooper JG, Hjortdahl P, Sandberg S, Vorland LH. Retningslinjer for diagnostikk og behand- ling av sar hals. Tidsskr Nor Laegeforen. 2000;120: 1754-1760.
37. Grimshaw J, Eccles M, Lavis J, Hill S, Squires J. Knowledge translation of research findings. Implementation Sci. 2012;7(1):50.
38. Southerst D, Nordin M, Co?te? P, et al. Is exercise effective for the management of neck pain and associated disorders or whiplash-associated disorders? A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Spine J. 2014;S1529-1530(14): 00210-1.
39. Sutton D, Cote P, Wong J, et al. Is multimodal care effective for the management of patients with whiplash-associated disorders or neck pain and associated disorders? A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Spine J. 2014 [S1529-9430(14):00650-0].
40. Yu H, Co?te? P, Southerst D, Wong J, et al. Does structured patient education improve the recovery and clinical outcomes of patients with neck pain? A systematic review from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Spine J. 2014;pii: S1529- 9430(14).
41. Varatharajan S, Co?te? P, Shearer H, et al. Are work disability prevention interventions effective for the management of neck pain or upper extremity disorders? A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. J Occup Rehabil. 2014;24(4): 692-708.
42. Wong JJ, Shearer HM, Mior S, et al. Are manual therapies, passive physical modalities, or acupuncture effective for the management of patients with whiplash-associated disorders or neck pain and associated disorders? An update of the Bone and Joint Decade Task Force on Neck Pain and Its Associated Disorders by the Optima Collaboration. Spine J. 2015;20(8 Suppl).
43. Shea B, Grimshaw J, Wells G, Boers M, Andersson N, Hamel C. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10.
44. Norman G, Streiner D. Biostatistics: The Bare Essentials. 3rd ed. Hamilton, ON: BC Decker; 2008.
45. Ricci S, Celani M, Righetti E. Development of clinical guidelines: methodological and practical issues. Neurol Sci. 2006;27(Suppl 3):S228-S230.
46. van der Velde G, van Tulder M, Co?te? P, et al. The sensitivity of review results to methods used to appraise and incorporate trial quality into data synthesis. Spine. 2007; 32(7):796-806.
47. Slavin R. Best evidence synthesis: an intelligent alternative to meta-analysis. J Clin Epidemiol. 1995;48(1):9-18.
48. Network GI, GRADE Working Group. Resources. Available at: www.g-i-n.net/working-groups/updating-guidelines/re- sources. Accessed May 5, 2016.
49. Guyatt G, Oxman A, Vist G, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-926.
50. Guyatt G, Oxman A, Akl E, Kunz R, Vist G, Brozek J, et al. GRADE guidelines 1. Introduction: GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):38-94.
51. Treweek S, Oxman A, Alderson P, et al. Developing and evaluating communication strategies to support informed decisions and practice based on evidence (DECIDE): protocol and preliminary results. Implementation Sci. 2013; 8(1):6.
52. McCarthy M, Grevitt M, Silcocks P, Hobbs G. The reliability of the Vernon and Mior neck disability index, and its validity compared with the short form-36 health survey questionnaire. Eur Spine J. 2007;16(12):2111-2117.
53. Stauffer M, Taylor S, Watson D, Peloso P, Morrison A. Definition of nonresponse to analgesic treatment of arthritic pain: an analytical literature review of the smallest detectable difference, the minimal detectable change, and the minimal clinically important difference on the pain visual analog scale. Int J Inflam. 2011;2011:231926.
54. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual analog scale for pain (VAS Pain), numeric rating scale for pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP. Arthritis Care Res. 2011;63(S11):S240-S252.
55. Blozik E, Himmel W, Kochen MM, Herrmann-Lingen C, Scherer M. Sensitivity to change of the Neck Pain and Disability Scale. Euro Spine J. 2011;20(6):882-889.
56. Andrews J, Guyatt G, Oxman AD, et al. GRADE guidelines: 14. Going from evidence to recommendations: the signifi- cance and presentation of recommendations. J Clin Epidemiol. 2013;66(7):719-725.
57. Andrews JC, Schu?nemann HJ, Oxman AD, et al. GRADE guidelines: Going from evidence to recommendation� determinants of a recommendation’s direction and strength. J Clinl Epidemiol. 2013;66(7):726-735.
58. Black N, Murphy M, Lamping D, McKee M, Sanderson C, Askham J. Consensus development methods: a review of best practice in creating clinical guidelines. J Health Serv Res Policy. 1999;4(4):236-248.
59. Seo H-J, Kim KU. Quality assessment of systematic reviews or meta-analyses of nursing interventions conducted by Korean reviewers. BMC Med Res Methodol. 2012;12:129.
60. Leaver A, Maher C, Herbert R, et al. A randomized controlled trial comparing manipulation with mobilization for recent onset neck pain. Arch Phys Med Rehabil. 2010;91(9):1313-1318.
61. Dunning J, Cleland J, Waldrop M, et al. Upper cervical and upper thoracic thrust manipulation versus nonthrust mobiliza- tion in patients with mechanical neck pain: a multicenter randomized clinical trial. J Orthop Sports Phys Ther. 2012; 42(1):5-18.
62. Nagrale A, Glynn P, Joshi A, Ramteke G. The efficacy of an integrated neuromuscular inhibition technique on upper trapezius trigger points in subjects with non-specific neck pain: a randomized controlled trial. J Man Manip Ther. 2010; 18(1):37-43.
63. McReynolds T, Sheridan B. Intramuscular ketorolac versus osteopathic manipulative treatment in the management of acute neck pain in the emergency department: a randomized clinical trial. JAOA. 2005;105(2):57-68.
64. Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop Effectiveness and Risks of Long-Term Opioid Therapy for Chronic Pain. Ann Inter Med. 2015;162(4):276-286.
65. Kuijper B, Tans J, Beelen A, Nollet F, de Visser M. Cervical collar or physiotherapy versus wait and see policy for recent onset cervical radiculopathy: randomised trial. BMJ. 2009;339:b3883.
66. Cassidy J. Mobilisation or immobilisation for cervical radiculo- pathy? BMJ. 2009;339(b):3952.
67. Konstantinovic L, Cutovic M, Milovanovic A, et al. Low-level laser therapy for acute neck pain with radiculopathy: a double- blind placebo-controlled randomized study. Pain Med. 2010; 11(8):1169-1178.
68. van den Heuvel S, de Looze M, Hildebrandt V, The? K. Effects of software programs stimulating regular breaks and exercises on work-related neck and upper-limb disorders. Scand J Work Environ Health. 2003;29(2):106-116.
69. Lamb S, Gates S, Williams M, et al. Emergency department treatments and physiotherapy for acute whiplash: a pragmatic, two-step, randomised controlled trial. Lancet. 2013;381(9866): 546-556.
70. Ferrari R, Rowe BH, Majumdar SR, et al. Simple educational intervention to improve the recovery from acute whiplash: results of a randomized, controlled trial. Acad Emerg Med. 2005;12(8): 699-706.
71. von Trott P, Wiedemann A, Lu?dtke R, Rei�hauer A, Willich S, Witt C. Qigong and exercise therapy for elderly patients with chronic neck pain (QIBANE): a randomized controlled study. J Pain. 2009;10(5):501-508.
72. Rendant D, Pach D, Ludtke R, et al. Qigong versus exercise versus no therapy for patients with chronic neck pain: a randomized controlled trial. Spine. 2011;36(6):419-427.
73. Michalsen A, Traitteur H, Lu?dtke R, et al. Yoga for chronic neck pain: a pilot randomized controlled clinical trial. J Pain. 2012; 13(11):1122-1130.
74. Jeitler M, Brunnhuber S, Meier L, et al. Effectiveness of jyoti meditation for patients with chronic neck pain and psychological distress-a randomized controlled clinical trial. J Pain. 2015;16(1): 77-86.
75. Hakkinen A, Kautiainen H, Hannonen P, Ylinen J. Strength training and stretching versus stretching only in the treatment of patients with chronic neck pain: a randomized one-year follow-up
study. Clin Rehabil. 2008;22(7):593-600.
76. Salo P, Ylonen-Kayra N, Hakkinen A, Kautiainen H, Malkia E,
Ylinen J. Effects of long-term home-based exercise on health- related quality of life in patients with chronic neck pain: a randomized study with a 1-year follow-up. Disabil Rehabil. 2012; 34(23):1971-1977.
77. Evans R, Bronfort G, Schulz G, et al. Supervised exercise with and without spinal manipulation performs similarly and better than home exercise for chronic neck pain: a randomized controlled trial. Spine. 2012;37(11):903-914.
78. Maiers M, Bronfort G, Evans R, et al. Spinal manipulative therapy and exercise for seniors with chronic neck pain. Spine J. 2014;14(9):1879-1889.
79. Griffiths C, Dziedzic K, Waterfield J, Sim J. Effectiveness of specific neck stabilization exercises or a general neck exercise program for chronic neck disorders: a randomized controlled trial. J Rheumatol. 2009;36(2):390-397.
80. Gustavsson C, Denison E, von Koch L. Self-management of persistent neck pain: a randomized controlled trial of a multi- component group intervention in primary health care. Eur J Pain. 2010;14(6):630.e1-11.
