The neck is vital in keeping the head upright in a casual relationship with the cervical spine. The neck is home to the thyroid organ and the surrounding muscles that help support the neck to the rest of the body. One of the muscles that help support the neck is the sternocleidomastoid muscle. When traumatic forces begin to affect the neck, over time can lead to the development of chronic conditions associated with pain. When individuals start to feel pain affecting their neck, it can cause them to be miserable and find ways to relieve the pain they are experiencing. Today’s article focuses on the sternocleidomastoid muscle, how trigger pain affects this muscle, and ways to relieve SCM pain. We refer patients to certified providers who specialize in musculoskeletal treatments to aid individuals suffering from SCM associated with trigger pain along the neck. We also guide our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure to find that education is the solution to asking our providers insightful questions. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
What Is The Sternocleidomastoid Muscle?
Have you been experiencing pain along the sides of your neck? What about limited mobility when you turn your neck from side to side? Or do headaches seem to worsen throughout the entire day? Some of these symptoms are associated with pain along the neck and could affect the surrounding muscles that are connected. One of the surrounding muscles that sit behind the thyroid is known as SCM or sternocleidomastoid muscle. The sternocleidomastoid muscle is a long muscle with dual innervation and multiple functions in the neck. The SCM is connected to the trapezius muscle that helps flex the neck, pulling the head forward while bringing the chin down to the chest. The SCM and the trapezius muscle work together to help stabilize and fix the head position while the host is talking or eating. When factors affect the neck over time, the SCM also gets involved.
How Does Trigger Pain Affect The Sternocleidomastoid?
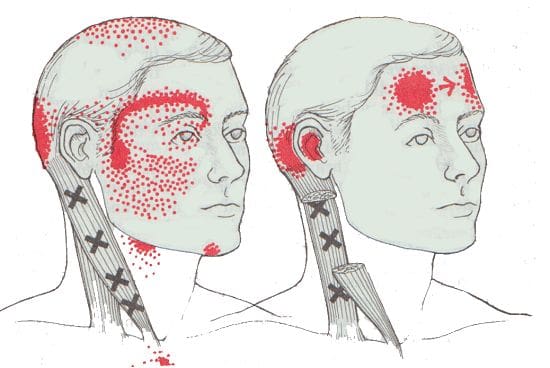
When factors affect SCM associated with the neck, many issues will start to affect the neck and overlap pain near the eyes, ears, sides of the cheeks, and forehead. Studies reveal that SCM may develop myofascial trigger points in the head, causing referred pain. Trigger points are usually formed when traumatic forces affect certain areas in the body. For SCM to be affected by trigger pain, tiny knots along the taut band of the SCM muscle fibers become sensitive to pressure when compressed, and many people often describe the pain as deep and dull. To that point, the symptoms associated with SCM trigger pain may appear in numerous combinations or together depending on how severe the pain is on the person. Some of the symptoms related to SCM trigger pain include:
Headaches (sinus, cluster, or tension)
Sore throat
Ear pain (popping sounds in the ears)
Blurred vision
Vertigo
Dizzyness
Balance issues
Muscle soreness
SCM Pain & Trigger Points- Video
Have you been dealing with headaches throughout the entire day? What about muscle tenderness in certain areas near your neck or shoulders? Or have you been feeling dizzy that it is affecting your daily activities? Many people with these symptoms may be dealing with SCM pain associated with trigger pain. The video above offers an insightful overview of how does trigger pain may be involved with SCM pain. SCM or sternocleidomastoid muscle is a long muscle that surrounds the sides of the neck and is connected to the trapezius muscle. When factors begin to affect the SCM, the muscle is at risk of developing trigger pain along the muscle fibers. Studies reveal that trigger pain along the SCM may affect SCM’s normal muscle functions, like chewing due to hyperactivity. Fortunately, there are ways to relieve SCM pain associated with trigger pain affecting the neck.
Ways To Relieve SCM Pain In The Neck
When it comes to SCM pain associated with trigger pain along the neck, many individuals find ways to relieve the related symptoms that are causing the pain. Some individuals will take over-the-counter medication to relieve their neck, shoulders, and head pain. At the same time, others do stretches to release the tension on their head, neck, and shoulders. However, trigger pain is a bit complex and challenging to diagnose since it mimics other conditions that affect the body. As luck would have it, many doctors will refer musculoskeletal specialists like massage therapists, physical therapists, and chiropractors who can help relieve SCM pain in the neck. Studies reveal that a combination of physiotherapy, classical massages, and stretching exercises can be applied to alleviate SCM pain in the neck. By stretching and massaging the SCM, many individuals can begin to feel pain relief in their neck, increase their range of motion, and have endurance in their neck. Integrating these various treatments for the SCM (sternocleidomastoid muscle) pain in the neck can help revitalize a person’s sense of well-being without being in pain.
Conclusion
The SCM, or sternocleidomastoid muscle, is a long muscle that sits behind the thyroid organ and is connected with the trapezius muscle. This muscle helps stabilize and holds the head position while flexing the neck and bringing the chin down to the chest. When environmental or traumatic factors affect the neck muscles, it can lead to chronic conditions over time, thus inflicting pain and tenderness along the SCM. These are known as trigger points and can be hard to diagnose due to them mimicking other chronic symptoms associated with the neck, head, and shoulders. Thankfully, various treatments like physiotherapy, stretching exercises, and classical massages can help relieve the trigger points along the SCM and relieve the neck and surrounding muscles.
References
Bordoni, Bruno, and Matthew Varacallo. “Anatomy, Head and Neck, Sternocleidomastoid Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 5 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK532881/.
Büyükturan, Buket, et al. “The Effects of Combined Sternocleidomastoid Muscle Stretching and Massage on Pain, Disability, Endurance, Kinesiophobia, and Range of Motion in Individuals with Chronic Neck Pain: A Randomized, Single-Blind Study.” Musculoskeletal Science & Practice, U.S. National Library of Medicine, 12 June 2021, https://pubmed.ncbi.nlm.nih.gov/34147954/.
Kohno, S, et al. “Pain in the Sternocleidomastoid Muscle and Occlusal Interferences.” Journal of Oral Rehabilitation, U.S. National Library of Medicine, July 1988, https://pubmed.ncbi.nlm.nih.gov/3171759/.
Missaghi, Babak. “Sternocleidomastoid Syndrome: A Case Study.” The Journal of the Canadian Chiropractic Association, Canadian Chiropractic Association, Sept. 2004, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1769463/.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Sternocleidomastoid (SCM)
Assessment for Shortness of Sternocleidomastoid�(see also Box 4.10)
Assessment for SCM is as for the scalenes � there is no absolute test for shortness but observation of posture (hyperlordotic neck, chin poked forward) and palpation of the degree of induration, fibrosis and trigger point activity can all alert to probable shortness of SCM. This is an accessory breathing muscle and, like the scalenes, will be shortened by inappropriate breathing patterns which have become habitual. Observation is an accurate assessment tool.
Box 4.10 Notes on Sternocleidomastoid
Sternocleidomastoid (SCM) is a prominent muscle of the anterior neck and is closely associated with the trapezius. SCM often acts as postural compensator for head tilt associated with postural distortions found elsewhere (spinal, pelvic or lower extremity functional or structural inadequacies, for instance) although they seldom cause restriction of neck movement.
SCM is synergistic with anterior neck muscles for flexion of the head and flexion of the cervical column on the thoracic column, when the cervical column is already flattened by the prevertebral muscles. However, when the head is placed in extension and SCM contracts, it accentuates lordosis of the cervical column, flexes the cervical column on the thoracic column, and adds to extension of the head. In this way, SCM is both synergist and antagonist to the prevertebral muscles (Kapandji 1974).
SCM trigger points are activated by forward head positioning, �whiplash� injury, positioning of the head to look upwardly for extended periods of time and structural compensations. The two heads of SCM each have their own patterns of trigger point referral which include (among others) into the ear, top of head, into the temporomandibular joint, over the brow, into the throat, and those which cause proprioceptive disturbances, disequilibrium, nausea and dizziness. Tenderness in SCM may be associated with trigger points in the digastric muscle and digastric trigger points may be satellites of SCM trigger points (Simons et al 1998).
Simons et al (1998) report: When objects of equal weight are held in the hands, the patient with unilateral trigger point [TrP] involvement of the clavicular division [of SCM] may exhibit an abnormal Weight Test. When asked to judge which is heaviest of two objects of the same weight that look alike but may not be the same weight (two vapocoolant dispensers, one of which may have been used) the patient will [give] evidence [of] dysmetria by underestimating the weight of the object held in the hand on the same side as the affected sternocleidomastoid muscle. Inactivation of the responsible sternocleidomastoid TrPs promptly restores weight appreciation by this test. Apparently, the afferent discharges from these TrPs disturb central processing of proprioceptive information from the upper limb muscles as well as vestibular function related to neck muscles.
Lymph nodes lie superficially along the medial aspect of the SCM and may be palpated, especially when enlarged. These nodes may be indicative of chronic cranial infections stemming from a throat infection, dental abscess, sinusitis or tumour. Likewise, trigger points in SCM may be perpetuated by some of these conditions (Simons et al 1998).
Lewit (1999) points out that tenderness noted at the medial end of the clavicle and/or at the transverse process of the atlas is often an indication of SCM hypertonicity. This will commonly accompany a forward head position and/or tendency to upper chest breathing, and will almost inevitably be associated with hypertonicity, shortening and trigger point evolution in associated musculature, including scalenes, upper trapezius and levator scapula (see crossed syndrome notes in Ch. 2).
Since SCM is only just observable when normal, if the clavicular insertion is easily visible, or any part of the muscle is prominent, this can be taken as a clear sign of tightness of the muscle.�If the patient�s posture involves the head being held forward of the body, often accompanied by cervical lordosis and dorsal kyphosis (see notes on upper crossed syndrome in Ch. 2), weakness of the deep neck flexors and tightness of SCM is suspected.
Functional SCM Test (see Fig. 5.14A, B)
The supine patient is asked to �very slowly raise your head and touch your chin to your chest�. The practitioner stands to the side with his head at the same level as the patient. At the beginning of the movement of the head, as the patient lifts this from the table, the practitioner would (if SCM were short) note that the chin was lifted first, allowing it to jut forwards, rather than the forehead leading the arc-like progression of the movement. In marked shortness of SCM the chin pokes forward in a jerk as the head is lifted. If the reading of this sign is unclear then Janda (1988) suggests that a slight resistance pressure be applied to the forehead as the patient makes the �chin to chest� attempt. If SCM is short this will ensure the jutting of the chin at the outset.
MET Treatment of Shortened SCM (Fig. 4.35)
The patient is supine with the head supported in a neutral position by one of the practitioner�s hands. The shoulders rest on a cushion or folded towel, so that when the head is placed on the table it will be in slight extension. The patient�s contralateral hand rests on the upper aspect of the sternum to act as a cushion when pressure is applied during the stretch phase of the operation (as in scalene and pectoral treatment). The patient�s head is fully but comfortably rotated, contralaterally.
Figure 4.35 MET of sternocleidomastoid on the right.
The patient is asked to lift the fully rotated head a small degree towards the ceiling, and to hold the breath. When the head is raised there is no need for the practitioner to apply resistance as gravity effectively provides this.
After 7�10 seconds of isometric contraction (ideally with breath held), the patient is asked to slowly release the effort (and the breath) and to place the head (still in rotation) on the table, so that a small degree of extension occurs.
The practitioner�s hand covers the patient�s �cushion� hand (which rests on the sternum) in order to apply oblique pressure/stretch to the sternum, to ease it away from the head and towards the feet.
The hand not involved in stretching the sternum caudally should gently restrain the tendency the head will have to follow this stretch, but should not under any circumstances apply pressure to stretch the head/neck while it is in this vulnerable position of rotation and slight extension.
The degree of extension of the neck should be slight, 10�15� at most.
This stretch, which is applied as the patient exhales, is maintained for not less than 20 seconds to begin the release/stretch of hypertonic and fibrotic structures. Repeat at least once. The other side should then be treated in the same manner.
CAUTION: Care is required, especially with middle aged and elderly patients, in applying this useful stretching procedure. Appropriate tests should be carried out to evaluate cerebral circulation problems. The presence of such problems indicates that this particular MET method should be avoided.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine