
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Athletes, PUSH-as-Rx, Sports Injuries
El Paso, TX. Chiropractor, Dr. Jimenez takes a look at top running shoes that are great for knee pain and Iliotibial (IT) Band Syndrome.
Running Shoes: Knee pain is one of the common problems with most active people. It could get worse for those who love running, especially the athletes. A majority of them suffer from knee pains each year. This pain hinders you from enjoying your daily sports activities and might even become worse with time if not treated correctly. There are causes and cures for such pains that this article is going to look at, but the main focus is on the best shoes for knee pain, also referred to as Iliotibial (IT) Band Syndrome.
This can happen due to various causes like overtraining, running many hills, and wrong running form, among others. These injuries are very frustrating as they can take up to months to go away. This is the reason different companies have designed shoes that will offer you support for any knee problem.
What Goes Wrong
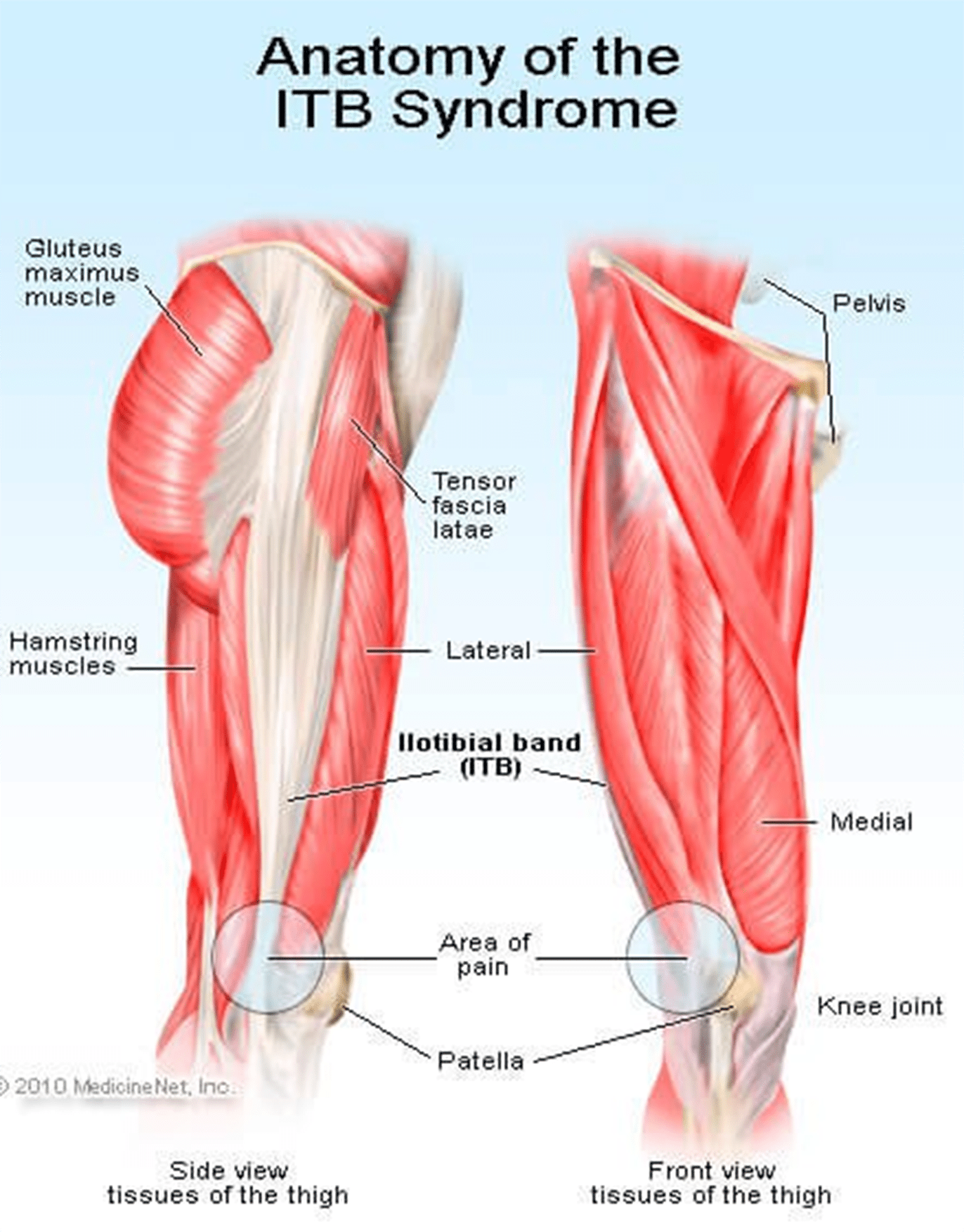
The iliotibial band (ITB) is usually a structure whose job is to provide leg stability whenever you take a step. It works with the hip muscles in a thigh’s outward movement and also helps counter the movements within the knee joint. This band starts in the hip and ends just under the knee joint.
Repeated use of the ITB leads to stress, causing knee pain. You will also notice clicking sensations from the joint as ITB snaps across it. This pain is always experienced when the heel comes into contact with the ground; running slowly or downhill tends to make the symptoms worse.
ITBS will usually start as tightness while running but continues to a point where the pain is severe and unbearable. Although ITB continues to tighten when overstressed or injured from training, this is not the main problem. What causes the injury is how the ITB functions and the weakness around it.
The ITB is generally a weak structure and any weakness around it will lead to injury. Most runners have weak core muscles due to the fact that they don’t do strength training or have never been in any sports with side-to-side movement.
 Signs Of IT Band Syndrome
Signs Of IT Band Syndrome
 If you are a runner, you will be able to distinguish ITBS by:
If you are a runner, you will be able to distinguish ITBS by:
- A swelling
- A cracking feeling when stretching the knee
- A feeling of burning, stinging and aching on the outer side of the knee that might migrate to the thigh. You will notice these discomforts especially, on your second half of the run.
- Bending the knee at 45 degrees causes severe external knee pain
Criteria You Should Follow When Selecting The Best Running Shoes for ITBS
?There are various things that you should always consider when buying running shoes. Since most runners experience knee pain, it is wise to look for shoes that will help alleviate this pain without slowing them down. Below are some of the features to look out for in running shoes:
Stability/ Support
Since it is common to have knee pains due to lack of motion control and lack of stability, it is good to choose shoes that will offer you the support you need while running. If your running shoes don’t have any stability, you will end up stressing out your knee, which will result in pain and discomfort while running.
Fit
 If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If your foot cannot move freely and the toes are restricted from spreading, it could lead to painful issues in your feet, legs, and knees.
Motion control footwear is not the whole solution; you need to ensure your feet can still function naturally as they are supposed to.
Comfort
No one wants to wear uncomfortable shoes! Each of these selected best shoes come with upper and underfoot comforts to ensure you get to enjoy your run.
Most of these shoes are made with DNA technology, Gel cushioning, and REVlite midsole for ultimate comfort.
Durability
Your running shoes should run their course without falling apart as this will cause you pain in the long-run. If they promise to offer you support, they should do just that and not start peeling off and tearing when you are on the run.
The ??below 5 shoes have passed the durability test to ensure they give you maximum performance.
Breathability
Although this has nothing to do with knees, it is paramount that your running shoes have enough breathing space to avoid accumulating excess moisture, which might bring discomfort and other feet related problems.
There is no magical cure for knee pain and you should always know the root cause. This way, you will be able to come up with the best solution of minimizing or even eliminating the pain entirely. Although there are various causes of knee pain, this article is focusing on ITB syndrome which happens to be one of the causes.
Reviews Of The Top 5 Shoes
These shoes have been selected with the runner’s welfare in mind. They will help deal with the ITBS, which is a problem for most of them. Since one way of dealing with this condition is getting good running shoes, here is a review of such products.
Asics Gel Kayano 23
 This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
PROS
- ?Gel cushioning will act as a shock absorber for more comfort
- ?Has superb breathability feature
- ?Is ideal for overpronation and knee pain
- ?The outsole’s traction will offer the intended support on various surfaces
CONS
New Balance 890v5
 It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
PROS
- ?It comes with one of a kind breathability and fit due to its great FantomFit design
- ?Its smooth upper construction will ensure no irritation occurs
- ?The REVlite midsole will give you much needed cushioning
CONS
- ?It has a narrow toe box and might not fit a person with a wide foot
?Puma Faas 600 V3
 Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
PROS
- ?Great breathability
- ?Comes at a reasonable price
- ?It’s lacing system and fit offers you a secure and comfortable run
- ?It is designed to fit perfectly
CONS
- ?There have been reported concerns about the outsole’s durability
New Balance 1080v7
 This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
PROS
- ?Very durable
- ?Enough breathability for long runs
- ?Good amount of cushioning and support from the Fresh Foam midsole
- ?It fits like a sock giving you a confident use
CONS
- ?The upper design is not seamless
- ?Can be stiff
Saucony Hurricane 16
 This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
PROS
- ?Superb stability
- ?Lightweight rubber offers protection and cushioning
- ?Great ground contact
- ?Reflective parts allow you to have a safe run
- ?Comes with Sauc-Fit Technology that enhances its comfortability
CONS
- ?It is a bit narrow
- ?Limited colors to choose from
- ?Might be heavy for fast runners
If you are a long-distance runner, it is good to know that your shoes cushioning will wear out quite easily and you might be tempted to continue using them since they look good on the outside. This is a big mistake. The following will help you prevent any more ITBS recurrences:
- Replace running shoes frequently to avoid wearing those with worn out inner cushioning
- Always give your shoes time to rest so that the cushioning can get restored; it would be wise to have two pairs of running shoes.
Although shoes can offer you relief from ITBS, it is better to look out for other ways of helping you cope with or eliminate the pain entirely. Also, know what triggers the problem and avoid it at all costs.
These shoes have been tried and tested and found to offer support and help in managing the iliotibial band syndrome. Asics takes the lead on these best shoes. It comes with gel cushioning that will offer you the best shock absorption and maximum comfort as seen above. Its sole is also made to help you tackle any terrain and you can be assured that your knees will thank you later. The only drawback is the price, which is on the upper-side. However, always remember that cheap is expensive.
If you are an active person or an athlete suffering from ITBS, go ahead and get yourself a pair of these shoes as per your preference and choice.
in running

Zoey Miller
Hey there, I’m Zoey, founder and the main editor of The Babble Out. I know nobody’s life is smooth as they wish, and it�s the same with mine. I had some terrible news a few years ago and running was the way I got through these issues. This has given me enough motivation to create this blog, so that I can give you a helping hand for as many daily problems as I can. If you are curious why “babble out” is the? name of the blog, then check the “About” page and find out more about me.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Chiropractic, Physical Rehabilitation
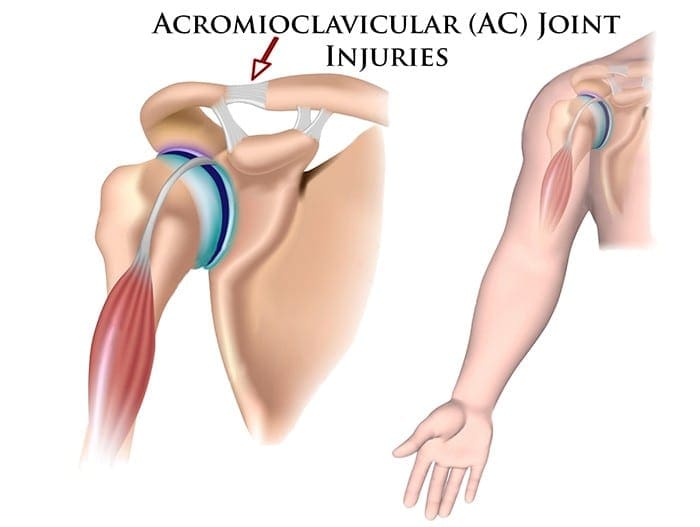
Two surgeons discuss the diagnosis and treatment of acromioclavicular injuries in athletes. El Paso, TX. Chiropractor, Dr. Alexander Jimenez follows the discussion.
Acromioclavicular (AC) joint injuries most often occur in athletic young adults involved in collision sports, throwing sports, along with overhead activities like upper-extremity strength training. They account for 3% of all shoulder injuries and 40% of shoulder sports injuries. Athletes in their second and third decade of life are more often affected(1), and men are injured more commonly than women (5:1 to 10:1)(1,2).
Acromioclavicular dislocation was known as early as 400 BC by Hippocrates(3). He cautioned against mistaking it for glenohumeral (shoulder joint) dislocation and advocated treating with a compressive bandage in an attempt to hold the distal (outer) end of the clavicle in a diminished position. Almost 600 decades later Galen (129 AD) recognized his own acromioclavicular dislocation, which he sustained while wrestling(3). He left the tight bandage holding the clavicle down as it was too uneasy. In today’s era this injury is better known, but its treatment remains a source of fantastic controversy.
Anatomy
The acromioclavicular joint combines the collarbone to the shoulder blade and therefore links the arm to the axial skeleton. The articular surfaces are originally hyaline cartilage, which affects to fibrocartilage toward the end of adolescence. The average joint size is 9mm by 19mm(4). The acromioclavicular joint contains an intra-articular, fibrocartilaginous disc which may be complete or partial (meniscoid). This helps absorb forces in compression. There is marked variability in the plane of the joint.
Stabilizers
There is little inherent bony stability in the AC joint. Stability is provided by the dynamic stabilizers — namely, the anterior deltoid muscle arising from the clavicle and the trapezius muscle arising from the acromion.
Additionally, there are ligamentous stabilizers. The AC ligaments are divided into four — superior, inferior, anterior and posterior. The superior is most powerful and blends with muscles. The acromioclavicular ligaments contribute around two- thirds of the constraining force to superior and posterior displacement; however, with greater displacement the coracoclavicular ligaments contribute the major share of the resistance. The coracoclavicular ligament consists of the conoid and trapezoid. The conoid ligament is fan-shaped and resists forwards motion of the scapula, while the more powerful trapezoid ligament is level and resists backward movement. The coracoclavicular ligament helps bunch scapular and glenohumeral (shoulder joint) motion and the interspace averages 1.3 cm.
Mechanism Of Injury
The athlete who sustains an acromioclavicular injury commonly reports either one of two mechanisms of harm: direct or indirect.
Direct force: This is when the athlete falls onto the point of the shoulder, with the arm usually at the side and adducted. The force drives the acromion downwards and medially. Nielsen(5) found that 70 percent of acromioclavicular joint injuries are caused by an direct injury.
Indirect force: This is when the athlete falls onto an outstretched arm. The pressure is transmitted via the humeral head into the acromion, therefore the acromioclavicular ligament is disrupted and the coracoclavicular ligament is stretched.
On Examination
The athlete presents soon after the severe injury with his arm splinted to his side. The patient may state that the arm feels better using superiorly directed support on the arm. Most motions are limited secondary to pain near the top of the shoulder; the degree varies with the grade of sprain. The hallmark finding is localized swelling and tenderness over the acromioclavicular joint.
In dislocations, the outer part of the collarbone will appear superiorly displaced using a noticeable step deformity (in fact, it is the shoulder which sags beneath the clavicle). Occasionally, the deformity may only be apparent later, if first muscle spasm reduces acromioclavicular separation. Forced cross-body adduction (yanking the affected arm across the opposite shoulder) provokes discomfort. The clavicle can frequently be moved relative to the acromion.
Acromioclavicular Visualisation
The typical joint width measures 1-3mm. It’s regarded as abnormal if it is more than 7mm in men, and 6mm in women. Routine anteroposterior views of the shoulder reveal the glenohumeral jointnonetheless, that the acromioclavicular joint is over penetrated and so dark to interpret. Reduced exposure enhances visualization. The individual stands with both arms hanging unsupported, both acromioclavicular joints on one film. Weighted viewpoints (stress X-rays) are obtained with 10-15 lb weights not held but suspended from the individual’s wrists. They help differentiate type II-III injuries, but are of little clinical significance and therefore are no longer recommended in our practice.
Classification Of AC Separation
The importance of identifying the injury kind can’t be over emphasized because the treatment and prognosis hinge on an accurate diagnosis. The injuries are graded on the basis of that ligaments are injured and how badly they’re torn.
Allman (6) classified acromioclavicular sprains as grades I, II and III, representing respectively, no involvement, partial tearing, and total disruption of the coracoclavicular ligaments. More recently, Rockwood (1) has further classified the more severe injuries as standard III-VI.
The injuries are classified into six categories:
Type I This is the most common injury encountered. Only a mild force is needed to sustain such an injury. The acromioclavicular ligament is sprained with an intact coracoclavicular ligament. The acromioclavicular joint remains stable and symptoms resolve in seven to 10 days. This injury has an excellent prognosis.
Type II The coracoclavicular ligaments are sprained; however, the acromioclavicular ligaments are ruptured. Most players can return to their sport within three weeks. There is anecdotal evidence to suggest that steroid injections into the acromioclavicular joint speed up the resolution of symptoms, but this practice is not universal.
Type III The acromioclavicular joint capsule and coracoclavicular ligaments are completely disrupted. The coracoclavicular interspace is 25-100% greater than the normal shoulder.
Type IV This is a type III injury with avulsion of the coracoclavicular ligament from the clavicle, with the distal clavicle displaced posteriorly into or through the trapezius.
Type V This is type III but with exaggeration of the vertical displacement of the clavicle from the scapula-coracoclavicular interspace 100-300% greater than the normal side, with the clavicle in a subcutaneous position.
Type VI This is a rare injury. This is type III with inferior dislocation of the lateral end of the clavicle below the coracoid
Treatment
The treatment of acromioclavicular joint injuries varies based on the seriousness or grade of the injury.
Initial treatment: These can be quite painful injuries. Ice packs, anti-inflammatories plus a sling are utilized to immobilize the shoulder and then take the weight of the arm. As pain starts to subside, it is important to start moving the fingers, wrist and elbow to prevent shoulder stiffness. Next, it’s important to begin shoulder motion in order to stop shoulder stiffness.
Un-displaced injuries only require rest, ice, and then a slow return to activity over two to six weeks. Major dislocations require surgical stabilization in athletes if their dominant arm is involved, and if they participate in upper-limb sports
Type I & II: Ice pack, anti-inflammatory agents and a sling are used. Early motion based on symptoms is introduced. Pain usually subsides in about 10 days. Range-of-motion exercises and strength training to restore normal motion and strength are instituted as the patient�s symptoms permit. Some symptoms may be relieved by taping (taking stress off acromioclavicular joint). The length of time needed to regain full motion and function depends upon the severity or grade of the injury. The sport and the position played determine when a player can return to a sporting activity. A football player, who does not have to elevate his arm, can return sooner than a tennis or rugby player. When a patient returns to practice and competition in collision sports, protection of the acromioclavicular joint with special padding is important. A simple �doughnut� cut from foam or felt padding can provide effective protection. Special shoulder- injury pads, or off-the-shelf shoulder orthoses, can be used to protect the acromioclavicular joint after injury.
Some Type II injuries may develop late degenerative joint changes and will need a resection of the distal end of the clavicle for pain relief. It is important to note that after a resection of the distal end of the clavicle, particularly in a throwing athlete, there may be formation of heterotopic bone on the under surface of the clavicle which can cause a painful syndrome which presents like shoulder impingement.
Type III: The treatment of type III injury is less controversial than in past years. In the 1970s, most orthopaedic surgeons recommended surgery for type III acromioclavicular sprains(7). By 1991, most type III injuries were treated conservatively(8). This change in treatment philosophy was prompted by a series of retrospective studies(9). These showed no outcome differences between operative and nonoperative groups.
What’s more, the patients treated non-operatively returned to full activity (work or athletics) earlier than surgically treated groups(10, 11). The exceptions to this recommendation include people who perform repetitive, heavy lifting, people who operate with their arms above 90 degrees, and thin patients who have prominent lateral ends of the clavicles. These patients may benefit from surgical repair(12).
Any discussion about the management of acute injuries to the AC joint must deal with which of the many methods of surgical therapy described is the best for their situation, but whether surgery should be considered at all. Surgery is generally avoided in athletes participating in contact sports since they will often re-injure the shoulder later on.
Type IV-VI: Account for more than 10-15% of total acromioclavicular dislocations and should be managed surgically. Failure to reduce and fix these will lead to chronic pain and dysfunction.
Surgery
Surgical repair can be divided into anatomical or non- anatomical, or historically into four types:
? Acromioclavicular repairs (intra-articular repair with wires/pins, percutaneous pins, hook plates).
? Coracoclavicular repairs (Bosworth screws(13), cerclage, Copeland and Kessel repair).
? Distal clavicular excision.
? Dynamic muscle transfers.
? Disadvantages of surgery are that there are risks of infection, a longer time to return to full function and continued pain in some cases.
For the individual with a chronic AC joint dislocation or subluxation that remains painful after three to six months of closed treatment and rehabilitation, surgery is indicated to improve functioning and comfort.
For sequelae of untreated type IV-VI, or painful type II and III injuries, the Weaver Dunn technique is advocated. This�entails removing the lateral 2cm of the clavicle and reattaching the acromial end of the coracoacromial ligament to the cut end of the clavicle, thus reducing the clavicle to a more anatomical position.
Postoperatively, the arm is supported in a sling for up to six weeks. Following the first two weeks, the patient is permitted to use the arm for daily activities at waist level. After six weeks, the sling or orthosis is discontinued, overhead actions are allowed, formal passive stretching is instituted, and light stretching using elastic straps is initiated. Stretching and strengthening are begun slowly and gradually. The athlete shouldn’t return to their sport without restriction until full strength and range of motion has been recovered. This usually occurs four to six months following operation.
Conclusion
AC joint injuries are an important source of pain at the shoulder area and have to be assessed carefully. The management of these injuries is nonoperative in the majority of cases. Type I and II injuries are treated symptomatically. The present trend in uncomplicated type III injuries are a non operative strategy. In the event the athlete develops following problems, a delayed reconstruction might be undertaken. In athletes involved in heavy lifting or prolonged overhead activities, surgery may be considered acutely. Type IV-VI injuries are generally treated operatively.
No matter what kind of treatment is chosen, the ultimate purpose is to restore painless function to the wounded AC joint so as to reunite the athlete safely and as quickly as possible back to their sport. It is possible in the vast majority of acromioclavicular joint injuries.
References
Reza Jenabzadeh and Fares Haddad
1. Rockwood CA Jr, Williams GR, Young CD. Injuries of the Acromioclavicular Joint. In CA Rockwood Jr, et al (eds), Fractures in Adults. Philadelphia: Lippincott-Raven, 1996; 1341-1431.
2. Dias JJ, Greg PJ. Acromioclavicular Joint Injuries in Sport: Recommendations for Treatment. Sports Medicine 1991; 11: 125-32.
3. Adams FL. The Genuine Works of Hippocrates (Vols 1,2). New York, William Wood 1886.
4. Bosworth BM. Complete Acromioclavicular Dislocation. N Eng J Med 2 41: 221-225,1949.
5. Nielsen WB. Injury to the Acromioclavicular Joint. J Bone Joint Surg 1963; 45B:434-9.
6. Allman FL Jr. Fractures and Ligamentous Injuries of the Clavicle and its Articulation. J Bone Joint Surg Am 1967;
49:774- 784.
7. Powers JA, Bach PJ: Acromioclavicular Separations: Closed or Open Treatment? Clin Orthop 1974; 104 (Oct): 213-223
8. Cox JS: Current Methods of Treatment of Acromioclavicular Joint Dislocations. Orthopaedics 1992; 15(9): 1041-1044
9. Clarke HD, Mc Cann PD: Acromioclavicular Joint Injuries. Orthop Clin North Am 2000; 31(2): 177-187
10. Press J, Zuckerman JD, Gallagher M, et al: Treatment of Grade III Acromioclavicular Separations: Operative versus
Nonoperative Management. Bull Hosp Jt Dis 1997;56(2):77-83
11. Galpin RD, Hawkins RJ, Grainger RW: A Comparative Analysis of Operative versus Nonoperative Treatment of Grade III Acromioclavicular Separations. Clin Orthop 1985; 193 (Mar): 150-155
12. Larsen E, Bjerg-Nielsen A, Christensen P: Conservative or Surgical Treatment of AC Dislocation: A Prospective, Controlled, Randomized Study. J Bone Joint Surg Am 1986;68(4):552-555
13. Bosworth BM. Complete Acromioclavicular Dislocation. N Engl. J. Med. 241: 221-225,1949.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Athletes, Complex Injuries, PUSH-as-Rx
For many athletes following any major endurance event they will return to their houses, to recover, celebrate, reflect and rebuild to their next career step. Some, like the athlete in this case study will need to now focus attention on delayed decisions concerning whether to go under the knife to sort out a chronic injury.�El Paso, TX’s Injury scientist, Dr. Alexander Jimenez takes a look at the study.
My client has been competing in triathlon for 10 or more years, although his career has included a range of serious injuries which have kept him from races for months on end. In the previous two to three decades, however, he’s enjoyed a sustained period of injury-free training and racing, and has climbed to the peak of the world rankings. But the emergence of hip pain has seen him once more return to the physio’s table.
The triathlete’s accident history highlights a common pattern among sportspeople: 2 tibial stress fractures, a femoral neck stress fracture and a serious ankle sprain — every one of these on his right side. The significant contributing element to the bone stress injuries is a 1.5cm leg-length gap (his right leg is shorter).
He’d first experienced comparable hip pain in 2004; it kept him from running for three months. At that time, nothing was detected on a bone scan or MRI, or so the pain went paralyzed. An intra-articular cortisone injection (CSI) elicited no improvement. The athlete remembers that he chose to train on his painful hip, never allowing the symptoms to settle. The nearest he ever came into an investigation was a hypothesis that he could have a little, undetected, labral lesion.
The present episode of hip pain began initially at night after a hard three-hour bicycle ride. Earlier this, however, he hadn’t cycled for five times. He described his initial symptom as a profound hip tightness (lateral and lateral), together with slight pain in his groin. He was able to continue to train however, was feeling that the hip tightness and pain following both cycling and running (swimming was symptom-free).
A week later his symptoms dramatically worsened when he flew from Australia to Singapore, on his way to a French high- altitude camp. As he got off the airplane, he felt deep hip pain as well as the tightness. As elite athletes tend to do, he coached anyway, running a tricky track session, which made the hip much worse: he was unable to ride or run without pain. He instantly started a course of anti- inflammatories.
I met him in Singapore and evaluated him in the airport, initially ruling out any prospect of a disease or systemic matter. He explained he had been feeling an ache during the night, lying in bed; on waking, the hip would be OK, but got worse the longer he walked.
On assessment, he had the following physical signs:
� walking with obvious limp
� pain on hopping (6/10)
�painful right hip quadrant/impingement test (full hip flexion/adduction)
� reduced right hip flexion (-10 degrees compared to left)
� reduced right hip internal rotation (-10 degrees compared to left)
� increased tone on palpation of TFL, adductors, hip flexors, gluteal, piriformis and deep rotators
� lumbar spine and SIJ were OK
� femoral shaft bone stress test was OK � leg length discrepancy (right side 1.5cm shorter)
� right innominate (pelvis) anteriorly rotated
� weakness in right hip abductors/extensors
� reduced calf endurance on right side (-5 reps)
� ankle dorsiflexion range of movement was OK
� reduced proprioception on right (single leg stance, eyes closed).
I thought the differential diagnoses were:
� femoral neck stress fracture
� labral tear, possibly with hip synovitis
� FAI (femoro-acetabular impingement), possibly with hip synovitis.
I initially treated the triathlete with soft- tissue techniques to reduce the tone around the hip joint. Trigger-point releases were performed on his TFL, adductors, gluteals, piriformis, deep rotators and iliopsoas.�This reduced his jump pain into 3/10. Manual long-leg grip further decreased the strain on hopping (2/10). He still had pain and stiffness on walking but it sensed “simpler. As he prepared to embark on his long run flight to Europe, I counseled him to not sit for too long and maintain his stylish as straight as possible to decrease any potential impingement from hip flexion.
Luckily, the hip didn’t get worse throughout the flight. On arrival at the French high-altitude training centre, we initiated a strategy of two swims and two intensive treatments a day, aiming at reducing muscle tone, restoring his range of hip movement and normal muscle control and stamina. We had been expecting that the problem was not a stress fracture, but just minor hip synovitis that could settle quickly. Following a week of conservative treatment, though, we were just able to keep his hop pain in 2/10, and that he still could not run 20 meters without any pain and limping.
In collaboration with medics, we flew to London to see a sports doctor and get MRI scans. The scans revealed no bone stress reaction, fracture or labral ripping — which was a big relief; however, it did show signs consistent with FAI (femoro-acetabular impingement). He had hip synovitis with a rectal lesion on his femur.
Hip injuries aren’t much reported among triathletes — in fact they are notably absent from reports on Olympic and Ironman triathlons, which mention knee, back, H/ Achilles, lower leg, ankle and shoulder as the most common accidents (1-3).
In this state, when the hip is in maximum flexion and internal rotation, the labrum and cartilage abut and impinge; damage to the articular cartilage and acetabular labrum results from this pathologic bony contact. The contact generally results in a structural abnormality of the femur (“camera impingement”) along with the acetabulum (“pincer impingement”) or a combination of both (“mixed impingement”). Over time, via repetitive micro-trauma, the aggravating motion hurts the hip cartilage or labrum (or both) during normal joint motion. This happens along the anterior femoral neck and the anterior–superior acetabular rim. FAI is a possible trigger of early hip joint degeneration (4).
Arthroscopic surgery is the direction of choice for FAI if symptoms do not settle; however as his next Competition was only three and a half a year off, surgery was not an option. Instead, over a five-day interval, the athlete had two cortisone (CSI) and local anesthetic injections into the hip joint (under ultrasound guidance) to settle the indicators.
Our aim was to grow the hip range of motion and extend the capsule to reduce any additional impingement, slowly returning to regular training. Following the competition, the athlete would then should see a hip arthroscopic surgeon to acquire a surgical opinion to the best option for long-term direction.

Injection Relief
After both shots my customer felt sore for five days. The initial CSI settled his pain on hopping to 1/10 and after seven days he managed to operate without symptoms. But minor hip stiffness and aching at the end of the day prevented him from progressing to optimal training, so that he then underwent a second steroid injection. This settled the hop pain into 0/10 and decreased the aching; so after five times he returned to mild cycling and after seven days he started running again, also.
The athlete admitted that, following the first shot, he had done more and gone tougher in training than directed, as he had felt “good. This mistake of “too much too soon — all too common in elite athletes — had led to excessive inflammation and aching in the hip nightly after training. After the next injection he returned to normal intensity slower and more gradually.
My client built his training up to regular levels by four months following the final injection (swimming five times per week, cycling four days and running six to seven days). He began with very easy cycling on a wind trainer for 30 minutes, building slowly to 90 minutes before cycling on the street. He cycled two days on and one day away and avoided hills to the first two weeks. He started jogging on the apartment for 15 minutes and slowly built up to 90 minutes after three weeks. He did not run hills or about the track; and as he ran only on every single day, he would diligently concentrate on technique.
From week six to week 11, my client remained on anti inflammatory medication and underwent two treatments a day.
The hands-on treatment continued to:
� increase hip range of movement
� stretch the hip capsule
� normalise pelvic symmetry and hip muscle tone
� improve muscle control and strength � improve proprioception
� ensure optimal biomechanics via video assessment (cycling and running).
Eleven weeks after he first felt his hip pain, the triathlete returned to racing; however he failed to finish the first race, partially because of minor hip stiffness but mainly due to “fitness. Fortunately there were not any prolonged symptoms after the race and a week after he successfully returned to competition, coming second in a really strong field. His very minor ongoing symptoms were handled with anti-inflammatory drugs and hands-on treatments.
If this athlete wants to pursue a long- term triathlon career up to the London Olympics, then he will now require surgery. The arthroscopic surgical technique initially assesses the cartilage and labral surfaces, debrides any abnormalities of the hip joint cartilage and hip labrum, removes the non-spherical segments of the femoral head�and any prominent sections of the anterior femoral neck and bony growths on the acetabular rim that may continue to contribute to hip joint impingement.�The alternative is early joint degeneration and onset of osteoarthritis.
References:
1. Wilk B et al: �The incidence of musculoskeletal injuries in an amateur triathlete racing club�. J Orthop Sports Phys
Ther 1995 Sep;22(3):108-12.
2. Collins K et al: �Overuse injuries in triathletes. A study of the 1986 Seafair Triathlon�. Am J Sports Med 1989 SepOct;17(5):675-80.
3. Korkia PK et al: �An epidemiological investigation of training and injury patterns in British triathletes�. Br J Sports Med 1994 Sep;28(3):191-6.
4. Ganz R. et al (2003): �Femoroacetabular impingement: a cause for osteoarthritis of the hip�. Clin Orthop Relat Res. 417:112�120. For more information see: www.hipfai.com
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Athletes, Chiropractic Examination, Complex Injuries, PUSH-as-Rx
Most of us will experience it at some point — but how does it influence on athletic performance? Chiropractic injury specialist, Dr. Alexander Jimenez investigates.
Research postulates that 80 percent of the populace will undergo an acute onset of back pain at least once in their lifetimes. This adds a considerable financial burden not just on the medical system (physician consultations, prescribed drugs, physiotherapy) but also the financing of the workforce in lost employee hours and loss in productivity.
The types of lower back pain that an individual may experience include (but are not limited to):
1. Lumbar spine disc herniation with/ without sciatica
2. Lumbar spine disc bulges
3. Lumbar spine disc degeneration
4. Lumbar spine disc annular tears
5. Ligament sprains
6. Muscle strains, particularly quadrutus lumborum
7. Osteoarthritis
8. Inflammatory arthritis such as rheumatoid and anklyosing spondylitis
9. Facet joint sprains
10. Bone injuries such as stress fractures, pars defects and spondylolisthesis.
The focus for this paper will be on the previous group — that the bone injuries. This may be simply postural (slow onset repetitive trauma) or related to sports; for instance, gymnastics.
The two demographic groups that tend to endure the most extension-related low back pain are:
1. People who endure all day, for instance, retailers, army, security guards etc.. Prolonged position will obviously force the pelvis to start to migrate to an anterior tilt management. This may begin to place compressive pressure on the facet joints of the spinal column as they also change towards an expansion position since they accompany the pelvic tilt.
2. Extension sports such as gymnastics, tennis, swimming, diving, football codes, volleyball, basketball, track and field, cricket fast bowlers. This is more pronounced in sports that involve extension/rotation.
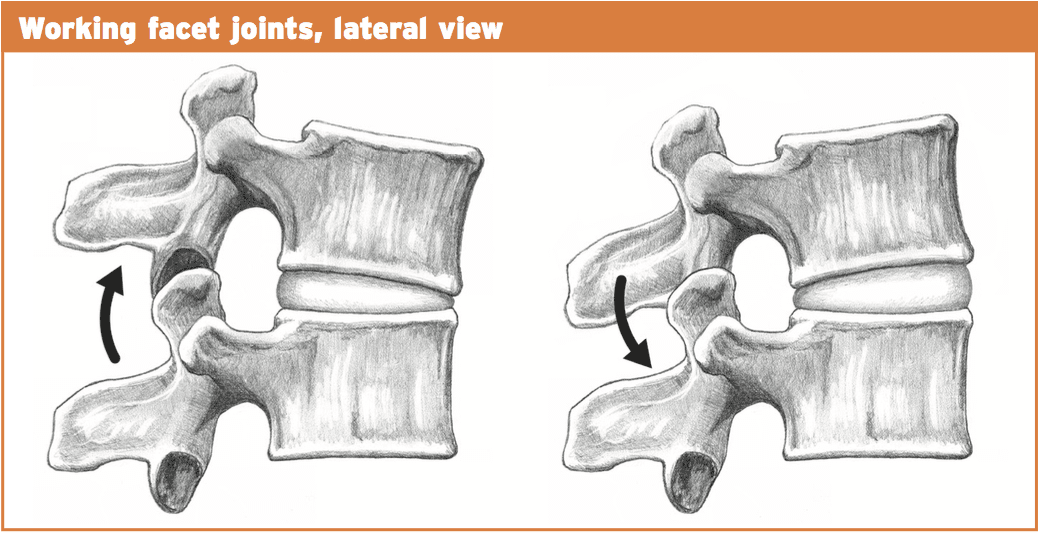
Pathomechanics
With normal extension of the lumbar spine (or backward bending), the facet joints begin to approximate each other and compress.�The articular processes of this facet above will abut the articular process of the facet below. This is a normal biomechanical movement. However, if the extension ranges are excessive, the procedures will impinge quite aggressively and damage to the cartilage surfaces within the facet joint can result. Sports such as gymnastics, functioning in tennis, and handling in American Soccer may all involve uncontrolled and excessive extension.
It would be unlikely that a bone stress response or even a stress fracture could be brought on by an isolated expansion injury. It would be more likely that a sudden forced extension injury may damage an already pre-existing bone strain reaction.
Similarly, if an individual stands daily and the pelvis migrates into lateral tilt, then the aspects will be placed under low load compression but for extensive intervals.
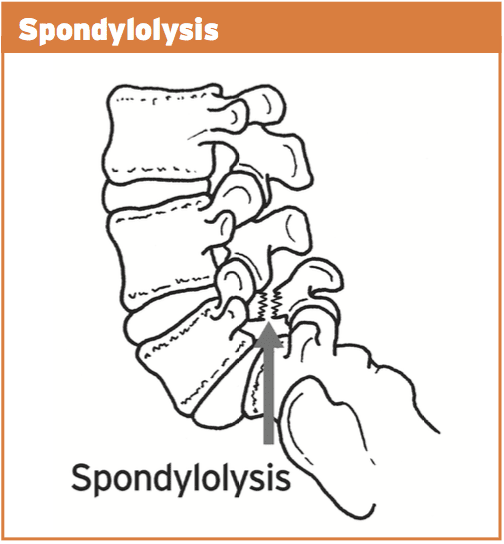
With ongoing uncontrolled loading, stress is then transferred from the facet joint to the bone below (pars interarticularis). This originally will manifest as a pressure reaction on the bone. This bone strain may advance to a stress fracture throughout the pars if uncorrected. This fracture is also referred to as a “pars flaw”, or spondylolysis.
It was initially considered that stress fractures of the pars was a congenital defect that introduced itself at the teenage years. However, it is now agreed that it is probably obtained through years of overuse into extension positions, especially in young sportspeople involved with expansion sports. What’s more, one-sided pars defects often occur more commonly in sport which also included a rotational component such as tennis serving or fast bowling in cricket.
The stress fracture can then advance to impact the opposite side, causing a bilateral strain fracture, with anxiety subsequently being transferred to the disk in between both levels.
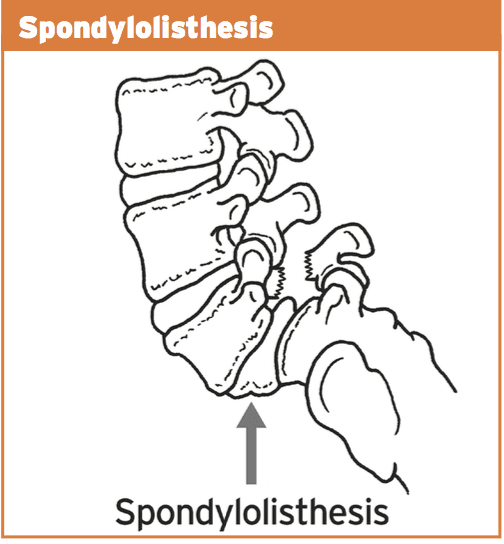
Spondylolisthesis features bilateral pars defects which could possibly be a result of repetitive stress into the bilateral pars in extension athletics, but more likely it is an independent pathology that manifests in the early growing stages (9-14) as this pathology is often viewed in this age category. If they become symptomatic in later years because of involvement in expansion sports, it is exceedingly likely that the defects were there by a young age but presented asymptomatically. As a result of rapid growth spurts in teenage years and the high-volume training experienced by teenaged athletes, it is possible that these dormant spondylolisthesis then pose as ‘acute onset’ back pain in teenage years.
In summary, the progression of this bone stress reactions tends to follow the following continuum:
1. Facet joint irritation
2. Pars interarticularis stress response
3. Stress fracture to the pars
4. Pars defect (or spondylolysis)
5. Spondylolisthesis due to activity or more likely congenital and found later in teenage years due to participation in�extension sports.
The landmark publication related to spondylolysis and spondylolisthesis was presented by Wiltse et al (1976) and they classified these injuries as follows:
1. Type I: dysplastic � congenital abnormalities of L5 or the upper sacrum allow anterior displacement of L5 on the sacrum.
2. Type II: isthmic � a lesion in the pars interarticularis occurs. This is subclassified as
a. lytic, representing a fatigue fracture of the pars,
b. elongated but intact pars, and c. acute fracture.
3. Type III: degenerative � secondary to long-standing intersegmental instability with associated remodeling of the articular processes.
4. Type IV: traumatic � acute fractures in vertebral arch other than the pars.
5. Type V: pathological � due to generalized or focal bone disease affecting the vertebral arch.
The vast majority of spondylolysis and sponylolisthesis accidents are Type II — the isthmic variety.
For the purposes of this paper, we will refer to the above stages as the posterior arch bone stress injuries (PABSI).
Epidemiology
It is a lot more widespread at the L5 level (85-90 percent). It’s a high asymptomatic prevalence in the general population and is often found unintentionally on x ray imaging. Nonetheless, in athletes, particularly young athletes, it is a common reason for persistent low back pain. From the young athlete, the problem is often referred to as ‘active spondylolysis’.
Active spondylolysis is normal in virtually every gamenevertheless, sports such as gymnastics and diving and cricket pose a much greater danger due to the extension and turning character of the sport. The progression from an active spondylolysis into a non-union type spondylolisthesis has been associated with a greater prevalence of spinal disk degeneration.
Early detection through screening and imaging, therefore, will highlight those early at the bone stress phase and if caught early enough and managed, the progression to the larger and more complicated pathologies are avoided as a result of therapeutic capacity of the pars interarticularis in the early stages.
It is more common to find teens and young adults afflicted by PABSI. This will highlight the rapid growth of the spine through growth spurts that is also characterized by a delay in the motor control of the muscle system during this period. Furthermore, it’s thought that the neural arch actually gets stronger in the fourth decade hence possibly explaining the low incidence of bone stress reactions in mid ages.
The incidence of spondylolysis has been reported to be around 4-6% in the Caucasian population (Friedrikson et al 1984). The rates seem to be lower in females and also in African-American males. It has also been suggested that a link exists between pars defects and spina bifida occulta.
The incidence of spondylolysis seems to be higher in the young athletic population than in the general population. Studies in gymnasts, tennis, weightlifting, divers and wrestlers all show disproportionately high incidence of spondylolysis compared with the general population of age-matched subjects.
Tennis
The tennis serve generates excessive extension and rotation force. In addition, the forehand shot may also produce elevated levels of spinning/ extension. The more traditional forehand shot demanded a great deal of weight shift through the legs to the torso and arms. However, a more favorite forehand shot is to currently face the ball and also generate the force of this shot utilizing hip rotation and lumbar spine extension. This action does increase ball speed but also puts more extension and compressive loads on the spine potentially resulting in a greater degree of stress on the bone components.
Golf
The most likely skill component involved in golf that may cause a PABSI are the tee shot with a 1 wood when forcing for distance. The follow-through of this shot entails a significant quantity of spine rotation with maybe a level of spine expansion.
Cricket
Fast bowlers in cricket are the most susceptible to PABSI. This will occur on the opposite side to the bowling arm. As the front foot engages on plant stage, the pelvis abruptly stops moving but the spine and chest continue to proceed. With the wind-up of this bowling action (rotation), when coupled with expansion this can place large forces on the anterior arch of the thoracic. More than 50% of fast bowlers will create a pars stress fracture. Young players (up to 25) are most vulnerable. Cricket governments have implemented training and competition guidelines to avoid such injuries by restricting the number of meals in training/games.
Field Events
The more common field events to cause a PABSI would be high leap followed by javelin. Both these sports create enormous ranges of backbone extension and under significant load.
Contact Sports
Sports like NFL, rugby and AFL all require skill components that need backbone expansion under load.
Gymnastics/Dancers
It goes without saying that gymnastics and dancing involves a substantial amount of repetitive spine expansion, particularly backflips and arabesques. It has been suggested that nearly all Olympic degree gymnasts could have suffered from a pars defect. Many organizing bodies now put limits on the number of hours young gymnasts can instruct to prevent the repetitive loading on the spine.
Diving
Spine extension injuries occur mostly off the spring board and on water entrance.
Diagnosis Of PABSI In Athletes
Clinical investigation
These can pose as preventable injuries. Research shows that the incidence was emphasized from the general population that have nil indicators of back pain. But, individuals will typically complain of back ache that is deep and generally unilateral (one side). This may radiate into the buttock area. The most offending movements tend to be described as expansion moves or backward bending movements. This may be a slow progression of pain or might be initiated by one acute episode of back pain in a competitive extension motion.
On clinical examination:
1. Pain may be elicited with a one-leg extension/rotation test (standing on the leg on the affected side) � stork test.
2. Tenderness over the site of the fracture.
3. Postural faults such as excessive anterior tilt and/or pelvic asymmetry.
The one-legged hyperextension test (stork test) was suggested to be pathognomonic for busy spondylolysis. A negative evaluation was stated to effectively exclude the diagnosis of a bone stress-type injury, thus creating radiological investigations unnecessary.
But, Masci et al (2006) examined the connection between the one-legged hyperextension test and gold standard bone scintigraphy and MRI. They discovered that the one-legged hyperextension test was neither sensitive nor specific for active spondylolysis. Moreover, its negative predictive value was so poor. Thus, a negative test can’t exclude energetic spondylolysis as a possible cause.
Masci et al (2006) go on to indicate that the bad relationship between imaging and the one-legged test may be because of a number of factors. The extension test would be expected to move a significant extension force on to the lower back spine. In addition to putting substantial strain on the pars interarticularis, it might also stress different regions of the spinal column like facet joints as well as posterior lumbar disks, and this may subsequently induce pain in the existence of other pathology such as facet joint arthropathy and spinal disc disease. This will explain the poor specificity of the test. Conversely, the inadequate sensitivity of the test may be related to the subjective reporting of pain by issues performing the maneuvre, which may vary based on individual pain tolerance. Additionally, this evaluation can preferentially load the fifth cervical vertebra, and so bone stress located in the upper lumbar spine may not test positive.
Grade 1 spondylolisthesis are normally asymptomatic; nonetheless, grade 2+ lesions often present with leg pain, either with or without leg pain. On examination, a palpable slip could be evident.
Imaging
Clinical assessment of active spondylolysis and the more severe pars defects and spondylolisthesis can be notoriously non-specific; this is, not all patients suffering PABSI will present with favorable abstract features or positive signs on analyzing. Thus, radiological visualization is important for diagnosis. The imaging methods available in the diagnosis of bone stress injury are:
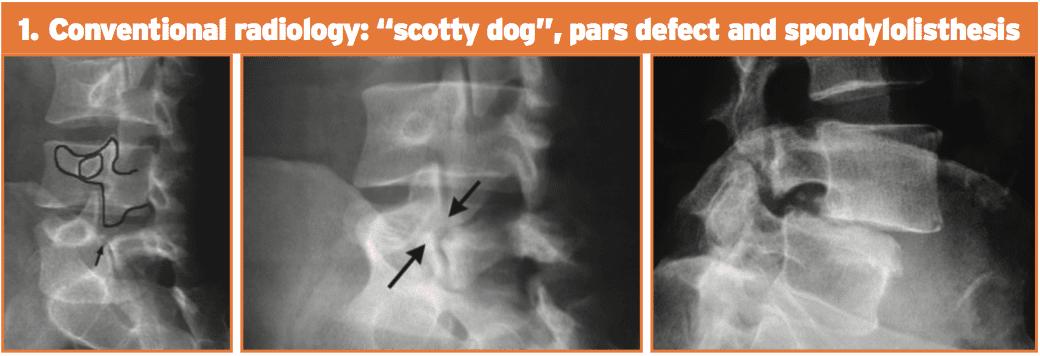
1. Conventional radiology. This test is not very sensitive but is highly unique. Its limits are partially because of the cognitive orientation of the pars defect. The oblique 45-degree films may show the timeless ‘Scotty Dog’ appearance. Spondylolisthesis can be looked at simply on a lateral movie x-ray.
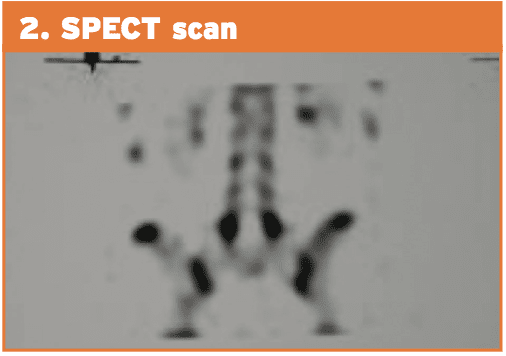
2. Planar bone scintigraphy (PBS) and single photon emission computed tomography (SPECT). SPECT enhances sensitivity in addition to specificity of PBS than straightforward radiographic study. Comparative research between PBS and conventional radiology have shown that scintigraphy is more sensitive. Patients with positive SPECT scan must then undergo a reverse gantry CT scan to assess whether the lesion is active or old.
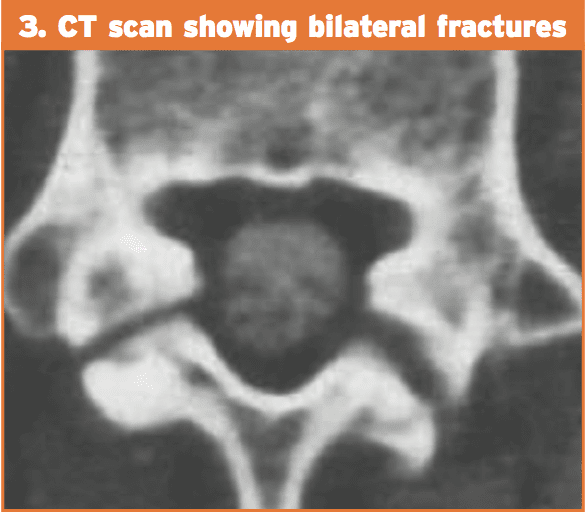
3. Computed tomography (CT). The CT scan is considered to be more sensitive than conventional radiology and with higher specificity than SPECT. Regardless of the type of cross-sectional image utilized, the CT scan provides information on the state of the flaw (intense fracture, unconsolidated flaw with geodes and sclerosis, pars in procedure for consolidation or repair). The “inverse gantry” perspective can evaluate this condition better. Repeat CT scan can be used to track progress and recovery of the pars defect.
4. Magnetic resonance imaging (MRI). This technique shows pronounced changes in the signal in the amount of the pars. This is recognized as “stress response” and can be classified into five different degrees of action. MRI can be helpful for evaluating elements that stabilize isthmic lesions, for example intervertebral disc, common anterior ligament, and related lesions. The MRI isn’t as specific or sensitive as SPECT and CT combination.
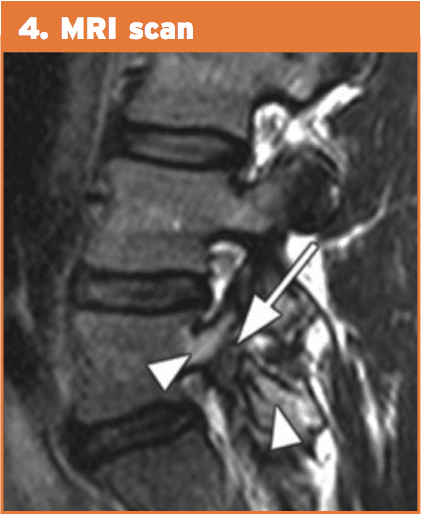
Therefore, the current gold standards of investigation for athletes with low back pain are:
1. bone scintigraphy with single photon emission computed tomography (SPECT); if positive then
2. limited reverse-gantry axial computed tomography .
MRI has many advantages over bone scintigraphy, for instance, noninvasive nature of the imaging along with the absence of ionizing radiation. MRI changes in active spondylolysis include bone marrow edema, visualized as increased signal in the pars interarticularis on edema-sensitive sequences, and fracture, visualized as reduced signal in the pars interarticularis on T1 and T2 weighted sequences.
However, there is greater difficulty in detecting the changes of busy spondylolysis from MRI. Detecting pathology from MRI relies on the interpretation of distinct contrasts of signals compared with normal tissue. Unlike stress fractures in different parts of the body, the little region of the pars interarticularis may make detection of those changes harder.
However, unlike MRI, computed tomography has the capability to differentiate between acute and chronic fractures, and this differentiation might be an important determinant of fracture healing. Accordingly, in areas using pars interarticularis fractures discovered by MRI, it might nonetheless be necessary to execute thin computed tomography slices to determine whether or not a fracture is severe or chronic — an important factor in fracture resolution.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | UTEP (Local) RSS
NORTHBROOK, Ill. – Allstate Insurance Company and the American Football Coaches Association (AFCA) announced on Monday that UTEP quarterback Ryan Metz one of 146 nominees for the 2017 Allstate AFCA Good Work Team, a prestigious off-the-field honor in college football.
“Allstate is immensely honored to partner with the AFCA for the 10th year to help pay tribute to these players and their off-the-field ‘good works’ that often go unnoticed and unrewarded,” said Thomas Clarkson, president of the west territory for Allstate Insurance Company and a member of the 2017 Allstate AFCA Good Works Team voting panel. “The individuals nominated to the 2017 Good Works Team are making a positive impact and uniting communities across the country through service, showing what’s possible when you put all hands in and give back.”
The El Paso native is known for his on-field achievements and has also made an impact off the field. The junior completed 25 hours of community service hours last season, while the signal caller is known for volunteering his time to children in the community. Metz volunteered over 15 hours at children’s camps, where he assisted with football drills and activities for the future gridiron greats.
Metz was also a member of Project MOVE, where he played with children in the community in various activities like kickball, football and soccer. Metz is active in assisting with the football team’s weekly dinner with the Child Crisis Center. Metz, along with his teammates, spend time with the children in the Crisis Center, playing, working on homework and eating dinner together.
The student-athletes nominated for this esteemed award embody the true spirit of teamwork and selflessness, donating their limited free time to helping and serving others. From founding a non-profit that helps orphans secure jobs in the workforce to raising funds and awareness for childhood cancer research, the 2017 Allstate AFCA Good Works Team® nominees may wear different jerseys on the field, but they all exemplify a superior commitment to giving back off of it.
Comprised of 11 players from the NCAA Football Bowl Subdivision and 11 players from the NCAA Football Championship Subdivision, Divisions II, III and the NAIA, the final roster of 22 award recipients will be unveiled in September. From the nominees submitted by sports information directors across the nation on behalf of their schools, a special voting panel consisting of former Allstate AFCA Good Works Team members and prominent college football media members will select the 2017 Good Works Team.
Two-time national champion, Heisman Trophy winner and 2009 Allstate AFCA Good Works Team member Tim Tebow will headline the Allstate AFCA Good Works Team voting panel.
Once the final team members are announced in September, college football fans are encouraged to visit the Allstate AFCA Good Works Team website on ESPN.com, featuring profiles and images of the players, for the opportunity to vote for the 2017 Allstate AFCA Good Works Team Captain. Throughout the season, fans can also follow along and join in on the conversation by searching and using #GoodWorksTeam on their social media channels.
In order to meet the criteria, set forth by Allstate and the AFCA, each player must be actively involved with a charitable organization or service group while maintaining a strong academic standing.
Metz has also excelled in the classroom, as he’s a three-time Conference USA Commissioner’s Honor Roll recipient with a 3.34 GPA in Mathematics. Metz completed 64.7 percent of his passes, ranked third in C-USA in 2016, while it’s the program’s second-best single-season performance. His 14 passing scores were the most for a UTEP quarterback since 2010.
Recently, Metz was one of 45 national collegiate quarterbacks, and the first UTEP quarterback, to be invited to the 2017 Manning Passing Academy supervised by the Manning Family (Archie, Cooper, Peyton and Eli). The camp was a four-day event that started on June 22 at Nicholls State University in which over 125 prep, college and professional coaches, counselors and staff members were involved.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | UTEP (Local) RSS
UTEP softball head coach Tobin Echo-Hawk announced the addition of pitcher Kira McKechnie on Wednesday. McKechnie played her first two years at Fresno State and will have two years of eligibility with the Miners.
McKechnie will join fellow transfer pitcher Julia Wright, and UTEP sophomore hurlers Devyn Cretz and Allie Johnson for the 2018 season.
“We are excited to have Kira on our roster for the upcoming season,” Echo-Hawk said. “It is always nice to add some depth to your pitching staff.”
McKechnie, a native of Sacramento, Calif., made a relief appearance in the circle during the 2017 campaign against San Diego and recorded a strikeout. In 2016, McKechnie made a pair of appearances in the circle, throwing 1.1 innings, while allowing two hits and no runs.
McKechnie attended Christian Brothers High School and was a dual-sport athlete. She was a four-year letterwinner in both softball and basketball. McKechnie was voted softball team captain in 2015 and capped her senior year with multiple accolades, which includes Sacramento Bee’s 2015 All-Metro first team, Cal-Hi first team All-State, CAL All-Optimist All-Star team, MaxPreps first team All-State and Cal-Hi D3 Athlete of Honor.
She was named Female Athlete of the Year by Character Combine, Bee Preps Show and MaxPreps Christian Brothers, while earning the Credit Union Athlete of the Week in 2015.
During her senior season, McKechnie hit .462 with 40 RBI, 11 doubles, a triple and eight home runs. She added 18 runs and was walked nine times. In the circle, McKechnie (12-7) fashioned a 1.95 ERA and recorded 195 Ks 140 innings (23 starts/25 appearances).
McKechnie has competed for the California Breeze (2005-09), Capital City Comets (2009-12), Nor Cal Patriots (2012-14) and Central Cal Dirt Dogs (2014-15). She also attended the 2012 OnDeck Elite Futures Camp and 2013 Colorado Sparkler All-Star/All-American game.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | UTEP (Local) RSS
UTEP’s freshman Emmanuel Korir had a phenomenal year and was awarded the Conference USA Athlete of the Year, announced by the league office on Friday afternoon.
Opening up the 2016-17 season, Korir clocked a world record 600m at the New Mexico Cherry and Silver meet with at time of 1:14.97. It was his first time ever running on a 200m banked track. At the 2017 NCAA Indoor Championships, the freshman captured his first title in the 800m running a time of 1:47.48.
During the outdoor season the Kenyan native ran a school record time of 44.67 in the 400m at the UTEP Invitational. Seven days later Korir clocked 1:43.73 in the 800m at the Brutus Hamilton Challenge. He is just on of three athletes in the world to run sub-1:44 and sub-44 in the 800m and 400m respectively.
At the C-USA Outdoor Championships Korir claimed the 400m title (44.53) and set the meet record at the NCAA West Region Preliminaries in the 800m with a time of 1:45.88. The mid-distance runner won his second NCAA title in the 800m (1:45.03) at the historic Hayward Field in Eugene, Ore.
Korir was named the USTFCCCA (U.S. Track and Field and Cross Country Coaches Association) Athlete of the Week twice during the indoor season, garnered four C-USA Athlete of the Week awards and made The Bowerman Watch List three times during the season.
He joins a list of Miners who have been named C-USA Athlete of the Year:
Anthony Rotich (2012-13, 2013-14, 2014-15/ Track and Cross Country)
Camilla Carrera (2011-12/Softball)
Blessing Okagbare (2009-10/Track and Field)
For more information on UTEP track and field, follow the Miners on Twitter (@UTEPTrack) and on Instagram (uteptrack).






