Physicians, neurologists, and other healthcare professionals may often run a cranial nerve examination as part of a neurological evaluation to analyze the operation of the cranial nerves. This involves a highly formalized series of tests that evaluate the status of each cranial nerve. A cranial nerve test begins with observation of the patient partly due to the fact that cranial nerve lesions may ultimately affect the symmetry of the face or eyes, among other signs and symptoms.
The visual fields for neural lesions or nystagmus�are tested via an evaluation of particular eye movements. The sensation of the face is tested by asking patients to execute different facial movements, like puffing out their cheeks. Hearing is tested through voice and tuning forks. The position of the individual’s uvula is also examined because asymmetry in its placement could indicate a lesion of the glossopharyngeal nerve. After the capability of the individual to use their shoulder to test the accessory nerve (XI), the patient’s tongue operation is generally assessed by detecting various tongue movements.
Damage or Injury of the Cranial Nerves
Compression
Cranial nerves may be compressed due to increased intracranial pressure, a profound effect of an intracerebral haemorrhage, or tumour which presses against the cranial nerves and interferes with the communication of impulses along the length of a nerve. In some instances, a loss of functionality of one cranial nerve may on occasion be the first symptom of an intracranial or skull base cancer.
An increase in intracranial pressure can lead to dysfunction of the optic nerves (II) because of the compression of the surrounding veins and capillaries, resulting in swelling of the eyeball, known as papilloedema. A cancer, such as an optic glioma, can also affect the optic nerve (II). A pituitary tumour can compress the optic tracts or the optic chiasm of the optic nerve (II), causing visual field loss. A pituitary tumour may also extend into the cavernous sinus, compressing the oculuomotor nerve (III), the trochlear nerve (IV) and the abducens nerve (VI), often leading to double-vision and strabismus. These cranial nerves may also be impacted by herniation of the temporal lobes of the brain via the falx cerebri.
The cause of trigeminal neuralgia, where one side of the face experiences painful signs and symptoms, is believed to be due to the compression of a cranial nerve by an artery as the nerve exits from the brain stem. An acoustic neuroma, especially at the junction between the pons and medulla, may compress the facial nerve (VII) and the vestibulocochlear nerve (VIII), resulting in hearing and sensory loss on the affected side.
Stroke
Occlusion of blood vessels which supply the cranial nerves or their nuclei, or an ischemic stroke, might cause specific signs and symptoms which could localize where the occlusion happened. A clot in a blood vessel draining the cavernous sinus, also known as the cavernous sinus thrombosis, may affect the oculomotor (III), the trochlear (IV), and the opthalamic branch of the trigeminal nerve (V1) and the abducens nerve (VI).
Inflammation
Inflammation caused by an infection may impair the operation of any of the cranial nerves. Infection of the facial nerve (VII), for instance, can result in Bell’s palsy. Multiple sclerosis, an inflammatory process which can produce a loss of the myelin sheathes that encircle the cranial nerves, may cause a variety of shifting signs and symptoms which can ultimately affect multiple cranial nerves.
Other
Trauma to the skull, bone disease like Paget’s disease, and damage or injury to the cranial nerves through neurosurgery, by way of instance, through tumor removal, are other potential causes of cranial nerve health issues.
Dr. Alex Jimenez’s Insight
There are 12 pairs of cranial nerves which exit the brain, one in each side. These cranial nerves are named and numbered (I-XII) according to their location in the brain as well as their specific function in the body. Common conditions, such as multiple sclerosis, may affect one or more of the cranial nerves, resulting in dysfunction of the specific regions innervated by them. Signs and symptoms associated with health issues affecting specific cranial nerves can help healthcare professionals determine the source of the problem. Testing the cranial nerves involves a number of steps in order to be certain which function of the human body has been ultimately affected.
Clinical Significance of the Cranial Nerves
Most commonly, humans are believed to have twelve pairs of cranial nerves which have been assigned Roman numerals I-XII for identification. The numbering of the cranial nerves is based on the order in which they emerge from the brain, or from the front to the back of the brainstem. These include: the olfactory nerve (I), the optic nerve (II), the oculomotor nerve (III), the trochlear nerve (IV), the trigeminal nerve (V), the abducens nerve (VI), the facial nerve (VII), the vestibulocochlear nerve (VIII), the glossopharyngeal nerve (IX), the vagus nerve (X), the accessory nerve (XI), and the hypoglossal nerve (XII). Below we will narrow down the clinical significance of the cranial nerves.
Olfactory Nerve (I)
The olfactory nerve (I) communicates the sensation of smell to the brain. Lesions resulting in anosmia, or loss of the sense of smell, have been previously described to occur through trauma, damage or injury to the head, especially in the instance that a patient hits the back of their head. In addition, frontal lobe masses, tumors, and SOL have also been associated with the loss of the sense of smell. Healthcare professionals have previously identified that the loss of the sense of smell is one of the first symptoms seen in Alzheimer’s and early dementia patients.
Healthcare professionals may test the function of the olfactory nerve (I) by having the patient close their eyes and cover one nostril at a time in order to have them breathe out through their nose while placing a scent under the nostril and having them breathe in. The doctor will ask the patient, “do you smell anything?”, and record the findings. This tests whether the nerve is operating appropriately. If the patient says yes, the doctor will then ask the patient to identify the scent. This tests whether the processing pathway, known as the temporal lobe, is functioning accordingly.
Optic Nerve (II)
The optic nerve (I) communicates visual information to the retina. Lesions to this cranial nerve can be the result of CNS disease, such as MS, or CNS tumors and SOL. Most health issues associated with the visual system emerge from direct trauma, metabolic or vascular diseases. FOV lost in the periphery can also indicate that SOL may be affecting the optic chiasm, including a pituitary tumor.
A healthcare professional will often test the function of the optic nerve (II) by asking whether the patient can see. If the patient describes having vision in each eye, the optic nerve is functional. Doctors may also perform visual acuity testing using the Snellen chart, first one eye at a time, then the two eyes together, or they may perform distance vision testing. Near vision testing will often involve the Rosenbaum chart, first one eye at a time, then the two eyes together. Additional associated testing for the visual system can include, the ophthalmoscopic or funduscopic exam, which assess the A/V ratio and vein/artery health as well as assess cup to disc ratio of the visual system. Other testing methods include field of vision testing, intraoccular pressure testing and the iris shadow test.
Oculomotor Nerve (III), Trochlear Nerve (IV), and Abducens Nerve (VI)
The oculomotor nerve (III), the trochlear nerve (IV), the abducens nerve (VI) and the ophthalmic division of the trigeminal nerve (V1) travel through the cavernous sinus to the superior orbital fissure, passing out of the skull into the orbit. These cranial nerves control the tiny muscles that move the eye and also offer sensory innervation to the eye and orbit.
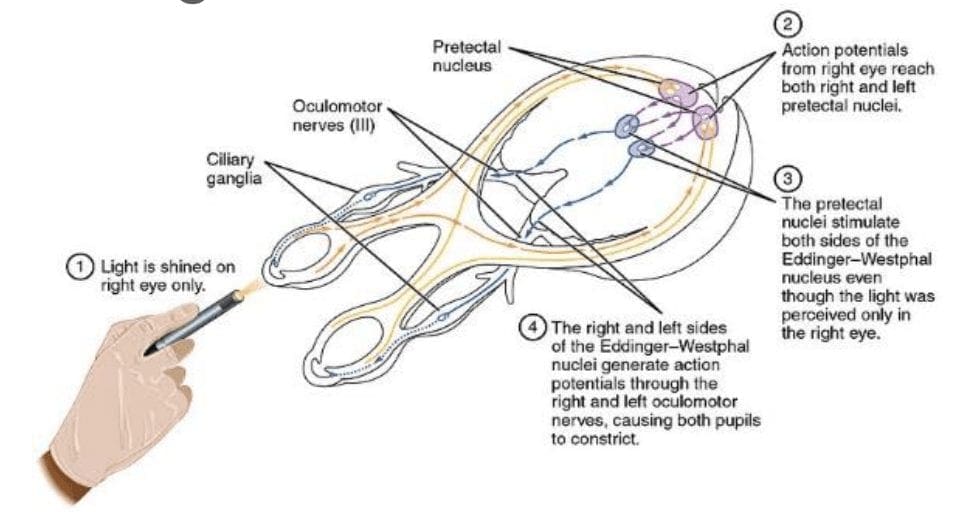
The clinical significance of the oculomotor nerve (III) includes diplopia, lateral strabismus (unopposed lateral rectus m.), head rotation away from the side of the lesion, a dilated pupil (unopposed dilator pupillae m.), and ptosis of the eyelid (loss of function of the levator palpebrae superioris m.). Lesions to the oculomotor nerve (III) can occur due to inflammatory diseases, such as syphilitic and tuberculous meningitis, aneurysms of the posterior cerebral or superior cebellar aa., and SOL in the cavernous sinus or displacing the cerebral peduncle to the opposite side. Testing this cranial nerve is performed by moving a light in front of the patient’s pupil from the lateral side and hold for 6 seconds. The doctor should watch for direct (ispilateral eye) and consensual (contralateral eye) pupillary constriction in order to distinguish dysfunction of the oculomotor nerve (III).
The clinical significance of the trochlear nerve (IV) is characterized where the patient presents diplopia and difficulty while maintaining a downward gaze, often complaining of having difficulties when walking down stairs, resulting in more frequent tripping and/or falling, followed by extortion of the affected eye (unopposed inferior oblique m.) and a head tilt to the unaffected side. Lesions to the trochlear nerve (IV) can commonly be the result of inflammatory diseases, aneurysms of the posterior cerebral or superior cerebellar aa., SOL in the cavernous sinus or superior orbital fissure and surgical damage during mesencephalon procedures. Head tilts in superior oblique palsy (CN IV failure) may also be identified.
The clinical significance of the abducens nerve (VI) includes diplopia, medial strabismus (unopposed medial rectus m.), and head rotation towards the side of the lesion. Lesions to this cranial nerve can be the result of aneurysms of the posterior inferior cerebellar or basilar aa., SOL in the cavernous sinus or 4th ventricle, such as a cerebellar tumor, fractures of the posterior cranial fossa, and increased intracranial pressure. Testing this cranial nerve is performed through the H-Pattern testing, where the healthcare professional will have the patient follow an object no bigger than 2 inches. It’s essential for the doctor to follow these specific guidelines as patient’s can have difficulties focusing on items that are too large, and it’s also important for the doctor not to hold the object too close to the patient. Convergence and accommodation testing is performed by bringing the object close to the bridge of the patient’s nose and back out at least 2 times. The physician must look for pupillary constriction response as well as convergence of the eyes.
Trigeminal Nerve (V)
The trigeminal nerve (V) is made up of three different parts: The . When put together, these nerves provide sensation to the skin of the face and also controls the muscles of mastication, or chewing. Cranial nerve dysfunction along any of the separate sections of the trigeminal nerve (V) can manifest as decreased bite strength on the ipsilateral side of the lesion, loss of sensation along the distribution of V1, V2, and V3, and loss of corneal reflex. Lesions to the trigeminal nerve (V) can be the result of aneurysms or SOL affecting the pons, particularly tumors at the cerebellopontine angle, skull fractures on the facial bones or damage to the foramen ovale, and Tic doloureux, most frequently referred to as trigeminal neuralgia, characterized by sharp pain along the distributions of the different parts of the trigeminal nerve (V). Physicians may utilize analgesic, anti-inflammatory or contralateral stimulation to control the signs and symptoms.
Testing the trigeminal nerve (V) includes pain & light touch testing along the ophthalmic (V1), the maxillary (V2), as well as the Mandibular (V3) nerves of the cranial nerve.�Testing is best done toward the more medial or proximal areas of
the face, where the V1, the V2 and the V3 are better delineated. A healthcare professional may also assess dysfunction along this cranial nerve using the blink/corneal reflex testing, performed by puffing air or doing a small tissue tap from the lateral side of the eye on the cornea. If normal, the patient blinks. The CN V provides the sensory (afferent) arc of this reflex. Bite strength may also be tested by having the patient bite down on a tongue depressor while the doctor tries to remove it. The jaw jerk/Masseter reflex may also be performed with the patient�s mouth slightly open, by placing the thumb on a patient�s chin and tapping the own thumb with a reflex hammer. Strong closure of the mouth indicates UMN lesion. CN V provides both the motor and sensory of this reflex.
Facial Nerve (VII) and Vestibulocochlear Nerve (VIII)
The facial nerve (VII) and the vestibulocochlear nerve (VIII) both input the inner auditory canal in the temporal bone. The facial nerve subsequently extends to the side of the face then distributes to control and reach all of the muscles in charge of facial expressions. The vestibulocochlear nerve reaches the organs which control equilibrium and hearing in the temporal bone.
As with all cranial nerves, signs and symptoms along the facial nerve (VII) describe the location of the lesion. Lesion in the lingual nerve will manifest as loss of taste, general sensation in the tongue and salivary secretion. Lesion proximal to the branching of the chorda tympani, such as in the facial canal, will result in the same signs and symptoms, without the loss of general sensation of the tongue, partly due because the V3 has not yet joined the facial nerve (VII). Corticobulbar innervation is asymmetric to the upper and lower parts of the facial motor nucleus. In the instance of an UMN lesion, or a lesion to the corticobulbar fibers, the patient will experience paralysis of the muscles in charge of facial expression in the contralateral lower quadrant. If there is an LMN lesion, or a lesion to the facial nerve itself, the patient will experience paralysis of the muscles of facial expression in the ipsilateral half of the face, otherwise known as Bell’s palsy.
A healthcare professional will test the facial nerve (VII) initially by asking the patient to mimic or follow specific instructions to make certain facial expressions. The doctor should make sure to evaluate all four quadrants of the face by asking the patient to raise their eyebrows, puff their cheeks, smile and then close their eyes tightly. Subsequently, the doctor will test the facial nerve (VII) by checking the strength of the buccinator muscle against resistance. The healthcare professional will achieve this by asking the patient to hold air in their cheeks as they press gently from the outside. The patient should be able to hold air in against the resistance.
Signs and symptoms of dysfunction in the vestibulocochlear nerve (VIII) often involve changes in hearing alone, most commonly as a result of infections in the otitis media and/or as a result of skull fractures. The most common lesion to this nerve is caused by an acoustic neuroma which affects the CN VII and the CN VIII, particularly the cochlear and vestibular divisions, as a result of proximity in the internal auditory meatus. Signs and symptoms of the health issue include nausea, vomiting, dizziness, hearing loss, tinnitus, and Bell’s palsy, etc.
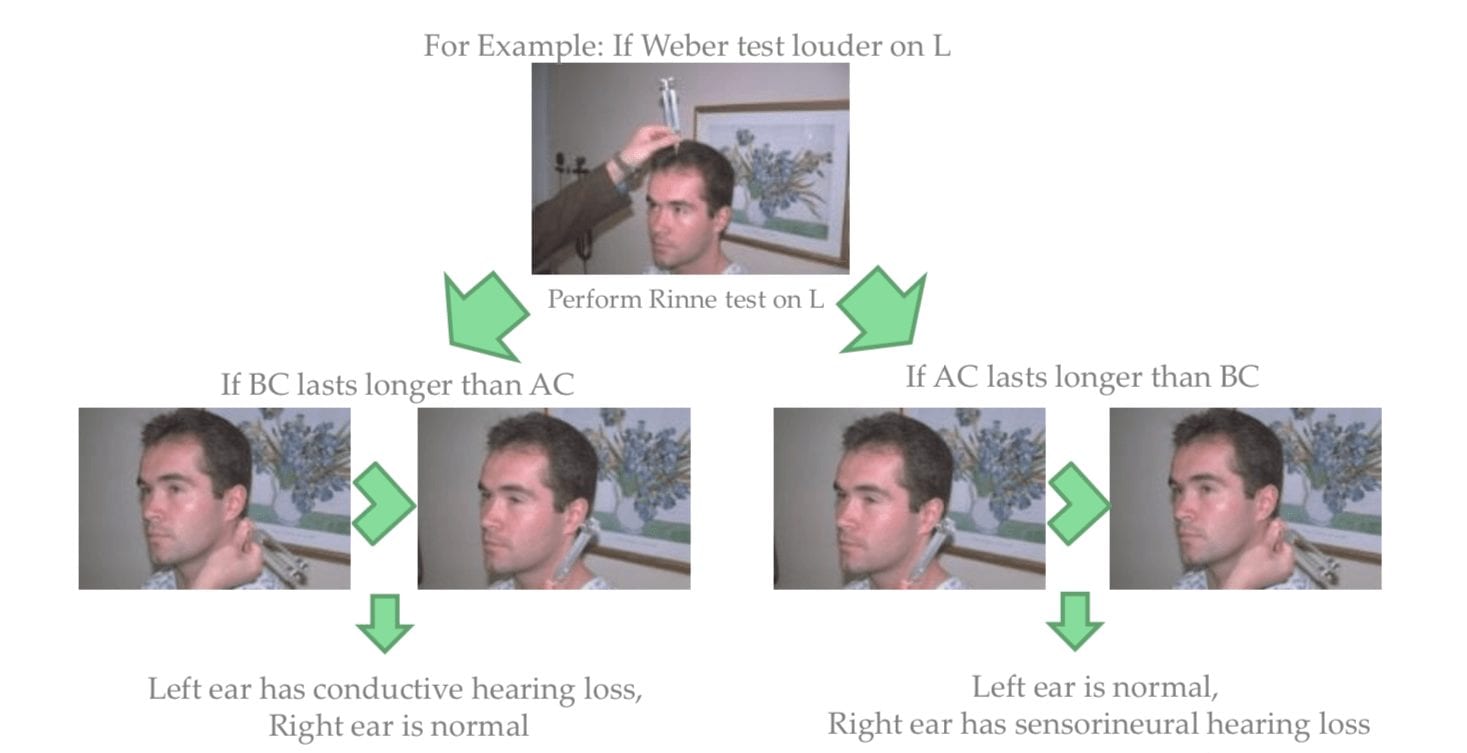
Testing the vestibulocochlear nerve (VIII) for dysfunction commonly involves an otoscopic exam, the scratch test, which determines whether a patient can hear equally on both sides, the Weber test, tests for lateralization, a 256 Hz tuning fork placed on top of the patient�s head in the center, which can help point out whether a patient hears it louder on one side than the other, and finally the Rinne test, which compares air conduction to bone conduction. Normally, air conduction should last twice as long as bone conduction.
Glossopharyngeal Nerve (IX), Vagus Nerve (X) and Accessory Nerve (XI)
The glossopharyngeal (IX), the vagus nerve (X) and the accessory nerve (XI) all emerge from the skull to enter the neck. The glossopharyngeal nerve (IX) provides innervation to the upper throat and the back of the tongue, the vagus nerve (X) offers innervation to the muscles at the voicebox, and proceeds down to provide parasympathetic innervation to the chest and abdomen. The accessory nerve (XI) controls the trapezius and sternocleidomastoid muscles at the neck and shoulder.
The glossopharyngeal nerve (IX) is rarely damaged alone, due to it�s proximity to the CN X and XI. A healthcare professional should perform a test to look for signs of CN X & XI damage as well if CN IX involvement is suspected.
Patients with clinical signs and symptoms caused by vagus nerve (X) dysfunction may experience dysarthria, or difficulty speaking clearly, as well as dysphagia, or difficulty swallowing. These may present as food or liquid coming out of their nose or frequent chocking or coughing when eating and/or drinking. Further clinical presentations include hyperactivity of a visceral motor component, leading to the hypersecretion of gastric acid and resulting in ulcers. Hyper-stimulation of the general sensory component can cause coughing, fainting, vomiting and reflex visceral motor activity. The visceral sensory component of this nerve only provides general feelings of un-wellness but visceral pain may transfer on to the sympathetic nerves.
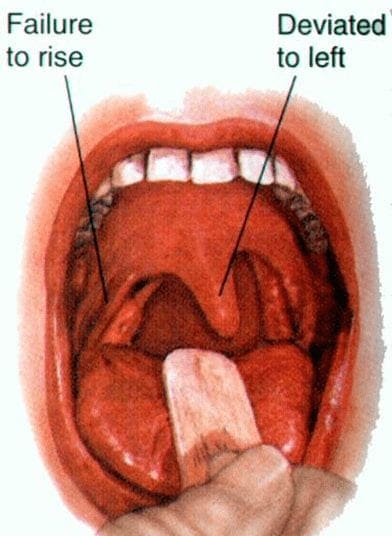
Testing for the glossopharyngeal nerve (IX) and the vagus nerve (X) can include the gag reflex, where the�CN IX provides the afferent (sensory) arc and the�CN X provides the efferent (motor) arc. Approximately 20 percent�of patients have a minimal or absent gag reflex. Other tests may include wwallowing, gargling, etc., as it requires CN X function. Healthcare professionals may also test palatal elevation because it requires CN X function. Furthermore, the doctor will see whether the palate elevates and uvula deviates
contralateral to damaged side. Finally, the healthcare professional will test the auscultation of the heart, since the R CN X innervates SA node (more rate regulation) and the L CN X the AV node (more rhythm regulation).
Lesions in the accessory nerve (XI)�may occur due to radical surgeries in the neck area, such as the removal of the laryngeal carcinomas. Testing for the accessory nerve (XI) may include the strength test SCM m. Patients with clinical signs and symptoms due to lesions in the accessory nerve (XI) will experience difficulties turning their head against the resistance of a healthcare professional, particularly toward the side opposite of the lesion. Testing for the accessory nerve (XI) may also include the strength test trapezius m. Patients with clinical signs and symptoms due to lesions in the accessory nerve (XI) will experience difficulties with shoulder elevation on the side of the lesion.
Hypoglossal Nerve (XII)
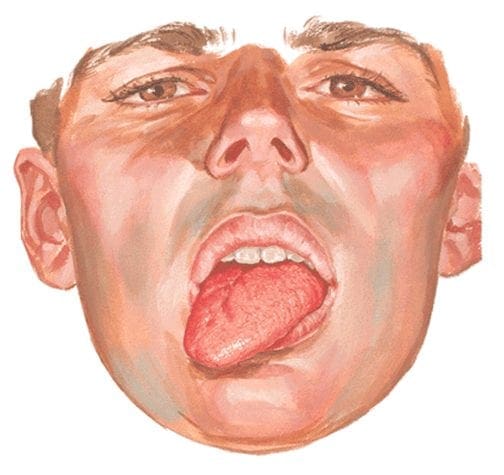
The hypoglossal nerve (XII) originates from the skull to reach the tongue in order to control essentially all of the muscles involved in the movements of the tongue. The clinical significance of health issues associated to the hypoglossal nerve (XII) can manifest as a deviating tongue towards the side of an inactive genioglossus m. upon tongue protrusion. This may often be contralateral to a corticobulbar, or UMN, lesion or from an ipsilateral to a hypoglossal n., or LMN, lesion.
Testing for the hypoglossal nerve (XII) involves the healthcare professional asking a patient to stick out their tongue. The doctor will look for any deviation which may signal a health issue along the length of the hypoglossal nerve (XII). Another test the doctor may perform as a part of the evaluation may include the physician asking the patient to place their tongue inside their cheek and apply light resistance, one side at a time. The patient should be able to resist moving their tongue with pressure.
The clinical significance of the signs and symptoms which manifest as a result of cranial nerve dysfunction are essential in order for the healthcare professional to properly diagnose the patient’s specific health issue. The clinical findings described above are often unique to the affected cranial nerve and the tests and evaluations for each can help confirm a diagnosis. Proper diagnosis is fundamental in order for the doctor to continue with the patient’s appropriate treatment. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
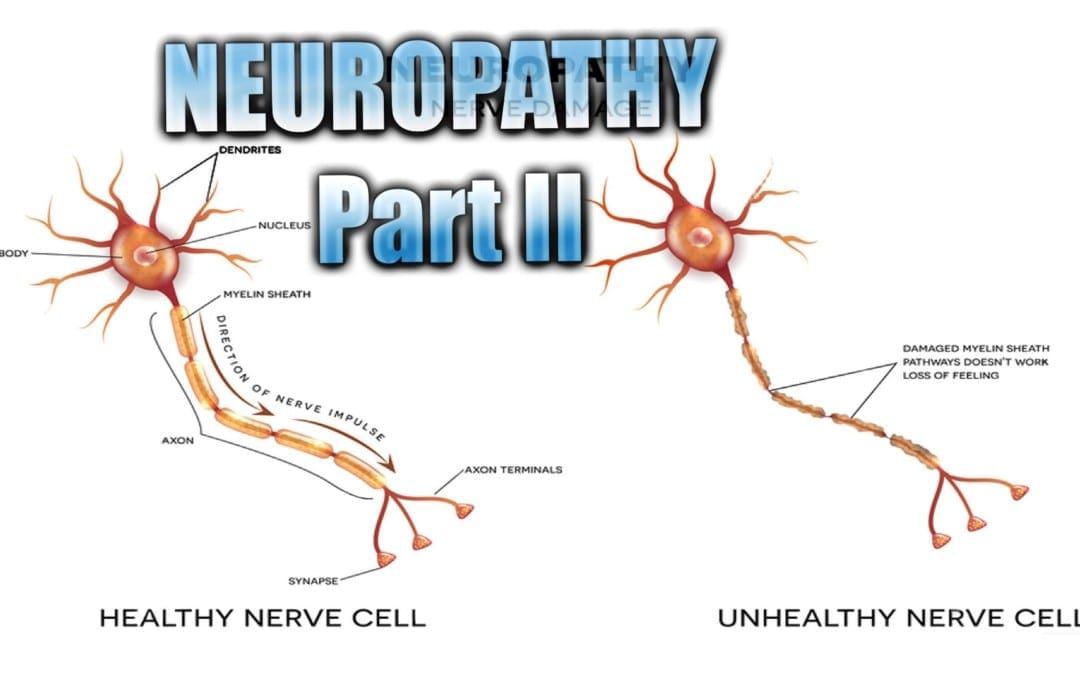
Neuropathy Presentation II:�El Paso, TX. Chiropractor, Dr. Alexander Jimenez�continues the overview with neuropathy part II. Continued are the most common neuropathies to be seen in practice. Because the human body is composed of many different kinds of nerves which perform different functions, nerve damage is classified into several types. Neuropathy can also be classified according to the location of the nerves being affected and according to the disease causing it. For instance, neuropathy caused by diabetes is called diabetic neuropathy. Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest. The complications which follow neuropathy depends on the type of nerves that are damaged. According to Dr. Jimenez, different neuropathies can cause numbness and/or tingling sensations, increased pain or the loss of ability to feel pain, muscle weakness along with twitching and cramps, even dizziness and/or loss of bladder control function.
Sciatic Nerve Entrapment
Piriformis Syndrome
Peroneal Nerve Entrapment
Tarsal Tunnel Syndrome
Sciatic N. Piriformis Syndrome
Causes
Anatomic variation
Piriformis overuse/tension
Exam
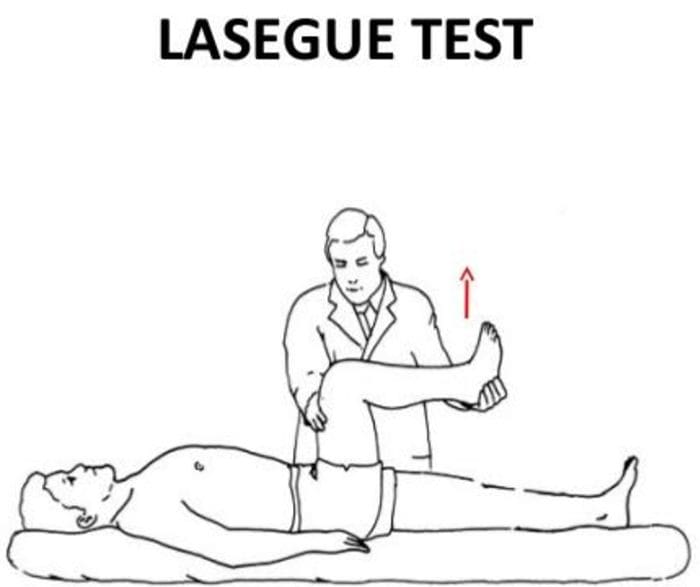
Positive Lase?gue test possible
Doctor extends patient�s leg passively, while patient is lying supine positive test if maneuver is limited by pain
Tenderness and palpable tension in piriformis muscle which elicits symptoms
Sciatic N. Peroneal Nerve Entrapment
Peroneal or Fibular branch of Sciatic nerve entrapped at the fibular head
Tinel�s sign may be present at fibular head/neck
Usually affects common peroneal nerve, therefore motor and sensory symptoms can be seen
Weakness of ankle dorsiflexion and eversion (tibialis anterior m.)
Sensory disruption on the dorsum of the foot and lateral aspect of the calf
Sciatic N. Tarsal Tunnel Syndrome
Tibial nerve impinged in the tarsal tunnel
Sensory changes in the sole of the foot
Tinel�s sign may be present with percussion posterior to the medial malleolus
Radiculopathy
A mononeuropathy � located in one specific area
Neuropathy involving spinal nerve roots
Presents as changes in sensory and/or motor function affecting a single or a few nerve root level(s)
Nerve sheath tumors (schwannomas and neurofibromas)
Guillain-Barre? syndrome
Herpes Zoster (shingles)
Lyme disease
Cytomegalovirus
Myxedema/Thyroid disorder
Idiopathic neuritis
Narrowing Down Common Causes Of Radiculopathy
Disc Herniation
Most commonly affected nerve roots are C6, C7, L5 & S1
Spinal Stenosis
Lumbar stenosis may produce neurogenic claudication
Pain & weakness with ambulation
Cervical stenosis may present with mixed picture of radiculopathy and myelopathy due to long tract involvement
Trauma
May cause compression, trauma or avulsion of the nerve roots
Diabetes
More likely to cause a polyneuropathy, but mononeuropathy is possible
Herpes Zoster (Shingles)
Most often on the trunk, accompanied by vesicular lesions in a single dermatome
If pain persits past vesicular regression = post-herpetic neuralgia
Patient History Of Radiculopathy
The patient will often complain of burning pain or tingling that radiates or shoots down an affected area in a dermatomal pattern.
Sometimes patient will complain of motor weakness, however if onset is recent, there is often no motor involvement
Exam Of Radiculopathy
Most often hypoesthesia in the affected dermatome level
Best to evaluate for pain, as light touch can be difficult for these patient�s to distinguish
Fasciculations and/or atrophy may be seen if radiculopathy is chronic, due to lower motor neuron being impinged
Motor weakness may be seen in muscles innervated by the same root level
Orthopedic tests:
Straight-leg raise test (SLR)
Pain between 10-60 degrees likely indicates nerve root compression
Well-leg raise/Crossed straight-leg raise test (WLR)
If positive, 90% specificity for L/S nerve root compression
Valsalva Maneuver
Positive if increase in radicular symptoms
Spinal Percussion
Pain may indicate metastatic disease, abscess or osteomyelitis
Examinations: Merck Manual Professional
How To Test Reflexes
How To Do A Sensory Exam
How To Do A Motor Examination
Dermatomes
Testing Cervical Nerve Roots
Testing Lumbosacral Nerve Roots
Specific Radiculopathy Patterns
T1 radiculopathy can cause Horner�s syndrome
This is due to affect on cervical sympathetic ganglia
Ptosis, miosis, anhidrosis
Below L1, radiculopathies can cause Cauda Equina syndrome
Saddle anesthesia (sensory loss in S2-S5 distribution)
Urinary retention or overflow incontinence
Constipation, decreased rectal tone or fecal incontinence
Loss of erectile function
Must be referred for emergency care immediately to prevent permanent dysfunction
Other Patterns Of Neuropathy
Cape/Shawl distribution of symptoms
Intramedullary lesion
Syringomyelia
Intramedullary tumor
Central cord damage
Stocking and Glove Distribution of Symptoms
Diabetes mellitus
B12 deficiency
Alcoholism/hepatitis
HIV
Thyroid dysfunction/myxedema
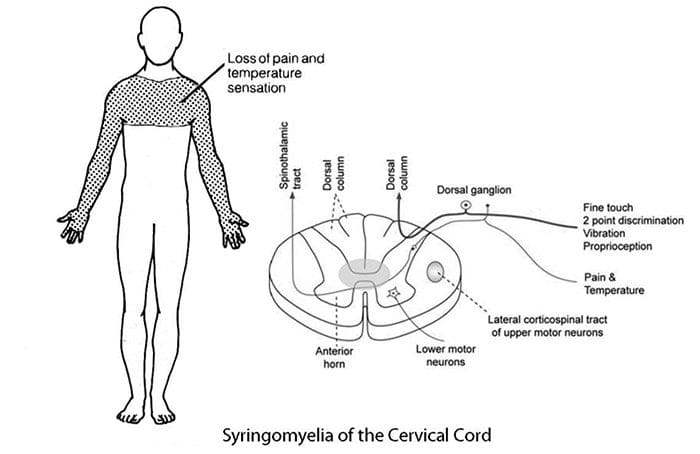
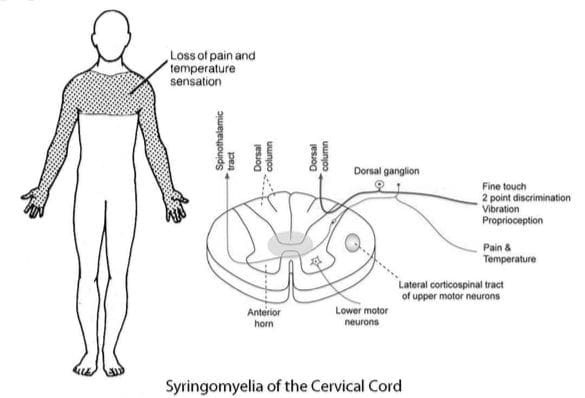
Cape/Shawl Pattern
Intramedullary lesion such as tumor, syringomyelia or hyperextension injury in patient with C/S spondylosis
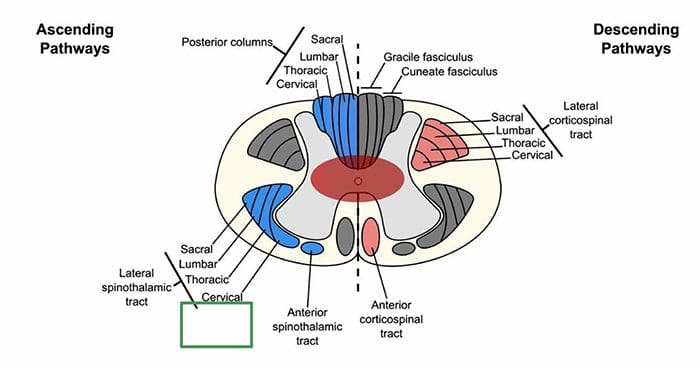
Loss of pain and temp sensation in C/T dermatomes because of arrangement of lateral spinothalamic tract
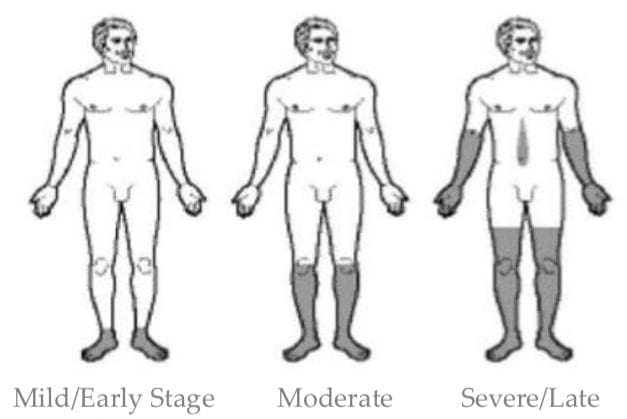
Stocking & Glove Pattern
Symmetrical polyneuropathy
Feet/legs usually affected first, followed by hands/arms
Vibration sensation in the smallest toes is usually the first thing lost and neuropathy progresses across foot to great toe and then upward through the ankle and leg, then hands, arms and finally trunk if sever
Most likely cause of this distribution is diabetes mellitus, but other possible causes include B12 deficiency, alcoholism, HIV, chemotherapy treatment, thyroid dysfunction and multiple other causes
Diabetic Neuropathy
Diabetic neuropathy often presents as a polyneuropathy but can also present as a mononeuropathy, usually with acute onset
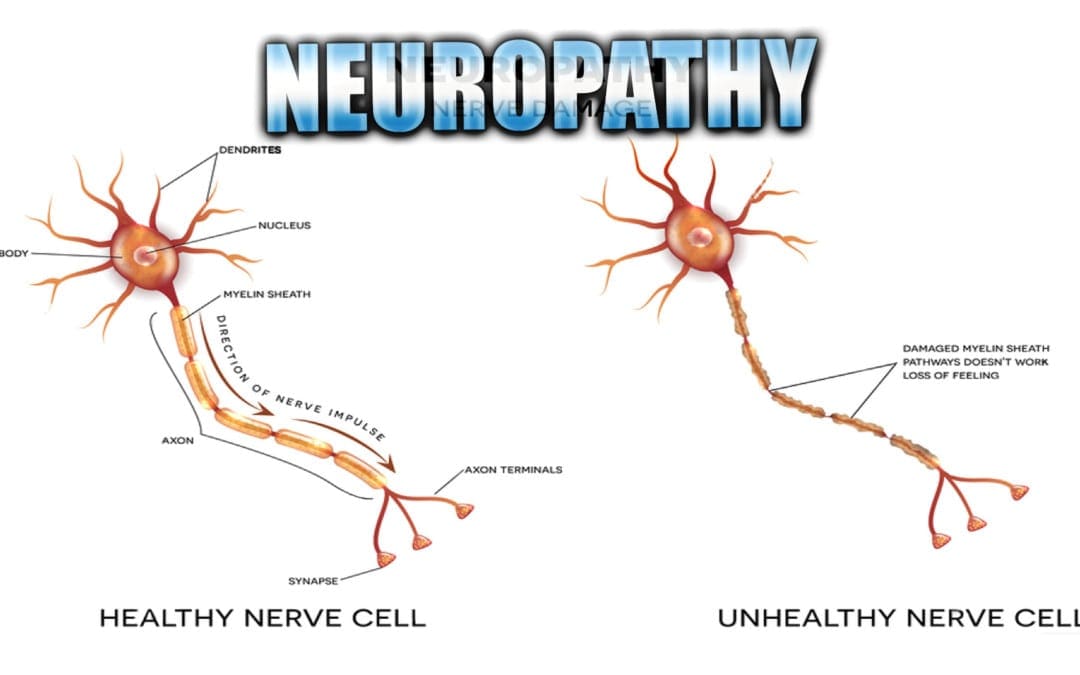
Neuropathy Presentation: El Paso, TX. Chiropractor, Dr. Alexander Jimenez�presents an overview of neuropathy. These are the most common neuropathies to be seen in practice.�Neuropathy is a medical term used to characterize damage or injury to the nerves, which refers to the peripheral nerves as opposed to the central nervous system. The complications which follow neuropathy depends largely on the type of nerves that are affected. According to Dr. Alex Jimenez, different neuropathies can cause numbness and tingling sensations, increased pain or the loss of ability to feel pain, muscle weakness along with twitching and cramps, even dizziness and/or loss of control over bladder function.
Neuropathy
Three primary classifications based on location of symptoms:
If sensory disruption is limited to certain modalities, it implies CNS is involved
If all sensation is affected in the area, implies PNS is involved
Determine Pattern Of Symptoms
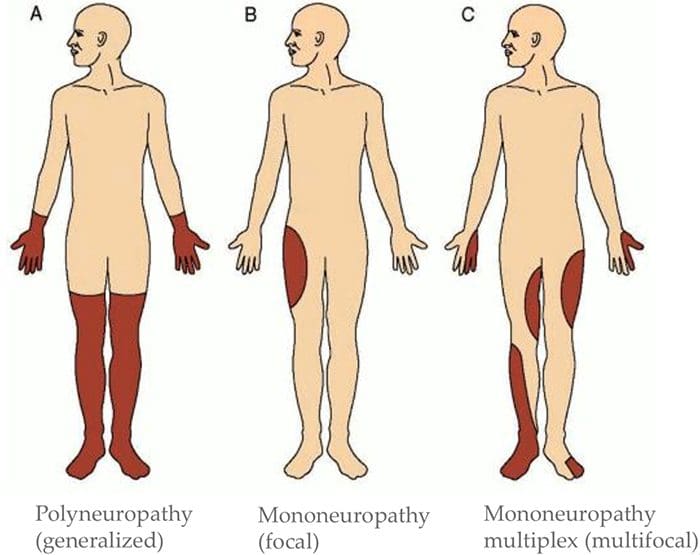
Mononeuropathy (focal)?
Mononeuropathy multiplex (multifocal)?
Polyneuropathy (generalized)?
Motor Exam
Determine if there is change to muscle strength
Determine if there is a change in muscle tone
Determine which muscles are affected
Determine if there has been a change in reflexes
This information can help determine the level(s) of involvement
Check For Autonomic�Signs
Auscultate heart
Palpate palms
Auscultate abdomen
Assess autonomic history
For example, is patient complaining about sweating more on one side than another? Complaining of stress levels?
Suggest ANS involvement
Exams: Merck Manual Professional Version
How To Test Reflexes
How To Do The Sensory Exam
How To Do The Motor Examination
Classification Of Nerve Injuries Resulting In Neuropathy
Neurapraxia – This is a transient episode of motor paralysis with little or no sensory or autonomic dysfunction; no disruption of the nerve or its sheath occurs; with removal of the compressing force, recovery should be complete
Axonotmesis – This is a more severe nerve injury, in which the axon is disrupted but the Schwann sheath is maintained; motor, sensory, and autonomic paralysis results; recovery can occur if the compressing force is removed in a timely fashion and if the axon regenerates
Neurotmesis – This is the most serious injury, in which both the nerve and its sheath are disrupted; although recovery may occur, it is always incomplete, secondary to loss of nerve continuity
Brachial Plexopathies
Erb�s Palsy
Klumke�s Palsy
Erb�s Palsy
AKA Erb�Duchenne palsy or Waiter’s tip palsy
Most common mechanism of injury in adults is a patient who fall forward while holding onto something behind them
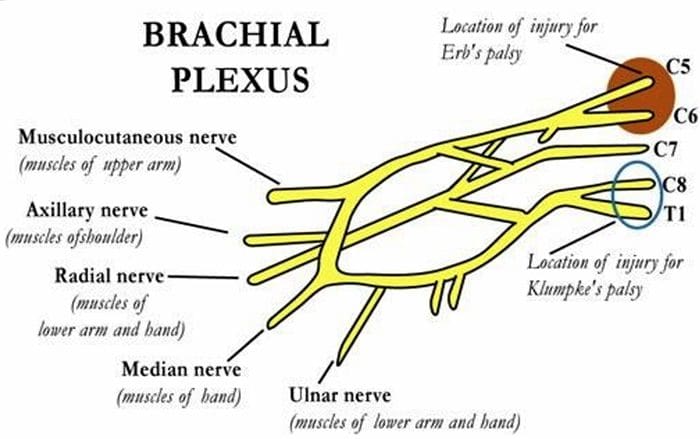
Can also happen to an infant during childbirth ? Results from damage to C5-6 nerve roots in the brachial plexus
Dermatomal distribution of sensory disruption
Weakness or paralysis in deltoid, biceps, and brachialis muscles resulting in �waiter�s tip� position
Klumke�s Palsy
AKA Dejerine�Klumpke palsy
Happens to infants during childbirth if arm is pulled overhead
Can also happen to adults with overhead traction injuries
Results from damage to C8-T1 nerve roots in the brachial plexus
Dermatomal distribution of sensory disruption
Weakness or paralysis in wrist flexors and pronators as well as muscles of the hand
May produce Horner�s syndrome due to T1 involvement
Results in a �claw hand� appearance
Forearm supinated with wrist hyperextended, with finger flexion
Neuropathy is a medical term used to describe a collection of general diseases or malfunctions which affect the nerves. The causes of neuropathy, or nerve damage, can vary greatly among each individual and these may be caused by a number of different diseases, injuries, infections and even vitamin deficiency states. However, neuropathy can most commonly affect the nerves that control the motor and sensory nerves. Because the human body is composed of many different kinds of nerves which perform different functions, nerve damage is classified into several types. Neuropathy can also be classified according to the location of the nerves being affected and according to the disease causing it. For instance, neuropathy caused by diabetes is called diabetic neuropathy. Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest as a result. Below we will discuss several specific types of neuropathies clinically treated by chiropractors, physical therapists and physical medicine doctors alike, as well as briefly describing their causes and their symptoms.
Brachial Plexopathies
Brachial plexopathy is a type of peripheral neuropathy, which affects the nerves that transmit messages from the brain and the spinal cord to the rest of the body. This kind of nerve damage occurs when harm affects the brachial plexus, a region found on each side of the neck where nerve roots from the spinal cord branch out into each arm’s nerves. Damage, injury or a condition that impacts these nerve roots can result in pain, decreased mobility and reduced sensation in the arm and shoulder. In some cases, no cause can be identified.
Erb’s Palsy
Erb’s Palsy, also known as�Erb�Duchenne palsy or Waiter’s tip palsy, is identified as a paralysis of the arm caused by damage or injury to the nerves in the neck which form part of the brachial plexus. The most common mechanism of injury in adults with Erb’s Palsy is a patient who fell forward while holding onto something behind them. Erb�Duchenne palsy can also happen to an infant during childbirth, most commonly, but not exclusively, from shoulder dystocia during a difficult birth. To be more precise, this type of brachial plexopathy results from damage to the C5-C6 nerve roots along the brachial plexus in the neck. Symptoms of Erb’s Palsy include dermatomal distribution of sensory disruption followed by weakness or paralysis in the deltoid, biceps, and brachialis muscles, leading to the �waiter�s tip� position associated with this type of neuropathy. While many infants can recover on their own from this type of brachial plexopathy, some may require rehabilitation.
Klumpke’s Palsy
Klumpke’s Palsy, also known as Klumpke’s paralysis or�Dejerine�Klumpke palsy, is a partial palsy in the nerve roots of the brachial plexus located along the cervical spine, or neck. It is named after�Augusta D�jerine-Klumpke, an American-born French medical doctor acknowledged for her work in neuroanatomy. Klumpke’s Palsy is characterized as a form of paralysis involving the muscles of the forearm and hand, which occurs to�infants during childbirth if their arm is pulled overhead.�Dejerine�Klumpke palsy can also occur to adults with overhead traction injuries caused by harm to the C8-T1 nerve roots in the brachial plexus and upper thoracic region of the spine. Symptoms of Klumpke’s paralysis include dermatomal distribution of sensory disruption, weakness or paralysis, in the wrist flexors and pronators as well as in the muscles of the hand. This type of brachial plexopathy may often lead to Horner�s syndrome, a collection of symptoms which manifest when a set of nerves, known as the sympathetic trunk, are damaged or injured due to T1 involvement. This form of neuropathy is identified by resulting�in a �claw hand� appearance, where the forearm is supinated with the wrist hyperextended, together with finger flexion.
Entrapment Neuropathies
Entrapment neuropathy, also known as nerve compression syndrome or compression neuropathy, is best-known as nerve damage or a type of neuropathy caused by direct pressure on a nerve. Common symptoms include pain and discomfort, tingling or burning sensations, numbness and muscle weakness which affects only a particular part of the human body, depending on which nerve is affected. A nerve can become compressed as a result of a constant external force or due to a lesion, such as a tumor. Additionally, some conditions can make the nerves more susceptible to compression, including diabetes, where the nerves are rendered more sensitive to minor degrees of compression due to their already compromised supply of blood. Nerve damage caused by a single episode of harm can be considered an entrapment neuropathy, however, it is generally not classified under this group of compression neuropathy or nerve compression syndrome.
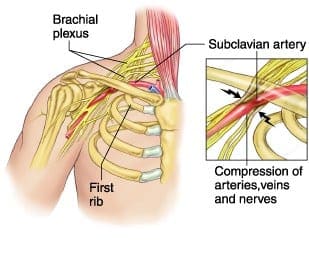
Thoracic Outlet Syndromes
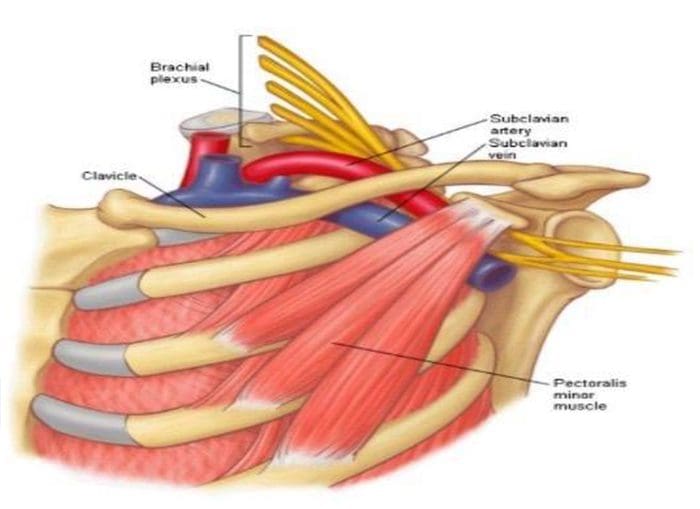
Thoracic outlet syndromes are a group of disorders which develop when the nerves or blood vessels between the collarbone and the thoracic outlet, located in the region of the first rib, are compressed. As a result, this can cause pain and discomfort in the neck and shoulders as well as numbness in the fingers. There are a number of types of thoracic outlet syndromes, including neurogenic, or neurological, thoracic outlet syndrome, specifically caused by the compression of the brachial plexus, vascular thoracic outlet syndrome, which is caused specifically by the compression of the veins, known as venous thoracic outlet syndrome, or arteries, known as arterial thoracic outlet syndrome, and nonspecific-type thoracic outlet syndrome, which is considered to be idiopathic and has been described to worsen with activity. Several healthcare professionals believe that nonspecific-type thoracic outlet syndrome doesn’t exist, while others claim it to be a common disorders. However, the majority of thoracic outlet syndromes are often classified as neurogenic.
Thoracic outlet syndromes are caused by the compression of the cervical rib, an extra “rib” in the seventh cervical vertebra, subclavius muscle tension, improper posture or�excessive thoracic kyphosis, physical trauma, repetitive activity, obesity and pregnancy. Thoracic outlet syndromes can vary depending on which structures are compressed. Thoracic outlet syndromes can be diagnosed using tests, such as the Adsons test, the Allen maneuver, the Costoclavicular maneuver, the Halstead maneuver, the�Reverse bakody maneuver, the Roos test, the Shoulder compression test and the Wright test. Thoracic outlet syndromes can cause permanent neurological damage if not diagnosed and treated early.
Median Nerve Entrapment
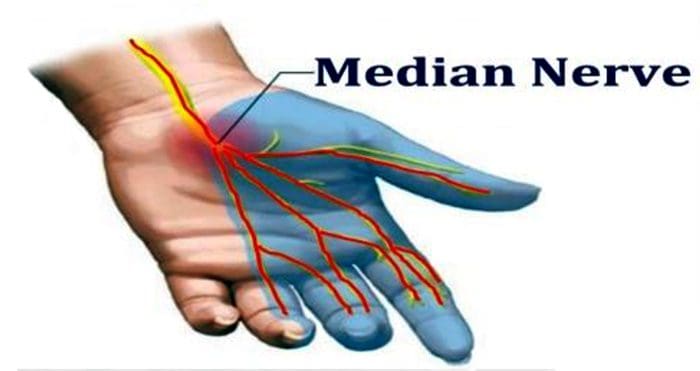
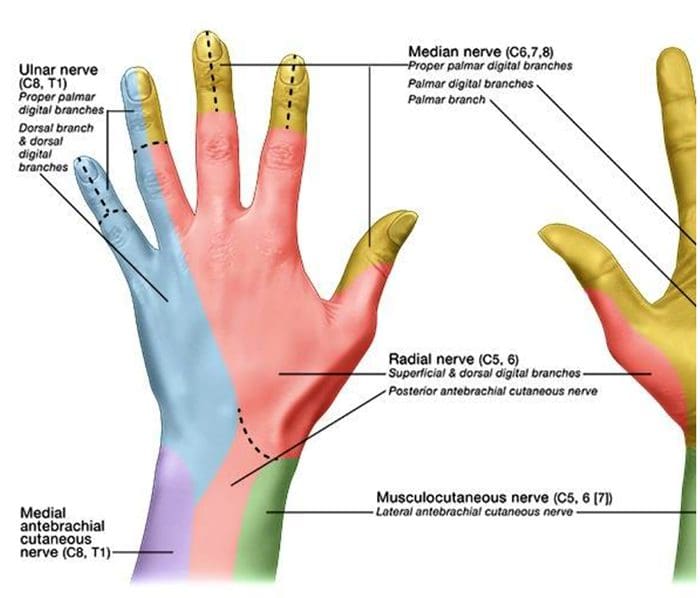
Median nerve entrapment or median nerve entrapment syndrome, is a mononeuropathy, a condition that impacts only a single nerve or nerve group outside the brain and spinal cord, which affects the movement of or sensation in the hand. Median nerve entrapment is caused by the compression of the median nerve found in the elbow or distally in the forearm or wrist. Symptoms include sensory disruption in the lateral portion of the palmar aspect of the hand and dorsal finger tips of the same fingers. In addition, motor fibers may also be affected in the forearm, if applicable, including the muscles of the thenar eminence, such as the abductor pollicis brevis, the opponens pollicis, and the flexor pollicis brevis. Other forms of median nerve entrapment syndromes include: pronator teres syndrome and carpal tunnel syndrome.
Pronator teres syndrome is characterized as the compression of the median nerve at the elbow. It is considered rare compared to carpal tunnel syndrome. Pronator teres syndrome is caused by repetitive movement, pronator teres muscle inflammation and thickened bicipital aponeurosis. Clinical findings for this type of neuropathy include, tenderness with palpation of the pronator teres muscle, pain with resisted pronation of the arm, flexor pollicus longus and flexor digitorum profundus involvement, otherwise, symptoms manifestations for pronator teres syndrome may appear similar to carpal tunnel syndrome but without positive wrist orthopedics.
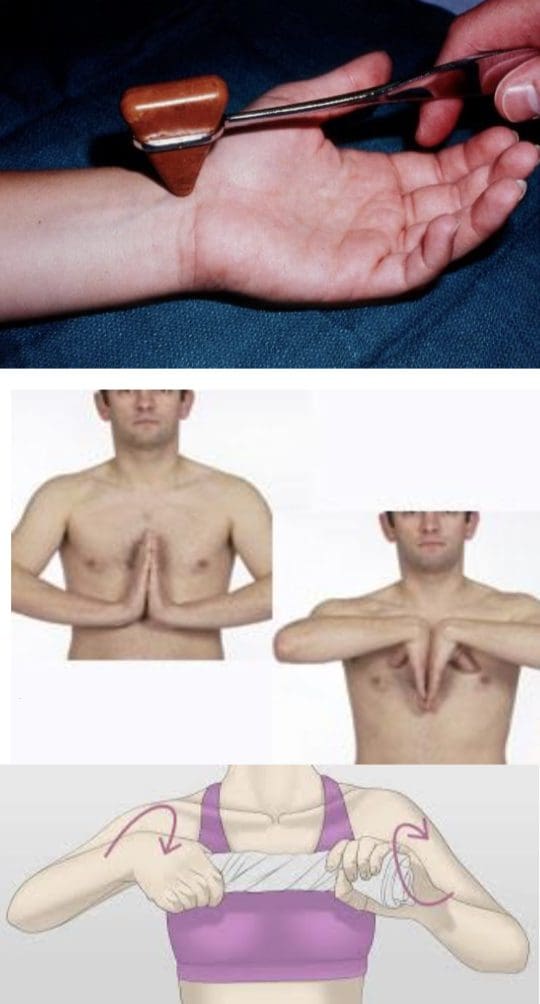
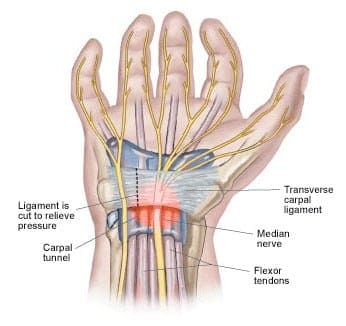
Carpal tunnel syndrome is characterized as the compression of the median nerve at the wrist. Carpal tunnel syndrome is identified by symptoms of pain and discomfort, tingling sensations in the thumb, index finger, middle finger and the thumb side of the ring fingers, and numbness. These can generally start gradually and may extend up the arm. Advanced instances of carpal tunnel syndrome may cause weakened grip strength where the muscles at the base of the thumb may waste away if left untreated for an extended period of time. In many cases, carpal tunnel syndrome may affect both hands or arms. Carpal tunnel syndrome is caused by repetitive movements, hypothyroidism, obesity, rheumatoid arthritis, diabetes and pregnancy. Orthopedic tests utilized to diagnose carpal tunnel syndrome include the use of the Tinel�s Sign, positive if tapping over the median nerve reproduces/exacerbates symptoms, the�Phalen�s Maneuver/Prayer Sign, performed by bringing the hands together, with wrists flexed, and is repeated in reverse with the wrists extended, for at least 60 seconds, and is considered positive if tests reproduce/exacerbate symptoms, and the�Wringing Test, if wringing a towel produces paresthesia.
Ulnar Nerve Entrapment
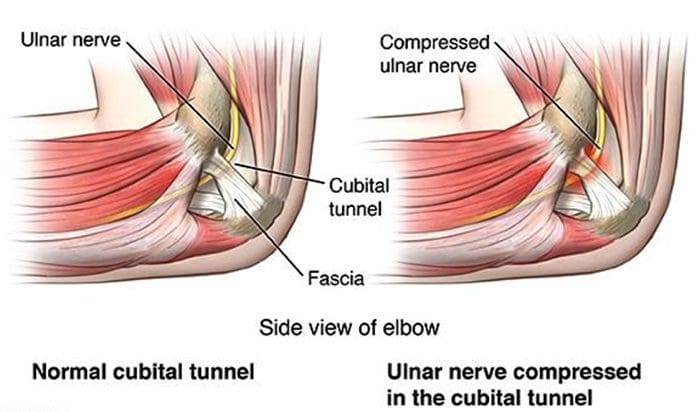
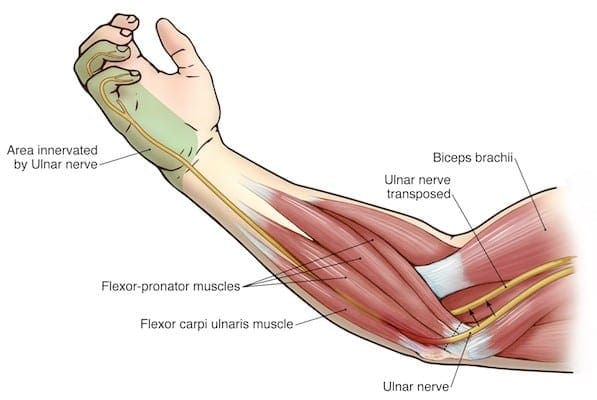
Ulnar nerve entrapment is a condition where the ulnar nerve itself becomes physically trapped or pinched, resulting in symptoms of pain, numbness and weakness which extends throughout the little finger, the ulnar half of the ring finger and throughout the intrinsic muscles of the hand. Symptoms or ulnar nerve entrapment ultimately involve sensory disruption in the medial two digits of the palmar and dorsal aspects of the hand. Symptoms of ulnar nerve entrapment may vary depending on the specific location of the ulnar nerve compression or impingement. These may also be classified as motor, sensory or both, depending on the location of the injury. If motor fibers are affected in the hand, all fingers, besides the thumb, may become weakened, described as general hand weakness. The most common location of ulnar nerve entrapment is within the cubital tunnel. Other forms of ulnar nerve entrapment include: cubital tunnel syndrome and tunnel of Guyon syndrome.
Cubital tunnel syndrome is identified by the compression or impingement of the ulnar nerve in the cubital tunnel at the elbow. It is considered to be the second most common entrapment neuropathy which affects the upper extremities, following carpal tunnel syndrome. Symptoms of cubital tunnel syndrome are characterized by pain and discomfort along the region of the ulnar nerve entrapment, along with sensory impairment, paresis and paresthesia.�Causes of cubital tunnel syndrome include, repetitive movements, hypothyroidism, obesity, diabetes, physical trauma or injury to the cubital tunnel, and prolonged sitting with pressure on bent elbow.
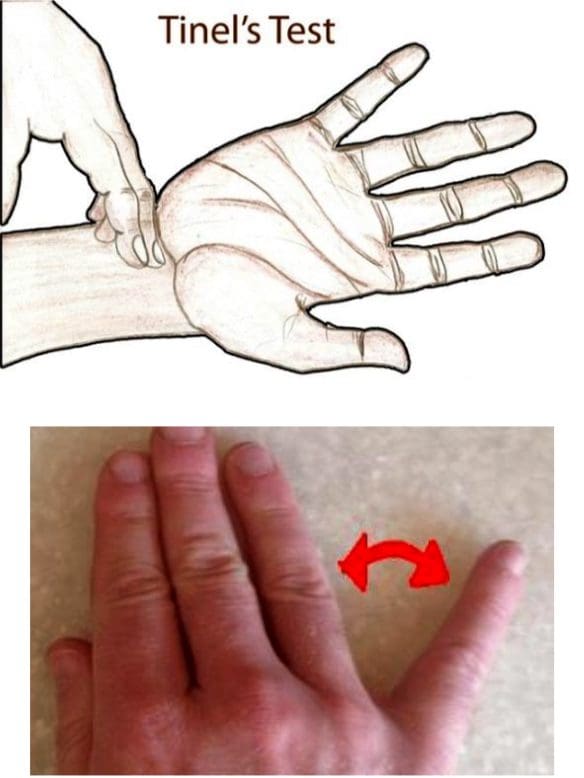
Tunnel of Guyon syndrome, or Guyon’s canal syndrome, is identified by the compression or impingement of the ulnar nerve at the wrist, particularly along an anatomical space in the wrist known as Guyon’s canal. Guyon’s canal syndrome may also be referred to as ulnar tunnel syndrome. Symptoms of tunnel of Guyon syndrome are similar to those of cubital tunnel syndrome with slight variations depending on the region of ulnar nerve entrapment.�Causes of tunnel of Guyon syndrome include, repetitive movements, long term crutch use, fracture of the hamate, a carpal bone, due to a ganglion cyst, hypothyroidism, obesity, rheumatoid arthritis and diabetes.�Orthopedic tests utilized to diagnose Guyon’s canal syndrome include the use of the�Tinel�s Sign, positive if test over the ulnar nerve at the wrist elicits symptoms, the Wartenberg Sign, positive if the 5th digit abducts when patient performs hard grip strength test or attempts to squeeze fingers together and reduced two-point discrimination in the hand.
Radial Nerve Entrapment
Radial nerve entrapment, also known as radial tunnel syndrome, is a condition caused by the compression of the radial nerve, which travels from the brachial plexus, to the hand and wrist. Healthcare professionals believe that radial tunnel syndrome occurs because the radial nerve becomes irritated or inflamed due to the friction caused by the impingement of the muscles in the forearm. Radial nerve entrapment manifests symptoms of sensory disruption in the lateral three and a half digits of the dorsal aspect of the hand. Motor�fibers may also be affected along the�posterior arm and extensor compartment of the forearm, and wrist drop may be seen. Other forms of radial tunnel syndrome include: spiral groove entrapment, where all radial nerve innervated muscles below entrapment are affected,�Saturday night palsy caused due to sleeping on your own arm and the brachioradialis & triceps reflexes are both diminished, supinator syndrome, caused by the compression at the arcade of Frohse with no change in reflexes. Posterior interosseous syndrome, or radial tunnel syndrome, also elicits no change in reflexes.
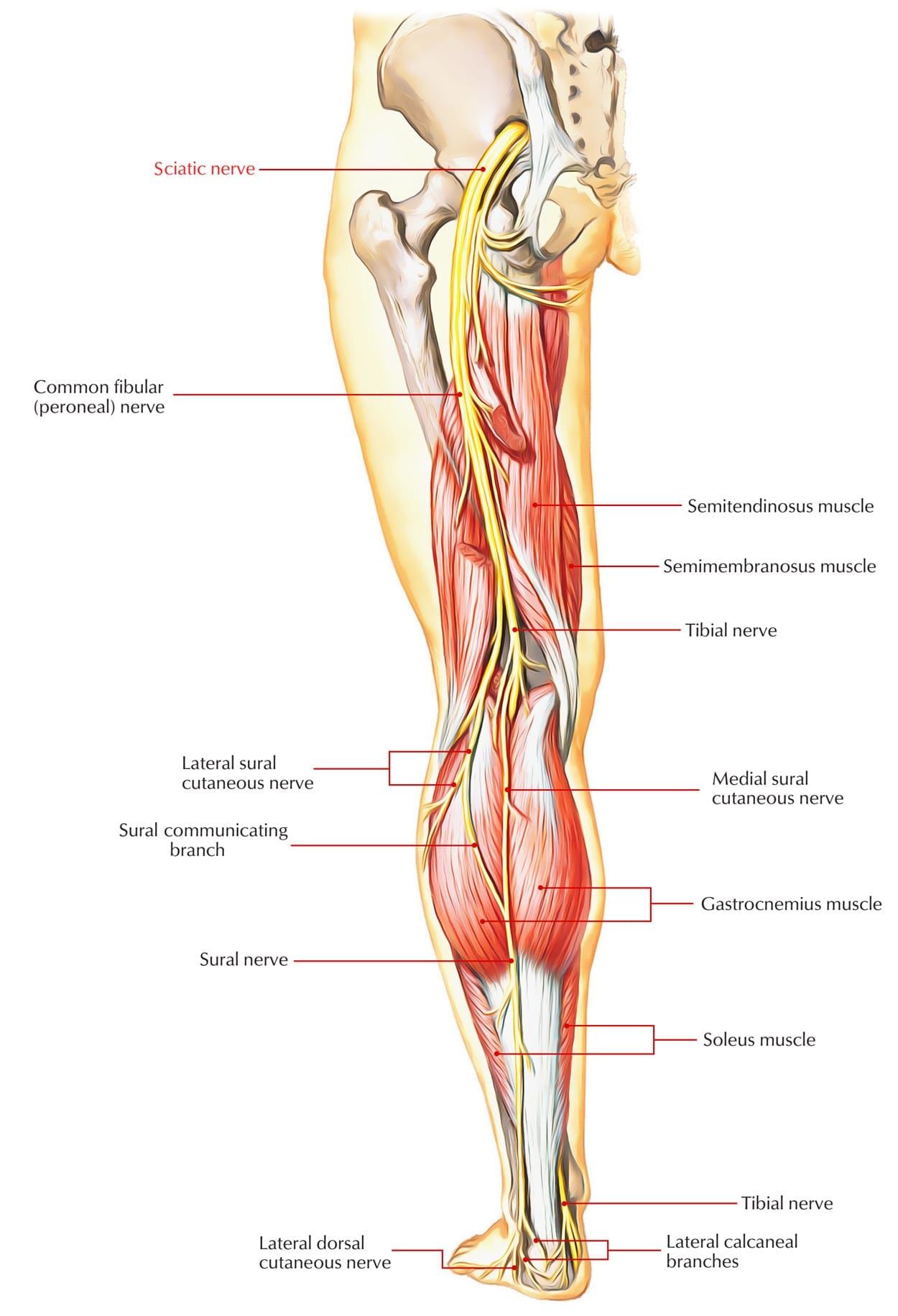
Sciatic Nerve Entrapment
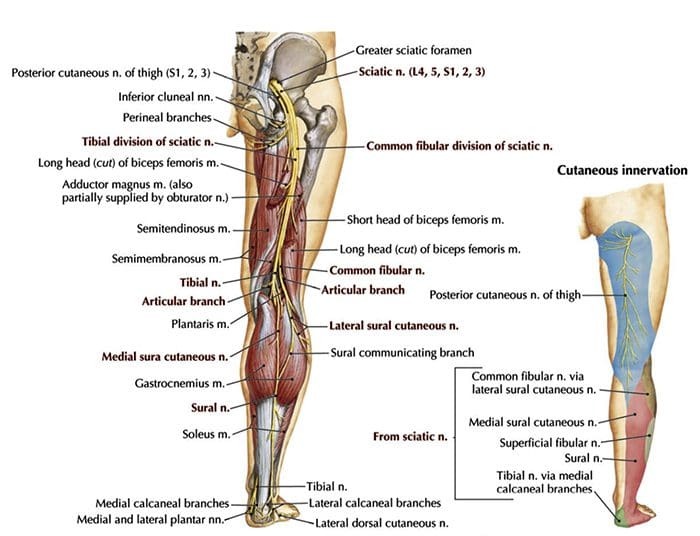
Sciatic nerve entrapment is a condition caused by the compression of the sciatic nerve, the longest and largest nerve in the human body, which travels from the low back, down through the buttocks, thighs, legs and into the foot. The collection of symptoms which manifest as a result of sciatic nerve entrapment, including pain and discomfort, tingling and burning sensations, and numbness as well as weakness in the lower extremitites, is commonly known as sciatica. Sciatic nerve entrapment, or sciatica, can be caused by a variety of injuries and/or aggravated conditions which can lead to the compression of the sciatic nerve, including, but not limited to, disc herniation and spinal stenosis. However, symptoms of sciatic nerve entrapment may vary depending on the location of the compression of the sciatic nerve. Other conditions caused by the compression of the sciatic nerve include: piriformis syndrome, peroneal nerve entrapment and tarsal tunnel syndrome.
Piriformis syndrome is a condition which occurs due to the compression of the sciatic nerve as a result of the irritation or inflammation of the piriformis muscle. Symptoms of piriformis syndrome may include pain and discomfort, followed by numbness in the buttocks and down the leg. Symptoms may worsen with regular activities, such as sitting and running. Piriformis syndrome is caused by anatomic variation or due to piriformis overuse/tension. Piriformis syndrome diagnosis exams include, a positive Lase?gue test, where the healthcare professional�extends the patient�s leg passively, while the patient is lying supine,�test is positive if the maneuver is limited by pain, and through the use of tenderness and palpable tension in piriformis muscle which elicits symptoms.
Peroneal nerve entrapment is a condition which occurs when the peroneal or the fibular branch of the sciatic nerve are compressed at the fibular head. Tinel�s sign may be present at the fibular region of the head and/or neck. Peroneal nerve entrapment generally affects the common peroneal nerve, therefore, motor and sensory symptoms may manifest, including, weakness of the ankle dorsiflexion and eversion, or the tibialis anterior. Other symptoms of peroneal nerve entrapment may include sensory disruption on the dorsum of the foot and lateral aspect of the calf. Common peroneal nerve entrapement at the fibular head is the most common nerve entrapment syndrome in the lower extremities.
Tarsal tunnel syndrome, also known as posterior tibial neuralgia, is a condition caused by the compression of the tibial nerve as it travels through the tarsal tunnel, found along the region of the inner leg, posterior to the medial malleolus, or the bump on the inside of the ankle. Tarsal tunnel syndrome can manifest symptoms of pain and discomfort, burning or tingling sensations, and numbness along the big toe and the first three toes. However, symptoms may vary slightly depending on the area of compression, where the entire foot may manifest the symptoms previously described. Other symptoms associated with posterior tibial neuralgia include sensory changes in the sole of the foot. Tinel�s sign may be present with percussion posterior to the medial malleolus. The exact cause of tarsal tunnel syndrome may be difficult to determine and it is essential to receive a proper diagnosis to determine the source of the symptoms.
Radiculopathy
Radiculopathy is a mononeuropathy,�a condition that impacts only a single nerve or nerve group outside the brain and spinal cord, which affects the movement of or sensation in one specific area. It is often associated with neuropathy involving spinal nerve roots and presents as changes in sensory and/or motor function affecting a single or a few nerve root level(s). The most common types of radiculopathies include: sciatica and cervical radiculopathy. The most prevalent causes of radiculopathy include, disc herniation, osteophytes, spinal stenosis, trauma, diabetes, epidural abscess or metastasis, nerve sheath tumors, such as schwannomas and neurofibromas, Guillain-Barre? syndrome, Herpes Zoster, or shingles, Lyme disease, cytomegalovirus, myxedema and/or thyroid disorder, and idiopathic neuritis.
Narrowing down some of the most common causes of radiculopathy, symptoms can manifest due to disc herniation which most commonly affects the nerve roots along the C6, C7, L5 & S1 vertebrae of the spine, spinal stenosis and lumbar stenosis which may produce neurogenic claudication, and pain and weakness with ambulation. Cervical stenosis may present with mixed radiculopathy and myelopathy due to long tract involvement. Symptoms may also manifest due to trauma, because it may lead to compression, trauma or avulsion of the nerve roots, diabetes, which is most�likely to cause a polyneuropathy, but mononeuropathy is possible, and Herpes Zoster, or shingles, most often on the trunk, accompanied by vesicular lesions in a single dermatome. If pain persists past vesicular regression, radiculopathy may instead be considered post-herpetic neuralgia.
Patients with a history of radiculopathy will often complain of burning pain or tingling sensations which radiates or shoots down an affected area in a “dermatomal” pattern. Occasionally, patients will complain of motor weakness, however if onset is recent, there is often no motor involvement. The diagnosis of radiculopathy can depend on a variety of exams.�Most often, hypoesthesia may be present in the affected dermatome level. It’s recommended to�evaluate for pain, as light touch can be difficult for these patient�s to distinguish. Fasciculations and/or atrophy may be seen if radiculopathy is chronic, due to the lower motor neuron being compressed or impinged. Motor weakness may be seen in muscles innervated by the same root level. Orthopedic tests for the diagnosis of radiculopathy may include: the straight-leg raise test (SLR), where pain between 10 to 60 degrees likely indicates nerve root compression, the�Well-leg raise/Crossed straight-leg raise test (WLR), where if positive, 90 percent specificity for L/S nerve root compression may be present, the Valsalva Maneuver, where its considered positive if there is an increase in radicular symptoms, and spinal percussion, where pain may indicate metastatic disease, abscess or osteomyelitis.
Specific radiculopathy patterns may also develop as a result of different regions being affected. Radiculopathy along the T1 can cause Horner�s syndrome, a combination of symptoms caused by the disruption of a nerve pathway from the brain to the face and eye on one side of the body. This is due to its effect on cervical sympathetic ganglia, includind ptosis, miosis, anhidrosis. Radiculopathy below the L1, can cause Cauda Equina syndrome, a condition caused by damage or injury to the bundle of nerves found below the end of the spinal cord, known as the cauda equina. This type of radiculopathy may manifest symptoms of saddle anesthesia, sensory loss in the S2-S5 distribution, urinary retention or overflow incontinence, constipation, decreased rectal tone or fecal incontinence, and loss of erectile function. Individuals with these signs and symptoms must be referred for emergency care immediately to prevent permanent dysfunction.
Other patterns of neuropathy can include the cape/shawl distribution of symptoms, identified by an intramedullary lesion, such as syringomyeli, intramedullary tumor and central cord damage. Stocking and glove distribution of symptoms may manifest as a result of diabetes mellitus,�B12 deficiency, alcoholism and/or hepatitis,�HIV, and thyroid dysfunction and/or myxedema.
The cape/shawl pattern of neuropathy is characterized by symptoms occurring due to an intramedullary lesion, such as a tumor, syringomyelia or a hyperextension injury in patient with C/S spondylosis. It can also be characterized by loss of pain and temperature sensation in C/T dermatomes because of the arrangement of the lateral spinothalamic tract. The stocking and glove pattern may progress gradually depending on its specific stage. It can also be characterized as a symmetrical polyneuropathy, where the feet and legs are generally affected first, followed by the hands and arms. A vibration-like sensation in the smallest toes are also typically the first to go and the neuropathy symptoms may progress across the foot to the big toe and then upward through the ankle and leg, then hands, arms and finally to the trunk if the condition becomes severe. The most likely cause of this pattern may be attributed to diabetes mellitus, but other possible causes include, B12 deficiency, alcoholism, HIV, chemotherapy treatment, thyroid dysfunction and multiple other causes.
Diabetic Neuropathy
Diabetic neuropathy is medically defined as a collection of nerve damaging disorders associated with diabetes. These conditions are believed to occur as a result of a diabetic microvascular injury involving the small blood vessels, known as the vasa nervorum, which supply the nerves. Additionally, macrovascular conditions have also been considered to accumulate and cause diabetic neuropathy.�Diabetic neuropathy often presents as a polyneuropathy, or the simultaneous damage or disease of many peripheral nerves throughout the body, but it can also present as a mononeuropathy, usually with acute onset. Diabetic neuropathy most commonly affects the CN III, femoral and sciatic nerves. Diabetic neuropathy can affect all peripheral nerves, including the sensory neurons, motor neurons and, although rarely, the autonomic nervous system. As a result, diabetic neuropathy can affect all organs and systems, as these are all innervated. Diabetic neuropathy can manifest into a wide array of symptoms, including, but not limited to, pain, burning or tingling sensations, numbness, dizziness and trouble with balance.
Demyelinating Neuropathies
Demyelinating neuropathies can be individually defined by its two types: Acute inflammatory demyelinating polyneuropathy, best known as�Guillain-Barre? syndrome, or Chronic inflammatory demyelinating polyneuropathy.�Guillain-Barre? syndrome, abbreviated as AIDP, is identified as a rapid-onset muscle weakness caused when the immune system damages, harms or destroys the peripheral nervous system. Onset has been reported by around one to two weeks following viral infection with progressive weakness, loss of DTRs/areflexia, paresthesia in the hands and feet, more motor involvement than sensory, potential autonomic fiber involvement, elevated CSF protein, and EMG/NCV studies indicating demyelination.�Guillain-Barre? syndrome may require treatment with plasmapheresis or IV Ig therapy.�Chronic inflammatory demyelinating polyneuropathy, abbreviated as CIDP,�is identified as an acquired immune-mediated inflammatory disorder of the peripheral nervous system which appears similar to AIDP but does not follow infection. Symptoms must be present for at least 8 weeks for this diagnosis to be considered positive.�Anti-inflammatory treatments may help treat CIDP.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
The vast array of symptoms caused by neuropathy, also known as peripheral neuropathy, reflect the fact that it may be caused by an equally broad range of ailments involving disease and damage to peripheral nerves.
Signs and Symptoms of Neuropathy
Depending on the reason and unique to each patient, signs and symptoms of neuropathy can include:�pain; tingling, burning or prickling sensations; increased sensitivity to touch; muscle weakness or wasting;�temporary or permanent numbness; paralysis; dysfunction in glands or organs; or impairment in urination and sexual functioning.
Such signs and symptoms are dependent on whether autonomic, sensory, or motor nerves, as well as a combination of them, are ultimately affected. Autonomic nerve damage can influence physiological functions like blood pressure or create gastrointestinal problems and issues. Damage or dysfunction in the sensory nerves may impact sensations and sense of equilibrium or balance, while harm to motor nerves may affect movement and reflexes. When both sensory and motor nerves are involved, the condition is known as sensorimotor polyneuropathy.
Diabetic Neuropathy Symptoms
Diabetic peripheral neuropathy, which affects between 12 and 50 percent of individuals with diabetes, is one of the most common types of neuropathy. Many times, symptoms include a gradual change in sensation, as well as pain and weakness in the feet and, although less commonly, the hands. As the neuropathy develops further, it can lead to a loss of sensation in the affected regions.
This lack of feeling raises the odds of harm to the affected areas, explains Matthew Villani, doctor of podiatric medicine at Central Florida Regional Hospital at Lake Mary. Without the pain to signal when there’s an issue, individuals with diabetic neuropathy may allow modest abrasions or blisters on their feet, for instance, to fester as sores or ulcers. “The ulcers can become infected since they are open wounds, which can also progress to bone infection. Unfortunately, it frequently requires amputations if it does progress to that point”, states Dr. Matthew Villani.
Chemotherapy-Associated Neuropathy Symptoms
Cancer patients may suffer with neuropathy induced by chemotherapy as well as by other drugs and/or medications used to treat the disease. Symptoms can include intense pain, impaired movement, changes in heart rate and blood pressure, issues with balance, difficulty breathing, paralysis, and even organ failure. After chemotherapy is done, the symptoms frequently abate swiftly, but occasionally they last more, or these may not go away at all.
HIV- and AIDS-Associated Neuropathy Symptoms
Individuals being treated for HIV or AIDS can develop neuropathy from effects of the virus and the drugs and/or medications used to treat it as well. Common symptoms include stiffness, burning, prickling, tingling, and loss of feeling in the toes and soles of their feet. Sometimes the nerves in the fingers, hands, and wrists are also affected. The drugs Videx (didanosine), Hivid (zalcitabine), and Zerit (stavudine) have been most commonly associated with neuropathic symptoms.
Inflammation-Associated Neuropathy Symptoms
Inflammation caused by infections, like herpes zoster (also known as shingles), Lyme disease, or hepatitis B and hepatitis C, may lead to neuropathy, as may inflammation caused by autoimmune disorders, such as vasculitis, sarcoidosis, or autoimmune disease. In such situations, the signs and symptoms generally include burning and tingling sensations or numbness.
Other Causes of Neuropathy Symptoms
Additional causes of neuropathy and associated signs and symptoms include metabolic disorders, such as hypoglycemia or kidney failure; autoimmune disorders, such as rheumatoid arthritis, lupus, Sjogren’s syndrome, and Guillain-Barr� syndrome; toxicity; hereditary disorders, such as Charcot-Marie-Tooth disorder; hormonal disorders; alcoholism; vitamin deficiencies; physical trauma or injury; compression; and repetitive stress. In addition, many individuals may experience idiopathic neuropathy signs and symptoms, meaning that healthcare professionals may not know the reason for their neuropathy.
Dr. Alex Jimenez’s Insight
Neuropathy can be caused by a variety of injuries and/or aggravated conditions, often manifesting into a plethora of associated signs and symptoms. While every type of neuropathy, such as diabetic neuropathy or autoimmune disease-associated neuropathy, develops its own unique group of signs and symptoms, many patients will often report common complaints. Individuals with neuropathy generally describe their pain as stabbing, burning or tingling in character. If you experience unusual or abnormal tingling or burning sensations, weakness and/or pain in your hands and feet, it’s essential to seek immediate medical attention in order to receive a proper diagnosis of the cause of your specific signs and symptoms. Early diagnosis may help prevent further nerve injury.
What are the Common Signs and Symptoms of Neuropathy?
“Although there’s a wide array of signs and symptoms associated with neuropathy, the type of pain that people encounter may be common in many aspects of the disorder”, notes Vernon Williams, MD, a sports neurologist and director of the Center for Sports Neurology and Pain Medicine at Cedars-Sini Kerlan-Jobe Institute in Los Angeles. “The character and quality of neuropathic pain will often be pain that is burning or electric in character.” Furthermore, he describes that the pain will frequently be associated with different symptoms, like paresthesia, or a lack of normal sensation associated with pain; allodynia, or a painful reaction to a stimulus that wouldn’t normally trigger pain signals; and hyperalgesia, or a striking or severe pain in response to a stimulus that normally causes moderate pain.
How is Neuropathy Diagnosed?
If you think you’re having any of the above neuropathy signs and symptoms, consult a healthcare professional. A number of tests can be done to diagnose neuropathy. “There are certain patterns of complaints that indicate neuropathy,” stated Dr. Williams, “so taking down a patient’s history which includes a description of these complaints is an important first step.”
“After that, your healthcare professional can perform a physical evaluation, including checking motor and sensory function, assessing deep tendon reflexes, as well as looking for signs and symptoms like allodynia and hyperalgesia,” Williams says. “Then we can even perform electrodiagnostic testing; the most common being electromyography and nerve conduction testing, where we can stimulate nerves and document responses, calculate the rate at which signals are being transmitted and see whether there are some areas where nerves are not transmitting signals normally,” Williams continues.
With needle tests, Williams states, “We can put modest needles into human muscles, and, according to what we see and listen together with all the needle in the muscle, we get details about the way the nerves supplying those muscle tissues are functioning. There are a number of unique tests that could be handy to identifying neuropathy, in addition to localizing where the abnormality is the most likely to be coming from”, concluded Dr.�Vernon Williams.
Often, blood tests may test for elevated blood glucose to see whether your neuropathy signs and symptoms could possibly be associated to type 2 diabetes, nutritional deficiencies, toxic elements, hereditary disorders, and evidence of an abnormal immune response. Your healthcare professional may also do a nerve biopsy, which normally involves removing a small segment of a sensory nerve to search for abnormalities, or even a skin biopsy to see if there’s a reduction in nerve endings.
To give yourself the best chance of an accurate diagnosis as well as relief from your neuropathy signs and symptoms, be prepared to describe everything you are experiencing in detail, even when you experience them, how long an episode persists, and the amount of pain, discomfort or loss of sensation or movement you experience. The more specific you are on the signs and symptoms you’re experiencing, the easier it’ll be for your doctor to understand what’s happening. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Sciatica Pain: Sandra Rubio discusses sciatica, its causes and its symptoms. Sciatica is the collection of symptoms caused by the compression of the sciatic nerve, the longest nerve in the human body which extends from the lower back to the feet. Sandra Rubio describes how she’s witnessed many patients come into Dr. Alex Jimenez’s office feeling painful and often severe symptoms of sciatica caused by a variety of spinal health issues. Fortunately, Dr. Alex Jimenez is the non surgical choice for the safe and effective treatment of sciatica symptoms.
Sciatica Pain Explained
Based upon how it’s defined, approximately 2 percent to 40 percent of individuals will experience sciatica symptoms at some point in their lifetime. It is most frequent during people’s 40’s and 50’s, and men are more frequently affected than women. About 90 percent of the time, sciatica symptoms are because of a disc herniation. Other issues that may bring about sciatica comprise of spondylolisthesis, spinal stenosis, piriformis syndrome, pelvic tumors, and compression by a baby’s head during pregnancy, among other spinal health issues.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last 2 decades while researching and testing methods with thousands of patients we have learned what works effectively at decreasing pain while increasing human vitality.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural, and use the body�s own ability to achieve goals of improvement, rather than introducing harmful chemicals, controversial hormone replacement, surgery, or addictive drugs.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of each and every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Sciatica Pain: The sciatic nerve is the largest single nerve found within the human body, running from each side of the lumbar spine, through the area of the lumbar plexus, and trailing down into the buttocks, the back of the thigh and into the foot.
Sciatica is a medical term used to define a group of symptoms rather than a single injury or condition. The most common symptom for sciatica is pain in the lower back and, although low back pain can be the result of numerous lumbar spine injuries or conditions, various other common symptoms associated with sciatica can closely suggest its presence. Often a result of damage or impingement of the sciatic nerve, many people affected with sciatica experience burning and tingling sensations along the back of the thigh, followed by numbness or cramping. People suffering from sciatica may have difficulty going through their regular activities but chiropractic care can help relieve the symptoms and treat many other underlying conditions causing the pain and discomfort.
Sciatica Pain: Surgery Vs. Chiropractic
Chiropractic treatment for mild to severe cases of sciatica most frequently involves chiropractic adjustments and manual manipulations, followed by a specialized series of stretches and exercises accommodated to each individual�s level of injury or condition and its symptoms. Both of these treatments together may speed up the rehabilitation process as well as improve the health of the spine and ultimately reduce the symptoms of sciatica.
Sciatica is used to identify a set of symptoms on the region of the lumbar spine, generally as a result of a previous injury or underlying condition. Regular symptoms of low back pain, stiffness, and burning or tingling sensations could indicate the presence of sciatica. For more information, please feel free to ask Dr. Jimenez or contact us at (915) 850-0900.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




 Causes
Causes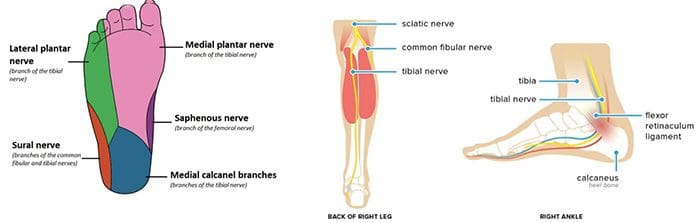 Radiculopathy
Radiculopathy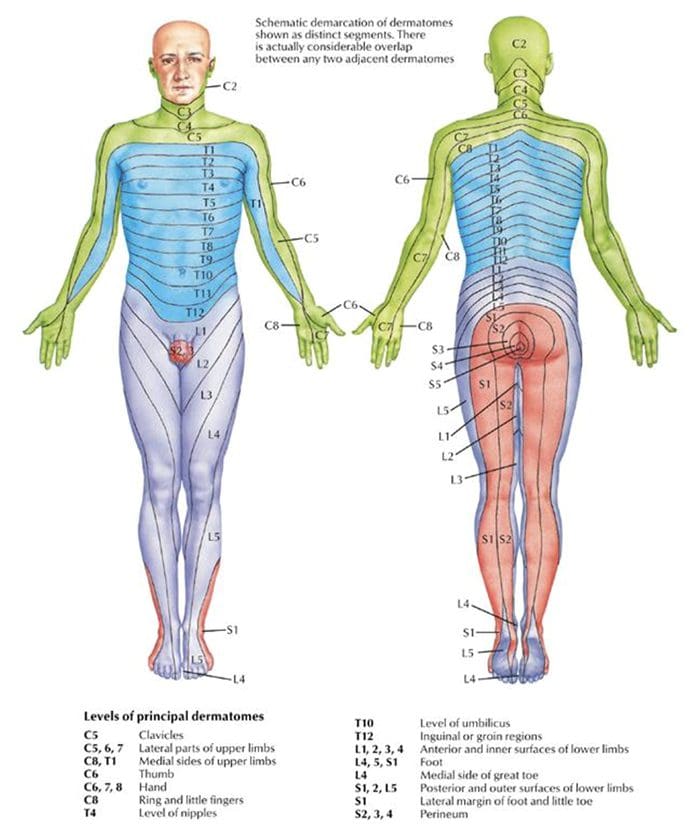 Testing Cervical Nerve Roots
Testing Cervical Nerve Roots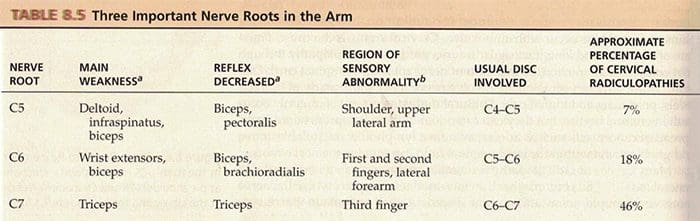 Testing Lumbosacral Nerve Roots
Testing Lumbosacral Nerve Roots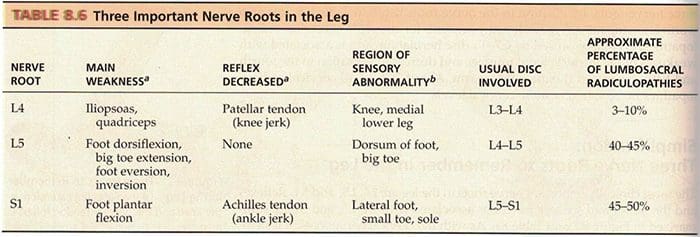
 Stocking & Glove Pattern
Stocking & Glove Pattern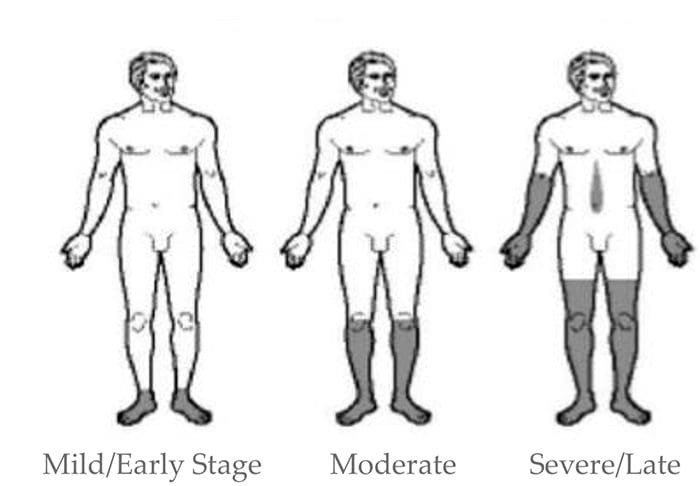
 Erb�s Palsy
Erb�s Palsy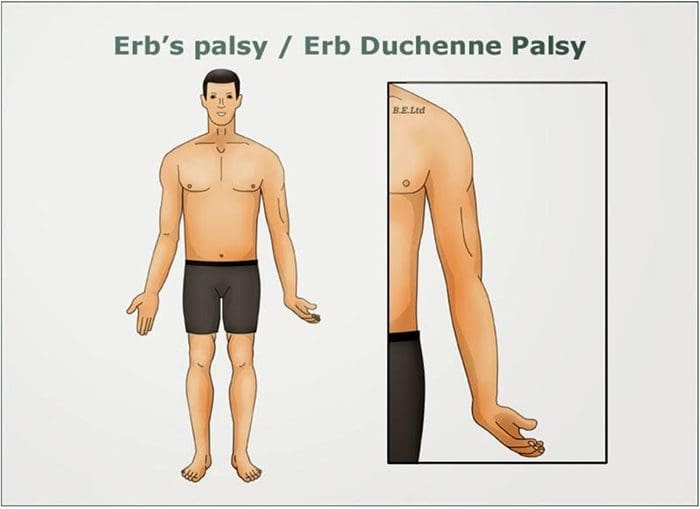 Klumke�s Palsy
Klumke�s Palsy Entrapment Neuropathies
Entrapment Neuropathies
 Median N. Pronator Teres Syndrome
Median N. Pronator Teres Syndrome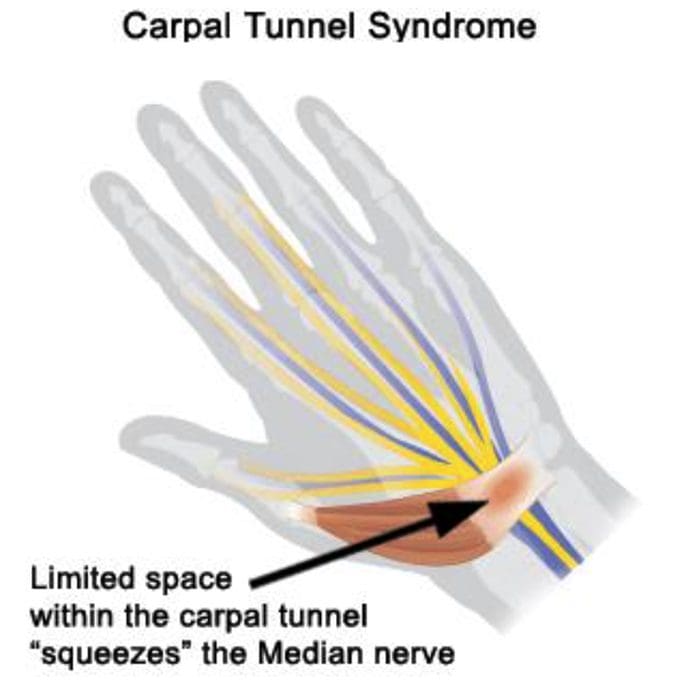
 Tinel�s Sign
Tinel�s Sign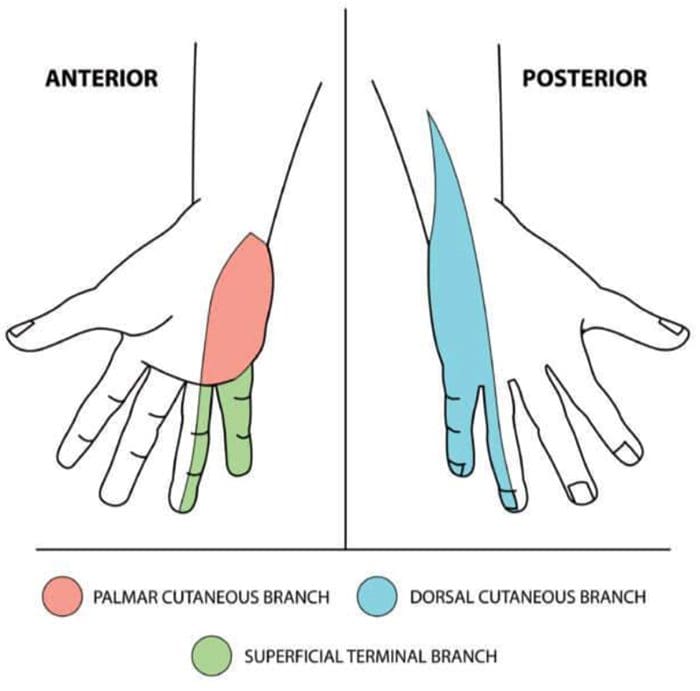
 Etiology
Etiology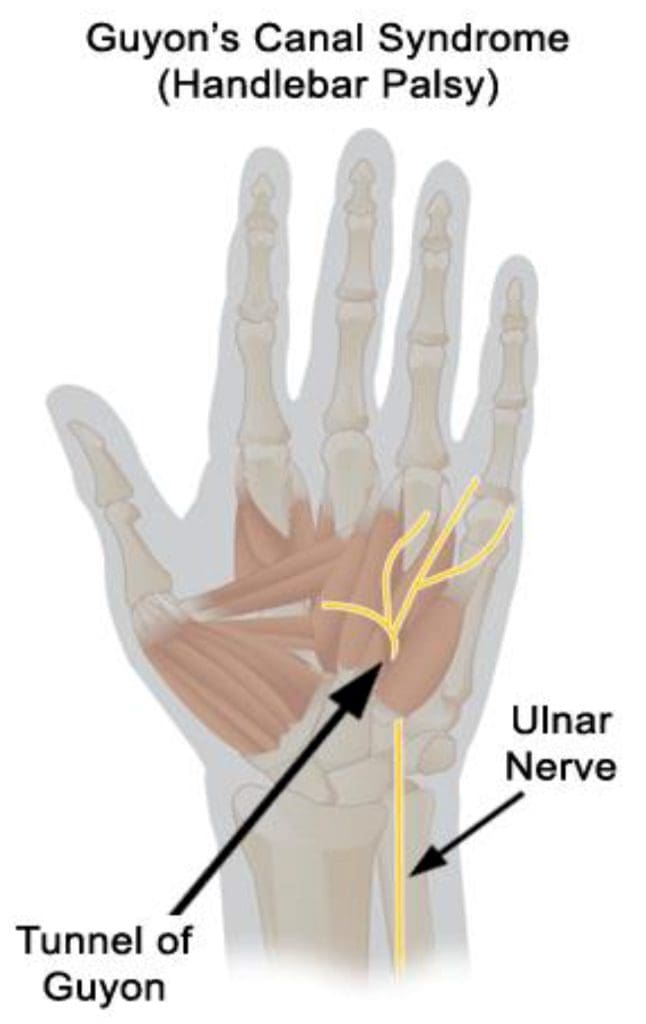



 When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last 2 decades while researching and testing methods with thousands of patients we have learned what works effectively at decreasing pain while increasing human vitality.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last 2 decades while researching and testing methods with thousands of patients we have learned what works effectively at decreasing pain while increasing human vitality.








