An improper diet and nutrition can often lead to a variety of health issues, such as cardiovascular disease and hypertension. Additionally, other food-related risk factors can include, high blood pressure, or BP, obesity and type 2 diabetes. Saturated and trans fats, for example, can increase cholesterol in the blood. It’s this build-up of fatty deposits in the coronary arteries, which can lead to cardiovascular disease, hypertension and even heart attacks.
Which vitamins and minerals can improve cardiovascular disease and hypertension?
A healthy balance of vitamins and minerals can help manage and maintain heart health. According to research studies, the right intake of potassium, magnesium, calcium and zinc can substantially improve cardiovascular disease and hypertension. A proper diet and nutrition can have similar effects as taking cardiovascular disease and hypertension drugs and medications, but through a much more natural approach.
Potassium
The average U.S. dietary intake of potassium (K+) is 45 mmol/d with a potassium to sodium (K+/Na+) ratio of less than 1:2. The suggested intake of K+ is 4700 mg/d (120 mmol) with a K+/Na+ ratio of about 4-5 to 1. Several clinical and observational trials have demonstrated a substantial decrease in BP with greater K+ intake in hypertensive patients. The normal blood pressure reduction with a K+ supplementation of 60 to 120 mmol/d is 4.4/2.5 mmHg in hypertensive patients but may be as far as 8/4.1 mmHg with 120 mmol/d (4700 mg). In hypertensive patients, the linear dose response relationship is 1.0 mmHg reduction in systolic blood pressure, or SBP, and 0.52 mmHg decrease in diastolic blood pressure, or DBP, that a 0.6 g/d growth in dietary fiber intake. The solution can involve race (black > white), sodium, magnesium and calcium intake. Those on a higher sodium intake have a greater decrease in BP. Alteration of this K+/Na+ ratio is very important to the two polyunsaturated and outcomes. High potassium intake reduces the prevalence of cardiovascular disease independent of their BP reduction. Furthermore, If the serum potassium is less than 4.0 meq/dL, there is a higher risk of CVD mortality, ventricular tachycardia, and ventricular fibrillation. Red blood cell potassium is a sign of overall body stores and CVD risk in comparison to the serum potassium. Gu et al discovered that potassium supplementation in 60 mmol of KCl Daily for 12 wk significantly reduced SBP -5.0 mmHg (range -2.13 into -7.88 mmHg) (p < 0.001) in 150 Chinese men and women aged 35 to 64 decades.
Insulin raises natriuresis, modulates sensitivity, vasodilates, reduces the sensitivity to catecholamines and Angiotensin II, raises nitric oxide ATPase and DNA synthesis in the vascular smooth muscle cells and decreases sympathetic nervous system activity. In addition, potassium increases bradykinin and prostate kallikrein, decreases NADPH oxidase, which reduces oxidative stress and inflammation, improves insulin sensitivity, reduces ADMA, reduces intracellular sodium and reduces production of TGF-?.Each 1000 mg increase in potassium intake per day reduces all cause mortality by approximately 20 percent. Potassium intake of 4.7 g/d is estimated to decrease CVA by 8 percent to 15 percent and MI by 6 percent to 11 percent. Numerous SNP’s, such as nuclear receptor subfamily 3 group C, angiotensin IItype receptor and hydroxysteroid 11 beta dehydrogenase (HSD11B1 and B2) determine an individual’s reaction to dietary potassium intake towards their overall health and wellness.
Each 1000 mg drop in sodium intake daily will reduce all cause mortality. A recent study indicated a dose related response to CVA. There has been a RRR of CVA of 23 percent at 1.5-1.99 gram, 27% at 2.0-2.49 g, 29 percent at 2.5-3 g and 32 percent more than 3 g/d of potassium urinary excretion. The recommended daily dietary intake for individuals with hypertension is 4.7 to 5.0 g of potassium and less than 1500 milligrams of sodium. Potassium used out of supplementation should be decreased with care in patients with renal impairment or those ARB, DRI and serum aldosterone receptor antagonists.
Magnesium
A high dietary intake of magnesium of at least 500-1000 mg/d reduces BP in the majority of the reported observational epidemiologic and clinical trials, but the outcomes are much less consistent than those seen with K + and Na +. There’s an inverse relationship between BP and dietary magnesium intake. A report on 60 essential hypertensive subjects given magnesium supplements showed a substantial decrease in blood pressure in an eight week interval reported by 24 h ambulatory BP, office and home BP. The maximum decrease in clinical trials has been 5.6/2.8 mmHg but some studies have shown no change in BP. The blend of high potassium and low sodium intake with increased magnesium intake had.
Magnesium also raises the effectiveness of all anti-hypertensive drugs and medications, according to research studies. Magnesium competes with Na+ for binding sites on vascular smooth muscle and also functions as a direct vasodilator, . Magnesium increases prostaglandin E (PGE), modulates intracellular sodium, potassium, calcium and pH, increases nitric oxide, improves adrenal function, reduces oxLDL, reduces HS-CRP, TBxA2, A-II, and norepinephrine. Magnesium also enhances insulin resistance, glucose and MS, binds at a necessary cooperative manner with potassium, causing EDV and BP reduction, reduces CVD and cardiac arrhythmias, reduces carotid IMT, reduces cholesterol, reduces cytokine production, inhibits nuclear factor Kb, reduces oxidative stress and inhibits platelet aggregation to reduce thrombosis. Magnesium is an essential co-factor because of its delta-6-desaturase enzyme that for conversion of linoleic acid (LA) to gamma linolenic acid (GLA) required for synthesis of this vasodilator and platelet inhibitor PGE1.
A meta-analysis of all 241378 patients utilizing 6477 strokes showed a reverse relationship of dietary magnesium to the incidence of stroke. For each 100 milligrams of magnesium intake, stroke diminished. The mechanism comprise inhibition of induced glutamate release, NMDA receptor blockade, CCB actions reduction in vasodilation and ATP depletion of the arteries. A meta-analysis showed discounts mmHg in 22 trials of 1173 patients. Intracellular level of calcium (RBC) is more indicative of overall body shops and should be quantified along with serum and urinary magnesium. Magnesium might be supplemented in doses of 500. Magnesium formulations may improve absorption and reduce the incidence of diarrhea. Adding taurine in 1000 increases the ramifications of magnesium. Magnesium supplements should be avoided or used with caution in individuals with renal insufficiency.
Calcium
Population studies reveal a link between hypertension and calcium, but clinical trials that handled calcium supplements have shown consequences on blood pressure. The heterogeneous responses to calcium supplementation have been clarified through research studies. This is really the “ionic hypothesis” of hypertension, cardiovascular disease and associated cognitive, cognitive and functional disorders. Calcium supplementation is not recommended at this time as an effective method to decrease blood pressure due to insufficient research studies on its use.
Zinc
Low serum zinc levels in observational research and hypertension correlate as well as CHD, type II DM, hyperlipidemia, elevated lipoprotein that a [Lp(a)], increased 2 h post-prandial plasma glucose levels and insulin resistance. Zinc is hauled to vascular and cardiac muscle and cells by metallothionein. Deficiencies of metallothionein with intramuscular zinc deficiencies can lead to cardiomyocyte oxidative stress , mitochondrial dysfunction, dysfunction and apoptosis with cardiac remodeling hypertension, cardiovascular disease, heart failure, or fibrosis. Intracellular calcium increases oxidative.
Bergomi et al assessed Zinc (Zn++) status in 60 hypertensive subjects compared to 60 normotensive control subjects. A reverse correlation of serum Zn++ and BP has been observed. The BP was inversely associated with a Zn++ dependent enzyme lysyl oxidase activity. Zn++ inhibits gene expression and transcription through NF-?Band activated protein-1 and is now a significant co-factor for SOD. These impacts plus those on insulin resistance and SNS consequences, membrane ion exchange, RAAS might account for Zn++ antihypertensive effects. Intake needs to be 50 mg/d.
Individuals with cardiovascular disease and hypertension can benefit from the proper diet and nutrition. Essential vitamins and minerals found in a balanced, healthy nutrition, such as potassium, magnesium, calcium and zing, among others, can help improve heart health. Deficiencies in these and a diet full of saturated and trans fats can increase the prevalence of cardiovascular disease. While diagnosis and drugs/medications can be prescribed to treat cardiovascular disease and hypertension, a balanced diet and nutrition can have similar effects.� The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The thyroid gland is a butterfly-shaped gland in your neck. Among its primary functions is to pump out a hormone called thyroxine. It is that hormone which sets the rate of the human body. It’s what regulates energy generation. Some of thyroid hormone’s imbalances common indicators include tiredness, bloating, hair loss, dry skin, joint pain, muscle stiffness, elevated cholesterol, sleep disturbance, infertility, melancholy, cold hands and feet, along with weight gain.
How do you recognize thyroid gland imbalances?
Patients eliminate weight with hypothyroidism while gaining weight is a textbook symptom of hypothyroidism. In some cases a part of their disease is that their gut is so broken down that their thyroid is malfunctioning however they’re currently slimming down and that they’re malabsorbing nourishment. If we fall into those health care conceptions with by each person who has hypothyroidism then we are likely to miss a great deal of individuals.
Identifying Thyroid Disease
Traditional diagnosis is made depending on the lab test TSH (thyroid stimulating hormone) normally ordered by a general physician, internist, or endocrinologist. One of the many problems with this strategy is that it isn’t comprehensive. If your TSH comes back high, the physician tends to diagnose you. This approach often times contributes to treatment with thyroid hormone replacement medication without further investigation. Keep in mind one fundamental point, taking thyroid medication and using a minimal thyroid diagnosis doesn’t fix the problem.
Ultimately, the objective of the healthcare professional and patient should be to recognize why the thyroid levels are abnormal. And that requires a basic knowledge of biochemistry and nutrition. Let us take a deeper look at a few of the common items, in the diet and nutrition standpoint, that can contribute to low thyroid hormone production:
Gluten
Sugar
Goitrogenic foods
Dairy
Nutritional deficiencies
Gluten and your Thyroid Gland
Gluten sensitivity contributes to thyroid disease in many of different ways. Gluten induced gastrointestinal harm is one of the mechanisms of action. It is this mechanism that leads to a domino-like effect. The very first step in this process is the invention of intestinal hyper-permeability, or Leaky Gut. When the barrier is compromised, a cascade of inflammation, immune over-stimulation, and mimicry may ensue. Over time these procedures can result in an autoimmune thyroid response leading to Hashimoto’s thyroid disease or Graves’ disease.
Gluten induced gastrointestinal damage may contribute to inadequate digestion and absorption of thyroid crucial nutrients. Gluten can alter gut bacteria that are ordinary. These bacteria play a important role in thyroid gland conversion. Physicians will assert that no study exists between thyroid free and gluten disorder. They are incorrect.
Where do we find gluten? Folks will say that barley, wheat and rye are the grains that contain gluten. In reality there are distinct sorts of gluten and they’re observed in all the different forms of grain.
Sugar
This refers specifically to processed sugar like dextrose, glucose, fructose, maltodextrin, all the different kinds of sugar that is processed, even organic processed sugars. Many of the food manufacturers have gotten wise about people wanting to prevent sugar so they’ve started saying it. For example sucanat is processed sugar. Avoidance of processed sugar must be a priority to prevent imbalances with the thyroid gland and thyroid disease.
Goitrogens
There are numerous foods that can suppress thyroid hormone production and bring about goiter (thyroid enlargement). Listed below are several foods which can cause this. You can get in trouble if you consume excessive quantities of these foods, for example if you are doing a great deal of juicing and using a pound of each time or if it’s raw and it hasn’t been cooked. If you also have a thyroid condition and if you’re eating cruciferous vegetables, its advice not to stop eating them just cook them and do not make them the key foods in your diet plan.
Soy (prevent soy, particularly GMO soy)
Brussels Sprouts
Bok choy
Cabbage
Cauliflower
Collards
Cassava
Broccoli
Kale
Bamboo shoots
Spinach
Radishes
Rutabaga
Turnips
Watercress
Kohlrabi
Mustard greens
Flax
Pine nuts
Peanuts
The protein casein in milk can mimic glutenfree. Therefore it may be the dairy in their diet that mimics gluten. Gluten, sugar, goitrogenic foods, and dairy are the most usual food-based causes for thyroid hormone disturbance.
Nutrition is Vital for a Healthy Thyroid
Now let’s discuss a food component that is going to be helpful for the thyroid gland to function. There are a number of nutrients necessary for thyroid function. Vitamins and minerals help drive the chemistry behind the production of the thyroid hormones. Additionally they help these hormones and other organs and both the DNA communicate to improve and regulate metabolism.
As mentioned before, often times healthcare professionals will only conduct one laboratory test known as TSH (thyroid stimulating hormone) for the identification and treatment of thyroid disease. If TSH is above normal, you’re diagnosed “hypothyroid”. If TSH is below normal, you’re diagnosed “hyperthyroid”. Simple, right? No, far from it.
TSH is a regulatory hormone produced in the brain from the pituitary gland. TSH then travels to the thyroid gland in your neck out of the brain and tells it to produce the thyroid hormone T4. TSH needs to be made first. What ingredients does your body need to generate TSH? The number one ingredient is protein. How much is enough protein? To get a mean calculation, take your body weight in kilograms (whatever you weigh in pounds split that by 2.2 to give you your weight in kilograms) and multiply that by 0.8 and that’s how many grams of protein you need daily. Another way to calculate this amount is to multiply the amount 0.36 by your weight in lbs. As an instance, for a woman, that could be 54 g of protein. This number is individual for each individual and varies by the individual’s level of physical activity. Speak with your doctor if you suffer from kidney dysfunction. What else does our body need to generate TSH? Magnesium, Vitamin B12, and zinc. Without adequate levels of these ingredients your body cannot produce TSH and you will have low thyroid function from the start.
Now lets discuss thyroxine, T4. Thyroid hormone is potassium and protein. Protein is crucial to form the thyroid hormone (particularly the amino acid in protein called tyrosine). The “4” in T4 signifies the number of molecules of iodine are present. You need iodine for that sport car to run smoothly. Where do we get iodine? Iodine is got by us from things found not in lakes, not from rivers. Seafood, kelp, and seaweed are great sources of iodine. Consider the thyroid gland as a car factory. Internally on your thyroid gland, your thyroid uses a ton of vitamin C. Vitamin C is very important to add those iodine tires to that thyroid gland. You also need vitamin B2. There is something in your thyroid gland known as. It when you consume the iodine and iodine-rich foods is absorbed into the bloodstream. The symporter necessitates B2 to function. Is vitamin B3. To make thyroid hormone T4, you need Vitamin B3, Vitamin B2, Vitamin C, C, and vitamin.
T4 is inactive thyroid hormone. Protein is responsible for carrying T4 to your own tissues including muscle and your liver in which it has converted to T3 thyroid gland through the blood stream. Think of the proteins into your bloodstream that take the T4 thyroid hormone. The inactive T4 thyroid hormone is being hauled to the liver, muscle, and other tissues in which they are converted to the active T3 hormone. There is a process called deiodinization, where the body takes that T4 thyroid gland and eliminates one molecule of iodine to convert it. A whole lot of the conversion of T4 to T3 happens in the liver and that is because their liver is not good at converting T4 to T3, the reason why a person who has liver problems can also have thyroid problems. This conversion takes place in the muscle which is the reason why people with muscle inflammation frequently have thyroid issues. Which nutrient is required for this conversion? Selenium. You require selenium to eliminate that one molecule of iodine to convert T4 into T3 thyroid gland. You need iron to the conversion of T4 into T3.
It’s T3 we consider the active thyroid hormone. Each cell of the body has. There are receptors that act like a gap. T3 is your key that activates the enzymes that ramp up your metabolism and binds to all those receptors around the nucleus. You need Vitamin vitamin D to bind to a T3 to make a super key that unlocks your DNA and fits the nuclear receptors.
In the conclusion, you need Omega-3 fatty acids around the membrane of these cells for the hormone to be received appropriately. If you’re missing even one of those nutrients, you will have some kind of biochemical thyroid suppression.
This seems different for different people. For instance, some people have severe selenium deficiency in which they are currently converting T4 thyroid hormone that is hardly any inactive . Their physician is prescribing a sort of synthetic thyroxine T4 thyroid hormone (levothyroxine, Synthroid, etc.), however they can not convert the T4 in thyroxine into the active T3. They believe much worse being on the medication. I see other people with a genetic susceptibility for Vitamin B2 deficiency who can’t get iodine. You can fix them with foods rich in the nutrients and/or with supplements, if you have one of those nutrient deficiencies. The first step is deciding whether or not you have one or more of these deficiencies.
The following is a summary of nutrition your doctor should measure when evaluating your thyroid:
Protein
Magnesium
Zinc
Selenium
Iodine
Iron
Vitamin C
Vitamin B2
Vitamin B3
Vitamin D
Vitamin A
Vitamin B12
Omega-3
If you don’t have your healthcare professional test for these nutrient deficiencies, then you’ll never know why you’ve got a thyroid problem. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The thyroid gland is a 2-inch butterfly-shaped organ located in the front part of the neck. Although small, the thyroid glans is a major gland in the endocrine system and affects virtually every organ in the body.
What is the function of the thyroid gland?
The thyroid gland regulates fat and carbohydrate metabolism, respiration, body temperature, brain growth, cholesterol levels, the heart and nervous system, blood glucose levels cycle, skin integrity, and more.
Thyroid Diseases Explained
Thyroid disease generally involves an underactive thyroid gland, also known as hypothyroidism. In the USA, an autoimmune reaction called autoimmune thyroiditis or Hashimoto’s disease usually causes hypothyroidism. As with all autoimmune disorders, the body identifies its own tissues as an invader and strikes until the organ is destroyed. This chronic attack will finally prevent the thyroid gland from producing thyroid hormones. The lack of these hormones may slow down metabolism and also cause weight gain, fatigue, dry skin and hair loss as well as lead to difficulty concentrating. Hashimoto’s thyroid disease affects approximately 5 percent of the US population, is seven times more prevalent in women than men, and generally occurs during middle age.
Hyperthyroidism, or an overactive thyroid gland, is another frequent thyroid disease. The form is Graves’ disease in which the body’s autoimmune reaction causes the thyroid gland to make too much T3 and T4. Symptoms of hyperthyroidism may include weight loss, high blood pressure, nausea, and a rapid heartbeat. The disease also disproportionately affects women and presents until the age of 40.
Hashimoto’s thyroid disease is more common than Graves’ disease, but both are known as autoimmune thyroid disease (ATD), which has a strong genetic link and is associated with other autoimmune disorders, such as type 1 diabetes, rheumatoid arthritis, lupus, and celiac disease. A goiter, or enlargement of the thyroid gland, may be caused by hypothyroidism, hyperthyroidism, excessive or insufficient consumption of iodine from the diet, or thyroid gland, the most frequent endocrine cancer whose prevalence studies imply is increasing.
Key Nutrients for Thyroid Disease
Many dietary factors play a role in optimizing thyroid function. But, excesses and both nutrient deficiencies could cause or exacerbate symptoms. Working in collaboration with a doctor is ideal to determine status for optimal thyroid health. Many functional medicine practitioners specialize in functional nutrition, which can help with thyroid disease.
Iodine
Iodine is a vital nutrient in the human body and essential to thyroid function; thyroid hormones have been constituted of iodine. Iodine deficiency is the cause while disorder is the primary cause of thyroid dysfunction in the United States
Iodine deficiency has been considered uncommon in america since the 1920s, largely as a result of widespread utilization of iodized salt. This, along with poultry, milk, and grains, is a major source of iodine in the conventional American diet.
However, iodine intake has decreased during the last few decades. Americans get approximately 70 percent of their salt intake from foods which, in the USA and Canada, don’t contain iodine. A 2012 Centers for Disease Control and Prevention report indicates that, on average, Americans are receiving sufficient amounts of iodine, together with the potential exclusion of women of childbearing age.
Both iodine deficiency and surplus have significant dangers; thus, supplementation ought to be approached with care. Supplemental iodine might lead to symptom flare-ups in individuals with Hashimoto’s thyroid disease because it stimulates antibodies.
Iodine intake often is not easily apparent on a dietary recall because the quantity in foods is largely determined by levels from the soil and extra salt. But, experts state that, “Clients carrying iodine tablets are a red flag. Frequent intake of foods such as seaweed or an avoidance of all iodized salt may serve as signals that further exploration is required.”
Vitamin D
Vitamin D deficiency is connected to Hashimoto’s, according to one study showing that over 90 percent of patients studied were deficient. It’s uncertain whether the low vitamin D levels were the direct cause of Hashimoto’s or the result of the disease process itself.
Hyperthyroidism, especially Graves’ disease, is known to cause bone loss, which can be compounded by the vitamin D deficiency commonly seen in people with hyperthyroidism. This bone mass could be recovered with therapy for hyperthyroidism, and specialists indicate that sufficient nourishment, such as vitamin D, which are particularly important during and following
Foods which contain some vitamin D include fatty fish, milk, legumes, eggs, and mushrooms. Sunlight also is a source, but the sum of vitamin production depends upon the season and latitude. Supplemental D3 could be necessary, if clients have low vitamin D levels, along with the customer’s doctor should monitor progress to ensure the individual’s levels stay within a suitable range.
Selenium
The maximum concentration of selenium is found in the thyroid gland, and it has been demonstrated to be a necessary element of enzymes integral to thyroid function. Selenium is a vital trace mineral and was shown to have a deep effect in the immune system, cognitive function, fertility in both women and men, and mortality rate.
A meta-analysis of randomized, placebo-controlled studies has shown advantages of selenium on both the thyroid antibody titers and mood in patients with Hashimoto’s, but this impact appears more pronounced in people who have a selenium deficiency or insufficiency in the outset. Conversely, an excessive intake of selenium can lead to gastrointestinal distress or perhaps raise the risk of type 2 diabetes and cancer. So clients will benefit from getting their selenium levels tested and integrating healthful foods into their diets, including Brazil nuts, tuna, crab, and lobster.
Vitamin B12
Studies show that about 30 percent of people with ATD experience a vitamin B12 deficiency. Food sources of B12 include salmon, sardines, mollusks, organ meats such as liver, muscle meat, and dairy. Vegan sources include fortified cereals and yeast. Severe B12 deficiency may be irreversible, therefore it is important for dietitians to suggest clients have their levels analyzed.
Goitrogens
Cruciferous vegetables like broccoli, cauliflower, and cabbage naturally discharge a chemical known as goitrin when they are hydrolyzed, or broken down. Goitrin can interfere with the synthesis of thyroid hormones. Nonetheless, this is usually a concern only when combined with an iodine deficiency. Heating cruciferous vegetables denatures much or all of this possible goitrogenic effect.
Soy is another possible goitrogen. The isoflavones in soy may lower thyroid hormone synthesis, but many studies have discovered that consuming soy does not result in hypothyroidism in individuals with adequate iodine stores. But Dean cautions clients to consume soy in moderation.
The potential exclusion is millet, a nutritious gluten-free grain, which might suppress thyroid function even in people with adequate iodine intake. If a dietary recall indicates frequent millet ingestion in patients with hypothyroidism, it may be wise to indicate they choose another grain.
Foods, Supplements, and Medication Interactions
When it comes to thyroid medications, it is very important to RDs to know the drugs can interact with common nutritional supplements. Calcium supplements have the capacity to interfere with absorption of thyroid medications, so when taking the two patients need to consider the timing. Studies recommend limiting calcium supplements and thyroid drugs by at least four hours. Coffee and fiber nutritional supplements reduced the absorption of thyroid drugs, so patients should take them one hour apart. Dietitians should affirm whether customers have received and are adhering to these guidelines for optimum wellness.
Chromium picolinate, which is marketed for blood sugar control and weight reduction, also impairs the absorption of thyroid medications. If clients decide to take chromium picolinate, then they ought to take it three to four hours apart from thyroid drugs. Flavonoids in vegetables, fruits, and tea have been shown to have potential cardiovascular benefits. But, high-dose flavonoid supplements can suppress thyroid function. The Natural Standards Database provides a comprehensive list of nutritional supplements with a possible impact on thyroid function, thus taking precautions and coordinating patient care with a knowledgeable practitioner is sensible.
Exercise
A discussion on thyroid disorder and good health is not complete without stressing the importance of physical activity. Lisa Lilienfield, MD, a thyroid disorder specialist in the Kaplan Center for Integrative Medicine in McLean, Virginia, and a certified yoga teacher, is a firm believer in the value of exercise, especially. “With hypothyroid patients, certainly exercise can assist with weight gain, fatigue, and depression. With hyperthyroidism, anxiety and sleep disturbances are so common, and exercise might help regulate both.”
In addition to the obvious impact exercise has on weight and metabolism, a study of patients with Graves’ disease found that a structured exercise plan revealed remarkable improvements in fatigue levels, and significantly more patients have been able to successfully quit taking antithyroid medications with no relapse.
In Conclusion
Celiac disease presents unique challenges as a result of unwanted weight changes, significant cardiovascular disease, and symptoms such as fatigue, mood changes, and gastrointestinal upset, which can hinder the growth of healthful behaviors. It’s vital that dietitians focus when counselling clients on setting goals that are realistic for adjustments and routine exercise. With so many nutrient deficiencies and interactions with medications and nutritional supplements, it will be important for dietitians to coordinate with their clients’ health care team for health outcomes.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Nutrition�Abstract: A number of factors contribute to success in sport, and diet is a key component. An athlete�s dietary requirements depend on several aspects, including the sport, the athlete�s goals, the environment, and practical issues. The importance of individualized dietary advice has been increasingly recognized, including day-to-day dietary advice and specific advice before, during, and after training and/or competition. Athletes use a range of dietary strategies to improve performance, with maximizing glycogen stores a key strategy for many. Carbohydrate intake during exercise maintains high levels of carbohydrate oxidation, prevents hypoglycemia, and has a positive effect on the central nervous system. Recent research has focused on athletes training with low carbohydrate availability to enhance metabolic adaptations, but whether this leads to an improvement in performance is unclear. The benefits of protein intake throughout the day following exercise are now well recognized. Athletes should aim to maintain adequate levels of hydration, and they should minimize fluid losses during exercise to no more than 2% of their body weight. Supplement use is widespread in athletes, with recent interest in the beneficial effects of nitrate, beta-alanine, and vitamin D on performance. However, an unregulated supplement industry and inadvertent contamination of supplements with banned substances increases the risk of a positive doping result. Although the availability of nutrition information for athletes varies, athletes will bene t from the advice of a registered dietician or nutritionist.
Introduction To The Importance & Influence Of Nutrition On Exercise
Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
Evidence supports a range of dietary strategies in enhancing sports performance. It is likely that combining several strategies will be of greater bene t than one strategy in isolation.5 Dietary strategies to enhance performance include optimizing intakes of macronutrients, micronutrients, and fluids, including their composition and spacing throughout the day. The importance of individualized or personalized dietary advice�is becoming increasingly recognized,6 with dietary strategies varying according to the individual athlete�s sport, personal goals, and practicalities (eg, food preferences). �Athlete� includes individuals competing in a range of sport types, such as strength and power (eg, weight-lifting), team (eg, football), and endurance (eg, marathon running). The use of dietary supplements can enhance performance, provided these are used appropriately. This manuscript provides an overview of dietary strategies used by athletes, the efficacy of these strategies, availability of nutrition information to athletes, and risks associated with dietary supplement intake.
Review Of Diet Strategies Employed By Athletes
Maximizing Muscle Glycogen Stores Prior To Exercise
Carbohydrate loading aims to maximize an athlete�s muscle glycogen stores prior to endurance exercise lasting longer than 90 minutes. Benefits include delayed onset of fatigue (approximately 20%) and improvement in performance of 2%�3%.7 Initial protocols involved a depletion phase (3 days of intense training and low carbohydrate intake) followed by a loading phase (3 days of reduced training and high carbo- hydrate intake).8,9 Further research showed muscle glycogen concentrations could be enhanced to a similar level without the glycogen-depletion phase,10 and more recently, that 24 hours may be sufficient to maximize glycogen stores.11,12 Current recommendations suggest that for sustained or intermittent exercise longer than 90 minutes, athletes should consume 10�12 g of carbohydrate per kg of body mass (BM) per day in the 36�48 hours prior to exercise.13
There appears to be no advantage to increasing pre- exercise muscle glycogen content for moderate-intensity cycling or running of 60�90 minutes, as signi cant levels of glycogen remain in the muscle following exercise.7 For exercise shorter than 90 minutes, 7�12 g of carbohydrate/kg of BM should be consumed during the 24 hours preceding.13 Some14,15 but not all16 studies have shown enhanced performance of intermittent high-intensity exercise of 60�90 minutes with carbohydrate loading.
Carbohydrate eaten in the hours prior to exercise (com- pared with an overnight fast) has been shown to increase muscle glycogen stores and carbohydrate oxidation,17 extend cycle time to exhaustion,5 and improve exercise performance.5,18 Specific recommendations for exercise of longer than 60 minutes include 1�4 g of carbohydrate/kg of BM in the 1�4 hours prior.13 Most studies have not found improvements in performance from consuming low glycemic�index (GI) foods prior to exercise.19 Any metabolic or performance effects from low GI foods appear to be attenuated when carbohydrate is consumed during exercise.20,21
Carbohydrate Intake During The Event
Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23
In longer events, carbohydrate improves performance primarily by preventing hypoglycemia and maintaining high levels of carbohydrate oxidation.6 The rate of exogenous carbohydrate oxidation is limited by the small intestine�s ability to absorb carbohydrate.6 Glucose is absorbed by the sodium- dependent transporter (SGLT1), which becomes saturated with an intake of approximately 1 g/minute. The simultaneous ingestion of fructose (absorbed via glucose transporter 5�[GLUT5]), enables oxidation rates of approximately 1.3 g/minute,24 with performance benefits apparent in the third hour of exercise.6 Recommendations reflect this, with 90 g of carbohydrate from multiple sources recommended for events longer than 2.5 hours, and 60 g of carbohydrate from either single or multiple sources recommended for exercise of 2�3 hours� duration (Table 1). For slower athletes exercising at a lower intensity,�carbohydrate requirements will be less due to lower carbohydrate oxidation.6 Daily training with high carbohydrate availability has been shown to increase exogenous carbohydrate oxidation rates.25
The �Train-Low, Compete-High� Approach
The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27
Fat As A Fuel During Endurance Exercise
There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues.
Nutrition: Protein
While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33
Fluid And Electrolytes
The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate.
Hydration requirements are closely linked to sweat loss, which is highly variable (0.5�2.0 L/hour) and dependent on type and duration of exercise, ambient temperature, and athletes� individual characteristics.35 Sodium losses linked to high temperature can be substantial, and in events of long duration or in hot temperatures, sodium must be replaced along with fluid to reduce risk of hyponatremia. 35
It has long been suggested that fluid losses greater than 2% of BM can impair performance,35 but there is controversy over the recommendation that athletes maintain BM by fluid ingestion throughout an event.37 Well-trained athletes who �drink to thirst� have been found to lose as much as 3.1% of BM with no impairment of performance in ultra-endurance events.38 Ambient temperature is important, and a review illustrated that exercise performance was preserved if loss was restricted to 1.8% and 3.2% of BM in hot and temperate conditions, respectively.39
Dietary Supplementation: Nitrates, Beta-Alanine & Vitamin D
Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
BA is a precursor of carnosine, which is thought to have a number of performance-enhancing functions including the reduction of acidosis, regulation of calcium, and antioxidant properties.45 Supplementation with BA has been shown to�2�state; 0.9% improvement in time trials), reduce fatigue, and�augment intracellular carnosine concentration.45 A systematic review concluded that BA may increase power output and working capacity and decrease feelings of fatigue, but that there are still questions about safety. The authors suggest caution in the use of BA as an ergogenic aid.46
Vitamin D is essential for the maintenance of bone health and control of calcium homeostasis, but is also important for muscle strength,47,48 regulation of the immune system,49 and cardiovascular health.50 Thus inadequate vitamin D status has potential implications for the overall health of athletes and performance. A recent review found that the vitamin D status of most athletes reflects that of the population in their locality, with lower levels in winter, and athletes who train predominantly indoors are at greater risk of deficiency.51 There are no dietary vitamin D recommendations for athletes; however, for muscle function, bone health, and avoidance of respiratory infections, current evidence supports maintenance of serum 25-hydroxy vitamin D (circulating form) concentrations of 80�100 nmol/L.51
Diets Specific For Post Exercise
Recovery from a bout of exercise is integral to the athlete�s training regimen. Without adequate recovery of carbohydrate, protein, fluids, and electrolytes, beneficial adaptations and performance may be hampered.
Muscle Glycogen Synthesis
Consuming carbohydrates immediately post exercise to coincide with the initial rapid phase of glycogen synthesis has been used as a strategy to maximize rates of muscle glycogen synthesis. An early study found delaying feeding by 2 hours after glycogen-depleting cycling exercise reduced glycogen synthesis rates.52 However the importance of this early enhanced rate of glycogen synthesis has been questioned in the context of extended recovery periods with sufficient carbohydrate consumption. Enhancing the rate of glycogen synthesis with immediate carbohydrate consumption after exercise appears most relevant when the next exercise session is within 8 hours of the first.53,54 Feeding frequency is also irrelevant with extended recovery; by 24 hours post exercise, consumption of carbohydrate as four large meals or 16 small snacks had comparable effects on muscle glycogen storage.55
With less than 8 hours between exercise sessions, it is recommended that for maximal glycogen synthesis, 1.0�1.2 g/kg/hour is consumed for the first 4 hours, followed by resumption of daily carbohydrate requirements.13 Additional protein has been shown to enhance glycogen�synthesis rates when carbohydrate intake is suboptimal.56 The consumption of moderate to high GI foods post exercise is recommended;13 however, when either a high-GI or low-GI meal was consumed after glycogen-depleting exercise, no performance differences were seen in a 5 km cycling time trial 3 hours later.57
Muscle Protein Synthesis
An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59
Only a few studies have investigated the effect of timing of protein intake post exercise. No significant difference in MPS was observed over 4 hours post exercise when a mixture of essential amino acids and sucrose was fed 1 hour versus 3 hours after resistance exercise.60 Conversely, when a protein and carbohydrate supplement was provided immediately versus 3 hours after cycling exercise, leg protein synthesis increased threefold over 3 hours.61 A meta-analysis found timed post exercise protein intake becomes less important with longer recovery periods and adequate protein intake,62 at least for resistance training.
Dose�response studies suggest approximately 20 g of high-quality protein is sufficient to maximize MPS at rest,63 following resistance,63,64 and after high-intensity aerobic exercise.65 Rate of MPS has been found to approximately triple 45�90 minutes after protein consumption at rest, and then return to baseline levels, even with continued availability of circulating essential amino acids (termed the �muscle full� effect).66 Since exercise-induced protein synthesis is elevated for 24�48 hours following resistance exercise67and 24�28 hours following high-intensity aerobic exercise,68 and feeding protein post exercise has an additive effect,58,64 then multiple feedings over the day post exercise might maximize muscle growth. In fact, feeding 20 g of whey protein every 3 hours was subsequently found to maximally stimulate muscle myofibrillar protein synthesis following resistance exercise.69,70
In resistance training, where post exercise intake of protein was balanced by protein intake later in the day, increased adaptation of muscle hypertrophy resulted in equivocal strength performance effects.71,72 Most studies have not found a subsequent bene t to aerobic performance with post exercise protein consumption.73,74 However, in two�well controlled studies in which post exercise protein intake was balanced by protein intake later in the day, improvements were seen in cycling time to exhaustion75 and in cycling sprint performance.76
Fluids And Electrolyte Balance
Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77
Availability Of Nutritional Information To Athletes At Varying Levels
The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78
Athletes eat several times per day, with snacks contributing to energy requirements.79 Dietary intake differs across sports, with endurance athletes more likely to achieve energy and carbohydrate requirements compared to athletes in weight-conscious sports.79 A review found daily intakes of carbohydrate were 7.6 g/kg and 5.7 g/kg of BM for male and female endurance athletes, respectively.80 Ten elite Kenyan runners met macronutrient recommendations but not guide- lines for fluid intake.81 A review of fluid strategies showed a wide variability of intake across sports, with several factors influencing intake, many outside the athlete�s control.82
Nutrition information may be delivered to athletes by a range of people (dietitians, nutritionists, medical practitioners, sports scientists, coaches, trainers) and from a variety of sources (nutrition education programs, sporting magazines, the media and Internet).83 Of concern is the provision of�nutrition advice from outside various professional�s scope of practice. For example, in Australia 88% of registered exercise professionals provided nutrition advice, despite many not having adequate nutrition training.84 A study of Canadian high-performance athletes from 34 sports found physicians ranked eighth and dietitians, 16th as choice of source of dietary supplement information.85
Risks Of Contravening The Doping Regulations
Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85
Athletes take supplements for many reasons, including for proposed performance benefits, for prevention or treatment of a nutrient deficiency, for convenience, or due to fear of �missing out� by not taking a particular supplement.41
The potential benefits (eg, improved performance) of taking a dietary supplement must outweigh the risks.86,87 There are few permitted dietary supplements available that have an ergogenic effect.87,89 Dietary supplementation cannot compensate for poor food choices.87 Other concerns include lack of efficacy, safety issues (toxicity, medical concerns), negative nutrient interactions, unpleasant side effects, ethical issues, financial expense, and lack of quality control.41,86,87 Of major concern, is the consumption of prohibited substances by the World Anti-Doping Agency (WADA).
Inadequate regulation in the supplement industry (com- pounded by widespread Internet sales) makes it difficult for athletes to choose supplements wisely.41,86,87 In 2000�2001, a study of 634 different supplements from 13 countries found that 94 (14.8%) contained undeclared steroids, banned by WADA.90 Many contaminated supplements were routinely used by athletes (eg, vitamin and mineral supplements).86 Several studies have confirmed these findings. 41,86,89
A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99
In an effort to educate athletes about sports-supplement use, the Australian Institute of Sport�s sports-supplement program categorizes supplements according to evidence�of efficacy in performance and risk of doping outcome.40 Category A supplements have sound evidence for use and include sports foods, medical supplements, and performance supplements. Category D supplements should not be used by athletes, as they are banned or are at high risk for contamination. These include stimulants, pro-hormones and hormone boosters, growth hormone releasers, peptides, glycerol, and colostrum.40
Conclusion
Athletes are always looking for an edge to improve their performance, and there are a range of dietary strategies available. Nonetheless, dietary recommendations should be individualized for each athlete and their sport and provided by an appropriately qualified professional to ensure optimal performance. Dietary supplements should be used with caution and as part of an overall nutrition and performance plan.
Disclosure
The authors report no conflicts of interest in this work.
Kathryn L Beck1 Jasmine S Thomson2 Richard J Swift1 Pamela R von Hurst1
1School of Food and Nutrition, Massey institute of Food Science and Technology, College of Health, Massey University Albany, Auckland, 2School of Food and Nutrition, Massey institute of Food Science and Technology, College of Health, Massey University Manawatu, Palmerston North, New Zealand
Blank
References:
1. Burke LM, Meyer NL, Pearce J. National nutritional programs for the
2012 London Olympic Games: A systematic approach by three different
countries. In: van Loon LJC, Meeusen R, editors. Limits of Human
Endurance. Nestle Nutrition Institute Workshop Series, volume 76.
Vevey, Switzerland: Nestec Ltd; 2013:103�120.
2. Hansen EA, Emanuelsen A, Gertsen RM, S�rensen SSR. Improved
marathon performance by in-race nutritional strategy intervention.
Int J Sport Nutr Exerc Metab. 2014;24(6):645�655.
3. Hottenrott K, Hass E, Kraus M, Neumann G, Steiner M, Knechtle B.
A scientific nutrition strategy improves time trial performance by ?6%
when compared with a self-chosen nutrition strategy in trained cyclists:
a randomized cross-over study. Appl Physiol Nutr Metab. 2012;
37(4):637�645.
4. Jeukendrup AE, Martin J. Improving cycling performance: how should
we spend our time and money. Sports Med. 2001;31(7):559�569.
5. Wright DA, Sherman WM, Dernbach AR. Carbohydrate feedings
before, during, or in combination improve cycling endurance
performance. J Appl Physiol (1985). 1991;71(3):1082�1088.
6. Jeukendrup A. A step towards personalized sports nutrition: carbohydrate
intake during exercise. Sports Med. 2014;44 Suppl 1:
S25�S33.
7. Hawley JA, Schabort EJ, Noakes TD, Dennis SC. Carbohydrateloading
and exercise performance. An update. Sports Med. 1997;24(2):
73�81.
8. Bergstr�m J, Hermansen L, Hultman E, Saltin B. Diet, muscle glycogen
and physical performance. Acta Physiol Scand. 1967;71(2):140�150.
9. Karlsson J, Saltin B. Diet, muscle glycogen, and endurance performance.
J Appl Physiol. 1971;31(2):203�206.
10. Sherman WM, Costill DL, Fink WJ, Miller JM. Effect of exercise-diet
manipulation on muscle glycogen and its subsequent utilization during
performance. Int J Sports Med. 1981;2(2):114�118.
11. Bussau VA, Fairchild TJ, Rao A, Steele P, Fournier PA. Carbohydrate
loading in human muscle: an improved 1 day protocol. Eur J Appl
Physiol. 2002;87(3):290�295.
12. Fairchild TJ, Fletcher S, Steele P, Goodman C, Dawson B, Fournier PA.
Rapid carbohydrate loading after a short bout of near maximal-intensity
exercise. Med Sci Sports Exerc. 2002;34(6):980�986.
13. Burke LM, Hawley JA, Wong SH, Jeukendrup AE. Carbohydrates for
training and competition. J Sports Sci. 2011;29 Suppl 1:S17�S27.
14. Raman A, Macdermid PW, M�ndel T, Mann M, Stannard SR. The
effects of carbohydrate loading 48 hours before a simulated squash
match. Int J Sport Nutr Exerc Metab. 2014;24(2):157�165.
15. Balsom PD, Wood K, Olsson P, Ekblom B. Carbohydrate intake and
multiple sprint sports: with special reference to football (soccer). Int J
Sports Med. 1999;20(1):48�52.
16. Abt G, Zhou S, Weatherby R. The effect of a high-carbohydrate diet
on the skill performance of midfield soccer players after intermittent
treadmill exercise. J Sci Med Sport. 1998;1(4):203�212.
17. Coyle EF, Coggan AR, Hemmert MK, Lowe RC, Walters TJ. Substrate
usage during prolonged exercise following a preexercise meal. J Appl
Physiol (1985). 1985;59(2):429�433.
18. Neufer PD, Costill DL, Flynn MG, Kirwan JP, Mitchell JB, Houmard J.
Improvements in exercise performance: effects of carbohydrate feedings
and diet. J Appl Physiol (1985). 1987;62(3):983�988.
19. Burke LM, Collier GR, Hargreaves M. Glycemic index � a new tool
in sport nutrition? Int J Sport Nutr. 1998;8(4):401�415.
20. Burke LM, Claassen A, Hawley JA, Noakes TD. Carbohydrate intake
during prolonged cycling minimizes effect of glycemic index of preexercise
meal. J Appl Physiol (1985). 1998;85(6):2220�2226.
21. Wong SH, Chan OW, Chen YJ, Hu HL, Lam CW, Chung PK. Effect of
preexercise glycemic-index meal on running when CHO-electrolyte
solution is consumed during exercise. Int J Sport Nutr Exerc Metab.
2009;19(3):222�242.
22. Burke LM, Maughan RJ. The Governor has a sweet tooth � mouth
sensing of nutrients to enhance sports performance. Eur J Sport Sci.
2015;15(1):29�40.
23. Gant N, Stinear CM, Byblow WD. Carbohydrate in the mouth immediately
facilitates motor output. Brain Res. 2010;1350:151�158.
24. Jentjens RL, Moseley L, Waring RH, Harding LK, Jeukendrup AE.
Oxidation of combined ingestion of glucose and fructose during
exercise. J Appl Physiol (1985). 2004;96(4):1277�1284.
25. Cox GR, Clark SA, Cox AJ, et al. Daily training with high carbohydrate
availability increases exogenous carbohydrate oxidation during endurance
cycling. J Appl Physiol (1985). 2010;109(1):126�134.
26. Bartlett JD, Hawley JA, Morton JP. Carbohydrate availability and
exercise training adaptation: too much of a good thing? Eur J Sport
Sci. 2015;15(1):3�12.
27. Burke LM. Fueling strategies to optimize performance: training high
or training low? Scand J Med Sci Sports. 2010;20 Suppl 2:48�58.
28. Yeo WK, Paton CD, Garnham AP, Burke LM, Carey AL, Hawley JA.
Skeletal muscle adaptation and performance responses to once a day
versus twice every second day endurance training regimens. J Appl
Physiol (1985). 2008;105(5):1462�1470.
29. Morton JP, Croft L, Bartlett JD, et al. Reduced carbohydrate availability
does not modulate training-induced heat shock protein adaptations but
does upregulate oxidative enzyme activity in human skeletal muscle.
J Appl Physiol (1985). 2009;106(5):1513�1521.
30. Horowitz JF, Mora-Rodriguez R, Byerley LO, Coyle EF. Lipolytic suppression
following carbohydrate ingestion limits fat oxidation during
exercise. Am J Physiol. 1997;273(4 Pt 1):E768�E775.
31. Volek JS, Noakes T, Phinney SD. Rethinking fat as a fuel for endurance
exercise. Eur J Sport Sci. 2015;15(1):13�20.
32. Stellingwerff T, Spriet LL, Watt MJ, et al. Decreased PDH activation
and glycogenolysis during exercise following fat adaptation
with carbohydrate restoration. Am J Physiol Endocrinol Metab.
2006;290(2):E380�E388.
33. van Loon LJ. Is there a need for protein ingestion during exercise?
Sports Med. 2014;44 Suppl 1:S105�S111.
34. Hillman AR, Turner MC, Peart DJ, et al. A comparison of hyperhydration
versus ad libitum fluid intake strategies on measures of
oxidative stress, thermoregulation, and performance. Res Sports Med.
2013;21(4):305�317.
35. Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ,
Stachenfeld NS; American College of Sports Medicine. American
College of Sports Medicine position stand. Exercise and fluid
replacement. Med Sci Sports Exerc. 2007;39(2):377�390.
36. Kristal-Boneh E, Glusman JG, Shitrit R, Chaemovitz C, Cassuto Y.
Physical performance and heat tolerance after chronic water loading and
heat acclimation. Aviat Space Environ Med. 1995;66(8):733�738.
37. Noakes TD. Drinking guidelines for exercise: what evidence is there that
athletes should drink �as much as tolerable�, �to replace the weight lost
during exercise� or �ad libitum�? J Sports Sci. 2007;25(7):781�796.
38. Hoffman MD, Stuempfle KJ. Hydration strategies, weight change
and performance in a 161 km ultramarathon. Res Sports Med.
2014;22(3):213�225.
Research suggests that illness recovery and prevention improve when supported by proper nutrition and supplementation. Nevertheless, clinicians don’t often get extensive training in nutrition and nutrient supplements in osteopathic and medical school, a study of pediatric residency interns that were incoming showed.
What’s the importance of nutrition towards health and wellness?
Unsurprisingly, many patients are malnourished, are experiencing record levels of disease, and therefore are likely being treated without learning about other, less invasive but exceptionally effective treatment options.
The Power of Nutrition
When high-quality nutrition is used consistently and efficiently, it may prevent potential chronic disease, enhance cognition in people with dementia, and improve outcomes in patients getting GI and colorectal oncological surgeries, to mention a few. In addition, nutrition support is associated with length of stays and infectious complications.
Integrative and functional medicine practitioners, specialists of any discipline certified in integrative and functional medicine, are educated healthcare providers, qualified and experienced on how best to use functional nutrition to effectively prevent and even reverse chronic illness, such as fibromyalgia, as well as to support general health and wellness. Functional nutrition aims at addressing the imbalances in the body by restoring proper function through food, lifestyle and supplement interventions, restoring a patients’ health and improving the patients’ outcomes.
To get started learning about functional nutrition, many healthcare professionals learn the basics of the way functional nutrition helps their patients through an extended series of specialized courses and training. Some integrative and functional medicine resources may contains over 10 food programs which could be personalized depending on the individual condition and the patient, to provide a personalized treatment experience.
When Standard Diets Don’t Work
Despite recent improvements in nutrigenomics, the thought that a given food is going to have precisely the same impact for all individuals is still widespread. A recent study found that after ingesting identical foods, blood sugar levels could vary by up to 20 percent in the exact same person and up to 25 percent across individuals.
Likewise, another study demonstrated that individuals may have radically different sugar responses to the exact same meal. Using continuous glucose monitoring and meals that were standardized, the investigators found that identical meals led to physiologic outcomes. As a result, any strategy that grades dietary components either “good” or “poor” based on their typical postprandial glycemic responses (PPGRs) will be of small use to the respective patient.
In contrast, the exciting and relatively new field of metabolomics is now being applied in nutrigenomics research. Because the molecules which vary between meals are identified by metabolomics, researchers guess it could be utilized to determine biomarkers of disease risk and also to track effects of foods for more efficient treatment.
In an era in which more personalized data is accessible than ever before, healthcare professionals can attain incredible outcomes by using this emerging study to evaluate and treat patients according to their individual needs. But how do you develop a framework for customizing therapy programs that takes into consideration all data that is applicable?
The Institute for Functional Medicine’s foundational five-day course, Applying Functional Medicine in Clinical Practice (AFMCP), for example, joins practitioners to personalized tests and clinical instruments which can be tailored to each individual’s particular physiology, including genetics, lifestyle, and readiness to change. A variety of specialized integrative and functional medicine training programs provides healthcare professionals the tools to prescribe effective treatment programs customized to individual patients’ needs across the spectrum.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Clinicians recognize that lifestyle changes can be difficult for patients. Research is currently helping us understand what patients actually need to have in order to produce effective and sustainable changes in their diet and physical activity.
How is nutrition and exercise effective for well-being?
Two intervention studies suggest direct access to healthy food enhance emotional well-being and metabolism respectively. When patients with chronic disease learn by performing lifestyle modification behaviors, even over a brief period of time, both their well-being and wellness improve.
Nutrition & Exercise Research Study
At a randomized controlled trial over a two-week interval, researchers investigated the effects of giving a group of young people a $10 voucher for fruits and vegetables and twice per day text-reminders versus giving yet another group of young people received the real fruits and vegetables worth $10 with no reminders.
Despite both classes consuming relatively the same amount of fruits and vegetables, such as a greater amount than ordinary even, only the group who had been given fruits and veggies flourished and showed improvements in their vitality and motivation. This study suggests that direct access to healthy food might be necessary for successful dietary modification, even if the clinician is providing “high-touch” support. Quite simply, clinicians might wish to think about exploring their patients’ access to standard meals prior to giving them other tools to help them eat better.
In a different study, over a 12-week period, a randomized controlled trial of 24 breast cancer survivors split them to either a fitness program or a management group instructed to continue their regular exercise routines. The exercise group saw increased muscle strength and endurance, as well as decreased body fat percentage, waist circumference, visceral fat area, insulin levels, leptin/adiponectin ratios, and DKK1 and SFRP1 levels. The researchers indicate that DKK1 and SFRP1 may be useful biomarkers to ascertain both long-term exercise’s advantages along with the prognosis of patients. In addition they suggest exercise might have a therapeutic advantage in those with chronic illnesses.
Fortunately, many integrative and functional medicine practitioners find innovative methods to place new science into practice, and new programs make it possible for clinicians to apply the results from studies such as these right away from the clinic. Many integrative and functional medicine practitioners offer a toolkit containing more than 200 items that help enhance patient compliance to professionals. General ill-being and chronic disorder decreases, when patients learn lifestyle modification behaviors.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
You’ve perhaps heard of functional medicine, the medical care strategy that requires a “systems” perspective of health by focusing on the sources of dysfunction in the body as well as also the interactions among genetic, environmental and lifestyle factors. Functional nutrition fits within this framework to analyze how food “functions” inside our own bodies to both provide nourishment but also to influence the body’s health (or disease) itself.
Beyond basic fuel, how does food help generate health each day?
Food is one of the most basic and potent inputs we provide our bodies, a clear and impactful message to our biochemistry. It’s one of several links between our internal and external environments. More than two thousand decades ago, the Greek physician Hippocrates offered the famous quote, “Let medicine be thy food and thy food be thy medicine.” Now it is a rallying cry for supporters of food nourishment. What should this mean for you?
Nutrition as a Part of Functional Medicine
If it comes to health care, too often we put energy, time and cash. We’ll never envision optimal health and well-being at this route. When we get to the underlying causes of our physical dysfunction (e.g. insulin resistance, high blood pressure, inflammatory conditions), we suddenly gain a panoramic view of what feeds (sometimes actually speaking) our dysfunction and that which, consequently, can nourish or excite it toward optimal operation.
Functional nutrition at its best both examines the balance of our personal dietary landscape to see how well we’re nourishing our bodies’ needs and targets specific foods that might have especially potent impact to tackle the delicate and not-so-subtle dysfunctions that we harbor.
As an example, if you have an inflammatory condition or your blood markers reveal higher than normal inflammatory amounts, you will not only need to be sure to steer clear of inflammation-promoting foods but also make the most of this anti-inflammatory effectiveness of certain foods (e.g. turmeric, omega-3’s found in fatty fish and caliber omega nutritional supplements, cruciferous vegetables, berries, etc.). Functional nutrition emphasizes that specific decisions can function to your own personal benefit and that your nutrition should get the job done for you.
Goals of Functional Nutrition
Functional nutrition should enhance your health status, improve vitality, satiety, and ability to heal from injury or illness. When our choices start to include fresh, fibrous, and minimally processed foods, our dietary patterns start to work in our favor in many respects when compared to diets of highly-processed, nutrient-poor foods. From there, proper individualized recommendations might help us incorporate targeted/therapeutic food choices that are additional.
Functional nutrition should foster resilience in spite of numerous challenges we experience as we age and accumulate stresses (i.e. physical and psychological decline, sleep deprivation, various kinds of psychological distress). Age-related functional decline is an inevitable part of the human life cycle. In the last few generations we’ve seen some of the biggest gains in average population life expectancy along with the fastest increases in debilitating chronic disease observed. For people to satisfy their quests to live a ‘better-than-average’ lifetime, they must stay more resilient than ever in the surface of the multiple stressors modern life gifts. Quality nutrition helps us avoid these conditions, and Practical Nutrition guidance/therapy can help us manage them or dial them back if we affected.
Maybe most powerful, comprehending functional nutrition can help us realign our relationship with food. When we think about food as medicine, our paradigm on eating may change. We can better appreciate the impact of our daily choices. We can examine the backdrop of these options with a different view we make the decisions we do. The range broadens to real life program, how functional nutrition can fit inside our lifestyle performance.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
 Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23
Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23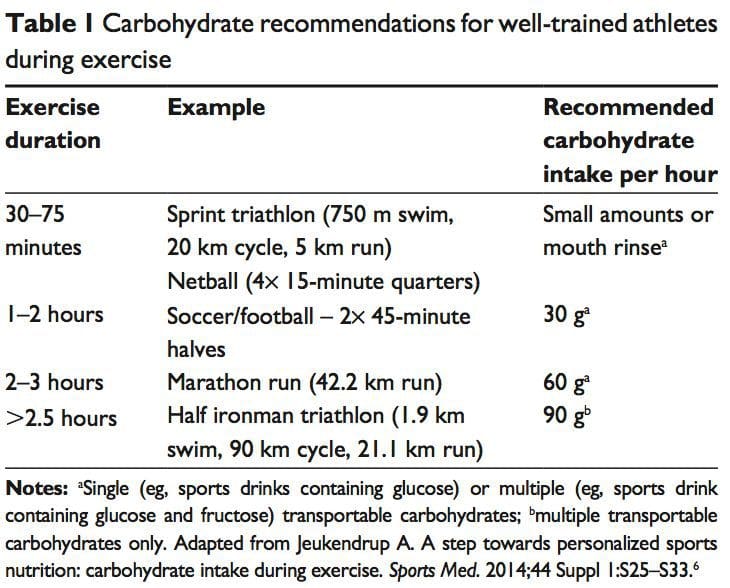
 The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27
The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27 There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues.
There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues. While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33
While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33 The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate.
The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate. Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
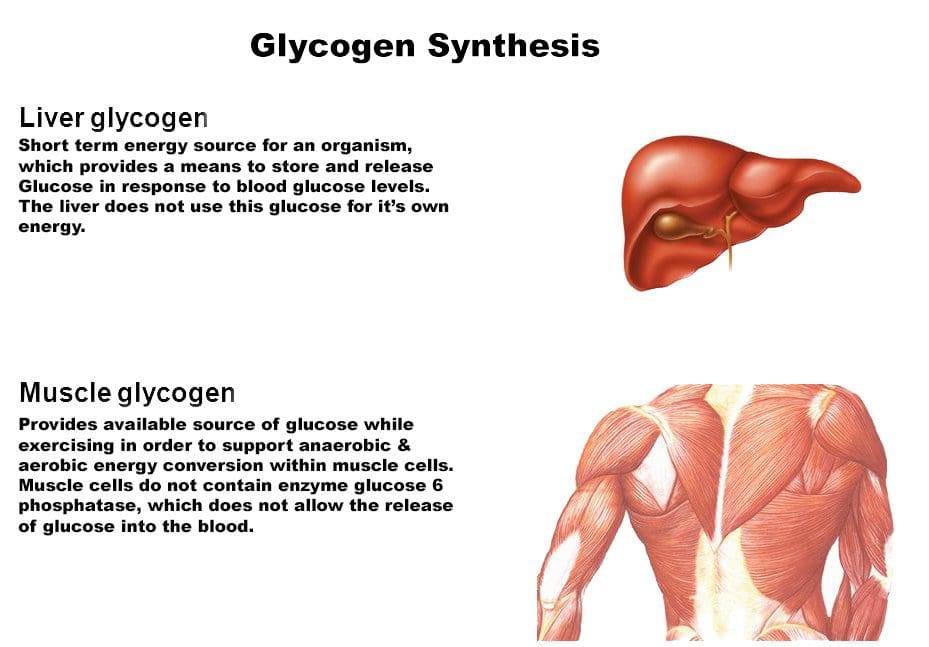 Consuming carbohydrates immediately
Consuming carbohydrates immediately  An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59
An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59 Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77
Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77 The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78
The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78 Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85
Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85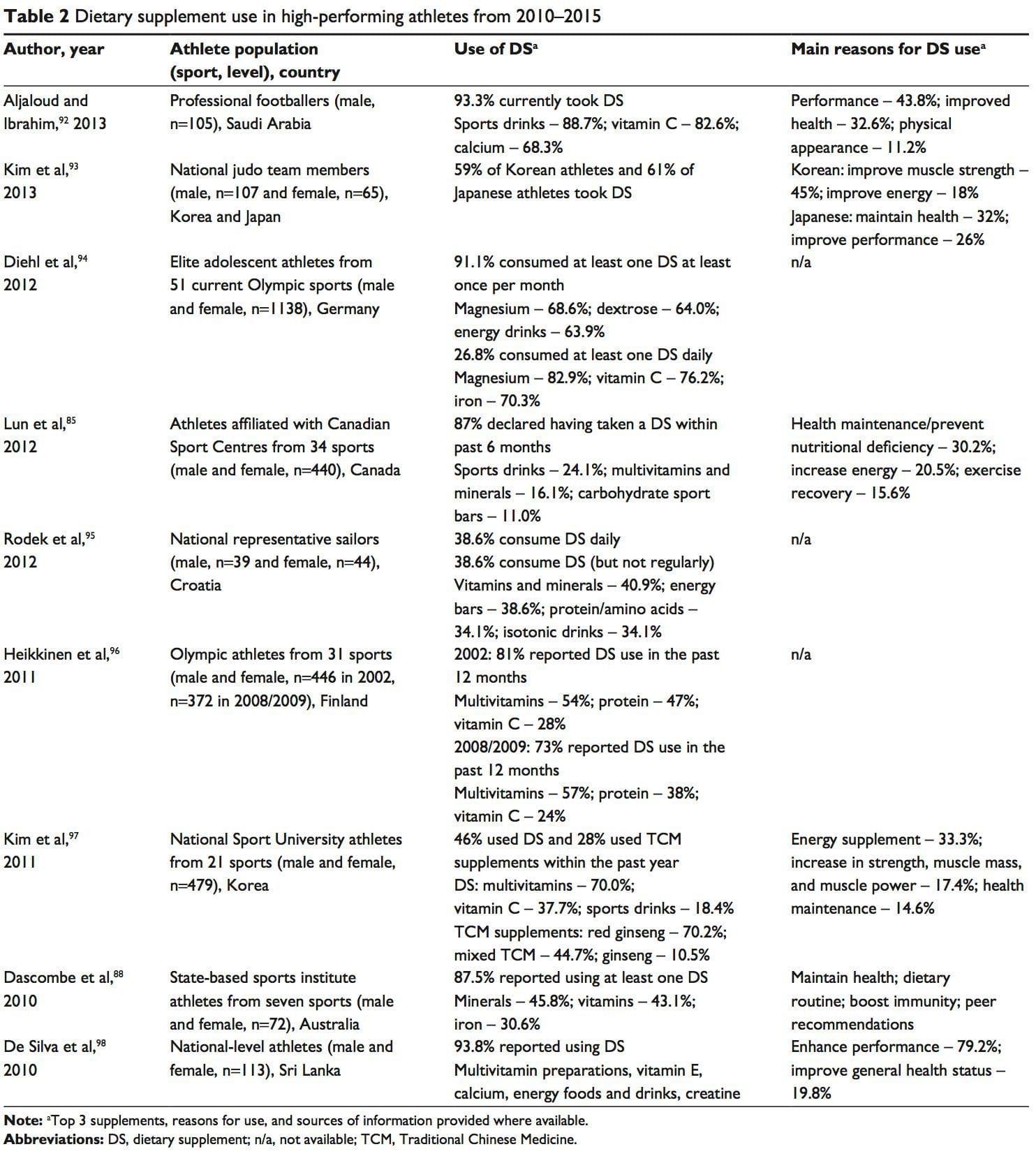 A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99
A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99









