Title: Conservative care and axial distraction therapy for the management of cervical and lumbar disc herniations and ligament laxity post motor vehicle collision.
Dr. Alex Jimenez, doctor of chiropractic, focuses on the diagnosis, treatment and prevention of a variety of injuries and conditions associated with the musculoskeletal and nervous systems, utilizing several chiropractic methods and techniques. The following procedures may be similar to his own but can differ according to the specific issue and complications by which the individual is diagnosed.
Abstract: This middle-aged female was injured in a vehicle collision causing her to sustain disc and additional ligament injuries in the cervical and lumbar spine. Diagnostic studies included physical examination, orthopedic and neurological testing, lumbar MRI, multiple cervical MRI�s, CRMA with motion cervical radiographs and EMG studies. Typically, conservative care is initiated prior to interventional procedures, and this case study seeks to explore the usage of passive therapy for mechanical spine pain and noted anatomic disc lesions after failure of interventional procedures. She reported both short term and long term success regarding pain reduction along with improvement in her activities of daily living after initiating conservative care, and continued to report further reductions in pain with periodic pain management using conservative care.
Introduction: The 49-year-old married female (Spanish speaking patient) reported that on March 4th, 2014 she was the seat-belted driver of a truck that was struck by a much larger fuel truck changing lines, hitting her vehicle at the front passenger side (far side, side impact). The force of the impact caused her truck to be lifted up and the right wheel popped off. Her head hit the window after impact and the spinal pain and complaints started approximately 24 hours later. Two days after the crash she went to the emergency department. Occupant pictures were taken describing an out of position occupant injury. She did not report any additional significant trauma after the collision.
Initial Diagnosis and Treatment for Disc Herniations
Prior to her evaluation at our clinic, she utilized multiple providers for diagnosis and treatment over the course of 11 months. She went to the emergency department, utilized 3 pain management medical doctors, neuropsychologist and a cognitive rehabilitation therapist. Imaging included radiographs and MRI of the right shoulder revealing rotator cuff tear; radiographs of the lumbar and thoracic spine, and left hand; CT of the head and cervical spine were performed; MRI cervical (3) and lumbar spine. Medications prescribed included Fentanyl, Percocet, Naprosyn, Cyclobenzaprine, Norco, Hydrocodone-acetaminophen, Soma, and Carisoprodol. Physical therapy was provided for spinal injuries and she did not respond to treatment. The neurosurgeon recommended epidural steroid injections and facet blocks. Cervical nerve blocks and cervical trigger point injections, cervical and lumbar epidural steroid injections (ESI), lateral epicondyle steroid injections were performed, none of which were palliative. Post-concussion disorder and PTSD with major depressive disorder were diagnosed.
On February 12th, 2015, she presented to our office with neck pain (average 6/10 VAS) that affected her vision, with paresthesia�s in both upper extremities radiating to the hands with numbness. She had low back pain (average 6/10 VAS), and she additionally reported paresthesia at the plantar surface of feet bilaterally. She had left elbow pain, right shoulder pain, knee pain, headaches and �anxiety� along with anterior sternal pain.
Her injuries were causing significant problems with her activities of daily living. Summarily she had increased pain with lifting, increased pain and restricted movement with bending, walking and carrying. She had been unable to perform any significant physical activity from the time of the crash in March 2014 until March 2015. Her right hand was always hurting and her forearms. She was not able to clean windows or do laundry, difficulty using stairs, problems with mopping, ironing and cleaning. She had to limit her walking and jogging primarily due to neck pain and right arm pain. She was not able to sit for long periods of time and sleeping was disrupted due to numbness in her hands. She was only able to walk on a treadmill for 10 minutes before having to stop due to pain, prior to the crash she would exercise for an hour.
Prior History: No significant prior musculoskeletal or contributory medical history was reported.
Research Study Conclusions
Clinical Findings (2/12/15): She had a height of 5�2�, measured weight of 127 lbs.
Visual analysis of the cervical spine revealed pain in multiple ranges of motion including flexion, extension, bilateral rotation and bilateral side bending. On extension pain was noted in the upper back, on rotation pain was noted in the posterior neck, and on lateral flexion pain was noted contralaterally.
Visual analysis of the lumbar spine revealed pain in the low back on all active ranges of motion, including flexion, extension and side bending, pain primarily at L5/S1.
Dual inclinometer testing was ordered based on visual active range of motion limitations with pain.
Sensory testing was performed of the extremities, C5-T1 and L4-S1. No neurological deficits other than right sided C5 hypoesthesia.
Foraminal compression test produced pain in the cervical spine. Foraminal distraction test caused an increase in pain in the neck. Jackson�s test on the right produced pain bilaterally in the neck. Straight leg raise bilaterally produced low back pain, double Straight leg raise produce pain at L5/S1 at 30 degrees.
Muscle testing of the upper extremities was tested at a 5/5 with the exception of deltoid bilaterally tested at a 4/5. The patient�s deep tendon reflexes of the upper and lower extremities were tested including Triceps, Biceps, Brachioradialis, Patella, Achilles: all were tested at 2+ bilaterally, equal and reactive. No evidence of clonus of the feet and Hoffman�s test was unremarkable.
C3-C5 right sided segmental dysfunction was noted on palpation. T5-T12 spinous process tenderness on palpation. Low back pain on palpation, particularly L5/S1.
Imaging Results
MRI Studies:
I reviewed the cervical MRI images taken May 2014 with the following conclusions (images attached):
Dramatic reversal of the normal cervical curvature, apex C5/6.
C5/6 herniation, indentation of the spinal cord anteriorly. High signal posterior on STIR.
Due to the angular kyphosis of the cervical spine and axial slices performed, C6/7 slices did not render a pure diagnostic image for disc disruption.
Fig. 1 (A) T2 Axial C5/6, 2 months post injury Fig. 1 (B) Sag T2 C5/6
I reviewed cervical MRI images taken September 17th, 2014 approximately 6-months post injury, and rendered the following conclusions:
Reversal of the normal cervical lordosis.
C5/C6 herniation (extrusion type) with indentation of spinal cord, appropriate CSF noted posteriorly.
I reviewed the cervical MRI dated October 24th, 2015 (images attached):
C4/5 herniation, extrusion type, left oriented into the lateral recess and neural canal causing moderate neural canal stenosis
Fig. 2 (A) 3D Axial C4/5, 19 months post injury Fig. 2 (B) Sag T2 C4/5
IMPRESSIONS: C4/5 herniation noted on 10/24/15 was not noted on prior images. The patient reported no additional injury or symptoms between MRI studies, so it is postulated that initial slices revealed a false negative; or due to the severity of abnormal cervical biomechanics, it is possible that the C4/5 disc herniated between the pre/post MRI�s with no significant increase in symptomatology. There was improvement at C5/6 related to disc abnormality and cord involvement (see below).
Fig. 3 (A) 3D Axial C5/6, 19 months post injuryFig. 3 (B) Sag T2 C5/6, 19 months post injury
The cervical flexion/extension images were digitized February 2016 and interpreted by myself and Robert Peyster MD, CAQ Neuroradiology, revealing a loss of Angular Motion Segment Integrity at intersegment C6/C7 measured at 19.7 degrees (maximum allowed 11 degrees), indicating a 25% whole person impairment according to the AMA Evaluation of Permanent Impairment Guidelines 5th edition1. CRMA provided from Spine Metrics, independent analysis.
Evidence of significant ligament injury causing functional subfailure was measured at C3/4 at 10.4 degrees and at C4/5 measuring 10.9 degrees regarding angular motion. Abnormal paradoxical translation motion measured at C6/7 and C7/T1.
Functional Testing:
EMG of the upper extremity revealed bilateral C6 radiculopathy, December 16th, 2015.
Range of Motion Cervical Dual Inclinometry:
Initial Max 4 months later % Improvement
Cervical Extension 44 42 -5%
Flexion 40 62 55%
Cervical Left 25 41 64%
Lateral flexion Right 12 26 117%
Cervical Left 46 59 28%
Rotation Right 43 73 70%
Conservative treatment rendered: A neurosurgical referral was made for assessment and surgical options. Conservative care was initiated despite failure of other medical procedures since there is �further evidence that chiropractic is an effective treatment for chronic whiplash symptoms�2-3. The patient was placed on an initial care plan of 2-3x/week for 5 months, with a gap in passive care for 1 month.
23 chiropractic visits. Instrument adjusting cervical spine was utilized with Arthrostim. Non-rotatory HVLA (high velocity low amplitude) spinal adjustments were performed thoracic and lumbar spine, applied A-P. No HVLA spinal adjustments to the cervical spine.
Prior to being placed at maximum medical improvement she had persistent low back symptoms, continued tingling in the fingertips and occasional neck pain at a 4/10, with her upper extremity paresthesia�s improved 50%. She continued with pain management chiropractic care after MMI, approximately 1 visit every 3-4 weeks with axial distraction to the cervical and lumbar spine, chiropractic adjustments as needed (PRN). 2 years/9 months post collision, and 1 year/9 months after initiating conservative care at our clinic, she reports only slight (1-2/10 VAS) spinal complaints with her primary concern being a torn rotator cuff injury from the crash that still requires surgical intervention. After initiating care at our clinic, no other interventional procedures were performed, although medication usage persisted. Due to improvement in symptoms and functional status, spinal surgery was not considered. She still utilizes Aleve PRN, 1-2 tablets. No significant active spinal rehabilitation was utilized. The patient was given at home active care consisting only of cervical and lumbar stretches, walking, and ice to affected areas.
Conclusion:While chiropractic care is safe even in the presence of herniations and radicular symptoms, �the likelihood of injury due to manipulation may be elevated in pathologically weakened tissues�4. Due to cord involvement, the provider decided to utilize low force procedures although HVLA spinal adjustments to the cervical spine could be considered safe due to lack of cord compression. HVLA spinal adjustments A-P were utilized in the lumbar and thoracic spine not only for short term pain relief but also as part of managing the chronic low back pain secondary to ligament/disc damage. While previously theorized to be only episodic, low back pain can be a lifelong condition requiring patients to seek ongoing care5. This care can be active, passive, pharmaceutical, interventional, or conservative in nature, but ongoing pain management therapy is often required for permanent ligament conditions. There is clear benefit to the patient population to be able to avoid surgical intervention due to risks, costs, ongoing prescription medication usage and adjacent level degeneration in the future6. Avoiding opioid usage is also a high priority in today�s environment.
Long term conservative care utilizing instrument spinal adjusting and targeted axial distraction therapy significantly reduced subjective reporting of pain, increased activities of daily living, and allowed the patient to avoid further spinal injections or surgical intervention. Considering that various interventional procedures failed prior to conservative care, it is important that providers work in an interdisciplinary environment such that the safest, and in this case the most effective, therapies are utilized first to reduce risk to the patient and maximize benefit and reduce costs.
In this case study, the patient utilized multiple pain management physicians, cervical nerve blocks and epidural steroid injections, and was not directed to conservative care for 11 months post injury. Utilizing chiropractic as conservative care would have enabled this patient to regain function and decrease pain while reducing costs and risks that are associated with medications and interventional procedures.
Competing Interest: There are no competing interests in the writing of this case report.
De-Identification: All of the patient�s data has been removed from this case.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Cocchiarella L., Anderson G. Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, 2001 AMA Press.
Khan S, Cook J, Gargan M, Bannister G. A symptomatic classification of whiplash injury and the implications for treatment. Journal of Orthopaedic Medicine 1999; 21(1):22-25.
Whedon J, Mackenzie T, Phillips R, Lurie J. Risk of traumatic injury associated with chiropractic spinal manipulation in Medicare Part B beneficiaries aged 66-99 years. Spine, 2015; 40:264�270.
Hestbaek L, Munck A, Hartvigsen L, Jarbol DE, Sondergaard J, Kongsted A: Low back pain in primary care: a description of 1250 patients with low back pain in Danish general and chiropractic practices. Int J Family Med, 2014.
Faldini C., Leonetti D., Nanni M. et al: Cervical disc herniation and cervical spondylosis surgically treated by Cloward procedure: a 10-year-minimum follow-up study. Journal of Orthopaedics and Traumatology, June 2010.Volume 11, Issue 2,pp 99-103.
Additional Topics: Recovering from Auto Injuries
After being involved in an automobile accident, many victims frequently report neck or back pain due to damage, injury or aggravated conditions resulting from the incident. There’s a variety of treatments available to treat some of the most common auto injuries, including alternative treatment options. Conservative care, for instance, is a treatment approach which doesn’t involve surgical interventions. Chiropractic care is a safe and effective treatment options which focuses on naturally restoring the original dignity of the spine after an individual suffered an automobile accident injury.
The importance of Magnetic Resonance Imaging to evaluate the integrity of the lumbar posterior ligament complex post trauma.
Abstract: Posterior ligamentous complex(PLC), consisting of the supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules is thought to contribute significantly to the stability of the lumbar spine. There has been much debate on whether Magnetic Resonance Imaging(MRI) is specific and sensitive in diagnosing pathology to the PLC. The objective is to determine the necessity of MRI imaging for evaluating the integrity of the lumbar posterior ligament complex post trauma.
Key Words: Magnetic Resonance Imaging(MRI), interspinous ligament, posterior ligament complex, low back pain, ligament laxity, electromyography, impairment rating
A 41-year-old male, presented to my office for an examination with complaints of low back pain with numbness, tingling and weakness into the left lower extremity after he was the restraint driver in a motor vehicle collision approximately three and a half months� post trauma.�He�rated the pain as a�3/10 on a visual analog scale with 10/10 being the worst and the pain and noted the pain as being�present most of the time.� He stated that he was on pain killers daily and this helped manage his daily activities. Without pain killers his pain levels are rated 8/10 being present most of the time. The pain killers stated by the patient are Oxycodone and Naproxen. He�reported that the pain would be aggravated by activities which required excessive standing, repetitive bending, and lifting. He further noted that in the morning the pain was increased and his left leg would be numb and weak for about the first hour.
The patient stated that his care to date had been managed by a pain management clinic and that he had minimal improvement with treatment which has included physical therapy and massage therapy. He reported the pain clinic next recommended steroid injections which he refused. He states there has been was no imaging ordered and that an Electromyography(EMG) had been performed. He was told the test was negative for pathology.
Prior History: No significant medical history was reported. Clinical Findings:�The patient is 6�0� and weighs 210 lbs.
Physical Exam Findings:
Cervical Spine:
Cervical spine range of motion is full and unrestricted. Maximum cervical compression is negative. Motor and other regional sensory exam are unremarkable at this time.
Thoracic Spine:
Palpation of the thoracic spine region reveals taught and tender fibers in the area of the bilateral upper and mid thoracic musculature. Thoracic spine range of motion is restricted in flexion, extension, bilateral lateral flexion, and bilateral rotation. Regional motor and sensory exam are unremarkable at this time.
Lumbar Spine:
Palpation of the lumbosacral spine region reveals taught and tender fibers in the area of the lumbar paraspinal musculature. Lumbar spine range of motion is limited in flexion, extension, bilateral lateral flexion and bilateral rotation. Extension restriction is due to pain and spasm. Straight leg raise causes pain at approximately 50 degrees when testing either side in the left low back. There is no radicular symptomatology down the leg. Kemp�s maneuver recreates pain in the L4 region on the left. No radicular symptoms are noted. The patient is able to heel and toe walk. Regional motor and sensory exam is unremarkable at this time other than L4, L5 and S1 dermatomes having decreased sensation with light touch.
Muscle testing of the upper and lower extremities was tested at a 5/5 with the exception of the left quadricep tested at a 4/5.� The patient�s deep tendon reflexes of the upper and lower extremities were tested including triceps, biceps, brachioradialis, patella, and Achilles and all were tested at 2+ bilaterally except the left patellar reflex was 1+.
RANGES OF MOTION EVALUATION
All range of motions are based on the�American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1�and performed by a dual inclinometer for the lumbar spine.
�� Range of Motion������Normal�������� Examination�������� % Deficit
Flexion
60
48
20
Extension
25
12
52
Left Lateral Flexion
25
16
36
Right Lateral Flexion
25
18
28
An MRI was ordered to rule out gross pathology.
Imaging:
�
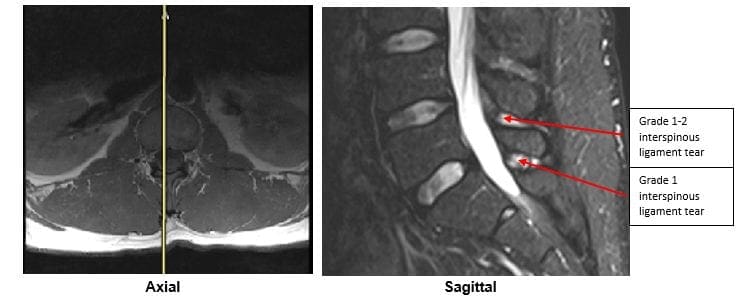
A lumbar MRI reveals;
1)��� Mild disc bulges at T11-T12, T12-L1, L1-L2 and L5-S1
2)��� Low disc signals indicative of disc desiccation at T11-T12, T12-L1, L1-L2, L2-L3, L3-L4 and L4-L5
3)��� Retrolisthesis of 2mm at L3-L4
4)��� Mild ligamentous hypertrophy at L1-L2, L2-L3, L3-L4, L4-L5 and L5-S1
5)��� L4-L5 has a Grade 1-2 tear of the interspinous ligament with mild inflammation
6)��� L5-S1 has a Grade 1 interspinous ligament tear with mild inflammation
After reviewing the MRI I ordered lumbar x-rays to rule out ligament laxity.
X-RAY STUDIES
Lumbar x-rays reveal the following:
1)��� Left lateral tilt
2)��� Retrolisthesis at L1 of 3mm
3)��� Retrolisthesis at L2 of 3mm
4)��� Combined excessive translation of 4mm of L1 during flexion-extension
5)��� Combined excessive translation of 4mm of L2 during flexion-extension
6)��� Excessive translation of L3 in extension posteriorly of 2.5mm
7)��� Decreased disc space at L5-S1
Chiropractic care was initiated. The patient was placed on an initial care plan of 2-3x/week for 3 months and then a recommended break in care for one month so the patient could be evaluated for permanency while he was not care dependent.
At maximum medical improvement, he had continued low back pain rated 4/10, continued numbness and tingling into his left leg and left quadricep weakness rated 4/5. He does not need pain killers for pain management anymore. He continues chiropractic care every two weeks to manage his symptoms.
Conclusion:
In this specific case, pathology to the posterior ligament complex diagnosed on MRI lead to the x-ray finding of excessive translation at L1-L2 and L2-L3. The patient was given a permanent impairment rating of 22% based on my interpretation of the American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1. The interspinous ligament tears at the L4-L5 and L5-S1 level would not have been diagnosed without the MRI.
There has been much debate on whether MRI imaging has a role in evaluating lumbar PLC. MRI is a powerful diagnostic tool that can provide important clinical information regarding the condition of the PLC. Useful sequences for spinal MRI in trauma include sagittal and axial T1-weighted images, T2-weighted FSE, fat-saturated T2-weighted FSE, and STIR sequences to highlight bone edema.2�Ligamentous injuries are best identified on T2-weighted images with fat saturation because the ligaments are thin and bonded on either side by fat, which can appear as hyperintense on both T1 and T2 images.3�T1-weighted images are inadequate in isolation for identifying ligamentous injuries.4�
The diagnostic accuracy for MRI was reported for both supraspinous ligament and interspinous ligament injury with a sensitivity of 89.4% and 98.5%, respectively, and a specificity of 92.3% and 87.2% in 35 patients.5
For patients with persistent symptoms after trauma an MRI may be indicated to evaluate posterior ligamentous complex integrity.
Competing Interests:� There are no competing interests in the writing of this case report.
De-Identification: All of the patient�s data has been removed from this case.
References:
1. Cocchiarella L., Anderson G. Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, 2001 AMA Press.
2. Cohen, W.A., Giauque, A.P., Hallam, D.K., Linnau, K.F. and Mann, F.A., 2003. Evidence-based approach to use of MR imaging in acute spinal trauma.�European journal of radiology,�48(1), pp.49-60.
3. Terk, M.R., Hume-Neal, M., Fraipont, M., Ahmadi, J. and Colletti, P.M., 1997. Injury of the posterior ligament complex in patients with acute spinal trauma: evaluation by MR imaging.�AJR. American journal of roentgenology,�168(6), pp.1481-1486.
4. Saifuddin, A., Green, R. and White, J., 2003. Magnetic resonance imaging of the cervical ligaments in the absence of trauma.�Spine,�28(15), pp.1686-1691.
5. Haba H, Taneichi H, Kotani Y, et al. Diagnostic accuracy of magnetic resonance imaging for detecting posterior ligamentous complex injury associated with thoracic and lumbar fractures.�J Neurosurg. 2003; 99(1 Suppl):20-26.
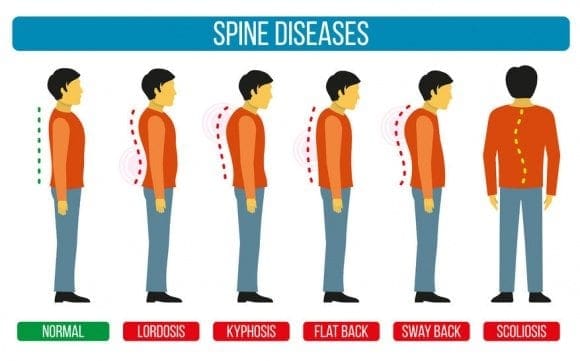
Scoliosis is described as lateral abnormal curvature of the backbone. Broadly speaking, there are two types of scoliosis, nonstructural and structural
Nonstructural Scoliosis: There is not any structural abnormality in the backbone although in this kind of scoliosis, the spine has a curvature. The curvature is to an illness process or routine in reaction to. The spine is structurally regular with a curvature, no rotation, with no asymmetry.
Types of nonstructural scoliosis:
Postural: This curvature is due to use of a wrong posture. When the kid is lies down it resolves.
Compensatory: It’s triggered by leg-length discrepancy. There’s no rotation of the vertebrae on sitting plus it typically goes off.
Sciatic: This curve results from attempting to prevent pain from an irritated nerve
Inflammatory: Here a curvature in the backbone is triggered through an infective process such as an appendicitis. The body curves to the disease or muscle spasm in reaction.
Hysterical: very rare and has an underlying component that is mental
Structural Scoliosis: A scoliosis is the one that requires both a curvature and rotation of the vertebrae. Most frequent type is the one where no cause may be found.
Idiopathic Scoliosis: Where the trigger isn’t known, most frequent type of scoliosis is idiopathic. Scoliosis is categorized based on the age when scoliosis develops. For example in a person less than 3 years old, it’s called infantile idiopathic scoliosis.
Non Idiopathic Scoliosis: Neuromuscular; It’s caused by an abnormal development of the bones of the spine for instance hemivertebra or due to other issues. Degenerative; Scoliosis occurs in older adults. Degenerative changes might lead to weakening of the ligaments that are typical and gentle tissues of the spine. In existence of arthritic changes abnormal curvature may result
Miscellaneous: Any pathology in the backbone like spine tumors may cause people to lean to the side that is contrary to reduce discomfort. Posturing may lead to scoliosis.
When no cause is known most common type of scoliosis is idiopathic, a term used in medical literature. Non structural scoliosis forms a small percentage of scoliosis.
Most common causes in this group are neuro muscular illnesses such as hemivertebra such as poliomyelitis, cerebral palsy or muscular dystrophy or delivery defects. Injury may be another cause. Infections or tumors also might give rise to curvature of the spine.
Here is the list of causes of non idiopathic structural scoliosis.
Cerebral palsy
Spinocerebellar degeneration
Friedreich�s ataxia
Hereditary Motor and Sensory Neuropathies
Trauma
Spinal tumor
Syringomyelia
Poliomyelitis
Spinal muscular atrophy I-IV (usually right sided curve)
Dysautonomia
Arthrogryposis
Muscular dystrophies
Fibre type disproportion
Congenital hypotonia
Myotonia dystrophica
Achondroplasia and hypochondroplasia � mainly lordosis or thoracolumbar kyphosis.
Spondylolisthesis
Mesenchymal disorders like Marfan�s syndrome or Ehler�s-Danlos syndrome
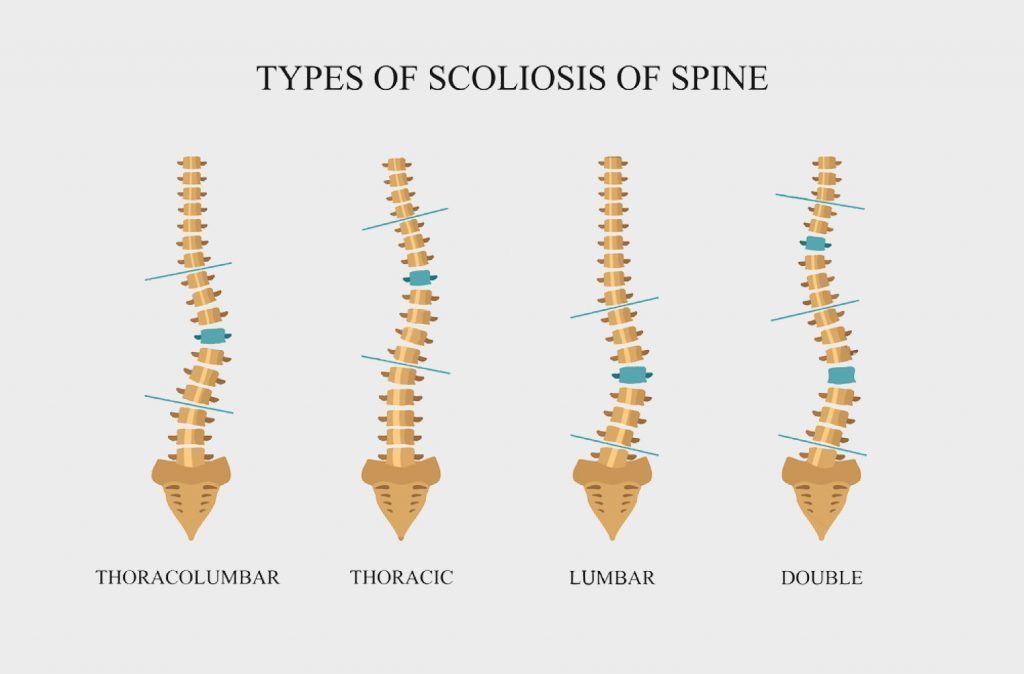
Neuromuscular Scoliosis: Neuromuscular scoliosis develops at a younger age than idiopathic curves along with a greater percentage of neuro muscular curves are progressive. Usually neuro muscular curves are long, C- shaped curves and associated pelvic obliquity is frequent.
The fundamental treatment methods are similar �?? observation, orthotic therapy, and surgery.
The objective of remedy is to maintain a backbone balanced in the sagittal and coronal planes over an amount pelvis.
These individuals generally are compliant with administration and surgery is linked complications like less bone inventory, improved bleeding, fusions that are lengthier, and also the the need for fusion to the pelvis.
More About the Types of Scoliosis
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Scoliosis Pain and Chiropractic
According to recent research studies, chiropractic care and exercise can substantially help correct scoliosis. Scoliosis is a well-known type of spinal misalignment, or subluxation, characterized by the abnormal, lateral curvature of the spine. While there are two different types of scoliosis, chiropractic treatment techniques, including spinal adjustments and manual manipulations, are safe and effective alternative treatment measures which have been demonstrated to help correct the curve of the spine, restoring the original function of the spine.
Mobility is more than moving from one place to another. It�s freedom and independence.
Whether you have a back or other condition that impacts how you walk, or your body doesn�t move as effortlessly as it once did, decreased mobility impacts a lot of people. But, if you notice changes early on, you and your doctor may be able to work on a plan to keep you moving comfortably for longer.
To see some red flags that may signal a decline in healthy mobility. Do any sound familiar?
Short Walks Become Long Walks
How do you feel after walking a quarter of a mile? Is it painful or taxing on your body?
Unless you have a spine condition or other disease that limits your ability to walk, you should be able to walk your entire life. If it�s challenging to complete short walks, that�s a red flag your mobility is at risk.
Changes In Gait
It�s not just walking distance that foreshadows a decline in mobility�how you walk is just as revealing.
Gait is the medical term for how you walk. While gait changes are a typical part of aging, some gait characteristics aren�t normal. For example: If you walk in a shuffling, unsteady, or cautious manner, you should see your doctor. He or she will help assess your gait and hopefully find the reason for it and ways to improve your movement.
Your �Get Up & Go� Is A Bit Slow
Another way to test your mobility is by doing the �get up and go� test.
You�ll need a friend to time you during this task. First, start by sitting in a chair. When your friend says �go,� get up and walk 10 feet in a straight line, then turn around and walk back to the chair and sit down. Most people who have healthy mobility can complete the exercise in 10 seconds or less.
While speed is an important part of this exercise, think about how you feel afterward. Do you feel any pain in your back muscles or in your legs or joints? If so, you should talk to your doctor to find ways to ease these movements� impact on your quality of life.
Golf & Chiropractic Care
Daily Tasks Aren�t So Routine
Is cooking a meal or taking a shower an ordeal when it used to be just a typical part of your day? Do you have work-arounds for tasks that were once easy?
One can overlook how a once simple part of your daily routine has slowly morphed into a challenging task. You may adjust your lifestyle to accommodate a decline in mobility (like putting a seat in the shower), but that�s a sign it�s time to see your doctor.
Your doctor can get to the bottom of your movement problems and suggest ways to help, such as using an assistive device, like a cane or walker, so you can move easier.
You Don�t Travel Far From Home
This isn�t about getting on a plane�you don�t travel to the other side of town. Avoiding going away from home, even if it�s a grocery store a few miles from your house, could be a sign your ability to move is declining.
Think about it: Running errands across town for an hour or two takes physical endurance. If you feel mentally and physically exhausted over the thought of completing a few errands, that�s a red flag your mobility health is at risk.
The Best Way To Improve Mobility
Want to keep walking well into your later years? The answer is simple: Stay active.
Physical activity is excellent for your heart, lungs, muscles, and spine, and helps preserve your independence. It�s never too late to start exercising.
Caring for your mobility is essential�not just for spine health but for your total health.
When diagnosed with degenerative disc disorder, among the primary things that lots of patients ask is, “Am I going to need surgery to repair this?” For many people, the answer is no. You in fact need to meet some rather stringent demands in order for your doctor to recommend operation:
You have attempted several months�ordinarily about six months�of non-operative treatments, plus they haven’t helped reduce your pain. What this means is that you simply have attempted physical therapy, medications, rest, among others, and your pain is still interfering with your life.
Your disc degeneration is at two levels not just one. When you have multi-level disc degeneration, you might not be the best candidate for surgery as you may lose an excessive amount of mobility in your back if you have a fusion (that sort of surgery is clarified below).
You’re comparatively young. Recovery from operation could be a tough procedure, so that your body requires in order to manage it. Younger individuals are somewhat more effective at recovering than older folks that are more prone to complications from operation. There’s not a certain “you should not have surgery if you are older than this” age. Your physician will probably be able to create that recommendation.
Operation could be required immediately for those who have among these red flags:
Loss in bladder or bowel control
Cauda equina syndrome is an incredibly serious ailment. Your cauda equina�or “horse’s tail”�is several nerves that resembles, competently enough, a horse’s tail. It is situated at the conclusion of the spinal cord, and it is a surgical emergency when the cauda equina is compressed. You might have extreme low back pain, weakness in your legs, radiculopathy (pain that goes out of your back and into your legs), and incontinence.
Types of Surgery for Degenerative Disc Disease
Up until lately, surgery for degenerative disc disease has called for two main parts: removal of what’s causing pain and then fusing the back to control movement. When the surgeon removes tissue that’s pressing on a nerve, it is called a decompression surgery. Fusion is a stabilization surgery, and frequently, a decompression and fusion are done at the exact same time.
Traditional surgical options that are decompression include:
Facetectomy: There are joints in your spine called facet joints; they help stabilize your back. Yet, facet joints can put pressure on a nerve. “Ectomy” means “removal of.” So a facetectomy involves removing the facet joint to reduce that pressure.
Foraminotomy: If part of the disc or a bone spur (osteophyte) is pressing on a nerve as it makes the vertebra (through an exit called the foramen), a foraminotomy might be done. “Otomy” means “to make an opening.” So a foraminotomy is making the opening of the foramen larger, therefore the nerve can depart without being compressed.
Laminectomy: At the rear of every vertebra, there is a bony plate that protects your spinal canal and spinal cord; it’s known as the lamina. It may be pressing in your spinal cord, hence by removing section or all of the lamina, the surgeon may make more room.
Laminotomy: Similar to the foraminotomy, a laminotomy makes a more substantial opening, this time in your bony plate shielding your spinal canal and spinal cord (the lamina). The lamina may be pressing therefore the surgeon may make more room for the nerves using a laminotomy.
All of the above decompression techniques are done from the back of the spine (posterior). Sometimes, though, a surgeon has to do a decompression from the front of the spine (anterior). As an example, a bulging disc or a herniated disc shoving into your spinal canal sometimes cannot be removed from behind because the spinal cord is in the way. In that case, the decompression procedure is normally performed from the front (anterior). The main anterior decompression techniques are:
Discectomy: It might be pressing on your own nerves in case you are in possession of a bulging disc or a herniated disc. In a discectomy, the surgeon will remove all or area of the disc. The surgeon can do a discectomy using a minimally invasive approach. Minimally invasive means that there are smaller incisions as well as the surgeon works with a microscope and very little surgical tools. You’ll possess a recovery period that is shorter when you possess a minimally invasive discectomy.
Corpectomy (or Vertebrectomy): Occasionally, surgeons will need to take the complete vertebral body out because disc substance becomes lodged between the spinal cord and also the vertebral body and can’t be removed by a discectomy. In other cases, osteophytes form between spinal cord and the vertebral body. In these situations, the whole vertebral body may need certainly to be removed to gain access to the disc material that is pressing on your nerve�that’s a corpectomy.
After portion of a disc or vertebra continues to be taken out, your back could be shaky, meaning that it proceeds in strange ways. That makes you more at risk for serious neurological harm, and you don’t want that. The surgeon will need to stabilize your spine. Traditionally, this has been done using a fusion, and it can be done from the back (posterior) or in the front (anterior).
In spine stabilization by fusion, the surgeon creates an environment where the bones in your back will fuse together over time (usually over several months or longer). The surgeon uses a bone graft (normally using bone from your own personal body, but it is possible to utilize donor bone as well) or a biological substance (which will stimulate bone growth). Your surgeon may use spinal instrumentation�wires, cables, screws, rods, and plates�to raise stability as the bones fuse. The fusion will cease movement between the vertebrae, providing long term stability.
New Surgical Options for Degenerative Disc Disease
A fruitful fusion restricts motion in the fused area. Now there’s a brand new surgical option that helps you keep freedom: an artificial disc. The surgeon will remove your disc (a discectomy), and insert an artificial disc in its area. The notion is that the artificial disc help you move more readily and with less pain and will keep your spine flexible.
Artificial discs have become new, but they’re a fascinating development in back surgery. But because they’re so new, there haven’t been many long-term studies in the US about the effectiveness of artificial discs. Short-term studies and studies from Europe are promising, though.
Risks of Spinal Surgery
As with absolutely any procedure, there are risks involved with spine surgery for degenerative disc disease. Before requesting one to sign a surgical consent form, your doctor will discuss possible risks along with you. Possible complications include, but are not limited to:
harm to nerves or your spinal cord
non-healing of the bony fusion (pseudoarthrosis)
failure to enhance
instrumentation breakage/failure
infection and/or bone graft site pain
pain and swelling in your leg veins (phlebitis)
urinary difficulties
Complications could result in more surgery, so again �make certain that you completely understand the risks along with your surgery before proceeding. The decision for surgery is yours and yours alone.
Recovering from Degenerative Disc Disease Surgery
After surgery for DDD, you will not immediately feel better. Should you have had a fusion, it will require some time (several months or longer) for the fusion to heal properly, and in the interim,, you could have pain in the region where you had surgery. Your incisions should heal in 7 to 14 days.
Your surgeon will provide you with special directions about what you’ll be able to and can’t do following surgery. Be sure to stick together with the healing plan and never overdo it or overstress your back. Report any issues�such as increased pain, temperature, or infection�to your physician immediately.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Preventing Spinal Degeneration
As we age, it’s natural for the spine, as well as the other complex structures of the spine, to begin degenerating. Without the proper care, however, the overall health and wellness of the spine can develop complications, such as degenerative disc disease, among others, which could potentially lead to back pain and other painful symptoms. Chiropractic care is a common alternative treatment option utilized to maintain and improve spine health.
Doctor of Chiropractic, Dr. Alexander Jimenez looks at four ways of reducing back pain.
1. Understand The Way Your Spine Works
The best approach to take care of your spine and prevent back pain is to begin with a superb understanding of how the spine works. By understanding how your backbone works when you’re performing jobs that are day-to-day or moving during your day, you may be able to take care of your spine and keep it working for a long time with fewer problems and less back pain.
2. Incorporate Safe Body Mechanics Into Activities
Use good body mechanics during day-to-day jobs at home and work. What does that mean? Good body mechanics means while you go, keeping your back in a safe posture that is balanced. You can help to prevent back pain and injury, by remembering several easy notions. You should employ your leg and arm muscles when lifting and stooping �not your back muscles. Second, keep your back straight when bending and lifting. And last but not the very least, be sure to bend at your hips and knees, not at your waist.
An example of correctly bending at the hips and knees
3. Exercise On A Regular Basis
Regular care of stuff we possess helps to keep them working efficiently, with less effort and safely. Exactly the same is true of the back.
Exercising on a regular basis really helps to keep up long term to a healthy back.
Regular exercise helps to increase endurance and reduces fatigue.
But Don’t I Get Enough Exercise At Work?
Many people believe their occupations provide enough exercise�specially occupations which are physical and could include manual labor. Regrettably this really isn’t accurate. Individuals need daily exercise to state and strengthen their muscles to perform job tasks safely and efficiently.
Exercise could be fun! There are lots of types of exercise. One method when selecting to start a workout program to ensure success would be to pick some form of exercise that fits into your lifestyle. If exercise is accessible and convenient, you’ll be prone to continue exercising on a longterm basis. As an example, determining to swim daily or do water aerobics without easy use of a pool year round would make success less likely and consistency difficult.
A typical exercise that a lot of people start successfully with is walking. Walking just takes a superb pair of walking shoes, may be done any day of the year, and is usually simple to fit right into a daily program.
Remember, whatever type of exercise you decide on, always start out small (10 minutes vs 60 minutes), and slowly increase your own exercise time. This may help to make sure your success at getting started and sticking with a fitness plan. Add two or one stretching exercises, like a calf stretch, for your routine for one more benefit.
An example of a calf stretch
4. Fuel Your Body With Proper Nutrition
Eating a healthy diet supplies the fuel your body has to make energy. And energy must do work, meaning the jobs we do throughout the day, like work tasks and exercise. Appropriate nutrition also helps to maintain your ideal body weight. Weight management is a great way to restrain stress on the joints in your body, including the spine.
Unsure where to start to understand about proper nutrition and establishing a healthier diet for you personally as well as your lifestyle? Then take a look at Introduction to Nutrition. By integrating these suggestions into your everyday life, you’ll be able to promote a healthier back�and lifestyle�for a long time.
El Paso, TX. Chiropractor Dr. Alex Jimenez examines scoliosis.
We all have curves in our backs, but scoliosis causes the spine to curve in the wrong direction. It causes sideways curves, and those are not the same as the normal curves of the spine. In case you looked at your spine from your side, you had see it curves out at your neck (cervical spine), in at your mid-back (thoracic spine), and out again at your low back (lumbar spine). Your back is likely to curve that way.
However, if your spine was looked at by you from behind, you shouldn’t see any curves. When there are sideways curves in the back from the back view, that is scoliosis. The curves can seem like an “S” or a “C.”
Spine Anatomy: Quick�Lesson
You first need to know what a healthy back looks like, to comprehend scoliosis. You will find four areas in your back:
Cervical Spine:
That is your neck, which begins at the base of your skull. It features seven little spinal bones (called vertebrae), which doctors label C1 to C7 (the “C” means cervical). The numbers one to seven signify the level of the vertebrae. C1 is closest for your skull, while C7 is closest to your torso.
Thoracic Spine:
Your mid-back has 12 vertebrae which are labeled T1 to T12 (the “T” means thoracic). Vertebrae in your thoracic spine connect to your own ribs, making this a part of your back comparatively stiff and stable. Your thoracic spine doesn’t move as the other areas of your back.
Lumbar Spine:
In your low back, you’ve got five vertebrae that are tagged L1 to L5 (the “L” means lumbar). These vertebrae are your strongest and biggest vertebrae, responsible for carrying lots of the weight of your body’s. The lumbar vertebrae are also your last “authentic” vertebrae; down from this region, your vertebrae are fused. The truth is, L5 may be fused with part of your sacrum.
Sacrum & Coccyx:
The sacrum has five vertebrae that usually fuse by adulthood to form one bone. The coccyx�commonly known as your tail bone�has four (but occasionally five) fused vertebrae.
Normal Spinal Curves: Lordosis & Kyphosis
When viewed in the side, you can observe the spine has both outward and inward curves. These curves help your back are also very important to flexibility and hold your weight.
There are just two types of normal curves in your back, and they’re called lordosis and kyphosis. Kyphosis means the spine curves inward, and lordosis means the spine curves out.
There are two spinal curves that are lordotic and two kyphotic in an ordinary back. Your cervical and lumbar spinal columns each possess a lordotic curve. Sacrum and your thoracic back have kyphotic curves.
While lordosis and kyphosis refer to a healthy curvature in your back, in addition they describe abnormal spinal curves which might be different than scoliosis. Lordosis that is strange is an extreme inward spinal curve. Kyphosis that is strange is a state that results in a hunchback or slouching posture, and you also will read about it in our Kyphosis Center.
Types Of�Scoliosis
Scoliosis is ordinarily associated with kids, but adults can have it, also. This generally occurs the disorder progresses aggressively or when scoliosis is not discovered during childhood. Most cases of scoliosis�more than 80%, in fact�are idiopathic, meaning they don�t possess a cause that is known.
Listed here are the various kinds of scoliosis:
Infantile idiopathic scoliosis is diagnosed in kids ages 0 to 3.
Congenital scoliosis happens when the spine doesn’t grow properly in the womb.
Neuromuscular scoliosis is caused by brain, spinal cord, and muscular system disorders..
Syndromic scoliosis grows as part of an illness or an underlying syndrome.
Juvenile idiopathic scoliosis is diagnosed in kids ages 4 to 10.
Adolescent idiopathic scoliosis is diagnosed in young people ages 11 to 18.
Adult degenerative or idiopathic scoliosis is diagnosed in individuals older than 18.
Along with the types noted above, your back specialist may refer to your scoliosis early-onset scoliosis�a term for scoliosis detected before 10 years of age. Syndromic scoliosis, congenital scoliosis, neuromuscular scoliosis, infantile idiopathic scoliosis, and juvenile idiopathic scoliosis may all be considered early-onset scoliosis.
Treating Scoliosis
Scoliosis brings up images of braces and perhaps memories of being examined for it by the school nurse. Bracing is one of the most common treatment choices for scoliosis as the curve may be fixed by it without back surgery.
Sometimes, though, the curve is too extreme and bracing does not help enough. Because scenario, you could have scoliosis surgery to correct the curve. You can find out more on the topic of surgical treatment for scoliosis in scoliosis surgery for scoliosis and adults operation for kids.
For kids, particularly, it can be frightening to learn they have scoliosis. Having that label makes them different at a time in their own lives when they do not need to be different. They may not enjoy the concept of wearing a brace, either. But scoliosis is nothing to be scared or ashamed of. With the correct treatment, scoliosis doesn’t have to define your life.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 De-Identification: All of the patient�s data has been removed from this case.
De-Identification: All of the patient�s data has been removed from this case.





 How do you feel after walking a quarter of a mile? Is it painful or taxing on your body?
How do you feel after walking a quarter of a mile? Is it painful or taxing on your body? It�s not just walking distance that foreshadows a decline in mobility�how you walk is just as revealing.
It�s not just walking distance that foreshadows a decline in mobility�how you walk is just as revealing.