Can physical therapy with instrument-assisted soft tissue mobilization or IASTM improve mobility, flexibility, and health for individuals with musculoskeletal injuries or illnesses?
Instrument Assisted Soft Tissue Mobilization
Instrument-assisted soft tissue mobilization or IASTM is also known as the Graston technique. It is a myofascial release and massage technique used in physical therapy where the therapist uses metal or plastic tools to improve soft tissue mobility in the body. The ergonomically shaped tool is gently or vigorously scraped and rubbed across the injured or painful area. The rubbing is used to locate and release tightness in the fascia/collagen covering the muscles and the tendons. This helps reduce pain and improve movement.
Individuals often develop tissue tightness or restrictions in the muscles and fascia after an injury. These soft tissue restrictions can limit the range of motion – ROM and can trigger pain symptoms. (Kim J, Sung DJ, Lee J. 2017)
History
The Graston technique of instrument-assisted soft tissue mobilization was developed by an athlete who created their instruments to treat soft tissue injuries. The practice has grown with input from medical experts, trainers, researchers, and clinicians.
Physical therapists use different types of tools to perform IASTM.
These massage instruments comprise various types for specific massage and release.
The Graston company designs some of the tools.
Other companies have their version of metal or plastic scraping and rubbing tools.
The objective is to help release soft tissue and myofascial restrictions to improve body movement. (Kim J, Sung DJ, Lee J. 2017)
How It Works
The theory is that scraping the tissues causes microtrauma to the affected area, activating the body’s natural inflammatory response. (Kim J, Sung DJ, Lee J. 2017)
The body activates to reabsorb the tightened or scar tissue, causing the restriction.
The therapist can then stretch the adhesions to alleviate pain and improve mobility.
Treatment
Certain conditions respond well to instrument-assisted soft tissue mobilization, including (Kim J, Sung DJ, Lee J. 2017)
Limited mobility
Decreased muscle recruitment
Loss of range of motion – ROM
Pain with movement
Excessive scar tissue formation
Augmented soft tissue mobilization or ASTM techniques can treat certain injuries and medical conditions that include:
A review compared hands-on myofascial release to instrument myofascial release for chronic low back pain. (Williams M. 2017)
Little difference was found between the two techniques for pain relief.
Another review compared IASTM to other methods for treating pain and function loss. (Matthew Lambert et al., 2017)
The researchers concluded that IASTM could positively affect blood circulation and tissue flexibility and reduce pain.
Another study examined the use of IASTM, pseudo-fake ultrasound therapy, and spinal manipulation for patients with thoracic/upper back pain. (Amy L. Crothers et al., 2016)
All groups improved over time with no significant negative events.
The researchers concluded that instrument-assisted soft tissue mobilization is no more or less effective than spinal manipulation or pseudo-ultrasound therapy for thoracic back pain.
Every case is different, and musculoskeletal conditions respond differently to various treatments. For any questions or concerns, contact your primary healthcare provider to determine if IASTM is an appropriate treatment that can help.
From Injury To Recovery
References
Kamali, F., Panahi, F., Ebrahimi, S., & Abbasi, L. (2014). Comparison between massage and routine physical therapy in women with sub acute and chronic nonspecific low back pain. Journal of back and musculoskeletal rehabilitation, 27(4), 475–480. https://doi.org/10.3233/BMR-140468
Kim, J., Sung, D. J., & Lee, J. (2017). Therapeutic effectiveness of instrument-assisted soft tissue mobilization for soft tissue injury: mechanisms and practical application. Journal of exercise rehabilitation, 13(1), 12–22. https://doi.org/10.12965/jer.1732824.412
Chughtai, M., Newman, J. M., Sultan, A. A., Samuel, L. T., Rabin, J., Khlopas, A., Bhave, A., & Mont, M. A. (2019). Astym® therapy: a systematic review. Annals of translational medicine, 7(4), 70. https://doi.org/10.21037/atm.2018.11.49
Williams M. (2017). Comparing pain and disability outcomes of instrumental versus hands-on myofascial release in individuals with chronic low back pain: a meta-analysis. Doctoral dissertation, California State University, Fresno. https://repository.library.fresnostate.edu/bitstream/handle/10211.3/192491/Williams_csu_6050D_10390.pdf?sequence=1
Matthew Lambert, Rebecca Hitchcock, Kelly Lavallee, Eric Hayford, Russ Morazzini, Amber Wallace, Dakota Conroy & Josh Cleland (2017) The effects of instrument-assisted soft tissue mobilization compared to other interventions on pain and function: a systematic review, Physical Therapy Reviews, 22:1-2, 76-85, DOI: 10.1080/10833196.2017.1304184
Crothers, A. L., French, S. D., Hebert, J. J., & Walker, B. F. (2016). Spinal manipulative therapy, Graston technique® and placebo for non-specific thoracic spine pain: a randomised controlled trial. Chiropractic & manual therapies, 24, 16. https://doi.org/10.1186/s12998-016-0096-9
For individuals dealing with ulcerative colitis, can acupuncture treatment benefit those with UC and other GI-related issues?
Acupuncture For Ulcerative Colitis
Acupuncture has been used to treat symptoms related to pain and inflammation. Studies suggest it may help reduce inflammation and symptoms like diarrhea and abdominal pain, which could benefit individuals with inflammatory bowel disease. Individuals with ulcerative colitis, an inflammatory bowel disease/IBD affecting the large intestine, may find acupuncture beneficial in managing symptoms, including pain and gastrointestinal symptoms. (Crohn’s and Colitis Foundation, 2019)
The pathways connecting the acupoints generate energy, which contributes to overall health.
A disruption to the energy flow can cause injury, illness, or disease.
When acupuncture needles are inserted, energy flow and health are improved.
Benefits
Acupuncture can be used for the relief of various conditions. Studies have shown that acupuncture can reduce inflammation and disease activity in individuals with an IBD, like UC and Crohn’s disease. It can help with: (Gengqing Song et al., 2019)
Pain symptoms
Gut microbiome imbalances
Gut motor dysfunction
Intestinal barrier function
Anxiety
Depression
Studies suggest the use of acupuncture with heat, known as moxibustion, can improve several GI symptoms including (Crohn’s and Colitis Foundation, 2019)
Studies found the use of acupuncture along with moxibustion reduced inflammation in individuals with Crohn’s disease and ulcerative colitis. (Crohn’s and Colitis Foundation, 2019)
Stress and Mood
Chronic conditions like ulcerative colitis can cause feelings of depression and/or anxiety. Acupuncture may be used to address symptoms related to stress and mood and can benefit emotional health issues that include: (Johns Hopkins Medicine. 2024)
Insomnia
Anxiety
Nervousness
Depression
Neurosis – mental health condition characterized by chronic distress and anxiety.
Side Effects
Acupuncture is considered a safe practice. The most common side effects are: (GI Society. 2024)
Needle shock is rare but more common in individuals:
Who are regularly nervous.
Who are nervous around needles.
Who are new to acupuncture.
Who have a history of fainting.
Who are extremely fatigued.
Who have low blood sugar.
For some, GI symptoms may worsen before they improve. It is recommended to try at least five sessions as this is part of the healing process. (Cleveland Clinic. 2023) However, individuals should contact their doctor if symptoms become severe or last more than two days. (GI Society. 2024) Individuals considering acupuncture to help manage symptoms of ulcerative colitis should speak with their healthcare provider to help determine the appropriate treatment and where to start.
Gastro-Intestinal Dysfunction Treatment
References
Crohn’s and Colitis Foundation. (2019). Acupuncture in Inflammatory Bowel Disease. IBDVisible Blog. https://www.crohnscolitisfoundation.org/blog/acupuncture-inflammatory-bowel-disease
Wilkinson J, Faleiro R. (2007). Acupuncture in pain management. Continuing Education in Anaesthesia, Critical Care and Pain. 7(4), 135-138. https://doi.org/10.1093/bjaceaccp/mkm021
Song, G., Fiocchi, C., & Achkar, J. P. (2019). Acupuncture in Inflammatory Bowel Disease. Inflammatory bowel diseases, 25(7), 1129–1139. https://doi.org/10.1093/ibd/izy371
Harvard Medical School. (2016). Relieving pain with acupuncture. Harvard Health Blog. https://www.health.harvard.edu/healthbeat/relieving-pain-with-acupuncture
Arthritis Foundation. (N.D.). Acupuncture for Arthritis. Health Wellness. https://www.arthritis.org/health-wellness/treatment/complementary-therapies/natural-therapies/acupuncture-for-arthritis
Harvard Medical School. (2023). Acupuncture: what is it? Harvard Health Publishing Harvard Medical School Blog. https://www.health.harvard.edu/a_to_z/acupuncture-a-to-z#:~:text=The%20most%20common%20side%20effects,injury%20to%20an%20internal%20organ.
Cleveland Clinic. (2023). Acupuncture. Health Library. https://my.clevelandclinic.org/health/treatments/4767-acupuncture
GI Society. (2024). Acupuncture and Digestion. badgut.org. https://badgut.org/information-centre/a-z-digestive-topics/acupuncture-and-digestion/
“Can understanding moderate exercise and how to measure the amount of exercise help expedite individuals’ health goals and well-being?”
Moderate Exercise
Various physical activity guidelines recommend regular, moderate exercise for achieving and maintaining health and wellness. Getting the minimum, moderate weekly physical activity can help prevent disease, increase mental well-being, support weight loss and maintenance, and improve quality of life.
Moderate-intensity cardiovascular exercise includes – brisk walking, yard work, mopping, vacuuming, and playing various sports that require consistent movement.
When engaged in moderate exercise, individuals should breathe harder but still be able to carry a conversation. (American Heart Association, 2024)
The talk test is a way to monitor whether the exercise is at moderate intensity.
A heart rate chart or calculator can determine an individual’s maximum heart rate.
To measure heart rate mid-exercise, individuals can take their pulse or use a heart rate monitor, app, fitness tracker, or smartwatch to ensure they stay at a moderate intensity.
MET
M.E.T. stands for Metabolic Equivalent for Task and refers to the amount of oxygen the body uses during physical activity.
Assigning METs to an activity allows individuals to compare the amount of exertion an activity takes.
This works for individuals with different weights.
During moderate physical activity, breathing and heart rate increase, and the body burns around 3.5 to 7 calories a minute.
The actual number burned depends on your weight and fitness level.
The body uses 1 MET for basic functions like breathing.
Grades of activity:
1 MET – Body at rest
2 METs – Light activity
3-6 METs – Moderate activity
7 or more METs – Vigorous activity
Perceived Exertion Scale
Individuals can also check their activity level using the Borg Rating of Perceived Exertion scale/RPE. (Centers for Disease Control and Prevention, 2022) Using this scale involves monitoring how an individual feels about how hard their body is working during physical activity. The scale starts at 6 and ends at 20. A perceived exertion between 11 and 14 is considered moderate physical activity.
6 – No exertion – sitting still or sleeping
7-8 – Extremely light exertion
9-10 – Very light exertion
11-12 – Light exertion
13-14 – Somewhat hard exertion
15-16 – Heavy exertion
17-18 – Very heavy exertion
20 – Maximum exertion
Examples
Many activities are counted as moderate-intensity exercise. Choose some appealing and learn to add them to a weekly routine.
Ballroom dancing
Line dancing
Gardening
House chores that get the heart pumping.
Softball
Baseball
Volleyball
Doubles tennis
Brisk walking
Light jogging
Walking or jogging on a treadmill
Using an elliptical trainer
Bicycling under 10 miles an hour on ground level
Leisurely swim
Water aerobics
Mobility Challenges
Individuals with mobility issues can achieve moderate intensity using a manual wheelchair or a handcycle and swimming or water aerobics.
Individuals who can use their legs but can’t tolerate walking or jogging can try bicycling or swimming.
Getting More Exercise
There are different ways to incorporate and increase moderate physical activities. These include:
10-minute Activity Bursts
Walk briskly for at least 10 minutes at a time.
Walk at an easy pace for a couple of minutes.
Pick up the pace for 10 minutes.
Try to walk during work breaks or lunch and/or before or after work.
Walking Workouts
Individuals can walk indoors, outdoors, or on a treadmill.
Proper posture and walking techniques make it easier to achieve a brisk pace.
Once comfortable walking briskly for 10 minutes, begin to extend walking time.
Try different walking workouts that offer fast walks, jogging intervals, and/or adding hills or treadmill inclines.
New Activities
Individuals are recommended to experiment with various exercises to find what works for them.
Consider roller skating, blading, or skateboarding to increase heart rate.
Moderate physical activity will get and keep the body in shape. Individuals should not become distressed if they can only do a little at first. Allow time to build endurance and gradually make time each day for enjoyable physical activities.
Transform Your Body
References
U.S. Department of Health & Human Services. (2018). Physical Activity Guidelines for Americans, 2nd edition. Retrieved from https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf
American Heart Association. (2024). American Heart Association recommendations for physical activity in adults and kids. (Healthy Living, Issue. https://www.heart.org/en/healthy-living/fitness/fitness-basics/aha-recs-for-physical-activity-in-adults
Centers for Disease Control and Prevention. (2022). Target heart rate and estimated maximum heart rate. Retrieved from https://www.cdc.gov/physicalactivity/basics/measuring/heartrate.htm
Centers for Disease Control and Prevention. (2022). Perceived exertion (Borg Rating of Perceived Exertion Scale). Retrieved from https://www.cdc.gov/physicalactivity/basics/measuring/exertion.htm
For individuals experiencing eye problems, can acupuncture treatment help and benefit overall eye health?
Acupuncture For Eye Health
Acupuncture is an alternative medical practice that involves inserting thin needles at specific points on the body. The objective is to restore balance and health by restoring and balancing energy circulation through pathways throughout the body. These pathways, known as meridians, are separate from nerve and blood pathways.
Studies have shown that the insertion of needles manipulates accumulations of certain neurotransmitters by nearby nerves and may be what causes beneficial health effects. (Heming Zhu 2014)
Scientists are not sure exactly how acupuncture works, but it has been shown to provide pain relief and alleviation of cancer treatment nausea. (Weidong Lu, David S. Rosenthal 2013)
Studies have shown that acupuncture can help treat eye conditions like dry eye syndrome. (Tae-Hun Kim et al., 2012)
Eye Problems
For some individuals, a body imbalance can be caused by eye problems or disease. With acupuncture, imbalance-causing symptoms are addressed. Acupuncture promotes the circulation of energy and blood around the eyes.
Acupuncture has been used as an alternative treatment for chronic dry eye syndrome. (Tae-Hun Kim et al., 2012)
Studies have shown acupuncture helps reduce the eye surface’s temperature to reduce the evaporation of tears.
The procedure is also sometimes used to treat glaucoma.
Glaucoma is an optic nerve disease usually caused by above-normal eye pressure levels.
Another study showed successful reduced allergic and inflammatory eye disease symptoms. (Justine R. Smith et al., 2004)
Eye Acupoints
The following acupoints are for eye health.
Jingming
Jingming – UB-1 is located in the inner corner of the eye.
This point is thought to increase energy and blood and to help with problems such as blurry vision, cataracts, glaucoma, night blindness, and conjunctivitis. (Tilo Blechschmidt et al., 2017)
Zanzhu
The Zanzhu point – UB-2 is in the crease at the inner end of the eyebrow.
This acupoint is used when individuals complain of headaches, blurred vision, pain, tearing, redness, twitching, and glaucoma. (Gerhard Litscher 2012)
Yuyao
Yuyao is in the middle of the eyebrow, above the pupil.
This point is used for treating eye strain, eyelid twitching, ptosis, or when the upper eyelid droops over, cloudiness of the cornea, redness, and swelling. (Xiao-yan Tao et al., 2008)
Sizhukong
The Sizhukog – SJ 23 area is in the hollow area outside the eyebrow.
It is thought to be a point where acupuncture can help with eye and facial pain, including headaches, redness, pain, blurred vision, toothache, and facial paralysis. (Hongjie Ma et al., 2018)
Tongzilia
The Tongzilia – GB 1 is located on the outside corner of the eye.
The point helps brighten the eyes.
Acupuncture also helps treat headaches, redness, eye pain, light sensitivity, dry eyes, cataracts, and conjunctivitis. (GladGirl 2013)
Early studies with acupuncture have shown promise for improving eye health. Individuals considering acupuncture are recommended to consult their primary healthcare provider to see if it can be an option for those who have not found a resolution by traditional means.
Neck Injuries
References
Zhu H. (2014). Acupoints Initiate the Healing Process. Medical acupuncture, 26(5), 264–270. https://doi.org/10.1089/acu.2014.1057
Lu, W., & Rosenthal, D. S. (2013). Acupuncture for cancer pain and related symptoms. Current pain and headache reports, 17(3), 321. https://doi.org/10.1007/s11916-013-0321-3
Kim, T. H., Kang, J. W., Kim, K. H., Kang, K. W., Shin, M. S., Jung, S. Y., Kim, A. R., Jung, H. J., Choi, J. B., Hong, K. E., Lee, S. D., & Choi, S. M. (2012). Acupuncture for the treatment of dry eye: a multicenter randomised controlled trial with active comparison intervention (artificial teardrops). PloS one, 7(5), e36638. https://doi.org/10.1371/journal.pone.0036638
Law, S. K., & Li, T. (2013). Acupuncture for glaucoma. The Cochrane database of systematic reviews, 5(5), CD006030. https://doi.org/10.1002/14651858.CD006030.pub3
Smith, J. R., Spurrier, N. J., Martin, J. T., & Rosenbaum, J. T. (2004). Prevalent use of complementary and alternative medicine by patients with inflammatory eye disease. Ocular immunology and inflammation, 12(3), 203–214. https://doi.org/10.1080/092739490500200
Blechschmidt, T., Krumsiek, M., & Todorova, M. G. (2017). The Effect of Acupuncture on Visual Function in Patients with Congenital and Acquired Nystagmus. Medicines (Basel, Switzerland), 4(2), 33. https://doi.org/10.3390/medicines4020033
Litscher G. (2012). Integrative laser medicine and high-tech acupuncture at the medical university of graz, austria, europe. Evidence-based complementary and alternative medicine : eCAM, 2012, 103109. https://doi.org/10.1155/2012/103109
Tao, X. Y., Sun, C. X., Yang, J. L., Mao, M., Liao, C. C., Meng, J. G., Fan, W. B., Zhang, Y. F., Ren, X. R., & Yu, H. F. (2008). Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 28(3), 191–193.
Can physical therapy treatment protocols aimed at improving range of motion and flexibility around the hip and relieving inflammation around the sciatic nerve help individuals experiencing deep buttock pain or piriformis syndrome?
Deep Buttock Pain
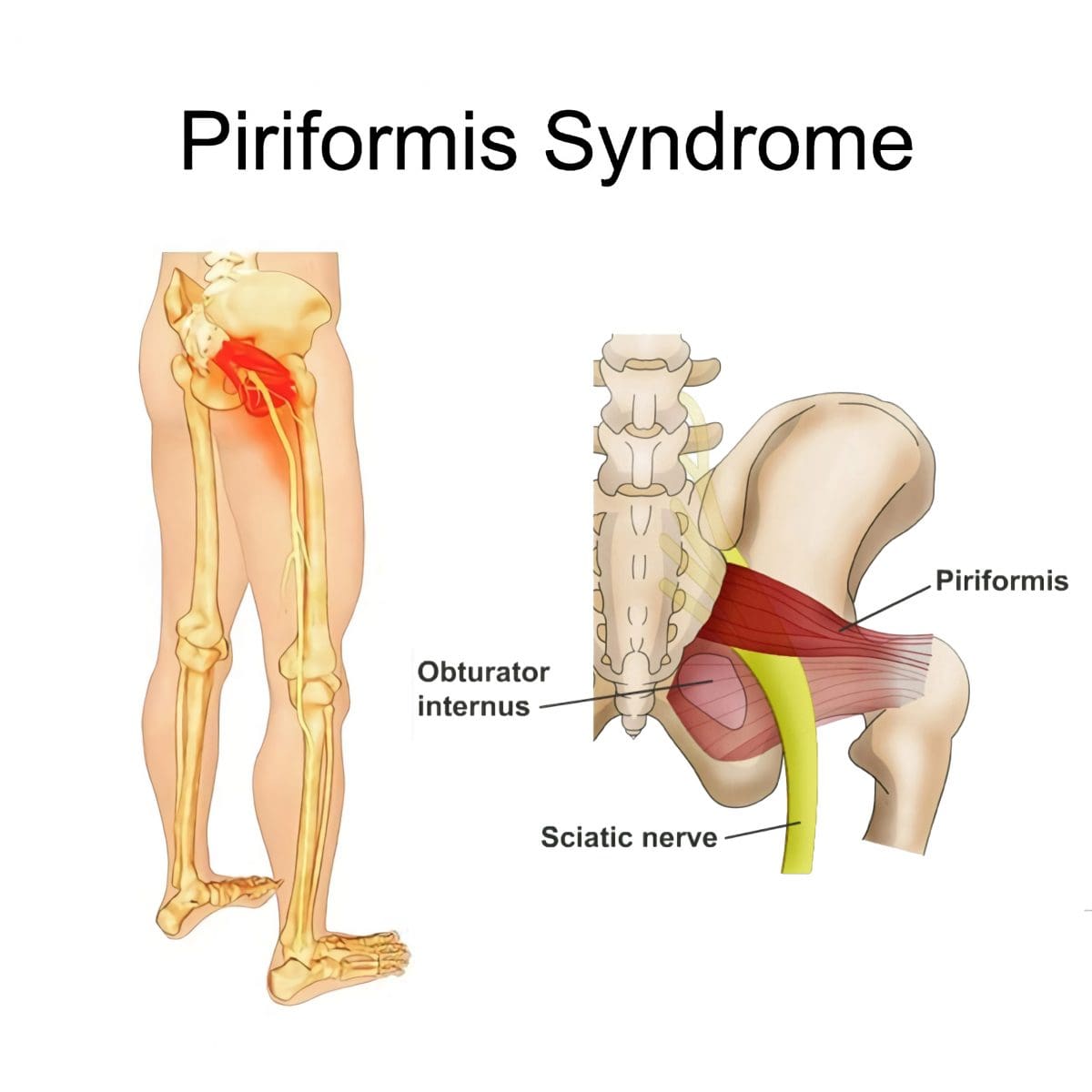
Piriformis syndrome, a.k .a. deep buttock pain, is described as sciatic nerve irritation from the piriformis muscle.
The piriformis is a small muscle behind the hip joint in the buttocks.
It is about one centimeter in diameter and functions in the hip joint’s external rotation or turning outward.
The piriformis muscle and tendon are close to the sciatic nerve, which supplies the lower extremities with motor and sensory functions.
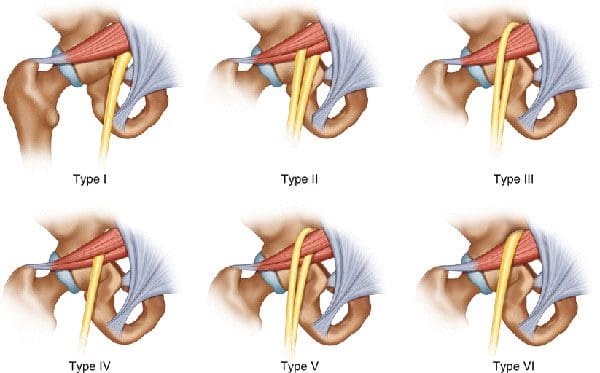
Depending on an individual’s anatomic variation of the muscle and tendon:
The two cross over, under, or through each other behind the hip joint in the deep buttock.
This relationship is thought to irritate the nerve, leading to sciatica symptoms.
Piriformis Syndrome
When diagnosed with piriformis syndrome, it is thought that the muscle and tendon bind to and/or spasm around the nerve, causing irritation and pain symptoms.
The theory supported is that when the piriformis muscle and its tendon tighten, the sciatic nerve becomes compressed or pinched. This decreases blood circulation and irritates the nerve from the pressure. (Shane P. Cass 2015)
Tenderness with pressure on the piriformis muscle.
Discomfort in the back of the thigh.
Deep buttock pain behind the hip.
Electric sensations, shocks, and pains travel down the back of the lower extremity.
Numbness in the lower extremity.
Some individuals develop symptoms abruptly, while others go through a gradual increase.
Diagnosis
Doctors will order X-rays, MRIs, and nerve conduction studies, which is normal.
Because piriformis syndrome can be challenging to diagnose, some individuals with minor hip pain may receive a piriformis syndrome diagnosis even if they don’t have the condition. (Shane P. Cass 2015)
It is sometimes referred to as deep buttock pain. Other causes of this type of pain include back and spinal problems like:
Herniated discs
Spinal stenosis
Radiculopathy – sciatica
Hip bursitis
A piriformis syndrome diagnosis is usually given when these other causes are eliminated.
When the diagnosis is uncertain, an injection is administered in the area of the piriformis muscle. (Danilo Jankovic et al., 2013)
Different medications can be used, but the injection itself is used to help determine the specific location of the discomfort.
When an injection is given into the piriformis muscle or tendon, it is often administered by ultrasound guidance to ensure the needle delivers the medication to the correct location. (Elizabeth A. Bardowski, J. W. Thomas Byrd 2019)
Avoiding activities that cause symptoms for at least a few weeks.
Physical Therapy
Emphasize stretching and strengthening the hip rotator muscles.
Non-Surgical Decompression
Gently pulls the spine to release any compression, allowing optimal rehydration and circulation and taking the pressure off the sciatic nerve.
Therapeutic Massage Techniques
To relax and release muscle tension and increase circulation.
Acupuncture
To help relax the piriformis muscle, sciatic nerve, and surrounding area.
Relieve pain.
Chiropractic Adjustments
Realignment rebalances the spine and musculoskeletal system to alleviate pain.
Anti-Inflammatory Medication
To decrease inflammation around the tendon.
Cortisone Injections
Injections are used to decrease inflammation and swelling.
Botulinum Toxin Injection
Injections of botulinum toxin paralyze the muscle to relieve pain.
Surgery
Surgery can be performed in rare cases to loosen the piriformis tendon, known as a piriformis release. (Shane P. Cass 2015)
Surgery is a last resort when conservative treatments have been tried for at least 6 months with little to no relief.
Recovery can take several months.
Sciatica Causes and Treatment
References
Cass S. P. (2015). Piriformis syndrome: a cause of nondiscogenic sciatica. Current sports medicine reports, 14(1), 41–44. https://doi.org/10.1249/JSR.0000000000000110
Jankovic, D., Peng, P., & van Zundert, A. (2013). Brief review: piriformis syndrome: etiology, diagnosis, and management. Canadian journal of anaesthesia = Journal canadien d’anesthesie, 60(10), 1003–1012. https://doi.org/10.1007/s12630-013-0009-5
Bardowski, E. A., & Byrd, J. W. T. (2019). Piriformis Injection: An Ultrasound-Guided Technique. Arthroscopy techniques, 8(12), e1457–e1461. https://doi.org/10.1016/j.eats.2019.07.033
Can acupuncture treatment help individuals dealing with or experiencing insomnia and sleep issues and/or disorders?
Acupuncture For Insomnia
Acupuncture is a type of holistic medicine that involves inserting sterile, disposable, thin needles at specific points known as acupoints on the body. Each needle is inserted into a different area to stimulate symptom relief of various conditions, like chronic pain and nausea. (Johns Hopkins Medicine. 2024) Recent research has looked into acupuncture for insomnia and found that it may be an effective alternative. (Mingming Zhang et al., 2019)
Insomnia
Insomnia causes individuals to have trouble falling or staying asleep. Individuals who have insomnia tend to wake up earlier than they intend to and find it difficult to impossible to get back to sleep once they are awake. The sleep disorder is quite common, with around 10% of individuals experiencing it at some point. (Andrew D. Krystal et al., 2019)
There are three categories, all characterized by the duration of the disorder. They include: (Andrew D. Krystal et al., 2019)
Acute/Short-Term
Lasting less than three months.
Episodic
Happens once in a while for less than three months.
Chronic
Lasting more than three months.
Health Issues
Insomnia can cause various health issues, and individuals can develop mood changes, irritability, fatigue, and problems with memory, impulse control, and concentration. (Andrew D. Krystal et al., 2019)
Insomnia has also been shown to increase the risk of heart failure, heart attack, and other chronic health conditions. (Mingming Zhang et al., 2019)
Benefits
Studies on the use of acupuncture for insomnia have found that it may improve sleep because of its influence on certain neurotransmitters. One review noted that specific neurotransmitters involved in the sleep-wake cycle are positively affected by acupuncture. (Kaicun Zhao 2013) The neurotransmitters include:
Norepinephrine
Helps with waking up and staying alert.
Melatonin
A hormone that helps the body calm down and prepare for sleep.
Gamma-aminobutyric acid – GABA
Helps the body fall asleep and stay asleep.
However, more research is needed to confirm the benefits of acupuncture for insomnia further.
Conditions
Certain conditions can contribute to insomnia, including:
Mood disorders
Chronic pain
Other sleep disorders
Acupuncture can help lower the effects of these disorders.
Pain
Because of the way acupuncture affects certain chemicals, it is a proven complementary treatment for pain.
The needles enhance chemicals like endorphins, dynorphins, and encephalins.
Acupuncture also releases corticosteroids, which are stress hormones.
Each of these chemicals has a role in pain symptoms.
Studies have found that individuals with anxiety can also benefit from acupuncture to help reduce symptoms. (Meixuan Li et al., 2019)
Sleep Apnea
Sleep apnea is a sleep-breathing disorder that causes an individual to stop breathing during the night temporarily.
The muscles in the nasal cavity, nose, mouth, or throat become overly relaxed.
Acupuncture can help stimulate the muscles and prevent over-relaxation, preventing apneas.
Data suggests that acupuncture may affect the apnea-hypopnea index, the number of times an individual stops and starts breathing during sleep. (Liaoyao Wang et al., 2020)
Session
Individuals should not feel pain and just a small amount of pressure in the needles’ insertion area.
If pain is present, it could be because the needles are not inserted in the right spot.
Bleeding or bruising where the needle was inserted.
Nausea
Fainting
Pins and needles sensation
Feeling more pain treatment
Prior to getting acupuncture, individuals are recommended to speak to their healthcare provider. They can advise on how it can help and any side effects that may occur due to the individual’s health, underlying conditions, and medical history. Once cleared, they can recommend a licensed acupuncturist.
Zhang, M., Zhao, J., Li, X., Chen, X., Xie, J., Meng, L., & Gao, X. (2019). Effectiveness and safety of acupuncture for insomnia: Protocol for a systematic review. Medicine, 98(45), e17842. https://doi.org/10.1097/MD.0000000000017842
Krystal, A. D., Prather, A. A., & Ashbrook, L. H. (2019). The assessment and management of insomnia: an update. World psychiatry: official journal of the World Psychiatric Association (WPA), 18(3), 337–352. https://doi.org/10.1002/wps.20674
Zhao K. (2013). Acupuncture for the treatment of insomnia. International review of neurobiology, 111, 217–234. https://doi.org/10.1016/B978-0-12-411545-3.00011-0
Patil, S., Sen, S., Bral, M., Reddy, S., Bradley, K. K., Cornett, E. M., Fox, C. J., & Kaye, A. D. (2016). The Role of Acupuncture in Pain Management. Current pain and headache reports, 20(4), 22. https://doi.org/10.1007/s11916-016-0552-1
Li, M., Xing, X., Yao, L., Li, X., He, W., Wang, M., Li, H., Wang, X., Xun, Y., Yan, P., Lu, Z., Zhou, B., Yang, X., & Yang, K. (2019). Acupuncture for treatment of anxiety, an overview of systematic reviews. Complementary therapies in medicine, 43, 247–252. https://doi.org/10.1016/j.ctim.2019.02.013
Wang, L., Xu, J., Zhan, Y., & Pei, J. (2020). Acupuncture for Obstructive Sleep Apnea (OSA) in Adults: A Systematic Review and Meta-Analysis. BioMed research international, 2020, 6972327. https://doi.org/10.1155/2020/6972327
Chan, M. W. C., Wu, X. Y., Wu, J. C. Y., Wong, S. Y. S., & Chung, V. C. H. (2017). Safety of Acupuncture: Overview of Systematic Reviews. Scientific reports, 7(1), 3369. https://doi.org/10.1038/s41598-017-03272-0
Ernst, G., Strzyz, H., & Hagmeister, H. (2003). Incidence of adverse effects during acupuncture therapy-a multicentre survey. Complementary therapies in medicine, 11(2), 93–97. https://doi.org/10.1016/s0965-2299(03)00004-9
“For individuals that have difficulty getting plenty of fruits and vegetables, can incorporating green powder supplements increase nutritional levels for a balanced diet?”
Green Powder Supplements
Meeting daily nutrient needs through whole, unprocessed foods can’t always be met when access is limited or for other reasons. A green powder supplement is a great way to fill in the gaps. Green powder supplements are a daily supplement that helps increase vitamin, mineral, and fiber intake and enhances overall health. Green powders are easy to mix in water with a favorite beverage or smoothie or bake into a recipe. They can help:
Increase energy
Nourish the immune system
Improve digestion
Promote mental clarity
Contribute to healthy blood sugar levels
Reduce the risk of chronic disease
Promote optimal liver and kidney function
What Are They?
Green powder supplements are forms of vitamins, minerals, fiber, antioxidants, phytochemicals, and other bioactive compounds.
They are derived from fruits, vegetables, herbs, and algae to combine ingredients into a convenient supplement. (Giulia Lorenzoni et al., 2019)
Nutrients
Because most green powders comprise a combination of ingredients, the nutrient density is high. Green powder supplements can be considered a vitamin and mineral product. They typically contain:
Vitamins A, C, and K
Iron
Magnesium
Calcium
Antioxidants
The recommended daily intake of vitamins and minerals can be helpful for individuals with limited access to produce or who want to supplement their diet with additional nutrients.
Energy
The phytochemicals found in fruits and vegetables have been shown to improve energy levels. Studies on their effects on physical performance and endurance have resulted in positive outcomes. Researchers found that phytonutrients like those in green powders helped to increase energy, improve agility, reduce fatigue perception, improve memory, and decrease recovery time. (Nicolas Monjotin et al., 2022)
Digestive Health
Green powders are rich in soluble and insoluble fiber, which contribute to feeling full and satisfied after a meal and are important for healthy digestion and regular bowel movements. Eating fiber-rich foods is associated with optimal blood sugar control and improved gut microbiota diversity. These factors are important for maintaining a healthy body weight and decreasing the risk of chronic disease, for example, type 2 diabetes. (Thomas M. Barber et al., 2020) Phytochemicals, including flavonoids, have been shown to have therapeutic effects on gas, bloating, constipation, and diarrhea associated with IBS. Other phytonutrients have been shown to reduce certain symptoms of ulcerative colitis. (Nicolas Monjotin et al., 2022)
Immune System Function
Supplemental green powder supplements have shown the ability to maintain a healthy immune system and reduce inflammation by their antioxidant content. Green powders containing seaweed or algae are rich in phytochemical and poly-unsaturated fatty acids that have antioxidant properties to reduce inflammation and prevent oxidative damage to cells. (Agnieszka Jaworowska, Aliza Murtaza 2022) A randomized trial found that a fruit, berry, and vegetable powder concentrate blend decreased oxidation and reduced inflammation, attributed to the phytochemicals found in fruits and vegetables.(Manfred Lamprecht et al., 2013)
Detoxification
The liver and kidneys are the main organs of natural detoxification. The liver helps the body absorb nutrients from consumed foods and removes waste and toxins through the kidneys. (National Library of Medicine. 2016) Plants are packed with antioxidants and phytochemicals that protect the liver and kidneys from free radical damage and oxidative stress. (Yong-Song Guan et al., 2015) The green powder supplements are made from these plants. When drinking green powders, fluid intake naturally increases as a standard serving of green powder is mixed with 8 to 12 ounces of water.
Whether mixed, blended, or made into a shake, powdered greens are a convenient and efficient way to get the daily dose of antioxidants, vitamins, minerals, and other nutrients.
The Healing Diet: Combat Inflammation, Embrace Wellness
References
Lorenzoni, G., Minto, C., Vecchio, M. G., Zec, S., Paolin, I., Lamprecht, M., Mestroni, L., & Gregori, D. (2019). Fruit and Vegetable Concentrate Supplementation and Cardiovascular Health: A Systematic Review from a Public Health Perspective. Journal of clinical medicine, 8(11), 1914. https://doi.org/10.3390/jcm8111914
Monjotin, N., Amiot, M. J., Fleurentin, J., Morel, J. M., & Raynal, S. (2022). Clinical Evidence of the Benefits of Phytonutrients in Human Healthcare. Nutrients, 14(9), 1712. https://doi.org/10.3390/nu14091712
Barber, T. M., Kabisch, S., Pfeiffer, A. F. H., & Weickert, M. O. (2020). The Health Benefits of Dietary Fibre. Nutrients, 12(10), 3209. https://doi.org/10.3390/nu12103209
Jaworowska, A., & Murtaza, A. (2022). Seaweed Derived Lipids Are a Potential Anti-Inflammatory Agent: A Review. International journal of environmental research and public health, 20(1), 730. https://doi.org/10.3390/ijerph20010730
Lamprecht, M., Obermayer, G., Steinbauer, K., Cvirn, G., Hofmann, L., Ledinski, G., Greilberger, J. F., & Hallstroem, S. (2013). Supplementation with a juice powder concentrate and exercise decrease oxidation and inflammation, and improve the microcirculation in obese women: randomised controlled trial data. The British journal of nutrition, 110(9), 1685–1695. https://doi.org/10.1017/S0007114513001001
InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. How does the liver work? 2009 Sep 17 [Updated 2016 Aug 22]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279393/
Guan, Y. S., He, Q., & Ahmad Al-Shatouri, M. (2015). Complementary and Alternative Therapies for Liver Diseases 2014. Evidence-based complementary and alternative medicine : eCAM, 2015, 476431. https://doi.org/10.1155/2015/476431
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine