Mr. and Mrs. Dominguez first received chiropractic care with Dr. Alex Jimenez after suffering automobile accident injuries. Martha Dominguez expresses how much their quality of life has changed since receiving chiropractic treatment and physical rehabilitation with Dr. Jimenez along with the trainers and staff at Push. Mr. and Mrs. Domingues are grateful for the services they’ve received for their automobile accident injuries and their sciatica pain.
Sciatica Pain Treatment And Chiropractic Care
Chiropractic care can help alleviate automobile accident injuries. Moreover, chiropractic care is totally non-invasive and drug-free, so there are fewer dangers involved with this holistic treatment. Furthermore, chiropractic techniques concentrate on treating the pain at its source, rather than masking it with prescription painkillers. Chiropractors will begin with an evaluation and appointment. From that point, they can perform a physical evaluation and run any required diagnostics to confirm the identification of the diagnosis. The chiropractor will then work on developing a customized treatment program with the patient’s needs and lifestyle in mind.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Auto Accidents: Mr. and Mrs. Dominguez were involved in an automobile accident which left them with pain and discomfort. In their search to find relief from their symptoms, Manuel Dominguez and his wife found chiropractic care with Dr. Alex Jimenez. The couple expresses how much their lives have changed since receiving chiropractic care and rehabilitation at Push. Mr. and Mrs. Dominguez are happy and grateful for the help they’ve received for their automobile accident injuries and they highly recommend and invite others to seek chiropractic care.
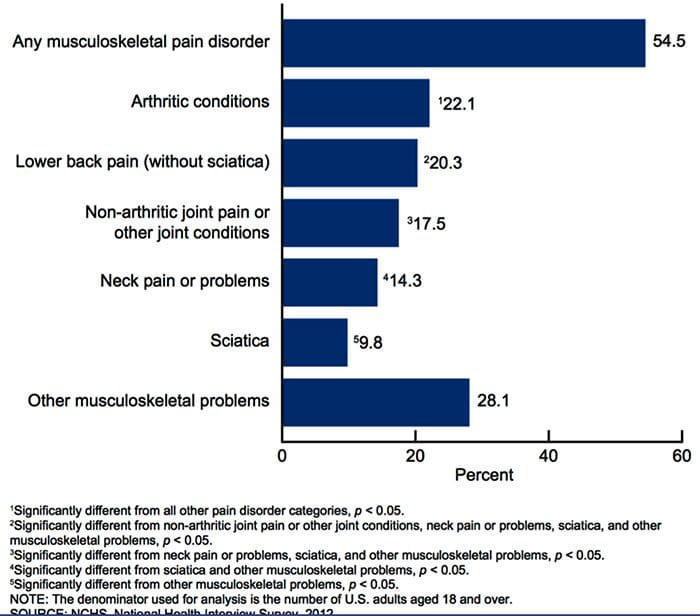
Mechanoreceptive Pain: According to the CDC, �more than 50% of U.S. adults (125 million) had a musculoskeletal pain disorder in 2012.�
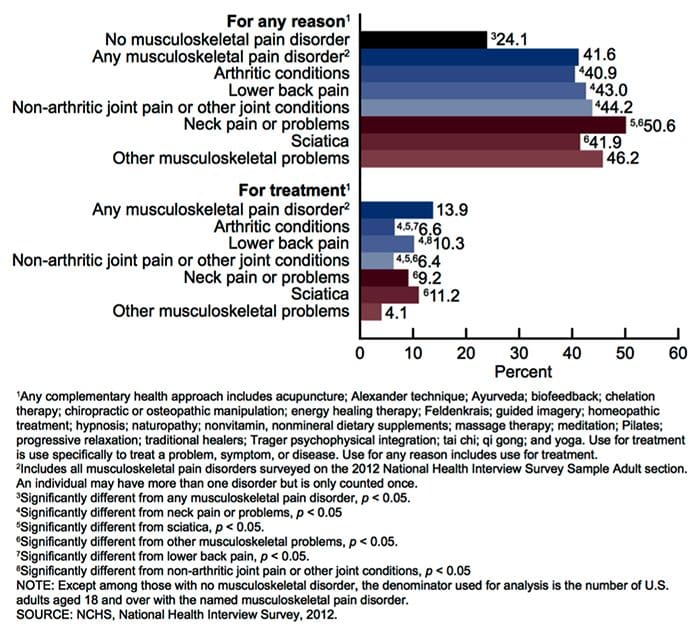
�More than 40% of adults with a musculoskeletal pain disorder used a complementary health approach for any reason in 2012. This was significantly higher than use among persons without a musculoskeletal pain disorder (24.1%). Use of complementary health approaches for any reason among persons with neck pain or problems was more than twice as high as use among persons without these problems.�
�Among adults with a musculoskeletal pain disorder, use of any complementary health approach was highest among those with neck pain or problems (50.6%), followed by persons with other musculoskeletal problems (46.2%).”
�Use of complementary health approaches for any reason among persons with neck pain or problems was more than twice as high as use among persons without these problems.�
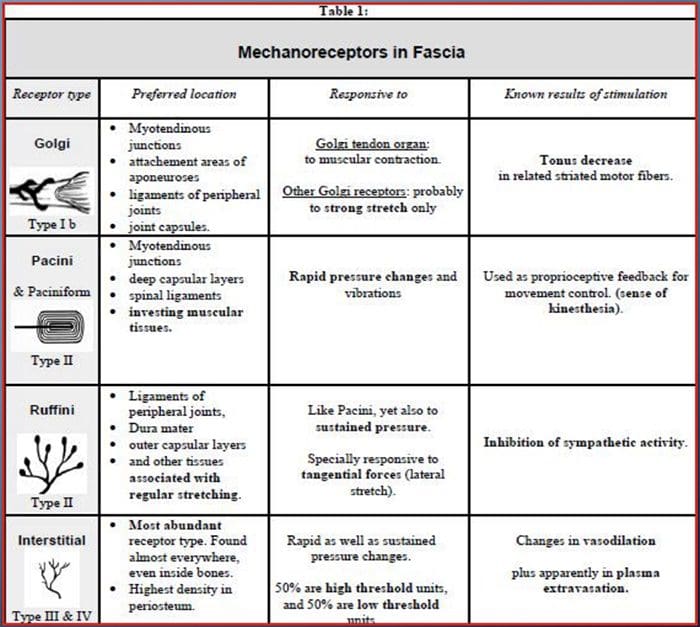
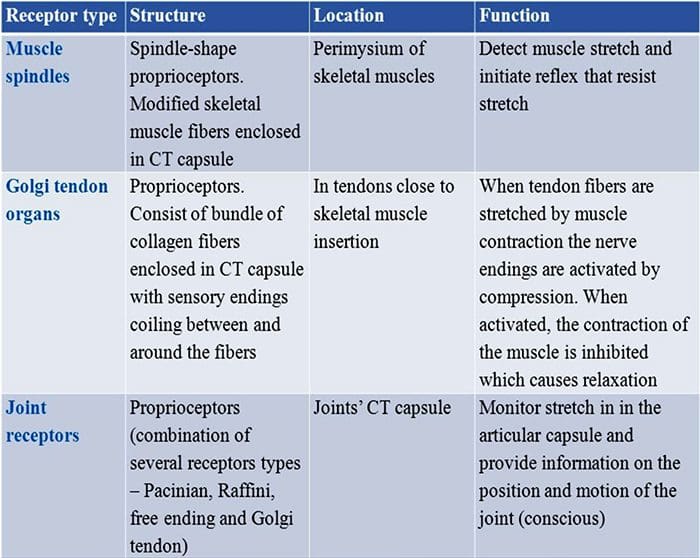
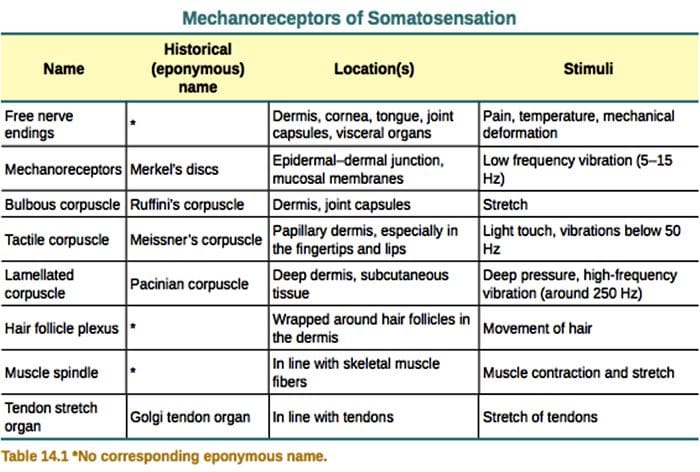
Mechanoreceptors are sensory receptors that respond to mechanical pressure or distortion.
These include cutaneous receptors for touch, receptors that monitor muscle length and tension, auditory and vestibular receptors and others.
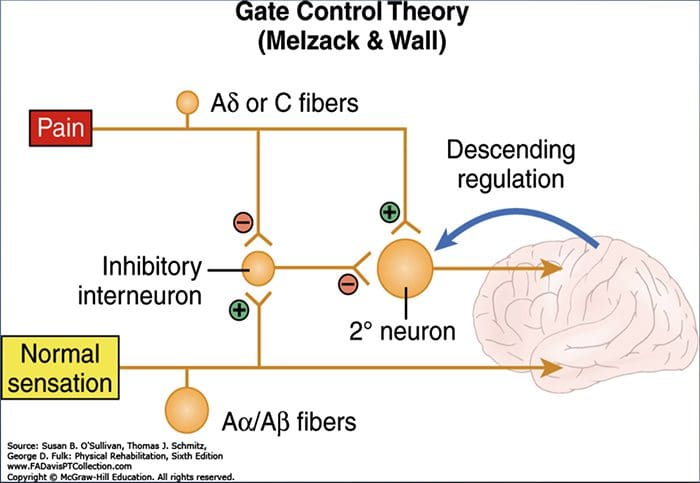
GATE CONTROL THEORY OF PAIN
Non-painful input closes the gates to painful input.
This prevents pain sensations from traveling to higher cortical levels
Small diameter afferents (pain) impede inhibition of pain
Large diameter afferents (vibration) tend to excite inhibition of pain.
This theory asserts non-nociceptive fibers can interfere with signals from pain fibers, therefore, inhibiting pain.
Large-diameter A? fibers are nonnociceptive (do not transmit pain stimuli) and inhibit the effects of firing by A? and C fibers.
DORSAL COLUMN MEDIAL LEMNISCAL PATHWAY
UTILIZATION OF PERIPHERAL MECHANORECEPTORS TO ALTER PAIN PERCEPTION
HOW CAN WE HELP?
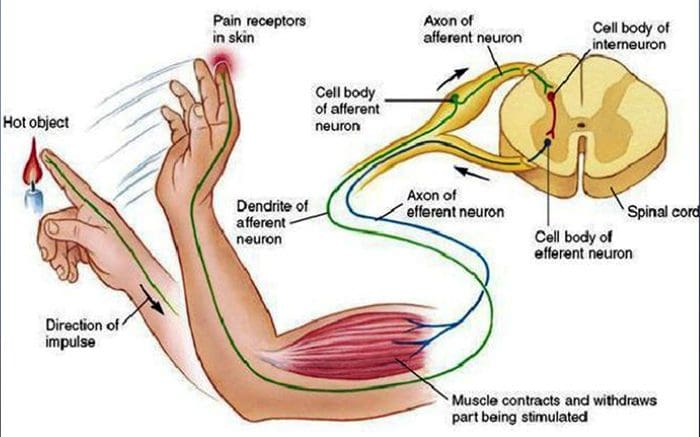
WITHDRAWAL REFLEX
An excited afferent neuron stimulates excitatory interneurons that in turn stimulate the efferent motor neurons supplying the biceps, the muscle in the arm that flexes (bends) the elbow joint. Contraction of the biceps pulls the hand away from the hot stove.
The afferent neuron also stimulates inhibitory interneurons that in turn inhibit the efferent neurons supplying the triceps to prevent it from contracting. This type of neuronal connection involving stimulation of the nerve supply to one muscle and simultaneous inhibition of the nerves to its antagonistic muscle is known as reciprocal inhibition.
The afferent neuron still stimulates other interneurons that carry the signal up the spinal cord to the brain via an ascending pathway. Only when the impulse reaches the sensory area of the cortex is the person aware of the pain, its location and the type of stimulus. Moreover, when the impulse reaches the brain, the information can be stored as memory and the person can think about what happened.
RECEPTOR BASED THERAPY
Adjustments
Activation of joint mechanoreceptors through chiropractic adjustments can modulate and �overshadow� the brains perception of smaller diameter fibers.
Repetition of activation of joint mechanoreceptors can create positive plasticity in afferent pathways.
Positive plasticity can shut down pain
Vibration
Vibratory stimulation at specific frequencies can alter pain perception
Repetition of activation of Merkel�s discs and Meissner�s corpuscles can create positive plasticity in afferent pathways.
Again, positive plasticity can shut down pain
VIBRATION
�This type of device applies sinusoidal vibrations and offers continuous selectable amplitude of 0-5.2mm depending on the foot position and a selectable frequency of 5-30Hz.�
�WBV training seems to be an effective, safe, and suitable intervention for seated working employees with chronic low-back pain.�
�Homotopic vibro-tactile stimulation resulted in 40% heat pain reductions in all subject groups. Distraction did not seem to affect experimental pain ratings.�
�Vibro-tactile stimulation effectively recruited analgesic mechanisms not only in NC but also in patients with chronic musculoskeletal pain, including FM.�
LIGHT TOUCH
�In total, 44 healthy volunteers experienced heat pain and CT optimal (slow brushing) and CT sub-optimal (fast brushing or vibration) stimuli. Three different experimental paradigms were used: Concurrent application of heat pain and tactile (slow brushing or vibration) stimulation; Slow brushing, applied for variable duration and intervals, preceding heat pain; Slow versus fast brushing preceding heat pain.�
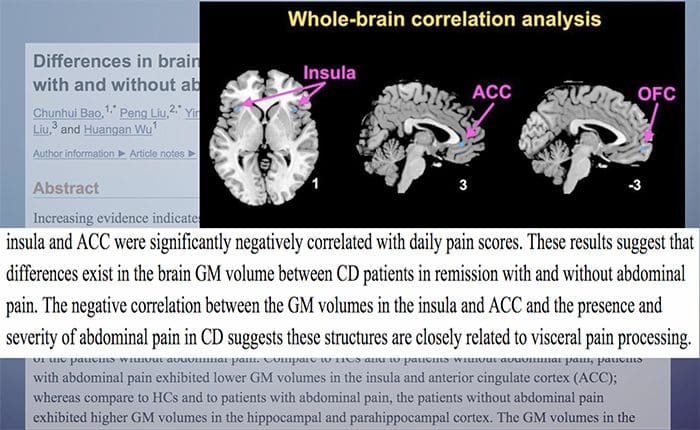
In humans, the main brain areas receiving C- LTMR information belong to the somatosensory system and affect processing brain networks like the contralateral posterior insular cortex or the medial prefrontal cortex. The intensity of CT targeted touch is encoded in the primary and secondary somatosensory cortex (S1 contralateral, S2 bilateral), whereas the pleasantness is encoded in the anterior cingulate cortex. C-LTMRs also activate regions involved in reward processing (putamen and orbitofrontal cortex) and in processing of social stimuli (posterior superior temporal sulcus).
EVERYTHING PERIPHERAL HAS A CENTRAL CONSEQUENCE
CASE STUDY
47-year-old male suffered left CVA in October of 2017.
Has not moved the right side of his body since the accident.
Presented to our clinic because he wants to �get back to it.�
PHYSICAL EXAMINATION HIGHLIGHTS
Dysarthria
Altered pain perception
Difficulty with simple math
Flaccid on RUE and RLE
PHYSICAL EXAMINATION HIGHLIGHTS
Patient had no movement until we began testing sensation and reflexes:
ALLODYNIA:�Refers to central pain sensitization ( increased response of neurons) following normally non-painful, often repetitive stimulation.
Allodynia can lead to the triggering of a pain response from stimuli, which does not normally provoke pain.
Temperature or physical stimuli can provoke allodynia, which may feel like a burning sensation and it often occurs after injury to a site.
Alldynia is different from Hyperalgesia, an extreme, exaggerated reaction to a stimulus, which is normally painful.
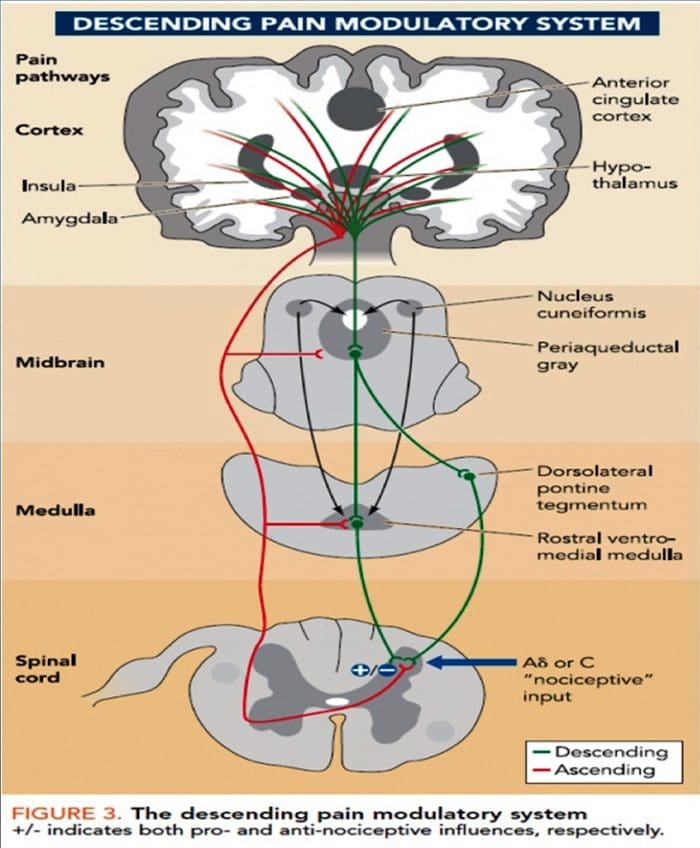
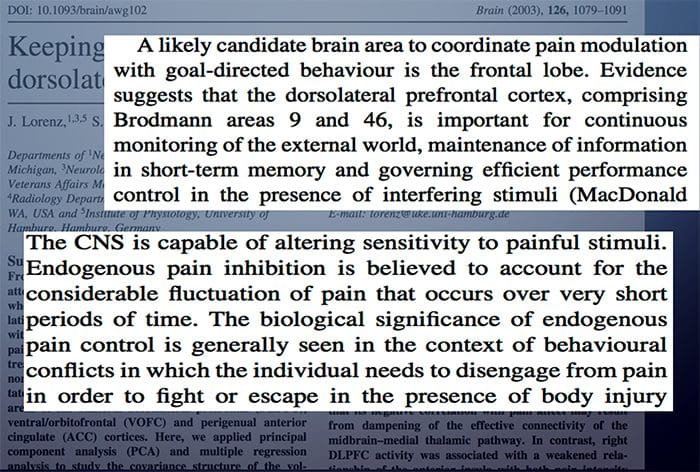
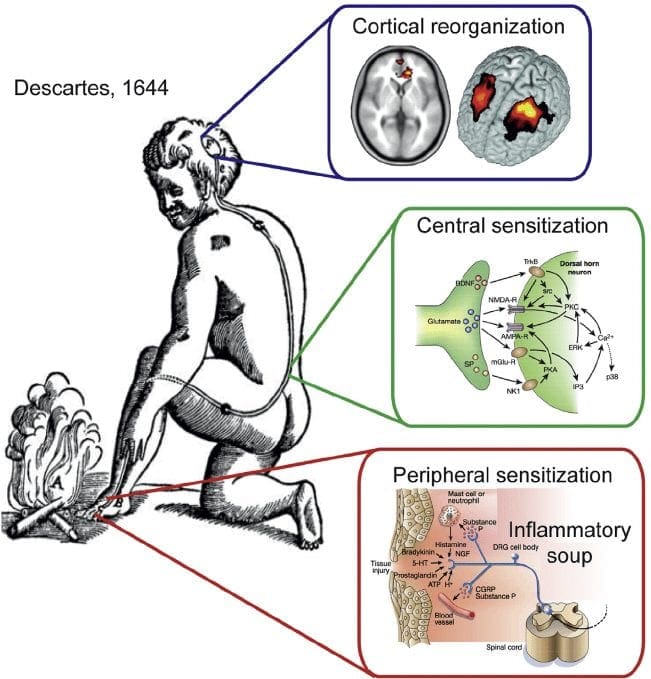
Why does localized damage or injury caused by trauma lead to chronic, intractable pain in certain patients? What’s in charge of the translation of local injury with acute pain into a chronic pain condition? Why does some pain respond to anti-inflammatory drugs and/or medications, whereas other forms of pain require opiates?
Pain is an intricate process involving both the peripheral nervous system (PNS) and the central nervous system (CNS). Tissue injury triggers the PNS, which transmits signals via the spinal cord into the brain, in which pain perception occurs. However, what causes the intense experience of pain to develop into an unremitting phenomenon? Can anything be done to prevent it? Evidence indicates that chronic pain results from a combination of mechanisms, such as neurological “memories” of preceding pain.
Nociception: The Simplest Pathway
Acute or nociceptive pain is characterized as the regular experience of discomfort which occurs in response to very basic damage or injury. It is protective, warning us to move away from the origin of the insult and take care of the trauma. The mechanisms that create nociceptive pain include transduction, which extends the external traumatic stimulation into electrical activity in specialized nociceptive primary afferent nerves. The afferent nerves then conduct the sensory information from the PNS to the CNS.
In the CNS, the pain data is transmitted by the primary sensory neurons into central projection cells. After the information is transferred to all those areas of the brain which are responsible for our perception, the actual sensory experience happens. Nociceptive pain is a relatively simple reaction to a particularly simple, acute stimulus. But the mechanics in charge of nociceptive pain cannot identify phenomena, such as pain that persists despite removal or healing of the stimulation, such as in the instance of phantom limb pain.
Pain and the Inflammatory Response
In circumstances of more severe injury, such as surgical wounds, tissue damage may stimulate an inflammatory reaction. However, other conditions, especially arthritis, can also be characterized by continuing cases of inflammation associated with intense pain symptoms. The mechanisms for this type of pain related to tissue damage and an inflammatory response are different from early-warning nociceptive pain.
Observing the incision or site of other damage or injury, a cascade of hyperexcitable events occur in the nervous system. This bodily “wind-up” phenomenon begins at the skin, where it is potentiated along the peripheral nerves, and culminates at a hypersensitivity response along the spinal cord (dorsal horn) and the brain. Inflammatory cells then surround the regions of tissue damage and also produce cytokines and chemokines, substances which are intended to mediate the process of healing and tissue regeneration. But, these agents may also be considered irritants and adjust the properties of the primary sensory neurons surrounding the area of trauma.
Thus, the major factors which trigger inflammatory pain include damage to the high-threshold nociceptors, known as peripheral sensitization, changes and alterations of the neurons in the nervous system, and the amplification of the excitability of neurons within the CNS. This represents central sensitization and is accountable for hypersensitivity, where areas adjacent to those of the true injury will experience pain as if these were injured. These tissues can also react to stimulation which normally doesn’t create pain, such as a touch, wearing clothing, light pressure, or even brushing your own hair, as if they were truly painful, referred to as allodynia.
Neuropathic pain results from damage or injury to the nervous system, such as carpal tunnel syndrome, postherpetic neuralgia and diabetic neuropathy. Although some of the mechanisms which seem to cause neuropathic pain overlap with those responsible for inflammatory pain, many of them are different, and thus will need a different approach towards their management.
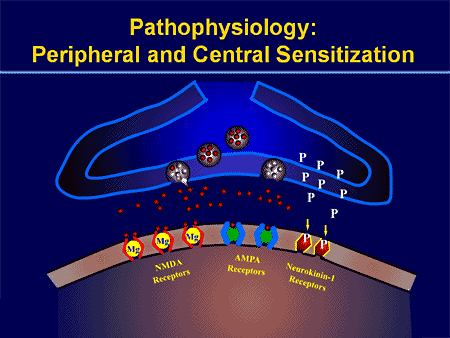
The process of peripheral and central sensitization is maintained, at least theoretically and experimentally, during the excitatory neurotransmitter, glutamate, which is believed to be released when the N-methyl-D-aspartate (NMDA) receptor is activated.
The nervous system is made up of either inhibitory or excitatory neurotransmitters. Most of what permits our nervous system to respond appropriately to damage or injury is the fine-tuning or inhibition of a variety of processes. The overexcitation of the nervous system is seen to be an issue in a number of different disorders. For instance, overactivation of an NMDA receptor can also be related to affective disorders, sympathetic abnormalities, and even opiate tolerance.
Even ordinary nociceptive pain, to some degree, activates the NMDA receptor and is believed to lead to glutamate release. Nonetheless, in neuropathic pain, oversensitivity to the NMDA receptor is key.
With other types of chronic pain, such as fibromyalgia and tension-type headaches, some of the mechanisms active in inflammatory and neuropathic pain may also create similar abnormalities in the pain system, including central sensitization, higher excitability of the somatosensory pathways, and reductions in central nervous system inhibitory mechanisms.
Peripheral Sensitization
Cyclo-oxygenase (COX) also plays an essential function in both peripheral and central sensitizations. COX-2 is one of the enzymes which are induced during the inflammatory process; COX-2 converts arachidonic acid into prostaglandins, which increase the sensitivity of peripheral nociceptor terminals. Virtually, peripheral inflammation also causes COX-2 to be produced from the CNS. Signals from peripheral nociceptors are partially responsible for this upregulation, but there also seems to be a humoral component to the transduction of the pain signals across the blood-brain barrier.
For instance, in experimental models, COX-2 is generated from the CNS even if animals receive a sensory nerve block prior to peripheral inflammatory stimulation. The COX-2 that is expressed over the dorsal horn neurons of the spinal cord releases prostaglandins, which act on the central terminals, or the presynaptic terminals of nociceptive sensory fibers, to increase transmitter release. Additionally, they act postsynaptically on the dorsal horn neurons to produce direct depolarization. And finally, they inhibit the activity of glycine receptor, and this is an inhibitory transmitter. Therefore, the prostaglandins create an increase in excitability of central neurons.
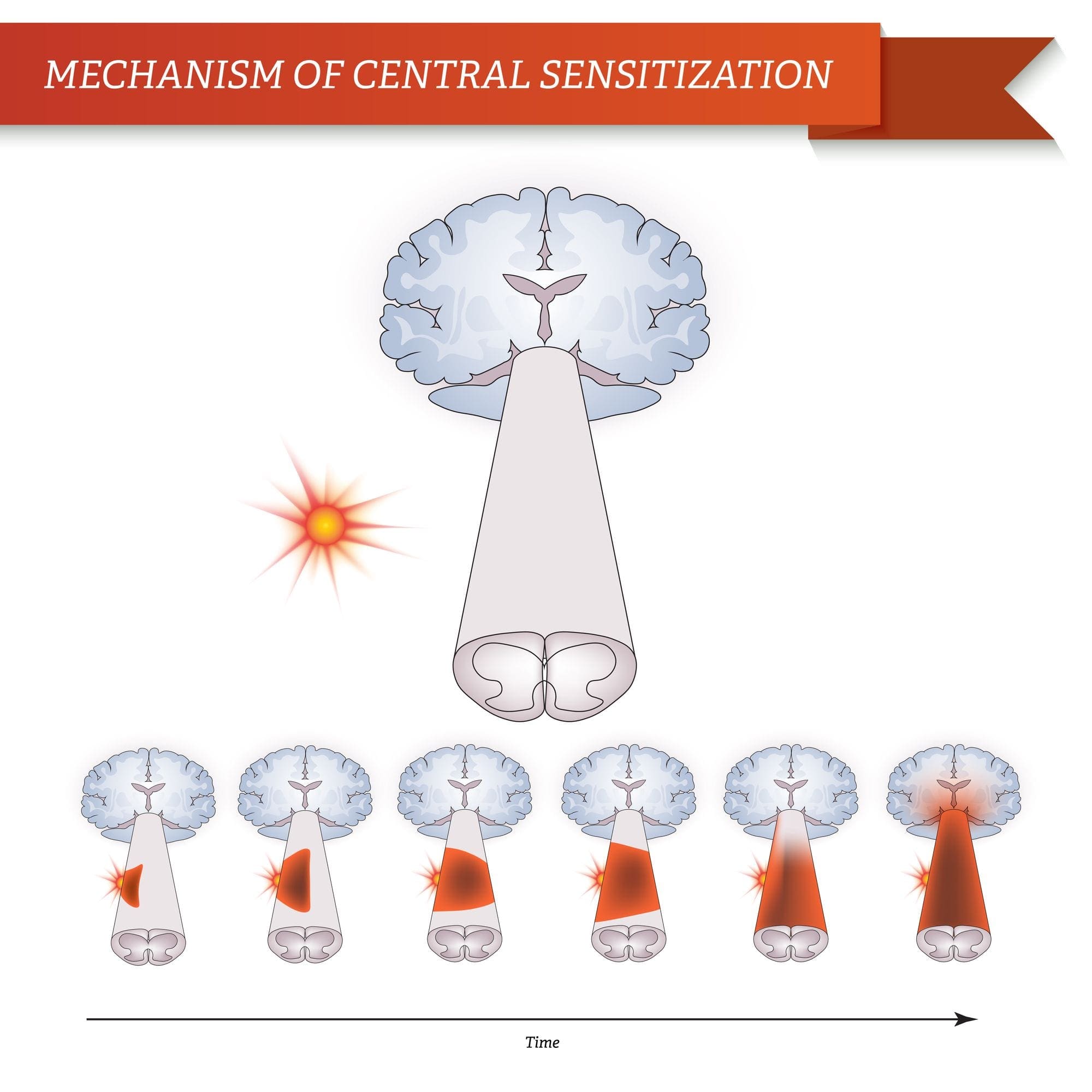
Brain Plasticity and Central Sensitization
Central sensitization describes changes which happen in the brain in reaction to repeated nerve stimulation. After repeated stimuli, amounts of hormones and brain electric signals change as neurons develop a “memory’ for reacting to those signs. Constant stimulation creates a more powerful brain memory, so the brain will respond more rapidly and effectively when undergoing the identical stimulation in the future. The consequent modifications in brain wiring and reaction are referred to as neural plasticity, which describe the capability of the brain to alter itself readily, or central sensitization. Therefore, the brain is activated or sensitized by previous or repeated stimuli to become more excitable.
