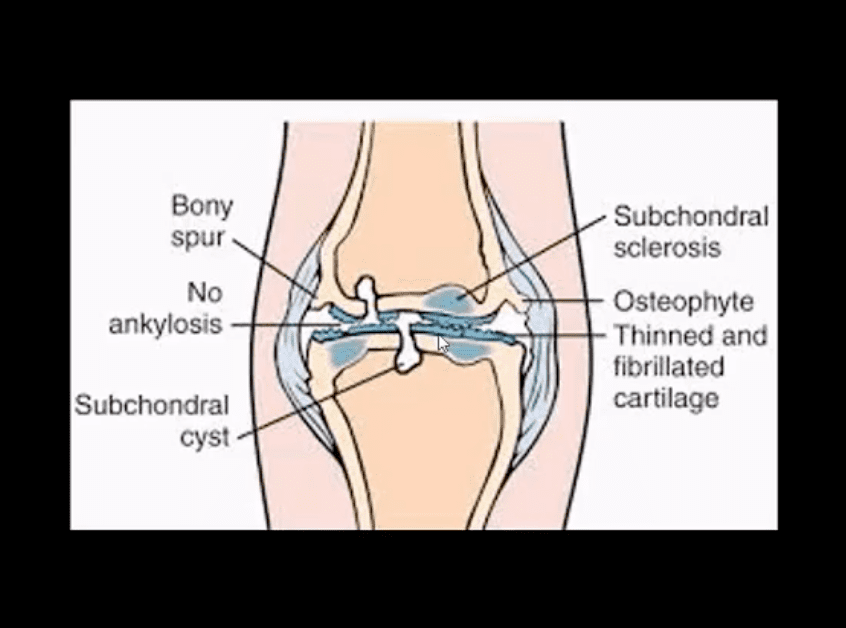
Pathology: da disease of the articular cartilage. Continuing mechanical stimulation follows by an initial increase in water and cartilage thickness. Gradual loss of proteoglycans and ground substance. Fissuring/splitting. Chondrocytes are damaged and release enzymes into the joint. Cystic progression and further cartilage loss. Subchondral bone is denuded and exposed to mechanical stresses. It becomes hypervascular forming osteophytes. Subchondral cysts and bone thickening/sclerosis develop.
Imaging plays a crucial role in Dx/grading and management
Clinically: pain on walking/rest, crepitus, swelling d/t synovitis, locking/catching d/t osseocartilaginous fragments and gradual functional loss. Knee OA typically presents as mono and oligoarthritis. DDx: morning pain/stiffness is >30-min DDx from inflammatory arthritis
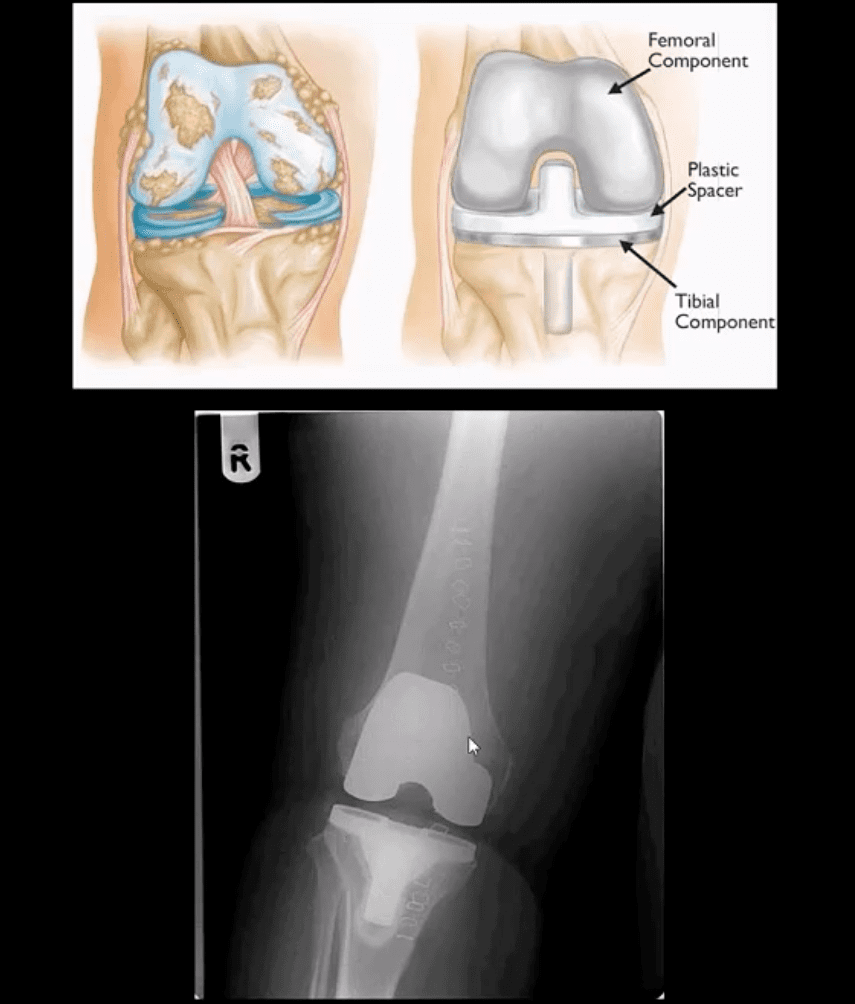
Treatment: in mild to moderate cases-conservative care. Severe OA-total knee arthroplasty
Grade 4: severe JSN, large osteophytes, marked subchondral sclerosis and definite bony deformity
Typical report language will state:
Minor, mild, moderate or severe aka advanced arthrosis
Technique
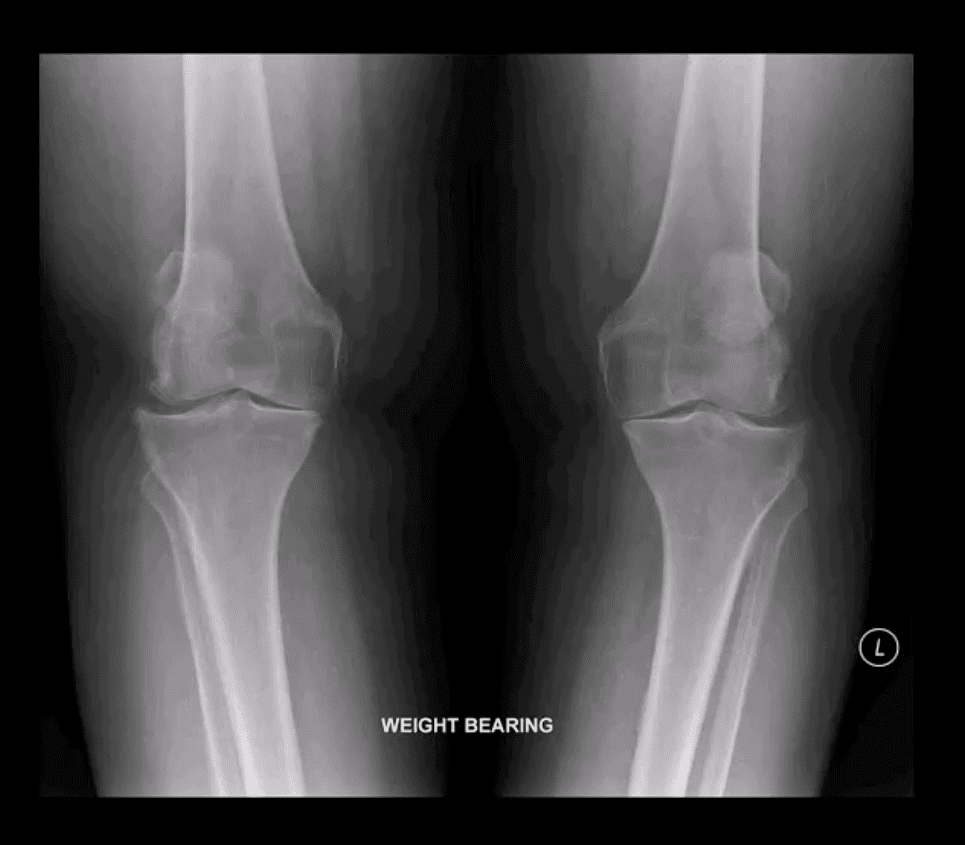
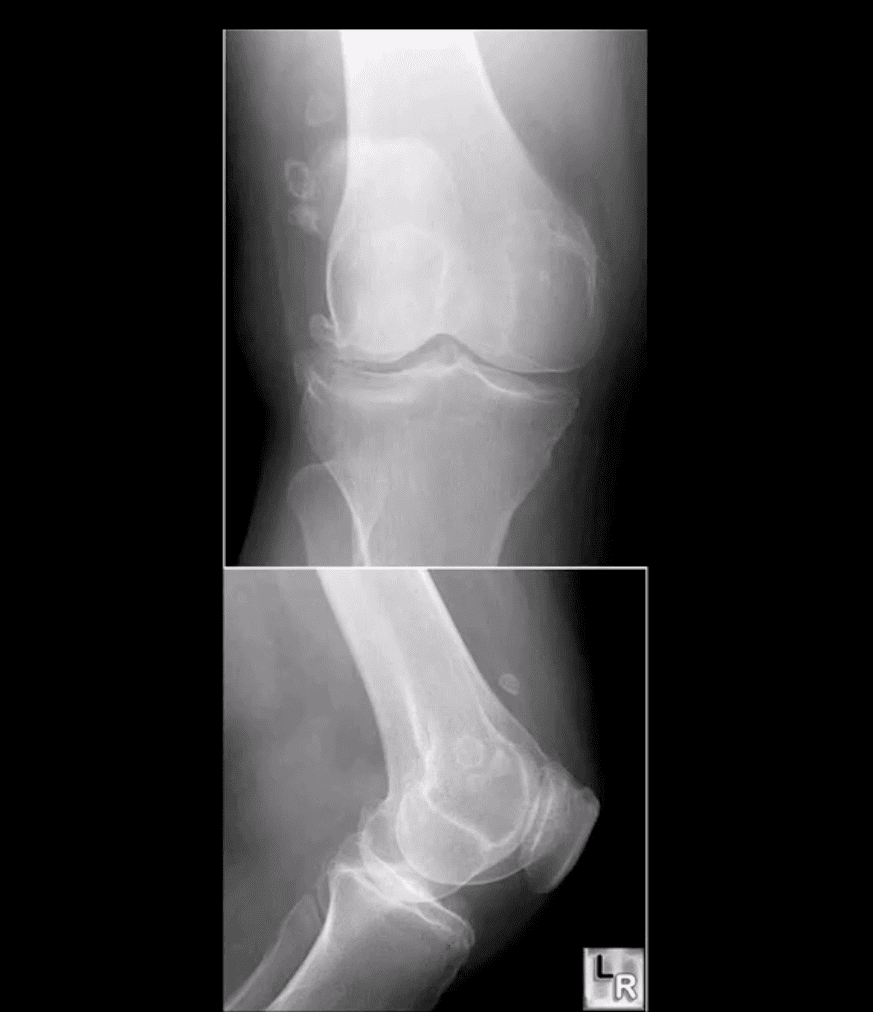
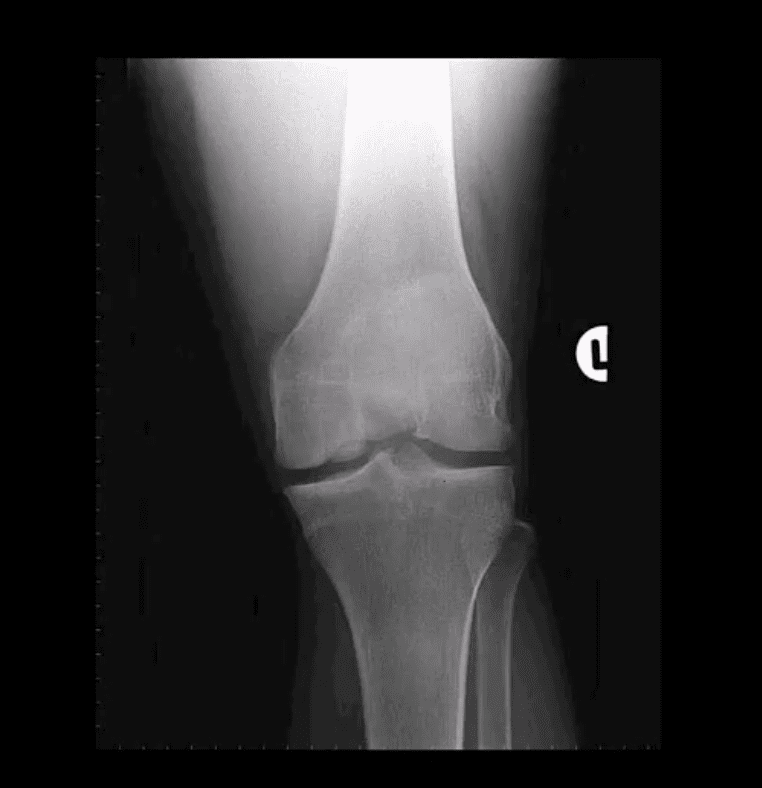
Radiography: AP weight-bearing knees: note severe JSN of the medial compartment more severely with lateral knee compartment. Osteophytes and marked genu varum deformity and bone deformation
Typically medial femorotibial compartment is affected early and more severely
The patellofemoral compartment is also affected and best visualized on the lateral and Sunrise views
Impressions: severe tri-compartmental knee arthrosis
Recommendations: referral to the orthopedic surgeon
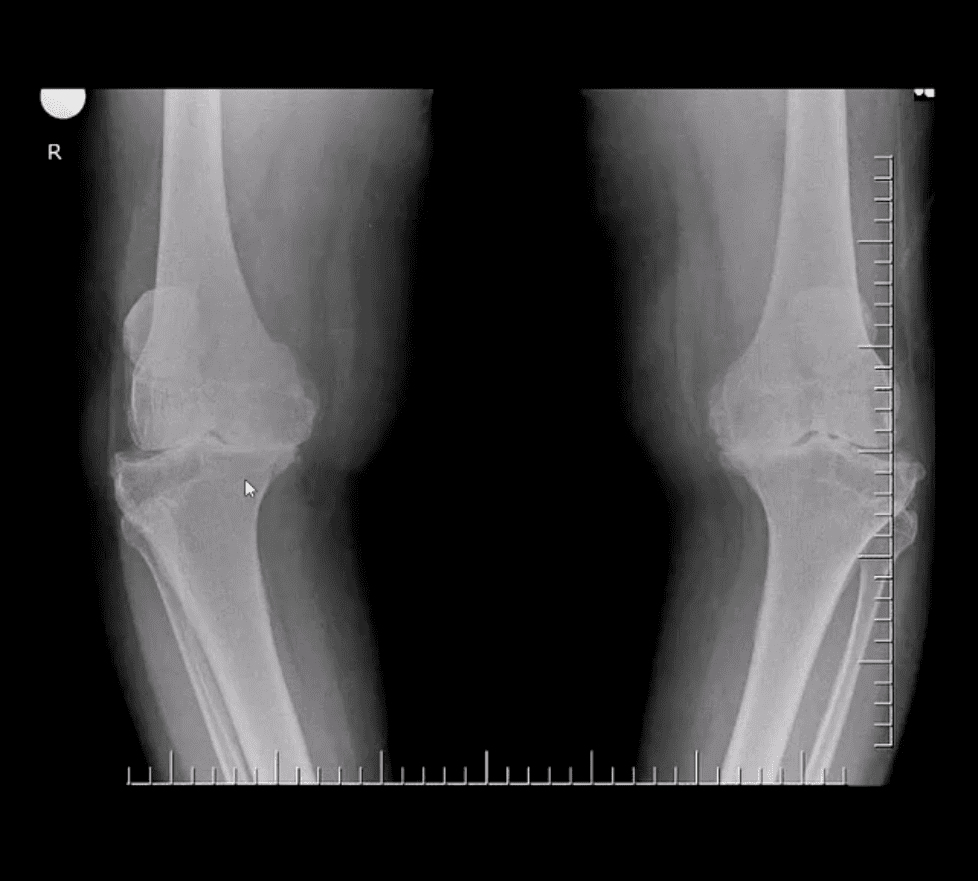
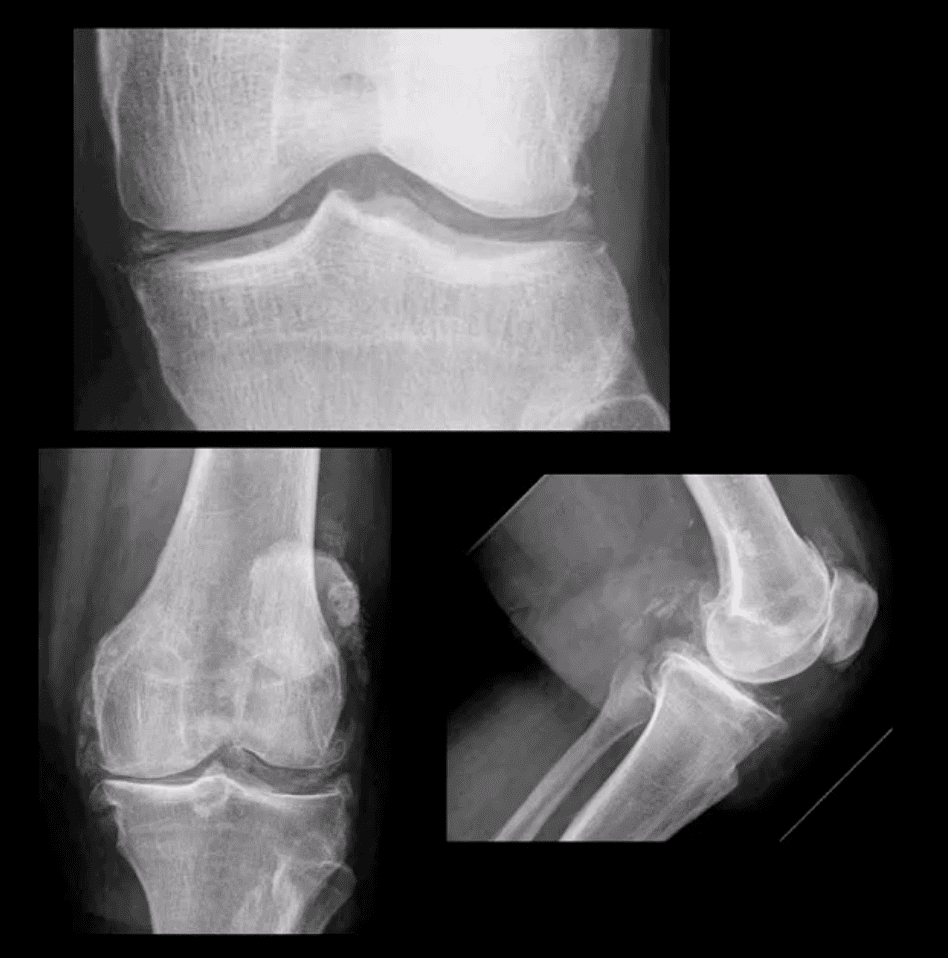
Moderate JSN
B/L AP weight-bearing view (above top image): Moderate JSN primarily of the medial femorotibial compartment. Osteophytosis, subchondral sclerosis and mild bone deformation (genu varum)
May present as asymptomatic chondrocalcinosis, CPPD arthropathy resembling DJD with pan predominance of large subchondral cysts. Often found as isolated PFJ DJD
Pseudogout with an acute attack of knee pain resembling gouty arthritis
Radiography is the 1st step and often reveals the Dx
Arthrocentesis with polarized microscopy may be helpful to DDx between CPPD and Gouty arthritis
Rheumatoid Arthritis
RA: an autoimmune systemic inflammatory disease that targets soft tissues of joints synovium, tendons/ligaments, bursae and extra-articular sites (e.g., eyes, lungs, cardiovascular system)
RA is the m/c inflammatory arthritis, 3% of women and 1% of men. Age: 30-50 F>M 3:1, but may develop at any age. True RA is uncommon in children and should not be confused with Juvenile Idiopathic Arthritis
RA most often affects small joints of the hands and feet as symmetrical arthritis (2nd 3rd MCP, 3rd PIPs, wrists & MTPs, sparing DIPs of fingers and toes)
Radiographically: RA presents with joint effusion leading to hyperemia and marginal erosions and periarticular osteoporosis. In the knee, the lateral compartment is affected more frequently leading to valgus deformity. Uniform aka concentric/symmetrical JSN affects all compartments and remains a key Dx clue
An absence of subchondral sclerosis and osteophytes. Popliteal cyst�(Baker’s cyst) may represent synovial pannus and inflammatory synovitis extending into the popliteal region that may rapture and extend into posterior leg compartment
N.B. Following initial RA joint destruction, it is not unusual to note superimposed 2nd OA
Radiography is the 1st step but early joint involvement may be undetectable by x-rays and can be helped by US and/or MRI.
Final Dx is based on Hx, clinical exam, labs, and radiology
Clinical pearls: patients with RA may present with a single knee being affected
Most patients are likely to have bilateral symmetrical hands/feet RA.
Cervical spine, particularly C1-2 is affected in 75-90% of cases throughout the course of the disease
N.B. Sudden exacerbation of joint pain in RA should not underestimate septic arthritis because patients with pre-existing RA are at higher risk of infectious arthritis. Joint aspiration may help with Dx.
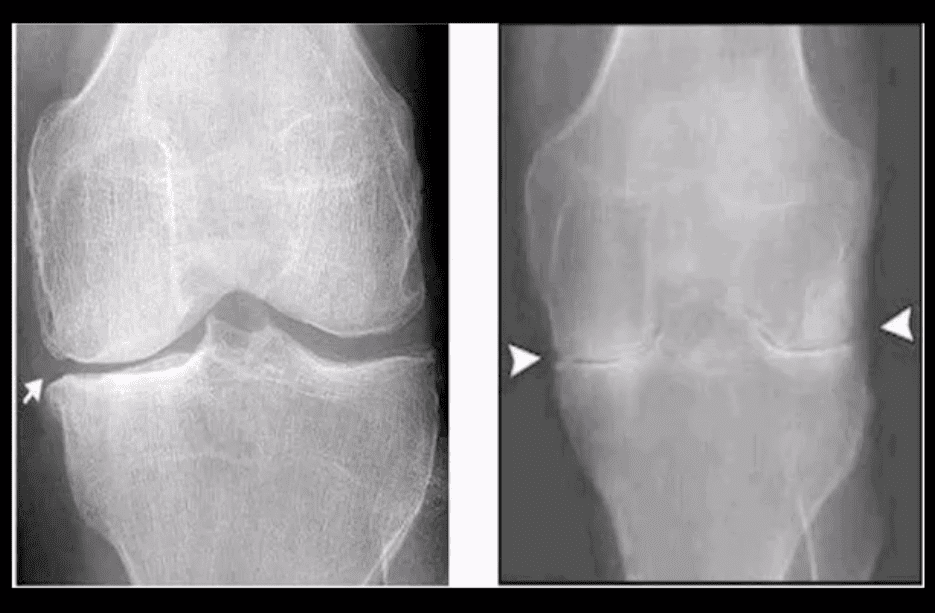
Radiographic DDx
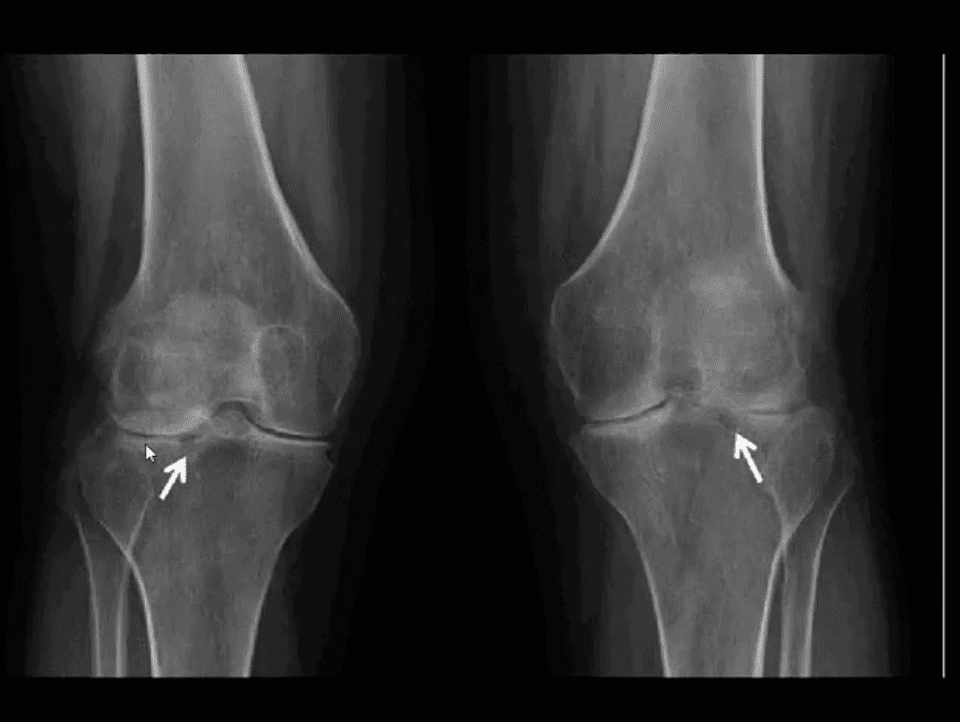
RA (above left) vs. OA (above right)
RA: concentric (uniform) joint space loss, lack of osteophytes and juxta-articular osteopenia.
Clinical Pearls: patients with RA may present radiographically with subchondral sclerosis d/t superimposed DJD. The latter feature should not be interpreted as OA but instead considered as secondary OA
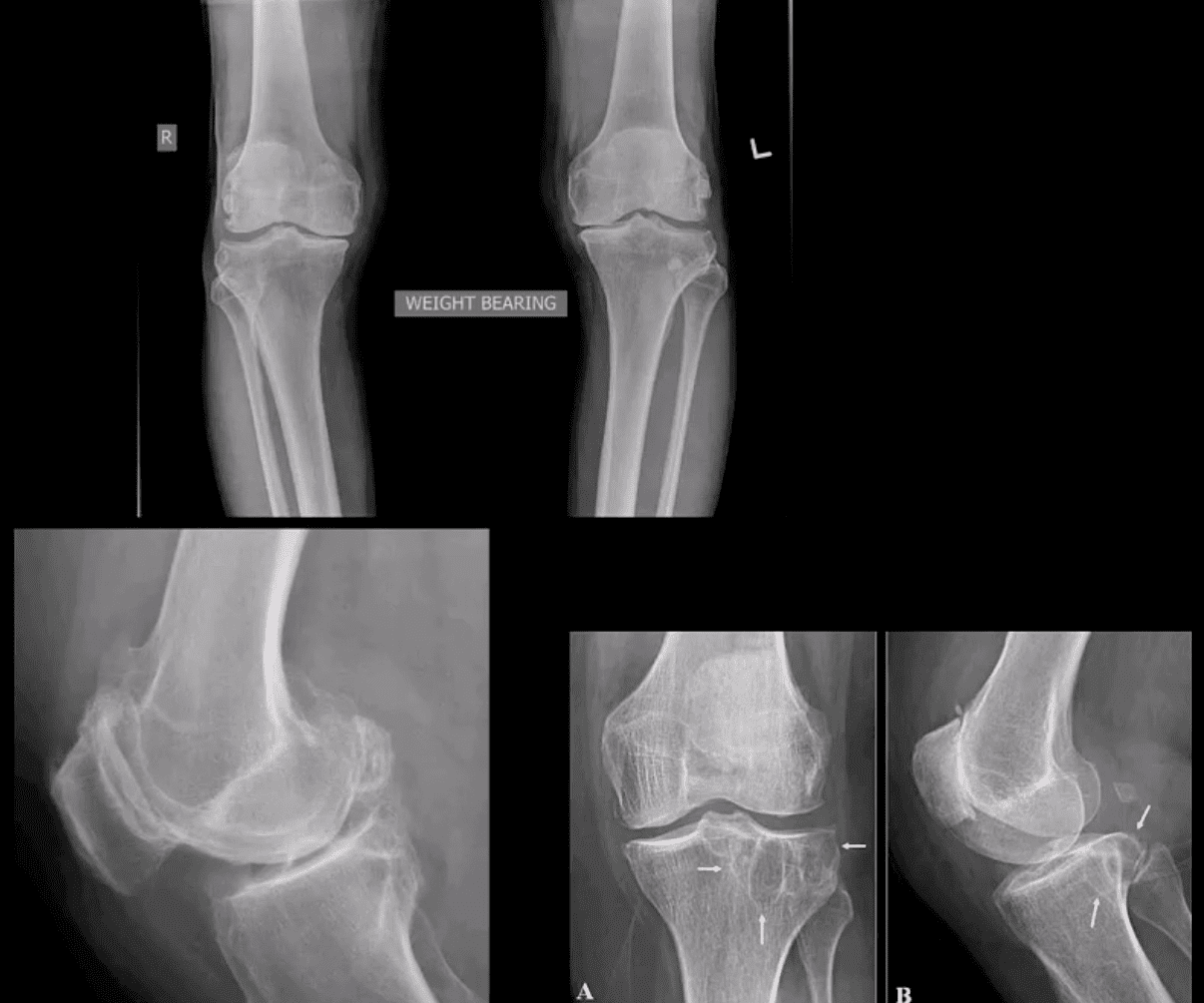
AP Knee Radiograph
Note marked uniform JSN, juxta-articular osteopenia and subchondral cystic changes
Clinical Pearls: subcortical cysts in RA will characteristically lack sclerotic rim noted in OA-associated subcortical cysts.
MRI Sensitivity
MRI is very sensitive and may aid during early Dx of RA.
T2 fat-sat or STIR and T1 + C gad contrast fat-suppressed sequences may be included
MRI Dx of RA: synovial inflammation/effusion, synovial hyperplasia, and pannus formation decreased cartilage thickness, subchondral cysts, and bone erosions
MRI is very sensitive to reveal juxt-articular bone marrow edema, a precursor to erosions
Intra-articular fibrinoid fragments known as “Rice bodies” are characteristic MR sign of RA
Note: T2 fat-sat sagittal MRI revealing large inflammatory joint effusion and pannus synovial proliferation (above arrowheads). No evidence of radiographic or MRI bone erosions present. Dx: RA
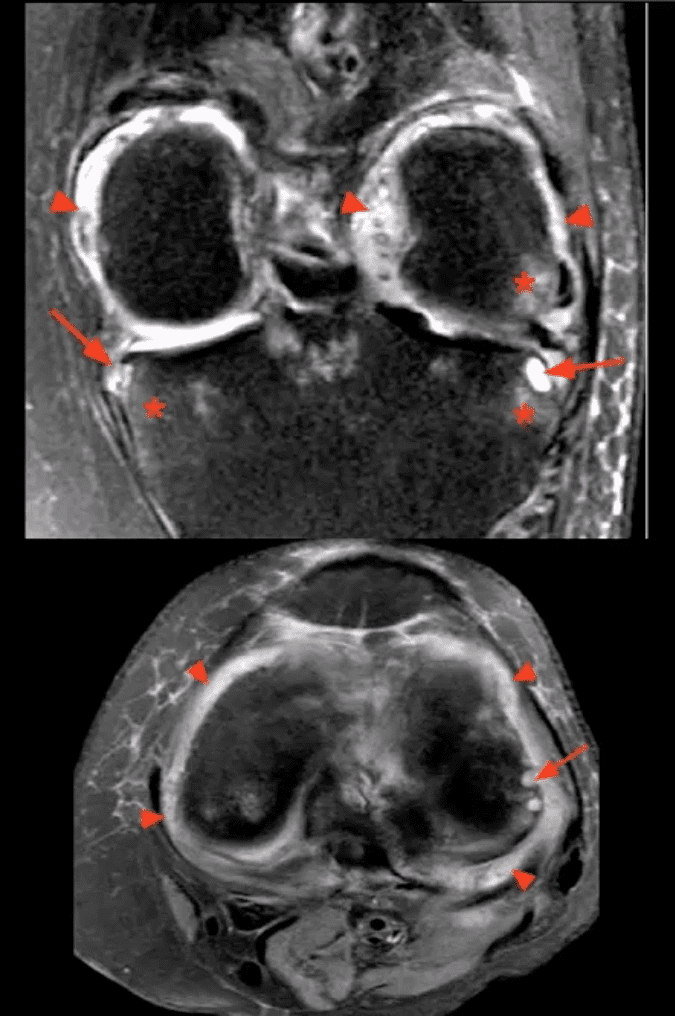
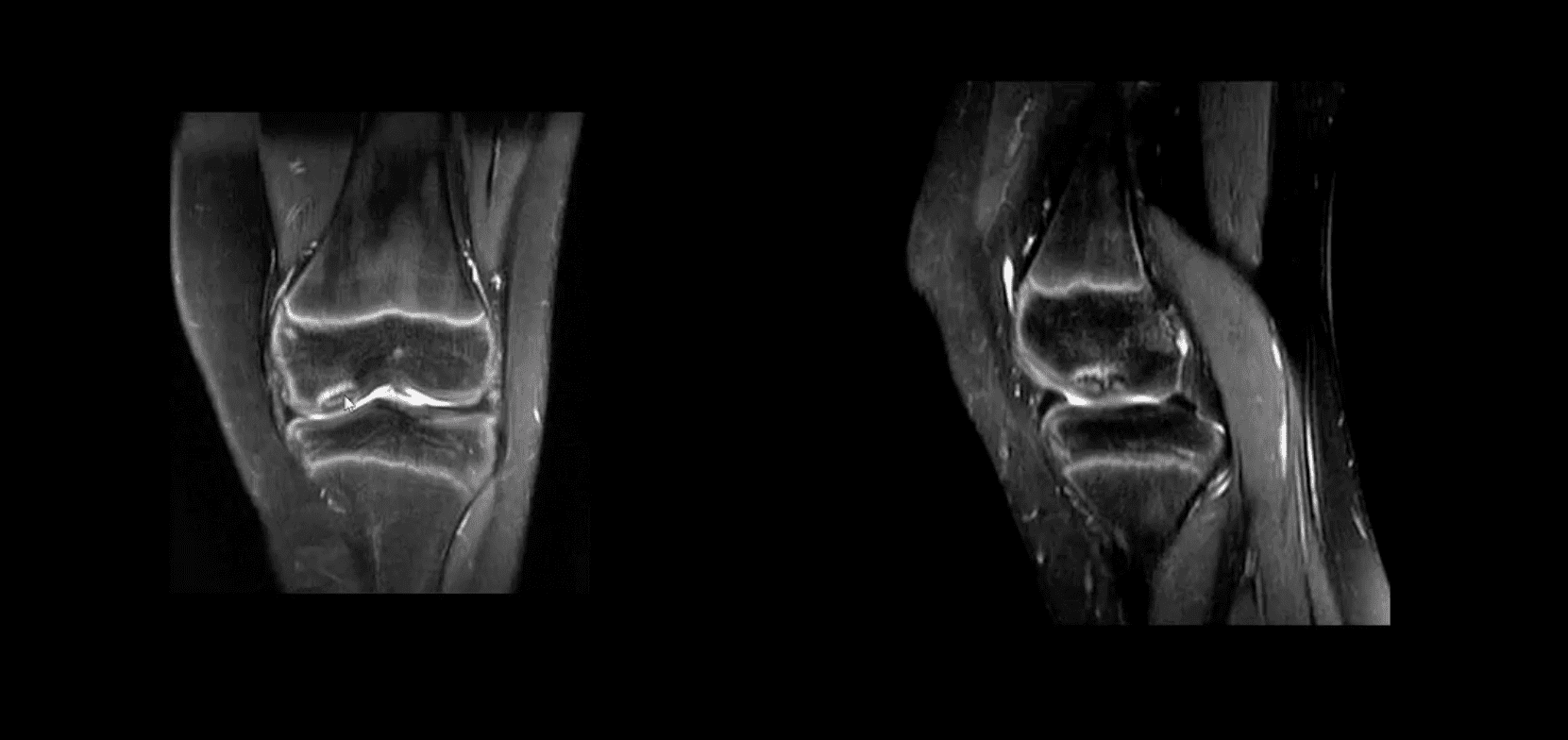
STIR MR Slices
Note: STIR MR slices in the axial (above bottom image) and coronal planes (above top image) demonstrate extensive synovitis/effusion (above arrowheads) and multiple erosions in the medial and lateral tibial plateau (above arrows)
Additionally, scattered patchy areas of bone marrow edema are noted (above asterisks) such marrow edema changes are indicative and predictive of future osseous erosions.
Additional features: note thinning and destruction of joint cartilage
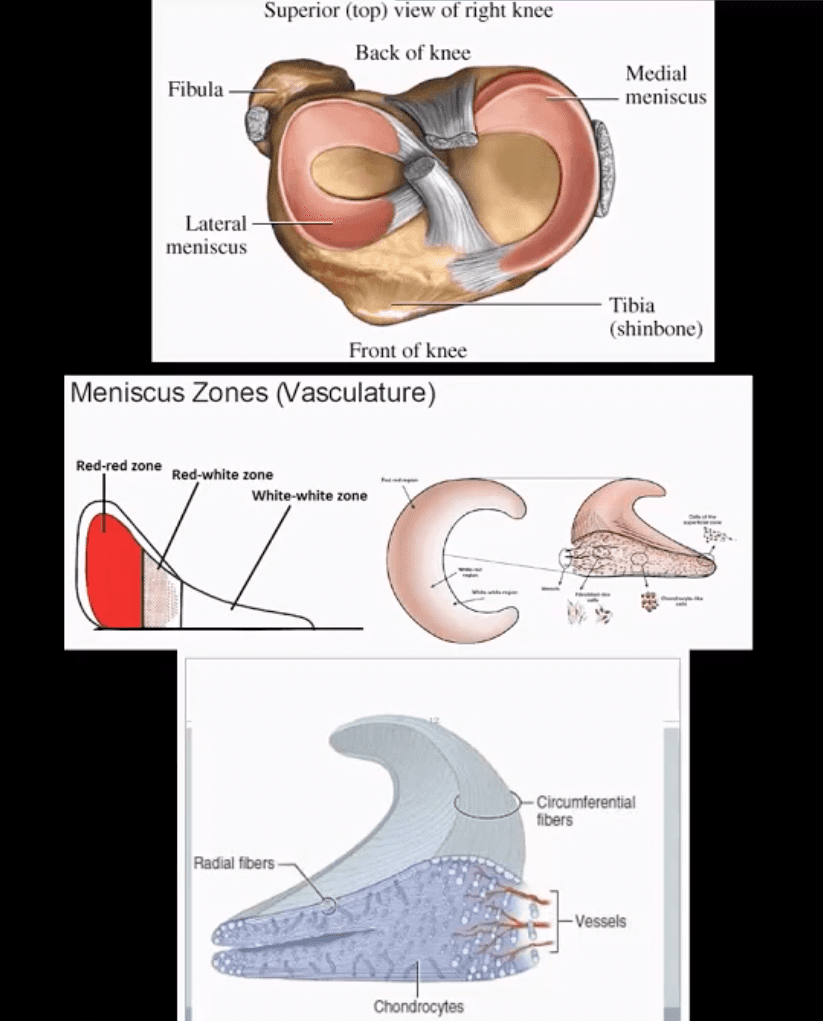
Knee pain is a common health issue among athletes and the general population alike. Although symptoms of knee pain can be debilitating and frustrating, knee pain is often a very treatable health issue. The knee is a complex structure made up of three bones: the lower section of the thighbone, the upper region of the shinbone, and the kneecap.
Powerful soft tissues, such as the tendons and ligaments of the knee as well as the cartilage beneath the kneecap and between the bones, hold these structures together in order to stabilize and support the knee. However, a variety of injuries and/or conditions can ultimately lead to knee pain. The purpose of the article below is to evaluate patients with knee pain.
Abstract
Family physicians frequently encounter patients with knee pain. Accurate diagnosis requires a knowledge of knee anatomy, common pain patterns in knee injuries, and features of frequently encountered causes of knee pain, as well as specific physical examination skills. The history should include characteristics of the patient�s pain, mechanical symptoms (locking, popping, giving way), joint effusion (timing, amount, recurrence), and mechanism of injury. The physical examination should include careful inspection of the knee, palpation for point tenderness, assessment of joint effusion, range-of-motion testing, evaluation of ligaments for injury or laxity, and assessment of the menisci. Radiographs should be obtained in patients with isolated patellar tenderness or tenderness at the head of the fibula, inability to bear weight or flex the knee to 90 degrees, or age greater than 55 years. (Am Fam Physician 2003; 68:907-12. Copyright� 2003 American Academy of Family Physicians.)
Introduction
Knee pain accounts for approximately one-third of musculoskeletal problems seen in primary care settings. This complaint is most prevalent in�physically active patients, with as many as 54 percent of athletes having some degree of knee pain each year.1 Knee pain can be a source of significant disability, restricting the ability to work or perform activities of daily living.
The knee is a complex structure (Figure 1),2 and its evaluation can present a challenge to the family physician. The differential diagnosis of knee pain is extensive but can be narrowed with a detailed history, a focused physical examination and, when indicated, the selective use of appropriate imaging and laboratory studies. Part I of this two-part article provides a systematic approach to evaluating the knee, and part II3 discusses the differential diagnosis of knee pain.
History
Pain Characteristics
The patient�s description of knee pain is helpful in focusing the differential diagnosis.4 It is important to clarify the characteristics of the pain, including its onset (rapid or insidious), location (anterior, medial, lateral, or posterior knee), duration, severity, and quality (e.g., dull, sharp, achy). Aggravating and alleviating factors also need to be identified. If knee pain is caused by an acute injury, the physician needs to know whether the patient was able to continue activity or bear weight after the injury or was forced to cease activities immediately.
Mechanical Symptoms
The patient should be asked about mechan- ical symptoms, such as locking, popping, or giving way of the knee. A history of locking episodes suggests a meniscal tear. A sensation of popping at the time of injury suggests liga- mentous injury, probably complete rupture of a ligament (third-degree tear). Episodes of giving way are consistent with some degree of knee instability and may indicate patellar sub- luxation or ligamentous rupture.
Effusion
The timing and amount of joint effusion are important clues to the diagnosis. Rapid onset (within two hours) of a large, tense effusion suggests rupture of the anterior cru- ciate ligament or fracture of the tibial plateau with resultant hemarthrosis, whereas slower onset (24 to 36 hours) of a mild to moderate effusion is consistent with meniscal injury or ligamentous sprain. Recurrent knee effusion after activity is consistent with meniscal injury.
Mechanism of Injury
The patient should be questioned about specific details of the injury. It is important to know if the patient sustained a direct blow to the knee, if the foot was planted at the time of injury, if the patient was decelerating or stopping suddenly, if the patient was landing from a jump, if there was a twisting component to the injury, and if hyperextension occurred.
A direct blow to the knee can cause serious injury. The anterior force applied to the proximal tibia with the knee in flexion (e.g., when the knee hits the dashboard in an automobile accident) can cause injury to the posterior cruciate ligament. The medial collateral ligament is most commonly injured as a result of direct lateral force to the knee (e.g., clipping in football); this force creates a val- gus load on the knee joint and can result in rupture of the medial collateral ligament. Conversely, a medial blow that creates a varus load can injure the lateral collateral ligament.
Noncontact forces also are an important cause of knee injury. Quick stops and sharp cuts or turns create significant deceleration forces that can sprain or rupture the anterior cruciate ligament. Hyperextension can result in injury to the anterior cruciate ligament or posterior cruciate ligament. Sudden twisting or pivoting motions create shear forces that can injure the meniscus. A combination of forces can occur simultaneously, causing injury to multiple structures.
Medical History
A history of knee injury or surgery is important. The patient should be asked about previous attempts to treat knee pain, including the use of medications, supporting devices, and physical therapy. The physician also should ask if the patient has a history of�gout, pseudogout, rheumatoid arthritis, or other degenerative joint diseases.
Knee pain is a common health issue which can be caused by sports injuries, automobile accident injuries, or by an underlying health issue, such as arthritis. The most common symptoms of knee injury include pain and discomfort, swelling, inflammation and stiffness. Because treatment for knee pain varies according to the cause, it’s essential for the individual to receive proper diagnosis for their symptoms. Chiropractic care is a safe and effective, alternative treatment approach which can help treat knee pain, among other health issues.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Physical Examination
Inspection and Palpation
The physician begins by comparing the painful knee with the asymptomatic knee and inspecting the injured knee for erythema, swelling, bruising, and discoloration. The mus- culature should be symmetric bilaterally. In particular, the vastus medialis obliquus of the quadriceps should be evaluated to determine if it appears normal or shows signs of atrophy.
The knee is then palpated and checked for pain, warmth, and effusion. Point tenderness should be sought, particularly at the patella, tibial tubercle, patellar tendon, quadriceps tendon, anterolateral and anteromedial joint line, medial joint line, and lateral joint line. Moving the patient�s knee through a short arc of motion helps identify the joint lines. Range of motion should be assessed by extending and flexing the knee as far as possible (normal range of motion: extension, zero degrees; flex- ion, 135 degrees).5
Patellofemoral Assessment
An evaluation for effusion should be conducted with the patient supine and the injured knee in extension. The suprapatellar pouch should be milked to determine whether an effusion is present.
Patellofemoral tracking is assessed by observing the patella for smooth motion while the patient contracts the quadriceps muscle. The presence of crepitus should be noted during palpation of the patella.
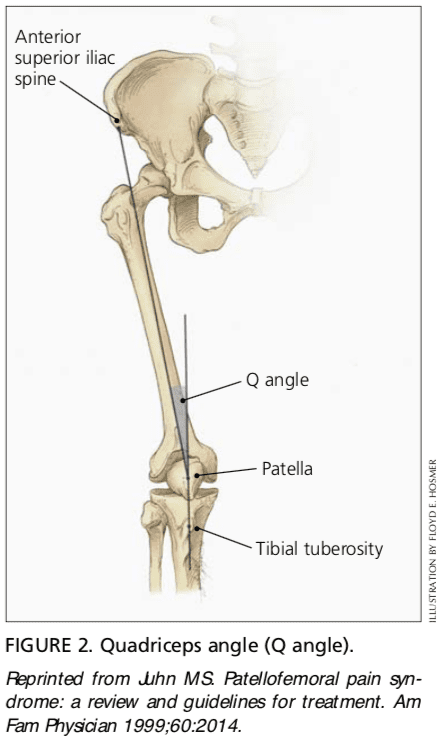
The quadriceps angle (Q angle) is determined by drawing one line from the anterior superior iliac spine through the center of the patella and a second line from the center of the patella through the tibial tuberosity (Figure 2).6 A Q angle greater than 15 degrees is a predisposing factor for patellar subluxation (i.e., if the Q angle is increased, forceful contraction of the quadriceps muscle can cause the patella to sublux laterally).
A patellar apprehension test is then performed. With fingers placed at the medial aspect of the patella, the physician attempts to sublux the patella laterally. If this maneuver reproduces the patient�s pain or a giving-way sensation, patellar subluxation is the likely cause of the patient�s symptoms.7 Both the superior and inferior patellar facets should be palpated, with the patella subluxed first medially and then laterally.
Cruciate Ligaments
Anterior Cruciate Ligament. For the anterior drawer test, the patient assumes a supine position with the injured knee flexed to 90 degrees. The physician fixes the patient�s foot in slight external rotation (by sitting on the foot) and then places thumbs at the tibial tubercle and fingers at the posterior calf. With the patient�s hamstring muscles relaxed, the physician pulls anteriorly and assesses anterior displacement of the tibia (anterior drawer sign).
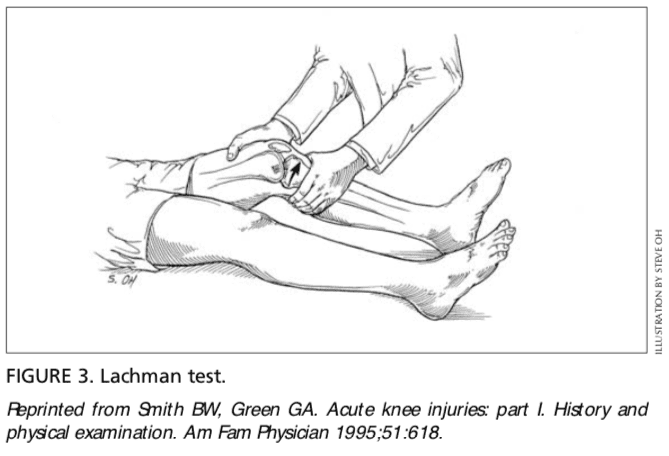
The Lachman test is another means of assessing the integrity of the anterior cruciate ligament (Figure 3).7 The test is performed with the patient in a supine position and the injured knee flexed to 30 degrees. The physician stabilizes the distal femur with one hand, grasps the proximal tibia in the other hand, and then attempts to sublux the tibia anteriorly. Lack of a clear end point indicates a positive Lachman test.
Posterior Cruciate Ligament. For the posterior drawer test, the patient assumes a supine position with knees flexed to 90 degrees. While standing at the side of the examination table, the physician looks for posterior displacement of the tibia (posterior sag sign).7,8 Next, the physician fixes the patient�s foot in neutral rotation (by sitting on the foot), positions thumbs at the tibial tubercle, and places fingers at the posterior calf. The physician then pushes posteriorly and assesses for posterior displacement of the tibia.
Collateral Ligaments
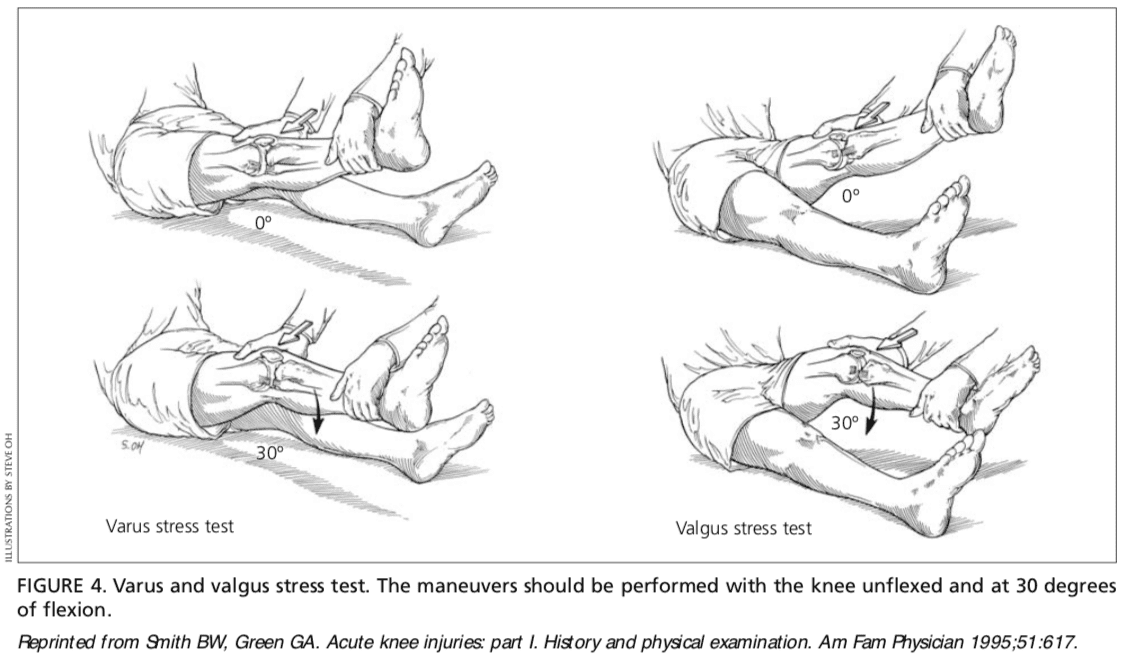
Medial Collateral Ligament. The valgus stress test is performed with the patient�s leg slightly abducted. The physician places one hand at the lateral aspect of the knee joint and the other hand at the medial aspect of the distal tibia. Next, valgus stress is applied to the knee at both zero degrees (full extension) and 30 degrees of flexion (Figure 4)7. With the knee at zero degrees (i.e., in full extension), the posterior cruciate ligament and the articulation of the femoral condyles with the tibial plateau should stabilize the knee; with the knee at 30 degrees of flexion, application of valgus stress assesses the laxity or integrity of the medial collateral ligament.
Lateral Collateral Ligament. To perform the varus stress test, the physician places one hand at the medial aspect of the patient�s knee and the other hand at the lateral aspect of the distal fibula. Next, varus stress is applied to the knee, first at full extension (i.e., zero degrees), then with the knee flexed to 30 degrees (Figure 4).7 A firm end point indicates that the collateral ligament is intact, whereas a soft or absent end point indicates complete rupture (third-degree tear) of the ligament.
Menisci
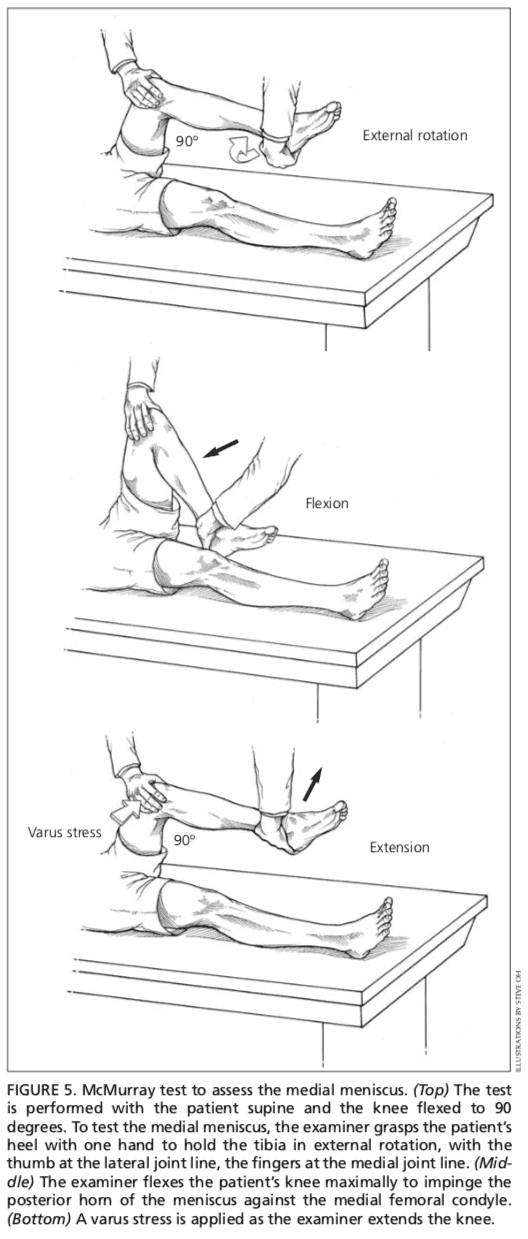
Patients with injury to the menisci usually demonstrate tenderness at the joint line. The McMurray test is performed with the patient lying supine9 (Figure 5). The test has been described variously in the literature, but the author suggests the following technique.
The physician grasps the patient�s heel with one hand and the knee with the other hand. The physician�s thumb is at the lateral joint line, and fingers are at the medial joint line. The physician then flexes the patient�s knee maximally. To test the lateral meniscus, the tibia is rotated internally, and the knee is extended from maximal flexion to about 90 degrees; added compression to the lateral meniscus can be produced by applying valgus stress across the knee joint while the knee is�being extended. To test the medial meniscus, the tibia is rotated externally, and the knee is extended from maximal flexion to about 90 degrees; added compression to the medial meniscus can be produced by placing varus stress across the knee joint while the knee is degrees of flexion. A positive test produces a thud or a click, or causes pain in a reproducible portion of the range of motion.
Because most patients with knee pain have soft tissue injuries, plain-film radiographs generally are not indicated. The Ottawa knee rules are a useful guide for ordering radiographs of the knee10,11.
If radiographs are required, three views are usually sufficient: anteroposterior view, lateral view, and Merchant�s view (for the patellofemoral joint).7,12 Teenage patients who report chronic knee pain and recurrent knee effusion require a notch or tunnel view (posteroanterior view with the knee flexed to 40 to 50 degrees). This view is necessary to detect radiolucencies of the femoral condyles (most�commonly the medial femoral condyle), which indicate the presence of osteochondritis dissecans.13
Radiographs should be closely inspected for signs of fracture, particularly involving the patella, tibial plateau, tibial spines, proximal fibula, and femoral condyles. If osteoarthritis is suspected, standing weight-bearing radiographs should be obtained.
Laboratory Studies
The presence of warmth, exquisite tenderness, painful effusion, and marked pain with even slight range of motion of the knee joint is consistent with septic arthritis or acute inflammatory arthropathy. In addition to obtaining a complete blood count with differential and an erythrocyte sedimentation rate (ESR), arthro- centesis should be performed. The joint fluid should be sent to a laboratory for a cell count with differential, glucose and protein measure- ments, bacterial culture and sensitivity, and polarized light microscopy for crystals.
Because a tense, painful, swollen knee may present an unclear clinical picture, arthrocentesis may be required to differentiate simple effusion from hemarthrosis or occult osteochondral fracture.4 A simple joint effusion produces clear, straw-colored transudative fluid, as in a knee sprain or chronic meniscal injury. Hemarthrosis is caused by a tear of the anterior cruciate ligament, a fracture or, less commonly, an acute tear of the outer portion of the meniscus. An osteochondral fracture causes hemarthrosis, with fat globules noted in the aspirate.
Rheumatoid arthritis may involve the knee joint. Hence, serum ESR and rheumatoid factor testing are indicated in selected patients.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
In conclusion, knee pain is a common health issue which occurs due to a variety of injuries and/or conditions, such as sports injuries, automobile accidents, and arthritis, among other problems. Treatment of knee pain depends largely on the source of the symptoms. Therefore, it is essential for the individual to seek immediate medical attention to receive a diagnosis.
Chiropractic care is an alternative treatment option which focuses on the treatment of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Rosenblatt RA, Cherkin DC, Schneeweiss R, Hart LG. The content of ambulatory medical care in the United States. An interspecialty comparison. N Engl J Med 1983;309:892-7.
2. Tandeter HB, Shvartzman P, Stevens MA. Acute knee injuries: use of decision rules for selective radiograph ordering. Am Fam Physician 1999;60: 2599-608.
3. Calmbach WL, Hutchens M. Evaluation of patients presenting with knee pain: part II. Differential diag- nosis. Am Fam Physician 2003;68:917-22
4. Bergfeld J, Ireland ML, Wojtys EM, Glaser V. Pin- pointing the cause of acute knee pain. Patient Care 1997;31(18):100-7.
6. Juhn MS. Patellofemoral pain syndrome: a review and guidelines for treatment. Am Fam Physician 1999;60:2012-22.
7. Smith BW, Green GA. Acute knee injuries: part I. History and physical examination. Am Fam Physi- cian 1995;51:615-21.
8. Walsh WM. Knee injuries. In: Mellion MB, Walsh WM, Shelton GL, eds. The team physician�s hand- book. 2d ed. St. Louis: Mosby, 1997:554-78.
9. McMurray TP. The semilunar cartilage. Br J Surg 1942;29:407-14.
10. Stiell IG, Wells GA, Hoag RH, Sivilotti ML, Cacciotti TF, Verbeek PR, et al. Implementation of the Ottawa knee rule for the use of radiography in acute knee injuries. JAMA 1997;278:2075-9.
11. Stiell IG, Greenberg GH, Wells GA, McKnight RD, Cwinn AA, Caciotti T, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Ann Emerg Med 1995;26:405-13.
12. Sartoris DJ, Resnick D. Plain film radiography: rou- tine and specialized techniques and projections. In: Resnick D, ed. Diagnosis of bone and joint disor- ders. 3d ed. Philadelphia: Saunders:1-40.
13. Schenck RC Jr, Goodnight JM. Osteochondritis dis- secans. J Bone Joint Surg [Am] 1996;78:439-56.
More than 80% of children will experience at least one ear infection before they turn three-years-old. Ear infection is one of the top reasons that parents seek medical treatment for their children, causing fever, irritability, and ear pain. Also known as otitis media, an ear infection is caused by fluid buildup behind the eardrum that results in inflammation. It is typically caused by bacteria. According to the Centers for Disease Control (CDC), antibiotics are not a recommended treatment for most ear infections.
Types of Childhood Ear Infections
There are three types of childhood ear infections. Each type has its own distinct set of symptoms that can aid in diagnosis and treatment.
Otitis Media with Effusion (OME) � This results from a fluid buildup that occurs in the middle ear although there are no symptoms or signs of infection. While it can happen when the fluid remains after an ear infection has run its course, other causes may include allergies, previous respiratory infections (like cold or flu), elevation changes, environmental irritants, air travel, and drinking while lying down (usually on the back). Antibiotics are not sufficient for this type of ear infection.
Acute Otitis Media (AOM) � This type of ear infection is the most common, affecting the middle ear, and is marked by infection, swelling, and trapped fluid behind the eardrum. Symptoms may include an earache and fever. It may be seasonal (most earaches occur in the winter and fall months), environmental pollutants (second-hand smoke), age (children under two years of age are more prone to earaches), and attendance at daycare. AOM may also be caused when the fluid from OME becomes infected. Antibiotics are sometimes prescribed for more acute cases.
Chronic Otitis Media with Effusion (COME) � This can be a serious condition if left untreated. It occurs when fluid in the middle ear continuously returns or remains trapped for a long time. Often infection is not present, and there are no symptoms. Children with COME have a more difficult time fighting new infections, and they may suffer from hearing damage or loss.
Risk Factors for Ear Infections
Children are more prone to ear infections than adults. This is because the eustachian tubes (connecting the middle ear to the upper part of the throat) are smaller in children and more level. This means that the fluid does not drain as easily and if a respiratory illness like a cold causes the eustachian tubes to become blocked or swollen, the fluid may become trapped because it can�t drain. Other risk factors include:
Drinking while laying on their back
Respiratory illness such as a cold
Allergies
Air travel (changes in air pressure)
Cigarette smoke and other environmental pollutants
Changes in elevation
Childhood Ear Infection Symptoms and Signs
Most of the time children get ear infections before they are old enough to verbalize their discomfort so parents must rely on telltale sure signs and symptoms.
Crying and fussiness
Fever (most prevalent in younger children and infants)
Pulling or tugging at the ears
Difficulty hearing or failure to respond to quiet sounds
Fluid draining from the ear
Difficulty sleeping
Balance problems or clumsiness
Chiropractic for Ear Infections
Several studies have shown Chiropractic for ear infections to be an effective, natural, antibiotic-free treatment. While full spine adjustments are commonly used, other techniques include occipital subluxation, atlas subluxation, and axis subluxations.
Chiropractic care not only treats ear infections, but it also improves their overall health and ability to function. It has a strong focus on whole-body wellness so the chiropractor may recommend diet and lifestyle adjustments in addition to treatment. Parents need to realize that they have a choice when it comes to the type of care their children receive for ear infections and other kinds of illnesses.
The tendons are powerful soft tissues which connect the muscles to the bones. One of these tendons, the quadriceps tendon, works together with the muscles found at the front of the thigh in order to straighten the leg. A quadriceps tendon rupture can affect an individual’s quality of life.
A quadriceps tendon rupture can be a debilitating injury and it usually requires rehabilitation and surgical interventions to restore knee function. These type of injuries are rare. Quadriceps tendon ruptures commonly occur among athletes who perform jumping or running sports.
Quadriceps Tendon Rupture Description
The four quadriceps muscles come together above the kneecap, or patella, to form the quadriceps tendon. The quadriceps tendon joins the quadriceps muscles into the patella. The patella is connected to the shinbone, or tibia, by the patellar tendon. Working collectively, the quadriceps muscles, the quadriceps tendon, and the patellar tendon, straighten the knee.
A quadriceps tendon rupture can be partial or complete. Many partial tears don’t completely disrupt the soft tissues. However, a full tear will divide the soft tissues�into two parts. If the quadriceps tendon ruptures entirely, the muscle is no longer attached to the kneecap or patella. As a result, the knee is unable to straighten�out when the quadriceps muscles contract.
Quadriceps Tendon Rupture Causes
A quadriceps tendon rupture frequently occurs due to an increased load on the leg where the foot is planted and the knee is somewhat flexed. By way of instance, when landing from an awkward jump, the power is too much for the soft tissues to bear, causing a partial or complete tear. Tears may also be due to falls, direct impacts to the knee, and lacerations or cuts.
A weakened quadriceps tendon is also more likely to rupture. Several factors may result in tendon weakness, including quadriceps tendinitis, the inflammation of the quadriceps tendon, called quadriceps tendinitis. Quadriceps tendinitis is one of the most common sports injuries in athletes who participate in sports or physicial�activities which involve jumping.
Weakened soft tissues may also be brought on by diseases that interrupt blood flow to the knee or patella. Utilizing corticosteroids and some antibiotics have also been connected to weakness associated with quadriceps tendon ruptures. Immobilization for an extended period of time can also decrease strength in the quadriceps tendons. Finally, quadriceps tendon ruptures can occur due to dislocations and/or surgery.
Quadriceps Tendon Rupture Symptoms
A popping or tearing feeling is one of the most common symptoms associated with a quadriceps tendon rupture. Pain followed by swelling and inflammation of the knee�might make the individual unable to straighten out their knee. Other symptoms of a quadriceps tendon rupture include:
An indentation at the top of the kneecap or patella of the affected site
Bruising
Tenderness
Cramping
Sagging or drooping of the kneecap or patella where the tendon tore
Difficulty walking because the knee is buckling or giving away
Quadriceps Tendon Rupture Evaluation
The healthcare professional will perform an evaluation to diagnose a quadriceps tendon rupture by first discussing the patient’s symptoms�and medical history.�After talking about the patient’s symptoms and medical history, the doctor will conduct a comprehensive evaluation of the knee.
To ascertain the precise cause of the patient’s symptoms, the healthcare professional will examine how well it is possible to stretch, or straighten,�the knee. Although this area of the evaluation can be debilitating, it’s essential to diagnose a quadriceps tendon rupture.
To verify a quadriceps tendon rupture diagnosis, the doctor may order some imaging tests, like an x-ray or magnetic resonance imaging, or MRI, scan. The kneecap moves from place once the quadriceps tendon ruptures. This can be quite evident on a sideways x-ray perspective of the knee.
Complete tears may frequently be identified with x-rays alone. The MRI can reveal the quantity of tendon torn along with the positioning of the tear. From time to time, an MRI will also rule out another injury with similar symptoms. Diagnostic imaging is helpful in the evaluation of sports injuries.
The quadriceps tendon is the large tendon found just above the kneecap, or patella, which allows us to straighten out our knee. While the quadriceps tendon is a strong, fibrous cord which can withstand tremendous amounts of force, sports injuries or other health issues may lead to a quadriceps tendon rupture. Quadriceps tendon ruptures are debilitating problems which can affect a patient’s quality of life.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Quadriceps Tendon Rupture Treatment
Non-Surgical Treatment
A majority of partial tears react well to non-surgical treatment approaches. The doctor may advise the patient to utilize a knee immobilizer or brace to allow the quadriceps tendon to heal. Crutches will help avoid placing weight onto the leg. A knee immobilizer or brace is used�for 3 to 6 months.
Once the initial pain, swelling, and inflammation have�decreased, alternative treatment options, such as chiropractic care and physical therapy, can be utilized. A doctor of chiropractic, or chiropractor, utilizes spinal adjustments and manual manipulations to carefully correct any spinal misalignments, or subluxations, which may be causing problems.
Furthermore, chiropractic care and physical therapy can provide lifestyle modifications, including physical activity and exercise programs to help speed up the recovery process. The patient may be recommended a variety of stretches and exercises to improve strength, flexibility and mobility. The healthcare professional will determine when it’s safe to return-to-play.
Surgical Treatment
Many individuals with complete tears require surgery to repair a quadriceps tendon rupture. Surgical interventions depend on the patient’s age, actions, and prior level of function. Surgery for quadriceps tendon ruptures involves re-attaching the tendon to the kneecap or patella. Surgery is carried out with regional spinal anesthetic or general anesthetic.
To reattach the tendon, sutures are put in the tendon and then threaded through drill holes at the kneecap. The stitches are attached in the base of the kneecap. The�physician will tie the sutures to find the ideal tension in the kneecap or patella. This will also make sure that the place of the kneecap closely matches that of the uninjured patella or kneecap.
A knee immobilizer, brace or a long leg cast may be utilized following the surgery. The patient may be allowed to set weight on their leg by means of crutches. Stretches and exercises are added into a rehabilitation program by a chiropractor or physical therapist after a surgical intervention.
The precise timeline for chiropractic care and physical therapy following a surgery for those patients that require it will be individualized personally. The patient’s rehabilitation program will be contingent upon the kind of tear, their surgery, medical condition, along with other requirements.
Conclusion
The majority of patients can return to their original routines after recovering from a quadriceps tendon rupture. The individual’s return will be addressed very carefully by the healthcare professional.�The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
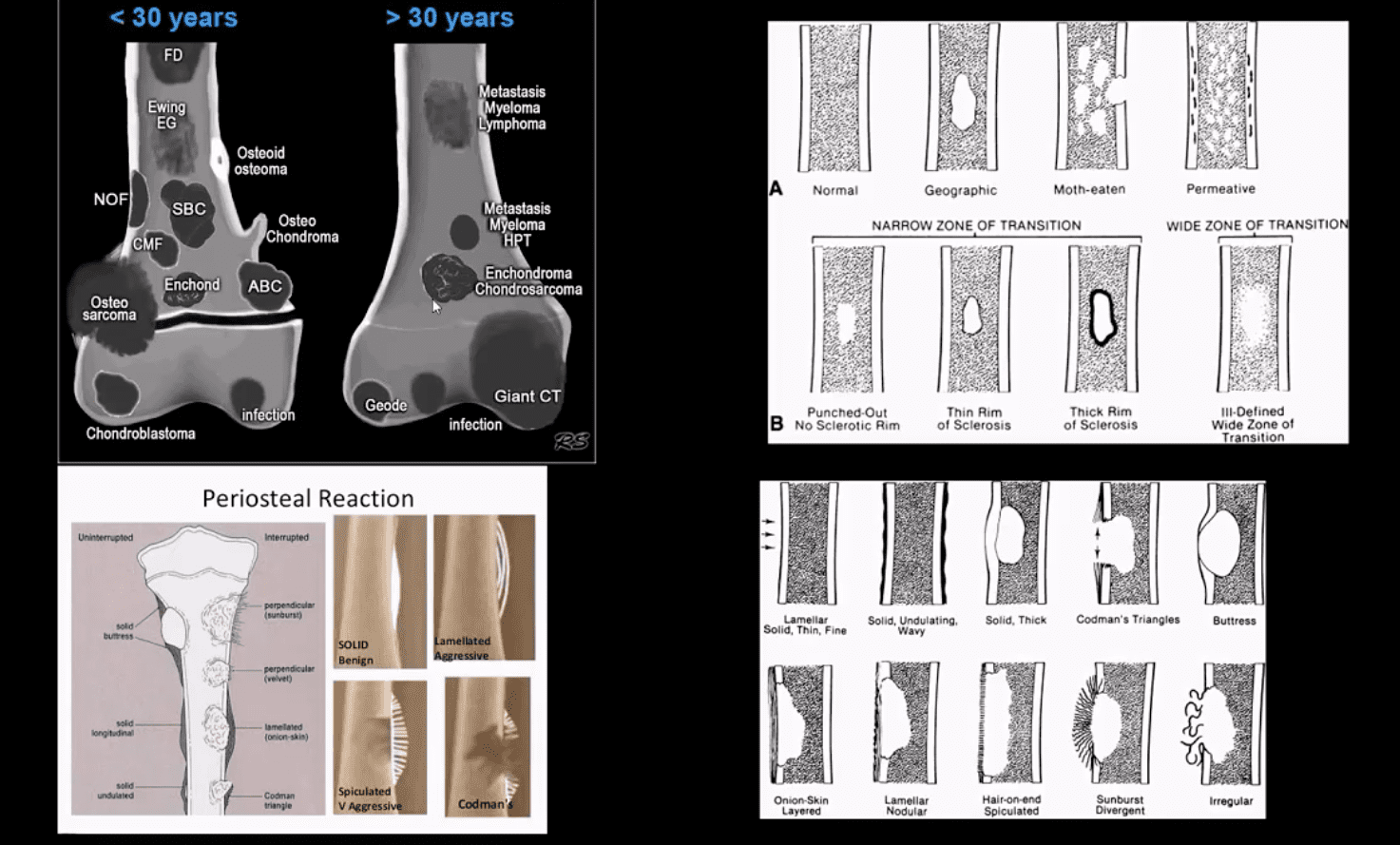
Bone neoplasms and tumor-like conditions affecting the knee can be benign or malignant. Age at Dx is crucial for DDx
In patients <40: Benign bone neoplasms: Osteochondroma, Enchondroma are relatively frequent
Fibrous cortical defect (FCD) & Non-ossifying fibroma (NOF) are particularly frequent in children
Giant cell tumor (GCT) is the m/c benign neoplasm of the knee in patients between 20-40 years of age
Malignant bone neoplasms in <40: m/c Osteosarcoma and 2nd m/c Ewing sarcoma
In patients >40: malignant neoplasms: m/c are secondaries d/t bone metastasis. Primary bone malignancy:�the m/c
Multiple Myeloma (MM). Less frequently:�a 2nd�peak of Osteosarcoma (post-radiation or Paget�s), Fibrosarcoma or Malignant�Fibrous�Histiocytoma�(MFH) of bone.
