Diagnosis of Central Nervous System Infections Part 1
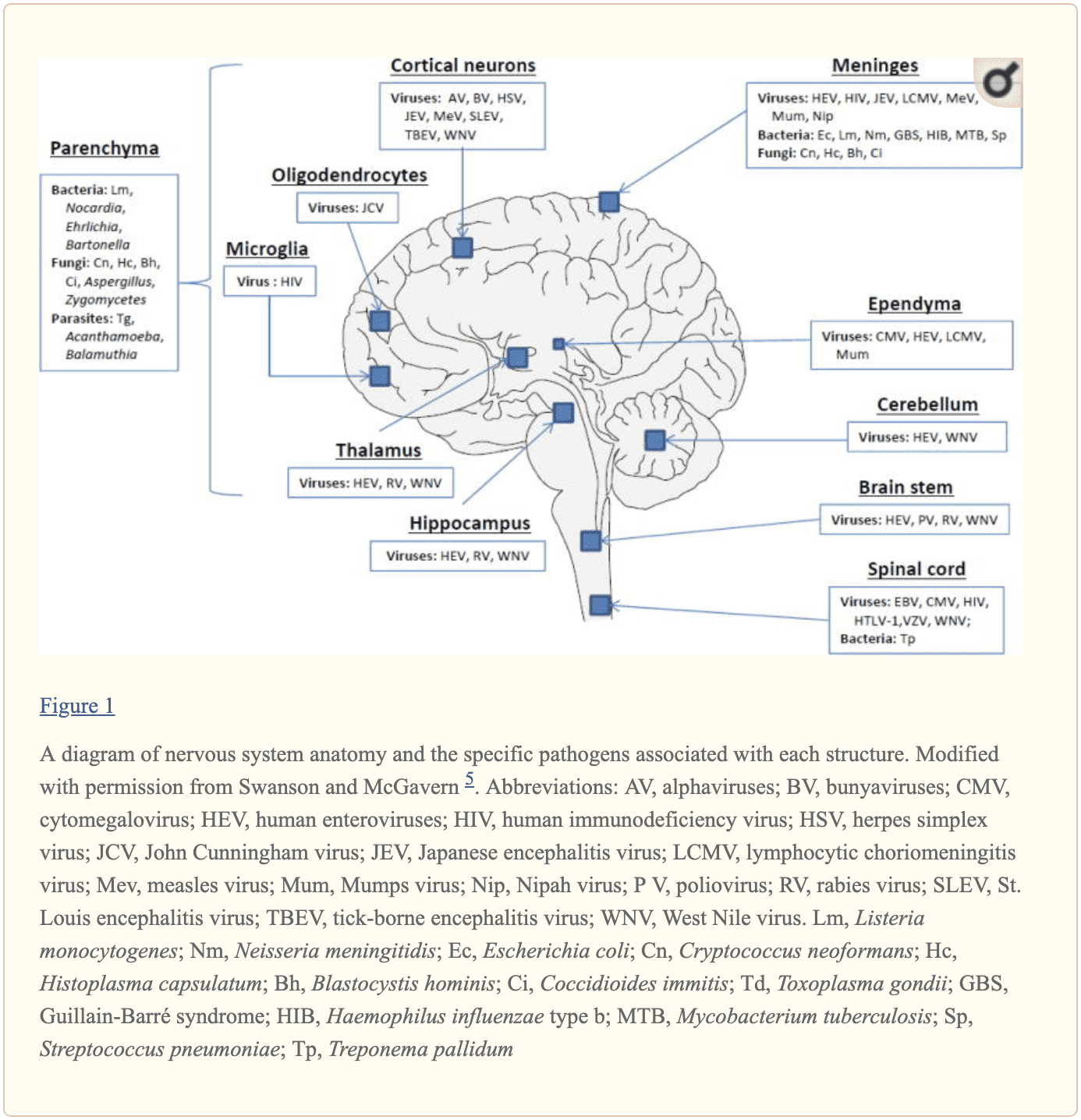
The central nervous system, or CNS, plays a fundamental role in the pathogenesis of infection. The CNS is regulated by the blood-brain barrier or BBB, however, it can still be exposed to a microbial invasion from a contiguous focus, hematogenous dissemination, or intraneural passage of organisms. A variety of environmental or commensal bacteria, viruses, fungi, protozoa, or parasites can enter the CNS and cause a variety of infections and health issues. Central nervous system infections can ultimately cause headache, stiff neck, vomiting, fever, photophobia, and focal neurological symptoms. �
What are Central Nervous System Infections?
CNS infections are characterized according to their affected region. Infection of the brain, spinal cord, and meninges results in meningitis, encephalitis, brain abscess, and myelitis. Infections can affect single or multiple regions of the brain, such as meningoencephalitis and encephalomyelitis. Moreover, CNS infections are characterized as acute, sub-acute, chronic, or recurrent based on their duration. Meningitis can cause headache, neck stiffness, fever, and photophobia over a period of hours to days. Encephalitis can cause brain parenchymal inflammation which can ultimately cause lethargy to coma. Last but not least, Myelitis can cause inflammation of the spinal cord including headache, fever, and paraparesis or paralysis. �
One of the most fatal CNS infections, acute bacterial meningitis, with three to five cases for every 100,000 people in the United States, has a mortality rate of 6 percent to 26 percent. Approximately 4,000 cases of acute bacterial meningitis occur in the U.S. every year with about 500 deaths. The frequent cause of acute bacterial meningitis includes Streptococcus pneumoniae, group B Streptococcus, Neisseria meningitides, Haemophilus influenzae, and Listeria monocytogenes. �
CNS infections caused by viruses are more common and are mostly mild and self-limited. However, these can manifest as meningitis and/or encephalitis. CNS infections caused by viruses can vary due to region and season. Non-polio enteroviruses are responsible for the majority of meningitis and/or encephalitis cases from late spring to fall. CNS infections due to herpes simplex viruses, or HSV, are associated with sporadic encephalitis and meningitis with severe sequelae if left untreated. �
Diagnosis of CNS Infections
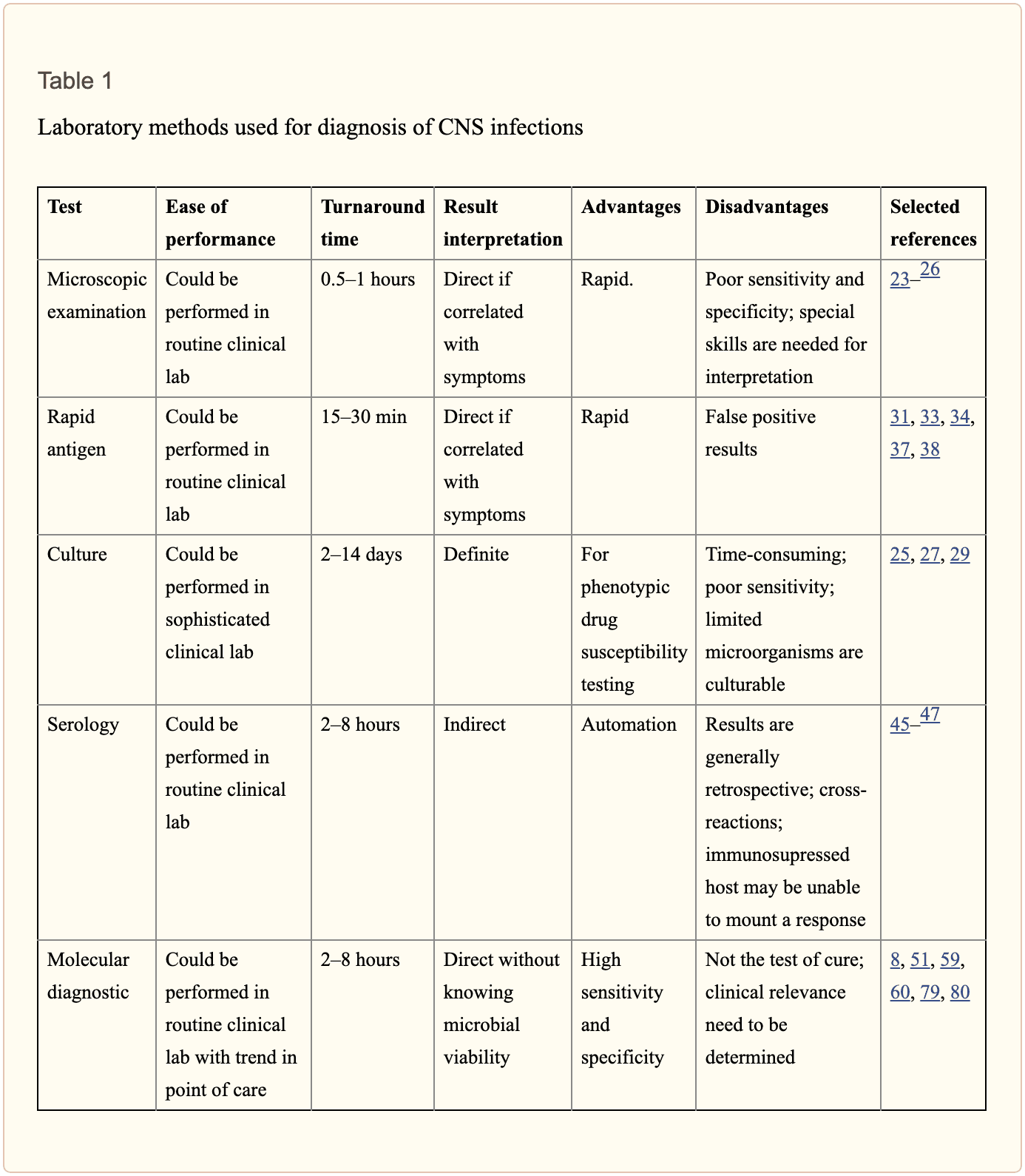
Diagnosis of microbial pathogens is fundamental for treatment. Methods and techniques utilized in clinical microbiology laboratories include direct microscopic examination, and culture techniques as well as antigen and antibody detection assays. However, each method and technique has several essential limitations. By way of instance, direct microscopic examination of CSF restricted sensitivity and specificity. The sensitivity of culture for enteroviruses is between 65 percent to 75 percent with average retrieval time of 3.7 to 8.2 days. Moreover, several serotypes of enteroviruses, especially Coxsackievirus A strains, are well-known to be non-cultivable and frequently grow poorly. Because enteroviruses are missing a common antigen found throughout a variety of serotypes, universal antigen and/or antibody diagnosis is impossible. Diagnosis of CNS HSV infections through methods and techniques utilized to determine culture sensitivity from CSF is tremendously poor. The presence of HSV IgG antibodies in CSF can ultimately be utilized to determine a diagnosis, however, the production is delayed until day 10 or day 12 after infection and it is not considered ideal for early diagnosis.
Diagnostic techniques, especially PCR based amplification, have developed a variety of mainstay tools to help determine the diagnosis of microbial pathogens in CSF. Molecular methods have demonstrated greater diagnosis rates than other diagnostic techniques. One research study demonstrated that 16S rRNA PCR-based assays were able to diagnose the causative organism in 65 percent of banked CSF samples compared to 35 percent when utilizing culture and microscopy. In another research study, diagnosis based on diagnostic techniques like molecular methods were utilized to optimize antibiotic treatment of patients with infectious meningitis when conventional methods and techniques demonstrated a negative outcome measure. Molecular methods and diagnostic techniques utilized on CSF samples are a fundamental standard when compared to the culture standard in the diagnosis of CNS infections caused by viruses which are challenging to diagnose. �
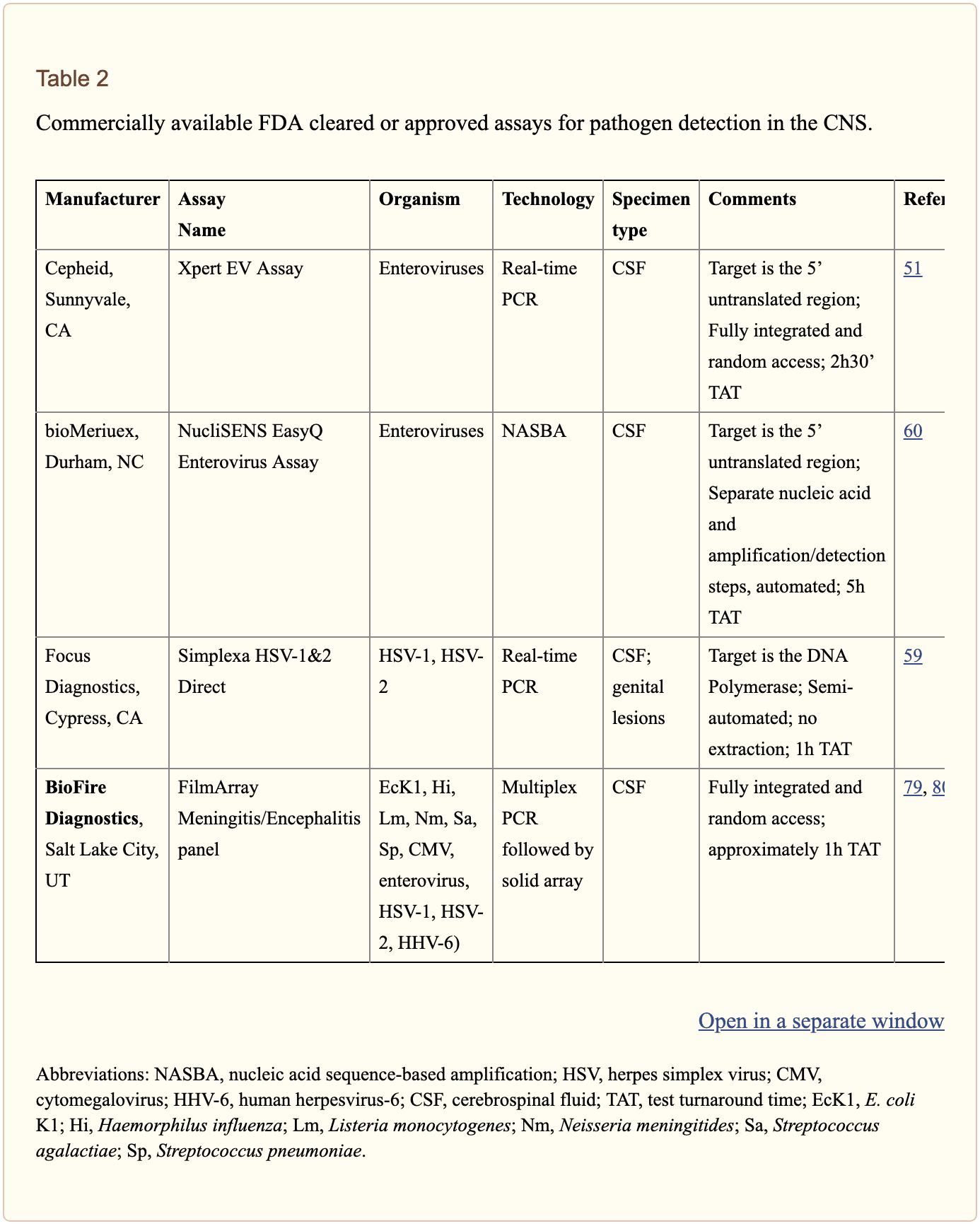
The diagnosis of CNS infections has tremendously changed over the last several years. PCR-based molecular methods have become a fundamental element in the clinical microbiology laboratory, providing tools for an accurate diagnosis. As demonstrated in Table 2, a variety of commercial molecular assays have been cleared by the Food and Drug Administration, or FDA, for the diagnosis of microbial pathogens. The approved assays for pathogen detection in the CNS are shown below. �
However, there are still several challenges in molecular diagnostic techniques and methods. Utilizing a combination of conventional diagnostic techniques and molecular methods, research studies demonstrated that in approximately 62 percent of patients with encephalitis, an etiologic organism could not be identified. Researchers have started to focus on developing advanced techniques and methods. In the following series of articles, we will demonstrate an update on the current conventional and molecular platforms utilized for the diagnosis of CNS infections. We will also demonstrate a preview on the potential clinical application of future technologies, including pan-omic assays. The emphasis of the following series of articles is to demonstrate optimal test selection in the clinical scenario for the diagnosis of CNS infection. �
Conventional Microbiology Methods and Techniques
Microscopic Examination
A positive CSF Gram stain confirms the diagnosis of bacterial meningitis. The sensitivity of the Gram stain for the diagnosis of bacterial meningitis is approximately 60 percent to 80 percent in patients not on antimicrobial treatment and approximately 40 percent to 60 percent in patients on antibacterial treatment. In one research study, Gram stain diagnosed as much as 90 percent Streptococcus pneumoniae and 50 percent Listeria monocytogenes in CSF collected from patients with bacterial meningitis confirmed by PCR 26 techniques and methods. Two organisms which are frequently diagnosed by microscopy include Mycobacterium tuberculosis by acid-fast bacillus, or AFB, staining and Cryptococcus neoformans by India ink or Gram stain. However,� the sensitivities of these techniques and methods are poor and culture is generally utilized instead. �
Culture
Culture of brain tissue can demonstrate a positive diagnosis of CNS infections, however, getting biopsies are tremendously invasive and frequently avoided unless a clinician determines that they are absolutely necessary. CSF sampling is most commonly performed to diagnose CNS infection. CSF viral, bacterial, including mycobacterial, and fungal cultures are fundamental in the diagnosis of infectious meningitis. However, CSF cultures in these cases are extremely low. Another disadvantage of CSF bacterial culture is that it generally requires up to 72 hours to determine a final diagnosis. A recent research study demonstrated that CSF mycobacterial culture had a sensitivity of 22 percent and a specificity of 100 percent in the diagnosis of tuberculosis meningitis. For viruses, utilizing monoclonal antibodies through culture increased the speed and specificity. However, due to time and sensitivity, CSF viral culture is frequently unable to determine a diagnosis. �
Rapid Antigen Detection
Cryptococcal antigen is the most commonly utilized antigen assay for CNS infections. The test utilizes Cryptococcus capsular polysaccharide antigens in CSF through enzyme immunoassay to determine a diagnosis. In a single research study which evaluated patients less than 35 years of age with CNS cryptococcosis, overall sensitivity and specificity of 93 percent to 100 percent and 93 percent to 98 percent were shown. Cryptococcus is a neurotropic fungus. Polysaccharide serum antigen titers with host immune status are frequently utilized to determine the need for a lumbar puncture to evaluate the patient for CNS health issues. The baseline peak titer of polysaccharide antigen in serum or CSF has demonstrated fundamental prognostic significance with an increased titer, or peak titer less than 1:1024, associated with antifungal therapy failure. �
The diagnosis of galactomannan, or GM, antigen and 1,3 ?-D-glucan, or BDG, in CSF, can help in the diagnosis of CNS aspergillosis or other invasive fungal infection such as fusariosis. Increased BDG in serum and CSF is associated with fungal infections. Measuring the levels of BDG is a beneficial biomarker in the evaluation of fungal CNS infection. It was recently demonstrated that patients receiving effective antifungal therapy demonstrated a decrease in CSF BDG concentrations with less than 31pg/ml and for this reason, BDG titers in CSF are a beneficial biomarker when monitoring response to treatment. �
For acute bacterial meningitis, a rapid antigen assay can help diagnose for a pneumococcal capsular antigen. Several research studies have demonstrated the utilization of M. tuberculosis-specific antigens in CSF for the diagnosis of tuberculosis meningitis. M. tuberculosis Early Secreted Antigenic Target 6, or ESAT-6, has been utilized for tuberculosis meningitis. �
Serology
Serological diagnosis of CNS infections is determined by identifying IgM antibodies or by demonstrating an increase in neutralizing antibody titers between acute- and convalescent-phase CSF. Due to a delay in antibody response when symptoms have manifested, a negative antibody test cannot be utilized to rule out infections and retesting may be required. Moreover, in specific populations, such as immunocompromised patients, the tests may not offer optimum sensitivity. In most instances, nucleic acid amplification tests have surpassed antibody-based detection as the test of choice. For several CNS infections, these assays play a fundamental role. CSF IgM is the most commonly utilized test for West Nile virus, or WNV, infections. Antibodies may manifest in as soon as 3 days and may continue for up to 3 months. However, its accuracy is challenged by high cross-reactivity with other flaviviruses and associated vaccines. Antibodies in recombinant WNV E proteins can determine where cross-reacting viruses co-circulate or determine which patients have been immunized. �
Fundamental serological assays for CNS infections are utilized for the diagnosis of neurosyphilis. Neurosyphilis is determined by a positive CSF venereal disease research laboratory, or VDRL, test. Diagnosis of varicella-zoster virus, or VZV, IgG in CSF is the most common technique and/or method for the diagnosis of VZV associated with CNS infection. �

Central nervous system, or CNS, infections can ultimately be life-threatening health issues if they are not diagnosed and treated early. Determining an accurate diagnosis of CNS infections can be challenging. Fortunately, a variety of diagnostic techniques and molecular methods can help determine the source of CNS infections. These diagnostic techniques and molecular methods have tremendously improved over the years and more and more of these evaluations are being utilized in clinical settings to accurately diagnose CNS infections for early treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
In part 2 of our “Diagnosis of Central Nervous System Infections” article, we will ultimately discuss the molecular methods and the pan-omic molecular assays which are utilized in the diagnosis of CNS infections as well as discuss how specific testing outcome measures are associated with clinical diseases and health issues. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�  �
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support

XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
![]()
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