81. Gustavsson C, Denison E, von Koch L. Self-management of persistent neck pain: two-year follow-up of a randomized controlled trial of a multicomponent group intervention in primary health care. Spine. 2011;36(25):2105-2115.
82. Sherman K, Cherkin D, Hawkes R, Miglioretti D, Deyo R. Randomized trial of therapeutic massage for chronic neck pain. Clin J Pain. 2009;25(3):233-238.
83. Lin J, Shen T, Chung R, Chiu T. The effectiveness of Long’s manipulation on patients with chronic mechanical neck pain: a randomized controlled trial. Manual Ther. 2013;18(4):308-315.
84. Lauche R, Materdey S, Cramer H, et al. Effectiveness of home- based cupping massage compared to progressive muscle relaxation in patients with chronic neck pain�a randomized controlled trial. PLoS One. 2013;8(6):e65378.
85. Sherman K, Cook A, Wellman R, et al. Five-week outcomes from a dosing trial of therapeutic massage for chronic neck pain. Ann Fam Med. 2014;12(2):112-120.
86. Walker MJ, Boyles RE, Young BA, et al. The effectiveness of manual physical therapy and exercise for mechanical neck pain: a randomized clinical trial. Spine (Phila Pa 1976). 2008;33(22): 2371-2378.
87. Boyles R, Walker M, Young B, Strunce J, Wainner R. The addition of cervical thrust manipulations to a manual physical therapy approach in patients treated for mechanical neck pain: a secondary analysis. J Orthop Sports Phys Ther. 2010;40(3): 133-140.
88. Hoving JL, de Vet HC, Koes BW, et al. Manual therapy, physical therapy, or continued care by the general practitioner for patients with neck pain: long-term results from a pragmatic randomized clinical trial. Clin J Pain. 2006;22(4):370-377.
89. Hoving JL, Koes BW, de Vet HCW, et al. Manual Therapy, physical therapy, or continued care by a general practitioner for patients with neck pain: a randomized, controlled trial. Ann Intern Med. 2002;136(10):713-722.
90. Monticone M, Baiardi P, Vanti C, et al. Chronic neck pain and treatment of cognitive and behavioural factors: results of a randomised controlled clinical trial. Euro Spine J. 2012;21(8): 1558-1566.
91. Zebis M, Andersen L, Pedersen M, et al. Implementation of neck/shoulder exercises for pain relief among industrial workers: a randomized controlled trial. BMC Musculoskelet Disord. 2011;12:205.
92. Zebis MK, Andersen CH, Sundstrup E, Pedersen MT, Sj�gaard G, Andersen LL. Time-wise change in neck pain in response to rehabilitation with specific resistance training: implications for
exercise prescription. PLoS One. 2014;9(4):e93867.
93. Andersen C, Andersen L, Gram B, et al. Influence of frequency and duration of strength training for effective management of neck and shoulder pain: a randomised controlled trial. Br J
Sports Med. 2012;46(14):1004-1010.
94. Andersen L, Jorgensen M, Blangsted A, Pedersen M, Hansen E,
Sjogaard GA. randomized controlled intervention trial to relieve and prevent neck/shoulder pain. Med Sci Sports Exerc. 2008; 40(6):983-990.
95. Sjogren T, Nissinen K, Jarvenpaa S, Ojanen M, Vanharanta H, Malkia E. Effects of a workplace physical exercise intervention on the intensity of headache and neck and shoulder symptoms and upper extremity muscular strength of office workers: a cluster randomized controlled cross-over trial. Pain. 2005;116(1-2):119-128.
96. Stewart M, Maher C, Refshauge K, Herbert R, Bogduk N, Nicholas M. Randomized controlled trial of exercise for chronic whiplash-associated disorders. Pain. 2007;128(1-2):59-68.
97. Michaleff Z, Maher C. Lin C-WC, et al. Comprehensive physiotherapy exercise programme or advice for chronic whiplash (PROMISE): a pragmatic randomised controlled trial. Lancet. 2014;384(9938):133-141.
98. Gram B, Andersen C, Zebis MK, et al. Effect of training supervision on effectiveness of strength training for reducing neck/shoulder pain and headache in office workers: cluster randomized controlled trial. BioMed Ress Int. 2014;2014:9.
99. Jull G, Sterling M, Kenardy J, Beller E. Does the presence of sensory hypersensitivity influence outcomes of physical reha- bilitation for chronic whiplash? A preliminary RCT. Pain. 2007; 129(1-2):28-34.
100. Jull G, Kenardy J, Hendrikz J, Cohen M, Sterling M. Management of acute whiplash: a randomized controlled trial of multidisciplin- ary stratified treatments. Pain. 2013;154(9):1798-1806.
101. Wiangkham T, Duda J, Haque S, Madi M, Rushton A. The effectiveness of conservative management for acute whiplash associated disorder (WAD) II: a systematic review and meta- analysis of randomised controlled trials. PLoS One. 2015;10(7): e0133415.
102. Guyatt G, Oxman AD, Sultan S, et al. GRADE guidelines: 11. Making an overall rating of confidence in effect estimates for a single outcome and for all outcomes. J Clin Epidemiol. 2013; 66(2):151-157.
103. Walsh D, Howe T, Johnson M, Sluka K. Transcutaneous electrical nerve stimulation for acute pain. Cochrane Database Syst Rev. 2009(2)CD006142.
104. Nnoaham K, Kumbang J. Transcutaneous electrical nerve stimulation (TENS) for chronic pain. Cochrane Database Syst Rev. 2008(3)CD003222.
105. French S, Cameron M, Walker B, Reggars J, Esterman A. Superficial heat or cold for low back pain. Cochrane Database Syst Rev. 2006(1)CD004750.
106. Malanga GA, Yan N, Stark J. Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgrad Med. 2015;127(1):57-65.
107. Carnes D, Mullinger B, Underwood M. Defining adverse events in manual therapies: a modified Delphi consensus study. lManual Ther. 2010;15(1):2-6.
108. Haldeman S, Carroll LJ, Cassidy JD. The empowerment of people with neck pain: introduction: the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine. 2008;33(4 Suppl):S8-S13.
109. Maiers M, Vihstadt C, Hanson L, Evans R. Perceived value of spinal manipulative therapy and exercise among seniors with chronic neck pain: a mixed methods study. J Rehabil Med. 2014;46(10):1022-1028.
110. Chou R, Deyo R, Friedly J, et al. Noninvasive treatments for low back pain. Comparative Effectiveness Review No. 169. (Prepared by the Pacific Northwest Evidence-based Practice Center under Contract No. 290-2012-00014-I.). AHRQ Publication No. 16-EHC004-EF. Rockville, MD. Available at: www.effectivehealthcare.ahrq.gov/reports/final.cfm. Accessed May 15, 2016.
111. Machado G, Maher C, Ferreira P, et al. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials. BMJ. 2015;350:h1225.
112. Miller M, Barber CW, Leatherman S, et al. Prescription opioid duration of action and the risk of unintentional overdose among patients receiving opioid therapy. JAMA Intern Med. 2015; 175(4):608-615.
113. Volkow N, McLellan A. Opioid abuse in chronic pain� misconceptions and mitigation strategies. N Engl J Med. 2016; 374(13):1253-1263.
114. Foster N, Hartvigsen J, Croft P. Taking responsibility for the early assessment and treatment of patients with musculoskeletal pain: a review and critical analysis. Arthritis Res Ther. 2012;14(1):205.
115. World Health Organization. WHO Guidelines on Basic Training and Safety in Chiropractic. Geneva, Switzerland: World Health Organization; 2005.
116. Guzman J, Haldeman S, Carroll L, et al. Clinical practice implications of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders: from concepts and findings to recommendations. Spine. 2008;33(4 Suppl):S199-S213.
117. Dietl M, Korczak D. Over-, under- and misuse of pain treatment in Germany. GMS Health Technol Assess. 2011; 7:Doc03. dx.doi.org/10.3205/hta000094.
118. Freburger J, Carey T, Holmes G, Wallace A, Castel L, Darter J. Exercise prescription for chronic back or neck pain: who prescribes it? Who gets it? What is prescribed? lArthritis Care Res. 2009;61:192-200.
119. Goode A, Freburger J, Carey T. Prevalence, practice patterns, and evidence for chronic neck pain. Arthritis Care Res. 2010;62(11):1594-1601.
120. Kamaleri Y, Natvig B, Ihlebaek CM, Bruusgaard D. Localized or widespread musculoskeletal pain: does it matter? Pain. 2008;138(1):41-46.
121. MacDermid J, Miller J, Gross A. Knowledge translation tools are emerging to move neck pain research into practice. lOpen Orthop J. 2013;20(7):582-593.
122. Medina-Mirapeix F, Escolar-Reina P, Gascon-Canovas J, Montilla-Herrador J, Jimeno-Serrano F, Collins S. Predictive factors of adherence to frequency and duration components in home exercise programs for neck and low back pain: an observational study. BMC Musculoskelet Disord. 2009;10(1):155.
123. Kay T, Gross A, Goldsmith C, et al. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. 2012;8:CD004250.
124. Bertozzi L, Gardenghi I, Turoni F, et al. Effect of
therapeutic exercise on pain and disability in the manage- ment of chronic nonspecific neck pain: systematic review and meta-analysis of randomized trials. Phys Ther. 2013; 93(8):1026-1036.
125. Hartvigsen J, Natvig B, Ferreira M. Is it all about a pain in the back? Best Pract Res Clin Rheumatol. 2013;27(5):613-623.
126. Ambrose K, Golightly Y. Physical exercise as non-pharmaco- logical treatment of chronic pain: why and when. Best Pract Res Clin Rheumatol. 2015;29(1):120-130.
127. Lee I, Shiroma E, Lobelo F, Puska P, Blair S, Katzmarzyk P. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219-229.
128. World Health Organization. Global Recommendations on Physical Activity for Health. Geneva, Switzerland: World Health Organization; 2010.
129. Carroll LJ, Ferrari R, Cassidy JD, Cote P. Coping and recovery in whiplash-associated disorders: early use of passive coping strategies is associated with slower recovery of neck pain and pain-related disability. Clin J Pain. 2014;30(1):1-8.
130. Gore M, Sadosky A, Stacey B, Tai K, Leslie D. The burden of chronic low back pain: clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine. 2012;37(11):E668-E677.
131. Bodenheimer T, MacGregor K, Charifi C. Helping patients manage their chronic conditions. Oakland, CA: California HealthCare Foundation; 2005.
132. Ritzwoller D, Crounse L, Shetterly S, Rublee D. The association of comorbidities, utilization and costs for patients identified with low back pain. BMC Musculoskelet Disord. 2006;7(1):72.
133. Sallis R, Franklin B, Joy L, Ross R, Sabgir D, Stone J. Strategies for promoting physical activity in clinical practice. Prog Cardiovasc Dis. 2015;57(4):375-386.
134. Von Korff M, Crane P, Lane M, et al. Chronic spinal pain and physical-mental comorbidity in the United States: results from the national comorbidity survey replication. Pain. 2005;113(3): 331-339.
135. Bussie?res A, Al Zoubi F, Quon J, et al. Fast tracking the design of theory-based KT interventions through a consensus process. Implementation Sci. 2015;10(1):18.
136. Gutnick D, Reims K, Davis C, Gainforth H, Jay M, Cole S. Brief action planning to facilitate behavior change and support patient self-management. J Clin Outcomes Manag. 2014;21: 17-29.
137. Dhopte P, Ahmed S, Mayo N, French S, Quon JA, Bussie?res A. Testing the feasibility of a knowledge translation intervention designed to improve chiropractic care for adults with neck pain disorders: study protocol for a pilot cluster-randomized controlled trial. Pilot and Feasibility Studies. 2016;2(1):1-11.
138. Turner L, Shamseer L, Altman D, et al. Consolidated standards of reporting trials (CONSORT) and the complete- ness of reporting of randomised controlled trials (RCTs) published in medical journals. Cochrane Database Syst Rev. 2012;11:MR000030.
139. Quinlan K, Annest J, Myers B, Ryan G, Hill H. Neck strains and sprains among motor vehicle occupants�United States, 2000. Accid Anal Prev. 2004;36(1):21-27.
140. Titler M. The evidence for evidence-based practice imple- mentation. Patient Safety and Quality: An Evidence-Based Handbook for Nurses, vol. 1. Rockville, MD: AHRQ; 2008. p. 113-161.
141. The Canadian Agency for Drugs and Technologies in Health. Rx for Change database. Available at: www.cadth.ca/rx-change. Accessed May 6, 2016.
142. Grimshaw J, Thomas R, MacLennan G, Fraser C, Ramsay C, Vale L. Effectiveness and efficiency of guideline dissemina- tion and implementation strategies. Health Technol Assess. 2004;8(6):1-72.
143. Bishop PB, Quon JA, Fisher CG, Dvorak MFS. The Chiropractic Hospital-based Interventions Research Outcomes (CHIRO) Study: a randomized controlled trial on the effectiveness of clinical practice guidelines in the medical and chiropractic management of patients with acute mechanical low back pain. Spine J. 2010;10(12):1055-1064.
144. Grimshaw J, Schunemann H, Burgers J, Cruz A, Heffner J, Metersky M. Disseminating and implementing guidelines. Article 13 in integrating and coordinating efforts in COPD guideline development. Proc Am Thorac Soc. 2012;9(5): 298-303.
145. Pronovost P. Enhancing physicians’ use of clinical guide- lines. JAMA. 2013;310(23):2501-2502.
146. Schuster, MA, Elizabeth A, McGlynn R, Brook H. How good is the quality of health care in the United States? Milbank. 2005;83(4):843-895.
147. Greenhalgh T, Howick J, Maskrey N. Evidence based medicine: a movement in crisis? BMJ. 2014;348:g3725. 148. Canadian Institutes of Health Research. Knowledge translation�
definition. 2008 Available at: www.cihr-irsc.gc.ca/e/29529.html.
Accessed May 6, 2016.
149. Gagliardi A, Marshall C, Huckson S, James R, Moore V.
Developing a checklist for guideline implementation planning: review and synthesis of guideline development and implemen- tation advice. Implementation Sci. 2015;10(1):19.
150. Cochrane-Effective Practice and Organisation of Care (EPOC). Available at: epoc.cochrane.org/our-reviews. Accessed May 6, 2016.
151. Gagliardi A, Brouwers M, Bhattacharyya O. A framework of the desirable features of guideline implementation tools (GItools): Delphi survey and assessment of GItools. Implementation Sci. 2014;9(1):98.
152. Okelo S, Butz A, Sharma R, et al. Interventions to modify health care provider adherence to asthma guidelines: a systematic review. Pediatrics. 2013;132(3):517-534.
153. Murthy L, Shepperd S, Clarke M, et al. Interventions to improve the use of systematic reviews in decision-making by health system managers, policy makers and clinicians. Cochrane Database Syst Rev. 2012;9CD009401.
154. Garg A, Adhikari N, McDonald H, et al. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA. 2005; 293(10):1223-1238.
155. Rebbeck T, Macedo L, Maher C. Compliance with clinical guidelines for whiplash improved with a targeted implemen- tation strategy: a prospective cohort study. BMC Health Serv Res. 2013;13(1):213.
156. Bussie?res A, Co?te? P, French S, et al. Creating a chiropractic practice-based research network (PBRN): enhancing the management of musculoskeletal care. J Can Chiropr Assoc. 2014;58(1):8-15.
157. Canadian Chiropractic Research Database (CCRD). National Report. The Canadian Chiropractic Association: A Compre- hensive Inventory of Practical Information About Canada�s Licensed Chiropractors; 2011.
158. Becker M, Neugebauer E, Eikermann M. Partial updating of clinical practice guidelines often makes more sense than full updating: a systematic review on methods and the development of an updating procedure. J Clin Epidemiol. 2014;67(1):33-45.
159. Alonso-Coello P, Marti?nez Garci?a L, Carrasco JM, Sola? I, Qureshi S, Burgers JS. The updating of clinical practice guidelines: insights from an international survey. Implementation Sci. 2011;6(1):1-8.
160. Marti?nez Garci?a L, Are?valo-Rodri?guez I, Sola? I, Haynes R, Vandvik P, Alonso-Coello P. Strategies for monitoring and updating clinical practice guidelines: a systematic review. Implementation Sci. 2012;7(1):1-10.
161. Moher D, Tsertsvadze A, Tricco A, et al. A systematic review identified few methods and strategies describing when and how to update systematic reviews. J Clin Epidemiol. 2007;60(11):1095. e1-11.
162. Shekelle P, Eccles M, Grimshaw J, Woolf S. When should clinical guidelines be updated? BMJ. 2001;323(7305):155-157.
163. Vernooij R, Sanabria A, Sola I, Alonso-Coello P, Martinez Garcia L. Guidance for updating clinical practice guidelines: a systematic review of methodological handbooks. Implement Sci. 2014;9:3.
164. Moher D, Pham B, Lawson M, Klassen T. The inclusion of reports of randomised trials published in languages other than English in systematic reviews. Health Technol Assess. 2003; 7(41):1-90.
165. Morrison A, Polisena J, Husereau D, et al. The effect of English-
language restriction on systematic review-based meta-analyses: a
systematic review of empirical studies. Int J Technol Assess
Health Care. 2012;28(20120426):138-144.
166. Harbour R, Miller JA. new system for grading recommen- dations in evidence based guidelines. BMJ. 2001;323(7308): 334-336.
167. Cleland J, Mintken P, Carpenter K, et al. Examination of a clinical prediction rule to identify patients with neck pain likely to benefit from thoracic spine thrust manipulation and a general cervical range of motion exercise: multi-center randomized clinical trial. Phys Ther. 2010;90(9):1239-1250.
168. Escortell-Mayor E, Riesgo-Fuertes R, Garrido-Elustondo S, et al. Primary care randomized clinical trial: Manual therapy effectiveness in comparison with TENS in patients with neck pain. Man Ther. 2011;16(1):66-73.
169. Lamb S, Williams M, Williamson E, et al. Managing Injuries of the Neck Trial (MINT): a randomised controlled trial of treatments for whiplash injuries. Health Technol Assess. 2012; 16(49:iii-iv):1-141.
170. Pool J, Ostelo R, Knol D, Vlaeyen J, Bouter L, de Vet HI. a behavioral graded activity program more effective than manual therapy in patients with subacute neck pain?: results of a randomized clinical trial. Spine. 2010;35(10): 1017-1024.
171. Skillgate E, Bohman T, Holm L, Vinga?rd E, Alfredsson L. The long-term effects of naprapathic manual therapy on back and neck pain. Results from a pragmatic randomized controlled trial. BMC Musculoskelet Disord. 2010;11(1): 1-11.
172. Kongsted A, Qerama E, Kasch H, et al. Education of patients after whiplash injury: is oral advice any better than a pamphlet? Spine. 2008;33(22):E843-E848.
173. Andersen L, Saervoll C, Mortensen O, Poulsen O, Hannerz H, Zebis M. Effectiveness of small daily amounts of progressive resistance training for frequent neck/shoulder pain: Rando- mised controlled trial. Pain. 2011;152(2):440-446.
174. Cheng A, Hung L. Randomized controlled trial of workplace- based rehabilitation for work-related rotator cuff disorder. lJ Occup Rehab. 2007;17(3):487-503.
175. Feuerstein M, Nicholas R, Huang G, Dimberg L, Ali D, Rogers H. Job stress management and ergonomic interven- tion for work-related upper extremity symptoms. Appl Ergon. 2004;35(6):565-574.
176. van Eijsden-Besseling M, Bart Staal J, van Attekum A, de Bie RA, van den Heuvel W. No difference between postural exercises and strength and fitness exercises for early, non- specific, work-related upper limb disorders in visual display unit workers: a randomised trial. Aust J Physiother. 2008; 54(2):95-101.
177. Cameron I, Wang E, Sindhusake DA. randomized trial comparing acupuncture and simulated acupuncture for subacute and chronic whiplash. Spine. 2011;36(26):E1659-E1665.
178. Cleland JA, Glynn PE, Whitman JM, et al. Short-term response of thoracic spine thrust versus non-thrust manipulation in patients with mechanical neck pain: preliminary analysis of a randomized clinical trial. J Manual Manipulat Ther. 2007;14: 172
179. Dundar U, Evcik D, Samli F, Pusak H, Kavuncu V. The effect of gallium arsenide aluminum laser therapy in the management of cervical myofascial pain syndrome: a double blind, placebo- controlled study. Clin Rheumatol. 2007;26(6):930-934.
180. Fu W, Zhu X, Yu P, Zhang J. Analysis on the effect of acupuncture in treating 5 cervical spondylosis with different syndrome types. Chin J Integr Med. 2009;15(6):426-430.
181. Kanlayanaphotporn R, Chiradejnant A, Vachalathiti R. The immediate effects of mobilization technique on pain and range of motion in patients presenting with unilateral neck pain: a randomized controlled trial. Arch Phys Med Rehabil. 2009; 90(2):187-192.
182. Kanlayanaphotporn R, Chiradejnant A, Vachalathiti R. Immediate effects of the central posteroanterior mobiliza- tion technique on pain and range of motion in patients with mechanical neck pain. Dis Rehab. 2010;32(8): 622-628.
183. Klein R, Bareis A, Schneider A, Linde K. Strain-counter- strain to treat restrictions of the mobility of the cervical spine in patients with neck pain: a sham-controlled randomized trial. Complement Ther Med. 2013;21(1):1-7.
184. Liang Z, Zhu X, Yang X, Fu W, Lu A. Assessment of a traditional acupuncture therapy for chronic neck pain: a pilot randomised controlled study. Complementary Ther Med. 2011; 19(Suppl 1):S26-S32.
185. Masaracchio M, Cleland JA, Hellman M, Hagins M. Short-term combined effects of thoracic spine thrust manipulation and cervical spine nonthrust manipulation in individuals with mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys. 2013;43(3):118-127.
186. Saavedra-Hernandez M, Castro-Sanchez A, Arroyo-Morales M, et al. Short term effects of kinesio taping versus cervical thrust manipulation in patients with mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. 2012;42: 724-730.
187. Sillevis R, Hellman M, Beekhuizen K. Immediate effects of a thoracic spine thrust manipulation on the autonomic nervous system: a randomized clinical trial. J Manual Manipulat Ther. 2010;18:181-190.
188. White P, Lewith G, Prescott P, Conway J. Acupuncture versus placebo for the treatment of chronic mechanical neck pain: a randomized, controlled trial. Ann Inter Med. 2004;141(12): 911-919.
189. Young I, Cleland J, Aguilera A, et al. Manual therapy, exercise, and traction for patients with cervical radiculopathy: a randomized clinical trial. Phys Ther. 2009;89:632-642.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine








 The role of epigenetic modification in sustaining the effects of environmental experience has also been demonstrated in the context of postnatal mother�infant interactions. Individual variations in maternal care during the immediate postpartum period in rats are associated with changes in offspring hypothalamic-pituitary-adrenal (HPA) activity, neuroendocrine systems involved in reproduction and hippocampal plasticity [13]. Analyses of levels of promotor methylation within the hippocampal GR 17 and hypothalamic ERa genes in offspring of rat dams that provide high vs. low levels of maternal care indicate that high levels of care are associated with decreased promotor methylation and thus increased gene expression [14,15]. Though the route through which these epigenetic changes are mediated is not yet clear, there is evidence for increased binding of nerve growth factor-inducible protein A (NGFI-A) to the GR exon 17 promoter amongst offspring who receive high levels of care in infancy [15] and in vitro models suggest that NGFI-A up-regulation is associated with histone acetylation, DNA demethylation, and activation of the exon 17 GR promoter [16]. The relevance of these effects in humans has recently been demonstrated by Oberlander et al. [17] in the analysis of methylation status of the GR promotor at NGFI-A binding sites in cord blood mononuclear cells of infants exposed to third trimester maternal depressed or anxious mood. Maternal depression was found to be associated with increased GR 1F promotor methylation in fetal blood samples and these methylation patterns predicted HPA reactivity in infants at 3 months of age [17]. Analysis of hippocampal tissue from suicide victims with a history of childhood abuse similarly indicates lower GR expression and higher GR 1F promotor methylation associated with disruptions of the early environment and confirms the findings from rodent studies that differential NGFI-A binding is a functional consequence of these epigenetic effects [18]. However, the impact of perinatal mother� infant interactions is not limited to GR regulation as illustrated by Roth et al. [19] examining the effects of postnatal abuse on offspring brain derived neurotrophic factor (BDNF) methylation [19]. In rats, an increase in methylation of exon IV of the BDNF promotor and consequent decrease in BDNF mRNA in the prefrontal cortex was found in association with exposure to periods of abusive maternal care (dragging, rough handling, etc.). As was the case with the effects of individual differences in maternal care, these effects emerged in infancy and were sustained into adulthood. Moreover, these effects on BDNF exon IV methylation are perpetuated to the F1 generation suggesting a role for epigenetic mechanisms in transgenerational effects [20].
The role of epigenetic modification in sustaining the effects of environmental experience has also been demonstrated in the context of postnatal mother�infant interactions. Individual variations in maternal care during the immediate postpartum period in rats are associated with changes in offspring hypothalamic-pituitary-adrenal (HPA) activity, neuroendocrine systems involved in reproduction and hippocampal plasticity [13]. Analyses of levels of promotor methylation within the hippocampal GR 17 and hypothalamic ERa genes in offspring of rat dams that provide high vs. low levels of maternal care indicate that high levels of care are associated with decreased promotor methylation and thus increased gene expression [14,15]. Though the route through which these epigenetic changes are mediated is not yet clear, there is evidence for increased binding of nerve growth factor-inducible protein A (NGFI-A) to the GR exon 17 promoter amongst offspring who receive high levels of care in infancy [15] and in vitro models suggest that NGFI-A up-regulation is associated with histone acetylation, DNA demethylation, and activation of the exon 17 GR promoter [16]. The relevance of these effects in humans has recently been demonstrated by Oberlander et al. [17] in the analysis of methylation status of the GR promotor at NGFI-A binding sites in cord blood mononuclear cells of infants exposed to third trimester maternal depressed or anxious mood. Maternal depression was found to be associated with increased GR 1F promotor methylation in fetal blood samples and these methylation patterns predicted HPA reactivity in infants at 3 months of age [17]. Analysis of hippocampal tissue from suicide victims with a history of childhood abuse similarly indicates lower GR expression and higher GR 1F promotor methylation associated with disruptions of the early environment and confirms the findings from rodent studies that differential NGFI-A binding is a functional consequence of these epigenetic effects [18]. However, the impact of perinatal mother� infant interactions is not limited to GR regulation as illustrated by Roth et al. [19] examining the effects of postnatal abuse on offspring brain derived neurotrophic factor (BDNF) methylation [19]. In rats, an increase in methylation of exon IV of the BDNF promotor and consequent decrease in BDNF mRNA in the prefrontal cortex was found in association with exposure to periods of abusive maternal care (dragging, rough handling, etc.). As was the case with the effects of individual differences in maternal care, these effects emerged in infancy and were sustained into adulthood. Moreover, these effects on BDNF exon IV methylation are perpetuated to the F1 generation suggesting a role for epigenetic mechanisms in transgenerational effects [20].