The fluctuations of central sensitization occur after repeated encounters with pain. Research in animals indicates that repeated exposure to a painful stimulation will change the animal’s pain threshold and lead to a stronger pain response. Researchers think that these modifications can explain the persistent pain that could occur even after successful back surgery. Although a herniated disc may be removed from a pinched nerve, pain may continue as a memory of the nerve compression. Newborns undergoing circumcision without anesthesia will react more profoundly to future painful stimulation, such as routine injections, vaccinations, and other painful processes. These children haven’t only a higher hemodynamic reaction, known as tachycardia and tachypnea, but they will also develop enhanced crying too.
This neurological memory of pain was studied extensively. In a report on his previous research studies, Woolf noted that the improved reflex excitability following peripheral tissue damage or injury doesn’t rely on continuing peripheral input signals; rather, hours after a peripheral trauma, spinal dorsal horn neuron receptive fields continued to enlarge. Researchers also have documented the significance of the spinal NMDA receptor to the induction and maintenance of central sensitization.
Significance for Pain Management
Once central sensitization is established, bigger doses of analgesics are often required to suppress it. Preemptive analgesia, or therapy before pain progresses, may lower the effects of all of these stimulation on the CNS. Woolf demonstrated that the morphine dose required to stop central hyperexcitability, given before short noxious electrical stimulation in rats, was one tenth the dose required to abolish activity after it had grown. This translates to clinical practice.
In a clinical trial of 60 patients undergoing abdominal hysterectomy, individuals who received 10 mg of morphine intravenously at the time of induction of anesthesia required significantly less morphine for postoperative pain control. Furthermore, pain sensitivity around the wound, referred to as secondary hyperalgesia, was also reduced in the morphine pretreated group. Preemptive analgesia was used with comparable success in an assortment of surgical settings, including prespinal operation and postorthopaedic operation.
A single dose of 40 or 60 mg/kg of rectal acetaminophen has a clear morphine-sparing effect in day-case surgery in children, if administered in the induction of anesthesia. Furthermore, children with sufficient analgesia with acetaminophen experienced significantly less postoperative nausea and vomiting.
NMDA receptor antagonists have imparted postoperative analgesia when administered preoperatively. Various reports exist in the literature supporting the use of ketamine and dextromethorphan in the preoperative period. In patients undergoing anterior cruciate ligament reconstruction, 24-hour patient-controlled analgesia opioid consumption was significantly less in the preoperative dextromethorphan category versus the placebo group.
In double-blind, placebo-controlled research studies, gabapentin was indicated as a premedicant analgesic for patients undergoing mastectomy and hysterectomy. Preoperative oral gabapentin reduced pain scores and postoperative analgesic consumption without gap in side effects as compared with placebo.
Preoperative administration of nonsteroidal anti-inflammatory drugs (NSAIDs) has demonstrated a significant decrease in opioid use postoperatively. COX-2s are preferable due to their relative lack of platelet effects and significant gastrointestinal safety profile when compared with conventional NSAIDs. Celecoxib, rofecoxib, valdecoxib, and parecoxib, outside the United States, administered preoperatively reduce postoperative narcotic use by more than 40 percent, with many patients using less than half of the opioids compared with placebo.
Blocking nerve conduction in the preoperative period appears to prevent the development of central sensitization. Phantom limb syndrome (PLS) has been attributed to a spinal wind-up phenomenon.�Patients with amputation
often have burning or tingling pain in the body part removed. One possible cause is that nerve fibers at the stump are stimulated and the brain interprets the signals as originating in the amputated portion. The other is the rearrangement within the cortical areas so that area say for the hand now responds to signals from other parts of the body but still interprets them as coming for the amputated hand.
However, for patients undergoing lower-extremity amputation under epidural anesthesia, not one of the 11 patients who received lumbar epidural blockade with bupivacaine and morphine for 72 hours before operation developed PLS. For people who underwent general anesthesia without prior lumbar epidural blockade, 5 of 14 patients had PLS at 6 weeks and 3 continued to experience PLS at 1 year.
Woolf and Chong have noted that perfect preoperative, intraoperative, and postoperative treatment comprises of “NSAIDs to reduce the activation/centralization of nociceptors, local anesthetics to block sensory inflow, and centrally acting drugs such as opiates.” Decreasing perioperative pain with preemptive techniques enhances satisfaction, hastens discharge, spares opioid use, along with diminished constipation, sedation, nausea, and urinary retention, and may even stop the development of chronic pain. Anesthesiologists and surgeons should consider integrating these techniques in their everyday practices.
When pain occurs as a result of damage or injury in consequence of surgery, the spinal cord can attain a hyperexcitable state wherein excessive pain reactions occur that may persist for days, weeks or even years.
Why does localized injury resulting from trauma result in chronic, intractable pain in some patients? Tissue injury leads to a constellation of changes in spinal excitability, including elevated spontaneous firing, greater response amplitude and length, decreased threshold, enhanced discharge to repeated stimulation, and expanded receptive fields. The persistence of these changes, which are collectively termed central sensitization, appears to be fundamental to the prolonged enhancement of pain sensitivity which defines chronic pain. Numerous drugs and/or medications as well as local anesthetic neural blockade may limit the magnitude of the central nervous system (CNS) windup, as evidenced by diminished pain and diminished opioid consumption in the preemptive analgesic models.
Dr. Alex Jimenez’s Insight
Chiropractic care is an alternate treatment option which utilizes spinal adjustments and manual manipulations to safely and effectively restore as well as maintain the proper alignment of the spine. Research studies have determined that spinal misalignments, or subluxations, can lead to chronic pain. Chiropractic care is commonly utilized for pain management, even if the symptoms are not associated to an injury and/or condition in the musculoskeletal and nervous system. By carefully re-aligning the spine, a chiropractor can help reduce stress and pressure from the structures surrounding the main component of out body’s foundation, ultimately providing pain relief.
Enteric Nervous System Function and Pain
When it comes to the diminished use of drugs and/or medications, including opioids, in order to prevent side-effects like gastrointestinal health issues, the proper function of the enteric nervous system may be at play.
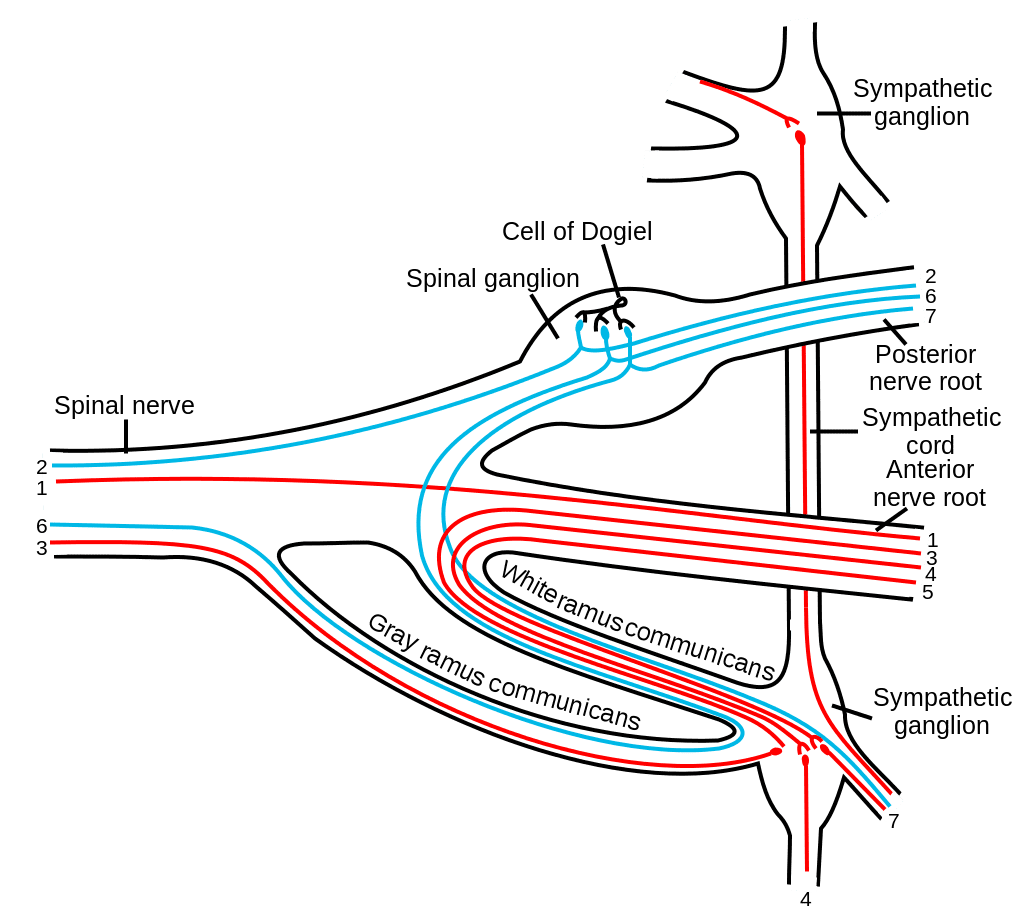
The enteric nervous system (ENS) or intrinsic nervous system is one of the key branches of the autonomic nervous system (ANS) and consists of a mesh-like system of nerves which modulates the role of the gastrointestinal tract. It’s capable of acting independently of the sympathetic and parasympathetic nervous systems, even though it might be affected by them. The ENS can also be called the second brain.�It is derived from neural crest cells.
The enteric nervous system in humans is made up of some 500 million neurons, including the numerous types of Dogiel cells, approximately one two-hundredth of the amount of neurons in the brain. The enteric nervous system is inserted into the lining of the gastrointestinal system, beginning at the esophagus and extending down to the anus. Dogiel cells, also known as cells of Dogiel, refers to some kind of multipolar adrenal tissues within the prevertebral sympathetic ganglia.
The ENS is capable of autonomous functions, such as the coordination of reflexes; even though it receives considerable innervation in the autonomic nervous system, it does and can operate independently of the brain and the spinal cord.�The enteric nervous system has been described as the “second brain” for a number of reasons. The enteric nervous system may operate autonomously. It normally communicates with the central nervous system (CNS) via the parasympathetic, or via the vagus nerve, and the sympathetic, that is through the prevertebral ganglia, nervous systems. However, vertebrate studies reveal that when the vagus nerve is severed, the enteric nervous system continues to function.
In vertebrates, the enteric nervous system includes efferent neurons, afferent neurons, and interneurons, all of which make the enteric nervous system capable of carrying reflexes and acting as an integrating center in the absence of CNS input. The sensory neurons report on mechanical and chemical conditions. The enteric nervous system has the ability to change its response based on such factors as nutrient and bulk composition. In addition, ENS contains support cells that are much like astroglia of the brain and a diffusion barrier around the capillaries surrounding ganglia that’s like the blood-brain barrier of blood vessels.
The enteric nervous system (ENS) plays a pivotal role in inflammatory and nociceptive processes. Drugs and/or medications that interact with the ENS have recently raised considerable interest because of their capacity to regulate numerous aspects of the gut physiology and pathophysiology. In particular, experiments in animals have demonstrated that�proteinase-activated receptors (PARs) may be essential to neurogenic inflammation in the intestine. Moreover, PAR2 agonists seem to induce intestinal hypersensitivity and hyperalgesic states, suggesting a role for this receptor in visceral pain perception.
Furthermore, PARs, together with the proteinases that activate them, represent exciting new targets for therapeutic intervention on the ENS. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Your mother always said don�t slouch – turns out she was right. And she has science to back it up. Your posture can have a profound effect on your health. Walking or sitting with a hunched back has been linked to a variety of health issues.
What�s more, poor posture can cause your body�s structure to change, leading to misalignment. While everyone slips a bit in the posture department now and then, the real damage occurs when it becomes a habit. In fact, you could be damaging your health with bad posture and not even realize it. Here are five ways that posture mistakes can harm your health.
Posture
Pain In The Neck, Back & Shoulders
Sitting in a slouched or hunched over position, drooping your shoulders, or rounding out your spine while standing or sitting can cause pain in your neck, back, and shoulders. Many people who work with computers as a regular part of their jobs experience this to some degree.
That is because the majority of workers do not have their computer monitors at the appropriate height, causing them to spend hours a day hunched over their keyboard. People who spend a lot of time on their smartphone and mobile devices experience text neck, which is caused by this type of poor posture.
Increased Depression & Stress
The connection between posture and mood has long been established. People who walk slouched over tend to feel more depressed and have a poorer self-image.
When you are slouched, you are restricting blood flow throughout your body, inhibiting proper oxygenation of your cells, and crowding your organs so that they are not able to function at an optimum level. If your spine or body is out of alignment, it can slow the neural processes that keep your body functioning as it should. When all these things are going on, your mood will definitely be affected, especially if you aren�t as active as you should be.
Pain/Weakness In The Lower Back, Hips, Knees & Ankles
This posture problem is common in people who are obese and pregnant women. The added weight causes the body to shift in unnatural positions in order to support it.
This postural problem can also be the result of inappropriate footwear. Feet are important! Take care of them by wearing shoes with good support. This can cause flat feet and cause the ankles to roll.
The calf muscles will tighten and your knees may even rotate inward. You can experience plantar fasciitis, pain in your toes, heel spurs, bunions, and hip problems. Weight loss can help and pregnant women can benefit from a pregnancy sling or pregnancy girdle to support the added girth.
Digestion Problems
Sitting in a hunched position crunches up everything inside, including your intestines. This will slow things down considerably, leading to constipation and even hemorrhoids.
The human body was designed to remain in a certain position so that all organs can function as they should. When things are out of alignment it can lead to indigestion, heartburn, and even acid reflux. Practicing good posture can make all the difference in a lot of things. Poor digestion can lead to obesity.
Spinal Misalignment Leading To Many Health Issues
When your spine is out of line it can cause headaches, dizziness, and a host of other issues. It puts your body under stress so even the normal processes like blood flow and organ function are thrown off kilter. When your body isn�t working as it should the risk of serious conditions like heart disease, diabetes, and hypertension are increased.
Many people don�t make the connection between good posture with a properly aligned spine and better health, but it is definitely there. Posture may seem simple, like it�s not that big of a deal, but when it is practiced on an ongoing basis, it can be detrimental to your health. It isn�t worth the risk; not when the fix is as simple as sitting up straight.
Injury Medical Clinic: Fibromyalgia Care & Treatment
Lower Back Injury: Isaiah Delgado, wrestler, began participating in a fitness and nutrition program at Push-as-RX in order to improve his performance in his physical activities. When he suffered a lower back sports injury, Isaiah Delgado once again came to Push for assistance, except this time, the trainers enrolled him in a rehabilitation program to help him return-to-play as soon as possible. Isaiah Delgado describes Push-as-Rx as a lifestyle and he recommends Push to anyone looking for the right type of support when it comes to recovery and increased performance.
Lower Back Injury And Chiropractic Care
Sports Therapy is an element of healthcare that’s specifically concerned with the prevention of injury and the rehabilitation of the individual back to optimum levels of practical, occupational and sports specific fitness, regardless of age and capacity. It utilizes the fundamentals of sport and exercise sciences incorporating behavioral and physiological processes to prepare the player for training, competition and where applicable, work. A variety of healthcare professionals are able to provide this type of treatment method.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
The aging process can usher in a variety of conditions and health issues that are confined (mostly) to the elderly. Chronic pain, arthritis, loss of mobility, and other issues can occur as a person get older, but senior citizens are finding that chiropractic provides some great benefits for the older demographic.
Senior Citizens
Better Range Of Motion
Regular chiropractic care has been shown to increase spinal range of motion as well as in the extremities. Limited range of motion can occur due to age or inactivity � sometimes a combination of the two.
Having the ability to move easier has many great benefits. It allows seniors to more actively engage with their environment. They can get on their hands and knees to work in the garden, bend down to pick up grandchildren, and improve leisure activities like golfing. Increased range of motion is one of the most common (and appreciated!) benefits of chiropractic treatment.
Decreased Degeneration Of Joints
When the spine is misaligned it can lead to other parts of the body becoming misaligned as well. This can lead to unusual and unnatural wearing of the joints. Over time, the joints can become worn down, painful, and cause difficulty in mobility and flexibility.
Chiropractic care is a very effective treatment for decreasing the degeneration of the spine and even other joints. When the body is in proper alignment it no longer has to adapt through postural compensation. This reduces stress on the spine and joints while relieving pain and restoring mobility.
Pain Relief
Chiropractic has long been recognized for its effectiveness in providing drug free pain relief for everything from back pain to headaches to arthritis. While pain medication and anti-inflammatory drugs only suppress the symptoms, chiropractic addresses the root of the problem.
Spinal alignments and other chiropractic techniques help to relieve pain for a variety of issues, not just back and neck pain. What�s more, chiropractic does not have the undesirable, sometimes dangerous side effects that drugs can.
Overall Better Health & Wellbeing
Proper spinal alignment can greatly benefit a person�s health, wellbeing, and even their mood. It allows them to become more active so they get exercise. They sleep better and have more energy.
An aligned spine also lets them more fully engage with their family, friends, and the world. They can get out and do things they were once unable to do and when they are active and happier the entire body benefits.
Improved Coordination & Balance
The aging process can have a significant impact on a person�s balance and coordination. This can have a variety of causes including degenerative changes to the spine, typically in the neck area. Injury to this area is another culprit.
There are special receptors that reside along the cervical spine in the rear of the joints. These receptors work to send vital messages to the brain regarding coordination and balance. When the spine and especially the neck are out of alignment, it can hinder how these receptors send and receive messages to the brain. The result is a condition called loss of proprioception, or sense of body awareness.
As the condition progresses, the patient relies on vision to determine the location of their feet, legs, and other limbs. The worse it gets, the less able the patient is in compensating and can become prone to falling.
Injuries from falling are one of the most common reasons elderly people visit emergency departments each year. Chiropractic can help realign the neck and spine, allowing the messages to move much easier, thus restoring balance and coordination.
Prevents Seniors From Being Confined To Nursing Homes
Senior citizens who are regular chiropractic patients are more likely to engage in exercise that is more strenuous. They are more active, have fewer injuries, and are basically happier and more positive.
The more active and mobile senior citizens are, the less likely they are to be placed in a nursing home due to medical conditions or the �typical� aging issues. Simply put, chiropractic for seniors changes the way many people look at aging � and places it in a much more positive, active light.
Injury Medical Clinic: Elderly & Geriatric Fitness
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
Our services are specialized and focused on injuries and the complete recovery process. Our areas of practice include:
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
Our services are specialized and focused on injuries and the complete recovery process. Our areas of practice include: 
 GATE CONTROL THEORY OF PAIN
GATE CONTROL THEORY OF PAIN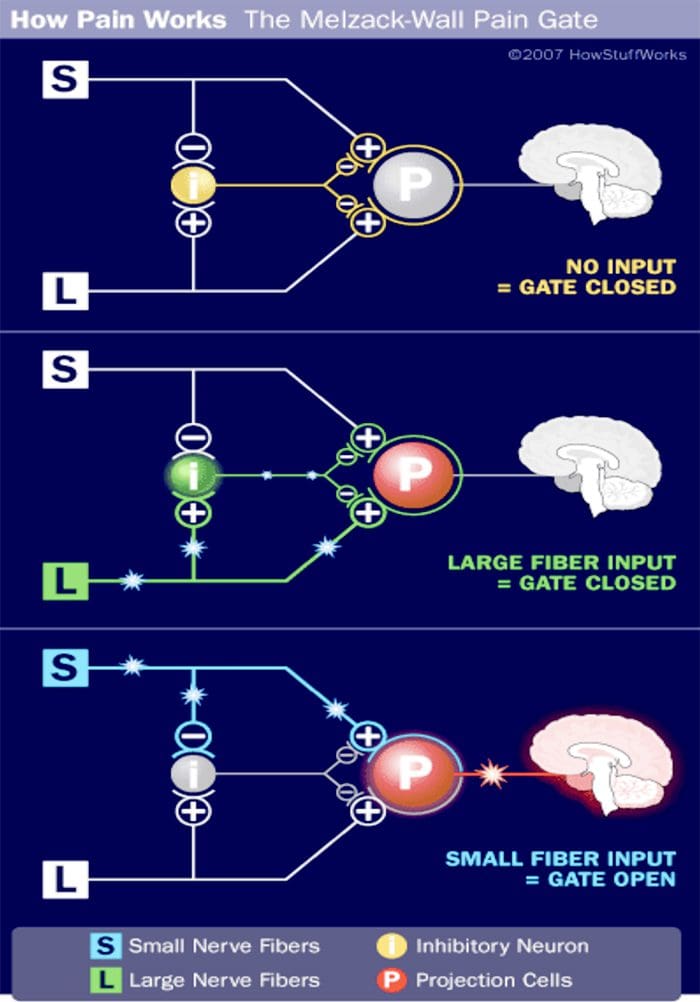
 DORSAL COLUMN MEDIAL LEMNISCAL PATHWAY
DORSAL COLUMN MEDIAL LEMNISCAL PATHWAY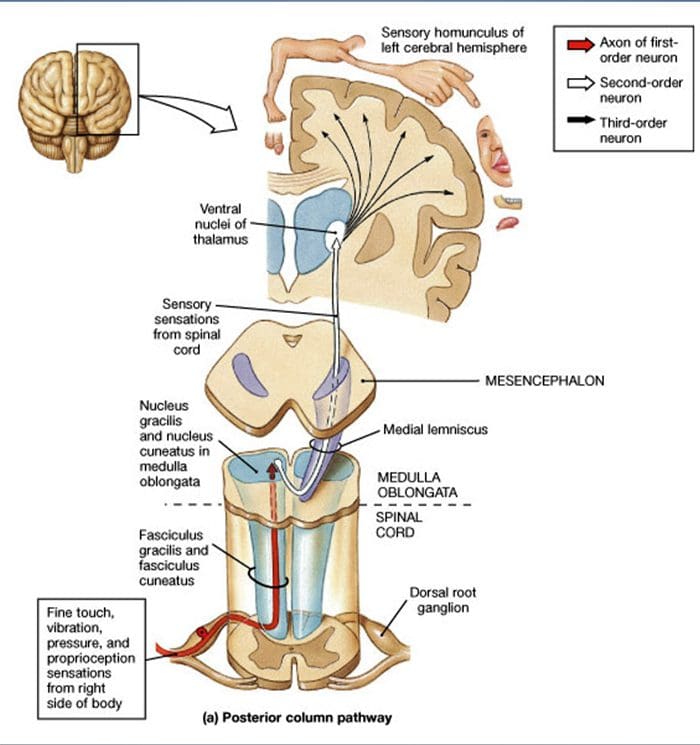 UTILIZATION OF PERIPHERAL MECHANORECEPTORS TO ALTER PAIN PERCEPTION
UTILIZATION OF PERIPHERAL MECHANORECEPTORS TO ALTER PAIN PERCEPTION
 VIBRATION
VIBRATION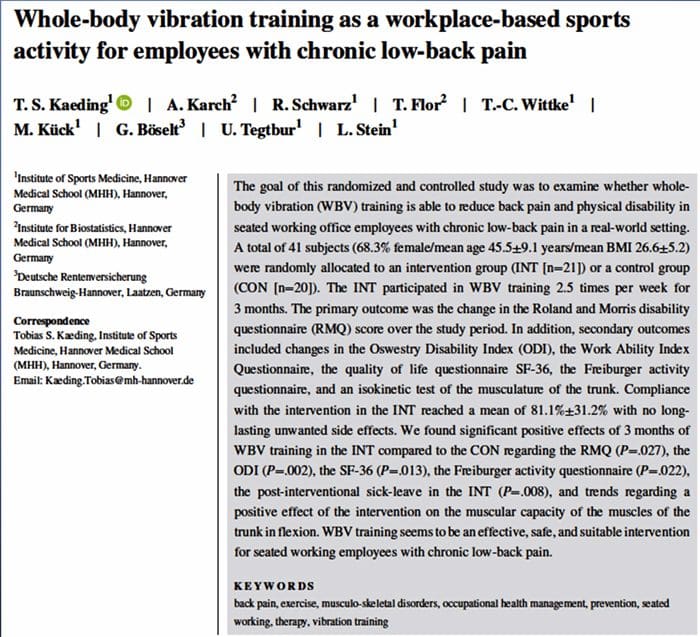
 LIGHT TOUCH
LIGHT TOUCH

 CASE STUDY
CASE STUDY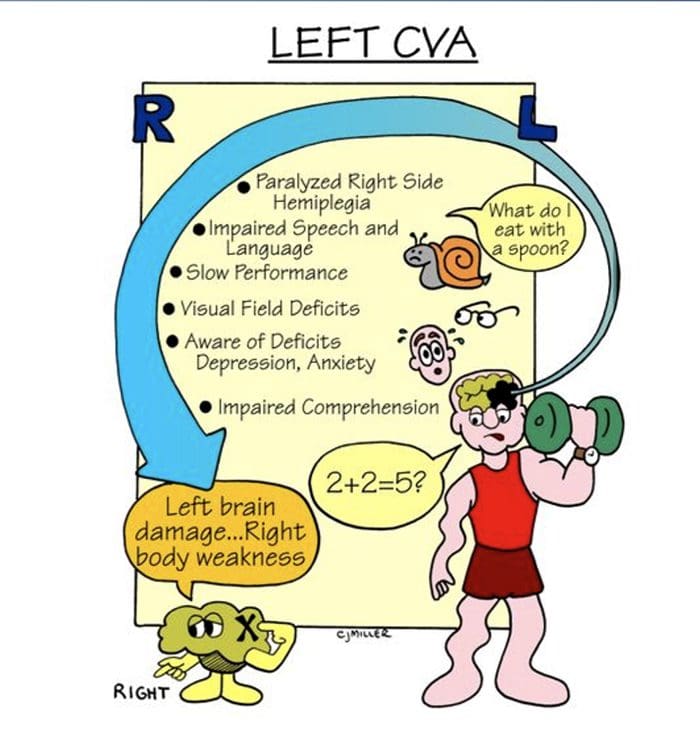 PHYSICAL EXAMINATION HIGHLIGHTS
PHYSICAL EXAMINATION HIGHLIGHTS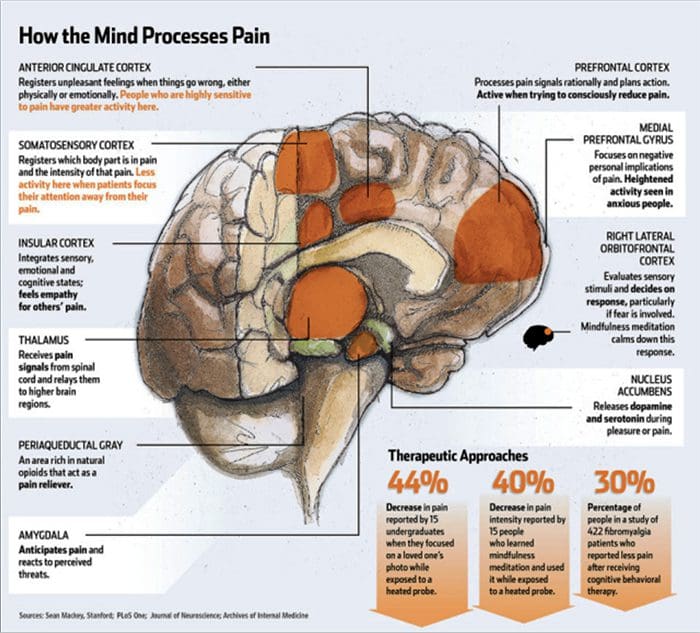 PHYSICAL EXAMINATION HIGHLIGHTS
PHYSICAL EXAMINATION HIGHLIGHTS
 AFTER TWO DAYS
AFTER TWO DAYS





 Pain/Weakness In The Lower Back, Hips, Knees & Ankles
Pain/Weakness In The Lower Back, Hips, Knees & Ankles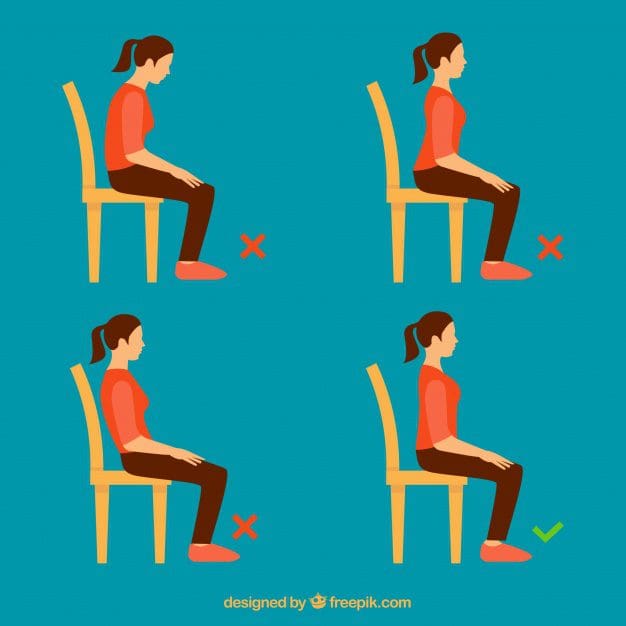

 We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.







