Gartland classification grades minimally displaced subtle injuries treated with simple immobilization vs. posterior elbow dislocation treated operatively
A potential risk of ischemic compromise if care is delayed (Volkmann contracture)
The Radiological exam is crucial: sail sign & posterior fat pad sign with anterior humeral line failed to intersect mid/2/3 of Capitellum.
Incomplete pediatric Fx:
Most in <10 y.o. Greenstick, Torus, Plastic aka Bowing deformity
Typically heal well, treated conservatively with immobilization
Plastic deformity if >20-degrees requires closed reduction
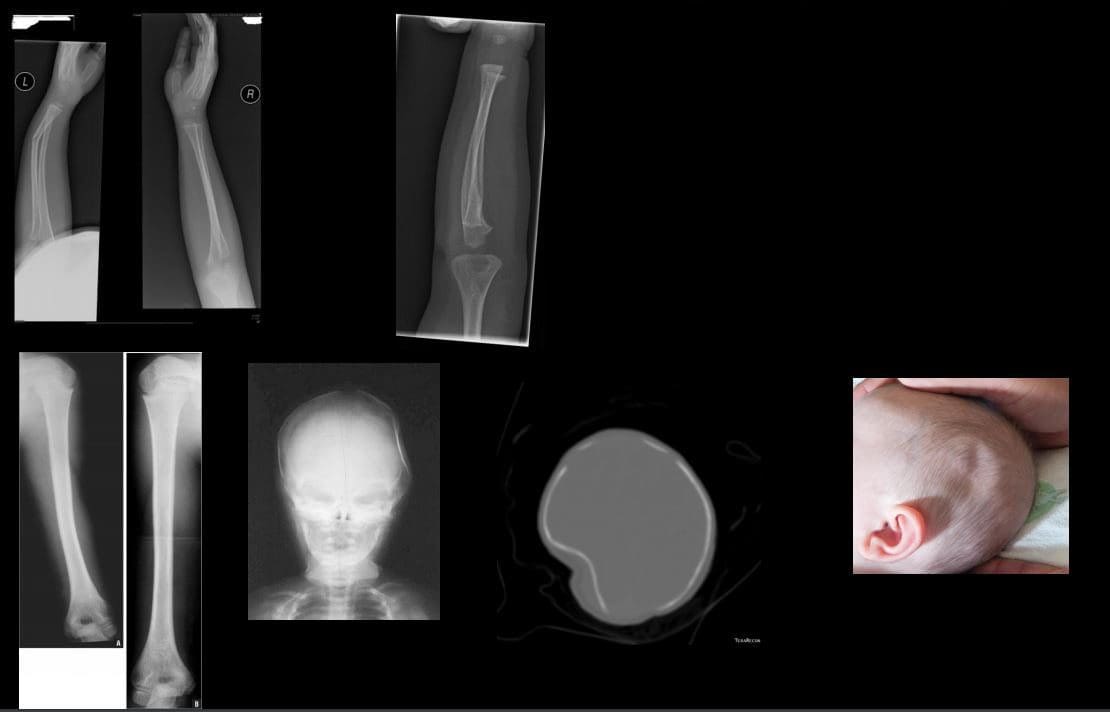
Ping pong skull fracture may develop following trauma, forceps delivery and complications of birth trauma. May need to be assessed by the pediatric neurosurgeo.n
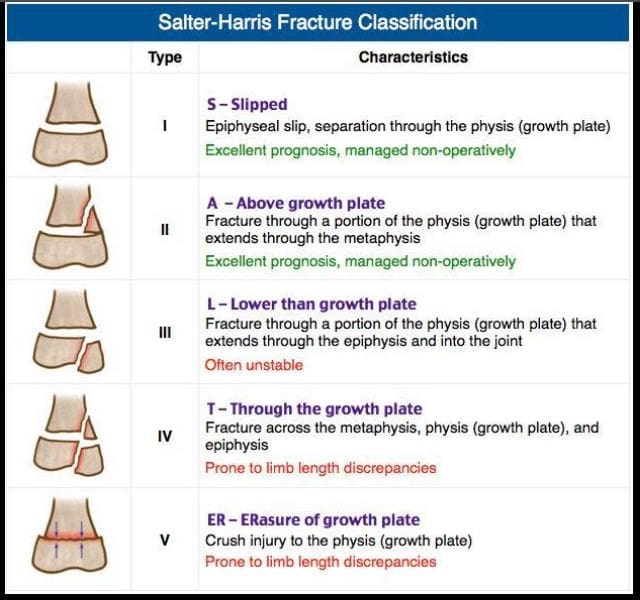
Salter-Harris types of physeal growth plate injuries
Type 1-slip. e.g., Slipped Capital Femoral Epiphysis. Typically no bone fracture noted
Type 2-M/C with good prognosis
Type 3- intra-articular, thus carries the risk of premature osteoarthritis and may require operative care d/t being unstable
Type 4- Fx through all regions about the physis. Unfavorable prognosis and limb shortening
Type 5- often no evidence of actual bone fracture. Poor prognosis d/t crush injury and vascular damage with limb shortening
Imaging evaluation is crucial
Non-Accidental Injury (NAI)in Children
There different forms of child abuse. Physical abuse may range from skin injuries to different MSK/systemic injuries affecting bones and soft tissues. Imaging is crucial and may identify definite signs alerting medical providers and informing child protection services and law enforcement agencies about physical abuse.
In an infant: �shaken baby syndrome� may present with CNS signs d/t tearing of immature bridging vein and subdural hematoma which can be fatal. Retinal hemorrhaging often a clue. Head CT is crucial.
MSK Radiological Red Flags:
1) major bone Fx in an un-ambulatory very young child (0-12 m.o.)
2) Posterior ribs Fx: naturally never occur d/t accidents. Most likely mechanisms: grabbing and squeezing a child or direct hit.
3) Multiple Fractures with different chronological healing rates, i.e., bone calluses indicating repeated physical trauma
4) Metaphyseal corner Fx aka Bucket handle Fx, often pathognomonic for NAI in children. Occurs when the affected extremity is held and violently twisted.
5) Spiral fracture of long bones in a young child is another example of NAI.
Other important clues of NAI. Inconsistent history provided by guardians/caregivers. No evidence of congenital/metabolic bone abnormalities like Osteogenesis Imperfecta or Rickets/osteomalacia etc.
N.B. When child�s guardians state a history that reports fall and accidents in the house, It is important to know that apparently most accidents/falls in the house are very rarely or unlikely result in major bone fractures.
Juvenile Idiopathic Arthritis (JIA)-considered M/C chronic disease of childhood. Clinical Dx: joint pain/swelling for 6-weeks or longer in a child <16-y.o. Different forms exist: Early Dx is crucial to prevent delayed complications
Most familiar forms of JIA:
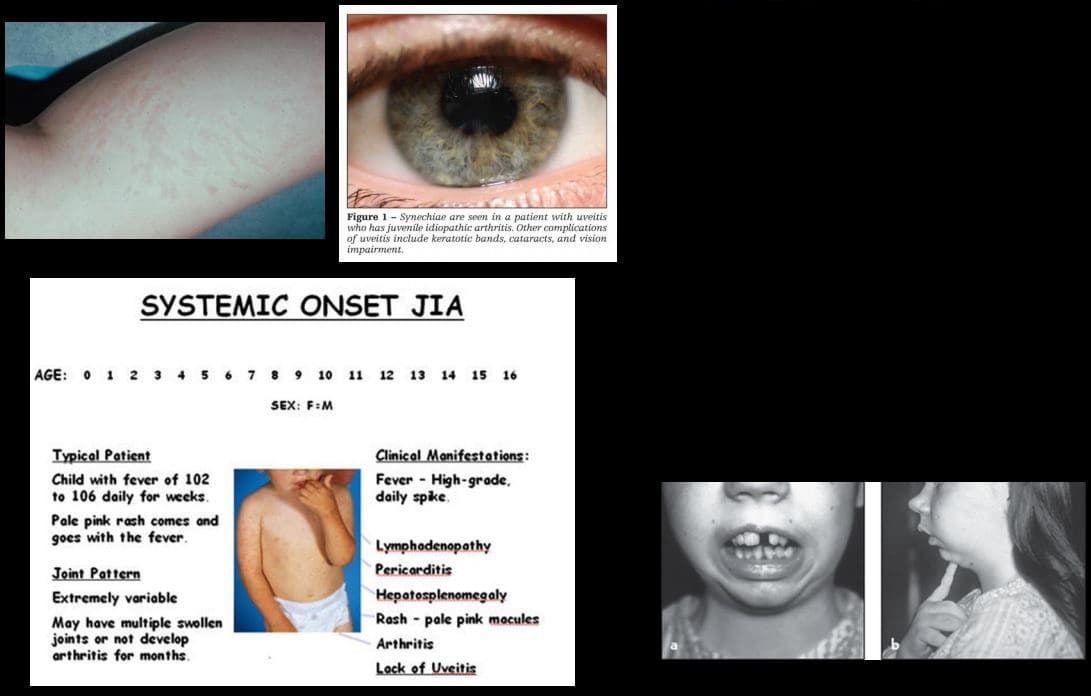
1) Pauciarticular disease (40%)- m/c form of JIA. Girls are at greater risk. Presents as arthritis in <4 joints: knees, ankles, wrist. Elbow. This type shows high association with ocular involvement as iridocyclitis (25%) that may potentially lead to blindness. Labs: RF-ve, ANA positive.
2) Polyarticular disease (25%): RF-ve. Girls are at greater risk. Affects small and large joints often affect Cervical spine
3) Systemic form of JIA (20%): often presents with acute systemic manifestation as spiking fevers, arthralgias, myalgias, lymphadeno[pathy, hepatosplenomegaly, polyserositis (pericardial/pleural effusion). Important Dx features characteristic evanescent salmon pink rash on the extremities and trunk. The Systemic form has a distinct lack of ocular involvement. Joints typically shoe no erosions compared to other types. Thus joint destruction is not typically seen
Imaging in JIA
Joint effusion bone overgrowth squaring of patella cartilage/bone erosion superimposed DJD
Fingers and long bones early physeal closure/limb shortening
Rad DDx knee/ankle: Hemophilic arthropathy Rx: DMARD.
Osteosarcoma (OSA) & Ewing�s sarcoma (ES) are 1 st and 2nd M/C primary malignant bone neoplasms of childhood (peak at 10-20 y.o.) Clinically: bone pain, change in activity, early metastasis especially pulmonary mets may occur. Poor prognosis
Ewing�s may present with bone pain, fever and elevated ESR/CRP mimicking infection. Early Dx with imaging and staging are crucial.
Imaging of OSA & ES: x-ray, followed by MRI, chest CT, PET/CT. On x-rays: OSA may affect any bone but most present as aggressive bone forming neoplasms about the knee (50% cases) especially as osteoid forming an aggressive lesion in the metaphysis with speculated/sunburst periostitis & Codman triangle. Marked soft tissue invasion.
ES may present in the shaft and show very early soft tissue spread. MRI is crucial to reveal the extent of bone and ST invasion, MRI required for surgical planning
OSA & ES Rx: A combination of surgery, radiation, chemo. Limb salvage techniques are performed in some cases. Poor prognosis if detected late.
Imaging of Ewing�s sarcoma
Permeating bone distraction
Early and extensive soft tissue invasion
Aggressive periosteal reaction with laminated (onion skin) response
Saucerisation of cortical bone (orange arrow)
A Lesion is typically diaphyseal with some metaphyseal extension
Known as Round cell tumor along with Multiple Myeloma and Lymphoma
Common Childhood Malignancies
Neuroblastoma (NBL) M/C malignancy of infancy. Derives from neural crest cells aka PNET tumors (e.g., sympathetic ganglia). Most occur in children <24-months. Some show good prognosis but >50% cases present with advanced disease. 70-80% at age 18-months or older present with advanced metastasis. NBL may develop in the adrenal medulla, sympathetic ganglia and other location. Presents as an abdominal mass, vomiting. >50% presents with bone pain d/t metastasis. Clinically: physical exam, labs, imaging: chest and abd x-rays, CT abdomen and chest is crucial to Dx. MRI may help. NBL may metastasize to the skull and infiltrate sutures with a characteristic presentation as pathological sutural diastasis.
Acute Lymphoblastic Leukemia is the m/c malignancy of childhood. Pathology: leukemic cell infiltration of bone marrow leading to bone pain and replacement of other normal marrow cells with anemia, thrombocytopenia, neutropenia and associated complications. Leukemic cells may infiltrate other sites including CNS, spleen, bone and other regions. Dx: CBC, serum lactate dehydrogenase levels, Bone marrow aspiration biopsy is the key. Imaging may help but not essential to diagnosis. On radiography, leukemic infiltration of the bone may typically appear as radiolucent bands along the physeal growth plate. Rx: chemotherapy and treating complications
Medulloblastoma: M/C malignant CNS neoplasm in children
Majority develop before 10-y.o.
M/C location: cerebellum and posterior fossa
Histologically represents a PNET type tumor not a glioma as was originally thought
MBL, as well as Ependymoma and CNS lymphoma, may lead to drop metastasis via CSF and additionally represent a unique that unlike other CNS tumors demonstrate metastatic spread outside CNS, m/c to the bone
50% of MBL may be fully resectable
If Dx and treatment begin before metastasis, 5- year survival is 80%
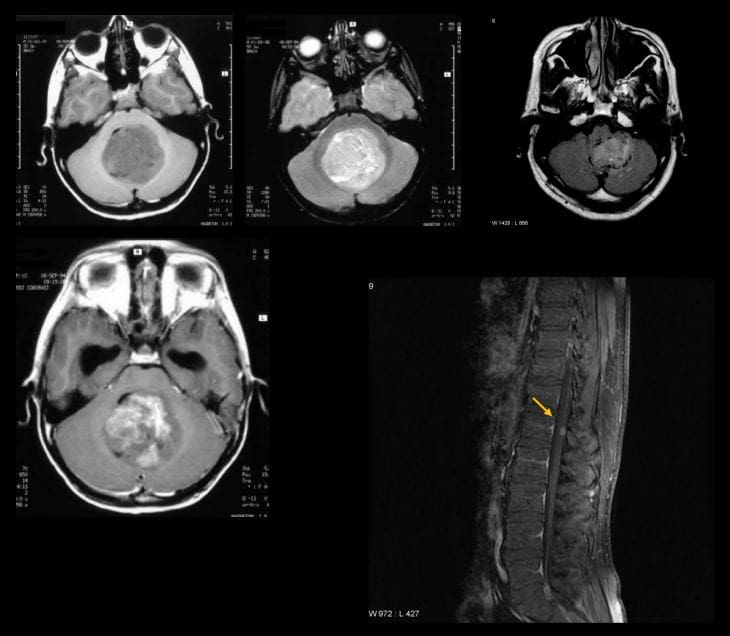
Imaging is crucial: CT scanning may be used but the imaging modality of choice is MRI that will additionally provide a more superior evaluation of the entire neuraxis for metastasis.
MBL typically appears as heterogenous hypo, iso and hyperintense lesion on T1, T2 and FLAIR scans (top images) if compare to surrounding brain tissue. Often compressing 4th ventricle with obstructive hydrocephalus. The tumor typically shows contrast enhancement on T1+C gad (bottom left image). Drop metastasis from MBL with T1+C enhancing lesion in the cord
Important Pediatric Infections
In the neonate/infant <1month: fever >100.4 (38C) may indicate bacterial and some viral infection. Strep B, Listeria, E. Coli may lead to sepsis, meningitis. Approach: chest x-ray, lumbar puncture with culture, blood culture, CBC, urinalysis.
In young children, Hemophilus influenza type B (HIB) may lead to Epiglottitis a rare but serious complication. The current vaccine helps to reduce the number of cases of Epiglottitis and other HIB related illnesses.
Parainfluenza or RSV virus may lead to Croup or acute Laryngotracheobronchitis.
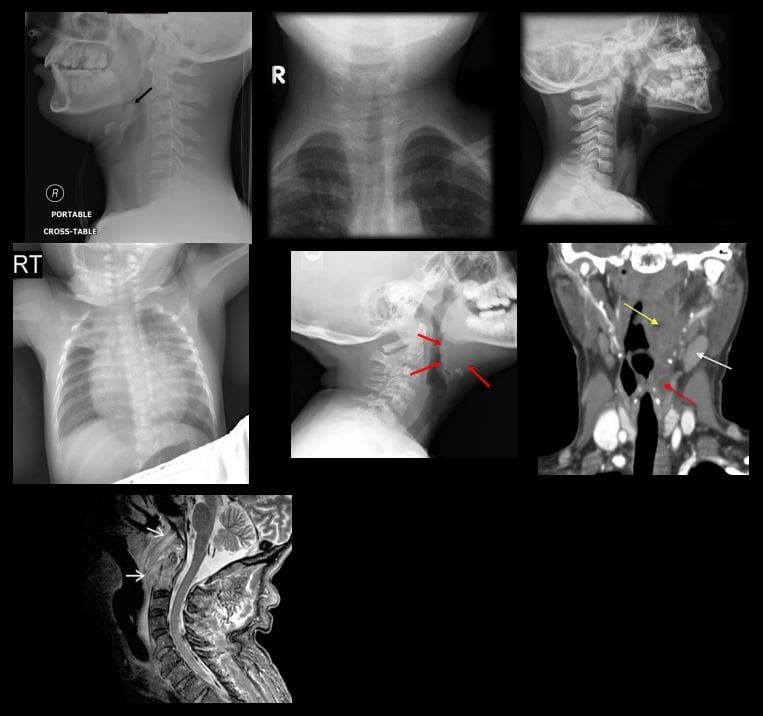
Epiglottitis and Croup are Dx clinically but AP and lateral soft tissue neck x-rays are very helpful
Epiglottitis presents with a characteristic �thumb sign� that is consistent with thickened epiglottis d/t epiglottic edema. This can be a life-threatening emergency compromising airways (top left)
Croup may show a �steeple sign� or �wine bottle sign� with distended hypopharynx as acute narrowing of subglottic airway on AP and lateral neck soft tissue x-ray (top right)
Respiratory Syncytia Virus (RSV) and influenza may lead to viral pneumonia potentially with life-threatening complications in the immunocompromised, very young and children with comorbidities. CXR is crucial (middle left)
Streptococcal pharyngitis with GABHS infection may lead to some acute or delayed complications (e.g., Rheumatic fever)
Peritonsillar abscess (above middle right) may develop in some cases and be complicated by spreading along soft tissue planes in the neck potentially leading to spread into sublingual/submandibular spaces (Ludwig Angina) when airways need to be controlled d/t base of tongue edema
Development of a retropharyngeal abscess may potentially lead to spread of the infection through freely communicating neck fascia resulting in necrotizing mediastinitis, Lemmier syndrome and invasion of carotid spaces (all are potentially life-threatening complications)
Griesel syndrome- (above bottom left) rare complication of regional tonsillar/pharyngeal oral infections that can spread to prevertebral space leading to C1-2 ligaments laxity and instability
Other important infections in children are typical bacterial (Pneumococcal) pneumonia, Urinary tract infection and Acute Pyelonephritis (especially in girls) and Meningococcal Meningitis
Pediatric Metabolic Disease
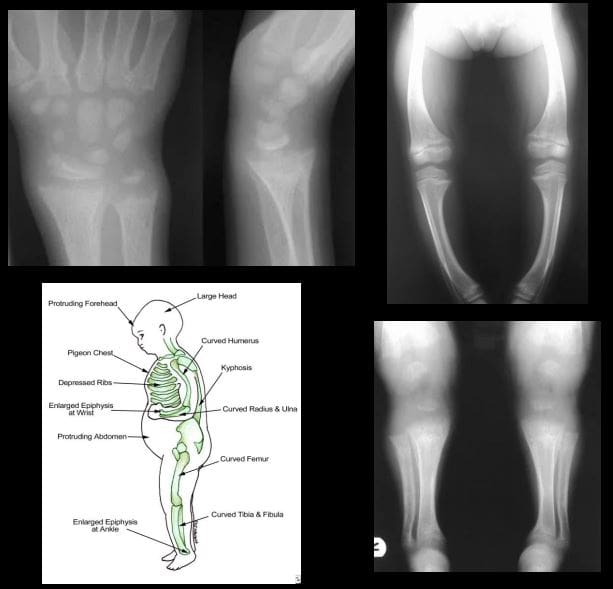
Rickets: considered osteomalacia in skeletally immature. Zone of provisional calcification of the epiphyseal growth plate is particularly affected
Clinically presents with growth retardation, extremity bowing, rachitic rosary, pigeon chest, depressed ribs, enlarged and swollen wrists, and ankles, skull deformity
Pathology: Vit D and calcium abnormality is the m/c cause. Lack of sun exposure esp. dark-skinned individual, restrictive clothing to light exposure, prolonged exclusive breastfeeding, veganism, malabsorption syndromes of the gut, renal damage and others
Imaging: frayed metaphysis aka paint brush metaphysis with flaring, widening of the growth plate, bulbous costochondral junction as a rachitic rosary, extremity bowing
Rx: treat underlying causes, correct nutritional deficit, etc.
Ear problems can be excruciatingly painful, especially in children. With 10 million new cases every year, ear infections (otitis media) are the most common illness affecting babies and young children and the number one reason for visits to the pediatrician�accounting for more than 35 percent of all pediatric visits.
Almost half of all children will have at least one middle ear infection before they�re a year old, and two-thirds of them will have had at least one such infection by age 3. The symptoms can include ear pain, fever, and irritability. Otitis media can be either bacterial or viral in origin, and frequently results from another illness such as a cold. For many children, it can become a chronic problem, requiring treatment year after year, and putting the child at risk of permanent hearing damage and associated speech and developmental problems.
Standard treatment for most cases of otitis media is with antibiotics, which can be effective if the culprit is bacterial (antibiotics, of course, do nothing to fight off viruses). But, according to many research studies, antibiotics are often not much more effective than the body�s own immune system. And repeated doses of antibiotics can lead to drug-resistant bacteria that scoff at the drugs, while leaving the child screaming in pain.
Frequent ear infections are also the second most common reason for surgery in children under 2 (with circumcision being the first). In severe cases�for example, when fluids from an ear infection haven�t cleared from the ear after several months, and hearing is affected�specialists sometimes prescribe myringotomy and tympanostomy, more commonly known as �ear tubes.� During the surgical procedure, a small opening is made in the eardrum to place a tube inside. The tube relieves pressure in the ear and prevents repeated fluid buildup with the continuous venting of fresh air. In most cases, the membrane pushes the tube out after a couple of months and the hole in the eardrum closes. Although the treatment is effective, it has to be repeated in some 20 to 30 percent of cases. And this kind of surgery requires general anesthesia, never a minor thing in a small child. If the infection persists even after tube placement and removal, children sometimes undergo adenoidectomy (surgical removal of the adenoids)�an option that is effective mostly through the first year after surgery.
Before yet another round of �maybe-they�ll-work-and-maybe-they-won�t� antibiotics or the drastic step of surgery, more parents are considering chiropractic to help children with chronic ear infections. Dr. Joan Fallon, a chiropractor who practices in Yonkers, New York, has published research showing that, after receiving a series of chiropractic adjustments, nearly 80 percent of the children treated were free of ear infections for at least the six-month period following their initial visits (a period that also included maintenance treatments every four to six weeks).
�Chiropractic mobilizes drainage of the ear in children, and if they can continue to drain without a buildup of fluid and subsequent infection, they build up their own antibodies and recover more quickly,� explains Dr. Fallon. She�d like to see her pilot study used as a basis for larger-scale trials of chiropractic as a therapeutic modality for otitis media.
Dr. Fallon uses primarily upper-cervical manipulation on children with otitis media, focusing particularly on the occiput, or back of the skull, and atlas, or the first vertebra in the neck. �Adjusting the occiput, in particular, will get the middle ear to drain. Depending on how chronic it�s been and on where they are in their cycle of antibiotics, children generally need to get through one bout of fluid and fight it off themselves.� That means, for the average child, between six and eight treatments. If a child�s case is acute, Dr. Fallon will check the ear every day, using a tympanogram to measure the ear and track the movement of the eardrum to make sure that it�s draining. �I�ll do adjustments every day or every other day for a couple of days if they�re acute, and then decrease frequency over time.�
Dr. Fallon, whose research garnered her the acclaim of childrearing magazines like�Parenting�and�Baby Talk, often sees great success when she treats a child for otitis media. �Once they fight it themselves, my kids tend to do very well and stay away from ear infections completely. Unless there are environmental factors like smoking in the house, an abnormally shaped Eustachian tube, or something like that, they do very well,� she says.
�I have two large pediatric groups that refer to me on a regular basis. In the winter, when otitis is most prevalent, I see five or six new children each week from each group,� says Dr. Fallon. �It�s safe and effective and something that parents should try, certainly before inserting tubes in their children�s ears.�
Chiropractic Care Can Help�
Come on in and talk to us about your child�s ear infections. Doctors of chiropractic are licensed and trained to diagnose and treat patients of all ages and will use a gentler type of treatment for children.�However, Texas chiropractors can answer any questions a patient�may have and refer them to a specialist, they must remain within the scope of their field which is the�Muscular�and the�Musculoskeletal system.
Though the most visible kinesiology tape users might be professional athletes, Olympians, or weekend warriors � a much smaller clientele is also proving the advantages of this unique treatment. With a special line designed for sensitive skin and playful prints and colors that will speak to the sticker and Band-Aid loving child, it�s not surprising that kinesiology tape is quickly becoming more than an athlete�s aid.
While the uses and applications of kinesiology tape for pediatric treatment are growing daily, here is a quick run down of how kinesiology tape is being used in pediatric care today:
Pain and Swelling Relief
� When kinesiology tape is applied to an injured or inflamed area, children can enjoy some relief without having to take pain medication or sit through icing and therapy treatments.
Orthopedic Treatment
� Children often don�t understand the purpose behind rehabilitation exercises, so kinesiology tape provides an additional or alternative treatment for children with orthopedic injuries, weak or underdeveloped muscles, gait abnormalities, paralysis � even poor posture.
Neuromuscular Disorders
� Kinesiology tape has proven effective to activate weak muscles and inhibit overactive muscles.� With a simple and safe taping application, children suffering from neuromuscular conditions like cerebral palsy, or muscular dystrophy could see improvements in symptoms and movement ability. It has also been shown to improve muscle tone in genetic disorders like Downs Syndrome and other conditions causing either spasticity, atrophy or poor muscle tone.
For children dealing with serious medical conditions, a colorful and painless treatment that can be worn for several days, even while playing and bathing, can make a big difference in their comfort level.
Interested in learning more about pediatric kinesiology taping? Dr. Kenzo Kaze, the creator of Kinesio Tape, provides step by step guidelines for taping infants and children in his manual, Kinesio Taping in Pediatrics available at Theratape.com.
For a list of successful case studies where kinesiology tape has provided improvement for children, check out Theratape�s research compilation as well as this case report (pdf) from Novel Physiotherapies. Hopefully, as more and more case studies document positive results, the use of kinesiology tape in pediatric care will continue to expand and increase.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine