Zinc may fight liver disease in a way scientists never expected, say Australian researchers who found that zinc naturally inhibits the inflammatory effects of interferon lambda 3 (IFN-λ3), a protein strongly associated with tissue damage in chronic liver disease. IFN-λ3 also decreases antiviral activity and increases viral replication both in vitro and in vivo.
The study’s lead author Dr. Scott Read said the study provides the first evidence that zinc can act as a potent and specific inhibitor of IFN-λ3 in viral infections such as hepatitis C and influenza.
“We have demonstrated that zinc inhibits numerous facets of the liver’s immune response to viruses that may be mediated by IFN-λ3,” Read said.
“Zinc also blocks the inflammatory activity of IFN-λ3, which has been strongly linked to accelerated progression to liver cirrhosis in viral and non-viral liver disease,” Read says.
In an article published in Nature Communications, Read concluded that the study showed zinc’s potential as a simple and effective treatment against acute and chronic liver inflammation.
Other natural substances have been found to be effective against liver disease. A 2016 study conducted at the University of Southampton found that two cups of coffee a day reduced the risk of liver cirrhosis — scarring due to alcohol and viruses like hepatitis C — by 44 percent. The study, which was published in the science journal Alimentary Pharmacology and Therapeutics, also found that coffee cut the risk of dying from cirrhosis by almost half.
Drugs have also been found to be effective against liver disease. The common anti-inflammatory drug called Nasalcrom (cromolyn sodium) that’s used to treat allergies and asthma could prevent liver disease and reduce the need for liver transplants, according to Texas researchers who found that the medication prevents cells from releasing an inflammatory compound called histamine.
More and more people are following a gluten-free diet, but if they have no medical reason to do so they could actually be risking their health, a top expert says.
“The evidence is mounting against any health benefits from a gluten-free diet for those people without a medical reason,” John Douillard tells Newsmax Health.
Gluten is a naturally occurring protein present in cereal grains, especially wheat, which is responsible for the elastic texture of dough.
Traditionally, gluten was considered harmless unless eaten by people with celiac disease, whose digestive systems are unable to handle it.
But recently the idea of eating gluten-free has caught on, and the number of people following such a diet tripled in the five years between 2009 and 2014, while the number of those with celiac disease remained stable, research shows.
On the other hand, a pair of large studies, published in the past few months, has found those people who eat little gluten could be at risk of developing coronary heart disease, as well as diabetes.
Douillard is a chiropractor, certified addiction professional, and the author of “Eat Wheat,” along with six previous health books.
An expert in the field of natural heath, he is also former player development director and nutrition counselor for the New Jersey Nets NBA team. He has also appeared on the Dr. Oz Show, and featured in many national publications.
Here are excerpts from his recent interview with Newsmax Health.
Q: How did you get interested in gluten?
A: People would come to me with digestive problems and I’d tell them to get off wheat and they’d feel better for a short time, but after awhile, their problems would return. The same thing happened with dairy, or nuts. The problem wasn’t actual these specific foods. But, as the medical profession started making medical recommendations to get off of wheat, people began treating it like a poison.
Q: Who should not eat gluten?
A: People with celiac disease shouldn’t eat wheat, but that’s only about 1 percent to 3 percent of the population. There also may be those that don’t have celiac disease, but say they are sensitive to it, so they may be right to avoid it. But that’s an estimated 2 percent to 13 percent of the population. This leaves a third of the population that eliminated gluten from their diet under the misperception it is unhealthy. They are the ones missing out on the benefits of wheat.
Q: How did the idea that gluten is bad catch on?
A: Originally, people with celiac disease were told to avoid gluten but the idea caught on that it was good for other people as well, and now gluten-free has become a buzzword and it’s grown into a $16 billion industry. They’re even put “gluten free” on foods that never had any gluten in them, like yogurt.
Q: What’s the problem with gluten?
A: People who promulgate a gluten-free diet contend we aren’t genetically capable of eating gluten but that’s wrong. The University of Utah did a study that found evidence of wheat and barley in the teeth of ancient humans 3 ½ million years ago. The Paleo diet says to avoid grains, but if you talk to anthropologists, you’ll find out there’s nothing Paleo about this. Ancient humans gathered wheat berries to fuel them for the whole day. Most experts agree we didn’t start cooking out own meat until 500,000 years ago, so we had wheat in our teeth millions of years before that.
Q: What are the gluten-free people missing out on?
A: In addition to new studies that show wheat may lower diabetes and heart disease risk, wheat is a natural probiotic, and people who don’t eat it have less good microbes in their microbiome and more bad ones. They also are more likely to have weaker immune systems, because research finds eating the indigestible part of wheat helps to strengthen to strengthen it. In addition, people who follow the MIND Diet and the Mediterranean diet, both which permit whole grains, reduce their risk of Alzheimer’s disease.
Q: If it’s not gluten, what is the problem with the way we eat?
A: The problem is our reliance on processed foods. One study showed that our reliance on processed food increases metabolic syndrome (the condition that hikes heart disease and diabetes risk) by 141 percent. On the other hand, eating whole gains and whole wheat reduced it by 38 percent. So it’s processed foods we need to eliminate from our diet.
Here are Douillard’s 5 tips to digest gluten more easily:
1. Choose bread with only these ingredients: Organic whole wheat, water, salt, and an organic starter.
2. Sprouted soaked breads typically found in the refrigerator section are much easier to digest.
3. Avoid any bread or any packaged foods with cooked or heated vegetable oils. These are preservatives and indigestible.
4. Think seasonal eating. Eat more grains in the fall when they are harvested and less in the spring and summer.
5. Start your day with a beet, apple, and celery drink to amp up your digestive strength and spice your food with spices such as: ginger, cumin, coriander, fennel, and cardamon.
Individuals with persistent low back pain can choose from a variety of proven nonsurgical treatments, including: medications, physical therapy, and exercise, to name a few. A 2017 study discussed another therapy for chronic low back pain and sciatica: massage.
In a first-of-its-kind study, researchers used a real world� strategy that was � compared to running the study in a managed setting.
More than 50 percent of the research participants reported, �clinically purposeful development� in their low back pain after their massage therapy plan, composed co-first authors William G. Elder, PhD, Family and Community Medicine at the University of Kentucky, and Niki Munk, PhD, LMT, School of Health and Rehabilitation Sciences at Indiana University-Purdue University Indianapolis.
�Clinical massage therapy appears to be effective for low back pain, and patients should discuss with their provider and consider clinical massage therapy before attempting highly debatable opioid drugs,� says Dr. Elder, who was the lead researcher of the study.
A Closer Look in the Study
The research team collaborated with primary care providers in Kentucky who referred patients for 10 massage sessions with licensed massage therapists in the community over a 12-week interval. The massage therapists crafted exceptional massage therapy recommendations on the foundation of the specific patient�s requirements.
The participants were measured before they began their massage program, in the close of the 12-week program, then at 24 weeks after the onset of system. At 12 weeks, 54.1 percent shown clinically significant development in their long-term low back pain. At 24 weeks, their development was kept by 75 percent of patients who demonstrated improvement at 12 weeks.
Some crucial insights related to drug regimen, and patients� age, weight were found by the researchers: Adults age 50 and over were more prone to possess significant progress inside their particular long-term low back pain as an outcome of massage therapy. The advantage didn�t hold, although heavy patients had great results from massage.
Patients who reported taking opioid pain drugs did report reduced pain as a result of the massage treatment, but they were two times not likely to have clinically significant change in comparison to patients not taking opioids.
While Dr. Munk, who is a licensed massage therapist, says she expected the patients to have favorable results from the course of massage treatment, some facets of the study results surprised her.
�I was a bit surprised the baby boomer generation was more likely to have better results,� Dr. Munk says.
Dr. Munk hypothesizes that old people may have a distinct perspective on pain tolerance. Since elderly individuals likely have had more time including every one of the state she also wonders if folks that are older might be more accustomed to living with pain and had heightened perceptions of pain alleviation.
Massage Drawbacks and Expectations
While the study suggests that massage could offer individuals with chronic low back pain with pain relief that is purposeful, it truly is not a fast repair. Dr. Munk says people should level-confirm their expectations by taking into consideration how long they�ve lived with their state when they go to their first massage.
�If you�ve had a state for 10-15 years, the chance that a one-hour session will fix it is probably not realistic,� Dr. Munk says.
Dr. Munk notes that massage, given its foundation as a muscle treatment, should be viewed as a care therapy�not a short term strategy.
The body goes back to routines its used to and has, and also �Muscle patterns grow to be retrained she says. � you also must take another dose for alleviation, and Like a pill that wears off after a couple of hours, it could take several sessions to get the job to �hold.��
Another consideration patients must understand is the cost of massage, as the treatment isn’t covered by most health insurance plans. Investing in massage is an individual decision that requires weighing pros and cons. If massage therapy can help you manage your chronic back pain without the significance of spinal column surgery or other treatments which can be more significant, you might find it’s worth the out of pocket price.
Tips on Making Massage Effective
In case your doctor recommends massage therapy, building a trusting and comfortable therapeutic relationship is significant. Request your doctor if he or she recommend a massage therapist in the locality.
Dr. Elder and Dr. Munk additionally propose asking the following questions to any prospective massage therapist before your first session:
Have you ever been a licensed massage therapist?
What kind of training and education have you ever received?
How long are you now practicing?
Would you work with other healthcare professionals?
Have you had further education in other illness-specific areas (like back and neck pain)?
Do you remain current on any specific medical conditions you focus on and improvement in the massage therapy field?
Persistent low back pain can take a crucial cost on your own own life. By good fortune, many nonsurgical treatments can help you manage the pain. The results with this particular study suggest massage is a legitimate decision to lessen pain while you could possibly believe massage is only a relaxing indulgence. Request your doctor if massage is a treatment worth investigating for the specified state.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Lower Back Pain After Auto Injury
After being involved in an automobile accident, neck injuries and aggravated conditions, such as whiplash, are some of the most commonly reported types of injuries, due to the force of the impact. A study discovered, however, that the seat of a vehicle can often lead to injuries as well, causing lower back pain and other symptoms. Lower back pain is also among one of the most common types of automobile accident injuries in the U.S. alone.
With the competitive season looming, chiropractor Dr. Alexander Jimenez�gives insights & examines the current best thinking on vaccination for athletes, and makes recommendations for sports clinicians.
Without doubt, vaccination is one of the greatest triumphs of modern medicine. Many serious diseases that used to routinely maim or kill large numbers of people are no longer a threat. More than that, vaccination can prevent outbreaks of less serious illness, which although not life threatening, are still unpleasant, leading to missed time from work and school.
Anyone with young children or who has travelled extensively abroad will (hopefully) understand that a programme of vaccination is either required or recommended. When it comes to the travelling athlete however, the situation is rather more complex. While the basic vaccinations (eg typhoid, hepatitis etc when travelling to certain regions of the tropics) are of course still required, clinicians will also want to ensure that their athletes stay as well as possible to compete at their full potential. A mild illness that is an inconvenience to a tourist may be a disaster for an athlete focusing on the peak of his/her season!
Sports clinicians may therefore wish to consider extra vaccinations to minimise the risk of more minor conditions. However, this approach raises a whole new set of issues. For example, which additional vaccinations may be use for athletes who regularly travel abroad? What are the possible side effects of these extra vaccinations and how should vaccines be timed to maximise immunity during the competition, while minimising disruption to training in the run up to competition?
Athletes Are Different
There exists some uncertainty about the most appropriate vaccination regimens in athletes among team doctors and other physicians because general public health vaccination guidelines cannot be easily transferred to elite athletes. Complicating factors include the typical circumstances of athletes� daily life, such as frequent travelling to foreign countries or close contact with teammates and opponents, which might indicate the need for a modification of recommended vaccination schedules. In addition, intense physical activity of training and competition with its possible effects on the immune function can affect decisions about execution and timing of vaccination.
Other complicating factors are that vaccination recommendations are formulated around a public health policy rather than for specific individuals and are likely to change over time(1-3). Also, there�s the issue of cost effectiveness; the majority of vaccines that are not generally recommended are not recommended because the medical benefit is not regarded sufficiently balanced with the costs if implemented across the whole population. This is despite the fact that they may be potentially beneficial in specific individuals(4,5). It�s also important to understand that generalised recommendations take no account of the implications of the effects of illness in athletes, which can be far more profound and far reaching than in the general public (see Box 1).
Further reasons as to why athletes are different when it comes to vaccination include the following:
Athletes are often in close contact with opponents and teammates, which increases the risk of transmission of many diseases, particularly respiratory- transmitted diseases(9,10). Typically, a contact of less than 1-2 metres distance is necessary to transmit diseases such as influenza or other respiratory- transmissible agents such as varicella(11,12).
For blood-borne diseases, the transmission risk due to sport is less pronounced but athletes are still at higher risk than the general population(13,14).
Even healthy non-vaccinated athletes being exposed to an infectious agent (eg contact with a diseased individual) may have to be excluded from training and competition for medical reasons. Usually, such an exclusion has to last for the complete incubation period of a disease, which may be up to three weeks.
Putting all these factors together, the recommendation is that elite, competitive athletes should be vaccinated more aggressively than the general public(15).
Which Vaccinations?
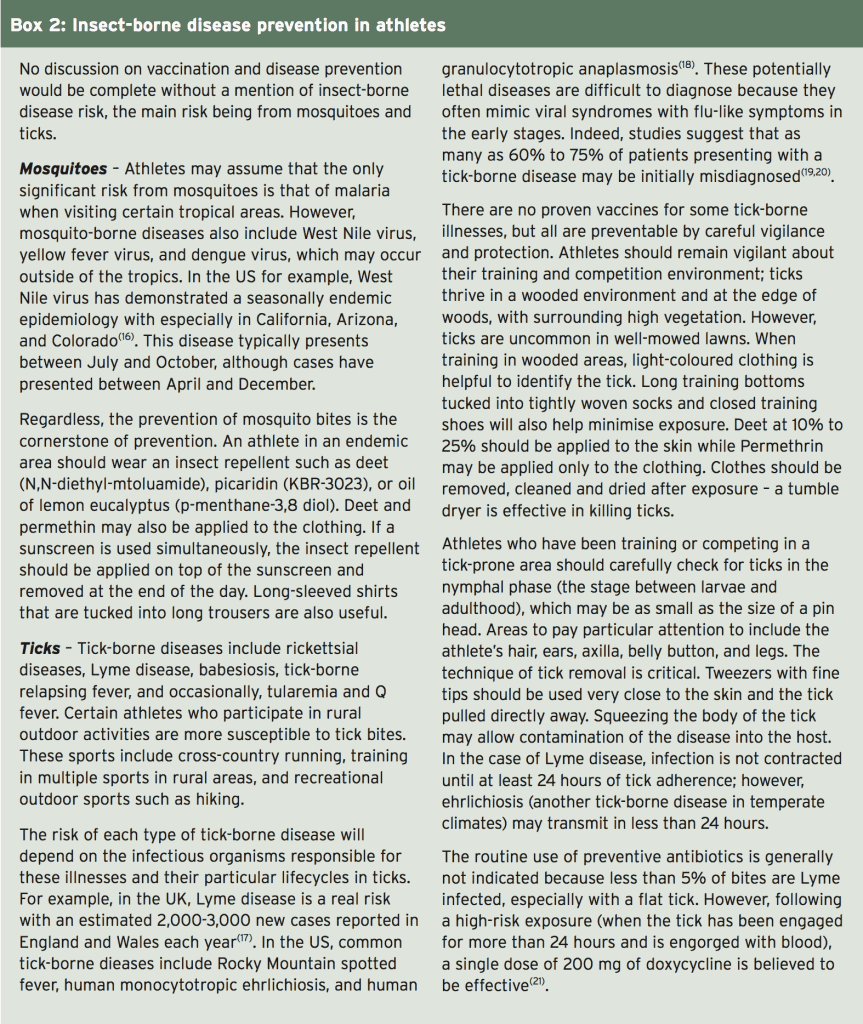
The decision as to which vaccinations are given prior to foreign travel will depend on a number of factors, including the travel�destination(s), the nature of the sport and the health/vaccination history of the individual involved. Regardless of these factors however, it is recommended that ALL adult athletes are routinely vaccinated against the following:
4. Influenza
5. Hepatitis A and B
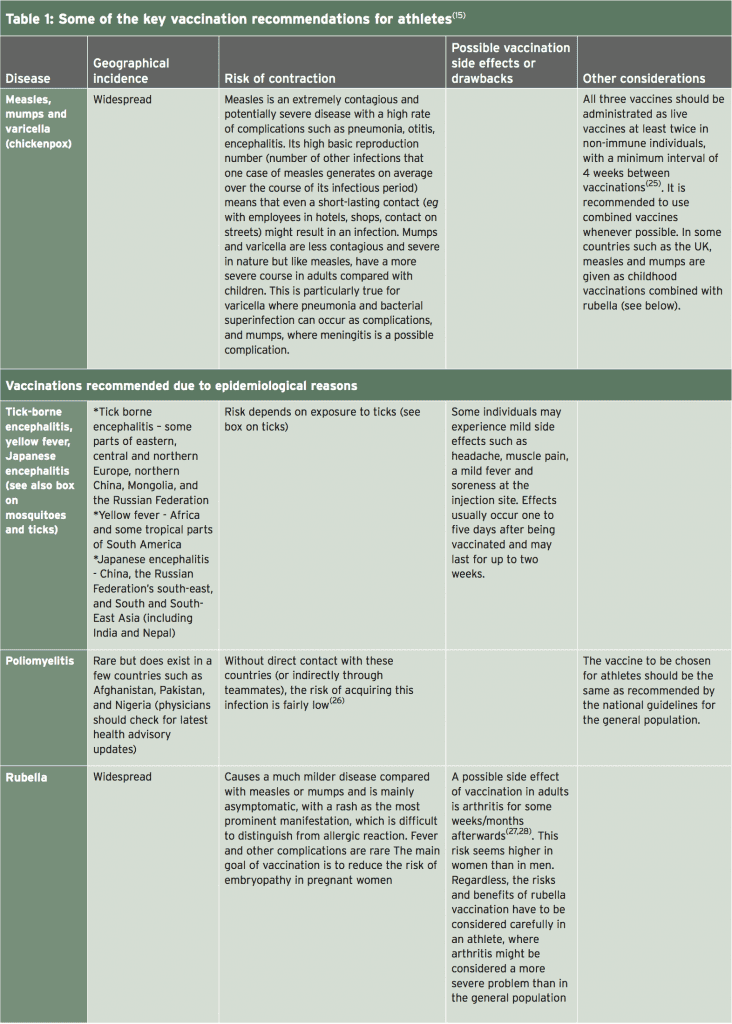
6. Measles, mumps and varicella (if immunity is not already proven by a natural infection)
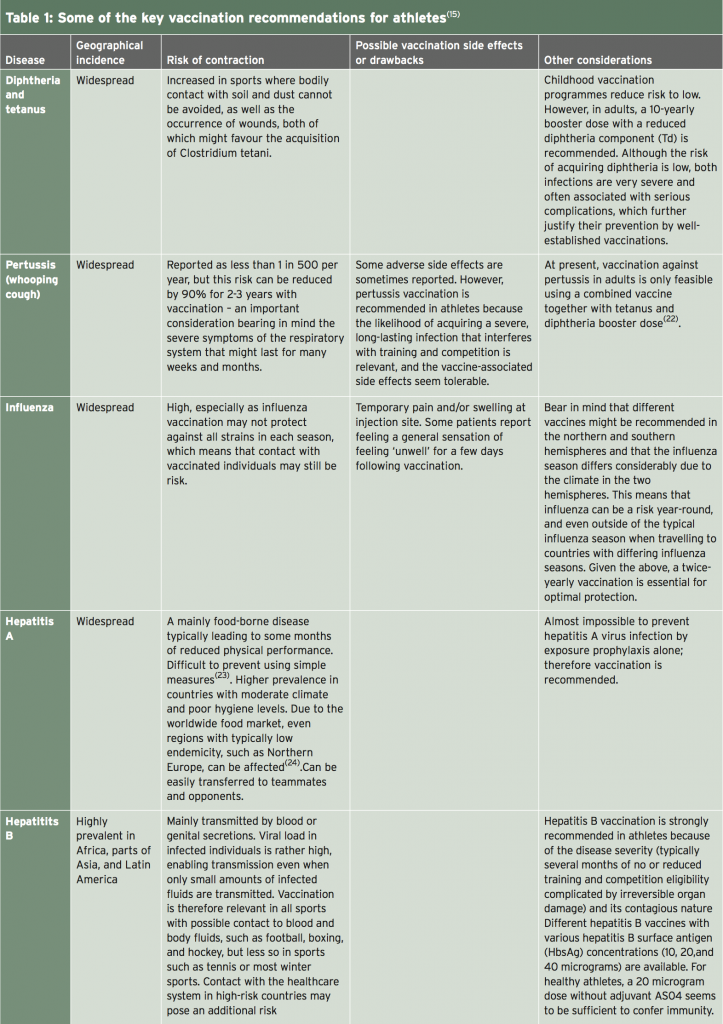
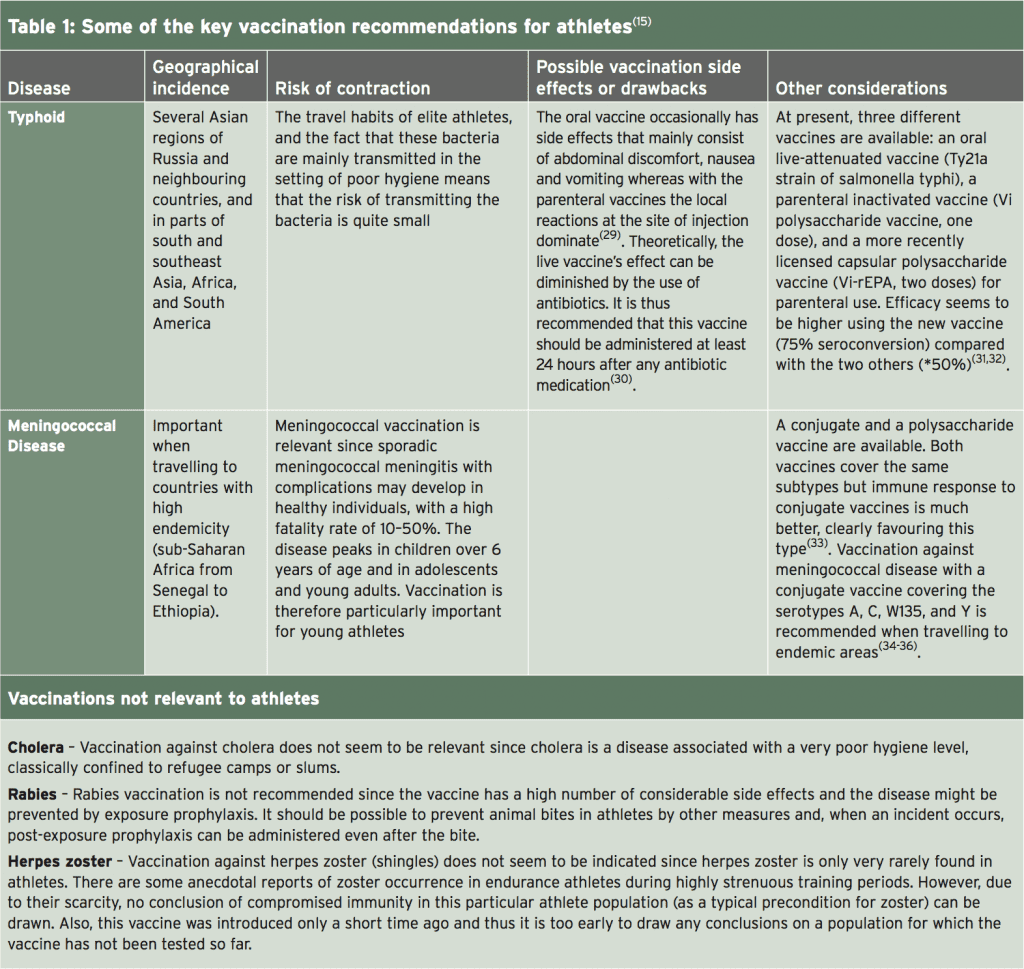
Of these, numbers 1-5 should be given as inactivated vaccines while measles, mumps and varicella (chickenpox) should be given as live vaccines(15). A full discussion on the detailed considerations regarding each and every possible vaccination is beyond the scope of this article (readers are directed to a full and recent review of this topic by Luke and D�Hemecourt(15)). However, Table 1 summarises most of the key recommendations.
Vaccination Timing
Timing of vaccinations should be chosen in order to minimise interference with training and competition, and to ensure the immune reaction is not temporarily impaired. Inactivated vaccines generally cause side effects within two days following vaccination. This is in contrast to live vaccinations where the peak of side effects is most likely to occur after 10-14 days when replication of the vaccines is at a maximum. Unless a vaccination needs to be administered urgently, the best time therefore for vaccination is at the onset of resting periods � for example at the beginning of the winter off season.
When a vaccination has to be carried out within a training and/or competition period (eg influenza), there is no major medical problem with training undertaken shortly before or after vaccination. However, it is recommended to vaccinate shortly after a competition in order to make the period of time to the next competition as long as possible. Many vaccinations given via injection can cause local pain and inflammation at the injection site. Clinicians may therefore wish to time vaccine administration so as to not coincide with delayed onset muscle soreness (DOMS) following strenuous exercise.
Vaccination Techniques
Dependent on the injection site, some sport- specific impairments may result (for example buttock pain in runners following a gluteal injection). Obviously, it is advisable to use the non-dominant side for injections in unilateral disciplines such as racquet sports. For vaccines that can be administered using either the intramuscular or the subcutaneous route, the intramuscular option seems to be preferable as it yields higher titer rate (more antibody production) and a lower risk of granuloma.
Injection into the deltoid muscle is preferred if possible, although other muscle sites are possible. Regardless, it is important that the athlete is sitting or lying, and the muscle is completely relaxed. Studies indicate that the use of longer needles (25 mm) and a fast speed of injection/ withdrawal of the needle (1-2 seconds) are associated with less pain(37). Also, an angle of injection of 90 degrees may also help reduce pain in intramuscular injections.
Syncopes or collapses following vaccination are uncommon but may occur; some studies on influenza vaccination suggest the frequency of syncope in younger athletes to be around 1%(38). However, the syncope itself may be less important than secondary injuries caused by the collapse such as skull fracture and cerebral haemorrhage. Given that the majority of syncopes (80 %) occur within 15 min of vaccine administration, it is recommended that athletes are observed for a period of 15-30 minutes following vaccination. This recommendation may be particularly important for endurance athletes because there are indications that, in these athletes, vasovagally-induced syncopes are more frequent(39).
Vaccination Schedule
The recommended vaccination schedules for disease prevention will be dependent on the previous vaccination record and disease history of the athlete in question. Also, some schedules are dependent of the type/brand of vaccines used and recommendations may also differ according to public health policy in each country. Readers are directed to the summary given by Luke and D�Hemecour(15); there are also some excellent downloadable resources on the US Centre for Disease Control and Prevention (CDC) � https://www.cdc.gov/vaccines/ schedules/hcp/adult.html.
Summary
The vaccination requirements for elite athletes are not the same as that for the general public. Not only are these athletes�potentially exposed to more disease pathogens as a result of international travel, even the mildest episode of illness that would be barely noticeable to most of us can be devastating for elite athletic performance. For these reasons, sports clinicians and doctors should take a much more aggressive approach to vaccination of their athletes. Together with steps to reduce exposure and the correct vaccination techniques and timing, clinicians can maximise the potential of their athletes to perform at all times of year across all regions of the globe.
References
1. World Health Organization. WHO vaccinepreventable
diseases: monitoring system. 2012
global summary 2013. http://www.who.int/
immunization_monitoring/data/data_subject/
en/index.html accessed 5th Feb 2017
2. Sta�ndige Impfkommission (STIKO).
Empfehlungen der Sta�ndigen Impfkommission
(STIKO) am Robert Koch-Institut. Epi Bull.
2012;283�10
3. Centers for Disease Control and Prevention.
General recommendations on immunization�
recommendations of the Advisory Committee
on Immunization Practices (ACIP). MMWR
Recomm Rep. 2011;60:1�64
4. Vaccine. 2013;31:6046�9
5. Pharmacoeconomics. 2005;23:855�74
6. J Exp Med. 1970;131:1121�36
7. Am Heart J. 1989;117:1298�302
8. Eur J Epidemiol. 1989;5:348�50
9. Clin J Sport Med. 2011;21:67�70
10. Sports Med. 1997;24:1�7
11. J Infect Dis. 2013;207:1037�46
12. Lancet. 1990;336:1315
13. Br J Sports Med. 2004;38:678�84
14. Clin Sports Med. 2007;26:425�31.
15. Sports Med 2014; 44:1361�1376
16. Vector Borne Zoonotic Dis 2004;4(1):61�70
17. http://www.nhs.uk/Conditions/Lymedisease/Pages/Introduction.aspx#symptoms accessed Feb 2017
18. J Infect Dis 1999;180(3):900�3
19. Ann N Y Acad Sci 2003;990: 295�30
20. J Infect Dis 1984;150(4):480�8
21. N Engl J Med 2001;345(2):79�84
22. Pediatrics. 2013;131:e1716�22.
23. Euro Surveill. 2005;10(6):E050609.2
24. Euro Surveill. 2013;18(7):20467
25. Centers for Disease Control and
Prevention. Epidemiology and prevention of
vaccine-preventable diseases. The pink
book:course textbook. 12th ed.; 2012.
26. World Health Organisation. Poliomyelitis;
2014. http://www.who.int/topics/poliomyelitis/en/
27. Clin Exp Rheumatol. 2001;19:724�6
28. JAMA. 1997;278:551�6
29. Clin Infect Dis. 2004;38:771�9
30. Travel Med. 1998;5:14�7
31. Cochrane Database Syst Rev.
2014;1:CD001261
32. Curr Opin Infect Dis. 2012;25:489�99
33. Drugs. 2013;73:1147�55
34. Hum Vaccin Immunother. 2014;10:995�1007
35. Popul Health Metr. 2013;11:17.
36. Vaccine. 2009;27(Suppl 2):B51�63
37. Arch Dis Child. 2007;92:1105�8
38. Vaccine. 2013;31:6107�12
39. Prog Cardiovasc Dis. 2012;54:438�44
Ohio Attorney General Mike DeWine is suing five makers of opioid painkillers for their role in the state’s opioid epidemic.
The five companies named in the suit are Purdue Pharma, Johnson & Johnson, Teva Pharmaceuticals, Endo Health Solutions and Allergan.
This is the second suit of its kind brought by a state, after Mississippi.
Ohio attorney general sues 5 pharma companies over their role in the opioid epidemic��
Ohio Attorney General Mike DeWine is suing five makers of opioid painkillers for their role in the state’s opioid epidemic.
The suit, which DeWine said is the second by a U.S. state, after Mississippi, claims the drugmakers violated multiple state laws, including the Ohio Corrupt Practices Act, and committed Medicaid fraud.
Purdue Pharma, Johnson & Johnson and its Janssen Pharmaceuticals unit, Teva Pharmaceuticals and its Cephalon unit, Endo Health Solutions and Allergan are all named in the suit.
“In 2014 alone, pharmaceutical companies spent $168 million through sales reps peddling prescription opioids to win over doctors with smooth pitches and glossy brochures that downplayed the risks” of the medicines,” DeWine said at a press conference Wednesday. Last year, he said, 2.3 million people in Ohio, or about a fifth of the state’s population, were prescribed opioids.
In a statement, a spokesman for Purdue Pharma, which manufactures OxyContin, said the company shares the attorney general’s concerns about the opioid crisis and that it is “committed to working collaboratively to find solutions.”
“OxyContin accounts for less than 2% of the opioid analgesic prescription market nationally, but we are an industry leader in the development of abuse-deterrent technology, advocating for the use of prescription drug monitoring programs and supporting access to Naloxone � all important components for combating the opioid crisis,” he said.
Allergan declined to comment, as did a Teva spokeswoman, who said, “We have not completed review of the complaint.”
J&J’s Janssen unit said the company believed the allegations in the lawsuit were “both legally and factually unfounded.”
“Janssen has acted appropriately, responsibly and in the best interests of patients regarding our opioid pain medications, which are FDA-approved and carry FDA-mandated warnings about the known risks of the medications on every product label,” said Jessica Castles Smith, a Janssen spokeswoman.
Endo officials weren’t immediately available to comment.
The Ohio action follows suits from counties and cities seeking to hold accountable the industry that produces, markets and distributes opioid painkillers. DeWine said the Ohio suit, filed Wednesday morning in Ross County, “would compel these companies to clean up this mess through several remedies,” including an injunction to stop “continued deception and misrepresentation in marketing,” damages paid to the state for money spent on the crisis, and repayment to consumers.
Sales of prescribed opioids � including oxycodone, hydrocodone and methadone � almost quadrupled in the U.S. between 1999 and 2015, according to the Centers for Disease Control and Prevention, contributing to a more than quadrupling of deaths from prescription opioids in that same period. Almost 2 million Americans either abused or were dependent on prescription opioid painkillers in 2014, according to the CDC.
“We understand what we’re taking on: five huge drug companies,” DeWine told reporters Wednesday. “I don’t want to look back 10 years from now and say we should have had the guts to file. � It’s something we have to do.”
Scoliosis is a well-known spinal condition which results in an abnormal, often lateral, curvature of the spine. While most cases of the issue are reported among children and teens, adults can also experience scoliosis, later in their lives. Fortunately, non-surgical procedures, such as the Schroth method of exercises for scoliosis, were created to correct this spinal condition, improving the lives of many affected with scoliosis.
Katharina Schroth (1894-1985) developed the Schroth Method, based on her personal experience with spinal issues as a teenager. When Katharina was told she had scoliosis and would require surgery the system originated. Unwilling to possess surgery, she instantly began to formulate a way to place scoliosis in check plus it became her life�s work. She dedicated countless hours attempting different corrections of her curve and detected certain positions, movements and breathing techniques which made her own torso deformity clear.
Trained as a teacher, Ms. Schroth began sharing her techniques with patients in the 1920’s and finally created her own clinic in Germany. The Schroth Approach was established in Germany in 1921, by Katharina Schroth. This curve design particular scoliosis technique was refined through the years by the creator�s daughter, physical therapist Christa Lehnert-Schroth PT, and grandson and orthopedic doctor, Dr. Hans-Rudolf Weiss, at the inpatient practice bearing the name of Katharina Schroth set in Germany�s Rhineland. Her daughter, Christa Lehnert-Schroth P.T. immensely helped her further develop the theory underlying the Schroth Method. Katharina�s grandson, Dr. Hans-Rudolph Weiss, MD has continued the tradition by developing his own unique program called Scoliologic in Germany.
The Schroth Method Today
The Schroth Method continues to be practiced in Germany since then, and it is only in the last few years that the Schroth Method has spread all around the world as wait and scoliosis patients search for options to observe , bracing, and surgery for scoliosis treatment. The Schroth family has authored publications, created numerous posts, and taught others on these nonsurgical techniques. Although possessed by the Schroth family today, over one thousand patients are treated annually at Asklepios Katharina-Schroth Klinic in Germany and there’s frequently a several month long waiting list.
Clinical research shows that the approach can reduce spinal curvatures. Surely, the success also depends upon the commitment of the patients. Schroth exercises could be broadly divided into two types. They are the old in patient Schroth Intensive Rehabilitation along with the more recent outpatient Schroth Best Practice. The latter essentially consists of exercises to enhance corrective exercises the sagittal spinal curves and adoption of appropriate corrective bearings during daily actions.
The physiologic exercises aim at preserving the natural lumbar lordosis in sitting and standing positions.
Corrective exercises are scoliosis special exercises. They differ together with the curvature sorts. Rotational breathing is incorporated to the treatment, to improve the vertebral rotation.
Although there are many other popular forms of treatments available for scoliosis, including surgical interventions, the Schroth method has been recognized by many healthcare professionals and researchers due to their effectiveness in treating the spinal condition in children, teens and even adults. Be sure to consult a qualified and experienced healthcare specialist regarding the best treatment method for scoliosis and/or seek a doctor/physician who has knowledge on the specific exercises of the Schroth method for scoliosis treatment.
Schroth Method Exercises for Scoliosis
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Lower Back Pain After Auto Injury
After being involved in an automobile accident, neck injuries and aggravated conditions, such as whiplash, are some of the most commonly reported types of injuries, due to the force of the impact. A study discovered, however, that the seat of a vehicle can often lead to injuries as well, causing lower back pain and other symptoms. Lower back pain is also among one of the most common types of automobile accident injuries in the U.S. alone.
Gabrielle Union has never been shy about sharing her secrets to a bangin� bod. The 44-year-old actress loves posting snippets of her grueling workouts to Instagram, and on Wednesday morning, she treated us to an Insta�story of her favorite�go-to exercise regimen.
This 7-move circuit routine�especially targets the star�s shoulders and back�so she�ll look extra fit for backless gowns on the red carpet this summer. Union has previously chronicled her quest to �build a booty,� as she put it, so her trainer threw in�a few glute-toning moves too.
Think you can handle Union�s workout? We say bring it on. But trust us,�you�ll definitely be feeling the burn once you finish.
Rope Shoulder Pulls
Union captioned this image �25 reps of rope shoulder pulls =�sexy shoulders,� and we can see why. It�ll seriously work your shoulders and upper back. Stand with your legs slightly bent and back straight. Hold a cable rope in both hands and pull toward your chest. Push the rope back in, then�repeat. (Union did 25 reps.)
Dumbbell Front Raise
Stand with your legs shoulder-width apart and knees slightly bent. Hold a dumbbell in each hand, palms facing in. Raise your arms straight in front of you and lower once they�re at shoulder level. Make sure your arms don�t go above 90 degrees. Repeat.
TRX Squats with Thigh Band
The caption says this is Union�s warm up,�but to us it looks like the main event. Stand with your feet shoulder-width apart. Holding�a TRX suspension rope, do a low squat, making sure your knees don�t sneak past your toes. To add a little extra fire, slip a resistance band around your thighs, just above your knees.
Suspended Thigh Pulses
Stay in a squat�position holding a TRX rope. With a resistance band around your thighs, pulse your legs in and out, keeping feet still. Judging by Union�s expression here, this will really pack a punch, but it�ll do wonders for your posterior.
Stand with your feet hip-width apart. Hold a kettlebell with both hands between your legs. Squat with your back straight, making�sure your knees don�t go past your toes. Repeat.
Medicine Ball Throw
Standing with one foot in front of the other, back straight and knees slightly bent, hold a medicine ball in both hands. Making sure you pull it across your whole body, throw the ball against�a nearby wall and catch it. Repeat.
Standing with your legs more than shoulder-width apart, hold a dumbbell with that arm�above your head, other arm extended out and parallel with the ground. Bring the dumbbell down to the ground in one move, squatting as you go. Bring the dumbbell back above your head and straighten out your legs. Repeat.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine