As research increases in regenerative medicine with the potential of being able to regrow thyroid tissue, could regeneration therapy eliminate the need for patients to take thyroid replacement hormones?
Thyroid Regenerative Therapy
A great hope for regenerative therapy is the ability to grow healthy organs. One of the organs being looked at is the thyroid gland. The goal is to re-grow thyroid tissue in:
Individuals who had to have the gland removed because of thyroid cancer.
Individuals who were born without a fully developed gland.
As science advances and research has expanded from laboratory and animal experiments to test tube human thyroid cell studies, the use of stem cell therapy for this purpose is not there yet, as more extensive research is needed for human consideration.
Human Research
Research on the use of thyroid regenerative therapy for thyroid disease has not published studies in which stem cell therapy has been attempted in human thyroid patients.
The studies that have been done were conducted in mice, and any findings of this research cannot automatically be applied to humans. (H. P. Gaide Chevronnay, et al., 2016)
In human thyroid tissue in test tube studies, the stimulation of cells was achieved in a way that raised the question of making cancerous transformations more likely if it were to be attempted in humans. (Davies T.F., et al., 2011)
Recent Studies
Current research involves advances in embryonic stem cell – ESC and induced pluripotent stem cell – iPSC. (Will Sewell, Reigh-Yi Lin. 2014)
ESCs, also known as pluripotent stem cells, can increase any type of cell in the body.
They are harvested from embryos that were produced, but not implanted, during IVF procedures.
iPSCs are pluripotent cells that have been developed using a reprogramming process of adult cells.
Follicular cells are thyroid cells that make thyroid hormones – T4 and T3 and have been produced from the embryonic stem cells of mice.
In a study published in the journal Cell Stem Cell in 2015, these cells had the ability to grow and were also able to start making thyroid hormone within two weeks. (Anita A. Kurmann, et al., 2015)
After eight weeks, cells that were transplanted into mice that did not have thyroid glands had normal amounts of thyroid hormone.
New Thyroid Gland
Investigators at Mount Sinai Hospital induced human embryonic stem cells into thyroid cells.
They were looking at the possibility of creating a new-like thyroid gland in individuals who have had their thyroid surgically removed.
The future looks promising for the ability to regrow thyroid tissue and eliminate thyroid replacement hormone. However, far more research is needed for this to even be considered a possibility.
Cracking the Low Thyroid Code Assessment Guide
References
Gaide Chevronnay, H. P., Janssens, V., Van Der Smissen, P., Rocca, C. J., Liao, X. H., Refetoff, S., Pierreux, C. E., Cherqui, S., & Courtoy, P. J. (2016). Hematopoietic Stem Cells Transplantation Can Normalize Thyroid Function in a Cystinosis Mouse Model. Endocrinology, 157(4), 1363–1371. https://doi.org/10.1210/en.2015-1762
Davies, T. F., Latif, R., Minsky, N. C., & Ma, R. (2011). Clinical review: The emerging cell biology of thyroid stem cells. The Journal of clinical endocrinology and metabolism, 96(9), 2692–2702. https://doi.org/10.1210/jc.2011-1047
Sewell, W., & Lin, R. Y. (2014). Generation of thyroid follicular cells from pluripotent stem cells: potential for regenerative medicine. Frontiers in endocrinology, 5, 96. https://doi.org/10.3389/fendo.2014.00096
Kurmann, A. A., Serra, M., Hawkins, F., Rankin, S. A., Mori, M., Astapova, I., Ullas, S., Lin, S., Bilodeau, M., Rossant, J., Jean, J. C., Ikonomou, L., Deterding, R. R., Shannon, J. M., Zorn, A. M., Hollenberg, A. N., & Kotton, D. N. (2015). Regeneration of Thyroid Function by Transplantation of Differentiated Pluripotent Stem Cells. Cell stem cell, 17(5), 527–542. https://doi.org/10.1016/j.stem.2015.09.004
Tuttle, R. M., & Wondisford, F. E. (2014). Welcome to the 84th annual meeting of the American Thyroid Association. Thyroid : official journal of the American Thyroid Association, 24(10), 1439–1440. https://doi.org/10.1089/thy.2014.0429
When it comes to our bodies, many functioning systems help the body regulate its temperature, provide mobility and stability when in motion, and protect the host from pathogens that enter inside to cause havoc. One of the systems that helps the body is the endocrine system, which produces many hormones to keep the body functioning properly. The thyroid, a small, butterfly-shaped organ at the base of the neck, produces the hormones in the body. The thyroid helps regulate hormone production; however, when pathogen factors affect the body’s hormonal production, it can lead to musculoskeletal pain and dysfunction. Today’s article examines how the thyroid produces hormones, how hormone imbalances are connected with musculoskeletal pain, and how MET therapy can help restore hormone imbalances from affecting the body in the future. We utilize information about our patients to certified medical providers using soft tissue therapies like MET to reduce musculoskeletal pain associated with hormonal imbalances. We encourage patients by referring them to associated medical providers based on their diagnosis while supporting the fact that education is a marvelous way to ask our providers the most interesting questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
How Does The Thyroid Produce Hormones?
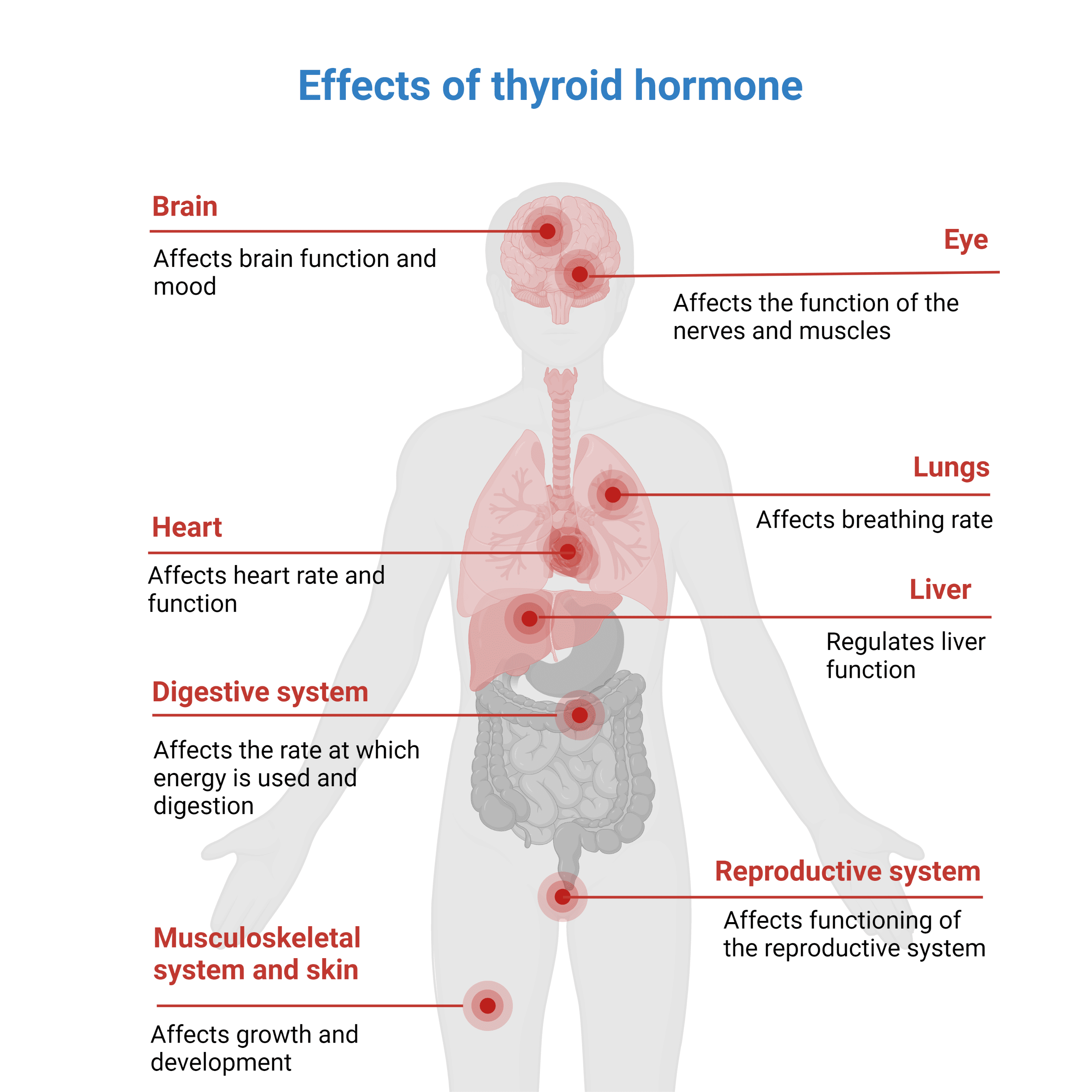
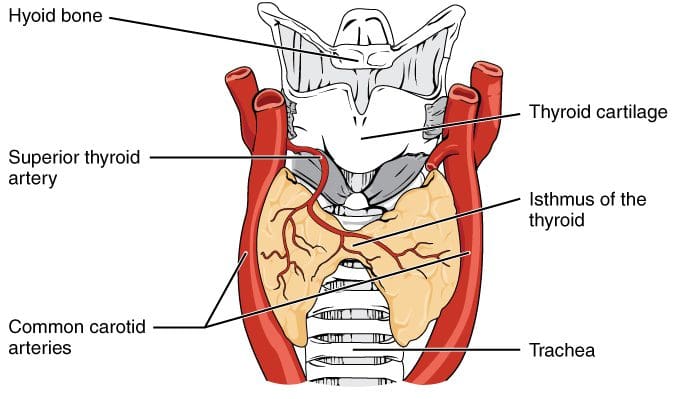
Do you feel muscle weakness or pain in certain parts of your body? Do you feel out of breath after walking for a short distance? Or do you feel sluggish throughout the entire day? When many individuals are dealing with these numerous issues, it could be due to their hormones being imbalanced from their thyroids. When it comes to the body, the endocrine system is the mastermind of producing different hormones for the body to help regulate all the biological processes. One of the vital organs of the endocrine system is the thyroid. Studies reveal that the thyroid is an endocrine gland located in the inferior anterior neck of the body and produces T4 and T3 hormones for the body to function properly. The thyroid hormones affect many of the vital organs and body tissues as they help with the following:
Cardio output and increased resting heart rate
Increases BMR (basal metabolic rate), heat production, and oxygen consumption
Stimulates resting respiratory rate and the nervous system
Plays a role in reproductive health and other endocrine organ function
Additional studies have revealed that thyroid hormones help control the body’s metabolism, growth, and other bodily functions while having a casual relationship with the HPT (hypothalamic-pituitary-thyroid) axis. What this relationship does is that it makes sure that the body is working properly in any environment. However, when unwanted pathogens start to affect thyroid hormone production, it can cause a hormone imbalance and lead to unwanted pain-like symptoms in the vital organs and musculoskeletal tissues.
Hormone Imbalances & Musculoskeletal Pain
When unwanted pathogens are associated with environmental factors affecting the body, it can lead to pain-like symptoms that can lead to musculoskeletal pain. In the book, “Clinical Applications of Neuromuscular Techniques,” written by Dr. Judith Walker DeLany, L.M.T., and Leon Chaitow, N.D., D.O., stated that there is a connection between hormonal imbalances and musculoskeletal pain as there are many environmental factors that can influence how much or how little hormone production is being produced from the thyroid. The book also mentions that some of the clinical signs of thyroid hormone deficiency include:
Dry skin and thinning hair
Unnatural fatigue
Unexplained weight increase
Aching muscles
Mental confusion
When the body is dealing with hormone imbalances associated with musculoskeletal pain, studies reveal that symptoms of fatigue, anxiety, irritability, and increased oxidative stress can cause the muscular tissues and ligaments to be weak and cause overlapping risk profiles when the body is in motion. To that point, hormone imbalances could lead to muscle and joint pain associated with myofascial trigger points and muscle shortness.
Finding Hormonal Harmony- Video
Have you been experiencing muscle or joint pain? Do you often feel anxious or irritable constantly? Or have you noticed that you are extremely sensitive to the cold? Many of these pain-like issues are signs and symptoms associated with hormone imbalances in the body and can lead to musculoskeletal pain. The body needs hormones to help regulate body temperature, control the body’s metabolism, and help stimulate the endocrine and body systems. Hormones are secreted from the thyroid and travel to the important muscles, organs, and tissues through the bloodstream to assist and help each body section function properly. When pathogens start to disrupt hormone production, the thyroid can overproduce or underproduce hormone secretion and cause many overlapping risk profiles to the body and musculoskeletal system. Fortunately, there are many ways to regulate hormones and reduce the effects of musculoskeletal pain. The video above explains that increasing certain vitamin intake, eating healthy, whole-nutritional foods, and getting adequate exercise and sleep can regulate hormone production and reduce the effects of musculoskeletal pain. These various treatments can be combined with therapy to help realign the body and restore it naturally.
MET Therapy Restoring Hormone Imbalances
Many available therapies can reduce the effects of hormonal imbalances associated with musculoskeletal pain. Treatments like MET (muscle energy techniques) allow many pain specialists to use soft tissue techniques to reduce pain-like symptoms and will enable the body to restore itself naturally. Research studies have revealed that soft tissue therapies like MET can reduce pain, improve body function, and reduce disability. MET therapy can be combined with nutritional foods, hormone therapies, and bodywork strategies that can help regulate hormone production in the thyroid. When a person starts to go to treatment for any ailments affecting their body, it allows these individuals to be more mindful of what is happening to their bodies and make small meaningful changes to their health and wellness.
Conclusion
When it comes to maintaining the body’s health and wellness, it’s important to ensure that unwanted pathogens don’t start affecting thyroid hormone production. The thyroid is a small gland located at the base of the neck that secretes out hormones to the rest of the body. When the thyroid over or under-produces hormones in the organs, muscles, and tissues, it can lead to pain-like symptoms that affect the body’s system and potentially lead to musculoskeletal disorders. Treatments like MET therapy combined with nutritional whole foods and exercises can reduce the effects of hormone imbalances associated with musculoskeletal disorders. This amazing combination allows the body to heal naturally and allows the individual to be pain-free.
References
Armstrong, Maggie, et al. “Physiology, Thyroid Function – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), 13 Mar. 2023, www.ncbi.nlm.nih.gov/books/NBK537039/.
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Day, Joseph M, and Arthur J Nitz. “The Effect of Muscle Energy Techniques on Disability and Pain Scores in Individuals with Low Back Pain.” Journal of Sport Rehabilitation, May 2012, pubmed.ncbi.nlm.nih.gov/22622384/.
Shahid, Muhammad A, et al. “Physiology, Thyroid Hormone – StatPearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), 8 May 2022, www.ncbi.nlm.nih.gov/books/NBK500006/.
VandeVord, Pamela J, et al. “Chronic Hormonal Imbalance and Adipose Redistribution Is Associated with Hypothalamic Neuropathology Following Blast Exposure.” Journal of Neurotrauma, 1 Jan. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4700394/.
The body is a functional being with the brain to control the host’s movements when going to places or resting, the immune system to battle viruses that enter the body, digest food through the gut system, and the endocrine system regulate hormones that maintain the body. The thyroid secretes hormones out and has a vital role in the body’s functionality, and when it gets affected, it can cause issues associated with the body. When the thyroid doesn’t produce more hormones in the body, it can be at risk of developing hypothyroidism. Today’s article looks at the thyroid’s role in the body, how hypothyroidism affects the body, and how to manage hypothyroidism in the body. We refer patients to certified providers specializing in endocrinology treatments to help many individuals with hypothyroidism. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What’s The Thyroid’s Role In The Body?
Have you been experiencing fatigue out of nowhere? What about having constipation issues in your lower abdominals? Or have you been experiencing frequent and heavy menstrual cycles? Some of these symptoms are associated with hypothyroidism. The thyroid is located at the neck’s base and produces hormones. Studies reveal that this small organ is mighty as it has a massive responsibility to the body by controlling its metabolism, growth, and functionality. As the thyroid secretes hormones for the body, these hormones travel with the bloodstream to different organs, muscles, and tissues throughout the body. Thyroxine(T4) and triiodothyronine (T3) are the two main hormones the thyroid gland produces. While the hypothalamus produces TRH (thyrotropin-releasing hormone), and the anterior pituitary glands produce TSH (thyroid-stimulating hormone). All three of these organs work in synchronized harmony with the body by maintaining the proper mechanism and homeostasis. The thyroid hormone affects not only the body but the vital organs like:
Heart
Central nervous system
Autonomic nervous system
Lungs
Skeletal muscles
Metabolism
GI tract
The Effects Of Hypothyroidism In The Body
Since the thyroid helps regulate hormones in the body, environmental factors play a role in hormone production. When environmental factors begin to affect the body, they potentially involve hormones. When the thyroid gland cannot produce sufficient hormones in the body, it risks developing hypothyroidism. Hypothyroidism is defined as a common condition that is the result of low hormone production overlapping various conditions and manifestations. When left untreated, hypothyroidism could associate with sympathetic and parasympathetic dysfunction. Studies reveal that the thyroid hormone influences the autonomic nervous system. Individuals suffering from hypothyroidism correlate to a dysfunctional autonomic system overlapping sympathetic reactivity. This means that hypothyroidism will cause the body’s metabolism to slow down and cause various symptoms to affect each vital organ.
An Overview Of Hypothyroidism-Video
Have you been experiencing chronic fatigue? How about muscle weakness in your arms or legs? What about feeling cold all the time? Individuals experiencing these symptoms are dealing with a condition known as hypothyroidism. The video above explains hypothyroidism, how it is diagnosed, and its symptoms in the body. Many environmental factors do play a role when it comes to the development of hypothyroidism. Some of the symptoms associated with hypothyroidism include:
Constipation
Decrease in sexual function
Depression
High cholesterol
Weight gain
Chronic fatigue
Brain fog
Hashimoto’s
When the body is being affected by environmental factors correlating with hypothyroidism, studies reveal that factors like spinal cord injuries do cause an impact on the body’s metabolic function and derange various hormonal axes. This causes issues that could potentially involve co-morbidities like urinary tract infections. Fortunately, there are ways to manage hypothyroidism and regulate the hormones to make the body functional again.
Managing Hypothyroidism
One cornerstone in managing hypothyroidism and reducing its associated symptoms is following a proper treatment for health and wellness. Maintaining healthy hormone levels in the body is achievable regarding hypothyroidism. Taking thyroid medication as prescribed by a doctor help improve symptoms associated with hypothyroidism while regulating T3 and T4 hormones. Eating nutritious foods may help relieve some symptoms of hypothyroidism. Exercising helps enhance energy levels and strengthen weak muscles for individuals with hypothyroidism. Incorporating chiropractic care can help reduce somato-visceral disorders associated with hypothyroidism through spinal manipulation. Utilizing these treatments to manage hypothyroidism benefits one’s health and wellness journey.
Conclusion
The thyroid is an organ at the neck’s base as part of the endocrine system. This organ is mighty as it helps the body by secreting hormones for all the various organs, muscles, and tissues. When the thyroid can’t produce sufficient hormones to regulate the body, it risks developing hypothyroidism. Hypothyroidism is a common condition that results in a low hormonal count, triggering symptoms that affect the body. If left untreated, it could become the mediator for sympathetic and parasympathetic dysfunction. Luckily, treatments are available to manage hypothyroidism and regulate hormonal secretion in the body. This allows the individual to incorporate healthy habits to maintain their hormones while their health and wellness journey continues impacting their lives.
References
Cheville, A L, and S C Kirshblum. “Thyroid Hormone Changes in Chronic Spinal Cord Injury.” The Journal of Spinal Cord Medicine, U.S. National Library of Medicine, Oct. 1995, https://pubmed.ncbi.nlm.nih.gov/8591067/.
Hardy, Katie, and Henry Pollard. “The Organisation of the Stress Response, and Its Relevance to Chiropractors: A Commentary.” Chiropractic & Osteopathy, BioMed Central, 18 Oct. 2006, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1629015/.
Mahajan, Aarti S, et al. “Evaluation of Autonomic Functions in Subclinical Hypothyroid and Hypothyroid Patients.” Indian Journal of Endocrinology and Metabolism, Medknow Publications & Media Pvt Ltd, May 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3712377/.
Patil, Nikita, et al. “Hypothyroidism.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 19 June 2022, https://www.ncbi.nlm.nih.gov/books/NBK519536/.
Shahid, Muhammad A, et al. “Physiology, Thyroid Hormone – StatPearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 8 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK500006/.
An examination of the cervical/neck region of the spine through chiropractic will help determine a thyroid diagnosis for individuals complaining of chronic fatigue. A thyroid dysfunction means going deeper into the body�s physiology and a thorough examination of the spine. Checking for subluxations in the cervical spine will reveal possible nerve blockage and any other contributing factors to a thyroid condition. Thyroid conditions tend to get overlooked because the symptoms are general. They range from:
Fatigue
Moodiness
Muscle pain
Brain fog
These are cornerstones of a thyroid condition. Under-active thyroid and/or thyroid cancer can have an impact on everyday life regardless of the severity. However, these symptoms can signify numerous other conditions.
The Cervical Spine
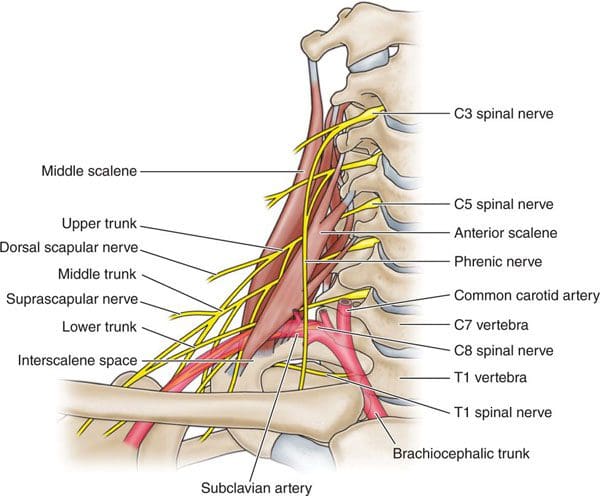
The nerves connected to the thyroid gland can be traced down the spine to the last neck/cervical vertebrae, which is C7. A chiropractor will examine this region when individuals complain of fatigue, brain fog, or moodiness. Subluxation, translation, or disc deterioration at C7 could mean that the nerve signals and blood circulation to the thyroid are limited, interrupted, or completely blocked.
Linking cervical spine dysfunction to thyroid dysfunction
Spinal subluxations are not the full cause of thyroid dysfunction. A single vertebra might not show signs of movement, which means a chiropractor could have to look further into the spine. A chiropractic examination will search for problems that correlate with thyroid issues. For example, individuals with a cervical dysfunction could experience general nerve issues in this area. It could be a contributor to nerve signals not being delivered to the thyroid gland. Diagnosis of a root condition that has secondary effects on the gland is another way to qualify a thyroid condition.
Medical History
Questions that will be asked by a chiropractor during an exam could consist of:
Is there a family history of hyper/hypothyroidism?
Is the individual under intense stress from work, home, etc?
Are there other symptoms that could be associated with thyroid dysfunction?
All details are necessary for connecting nerve interruption to thyroid conditions then factoring how spinal manipulation could alleviate symptoms.
Cervical Misalignment Treatment
Combining the evidence of:
Subluxations
Blocked nerves
Cervical spine dysfunction
Any further symptoms/details will help form a complete picture of a thyroid condition. If that condition is being tested or treated by a general physician, it may still benefit from a chiropractic adjustment. Physicians could recommend diet and medication to bring the thyroid back to proper function, and chiropractic can help improve the nerve function of the gland. This includes:
Re-opening pinched pathways
Restored blood flow to the region
Helping nerve signals fire transmit properly
We advocate for an incremental, customized approach to restore cervical spine curvature and optimal nerve health. We have worked with a variety of individuals experiencing chronic fatigue, mental fog, and moodiness, and have helped link these symptoms to thyroid dysfunction. If it seems that there is constant confusion or disorganized thought patterns, schedule an appointment with us today to learn more about our chiropractic approach.
Neck Pain Chiropractic Care
��
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Arick, Christopher T. �Chiropractic Management of a Patient With Chronic Fatigue: A Case Report.��Journal of chiropractic medicine�vol. 15,4 (2016): 314-320. doi:10.1016/j.jcm.2016.08.006
The thyroid gland plays a major role in the human body; it produces the hormones necessary for appropriate energy levels and an active life. These hormones have a critical impact on early brain development and somatic growth. At the same time, the thyroid is highly vulnerable to autoimmune thyroid diseases (AITDs). They arise due to the complex inter- play of genetic, environmental, and endogenous factors, and the specific combination is required to initiate thyroid autoimmunity. When the thyroid cell becomes the target of autoimmunity, it interacts with the immune system and appears to affect disease progression. It can produce different growth factors, adhesion molecules, and a large array of cytokines. Preventable environmental factors, including high iodine intake, selenium deficiency, and pollutants such as tobacco smoke, as well as infectious diseases and certain drugs, have been implicated in the development of AITDs in genetically predisposed individuals. The susceptibility of the thyroid to AITDs may come from the complexity of hormonal synthesis, peculiar oligoelement requirements, and specific capabilities of the thyroid cell�s defense system. An improved understanding of this interplay could yield novel�treatment pathways, some of which might be as simple as identifying the need to avoid smoking or to control the in- take of some nutrients.
Introduction
The thyroid gland is important in the human body because of its ability to produce hormones necessary for appropriate energy levels and an active life. These molecules have pleiotropic effects, playing critical roles in early brain development, somatic growth, bone maturation, and the mRNA synthesis of more than 100 proteins that constantly regulate each and every bodily function.
At the same time, the thyroid is highly vulnerable to autoimmune diseases. The incidence of chronic autoimmune thyroiditis (CAT) and Graves� disease (GD) has in- creased dramatically over the past few decades, afflicting up to 5% of the general population. In children, CAT is the most common cause of acquired hypothyroidism in non-endemic goiter areas.
Initial studies on the association between early fetal nutrition and the pathogenesis of autoimmune thyroid diseases (AITDs) resulted in controversial data. In twin studies, Phillips et al. [1] found that among monozygotic twins the smaller twin had higher levels of thyroid per- oxidase (TPO) antibodies. However, these data were not�confirmed in another twin study in which a larger cohort was analyzed [2]. The �accelerator hypothesis� and the influence of rapid childhood growth due to energy-dense food and adipokine imbalance have not been investigated in childhood AITDs. In both type 1 and type 2 diabetes, the accelerator hypothesis proposes a critical influence of obesity as an exogenous factor contributing to disease; even in a population of children with type 1 diabetes, the fattest presented with disease the earliest (evidence of true acceleration) [3]. With regard to AITDs, other accelerators in addition to obesity include low selenium (Se) and a high iodine intake. Obese children are hyperleptinemic, and leptin, with its numerous functions including the promotion of cell-mediated immune responses, is a good candidate for contributing to the pathogenesis of autoimmune diseases. Obese children have been found to have increased interferon (IFN)- -secreting T helper cells and altered thyroid structure and hormonal status [4�8].
Autoimmunity is generally considered to be only a cause of disease; nevertheless, human T cell repertoires naturally comprise autoimmune lymphocytes. Autoimmune T cells can help heal damaged tissues, indicating that natural autoimmunity can also contribute to health and benefit self-maintenance [9]. The immune system makes its decisions and acts by integrating multiple signals in an ongoing dialog with tissues. It is likely that the tissue itself provides signals that trigger the type of inflammation that is required for tissue self-maintenance and repair [9, 10].
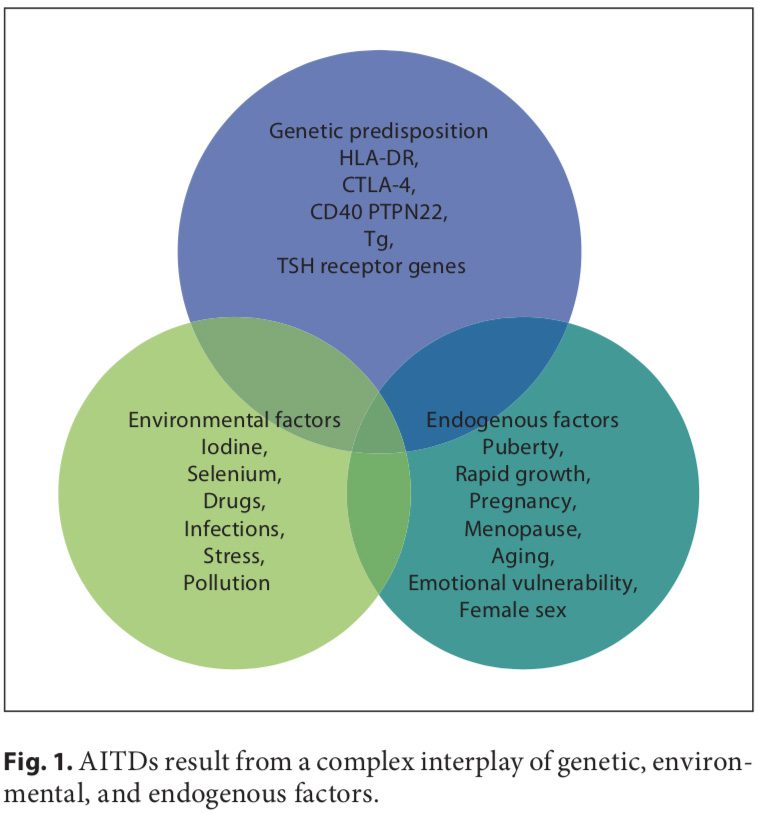
Autoimmune disorders result from a complex interplay of genetic, environmental, and endogenous factors (fig. 1), and a combination of these factors is required to initiate thyroid autoimmunity [11, 12]. Recent advances in genome-wide studies have made it possible to efficient- ly identify complex disease-associated genes. Using both the candidate gene approach and whole-genome linkage studies, 6 AITD susceptibility genes have been identified and confirmed; the first group includes the immunomodulatory gene products HLA-DR, CD40, cytotoxic T lymphocyte-associated factor (CTLA-4), and protein tyrosine phosphatase 22 (PTPN22), and the second group includes the thyroid-specific gene products thyroglobulin (Tg) and thyroid-stimulating hormone receptor (TSHR). Genetic factors predominate, accounting for approximately 80% of the likelihood of developing AITDs, whereas at least 20% is due to environmental factors (fig. 1). In recent years, a number of excellent reviews have been published on the genetic background of AITDs [13, 14].
An increased frequency of AITDs is reported in Turner syndrome (TS) and in other nondisjunctional chromosomal disorders such as Down and Klinefelter syndromes. The theory that maternal autoimmunity may lead to the preferential survival of a fetus with chromosomal aneuploidy is attractive but remains unproven [15]. The most prevalent autoimmune disorder in TS appears to be CAT, with a reported thyroid autoantibody incidence of 30� 50%. Hypothyroidism of autoimmune origin is so common in TS that almost every other TS woman will prob- ably develop hypothyroidism, and it increases with age [16, 17].
We know more about the minor details of AITDs, but the main question remains unanswered: why is the thyroid so prone to autoimmune disease? This review seeks to emphasize the role of the thyroid cell per se in AITDs and to focus attention on preventable exogenous factors.
Thyroid Cell Specificity
The thyroid cell produces a variety of immunologically active factors (table 1) and has complex nutrient requirements for hormonal synthesis and function (table 2), both of which influence susceptibility to AITDs. Thus, the thyroid cell is not just the innocent victim of an�unchecked and disordered immune system. It is increasingly obvious that the target cells interact with the immune system, often in ways that seem defensive and protective, yet they can go awry and exacerbate autoimmunity under particular circumstances [11].
In most human autoimmune diseases, the events that trigger autoimmunity remain elusive. Most importantly, it is unclear whether autoimmunity results primarily from an immune defect, is secondary to target organ alterations, or both. The thyroid shows increased iodine uptake and oxidation prior to lymphocytic infiltration concomitant with decreased thyroid epithelial cell proliferation in vitro. Modifying thyroid function influences the development of thyroid autoimmunity [18]. The thyroid cell, unlike other epithelial cells in the endocrine system, is unique because it releases hormonal products on its basal surface instead of its apical surface, thus allowing for the trafficking of precious iodine twice across the cell.
Thyroid cells are capable of producing different factors (table 1), including IGF I, IGF II, and EGF, that can stimulate angiogenesis. The half-life of these molecules is short and they induce only local (non-systemic) effects. Stimulated thyroid follicular cells secrete several growth factors [19]. The expression of intercellular adhesion molecule-1 (ICAM-1) and lymphocyte function-associated antigen-3 (LFA-3) by thyroid cells is enhanced by IFN- , tumor necrosis factor (TNF), and interleukin (IL)-1. Thyroid cells express CD44, which acts as a homing receptor for hyaluronan, mediates leukocyte rolling (the first step in tissue homing), and may (like ICAM-1) induce lymphocyte activation under certain circumstances. Thyroid cells are now known to produce many cytokines (especially after stimulation with IL-1), including IL-1, IL-6, IL-8, IL-12, IL-13, and IL-15 [11]. Activated lymphocytes can produce TSH, which could have a variety of implications [20].
Low dose tolerance can easily be broken, and the thyroid is not well tolerated by the immune system. Auto- antigens in AITDs, as in other autoimmune endocrine diseases, include tissue-specific membrane receptors, enzymes, and secreted hormones. Mixed cellular and anti- body autoimmune responses are likely pathogenic to some degree. Circulating anti-Tg autoantibodies are also found in GD and CAT, as are autoantibodies to triiodothyronine (T3) and thyroxine (T4). The human (h) TSHR is the primary antigenic target in autoimmune hyperthyroidism [21]. The TPO autoantibody seems unlikely to have much pathogenic importance as it has limited access to TPO in vivo due to its location inside the cell. Further- more, anti-TPO autoantibodies do not inhibit the activity�of the enzyme. Thus, their clinical value is principally to document thyroid gland autoimmunity. However, TPO may act as a hidden antigen because it is not adjacent to the vasculature.
In humans, excess thyroid hormone results in the attenuation of natural killer (NK) cell activity, which in theory could lead to the continuation of an autoimmune disorder. Upon return to a euthyroid status and the resulting normalization of NK activity, a reversion to control of the abnormal immune reaction would occur with perpetuation of GD. Additionally, an anti-idiotype might function as an agonist for the original antigen. Thus, an antibody to an antibody (anti-idiotype) to TSH might bind to the TSHR and stimulate the thyroid [22]. A more likely hypothesis is that anti-idiotypic antibodies are rarely produced at a detectable level. Hodkinson et al. [23] recently found a positive association between thyroid hormone concentration and NK-like T cells in the elderly. This relationship has not been investigated in young patients.
Antigen Presentation By The Thyroid Cell
Bottazzo et al. [24] first suggested that antigen presentation by HLA-DR-expressing thyroid cells may be a critical aspect of thyroid autoimmune disease. It quickly became apparent that the only stimulus able to induce MHC class II expression on thyroid cells was the T cell cytokine IFN- . Normal cells respond exactly the same as AITD thyroid cells to IFN- , and in animal models of AITDs class II expression on thyroid cells is always followed by the appearance of lymphocytes in the gland. In addition to inducing MHC class II expression, IFN- increases MHC class I expression on thyroid cells, thus allowing potential for the recognition of thyroid cells by cytotoxic CD8+ T cells [11].
It is possible that direct antigen presentation by the thyroid cell itself may occur in individuals who inherit thyroid-reactive T cells; such a circumstance would effectively bypass the classical macrophage-processing mechanism. The HLA-DR antigen-expressing thyroid cell may be as effective as the macrophage at presenting thyroid- specific antigens to the immune system [25], but the thyroid cell is incapable of supplying the costimulatory signals that professional antigen-presenting cells (APCs) do [11]. Any stimulus that causes increased DR expression on thyrocytes, such as IFN- produced by T cells in response to infection, combined with increased TSH stimulation may allow thyrocytes to function as APCs. Although thyroid cells may perform this function poorly, they are numerous and localized in one area, therefore allowing for increased production of the already established normally occurring low levels of antibodies [12].
Environmental Factors
A number of environmental factors have been implicated in the development of AITD in genetically predisposed individuals, including high iodine intake, Se deficiency, pollutants such as tobacco smoke, infectious dis- eases, certain drugs, and physical and emotional stress [26�30]. Herein, we focus on these preventable triggers. Individual susceptibility suggests that, in addition to genetics, some endogenous factors are also important to the development of AITDs, such as growth spurts in childhood, puberty, pregnancy, menopause, aging, and gender (fig. 1, 2).
Iodine
Dietary iodine plays an important role in the expression of AITDs. Epidemiological studies have suggested that AITDs are more common in areas of iodine sufficiency than in areas of iodine deficiency and that general increases in AITDs occur in parallel with increases in dietary iodine. CAT is less common in countries with a low iodine intake [27].
The thyroid requires the right amount of iodine. Either too much or too little causes problems. Too little io- dine brings all of the adaptive immune mechanisms of the thyroid into play, but despite these responses iodine deficiency disorders may still result. Too much iodine also affects the thyroid. Protective mechanisms include diminished trapping of iodide by the thyroid and de- creased iodide organification. In experimental thyroiditis several types of Tg epitopes have been found, including some containing iodine and/or hormones as well as some conformational epitopes. Experimentally increasing the iodination of Tg makes the protein more antigen- ic [28, 31]. Optimally, the iodine intake of a population should be kept within a relatively narrow interval that prevents iodine disorders, but not higher [29].
The mechanism of action of iodine in contributing to thyroid autoimmunity is not clear. Iodine may stimulate B lymphocytes to increase the production of immunoglobulin and thus induce AITDs by enhancing the activity of lymphocytes that have been primed by thyroid- specific antigens [30]. Iodine may enhance the antigen- presenting capabilities of macrophages, resulting in increased macrophage activity and enhanced lymphocyte stimulation. In addition, a high iodine intake in- creases the iodine content of the Tg molecule, which may increase its immunogenicity [31]. Lastly, iodine may provoke thyroid follicular cells to become APCs and thus potentiate AITDs by turning genetically predisposed normal thyrocytes into antigen-presenting thyrocytes.
Table 2 shows several minerals and trace elements that are essential for normal thyroid hormone metabolism. The role of these elements in childhood AITDs has not been well investigated.
Selenium
The second factor that has been strongly implicated in the development of autoimmune thyroiditis is the trace element Se. Se is a constituent of selenoproteins (SePs), in which it is incorporated as selenocysteine. Relevant actions of Se and SePs include antioxidant effects, appropriate functioning of the immune system, antiviral effects, influence on fertility, and a beneficial effect on mood [32]. Se deficiency is thought to be involved in the pathogenesis of autoimmune thyroiditis by lengthening the duration and exacerbating the severity of the disease; these effects may occur via reduced activity of the SeP glutathione peroxidase, which leads to an increased production of hydrogen peroxide. Another important class of SePs are the iodothyronine selenodeiodonases D1 and D2, which are responsible for producing biologically active T3 via 5 -deiodination in extrathyroidal tissues [33, 34].
Combined Se and iodine deficiencies lead to myxedematous cretinism. Adequate Se nutrition supports efficient thyroid hormone synthesis and metabolism and protects the thyroid gland from damage from excessive iodine exposure. In regions having severe combined deficiencies of iodine and Se, it is mandatory to normalize the Se supply before the initiation of iodine supplementation to prevent hypothyroidism [35].
In celiac disease, the inability to absorb Se may modulate SeP gene expression and promote intestinal mucosal damage, and this deficiency could additionally predispose to complications such as AITDs [34, 36].
Derumeaux et al. [37] discovered an inverse association between Se status and thyroid volume and echo- structure in French adults and concluded that Se may protect against AITDs. Duntas et al. [38] found beneficial effects when treating patients with autoimmune thyroiditis with selenomethionine for 6 months due to its ability to reduce anti-TPO antibodies. In the group treat- ed with LT4 combined with Se, these effects were very prominent in the first 3 months and were further sustained after 6 months of treatment. A striking majority of the patients reported an improvement in mood and well-being.
Environmental Pollutants
Various environmental toxins and pollutants have been implicated in the induction of AITDs.
Polyhalogenated biphenyls are commonly used com- pounds with a wide variety of industrial applications. Polybrominated biphenyls are flame retardant, and polychlorinated biphenyls (PCBs) are used as lubricants, adhesives, inks, and plasticizers. PCBs are known to accumulate in lakes and rivers and subsequently in the adipose tissue of fish and humans [27]. These compounds might trigger AITDs by interfering with iodide transport and inducing oxidative stress. There is evidence that peri- natal PCB exposure decreases thyroid hormone levels in rat pups. In adults, adolescents, and children from highly PCB-exposed areas, the concentration of PCBs in blood samples negatively correlated with levels of circulating thyroid hormones [39, 40]. Populations with long-term exposure to PCBs have increased prevalences of anti-TPO antibodies, which is probably related to the immunomodulatory effects of PCBs. Pollutants from car emissions and heavy industry as well as coal pollution and agricultural fungicides are also implicated in AITD development [26, 27].
Smoking is associated with an increased risk of developing GD and with a reduced remission rate after thionamide treatment. Even more striking is the effect of smoking on Graves� orbitopathy, which tends to be more severe in smokers [32, 41]. Smoking might contribute to the pathogenesis of GD by altering the structure of the thyrotropin receptor, making it more immunogenic and leading to the production of thyrotropin receptor-stimulating antibodies that react strongly with retroorbital tissue [41]. Smoking induces the polyclonal activation of B and T cells and increases presentation of antigens by damaged cells. Hypoxia may play a role in Graves� orbitopathy because retrobulbar fibroblasts show a significant increase in proliferation and glycosaminoglycan production when cultured under hypoxic conditions [42, 43]. The effects of parental smoking on thyroid function in fetuses or 1-year-old infants [44] provide additional insight into the interrelationship between smoking and thyroid dysfunction. The latter study found that infants whose mothers and fathers smoked had higher cord serum concentrations of Tg and thiocyanate than did infants whose parents did not smoke. The clinical picture observed in adolescents exposed to passive smoking could be due to direct stimulation of sympathetic nervous activity by nicotine in addition to the smoking-induced increase in thyroid hormone secretion [45].
The association of smoking with CAT is less well defined. Although a relationship with autoimmune hypothyroidism or postpartum thyroiditis has been reported, this finding was not supported by meta-analysis of the published papers [32, 45].
Infections
In some individuals, autoimmunity is the price that must be paid for the eradication of an infectious agent. Infections have been implicated in the pathogenesis of several autoimmune, endocrine, and non-endocrine diseases. Either viral or bacterial infections might represent a risk factor for the development of AITDs. Viruses have long been suspected as etiological agents in many auto- immune diseases, including AITDs; moreover, a viral cause of AITDs, infecting either the thyroid or immune cells, has been demonstrated in an avian model. Although viruses may be likely etiological agents in human AITDs, this possibility remains unproven [25, 27, 30].
An increased frequency of antibodies to the influenza B virus has been observed in a group of patients with thyrotoxicosis. In addition, virus-like particles have been found in the thyroids of chickens with autoimmune thyroiditis, with similar particles detected in the thyroids of humans. Serological evidence of prior staphylococcal and streptococcal illnesses has been described in a few patients with AITDs [27].
Some of the strongest evidence linking infectious agents to the induction of AITDs has been the association of Yersinia enterocolitica infection with thyroid disease. This Gram-negative coccobacillus commonly causes diarrhea along with a variety of abnormalities that suggest autoimmune disease, including arthralgias, arthritis, erythema nodosum, carditis, glomerulonephritis, and iritis. Weiss et al. [46] demonstrated that Y. enterocolitica had a saturable, hormone-specific binding site for the mammalian TSH that resembled the receptor for TSH in the human thyroid gland.
An immune response against a viral antigen that shares homology with the TSHR may be the inductive event that ultimately leads to TSHR autoimmunity [21]. A significant association between hepatitis C and AITDs has been found. Anti-TPO antibody titers have been shown to increase at the end of treatment with IFN- in patients with the hepatitis C virus, and these patients were more susceptible to AITDs than were hepatitis B patients. These patients should be screened for autoimmune thyroiditis before and after IFN treatment [47, 48].
Infection might induce an autoimmune response by various mechanisms, such as molecular mimicry, polyclonal T cell activation by microbial superantigens, and increased thyroid expression of human leukocyte anti- gens [49]. Inflammation induced by viral infections or by pollutants can modify cell signaling pathways and influence T cell activity and cytokine secretion profiles [26].
Drugs
Several drugs have been implicated in the pathogenesis of AITDs. Amiodarone is an iodine-containing drug with diverse effects on thyroid function. Serum titers of TPO antibodies are elevated in approximately half of the patients who develop amiodarone-induced hypothyroid- ism. Amiodarone has also been shown to affect T cell function [27]. Thyroid antibodies disappeared from the circulation 6 months after amiodarone discontinuation [32].
Lithium, a psychopharmaceutical and well-known goitrogen, has been shown to inhibit thyroid hormone release. Antithyroid antibodies are found more frequently in psychiatric patients on lithium therapy than in similar psychiatric patients treated with other drugs. Lithium-induced increases in serum TSH concentrations might enhance autoantigen expression on the surface of thyrocytes, thereby exacerbating autoimmune responses [32, 50].
Other agents involved in thyroid autoimmunity are IL-2 (thyroid autoimmune phenomena with or without hypothyroidism), IFN- (thyroid dysfunction, hypothyroidism, and occurrence of thyroid autoantibodies), highly active antiretroviral therapy (HAART; possible occurrence of thyroid autoimmune phenomena and dysfunction), and Campath-1H, a humanized monoclonal antibody targeting the CD52 antigen on lymphocytes and monocytes that is used after transplantation (occurrence of GD) [32].
Stress
Although numerous anecdotal reports have associated the onset of AITDs, and particularly GD, with stressful events, objective evidence has been difficult to obtain. Both psychological stress, such as bereavement, and physical stress, such as trauma or major illness, have been implicated [27].
Neuroendocrine immune mechanisms responsible for the putative effects of stress on the onset and course of GD are poorly defined, but they might include activation of the HPA axis (although this should cause immunosuppression) and a shift from a Th1 (cell-mediated) immune response to a Th2 (humoral) immune response [32, 51].
Additionally, heat shock proteins (HSPs), which are well-known stress proteins, could share epitopes with the TSHR. Heufelder et al. [52] found that high levels of HSP- 72 expression in AITDs may reflect a state of chronic cellular stress, but this finding could also indicate an immunomodulatory function of HSP-72 in AITDs. HSPs are ubiquitous, highly conserved proteins that are expressed in response to a wide variety of physiological and environmental insults. They allow cells to survive otherwise lethal conditions. HSPs have been postulated to be critical antigens in both autoimmune diseases and experimental models of autoimmunity [53, 54].
Improving stress by the prolonged use of bromazepam has been shown to increase the remission rate of hyper- thyroidism after a thionamide course [55]. The relation- ship between stress and CAT is less evident. Graves� patients might be stressed because of hyperthyroidism and not hyperthyroid because of stress, whereas CAT patients are not stressed because they are euthyroid or hypothyroid [32]. Whatever the mechanism of action, stress may cause decompensation in a genetically susceptible individual and lead to the induction or exacerbation of an AITD.
Pregnancy And Postpartum
AITDs tend to be more frequent in women. The reason for this gender-related difference is not clear and is not explained by the additional X chromosome in females [42]. The possibility that genes responsible for immune responses are located on the X chromosome has been considered but not confirmed. Sex steroids could modify immune responses by acting directly on immune cells. Estrogens are well-known stimulators of TSH secretion, which could enhance HLA-DR expression. Parity per se does not seem to play a significant role [32, 56].
The accumulation of fetal cells in the maternal thyroid gland during pregnancy (painless postpartum thyroiditis) may induce autoimmune thyroiditis [57]. Pregnancy is accompanied by a suppression of the immune system with a shift in the Th1/Th2 balance towards Th2 immunity, a process that is aimed at protecting the fetus. A possible link between pregnancy and the postpartum occurrence of AITDs might be represented by fetal microchimerism. Fetal cells pass into the maternal circulation and may persist in the maternal blood. Microchimerism of presumed fetal origin has been shown in thyroid tissue specimens of women with previous pregnancies, particularly in those with AITDs. The persistence of activated�intrathyroidal fetal cells might influence thyroid autoimmunity in genetically susceptible women by modulating or even initiating maternal immune responses in a graft- versus-host reaction upon termination of pregnancy-re- lated immune suppression. It cannot presently be ruled out, however, that intrathyroidal fetal cells are only innocent bystanders and do not participate in triggering or exacerbating thyroid autoimmune responses [32, 54, 58]. Mothers who have given birth to sons have thyroidal Y chromosome-positive cells more frequently if they are affected by either CAT or GD than if they have thyroid adenomas [59].
The presence of elevated TPO antibodies in about 10% of pregnant women is associated with an increased risk of miscarriage, gestational thyroid dysfunction, and postpartum thyroiditis [48]. Maternal-to-fetal transfer of TSHR antibodies with polyclonal activity and a different half-life can lead to a transient perinatal thyroid dysfunction, opposite to a maternal one [60].
Conclusion
A rapidly growing body of evidence on the interplay between genetic, environmental, and endogenous factors has expanded our knowledge of the complex etiopathogenesis of AITDs. Autoimmune thyroid disorders are examples of common diseases in which immunogenetic factors play an important role.
The thyroid cell itself appears to play a major role in disease progression by interacting with the immune system. The complexity of hormonal synthesis, unique oligoelement requirements, and the specific capabilities of the thyroid cell defense system probably make the thyroid prone to AITDs. The initial insult to the human thyroid gland that activates the onset of AITDs remains un- known and seems to be strongly individual. Understand- ing more about the interaction between genes and the environment could yield entirely novel pathways, some of which might be as simple as identifying the need to avoid smoking or to control the intake of particular nutrients. Evidence for many causal agents is, however, scarce, and more data are certainly required. We believe that it is particularly important to draw attention to this problem in pediatric patients. Lessons learned from the enigmatic questions raised in AITD studies could clarify the pathogenesis of other organ-specific autoimmune disorders.
L. Saranac S. Zivanovic B. Bjelakovic H. Stamenkovic M. Novak B. Kamenov Pediatric Clinic, University Clinical Center, Nis, Serbia
Blank
References:
1 Phillips DI, Osmond C, Baird J, Huckle A,
Rees-Smith B: Is birthweight associated with
thyroid autoimmunity? A study in twins.
Thyroid 2002;12:377�380.
2 Brix TH, Hansen PS, Rudbeck AB, Hansen
JB, Skythe A, Kyvik KO, Hegedus L: Low
birth weight is not associated with thyroid
autoimmunity: a population-based twin
study. J Clin Endocrinol Metab 2006;91:
3499�3502.
3 Wilkin TJ: The great weight gain experiment,
accelerators and their implications for
autoantibodies in diabetes. Arch Dis Child
2006;91:456�458.
4 Matarese G, La Cava A, Sanna V, Lord MG,
Lechler RI, Fontana S, Zappacosta S: Balancing
susceptibility to infection and autoimmunity:
a role of leptin? Trends Immunol
2002;23:182�187.
5 Radetti G, Kleon W, Buzi F, Crivellero C,
Pappalardo L, Di Lorgi N, Maghnie M: Thyroid
structure and function are affected in
childhood obesity. J Clin Endocrinol Metab
2008;93:4749�4754.
6 Pacifico L, Di Renzo L, Anania C, Osborn JF,
Ippoliti F, Schiavo E, Chiesa C: Increased Thelper
interferon-gamma-secreting cells in
obese children. Eur J Endocrinol 2006;154:
691�697.
7 Marras V, Casini MR, Pilia S, Carta D, Civolani
P, Porcu M, Uccheddu AP, Loche S: Thyroid
function in obese children and adolescents.
Horm Res Paediatr 2010;73:193�197.
8 Saranac L, Zivanovic S, Novak M: High fT3
(free triiodothyronine), new syndrome or innocent
bystander. Endocr Abstracts Eur
Congr Endocrinol, Prague, 2010, p 771.
9 Schwartz M, Cohen IR: Autoimmunity can
benefit self-maintenance. Immunol Today
2000;21:265�268.
10 Cohen IR, Schwartz M: Autoimmune maintenance
and neuroprotection of the central
nervous system. J Neuroimmunol 1999;100:
111�114.
11 Weetman AP: Autoimmune thyroid disease:
propagation and progression. Eur J Endocrinol
2003;148:1�9.
12 Weetman AP: New aspects of thyroid autoimmunity.
Horm Res 1997;48(suppl 4):51�
54.
13 Jacobson EM, Tomer Y: The CD40, CTLA-4,
thyroglobulin, TSH receptor, and PTPN22
gene quintet and its contribution to thyroid
autoimmunity: back to the future. J Autoimmun
2007;28:85�98.
14 Tomer Y, Huber A: The etiology of autoimmune
thyroid disease: a story of genes and
environment. J Autoimmun 2009;32:231�
239.
15 Saenger P: Turner syndrome; in Sperling MA
(ed): Pediatric Endocrinology, ed 3. Philadelphia,
Saunders Elsevier, 2008, pp 610�661.
16 El-Mansoury M, Bryman I, Berntorp K,
Hanson C, Wilhelmsen L, Landin-Wilhelmsen
K: Hypothyroidism is common in Turner
syndrome: results of a five-year follow up.
J Clin Endocrinol Metab 2005;90:2131�2135.
17 Mortensen KH, Cleemann L, Hjerrild BE,
Nexo E, Locht H, Jeppesen EM, Gravholt
CH: Increased prevalence of autoimmunity
in Turner syndrome � influence of age. Clin
Experim Immunol 2009;156:205�210.
18 Homo-Delarche F, Boitard C: Autoimmune
diabetes: the role of the islets of Langerhans.
Immunol Today 1996;17:456�460.
19 Denef JF, Ovaert C, Many MC: Experimental
goitrogenesis (in French). Ann Endocrinol
(Paris) 1989;50:1�15.
20 Fabry Z, Raine CS, Hart MN: Nervous tissue
as an immune compartment: the dialect of
the immune response in the CNS. Immunol
Today 1994;15:218�224.
21 Song YH, Li Y, Maclaren NK: The nature of
autoantigens targeted in autoimmune endocrine
diseases. Immunol Today 1996;17:232�
238.
22 Zakarija M, McKenzie JM: The spectrum
and significance of autoantibodies reacting
with the thyrotropin receptor. Endocrinol
Metab Clin North Am 1987;16:343�364.
23 Hodkinson CF, Simpson EEA, Beattie JH,
O�Conor JM, Campbell DJ, Strain JJ, Wallace
JM: Preliminary evidence of immune function
modulation by thyroid hormones in
healthy men and women aged 55�70 years. J
Endocrinol 2009;202:55�63.
24 Botazzo GF, Pujol-Borrell R, Hanafusa T,
Feldmann M: Role of aberrant HLA-DR expression
and antigen presentation in induction
of endocrine autoimmunity. Lancet
1983;2:1115�1119.
25 Davies TF, Piccini LA: Intrathyroidal MHC
class II antigen expression and thyroid autoimmunity.
Endocrinol Metab Clin North
Am 1987;16:247�268.
26 Duntas LH: Environmental factors and autoimmune
thyroiditis. Nat Clin Pract Endocrinol
Metab 2008;4:454�460.
27 Safran M, Paul TL, Roti E, Braverman LE:
Environmental factors affecting autoimmune
thyroid disease. Endocrinol Metab
Clin North Am 1987;6:327�342.
28 Dunn JT: What is happening with our iodine?
J Clin Endocrinol Metab 1998;3398�
3400.
29 Laurberg P, Cerqueira C, Ovesen L, Rasmusen
LB, Perrild H, Andersen S, Pedersen IB,
Carle A: Iodine intake as a determinant of
thyroid disorders in population. Best Pract
Res Clin Endocrinol Metab 2010;24:13�27.
30 Weetman AP, McGregor AM: Autoimmune
thyroid disease: developments in our understanding.
Endocr Rev 1984;5:309�355.
31 Carayanniotis G, Rao VP: Searching for
pathogenic epitopes in thyroglobulin: parameters
and caveats. Immunol Today 1997;
18:83�88.
32 Bartalena L, Tanda ML, Piantanida E, Lai A,
Compri E, Lombardi V: Environment and
thyroid autoimmunity; in Wiersinga WM,
Drexhage HA, Weetman AP, et al (eds): The
Thyroid and Autoimmunity: Merck European
Thyroid Symposium Noordwijk 2006,
June 15�18. Stuttgart, Thieme, 2007 pp 60�
73.
33 Berry MJ, Bany L, Larsen PR: Type I iodothyronine
deiodinase is a selenocysteine-containing
enzyme. Nature 1991;349:438�440.
34 Duntas LH: Selenium and inflammation:
underlying anti-inflammatory mechanisms.
Horm Metab Res 2009;41:443�447.
35 Zimmerman MB, Kohrle J: The impact of
iron and selenium deficiencies on iodine and
thyroid metabolism: biochemistry and relevance
to public health. Thyroid 2002;12:
867�878.
36 Duntas LH: Does celiac disease trigger autoimmune
thyroiditis. Nat Rev Endocrinol
2009;5:190�191.
37 Derumeaux E, Valeix P, Castetbon K, Bensimon
M, Boutron-Ruault MC, Arnaud JH,
Hercberg S: Association of selenium with
thyroid volume and echostructure in 35- to
60-year-old French adults. Eur J Endocrinol
2003;148:309�315.
38 Duntas LH, Mantzou E, Koutras DA: Effects
of a six month treatment with selenomethionine
in patients with autoimmune thyroiditis.
Eur J Endocrinol 2003;148:389�393.
39 Meerts IA, Assink Y, Cenijn PH, Van Den
Berg JH, Weijers BM, Bergman A, Koeman
JH, Brouwer A: Placental transfer of a hydroxylated
polychlorinated biphenyl and effects
on fetal and maternal thyroid hormone
homeostasis in the rat. Toxicol Sci 2002;68:
361�372.
40 Boas M, Feldt-Rasmussen U, Skakkebaek
NE, Main KM: Environmental chemicals
and thyroid function. Eur J Endocrinol 2006;
154:599�611.
41 Utiger RD: Effects of smoking on thyroid
function. Eur J Endocrinol 1998;138:368�
369.
42 Prummel MF, Strieder T, Wiersinga WM:
The environment and autoimmune diseases.
Eur J Endocrinol 2004;150:605�618.
43 Pontikides N, Krassas GE: Influence of cigarette
smoking on thyroid function, goiter
formation and autoimmune thyroid disorders.
Hormones (Athens) 2002;1:91�98.
44 Gasparoni A, Autelli M, Ravagni-Probizer
MF, Bartoli A, Regazzi-Bonora M, Chirico
G, Rondini G: Effect of passive smoking on
thyroid function in infants. Eur J Endocrinol
1998;138:379�382.
45 Vestergaard P: Smoking and thyroid disorders
� a meta-analysis. Eur J Endocrinol
2002;146:153�161.
46 Weiss M, Ingbar SH, Winblad S, Kasper DL:
Demonstration of a saturable binding site for
thyrotropin in Yersinia enterocolitica . Science
1983;219:1331�1333.
47 Fernandez-Soto L, Gonzales A, Escobar-Jimenez
F, Vazquez R, Ocete E, Olea N, Salmeron
J: Increased risk of autoimmune thyroid
disease in hepatitis C vs B before, during and
after discontinuing interferon therapy. Arch
Intern Med 1998;158:1445�1448.
48 Testa A, Castaldi P, Fanti V, Fiore GF, Grieco
V, De Rosa A, Pazardjklian MG, De Rosa G:
Prevalence of HCV antibodies in autoimmune
thyroid disease. Eur Rev Med Pharmacol
Sci 2006;10:183�186.
49 Davies TF: Infection and autoimmune thyroid
disease. J Clin Enocrinol Metab 2008;93:
674�676.
50 Lazarus JH, John R, Bennie EH, Chalmers
RJ, Crockett G: Lithium therapy and thyroid
function: a long-term study. Psychol Med
1981;11:85�92.
51 Dayan CM: Stressful life events and Graves�
disease revisited. Clin Endocrinol (Oxf)
2001;55:13�14.
52 Heufelder AE, Goellner JR, Wenzel BE,
Bahn RS: Immunohistochemical detection
and localization of a 72-kilodalton heat
shock protein in autoimmune thyroid disease.
J Clin Endocrinol Metab 1992;74:724�
731.
53 Parcellier A, Gurbuxani S, Schmitt E, Solary
E, Garrido C: Heat shock proteins, cellular
chaperones that modulates mitochondrial
cell death pathways. Biochem Biophys Res
Commun 2003;304:505�512.
54 Gaston JS: Are heat shock proteins involved
in autoimmunity? Int Clin Lab Res 1992;22:
90�94.
55 Benvenga S: Benzodiazepine and remission
of Graves� disease. Thyroid 1996;6:659�660.
56 Adams D: How the immune system works
and why it causes autoimmune diseases. Immunol
Today 1998;17:300�303.
57 Pierce EN, Farwel AP, Braverman LE: Thyroiditis.
N Engl J Med 2003;348:2646�2655.
58 Badenhoop K: Microchimerism and the
model of postpartum thyroiditis; in Wiersinga
WM, Drexhage HA, Weetman AP, et
al (eds): The Thyroid and Autoimmunity:
Merck European Thyroid Symposium
Noordwijk 2006, June 15�18. Stuttgart,
Thieme, 2007, pp 99�103.
59 Szabolcs I: Clinical relevance of thyroid peroxidase
autoantibodies in euthyroid individuals;
in Wiersinga WM, Drexhage HA,
Weetman AP, et al (eds): The Thyroid and
Autoimmunity: Merck European Thyroid
Symposium Noordwijk 2006, June 15�18.
Stuttgart, Thieme, 2007, pp 133�142.
60 Saranac L, Miljkovic M, Stamenkovic H, Mileusnic-Milenovic
R, Petrovic G, Kamenov
B: Late onset transient thyroid dysfunction
in children born to mothers with autoimmune
thyroid disease. Facta Univ Ser Med
Biol 2003;10:52�56.
Thyroid disorder is one of the most common disorders. It happens due to under or over functioning of the thyroid gland. According to the statistics on the American Thyroid Association�s website, around 12% of Americans are likely to suffer from some thyroid disease. Moreover, more than 60% of the people are not even aware of their thyroid disorder. There are many kinds of thyroid diseases, and some of them are Goiter, Hyperthyroidism, Thyroid Nodules, Thyroid cancer, and hypothyroidism.
These types of thyroid disorder can be annoying. It is better to treat this type of disorder. First of all, Doctors use various tests to diagnose your disorder to suggest different types of available treatment methods for your thyroid disorder. You should know about the symptoms of thyroid disorder first because you won�t go to the doctor without any reason, will you?
What are the 8 symptoms of thyroid disorder you should not ignore?
As I said before, 60% of the people are not even aware of their thyroid disorder. This shows how important this article is. Here are the 8 symptoms of thyroid disorder you cannot afford to ignore.
Unexplainable Weight Loss
The amount of hormones released by your thyroid gland has an impact on your weight. When your thyroid gland releases more hormones than usual, you are likely to lose weight. This condition is called hyperthyroidism. However, it is the symptom of hyperthyroidism only if it is unexplainable, and i.e. without any change in your regular diet or fitness routine.
Sadness or Depression
Both overactive and under-active thyroid can have an impact on your mood. Too much thyroid hormone can make you feel anxious, irritable, or restless; whereas too less thyroid hormone can make you sad or depressed. It is one of the common thyroid symptoms.
Constipation
If you are having the problem with constipation, and you are not able to kick it, then it could be because of disruption in the production of thyroid hormone. It can slow down your digestion process. This is one of the most common symptoms of hypothyroidism.
Heart Rate
Your thyroid has an impact on many organs of your body, and it includes your heart too. If the rate of your heartbeat is more or less than normal, then it is likely to be a symptom of thyroid disorder. The normal heartbeat is between 60-100 beats per minute, and it depends on various factors like weight, age, height, and other physical conditions.
Swelling In Neck
If your neck is swollen, then it is obvious that something is not right with your thyroid. You just cannot ignore this symptom. It should be taken very seriously, and you should immediately see your doctor. The inflammation in your neck could also have the presence of cancer or nodules. Because many people are not even aware of the common symptoms of thyroid.
Hair Loss
Can your hair loss be the result of thyroid disorder? Yes, it can be. The study shows that abnormal function of your thyroid can lead to hair loss. This is a common symptom, which is shared by both hyperthyroidism and hypothyroidism. Some people look for many different problems to tackle the problem of hair loss, but they don�t have a clue that it could be because of thyroid disorder.
Too Much Sleep
It is obviously very good for your health to have an adequate level of sleep. However, if you are sleeping too much, then there is a problem. If your thyroid is not functioning in a normal manner, then it can have an adverse impact on your body functions. It can slow down your body functions. You may even feel sleepy during daytime if you have a thyroid disorder.
No Interest In Sex
If your mind and body are in the right condition, then you will feel very excited even to hear the word �sex.� However, if you are losing interest in sex, then you should realize that there is something seriously wrong with your health. The study shows that thyroid disorder may cause sexual dysfunction among men, and it can also affect sexual health of women. If you�re having the problem of low libido, then you should be concerned about your health.
Conclusion
By now you are aware of all the 8 symptoms of thyroid disorder you cannot afford to ignore. If you experience any of these symptoms, then you must be alert. Some types of thyroid disorder demand a regular visit to the doctor along with regular treatments.
Neither you should keep your thyroid disorder untreated, nor you should be careless regarding your treatment by keeping it under-treated because this can lead to serious consequences. This may also result in life-threatening problems. The study shows that thyroid disorder is also linked to the increased risk of sudden cardiac death. Analyze your body conditions and stay safe.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine








 Autoimmune disorders result from a complex interplay of genetic, environmental, and endogenous factors (fig. 1), and a combination of these factors is required to initiate thyroid autoimmunity [11, 12]. Recent advances in genome-wide studies have made it possible to efficient- ly identify complex disease-associated genes. Using both the candidate gene approach and whole-genome linkage studies, 6 AITD susceptibility genes have been identified and confirmed; the first group includes the immunomodulatory gene products HLA-DR, CD40, cytotoxic T lymphocyte-associated factor (CTLA-4), and protein tyrosine phosphatase 22 (PTPN22), and the second group includes the thyroid-specific gene products thyroglobulin (Tg) and thyroid-stimulating hormone receptor (TSHR). Genetic factors predominate, accounting for approximately 80% of the likelihood of developing AITDs, whereas at least 20% is due to environmental factors (fig. 1). In recent years, a number of excellent reviews have been published on the genetic background of AITDs [13, 14].
Autoimmune disorders result from a complex interplay of genetic, environmental, and endogenous factors (fig. 1), and a combination of these factors is required to initiate thyroid autoimmunity [11, 12]. Recent advances in genome-wide studies have made it possible to efficient- ly identify complex disease-associated genes. Using both the candidate gene approach and whole-genome linkage studies, 6 AITD susceptibility genes have been identified and confirmed; the first group includes the immunomodulatory gene products HLA-DR, CD40, cytotoxic T lymphocyte-associated factor (CTLA-4), and protein tyrosine phosphatase 22 (PTPN22), and the second group includes the thyroid-specific gene products thyroglobulin (Tg) and thyroid-stimulating hormone receptor (TSHR). Genetic factors predominate, accounting for approximately 80% of the likelihood of developing AITDs, whereas at least 20% is due to environmental factors (fig. 1). In recent years, a number of excellent reviews have been published on the genetic background of AITDs [13, 14].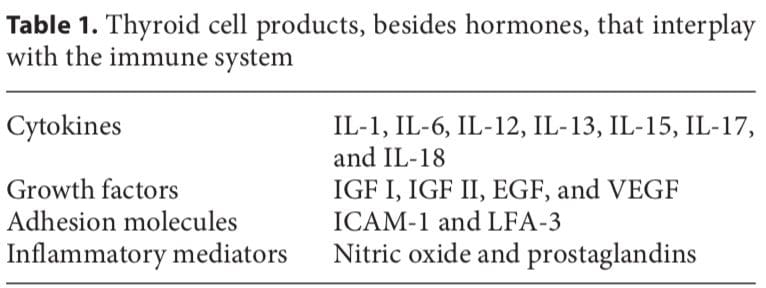
 In most human autoimmune diseases, the events that trigger autoimmunity remain elusive. Most importantly, it is unclear whether autoimmunity results primarily from an immune defect, is secondary to target organ alterations, or both. The thyroid shows increased iodine uptake and oxidation prior to lymphocytic infiltration concomitant with decreased thyroid epithelial cell proliferation in vitro. Modifying thyroid function influences the development of thyroid autoimmunity [18]. The thyroid cell, unlike other epithelial cells in the endocrine system, is unique because it releases hormonal products on its basal surface instead of its apical surface, thus allowing for the trafficking of precious iodine twice across the cell.
In most human autoimmune diseases, the events that trigger autoimmunity remain elusive. Most importantly, it is unclear whether autoimmunity results primarily from an immune defect, is secondary to target organ alterations, or both. The thyroid shows increased iodine uptake and oxidation prior to lymphocytic infiltration concomitant with decreased thyroid epithelial cell proliferation in vitro. Modifying thyroid function influences the development of thyroid autoimmunity [18]. The thyroid cell, unlike other epithelial cells in the endocrine system, is unique because it releases hormonal products on its basal surface instead of its apical surface, thus allowing for the trafficking of precious iodine twice across the cell.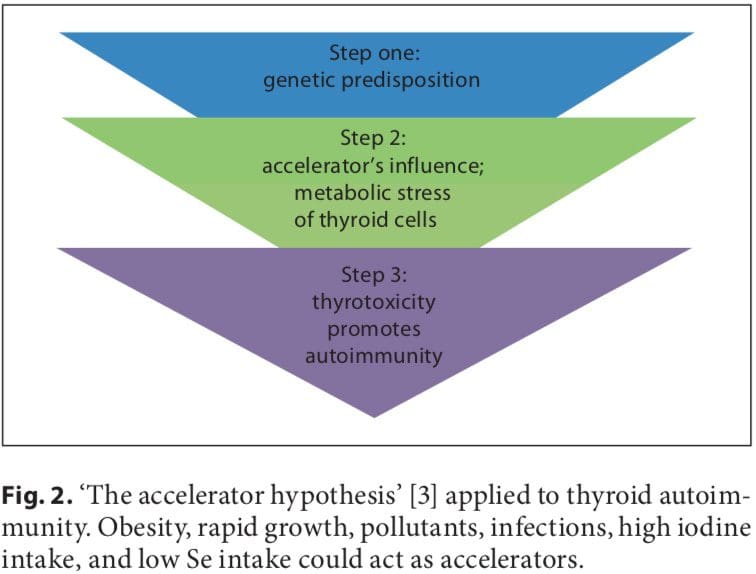 Iodine
Iodine