Clinically: knee pain, pathological fracture
Some tumor-like conditions like FCD/Non-ossifying fibroma are asymptomatic and may regress spontaneously. Occasionally NOF may present with pathologic fracture. N.B. any knee/bone pain in a child/adolescents should be�treated with clinical suspicion and adequately investigated.
Imaging: 1st step: radiography
MRI with T1+C is crucial for lesion characterization/regional extent, staging and pre-operative planning. CT may�help with pathologic Fxs detection. If malignant bone neoplasms considered, CXR/CT, PET-CT to investigate�metastatic spread and staging are important
Imaging Approach Bone Neoplasms
Approach to imaging Dx of bone neoplasms includes age, bone location (epiphysis vs. metaphysis vs. diaphysis), zone of transition surrounding the lesion, periosteal response, type of matrix, permeating or moth-eaten destruction vs. sclerotic, ground-glass, osteoid, cartilaginous matrix, soft tissue invasion, etc.
Key x-radiography features to DDx benign vs. malignant bone neoplasm:
Zone of transition: lesion is geographic with a narrow zone of transition vs. ill-defined wide zone of transition suggesting aggressive bone resorption
What type of bone destruction occurred: soap-bubbly appearance vs. osteolytic vs. osteosclerotic changes
Is there a round-glass matrix? Is there a well-defined rim of the sclerotic border with septations potentially suggesting slow growth and encapsulation like most benign processes.
Periosteal proliferation: solid vs. aggressive spiculated/sunburst/hair-on-end with local soft tissue invasion and Codman triangle (study next slide)
FCD & NOF
FCD & NOF or more appropriately Fibroxanthoma of the bone are benign bone processes that m/c seen in children. DDx based on the size with FCD presenting as <3-cm and NOF >3cm lesion composed of a fibrous heterogeneous matrix. FCD are asymptomatic and may regress in many cases. Some may progress to NOF. Location: identified in the knee region as an eccentric cortical based lesion.
FCD must be DDx from an avulsive irregularity d/t repeated stress along Linea aspera by extensors muscles
Dx: radiography
Management: leave-me-alone lesion. Occasionally NOF may progress and lead to pathologic fracture requiring orthopedic consult
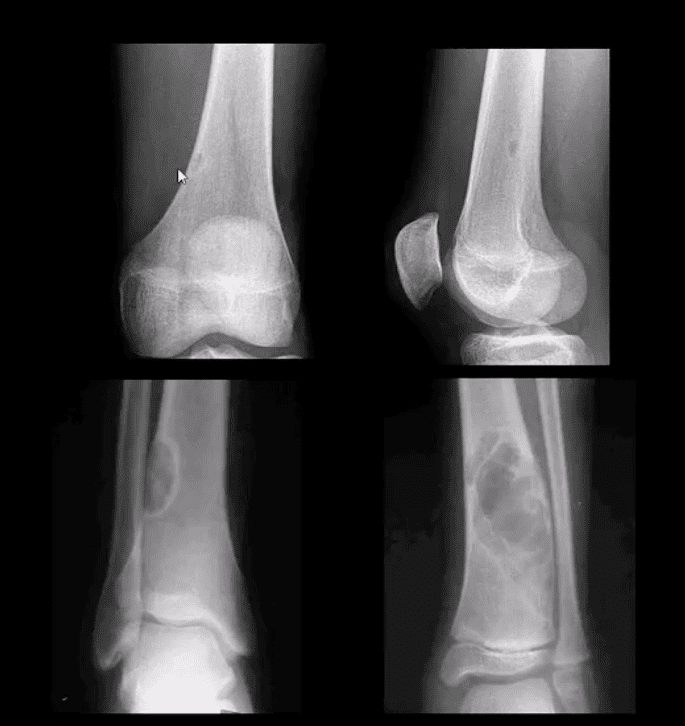
Osteochondroma
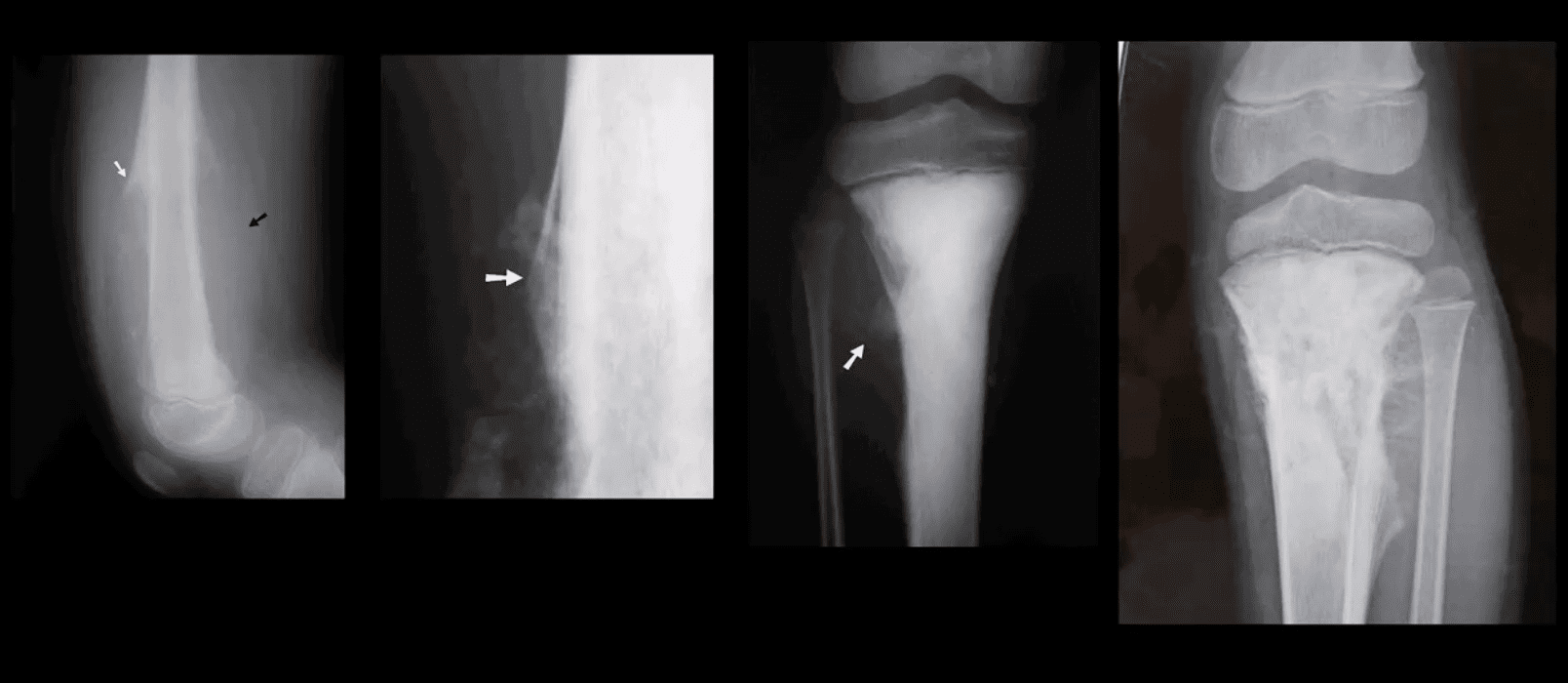
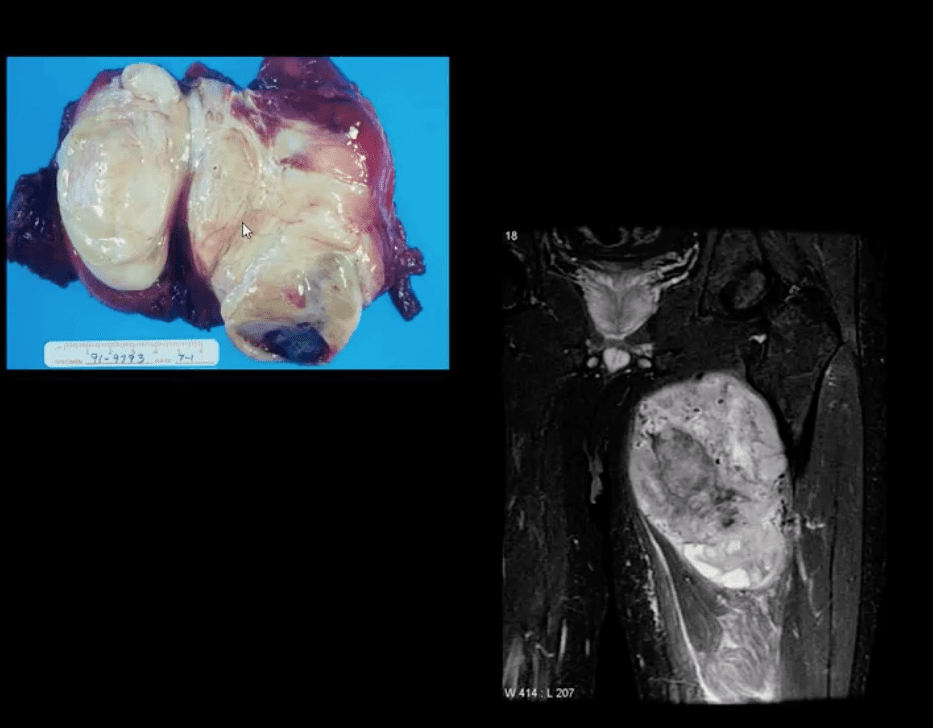
Osteochondroma: m/c benign bone neoplasm. Knee is the m/c location. Contains all bone elements with a cartilaginous cap. Presented as pedunculated or sessile bone exostosis pointing away from the joint.
1% malignant degeneration to chondrosarcoma if solitary lesion and 10-15% in cases of HME
Other complications: fracture (top left image) pseudoaneurysm of the Popliteal artery, adventitious bursa formation
Hereditary Multiple Exostosis (HME)– autosomal dominant process. Presents with multiple osteochondromas (sessile-type dominates). May lead to limb deformities (Madelung deformity, coxa valga) reactive ST pressure, malignant degeneration
Dx: radiography, MRI helps to Dx malignant degeneration to chondrosarcoma by changes in size and activity of cartilaginous cap (>2-cm in adults may manifest malignant degeneration). MRI will also help with Dx of regional complications
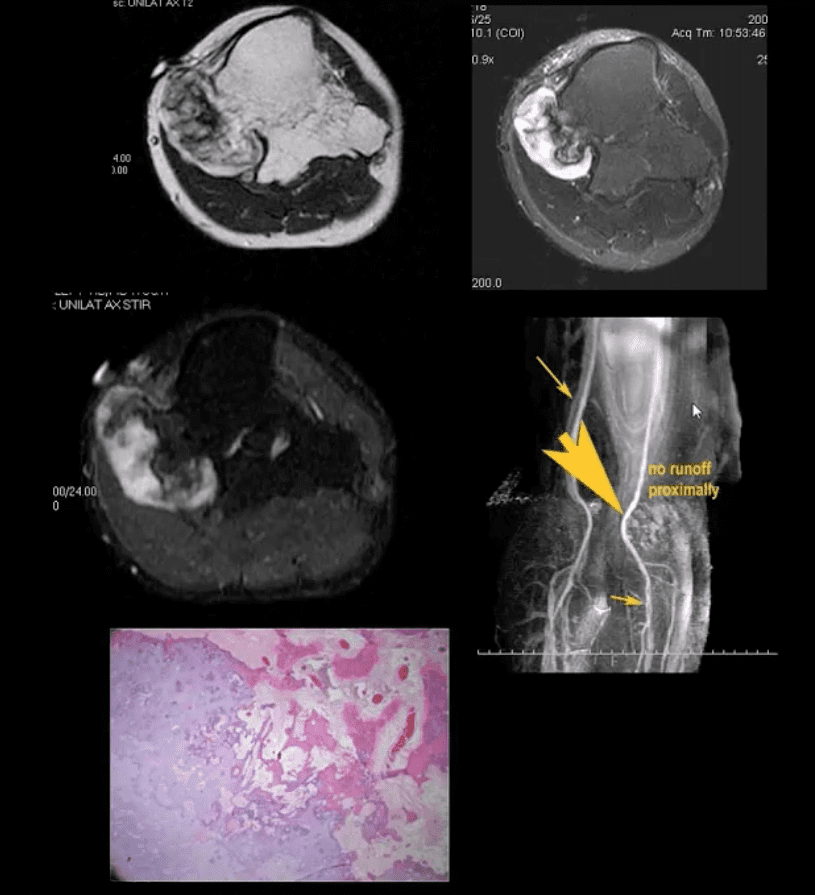
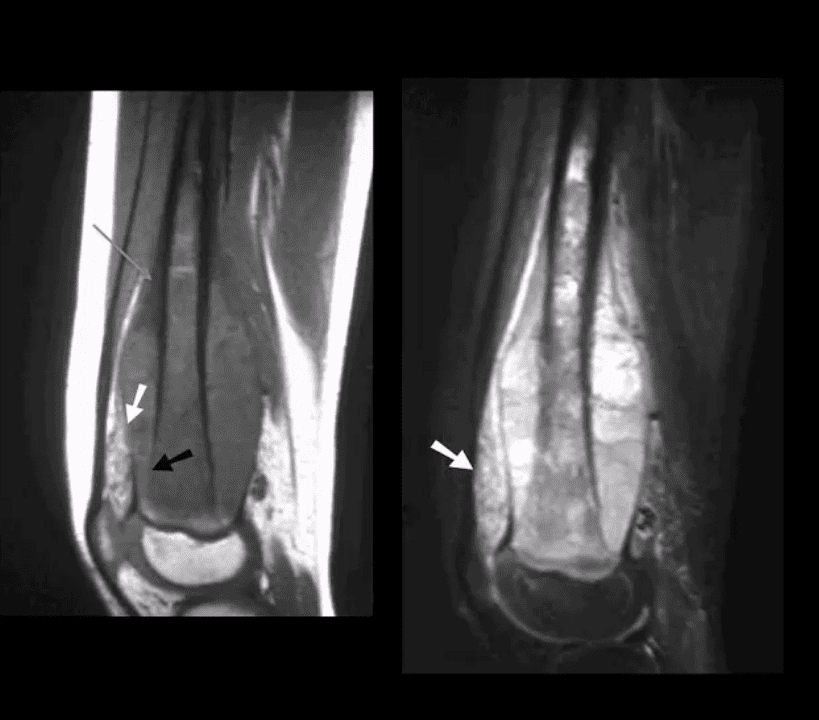
HME & Knee Pain
37-y.o male with HME and knee pain. Axial T1, T2 and STIR MRI slices at the popliteal region. Large cartilaginous cap and possible compression of the popliteal artery by osteochondroma. MRA was performed to evaluate popliteal A. pseudoaneurysm (large arrow). Pathology specimen obtained from the cartilaginous cap showed increased cellularity suggestive of malignant degeneration. Operative care was planned
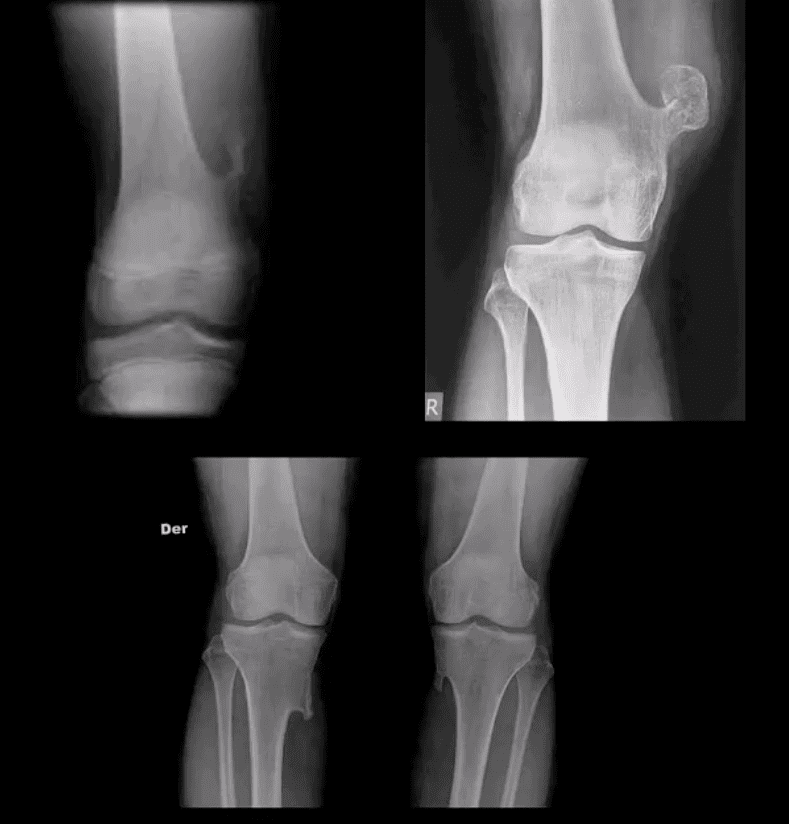
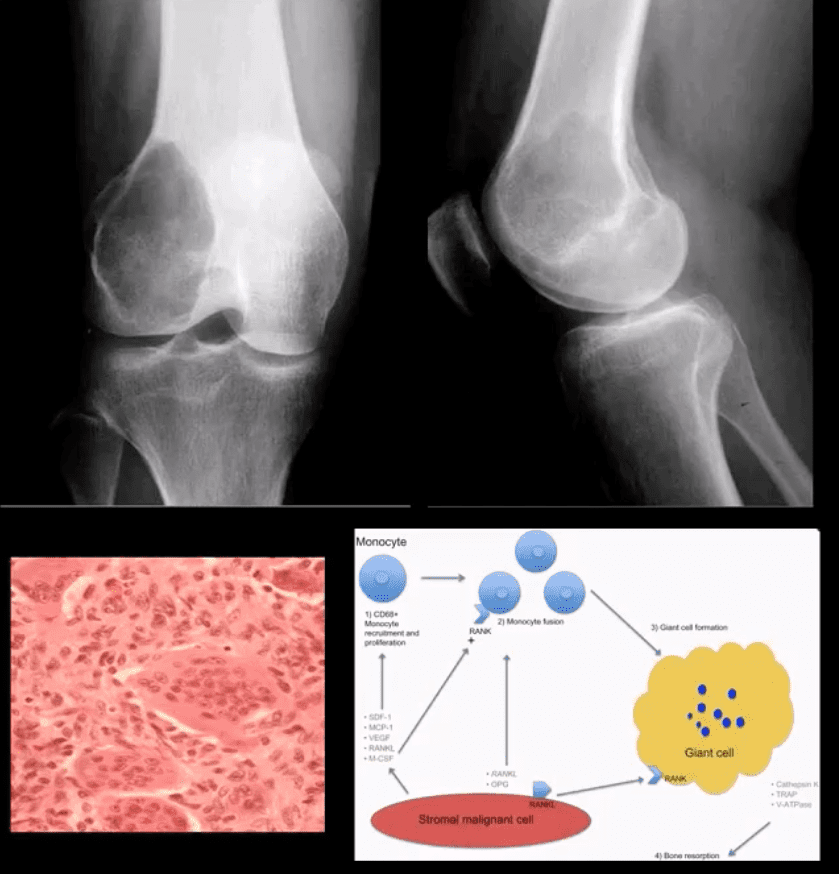
Giant Cell Tumor (GCT) aka Osteoclastoma
GCT- is a relatively common primary benign bone neoplasm. Age 25-40. M>F slightly.
GCT is the M/C benign sacral tumor. In 50% of cases, GCT occurs about the knee.
GCT is histologically benign, but lung Mets may develop esp. if in distal radius and hands, often termed Malignant GCT
<1% unresponsive/recurring GCTs may undergo malignant transformation to high-grade bone sarcoma
Pathology: histologically composed of osteoclasts-multinucleated giant cells with stromal cells derived from precursors monocyte-macrophage type. Produces cytokines and osteolytic enzymes. GCT may contain blood and associated with secondary Aneurysmal Bone Cyst (ABC)
Clinically: knee pain unresponsive to conservative care. Pathologic Fx may occur
Imaging: always begins with radiography followed by MRI and surgical biopsy that are crucial to Dx.
Rx: operative with curettage and cementing, a surgical appliance may be used if pathological fx present and cortical breach. In more severe cases other options available
Radiologic-Pathologic Dx
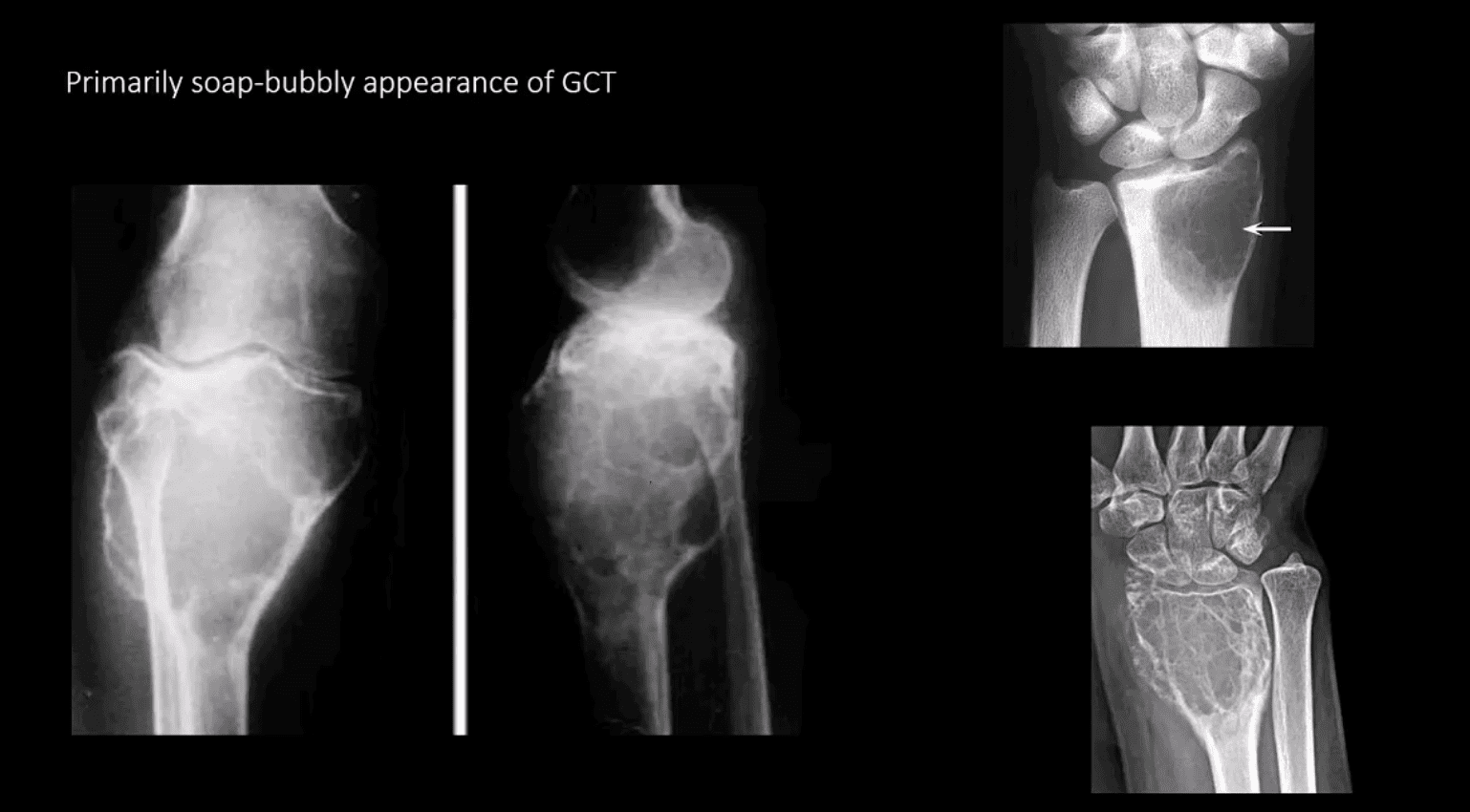
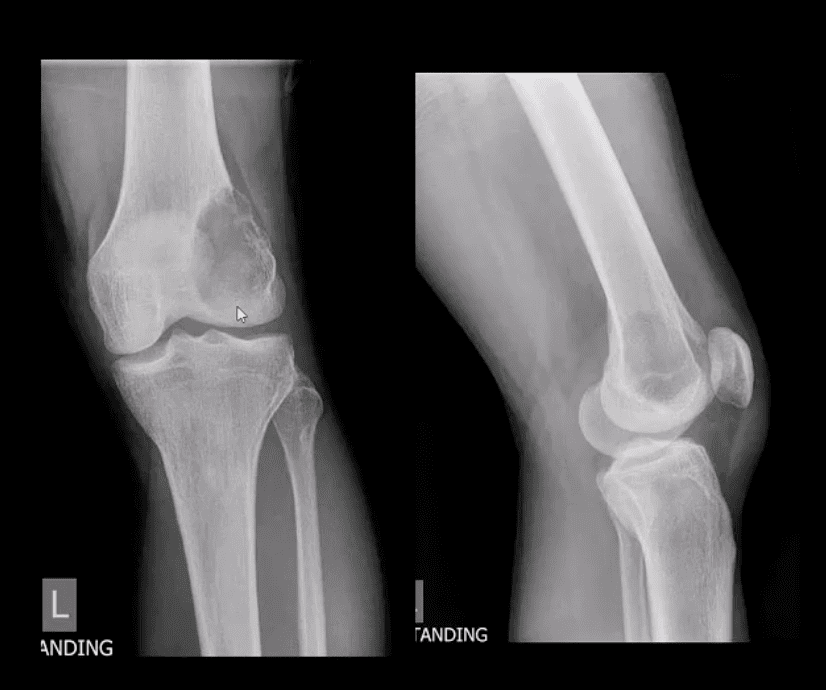
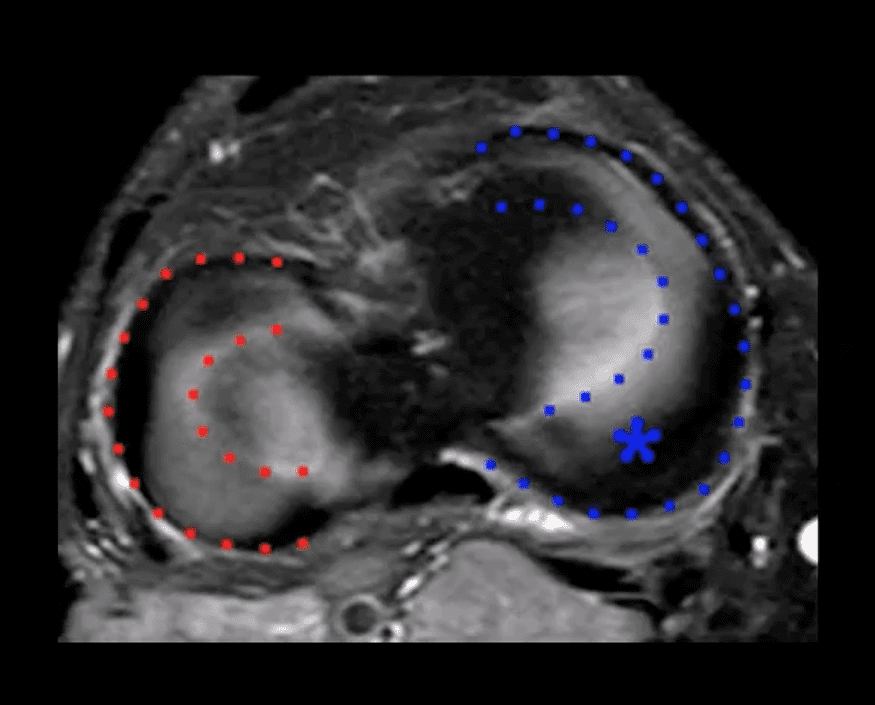
Radiologic-pathologic Dx: osteolytic and soap-bubbly lesion typically involving metaphysis and into epiphysis (classic key feature) with subarticular extension. Zone of transition is generally narrow but occasionally in aggressive lesions wide zone of transition may be seen.
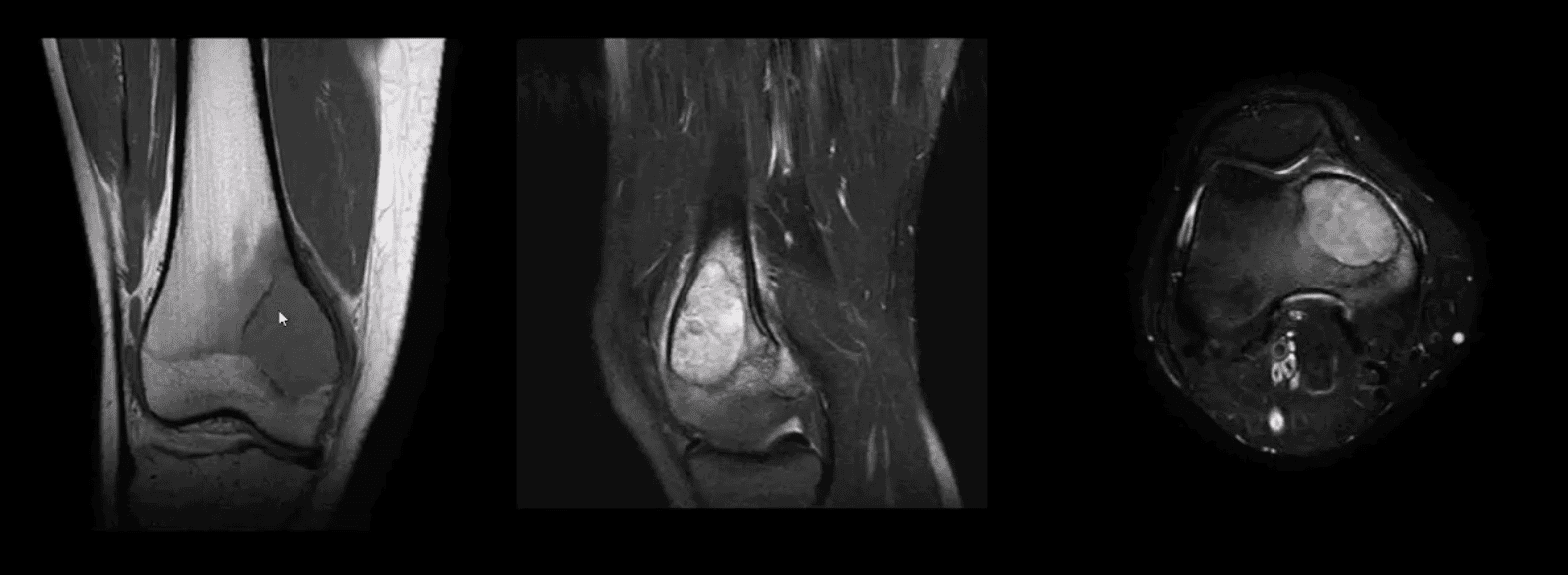
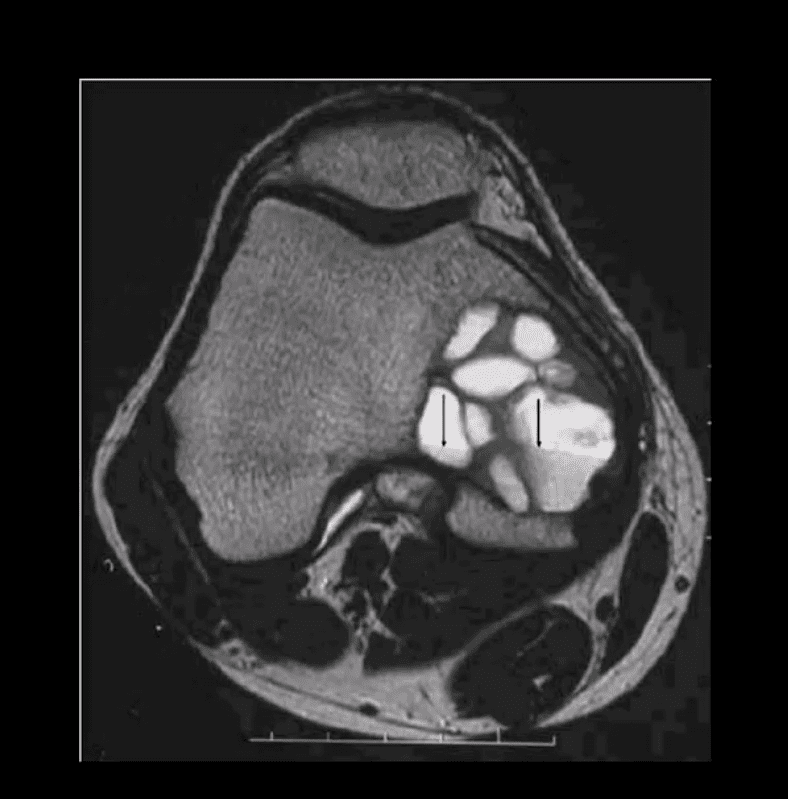
MRI: low T1, highT2/STIR, characteristic fluid-fluid levels noted that are present in GCT and ABC. Histology is crucial to Dx.
DDx: ABC, Brown cell tumor of HPT (osteoclastoma), Telangiectatic Osteosarcoma
Radiological rule: if the physeal growth plate is present Dx of GCT is taken off the list in favor of chondroblastoma and vice versa.
Primarily Soap-Bubbly Appearance of GCT
Coronal, Fat-Sat Sagittal & Axial MRI Slices of GCT
T1 coronal, T2 fat-sat sagittal and T2 axial MRI slices of GCT. Typically: low T1, highT2/STIR and fluid-fluid levels
Characteristic MRI Appearance of GCT
Fluid-fluid levels d/t different composition of blood degradation products
Important DDx: ABC
Malignant Neoplasms About the Knee
In children and very young adults, m/c primary malignant neoplasm is central aka intramedullary (osteogenic) osteosarcoma (OSA). Second peak of OS: >70 y.o d/t Paget�s (1%) and/or post radiation OSA.
The knee is the m/c location of OSA (distal femur, prox. Tibia)
A 2nd m/c malignant pediatric primary is Ewing sarcoma.
In adults >40 y.o. the m/c primary is Multiple Myeloma (MM) or Solitary Plasmacytoma
Overall m/c bone neoplasms in adults d/t bone Mets from lung, breast, prostate, renal cell, thyroid (discussed)
Dx: clinical and radiological with surgical biopsy
Imaging is crucial to Dx. 1st step x-radiography. MRI+ gad C is vital
CT scanning occasionally helps to evaluate pathological fracture
Central (Intramedullary) Osteosarcoma (OSA)
m/c age: 10-20. m/c location: knee, males>females. Increased risk in some
congenital syndromes and mutation of the retinoblastoma gene: Rothmund-Thompson AR syndrome.
Early Dx is important d/t 10-20% present with Lung Mets at Dx. Prognosis depends on stages. Early stages with local bone invasion and no
mets 76% of survival.
Rx: limb salvage procedures preferred with 8-12 weeks of chemo, amputation if encased neurovascular tissue, path Fx, etc.
Imaging: radiography and MRI.
Clinically: bone pain, Inc. Alkaline Phosphatase
Chest CT if lung Mets considered
Classic Rad Features of OSA
Osteoid forming a sclerotic mass with aggressive hair-on-end/speculated/sun-burst periosteal reaction, Codman’s triangle and soft tissue invasion. Order MRI for staging and extent. Chest CT is crucial for Lung Mets dx.
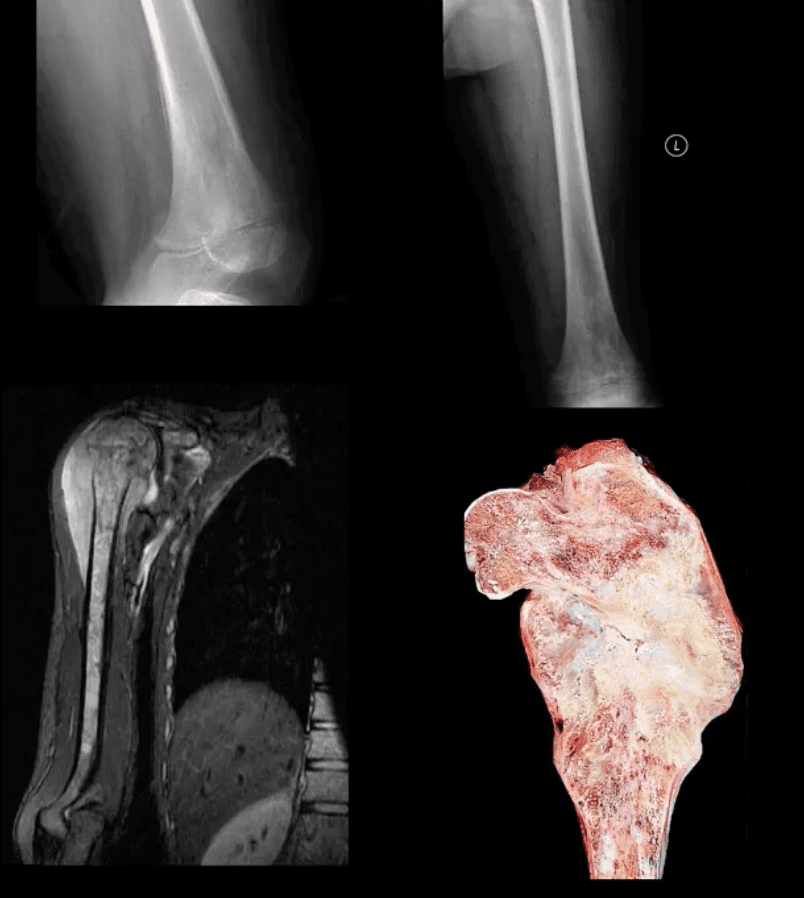
MRI is Crucial for Dx/Staging
Note sagittal T1 (left) and STIR (right) MR slices: large mass extending from distal femoral metaphysis to remaining shaft. A low signal on T1 and high on STIR d/t marrow invasion with edema, hemorrhaging and tumor invasion. Local ST invasion seen (white arrows). Periosteal lifting and Codman�s triangle (green arrow) are additional signs of aggressive neoplasm.
Note an interesting feature that the epiphysis is spared d/t physeal plate serving temporarily as an additional barrier to the tumor spread.
Ewing Sarcoma
Ewing sarcoma: age: 2-20, uncommon in black patients. 2nd m/c highly malignant bone neoplasm in children that typically arises from medullary cavity (Round cell tumors). Key symptom: bone pain that may mimic infection (ESR/CRP/WBC) Considered PNET Key Rad Dx: aggressive moth-eaten/permeative lucent lesions in the shaft of long bones with sizeable soft tissue invasion/typical onion skin periostitis. May produce saucerisation May affect flat bones. May appear as sclerotic in 33%. Early lung Mets (25-30%) bone-to-bone Mets Poor prognosis if delayed Dx. Imaging steps: 1st step x-rad, MRI is v. important followed by a biopsy. CXR/CT PET-CT Rx: combined rad-chemo, operative.
Note aggressive expansile osteolytic lesion in the distal femur metaphysis into epiphysis. No periosteal reaction present. Following further work up with abdominal and chest CT scanning, Dx of Renal cell carcinoma was established
Distal Mets into lower extremity are more common with lung, renal cell, thyroid and breast CA.
Renal cell and Thyroid will typically present with aggressive osteolytic expansile mass aka �blowout Mets.�
In general, imaging approach should consist of Radiographic knee series, followed by MRI if x-rays are unrewarding
Tc99 Bone scintigraphy is the modality of choice to evaluate metastatic bone disease
Soft Tissue Neoplasms About the Knee
Malignant fibrous histiocytoma (MFH) reclassified as Pleomorphic Undifferentiated Sarcoma (PUS) is the m/c S.T. sarcoma. MFH is aggressive biologically with poor prognosis M>F (1.2:1) 30-80 with a peak in a 6th decade. 25-40% of all adults sarcomas m/c extremities. Retroperitoneum next (worst prognosis d/t late Dx and large growth w/o symptoms) Clinically: painful, hard mass typically about the knee or thigh. Histology: poorly differentiated/undifferentiated malignant fibroblasts, myofibroblasts, and other mesenchymal cells Imaging: MRI is the modality of choice with T1, T2, T1+C. Typically appears as an aggressive heterogeneous mass intermediate to low signal on T1 and high signal on T2 with areas of necrosis and enhancement on T1+C. May appear misleadingly encapsulated w/o true capsule Management: operative with radiation and chemotherapy. Tumor depth is crucial for prognosis. 80% 5-year survival if <5cm deep in ST and 50% if >5-cm deep in ST.
Synovial Sarcoma
Synovial sarcoma: common malignant ST neoplasm esp. in younger patients or older children/adolescents. M/C found in knee area Clinically: can present slowly as a palpable mass in the extremity often ignored d/t slow growth Imaging is the key: radiography may reveal ST. density/mass. Some synovial sarcomas may show calcification and mistaken for Myositis Ossificanse or heterotopic bone formation MRI with T1, T2 and T1+C are Dx modality of choice. Other modalities: US, CT are non-specific DDx: MFH Management: operative, chemo-radiation Prognosis: variable depending on size, invasion, metastasis
When dealing with a sports injury or a similar type of injury, many people are familiar with the R.I.C.E. protocol for injury care. R.I.C.E. stands for Rest, Ice, Compression, and Elevation and has long been used when treating everything from sprained ankles to banged up knees. With acute injury patients, experts recommend adding �P� for protection because of the protection of the area is vital in the healing process. It is crucial that this is implemented as soon after the injury as possible and it should be maintained for anywhere from 24 hours to 72 hours afterward. Of course, this depends on the severity of the injury.
P is for Protection: Injuries hurt and pain can be a good thing because it prevents you from further injuring that area. It encourages you to protect it.
It is essential to listen to your body and protect the injured area through full or partial immobilization and restricted use. The way you do this depends on the body part.
An arm or shoulder injury can be protected with the use of a sling. An ankle injury may require a brace or splint, and you may have to avoid or limit weight bearing for a while. This means using crutches a walker, or a cane.
R is for Rest: The body needs rest to heal. This could mean complete rest, but in many cases, it means what is known as �relative rest.� This means that it allows for enough rest to heal but is not entirely restrictive which could slow or inhibit recovery.
This means avoiding activities that are stressful to the area to the point that they cause pain or that they might compromise healing. Many times, though, some movement is a good thing, even beneficial. Some gentle movements can speed recovery.
Isometric contractions of the muscles and joints that surround the injury and even some range of motion exercises can help. The key is to keep the movements gentle and to listen to your body for guidance on how much and how far to push.
I is for Ice:Cryotherapy or cold treatments can come in the form of actual ice, or there can be other types such as a cold soak. When treating acute injuries at home, the best known, and probably most straightforward way is to put some crushed ice in a freezer bag with a zip lock closure and wrap it in a small towel to keep the pack from directly touching the skin.
Frozen vegetables, like green beans, peas, or edamame work well too � remember to use the towel as a barrier between the skin and the pack. You should not use the pack more than 10 to 15 minutes as a time. The recommended cycle is 10 to 15 minutes on and 1 to 2 hours off.
In some cases, you may not be able to apply ice directly to the site. In those cases, you can use the pack at the joint above the affected area. For instance, a tightly wrapped ankle can still benefit from ice, you just apply the ice pack to the back on the knee on the same leg.
C is for Compression: A compression wrap can offer mild support and reduce swelling. Typically, an elastic bandage is used to compress or apply pressure to the injured tissue.
When applying a compression bandage, start it several inches below the area that is injured. It should be applied directly to your skin.
Use some tension as you wrap, but not to the point that it cuts off circulation (characterized by tingling or numbness and the soft tissue should not change color). Wrap the bandage in a figure eight configuration or spiral, depending on the area, stopping a few inches above the injury.
E is for Elevation: When an injured joint or extremity is not elevated, fluid can pool in the area and swelling can occur. This can lead to increased pain and limited range of motion. Elevation helps prevent these things from happening and can even help to speed up recovery.
The key to elevation is positioning the injured area at a level that is above the heart. The most effective way to accomplish this is to keep the area elevated as much as possible while awake and prop it up with pillows while sleeping for at least the first 24 to 48 hours. Some injuries may require more time though, so listen to your body.
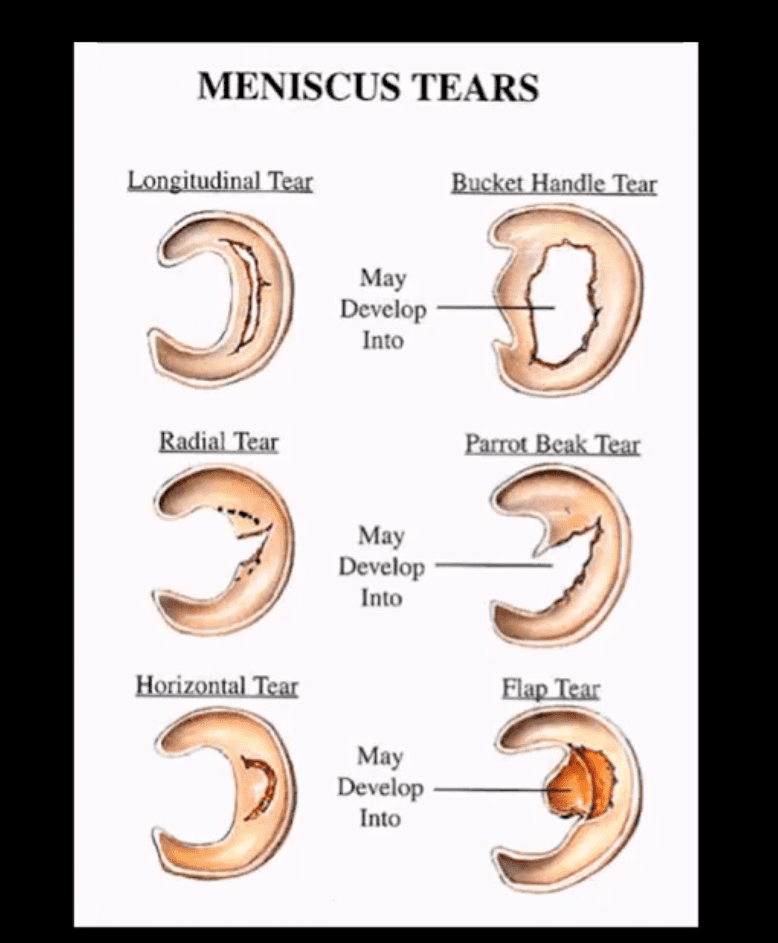
Types, location, and stability of tears are v. important during MRI Dx
Vertical/longitudinal tears especially occur in acute ACL tears. Some longitudinal tears found at the periphery or “red zone” may heal
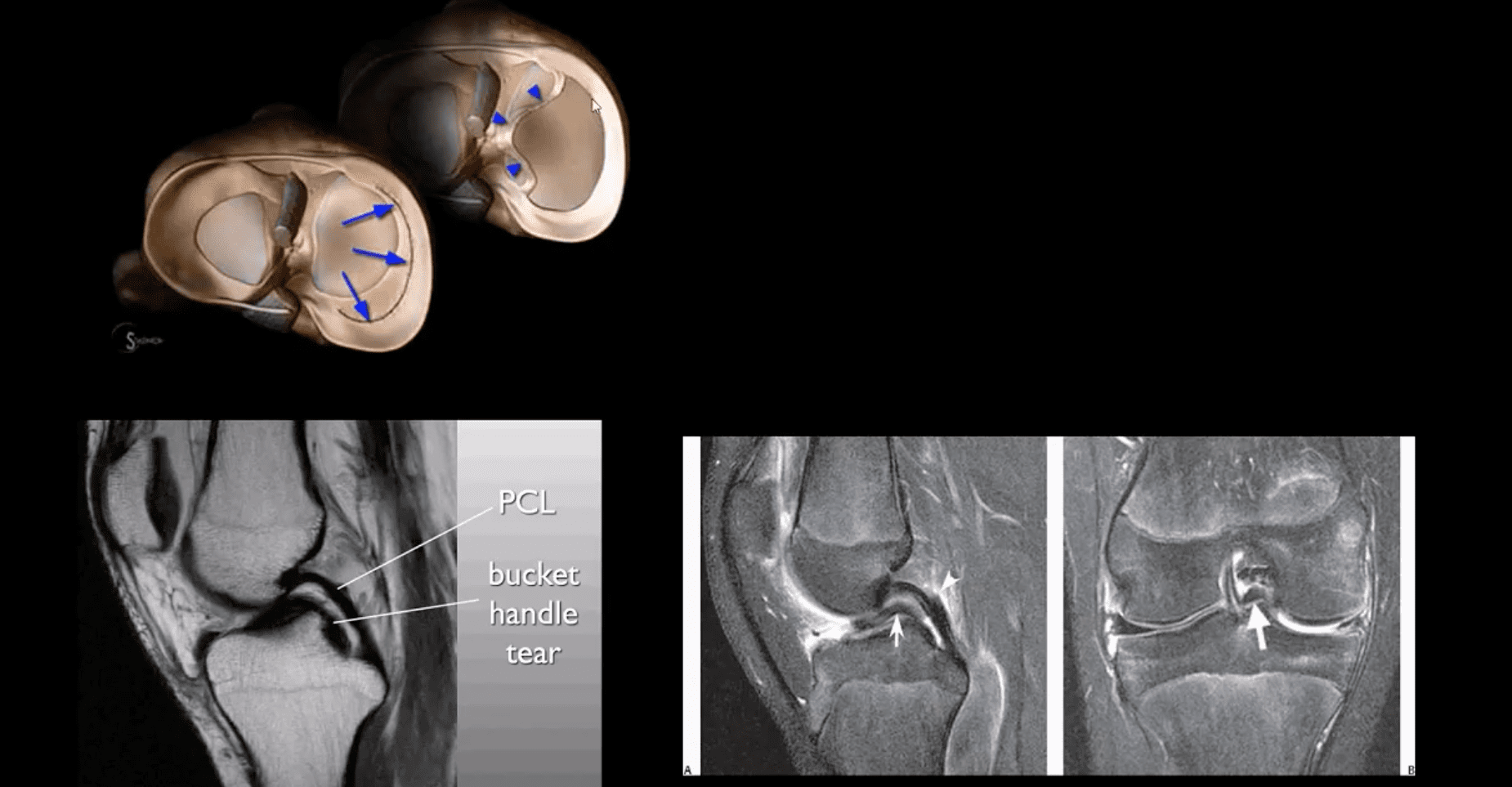
Bucket handle tear: longitudinal tear in the inner edge that is deep and vertical extending through the long axis and may displace into a notch
Oblique/flap/parrot-beak are complex tears
Radial tear at 90-degree to plateau
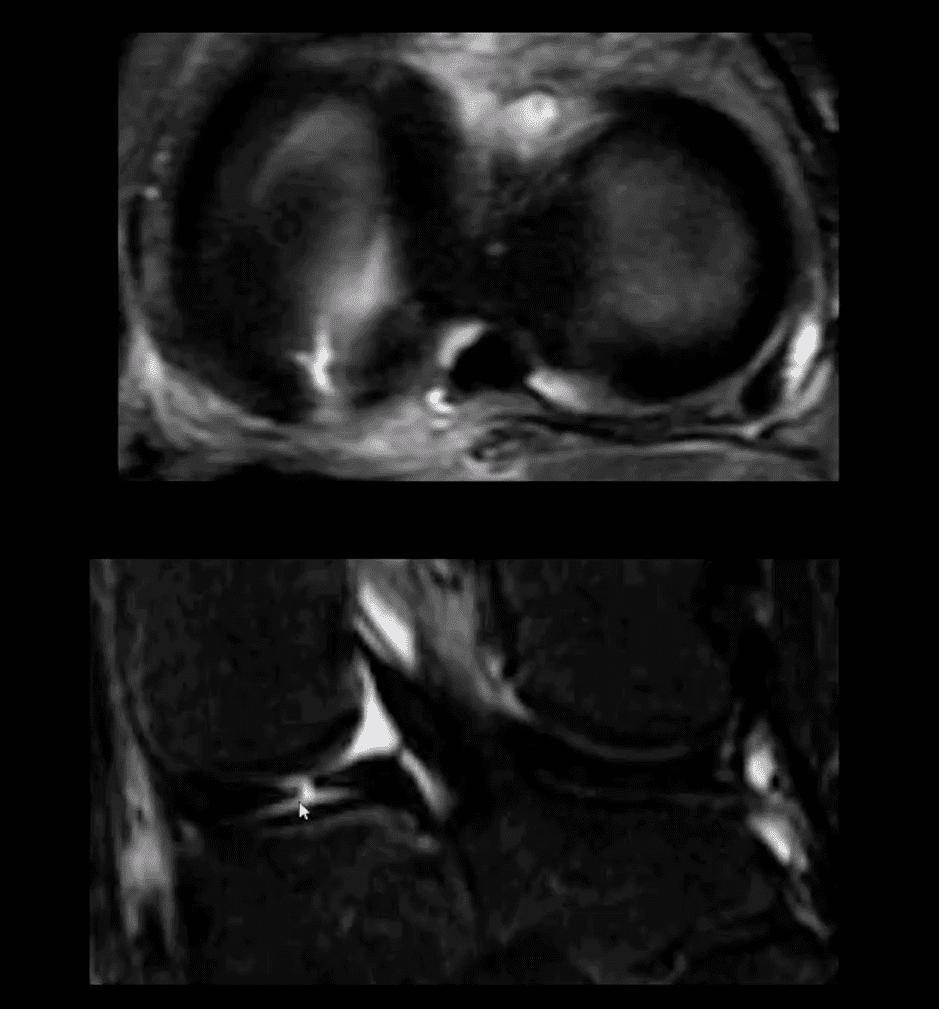
Axial T2
Axial T2 WI fat-sat and coronal STIR slices of the posterior horn of the medial meniscus.
Note a radial tear of the posterior horn of the medial meniscus near the meniscal root. This is potentially an unstable lesion requiring operative care
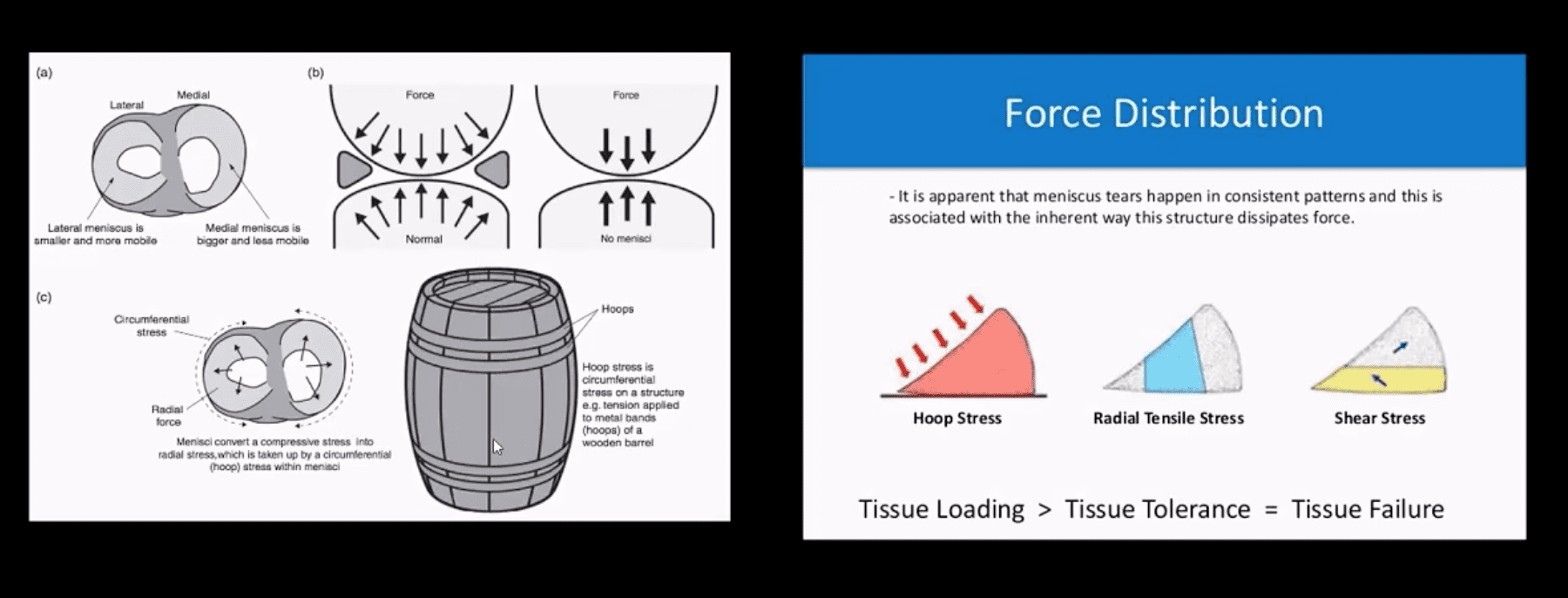
The meniscus, in this case, is unable to provide a “hoop-stress mechanism.”
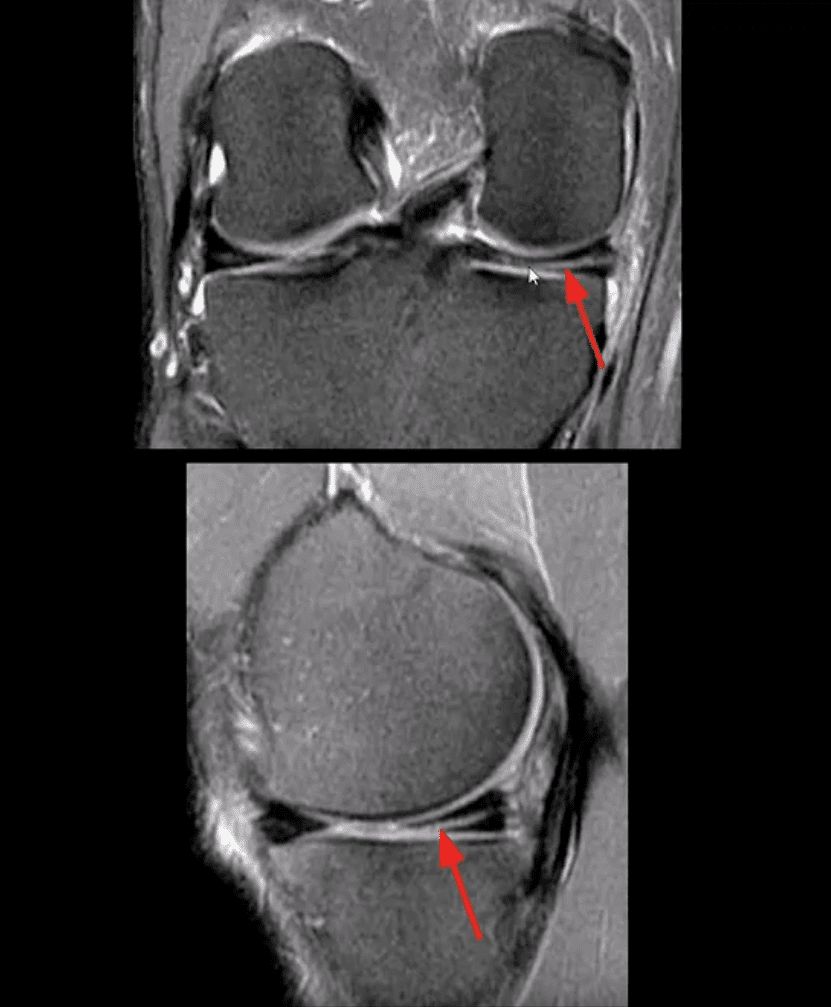
MRI Slices Coronal & Sagittal
Fat-sat coronal and sagittal proton density MRI slices revealing horizontal (cleavage) tear that is more typical in the aged meniscus
In some cases, when this tear does not contain a radial component, it may partially heal obviating the need for operative care
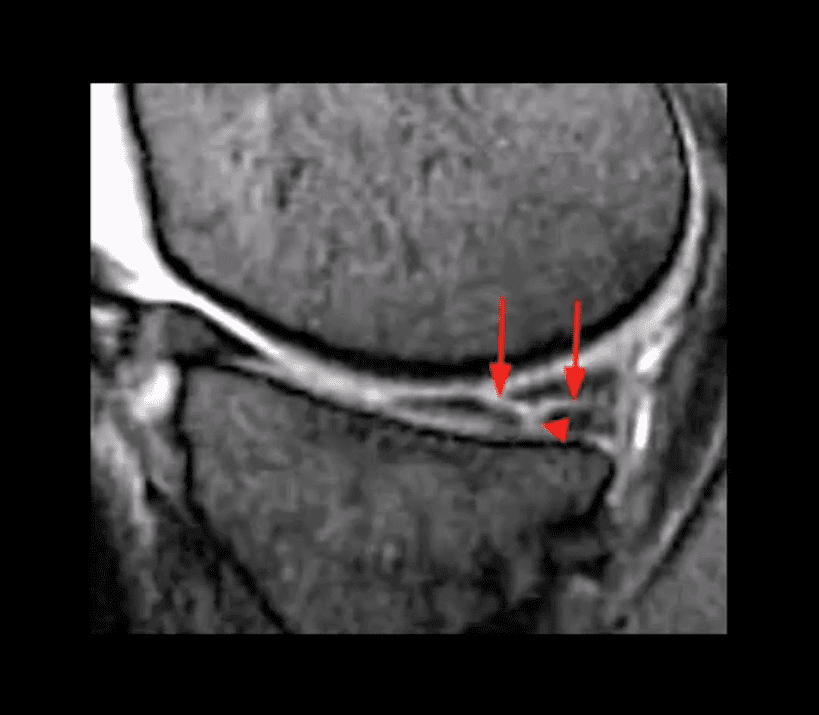
T2 w GRE Sagittal MRI Slice
Complex tear with a horizontal oblique and radial component.
This type of tear is very unstable and in most cases may need operative care
Bucket Handle Tear
Bucket handle tear are m/c in the medial meniscus esp. with acute ACL and MCL tear
MRI signs; double PCL sign on sagittal slices
Absent “bow-tie” sign and others
Most cases require operative care
DDx From Meniscal Degeneration
Occasionally meniscal tears need to be DDx from meniscal degeneration which may also appear bright (high signal) on fluid-sensitive MRI
The simplest rule is that if there is a true meniscal tear aka Grade 3 lesion, it always reaches/extends to the tibial plateau surface
The Role of MSK Ultrasound (US) in Knee Examination
MSK US of the knee permits high resolution and dynamic imaging of primarily superficial anatomy (tendons, bursae, capsular ligaments)
MSK US cannot adequately evaluate cruciate ligaments and the menisci in their entirety
Thus MR imaging remains modality of choice
Potential Pathologies Successfully Evaluated by MSK US
Patellar tendionosis/patellar tendon rupture
Quadriceps tendon tear
Prepatellar bursitis
Infrapatellar bursitis
Pes Anserine bursitis
Popliteal cyst (Baker cyst)
Inflammation/joint effusion with synovial thickening and hyperemia can be imaged with US (e.g., RA) especially with the addition of color power Doppler
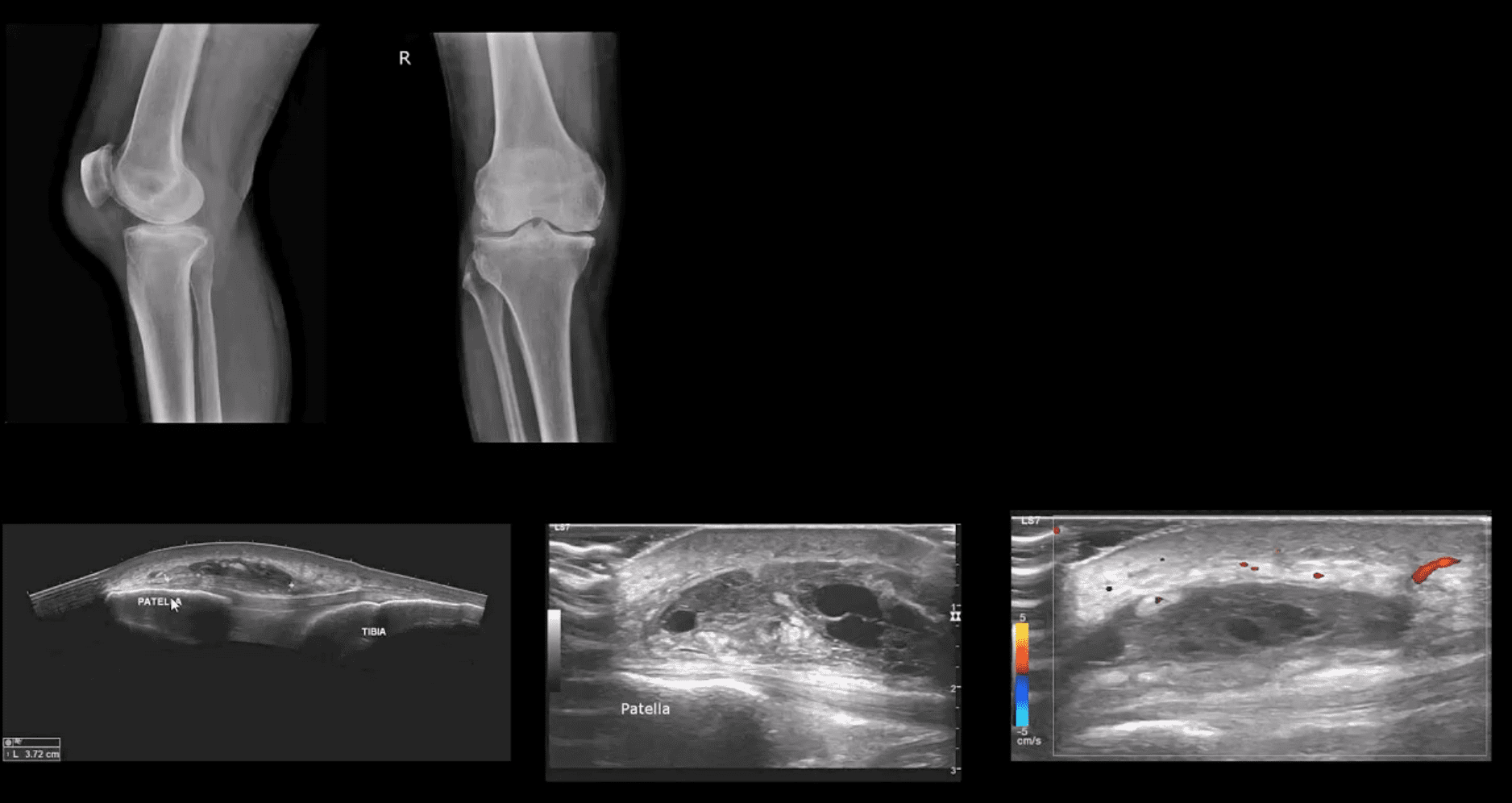
Patient Presented With Atraumatic Knee Pain & Swelling
Radiography revealed sizeable soft tissue density within the superficial pre-patella region along with mild-to-moderate OA
MSK US demonstrated large septated heterogeneous fluid collection with mild positive Doppler activity on the periphery indicating inflammation d/t Dx of Superficial pre-patella bursitis
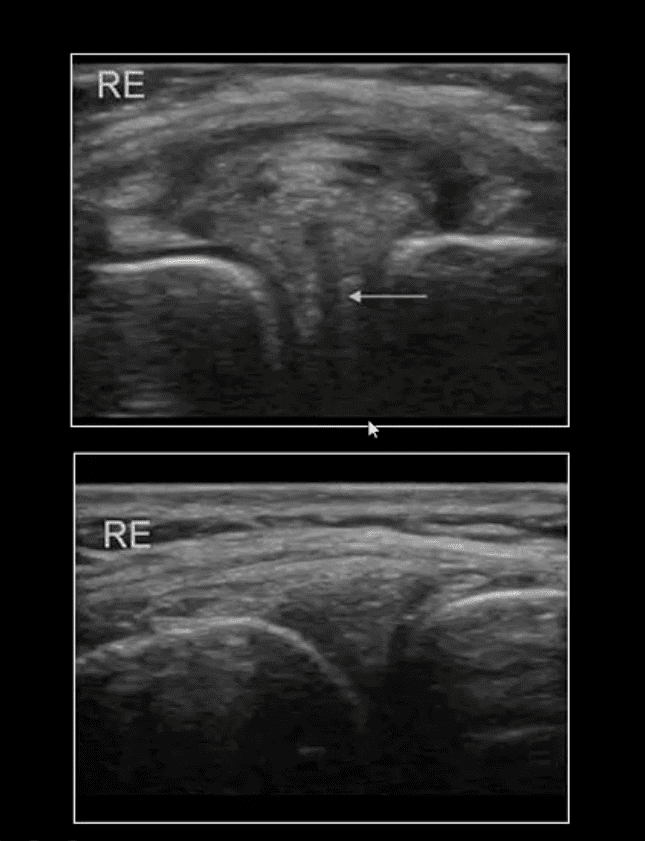
Long Axis US Images
Note normal lateral meniscus and fibers of LCL (above bottom image) compared to
Horizontal degenerative cleavage tear along with protrusion of lateral meniscus and LCL bulging (above top image)
Major limitation: unable to visualize the entire meniscus and the ACL/PCL
MRI referral is suggested
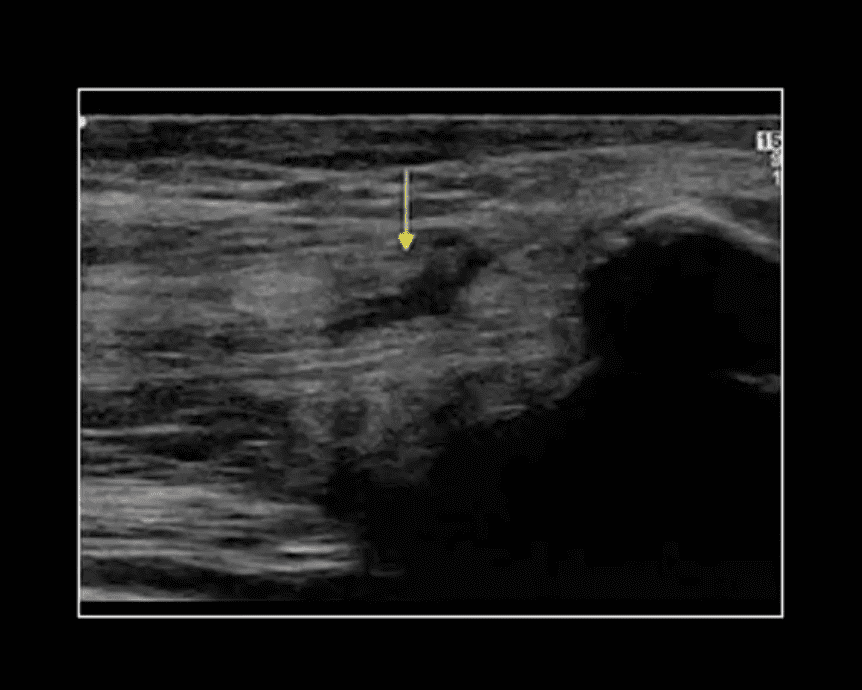
Rupture of Distal Tendon of Quadriceps
Note rupture of distal tendon of the Quadriceps muscle presented as fiber separation and fluid (hypo to anechoic) fluid collection within the substance of the tendon
Advantages of MSK US over MRI to evaluate superficial structures:
Dynamic imaging
Availability
Cost-effective
Patient’s preparation
Disadvantages: limited depth of structures, inability to evaluated bone and cartilage, etc.
Osteochondral Knee Injuries (OI)
osteochondral knee injuries can occur in children 10-15 y.o presented as Osteochondritis Dissecance (OCD) and in mature skeleton m/c following hyperextension and rotation trauma, particularly in ACL tear.
OCD-typically develops from repeated forces in immature bone and affects m/c postero-lateral portion of the medial femoral condyle.
OI in mature bone occurs m/c during ACL tears mainly affecting so-called terminal sulcus of the lateral femoral condyle at the junction of the weight-bearing portion opposed to tibial plateau and the part articulating with the patella
Osteochondral injuries may potentially damage the articular cartilage causing secondary OA. Thus need to be evaluated surgically
Imaging plays an important role and should begin with radiography often followed by MR imaging and orthopedic referral.
OCD Knee
95% associated with some trauma. Other etiology: ischemic bone necrosis especially in adults
Other common location for osteochondral injuries: elbow (capitellum), talus
1st step: radiography may detect osteochondral fragment potentially attached or detached
Location: a posterior-lateral aspect of the medial femoral condyle. Tunnel (intercondylar notch) view is crucial
MRI: modality of choice >90% specificity and sensitivity. Crucial for further management. T1-low signal demarcating line with T2 high signal demarcating line that signifies detachment and unlikely healing. Refer to orthopedic surgeon
Management: stable lesion esp. in younger children>off weight-bearing-heals in 50-75%
Unstable lesion and older child or impending physeal closure>operative fixation.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine