Chiropractor, Dr. Alexander Jimenez looks at the way this common injury shows itself.
Introduction
Iliotibial band syndrome (ITBS) between the knee is frequently diagnosed in sport injury clinics. ITBS presents having an incidence rate of around 22% in most lower extremity running-related injuries (1) also has been said to be the second most common complaint amongst distance runners (2). ITBS has been given the expression ‘runner’s knee’.
Trainers like endurance runners who perform flexion and extension combined with loading are subjected to this illness. ITBS presents during the first two or three miles in running with no mechanism of injury, which can make identifying the cause more interesting. With plenty of factors having been considered within the literature, changes are often purported to be a cause of ITBS. But some biomechanical factors have been researched and have been found to have little or no effect in the start of ITBS. Therefore this text’s point would be to examine the biomechanical changes which may induce an individual to the beginning of ITBS. The research published reviewed is largely based on a current systematic review that was published in Physical Therapy in Sport in 2014 (3).
Anatomy & Function
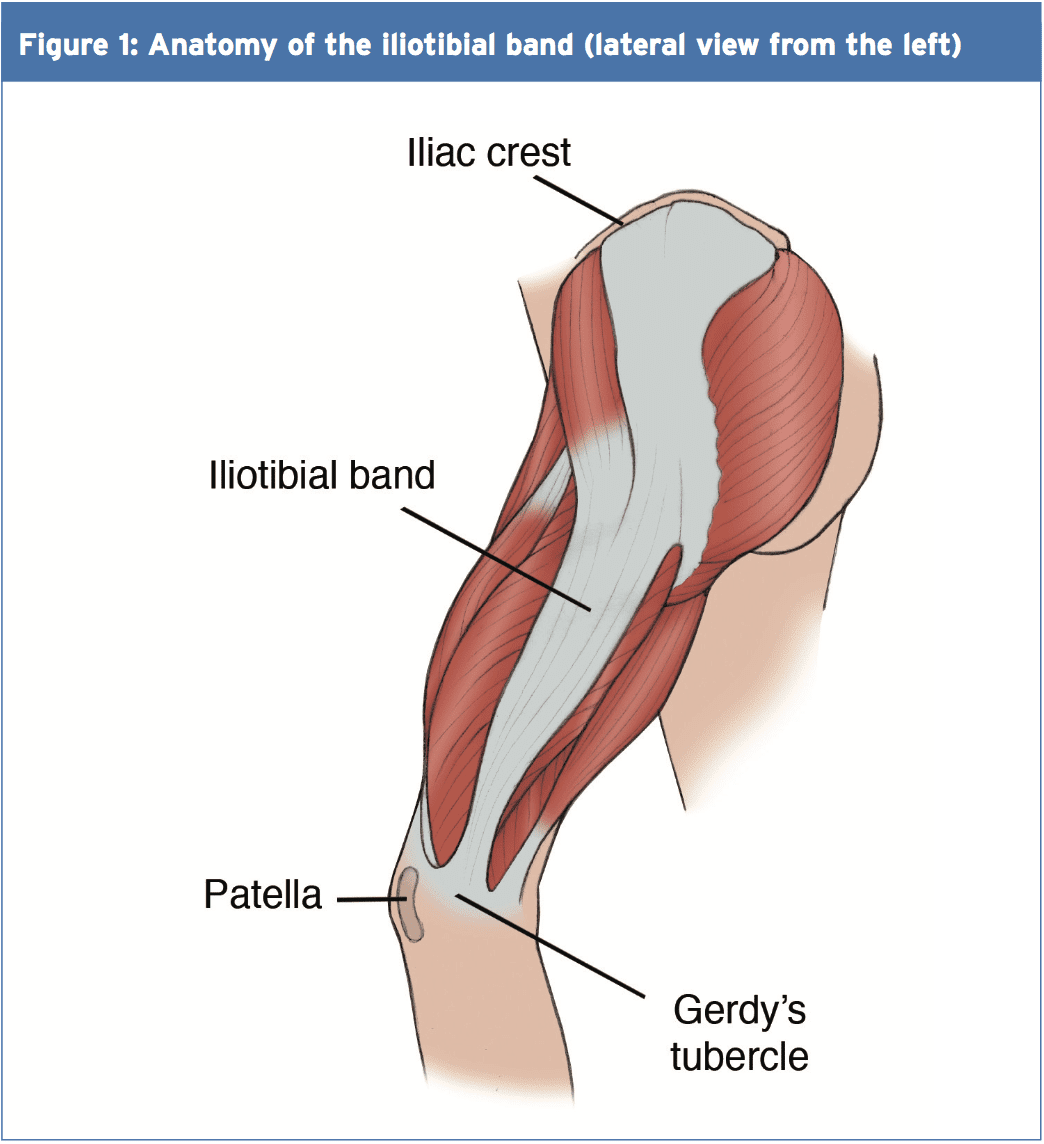
The iliotibial band (ITB) encapsulates the tensor fascia latae (TFL) presenting with both deep and superficial fibre attachments at the pelvis (4). In addition to attaching to the TFL, approximately three-quarters of the gluteus maximus tendon also conjoins with the ITB (4). The ITB courses along the lateral aspect of the hip and passes the greater trochanter. The ITB maintains an attachment on the posterior ridge of the femur whilst attaching itself to the fascia. The ITB has a fixed attachment at the lateral femoral condyle where it then divides into three segments with the first being the lateral patella (3). The remaining two segments cross the knee joint to insert at the head of fibula and most distally at the infrapatellar tubercle also known as Gerdy’s tubercle on the tibia (3). Figure 1 illustrates the location of the ITB.
The ITB passively functions to resist hip adduction, hip internal rotation and internal rotation of the knee in accordance with its attachments at the pelvis, femur and tibia(3). The gluteus maximus functions, through its attachment, to increase stability through the hip and knee complex by increasing the tension of the ITB(4). It is possible to see, based on its attachments at both the knee and hip, how changes could bring about the onset of ITBS.
Studies have proposed that as the knee flexes and extends the ITB ‘slides or flicks’ over the lateral femoral condyle of the knee causing an irritation beneath. This notion was debated by Falvey and colleagues (5), who stated that it was highly unlikely that the ITB would flick or slide over the bone during knee flexion due to it not being a loose structure. But the authors did agree that the impact of compression on the richly innervated fat pad was pain’s cause but by strain of the ITB where pain presents crossing the lateral femoral condyle. Strain rate and strain magnitude were measured in a prospective study involving female runners (6). The results indicated that frequency of strain of the ITB at the lateral femoral condyle was greater that the strain magnitude. This implies that a runner might have the ability to run for a short period but then incur lateral knee pain because of the strain to the ITB.
MRI scans have ascertained the knee flexion angle of 30� elicited the greatest compression of the ITB at the point of heel strike, whereas others have said that maximal compression occurs between 20-30�(2,6). A knee flexion angle at the point of heel strike has been found to be significantly different with 20.6� in ITBS patients compared to 15.3� in the control(7). Downhill running produces a greater knee flexion angle at the point of heel strike eliciting a larger strain load to the ITB and therefore this is often a main precursor to ITBS (6). Although an elevated knee flexion angle at the point of heel strike has been considered to contribute to ITBS, it is essential to examine the lower extremity from the frontal and transverse planes too and not solely from the sagittal plane (2).
Rearfoot Eversion
It’s possible to envisage how rear foot eversion could contribute to ITBS causing internal rotation of the tibia resulting at the distal attachment in greater strain of the ITB. In contrast Ferber and colleagues (2) indicated that there was no significant difference in the peak eversion angle of the female subjects, who were previously diagnosed with ITBS but were now symptom free, compared to controls. In a similar study non-significant differences were found between the currently symptomatic ITBS patients and controls for rear foot eversion (8).
Louw & Deary(3) found that ITBS patients sometimes demonstrated decreased eversion angles, accompanied by decreased internal rotation of the knee, at the point of heel strike. Ferber and colleagues (2) noted an increased inversion moment in the ITBS group which was suggested to control and limit the eversion moment. By comparison, currently symptomatic ITBS patients demonstrated a substantial difference compared to a control group with twice the rear foot motion during running (9).
Knee Internal Rotation
Peak internal rotation angle of the knee was found to be significantly greater in the ITBS patients when compared with controls at the point of heel strike (2). This research was supported by other studies who also found a significant effect for increased internal rotation of the knee following a run of moderate intensity to physical exhaustion(7). With excessive rotation comes compression due to increased strain of the ITB at the attachment.
An explanation of increased internal rotation of the knee was attributed to excessive external rotation of the femur perhaps due to shortening of the piriformis, gemellus inferior and superior and the obutrator externus (8). The authors added that excessive rotation at the hip might result from muscular activity of the rotators that were hip being the medius, minimus and the tensor fascia latae. These studies(2,7) were retrospective in design in that they tested healthy runners with a history of ITB pain, whereas(8) was a prospective study of patients with ITBS at the point of testing.
Hip Adduction Angle & Hip Abductor Strength
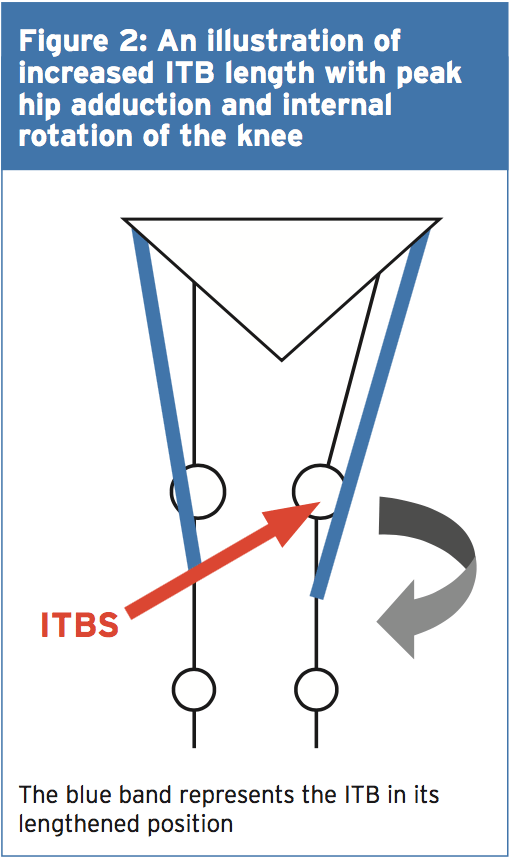
The hip adduction angle during the stance phase has been suggested to be greater. Ferber and colleagues(2) found that the peak hip adduction angle was significantly greater in the ITBS cohort and stated that with 95% confidence. Increased angle results in increased stress to the ITB and consequently increased compression at the lateral femoral condyle when combined with increased internal rotation of the tibia.
Figure 2 illustrates, when peak hip adduction and internal rotation combine, how this may result in increased the compression of the ITB at the lateral femoral condyle. Louw and Deary(3), however, stated that it remained inconclusive whether the peak hip adduction angle was a substantial element. Additional research is therefore required to support Ferber and colleagues'(2) initial findings as this study was a retrospective study carried out on healthy female runners with a history of ITBS.
Hip Abductor Strength
It’s been proposed that an increased peak hip adduction angle may coincide with hip abductor activity involving the gluteus medius in this group. During the stance phase of gait the gluteus medius functions to keep stability. Research has indicated that during stance the adduction forces can exceed three times an individual’s body weight(3). What’s more, it was stated that these forces were beyond the metabolic capacity of the gluteus medius to main pelvic stability during the stance phase using just this muscle alone(3).
Louw and Deary (3) were not able to identify a heightened hip abductor moment in the ITBS patients with increased peak hip adductor angles and suggested that it was more of an issue of timing as opposed to the size of the hip abductors. Louw and Deary (3) stated that the research is yet to examine trunk and pelvic movements in ITBS patients and it is plausible to suggest that biomechanical changes from higher up the kinetic chain has the potential to be a contributing element in ITBS etiology.
A research study of 24 (14 female, 10 male) patients with ITBS undertook a six-week rehabilitation programme to increase the strength of the hip abductors(10). Following six weeks of hip abductor strengthening to running 22 patients reported being pain-free and had returned. The female patients reported an average hip abductor torque increase of 34.9% and the male patients found 51.4% increase. However this study used a hand held dynamometer to measure isometric strength and therefore Fedricson (10) findings should be viewed with caution.
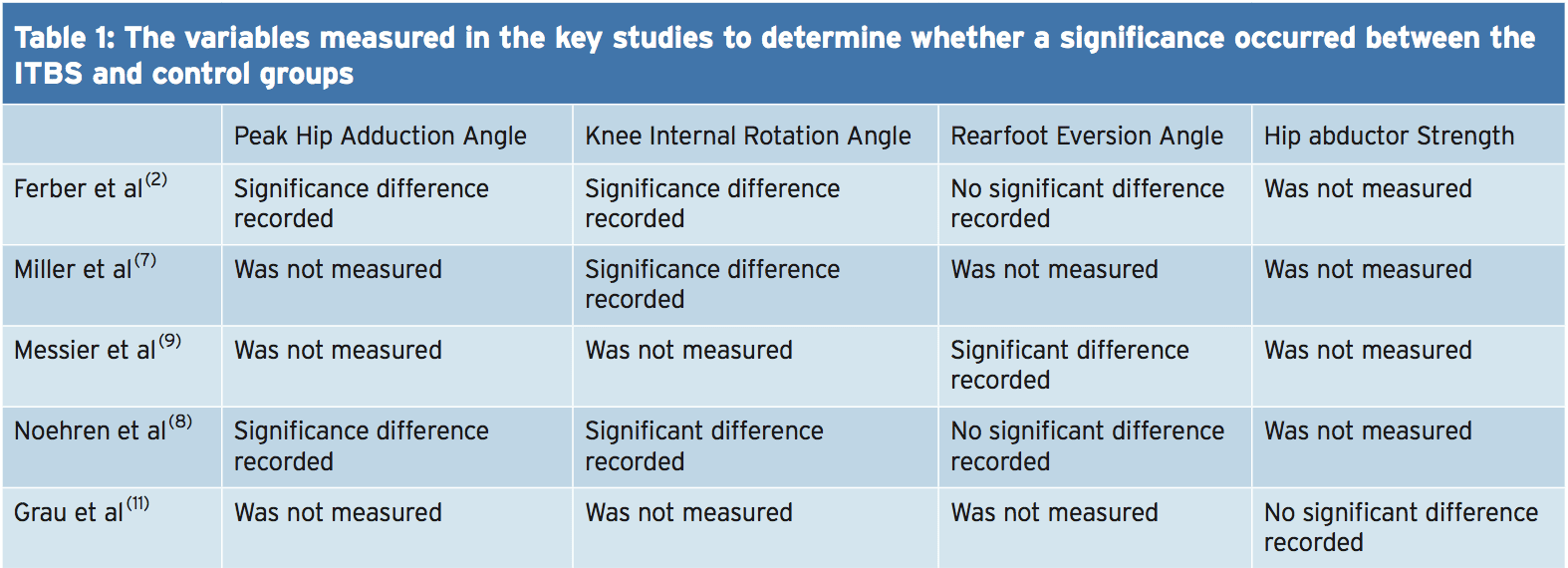
A more recent study assessed the hip abductor strength of currently symptomatic patients with healthy controls in a fixed position(11). The results indicated that no substantial differences occurred for static and dynamic hip abductor strength between the groups. Further research should look into the EMG and strength of the hip abductors in the role of managing ITBS. Table 1 shows of significance in the some of the variables of the studies used in this text.
Rehabilitation programs, following periods of immobilization and during, should include gluteal exercises to provide stability to the leg that is involved. If active exercises for the gluteal muscles are provided in a manner that is secure and effective then this can influence the period of transition from non weight. It’s prudent based on the research provided to date to develop function although research is lacking in terms of quality and volume as to the biomechanical influences on the etiology of ITBS. This guarantees that once load bearing commences that the leg that is involved has the stability and control that is active to keep the beginning of load of the ITB.
Summary
The recent review published by Louw and Deary(3) indicates that much of the research published within the literature depending on the etiology of ITBS is inconclusive. The level of research is relatively low and is based on retrospective trials. The research does indicate that knee biomechanics and abnormal hip is involved in the occurrence of ITBS. The authors ascertain that muscle strength is involved as is foot biomechanics that are abnormal. It is recommended that future research should measure kinematic movements of the hip and knee during downhill running as this is a complaint of ITBS onset.
References
1.Clini J of Sports Med, May 2006,16, (3), 261-268
2.J of Sports Phys Therap, Feb, 2010, 40, 2, 52-58.
3.Phys Therap in Sport, 2014, 15, 64 e75.
4.Surgic and Radiologic Anatomy (Dec) 2004; 26, (6), 433 – 446
5.Scand J of Med & Sci in Sports, Aug 2010, 20 (4), 580-587.
6.Clini Biomech, 2008, 23, 1018-1025.
7.Gait Posture. 2007 Sep, 26 (3), 407-13
8.Clini Biomech, Nov 2007, 22 (9), 951-956.
9.Med Sci in Sport & Ex, 1995, 27, 951-960.
10.Clini J of Sports Med, 2000, 10:169�175.
11. Int J of Sports Med, Jul, 2008, 29 (7), 579-583.
In the first part of the 2-part article on femoro-acetabular impingement (FAI), chiropractor, Dr. Alexander Jimenez discussed FAI and how it can lead to insidious onset abdominal pain and damage the hip joint labrum, leading to early arthritic changes. Given that conservative management generally fails in young athletes and needs operation, part two describes the post-operative rehabilitation period required to take an athlete back to full competition.
The post-operative rehabilitation period is highly dependent on the magnitude of pathology and the subsequent procedure; weight-bearing development is consequently variably reported in the literature.
If the labrum is surgically repaired, then protected weight bearing is encouraged to allow the repair site in order to be protected during the early healing phase. Also, avoiding extremes of flexion (beyond 60�) and also internal/external rotation for the initial 4 to 6 weeks is important to safeguard the repaired labrum. Any positions that possibly create an impingement and boost inflammation ought to be prevented. These include:
Deep squatting
Prolonged sitting
Low couch sitting
Lifting off the ground
Pivoting on a fixed foot
These positions are more safely tolerated following the six week post-operative period. But on account of the selection of hip flexion limitations imposed in the initial six months, usual activities of daily living are rather restricted, making yield to work and daily chores challenging if not impossible from the first few weeks following surgery. Therefore, the post- surgical patient does have to make substantial lifestyle changes and they need assistance in the first six weeks following surgery.
Special precautions in certain types of FAI processes. Reshaping of the femoral head- neck junction can weaken the rectal neck so particular care must be taken in this post- operative period. Fracture of the femoral neck is an unlikely but potentially serious complication after a reshaping process. The athlete may be allowed to bear full weight, but crutches are needed to avoid twisting movements during the initial four weeks after surgery. High impact pursuits and high torsion moves should be prevented in the first 3 months, as bone grafting requires around three weeks to attain full structural integrity.
Furthermore, if microfracture of this femoral head is also done for femoral head cartilage defects, then the athlete ought to be restricted to partial weight- bearing for two weeks so as to optimize the premature maturation of the fibrocartilaginous healing response.
Key points
1. Weight bearing status is dependent on the kind of reshaping procedure, whether the labrum was repaired, and also what the surgeon favors
2. Steer clear of hip flexion beyond 60� in the first 4-6 Weeks
3. Avoid extremes of rotation
Post-Surgical Rehab
Rehabilitation protocols provided in the literature have a tendency to be quite generic in their own advice and at best explain broad transitional phases during the rehab process. They usually describe the transition in weight bearing status, the development of gait through walking into jogging, and give general guidelines as to how to and when to progress activity based on a time dependant strategy.
They then progress describing transitions into twisting and affect actions — usually explained as beginning at 3 weeks following surgery — and generally the guidance is that the speed with which the athlete progresses is variable and might need yet another 1 to 3 months to get full return based on the game. Trainers are usually advised that return to sports after surgical correction of FAI can require 4 to 6 weeks. However it’s critical that progression through rehabilitation phases is driven more by subjective and objective measures during the transition phases. This allows the athlete and therapist to track load (type and quantity) and ascertain whether the joint arrangements are able to withstand changes in load securely.
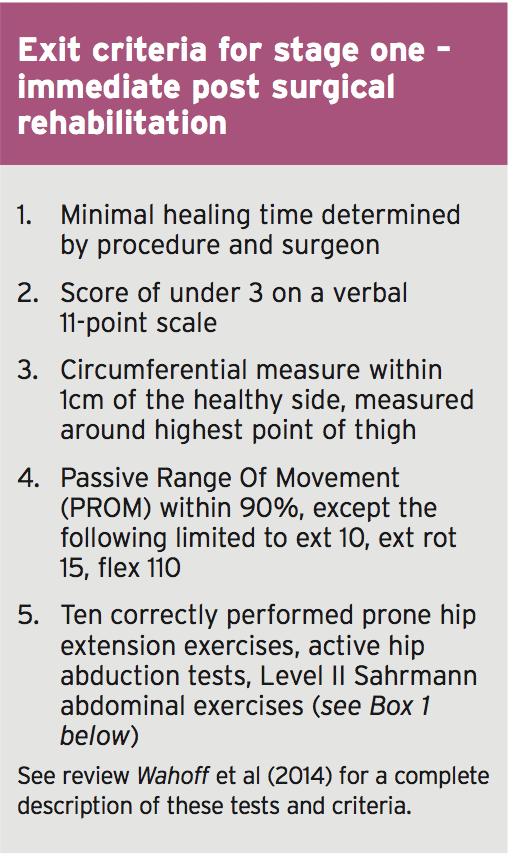
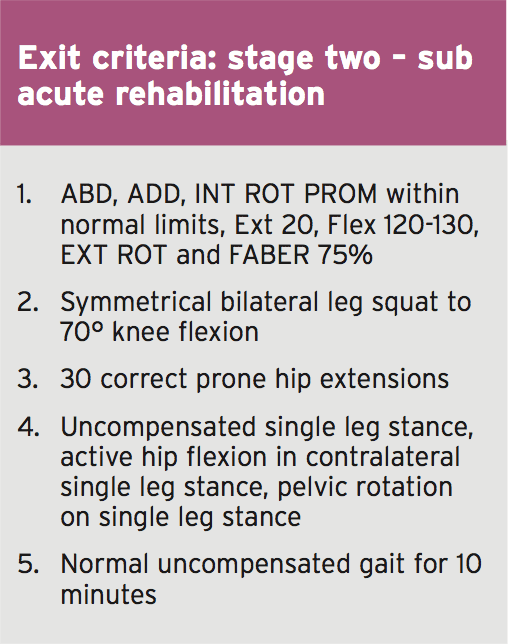
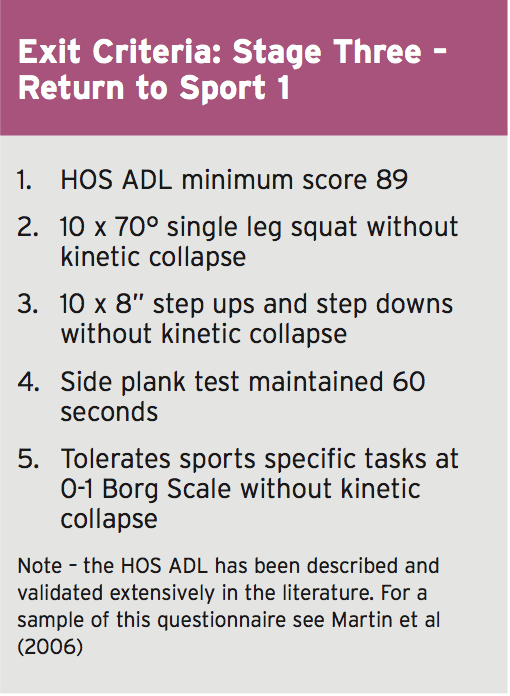
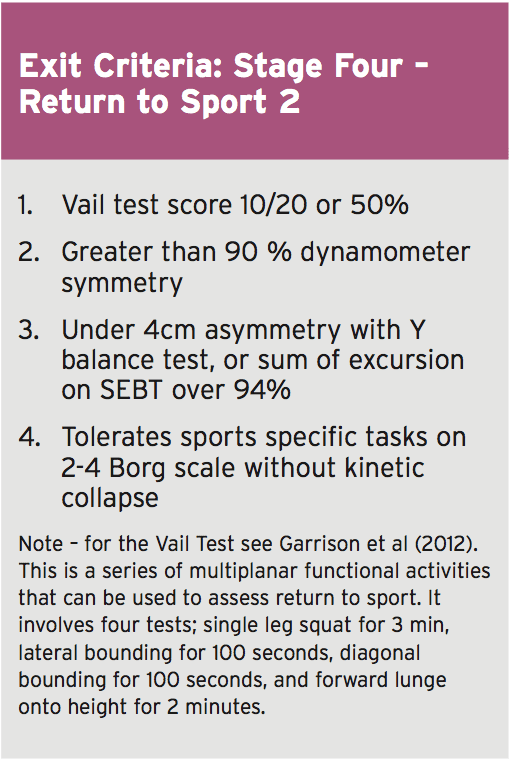
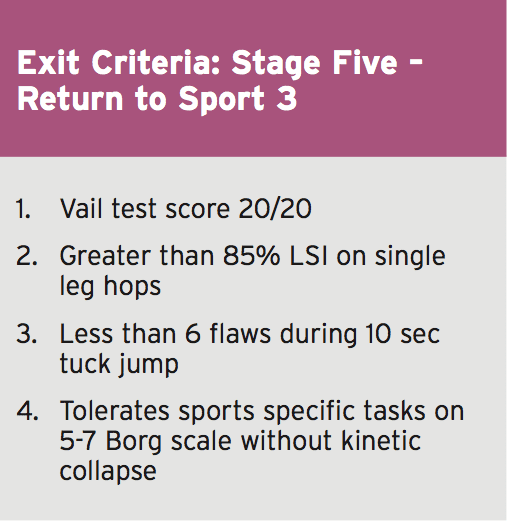
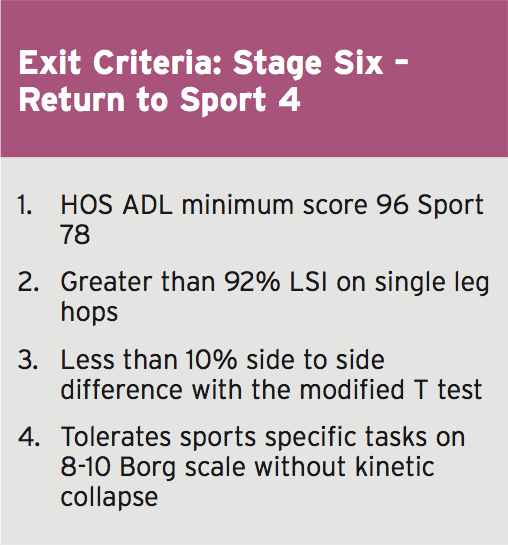
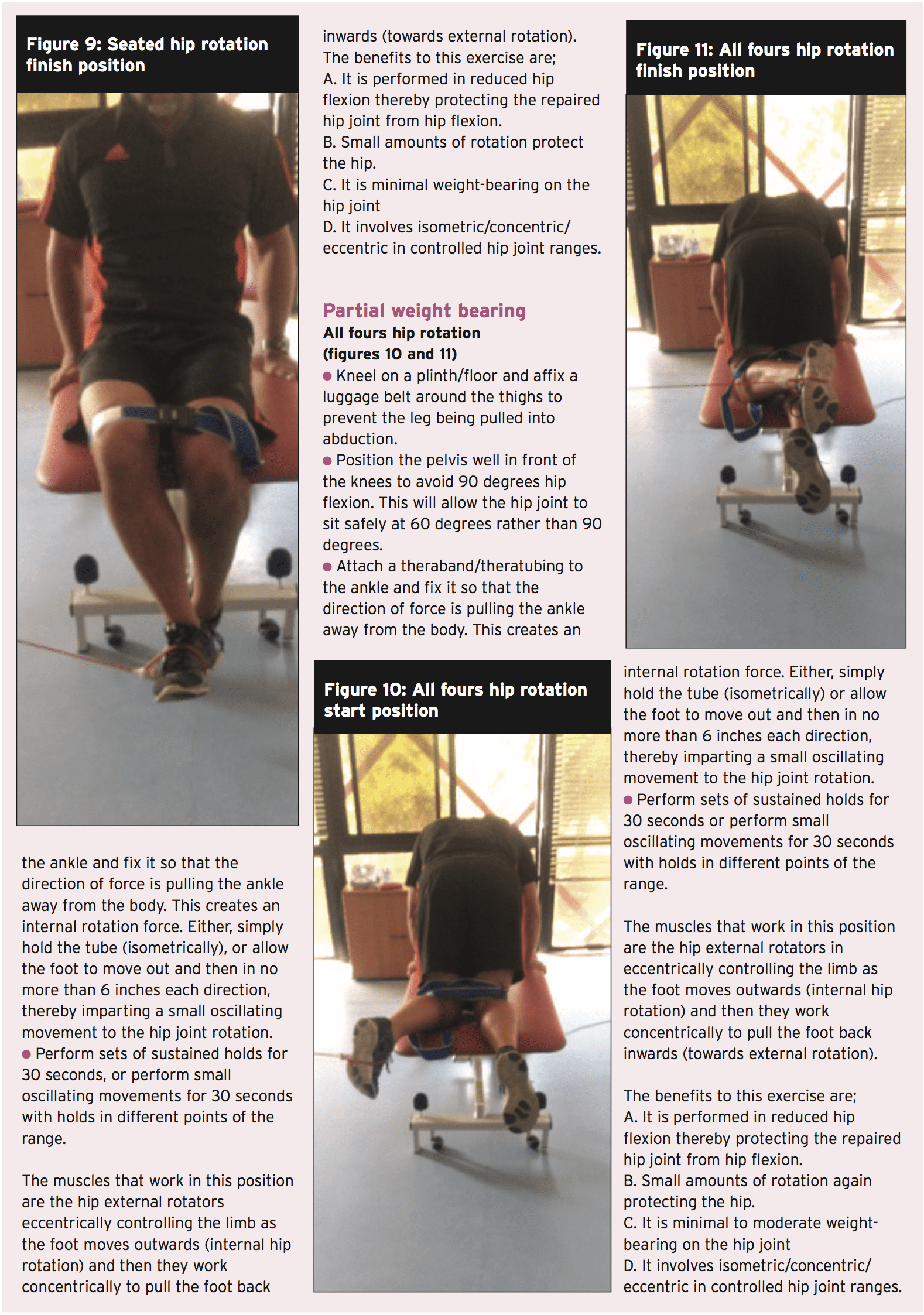
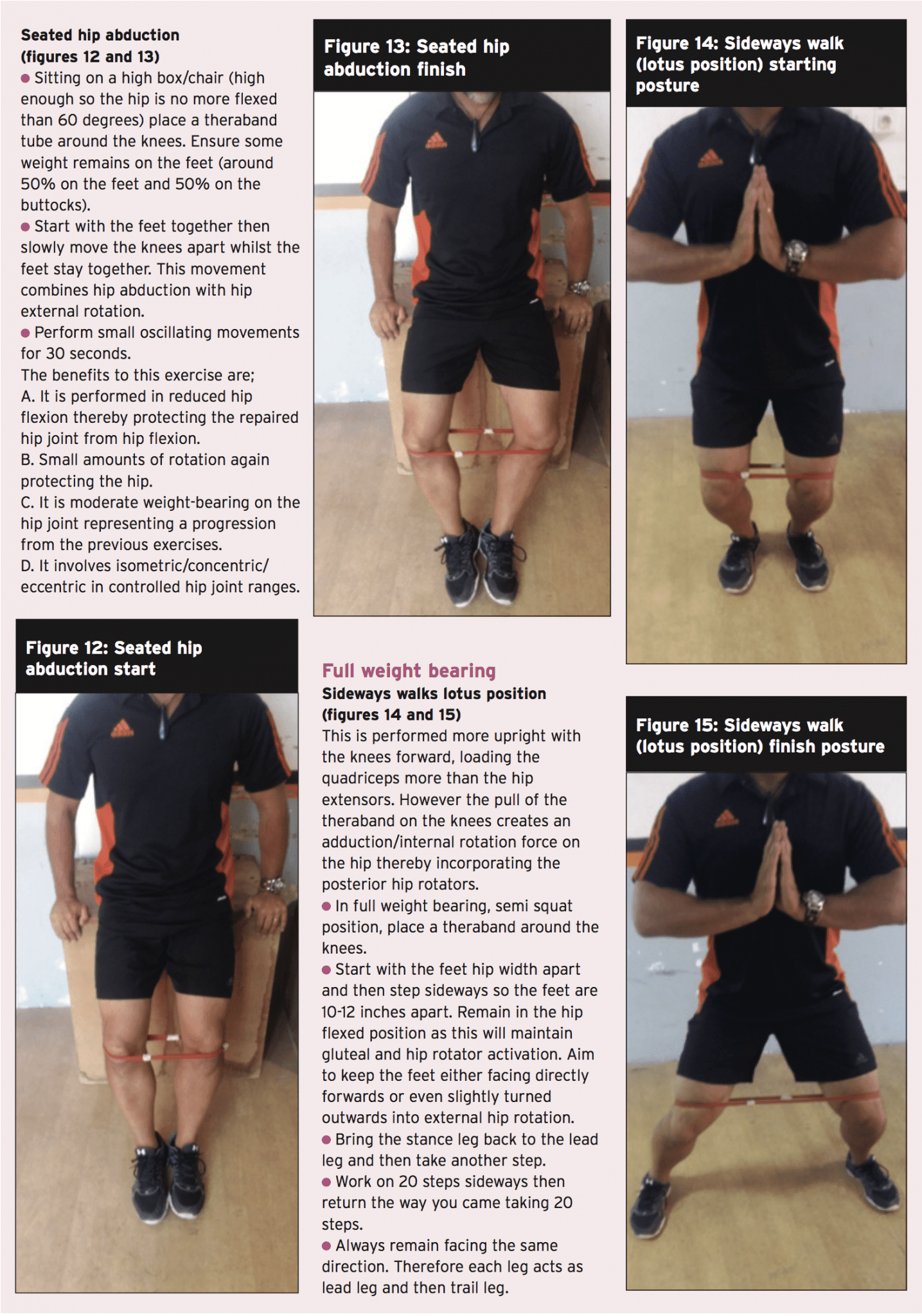
Wahoff et al (2014) have provided some standards which may be utilized to guide the transition from one point to the next(1). They describe their rationale and supply a complete description of all of the cited tests in their printed clinical comment. Essentially, the exit criteria they offer in each phase are as follows;
So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading.
But more direct physiotherapy Interventions have been devised to direct the physiotherapist through the rehabilitation protocol. The Takla-O�Donnell Protocol (TOP) is a validated physiotherapy intervention program which may be utilized to induce the arthroscopically handled FAI patient (Bennel et al)(2).)�This protocol is shown in box 2.
Hip Muscle Control
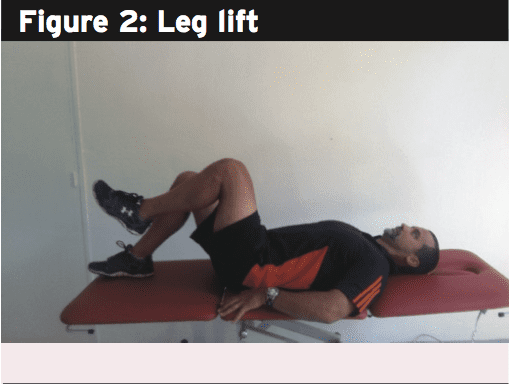
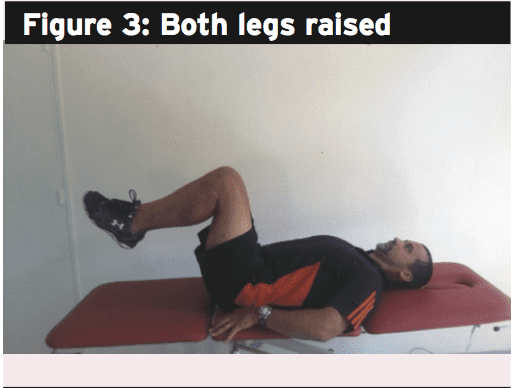
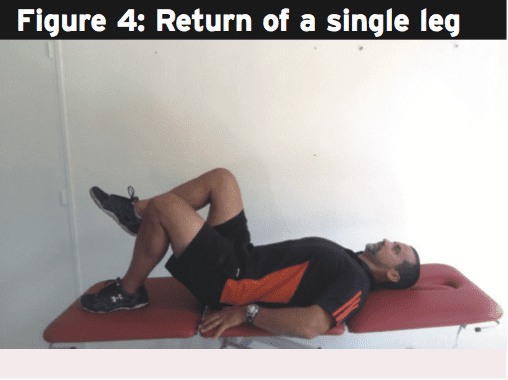
The focus of the rest of this article Will be to summarize some common yet powerful hip strengthening exercises which may be used to progress the hip muscle control throughout the rehabilitation phases.
Regaining hip muscle power, particularly in the heavy hip external rotator group, is imperative from the FAI recovering athlete. Good muscle endurance and strength in those muscle groups will ensure adequate hip joint compression happens with motion to reduce any shearing effect between the head of femur and acetabulum(3). The muscle groups needing focus are (see figure 5):
Posterior fibres Gluteus Medius (PGMed)
Gluteus minimus
Superior and Inferior Gemellus
Internal and External Obturator
Quadratus Femoris
Piriformis
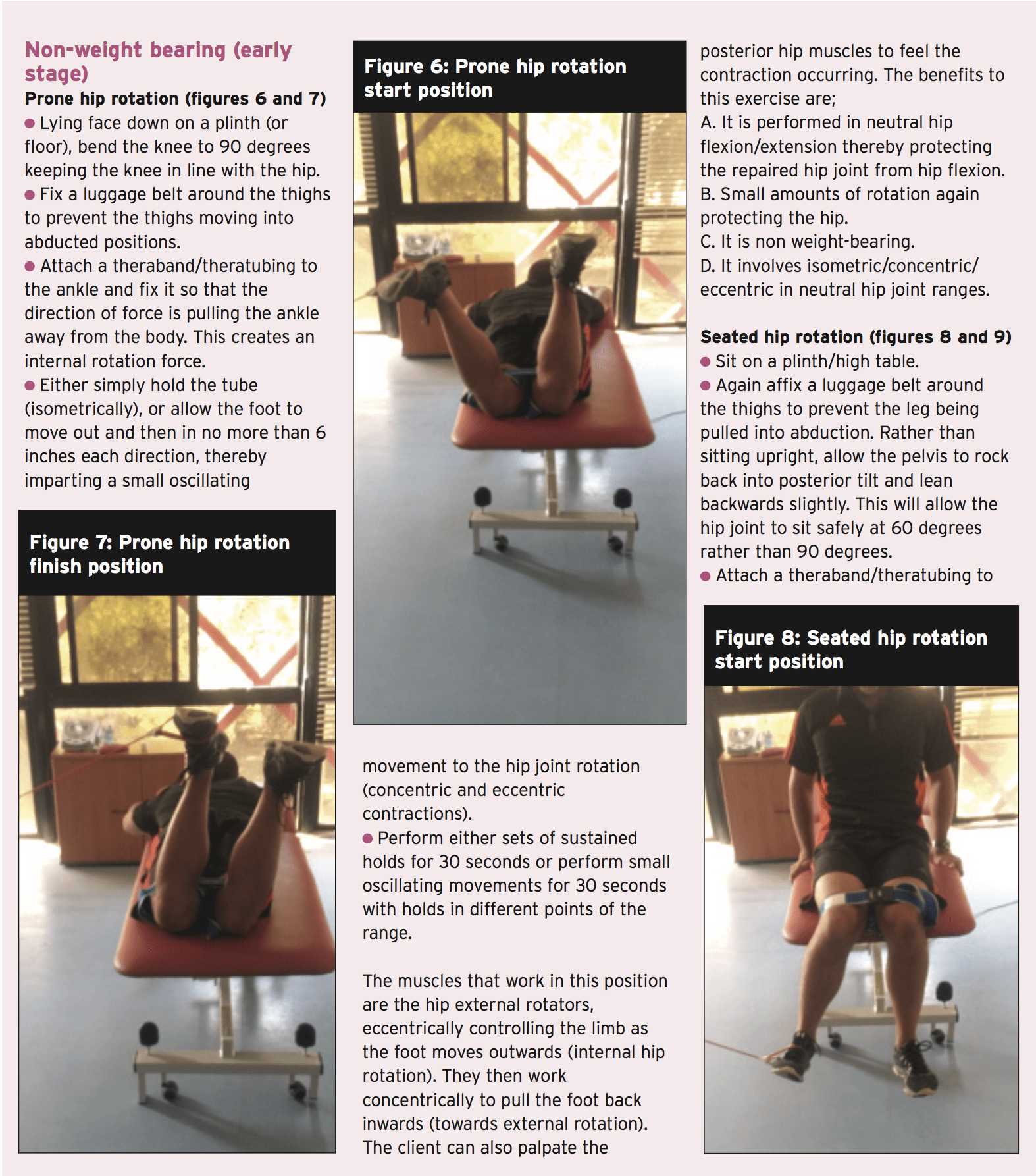
There’s plenty of exercises that can be utilized to fortify the hip joint musculature. The chosen ones below are a sample of some effective exercises that can be used throughout the rehabilitation phases. However, the key requirements of the contained exercises include:
1. Performed in neutral stylish places to no more than 60 degrees hip flexion. This range of movement protects the hip joint from any possibly damaging impingement.
2. Minimal rotation of the hip, letting them be used in most stages of the rehabilitation process.
3. Performed isometrically or utilizing little oscillating concentric/eccentric contractions — to contract and hold to maintain the hip joint compacted and stable. This represents how these muscles work in individual function.
Summary
In many ways. hip joint labral tears, capsule sprains, cartilage and muscle accidents and bony architectural issues like FAI can all lead to debilitating hip pain. FAI is a real concern for the athlete as the existence of a bone abnormality may lead to a painful hip impingement, damage to the acetabular labrum and premature onset degeneration. FAI’s don’t respond to conservative management. If the athlete suffers debilitating pain that affects competition then the options are either to cease competition all together or have the FAI surgically corrected. Once corrected by the surgeon, regaining complete motion and muscle strength and ultimate game related functional skills will require some time. Hip rotator muscle strengthening must shape the foundation of all handling post-surgical FAI issues.
References
1. International Journal of Sports Physical Therapy. 9(6); pp 813-826
2. Arthroscopy. 2006;22(12):1304-1311
3. Int J Sports Phys Ther. 2012;7(1):20-30.
In the last two writings we explored how low speed collisions can have substantial energy transfers with minimal (if any) damage. Here we will discuss the myth of “no damage = no injury” from a vehicle appearance / design point of view and how it relates to injury in a collision.
So as to get into this subject, we need a little history lesson first. With vehicle style being the topic of focus, the industry exploded after World War II. The jet age influenced bumpers, headlights and taillight’s fins. Something else happened too, for the first time in the automobile’s history, vehicles were more than “around town” horse-less buggies; the power of their engines and speeds potential dawned a whole new arena — security. In the 1960’s vehicle aesthetics began to compromise with safety. Automotive designers started to consider topics like; occupant restraints structural integrity, and crash worthiness.
The industry faced slow growth and change into the 1980’s, each revision or change did bring with it progress and progress but not enough at any one time to be a huge leap forward. The changes which were necessary, were too experimental, too cost prohibitive, or just too market risky. Then in the 1980’s a revolution in business started to take hold — the computer. The personal computer allowed for design changes to be done with efficiency. Once plugged in and switched on the days spend calculating double function and variables became complicated than a few clicks.
The computer made it possible for car manufacturers to reduce years of conventional design and research practices into only a month or two and at the same time it allowed for much more cost effective experimentation and new process development.
No Vehicle Damage Doesn’t Guarantee No Injuries
Now that We’ve completed history 101 let Us discuss the topic of Stage – “no damage = no injury”
Vehicle layout, as an approach or concept, has undergone a considerable overhaul in recent years. The change has influenced the use of bumper covers. The long standing tradition in design is to make them of a alloy and to put the outside or separate from the body. (Consider all those classics in “American Graffiti”). The bumper was designed to function as a compliment to the vehicle’s appearance. The safety perspective was non-existent with respect as they were no longer than a sacrificial lamb to save the body.
In the early 1970’s federal mandates designed to make vehicles safer forced the producers to engineer larger and much more structurally sound designs. The most noted changes where the moving of bumper away from the body itself to an essential part of the car’s body. This “afterthought” look borrowed from the truck world was the standard until the late 1980’s. Three things changed in the 1980’s: First, bumpers began to move to behind urethane bumper covers in usage.
This gave a look to vehicles and assisted with aerodynamics. Because aesthetics were no more part of the equation, bumpers became stronger and included the use of energy absorbing material between the bumper structure and the bumper cover. Finally, automotive paints had also advanced, including the ability to resist cracking & flaking, and paint had become elastic.
These changes also had another positive side effect; because of the elastic properties of urethane and the paint, minor collisions, even those which damaged the bumper behind them, no longer seemed as serious. Often times a bumper cover needed more than some paint and prep, where past designs necessitated changing the bumper.
The largest change between older design and the new one, is the inherent elasticity of the new bumper covers. These covers can, and do, rebound into the design they have been formed in and the use of paint that is elastic means the paint is likely to rebound as well. The assessment of speed from damage is currently poorer while signs of impact are evident. Obviously when a steel bumper is distorted it remains that way leaving no room for underestimation.
Notice how we have not discussed these design changes have gained energy transfer; and this isn’t any mistake. There are no groundbreaking points. Changes in vehicle design is not going to ease violation of laws of physics. All these design changes is make the energy transfer in a low speed crash less costly and less apparent.
Evaluating Vehicle Damage
However, there are Just demonstrable measures that can be taken to assess the effects of energy transfer in no apparent damage collisions:
Remove the cover of the bumper and inspect the materials below the “skin” of the bumper for internal damage
Check the angle of the passenger seat. The factory at a angle and when the occupant is thrown backwards, often the seat angle changes rendering evidence of force transfer sets seats
Have the swivel tested with a laser apparatus most repair shops use to make sure the frame of the car is “plumb.” Even a 1-degree variation will be evident and often the chassis gets distorted and that requires energy transfer.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
“The clinical diagnosis shows a disc bulge in their neck and some arthritis, so their neck symptoms are not associated with the crash. Lots of folks have those and do not have pain although it could be a minimal herniation. It’s our diagnosis that it was there before the crash.” This statement from an adjuster is an argument that has been made for many years, allowing insurance companies to inappropriately reduce settlements to their clients based on the client’s inability to prove when or how the damage or injury occurred. To factually counter this sort of statement, an individual must use imaging and age dating to discuss causality. Without medical experts utilizing the current medical and academic research available, it will continue to be difficult for any argument to be made explaining effects of these injuries and their mechanism based on fact vs. rhetoric.
Imaging of the spine is critically important in most cases of injured clients. In cases, imaging is necessary for proper diagnosis and future management of injuries. Imaging needs to be performed as per the academic and modern criteria to ensure an accurate diagnosis. The most common injuries in car accidents are spinal related, and the simple imaging available includes x-rays, CAT scans and magnetic resonance imaging (MRI), allowing medical providers to make an accurate diagnosis, when medically indicated.
Every medical provider has a permit to see and treat automobile related injuries. However a “license” is not the same as “specialization.” By way of example, though psychiatrists may have a license to do heart surgery and are MDs, it would not be in the patient’s best interest. Nor would I go to a spine surgeon for psychological concerns although they are licensed to treat medical conditions. In spinal trauma, certain suppliers specialize in connective tissue injuries of the spine, allowing us to go one step farther in diagnosis, prognosis and management, including “age-dating” these generally found disc and ligament injuries.
Understanding Age-Dating of Injuries
To understand age-dating, one wants to have a basic medical understanding of anatomy and physiology, and what tissue is commonly injured and the probable “pain generator”. Since neck injuries are the most common injuries cervical joints will be our focus. Related to anatomy, every set of two vertebrae in the neck is connected with three joints; two facet joints and a single disc. These joints allow for normal movement of the spine (mobility). There are multiple ligaments that are responsible for stability and hold together these joints. The correct balance of mobility and stability is critical when looking at the part of patient’s injuries, meaning that too little or too much movement in spinal joints can lead to pain, secondary to damaged tissue. The tissue most commonly hurt in a car crash is nerve, ligament, disc, facet and muscle/tendon. Spinal cord and bone injuries also happen although less frequently. To determine causality, the supplier should comment on what tissue is injured, and also use imaging to help determine if this injury occurred (age-dating).
There are two fundamental problems that must be addressed. Fardon and Milette (2001) reported, “The phrase ‘herniated disc’ does not infer knowledge of cause, relation to trauma or activity, concordance with symptoms, or need for treatment” (p. E108). Simply having a disc herniation’s presence, without a physical exam or without symptom documentation that is appropriate, does not allow one to comment on the cause of the injury. In a rear impact collision by way of example, even if the diagnosis is confirmed, additional criteria will need to be fulfilled to answer the question of “Was there sufficient force generated into the vehicle and the occupant to induce the cervical/lumbar herniation?” Fardon, in a follow-up study (2014) reported that disc injury “in the absence of significant imaging evidence of associated violent injury, should be classified as degeneration rather than trauma.” (p. 2531). Thus, we must more objectively define the subjective connotations of “violent injury” and address the issue of “degeneration as opposed to trauma”. Although this statement can frequently be misleading, it gives the trauma trained expert doctor a basis in going forward understanding that every patient’s physiology is unique and not subject to rhetoric, but clinical findings.
Violent injury to the occupant can occur when there are sudden acceleration and deceleration forces (g’s) generated to the neck and head which overwhelm connective tissue or pull them past their physiological limit. To determine the acceleration force, ?V (delta V) is utilized. ?V is the change in speed of the occupant vehicle when it is hit from behind (i.e., going from a stopped position to seven mph in 0.5 seconds because of forces moved from the “bullet” vehicle to the “target” vehicle). Utilizing these data, research allows us to make specific comments related to violent injury. Since the cervical spine is subjected to shearing forces, and compression, tension we are oversimplifying. Along with g-forces and the elastic nature of the majority of rear impact crashes makes it almost impossible to discover an actual minimum threshold for injury even though the literature has given us many examples of low-speed crashes which are dependent not simply on speed, but the mass (weight) of the subject vehicles. Each individual’s susceptibility to injury is unique. While g-forces alone are insufficient to predict injury, Krafft et al. (2002) reported that in low-speed collisions there’s an injury threshold of 4.2 g’s for males and 3.6 g’s for females. Krafft’s analysis is unique in that she has access to insurance data inaccessible to researchers. Panjabi (2004) revealed that forces as low as 3.5g impacts would lead to damage to the front of the disc, and 6.5g and 8g impacts would lead to disc damage posteriorly where the neurological components are.
Diagnosis for Disc and Ligament Injuries
A spinal biomechanical expert can look for evidence that is conclusive by disc and pathology, according to two phenomena. First, it is recognized that the body is electric. We’re measuring activity to diagnose when an EMG is done. Second, there are bioelectrical fields in all tissues. This typical field is disrupted when an injury occurs, and in the case of joints calcium is drawn to the damaged tissue. Issacson and Bloebaum (2010) reported “The particular loading pattern of bone has been documented as a significant piezoelectric parameter since potential gaps in bone have been known to be due to charge displacement during the deformation period” (p. 1271). For the patient, we have the ability to tell just how much of this process has occurred before or after their crash, especially if we take into consideration the tissue damage and signs of bone/calcium deposition.
In addition, the body begins a healing process that includes regeneration and remodeling of the soft and hard tissue as reported by Issacson and Bloebaum (2010). Spinal vertebrae have a unique structure of bone which allows it to adapt to abnormal mobility and stability (injury) by changing shape, which can be found on radiographs or MRI. Moreover, shape will change according to patterns based on the pressure or load it undergoes post-injury. Issacson and Bloebaum stated that “Physical forces exerted on a bone change bone structure and is a well-established principle…” (p. 1271). This is a further understanding of a scientific principle called Wolff’s law established in the 1800’s. Because we know what “normal” is, when we see “abnormal” findings as a result of mechanical stress we could broach the topic of an acute injury versus a degenerative process being the cause of the abnormality and create specific medical predictions accordingly.
He and Xinghua (2006) studied the predictability of the bone remodeling process and were able to make predictions of pathological changes that will occur in bone, specifically the osteophyte (bone spur) on the edge of a bone structure. Significantly, they noted their findings “confirmed that osteophyte formation was an adaptive process in response to this change of mechanical environment”. They noted that factors are crucial to the morphology of bones, particularly bones such as the femur and vertebrae.
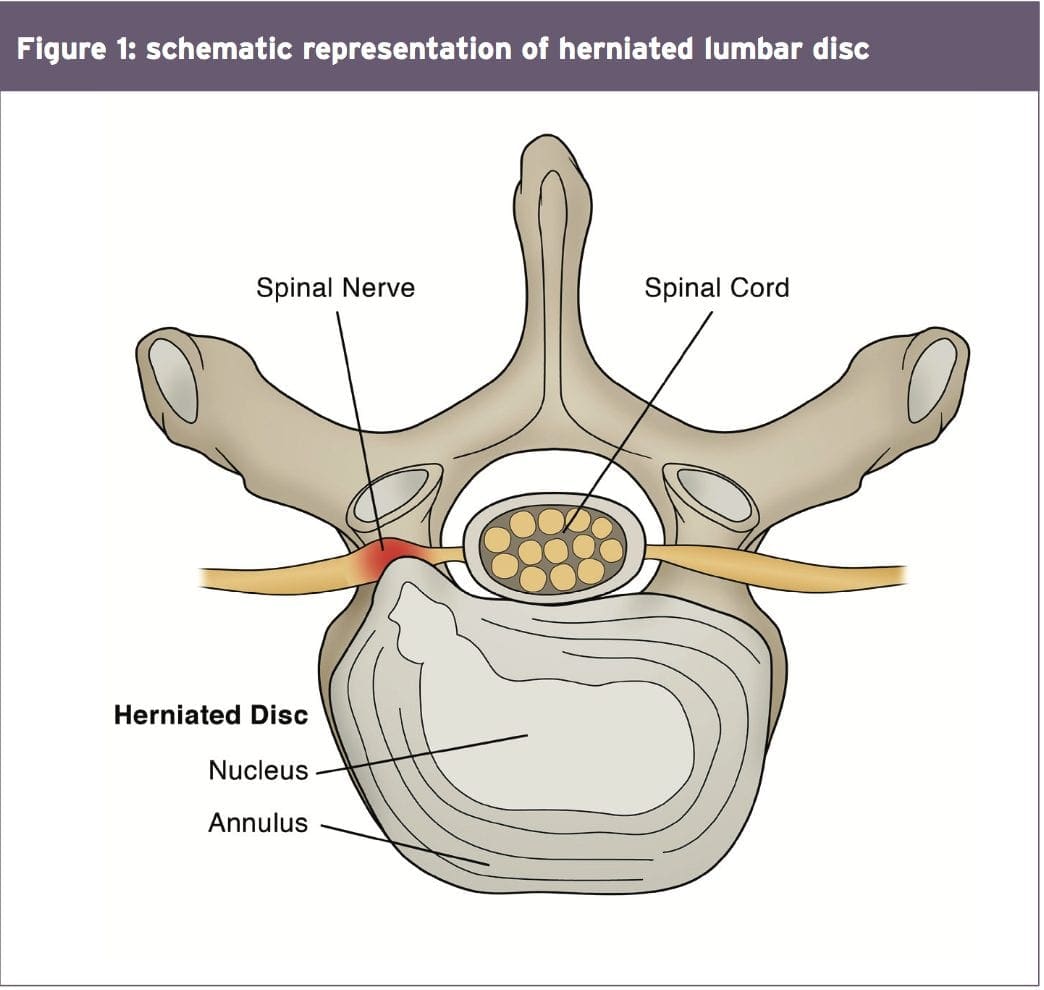
For readers familiar with current academic and medical accepted nomenclature for disc injury, recognized from the combined task forces of the North American Spine Society (NASS), the American Society of Spine Radiology (ASSR) and the American Society of Neuroradiology (ASNR), disc herniations must have a directional component. When this occurs, the additional and abnormal pressure at the level of the disc damage matched with the direction of the herniation will cause that section of the vertebrae.
Thus, if there’s a C5/6 right sided herniation (protrusion/extrusion) secondary to a cervical acceleration/deceleration injury, then only that side of the vertebrae will change shape, creating an osteophyte. Facet arthritis is additionally caused by this compounded loading on the facet joint. This process is very similar to the formation of a callous on your hand or foot. The callous is a recognized and expected tissue response to increased load/friction exposure. Similarly, an osteophyte is a known and anticipated bone response to a rise in load/friction exposure.
At a basic level, the body has an electrical and mechanical response to injury leading to additional stress that leads to calcium (bone) to flow in the region of injury to further support the joint. The joint then abnormally grows, developing a called hypertrophy, degeneration, disc osteophyte complex, or arthritis/arthropathy, common terms seen in the reports of doctor and radiology.
Everybody is subject to these morphological (structural) changes, always and predictably determined by mechanical imbalances in the spine. He and Xinghua (2006) concluded that, “…it will actually take about over half a year to discover the bone morphological changes…” (p. 101). This indicates that it takes approximately six months to get an osteophyte (bone spur) to be demonstrable post-mechanical breakdown or failure. This again provides a time frame to better understand whether pathology of the intervertebral disc has been present for a long period of time (pre-existing) or has been produced as the direct result of the specific traumatic event by deficiency of the existence of an osteophyte, meaning the disc pathology is less than six months old, dependent on location and management of the pathology.
Conclusion
In conclusion, that by definition, a disc is a ligament connecting a bone to a bone and it has the structural responsibility to the vertebrae above and below to maintain the spinal system in equilibrium. Damage to the disc because of a tear (herniation or annular fissure) or a bulge will create abnormal load-bearing forces in the injury site. These present differently based on [1] if traumatic failure on the side of the disc lesion, or [2] if age related, as a general complex. Since other research and human subject crash testing have defined the term “violent trauma” as not being dependent upon the amount of damage done to the vehicle but rather to the forces to which the neck and head are exposed, we can now accurately predict in a demonstrable way the timing of causality of this disc lesion. This depends upon the symptomatology of the the morphology of the structure and is a subject that can be predicated upon speculation or rhetoric.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
Fardon, D. F., & Milette, P. C. (2001). Nomenclature and classification of lumbar disc pathology: Recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology.�Spine, 26(5), E93�E113.
Fardon, D. F., Williams, A. L., Dohring, E. J., Murtagh, F. R., Rothman, S. L. G., & Sze, G. K. (2014). Lumbar Disc Nomenclature: Version 2.0:�Recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology.�Spine,�14(11), 2525-2545.
Krafft, M., Kullgren, A., Malm, S., and Ydenius, A. (2002). Influence of crash severity on various whiplash injury symptoms: A study based on real life rear end crashes with recorded crash pulses.� In�Proc. 19th�Int. Techn. Conf. on ESV, Paper�No. 05-0363, 1-7
Batterman, S.D., Batterman, S.C. (2002). Delta-V, Spinal Trauma, and the Myth of the Minimal Damage Accident.�Journal of Whiplash & Related Disorders, 1:1, 41-64.
Panjabi, M.M. et al. (2004). Injury Mechanisms of the Cervical Intervertebral Disc During Simulated Whiplash.�Spine 29 (11): 1217-25.
Issacson, B. M., & Bloebaum, R. D. (2010). Bone electricity: What have we learned in the past 160 years?�Journal of Biomedical Research, 95A(4), 1270-1279.
Studin, M., Peyster R., Owens W., Sundby P. (2016) Age dating disc injury: Herniations and bulges, Causally Relating Traumatic Discs.
Frost, H. M. (1994). Wolff’s Law and bone’s structural adaptations to mechanical usage: an overview for clinicians.�The Angle Orthodontist, 64(3), 175-188.
He, G., & Xinghua, Z. (2006). The numerical simulation of osteophyte formation on the edge of the vertebral body using quantitative bone remodeling theory.�Joint Bone Spine 73(1), 95-101.
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
In the first part of this 2-part series, chiropractor, Dr. Alexander Jimenez looked at the likely signs and symptoms of disc Herniation, in addition to the selection standards for micro-discectomy surgery in athletes. In this report he discusses the lengthy rehab period following a micro-discectomy procedure, and provides a plethora of strength based exercises.
Surgeries to ease disc herniation, with or without nerve root compromise, comprise traditional open discectomy, micro-discectomy, percutaneous laser discectomy, percutaneous discectomy and micro- endoscopic discectomy (MED). Other surgical conditions are employed in The literature like herniotomy that’s interchangeable with fragmentectomy or sequestrectomy. The saying ‘herniotomy’ is defined as removal of the herniated disc fragment just, and the ‘standard discectomy’ as elimination of the herniated disc along with its degenerative nucleus in the intervertebral disc space.
When surgery is required, minimizing tissue disruption and strict adherence to an aggressive rehabilitation regimen may expedite an athlete’s return to perform(1), that explains why micro discectomy is a favored surgical procedure for athletes. Micro discectomy procedures entails Removing a small part of the vertebral bone over a nerve, or removing the fragmented disc stuff from under the compressed nerve root.
The surgeon can then enter the spine by removing the ligamentum flavum that insures the nerve roots. The nerve roots can be visualized with functioning eyeglasses or with an operating microscope. The surgeon will then move the nerve to your side and to subsequently remove the disc material from beneath the nerve root.
It’s also sometimes required to eliminate A small portion of the related facet joint to permit access into the nerve root, and additionally to relieve pressure on the nerve root resulting in the facet joint. This procedure is minimally invasive since the joints, muscles and ligaments are left intact, and the process doesn’t interfere with the mechanical construction of the spinal column.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques.�From the El Paso, TX. Spine Center.
Surgical Outcomes
In general, athletes with lumbar disc Herniation have a favorable prognosis with traditional therapy; more than 90 percent of athletes using a disc herniation improve with non-operative treatment. Many demonstrate a response to conservative treatment with increased pain and sciatica within 6 weeks of the initial onset(2). This implies that the requirement to function immediately could be considered hasty.
However, in case of failed Conservative therapy, or together with the pressure of a significant upcoming competition, surgery might be needed in some instances. Even though it involves surgical therapy, micro-discectomy has been reported to have a high success rate — over 90 percent in some studies(3,4). Patients generally have hardly any pain, are able to return to preinjury activity levels, and therefore are subjectively happy with their results.
The achievement rate of micro-discectomy is The following studies have been summarised to underline the success rate of micro-discectomy procedures:
1. In a survey on 342 professional athletes Diagnosed with lumbar disc herniation in sports like hockey, football, basketball and baseball, it was discovered that powerful return to perform occurred 82% of this time, and 81 percent of surgically treated athletes returned for an additional average of 3.3 years(5).
2. From a limb paresis which might be associated with a disc herniation following surgical treatment. If the preoperative paresis was mild then they could anticipate an 84% likelihood of full recovery. Patients with more severe paresis have less chance of recovery (55%)(6).
3. Wang et al (1999) in a study on 14 athletes demanding discectomy processes found that in single degree disc procedures, the return to game was 90%. However when the procedure involved 2 levels enjoyed considerably less favorable results(7).
4. In a study of 137 National Football League players with lumbar disc herniation, surgical treatment of lumbar disc herniation led to a significantly more career and greater return to play rate than those treated non-operatively(8).
5. Schroeder et al (2013) reported 85% RTP rates in 87 hockey players, with no substantial difference in outcomes or rates between the surgical and nonsurgical cohorts(9).
6. A study by Watkins et al (2003) coping with professional and Olympic athletes revealed the acceptable outcomes of micro-discectomy concerning return to play, since elite athletes in general were highly encouraged to return to perform(10). Also, athletes who had single-level micro- discectomy were more likely to come back to their original heights of sports activities than were people who’d two-level micro- discectomies.
7. A study by Anakwenze et al (2010) investigating open discectomy at National Basketball Association participants demonstrated that 75% of patients returned to perform again compared with 88 percent in control subjects who did not undergo the operation(11).
8. A recent review found that conservative therapy, or micro-discectomy, in athletes using lumbar disc herniation seemed to be satisfactory concerning returning the injured athletes into their initial levels of sports activities(12).
These studies conclude that though a Analysis of lumbar disc herniation has career-ending potential, most gamers have the ability to return to play and generate excellent performance-based outcomes, even if surgery is required.
What is also apparent from research Studies is the level of this disc herniation can also determine prognosis after surgery. Athletes shower a greater difference in progress between surgical and non-operative treatment for upper amount herniations (L2-L3 and L3-L4) compared to herniations at the L4-L5 and L5-S1 levels. Patients using the upper level herniations needed less progress with non-operative treatment and marginally better operative outcomes than those with lower degree herniations(13).
There are several possible explanations A range of studies have revealed that low spinal canal cross-sectional area is associated with an increased likelihood of symptomatic disc herniation, and increased intensity of herniation symptoms. The spinal cross-sectional region is the smallest (thus contains a larger possibility of nerve compromise) at the most upper posterior section and the cross-sectional region increases further down to the lower lumbar spine(14).
The location of the disc herniation�(foraminal, posterolateral or central) may also contribute to differences.�In this study, upper lumbar herniations were more likely to happen in the much lateral and foraminal positions than were people in the lower two intervertebral degrees(13).
Post-Surgical Rehab
After micro-discectomy surgery, the Small incision and restricted soft tissue injury makes it possible for the patient to be ambulatory reasonably fast, and they’re usually encouraged to start rehabilitation sooner or later during the 2-6 weeks after surgery.
In a review on the efficacy of busy Rehabilitation in patients following lumbar spine discectomy, it may be reasoned that individuals can safely take part in high or low-intensity supervised or home-based exercises initiated at 4 to 6 weeks following first-time lumbar discectomy(15).
Herbert et al (2010) discovered that with Effective post-surgical rehabilitation plans, there was a key accent on lumbar stabilisation exercises(16). Second, positive trials tended to initiate rehabilitation earlier in the postoperative interval compared to negative trials (about 4 vs 7 weeks).
Outcome Measures
The most widely used result Measure following back injury and/or disc surgery is the Oswestry Disability Questionnaire(17). This questionnaire is reported to have good levels of test-retest reliability, responsiveness, and also a minimum clinically important difference estimated as 6 percent(18) Furthermore, treatment success has been defined as a 50 percent decrease in the Modified Oswestry Disability Questionnaire score(19).
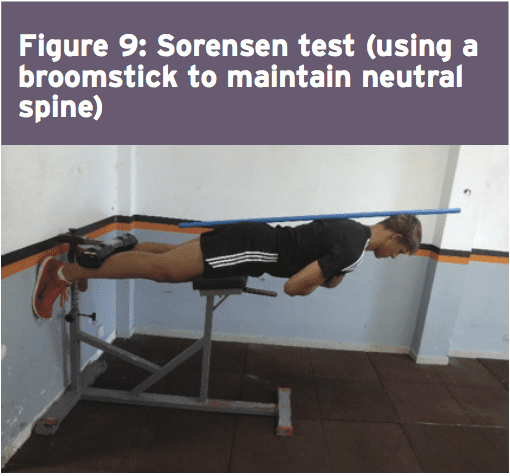
Concerning physical performance measures following back disc or pain operation, a commonly used clinical examination is that the Beiring-Sorensen Back Extension examination (see Figure 1)(20). This test is performed in a prone/horizontal body position with the spine and lower extremity joints at neutral position, arms crossed at the chest, lower extremities and pelvis supported with the top back unsupported against gravity.
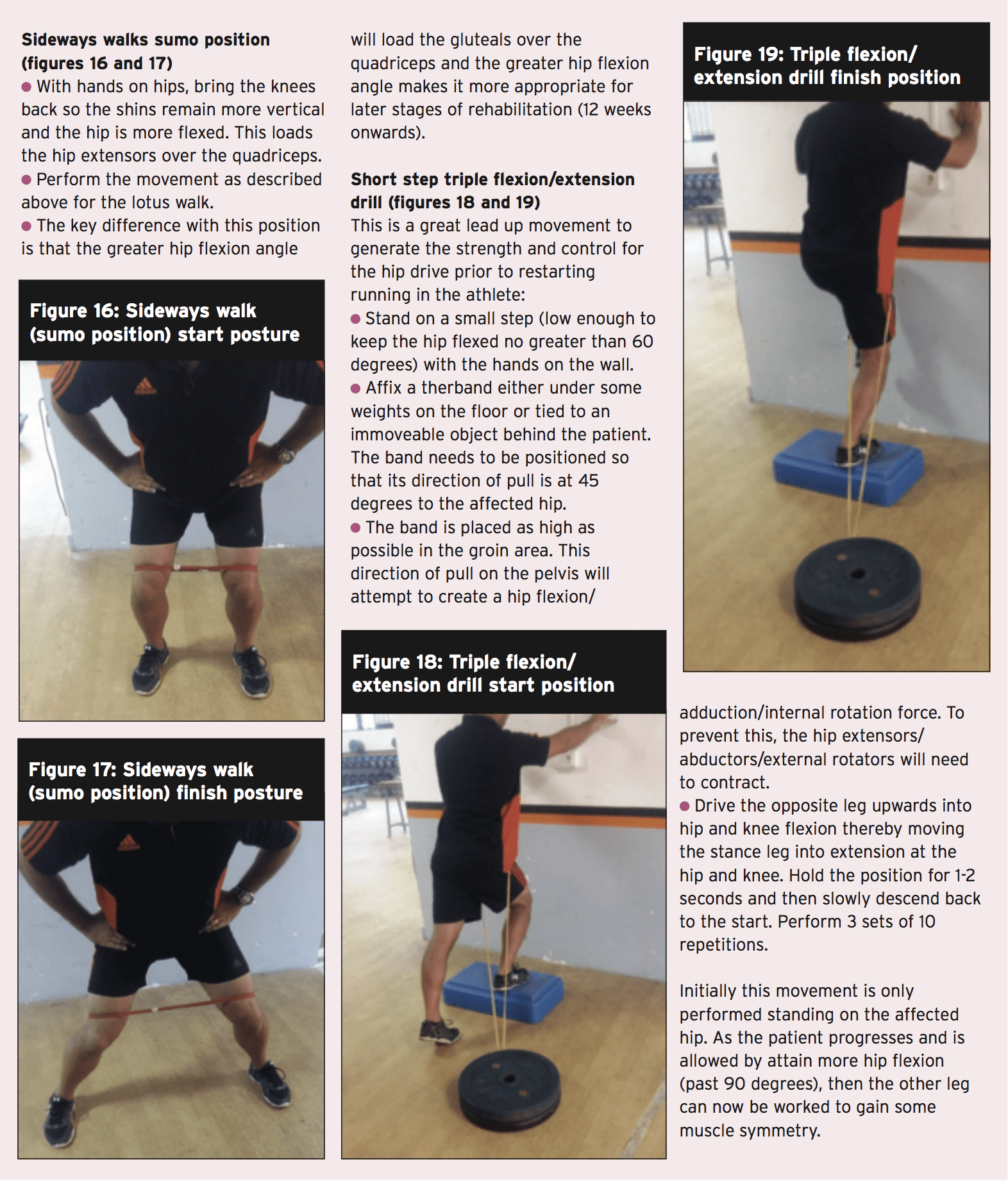
Rehabilitation Program
Presented below is a five-stage rehabilitation program. The stages involved in rehabilitation are:
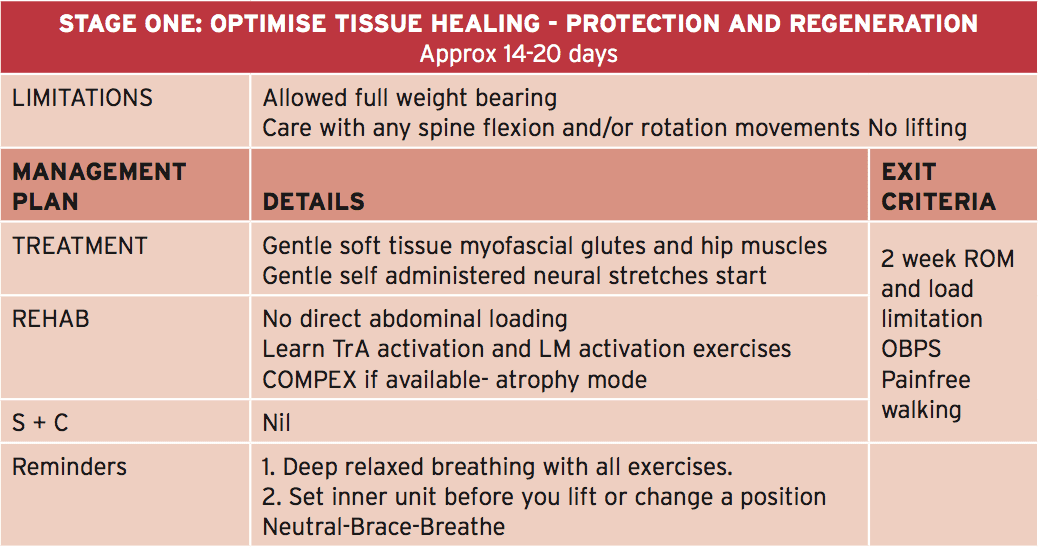
1. Optimize tissue healing — protection and regeneration
2. Early loading and foundation
3. Progressive loading
4. Load buildup
5. Maximum load
This program has been designed to get a field hockey player with had a L5/S1 lumbar spine discectomy. Even though the progressions from one point to the next are driven by the exit standards related to that stage, it might be anticipated that the athlete could progress in post-surgery to ‘fit to compete’ in about 12-13 weeks.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
The athlete can begin with the physiotherapist with the objective to manage any gluteal and lumbar muscle trigger points and start�nerve mobilization techniques that show how to engage the TrA and LM muscles (see Figures 2a and 2b).�If the physiotherapist has access to your muscle stimulator (Compex), then this can be utilized in atrophy manner on the lumbar spine multifidus and erector spinae. The key criteria to exit this early phase are curable walking as well as also an Oswestry Disability Score of 41-60%.
Early Loading & Foundation
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The athlete can also be encouraged to start hydrotherapy in the form of walking in water (waist high) along with swimming fitnesscenter. In addition, he/she must start a string of low degree muscle activation drills in this stage (see Figure 3) that can be performed every day. This exercise teaches the athlete to hip flex (fashionable hinge) whilst maintaining a neutral spine. The neutral spine is maintained by using a light broomstick aligned with the back with the touch points being the occiput, the 6th thoracic vertebrae (T6) and the posterior sacrum.
Progressive Loading
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�Two exercises here are the �standing twisties� and the �crook lying pelvic rotation� exercise (Figures 4 and 5).�These movements are the introductory spinning based movements. The primary progression about fitness drills is the athlete can begin pool running drills.
Load Accumulation
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
Maximum Load
In this final stage, the athlete spreads all core and strength exercises to maximum loads, and they work with the fitness trainer on coming to squat and functional fitness center lift movements. Skill progression can also be advanced alongside sprint and agility drills. The last exit standards prior to advancing to endless strength and training work is they have to keep the ‘Sorensen test’ for 180 seconds and their self documented Oswestry scale ought to be someplace between 0-20%.
Chiropractor, Dr. Alex Jimenez looks at lumbar spine disc herniation. What are the Likely signs and symptoms associated with disc herniation, and what would be the selection criteria for micro-discectomy operation in athletes? Complaint in the young college age athlete and professional athlete, and it’s been estimated that over 30% of athletes complain of back pain at least once in the profession(1).
Lumbar spinal disc herniation is one kind Of lumbar injury that can’t just cause painful low back pain, but can also compress nerve roots and create radicular referral of pain into the lower leg with related sensation changes and muscle contraction. This injury will not only influence the short-term opponent ability of the athlete, but might also reoccur and eventually become persistent possibly causing a career ending injury.
Managing disc herniation from the athlete Usually begins with conservative therapy and if this fails, surgical solutions are considered. But often elite athletes will request a quicker resolution to their symptoms to minimize time away from competitors. Therefore, providing the criteria for lumbar spine surgery are suggested, the conservative period will often be compressed, and surgery will be sought earlier. The favored surgical process for the athlete with a disc herniation is that the lumbar disc micro-discectomy.
Anatomy & Biomechanics
A significant biomechanical role in the spine, allowing for motion between the spinal segments while spreading compressive, shear, and torsional forces(2). These discs include a thick outer ring of fibrous cartilage termed the annulus fibrosis (akin to the onion rings enclosing the center of the onion), which encompasses a more gelatinous core called the nucleus pulposus, which is included within the cartilage end plates inferiorly and superiorly.
The intervertebral disc consists of Cells and substances such as collagen, proteoglycans, and thin fibrochondrocytic tissues, which enable transmission and absorption of forces arising from body weight and muscle activity. To do so, the disc depends mainly on the structural condition of the nucleus pulposus, annulus fibrosis and the vertebra lend plate. If the disc is normal and is functioning optimally, then forces are spread across the disc evenly(3).
But disc degeneration (mobile Degradation, lack of hydration( disc failure) may decrease the capacity of the disc to withstand extrinsic forces, as forces are no longer distributed and spread evenly. Tears and fissures from the annulus can lead, and with adequate external forces, the disc material may herniate. Alternatively, a sizable biomechanical force set on a healthy, ordinary disc may cause extrusion of disc material as a result of crushing failure of this annular fibers — illustrations include a hefty compression type mechanism because of a fall on the tailbone, or strong muscle contraction such as heavy weight lifting(4).
Herniations represent protrusions of Disc material beyond the confines of this annular lining and in the spinal canal (see Figure 1)(5). If the protrusion does not invade the canal or undermine nerve roots then back pain may be the only symptom.
Endoscopic Discectomy 3D Simulation
The pain associated with lumbar Radiculopathy happens due to a mix of nerve root ischemia (due to compression) and inflammation (because of neurochemical inflammatory mediators released from the disc). Throughout a herniation, the nucleus pulposus puts pressure on weakened regions of the annulus, and proceeds through the diminished websites in the annulus in which it ultimately forms a herniation(6 ft). It follows from this that some kind of disc degeneration may exist prior to the disc may really herniated(7).
In contrast to other respiratory Tissues, discs have a inclination to degenerate earlier in life, with some studies demonstrating adolescents presenting signs of degeneration between the ages of 11 to 16(8). With increasing age, there’s further degeneration of the intervertebral discs.
While the disc might be in danger of harm in All fundamental planes of motion, it’s particularly susceptible during repetitive flexion, or hyper-flexion, combined with lateral bending or rotation(10). Traumatic events such as excessive axial compression may also damage the inner structure of the disc. This can occur as a result of a fall or powerful muscular forces developed during tasks such as heavy lifting.
Athletes are generally exposed to high loading conditions. Examples of this include:
1. World-class power lifters, in which the calculated compressive loads on the backbone are involving 18800 Newtons (N) and also 36400N acting in the L3-4 motion segment(11).
2. Elite level football linesmen who have Been proven to present time-related hypertrophy of this disc and changes in vertebrae endplate in response to this repetitive high loading and axial pressure(12).
3. Long distance runners have been Shown to undergo significant strain into the intervertebral disc, indicated by a reduction in disc height(13).
Herniations could be classified depending on Ultimately, herniations are also identified based on level, with most herniations happening at the L4/5 and L5/S1 intervertebral disc level; these can then in turn affect the L5 and S1 nerve roots resulting in clinical sciatica(15). Upper level herniations are less common, and when they do occur with radiculopathy, they will affect the femoral nerve. Finally, the prevalence of disc injury rises increasingly caudally, with the best numbers at the L5/S1 degrees(16).
Herniation In Athletes
The offending movements implicated in The 20-35 age group are the most common group to herniate a disc, most likely because of the fluid nature of the nucleus pulposis and due to behavior(18). This age group are more likely to participate in sports which need high lots of flexion and spinning or are reckless with their positions and positions during loading.
The sports most at risk of disc herniation are:
Hockey
Wrestling
Soccer
Swimming
Basketball
Golf
Tennis
Weightlifting
Rowing
Throwing events
These are the sports that involve either significant Furthermore, those who take part in more and more severe training regimes seem to be at higher risk of spinal pathologies, as do people involved in sports.
Signs & Symptoms Indicating Discectomy
The efficacy of management programs for lumbar spine disc herniation — in terms of the decision to operate or treat conservatively — will be discussed in greater depth in part 2 of this series. However, the decision to operate within an athlete is generally driven by the motivation and approaching goals the athlete has put themselves. They may in fact favor a comparatively simple micro-discectomy instead of waiting for symptoms to abate through an extended period of rehabilitation.
This conservative period of Management may involve medicine therapy, epidural injections, relative back and back muscle recovery, acupuncture, osteo/chiropractic interventions. On the other hand, the normal presenting symptoms and signs that suggest a substantial disc herniation that will require surgical intervention in the athlete comprise:
Low back pain with pain radiating down one or both legs
Positive straight leg raise test
Radicular pain and neurological signs consistent with the nerve root level affected
Mild weakness of distal muscles such as extensor hallucis longus, peroneals, tibialis anterior and soleus. These would fit with the myotome relevant for the disc level
MRI confirming a disc herniation
Possible bladder and bowel symptoms
Failed conservative rehabilitation
Time span in which to enable conservative rehabilitation to be effective. In the overall population, medical practitioners will most likely prescribe a minimal 6-week traditional period of treatment with an overview at 6 weeks as to whether to expand the rehabilitation a further 6 weeks or to seek a specialist opinion. The expert may then attempt more medically orientated interventions such as epidural injections.
The athlete nevertheless will have these They might be more inclined to experience an epidural very early in the conservative period to assess the effectiveness of this procedure. If no signs of progress are evident in a couple of weeks then they may choose to get an immediate lumbar spine micro- discectomy.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques. From the El Paso, TX. Spine Center.
Imaging
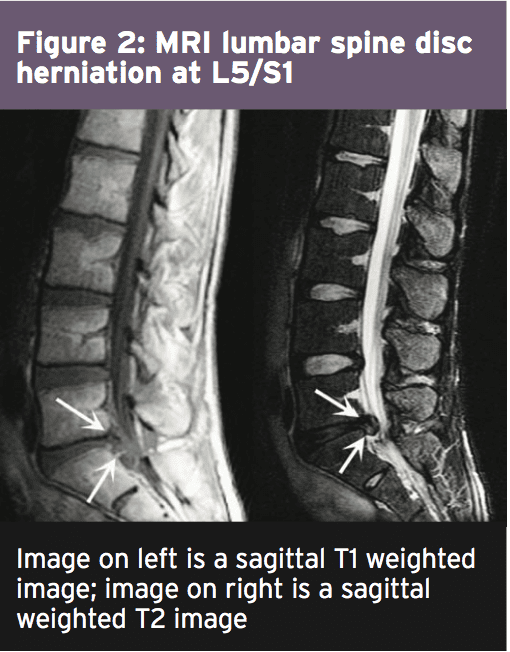
MRI remains the favored system of Identifying lumbar spine disc herniation, since it’s also very sensitive to detecting nerve root impingements(23). However, abnormal MRI scans can occur in otherwise asymptomatic patients(25); hence, clinical correlation is always essential before any surgical thought. What’s more, patients can present with clinical signs and symptoms which suggest the diagnosis of acute herniated disc, and yet lack evidence of sufficient pathology on MRI to warrant operation.
Therefore it has been proposed that a Volumetric analysis of a herniated disc on MRI may be potentially beneficial in checking the suitability for operation. Several writers have previously mentioned the possible value of volumetric evaluation of herniated disc on MRI as part of their selection criteria for lumbar surgery(26).
In a survey conducted in Michigan State University, it was found that the size and positioning of the herniated disc determined that the likelihood for operation with what researchers called ‘types 2-B’ and ‘types 2-AB’ being the most likely candidates for surgery(27).
The MRI protocol to your lumbar spine consists of (see Figure 2)
1.Sagittal plane echo T1- weighted sequence
2. Sagittal fast spin echo proton density sequence
3. Sagittal fast spin echo inversion recovery sequence
4.Axial spin echo T1- weighted sequence
Summary
Disc herniations are not a common Complaint in athletes, but they do happen in sports which involve high loads or repetitive flexion and rotation movements. Sufferers of a disc herniation will normally feel focused low-back pain, maybe with referral in the lower limb with associated neurological symptoms if the nerve root was compressed.
Managing a disc herniation within an General population as frequently the risk of a Protracted failed rehabilitation period is Bypassed for the protected and low risk Micro-discectomy procedure. In the Discuss the exact surgical alternatives involved Observing a lumbar spine micro-discectomy.
References
1. Sports Med. 1996;21(4):313�20
2. Radiology. Oct 2007;245(1):62-77
3. Arthritis Research & Therapy. 2003;5(3):120-30
4. The Journal of Bone and Joint Surgery. American volume. Feb 2004;86-A(2):382 � 96
5. Radiology. Oct 2007;245(1):43-61
6. Spine. Sep 15 1996;21(18):2149-55
7. Spine. May-Jun 1982;7(3):184-91
8. Spine. Dec 1 2002;27(23):2631-44
9. Lancet 1986;2:1366�7
10. Disease-A-Month:DM. Dec 2004;50(12):636-69
11. Spine. Mar 1987;12(2):146-9
12. The American Journal of Sports Medicine. Sep 2004;32(6):1434-9
13. The Journal of International Medical Research. 2011;39(2):569-79
14. Spine. 2001;26:E93-113
15. Spine. 1990;15:679-82
16. British Journal of Sports Medicine. Jun 2003;37(3):263-6
17. Prim Care. 2005;32(1):201�29
18. McGill, S.M. Low back disorders: Evidence based prevention and rehabilitation, Human Kinetics Publishers, Champaign, IL, U.S.A., 2002. Second Edition, 2007
19. Spine. Apr 1991;16(4):437-43
20. Skeletal radiology. Jul 2006;35(7):503-9
21. British Journal of Sports Medicine. Nov 2007;41(11):836-41
22. The American Journal of Sports Medicine. Jun 2009;37(6):1208-13
23. Spine. Mar 15 1995;20(6):699-709
24. Phys Sportsmed. 2005;33(4):21�7
25. J Bone Joint Surg Am 1990 . 2:403�408
26. J Orthop Surg (Hong Kong) 2001. 9:1�7
27. Eur Spine J (2010) 19:1087�1093
Chiropractor, Dr. Alexander Jimenez examines the role of biomechanics in medial tibial stress syndrome…
Medial tibial stress syndrome (MTSS � commonly known as shin splints) is not medically serious, yet can suddenly side- line an otherwise healthy athlete. Roughly five percent of all athletic injuries are diagnosed as MTSS(1).
The incidence increases in specific populations, accounting for 13-20% of injuries in runners and up to 35% in military recruits(1,2). MTSS is defined as pain along the posterior-medial border of the lower half of the tibia, which is present during exercise and (usually) diminishes during rest. Athletes identify the lower front half of the leg or shin as the location of discomfort. Palpation along the medial tibia usually reproduces the pain.
Causes Of MTSS
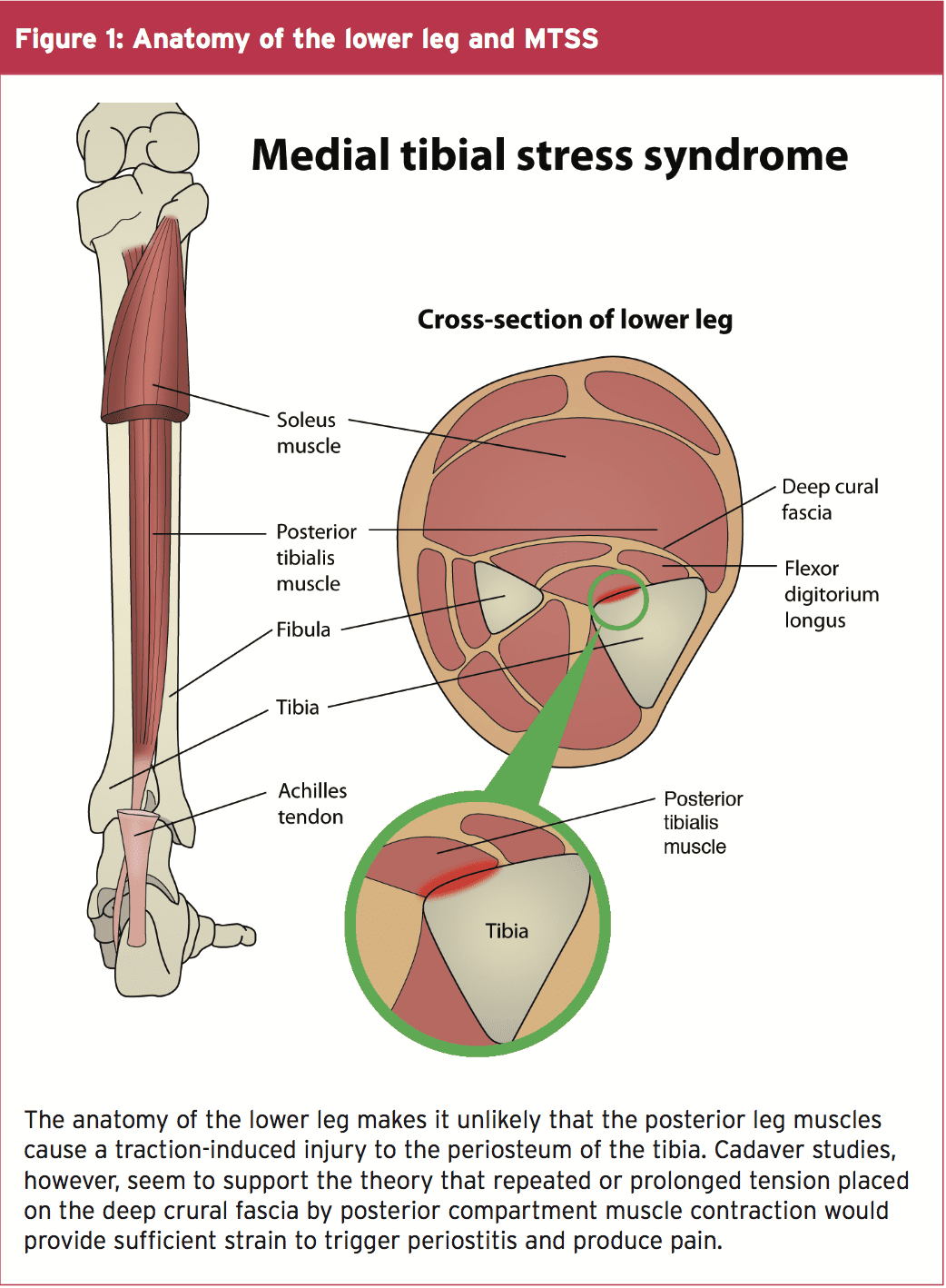
There are two main hypothesized causes for MTSS. The first is that contracting leg�muscles place a repeated strain upon the medial portion of the tibia, inducing periostitis � inflammation of the periosteal outer layer of bone. While the pain of a shin splint is felt along the anterior leg, the muscles that arise from this area are the posterior calf muscles (see figure 1). The tibialis posterior, flexor digitorum longus, and the soleus all arise from the posterior- medial aspect of the proximal half of the tibia. Therefore, the traction force from these muscles on the tibia is unlikely to be the cause of the pain typically felt on the distal portion of the leg.
A variation of this tension theory is that the deep crural fascia (DCF) � the though- connective tissue that surrounds the deep posterior compartment muscles of the leg � pulls excessively on the tibia, again causing trauma to the bone. Researchers at�the University of Honolulu examined a single leg from five male and 11 female adult cadavers. They confirmed that in these specimens, the muscles of the posterior compartment originated above the portion of the leg that is typically painful in MTSS, and the DCF indeed attached along the entire length of the medial tibia(3).
Doctors at the Swedish Medical Centre in Seattle, Washington wondered if, given the anatomy, could the tension from the posterior calf muscles produce a related strain on the tibia at the insertion of the DCF, and thus be the mechanism of injury(4)?
In a descriptive laboratory pilot study of three fresh cadaver specimens, they found that strain at the insertion site of the DCF along the medial tibia progressed linearly as tension increased in the posterior leg muscles. This confirmed that a mechanism for a tension-induced injury at the medial tibia is plausible. However, studies of bone periosteum in MTSS patients have yet to find inflammatory markers consistently enough to confirm the periostitis theory(5).
Tibial Bowing
The second causation theory for MTSS is that repetitive or excessive loading causes a bone-stress reaction in the tibia. The tibia, unable to adequately bear the load, bends during weight bearing. The overload results in micro damage within the bone, and not just along the outer layer. When the repetitive loading outpaces the bone�s ability to repair, localized osteopenia can result. Thus, some consider a tibial stress fracture to be the result of a continuum of bone stress reactions that include MTSS(1).
Magnetic resonance imaging (MRI) of the symptomatic leg often shows bone�marrow edema, periosteal lifting, and areas of increased bony resorption in patients with MTSS(1,5). This supports the bone- stress reaction theory. Magnetic resonance imaging of an athlete with a clinical presentation of MTSS can also help rule out other causes of lower leg pain such as tibial stress fracture, deep posterior compartment syndrome, and popliteal artery entrapment syndrome.
Risk Factors For MTSS
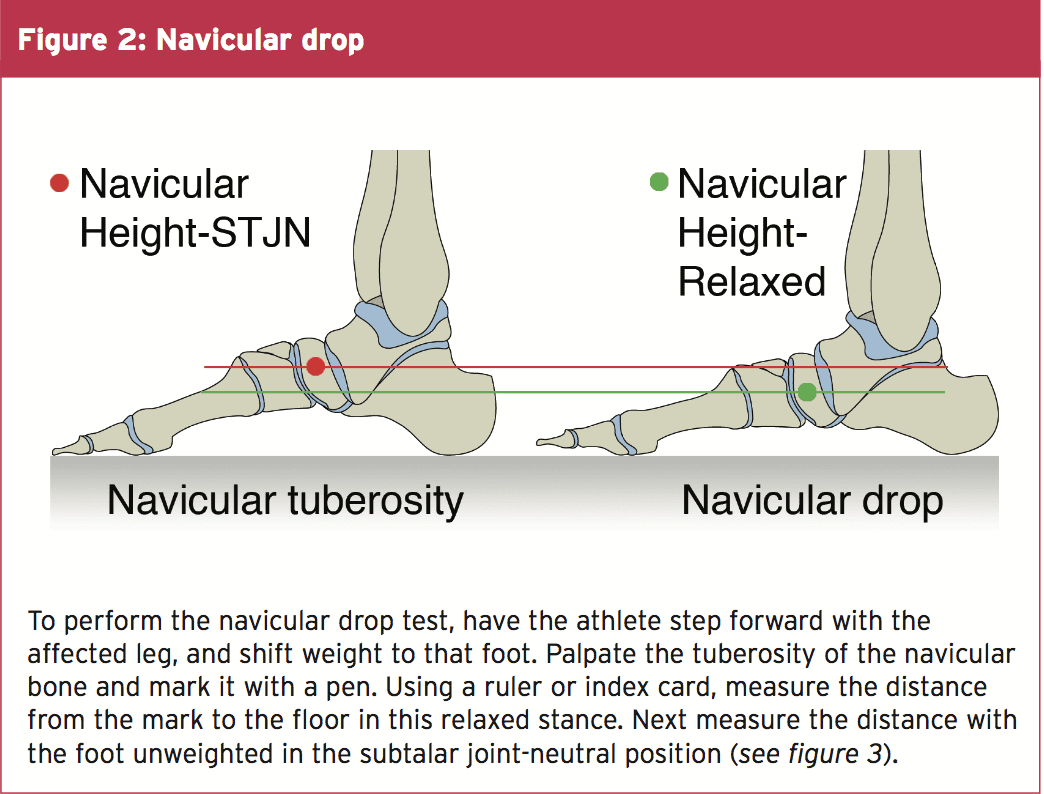
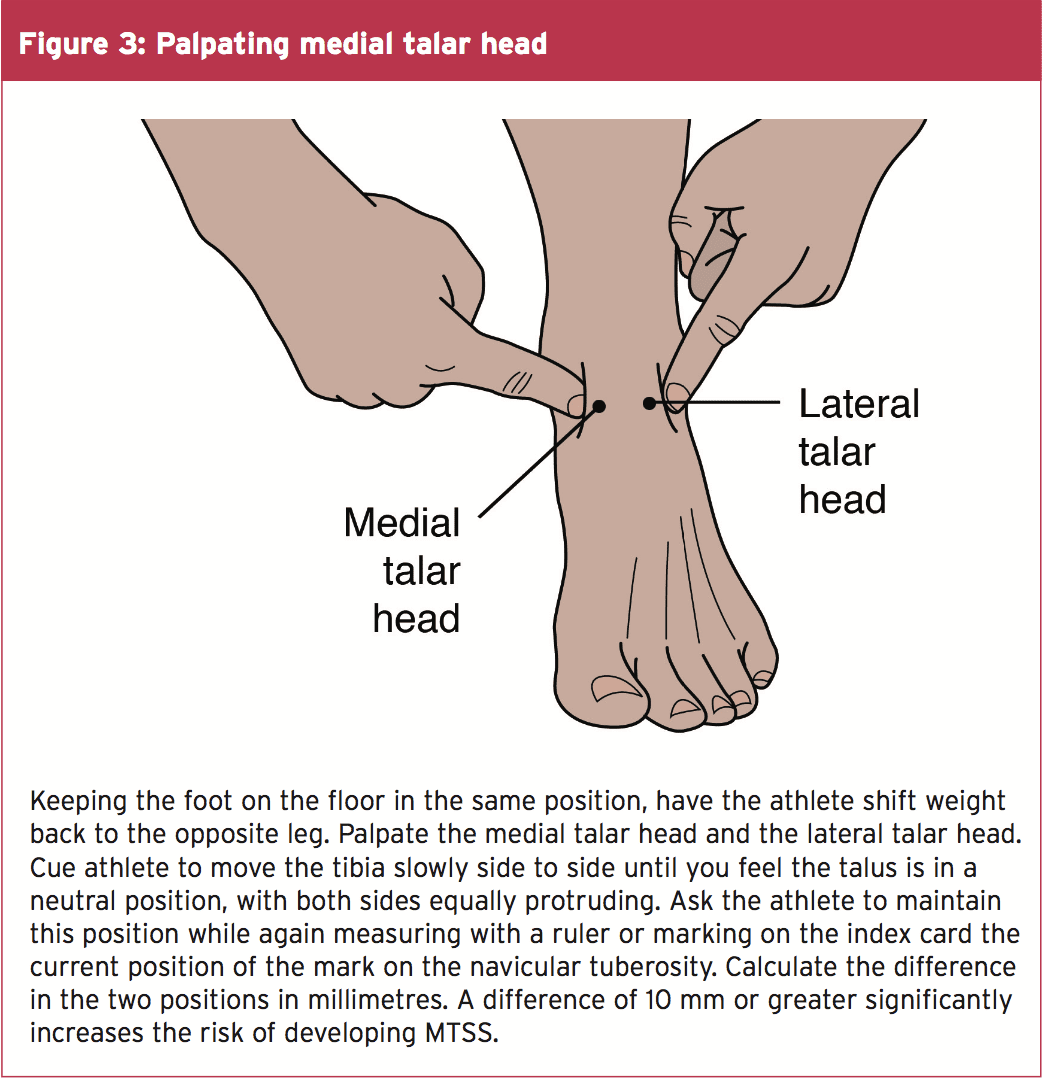
While the aetiology of MTSS is still theoretical, the risk factors for athletes developing it are well determined. A large navicular drop, as determined by the navicular drop test (NDT), significantly correlates with a diagnosis of MTSS(2,5). The NDT measures the difference in height position of the navicular bone, from a neutral subtalar joint position in supported non-weight bearing, to full weight bearing (see figures 2 and 3). The NDT is an indication of the degree of arch collapse during weight bearing. An excursion of more than 10 mm is considered excessive and a significant risk factor for the development of MTSS(5).
Research suggests that athletes with MTSS are found more likely to be female, have a higher BMI, less running experience, and a previous history of MTSS(2,5). Running kinematics for females can differ from males and fit a pattern that is known to leave them vulnerable to anterior cruciate ligament tears and patellofemoral pain syndrome(5). This same biomechanical pattern may also predispose females to MTSS. Hormonal considerations and low bone density are possibly contributing factors in increasing the risk of MTSS in the female athlete as well.
A higher BMI in an athlete likely indicates they have more muscle mass rather than they are overweight. The end result, however, is the same in that the legs bear a significantly heavy load. It is thought that in these instances, the bone growth�stimulated by the tibial bowing may not progress rapidly enough, and injury to the bone occurs. Therefore, those with a higher BMI may need to progress their training programs more slowly, to allow for adaptation.
Those with less running experience are more likely to make training errors (often identified by the athlete) as the catalyst for MTSS. These include increasing distance�too rapidly, changing terrain, overtraining, poor equipment (shoes), etc. Inexperience may also lead the athlete to return to activity too soon, thus accounting for the higher prevalence of MTSS in those who had suffered MTSS previously. Full recovery from MTSS can take anywhere from six to ten months, and if the cause of injury was not rectified or the athlete returns to training too soon, the chances are good the pain will return(5).
Biomechanical Considerations
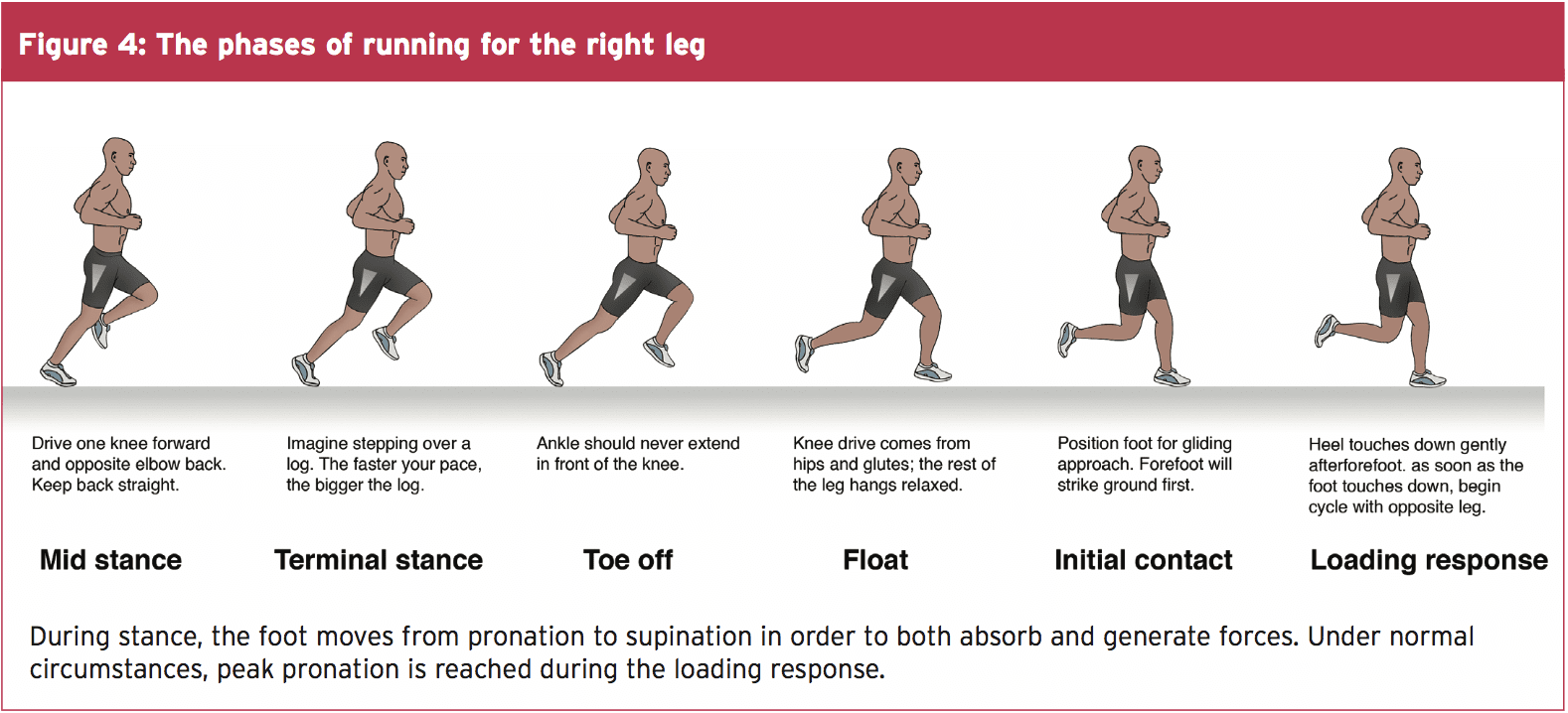
The NDT is used as a measurable indication of foot pronation. Pronation is a tri-planar movement comprised of eversion at the hind foot, abduction of the forefoot, and dorsiflexion of the ankle. Pronation is a normal movement, and essential in walking and running. When the foot strikes the ground at the initial contact phase of running, the foot begins to pronate and the joints of the foot assume a loose-packed position. This flexibility helps the foot absorb ground reaction forces (see figure 4).
During the loading response phase, the foot further pronates, reaching peak pronation by around 40% of stance phase(6). In mid stance, the foot moves out of pronation and back to a neutral position. During terminal stance, the foot supinates, moving the joints into a closed packed position and creating a rigid lever arm from which to generate the forces for toe off.
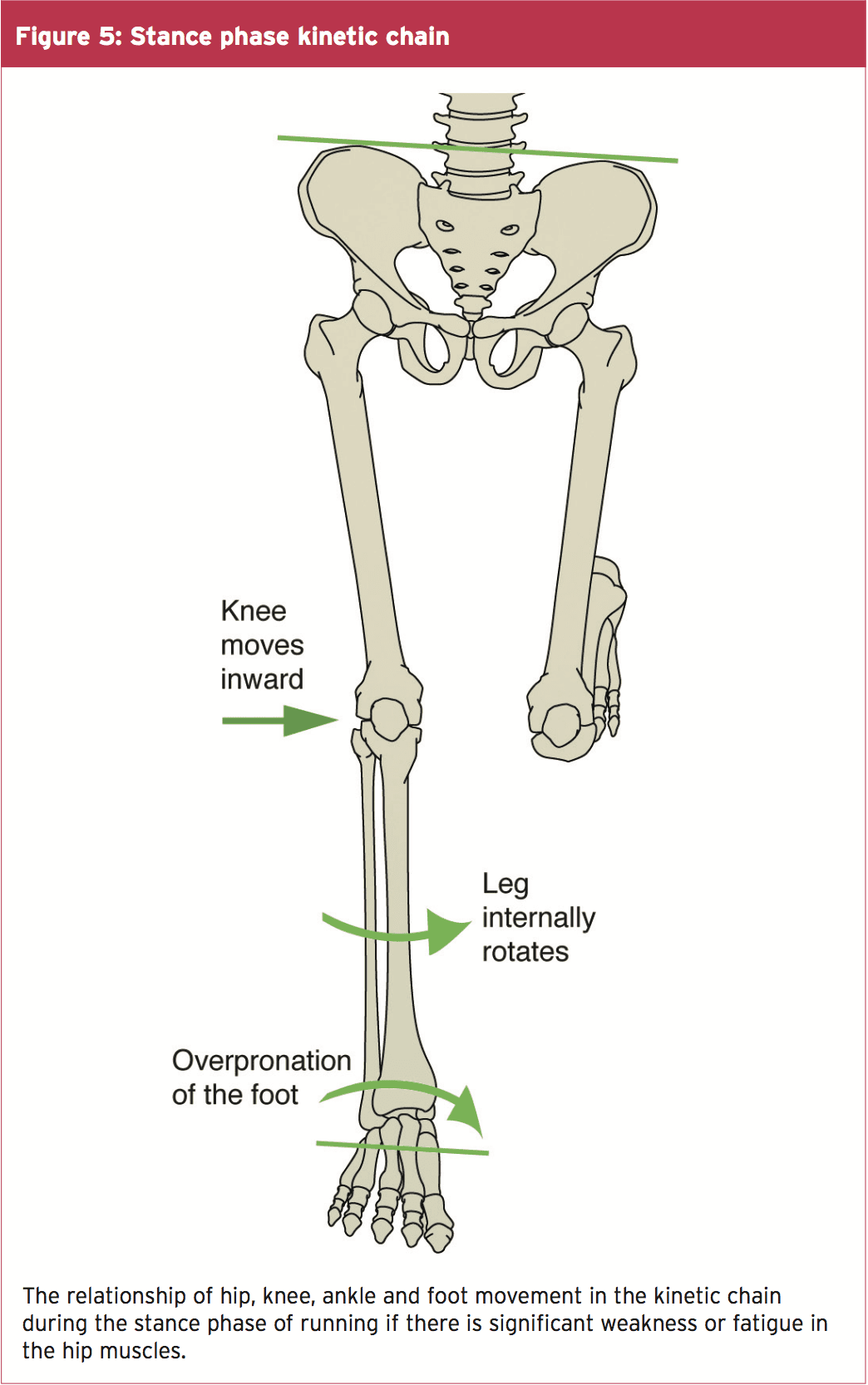
Beginning with the loading response phase and throughout the remainder of the single leg stance phase of running, the hip is stabilized, extended, abducted and externally rotated by the concentric contraction of the hip muscles of the stance�leg (the gluteals, piriformis, obturator internus, superior gemellus and inferior gemellus). Weakness or fatigue in any of these muscles can result in internal rotation of the femur, adduction of the knee, internal rotation of the tibia, and over-pronation (see figure 5). Overpronation therefore, can be a result of muscle weakness or fatigue. If this is the case, the athlete may have a quite normal NDT, and yet when the hip muscles don�t function as needed, can overpronate.
In a runner who has significant over pronation, the foot may continue to pronate into mid stance, resulting in a�delayed supination response, and thus less power generation at toe off. The athlete may attempt two biomechanical fixes here that could contribute to the development of MTSS. Firstly, the tibialis posterior will strain to prevent the over pronation. This can add tension to the DCF and strain the medial tibia. Secondly, the gastroc-soleus complex will contract more forcefully at toe off to improve the power generation. Again, the increased force within these muscle groups can theoretically add tension to the medial tibia through the DCF and possibly irritate the periosteum.
Evaluating The Injured Athlete
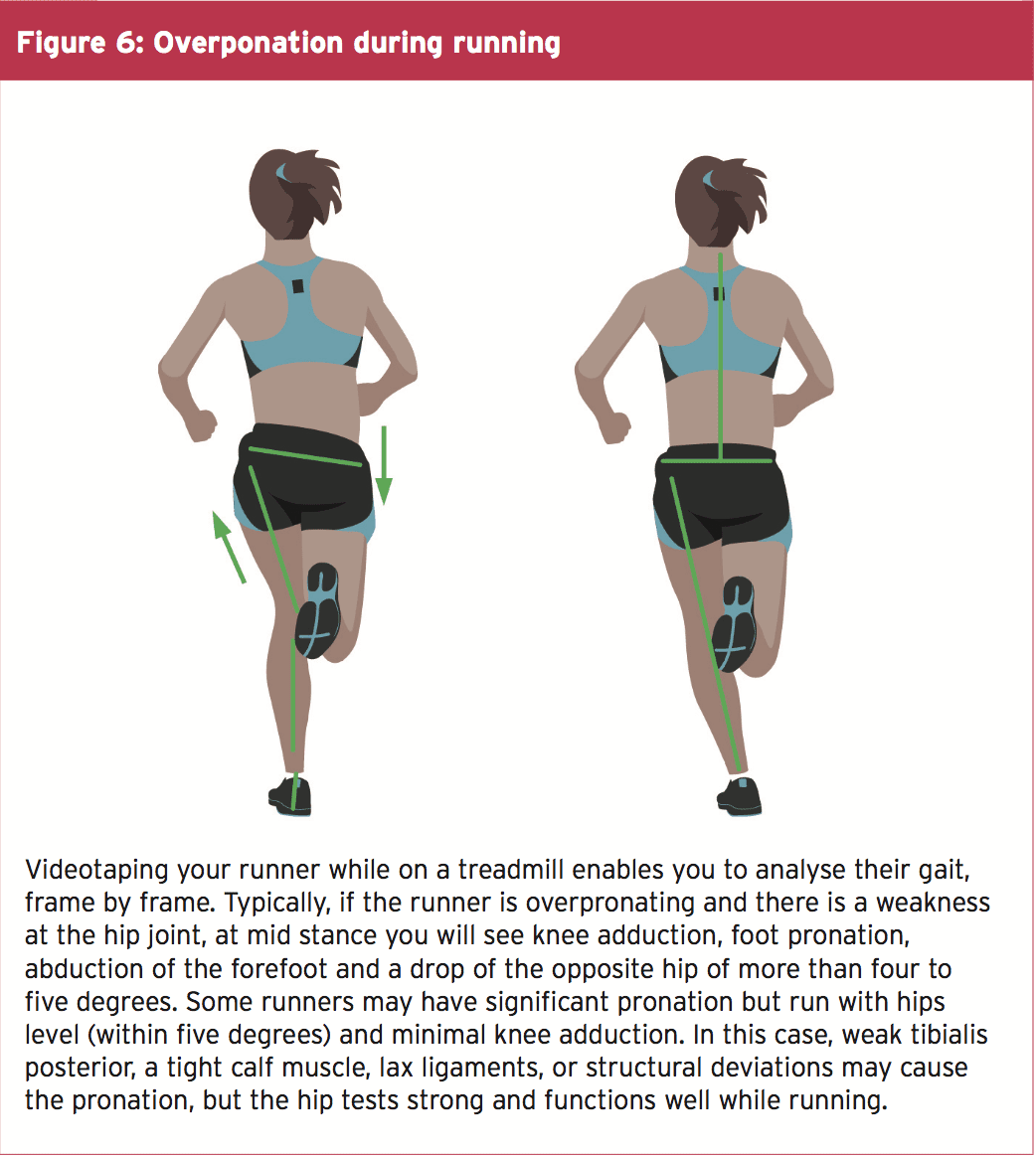
Knowing that over pronation is one of the leading risk factors for MTSS, start your evaluation at the ground and work your way up. First, perform the NDT, noting if the difference is more than 10mm. Analyze the athlete�s running gait on a treadmill, preferably when the muscles are fatigued, as at the end of a training run. Even with a normal NDT, you may see evidence of over pronation in running (see figure 6).
Next evaluate the knee. Is it adducted? Notice if the hip is level or if either hip is more than 5 degrees from level. These are indications that there is likely weakness at the hip. Traditional muscle testing may not reveal the weakness; therefore, functional muscle testing is required.
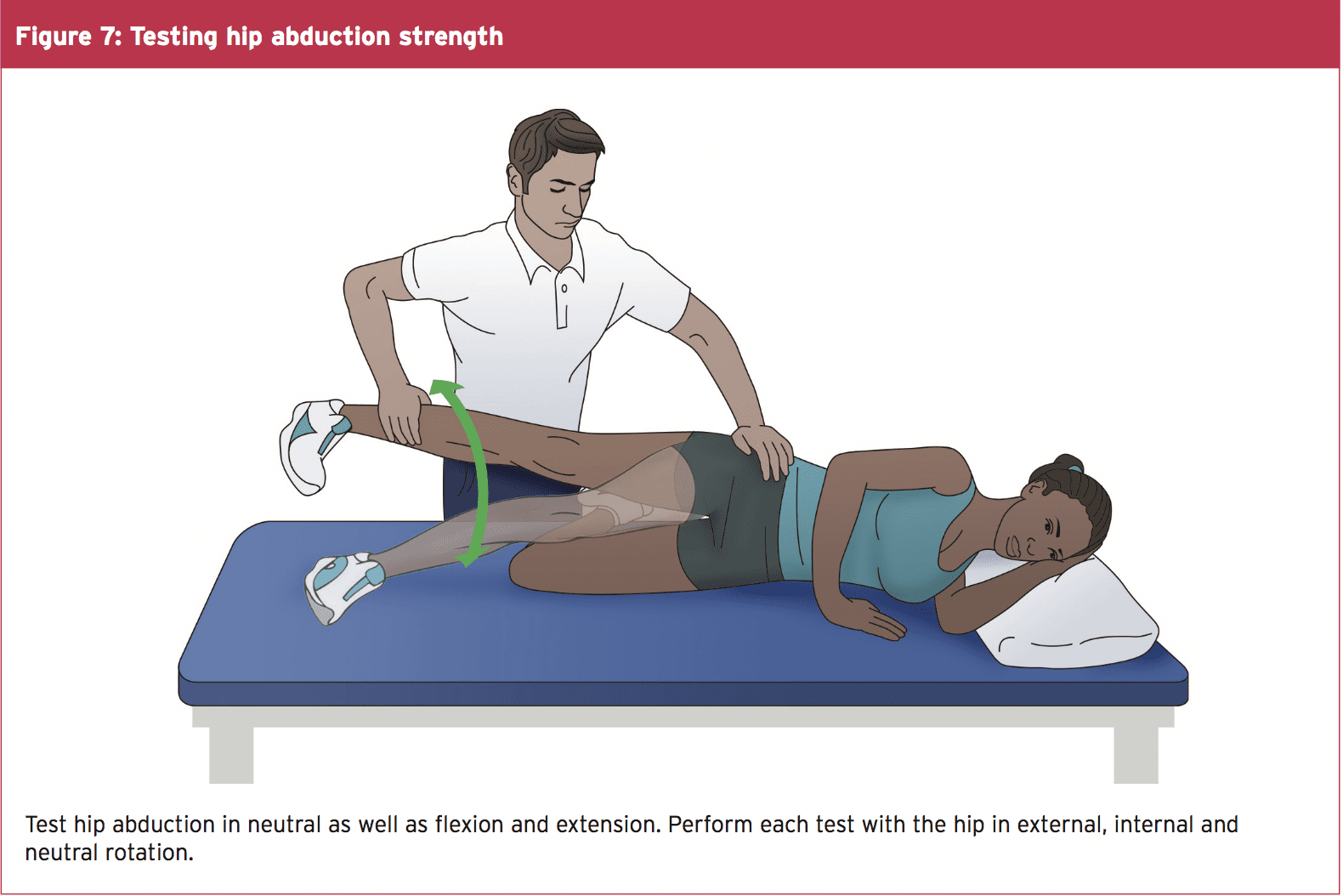
Observe the athlete perform a one-legged squat with arms in and arms overhead. Does the hip drop, the knee adduct and the foot pronate? Test the strength of hip abductors in side lying, with hip in neutral, extended, and flexed, keeping the knee straight (see figure 7). Test all three positions with hip rotated in neutral, and at end ranges of external and internal rotation. Test hip extension in prone with the knee straight and bent, in all three positions of hip rotation: external, neutral and internal. The position where you find the weakness is where you should begin strengthening activities.
Treat The kinetic Chain
If there is weakness in the hip, begin by having the athlete perform isometric exercises in the position of weakness. For instance, if you find weakness in hip abduction with extension, then begin isolated isometrics in this position. Not until the muscles consistently fire isometrically in this position for three to five sets of 10 to 20 seconds should you add movement. Once the athlete achieves this level, begin concentric contractions, in that same position, against gravity. Some examples are unilateral bridging and side lying abduction. Eccentric contractions should follow, and then sport specific drills.
Keep in mind if there are other biomechanical compensations, they must also be addressed. If the tibialis posterior is also weak, begin strengthening there. If the calf muscles are tight, initiate a stretching program. Utilise whatever modalities might be helpful. Lastly, consider a stabilising shoe if the ligaments in the foot are over stretched. Using a stabilising shoe for a short time during rehabilitation can�be helpful in cuing the athlete to adopt new movement patterns.
Conclusion
The best way to prevent shin pain from MTSS is to decrease the athlete�s risk factors. Ideally, each athlete should have a basic running gait analysis and proper shoe fitting. Include hip strengthening in functional positions such as unilateral stance as part of the strengthening program. Pair inexperienced athletes with a more experienced mentor to ensure proper training, use of equipment, and investigation of pain at onset. They may be more likely to tell a teammate they are feeling pain than a coach or trainer. Progress the running schedule of heavier athletes more slowly to allow adaptation of the bone. Ensure that athletes fully rehabilitate before returning to play because the chances of recurrence of MTSS are high.
References
1. Am J Sports Med. 2015 Jun;43(6):1538-47
2. Br J Sports Med. 2015 Mar;49(6):362-9
3. Med Sci Sports Exerc. 2009;41(11):1991-1996
4. J Am Podiatr Med Assoc. 2007 Jan;97(1):31-6
5. J Sports Med. 2013;4:229-41
6. Gait and Posture. 1998;7:77�95
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading.
So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading.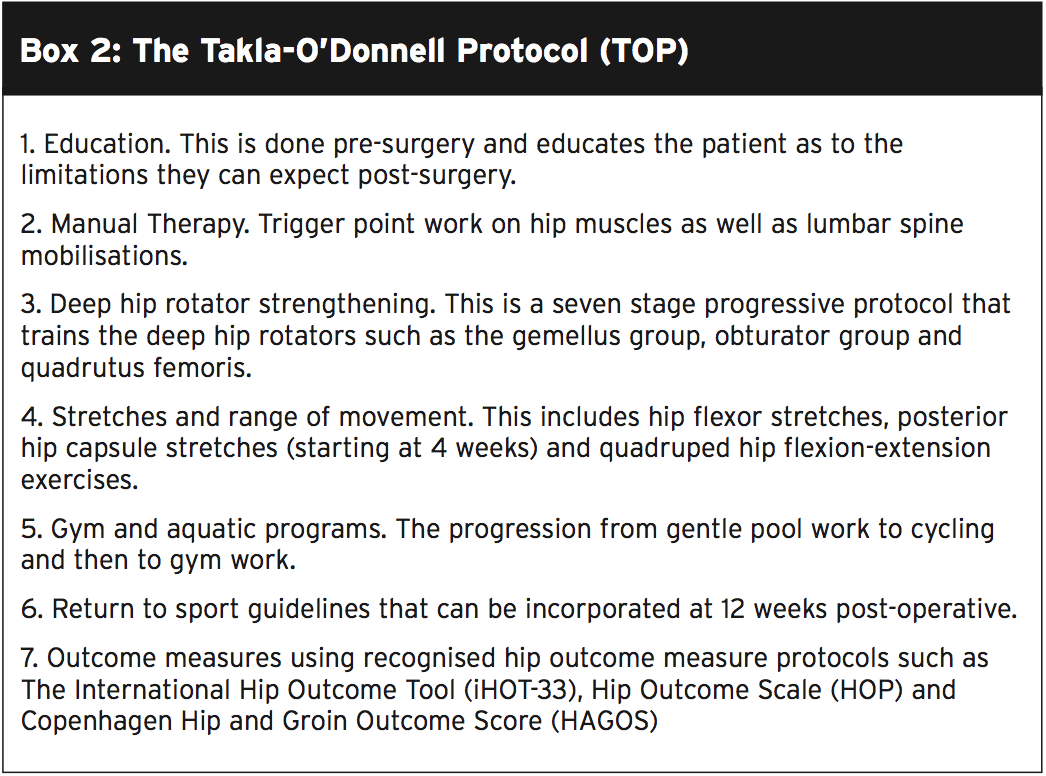 Hip Muscle Control
Hip Muscle Control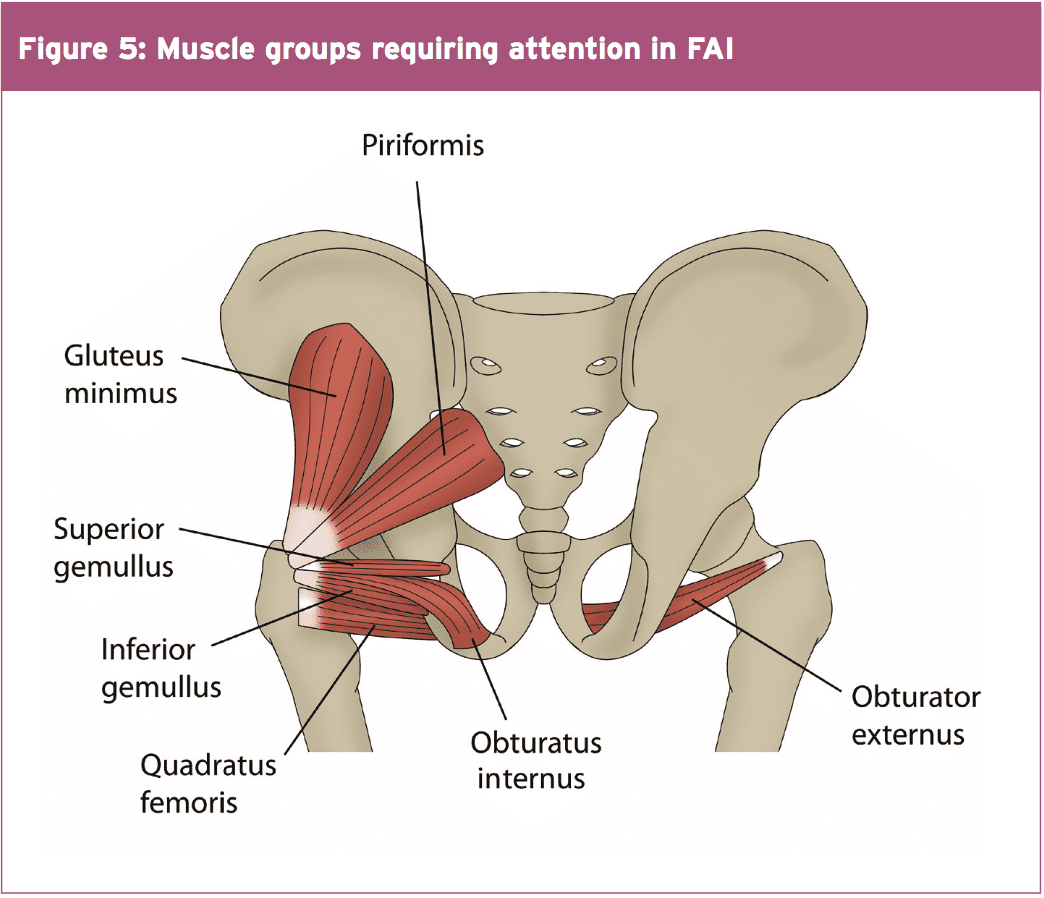
 Summary
Summary


 In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.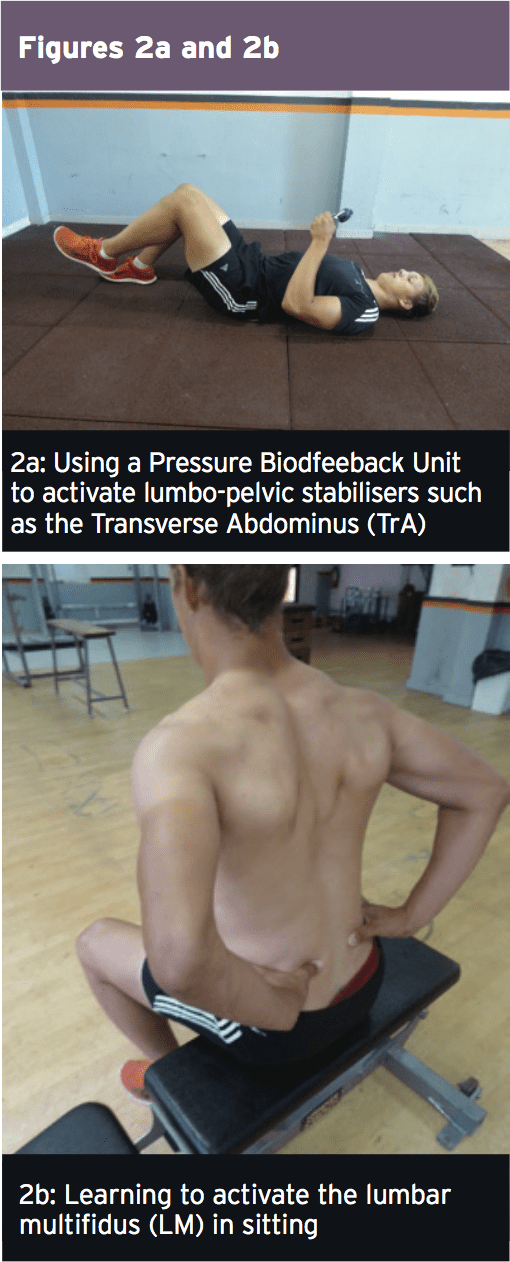 Early Loading & Foundation
Early Loading & Foundation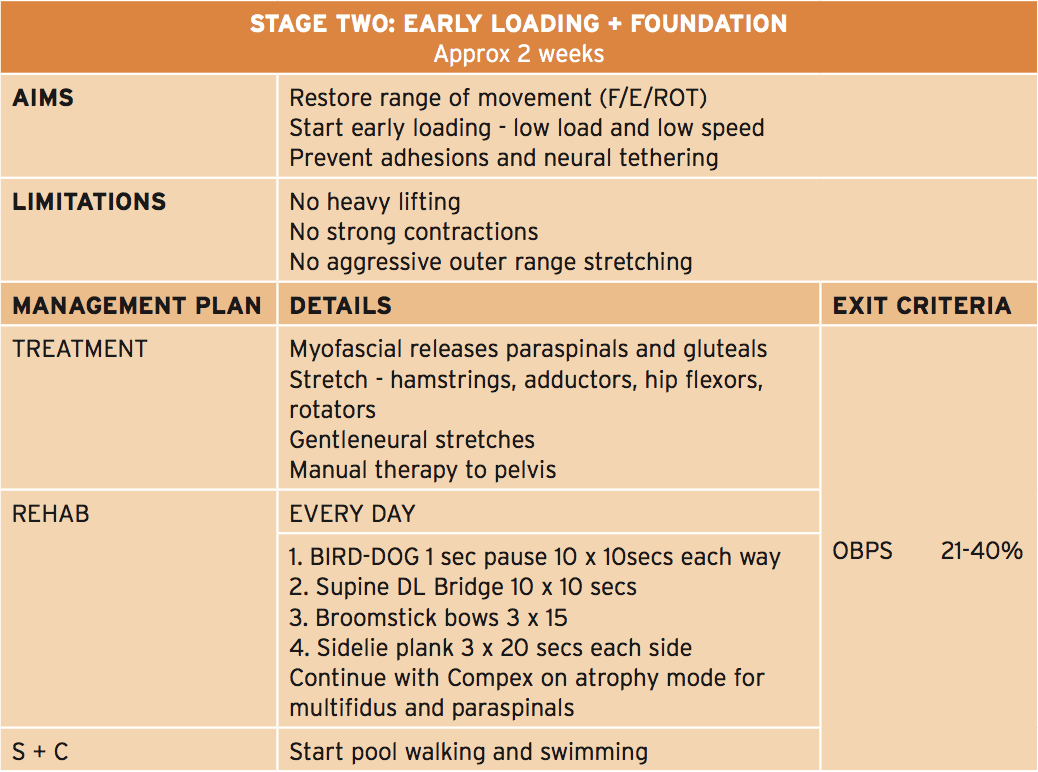 The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.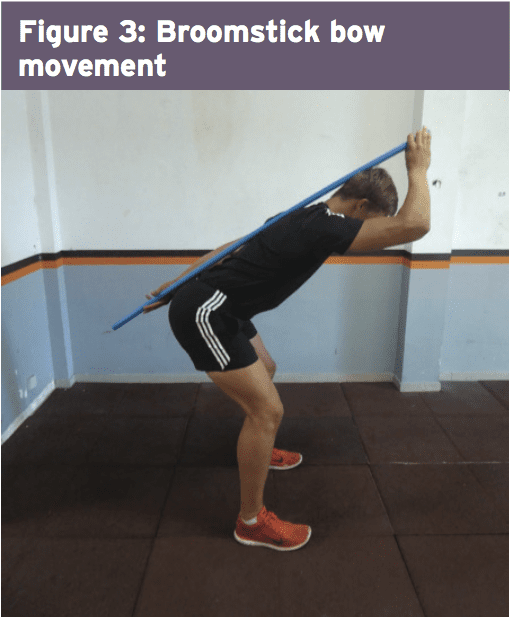 Progressive Loading
Progressive Loading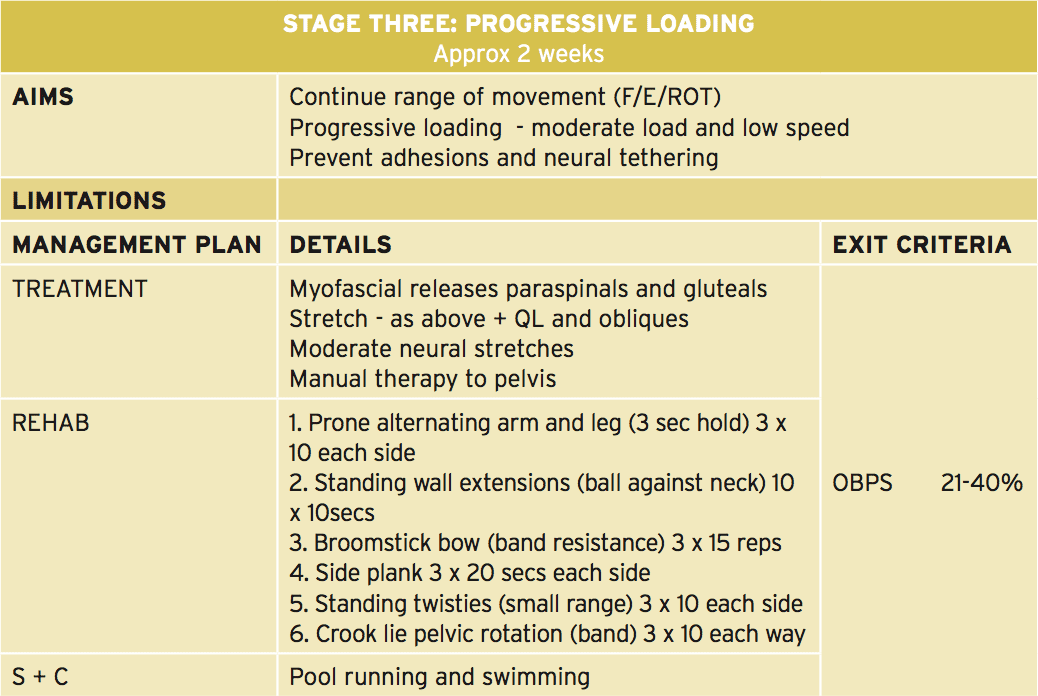 In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�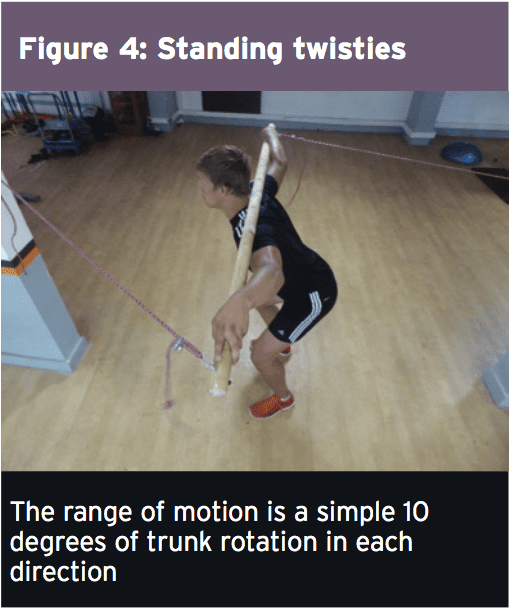
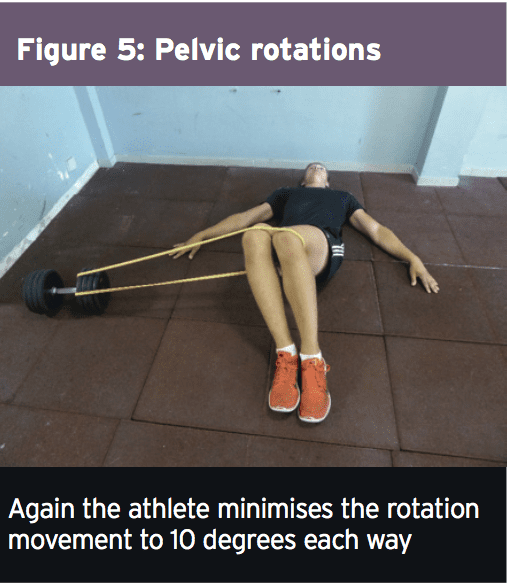 Load Accumulation
Load Accumulation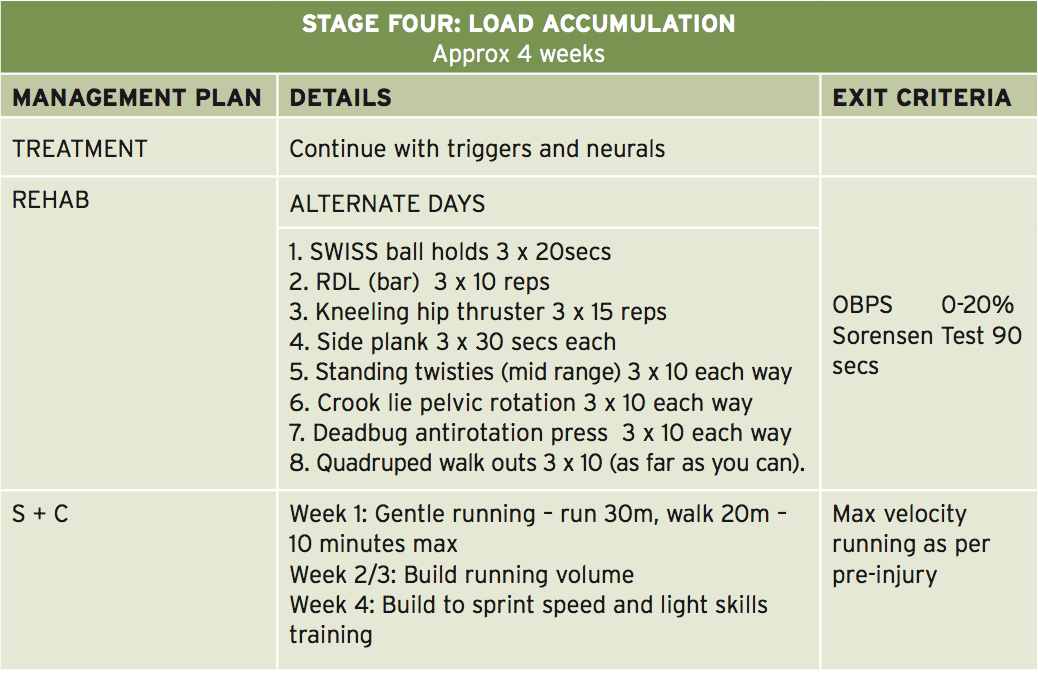 This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).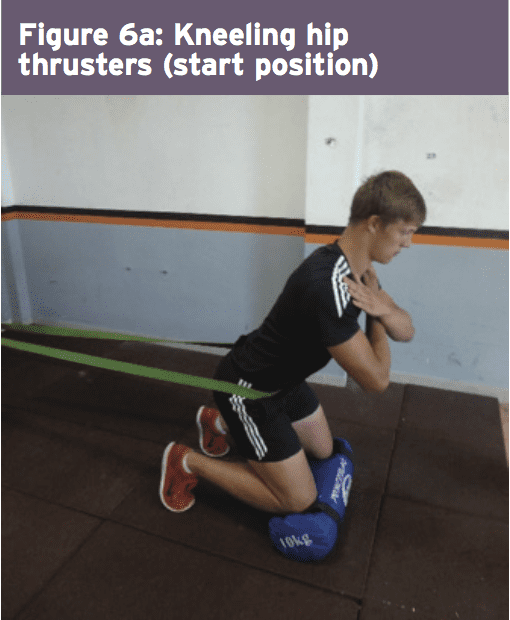
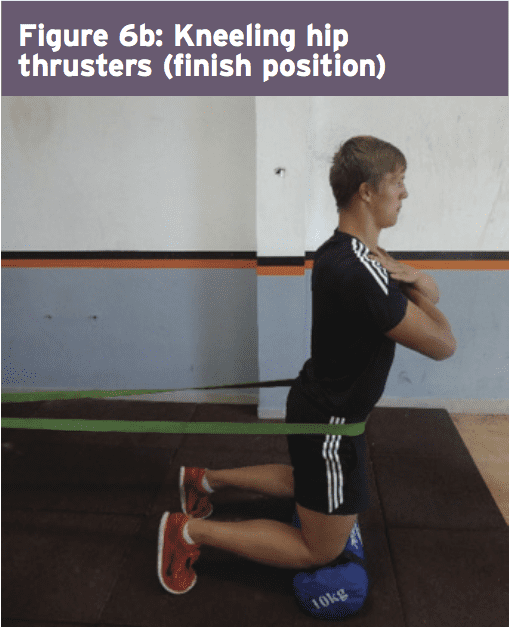
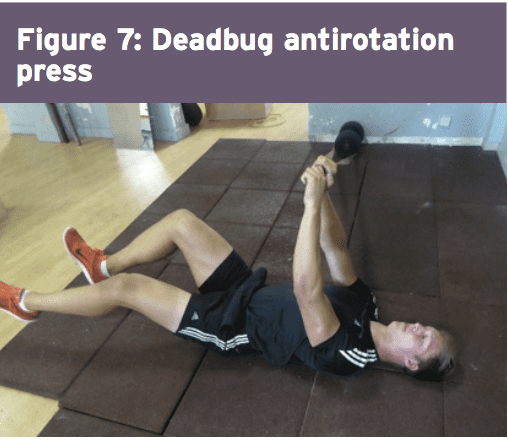
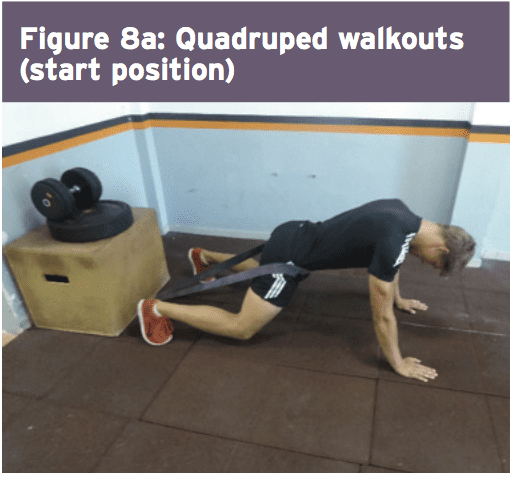
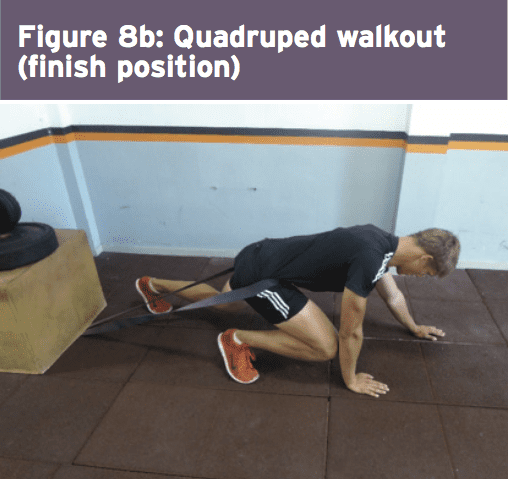 The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.