Alzheimer�s disease (AD) is one of the most common types of dementia among older adults. Research studies have demonstrated that pathological changes in the human brain, whether directly or indirectly, can ultimately cause loss of synaptic function, mitochondrial damage, microglial cell activation, and neuronal cell death. However, the pathogenesis of AD is not yet fully understood and there is currently no definitive treatment for the neurological disease. Research studies have demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. �
A proinflammatory status of the central nervous system (CNS) can also cause changes in the function of the microglial cells or microglia. Neuroinflammation is closely associated with the activation of microglia and astrocytes which are connected to a variety of neurological diseases by the synthesis and secretion of inflammatory mediators such as iNOS, ROS, and proinflammatory cytokines. According to research studies, microglial priming is also caused by the inflammation of the CNS. �
Therefore, whether microglial priming is the result or the cause of neuroinflammation is still controversial. Microglial cell activation commonly causes an increase of A? and tau proteins as well as a decrease of neurotrophic factors, ultimately leading to the loss of healthy brain cells or neurons and the development of neuritic plaques and neurofibrillary tangles which are closely associated with AD. With the progression of Alzheimer’s disease, changes from neuronal dysfunctions which may have no obvious symptoms to memory loss and cognitive impairment may become more noticeable. �
Microglial Priming, Neuroinflammation, and AD
Although the accurate and detailed, fundamental role of the microglial cells continues to be discovered and explained, there is a consensus among many researchers that primed microglia are associated with the inflammatory response of the CNS in AD. It has also been determined that neuroinflammation caused by microglial priming is mainly associated with aging, systemic inflammation, gene regulation, and blood-brain barrier impairment. The purpose of the article below is to discuss how microglial priming and neuroinflammation in Alzheimer’s disease can be caused due to a variety of risk factors. �
Aging
Aging is considered to be one of the main risk factors for AD and it is generally followed by chronic, systemic up-regulation of pro-inflammatory factors and a considerable decrease in an anti-inflammatory response. This change from homeostasis to an inflammatory state occurs through age-related elements which cause an imbalance between anti-inflammatory and pro-inflammatory systems. Microglia is primed into an activated state which can increase the consistent neuroinflammation and inflammatory reactivity in the aged human brain. Research studies have demonstrated that microglia in the brain of rodents developed an activated phenotype during aging characterized by the increased expression of CD11b, CD11c, and CD68. �
Systemic Inflammation
Recent research studies have determined that the neuroinflammation from primed microglial cells can also cause the pathogenesis of AD. Continuous activation of microglia can promote the synthesis and secretion of pro-inflammatory cytokines and trigger a pro-inflammatory response, ultimately causing neuronal damage. Neuroinflammation is an early symptom in the progression of AD. The microglia can have a tremendous effect on the inflammation of the human brain. �
The inflammation and health issues of the CNS can be associated with systemic inflammation through molecular pathways. One research study demonstrated that ROS development of primed microglia decreases the levels of intracellular glutathione and increases nitric oxide in NADPH oxidase subunit NOX2. Moreover, researchers demonstrated that these simultaneously occurring processes ultimately cause the development of more neurotoxic peroxynitrite. This is demonstrated in rodents with peripheral LPS or proinflammatory cytokines, such as TNF-?, IL-1?, and IL-6, IL-33. �
The outcome measures of numerous research studies have demonstrated that systemic inflammation can cause microglial activation. The results of the research studies emphasize the variability of the inflammatory response in the human brain associated with AD and the underlying health issues associated with systemic inflammation and neuroinflammation, as shown in Table 1. MAPK (mitogen-activated protein kinase) signaling pathways regulate mechanisms of the eukaryotic cell and microglial MAPK can also cause an inflammatory response to the aged brain with AD. Furthermore, chronic or continuous systemic inflammation causes neuroinflammation, resulting in the onset and accelerating the progression of AD. �
�
Genetic Regulation
In the aging human brain, gene regulation has ultimately been associated with an innate immune response. Recent preclinical, bioinformatics, and genetic data have demonstrated that the activation of the brain immune system is associated with the pathology of AD and causes the pathogenesis of this neurological disease. Genome-wide association studies (GWAS), functional genomics, and even proteomic evaluations of cerebrospinal fluid (CSF) and blood have demonstrated that dysfunctional immune pathways from genic mutation are risk factors in LOAD, which is the vast majority of AD. �
GWAS have become a fundamental tool in the screening of genes as well as demonstrating several new risk genes associated with AD. Apolipoprotein E (APOE) ?4allele is one of the most considerable and well-known risk genes for sporadic AD and this mutation ultimately increases the risk of neurological disease onset by 15 times in homozygous carriers and by three times in heterozygous carriers. Further research studies have demonstrated how microglial cell function can be affected through a variety of rare mutations which have demonstrated to have an increased risk factor of Alzheimer’s disease. �
An extracellular domain mutation of the TREM2 gene has also demonstrated an almost identical extent with APOE?4 in increasing the risk factor of AD. TREM2 is increasingly demonstrated on the surface of microglia and mediates phagocytosis as well as the removal of neuronal debris. Additionally, several other genes, such as PICALM, Bin1, CLU, CR1, MS4A, and CD33 have been demonstrated as risk genes for AD. Most of the risk mutation genes are expressed by microglial cells. �
Blood-Brain Barrier (BBB) Impairment
The blood-brain barrier (BBB) is a specialized barrier commonly developed between the blood and the brain by tight liner sheets consisting of specific endothelial cells and tight junctions or structures which connects a variety of cells together. The CNS is fundamental for the human body, and the BBB is fundamental for the CNS. The BBB and the blood-nerve barrier develop a defense system to control the communications of cells and soluble factors between blood and neural tissue where it plays a considerable role in maintaining and regulating the homeostasis of the CNS and peripheral nervous system. �
With development, continuous inflammation can also cause damage to the BBB. This damage can ultimately cause loss of hypersensitive neurons, neuroinflammatory regions, and focal white matter impairment following the damage. The compromised BBB also allows more leukocytes to enter into the CNS where an immune response can be aggravated by brain microglia under the condition of peripheral inflammation. These processes may ultimately be under the control of chemokine and cytokine signaling which can also have an effect on brain microglial cells as well as other health issues in AD. �
By way of instance, it has been determined that TNF-?, IL-17A, and IL-1? can reduce the tight junctions and eliminate the BBB. Loss of BBB integrity and abnormal expression of tight junctions are associated with neuroinflammation. Several research studies also demonstrated in an animal model of AD that the vulnerability of BBB to inflammation increases. Current evidence has also demonstrated that the BBB integrity is fundamental while further evidence of the BBB may demonstrate a new treatment approach for AD associated with microglial priming as shown in Figure 2 below. �
�
Conclusion
Microglia play a fundamental role in maintaining and regulating the homeostasis of the CNS’s micro-environment. If the balance of the homeostasis of the human brain is interrupted, the microglial cells can be activated to restore the balance in the CNS by defending against the stimulation and protecting the structure and function of the brain. However, chronic and continuous stimulation can trigger microglia into a state known as microglial priming, which is more sensitive to potentially minor stimulation, causing a variety of health issues, such as central sensitization, chronic pain, and fibromyalgia. �
Microglial priming mainly causes the boost of A?, tau protein as well as neuroinflammation and reduces neurotrophic factors which can cause the loss of healthy brain cells or neurons as well as the development of neuritic plaques and neurofibrillary tangles which are associated with Alzheimer’s disease. Although this �double-edged sword� plays a fundamental role, it can increase the progression of abnormal protein development and aggravate neuronal loss and dysfunction. However, research studies have ultimately demonstrated that aging can cause the progression of AD and there’s not much we can do about it. �
Microglial cells play a fundamental role as the protectors of the brain and they ultimately help maintain as well as regulate the homeostasis of the CNS microenvironment. However, continuous stimulation can cause the microglia to trigger and activate at a much stronger state which is known as microglial priming. Once the microglial cells go into protective mode, however, primed microglia can become much more sensitive to even minor stimulation and they have a much stronger possibility of reacting towards normal cells. Microglial priming has been associated with neuroinflammation and Alzheimer’s disease (AD) as well as central sensitization and fibromyalgia. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
AD is one of the most common types of dementia among older adults. However, the pathogenesis of AD is misunderstood and there is no definitive treatment for the neurological disease. Research studies have ultimately demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS by changing their morphology, phenotype and function. In an average physiological state, the microglial cells are continuously in charge of controlling their environment. �
However, when the homeostasis of the brain is interrupted, the microglia change into an amoeba-like shape and become a phagocyte where they can actively reveal a variety of antigens. If the homeostasis interruption in the CNS continues, the microglial cells will then trigger at a much stronger state, which is known as microglial priming. Microglia are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �
�
Microglial priming can become a double-edged sword. As a matter of fact, primed microglia are created from different phenotypes of microglia and the phenotypes are context-dependent, which means they are associated to the sequence and duration of their exposure to different varieties of stimulation in a variety of pathologies. In the article below, we will demonstrate the effect of microglial priming on the central nervous system (CNS), especially in neurological diseases. �
Role of Microglial Cells in the CNS
Microglial cells are commonly found in the central nervous system (CNS), where they are considered to be one of the most flexible types of brain cells. Microglial cells are created from precursor cells found within mesoderm bone marrow, or more specifically found in the mesodermal yolk sac, and they are divided in different densities throughout several regions of the brain. As mentioned above, microglia will remain in a dormant state when the homeostasis of the brain remains stable. �
Microglia have a small cell body and morphological branches which extend towards all directions to help maintain and regulate the overall function of the CNS. Changes in their microenvironment can trigger microglia into an “activated� state. Research studies have demonstrated that microglia play a fundamental role in brain development and a variety of functions, including synaptic pruning and clearing out cell debris. Moreover, microglia create an immune surveillance system in the human brain and control fundamental processes associated with a variety of pathologies, including the clearance and uptake of A? and abnormal tau protein as well as the production of neurotrophic factors and neuroinflammatory factors. �
Microglial Priming Overview
Microglial priming activates when continuous interruptions in the brain’s microenvironment trigger a much stronger microglial response compared to an initial interruption which simply triggers microglial activation. Primed microglia in the CNS are also much more sensitive to possibly minor stimulation. This increased response involves microglial proliferation, morphology, physiology, and biochemical markers or phenotype. However, these changes will ultimately promote an increase in cytokines and inflammation mediator production which can have a tremendous impact on synaptic plasticity, neuronic survival, individual cognitive and behavioral function. Below is an overview of the effects of microglial priming in the CNS. �
Mechanisms of Microglial Priming in the CNS
The microenvironment of the central nervous system (CNS), by way of instance, is one of the main factors which can affect the microglial cells. Increased oxidative stress, lipid peroxidation and DNA damage associated with brain aging can all commonly trigger microglial priming. Another common factor for microglial priming includes traumatic brain injury. Research studies have shown that traumatic CNS injury activates microglia as well as the development of primed microglia. �
Many research studies have also shown that both focal and diffuse traumatic brain injury increase inflammation in the brain associated with microglia and astrocytes. CNS infections can also trigger microglial priming where viruses are the main cause of CNS infection. Both DNA and RNA viruses can trigger microglial priming including microglia and astrocytes. Recent research studies have shown that complement dysfunction can change the expression of complement receptors and trigger microglial priming after continuous activation following a variety of functions, including synapse maturation, immune product clearance, hematopoietic stem/progenitor cells (HSPC) mobilization, lipid metabolism, and tissue regeneration. �
Moreover, research studies have shown that there is increased priming of the microglia in a variety of neurological diseases. By way of instance, microglial cells with a morphological phenotype are found in large numbers in the human brain. In the last several years, research studies have suggested that neuroinflammation can continuously activate the microglia and trigger microglial priming. Furthermore, all of the previously mentioned situations are closely associated with neuroinflammation. Research studies have also demonstrated that neuroinflammation, as well as microbial debris and metabolic effects, are associated with central sensitization in neurological diseases, such as fibromyalgia, also referred to as the “brain on fire”. �
In the context of the previous situations mentioned above, microglia are primed though a series of pro-inflammatory stimulation, such as lipopolysaccharide (LPS), pathogenetic proteins (e.g., A?), ?synuclein, human immunodeficiency virus (HIV)-Tat, mutant huntingtin, mutant superoxide dismutase 1 and chromogranin A. There is also a variety of signaling pathways and it is common for different types of cells to express special pattern recognition receptors (PRRs) which can affect inflammatory signaling pathways. By way of instance, several signaling pathways, known as pathogen-associated molecular patterns (PAMPs), which can commonly increase in infected tissue, could also control microbial molecules. �
Additionally, peptides or mislocalized nucleic acids identified as misfolded proteins through a series of pathways, known as danger-associated molecular patterns (DAMPs), can also cause microglial priming. Toll-like receptors (TLRs) and carbohydrate-binding receptors commonly function in these pathways. There are also many different receptors found in microglia, including triggering receptors expressed on myeloid cells (TREM), Fc? receptors (Fc?Rs), CD200 receptor (CD200R), receptor for advanced glycation end products (RAGE), chemokine receptors (CX3CR1, CCR2, CXCR4, CCR5, and CXCR3), which can be recognized and mixed in with other signaling pathways, although some pathways are still not clear. �
Consequences of Microglial Priming in the CNS
Microglia show a low rate of mitosis in their normal state and a high rate of proliferation after microglial priming, showing that the microglia have the ability to affect cell turnover and pro-inflammation stimulation. With continued stimulation, microglia activate from their resting state, changing into amoeboid microglial cells in morphology. However, the changes in the shape of the microglia cannot differentiate the characteristics of microglial activation and the function of primed microglia depends on their phenotypes which are associated with receptors and molecules which they create and recognize. �
The different types of tissue macrophages, under microenvironmental impetus, are able to differentiate M1 and M2 phenotypes. First, M1 polarization, also known as classical activation, ultimately needs interferon-? (IFN-?) to be mixed with TLR4 signaling which then causes the production of inducible nitric oxide synthases (iNOS), reactive oxygen species (ROS), proinflammatory cytokines, and finally, ultimately reduces the release of neurotrophic factors, ultimately causing inflammation with increased markers of main histocompatibility complex II (MHC II), interleukin-1? (IL-1?) and CD68. �
Moreover, M2 polarization, also known as alternative activation, is ultimately believed to be associated with tissue-supportive in the situation of wound healing, reducing inflammation and improving tissue repair of collagen form. They trigger in response to IL-4 and IL-13 in vivo. M2 polarization is characterized by the increased expression of neurotrophic factors, proteases, enzymes arginase 1 (ARG1), IL-10 transforming growth factor-? (TGF-?), scavenger receptor CD206 and coagulation factors as well as improving phagocytic activity. As a matter of fact, there are currently no clear boundaries between the two polarizations and the M1 phenotype shares many similar characteristics with the M2 phenotype. �
Another phenotype of primed microglia, known as acquired deactivation, has been recently discovered. This new phenotype overlaps with M2 and has the ability to improve anti-inflammatory and functional recovery. Additionally, a research study conducted ultra-structural analyses and identified a brand-new phenotype, known as �dark microglia�, which is rarely seen in the microglial cell’s resting state. Systemic inflammation triggers microglia into an activated state to promote cell and tissue recovery and achieve homeostasis. Microglial priming is ultimately the second interruption in the CNS microenvironment. �
The primed microglia is a double-edged sword for brain health. Many research studies in vivo and in vitro have shown that neurological diseases are associated with microglial activation. The inflammatory phenotypes of the microglia create neurotoxic factors, mediators and ROS which can affect the CNS. Primed microglia play a fundamental and beneficial role in neuronal regeneration, repair, and neurogenesis. Primed microglia are also much more sensitive and respond much stronger to brain injury, inflammation, and aging as well as increase the activation of microglial cells by switching from an anti-inflammation, potentially protective phenotype to a pro-inflammation destructive phenotype, as shown in (Figure 1). �
�
In the early stages of microglial priming, the ability and function to phagocytize cell debris, misfolded proteins, and inflammatory medium are increased where more protective molecules, such as IL-4, IL-13, IL-1RA, and scavenging receptors, are created. The changes can affect wound healing and damage tissue repairment, neuron protection, and homeostasis recovery. Classically activated microglia (M1) make up a large proportion of all microglia and promote an increased creation of neurotoxic factors, such as IL-1?, TNF-?, NO and H2O2 (6), where more microglia are primed immediately afterward. �
This increased and extended neuroinflammation caused by primed microglia can ultimately be associated with the development and clustering of the protein tau and A?. Furthermore, it can lead to loss of neurons as well as the decrease of cognitive function and memory, such as in Alzheimer’s disease. Although the mechanisms are not clear enough, people have reached an agreement that primed microglia cause a chronic proinflammatory response and a self-perpetuating cycle of neurotoxicity. And this is believed to be the key factor in brain health issues resulting in neurological diseases. �
Microglia are known as the protectors of the brain and they play a fundamental role in maintaining as well as regulating the homeostasis of the CNS microenvironment. Constant stimulation causes the microglia to trigger at a much stronger state, which is known as microglial priming. Microglial cells are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download�
* All of the above XYMOGEN policies remain strictly in force.
Central nervous system, or CNS, infections can be life-threatening if they are not diagnosed and treated early. Because CNS infections are non-specific, determining an accurate diagnosis can be challenging. The nucleic acid in vitro amplification-based molecular methods are starting to be utilized for routine microbial diagnosis. These molecular methods have improved beyond conventional diagnostic techniques with increased sensitivity and specificity. Moreover, molecular methods utilized on cerebrospinal fluid samples are considered the new standard for diagnosis of CNS infections caused by pathogens. �
Molecular methods for the diagnosis of CNS infections offers a variety of monoplex and multiplex PCR assays to diagnose several types of health issues. Pan-omic molecular platforms can also help diagnose CNS infections. Although molecular methods are utilized for the diagnosis of CNS infections, the outcome measures for these diagnostic techniques must be carefully identified by healthcare professionals. The following article discusses conventional diagnostic techniques and molecular methods utilized for the diagnosis of central nervous system infections, their application, and future approaches. �
Molecular Methods in the Diagnosis of CNS Infections
Because of increased sensitivity and specificity, nucleic acid in vitro amplification-based molecular methods has tremendously improved the ability to diagnose CNS infections in a reasonable and effective time frame. Several PCR-derived techniques have also ultimately increased the flexibility and rigor of currently available diagnostic techniques. �
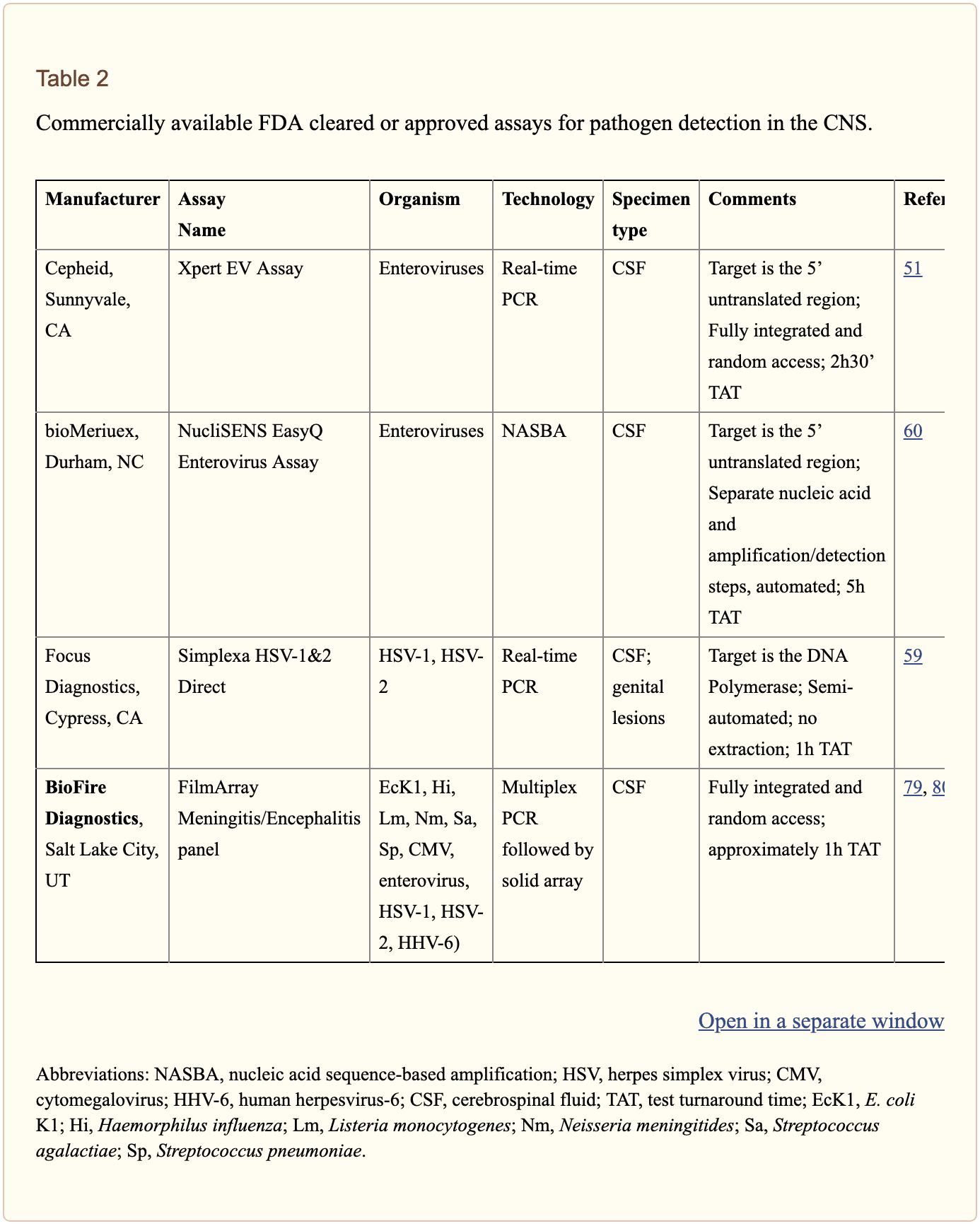
Reverse transcriptase, or RT,-PCR was developed to increase RNA targets. Its utilization plays a fundamental role in the diagnosis of RNA-virus infections as well as managing their reaction to treatment. Timely access to enterovirus RT-PCR outcome measures has demonstrated shorter hospital stays, reduced unnecessary antibiotic utilization, and decreased ancillary laboratory evaluations and tests. Broad-range rRNA PCR techniques, which utilize a single pair of primers targeting conserved regions of genes, have been utilized to diagnose bacterial pathogens and herpes viruses in the CSF. Isothermal amplification-based techniques. including loop-mediated isothermal amplification or LAMP, have been developed to offer a diagnosis within several minutes to hours. Table 2 demonstrates commercial molecular in vitro diagnostic devices, or IVD, which have been cleared by the US Food and Drug Administration, or FDA, for diagnosis of microbial pathogens in CSF. �
Monoplex Assays
A conventional molecular method involves three phases: sample extraction, target nucleic acid amplification, and amplicon detection. One of the first molecular assays successfully utilized for the diagnosis of CNS infections was utilized for the diagnosis of HSV in cerebrospinal fluid or CSF. PCR became the test of choice when research studies demonstrated that CSF PCR was similar to culture of brain tissue for diagnosis of HSV encephalitis and meningitis. Many PCR based methods for the diagnosis of herpes and enteroviruses have become available with increased sensitivity compared to viral culture. �
Real-time PCR with nucleic acid amplification and amplicon detection further improved the transition to molecular methods in clinical laboratories. Unlike conventional PCR, the real-time system is a �closed� system and it overcomes the fundamental problem of carryover contamination. At the time of manuscript preparation, three molecular assays utilized to help diagnose HSV and enteroviruses in CSF have ultimately been approved by the FDA as demonstrated in Table 2 of the previous article. � Real-time PCR-based methods are the main diagnostic technique utilized to help diagnose the Zika virus, which was first reported in Uganda in 1947, and is now a worldwide concern after the virus spread widely in Brazil and Central America. Research studies developed a one-step RT-PCR assay utilized to diagnose the Zika virus in human serum with a limited detection of 7.7pfu/reaction. Along with plasma, the Zika virus RNA can be diagnosed through urine and plasma within the first 2 weeks after symptoms have manifested. In March 2016, the FDA approved a trioplex-PCR assay under emergency use authorization for the simultaneous diagnosis of Zika, Chikungunya, and Dengue viruses in serum, urine, CSF and amniotic fluid. The RT-PCR assay utilizes dual labeled hydrolysis probes with a LOD of 1.54�10 4 GCE/ ml of Zika virus in serum. �
Introduction of real-time PCR based diagnostic assays have affected early and effective diagnosis of several bacterial infections. Isothermal amplification-based molecular assays have excellent performance characteristics and they don’t require any specialized equipment. These assays are fundamental for the utilization of on or near point-of-care testing. LAMP-based methods have been utilized to diagnose Neisseria meningitis, Streptococcus pneumoniae, Haemophilus influenzae type b, M. tuberculosis, and JEV in the CSF. The Xpert MTB/RIF assay has tremendously improved regulation of tuberculosis by offering an integrated and automated system which allows quick clinical decision making in a POC or near-care context. Several research studies have utilized the Xpert MTB/RIF to evaluate the diagnosis of M. tuberculosis in CSF from TB meningitis. In a meta-analysis of thirteen research studies, the pooled sensitivity of the Xpert assay was 80.5 percent, or 95 percent CI 59.0 percent to 92.2 percent, against culture and 62.8 percent, or 95 percent CI 47.7 percent to 75.8 percent, against composite standard. Utilizing a large volume of sample, of at least 8�10 ml, is necessary for testing CSF and centrifugation can cause considerable improvements in yield. Despite the lack of standardization for sample processing, WHO has allowed testing CSF with the automated Xpert MTB/RIF assay as the first-line test over conventional microscopy. �
Multiplex Assays
Simplicity makes multiplex molecular assays fundamental for the diagnosis of a panel of microbial targets. Several multiplex PCR assays have been developed to diagnose bacterial pathogens in CSF targeting the most common causes of meningitis: S. pneumoniae, N. meningitis, H. influenzae, L. monocytogenes, S. agalactiae, S. aureus, E. coli, and M. pneumoniae. A multiplex PCR followed by Luminex suspension array can simultaneously diagnose eight bacterial and viral pathogens in CSF, including N. meningitis, S. pueumoniae, E. coli, S. aureus, L. monocytogenes, S. agalactiae, HSV-1/2, and VZV, among others. �
Considering the variety of pathogens involved in CNS infection, application of comprehensive molecular panels with multiple bacterial and viral targets have improved the efficiency of diagnosis. The BioFire FilmArray Meningitis/Encephalitis panel is currently the only FDA cleared multiplex assay utilized for the diagnosis of six bacterial, such as Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria meningitides, Streptococcus agalactiae and Streptococcus pneumoniae, seven viral, such as cytomegalovirus, enterovirus, HSV-1, HSV-2, human herpesvirus 6 or HHV-6, human parechovirus and VZV, as well as a single fungal, such as Cryptococcus neoformans/gattii, target in CSF as demonstrated in Table 2. The integrated FilmArray system takes about an hour, with only 2 minutes of hands-on time. During the preparation of the manuscript, two research studies demonstrated the performance of this assay. Utilizing 48 samples from gram stain negative CSF samples from suspected cases of meningitis, research studies demonstrated that this system diagnosed more viral pathogens, such as EBV. Four cases of WNV and a single case of Histoplasma were not diagnosed by this assay. Among HIV infected patients in Uganda, the test performance demonstrated increased sensitivity and specificity for the diagnosis of Cryptococcus. Although the FilmArray Meningitis/Encephalitis panel offers a quick diagnosis of CNS infections, further research studies are needed to determine its performance for a variety of targets and other high-risk populations. �
Co-infections are frequently found among immunocompromised patients and can ultimately be challenging to diagnose for clinicians. The multiplex design allows simultaneous diagnosis of multiple targets on the same sample. One research study utilized a panel of monoplex and multiplex molecular assays to conduct a prospective cohort research study in Uganda to comprehensively evaluate the etiology of meningitis among HIV-infected adults. Among the 314 HIV-infected patients with meningitis, EBV co-infection was diagnosed with Cryptococcus, M. tuberculosis, or other viral pathogens. EBV in CSF in these settings is not completely understood although a single research study associated increased EBV viral load as a marker of poor outcome measures in patients with bacterial meningitis and EBV co-infection/ reactivation, among others. �
Pan-Omic Molecular Assays
Technological improvements in metagenomic deep sequencing have increased its utilization for clinical diagnosis of CNS infections. Several research studies have demonstrated its ability to solve diagnostic technique problems which challenge the limits of traditional laboratory testing. Due to sterile status and protection by BBB, CSF and brain biopsies are fundamental to further explore the utilization of this technology for pathogen diagnosis. Metagenomics was successfully utilized to establish a diagnosis of neuroleptospirosis in a 14-year-old boy with severe combined immunodeficiency who also suffered from recurrent bouts of fever, headache, and coma. Similarly, high-throughput RNA sequencing performed on brain biopsy from an 18-month-old boy with encephalopathy diagnosed a new Astrovirus as the cause. Despite the utilization of metagenomics for the diagnosis of infectious disease, there are many technological and practical concerns which need to be addressed before this form of diagnostic testing can become mainstream and part of the clinical standard of care. �
Other promising advances have occurred in transcriptomics, proteomics and metabolomics. Host and microbial microRNA or miRNA, profiles have been utilized for a variety of inflammatory and infectious diseases. Two miRNAs, miR-155 and miRNA-29b, were reported as potential biomarkers for JEV infection and treatment targets for anti-JEV therapy. Host neural epidermal growth factor, including 2 and apolipoprotein B in CSF, was able to diagnose tuberculous meningitis with 83.3 percent to 89.3 percent sensitivity and 75 percent to 92 percent specificity. CSF metabolite profiling has been reported to be useful in the classification, diagnosis, epidemiology, and treatment assessment of CNS infections in HIV patients. CSF metabolic profile analysis demonstrated bioenergetic adaptation in regulating shifts of HIV-infected patients. �
Outcome Measures Associated with Diseases
Diagnosis of an etiologic agent in patients with CNS infections needs consideration of the most common causative organisms, the available diagnostic techniques and molecular methods for these agents, and the highest-yield clinical specimens for evaluation and testing. Knowledge of the epidemiology and clinical presentation of specific agents is fundamental in selecting which diagnostic methods are appropriate for patients. Animal or vector exposures, geographic location, recent travel history, season of the year, exposure of ill contacts, and occupational exposures should be considered. �
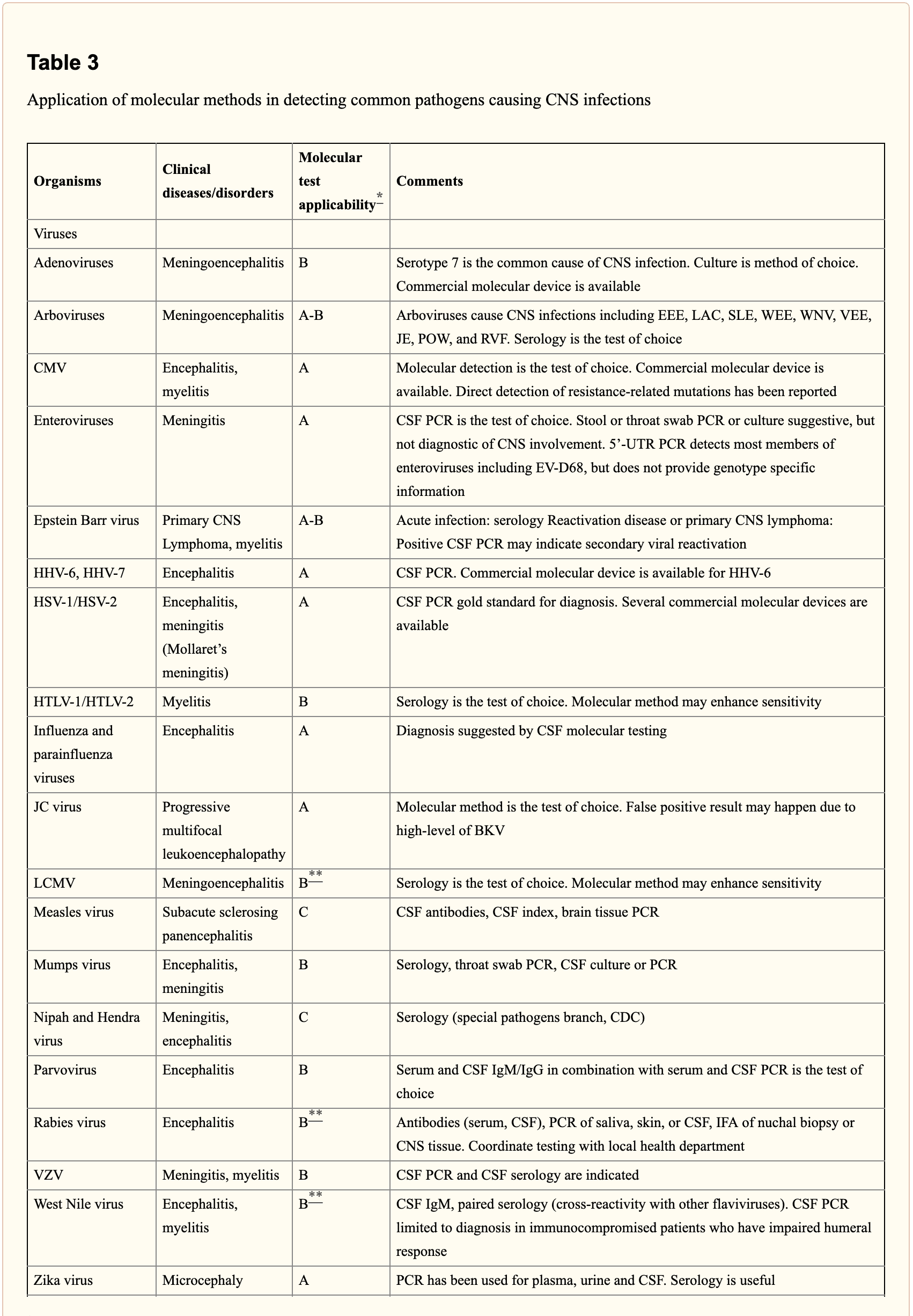
When selecting appropriate pathogen-specific molecular diagnostic methods, the following factors should be considered. CSF is the optimal specimen for PCR testing for patients with meningitis or meningoencephalitis. While indirect evidence can be determined by testing other specimen types, attempts should be made to obtain CSF samples early before treatment can compromise yield. Time of testing from the manifestation of symptoms is fundamental to understand and rule out false-negative results and recommend retesting within a certain time frame. By way of instance, HSV PCR can commonly render false-negative results if CSF sample is obtained very early or late in the process of HSE infection. Host health is also known to affect test performance characteristics. Immunocompromised patients are at risk for infection by a variety of opportunistic pathogens, by way of instance HHV-6, JC virus, Toxoplasma encephalitis in bone marrow transplant recipients and patients with HIV. Often, infection can be more severe, such as WNV, and challenging to diagnose in this population. Table 3 below demonstrates practical recommendations on application and pitfalls of molecular test for the diagnosis of CNS infections. �
Furthermore, a positive nucleic acid amplification testing results are considered to be complicated by the fact that some viruses survive latently in macrophages or neurologic tissues even if they’re incidentally diagnosed by sensitive molecular techniques without an actual pathogenic role which can potentially lead to overtreatment. Utilization of adjunctive biomarkers which help determine active replication is being explored to overcome this drawback in research studies. �
Historically, the diagnosis of microbiologic agents in patients with CNS infections has been hindered by the low yield of CSF culture for viral and fastidious bacterial organisms, delays in CNS production of organism-specific antibodies, and challenges in determining optimum samples for testing. The nucleic acid in vitro amplification-based molecular diagnostic methods and techniques have a wider and better application in clinical microbiology practice. The monoplex assay will likely be the main platform utilized for urgent, random-access, low throughput assays. Multiplex assays have the additional benefit of diagnosing multiple targets and mixed infections. As the volume of CSF sample retrieved is often small, multiplex assays enable comprehensive diagnostic analysis with a low amount of sample, obviating the need for repeated lumbar punctures. The clinical relevance and cost-effectiveness of simultaneous multi-pathogen diagnosis strategies need further research studies. Application of pan-omic techniques in challenging to diagnose CNS infections is the new exciting frontier, the technology is promising but routine implementation is expected to be slow due to various challenges, such as lack of applicable regulatory guidelines and adaptation in the clinical setting, although the outcome measures are promising. �
As previously mentioned, central nervous system, or CNS, infections can be life-threatening health issues if they are not accurately diagnosed and properly treated. However, determining a diagnosis of CNS infections can be challenging for many clinicians. Fortunately, a variety of diagnostic techniques and molecular methods can ultimately help determine the source of CNS infections and other health issues. These diagnostic techniques and molecular methods have tremendously improved over the years, as previously mentioned, and more of these evaluations are being utilized in clinical settings to accurately diagnose CNS infections for proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
In part 2 of our “Diagnosis of Central Nervous System Infections” article, we discussed the molecular methods and the pan-omic molecular assays which are utilized in the diagnosis of CNS infections as well as how specific testing outcome measures have ultimately been associated with clinical diseases and health issues. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
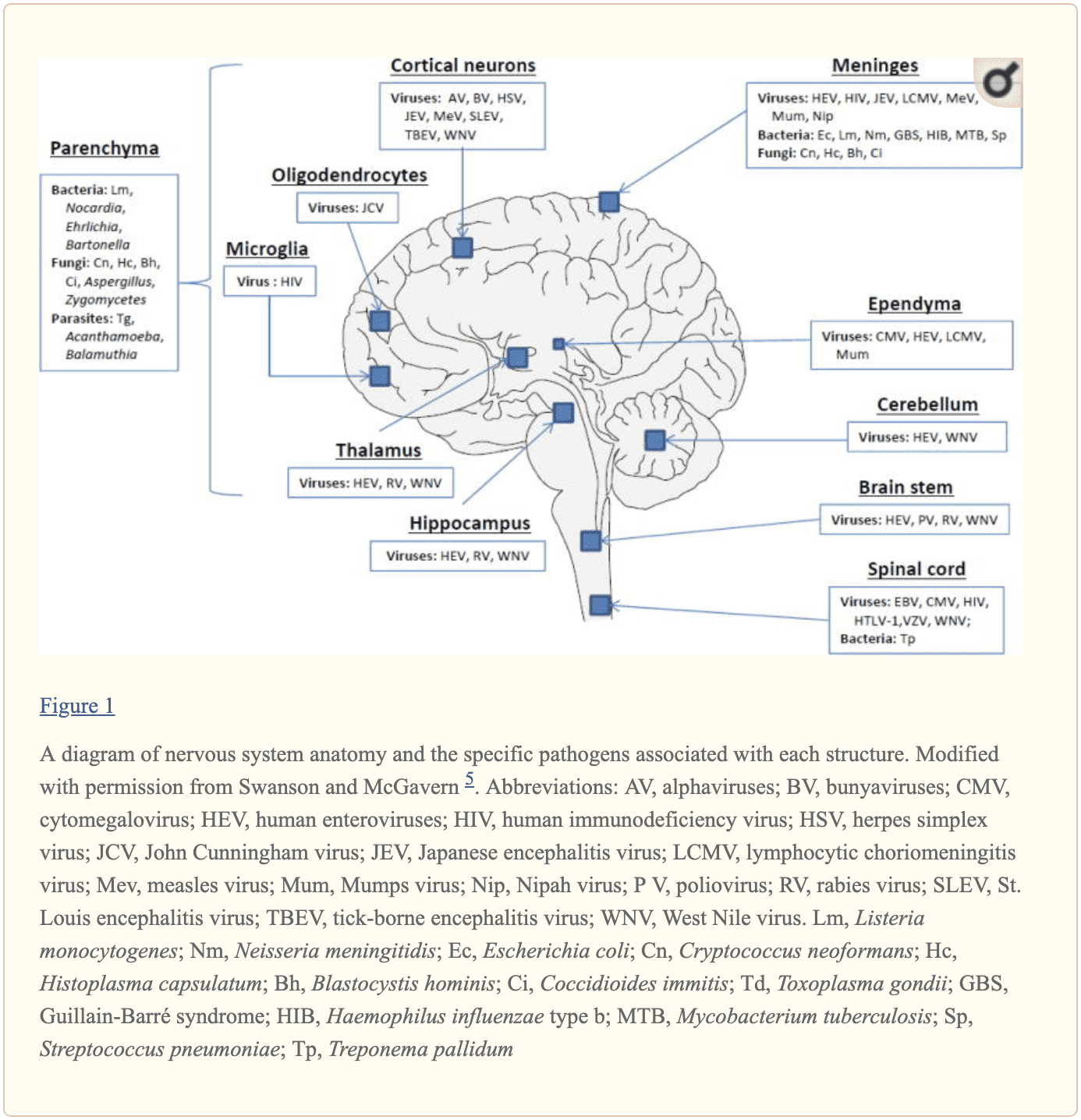
The central nervous system, or CNS, plays a fundamental role in the pathogenesis of infection. The CNS is regulated by the blood-brain barrier or BBB, however, it can still be exposed to a microbial invasion from a contiguous focus, hematogenous dissemination, or intraneural passage of organisms. A variety of environmental or commensal bacteria, viruses, fungi, protozoa, or parasites can enter the CNS and cause a variety of infections and health issues. Central nervous system infections can ultimately cause headache, stiff neck, vomiting, fever, photophobia, and focal neurological symptoms. �
What are Central Nervous System Infections?
CNS infections are characterized according to their affected region. Infection of the brain, spinal cord, and meninges results in meningitis, encephalitis, brain abscess, and myelitis. Infections can affect single or multiple regions of the brain, such as meningoencephalitis and encephalomyelitis. Moreover, CNS infections are characterized as acute, sub-acute, chronic, or recurrent based on their duration. Meningitis can cause headache, neck stiffness, fever, and photophobia over a period of hours to days. Encephalitis can cause brain parenchymal inflammation which can ultimately cause lethargy to coma. Last but not least, Myelitis can cause inflammation of the spinal cord including headache, fever, and paraparesis or paralysis. �
One of the most fatal CNS infections, acute bacterial meningitis, with three to five cases for every 100,000 people in the United States, has a mortality rate of 6 percent to 26 percent. Approximately 4,000 cases of acute bacterial meningitis occur in the U.S. every year with about 500 deaths. The frequent cause of acute bacterial meningitis includes Streptococcus pneumoniae, group B Streptococcus, Neisseria meningitides, Haemophilus influenzae, and Listeria monocytogenes. �
CNS infections caused by viruses are more common and are mostly mild and self-limited. However, these can manifest as meningitis and/or encephalitis. CNS infections caused by viruses can vary due to region and season. Non-polio enteroviruses are responsible for the majority of meningitis and/or encephalitis cases from late spring to fall. CNS infections due to herpes simplex viruses, or HSV, are associated with sporadic encephalitis and meningitis with severe sequelae if left untreated. �
Diagnosis of CNS Infections
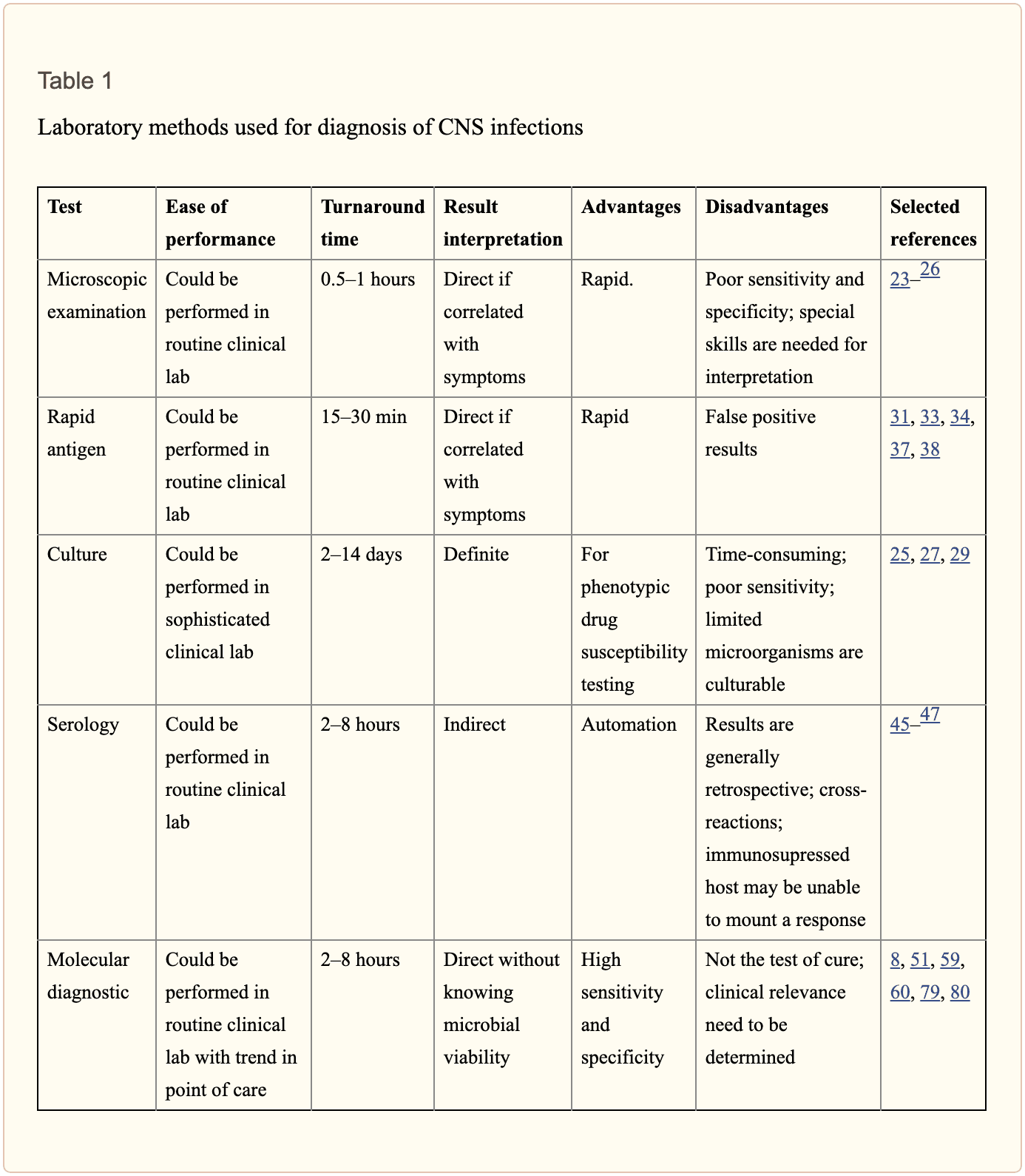
Diagnosis of microbial pathogens is fundamental for treatment. Methods and techniques utilized in clinical microbiology laboratories include direct microscopic examination, and culture techniques as well as antigen and antibody detection assays. However, each method and technique has several essential limitations. By way of instance, direct microscopic examination of CSF restricted sensitivity and specificity. The sensitivity of culture for enteroviruses is between 65 percent to 75 percent with average retrieval time of 3.7 to 8.2 days. Moreover, several serotypes of enteroviruses, especially Coxsackievirus A strains, are well-known to be non-cultivable and frequently grow poorly. Because enteroviruses are missing a common antigen found throughout a variety of serotypes, universal antigen and/or antibody diagnosis is impossible. Diagnosis of CNS HSV infections through methods and techniques utilized to determine culture sensitivity from CSF is tremendously poor. The presence of HSV IgG antibodies in CSF can ultimately be utilized to determine a diagnosis, however, the production is delayed until day 10 or day 12 after infection and it is not considered ideal for early diagnosis.
Diagnostic techniques, especially PCR based amplification, have developed a variety of mainstay tools to help determine the diagnosis of microbial pathogens in CSF. Molecular methods have demonstrated greater diagnosis rates than other diagnostic techniques. One research study demonstrated that 16S rRNA PCR-based assays were able to diagnose the causative organism in 65 percent of banked CSF samples compared to 35 percent when utilizing culture and microscopy. In another research study, diagnosis based on diagnostic techniques like molecular methods were utilized to optimize antibiotic treatment of patients with infectious meningitis when conventional methods and techniques demonstrated a negative outcome measure. Molecular methods and diagnostic techniques utilized on CSF samples are a fundamental standard when compared to the culture standard in the diagnosis of CNS infections caused by viruses which are challenging to diagnose. �
The diagnosis of CNS infections has tremendously changed over the last several years. PCR-based molecular methods have become a fundamental element in the clinical microbiology laboratory, providing tools for an accurate diagnosis. As demonstrated in Table 2, a variety of commercial molecular assays have been cleared by the Food and Drug Administration, or FDA, for the diagnosis of microbial pathogens. The approved assays for pathogen detection in the CNS are shown below. �
However, there are still several challenges in molecular diagnostic techniques and methods. Utilizing a combination of conventional diagnostic techniques and molecular methods, research studies demonstrated that in approximately 62 percent of patients with encephalitis, an etiologic organism could not be identified. Researchers have started to focus on developing advanced techniques and methods. In the following series of articles, we will demonstrate an update on the current conventional and molecular platforms utilized for the diagnosis of CNS infections. We will also demonstrate a preview on the potential clinical application of future technologies, including pan-omic assays. The emphasis of the following series of articles is to demonstrate optimal test selection in the clinical scenario for the diagnosis of CNS infection. �
Conventional Microbiology Methods and Techniques
Microscopic Examination
A positive CSF Gram stain confirms the diagnosis of bacterial meningitis. The sensitivity of the Gram stain for the diagnosis of bacterial meningitis is approximately 60 percent to 80 percent in patients not on antimicrobial treatment and approximately 40 percent to 60 percent in patients on antibacterial treatment. In one research study, Gram stain diagnosed as much as 90 percent Streptococcus pneumoniae and 50 percent Listeria monocytogenes in CSF collected from patients with bacterial meningitis confirmed by PCR 26 techniques and methods. Two organisms which are frequently diagnosed by microscopy include Mycobacterium tuberculosis by acid-fast bacillus, or AFB, staining and Cryptococcus neoformans by India ink or Gram stain. However,� the sensitivities of these techniques and methods are poor and culture is generally utilized instead. �
Culture
Culture of brain tissue can demonstrate a positive diagnosis of CNS infections, however, getting biopsies are tremendously invasive and frequently avoided unless a clinician determines that they are absolutely necessary. CSF sampling is most commonly performed to diagnose CNS infection. CSF viral, bacterial, including mycobacterial, and fungal cultures are fundamental in the diagnosis of infectious meningitis. However, CSF cultures in these cases are extremely low. Another disadvantage of CSF bacterial culture is that it generally requires up to 72 hours to determine a final diagnosis. A recent research study demonstrated that CSF mycobacterial culture had a sensitivity of 22 percent and a specificity of 100 percent in the diagnosis of tuberculosis meningitis. For viruses, utilizing monoclonal antibodies through culture increased the speed and specificity. However, due to time and sensitivity, CSF viral culture is frequently unable to determine a diagnosis. �
Rapid Antigen Detection
Cryptococcal antigen is the most commonly utilized antigen assay for CNS infections. The test utilizes Cryptococcus capsular polysaccharide antigens in CSF through enzyme immunoassay to determine a diagnosis. In a single research study which evaluated patients less than 35 years of age with CNS cryptococcosis, overall sensitivity and specificity of 93 percent to 100 percent and 93 percent to 98 percent were shown. Cryptococcus is a neurotropic fungus. Polysaccharide serum antigen titers with host immune status are frequently utilized to determine the need for a lumbar puncture to evaluate the patient for CNS health issues. The baseline peak titer of polysaccharide antigen in serum or CSF has demonstrated fundamental prognostic significance with an increased titer, or peak titer less than 1:1024, associated with antifungal therapy failure. �
The diagnosis of galactomannan, or GM, antigen and 1,3 ?-D-glucan, or BDG, in CSF, can help in the diagnosis of CNS aspergillosis or other invasive fungal infection such as fusariosis. Increased BDG in serum and CSF is associated with fungal infections. Measuring the levels of BDG is a beneficial biomarker in the evaluation of fungal CNS infection. It was recently demonstrated that patients receiving effective antifungal therapy demonstrated a decrease in CSF BDG concentrations with less than 31pg/ml and for this reason, BDG titers in CSF are a beneficial biomarker when monitoring response to treatment. �
For acute bacterial meningitis, a rapid antigen assay can help diagnose for a pneumococcal capsular antigen. Several research studies have demonstrated the utilization of M. tuberculosis-specific antigens in CSF for the diagnosis of tuberculosis meningitis. M. tuberculosis Early Secreted Antigenic Target 6, or ESAT-6, has been utilized for tuberculosis meningitis. �
Serology
Serological diagnosis of CNS infections is determined by identifying IgM antibodies or by demonstrating an increase in neutralizing antibody titers between acute- and convalescent-phase CSF. Due to a delay in antibody response when symptoms have manifested, a negative antibody test cannot be utilized to rule out infections and retesting may be required. Moreover, in specific populations, such as immunocompromised patients, the tests may not offer optimum sensitivity. In most instances, nucleic acid amplification tests have surpassed antibody-based detection as the test of choice. For several CNS infections, these assays play a fundamental role. CSF IgM is the most commonly utilized test for West Nile virus, or WNV, infections. Antibodies may manifest in as soon as 3 days and may continue for up to 3 months. However, its accuracy is challenged by high cross-reactivity with other flaviviruses and associated vaccines. Antibodies in recombinant WNV E proteins can determine where cross-reacting viruses co-circulate or determine which patients have been immunized. �
Fundamental serological assays for CNS infections are utilized for the diagnosis of neurosyphilis. Neurosyphilis is determined by a positive CSF venereal disease research laboratory, or VDRL, test. Diagnosis of varicella-zoster virus, or VZV, IgG in CSF is the most common technique and/or method for the diagnosis of VZV associated with CNS infection. �
Central nervous system, or CNS, infections can ultimately be life-threatening health issues if they are not diagnosed and treated early. Determining an accurate diagnosis of CNS infections can be challenging. Fortunately, a variety of diagnostic techniques and molecular methods can help determine the source of CNS infections. These diagnostic techniques and molecular methods have tremendously improved over the years and more and more of these evaluations are being utilized in clinical settings to accurately diagnose CNS infections for early treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
In part 2 of our “Diagnosis of Central Nervous System Infections” article, we will ultimately discuss the molecular methods and the pan-omic molecular assays which are utilized in the diagnosis of CNS infections as well as discuss how specific testing outcome measures are associated with clinical diseases and health issues. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
We often think of proteins are nutrients found in the food we eat and the main component of muscles, however, proteins are microscopic molecules located inside of cells which actually perform a variety of fundamental roles. The function of a protein depends on its shape, and when protein formation goes awry, the resulting misshapen proteins can cause numerous health issues, such as when proteins neglect their essential roles or when they form a sticky, clumpy clutter inside of cells. Protein formation is an error-prone procedure and mistakes along the way have been associated with neurological diseases. �
There are approximately 20,000 to over 100,000 unique types of proteins found inside a common human cell. Why so many? Proteins are the workhorses of the human cell. By way of instance, several of these proteins are structural, lending stiffness and rigidity to thin neurons or muscle tissues. Other proteins shuttle them to new places and bind to specific molecules and others catalyze responses. A property of proteins is possible through diversity and specificity in their role when they fold. �
Why Proteins Fold into a Functional Shape
A protein generally begins in the cell as a lengthy chain of about 300 building blocks known as amino acids. There are 22 different types of amino acids and their order decides what protein chain will fold onto itself. After folding, two types of structures will generally form. Several regions of the protein chain coil into slinky-like formations known as “alpha-helices,” while other regions fold into zigzag patterns known as “beta-sheets,” which resemble the folds of a paper fan. �
Both of these structures may interact to form complex structures. In one protein structure, many beta-sheets wrap themselves around to form a hollow tube. The tube is also generally short where the overall structure resembles snakes (alpha-helices) emerging out of a can (beta-sheet tubing ). Moreover, several other protein structures with descriptive names include the “beta-barrel,” that the”beta-propeller,” the”alpha/beta-horseshoe,” as well as the “jelly-roll fold”. �
These intricate structures allow proteins to perform their variety of roles in the cell. The “snakes in a can” protein, when embedded into a cell membrane, creates a tube which enables traffic in and out of cells. Other proteins form contours with pockets known as “active sites” which are perfectly shaped to bind to a certain molecule like a lock and key. By bending into different shapes, proteins can do different functions. To draw an analogy, all vehicles are made from steel, while a bus, dump truck, crane, or Zamboni are shaped to execute their very own tasks however races are won by the slick shape of a racecar. �
Why Protein Folding Sometimes Fails
Protein folding ultimately allows a protein to take a functional shape, however, it’s an intricate procedure which can sometimes fail. According to research studies, protein folding can go wrong due to three major reasons: �
A person may have a mutation which affects an amino acid in the protein chain, making it difficult for a specific protein to locate its favored fold or “native” state. This is how it is for mutations, such as those contributing to cystic fibrosis or sickle cell anemia. These mutations are found in the DNA sequence or “gene” which encodes one special protein. Therefore, these types of inherited mutations affect only that protein and its related function.
On the other hand, protein folding failure can be seen as an ongoing and much more general procedure which affects several proteins. When proteins are made, the structure which reads the instructions from DNA to produce the long chains of amino acids can make errors. Researchers estimate that the ribosome makes mistakes in as many as 1 in every 7 proteins. These mistakes can make the proteins which are resultantly inclined to continue to fold improperly.
Even though an amino acid chain does not have any mutations or mistakes, it may still not reach its own preferred folded shape because proteins don’t fold properly 100 percent of their time. Protein folding becomes much more difficult if the conditions in the cell change due to external factors such as temperature and acidity.
A collapse in protein folding can cause a variety of neurological diseases and researchers hypothesize that many health issues are associated with folding problems. There are two problems which exist in cells which don’t protein fold correctly. �
One type of problem, known as “loss of function,” results when not enough of a particular protein folds correctly, causing a lack of “specialized functions” necessary to perform a particularly important role. By way of instance, imagine a correctly folded protein is shaped to bind a toxin and split it into noxious compounds. Without enough of that protein accessible, the toxin will build-up to damaging levels. In another instance, a protein may be responsible for metabolizing sugar which can then be utilized by the cell for energy. The cell will grow due to lack of energy if not enough of this protein is accessible. The reason the cell becomes ill, in these cases, is because of a lack of one particular folded, functional protein. Cystic fibrosis, Tay-Sachs disease, Marfan syndrome, and some types of cancer are examples of health issues which result when one type of protein is unable to perform its role. Who knew that one type of protein out of thousands may be so significant? �
Proteins folding may also impact the overall health and wellness of the cell regardless of the utilization of the protein. When proteins fail to fold into their functional state, the consequent misfolded proteins could be contorted into shapes which are harmful to the crowded cell environment. Most proteins have sticky, “water-hating” amino acids which they bury deep inside their own core. Misfolded proteins utilize these parts on their exterior, such as a chocolate-covered candy which has been crushed to reveal a gooey center. These misfolded proteins commonly stick together to form clumps known as “aggregates.” Researchers discovered that the accumulation of misfolded proteins plays a fundamental role in several neurological diseases, including Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, and Lou Gehrig’s (ALS) disease, however, researchers are still working to discover exactly how these misfolded molecules affect the well-being of the cells. �
One misfolded protein ultimately stands out from among the rest and it deserves particular attention. The “prion” protein in Creutzfeldt-Jakob disease, also known as mad cow disease, is an illustration of a misfolded protein gone rogue. This protein isn’t simply irreversibly misfolded, however, it also transforms other functional proteins into a similar twisted condition. �
How Cells Protect from Misfolded Proteins
Recent research studies have demonstrated that protein misfolding often occurs inside of cells. Fortunately, cells also have many systems in place and are accustomed to coping with this issue by refolding or destroying aberrant protein formations. � Appropriately known as chaperones, these structures accompany proteins throughout the folding procedure, enhancing a protein’s odds of folding properly and even allowing several misfolded proteins the opportunity to refold. Chaperones are proteins themselves. There are many distinct types of chaperones. A few chaperones supply safety to proteins, isolated from other molecules. Production of many chaperones is fostered when a cell encounters high temperatures or other states which can ultimately make protein folding more difficult, therefore, providing these chaperones the alias, “heat shock proteins.” �
The following line of cell defense against misfolded proteins is known as the proteasome. If misfolded proteins linger in the cell, they will be targeted for destruction by this structure, which chews proteins up and spits them out. The proteasome is similar to a center, permitting the cell to reuse amino acids to create proteins. The proteasome itself is not a single protein but many acting collectively. Proteins frequently interact to form larger structures. By way of instance, a human sperm’s tail is a structure made of various types of proteins which work together to produce a rotary engine which propels the sperm. �
Protein Folding and Misfolding Overview
Why is it that some misfolded proteins can evade systems such as chaperones and the proteasome? How can the neurological diseases previously mentioned above be caused by sticky misfolded proteins? Do some proteins misfold more often than others? These questions are at the forefront of research studies seeking to understand the health issues which ultimately result if protein fold goes awry as well as protein biology. The broad world of proteins, using its great assortment of shapes, bestows cells with capacities that allow for life to exist and allow for its diversity (e.g., the differences between eye, skin, lung or heart cells, and also the differences between species). But perhaps this is one of the many reasons why the word “protein” comes from the Greek word “protas,” meaning “of primary significance” and indeed they seem to be. �
Protein folding is a complex, physiochemical process by which a protein “folds” or assumes a functional shape to be able to perform their biological function. Proteins are nutrients we obtain from the food we eat and they are considered to be one of the main components of muscles, however, proteins play a wide variety of fundamental roles in the human body. According to research studies, protein misfolding can cause a variety of health issues, including neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to describe protein folding and how it’s associated with neurological diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Cerebrovascular disease is characterized as a group of diseases, conditions, and disorders which ultimately affects the blood vessels and the blood supply to the human brain. Brain damage can occur when a blockage, malformation, or hemorrhage prevents the brain cells from receiving enough oxygen. Cerebrovascular disorders can include stroke, transient ischemic attack or TIA, aneurysm, and vascular malformation. �
Cerebrovascular disease can develop due to a variety of health issues, such as atherosclerosis, where the arteries become narrow; thrombosis or embolic arterial blood clot, which is a blood clot in an artery of the brain; or cerebral venous thrombosis, which is a blood clot in a vein of the brain. �
In the United States, cerebrovascular disease is one of the most common causes of death. In 2017, it caused about 44.9 deaths per 100,000 individuals or 146,383 deaths in total. Fortunately, people can decrease their risk of developing cerebrovascular disease. In the following article, we will describe the types, the symptoms, the diagnosis, and the treatment for cerebrovascular disease and how to prevent them. �
Cerebrovascular Disease Symptoms
The symptoms of cerebrovascular disease are commonly based on the region of the health issue and its effect on the brain. � Different types of cerebrovascular disease may have different symptoms, however, common symptoms can include: �
a severe and sudden headache
hemiplegia or paralysis on one side of the human body
weakness on one side, also known as hemiparesis
confusion
difficulty communicating, including slurred speech
losing vision on one side
loss of balance
becoming unconscious
Emergency Response
The American Stroke Association promotes the public knowledge of the F.A.S.T. acronym as a way to help people recognize the warning signs of a stroke or any other type of cerebrovascular disease to take action immediately, including: �
face drooping
arm weakness
speech difficulty
time to call 911
Immediate medical attention is fundamental if anyone demonstrates symptoms of a cerebrovascular disease attack because these may ultimately have long-term effects if not treated immediately, such as cognitive impairment and paralysis. �
Types of Cerebrovascular Disease
Stroke, TIA, and subarachnoid hemorrhage are several types of cerebrovascular disease. Aneurysms and hemorrhages may cause acute health issues. Blood clots can affect the brain directly or indirectly from other regions of the human body.
Ischemic Stroke
Ischemic strokes occur when a blood clot or atherosclerotic plaque blocks a blood vessel which supplies blood to the brain. A clot or thrombus may develop in a narrow artery. A stroke occurs when a blood supply deficiency causes brain cell death.
Embolism
An embolic stroke is the most common type of ischemic stroke. An embolism occurs when a clot breaks off from another region in the human body and travels to the brain and blocks a smaller artery. People who have arrhythmias, which are health issues associated with irregular heart rhythm, are more vulnerable to developing an embolism as well as other health issues. �
A tear in the lining of the carotid artery, which is found in the neck, can ultimately cause an ischemic stroke. The tear allows blood circulation to flow between the layers of the artery, reducing blood flow to the brain, and causing it to become narrow. �
Hemorrhagic Stroke
Hemorrhagic strokes occur when a blood vessel in part of the brain weakens and pops open, causing blood to flow into the brain. The leaking blood puts pressure on the brain tissue, causing edema, which can ultimately damage brain tissue. The hemorrhage may cause parts of the brain to lose their supply of oxygen-rich blood, causing a variety of other health issues. �
Cerebral Aneurysm or Subarachnoid Hemorrhage
A cerebral aneurysm or subarachnoid hemorrhage can occur due to structural health issues associated with the blood vessels of the brain. An aneurysm is a bulge which in the arterial wall which may rupture and bleed. A subarachnoid hemorrhage occurs when a blood vessel ruptures and bleeds between two membranes in the brain, damaging brain cells. �
Cerebrovascular Disease Causes
Cerebrovascular disease develops due to a variety of factors. If damage occurs to a blood vessel in the brain, it won’t be able to deliver enough or any blood to the necessary region of the brain. The deficiency of blood can affect the delivery of oxygen and brain cells can begin to die. Brain damage is irreversible. �
Immediate medical attention is fundamental to decrease a person’s risk of long-term brain damage and increase their chances of survival. Atherosclerosis is a key cause of cerebrovascular disease. This occurs when cholesterol levels, as well as inflammation in the brain’s arteries, cause cholesterol to build-up. This plaque may restrict or completely obstruct blood circulation into the brain, causing a cerebrovascular disease attack, including a stroke or TIA. �
Risk Factors
Stroke is the most common type of cerebrovascular disease. The risk of stroke increases with age, especially if a person or their close relatives have previously had a cerebrovascular disease attack. The risk doubles every 10 years, between 55 and 85 years of age. However, a stroke can occur at any age, even during infancy. � Factors which increase the risk of stroke and other types of cerebrovascular disease include: �
hypertension, which the American College of Cardiology defines as blood pressure of 130/80 mm Hg or higher
smoking
obesity
poor diet and lack of exercise
diabetes
blood cholesterol levels of 240 milligrams per deciliter (mg/dl) or higher
The same factors can increase a person’s risk of developing a cerebral aneurysm. However, people with a congenital anomaly or previous head trauma may also be at risk of developing a cerebral aneurysm. Pregnancy can also increase the risk of developing cerebral venous thrombosis which is a blood clot affecting a vein in the human brain. � Other risk factors of cerebrovascular disease include: �
Moyamoya disease, a progressive condition which causes a blockage of the cerebral arteries and their major branches
venous angiomas, which affect around 2 percent of the U.S. population and rarely bleed or cause symptoms
a vein of Galen malformation, an arterial disorder which develops in a fetus during pregnancy
Certain drugs and/or medication, as well as other health issues, can make the blood more likely to clot and also increase the risk of ischemic stroke. Hormone replacement therapy or HRT may also increase the risk of a cerebrovascular disease attack in people who currently have atherosclerosis or carotid artery disease, among other health issues. �
Cerebrovascular Disease Diagnosis
Any cerebrovascular disease can be considered a medical emergency and anybody who recognizes the symptoms must contact 911 for support and evaluation. Early diagnosis is fundamental to reduce brain damage. In the clinic, a doctor will ask about the person’s medical history and search for specific neurological, motor, and sensory health issues, including: �
changes in vision or visual fields
reduced or altered reflexes
abnormal eye movements
muscle weakness
decreased sensation
A doctor may also utilize a cerebral angiography, vertebral angiogram, or carotid angiogram to identify a vascular abnormality, such as a blood clot or a blood vessel health issue. These include injecting dye to demonstrate any clots as well as their size and form on MRI or CT imaging. �
A CAT scan will also help a doctor diagnose hemorrhagic strokes as it can distinguish between blood, bone, and brain tissue. However, it does not reveal damage from an ischemic stroke in the first phases. An MRI scan may detect early-stage strokes. An electrocardiogram (EKG or ECG) may diagnose cardiac arrhythmia which is a risk factor for embolic strokes. �
Cerebrovascular Disease Treatment
A cerebrovascular disease requires emergency treatment. Rapid diagnosis and treatment are crucial because a person must receive stroke drugs and/or medications from the beginning of their symptoms. In the case of an acute stroke, the emergency group may administer a medicine known as tissue plasminogen activator (tPA) which breaks up the blood clot. �
A neurosurgeon must evaluate a person who has had a brain hemorrhage. They may perform surgery to decrease the pressure which bleeding causes in the brain. A carotid endarterectomy involves making an incision in the carotid artery and removing the plaque. This allows blood to flow again. The surgeon then repairs the artery with sutures or a graft. �
Several patients may need carotid angioplasty and stenting which involves a doctor inserting a balloon-tipped catheter into the artery so that the artery reopens when they inflate the balloon. Then, the doctor matches a slim, metal mesh tube, or stent, within the carotid artery to improve blood flow in the formerly blocked artery. The stent helps to prevent the artery from closing-up or collapsing following the procedure.
Cerebrovascular Disease Rehabilitation
Because a cerebrovascular disease attack can cause irreversible brain damage, people can experience temporary or permanent disability. For this reason, they may require a variety of supportive and rehabilitative treatments so that they can keep as much function as possible. These may ultimately include: �
Physical therapy: The goal is to restore mobility, flexibility, and upper and/or lower extremity function.
Speech therapy: This helps improve communication and regain speech after a stroke or cerebrovascular disease attack.
Occupational therapy: This can help access facilities which support a return to work and daily life.
Psychological therapy: Physical disability can create unexpected emotional demands and often requires intensive readjustment. A person may benefit from visiting a psychiatrist, psychologist, or counselor after experiencing a cerebrovascular disease attack if they feel overwhelmed.
Cerebrovascular Disease Prevention
Techniques and methods which can ultimately help reduce the risk of cerebrovascular disease include: �
no smoking
getting at least 150 minutes of moderate to intense exercise and/or physical activity every week
eating a balanced diet which supports vascular health, such as the DASH diet
maintaining a healthy body weight
managing blood cholesterol and blood pressure with diet as well as drugs and/or medications, if necessary
People with heart arrhythmia should seek immediate medical attention from a healthcare professional and discuss whether they should be taking a blood thinner to prevent strokes. �
Stroke and other cerebrovascular diseases may lead to death but with immediate medical attention, a partial or full recovery is possible. Patients with cerebrovascular disease should follow their healthcare professional’s instructions and lifestyle modifications to ultimately help decrease the prospect of a cardiovascular disease attack. �
Decreasing the Risk of Stroke
Taking blood platelet inhibitors, including, Dipyridamole, Ticlopidine, and clopidogrel, can decrease the chance of stroke before it occurs. These can help prevent stroke in people who have a medical history or higher prospect of experiencing a cerebrovascular disease attack. �
Doctors recommended people to take a daily dose of aspirin to decrease the chance of a heart attack or stroke. However, current guidelines recommend people to take aspirin only if they’re at risk of experiencing cardiovascular disease because aspirin increases the risk of bleeding. � Doctors prescribe statins to manage high cholesterol levels and reduce the risk of ischemic stroke and heart attack. �
As previously mentioned above, cerebrovascular disease is identified as a group of diseases, conditions, and disorders which affects the blood vessels and the blood flow supply to the human brain. There are several types of cerebrovascular diseases and their diagnosis and treatment depends on the type and severity. Prompt treatment and lifestyle modifications can improve the outlook of a patient with cerebrovascular disease. Chiropractors are qualified and experienced to help patients with cerebrovascular disease recover from their symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to describe cerebrovascular disease and its effect on overall health and wellness. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Cerebral perfusion pressure, or CPP, is the net pressure gradient which carries oxygen to brain tissue. It is measured by the difference between the mean arterial pressure, or MAP, and the Intracranial Pressure, or ICP,� which is measured in millimeters of mercury (mm Hg). Regulating CPP is fundamental in the treatment of patients with intracranial pathology, including shock, hemodynamic distress, and traumatic brain injury. �
Although the average CPP is generally between 60 and 80 mm Hg, these values may change to the left or to the right depending on individual physiology. MAP and ICP has to be measured together because CPP is a calculated measure. Regulating CPP at hemodynamically unstable conditions with abnormal ICP or in cases of intracranial pathology will reduce the chance of ischemic brain injury. �
CPP = MAP – ICP
Cerebral Perfusion Pressure Physiology
CPP and ICP
At its own average range of 60 to 80 mm Hg, the CPP is determined by the ICP and the mean arterial pressure. Under regular standards, the ICP is between 5 and 10 mm Hg which has a reduced effect on the CPP than the MAP in clinical circumstances not associated with intracranial pathology. ICP is generally measured through intracranial pressure transduction.
Physiologically, the ICP is a function of intracranial compliance. Intracranial compliance is the relationship between the ICP and the volume of the intracranial cavity including cerebrospinal fluid, or CSF, brain tissue as well as arterial and venous blood volume. Because the skull is a fixed and rigid anatomic space, the ICP can increase if the intracranial volume increases while intracranial compliance decreases. As the ICP increases or intracranial compliance decreases, CPP also decreases. �
Several processes determine that ICP continues to stay within the average range for the longest extended period of time possible, especially throughout periods of affected intracranial volume and compliance. As volume adds to the intracranial space, CSF can shift into the spinal subarachnoid space, causing the ICP to continue significantly unchanged. As volume increases due to a growing space-occupying lesion, brain tissue edema or blood, this process ultimately becomes overwhelming, and ICP begins to increase substantially. �
Cerebral blood flow, or CBF, is also a fundamental factor in ICP homeostasis. Cerebral auto-regulation makes sure that steady blood flow is maintained in the brain over a wide range of physiologic alterations. When blood pressure decreases, auto-regulation causes cerebral vasodilation and an increase in CBF and cerebral blood volume, maintaining ICP and CPP. However, when blood pressure increases, auto-regulation causes cerebral vasoconstriction and a decrease in CBF with a decrease in cerebral blood volume, also regulating ICP and CPP. Too many changes outside of average CBF ranges can cause brain ischemia and injury. �
CPP and MAP
Because ICP in its average ranges is a considerably small number, the CPP generally depends on the mean arterial pressure. MAP is the normal blood pressure during one cardiac cycle which can be measured through invasive hemodynamic monitoring or calculated by the systolic blood pressure, plus two times the diastolic blood pressure, divided by three. The average range of MAP is 70 to 100 mm Hg. �
The average arterial pressure can be affected due to everyday activities, such as rest, stress, and exercise or physical activities. However, if the ICP continues to stay the same, the average arterial pressure can change across its significantly wide range without tremendously decreasing or increasing the CPP. As a matter of fact, CPP and CBF will continue to stay considerably unchanged across a wider range of MAP (50 � 150 mm Hg) than normal due to cerebral auto-regulation and vasoconstriction or vasodilation of cerebral vasculature. �
For patients with hypertension, the auto-regulation setpoint changes, decreasing the average arterial pressure associated with the patient�s normal arterial pressure, which causes vasodilation to increase CBF. Patients with lower than normal average arterial pressure at baseline will have auto-regulatory vasoconstriction as a reaction to an increase in their significant average MAP, to return CBF to baseline. When looking at CBF and CPP in the context of the patient�s average MAP, it is clinically significant based on the regulation of intracranial pathology and hemodynamic derangements. �
Cerebral Perfusion Pressure Complications
Diagnosing and treating cerebral perfusion pressure complications necessitates measuring both the ICP and the MAP. The MAP may be quantified through the utilization of invasive hemodynamic processes, most frequently cannulation of a peripheral artery such as the radial or femoral artery. The MAP may also be measured with a non-invasive blood pressure cuff by applying the formula mentioned above utilizing the systolic and diastolic blood pressures. � Intracranial pressure is generally measured through an intracranial pressure transduction device. The most common and most accurate method or technique is utilizing an intraventricular monitor. The intraventricular dimension of ICP is the normal standard. An intraventricular catheter is inserted into a hole drilled in the skull and into the lateral ventricle to gauge the pressure of the CSF. The benefit of an intraventricular catheter is that CSF could be eliminated, if needed, to decrease ICP. Considerable complications for the ICP include a possibility of bleeding, infection, and difficulty with proper placement. Options include sub-dural and intra-parenchymal monitors. �
The ICP can be measured non-invasively through several methods and techniques, including transcranial Doppler ultrasonography or TCD. TCD utilizes a temporal window to evaluate the speed of blood flow through the middle cerebral artery. Systolic and diastolic average flow velocity is utilized to determine a pulsatility index. The pulsatility index was determined to be closely associated with ICP in several research studies as well as be associated with ICP in other research studies. Therefore, it is not suggested to use TCD as a substitute for direct ICP dimension. Invasive diagnosis and treatment of the MAP through an arterial cannula and the ICP through an intraventricular catheter will give a continuous and accurate calculation of CPP. �
Cerebral Perfusion Pressure Clinical Significance
Two general types of pathologic health issues can ultimately occur where the regulation of the CPP is fundamental, such as intracranial pathology, where ICP regulation is essential and hemodynamic instability/shock where MAP regulation is the most essential. Intracranial pathology involves space-occupying lesions, such as tumors, epidural and subdural hematoma or severe intraparenchymal hemorrhage and cerebral edema as seen after ischemic injury, traumatic brain injury or acute hepatic encephalopathy. In these circumstances, average CPP depends on decreasing the ICP into a normal range as soon as possible while regulating the MAP. When CPP is normal, it’s fundamental to keep in mind that every individual’s brain tissue has a CPP that is “normal” in the context of that individual patient’s physiology, which may be affected by other health issues, such as hypertension or cardiovascular disease. Moving towards a more dynamic direction of the average CPP utilizing the patient’s personal auto-regulatory capacity. These diagnosis and treatment approaches involve more frequent and sophisticated monitoring and might not be readily available for widespread utilization. �
In the instance of considerable traumatic brain injury, significant cerebral edema can decrease intracranial compliance and CSF, developing an increased ICP or intracranial hypertension. Auto-regulatory mechanisms and techniques may or may not function normally and when ICP continues to be elevated, CPP will decrease causing further injury through an ischemic process. In circumstances such as these, together with starting the measures for decreasing the ICP, it is essential to prevent hypotension (MAP – ICP = CPP) and in some instances, allowing hypertension to reasonably occur. �
In circumstances of instability, the ICP is considerably stable as cerebral auto-regulation is undamaged. In the instance of hypotension, the MAP decreases due to blood loss, or hemorrhagic shock, intravascular leak, or distributive shock, and decreased cardiac output, or cardiogenic shock, and the CPP also decreases. It’s the association between MAP and CPP which carries resuscitation guidelines to recommend regulating a MAP greater than or equal to 65 mm Hg. With a normal ICP, this threshold must make sure that a CPP of 55 to 60, the minimum necessary to stop cerebral ischemic injury, is ultimately maintained. As in the circumstance of ICP and cerebral auto-regulation, the goal of MAP is to be within the context of an individual patient’s evaluation hemodynamic function. Patients with untreated hypertension must have increased MAP goals to maintain proper CBF and CPP. �
As previously mentioned in the following article, cerebral perfusion pressure, or CPP, is the net pressure gradient which affects cerebral blood flow to the brain, also known as brain perfusion. According to healthcare professionals, the CPP, or cerebral perfusion pressure, must be constantly regulated within a specific limit because too little pressure or too much pressure could potentially cause a variety of brain health issues. Cerebral perfusion pressure may be associated with a variety of neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article is to discuss cerebral perfusion pressure and its association with neurodegenerative diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

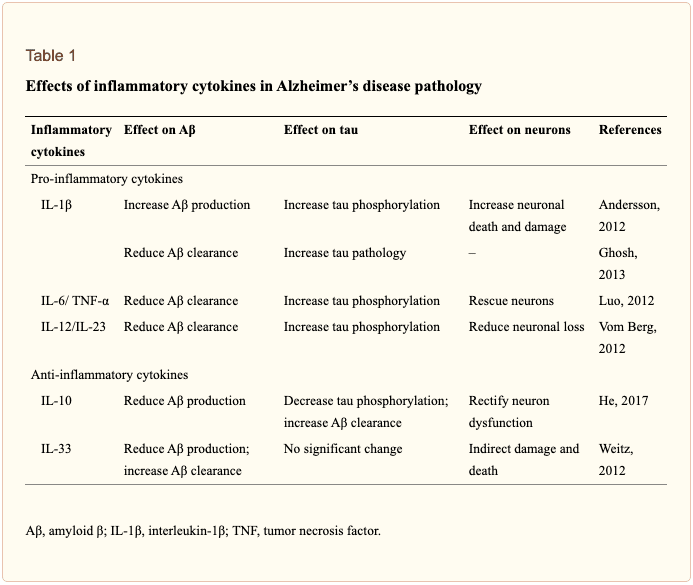 �
�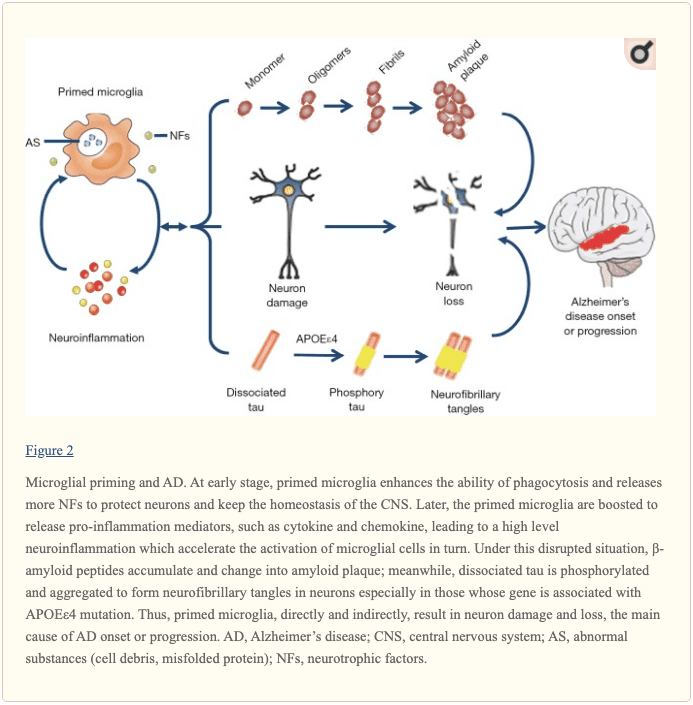 �
�


 �
�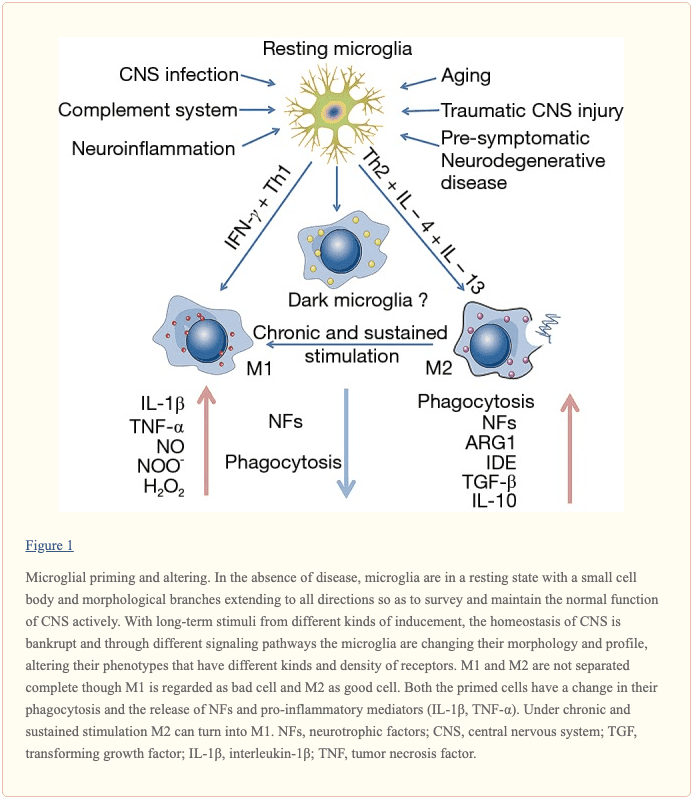 �
