The levator scapulae muscles could be overstretched for individuals experiencing upper back, shoulder, and neck pain. Can physical therapies help relieve pain and retrain the muscles to function properly?
Levator Scapulae Muscles
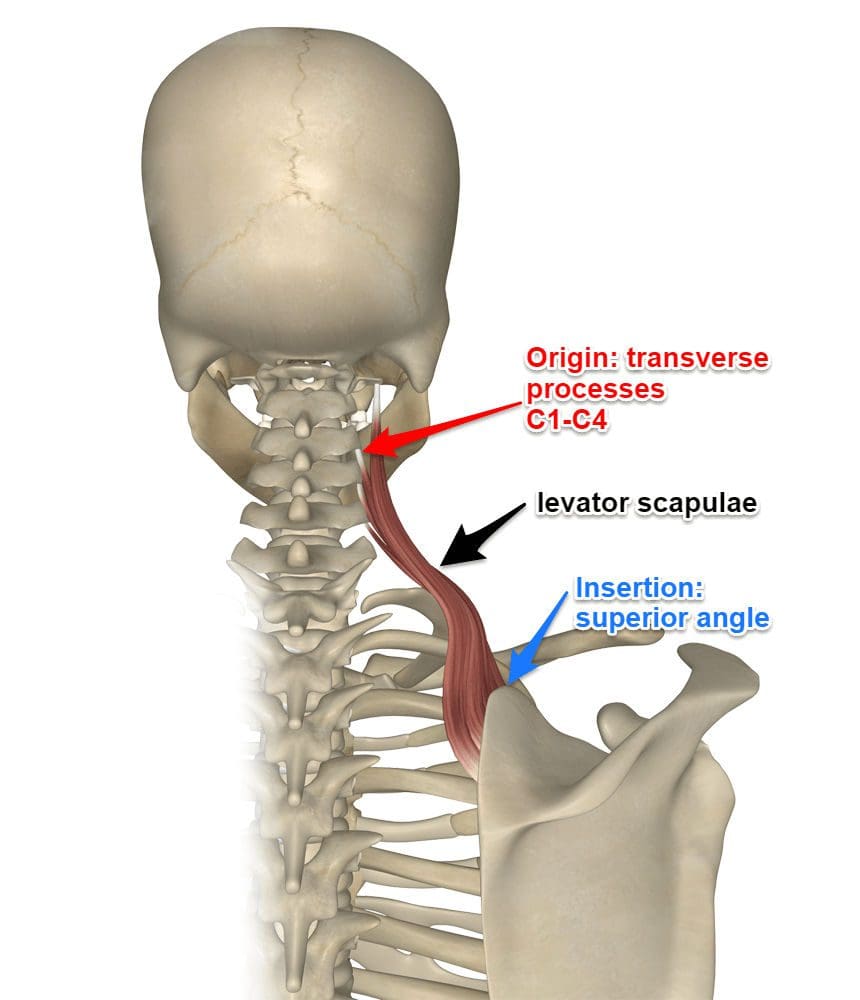
The levator scapulae muscles stretch along the spine across the upper back and neck. They originate from the cervical vertebrae C1 to C4 and attach to the inside top edge of the scapula. (Chotai P. N. et al., 2015) They elevate the shoulder blades, tilt the head, and work with other muscles to stabilize the spine and influence neck motion and upper back posture. The shoulder blade/scapula is the flat, triangular-shaped bone that sits on top of the upper part of the rib cage. Where the levator scapulae attaches, the muscles raise the shoulder blade, a movement called elevation, and indirectly rotates the scapula’s bottom tip downward towards the spine. These shoulder blade movements are part of the shoulder joint’s larger flexion and abduction movements.
Flexion occurs when moving the arm forward and up, and abduction occurs when moving the arm out to the side.
The levator scapulae muscles contract during flexion and/or abduction,
The muscles also contract when moving the neck in side bending, lateral flexion, rotation, or twisting.
Symptoms
Neck and shoulder pain are common problems for office workers, truck drivers, and others who sit most of the day for their jobs. It can worsen when there is no spinal support for maintaining correct alignment. Poorly designed work chairs may contribute to chronic muscle tension and spasms, plus they may contribute to muscle weakness. One of the primary functions of the levator scapulae muscles is to keep the shoulder blade in a position that supports a vertical alignment of the head and to prevent forward head posture. (Yoo W. G. 2018)
However, the shoulder blade is an extremely movable bone. Maintaining stability and correct neck posture is not easy. The levator scapulae muscles may not be strong enough to keep the shoulder blade where it’s supposed to be for healthy posture, and instead, they become overstretched. When muscles are overstretched, they often become taut to try to maintain some form of stability. It can feel like muscle tension because the muscles shorten, but there is a difference. The situation can worsen if one slouches, has no lumbar support, and/or the desk or steering wheel is too high or too low, which may force the shoulder blade upward or downward.
Pain Relief
The levator scapulae muscles are two of several shoulder muscles that may contribute when neck pain presents. This is why a qualified, licensed health professional should diagnose any pain or dysfunction in the area. Physical therapy can help get the body back on track. (Yoo W. G. 2018) Treatment may consist of restoring muscle strength and flexibility in the shoulder, neck, and upper back muscles and developing better posture habits. Physical therapy exercises, particularly those that address upper back posture, can help reduce the stress placed on the levator scapulae muscles and can help decrease kyphosis, often a precursor to forward head posture. Stretching, strengthening, and posture lessons will help relieve pain and increase the physical functioning of the upper body. Other tips for avoiding and relieving muscle pain include:
Stretching regularly by gently rotating the neck and shoulders.
Applying heat to promote relaxation.
Regular massage therapy.
Adjusting chairs and/or monitor height to align with a straight line of sight.
Not carrying heavy bags, especially on one shoulder.
Avoiding side sleeping without proper head support.
Injury Medical Chiropractic Clinic
Visiting a chiropractic and physical therapy team can help treat injuries and chronic pain syndromes, relieve pain, resolve musculoskeletal issues, and prevent future symptoms. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized care program for each patient through an integrated approach to help return to normal and optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
The Natural Way to Heal: Non-Surgical Chiropractic Care for Pain Relief
References
Chotai, P. N., Loukas, M., & Tubbs, R. S. (2015). Unusual origin of the levator scapulae muscle from mastoid process. Surgical and radiologic anatomy : SRA, 37(10), 1277–1281. https://doi.org/10.1007/s00276-015-1508-6
Yoo W. G. (2018). Effects of thoracic posture correction exercises on scapular position. Journal of physical therapy science, 30(3), 411–412. https://doi.org/10.1589/jpts.30.411
The muscles in the body help provide motion and protect the skeletal joints from harm. Each muscle group has ligaments, tissues, and muscle fibers that retract, stretch, and contract the body while helping the host to do everyday movements, breath, digest food, stabilize, and even rest. When a person is dealing with pain from a traumatic event or making repetitive motions, it can affect the muscles over time. Factors like not drinking enough water, constantly looking down on the phones, and being hunched over can cause strain on the muscles, causing overlapping pain on top of other chronic issues that may develop. When the muscles begin to cause pain along the shoulders and neck, it can become a risk of developing trigger points in the levator scapulae muscles. Today’s article examines the levator scapulae muscles, how trigger points affect these muscles, and how treatments can help manage the trigger points on the levator scapulae muscles. We refer patients to certified providers who specialize in musculoskeletal treatments to aid individuals suffering from trigger points associated with the neck and shoulders affecting the levator scapulae muscles. We also guide our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure to find that education is the solution to asking our providers insightful questions. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
What Is The Levator Scapulae?
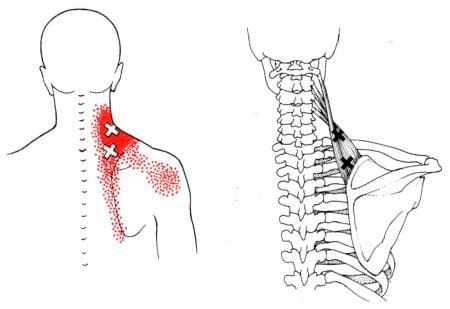
Have you been dealing with pain along the neck or shoulders? Do you feel stiffness when turning your head from side to side? Or do you feel tenderness in the base of your neck and shoulders? Many individuals with shoulder and neck pain risk developing trigger points along the levator scapulae. The levator scapulae muscles originate from the posterior tubercles of the C1 through C4 vertebrae in the neck that is between the superior angle and the root of the scapulae spine. This superficial muscle’s primary function is to elevate the scapulae or the shoulder blades while working together with the trapezius and rhomboid muscles to assist the movement. The levator scapulae muscles also assist in providing neck extension, ipsilateral rotation, and lateral flexion. When pathologies like fibromyalgia, levator scapulae syndrome, or cervical myofascial pain begin to affect the levator scapulae muscles, the symptoms can potentially involve the shoulders and neck to cause referred pain to the upper extremities.
How Trigger Points Affect The Levator Scapulae?
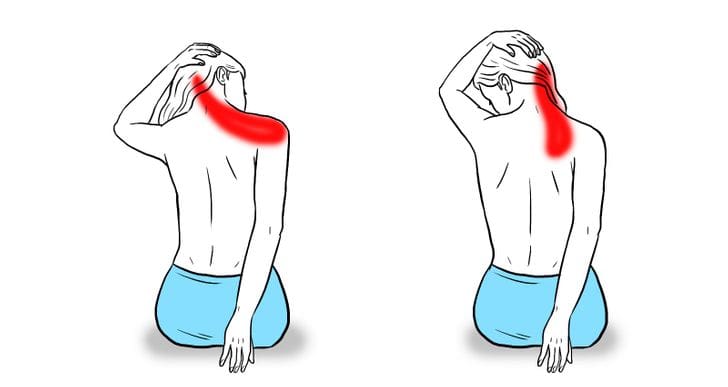
Many individuals with shoulder and neck pain have described radiating pain from their neck to their shoulders. Known as referred pain, the pain is located in one area of the body but in a different location. Studies reveal that when pain radiates from the neck and shoulders, any movements that are overstretching the levator scapulae can aggravate overlapping symptoms on the affected side. This allows small nodules to form along the levator scapulae muscle fibers, causing trigger points to affect the shoulder and neck muscles.
Trigger point associated with the levator scapulae muscles causes the individual to have pain-like symptoms in the neck that causes muscle stiffness. This causes an emphasis on referred pain symptoms from the levator scapulae, like neck tension and restriction of range of motion on the neck. Studies reveal that pain over the superior angle of the levator scapulae is a common musculoskeletal disorder that is often accompanied by radiating pain on the neck, head, and shoulders. Some of the ways that trigger points form along the levator scapulae muscle can be due to ordinary factors like:
Stress
Posture
Over-exercising
Upper respiratory infections
Some of these factors above can shorten the levator scapulae muscle and restrict muscle movement to provide a full range of motion for the head and neck to turn. To that point, treatments are available to help loosen up and stretch the levator scapulae muscles to allow rotation and flexion on the neck and shoulders.
Trigger Points Anatomy On The Levator Scapulae- Video
Have you been dealing with stress that is affecting your neck and shoulders? Have you been dealing with neck stiffness when turning your head? Or have you been feeling muscle tenderness between the neck and shoulders? Some of these symptoms are associated with trigger points affecting the levator scapulae muscles between the neck and shoulder. The video above overviews common trigger points and how they affect the levator scapulae, causing shoulder and neck pain. Since the levator scapulae muscles lay behind the trapezius muscle, studies reveal that trigger points or myofascial pain syndrome can cause hyperirritability in the muscle tissues and affect mobility functions in the nerve ends. Even though referred pain affects the neck and shoulder of the body, treatments are available to manage trigger points on the levator scapulae and relieve neck and shoulder pain.
Treatments To Manage Trigger Points On The Levator Scapulae
When there is trigger point pain affecting the levator scapulae, some common complaints that many individuals often complain about are neck and shoulder pain. However, various ways can alleviate the pain symptoms from the neck and shoulders while managing trigger points associated with the levator scapulae. Studies reveal that stretching the levator scapulae muscle in a seated position can improve muscle length along the levator scapulae and the cervical range of motion. Stretching the levator scapulae muscle can help reduce the pain along the levator muscle. To that point, it even helps reduce muscle imbalances and movement dysfunction along the cervical joints. Many individuals are referred to pain specialists like chiropractors by their doctors to reduce pain and functionality disability in the neck and realign the spine to loosen up the stiff muscles caused by subluxation. Realigning the cervical spine and stretching can reduce future trigger points and reduce pain symptoms from affecting the muscle.
Conclusion
The levator scapulae muscles in the body provide movement functionality to the neck and shoulders. The levator scapulae work together with the trapezius and rhomboid muscles to elevate the shoulder blades and assist with neck extension, ipsilateral rotation, and lateral flexion. When pathologies affect the levator scapulae muscles, they can develop trigger point pain along the muscle and cause neck and shoulder pain. The factors that cause trigger point pain can either be ordinary or traumatic and cause referred pain to the neck and shoulders. Fortunately, treatments like stretching and adjustments can help reduce the pain and loosen up stiff muscles along the levator scapulae. This will allow a cervical range of motion back to the neck and shoulder and elongate the levator scapulae.
References
Akamatsu, Flávia Emi, et al. “Trigger Points: An Anatomical Substratum.” BioMed Research International, Hindawi Publishing Corporation, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4355109/.
Henry, James P, and Sunil Munakomi. “Anatomy, Head and Neck, Levator Scapulae Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 13 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK553120/.
Jeong , Hyo-Jung, et al. “Stretching Position Can Affect Levator Scapular Muscle Activity, Length, and Cervical Range of Motion in People with a Shortened Levator Scapulae.” Physical Therapy in Sport : Official Journal of the Association of Chartered Physiotherapists in Sports Medicine, U.S. National Library of Medicine, 4 Apr. 2017, https://pubmed.ncbi.nlm.nih.gov/28578252/.
Kulow, Charlotte, et al. “Levator Scapulae and Rhomboid Minor Are United.” Annals of Anatomy = Anatomischer Anzeiger : Official Organ of the Anatomische Gesellschaft, U.S. National Library of Medicine, Aug. 2022, https://pubmed.ncbi.nlm.nih.gov/35367623/.
Menachen, A, et al. “Levator Scapulae Syndrome: An Anatomic-Clinical Study.” Bulletin (Hospital for Joint Diseases (New York, N.Y.)), U.S. National Library of Medicine, 1993, https://pubmed.ncbi.nlm.nih.gov/8374486/.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Levator Scapulae (As Seen on Fig. 4.36 Below)
Assessment of the Levator Scapulae
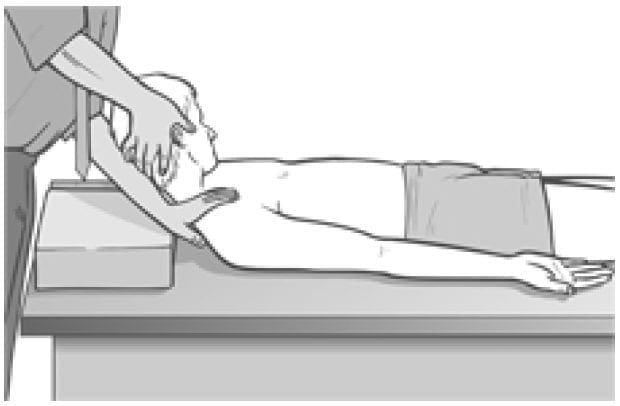
Levator scapula �springing� test (a) The patient lies supine with the arm of the side to be tested stretched out with the supinated hand and lower arm tucked under the buttocks, to help restrain movement of the shoulder/scapula. The practitioner�s contralateral arm is passed across and under the neck to cup the shoulder of the side to be tested, with the forearm supporting the neck. 11 The practitioner�s other hand supports the head. The forearm is used to lift the neck into full pain-free flexion (aided by the other hand). The head is placed fully towards side-flexion and rotation, away from the side being treated.
Figure 4.36 MET test (a) and treatment position for levator scapula (right side).
With the shoulder held caudally and the head/ neck in the position described (each at its resistance barrier) stretch is being placed on levator from both ends.
If dysfunction exists and/or levator scapula is short, there will be discomfort reported at the attachment on the upper medial border of the scapula and/or pain reported near the levator attachment on the spinous process of C2.
The hand on the shoulder gently �springs� it caudally.
If levator is short there will be a harsh, wooden feel to this action. If it is normal there will be a soft feel to the springing pressure.
Levator scapula observation test (b) A functional assessment involves applying the evidence we have seen (see Ch. 2) of the imbalances which commonly occur between the upper and lower stabilisers of the scapula. In this process shortness is noted in pectoralis minor, levator scapulae and upper trapezius (as well as SCM), while weakness develops in serratus anterior, rhomboids, middle and lower trapezius � as well as the deep neck flexors.
Observation of the patient from behind will often show a �hollow� area between the shoulder blades, where interscapular weakness has occurred, as well as an increased (over normal) distance between the medial borders of the scapulae and the thoracic spine, as the scapulae will have �winged� away from it.
Levator scapula test (c) To see the imbalance described in test (b) in action, Janda (1996) has the patient in the press-up position (see Fig. 5.15). On very slow lowering of the chest towards the floor from a maximum push-up position, the scapula(e) on the side(s) where stabilisation has been compromised will move outwards, laterally and upwards � often into a winged position � rather than towards the spine.
This is diagnostic of weak lower stabilisers, which implicates tight upper stabilisers, including levator scapulae, as inhibiting them.
MET Treatment of Levator Scapula (Fig. 4.36)
Treatment of levator scapulae using MET enhances the lengthening of the extensor muscles attaching to the occiput and upper cervical spine. The position described below is used for treatment, either at the limit of easily reached range of motion, or a little short of this, depending upon the degree of acuteness or chronicity of the dysfunction.
The patient lies supine with the arm of the side to be tested stretched out alongside the trunk with the hand supinated. The practitioner, standing at the head of the table, passes his contralateral arm under the neck to rest on the patient�s shoulder on the side to be treated, so that the practitioner�s forearm supports the patient�s neck. The practitioner�s other hand supports and directs the head into subsequent movement (below).
The practitioner�s forearm lifts the neck into full flexion (aided by the other hand). The head is turned fully into side-flexion and rotation away from the side being treated.
With the shoulder held caudally by the practitioner�s hand, and the head/neck in full flexion, sideflexion and rotation (each at its resistance barrier), stretch is being placed on levator from both ends.
The patient is asked to take the head backwards towards the table, and slightly to the side from which it was turned, against the practitioner�s unmoving resistance, while at the same time a slight (20% of available strength) shoulder shrug is also asked for and resisted.
Following the 7�10 second isometric contraction and complete relaxation of all elements of this combined contraction, the neck is taken to further flexion, sidebending and rotation, where it is maintained as the shoulder is depressed caudally with the patient�s assistance (�as you breathe out, slide your hand towards your feet�). The stretch is held for 20�30 seconds.
The process is repeated at least once.
CAUTION: Avoid overstretching this sensitive area.
Facilitation of Tone in Lower Shoulder Fixators Using Pulsed MET (Ruddy 1962)
In order to commence rehabilitation and proprioceptive re-education of a weak serratus anterior:
The practitioner places a single digit contact very lightly against the lower medial scapula border, on the side of the treated upper trapezius of the seated or standing patient. The patient is asked to attempt to ease the scapula, at the point of digital contact, towards the spine (�press against my finger with your shoulder blade, towards your spine, just as hard [i.e. very lightly] as I am pressing against your shoulder blade, for less than a second�).
Once the patient has learned to establish control over the particular muscular action required to achieve this subtle movement (which can take a significant number of attempts), and can do so for 1 second at a time, repetitively, they are ready to begin the sequence based on Ruddy�s methodology (see Ch. 10, p. 75).
The patient is told something such as �now that you know how to activate the muscles which push your shoulder blade lightly against my finger, I want you to try do this 20 times in 10 seconds, starting and stopping, so that no actual movement takes place, just a contraction and a stopping, repetitively�.
This repetitive contraction will activate the rhomboids, middle and lower trapezii and serratus anterior � all of which are probably inhibited if upper trapezius is hypertonic. The repetitive contractions also produce an automatic reciprocal inhibition of upper trapezius, and levator scapula.
The patient can be taught to place a light finger or thumb contact against their own medial scapula (opposite arm behind back) so that home application of this method can be performed several times daily.
Treatment for Eye Muscles (Ruddy 1962)
Ruddy�s treatment method for the muscles of the eye is outlined in the notes below.
Ruddy�s Treatment for the Muscles of the Eye (Ruddy 1962)
Osteopathic eye specialist Dr T. Ruddy described a practical treatment method for application of MET principles to the muscles of the eye:
The pads of the practitioner�s index, middle and ring finger and the thumb are placed together to form four contacts into which the eyeball (eye closed) can rest (middle finger is above the cornea and the thumb pad below it).
These contacts resist the attempts the patient is asked to make to move the eyes downwards, laterally, medially and upwards � as well as obliquely between these compass points � up and half medial, down and half medial, up and half lateral, down and half lateral, etc.
The fingers resist and obstruct the intended path of eye motion.
Each movement should last for a count �one� and then rest between efforts for a similar count, and in each position there should be 10 repetitions before moving on around the circuit. Ruddy maintained the method released muscle tension, permitted better circulation, and enhanced drainage. He applied the method as part of treatment of many eye problems.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine