Muscular energy techniques, or METs, are considered to be some of the most valuable tools any healthcare professional can have and there are several reasons for it. METs have a wide application range and essential modifications can be made for each of them for a variety of injuries and/or conditions. Muscular energy techniques also represent an important aspect of rehabilitation. Furthermore, METs are both gentle and effective. But most importantly, METs actively involve the patient in the recovery process. Unlike other types of treatment therapies, the patient is involved in every step, contracting at the appropriate time, relaxing at the appropriate time, engaging in eye movement, and even breathing when instructed by the healthcare professional.
Muscular energy techniques have been used with other treatment modalities, such as the McKenzie method, to improve the outcome measures of injuries or conditions. The following research study demonstrates clinical and experimental evidence on the impact of the McKenzie method with METs for low back pain, one of the most common complaints affecting spine health. The purpose of the article is to educate and advice patients with low back pain on the use of METs with the McKenzie method.
Impact of McKenzie Method Therapy Enriched by Muscular Energy Techniques on Subjective and Objective Parameters Related to Spine Function in Patients with Chronic Low Back Pain
Abstract
Background: The high incidence and inconsistencies in diagnostic and therapeutic process of low back pain (LBP) stimulate the continuing search for more efficient treatment modalities. Integration of the information obtained with various therapeutic methods and a holistic approach to the patient seem to be associated with positive outcomes.The aim of this study was to analyze the efficacy of combined treatment with McKenzie method and Muscle Energy Technique (MET), and to compare it with the outcomes of treatment with McKenzie method or standard physiotherapy in specific chronic lumbar pain.
Material/Methods: The study included 60 men and women with LBP (mean age 44 years). The patients were randomly assigned to 1 of 3 therapeutic groups, which were further treated with: 1) McKenzie method and MET, 2) McKenzie method alone, or 3) standard physiotherapy for 10 days. The extent of spinal movements (electrogoniometry), level of experienced pain (Visual Analogue Scale and Revised Oswestry Pain Questionnaire), and structure of the spinal discs (MRI) were examined prior to the intervention, immediately thereafter, and 3 months after the intervention.
Results: McKenzie method enriched with MET had the best therapeutic outcomes. The mobility of cervical, thoracic, and lumbar spine normalized at levels corresponding to 87.1%, 66.7%, and 95% of respective average normative values. Implementation of McKenzie method, both alone and combined with MET, was associated with a significant decrease in Oswestry Disability Index, significant alleviation of pain (VAS), and significantly reduced size of spinal disc herniation.
Conclusions: The combined method can be effectively used in the treatment of chronic LBP.
MeSH Keywords:Low Back Pain, Manipulation, Chiropractic, Manipulation, Spinal
Background
Low back pain (LBP) is the most prevalent form of musculoskeletal disorder. According to published statistical data, 70�85% of people experience LBP at some stage of their lives [1�7]. Only 39�76% of the patients recover completely after an acute episode of pain, suggesting that a considerable fraction of them develop a chronic condition [8].
The goals of physiotherapy in patients with chronic LBP include elimination of pain, restoration of the lost extent of movements, functional improvement, and improvement of the quality of life. These objectives are achieved by various protocols of exercise, manipulation, massage, relaxation techniques, and counselling. Although numerous previously published studies have dealt with various therapeutic modalities of LBP, the evidence of their efficacy is highly inconclusive [9�12]. At present the management of chronic LBP still raises many controversies. Inconsistency of established diagnoses and implemented protocols of management points to the importance of the problem in question. Despite extensive research, the issue of spinal pain management still constitutes a challenge for physicians, physiotherapists, and researchers [8,13].
McKenzie method is 1 of many treatment modalities of LBP. It is a system of mechanical diagnosis and management of spinal pain syndromes, based on comprehensive and reproducible evaluation, knowledge of symptoms patterns, directional preference, and centralization phenomenon. This method is focused on the spinal disc disorders [14]. McKenzie method is based on the phenomenon of movement of the nucleus pulposus inside the intervertebral disc, depending on the adopted position and the direction of the movements of the spine. The nucleus pulposus that is exposed to the pressure from both surfaces of the vertebral bodies takes the shape of a spherical joint. This means that it has the ability to perform 3 rotary movements in all directions and has 6 degrees of freedom of movement. The nucleus pulposus performs the movements of flexion, extension, lateral bend (left and right), rotation (right and left), linear displacement (slip) along the sagittal axis, linear displacement along the transverse axis and the separation or approximation along the vertical axis [15].Numerous studies have shown that during forward bend of the spine it is possible to observe extension of the rear surface of the fibrous ring, compressing of the front part of the intervertebral disc and the shift of nucleus pulposus to the dorsal side. When stretching, the mechanism is the opposite [16].
The musculoskeletal system is vital for the maintenance of the balanced tension of the body. Musculofascial disorders can be associated with various problems, pain, or even loss of some motor function. Muscle Energy Techniques (MET) are among the most popular therapeutic modalities aimed at the improvement of elasticity in contractile and non-contractile tissues [17].
High incidence, inconsistencies in diagnostic and therapeutic process, and huge costs associated with the management of chronic spinal disorders stimulate the continuing search for more efficient treatment modalities. This requires the knowledge of neurophysiological processes, proper interpretation of pain, identification of unfavorable motor and postural patterns, holistic approach to the patient, and integration of the information obtained with various therapeutic methods [18].
The aim of this study was to analyze the efficacy of combined treatment with McKenzie method and MET, and to compare it with the outcomes of treatment with McKenzie method or standard physiotherapy in chronic lumbar pain. We evaluated the effect exerted by each of the interventions on the extent of movements, level of experienced pain, and structure of the spinal discs as assessed by means of magnetic resonance imaging.
Material and Methods
Patients
The randomized study included 60 men and women with mean age of 44 years. All individuals were diagnosed by a specialist physician and referred for rehabilitation. The protocol of the study was approved by the Local Bioethical Committee of the Poznan University of Medical Sciences (decision no. 368/0). All patients were diagnosed with chronic spinal pain persisting for longer than 1 year. The inclusion criteria of the study were: 1) documented magnetic resonance imaging (MRI) of the spine, 2) confirmed protrusion or bulging in the lumbosacral spine, 3) intermittent lumbosacral pain, 4) projection of pain to the buttock or thigh, 5) unilateral character of the symptoms. The exclusion criteria were: 1) confirmed extrusion or sequestration of nucleus pulposus of the spinal disc, 2) symptoms manifesting below the knee, 3) history of spinal surgery, 4) structural disorders of spinal discs in more than 2 spinal segments, 5) evident stenosis of the spinal canal, 6) focal lesions of the spinal cord, and 7) spondylolisthesis.
Patients showed great interest and all completed the study.
Protocol
The following tests were used to determine the baseline (i.e. pre-intervention) parameters of the studied patients: 1) electrogoniometric determination of the extent of movement in all spinal segments and angular values of physiological curvatures, 2) Oswestry questionnaire, and 3) Visual Analogue Scale (VAS). Subsequently, the patients were randomly assigned to 1 of 3 therapeutic groups (20 persons each), which were further treated with: 1) McKenzie method and MET, 2) McKenzie method alone, 3) standard physiotherapy. Each of the 3 therapeutic protocols included 10 daily sessions, performed during 5 consecutive weekdays. 24 hours following the last therapeutic session, the same parameters as at the baseline were determined by the investigator blinded to the treatment assignment. Moreover, all patients were subjected to repeated magnetic resonance.
Therapeutic Intervention
McKenzie group One session lasted 30 minutes. On the basis of the McKenzie spinal pain classification, the derangement syndrome was diagnosed in all patients [14]. The therapy included hyperextension techniques, hyperextension with self-pressure or pressure by the therapist, and hyperextensive mobilization. These techniques were applied in the sagittal plane, following the rule of force progression [14]. Moreover, the patients were asked to self-perform the therapeutic procedure at home (5 cycles per day with 2-hour intervals, 15 repetitions each).
McKenzie + MET group The classic McKenzie method enriched with Muscle Energy Technique was implemented. McKenzie protocol in both groups (McKenzie McKenzie + MET) was the same. All patients in this therapeutic group were also diagnosed with the derangement syndrome. A technique of post-isometric relaxation was used at the end of each therapeutic session. It was characterized by the following parameters: 1) time of contraction equal to 7�10 seconds, 2) intensity of contraction corresponding to 20�35%, 3) beginning in the intermediate extent of movement for a given patient, 4) 3 seconds of interval between consecutive contraction phases, 5) 3 repetitions, 6) contraction of antagonist muscle at the terminal phase of the procedure, 7) passive return to the baseline position. The procedure involved relaxation of the erector spinae muscle group and was performed in a sitting position. The exercise was performed in an anterior and lateral flexion, and in rotation. The therapy involved bilateral parts of the erector spinae so as to balance the muscular tension [17]. The duration of 1 combined session was 40 minutes. Patients treated with the combined method were also asked to exercise at home (5 cycles per day with 2-hour intervals, 15 repetitions each).
Standard treatment group Individuals randomized to this therapeutic group were treated with classical massage, laser therapy, and transcutaneous electrical nerve stimulation (TENS) applied to the lumbosacral region. Additionally, the patients were asked to perform general exercises strengthening spinal and abdominal muscles (once a day at home). The exercises were to be performed for 15 minutes, in a prone, supine, and lateral position. The aim of the training was to strengthen the muscles stabilizing the pelvic girdle, i.e. the erector spinae, quadratus lumborum, rectus abdominis, oblique abdominal, gluteal, and iliopsoas muscles. The classical massage lasted 20 minutes. The laser therapy was conducted with a contact technique with Lasertronic LT-2S device. The duration of laser therapy was 80 seconds (2�40 s). The treatment was applied on both sides of the spinous processes of the lumbar spine. The parameters of the procedure were as follows: energy 32 J, power of radiation 400 mW, wavelength 810 nm, continuous mode. TENS electrotherapy was performed with Diatronic DT-10B device. The electrodes were placed on both sides of the lumbosacral spine. The parameters of the TENS procedure were as follows: duration 15 minutes, frequency 50 Hz, current 20�30 mA (subjectively adjusted), duration of a single impulse 50 microseconds. The total time per session=36 min 20 sec + 15 min as home exercises once a day.
Evaluation of Therapeutic Effect
Electrogoniometry The extent of movements and the angles of spinal curvatures were determined with tensiometric Penny & Giles electrogoniometer in Boocok�s modification [19], which prevents potential measurement bias associated with shifting skin and soft tissues in relation to bones. The electrogoniometer enables linear measurement with a bias no greater than 1�. The measurements were taken according to Lewandowski�s methodology [20]. The reliability of these measurements was previously verified by Szulc et al.21 The reference values used in our study were calculated on the basis of Lewandowski�s measurements taken in a group of about 20 000 individuals [20].
Revised Oswestry pain questionnaire The degree to which the dysfunction of the lumbar spine limited the performance of the activities of daily living was determined with the Revised Oswestry Pain Questionnaire [22,23]. We used the revised version of the questionnaire as it is the only variant of this instrument which examines the changes in the level of lumbar pain. The survey was conducted twice, prior to and after the therapy.
Visual analogue scale (VAS) To verify the efficacy of the therapy, the participants were examined with the visual analogue scale (VAS) at the baseline (prior to the intervention) and 24 hours after completing the treatment [24].
Magnetic resonance imaging The degree of degeneration of the spinal discs and the therapeutic outcome were verified on magnetic resonance imaging performed prior to and after the intervention, at the same time of the day. The examination was conducted in sagittal and axial planes, and used T1- and T2-weighted images. The displacement of the nucleus pulposus was expressed in mm. The methodology of examination was described previously by Fazey et al. [25].
Statistical Analysis
Statistical analysis was conducted with Statistica 10.0 software. Bivariate analysis of variance (AVOVA) with 1 intergroup factor (type of intervention) and 1 intragroup factor (measurement prior to intervention, 24 hours and 3 months after the intervention) was used to analyze the differences in studied parameters resulting from the type of the implemented therapy, and to verify the efficacy of various therapeutic protocols. The significance of differences in multiple comparisons was verified with the Scheff�s post-hoc test.
Dr. Alex Jimenez’s Insight
Low back pain is a common symptom that can be treated in a number of ways. Chiropractic care is one of the most common alternative treatment options for LBP, however, healthcare professionals have started using other treatment modalities to help improve symptoms of low back pain. Physical therapy and exercise have commonly been used together, alongside well-known treatment modalities, to help speed up the patient’s recovery process. The research study aims to determine how the McKenzie method and muscular energy techniques can improve low back pain and promote overall health and wellness. As a doctor of chiropractic, the positive effects of physical therapy and exercise is reflected on the recovery of patients.
Results
The significant effects of bivariate interaction (method � time) suggest that the implemented therapeutic methods exerted variable time-dependent effect on the functional parameters of the spine, Oswestry questionnaire scores, values of visual analog scale, and the results of magnetic resonance imaging in patients with chronic low back pain.
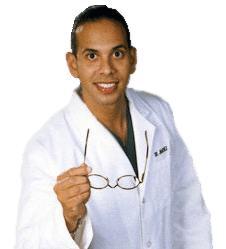
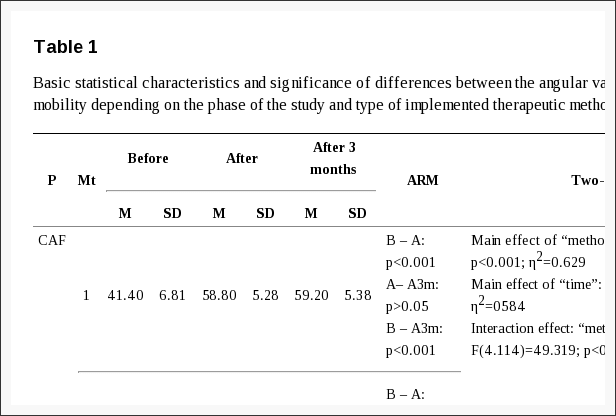
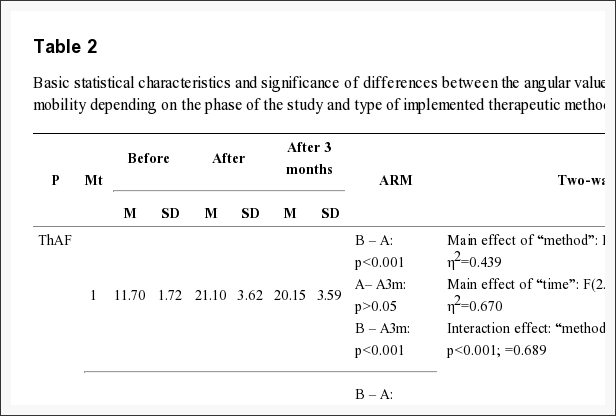
Data on the mobility of various spinal segments prior to the intervention, and 24 hours and 3 months after the intervention suggests that the implementation of McKenzie method enriched with MET was reflected by better therapeutic outcome compared to classical McKenzie method and standard physiotherapy. Mobility of various spinal segments in all axes and planes improved significantly as a result of the therapy with McKenzie method enriched in MET. In contrast, the least pronounced improvement of spinal mobility was documented in the case of standard physiotherapy (Tables 1?�3).
Table 1: Basic statistical characteristics and significance of differences between the angular values of the cervical spine mobility depending on the phase of the study and type of implemented therapeutic method.
Table 2: Basic statistical characteristics and significance of differences between the angular values of the thoracic spine mobility depending on the phase of the study and type of implemented therapeutic method.
Table 3: Basic statistical characteristics and significance of differences between the angular values of the lumbar spine mobility depending on the phase of the study and type of implemented therapeutic method.
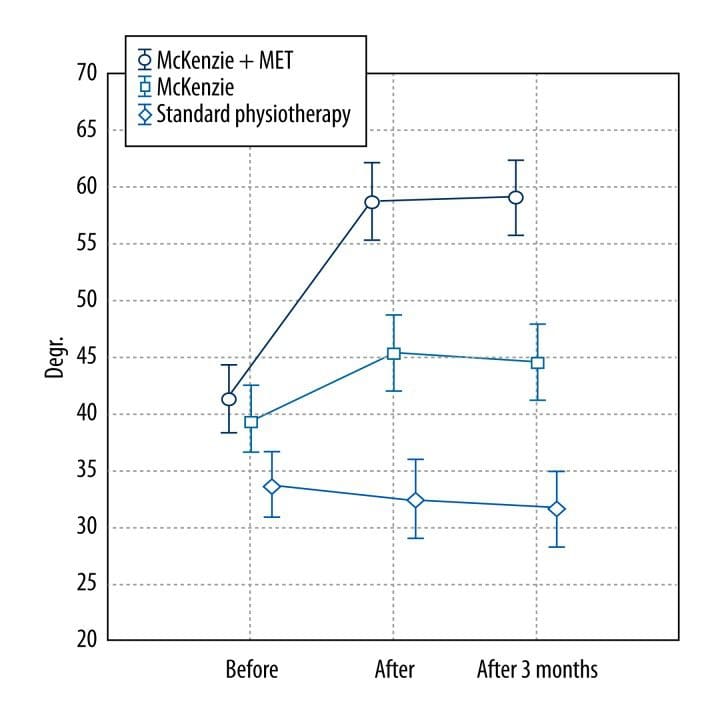
The analysis of the anterior flexion of the cervical spine revealed that the improvement of mobility was most pronounced in McKenzie + MET group (?%=42.02). The lack of significant difference between the measurement taken immediately after the intervention and 3 months thereafter suggests that the therapeutic effect was persistent. Less pronounced, albeit significant, improvement of the mobility was also documented in the case of McKenzie method alone (?%=14.79); also this effect persisted after 3 months. In contrast, no significant changes in the extent of anterior flexion of the cervical spine were documented in the group subjected to standard physiotherapy (Figure 1).
Figure 1: Mean angular values of the anterior flexion of the cervical spine determined at various phases of the study in patients treated with three different therapeutic methods (McKenzie method + MET, McKenzie method alone, standard physiotherapy).
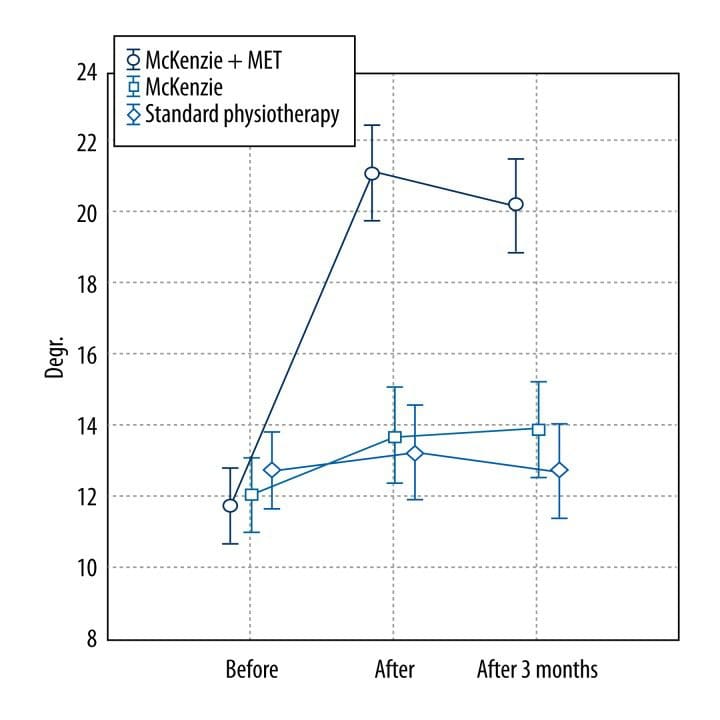
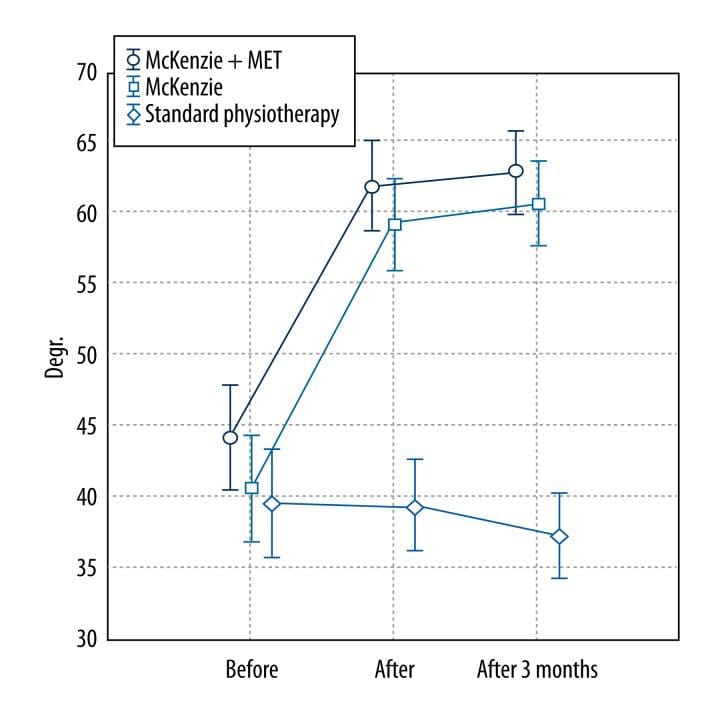
Also, the analysis of changes in the degree of thoracic and lumbar spine anterior flexion revealed variability in the outcomes of the studied methods (Figures 2, ?3).
Figure 2: Mean angular values of the anterior flexion of the thoracic spine determined at various phases of the study in patients treated with three different therapeutic methods (McKenzie method + MET, McKenzie method alone, standard physiotherapy).
Figure 3: Mean angular values of the anterior flexion of the lumbar spine determined at various phases of the study in patients treated with three different therapeutic methods (McKenzie method + MET, McKenzie method alone, standard physiotherapy).
The greatest improvement of the mobility, equal to ?%=80.34 and ?%=40.43 in the thoracic and lumbar segment, respectively, was documented in the McKenzie + MET group. The lack of significant difference between the measurements of both the segments taken immediately after the intervention and 3 months thereafter suggests that the therapeutic effect was persistent (Tables 2, ?3). The changes in the remaining functional spinal parameters followed a similar pattern and are summarized in Tables 1?�3.
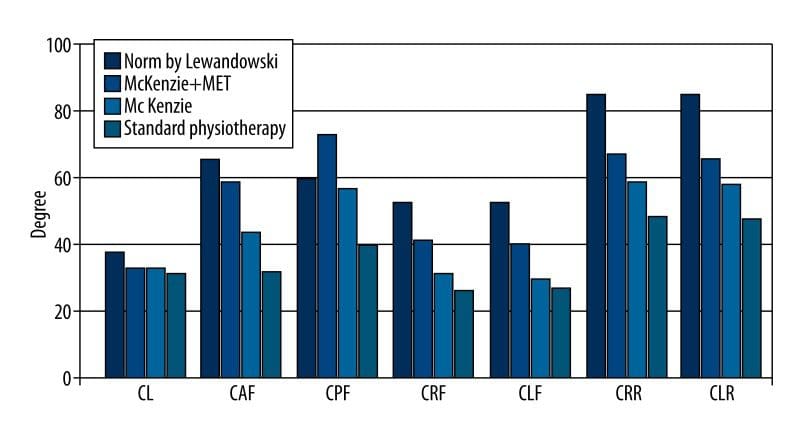
The degree of mobility in various spinal segments observed after implementation of studied therapeutic methods was compared with respective average normative values published by Lewandowski [20[ (Figures 4?�6). Implementation of McKenzie method enriched with MET was reflected by the most pronounced improvement in the spinal mobility, which fit within the respective normative ranges. The functional parameters of cervical, thoracic, and lumbar spine normalized at levels corresponding to 87.1%, 66.7%, and 95% of respective average normative values.
Figure 4: Functional parameters of the cervical spine (CL � cervical lordosis; CAF � cervical anterior flexion; CPF � cervical posterior flexion; CRF � cervical right flexion; CLF � cervical left flexion; CRR � cervical right rotation; CLR � cervical left rotation) � comparison between values determined in patients treated with three different therapeutic methods and respective normative values published by Lewandowski.
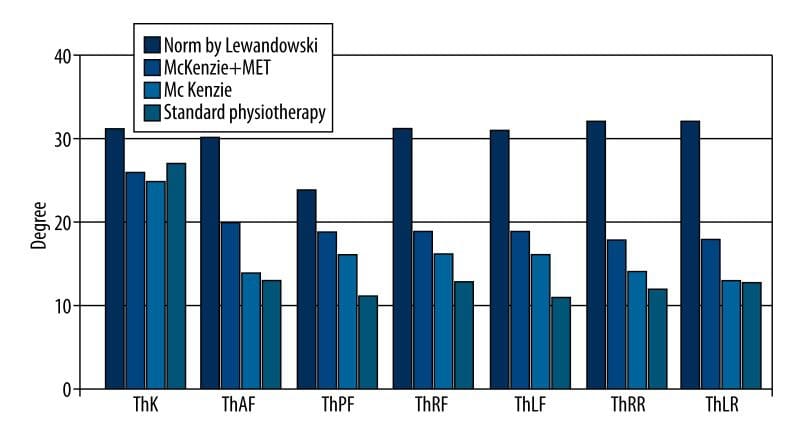
Figure 5: Functional parameters of the thoracic spine (ThK � thoracic kyphosis; ThAF � thoracic anterior flexion; ThPF � thoracic posterior flexion; ThRF � thoracic right flexion; ThLF � thoracic left flexion; ThRR � thoracic right rotation; ThLR � thoracic left rotation) � comparison between values determined in patients treated with three different therapeutic methods and respective normative values published by Lewandowski.
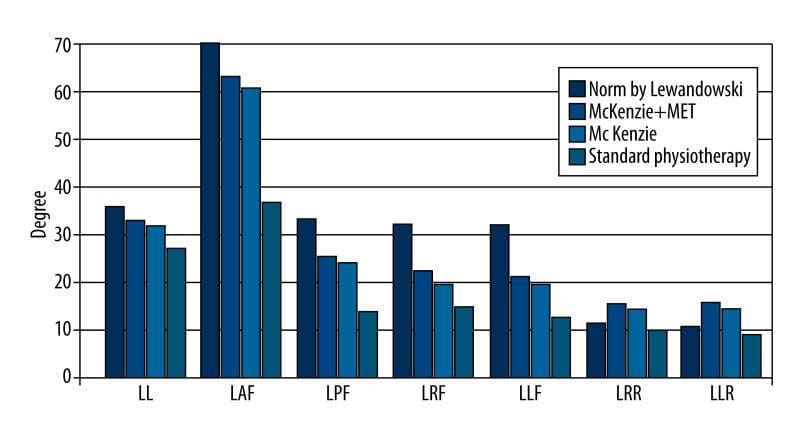
Figure 6: Functional parameters of the lumbar spine (LL � lumbar lordosis; LAF � lumbar anterior flexion; LPF � lumbar posterior flexion; LRF � lumbar right flexion; LLF � lumbar left flexion; LRR � lumbar right rotation; LLR � lumbar left rotation) � comparison between values determined in patients treated with three different therapeutic methods and respective normative values published by Lewandowski.
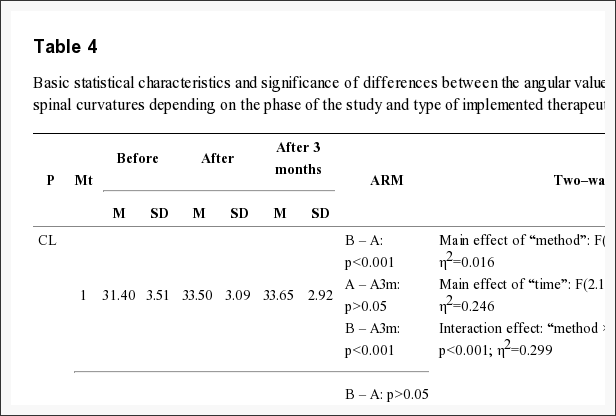
Irrespective of the therapeutic method and timing of measurement, the angular values of all spinal curvatures fit within the respective normative values and no significant inter- and intragroup differences were documented (Table 4).
Table 4: Basic statistical characteristics and significance of differences between the angular values of the physiological spinal curvatures depending on the phase of the study and type of implemented therapeutic method.
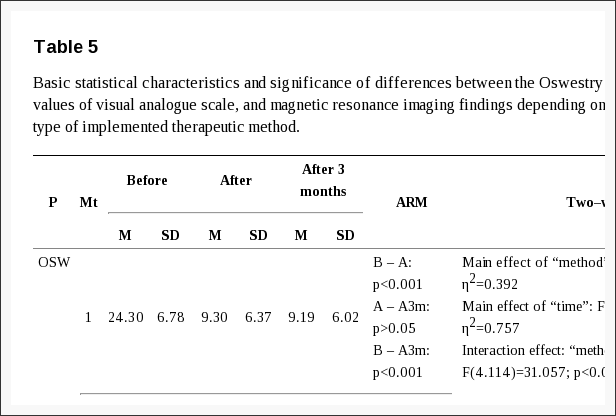
The scores of Oswestry questionnaire also differed depending on the type of implemented intervention. Implementation of McKenzie method, both alone and combined with MET, was reflected by a significant decrease in Oswestry Disability Index. No significant differences were documented between the outcomes of these 2 methods. In contrast, standard physiotherapy had the least pronounced effect on the Oswestry Disability Index (Table 5).
Table 5: Basic statistical characteristics and significance of differences between the Oswestry questionnaire scores, values of visual analogue scale, and magnetic resonance imaging findings depending on the phase of the study and type of implemented therapeutic method.
The analysis of visual analogue scale values suggests that both McKenzie method enriched with MET and classical McKenzie method produced the strongest therapeutic effects, i.e. alleviation of pain. Implementation of both these methods was reflected by marked augmentation of experienced pain, without any significant intergroup differences. In contrast, standard physiotherapy reduced pain to a minimal extent, and no significant differences were observed between VAS scores obtained prior to and after this intervention (Table 5).
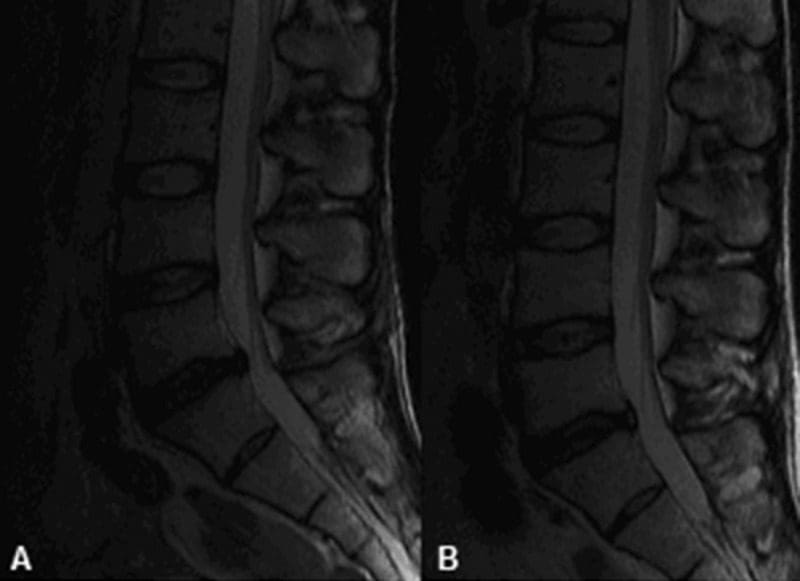
Magnetic resonance imaging performed prior to and after the intervention confirmed that McKenzie method enriched with MET produced the best therapeutic outcome manifested by a reduced size of spinal disc herniation. Smaller, albeit significant, improvement of this parameter was also documented in the case of classical McKenzie method. These 2 therapeutic methods did not differ significantly in terms of the post-intervention size of the spinal disc herniation. In contrast, no reduction in the size of the spinal disc herniation was documented after implementation of standard physiotherapy (Table 5).
Discussion
The number of studies validating the efficacy of combined therapeutic methods and techniques is sparse [3,21,26,27]. Wilson et al. [26] concluded that MET is an optimal adjunct technique for other therapeutic modalities [26].
Many studies confirmed the positive effects of McKenzie method [28�36]. Similarly, a body of evidence confirms the therapeutic value of MET [37�44]. Moreover, positive outcomes of both these techniques were documented in patients with spinal pain, including LBP [45,46]. However, to the best of our knowledge, none of the previous studies verified whether the combination of these methods improves the therapeutic outcome.
Noticeably, both the therapies are based on different concepts and involve different therapeutic techniques. The McKenzie method is oriented at the management of all structural abnormalities of the spinal discs. The aim of this therapy is to eliminate pain and normalize function of the affected spinal segment [14]. Therefore, McKenzie method focuses on the treatment of spinal disc pathologies as the principal cause of pain. Takasaki et al. [35] documented positive changes in the spinal disc, i.e. the resolution of herniation, in patient treated with McKenzie method.
However, various injuries and other medical conditions, as well as repetitive negative motor pattern, are also reflected by the disorders of the musculofascial system. This can be reflected by the development of certain compensatory mechanisms, accumulation of muscular tension, motor limitation, and functional disorders [17,40,42]. In contrast, the treatment of the musculofascial system is not included in the concept of McKenzie method. Therefore, the aim of including the muscle energy techniques in the proposed protocol of combined therapy was to potentiate its therapeutic effect through the relaxation and stretching of contracted musculature, strengthening of weakened muscles, reduction of passive muscular tension, improvement of joint mobility, and normalization of motor function [26,43].
The differences observed with regards to the mobility of various spinal segments prior to and after the intervention point to better therapeutic outcome of the combined methods. Noticeably, improved mobility was documented not only in the lumbar spine but also in the cervical and thoracic segment. Therefore, the implementation of MET improved the scope of the combined method (McKenzie + MET) as compared to the classical McKenzie method. Our findings suggest that musculofascial disorders may to a large extent be responsible for limited spinal mobility in patients with chronic LBP. In their papers on the therapeutic effects of manual therapy, Pool et al. [12] and Zaproudina et al. [47] emphasize the importance of limitations in spinal mobility as a sensitive marker of pathological changes.
The magnetic resonance findings documented in patients treated with combined McKenzie method and MET suggest that this combination has no negative effect on the size of spinal disc herniation (Figure 7). This confirms the safety of MET and plausibility of its application in patients with spinal disc pathologies [26]. Of note, relatively large subjective and objective improvements were achieved despite the short duration of the treatment, which included only 10 sessions throughout a 2-week period.
Figure 7: Magnetic resonance images of the structural changes of the L5�S1 spinal disc: (A) prior to, and (B) after the combined therapy (McKenzie method + MET).
Furthermore, control electrogoniometry conducted 3 months after the intervention confirmed the persistent effect of the combined treatment. Moreover, a slight improvement was documented in the case of some functional parameters examined immediately after the intervention and 3 months thereafter. Perhaps, this phenomenon reflected proper education of our patients and further prophylactic self-exercising according to McKenzie method.
Chronic low back pain (CLBP) has a multifactorial etiology [18], and as such requires multimodal treatment. The evidence of therapeutic effects should not be limited to the diagnostic imaging, but mostly be reflected by functionality of a patient, level of experienced pain, extent of movements, and normalization of motor function.
Conclusions
The following conclusions can be formulated on the basis of our findings:
Comparison of the subjective and objective outcomes of 3 therapeutic methods � standard physiotherapy, McKenzie method alone, and McKenzie method combined with MET � in patients with chronic low back pain suggests that the combined method is the most effective.
The use of the combined method (McKenzie + MET) exerts a positive effect on structural (resolution of spinal disc herniation documented on MRI) and functional parameters (improved mobility of various spinal segments), improves the quality of life, and reduces the level of experienced pain.
Acknowledgements
The study was conducted under the auspices of the University School of Physical Education in Poznan. The authors express their gratitude to the owners of the Private Rehabilitation Practice �Antidotum� for consent to perform the study in their facility.
Footnotes
Source of support: The study was supported by the resources from the Ministry of Science and Higher Education for the statutory activity of the Department of Anatomy of the University School of Physical Education in Poznan
Conflict of interest: None declared.
In conclusion, the research study demonstrating clinical and experimental evidence on the impact of the McKenzie method with METs for low back pain, one of the most common complaints affecting spine health, concluded that the combined treatment modalities were effectively used in the improvement of chronic low back pain. The purpose of the article was to educate and advice patients with low back pain on the use of METs with the McKenzie method. Furthermore, the use of the combined treatment modalities demonstrated a positive effect on structural and functional parameters, improving the patient’s quality of life and reducing the level of pain they experienced. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
[accordions title=”References”]
[accordion title=”References” load=”hide”]1. Drozda K, Lewandowski J, G�rski P. Back pain in lower and upper secondary school pupils living in urban areas of Poland. The case of Poznan. Ortopedia, Traumatologia, Rehabilitacja. 2011;13(5(6)):489�503. [PubMed]
2. Drozda K, Lewandowski J. Epidemiology of back pain among secondary school pupils in Poznan. Fizjoterapia Polska. 2011;4(1):31�40.
3. Dunsford A, Kumar S, Clarke S. Integrating evidence into practice: use of McKenzie-based treatment for mechanical low back pain. J Multidiscip Healthc. 2011;4:393�402. [PMC free article] [PubMed]
4. Joud A, Petersson IF, Englund M. Low back pain: epidemiology of consultations. Arthritis Care Res (Hoboken) 2012;64:b1084�88. [PubMed]
5. Lewandowski J, Szulc P, Boch-Kmieciak J, et al. Epidemiology of low back pain in students of physical education and physiotherapy. Studies in Physical Culture and Tourism. 2011;18(3):265�69.
6. Pereira LM, Obara K, Dias JM, et al. Comparing the Pilates method with no exercise or lumbar stabilization for pain and functionality in patients with chronic low back pain: systematic review and meta-analysis. Clin Rehabil. 2012;26:10�20. [PubMed]
7. Werneke MW, Hart D, Oliver D, et al. Prevalence of classification methods for patients with lumbar impairments using the McKenzie syndromes, pain pattern, manipulation, and stabilization clinical prediction rules. J Man Manip Ther. 2010;18:197�204. [PMC free article] [PubMed]
8. da C Menezes Costa L, Maher CG, Hancock MJ, et al. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012;184:E613�24. [PMC free article] [PubMed]
9. Borges TP, Greve JM, Monteiro AP, et al. Massage application for occupational low back pain in nursing staff. Rev Lat Am Enfermagem. 2012;20:511�19. [PubMed]
10. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized, controlled trial. Ann Intern Med. 2011;155:1�9. [PMC free article] [PubMed]
11. Kilpikoski S, Al�n M, Paatelma M, et al. Outcome comparison among working adults with centralizing low back pain: Secondary analysis of a randomized controlled trial with 1-year follow-up. Adv Physiother. 2009;11:210�17.
12. Pool JJ, Ostelo RW, Knol DL, et al. Is a behavioral graded activity program more effective than manual therapy in patients with subacute neck pain? Results of a randomized clinical trial. Spine. 2010;35:1017�24. [PubMed]
13. Frankel BS, Moffett JK, Keen S, et al. Guidelines for low back pain: changes in GP management. Fam Pract. 1999;16:216�22. [PubMed]
14. McKenzie R, May S. The lumbar spine: mechanical diagnosis and therapy. 2nd ed. Waikanae: Spinal Publications; 2003.
15. Kanpandji AI. Anatomia funkcjonalna staw�w. Tom 3.6 ed. Wroc?aw: Elsevier Urban & Partners; 2010. [in Polish]
16. Alexander LA, Hancock E, Agouris I, et al. The response of the nucleus pulposus of the lumbar intervertebral discs to functionally loaded positions. Spine. 2007;32(14):1508�12. [PubMed]
17. Chaitow L. Muscle energy techniques. 3rd ed. Edinburgh: Churchill Livingstone; 2006.
18. O�Sullivan P. It�s time for change with the management of non-specific chronic low back pain. Br J Sports Med. 2012;46:224�27. [PubMed]
19. Boocock MG, Jackson JA, Burton AK, et al. Continuous measurement of lumbar posture using flexible electrogoniometers. Ergonomics. 1994;37:175�85. [PubMed]
20. Lewandowski J. Formation of physiological curvatures and segmental mobility of the human spine aged from 3 to 25 years in electrogoniometric studies. 1st ed. Poznan: AWF Poznan; 2006.
21. Szulc P, Lewandowski J, Marecki B. Verification of selected anatomic landmarks used as reference points for universal goniometer positioning during knee joints mobility range measurements. Med Sci Monit. 2001;7:312�15. [PubMed]
22. Fairbank JC, Pynsent PB. The Oswestry disability index. Spine. 2000;25:2940�52. [PubMed]
23. Hicks GE, Manal TJ. Psychometric properties of commonly used low back disability questionnaires: are they useful for older adults with low back pain? Pain Med. 2009;10:85�94. [PMC free article] [PubMed]
24. Mudgalkar N, Bele SD, Valsangkar S, et al. Utility of numerical and visual analog scales for evaluating the post-operative pain in rural patients. Indian J Anaesth. 2012;56:553�57. [PMC free article] [PubMed]
25. Fazey PJ, Takasaki H, Singer KP. Nucleus pulposus deformation in response to lumbar spine lateral flexion: an in vivo MRI investigation. Eur Spine J. 2010;19(11):1115�20. [PMC free article] [PubMed]
26. Wilson E, Payton O, Donegan-Shoaf L, et al. Muscle energy technique in patients with acute low back pain: a pilot clinical trial. J Orthop Sports Phys Ther. 2003;33:502�12. [PubMed]
27. Bronfort G, Goldsmith CH, Nelson CF, et al. Trunk exercise combined with spinal manipulative or NSAID therapy for chronic low back pain: a randomized, observer-blinded clinical trial. J Manipulative Physiol Ther. 1996;19:570�82. [PubMed]
28. Bybee RF, Olsen DL, Cantu-Boncser G, et al. Centralization of symptoms and lumbar range of motion in patients with low back pain. Physiother Theory Pract. 2009;25:257�67. [PubMed]
29. Chen J, Phillips A, Ramsey M, et al. A case study examining the effectiveness of mechanical diagnosis and therapy in a patient who met the clinical prediction rule for spinal manipulation. J Man Manip Ther. 2009;17:216�20. [PMC free article] [PubMed]
30. Garcia AN, Gondo FL, Costa RA, et al. Effects of two physical therapy interventions in patients with chronic non-specific low back pain: feasibility of a randomized controlled trial. Rev Bras Fisioter. 2011;15:420�27. [PubMed]
31. Hosseinifar M, Akbari M, Behtash H, et al. The effects of stabilization and Mckenzie exerciseson transverse abdominis and multifidus muscle thickness, pain, and disability: A randomized controlled trial in nonspecific chronic low back pain. J Phys Ther Sci. 2012;25:1541�45. [PMC free article] [PubMed]
32. Mbada CE, Ayanniyi O, Ogunlade SO, et al. Influence of Mckenzie protocol and two modes of endurance exercises on health-related quality of life of patients with long-term mechanical low-back pain. Pan Afr Med J. 2014;17(Supp 1):5. [PMC free article] [PubMed]
33. Garcia AN, da Cunha Menezes Costa L, Hancock MJ, et al. Efficacy of the McKenzie method in patients with chronic nonspecific low back pain: a protocol of randomized placebo-controlled trial. Phys Ther. 2015;95:267�73. [PubMed]
34. Schenk RJ, Jozefczyk C, Kopf A. A randomized trial comparing interventions in patients with lumbar posterior derangement. J Man Manip Ther. 2003;11:95�102.
35. Takasaki H, May S, Fazey PJ, et al. Nucleus pulposus deformation following application of mechanical diagnosis and therapy: a single case report with magnetic resonance imaging. J Man Manip Ther. 2010;18:153�58. [PMC free article] [PubMed]
36. Williams B, Vaughn D, Holwerda T. A mechanical diagnosis and treatment (MDT) approach for a patient with discogenic low back pain and a relevant lateral component: a case report. J Man Manip Ther. 2011;19:113�18. [PMC free article] [PubMed]
37. Chugh R, Kalra S, Sharma N, et al. Effects of muscle energy techniques and its comparison to self stretch of bilateral ankle plantarflexors on performance of balance scores in healthy elderly subjects. Physiother Occup Ther J. 2011;4:61�71.
38. Fryer G, Ruszkowski W. The influence of contraction duration in muscle energy technique applied to the atlanto-axial joint. J Osteopath Med. 2004;7:79�84.
39. Fryer G, Pearce AJ. The effect of muscle energy technique on corticospinal and spinal reflex excitability in asymptomatic participants. J Bodyw Mov Ther. 2013;17(4):440�47. [PubMed]
40. Gugliotti M. The use of mobilization, muscle energy technique, and soft tissue mobilization following a modified radical neck dissection of a patient with head and neck cancer. Rehabil Oncol. 2011;29:3�8.
41. K???k?en S, Yilmaz H, Sall? A, U?urlu H. Muscle energy technique versus corticosteroid injection for management of chronic lateral epicondylitis: Randomized controlled trial with 1-year follow-up. Arch Phys Med Rehabil. 2013;94:2068�74. [PubMed]
42. Moore SD, Laudner KG, McLoda TA, et al. The immediate effects of muscle energy technique on posterior shoulder tightness: a randomized controlled trial. J Orthop Sports Phys Ther. 2011;41:400�7. [PubMed]
43. Rajadurai V. The effect of muscle energy technique on temporomandibular joint dysfunction: a randomized clinical trail. Asian J Sci Res. 2011;4:71�77.
44. Shadmehr A, Hadian MR, Naiemi SS, et al. Hamstring flexibility in young women following passive stretch and muscle energy technique. J Back Musculoskelet Rehabil. 2009;22:143�48. [PubMed]
45. Day JM, McKeon P, Nitz A. The efficacy of cervical/thoracic active range of motion for detecting changes associated with individuals receiving muscle energy techniques. Phys Ther Rev. 2010;15:453�61.
46. Day JM, Nitz AJ. The effect of muscle energy techniques on disability and pain scores in individuals with low back pain. J Sport Rehabil. 2012;21:194�98. [PubMed]
47. Zaproudina N, Hietikko T, Hanninen OO, et al. Effectiveness of traditional bone setting in treating chronic low back pain: a randomised pilot trial. Complement Ther Med. 2009;17:23�28. [PubMed][/accordion]
[/accordions]
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Scalenes
Box 4.9 Notes on Scalenes
The scalenes are a controversial muscle since they seem to be both postural and phasic (Lin et al 1994), their status being modified by the type(s) of stress to which they are exposed (see Ch. 3 for discussion of this topic).
Janda (1988) reports that �spasm and/or trigger points are commonly present in the scalenes as also are weakness and/or inhibition�.
The attachment sites of the scalene muscles vary, as does their presence. The scalene posterior is sometimes absent, and sometimes blends with the fibres of medius.
Scalene medius is noted to frequently attach to the atlas (Gray 1995) and sometimes extend to the 2nd rib (Simons et al 1998).
The scalene minimus (pleuralis), which attaches to the pleural dome, is present in onethird (Platzer 1992) to three-quarters (Simons et al 1998) of people, on at least one side and, when absent, is replaced by a transverse cupular ligament (Platzer 1992).
The brachial plexus exits the cervical column between the scalenus anterior and medius. These two muscles, together with the 1st rib, form the scalene hiatus (also called the �scalene opening� or �posterior scalene aperture�) (Platzer 1992). It is through this opening�that the brachial plexus and vascular structures for the upper extremity pass. When scalene fibres are taut, they may entrap the nerves (scalene anticus syndrome) or may elevate the 1st rib against the clavicle and indirectly crowd the vascular, or neurologic, structures (simultaneous compromising of both neural and vascular structures is rare) (Stedman 1998). Any of these conditions may be diagnosed as �thoracic outlet syndrome�, which is �a collective title for a number of conditions attributed to compromise of blood vessels or nerve fibers (brachial plexus) at any point between the base of the neck and the axilla� (Stedman 1998).
Assessment of Shortness in Scalenes (14)
Assessment of cervical sidebending (lateral flexion) strength. This involves the scalenes and levator scapulae (and to a secondary degree the rectus capitis lateralis and the transversospinalis group).
The practitioner places a stabilising hand on the top of the shoulder to prevent movement and the other on the head above the ear, as the seated patient attempts to flex the head laterally against this resistance. Both sides are assessed.
Observation assessment (a) There is no easy test for shortness of the scalenes apart from observation, palpation and assessment of trigger point activity/tautness and a functional observation as follows:
In most people who have marked scalene shortness there is a tendency to overuse these (and other upper fixators of the shoulder and neck) as accessory breathing muscles.
There may also be a tendency to hyperventilation (and hence for there to possibly be a history of anxiety, phobic behaviour, panic attacks and/or fatigue symptoms).
These muscles seem to be excessively tense in many people with chronic fatigue symptoms.
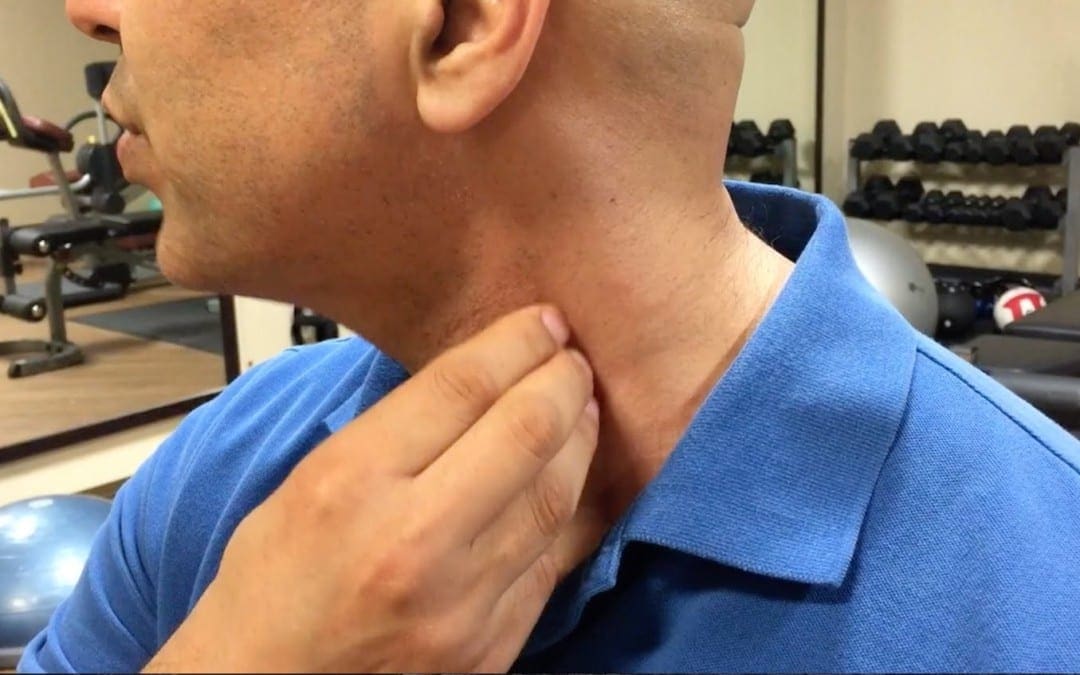
The observation assessment consists of the practitioner placing his relaxed hands over the patient�s shoulders so that the fingertips rest on the clav-icles, at which time the seated patient is asked to inhale deeply. If the practitioner�s hands noticeably rise towards the patient�s ears during inhalation then there exists inappropriate use of scalenes, which indicates that they are stressed, which also means that, by definition, they will have become shortened and require stretching treatment.
Observation assessment (b) (Fig. 4.33) Alternatively, during the history taking interview, the patient can be asked to place one hand on the abdomen just above the umbilicus and the other flat against the upper chest.
Figure 4.33 Observation assessment of respiratory function. Any tendency for the upper hand to move cephalad, or earlier than the caudad hand, suggests scalene overactivity.
On inhalation, the hands are observed: if the upper hand initiates the breathing process and rises significantly towards the chin, rather than moving forwards, a pattern of upper chest breathing can be assumed, and therefore stress, and therefore shortness of the scalenes (and other accessory breathing muscles, notably sternomastoid).
MET Treatment of Short Scalenes (Fig. 4.34A, B, C)
Patient lies supine with a cushion or folded towel under the upper thoracic area so that, unless supported by the practitioner�s contralateral hand, the head would fall into extension. The head is rotated contralaterally (away from the side to be treated). There are three positions of rotation required:
Full contralateral rotation of the head/neck produces involvement of the more posterior fibres of the scalenes
A contralateral 45� rotation of the head/neck involves the middle fibres
A position of only slight contralateral rotation involves the more anterior fibres.
The practitioner�s free hand is placed on the side of the patient�s head to restrain the isometric contraction which will be used to release the scalenes. The patient�s head is in one of the above degrees of rotation, supported by the practitioner�s contralateral hand.
Figure 4.34A MET for scalenus posticus. On stretching, following the isometric contraction, the neck is allowed to move into slight extension while a mild stretch is introduced by the contact hand which rests on the second rib, below the lateral aspect of the clavicle.
Figure 4.34B MET treatment for the middle fibres of scalenes. The hand placement (thenar or hypothenar eminence of relaxed hand) is on the 2nd rib below the centre of the clavicle.
Figure 4.34C MET treatment of the anterior fibres of the scalenes; hand placement is on the sternum
The patient is instructed to try to lift the forehead a fraction and to attempt to turn the head towards the affected side, with appropriate breathing cooperation, while resistance is applied by the practitioner�s hand to prevent both movements (�breathe in and hold your breath as you �lift and turn�, and hold this for 7�10 seconds�). Both the effort and, the counter-pressure should be modest and painless at all times.
After a 7�10 second contraction, the head is placed into extension and one hand remains on it to prevent movement during the scalene stretch.
The patient�s contralateral hand is placed (palm down) just inferior to the lateral end of the clavicle on the affected side (for full rotation of the head, posterior scalenes). The practitioner�s hand which was acting to produce resistance to the isometric contraction is now placed onto the dorsum of the patient�s �cushion� hand.
As the patient slowly exhales, the practitioner�s contact hand, resting on the patient�s hand, which is itself resting on the 2nd rib and upper thorax, pushes obliquely away and towards the foot on that same side, following the rib movement into its exhalation position, so stretching the attached musculature and fascia. This stretch is held for at least 20 seconds after each isometric contraction. The process is then repeated at least once more.
The head is rotated 45� contralaterally and the �cushion� hand contact, which applies the stretch of the middle scalenes, is placed just inferior to the middle aspect of the clavicle. When the head is in the almost upright facing position for the anterior scalene stretch, the �cushion� hand contact is on the upper sternum itself.
In all other ways the methodology is as described for the first position above.
NOTE: It is important not to allow heroic degrees of neck extension during any phase of this treatment. There should be some extension, but it should be appropriate to the age and condition of the individual.
A degree of eye movement can assist scalene treatment and may be used as an alternative to the �lift and turn� muscular effort described above. If the patient makes the eyes look caudally (towards the feet) and towards the affected side during the isometric contraction, she will increase the degree of contraction in the muscles. If during the resting phase, when stretch is being introduced, she looks away from the treated side, with eyes looking towards the top of the head, this will enhance the stretch of the muscle.
This whole procedure should be performed bilaterally several times in each of the three head positions. Scalene stretches, with all their variable positions, clearly also influence many of the anterior neck structures.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Acknowledging statistical data, low back pain can be the result of a variety of injuries and/or conditions affecting the lumbar spine and its surrounding structures. Most cases of low back pain, however, will resolve on their own in a matter of weeks. But when symptoms of low back pain become chronic, its essential for the affected individual to seek treatment from the most appropriate healthcare professional. The McKenzie method has been used by many healthcare specialists in the treatment of low back pain and its effects have been recorded widely throughout various research studies. The following two articles are being presented to evaluate the McKenzie method in the treatment of LBP in comparison to other types of treatment options.
Efficacy of the McKenzie Method in Patients With Chronic Nonspecific Low Back Pain: A Protocol of Randomized Placebo-Controlled Trial
Presented Abstract
Background: The McKenzie method is widely used as an active intervention in the treatment of patients with nonspecific low back pain. Although the McKenzie method has been compared with several other interventions, it is not yet known whether this method is superior to placebo in patients with chronic low back pain.
Objective: The purpose of this trial is to assess the efficacy of the McKenzie method in patients with chronic nonspecific low back pain.
Design: An assessor-blinded, 2-arm, randomized placebo-controlled trial will be conducted.
Setting: This study will be conducted in physical therapy clinics in S�o Paulo, Brazil.
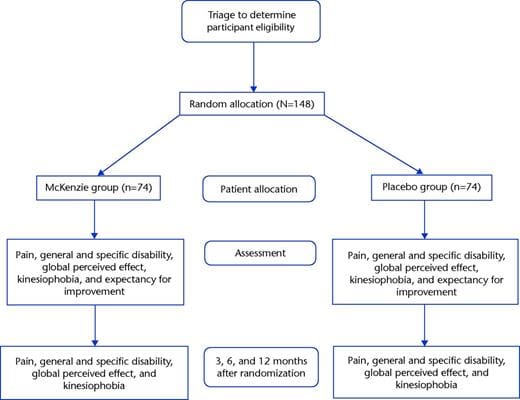
Participants: The participants will be 148 patients seeking care for chronic nonspecific low back pain.
Intervention: Participants will be randomly allocated to 1 of 2 treatment groups: (1) McKenzie method or (2) placebo therapy (detuned ultrasound and shortwave therapy). Each group will receive 10 sessions of 30 minutes each (2 sessions per week over 5 weeks).
Measurements: The clinical outcomes will be obtained at the completion of treatment (5 weeks) and at 3, 6, and 12 months after randomization. The primary outcomes will be pain intensity (measured with the Pain Numerical Rating Scale) and disability (measured with the Roland-Morris Disability Questionnaire) at the completion of treatment. The secondary outcomes will be pain intensity; disability and function; kinesiophobia and global perceived effect at 3, 6, and 12 months after randomization; and kinesiophobia and global perceived effect at completion of treatment. The data will be collected by a blinded assessor.
Limitations: Therapists will not be blinded.
Conclusions: This will be the first trial to compare the McKenzie method with placebo therapy in patients with chronic nonspecific low back pain. The results of this study will contribute to better management of this population.
Subject:Therapeutic Exercise, Injuries and Conditions: Low Back, Protocols
Issue Section:Protocol
Low back pain is a major health condition associated with a high rate of absenteeism from work and a more frequent use of health services and work leave entitlements.[1] Low back pain recently was rated by the Global Burden of Disease Study as one of the 7 health conditions that most affect the world’s population,[2] and it is considered a debilitating health condition that affects the population for the greatest number of years over a lifetime.[2] The point prevalence of low back pain in the general population is reported to be up to 18%, increasing to 31% in the last 30 days, 38% in the last 12 months, and 39% at any point in life.[3] Low back pain also is associated with high treatment costs.[4] It is estimated that in European countries, the direct and indirect costs vary from �2 to �4 billion a year.[4] The prognosis of low back pain is directly related to the duration of the symptoms.[5,6] Patients with chronic low back pain have a less favorable prognosis compared with patients with acute low back pain[5,7] and are responsible for most of the costs for management of back pain, generating the need for research aimed at finding better treatments for these patients.
There is a great variety of interventions for the treatment of patients with chronic low back pain, including the McKenzie method developed by Robin McKenzie in New Zealand in 1981.[8] The McKenzie method (also known as Mechanical Diagnosis and Therapy [MDT]) is an active therapy that involves repeated movements or sustained positions and has an educational component with the purpose of minimizing pain and disability and improving spinal mobility.[8] The McKenzie method involves the assessment of symptomatic and mechanical responses to repeated movements and sustained positions. Patients’ responses to this assessment are used to classify them into subgroups or syndromes called derangement, dysfunction, and posture.[8�10] Classification according to one of these groups guides the treatment principles.
Derangement syndrome is the largest group and characterized by patients who demonstrate centralization (transition of pain from distal to proximal) or disappearance of pain[11] with repeated movement testing in one direction. These patients are treated with repeated movements or sustained positions that could reduce pain. Patients classified as having dysfunction syndrome are characterized by pain that occurs only at the end of the range of motion of only one movement.[8] The pain does not change or centralize with repeated movement testing. The treatment principle for patients with dysfunction is repeated movements in the direction that generated the pain. Finally, patients classified as having postural syndrome experience intermittent pain only during sustained positioning at the end of the range of motion (eg, sustained slumped sitting).[8] The treatment principle for this syndrome consists of posture correction.[11]
The McKenzie method also includes a strong educational component based on the books titled The Lumbar Spine: Mechanical Diagnosis & Therapy: Volume Two[11] and Treat Your Own Back.[12] This method, unlike other therapeutic methods, aims to make the patients as independent of the therapist as possible and thus capable of controlling their pain through postural care and the practice of specific exercises for their problem.[11] It encourages patients to move the spine in the direction that is not harmful to their problem, thus avoiding movement restriction due to kinesiophobia or pain.[11]
Two previous systematic reviews have analyzed the effects of the McKenzie method[9,10] in patients with acute, subacute, and chronic low back pain. The review by Clare et al[9] demonstrated that the McKenzie method showed better results in short-term pain relief and improvement of disability compared with active interventions such as physical exercise. The review by Machado et al[10] showed that the McKenzie method reduced pain and disability in the short term when compared with passive therapy for acute low back pain. For chronic low back pain, the 2 reviews were unable to draw conclusions about the effectiveness of the McKenzie method due to the lack of appropriate trials. The randomized controlled trials that have investigated the McKenzie method in patients with chronic low back pain[13�17] compared the method with other interventions such as resistance training,[17] the Williams method,[14] unsupervised exercises,[16] trunk strengthening,[15] and stabilization exercises.[13] Better results in reducing pain intensity were obtained with the McKenzie method compared with resistance training,[17] the Williams method,[14] and supervised exercise.[16] However, the methodological quality of these trials[13�17] is suboptimal.
It is known from the literature that the McKenzie method yields beneficial results when compared with some clinical interventions in patients with chronic low back pain; however, to date, no studies have compared the McKenzie method against a placebo treatment in order to identify its actual efficacy. Clare et al[9] highlighted the need to compare the McKenzie method with placebo therapy and to study the effects of the method in the long term. In other words, it is not known whether the positive effects of the McKenzie method are due to its real efficacy or simply to a placebo effect.
The objective of this study will be to assess the efficacy of the McKenzie method in patients with chronic nonspecific low back pain using a high-quality randomized placebo-controlled trial.
Method
Study Design
This will be an assessor-blinded, 2-arm, randomized placebo-controlled trial.
Study Setting
This study will be conducted in physical therapy clinics in S�o Paulo, Brazil.
Eligibility Criteria
The study will include patients seeking care for chronic nonspecific low back pain (defined as pain or discomfort between the costal margins and the inferior gluteal folds, with or without referred symptoms in the lower limbs, for at least 3 months[18]), with a pain intensity of at least 3 points as measured with the 0- to 10-point Pain Numerical Rating Scale, aged between 18 and 80 years, and able to read Portuguese. Patients will be excluded if they have any contraindication to physical exercise[19] or ultrasound or shortwave therapy, evidence of nerve root compromise (ie, one or more motor, reflex, or sensation deficits), serious spinal pathology (eg, fracture, tumor, inflammatory and infectious diseases), serious cardiovascular and metabolic diseases, previous back surgery, or pregnancy.
Procedure
First, the patients will be interviewed by the study’s blinded assessor, who will determine eligibility. Eligible patients will be informed about the objectives of the study and asked to sign a consent form. Next, the patient’s sociodemographic data and medical history will be recorded. The assessor will then collect the data related to the study outcomes at the baseline assessment, after completion of 5 weeks of treatment, and 3, 6, and 12 months after randomization. With the exception of baseline measurements, all other assessments will be collected over the telephone. All data entry will be coded, entered into an Excel (Microsoft Corporation, Redmond, Washington) spreadsheet, and double-checked prior to the analysis.
Outcome Measures
The clinical outcomes will be measured at the baseline assessment, after treatment, and 3, 6, and 12 months after random allocation. The primary outcomes will be pain intensity (measured with the Pain Numerical Rating Scale)[20] and disability (measured with the Roland-Morris Disability Questionnaire)[21,22] after completion of 5 weeks of treatment. The secondary outcomes will be pain intensity and disability 3, 6, and 12 months after randomization and disability and function (measured by the Patient-Specific Functional Scale),[20] kinesiophobia (measured with the Tampa Scale of Kinesiophobia),[23] and global perceived effect (measured with the Global Perceived Effect Scale)[20] after treatment and 3, 6, and 12 months after randomization. On the day of the baseline assessment, each patient’s expectancy for improvement also will be assessed using the Expectancy of Improvement Numerical Scale,[24] followed by assessment using the McKenzie method.[8] Patients may experience an exacerbation of symptoms after the baseline assessment due to the MDT physical examination. All measurements were previously cross-culturally adapted into Portuguese and clinimetrically tested and are described below.
Pain Numerical Rating Scale
The Pain Numerical Rating Scale is a scale that assesses the levels of pain intensity perceived by the patient using an 11-point scale (varying from 0 to 10), in which 0 represents �no pain� and 10 represents the �worst possible pain.�[20] The participants will be instructed to select the average of pain intensity based on the last 7 days.
Roland-Morris Disability Questionnaire
This questionnaire consists of 24 items that describe daily activities that patients have difficulty performing due to low back pain.[21,22] The higher the number of affirmative answers, the higher the level of disability associated with low back pain.[21,22] The participants will be instructed to complete the questionnaire based on the last 24 hours.
Patient-Specific Functional Scale
The Patient-Specific Functional Scale is a global scale; therefore, it can be used for any part of the body.[25,26] The patients will be asked to identify up to 3 activities that they feel unable to perform or that they have difficulty performing due to their low back pain.[25,26] Measurement will be taken using Likert-type, 11-point scales for each activity, with higher average scores (ranging from 0 to 10 points) representing better ability to perform the tasks.[25,26] We will calculate the average of these activities based on the last 24 hours, with a final score ranging from 0 to 10.
Global Perceived Effect Scale
The Global Perceived Effect Scale is a Likert-type, 11-point scale (ranging from ?5 to +5) that compares the patient’s current condition with his or her condition at the onset of symptoms.[20] Positive scores apply to patients who are better and negative scores apply to patients who are worse in relation to the onset of symptoms.[20]
Tampa Scale of Kinesiophobia
This scale assesses the level of kinesiophobia (fear of moving) by means of 17 questions that deal with pain and intensity of symptoms.[23] The scores from each item vary from 1 to 4 points (eg, 1 point for �strongly disagree,� 2 points for �partially disagree,� 3 points for �agree,� and 4 points for �strongly agree�).[23] For the total score, it is necessary to invert the scores of questions 4, 8, 12, and 16.[23] The final score can vary from 17 to 68 points, with higher scores representing a higher degree of kinesiophobia.[23]
Expectancy of Improvement Numerical Scale
This scale assesses the patient’s expectancy for improvement after treatment in relationship to a specific treatment.[24] It consists of an 11-point scale varying from 0 to 10, in which 0 represents �no expectancy for improvement� and 10 represents �expectancy for the greatest possible improvement.�[24] This scale will be administered only on the first day of assessment (baseline) before the randomization. The reason for including this scale is to analyze whether the expectation of improvement will influence the outcomes.
Random Allocation
Before the treatment begins, the patients will be randomly allocated to their respective intervention groups. The random allocation sequence will be implemented by one of the researchers not involved with recruiting and assessing the patients and will be generated on Microsoft Excel 2010 software. This random allocation sequence will be inserted into sequentially numbered, opaque, sealed envelopes (to ensure that allocation is concealed from the assessor). The envelopes will be opened by the physical therapist who will treat the patients.
Blinding
Given the nature of the study, it is not possible to blind the therapists to the conditions of treatment; however, the assessor and the patients will be blinded to the treatment groups. At the end of the study, the assessor will be asked whether the patients were allocated to the real treatment group or to the placebo group in order to measure assessor blinding. A visual representation of the study design is presented in the Figure.
Figure 1: Flow Diagram of the Study.
Interventions
The participants will be allocated to groups receiving 1 of 2 interventions: (1) placebo therapy or (2) MDT. Participants in each group will receive 10 sessions of 30 minutes each (2 sessions per week over 5 weeks). The studies on the McKenzie method do not have a standard number of sessions given that some studies propose low doses of treatment,[16,17,27] and others recommend higher doses.[13,15]
For ethical reasons, on the first day of treatment, patients from both groups will receive an information booklet called The Back Book,[28] based on the same recommendations as the existing guidelines.[29,30] This booklet will be translated into Portuguese so that it can be completely understood by the study’s participants, who will receive additional explanations regarding the content of the booklet, if needed. Patients will be asked in each session if they have felt any different symptom. The chief investigator of the study will periodically audit the interventions.
Placebo Group
The patients allocated to the placebo group will be treated with detuned pulsed ultrasound for 5 minutes and detuned shortwave diathermy in pulsed mode for 25 minutes. The devices will be used with the internal cables disconnected to obtain the placebo effect; however, it will be possible to handle them and adjust doses and alarms as if they were connected to simulate the pragmatism of clinical practice as well as to increase credibility of use of these devices on the patients. This technique has been used successfully in previous trials with patients with low back pain.[31�35]
McKenzie Group
The patients of the McKenzie group will be treated according to the principles of the McKenzie method,[8] and the choice of therapeutic intervention will be guided by the physical examination findings and classification. Patients also will receive written instructions from the Treat Your Own Back[12] book and will be asked to perform home exercises based on the principles of McKenzie method.[11] The descriptions of the exercises that will be prescribed in this study are published elsewhere.[27] Adherence to home exercises will be monitored by means of a daily log that the patient will fill in at home and bring to the therapist at each subsequent session.
Statistical Methods
Sample Size Calculation
The study was designed to detect a difference of 1 point in pain intensity measured with the Pain Numerical Rating Scale[20 ](estimate for standard deviation=1.84 points)[31] and a difference of 4 points in disability associated with low back pain measured with the Roland-Morris Disability Questionnaire[21,22] (estimate for standard deviation=4.9 points).[31] The following specifications were considered: statistical power of 80%, alpha level of 5%, and follow-up loss of 15%. Therefore, the study will require a sample of 74 patients per group (148 in total).
Analysis of the Effects of Treatment
The statistical analysis of our study will follow intention-to-treat principles.[36] The normality of the data will be tested by visual inspection of histograms, and the characterization of the participants will be calculated using descriptive statistical tests. The between-group differences (effects of treatment) and their respective 95% confidence intervals will be calculated by constructing mixed linear models[37] using interaction terms of treatment groups versus time. We will conduct a secondary exploratory analysis to assess whether patients classified as having derangement syndrome have a better response to the McKenzie method (compared with placebo) than those with other classifications. For this assessment, we will use a 3-way interaction for group, time, and classification. For all of these analyses, we will use the IBM SPSS software package, version 19 (IBM Corp, Armonk, New York).
Ethics
This study was approved by the Research Ethics Committee of the Universidade Cidade de S�o Paulo (#480.754) and prospectively registered at ClinicalTrials.gov (NCT02123394). Any protocol modifications will be reported to the Research Ethics Committee as well as to the trial registry.
Dr. Alex Jimenez’s Insight
Low back pain is one of the most common reasons people seek immediate medical attention for every year. Although many healthcare professionals are qualified and experienced in the diagnosis of the source of the patient’s low back pain, finding the right healthcare specialist who can provide the proper treatment for the individual’s LBP can be the real challenge. A variety of treatments can be used to treat low back pain, however, a wide array of healthcare professionals have started utilizing the McKenzie method in the treatment of patients with nonspecific low back pain. The purpose of the following article is to evaluate the effectiveness of the McKenzie method for low back pain, carefully analyzing the data of the research study.
Discussion
Potential Impact and Significance of the Study
The existing randomized controlled trials investigating the McKenzie method in patients with chronic low back pain have all used an alternative intervention as the comparison group.[14�17] To date, no study has compared the McKenzie method with a placebo treatment in patients with low back pain in order to identify its real efficacy, which is an important gap in the literature.[9] Interpretation of the previous comparative effectiveness studies is limited by the lack of knowledge of the efficacy of the McKenzie method for people with chronic low back pain. This study will be the first to compare McKenzie method with placebo therapy in patients with chronic nonspecific low back pain. A proper comparison against a placebo group will provide more unbiased estimates of the effects of this intervention. This type of comparison has already been done in trials aiming to assess the efficacy of motor control exercises for patients with chronic low back pain,[31] spinal manipulative therapy and diclofenac for patients with acute low back pain,[38] and exercise and advice for patients with subacute low back pain.[39]
Contribution to the Physical Therapy Profession and for Patients
The McKenzie method is one of the few methods used in physical therapy that advocates for the independence of patients.[8,12] This method also provides patients with tools to promote their autonomy in managing the current pain and even future recurrences.[12] We expect that patients treated with the McKenzie method will benefit more than the patients treated with the placebo treatment. If this hypothesis is confirmed in our study, the results will contribute to better clinical decision making of physical therapists. Moreover, the approach has the potential to reduce the burden associated with the recurrent nature of low back pain if patients can better self-manage future episodes.
Strengths and Weaknesses of the Study
This trial contemplates a substantial number of patients to minimize bias, and it was prospectively registered. We will use true randomization, concealed allocation, blinded assessment, and an intention-to-treat analysis. The treatments will be conducted by 2 therapists who were extensively trained to perform the interventions. We will monitor the home exercise program. Unfortunately, due to the interventions, we will not be able to blind the therapists to the treatment allocation. It is known from the literature that the McKenzie method yields beneficial results when compared with some clinical interventions in patients with chronic low back pain.[14�17] To date, however, no studies have compared the McKenzie method with a placebo treatment in order to identify its actual efficacy.
Future Research
The intention of this study group is to submit the results of this study to a top-level, international peer-reviewed journal. These published results may provide a basis for future trials that investigate the effectiveness of the McKenzie method when delivered at different doses (different numbers of sets, repetitions, and sessions), which is still unclear in the literature. Our secondary exploratory analysis aims to assess whether patients classified as having derangement syndrome have a better response to the McKenzie method (compared with placebo treatment) than those with other classifications. This assessment will contribute to a better understanding of possible subgroups of patients with chronic low back pain who respond best to specific interventions. This is an important issue, as exploring subgroups is currently considered the most important research priority in the field of low back pain.[40]
This study was fully funded by S�o Paulo Research Foundation (FAPESP) (grant number 2013/20075-5). Ms Garcia is funded by a scholarship from the Coordination for the Improvement of Higher Education Personnel/Brazilian Government (CAPES/Brazil).
The study was prospectively registered at ClinicalTrials.gov (trial registration: NCT02123394).
Predicting a Clinically Important Outcome in Patients with Low Back Pain Following McKenzie Therapy or Spinal Manipulation: A Stratified Analysis in a Randomized Controlled Trial
Presented Abstract
Background: Reports vary considerably concerning characteristics of patients who will respond to mobilizing exercises or manipulation. The objective of this prospective cohort study was to identify characteristics of patients with a changeable lumbar condition, i.e. presenting with centralization or peripheralization, that were likely to benefit the most from either the McKenzie method or spinal manipulation.
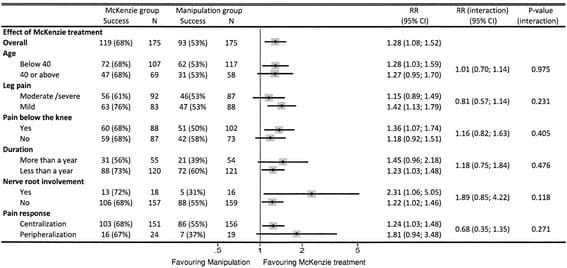
Methods: 350 patients with chronic low back pain were randomized to either the McKenzie method or manipulation. The possible effect modifiers were age, severity of leg pain, pain-distribution, nerve root involvement, duration of symptoms, and centralization of symptoms. The primary outcome was the number of patients reporting success at two months follow-up. The values of the dichotomized predictors were tested according to the prespecified analysis plan.
Results: No predictors were found to produce a statistically significant interaction effect. The McKenzie method was superior to manipulation across all subgroups, thus the probability of success was consistently in favor of this treatment independent of predictor observed. When the two strongest predictors, nerve root involvement and peripheralization, were combined, the chance of success was relative risk 10.5 (95% CI 0.71-155.43) for the McKenzie method and 1.23 (95% CI 1.03-1.46) for manipulation (P?=?0.11 for interaction effect).
Conclusions: We did not find any baseline variables which were statistically significant effect modifiers in predicting different response to either McKenzie treatment or spinal manipulation when compared to each other. However, we did identify nerve root involvement and peripheralization to produce differences in response to McKenzie treatment compared to manipulation that appear to be clinically important. These findings need testing in larger studies.
Electronic supplementary material: The online version of this article (doi:10.1186/s12891-015-0526-1) contains supplementary material, which is available to authorized users.
Keywords:Low back pain, McKenzie, Spinal manipulation, Predictive value, Effect modification
Background
The most recent published guidelines for the treatment of patients with persistent non-specific low back pain (NSLBP) recommend a program focusing on self-management after initial advice and information. These patients should also be offered structured exercises tailored to the individual patient and other modalities such as spinal manipulation [1,2].
Previous studies have compared the effect of the McKenzie-method, also known as Mechanical Diagnosis and Therapy (MDT), with that of spinal manipulation (SM) in heterogeneous populations of patients with acute and subacute NSLBP and found no difference in outcome [3,4].
Recently, the need for studies testing the effect of treatment strategies for subgroups of patients with NSLBP in primary care has been emphasized in consensus-papers [5,6] as well as the current European guidelines [7], based on the hypothesis that subgroup analyses, preferably complying with the recommendations of �Prognostic Factor Research�[8], will improve decision making towards the most effective management strategies. Although initial data show promising results, there is presently insufficient evidence to recommend specific methods of subgrouping in primary care [1,9].
Three randomized studies, comprising patients with predominantly acute or subacute low back pain (LBP), have tested the effects of MDT versus SM in a subgroup of patients that presented with centralization of symptoms or directional preference (favorable response to end range motions) during physical examination [10-12]. The conclusions drawn from these studies were not in concurrence and the usefulness was limited by a low methodological quality.
Our recent randomized study, comprising patients with predominantly chronic LBP (CLBP), found a marginally better overall effect of MDT versus SM in an equivalent group [13]. In order to pursue the idea of subgrouping further, it was part of the study plan to explore predictors based on patient characteristics that could assist the clinician in targeting the most favorable treatment to the individual patient.
The objective of this study was to identify subgroups of patients with predominantly CLBP, presenting with centralization or peripheralization, which were likely to benefit from either MDT or SM two months after the completion of treatment.
Methods
Data Collection
The present study is a secondary analysis of a previously published randomized controlled trial [13]. We recruited 350 patients from September 2003 through May 2007 at an outpatient back care centre in Copenhagen, Denmark.
Patients
Patients were referred from primary care physicians for treatment of persistent LBP. Eligible patients were between 18 and 60 years of age, suffering from LBP with or without leg pain for a period of more than 6 weeks, able to speak and understand the Danish language, and fulfilled the clinical criteria for centralization or peripheralization of symptoms during initial screening. Centralization was defined as the abolition of symptoms in the most distal body region (such as the foot, lower leg, upper leg, buttocks, or lateral low back) and peripheralization was defined as the production of symptoms in a more distal body region. These findings have previously been found to have acceptable degree of inter-tester reliability (Kappa value 0.64) [14]. The initial screening was performed prior to randomization by a physical therapist with a diploma in the MDT examination system. Patients were excluded if they were free of symptoms at the day of inclusion, demonstrated positive non-organic signs [15], or if serious pathology, i.e. severe nerve root involvement (disabling back or leg pain in combination with progressive disturbances in sensibility, muscle strength, or reflexes), osteoporosis, severe spondylolisthesis, fracture, inflammatory arthritis, cancer, or referred pain from the viscera, was suspected based on physical examination and/or magnetic resonance imaging. Other exclusion criteria were application for disability pension, pending litigation, pregnancy, co-morbidity, recent back surgery, language problems, or problems with communication including abuse of drugs or alcohol.
The trial population had predominantly CLBP lasting on average 95 weeks (SD 207), mean age was 37 years (SD10), mean level of back and leg pain was 30 (SD 11.9) on a Numeric Rating Scale ranging from 0 to 60, and mean level of disability was 13 (SD 4.8) on Roland Morris Disability Questionnaire (0-23). Our method of pain measurement reflects that back pain is often a fluctuating condition where pain location and severity might vary on a daily basis. Therefore, a validated comprehensive pain questionnaire [16] was used in order to guarantee that all aspects of back and leg pain intensity were recorded. The scales are outlined in the legend to Table 1.
After baseline measures were obtained, randomisation was carried out by a computer-generated list of random numbers in blocks of ten using sealed opaque envelopes.
Ethics
Ethical approval of the study was granted by Copenhagen Research Ethics Committee, file no 01-057/03. All patients received written information about the study and gave their written consent prior to participation.
Treatments
The practitioners performing the treatments had no knowledge of the results of the initial screening. The treatment programs were designed to reflect daily practice as much as possible. Detailed information on these programs have been published earlier [13].
The MDT treatment was planned individually following the therapist�s pre-treatment physical assessment. Specific manual vertebral mobilization techniques including high velocity thrust were not allowed. An educational booklet describing self care [17] or a �lumbar roll� for correction of the seated position was sometimes provided to the patient at the discretion of the therapist. In the SM treatment, high velocity thrust was used in combination with other types of manual techniques. The choice of combination of techniques was at the discretion of the chiropractor. General mobilizing exercises, i.e. self-manipulation, alternating lumbar flexion/extension movements, and stretching, were allowed but not specific exercises in the directional preference. An inclined wedged pillow for correction of the seated position was available to the patients if the chiropractor believed this to be indicated.
In both treatment groups, patients were informed thoroughly of the results of the physical assessment, the benign course of back pain, and the importance of remaining physically active. Guidance on proper back care was also given. In addition, all patients were provided with a Danish version of �The Back Book� which previously has been shown to have beneficial effect on patients� beliefs about back pain [18]. A maximum of 15 treatments for a period of 12 weeks were given. If considered necessary by the treating clinician, patients were educated in an individual program of self-administered mobilizing, stretching, stabilizing, and/or strengthening exercises at the end of the treatment period. Treatments were performed by clinicians with several years of experience. Patients were instructed to continue their individual exercises at home or at a gym for a minimum of two months after completion of the treatment at the back center. Because the patients suffered predominantly from CLBP we expected this period of self administered exercises to be necessary for the patients to experience the full effect of the intervention. Patients were encouraged not to seek any other kind of treatment during this two months period of self-administered exercises.
Outcome Measures
The primary outcome was the proportion of patients reporting success at follow-up two months after end of treatment. Treatment success was defined as a reduction of at least 5 points or a final score below 5 points on the 23-item modified Roland Morris Disability Questionnaire (RMDQ) [19]. A validated Danish version of RMDQ was used [20]. The definition of treatment success was based on the recommendations by others [21,22]. A sensitivity analysis using 30% relative improvement on RMDQ as definition of success was also performed. In accordance with the protocol [13], we considered a relative between-group difference of 15% in the number of patients with successful outcome to be minimal clinically important in our analysis of interaction.
Prespecified Predictor Variables
In order to reduce the likelihood of spurious findings [23], we restricted the number of candidate effect modifiers in the dataset to six. To increase the validity of our findings, a directional hypothesis was established for each variable according to the recommendations of Sun et al. [24] Four baseline variables have previously been suggested in randomized studies to be predictive of long term good outcome in patients with persistent LBP following MDT in comparison with strengthening training: centralization [25,26], or following SM in comparison to physiotherapy or treatment chosen by a general practitioner: age below 40 years [27,28], duration of symptoms more than 1 year [27], and pain below the knee [29]. As recommended by others [30], another two variables were added based on the participating experienced clinicians� judgments of which characteristics they would expect to predict good outcome from their treatment compared to the other. The additional variables prioritized by the physiotherapists in the MDT group were signs of nerve root involvement and substantial leg pain. The additional variables prioritized by the chiropractors in the SM group were no signs of nerve root involvement and not substantial leg pain.
In a supplementary analysis, we took the opportunity to explore whether the inclusion of further six baseline variables, assumed to have prognostic value for good outcome in either of the treatment groups, would appear to have an effect modifying effect as well. To our knowledge, no further variables from previous one arm studies have been reported to have prognostic value of long term good outcome in patients with persistent LBP following MDT, whereas three variables have been reported to have prognostic value following SM: male gender [28], mild disability [28], and mild back pain [28]. Another three variables were agreed upon by the clinicians to be included in the supplementary analysis as they were assumed by experience from clinical practice to have prognostic value for good outcome regardless of treatment with MDT or SM: low number of days on sick leave past year, high patient expectations to recovery, and high patient expectations about coping with work tasks six weeks after initiation of treatment.
Dichotomization of possible predictor variables were made to allow for comparisons to be made with those of earlier studies. In cases where no cut off values could be found in the literature, dichotomization was performed above/below the median found in the sample. Definitions of variables are presented in the legend to Table 1.
Statistics
The entire intention-to-treat (ITT) population was used in all the analyses. The last score was carried forward for subjects with missing two months RMDQ scores (7 patients in the MDT group and 14 patients in the SM group). In addition, a post hoc per protocol analysis was carried out comprising only those 259 patients that completed the full treatment. The analysis plan was agreed in advance by the trial management group.
The possible predictors were dichotomized and the chance of success was investigated by estimating the relative risk (RR) of success in each of the two strata. The impact of the investigated predictors was estimated by comparing the chance of success between the treatment groups when divided into the two strata. To test for treatment effect modification of the predictors we performed chi-squared tests for interaction between intervention and the two different strata for each of the predictors. This is basically the same as an interaction from a regression model. Confidence intervals were also inspected for potential clinically important effects.
Following the univariate analysis, a multivariate analysis was planned including effect modifiers with a p-value below 0.1.
Dr. Alex Jimenez’s Insight
Low back pain can occur due to several types of injuries and/or conditions and its symptoms may be acute and/or chronic. Patients with low back pain can benefit from a variety of treatments, including chiropractic care. Chiropractic treatment is one of the most common alternative treatment options utilized to treat low back pain. According to the article, the results of the improvement of LBP with spinal adjustments and manual manipulations, along with the use of exercise, vary considerably among the participants. The focus of the following research study is to determine which patients are most likely to benefit from the McKenzie method as compared to spinal adjustments and manual manipulations.
Results
Participants were similar with respect to socio-demographic and clinical characteristics at baseline in the treatment groups. An overview of the distribution of the included dichotomized variables at baseline is provided in Table 1. No differences were found between the treatment groups.
Overall, the post hoc per protocol analysis did not produce outcome results that were different from the results of the ITT analysis and therefore only the results of the ITT analysis will be reported.
Figure 1 presents the distribution of predictors with regards to effect modification in the MDT group versus SM. In all subgroups, the probability of success with MDT was superior to that of SM. Because of low sample size, confidence intervals were wide and none of the predictors had a statistically significant treatment modifying effect. The predictors with a clinically important potential effect in favor of MDT compared to SM were nerve root involvement (28% higher proportion of patients with success when nerve root involvement was present than when absent) and peripheralization of symptoms (17% higher proportion of patients with success in case of peripheralization than in case of centralization). If present, nerve root involvement increased the chance of success following MDT 2.31 times compared to that of SM and 1.22 times if not present. This means that for the subgroup of patients with nerve root involvement receiving MDT, compared to those receiving SM, the relative effect appeared to be 1.89 times (2.31/1.22, P?= 0.118) higher than for the subgroup with no nerve root involvement.
Figure 1: Treatment effect modified by predictors. The top point estimate and confidence intervals indicate overall effect without subgrouping. Subsequent pairs of point estimates and confidence intervals show the chances of treatment success.
Figure 2 presents the modifying effect of a composite of the two predictors with a clinically important potential effect. If signs of nerve root involvement and peripheralization were present at baseline, the chance of success with MDT compared to SM appeared 8.5 times higher than for the subgroup with no centralization and nerve root involvement. The number of patients was very small and the differences were not statistically significant (P?=?0.11).
Figure 2: Impact of the two clinically important predictors combined on treatment effect. RR?=?Relative Risk with Yates correction.
None of the prognostic candidate variables explored in the supplementary analysis appeared to have any clinically important modifying effect (Additional file 1: Table S1).
The results from the sensitivity analysis using 30% relative improvement on RMDQ as definition of success were not markedly different from those presented above (Additional file 2: Table S2).
Discussion
To our knowledge, this is the first study trying to identify effect modifiers when two mobilizing strategies, i.e. MDT and SM, are compared in a sample of patients with as changeable condition characterized by centralization or peripheralization.
Our study found that none of the potential effect modifiers were able to statistically significantly increase the overall effect of MDT compared to that of SM. However, the between-group difference for two of the variables exceeded our clinically important success-rate of 15% in number of patients with successful outcome, so our study is likely to have missed a true effect and, in that sense, did not have a large enough sample size.
The most apparent finding is that in our small subgroup of patients with signs of nerve root involvement, the relative chance of success appeared 1.89 times (2.31/1.22) higher than in patients with no nerve root involvement when treated with MDT, compared to those treated with SM. The difference was in the expected direction.
Although not statistically significant in our small sample, the variable peripheralization exceeded our clinically important success-rate of 15%, but was found not to be in the expected direction. No previous studies have assessed the effect modification of centralization or peripheralization in patients with CLBP. The RCT by Long et al. [25,26] concluded that patients with directional preference, including centralization, fared better 2 weeks after baseline than patients with no directional preference when treated with MDT in comparison with strengthening training. However, the outcome among peripheralizers was not reported, so the poor outcome reported in patients with no directional preference might be related to the subgroup of patients who responded with no change in symptoms during initial examination and not to those that responded with peripheralization. An alternative explanation might be that the effect modifying impact of centralization or peripheralization on MDT is dependent on the control treatment. Our findings suggest that future studies in this area need to involve predictive value of peripheralization as well as centralization.
When a composite of the two most promising predictors, peripheralization and signs of nerve root involvement, were present at baseline, the relative chance of success with MDT compared to SM appeared 8.5 times higher than for the subgroup with no centralization and nerve root involvement. The number of patients was very small and the confidence interval was wide. Therefore only a preliminary conclusion about interaction can be drawn and it calls for a validation in future studies.
In our study, there appeared to be no characteristic by which SM had better results compared to MDT. Thus, we could not support the results of two studies with a similar design as ours (two arms, sample of patients with persistent LBP, and outcome reported in terms of reduction of disability at long term follow up) [27,29]. In those studies, Nyiendo et al. [29] found a modifying effect of leg pain below knee on treatment by SM compared to that of the general practitioner six months after baseline, and Koes et al. [27] found a modifying effect of age below 40 years and symptom duration more than a year on treatment by SM compared to that of physiotherapy 12 months after baseline. However, results from those, as well as other previous RCTs comprising patients with persistent LBP, have supported our findings regarding the lack of effect modification of age [27,29,31], sex [29,31], baseline disability [27,29,31], and duration of symptoms [31], on SM when measured on reduction of disability 6-12 months after randomization. So, although evidence is emerging in patients with acute LBP regarding subgroup characteristics predictive of better results from SM compared to other types of treatment [32], we are still in the dark with respect to patients with persistent LBP.
The usefulness of choosing a criterion for success by combining an improvement of at least 5 points or an absolute score below 5 points on RMDQ is debatable. A total of 22 patients were considered successful based on score below 5 at follow up without having an improvement of at least 5 points. We therefore performed a sensitivity analysis using a relative improvement of at least 30% as criterion of success as recommended by others [22] (see Additional file 2: Table S2). As a result, the percentage of patients with successful outcome in the MDT group remained the same whereas 4 more patients were defined as successes in the SM group. Overall the sensitivity analysis did not produce outcome results that were markedly different from those of the primary analysis and therefore only those have been discussed above.
Strengths and Limitations
This study used data from a RCT, whereas many others have used single arm designs not suitable for the purpose of evaluating treatment effect modification [33]. In accordance with the recommendations by the PROGRESS group [8] we prespecified the possible predictors and also the direction of the effect. Furthermore, we limited the number of predictors included in order to minimize the chance of spurious findings.
The main limitation in secondary studies to previously conducted RCTs is that they are powered to detect overall treatment effect rather that effect modification. In recognition of the post hoc nature of our analysis, reflected in wide confidence intervals, we must emphasize that our findings are exploratory and require formal testing in a larger sample size.
Conclusions
In all subgroups, the probability of success with MDT was superior to that of SM. Although not statistically significant, the presence of nerve root involvement and peripheralization appear promising effect modifiers in favour of MDT. These findings need testing in larger studies.
Acknowledgements
The authors thank Jan Nordsteen and Steen Olsen for clinical expert advice, and Mark Laslett for comments and language correction.
This study was in part supported by grants from The Danish Rheumatism Association, The Danish Physiotherapy Organization, The Danish Foundation for Chiropractic Research and Continuous Education, and The Danish Institute for Mechanical Diagnosis and Therapy. RC/The Parker Institute acknowledge the funding support from the Oak Foundation. The funds were independent of the management, analyses, and interpretation of the study.
Footnotes
Competing interests: The authors declare that they have no competing interests.
Authors� contributions: All authors were involved in the data analysis and the writing process, and the requirements for authorship have been met. All analyses were conducted by TP, RC, and CJ. TP conceived and led the study and was responsible for writing the first draft of the paper, but the other authors have participated throughout the writing process and have read and approved the final version.
In conclusion,�the above two articles were presented in order to evaluate the McKenzie method in the treatment of LBP in comparison to other types of treatment options. The first research study compared the McKenzie method with placebo therapy in patients with low back pain, however, the results of the study still need additional evaluations. In the second research study, no significant results could predict a different response in the use of the McKenzie method. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
[accordions title=”References”]
[accordion title=”References” load=”hide”]1
Waddell
G
. The Back Pain Revolution
. 2nd ed
. New York, NY
: Churchill Livingstone
; 2004
.
2
Murray
CJ
, Lopez
AD
. Measuring the global burden of disease
. N Engl J Med
. 2013
;369
:448
�457
.
Google Scholar
CrossRef
PubMed
3
Hoy
D
, Bain
C
, Williams
G
, et al.
. A systematic review of the global prevalence of low back pain
. Arthritis Rheum
. 2012
;64
:2028
�2037
.
Google Scholar
CrossRef
PubMed
4
van Tulder
MW
. Chapter 1: European guidelines
. Eur Spine J
. 2006
;15
:134
�135
.
Google Scholar
CrossRef
5
Costa Lda
C
, Maher
CG
, McAuley
JH
, et al.
. Prognosis for patients with chronic low back pain: inception cohort study
. BMJ
. 2009
;339
:b3829
.
Google Scholar
CrossRef
PubMed
6
da C Menezes Costa
, Maher
CG
, Hancock
MJ
, et al.
. The prognosis of acute and persistent low-back pain: a meta-analysis
. CMAJ
. 2012
;184
:E613
�E624
.
Google Scholar
CrossRef
PubMed
7
Henschke
N
, Maher
CG
, Refshauge
KM
, et al.
. Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study
. BMJ
. 2008
;337
:154
�157
.
Google Scholar
CrossRef
8
McKenzie
R
, May
S
. The Lumbar Spine: Mechanical Diagnosis & Therapy: Volume One
. 2nd ed
. Waikanae, New Zealand
: Spinal Publications
; 2003
.
9
Clare
HA
, Adams
R
, Maher
CG
. A systematic review of efficacy of McKenzie therapy for spinal pain
. Aust J Physiother
. 2004
;50
:209
�216
.
Google Scholar
CrossRef
PubMed
10
Machado
LA
, de Souza
MS
, Ferreira
PH
, Ferreira
ML
. The McKenzie method for low back pain: a systematic review of the literature with a meta-analysis approach
. Spine (Phila Pa 1976)
. 2006
;31
:254
�262
.
Google Scholar
CrossRef
PubMed
11
McKenzie
R
, May
S
. The Lumbar Spine: Mechanical Diagnosis & Therapy: Volume Two
. 2nd ed
. Waikanae, New Zealand
: Spinal Publications
; 2003
.
12
McKenzie
R
. Trate Noc� Mesmo a sua Coluna [Treat Your Own Back]
. Crichton, New Zealand
: Spinal Publications New Zealand Ltd
; 1998
.
13
Miller
ER
, Schenk
RJ
, Karnes
JL
, Rousselle
JG
. A comparison of the McKenzie approach to a specific spine stabilization program for chronic low back pain
. J Man Manip Ther
. 2005
;13
:103
�112
.
Google Scholar
CrossRef
14
Nwuga
G
, Nwuga
V
. Relative therapeutic efficacy of the Williams and McKenzie protocols in back pain management
. Physiother Theory Pract
. 1985
;1
:99
�105
.
Google Scholar
CrossRef
15
Petersen
T
, Larsen
K
, Jacobsen
S
. One-year follow-up comparison of the effectiveness of McKenzie treatment and strengthening training for patients with chronic low back pain: outcome and prognostic factors
. Spine (Phila Pa 1976)
. 2007
;32
:2948
�2956
.
Google Scholar
CrossRef
PubMed
16
Sakai
Y
, Matsuyama
Y
, Nakamura
H
, et al.
. The effect of muscle relaxant on the paraspinal muscle blood flow: a randomized controlled trial in patients with chronic low back pain
. Spine (Phila Pa 1976)
. 2008
;33
:581
�587
.
Google Scholar
CrossRef
PubMed
17
Udermann
BE
, Mayer
JM
, Donelson
RG
, et al.
. Combining lumbar extension training with McKenzie therapy: effects on pain, disability, and psychosocial functioning in chronic low back pain patients
. Gunders Lutheran Medical Journal
. 2004
;3
:7
�12
.
18
Airaksinen
O
, Brox
JI
, Cedraschi
C
, et al.
. Chapter 4: European guidelines for the management of chronic nonspecific low back pain
. Eur Spine J
. 2006
;15
:192
�300
.
Google Scholar
CrossRef
19
Kenney
LW
, Humphrey
RH
, Mahler
DA
. ACSM’s Guidelines for Exercise Testing and Prescription
. Baltimore, MD
: Williams & Wilkins
; 1995
.
20
Costa
LO
, Maher
CG
, Latimer
J
, et al.
. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: which one is the best?
Spine (Phila Pa 1976)
. 2008
;33
:2459
�2463
.
Google Scholar
CrossRef
PubMed
21
Costa
LO
, Maher
CG
, Latimer
J
, et al.
. Psychometric characteristics of the Brazilian-Portuguese versions of the Functional Rating Index and the Roland-Morris Disability Questionnaire
. Spine (Phila Pa 1976)
. 2007
;32
:1902
�1907
.
Google Scholar
CrossRef
PubMed
22
Nusbaum
L
, Natour
J
, Ferraz
MB
, Goldenberg
J
. Translation, adaptation and validation of the Roland-Morris questionnaire: Brazil Roland-Morris
. Braz J Med Biol Res
. 2001
;34
:203
�210
.
Google Scholar
CrossRef
PubMed
23
de Souza
FS
, Marinho Cda
S
, Siqueira
FB
, et al.
. Psychometric testing confirms that the Brazilian-Portuguese adaptations, the original versions of the Fear-Avoidance Beliefs Questionnaire, and the Tampa Scale of Kinesiophobia have similar measurement properties
. Spine (Phila Pa 1976)
. 2008
;33
:1028
�1033
.
Google Scholar
CrossRef
PubMed
24
Devilly
GJ
, Borkovec
TD
. Psychometric properties of the credibility/expectancy questionnaire
. J Behav Ther Exp Psychiatry
. 2000
;31
:73
�86
.
Google Scholar
CrossRef
PubMed
25
Chatman
AB
, Hyams
SP
, Neel
JM
, et al.
. The Patient-Specific Functional Scale: measurement properties in patients with knee dysfunction
. Phys Ther
. 1997
;77
:820
�829
.
Google Scholar
PubMed
26
Pengel
LH
, Refshauge
KM
, Maher
CG
. Responsiveness of pain, disability, and physical impairment outcomes in patients with low back pain
. Spine (Phila Pa 1976)
. 2004
;29
:879
�883
.
Google Scholar
CrossRef
PubMed
27
Garcia
AN
, Costa
LCM
, da Silva
TM
, et al.
. Effectiveness of Back School versus McKenzie exercises in patients with chronic nonspecific low back pain: a randomized controlled trial
. Phys Ther
. 2013
;93
:729
�747
.
Google Scholar
CrossRef
PubMed
28
Manchester
MR
, Glasgow
GW
, York
JKM
, et al.
. The Back Book: Clinical Guidelines for the Management of Acute Low Back Pain
. London, United Kingdom
: Stationery Office Books
; 2002
:1
�28
.
29
Delitto
A
, George
SZ
, Van Dillen
LR
, et al.
. Low back pain
. J Orthop Sports Phys Ther
. 2012
;42
:A1
�A57
.
Google Scholar
CrossRef
PubMed
30
van Tulder
M
, Becker
A
, Bekkering
T
, et al.
. Chapter 3: European guidelines for the management of acute nonspecific low back pain in primary care
. Eur Spine J
. 2006
;15
:169
�191
.
Google Scholar
CrossRef
31
Costa
LO
, Maher
CG
, Latimer
J
, et al.
. Motor control exercise for chronic low back pain: a randomized placebo-controlled trial
. Phys Ther
. 2009
;89
:1275
�1286
.
Google Scholar
CrossRef
PubMed
32
Balthazard
P
, de Goumoens
P
, Rivier
G
, et al.
. Manual therapy followed by specific active exercises versus a placebo followed by specific active exercises on the improvement of functional disability in patients with chronic non specific low back pain: a randomized controlled trial
. BMC Musculoskelet Disord
. 2012
;13
:162
.
Google Scholar
CrossRef
PubMed
33
Kumar
SP
. Efficacy of segmental stabilization exercise for lumbar segmental instability in patients with mechanical low back pain: a randomized placebo controlled crossover study
. N Am J Med Sci
. 2012
;3
:456
�461
.
34
Ebadi
S
, Ansari
NN
, Naghdi
S
, et al.
. The effect of continuous ultrasound on chronic non-specific low back pain: a single blind placebo-controlled randomized trial
. BMC Musculoskelet Disord
. 2012
;13
:192
.
Google Scholar
CrossRef
PubMed
35
Williams
CM
, Latimer
J
, Maher
CG
, et al.
. PACE�the first placebo controlled trial of paracetamol for acute low back pain: design of a randomised controlled trial
. BMC Musculoskelet Disord
. 2010
;11
:169
.
Google Scholar
CrossRef
PubMed
36
Hollis
S
, Campbell
F
. What is meant by intention to treat analysis? Survey of published randomised controlled trials
. BMJ
. 1999
;319
:670
�674
.
Google Scholar
CrossRef
PubMed
37
Twisk
JWR
. Applied Longitudinal Data Analysis for Epidemiology: A Practical Guide
. New York, NY
: Cambridge University Press
; 2003
.
38
Hancock
MJ
, Maher
CG
, Latimer
J
, et al.
. Assessment of diclofenac or spinal manipulative therapy, or both, in addition to recommended first-line treatment for acute low back pain: a randomised controlled trial
. Lancet
. 2007
;370
:1638
�1643
.
Google Scholar
CrossRef
PubMed
39
Pengel
LH
, Refshauge
KM
, Maher
CG
, et al.
. Physiotherapist-directed exercise, advice, or both for subacute low back pain: a randomized trial
. Ann Intern Med
. 2007
;146
:787
�796
.
Google Scholar
CrossRef
PubMed
40
Costa Lda
C
, Koes
BW
, Pransky
G
, et al.
. Primary care research priorities in low back pain: an update
. Spine (Phila Pa 1976)
. 2013
;38
:148
�156
.
Google Scholar
CrossRef
PubMed[/accordion]
[accordion title=”References” load=”hide”]1. Chou R, Qaseem A, Snow V, Casey D, Cross JT, Jr, Shekelle P, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(7):478�91. doi: 10.7326/0003-4819-147-7-200710020-00006. [PubMed] [Cross Ref]
2. NHS Early management of persistent non-specific low back pain. NICE Clinical Guideline. 2009;88:1�30.
3. Cherkin DC, Battie MC, Deyo RA, Street JH, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med. 1998;339(15):1021�9. doi: 10.1056/NEJM199810083391502. [PubMed] [Cross Ref]
4. Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alen M, Videman T. Orthopaedic manual therapy, McKenzie method or advice only for low back pain in working adults. A randomized controlled trial with 1 year follow-up. J Rehabil Med. 2008;40(10):858�63. doi: 10.2340/16501977-0262. [PubMed] [Cross Ref]
5. Foster NE, Dziedzic KS, van Der Windt DA, Fritz JM, Hay EM. Research priorities for non-pharmacological therapies for common musculoskeletal problems: nationally and internationally agreed recommendations. BMC Musculoskelet Disord. 2009;10:3. doi: 10.1186/1471-2474-10-3. [PMC free article] [PubMed] [Cross Ref]
6. Kamper SJ, Maher CG, Hancock MJ, Koes BW, Croft PR, Hay E. Treatment-based subgroups of low back pain: a guide to appraisal of research studies and a summary of current evidence. Best Pract Res Clin Rheumatol. 2010;24(2):181�91. doi: 10.1016/j.berh.2009.11.003. [PubMed] [Cross Ref]
7. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(Suppl 2):S192�300. doi: 10.1007/s00586-006-1072-1. [PMC free article] [PubMed] [Cross Ref]
8. Hingorani AD, Windt DA, Riley RD, Abrams K, Moons KG, Steyerberg EW, et al. Prognosis research strategy (PROGRESS) 4: Stratified medicine research. BMJ. 2013;346:e5793. doi: 10.1136/bmj.e5793. [PMC free article] [PubMed] [Cross Ref]
9. Fersum KV, Dankaerts W, O�Sullivan PB, Maes J, Skouen JS, Bjordal JM, et al. Integration of sub-classification strategies in RCTs evaluating manual therapy treatment and exercise therapy for non-specific chronic low back pain (NSCLBP): a systematic review. Br J Sports Med. 2010;44(14):1054�62. doi: 10.1136/bjsm.2009.063289. [PubMed] [Cross Ref]
10. Erhard RE, Delitto A, Cibulka MT. Relative effectiveness of an extension program and a combined program of manipulation and flexion and extension exercises in patients with acute low back syndrome. Phys Ther. 1994;74(12):1093�100. [PubMed]
11. Schenk RJ, Josefczyk C, Kopf A. A randomized trial comparing interventions in patients with lumbar posterior derangement. J Man Manipul Ther. 2003;11(2):95�102. doi: 10.1179/106698103790826455. [Cross Ref]
12. Kilpikoski S, Alen M, Paatelma M, Simonen R, Heinonen A, Videman T. Outcome comparison among working adults with centralizing low back pain: Secondary analysis of a randomized controlled trial with 1-year follow-up. Adv Physiol Educ. 2009;11:210�7. doi: 10.3109/14038190902963087. [Cross Ref]
13. Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The McKenzie method compared with manipulation when used adjunctive to information and advice in low back pain patients presenting with centralization or peripheralization. A randomized controlled trial. Spine (Phila Pa 1976) 2011;36(24):1999�2010. doi: 10.1097/BRS.0b013e318201ee8e. [PubMed] [Cross Ref]
14. Petersen T, Olsen S, Laslett M, Thorsen H, Manniche C, Ekdahl C, et al. Inter-tester reliability of a new diagnostic classification system for patients with non-specific low back pain. Aust J Physiother. 2004;50:85�94. doi: 10.1016/S0004-9514(14)60100-8. [PubMed] [Cross Ref]
15. Waddell G, McCulloch JA, Kummel E, Venner RM. Nonorganic physical signs in low-back pain. Spine. 1980;5(2):117�25. doi: 10.1097/00007632-198003000-00005. [PubMed] [Cross Ref]
16. Manniche C, Asmussen K, Lauritsen B, Vinterberg H, Kreiner S, Jordan A. Low Back Pain Rating scale: validation of a tool for assessment of low back pain. Pain. 1994;57(3):317�26. doi: 10.1016/0304-3959(94)90007-8. [PubMed] [Cross Ref]
17. McKenzie RA. Treat your own back. Waikanae: Spinal Publications New Zealand Ltd; 1997.
18. Burton AK, Waddell G, Tillotson KM, Summerton N. Information and advice to patients with back pain can have a positive effect. A randomized controlled trial of a novel educational booklet in primary care. Spine. 1999;24(23):2484�91. doi: 10.1097/00007632-199912010-00010. [PubMed] [Cross Ref]
19. Patrick DL, Deyo RA, Atlas SJ, Singer DE, Chapin A, Keller RB. Assessing health-related quality of life in patients with sciatica. Spine. 1995;20(17):1899�908. doi: 10.1097/00007632-199509000-00011. [PubMed] [Cross Ref]
20. Albert H, Jensen AM, Dahl D, Rasmussen MN. Criteria validation of the Roland Morris questionnaire. A Danish translation of the international scale for the assessment of functional level in patients with low back pain and sciatica [Kriterievalidering af Roland Morris Sp�rgeskemaet – Et oversat internationalt skema til vurdering af �ndringer i funktionsniveau hos patienter med l�ndesmerter og ischias] Ugeskr Laeger. 2003;165(18):1875�80. [PubMed]
21. Bombardier C, Hayden J, Beaton DE. Minimal clinically important difference. Low back pain: outcome measures. J Rheumatol. 2001;28(2):431�8. [PubMed]
22. Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, Von KM, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90�4. doi: 10.1097/BRS.0b013e31815e3a10. [PubMed] [Cross Ref]
23. Moons KG, Royston P, Vergouwe Y, Grobbee DE, Altman DG. Prognosis and prognostic research: what, why, and how? BMJ. 2009;338:1317�20. doi: 10.1136/bmj.b1317. [PubMed] [Cross Ref]
24. Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect believable? Updating criteria to evaluate the credibility of subgroup analyses. BMJ. 2010;340:c117. doi: 10.1136/bmj.c117. [PubMed] [Cross Ref]
25. Long A, Donelson R, Fung T. Does it matter which exercise? A randomized control trial of exercise for low back pain. Spine. 2004;29(23):2593�602. doi: 10.1097/01.brs.0000146464.23007.2a. [PubMed] [Cross Ref]
26. Long A, May S, Fung T. The comparative prognostic value of directional preference and centralization: a useful tool for front-line clinicians? J Man Manip Ther. 2008;16(4):248�54. doi: 10.1179/106698108790818332. [PMC free article] [PubMed] [Cross Ref]
27. Koes BW, Bouter LM, van Mameren H, Essers AH, Verstegen GJ, Hofhuizen DM, et al. A randomized clinical trial of manual therapy and physiotherapy for persistent back and neck complaints: subgroup analysis and relationship between outcome measures. J Manipulative Physiol Ther. 1993;16(4):211�9. [PubMed]
28. Leboeuf-Yde C, Gronstvedt A, Borge JA, Lothe J, Magnesen E, Nilsson O, et al. The nordic back pain subpopulation program: demographic and clinical predictors for outcome in patients receiving chiropractic treatment for persistent low�back pain. J Manipulative Physiol Ther. 2004;27(8):493�502. doi: 10.1016/j.jmpt.2004.08.001. [PubMed] [Cross Ref]
29. Nyiendo J, Haas M, Goldberg B, Sexton G. Pain, disability, and satisfaction outcomes and predictors of outcomes: a practice-based study of chronic low back pain patients attending primary care and chiropractic physicians. J Manipulative Physiol Ther. 2001;24(7):433�9. doi: 10.1016/S0161-4754(01)77689-0. [PubMed] [Cross Ref]
30. Foster NE, Hill JC, Hay EM. Subgrouping patients with low back pain in primary care: are we getting any better at it? Man Ther. 2011;16(1):3�8. doi: 10.1016/j.math.2010.05.013. [PubMed] [Cross Ref]
31. Underwood MR, Morton V, Farrin A. Do baseline characteristics predict response to treatment for low back pain? Secondary analysis of the UK BEAM dataset. Rheumatology (Oxford) 2007;46(8):1297�302. doi: 10.1093/rheumatology/kem113. [PubMed] [Cross Ref]
32. Slater SL, Ford JJ, Richards MC, Taylor NF, Surkitt LD, Hahne AJ. The effectiveness of sub-group specific manual therapy for low back pain: a systematic review. Man Ther. 2012;17(3):201�12. doi: 10.1016/j.math.2012.01.006. [PubMed] [Cross Ref]
33. Stanton TR, Hancock MJ, Maher CG, Koes BW. Critical appraisal of clinical prediction rules that aim to optimize treatment selection for musculoskeletal conditions. Phys Ther. 2010;90(6):843�54. doi: 10.2522/ptj.20090233. [PubMed] [Cross Ref][/accordion]
[/accordions]
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Low back pain, or LBP, is a very common condition which affects the lumbar spine, or the lower section of the spine. Approximately more than 3 million cases of LBP are diagnosed in the United States aline every year and about 80 percent of adults worldwide experience low back pain at some point during their lifetime. Low back pain is generally caused by injury to a muscle (strain) or ligament (sprain) or due to damage from a disease. Common causes of LBP include poor posture, lack of regular exercise,�improper lifting, fracture, herniated discs and/or arthritis. Most cases of low back pain may often go away on their own, however, when LBP becomes chronic, it may be important to seek immediate medical attention. Two therapeutic methods have been utilized to improve LBP. The following article compares the effects of Pilates and McKenzie training on LBP.
A Comparison of the Effects of Pilates and McKenzie Training on Pain and General Health in Men with Chronic Low Back Pain: A Randomized Trial
Abstract
Background: Today, chronic low back pain is one of the special challenges in healthcare. There is no unique approach to treat chronic low back pain. A variety of methods are used for the treatment of low back pain, but the effects of these methods have not yet been investigated adequately.
Aim: The aim of this study was to compare the effects of Pilates and McKenzie training on pain and general health of men with chronic low back pain.
Materials and Methods: Thirty-six patients with chronic low back pain were chosen voluntarily and assigned to three groups of 12 each: McKenzie group, Pilates group, and control group. The Pilates group participated in 1-h exercise sessions, three sessions a week for 6 weeks. McKenzie group performed workouts 1 h a day for 20 days. The control group underwent no treatment. The general health of all participants was measured by the General Health Questionnaire 28 and pain by the McGill Pain Questionnaire.
Results: After therapeutic exercises, there was no significant difference between Pilates and McKenzie groups in pain relief (P = 0.327). Neither of the two methods was superior over the other for pain relief. However, there was a significant difference in general health indexes between Pilates and McKenzie groups.
Conclusion: Pilates and McKenzie training reduced pain in patients with chronic low back pain, but the Pilates training was more effective to improve general health.
Keywords:Chronic back pain, general health, Mckenzie training, pain, Pilates training
Introduction
Low back pain with a history of more than 3 months and without any pathological symptom is called chronic low back pain. For patient with chronic low back pain, the physician should take into consideration the likelihood of muscle pain development with spinal origin, in addition to low back pain with unknown origin. This type of pain may be mechanical (increase in pain with movement or physical pressure) or nonmechanical (increase in pain at the rest time).[1] Low back pain or spine pain is the most common musculoskeletal complication.[2] About 50%�80% of healthy people may experience low back pain during their lifetime, and about 80% of the problems are related to the spine and occur in the lumbar area.[3] Low back pain may be caused by trauma, infection, tumors, etc.[4] Mechanical injuries which are caused by overuse of a natural structure, deformity of an anatomical structure, or the injury in the soft tissue are the most common reasons for back pain. From occupational health perspective, back pain is among the most important reasons for the absence from work and occupational disability;[5] in fact, the longer the period of disease,[6] the less likely it is to improve and return to work.[1] Disability due to low back pain in addition to disturbance in doing daily and social activities has a very negative effect, from social and economic perspectives, on the patient and the community, which makes chronic low back pain highly important.[3] Today, chronic low back pain is one of the critical challenges in medicine. Patients with chronic low back pain are responsible for 80% of the costs paid for the treatment of low back pain that is also the reason for mobility restrictions in most people under 45 years.[7] In the developed countries, the overall cost paid for low back pain per year is 7.1 of total share of the gross national product. Clearly, most of the cost is related to counseling and treatment of patients with chronic low back pain rather than with intermittent and recursive low back pain.[8] The existence of various methods of treatment is because of no single cause of low back pain.[9] A variety of methods such as pharmacotherapy, acupuncture, infusions, and physical methods are the most common interventions for treatment of low back pain. However, the effects of these methods remain to be fully known.[6] An exercise program, developed based on the physical conditions of patients, can promote the quality of life in patients with chronic disease.[10,11,12,13,14]
Literature shows that the effect of exercise in controlling chronic low back pain is under study and there is strong evidence about the fact that movement therapy is effective to treat low back pain.[15] However, no specific recommendations exist about the type of exercise, and the effects of certain types of movement therapies have been determined in few studies.[9] Pilates training consists of the exercises that focus on improving flexibility and strength in all the body organs, without increasing the mass of muscles or destroying them. This training method consists of controlled movements that form a physical harmony between the body and brain, and can raise the ability of the body of people at any age.[16] In addition, people who do Pilates exercise would have better sleep and less fatigue, stress, and nervousness. This training method is based on standing, sitting, and lying positions, without intervals, jumping, and leaping; thus, it may reduce injuries resulting from the joint damage because the exercise movements in the ranges of motion in the above three positions are performed with deep breathing and muscle contraction.[17] McKenzie method, also called mechanical diagnosis and therapy and based on the patient’s active participation, is used and trusted by patients and the people who use this method worldwide. This method is based on physical therapy which has been frequently studied. The distinctive characteristic of this method is the principle of initial assessment.[18] This principle is a reliable and safe method to make a diagnosis that makes the correct treatment planning possible. In this way, the time and energy are not spent for costly tests, rather McKenzie therapists, using a valid indicator, quickly recognize that how much and how this method is fruitful for the patient. More appropriately, McKenzie method is a comprehensive approach based on the correct principles whose full understanding and following is very fruitful.[19] In the recent years, non-pharmacological approaches have attracted the attention of physicians and patients with low back pain.[20] Complementary therapies[21] and treatments with holistic nature (to increase physical and mental well-being) are appropriate to manage physical illness.[13] Complementary therapies can slow down disease progression and improve capacity and physical performance. The aim of the present study is to compare the effect of the Pilates and McKenzie training on pain and general health in men with chronic low back pain.
Materials and Methods
This randomized clinical trial was conducted in Shahrekord, Iran. The total study population screened was 144. We decided to enroll at least 25% of the population, 36 individuals, using a systematic random sampling. First, the participants were numbered and a list was developed. The first case was selected using random number table and then one out of four patients was randomly enrolled. This process continued till a desired number of participants were enrolled. Then, the participants were randomly assigned to experimental (Pilates and McKenzie training) groups and control group. After explaining the research purposes to the participants, they were asked to complete the consent form for participation in the study. Furthermore, the patients were ensured that the research data are kept confidential and used only for research purposes.
Inclusion Criteria
The study population included men aged 40�55 years in Shahrekord, South-West Iran, with chronic back pain, that is, history of more than 3 months of low back pain and no specific disease or other surgery.
Exclusion Criteria
The exclusion criteria were low back arch or so-called army back, serious spinal pathology such as tumors, fractures, inflammatory diseases, previous spinal surgery, nerve root compromise in the lumbar region, spondylolysis or spondylolisthesis, spinal stenosis, neurological disorders, systemic diseases, cardiovascular diseases, and receiving other therapies simultaneously. The examiner who assessed the outcomes was blinded to group assignment. Twenty-four hours before the training, a pretest was administered to all three groups to determine pain and general health; and then, the training began after completion of the McGill Pain Questionnaire (MPQ) and the General Health Questionnaire-28 (GHQ-28). The MPQ can be used to evaluate a person experiencing significant pain. It can be used to monitor the pain over time and to determine the effectiveness of any intervention. Minimum pain score: 0 (would not be seen in a person with true pain), maximum pain score: 78, and the higher the pain score the more severe the pain. Investigators reported that the construct validity and the reliability of the MPQ were reported as a test-retest reliability of 0.70.[22] The GHQ is a self-administered screening questionnaire. Test-retest reliability has been reported to be high (0.78�0 0.9) and inter- and intra-rater reliability have both been shown to be excellent (Cronbach’s ? 0.9�0.95). High internal consistency has also been reported. The lower the score is, the better the general health is.[23]
The participants in the experimental groups started training program under supervision of a sports medicine specialist. The training program consisted of 18 sessions of supervised individual training for both groups, with the sessions held three times per week for 6 weeks. Each training session lasted for an hour and was performed at the Physiotherapy Clinic in the School of Rehabilitation of the Shahrekord University of Medical Sciences in 2014�2015. The first experimental group performed Pilates training for 6 weeks, three times a week about an hour per session. In each session, first, a 5-min warm-up and preparation procedures were run; and at the end, stretching and walking were done to return to the baseline condition. In the McKenzie group, six exercises were used: Four extension-type exercises and two flexion-types. The extension-type exercises were performed in prone and standing positions, and the flexion-type exercises in the supine and sitting positions. Each exercise was run ten times. In addition, the participants conducted twenty daily individual training sessions for an hour.[18] After training of both groups, the participants filled out the questionnaires and then the collected data were presented in both descriptive and inferential statistics. Furthermore, the control group without any training, at the end of a period when other groups have completed, filled the questionnaire. Descriptive statistics were used for central tendency indicators such as mean (� standard deviation) and relevant diagrams were used to describe the data. Inferential statistics, one-way ANOVA and post hoc Tukey’s test, were used to analyze the data. Data analysis was done by SPSS Statistics for Windows, Version 21.0 (IBM Corp. Released 2012. IBM Armonk, NY: IBM Corp). P < 0.05 was considered statistically significant.
Dr. Alex Jimenez’s Insight
Alongside the use of spinal adjustments and manual manipulations for low back pain, chiropractic care commonly utilizes therapeutic exercise methods to improve LBP symptoms, restoring the affected individual’s strength, flexibility and mobility as well as promoting a faster recovery. The Pilates and McKenzie method of training, as mentioned in the article, are compared to determine which therapeutic exercise is best for treating low back pain. As�a Level I Certified Pilates Instructor, Pilates training is implemented with chiropractic treatment to improve LBP more effectively. Patients participating in a therapeutic exercise method alongside a primary form of treatment for low back pain can experience additional benefits. McKenzie training can also be implemented with chiropractic treatment to further improve LBP symptoms. The purpose of this research study is to demonstrate evidence-based information on the benefits of Pilates and McKenzie methods for low back pain as well as to educate patients on which of the two therapeutic exercises should be considered to help treat their symptoms and achieve overall health and wellness.
Level I Certified Pilates Instructors at Our Location
Dr. Alex Jimenez D.C., C.C.S.T | Chief Clinical Director and Level I Certified Pilates Instructor
Truide Torres | Director of Patient Relations Advocate Dept. and Level I Certified Pilates Instructor
Results
The results showed no significant difference between the case and control groups regarding the gender, marital status, job, educational level, and income. The results showed changes in pain index and general health in the participants before and after Pilates and McKenzie training in the two experimental and even control groups [Table 1].
A significant difference was seen in pain and general health between the control and the two experimental groups at the pre- and post-test, so that the exercise training (both Pilates and McKenzie) resulted in reduced pain and promoted general health; while in the control group, pain increased and general health declined.
Discussion
The results of this study indicate that back pain reduced and general health enhanced after exercise therapy with both Pilates and McKenzie training, but in the control group, pain was intensified. Petersen et al. study on 360 patients with chronic low back pain concluded that at the end of 8 weeks of McKenzie training and high-intensity endurance training and 2 months training at home, pain and disability decreased in McKenzie group at the end of 2 months, but at the end of 8 months, no differences were seen among the treatments.[24]
The results of another study show that McKenzie training is a beneficial method for reducing pain and increasing the movements of the spine in patients with chronic low back pain.[18] Pilates training can be an effective method for improving general health, athletic performance, proprioception, and reduction of pain in patients with chronic low back pain.[25] The improvements in strength seen in the participants in the present study were more likely to be due to decrease in pain inhibition than to neurological changes in muscle firing/recruitment patterns or to morphological (hypertrophic) changes in the muscle. In addition, neither of the treatments was superior over the other in view of reducing the intensity of pain. In the present study, 6 weeks of McKenzie training led to significant reduction in pain levels in men with chronic low back pain. The rehabilitation of patients with chronic low back pain is aimed to restore strength, endurance, and flexibility of soft tissues.
Udermann et al. showed that McKenzie training improved pain, disability, and psychosocial variables in patients with chronic low back pain, and back stretching training did not have any additional effect on pain, disability, and psychosocial variables.[26] The results of another study show that there is a reduction in pain and disability due to McKenzie method for at least 1 week in comparison with the passive treatment in patients with low back pain, but reduction in pain and disability due to McKenzie method in comparison with the active treatment methods is desirable within 12 weeks after treatment. Overall, McKenzie treatment is more effective than passive methods to treat low back pain.[27] One of the popular exercise therapies for patients with low back pain is McKenzie training program. McKenzie method leads to improvement of low back pain symptoms such as pain in the short-term. Moreover, McKenzie therapy is more effective in comparison with passive treatments. This training is designed to mobilize the spine and to strengthen the lumbar muscles. Previous studies have shown that weakness and atrophy in the body central muscles, particularly the transverse abdominal muscle in patients with low back pain.[28] The results of this research also showed that there was a significant difference in the general health indexes between Pilates and McKenzie groups. In the present study, 6 weeks of Pilates and McKenzie training led to a significant reduction in the level of general health (physical symptoms, anxiety, social dysfunction, and depression) in men with chronic low back pain and the general health in Pilates training group improved. The results of most studies show that exercise therapy reduces pain and improves general health in patients with chronic low back pain. Importantly, the agreement about the duration, type, and intensity of the training remains to be achieved and there is no definite training program that can have the best effect on patients with chronic low back pain. Therefore, more research is needed to determine the best duration and treatment method to reduce and improve general health in patients with low back pain. In the Al-Obaidi et al. study, pain, fear, and functional disability improved after 10 weeks of treatment in patients.[5]
Besides that McKenzie training increases the range of motion of lumbar flexion. Overall, neither of the two methods of treatment was superior over the other.[18]
Borges et al. concluded that after 6 weeks of treatment, the average index of pain in experimental group was lower than the control group. Furthermore, the general health of the experimental group exhibited greater improvement than the control group. The results of this research support recommending Pilates training to patients with chronic low back pain.[29] Caldwell et al. on the university students concluded that Pilates training and Tai chi guan improved mental parameters such as self-sufficiency, quality of sleep, and morality of students but had no effect on physical performance.[30] Garcia et al. study on 148 patients with nonspecific chronic low back pain concluded that treating patients with nonspecific chronic low back pain by McKenzie training and back school caused disability to improve after treatment, but quality of life, pain, and the range of motor flexibility did not change. McKenzie treatment is typically more effective on disability than back school program.[19]
The overall findings of this study are supported by the literature, demonstrating that a Pilates program may offer a low-cost, safe alternative to the treatment of low back pain in this specific group of patients. Similar effects have been found in patients with unspecific chronic low back pain.[31]
Our study had good levels of internal and external validity and thus can guide therapists and patients considering therapies of choice for back pain. The trial included a number of features to minimize bias such as prospectively registering and following a published protocol.
Study Limitation
Small sample size enrolled in this study limits the generalization of the study findings.
Conclusion
The results of this study showed that 6-week Pilates and McKenzie training reduced pain in patients with chronic low back pain, but there was no significant difference between the effect of two therapeutic methods on pain and both exercise protocols had the same effect. In addition, Pilates and McKenzie training improved general health; however, according to the mean general health changes after the exercise therapy, it can be argued that the Pilates training has a greater effect in improving general health.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
In conclusion,�when comparing the effects of Pilates and McKenzie training on general health as well as on painful symptoms in men with chronic low back pain, the evidence-based research study determined that both the Pilates and the McKenzie method of training effectively reduced pain in patients with chronic LBP. There was no significant difference between the two therapeutic methods altogether, however, the mean results of the research study demonstrated that Pilates training was more effective towards improving general health in men with chronic low back pain than McKenzie training.� Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Bergstr�m C, Jensen I, Hagberg J, Busch H, Bergstr�m G. Effectiveness of different interventions using a psychosocial subgroup assignment in chronic neck and back pain patients: A 10-year follow-up. Disabil Rehabil. 2012;34:110�8. [PubMed]
2. Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24:783�92. [PubMed]
3. Balagu� F, Mannion AF, Pellis� F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379:482�91. [PubMed]
4. Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. New York: Lippincott Williams & Wilkins; 2011.
5. Al-Obaidi SM, Al-Sayegh NA, Ben Nakhi H, Al-Mandeel M. Evaluation of the McKenzie intervention for chronic low back pain by using selected physical and bio-behavioral outcome measures. PM R. 2011;3:637�46. [PubMed]
6. Dehkordi AH, Heydarnejad MS. Effect of booklet and combined method on parents’ awareness of children with beta-thalassemia major disorder. J Pak Med Assoc. 2008;58:485�7. [PubMed]
7. van der Wees PJ, Jamtvedt G, Rebbeck T, de Bie RA, Dekker J, Hendriks EJ. Multifaceted strategies may increase implementation of physiotherapy clinical guidelines: A systematic review. Aust J Physiother. 2008;54:233�41. [PubMed]
8. Maas ET, Juch JN, Groeneweg JG, Ostelo RW, Koes BW, Verhagen AP, et al. Cost-effectiveness of minimal interventional procedures for chronic mechanical low back pain: Design of four randomised controlled trials with an economic evaluation. BMC Musculoskelet Disord. 2012;13:260. [PMC free article][PubMed]
9. Hernandez AM, Peterson AL. Handbook of Occupational Health and Wellness. Springer: 2012. Work-related musculoskeletal disorders and pain; pp. 63�85.
10. Hassanpour Dehkordi A, Khaledi Far A. Effect of exercise training on the quality of life and echocardiography parameter of systolic function in patients with chronic heart failure: A randomized trial. Asian J Sports Med. 2015;6:e22643. [PMC free article][PubMed]
11. Hasanpour-Dehkordi A, Khaledi-Far A, Khaledi-Far B, Salehi-Tali S. The effect of family training and support on the quality of life and cost of hospital readmissions in congestive heart failure patients in Iran. Appl Nurs Res. 2016;31:165�9. [PubMed]
12. Hassanpour Dehkordi A. Influence of yoga and aerobics exercise on fatigue, pain and psychosocial status in patients with multiple sclerosis: A Randomized Trial. J Sports Med Phys Fitness. 2015 [Epub ahead of print] [PubMed]
13. Hassanpour-Dehkordi A, Jivad N. Comparison of regular aerobic and yoga on the quality of life in patients with multiple sclerosis. Med J Islam Repub Iran. 2014;28:141. [PMC free article][PubMed]
14. Heydarnejad S, Dehkordi AH. The effect of an exercise program on the health-quality of life in older adults. A randomized controlled trial. Dan Med Bull. 2010;57:A4113. [PubMed]
15. van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Best Pract Res Clin Rheumatol. 2010;24:193�204. [PubMed]
16. Critchley DJ, Pierson Z, Battersby G. Effect of pilates mat exercises and conventional exercise programmes on transversus abdominis and obliquus internus abdominis activity: Pilot randomised trial. Man Ther. 2011;16:183�9. [PubMed]
17. Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. J Strength Cond Res. 2010;24:661�7. [PubMed]
18. Hosseinifar M, Akbari A, Shahrakinasab A. The effects of McKenzie and lumbar stabilization exercises on the improvement of function and pain in patients with chronic low back pain: A randomized controlled trial. J Shahrekord Univ Med Sci. 2009;11:1�9.
19. Garcia AN, Costa Lda C, da Silva TM, Gondo FL, Cyrillo FN, Costa RA, et al. Effectiveness of back school versus McKenzie exercises in patients with chronic nonspecific low back pain: A randomized controlled trial. Phys Ther. 2013;93:729�47. [PubMed]
20. Hassanpour-Dehkordi A, Safavi P, Parvin N. Effect of methadone maintenance treatment of opioid dependent fathers on mental health and perceived family functioning of their children. Heroin Addict Relat Clin. 2016;18(3):9�14.
21. Shahbazi K, Solati K, Hasanpour-Dehkordi A. Comparison of hypnotherapy and standard medical treatment alone on quality of life in patients with irritable bowel syndrome: A Randomized Control Trial. J Clin Diagn Res. 2016;10:OC01�4. [PMC free article][PubMed]
22. Ngamkham S, Vincent C, Finnegan L, Holden JE, Wang ZJ, Wilkie DJ. The McGill Pain Questionnaire as a multidimensional measure in people with cancer: An integrative review. Pain Manag Nurs. 2012;13:27�51. [PMC free article][PubMed]
23. Sterling M. General health questionnaire-28 (GHQ-28) J Physiother. 2011;57:259. [PubMed]
24. Petersen T, Kryger P, Ekdahl C, Olsen S, Jacobsen S. The effect of McKenzie therapy as compared with that of intensive strengthening training for the treatment of patients with subacute or chronic low back pain: A randomized controlled trial. Spine (Phila Pa 1976) 2002;27:1702�9. [PubMed]
25. Gladwell V, Head S, Haggar M, Beneke R. Does a program of pilates improve chronic non-specific low back pain? J Sport Rehabil. 2006;15:338�50.
26. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining lumbar extension training with McKenzie therapy: Effects on pain, disability, and psychosocial functioning in chronic low back pain patients. Gundersen Lutheran Med J. 2004;3:7�12.
27. Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: A randomized controlled trial. BMC Med. 2010;8:10. [PMC free article][PubMed]
28. Kilpikoski S. The McKenzie Method in Assessing, Classifying and Treating Non-Specific Low Back Pain in Adults with Special Reference to the Centralization Phenomenon. Jyv�skyl� University of Jyv�skyl� 2010
29. Borges J, Baptista AF, Santana N, Souza I, Kruschewsky RA, Galv�o-Castro B, et al. Pilates exercises improve low back pain and quality of life in patients with HTLV-1 virus: A randomized crossover clinical trial. J Bodyw Mov Ther. 2014;18:68�74. [PubMed]
30. Caldwell K, Harrison M, Adams M, Triplett NT. Effect of pilates and taiji quan training on self-efficacy, sleep quality, mood, and physical performance of college students. J Bodyw Mov Ther. 2009;13:155�63. [PubMed]
31. Altan L, Korkmaz N, Bingol U, Gunay B. Effect of pilates training on people with fibromyalgia syndrome: A pilot study. Arch Phys Med Rehabil. 2009;90:1983�8. [PubMed]
Chiropractic Management of Low Back Pain and Low Back-Related Leg Complaints: A Literature Synthesis
Chiropractic care is a well-known complementary and alternative treatment option frequently used to diagnose, treat and prevent injuries and conditions of the musculoskeletal and nervous systems. Spinal health issues are among some of the most common reasons people seek chiropractic care, especially for low back pain and sciatica complaints. While there are many different types of treatments available to help improve low back pain and sciatica symptoms, many individuals will often prefer natural treatment options over the use of drugs/medications or surgical interventions. The following research study demonstrates a list of evidence-based chiropractic treatment methods and their effects towards improving a variety of spinal health issues.
Abstract
Objectives: The purpose of this project was to review the literature for the use of spinal manipulation for low back pain (LBP).
Methods: Asearch strategymodified fromthe Cochrane Collaboration reviewforLBP was conducted through the following databases: PubMed, Mantis, and the Cochrane Database. Invitations to submit relevant articles were extended to the profession via widely distributed professional news and association media. The Scientific Commission of the Council on Chiropractic Guidelines and Practice Parameters (CCGPP) was charged with developing literature syntheses, organized by anatomical region, to evaluate and report on the evidence base for chiropractic care. This article is the outcome of this charge. As part of the CCGPP process, preliminary drafts of these articles were posted on the CCGPP Web site www.ccgpp.org (2006-8) to allow for an open process and the broadest possible mechanism for stakeholder input.
Results: A total of 887 source documents were obtained. Search results were sorted into related topic groups as follows: randomized controlled trials (RCTs) of LBP and manipulation; randomized trials of other interventions for LBP; guidelines; systematic reviews and meta-analyses; basic science; diagnostic-related articles, methodology; cognitive therapy and psychosocial issues; cohort and outcome studies; and others. Each group was subdivided by topic so that team members received approximately equal numbers of articles from each group, chosen randomly for distribution. The team elected to limit consideration in this first iteration to guidelines, systematic reviews, meta-analyses, RCTs, and coh ort studies. This yielded a total of 12 guidelines, 64 RCTs, 13 systematic reviews/meta-analyses, and 11 cohort studies.
Conclusions: As much or more evidence exists for the use of spinal manipulation to reduce symptoms and improve function in patients with chronic LBP as for use in acute and subacute LBP. Use of exercise in conjunction with manipulation is likely to speed and improve outcomes as well as minimize episodic recurrence. There was less evidence for the use of manipulation for patients with LBP and radiating leg pain, sciatica, or radiculopathy. (J Manipulative Physiol Ther 2008;31:659-674)
The Council on Chiropractic Guidelines and Practice Parameters (CCGPP) was formed in 1995 by the Congress of Chiropractic State Associations with assistance from the American Chiropractic Association, Association of Chiropractic Colleges, Council on Chiropractic Education, Federation of Chiropractic Licensing�Boards, Foundation for the Advancement of Chiropractic Sciences, Foundation for Chiropractic Education and Research, International Chiropractors Association, National Association of Chiropractic Attorneys, and the National Institute for Chiropractic Research. The charge to the CCGPP was to create a chiropractic �best practices� document. The Council on Chiropractic Guidelines and Practice Parameters was delegated to examine all existing guidelines, parameters, protocols, and best practices in the United States and other nations in the construction of this document.
Toward that end, the Scientific Commission of CCGPP was charged with developing literature syntheses, organized by region (neck, low back, thoracic, upper and lower extremity, soft tissue) and the nonregional categories of nonmusculoskeletal, prevention/health promotion, special populations, subluxation, and diagnostic imaging.
The purpose of this work is to provide a balanced interpretation of the literature to identify safe and effective treatment options in the care of patients with low back pain (LBP) and related disorders. This evidence summary is intended to serve as a resource for practitioners to assist them in consideration of various care options for such patients. It is neither a replacement for clinical judgment nor a prescriptive standard of care for individual patients.
Methods
Process development was guided by experience of commission members with the RAND consensus process, Cochrane collaboration, Agency for Health Care and Policy Research, and published recommendations modified to the needs of the council.
Identification and Retrieval
The domain for this report is that of LBP and low backrelated leg symptoms. Using surveys of the profession and publications on practice audits, the team selected the topics for review by this iteration.
Topics were selected based on the most common disorders seen and most common classifications of treatments used by chiropractors based on the literature. Material for review was obtained through formal hand searches of published literature and of electronic databases, with assistance from a professional chiropractic college librarian. A search strategy was developed, based upon the CochraneWorking Group for Low Back Pain. Randomized controlled trials (RCTs), systematic reviews/meta-analyses, and guidelines published through 2006 were included; all other types of studies were included through 2004. Invitations to submit relevant articles were extended to the profession via widely distributed professional news and association media. Searches focused on guidelines, meta-analyses, systematic reviews, randomized clinical trials, cohort studies, and case series.
Evaluation
Standardized and validated instruments used by the Scottish Intercollegiate Guidelines Network were used to evaluate RCTs and systematic reviews. For guidelines, the Appraisal of Guidelines for Research and Evaluation instrument was used. A standardized method for grading the strength of the evidence was used, as summarized in Figure 1. Each team’s multidisciplinary panel conducted the review and evaluation of the evidence.
Search results were sorted into related topic groups as follows: RCTs of LBP and manipulation; randomized trials of other interventions for LBP; guidelines; systematic reviews and meta-analyses; basic science; diagnosticrelated articles; methodology; cognitive therapy and psychosocial issues; cohort and outcome studies; and others. Each group was subdivided by topic so that team members received approximately equal numbers of articles from each group, chosen randomly for distribution. On the basis of the CCGPP formation of an iterative process and the volume of work available, the team elected to limit consideration in this first iteration to guidelines, systematic reviews, meta-analyses, RCTs, and cohort studies.
Dr. Alex Jimenez’s Insight
How does chiropractic care benefit people with low back pain and sciatica?�As a chiropractor experienced in the management of a variety of spine health issues, including low back pain and sciatica, spinal adjustments and manual manipulations, as well as other non-invasive treatment methods, can be safely and effectively implemented towards the improvement of back pain symptoms. The purpose of the following research study is to demonstrate the evidence-based effects of chiropractic in the treatment of injuries and conditions of the musculoskeletal and nervous systems. The information in this article can educate patients on how alternative treatment options can help improve their low back pain and sciatica. As a chiropractor, patients may also be referred to other healthcare professionals, such as physical therapists, functional medicine practitioners and medical doctors, to help them further manage their low back pain and sciatica symptoms. Chiropractic care can be used to avoid surgical interventions for spine health issues.
Results and Discussion
A total of 887 source documents were initially obtained. This included a total of 12 guidelines, 64 RCTs, 20 systematic reviews/meta-analyses, and 12 cohort studies. Table 1 provides an overall summary of the number of studies evaluated.
Assurance and Advice
The search strategy used by the team was that developed by van Tulder et al, and the team identified 11 trials. Good evidence indicates that patients with acute LBP on bed rest have more pain and less functional recovery than those who stay active. There is no difference in pain and functional status between bed rest and exercises. For sciatica patients, fair evidence shows no real difference in pain and functional status between bed rest and staying active. There is fair evidence of no difference in pain intensity between bed rest and physiotherapy but small improvements in functional status. Finally, there is little difference in pain intensity or functional status between shorter-term or longer-term bed rest.
A Cochrane review by Hagen et al demonstrated small advantages in short-term and long-term for staying active over bed rest, as did a high-quality review by the Danish Society of Chiropractic and Clinical Biomechanics, including 4 systematic reviews, 4 additional RCTS, and 6 guidelines, on acute LBP and sciatica. The Cochrane review by Hilde et al included 4 trials and concluded a small beneficial effect for staying active for acute, uncomplicated LBP, but no benefit for sciatica. Eight studies on staying active and 10 on bed rest were included in an analysis by the group of Waddell. Several therapies were coupled with advice to stay active and include analgesic medication, physical therapy, back school, and behavioral counseling. Bed rest for acute LBP was similar to no treatment and placebo and less effective than alternative treatment. Outcomes considered across the studies were rate of recovery, pain, activity levels, and work time loss. Staying active was found to have a favorable effect.
Review of 4 studies not covered elsewhere assessed the use of brochures/booklets. The trend was for no differences in outcome for pamphlets. One exception was noted�that those who received manipulation had less bothersome symptoms at 4 weeks and significantly less disability at 3 months for those who received a booklet encouraging staying active.
In summary, assuring patients that they are likely to do well and advising them to stay active and avoid bed rest is a best practice for management of acute LBP. Bed rest for short intervals may be beneficial for patients with radiating leg pain who are intolerant of weight bearing.
Adjustment/Manipulation/Mobilization Vs Multiple Modalities
This review considered literature on high-velocity, lowamplitude (HVLA) procedures, often termed adjustment or manipulation, and mobilization. The HVLA procedures use thrusting maneuvers applied quickly; mobilization is applied cyclically. The HVLA procedure and mobilization may be mechanically assisted; mechanical impulse devices are considered HVLA, and flexion-distraction methods and continuous passive motion methods are within mobilization.
The team recommends adopting the findings of the systematic review by Bronfort et al, with a quality score (QS) of 88, covering literature up to 2002. In 2006, the Cochrane collaboration reissued an earlier (2004) review of spinal manipulative therapy (SMT) for back pain performed by Assendelft et al. This reported on 39 studies up to 1999, several overlapping with those reported by Bronfort et al using different criteria and a novel analysis. They report no difference in outcome from treatment with manipulation vs alternatives. As several additional RCTs had appeared in the interim, the rationale for reissuing the older review without acknowledging new studies was unclear.
Acute LBP. There was fair evidence that HVLA has better short-term efficacy than mobilization or diathermy and limited evidence of better short-term efficacy than diathermy, exercise, and ergonomic modifications.
Chronic LBP. The HVLA procedure combined with strengthening exercise was as effective for pain relief as nonsteroidal antiinflammatory dugs with exercise. Fair evidence indicated that manipulation is better than physical therapy and home exercise for reducing disability. Fair evidence shows that manipulation improves outcomes more than general medical care or placebo in the short-term and to physical therapy in the long-term. The HVLA procedure had better outcomes than home exercise, transcutaneous�electrical nerve stimulation, traction, exercise, placebo and sham manipulation, or chemonucleolysis for disk herniation.
Mixed (Acute and Chronic) LBP. Hurwitz found that HVLA was the same as medical care for pain and disability; adding physical therapy to manipulation did not improve outcomes. Hsieh found no significant value for HVLA over back school or myofascial therapy. A short-term value of manipulation over a pamphlet and no difference between manipulation and McKenzie technique were reported by Cherkin et al. Meade contrasted manipulation and hospital care, finding greater benefit for manipulation over both short-term and long-term. Doran and Newell found that SMT resulted in greater improvement than physical therapy or corsets.
Acute LBP
Sick List Comparisons. Seferlis found that sick patients listed were significantly improved symptomatically after 1 month regardless of the intervention, including manipulation. Patients were more satisfied and felt that they were provided better explanations about their pain from practitioners who used manual therapy (QS, 62.5). Wand et al examined the effects of sick-listing oneself and noted that a group receiving assessment, advice, and treatment improved better than did a group getting assessment, advice, and who were put on a wait list for a 6-week period. Improvements were observed in disability, general health, quality of life, and mood, though pain and disability were not different at longterm follow-up (QS, 68.75).
Physiologic Therapeutic Modality and Exercise. Hurley and colleagues tested the effects of manipulation combined with interferential therapy compared to either modality alone. Their results showed all 3 groups improved function to the same degree, both at 6-month and at 12-month follow-up (QS, 81.25). Using a single-blinded experimental design to compare manipulation to massage and low-level electrostimulation, Godfrey et al found no differences between groups at the 2 to 3-week observation time frame (QS, 19). In the study by Rasmussen, results showed that 94% of the patients treated with manipulation were symptom-free within 14 days, compared to 25% in the group that received short-wave diathermy. Sample size was small, however, and as a result, the study was underpowered (QS, 18). The Danish systematic review examined 12 international sets of guidelines, 12 systematic reviews, and 10 randomized clinical trials on exercise. They found no specific exercises, regardless of type, that were useful for the treatment of acute LBP with the exception of McKenzie maneuvers.
Sham and Alternate Manual Method Comparisons. The study of Hadler balanced for effects of provider attention and physical contact with a first effort at a manipulation sham procedure. Patients in the group that entered the trial with greater prolonged illness at the outset were reported to have benefited from the manipulation. Similarly, they improved faster and to a greater degree (QS, 62.5). Hadler demonstrated that there was a benefit for a single session of manipulation compared to a session of mobilization (QS, 69). Erhard reported that the rate of positive response to manual treatment with a hand-heel rocking motion was greater than with extension exercises (QS, 25). Von Buerger examined the use of manipulation for acute LBP, comparing rotational manipulation to soft tissue massage. He found that the manipulation group responded better than the soft tissue group, although the effects occurred mainly in the short-term. The results were also hampered by the nature of the forced multiple choice selections on the data forms (QS, 31). Gemmell compared 2 forms of manipulation for LBP of less than 6 weeks of duration as follows: Meric adjusting (a form of HVLA) and Activator technique (a form of mechanically assisted HVLA). No difference was observed, and both helped to reduce pain intensity (QS, 37.5). MacDonald reported a short-term benefit in disability measures within the first 1 to 2 weeks of starting therapy for the manipulation group that disappeared by 4 weeks in a control group (QS, 38). The work of Hoehler, although containing mixed data for patients with acute and chronic LBP, is included here because a larger proportion of patients with acute LBP were involved in the study. Manipulation patients reported immediate relief more often, but there were no differences between groups at discharge (QS, 25).
Medication. Coyer showed that 50% of the manipulation group was symptom-free within 1 week and 87% were discharged symptom-free in 3 weeks, compared to 27% and 60%, respectively, of the control group (bed rest and analgesics) (QS, 37.5). Doran and Newell compared manipulation, physiotherapy, corset, or analgesic medication, using outcomes that examined pain and mobility. There were no differences between groups over time (QS, 25). Waterworth compared manipulation to conservative physiotherapy and 500 mg of diflunisal twice per day for 10 days. Manipulation showed no benefit for the rate of recovery (QS, 62.5). Blomberg compared manipulation to steroid injections and to a control group receiving conventional activating therapy. After 4 months, the manipulation group had less restricted motion in extension, less restriction in side-bending to both sides, less local pain on extension and right sidebending, less radiating pain, and less pain when performing a straight leg raise (QS, 56.25). Bronfort found no outcome differences between chiropractic care compared to medical care at 1 month of treatment, but there were noticeable improvements in the chiropractic group at both 3 and 6-month follow-up (QS, 31).
Subacute Back Pain
Staying Active. Grunnesjo compared combined effects of manual therapy with advice to stay active to advice alone in patients with acute and subacute LBP. The addition of�manual therapy appeared to reduce pain and disability more effectively than the �stay active� concept alone (QS, 68.75).
Physiologic Therapeutic Modality and Exercise. Pope demonstrated that manipulation offered better pain improvement than transcutaneous electrical nerve stimulation (QS 38). Sims-Williams compared manipulation to �physiotherapy.� Results demonstrated a short-term benefit for manipulation on pain and ability to do light work. Differences between groups waned at 3 and 12-month follow-ups (QS, 43.75, 35). Skargren et al compared chiropractic to physiotherapy for patients with LBP who had no treatment for the prior month. No differences in health improvements, costs, or recurrence rates were noted between the 2 groups. However, based on Oswestry scores, chiropractic performed better for patients who had pain for less than 1 week, whereas the physiotherapy seemed to be better for those who had pain for more than 4 weeks (QS, 50).
The Danish systematic review examined 12 international sets of guidelines, 12 systematic reviews, and 10 randomized clinical trials on exercise. Results suggested that exercise, in general, benefits patients with subacute back pain. Use of a basic program that can be readily modified to meet individual patient needs is recommended. Issues of strength, endurance, stabilization, and coordination without excessive loading can all be addressed without the use of high-tech equipment. Intensive training consisting of greater than 30 and less than 100 hours of training are most effective.
Sham and Alternate Manual Method Comparisons. Hoiriis compared efficacy of chiropractic manipulation to placebo/ sham for subacute LBP. All groups improved on measures of pain, disability, depression, and Global Impression of Severity. Chiropractic manipulation scored better than placebo in reducing pain and Global Impression of Severity scores (QS, 75). Andersson and colleagues compared osteopathic manipulation to standard care to patients with subacute LBP, finding that both groups improved for a 12-week period at about the same rate (QS, 50).
Medication Comparisons. In a separate treatment arm of the study of Hoiriis, the relative efficacy of chiropractic manipulation to muscle relaxants for subacute LBP was studied. In all groups, pain, disability, depression, and Global Impression of Severity decreased. Chiropractic manipulation was more effective than muscle relaxants in reducing Global Impression of Severity scores (QS, 75).
Chronic LBP
Staying Active Comparisons. Aure compared manual therapy to exercise in patients with chronic LBP who were sick listed. Although both groups showed improvements in pain intensity, functional disability, general health, and return to work, the manual therapy group showed significantly greater improvements than did the exercise group for all outcomes. Results were consistent for both the short-term and the longterm (QS, 81.25).
Physician Consult/Medical Care/Education. Niemisto compared combined manipulation, stabilization exercise, and physician consultation to consultation alone. The combined intervention was more effective in reducing pain intensity and disability (QS, 81.25). Koes compared general practitioner treatment to manipulation, physiotherapy, and a placebo (detuned ultrasound). Assessments were made at 3, 6, and 12 weeks. The manipulation group had a quicker and larger improvement in physical function compared to the other therapies. Changes in spinal mobility in the groups were small and inconsistent (QS, 68). In a follow-up report, Koes found during subgroup analysis that improvement in pain was greater for manipulation than for other treatments at 12 months when considering patients with chronic conditions, as well as those who were younger than 40 years (QS, 43). Another study by Koes showed that many patients in the nonmanipulation treatment arms had received additional care during follow-up. Yet, improvement in the main complaints and in physical functioning remained better in the manipulation group (QS, 50). Meade observed that chiropractic treatment was more effective than hospital outpatient care, as assessed using the Oswestry Scale (QS, 31). An RCT conducted in Egypt by Rupert compared chiropractic manipulation, after medical and chiropractic evaluation. Pain, forward flexion, active, and passive leg raise all improved to a greater degree in the chiropractic group; however, the description of alternate treatments and outcomes was ambiguous (QS, 50).
Triano compared manual therapy to educational programs for chronic LBP. There was greater improvement in pain, function, and activity tolerance in the manipulation group, which continued beyond the 2-week treatment period (QS, 31).
Physiologic Therapeutic Modality. A negative trial for manipulation was reported by Gibson (QS, 38). Detuned diathermy was reported to achieve better results over manipulation, although there were baseline differences between groups. Koes studied the effectiveness of manipulation, physiotherapy, treatment by a general practitioner, and a placebo of detuned ultrasound. Assessments were made at 3, 6, and 12 weeks. The manipulation group showed a quicker and better improvement in physical function capacity compared to the other therapies. Flexibility differences between groups were not significant (QS, 68). In a follow-up report, Koes found that a subgroup analysis demonstrated that improvement in pain was greater for those treated with manipulation, both for younger (b40) patients and those with chronic conditions at 12-month follow-up (QS, 43). Despite many patients in the nonmanipulation groups received additional care during follow-up, improvements remained better in the manipulation group than in the physical therapy group (QS, 50). In a separate report by the same group, there were improvements in both the physiotherapy and manual therapy groups with regard to severity of complaints and global perceived effect compared to general practitioner care;�however, the differences between the 2 groups was not significant (QS, 50). Mathews et al found that manipulation hastened recovery from LBP more than the control did.
Exercise Modality. Hemilla observed that SMT led to better long-term and short-term disability reduction compared to physical therapy or home exercise (QS, 63). A second article by the same group found that neither bone-setting nor exercise differed significantly from physical therapy for symptom control, though bone-setting was associated with improved lateral and forward-bending of the spine more than exercise (QS, 75). Coxhea reported that HVLA provided better outcomes when compared to exercise, corsets, traction, or no exercise when studied in the short-term (QS, 25). Conversely, Herzog found no differences between manipulation, exercise, and back education in reducing either pain or disability (QS, 6). Aure compared manual therapy to exercise in patients with chronic LBP who were also sick listed. Although both groups showed improvements in pain intensity, functional disability, and general health and returned to work, the manual therapy group showed significantly greater improvements than did the exercise group for all outcomes. This result persisted for both the short-term and the long-term (QS, 81.25). In the article by Niemisto and colleagues, the relative efficacy of combined manipulation, exercise (stabilizing forms), and physician consultation compared to consultation alone was investigated. The combined intervention was more effective in reducing pain intensity and disability (QS, 81.25). The United Kingdom Beam study found that manipulation followed by exercise achieved a moderate benefit at 3 months and a small benefit at 12 months. Likewise, manipulation achieved a small to moderate benefit at 3 months and a small benefit at 12 months. Exercise alone had a small benefit at 3 months but no benefit at 12 months. Lewis et al found improvement occurred when patients were treated by combined manipulation and spinal stabilization exercises vs use of a 10-station exercise class.
The Danish systematic review examined 12 international sets of guidelines, 12 systematic reviews, and 10 randomized clinical trials on exercise. Results suggested that exercise, in general, benefits patients with chronic LBP. No clear superior method is known. Use of a basic program that can be readily modified to meet individual patient needs is recommended. Issues of strength, endurance, stabilization, and coordination without excessive loading can all be addressed without the use of high-tech equipment. Intensive training consisting of greater than 30 and less than 100 hours of training are most effective. Patients with severe chronic LBP, including those off work, are treated more effectively with a multidisciplinary rehabilitation program. For post surgical rehabilitation, patients starting 4 to 6 weeks after disk surgery under intensive training receive greater benefit than with light exercise programs.
Sham and Alternate Manual Methods. Triano found that SMT produced significantly better results for pain and disability relief for the short-term, than did sham manipulation (QS, 31). Cote found no difference over time or for comparisons within or between the manipulation and mobilization groups (QS, 37.5). The authors posed that failure to observe differences may have been due to low responsiveness to change in the instruments used for algometry, coupled with a small sample size. Hsieh found no significant value for HVLA over back school or myofascial therapy (QS, 63). In the study by Licciardone, a comparison was made between osteopathic manipulation (which includes mobilization and soft tissue procedures as well as HVLA), sham manipulation, and a no-intervention control for patients with chronic LBP. All groups showed improvement. Sham and osteopathic manipulation were associated with greater improvements than seen in the no-manipulation group, but no difference was observed between the sham and manipulation groups (QS, 62.5). Both subjective and objective measures showed greater improvements in the manipulation group compared to a sham control, in a report by Waagen (QS, 44). In the work of Kinalski, manual therapy reduced the time of treatment of patients with LBP and concomitant intervertebral disk lesions. When disk lesions were not advanced, a decreased muscular hypertonia and increased mobility was noted. This article, however, was limited by a poor description of patients and methods (QS, 0).
Harrison et al reported a nonrandomized cohort controlled trial of treatment of chronic LBP consisting of 3-point bending traction designed to increase curvature of the lumbar spine. The experimental group received HVLA for pain control during the first 3 weeks (9 treatments). The control group received no treatment. Follow-up at a mean of 11 weeks showed no change in pain or curvature status for controls but a significant increase in curvature and reduction of pain in the experimental group. Average number of treatments to achieve this result was 36. Long-term followup at 17 months showed retention of benefits. No report of relationship between clinical changes and structural change was given.
Haas and colleagues examined the dose-response patterns of manipulation for chronic LBP. Patients were randomly allocated to groups receiving 1, 2, 3, or 4 visits per week for 3 weeks, with outcomes recorded for pain intensity and functional disability. A positive and clinically important effect of the number of chiropractic treatments on pain intensity and disability at 4 weeks was associated with the groups receiving the higher rates of care (QS, 62.5). Descarreaux et al extended this work, treating 2 small groups for 4 weeks (3 times per week) after 2 baseline evaluations separated by 4 weeks. One group was then treated every 3 weeks; the other did not. Although both groups had lower Oswestry scores at 12 weeks, at 10 months, the improvement only persisted for the extended SMT group.
Medication. Burton and colleagues demonstrated that HVLA led to greater short-term improvements in pain and disability than did chemonucleolysis for managing disk�herniation (QS, 38). Bronfort studied SMT combined with exercise vs a combination of nonsteroidal antiinflammatory drugs and exercise. Similar results were obtained for both groups (QS, 81). Forceful manipulation coupled with sclerosant therapy (injection of a proliferant solution composed of dextrose-glycerine-phenol) was compared to lower force manipulation combined with saline injections, in a study by Ongley. The group receiving forceful manipulation with sclerosant fared better than the alternate group, but effects cannot be separated between the manual procedure and the sclerosant (QS, 87.5). Giles and Muller compared HVLA procedures to medication and acupuncture. Manipulation showed greater improvement in frequency of back pain, pain scores, Oswestry, and SF-36 compared to the other 2 interventions. Improvements lasted for 1 year. Weaknesses of the study were use of a compliers-only analysis as intention to treat for the Oswestry, and Visual Analogue Scale (VAS) was not significant.
Sciatica/Radicular/Radiating Leg Pain
Staying Active/Bed Rest. Postacchini studied a mixed group of patients with LBP, with and without radiating leg pain. Patients could be classified as acute or chronic and were evaluated at 3 weeks, 2 months, and 6 months postonset. Treatments included manipulation, drug therapy, physiotherapy, placebo, and bed rest. Acute back pain without radiation and chronic back pain responded well to manipulation; however, in none of the other groups did manipulation fare as well as other interventions (QS, 6).
Physician Consult/Medical Care/Education. Arkuszewski looked at patients with lumbosacral pain or sciatica. One group received drugs, physiotherapy, and manual examination, whereas the second added manipulation. The group receiving manipulation had a shorter treatment time and a more marked improvement. At 6-month follow-up, the manipulation group showed better neuromotor system function and a better ability to continue employment. Disability was lower in the manipulation group (QS, 18.75).
Physiologic Therapeutic Modality. Physiotherapy combined with manual manipulation and medication was examined by Arkuszewski, in contrast to the same scheme with manipulation added, as noted above. Outcomes from manipulation were better for neurologic and motor function as well as disability (QS, 18.75). Postacchini looked at patients with acute or chronic symptoms evaluated at 3 weeks, 2 months, and 6 months postonset. Manipulation was not as effective for managing the patients with radiating leg pain as the other treatment arms (QS, 6). Mathews and colleagues examined multiple treatments including manipulation, traction, sclerosant use, and epidural injections for back pain with sciatica. For patients with LBP and restricted straight leg raise test, manipulation conferred highly significant relief, more so than alternate interventions (QS, 19). Coxhead et al included among their subjects patients who had radiating pain at least to the buttocks. Interventions included traction, manipulation, exercise, and corset, using a factorial design. After 4 weeks of care, manipulation showed a significant degree of benefit on one of the scales used to assess progress. There were no real differences between groups at 4 months and 16 months posttherapy, however (QS, 25).
Exercise Modality. In the case of LBP after laminectomy, Timm reported that exercises conferred benefit both for pain relief and cost-effectiveness (QS, 25). Manipulation had only a small influence on improvement of either symptoms or function (QS, 25). In the study by Coxhead et al, radiating pain to at least the buttocks was better after 4 weeks of care for manipulation, in contrast to other treatments that disappeared 4 months and 16 months posttherapy (QS, 25).
Sham and Alternate Manual Method. Siehl looked at the use of manipulation under general anesthesia for patients with LBP and unilateral or bilateral radiating leg pain. Only temporary clinical improvement was noted when traditional electromyographic evidence of nerve root involvement was present. With negative electromyography, manipulation was reported to provide lasting improvement (QS, 31.25) Santilli and colleagues compared HVLA to soft tissue pressing without any sudden thrust in patients with moderate acute back and leg pain. The HVLA procedures were significantly more effective in reducing pain, reaching a pain-free status, and the total number of days with pain. Clinically significant differences were noted. The total number of treatment sessions was capped at 20 on a dosage of 5 times per week with care depending on pain relief. Follow-up showed relief persisting through 6 months.
Medication. Mixed acute and chronic back pain with radiation treated in a study using multiple treatment arms were evaluated at 3 weeks, 2 months, and 6 months postonset by the group of Postacchini. Medication management fared better than did manipulation when radiating leg pain was present (QS, 6). Conversely, for the work of Mathews and colleagues, the group of patients with LBP and limited straight leg raise test responded more to manipulation than to epidural steroid or sclerosants (QS, 19).
Disk Herniation
Nwuga studied 51 subjects who were having a diagnosis of prolapsed intervertebral disk and who had been referred for physical therapy. Manipulation was reported to be superior to conventional therapy (QS, 12.5). Zylbergold found that there were no statistical differences between 3 treatments�lumbar flexion exercises, home care, and manipulation. Short-term follow-up and a small sample size were posed by the author as a basis for failing to reject the null hypothesis (QS, 38).
Exercise
Exercise is one of the most well-studied forms of treatment of low back disorders. There are many different approaches to�exercise. For this report, it is important only to differentiate multidisciplinary rehabilitation. These programs are designed for patients with especially chronic condition with significant psychosocial problems. They involve trunk exercise, functional task training including work simulation/vocational training, and psychological counseling.
In a recent Cochrane review on exercise for the treatment of nonspecific LBP (QS, 82), effectiveness of exercise therapy in patients classified as acute, subacute, and chronic was compared to no treatment and alternate treatments. Outcomes included the assessment of pain, function, return to work, absenteeism, and/or global improvements. In the review, 61 trials met the inclusion criteria, most of which dealt with chronic (n = 43), whereas smaller numbers addressed acute (n = 11) and subacute (n = 6) pain. The general conclusions were as follows:
exercise is not effective as a treatment of acute LBP,
evidence that exercise was effective in chronic populations relative to comparisons made at follow-up periods,
mean improvements of 13.3 points for pain and 6.9 points for function were observed, and
there is some evidence that graded-activity exercise is effective for subacute LBP but only in the occupational setting
The review examined population and intervention characteristics, as well as outcomes to reach its conclusions. Extracting data on return to work, absenteeism, and global improvement proved so difficult that only pain and function could be quantitatively described.
Eight studies scored positively on key validity criteria. With regard to clinical relevance, many of the trials presented inadequate information, with 90% reporting the study population but only 54% adequately describing the exercise intervention. Relevant outcomes were reported in 70% of the trials.
Exercise for Acute LBP. Of the 11 trials (total n = 1192), 10 had nonexercise comparison groups. The trials presented conflicting evidence. Eight low-quality trials showed no differences between exercise and usual care or no treatment. Pooled data showed that there was no difference in shortterm pain relief between exercise and no treatment, no difference in early follow-up for pain when compared to other interventions, and no positive effect of exercise on functional outcomes.
Subacute LBP. In 6 studies (total n = 881), 7 exercise groups had a nonexercise comparison group. The trials offered mixed results with regard to evidence of effectiveness, with fair evidence of effectiveness for a graded-exercise activity program as the only notable finding. Pooled data did not show evidence to either support or refute the use of exercise for subacute LBP, either for decreasing pain or improving function.
Chronic LBP. There were 43 trials included in this group (total n = 3907). Thirty-three of the studies had nonexercise comparison groups. Exercise was at least as effective as other conservative interventions for LBP, and 2 high-quality studies and 9 lower-quality studies found exercise to be more effective. These studies used individualized exercise programs, focusing mainly on strengthening or trunk stabilization. There were 14 trials that found no difference between exercise and other conservative interventions; of these, 2 were rated highly and 12 rated lower. Pooling the data showed a mean improvement of 10.2 (95% confidence interval [CI], 1.31-19.09) points on a 100-mm pain scale for exercise compared to no treatment and 5.93 (95% CI, 2.21- 9.65) points compared to other conservative treatments. Functional outcomes also showed improvements as follows: 3.0 points at earliest follow-up compared to no treatment (95% CI, ?0.53 to 6.48) and 2.37 points (95% CI, 1.04-3.94) compared to other conservative treatments.
Indirect subgroup analysis found that trials examining health care study populations had higher mean improvements in pain and physical functioning compared to their comparison groups or to trials set in occupational or general populations.
The review authors offered the following conclusions:
In acute LBP, exercises are not more effective than other conservative interventions. Meta-analysis showed no advantage over no treatment of pain and functional outcomes over the short or long-term.
There is fair evidence of effectiveness of a gradedactivity exercise program in subacute LBP in occupational settings. The effectiveness for other types of exercise therapy in other populations is unclear.
In chronic LBP, there is good evidence that exercise is at least as effective as other conservative treatments. Individually designed strengthening or stabilizing programs appear to be effective in health care settings. Meta-analysis found functional outcomes significantly improved; however, the effects were very small, with a less than 3-point (of 100) difference between the exercise and comparison groups at earliest follow-up. Pain outcomes were also significantly improved in groups receiving exercises relative to other comparisons, with a mean of approximately 7 points. Effects were similar over longer follow-up, though confidence intervals increased. Mean improvements in pain and functioning may be clinically meaningful in studies from health care populations in which improvements were significantly greater than those observed in studies from general or mixed populations.
The Danish group review of exercise was able to identify 5 systematic reviews and 12 guidelines that discussed exercise for acute LBP, 1 systematic review and 12 guidelines for subacute, and 7 systematic reviews and 11 guidelines for chronic. Furthermore, they identified 1 systematic review that selectively evaluated for postsurgical�cases. Conclusions were essentially the same as the Cochrane review, with the exceptions that there was limited support for McKenzie maneuvers for patients with acute condition and for intensive rehabilitation programs for 4 to 6 weeks after disk surgery over light exercise programs.
Natural and Treatment History for LBP
Most studies have demonstrated that nearly half of LBP will improve within 1 week, whereas nearly 90% of it will be gone by 12 weeks. Even more, Dixon demonstrated that perhaps as much as 90% of LBP will resolve on its own, without any intervention whatsoever. Von Korff demonstrated that a significant number of patients with acute LBP will have persistent pain if they are observed up to 2 years.
Phillips found that nearly 4 of 10 people will have LBP after an episode at 6 months from onset, even if the original pain has disappeared because more than 6 in 10 will have at least 1 relapse during the first year after an episode. These initial relapses occur within 8 weeks most commonly and may reoccur over time, though in decreasing percentages.
Workers’ compensation injury patients were observed for 1 year to examine symptom severity and work status. Half of those studied lost no work time in the first month after injury, but 30% did lose time from work due to their injury over the course of 1 year. Of those who missed work in the first month due to their injury and had already been able to return to work, nearly 20% had absence later in that same year. This implies that assessing return to work at 1 month after injury will fail to give an honest depiction of the chronic, episodic nature of LBP. Although many patients have returned to work, they will later experience continuing problems and work-related absences. Impairment present at more than 12 weeks postinjury may be far higher than what has been previously reported in the literature, where rates of 10% are common. In fact, the rates may go up to 3 to 4 times higher.
In a study by Schiotzz-Christensen and colleagues, the following was noted. In relation to sick leave, LBP has a favorable prognosis, with a 50% return to work within the first 8 days and only 2% on sick leave after 1 year. However, 15% had been on sick leave during the following year and about half continued to complain of discomfort. This suggested that an acute episode of LBP significant enough to cause the patient to seek a visit to a general practitioner is followed by a longer period of low-grade disability than previously reported. Also, even for those who returned to work, up to 16% indicated that they were not functionally improved. In another study looking at outcomes after 4 weeks after initial diagnosis and treatment, only 28% of patients did not experience any pain. More strikingly, the persistence of pain differed between groups that had radiating pain and those that did not, with 65% of the former feeling improvement at 4 weeks, vs 82% of the latter. The general findings from this study differ from others in that 72% of patients still experienced pain 4 weeks after initial diagnosis.
Hestbaek and colleagues reviewed a number of articles in a systematic review. The results showed that the reported proportion of patients who still experienced pain after 12 months after onset was 62% on average, with 16% sick-listed 6 months after onset, and with 60% experiencing relapse of work absence. Also, they found that the mean reported prevalence of LBP in patients who had past episodes of LBP was 56%, compared to just 22% for those who had no such history. Croft and colleagues performed a prospective study looking at the outcomes of LBP in general practice, finding that 90% of patients with LBP in primary care had stopped consulting with symptoms within 3 months; however, most were still experiencing LBP and disability 1 year after the initial visit. Only 25% had fully recovered within that same year.
There are even different results in the study by Wahlgren et al. Here, most patients continued to experience pain at both 6 and 12 months (78% and 72%, respectively). Only 20% of the sample had fully recovered by 6 months and only 22% by 12 months.
Von Korff has provided a lengthy list of data he considers relevant to assessing the clinical course of back pain as follows: age, sex, race/ethnicity, years of education, occupation, change in occupation, employment status, disability insurance status, litigation status, recency/age at first onset of back pain, recency/age when care was sought, recency of back pain episode, duration of current/most recent episode of back pain, number of back pain days, current pain intensity, average pain intensity, worst pain intensity, ratings of interference with activities, activity limitation days, clinical diagnosis for this episode, bed rest days, work loss days, recency of back pain flare-up, and duration of the most recent flare-up.
In a practice-based observational study by Haas et al of almost 3000 patients with acute and chronic condition treated by chiropractors and primary care medical doctors, pain was noted in patients with acute and chronic condition up to 48 months after enrollment. At 36 months, 45% to 75% of patients reported at least 30 days of pain in the prior year, and 19% to 27% of patients with chronic condition recalled daily pain over the previous year.
The variability noted in these and many other studies can be explained in part by the difficulty in making an adequate diagnosis, by the different classification schemes used in classifying LBP, by the different outcome tools used in each study and by many other factors. It also points up the extreme difficulty in getting a handle on the day-to-day reality for those who have LBP.
Common Markers and Rating Complexity for LBP
What Are the Relevant Benchmarks for Evaluating Process of Care?. One benchmark is described above, that being natural history. Complexity and risk stratification are important, as�are cost issues; however, cost-effectiveness is beyond the scope of this report.
It is understood that patients with uncomplicated LBP improve faster than those with various complications, the most notable of which is radiating pain. Many factors may influence the course of back pain, including comorbidity, ergonomic factors, age, the level of fitness of the patient, environmental factors, and psychosocial factors. The latter is receiving a great deal of attention in the literature, though as noted elsewhere in this book, such consideration may not be justified. Any of these factors, alone or in combination, may hamper or retard the recovery period after injury.
It seems that biomechanical factors play an important role in the incidence of first-time episodes of LBP and its attendant problems such as work loss; psychosocial factors come into play more in subsequent episodes of LBP. The biomechanical factors can lead to tissue tearing, which then create pain and limited ability for years to follow. This tissue damage cannot be seen on standard imaging and may only be apparent upon dissection or surgery.
abnormal joint motion or decreased body mechanics;
prolonged static posture or poor motor control;
work-related such as vehicle operation, sustained loads, materials handling;
employment history and satisfaction; and
wage status.
IJzelenberg and Burdorf investigated whether demographic, work-related physical, or psychosocial risk factors involved in the occurrence of musculoskeletal conditions determine subsequent health care use and sick leave. They found that within 6 months, nearly one third of industrial workers with LBP (or neck and upper extremity problems) had a recurrence of sick leave for that same problem and a 40% recurrence of health care use. Work-related factors associated with musculoskeletal symptoms were similar to those associated with health care use and sick leave; but, for LBP, older age and living alone strongly determined whether patients with these problems took any sick leave. The 12- month prevalence of LBP was 52%, and of those with symptoms at baseline, 68% had a recurrence of the LBP. Jarvik and colleagues add depression as an important predictor of new LBP. They found the use of MRI to be a less important predictor of LBP than depression.
What Are the Relevant Outcome Measures?. The Clinical Practice Guidelines formulated by the Canadian Chiropractic Association and the Canadian Federation of Chiropractic Regulatory Boards note that there are a number of outcomes that may be used to demonstrate change as a result of treatment. These should be both reliable and valid. According to the Canadian guidelines, appropriate standards are useful in chiropractic practice because they are able to perform the following:
consistently evaluate the effects of care over time;
help indicate the point of maximum therapeutic improvement;
uncover problems related to care such as noncompliance;
document improvement to the patient, doctor, and third parties;
suggest modifications of the goals of treatment if necessary;
quantify the clinical experience of the doctor;
justify the type, dose, and duration of care;
help provide a database for research; and
assist in establishing standards of treatment of specific conditions.
The broad general classes of outcomes include functional outcomes, patient perception outcomes, physiologic outcomes, general health assessments, and subluxation syndrome outcomes. This chapter addresses only functional and patient perception outcomes assessed by questionnaires and functional outcomes assessed by manual procedures.
Functional Outcomes. These are outcomes that measure the patient’s limitations in going about his or her normal daily activities. What is being looked at is the effect of a condition or disorder on the patient (ie, LBP, for which a specific diagnosis may not be present or possible) and its outcome of care. Many such outcome tools exist. Some of the better known include the following:
Roland Morris Disability Questionnaire,
Oswestry Disability Questionnaire,
Pain Disability Index,
Neck Disability Index,
Waddell Disability Index, and
Million Disability Questionnaire.
These are only some of the existing tools for assessing function.
In the existing RCT literature for LBP, functional outcomes have been shown to be the outcome that demonstrates the greatest change and improvement with SMT. Activities of daily living, along with patient selfreporting of pain, were the 2 most notable outcomes to show such improvement. Other outcomes fared less well, including trunk range of motion (ROM) and straight leg raise.
In the chiropractic literature, the outcome inventories used most frequently for LBP are the Roland Morris Disability Questionnaire and the Oswestry Questionnaire. In a study in 1992, Hsieh found that both tools provided consistent results over the course of his trial, although the results from the 2 questionnaires differed.
Patient Perception Outcomes. Another important set of outcomes involve patient perception of pain and their satisfaction with care. The first involves measuring changes in pain perception over time of its intensity, duration, and frequency. There are a number of valid tools available that can accomplish this, including the following:
Visual analog scale�this is a 10-cm line that has pain descriptions noted at both ends of that line representing no pain to intolerable pain; the patient is asked to mark a point on that line that reflects their perceived pain intensity. There are a number of variants for this outcome, including the Numerical Rating Scale (where the patient provides a number between 0 and 10 to represent the amount of pain they have) and the use of pain levels from 0 to 10 depicted pictorially in boxes, which the patient may check. All of these appear to be equally reliable, but for ease of use, either the standard VAS or Numerical Rating Scale is commonly used.
Pain diary�these may be used to help monitor a variety of different pain variables (for example, frequency, which the VAS cannot measure). Different forms may be used to collect this information, but it is typically completed on a daily basis.
McGill Pain Questionnaire�this scale helps quantify several psychologic components of pain as follows: cognitive-evaluative, motivational-affective, and sensory discriminative. In this instrument, there are 20 categories of words that describe the quality of pain. From the results, 6 different pain variables can be determined.
All of the above instruments have been used at various times to monitor the progress of treatment of back pain with SMT.
Patient satisfaction addresses both the effectiveness of care as well as the method of receiving that care. There are numerous methods of assessing patient satisfaction, and not all of them were designed to be specifically used for LBP or for manipulation. However, Deyo did develop one for use with LBP. His instrument examines the effectiveness of care, information, and caring. There is also the Patient Satisfaction Questionnaire, which assesses 8 separate indices (such as efficacy/outcomes or professional skill, for example). Cherkin noted that the Visit Specific Satisfaction Questionnaire can be used for chiropractic outcome assessment.
Recent work has shown that patient confidence and satisfaction with care are related to outcomes. Seferlis found that patients were more satisfied and felt that they were provided better explanations about their pain from practitioners who used manual therapy. Regardless of treatment, highly satisfied patients at 4 weeks were more likely than less satisfied patients to perceive greater pain improvement throughout 18-month follow-up in a study by Hurwitz et al. Goldstein and Morgenstern found a weak association between treatment confidence in the therapy they received and greater improvement in LBP. A frequent assertion is that benefits observed from application of manipulation methods are a result of physician attention and touching. Studies directly testing this hypothesis were conducted by Hadler et al in patients with acute condition and by Triano et al in patients with subacute and chronic condition. Both studies compared manipulation to a placebo control. In the study of Hadler, the control balanced for provider time attention and frequency, whereas Triano et al also added an education program with home exercise recommendations. In both cases, results demonstrated that although attention given to patients was associated with improvement over time, patients receiving manipulation procedures improved more quickly.
General Health Outcome Measures. This has traditionally been a difficult outcome to effectively measure but a number of more recent instruments are demonstrating that it can be done reliably. The 2 major instruments for doing so are the Sickness Impact Profile and the SF-36. The first assesses dimensions such as mobility, ambulation, rest, work, social interaction, and so on; the second looks primarily at well being, functional status, and overall health, as well as 8 other health concepts, to ultimately determine 8 indices that can be used to determine overall health status. Items here include physical functioning, social functioning, mental health, and others. This tool has been used in many settings and has also been adapted into shorter forms as well.
Physiologic Outcome Measures. The chiropractic profession has a number of physiologic outcomes that are used with regard to the patient care decision-making process. These include such procedures as ROM testing, muscle function testing, palpation, radiography, and other less common procedures (leg length analysis, thermography, and others). This chapter addresses only the physiologic outcomes assessed manually.
Range of Motion. This examination procedure is used by nearly every chiropractor and is used to assess impairment because it is related to spinal function. It is possible to use ROM as a means to monitor improvement in function over time and, therefore, improvement as it relates to the use of SMT. One can assess regional and global lumbar motion, for example, and use that as one marker for improvement.
Range of motion can be measured via a number of different means. One can use standard goniometers, inclinometers, and more sophisticated tools that require the use of specialized equipment and computers. When doing so, it is important to consider the reliability of each individual method. A number of studies have assessed various devices as follows:
Zachman found the use of the rangiometer moderately reliable,
Nansel found that using 5 repeated measures of cervical spine motion with an inclinometer to be reliable,
Liebenson found that the modified Schrober technique, along with inclinometers and flexible spinal rulers had the best support from the literature,
Triano and Schultz found that ROM for the trunk, along with trunk strength ratios and myoelectrical activity, was good indicator for LBP disability, and
a number of studies found that the kinematic measurement of ROM for spinal mobility is reliable.
Muscle Function. Evaluating muscle function may be done using an automated system or by manual means. Although manual muscle testing has been a common diagnostic practice within the chiropractic profession, there are few studies demonstrating clinical reliability for the procedure, and these are not considered to be of high quality.
Automated systems are more reliable and are capable of assessing muscle parameters such as strength, power, endurance, and work, as well as assess different modes of muscle contraction (isotonic, isometric, isokinetic). Hsieh found that a patient-initiated method worked well for specific muscles, and other studies have shown the dynamometer to have good reliability.
Leg Length Inequality. Very few studies of leg length have shown acceptable levels of reliability. The best methods for assessing reliability and validity of leg length involve radiographic means and are therefore subject to exposure to ionizing radiation. Finally, the procedure has not been studied as to validity, making the use of this as an outcome questionable.
Soft Tissue Compliance. Compliance is assessed by both manual and mechanical means, using the hand alone or using a device such as an algometer. By assessing compliance, the chiropractor is looking to assess muscle tone.
Early tests of compliance by Lawson demonstrated good reliability. Fisher found increases in tissue compliance with subjects involved in physical therapy. Waldorf found that prone segmental tissue compliance had good test/retest variation of less than 10%.
Pain tolerance assessed using these means has been found reliable, and Vernon found it was a useful measure in assessing the cervical paraspinal musculature after adjusting. The guidelines group from the Canadian Chiropractic Association and the Canadian Federation of Chiropractic Regulatory Boards concluded that �the assessments are safe and inexpensive and appear to be responsive to conditions and treatments commonly seen in chiropractic practice.�
Conclusion
Existing research evidence regarding the usefulness of spinal adjusting/manipulation/mobilization indicates the following:
As much or more evidence exists for the use of SMT to reduce symptoms and improve function in patients with chronic LBP as for use in acute and subacute LBP.
Use of exercise in conjunction with manipulation is likely to speed and improve outcomes as well as minimize episodic recurrence.
There was less evidence for the use of manipulation for patients with LBP and radiating leg pain, sciatica, or radiculopathy.
Cases with high severity of symptoms may benefit by referral for comanagement of symptomswith medication.
There was little evidence for the use of manipulation for other conditions affecting the low back and very few articles to support a higher rating.
Exercise and reassurance have been shown to be of value primarily in chronic LBP and low back problems associated with radicular symptoms. A number of standardized, validated tools are available to help capture meaningful clinical improvement over the course of low back care. Typically, functional improvement (as opposed to simple reported reduction in pain levels) may be clinically meaningful for monitoring responses to care. The literature reviewed remains relatively limited in predicting responses to care, tailoring specific combinations of intervention regimens (although the combination of manipulation and exercise may be better than exercise alone), or formulating condition-specific recommendations for frequency and�duration of interventions. Table 2 summarizes the recommendations of the team, based on the review of the evidence.
Practical Applications
Evidence exists for the use of spinal manipulation to reduce symptoms and improve function in patients with chronic, acute, and subacute LBP.
Exercise in conjunction with manipulation is likely to speed and improve outcomes and minimize recurrence
In conclusion,�more evidence-based research studies have become available regarding the effectiveness of chiropractic care for low back pain and sciatica. The article also demonstrated that exercise should be used together with chiropractic to help speed up the rehabilitation process and further improve recovery. In most cases, chiropractic care can be used for the management of low back pain and sciatica, without the need for surgical interventions. However, if surgery is required to achieve recovery, a chiropractor may refer the patient to the next best healthcare professional. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Leape, LL, Park, RE, Kahan, JP, and Brook, RH. Group judgments of appropriateness: the effect of panel composition. Qual Assur Health Care. 1992; 4: 151�159
Bigos S, Bowyer O, Braen G, et al. Acute low back problems in adults. Rockville (Md): Agency for Health Care Policy and Research, Public Health Service, U.S. Dept of Health and Human Services; 1994.
National Health and Medical Research Council. A guide to the development, implementation and evaluation of clinical practice guidelines. AusInfo, Canberra, Australia; 1999
McDonald, WP, Durkin, K, and Pfefer, M. How chiropractors think and practice: the survey of North American Chiropractors. Semin Integr Med. 2004; 2: 92�98
Hurwitz, E, Coulter, ID, Adams, A, Genovese, BJ, and Shekelle, P. Use of chiropractic services from 1985 through 1991 in the United States and Canada. Am J Public Health. 1998; 88: 771�776
Coulter, ID, Hurwitz, E, Adams, AH, Genovese, BJ, Hays, R, and Shekelle, P. Patients using chiropractors in North America. Who are they, and why are they in chiropractic care?. Spine. 2002; 27: 291�296
Bronfort, G, Haas, M, Evans, RL, and Bouter, LM. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis. Spine J. 2004; 4: 335�356
Petrie, JC, Grimshaw, JM, and Bryson, A. The Scottish Intercollegiate Guidelines Network Initiative: getting validated guidelines into local practice. Health Bull (Edinb). 1995; 53: 345�348
Cluzeau, FA and Littlejohns, P. Appraising clinical practice guidelines in England and Wales: the development of a methodologic framework and its application to policy. Jt Comm J Qual Improv. 1999; 25: 514�521
Stroup, DF, Berlin, JA, Morton, SC et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000; 283: 2008�2012
Shekelle, P, Morton, S, Maglione, M et al. Ephedra and ephedrine for weight loss and athletic performance enhancement: clinical efficacy and side effects. Evidence Report/Technology Assessment No. 76 [Prepared by Southern California Evidence-based Practice Center, RAND, under contract no. 290-97-0001, Task Order No. 9]. AHRQ Publication No. 03-E022. Agency for Health Care Research and Quality, Rockville (Md); 2003
van Tulder, MW, Koes, BW, and Bouter, LM. Conservative treatment of acute and chronic nonspecific low back pain: a systematic review of randomized controlled trials of the most common interventions. Spine. 1997; 22: 2128�2156
Hagen, KB, Hilde, G, Jamtvedt, G, and Winnem, M. Bed rest for acute low back pain and sciatica (Cochrane Review). in: The Cochrane Library. vol. 2. Update Software, Oxford; 2000
(L�ndesmerter og kiropraktik. Et dansk evidensbaseret kvalitetssikringsprojekt)in: Danish Society of Chiropractic and Clinical Biomechanics (Ed.) Low back pain and Chiropractic. A Danish evidence-based quality assurance project report. 3rd ed.�Danish Society of Chiropractic and Clinical Biomechanics, Denmark; 2006
Hilde, G, Hagen, KB, Jamtvedt, G, and Winnem, M. Advice to stay active as a single treatment for low back pain and sciatica. Cochrane Database Syst Rev. 2002; : CD003632
Waddell, G, Feder, G, and Lewis, M. Systematic reviews of bed rest and advice to stay active for acute low back pain. Br J Gen Pract. 1997; 47: 647�652
Hurwitz, EL, Morgenstern, H, Harber, P et al. Second prize: the effectiveness of physical modalities among patients with low back pain randomized to chiropractic care: findings from the UCLA low back pain study. J Manipulative Physiol Ther. 2002; 25: 10�20
Hsieh, CY, Phillips, RB, Adams, AH, and Pope, MH. Functional outcomes of low back pain: comparison of four treatment groups in a randomized clinical trial. J Manipulative Physiol Ther. 1992; 15: 4�9
Cherkin, DC, Deyo, RA, Battie, M, Street, J, and Barlow, W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for low back pain. N Engl J Med. 1998; 339: 1021�1029
Meade, TW, Dyer, S, Browne, W, Townsend, J, and Frank, AO. Low back pain of mechanical origin: randomized comparison of chiropractic and hospital outpatient treatment. Br Med J. 1990; 300: 1431�1437
Meade, TW, Dyer, S, Browne, W, and Frank, AO. Randomized comparison of chiropractic and hospital outpatient management for low back pain: results from extended follow-up. Br Med J. 1995; 311: 349�351
Seferlis, T, Nemeth, G, Carlsson, AM, and Gillstrom, P. Conservative treatment in patients sick-listed for acute low-back pain: a prospective randomized study with 12 months’ follow up. Eur Spine J. 1998; 7: 461�470
Wand, BM, Bird, C, McAuley, JH, Dore, CJ, MacDowell, M, and De Souza, L. Early intervention for the management of acute low back pain. Spine. 2004; 29: 2350�2356
Hurley, DA, McDonough, SM, Dempster, M, Moore, AP, and Baxter, GD. A randomized clinical trial of manipulative therapy and interferential therapy for acute low back pain. Spine. 2004; 29: 2207�2216
Hadler, NM, Curtis, P, Gillings, DB, and Stinnett, S. A benefit of spinal manipulation as adjunctive therapy for acute low-back pain: a stratified controlled trial. Spine. 1987; 12: 703�706
Hadler, NM, Curtis, P, Gillings, DB, and Stinnett, S. Der nutzen van manipulationen als zusatzliche therapie bei akuten lumbalgien: eine gruppenkontrollierte studie. Man Med. 1990; 28: 2�6
Erhard, RE, Delitto, A, and Cibulka, MT. Relative effectiveness of an extension program and a combined program of manipulation and flexion and extension exercises in patients with acute low back syndromes. Phys Ther. 1994; 174: 1093�1100
Gemmell, H and Jacobson, BH. The immediate effect of Activator vs. Meric adjustment on acute low back pain: a randomized controlled trial. J Manipulative Physiol Ther. 1995; 18: 5453�5456
Waterworth, RF and Hunter, IA. An open study of diflunisal, conservative and manipulative therapy in the management of acute mechanical low back pain. N Z Med J. 1985; 98: 372�375
Blomberg, S, Hallin, G, Grann, K, Berg, E, and Sennerby, U. Manual therapy with steroid injections- a new approach to treatment of low back pain: a controlled multicenter trial with an evaluation by orthopedic surgeons. Spine. 1994; 19: 569�577
Bronfort, G. Chiropractic versus general medical treatment of low back pain: a small scale controlled clinical trial. Am J Chiropr Med. 1989; 2: 145�150
Grunnesjo, MI, Bogefledt, JP, Svardsudd, KF, and Blomberg, SIE. A randomized controlled clinical trial of stay-active care versus manual therapy in addition to stay-active care: functional variables and pain. J Manipulative Physiol Ther. 2004; 27: 431�441
Pope, MH, Phillips, RB, Haugh, LD, Hsieh, CY, MacDonald, L, and Haldeman, S. A prospective, randomized three-week trial of spinal manipulation, transcutaneous muscle stimulation, massage and corset in the treatment of subacute low back pain. Spine. 1994; 19: 2571�2577
Sims-Williams, H, Jayson, MIV, Young, SMS, Baddeley, H, and Collins, E. Controlled trial of mobilization and manipulation for patients with low back pain in general practice. Br Med J. 1978; 1: 1338�1340
Sims-Williams, H, Jayson, MIV, Young, SMS, Baddeley, H, and Collins, E. Controlled trial of mobilization and manipulation for low back pain: hospital patients. Br Med J. 1979; 2: 1318�1320
Skargren, EI, Carlsson, PG, and Oberg, BE. One-year follow-up comparison of the cost and effectiveness of chiropractic and physiotherapy as primary management for back pain: subgroup analysis, recurrent, and additional health care utilization. Spine. 1998; 23: 1875�1884
Andersson, GBJ, Lucente, T, Davis, AM, Kappler, RE, Lipton, JA, and Leurgens, S. A comparison of osteopathic spinal manipulation with standard care for patients with low back pain. N Engl J Med. 1999; 341: 1426�1431
Aure, OF, Nilsen, JH, and Vasseljen, O. Manual therapy and exercise therapy in patients with chronic low back pain: a randomized, controlled trial with 1-year follow-up. Spine. 2003; 28: 525�538
Niemisto, L, Lahtinen-Suopanki, T, Rissanen, P, Lindgren, KA, Sarno, S, and Hurri, H. A randomized trial of combined manipulation, stabilizing exercises, and physical consultation compared to physician consultation alone for chronic low back pain. Spine. 2003; 28: 2185�2191
Koes, BW, Bouter, LM, van Mameren, H, Essers, AHM, Verstegen, GMJR, Hafhuizen, DM, Houben, JP, and Knipschild, P. A blinded randomized clinical trial of manual therapy and physiotherapy for chronic back and neck complaints: physical outcome measures. J Manipulative Physiol Ther. 1992; 15: 16�23
Koes, BW, Bouter, LM, van mameren, H, Essers, AHM, Verstegen, GJMG, Hofhuizen, DM, Houben, JP, and Knipschild, PG. A randomized trial of manual therapy and physiotherapy for persistent back and neck complaints: subgroup analysis and relationship between outcome measures. J Manipulative Physiol Ther. 1993; 16: 211�219
Koes, BM, Bouter, LM, van Mameren, H, Essers, AHM, Verstegen, GMJR, hofhuizen, DM, Houben, JP, and Knipschild, PG. Randomized clinical trial of manipulative therapy and physiotherapy for persistent back and neck complaints: results of a one-year follow-up. Br Med J. 1992; 304: 601�605
Triano, JJ, McGregor, M, Hondras, MA, and Brennan, PC. Manipulative therapy versus education programs in chronic low back pain. Spine. 1995; 20: 948�955
Gibson, T, Grahame, R, Harkness, J, Woo, P, Blagrave, P, and Hills, R. Controlled comparison of short-wave diathermy treatment with osteopathic treatment in non-specific low back pain. Lancet. 1985; 1: 1258�1261
Koes, BW, Bouter, LM, van Mameren, H, Essers, AHM, Verstegen, GMJR, Hofhuizen, DM, Houben, JP, and Knipschild, PG. The effectiveness of manual therapy, physiotherapy, and treatment by the general practitioner for nonspecific back and neck complaints: a randomized clinical trial. Spine. 1992; 17: 28�35
Hemilla, HM, Keinanen-Kiukaanniemi, S, Levoska, S, and Puska, P. Long-term effectiveness of bone-setting, light exercise therapy, and physiotherapy for prolonged back pain: a randomized controlled trial. J Manipulative Physiol Ther. 2002; 25: 99�104
Hemilla, HM, Keinanen-Kiukaanniemi, S, Levoska, S, and Puska, P. Does folk medicine work? A randomized clinical trial on patients with prolonged back pain. Arch Phys Med Rehabil. 1997; 78: 571�577
Coxhead, CE, Inskip, H, Meade, TW, North, WR, and Troup, JD. Multicentre trial of physiotherapy in the management of sciatic symptoms. Lancet. 1981; 1: 1065�1068
Herzog, W, Conway, PJ, and Willcox, BJ. Effects of different treatment modalities on gait symmetry and clinical measurements for sacroiliac joint patients. J Manipulative Physiol Ther. 1991; 14: 104�109
Brealey, S, Burton, K, Coulton, S et al. UK Back Pain Exercise and Manipulation (UK BEAM) trial�national randomized trial of physical treatments for back pain in primary care: objectives, design and interventions [ISRCTN32683578]. BMC Health Serv Res. 2003; 3: 16
Lewis, JS, Hewitt, JS, Billington, L, Cole, S, Byng, J, and Karayiannis, S. A randomized clinical trial comparing two physiotherapy interventions for chronic low back pain. Spine. 2005; 30: 711�721
Cote, P, Mior, SA, and Vernon, H. The short-term effect of a spinal manipulation on pain/pressure threshold is patients with chronic mechanical low back pain. J Manipulative Physiol Ther. 1994; 17: 364�368
Waagen, GN, Haldeman, S, Cook, G, Lopez, D, and DeBoer, KF. Short term of chiropractic adjustments for the relief of chronic low back pain. Manual Med. 1986; 2: 63�67
Kinalski, R, Kuwik, W, and Pietrzak, D. The comparison of the results of manual therapy versus physiotherapy methods used in treatment of patients with low back pain syndromes. J Man Med. 1989; 4: 44�46
Harrison, DE, Cailliet, R, Betz, JW, Harrison, DD, Colloca, CJ, Hasas, JW, Janik, TJ, and Holland, B. A non-randomized clinical control trial of Harrison mirror image methods (lateral translations of the thoracic cage) in patients with chronic low back pain. Eur Spine J. 2005; 14: 155�162
Descarreaux, M, Normand, MC, Laurencelle, L, and Dugas, C. Evaluation of a specific home exercise program for low back pain. J Manipulative Physiol Ther. 2002; 25: 497�503
Burton, AK, Tillotson, KM, and Cleary, J. Single-blind randomized controlled trial of hemonucelolysis and manipulation in the treatment of symptomatic lumbar disc herniation. Eur Spine J. 2000; 9: 202�207
Giles, LGF and Muller, R. Chronic spinal pain syndromes: a clinical pilot trial comparing acupuncture, a nonsteroidal anti-inflammatory drug, and spinal manipulation. J Manipulative Physiol Ther. 1999; 22: 376�381
Timm, KE. A randomized-control study of active and passive treatments for chronic low back pain following L5 laminectomy. J Orthop Sports Phys Ther. 1994; 20: 276�286
Siehl, D, Olson, DR, Ross, HE, and Rockwood, EE. Manipulation of the lumbar spine under general anesthesia: evaluation by electromyography and clinical-neurologic examination of its use for lumbar nerve root compression syndrome. J Am Osteopath Assoc. 1971; 70: 433�438
Santilli, V, Beghi, E, and Finucci, S. Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. ([Epub 2006 Feb 3])Spine J. 2006; 6: 131�137
Nwuga, VCB. Relative therapeutic efficacy of vertebral manipulation and conventional treatment in back pain management. Am J Phys Med. 1982; 61: 273�278
Hayden, JA, van Tulder, MW, and Tomlinson, G. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann Intern Med. 2005; 142: 776�785
Butler, RJ, Johnson, WG, and Baldwin, ML. Measuring success in managing work-disability. Why return to work doesn’t work. Ind Labor Relat Rev. 1995; : 1�24
Schiotzz-Christensen, B, Nielsen, GL, Hansen, VK, Schodt, T, Sorenson, HT, and Oleson, F. Long-term prognosis of acute low back pain in patients seen in general practice: a 1-year prospective follow-up study. Fam Pract. 1999; 16: 223�232
Chavannes, AW, Gubbles, J, Post, D, Rutten, G, and Thomas, S. Acute low back pain: patients’ perception of pain after initial diagnosis and treatment in general practice. J R Coll Gen Pract. 1986; 36: 271�273
Hestbaek, L, Leboeuf-Yde, C, and Manniche, C. Low back pain: what is the long-term course? A review of studies of general patient populations. Eur Spine J. 2003; 12: 149�165
Croft, PR, MacFarlane, GJ, Papageorgiou, AC, Thomas, E, and Silman, AJ. Outcome of low back pain in general practice: a prospective study. Br Med J. 1998; 316: 1356�1359
Haas, M, Goldberg, B, Aickin, M, Ganger, B, and Attwood, M. A practice-based study of patients with acute and chronic low back pain attending primary care and chiropractic physicians: two-week to 48-month follow-up. J Manipulative Physiol Ther. 2004; 27: 160�169
Spitzer, WO, LeBlanc, FE, and Dupuis, M. Scientific approach to the assessment and management of activity-related spinal disorders: a monograph for physicians: report of the Quebec Task Force on Spinal Disorders. Spine. 1987; 12: S1�S59
Jarvik, C, Hollingworth, W, Martin, B et al. Rapid magnetic resonance imaging vs. radiographs for patients with low back pain: a randomized controlled trial. JAMA. 2003; 289: 2810�2818
Henderson, D, Chapman-Smith, DA, Mior, S, and Vernon, H. Clinical Guidelines for Chiropractic Practice in Canada. Canadian Chiropractic Association, Toronto (ON); 1994
Hsieh, C, Phillips, R, Adams, A, and Pope, M. Functional outcomes of low back pain: comparison of four treatment groups in a randomized controlled trial. J Manipulative Physiol Ther. 1992; 15: 4�9
Deyo, RA, Walsh, NE, Martin, DC, Schoenfeld, LS, and Ramamurthy, S. A controlled trial of transcutaneous electrical nerve stimulation (TENS) and exercise for chronic low back pain. N Engl J Med. 1990; 322: 1627�1634
Elnaggar, IM, Nordin, M, Sheikhzadeh, A, Parnianpour, M, and Kahanovitz, N. Effects of spinal flexion and extension exercises on low-back pain and spinal mobility in chronic mechanical low-back pain patients. Spine. 1991; 16: 967�97299
Hurwitz, EL, Morgenstern, H, Kominski, GF, Yu, F, and Chiang, LM. A randomized trial of chiropractic and medical care for patients with low back pain: eighteen-month follow-up outcomes from the UCLA low back pain study. Spine. 2006; 31: 611�621
Goldstein, MS, Morgenstern, H, Hurwitz, EL, and Yu, F. The impact of treatment confidence on pain and related disability among patients with low-back pain: results from the University of California, Los Angeles, low-back pain study. Spine J. 2002; 2: 391�399
Zachman, A, Traina, A, Keating, JC, Bolles, S, and Braun-Porter, L. Interexaminer reliability and concurrent validity of two instruments for the measurement of cervical ranges of motion. J Manipulative Physiol Ther. 1989; 12: 205�210
Triano, J and Schultz, A. Correlation of objective measures of trunk motion and muscle function with low-back disability ratings. Spine. 1987; 12: 561�565
Nicholas, J, Sapega, A, Kraus, H, and Webb, J. Factors influencing manual muscle tests in physical therapy. The magnitude and duration of force applied. J Bone Joint Surg Am. 1987; 60: 186�190
Waldorf, T, Devlin, L, and Nansel, D. The comparative assessment of paraspinal tissue compliance on asymptomatic female and male subjects in both prone and standing positions. J Manipulative Physiol Ther. 1991; 4: 457�461
Ohrbach, R and Gale, E. Pressure pain threshold in normal muscles: reliability, measurement effects, and topographic differences. Pain. 1989; 37: 257�263
Vernon, H. Applying research-based assessments of pain and loss of function to the issue of developing standards of care in chiropractic. Chiropr Technique. 1990; 2: 121�126
Even though chiropractic excels in wellness care, it is becoming more common for people to visit chiropractors to treat a variety of different kinds of pain. Because of this, chiropractic adjustments provide many benefits to people and patients who suffer from a wide variety of conditions like arthritis. In today�s article, we�ll explore how chiropractic can help patients who suffer from arthritis and give you additional suggestions on how to alleviate the pain that�s associated with it.
Arthritis: What a Chiropractor Does
A Doctor of Chiropractic, also known as a chiropractor, is a health professional that focuses primarily on wellness care instead of sickness care. Their specialty focuses on adjusting the spine to correct misalignments that may be impinging on nerves.
Regular visits to a chiropractor can not only restore health throughout the body but also help alleviate back pain and other symptoms associated with an improperly aligned spinal column. They can also work with their patients to plan exercise routines and alterations in diet to assist management of inflammation and pain. Most insurance carriers cover visits to a chiropractor on at least some level.
What Is Arthritis?
Put simply, arthritis is inflammation in the joints which result in joint pain, stiffness and limited range of movement. There are over 200 different varieties of the ailment. While it is generally associated with age, it can also affect young people. It can strike almost any area of the body, with each region having a different cause and name. In some cases, can cause damage to soft tissues and muscles, like the heart and lungs.
Osteoarthritis, also called degenerative joint disease, is the most common type of arthritis. It results from repeated trauma to the joint and becomes more common in the elderly.
Other common forms of include:
Rheumatoid arthritis, the second most common form in which the body�s immune system attacks the joint.
Psoriatic arthritis, another autoimmune form.
Ankylosing spondylitis, also a type where the body attacks itself.
Septic arthritis, which is caused by a viral or bacterial infection of the joint.
Diagnosis
Diagnosing arthritis involves a complete and thorough examination. If a chiropractor feels the need to co-manage the case, a medical work-up by a rheumatologist may be recommended. This can include radiology (x-ray) or an MRI, urine and blood analysis and physical examinations.
It is important to have your condition properly diagnosed so you can more effectively treat the symptoms of the disease.
Chiropractors and Arthritis
The most common treatment for arthritis is medication, which can take down the inflammation and swelling and reduce pain. However, chiropractors can be of great help in managing arthritis. While medications work, it has long-term health risks such as impairing healing, damage to the stomach lining and internal bleeding.
By visiting a chiropractor you may be able to reduce your reliance upon these medications while managing your pain and symptoms naturally. A chiropractor can:
Improve your range of motion by keeping your spine in line
Improve endurance and flexibility
Increase your strength and muscle tone
Help you develop a dietary and nutritional plan to reduce inflammation naturally
In addition, chiropractors can recommend an exercise regimen that�s conducive to arthritis. According to the American Chiropractic Association, this is a vital component in managing your arthritis symptoms.
Treating the Symptoms
Please understand that chiropractors cannot cure arthritis. At this time, there is no cure for this ailment. They can, however, help to alleviate the symptoms and slow the progression of the illness. They may use spinal adjustments in conjunction with other treatments to address the disease. These options can include:
Hot and cold therapy
Ultrasound treatments
Massage
Electronic muscle stimulation
Physical rehabilitation
Magnet therapy
The Best Results
With an inflammatory disease like arthritis, the best results are achieved from attacking it at all angles. This means working with your chiropractor and rheumatologist to combine treatments, if necessary. In addition to their care, a healthy diet and active exercise regime will help move you in the right direction toward a healthier outcome.
If you or a loved one are suffering with, don�t hesitate to give us a call today.�We�re here to help in any way we can!
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Remember how your mom always said, “Nothing in life is free”? Well, she was right. High-tech gadgets and smart phones advancing at the speed of light are a modern convenience unlike little else, but the advantages of communication at our fingertips come with a price: text neck.
Here are 5 things chiropractic patients ought to know about text neck, the epidemic that is taking the world by storm:
1. Text neck is caused by poor posture.
Specifically, habitually looking down at a phone or laptop puts extra pounds of unwanted pressure on the cervical spine, causing wear and tear and even degeneration over time. Additionally, in the space between the neck and shoulder is a cluster of nerves. If these nerves are compressed, misaligned, or damaged, the pain is excruciating and difficult to treat.
In short: Text neck puts the head, neck, and spine at risk.
2. Text neck is increasingly common among young people.
Spending as little as two to four hours a day hunched over a smart phone is enough to make a serious impact on the body over time. And though two to four hours may not seem like a long time, it isn’t hard to arrive at two hours by adding several 15-minute or half-hour segments together.
For teenagers, specifically, two to four hours on a smart phone is not unfathomable. Some teens likely spend twice that much time in a given afternoon or the space between classes or over lunch. Consider the impact of 1500+ hours of bad posture in a year. It is no surprise that teenagers are at risk.
The lasting impact of text neck on today’s young people could be costly.
3. Text neck in combination with a sedentary lifestyle is a recipe for disaster.
With hours of looking down at a smart phone often come hours of relaxing on the couch or sitting still. Generally speaking, we aren’t prone to be active when we are engaged in surfing the Internet or texting our friends.
Though the list of ailments for poor posture is long and discouraging, it is made worse by sluggishness or inactivity. The best thing to do is to put the phone down on occasion, stretch, exercise, and return to the technology only once in a while.
The benefits of technology do not outweigh the consequences of inactivity.
4. Text neck can be corrected.
Practicing good posture is the easiest place to start. Making an appointment with a chiropractor is a good move for anyone who is facing the painful side effects of hours spent looking down.
Taking small steps toward better posture can save money and pain in the long run. Choosing to engage in technology as a treat instead of around the clock is a good practice for anyone who wants to live a long and healthy life.
5. Text neck can be avoided.
To be clear: No one is asking anyone to stop using cell phones. Text neck can be avoided without going 1980 on cell phone usage. But avoiding extra pressure on the neck and spine does require forethought and follow-through.
In today’s ever-increasing technological age, choosing to dodge smart phone usage doesn’t happen accidentally. One good strategy is to look with the eyes instead of moving the neck. Another strategy is to ask friends and family to say something when they notice prolonged periods of poor posture.
In short, text neck is nothing to LOL about. Take it seriously and make any necessary changes before text neck gets the best of you. Let us know how we can help by giving us a call today.
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine