IT Iliotibial band syndrome is a very common injury among runners. If it is diagnosed early and treatment commences immediately the chances of it becoming a chronic condition are reduced. It responds very well to chiropractic since it involves the pelvis and related muscles. When pelvic mechanics are not functioning properly the muscle don�t work efficiently which hinders flexibility and mobility. This can lead to tight muscles which may inhibit motion and cause pain. Chiropractic adjustments have been proven to help with the condition.
What Is The Iliotibial Band?
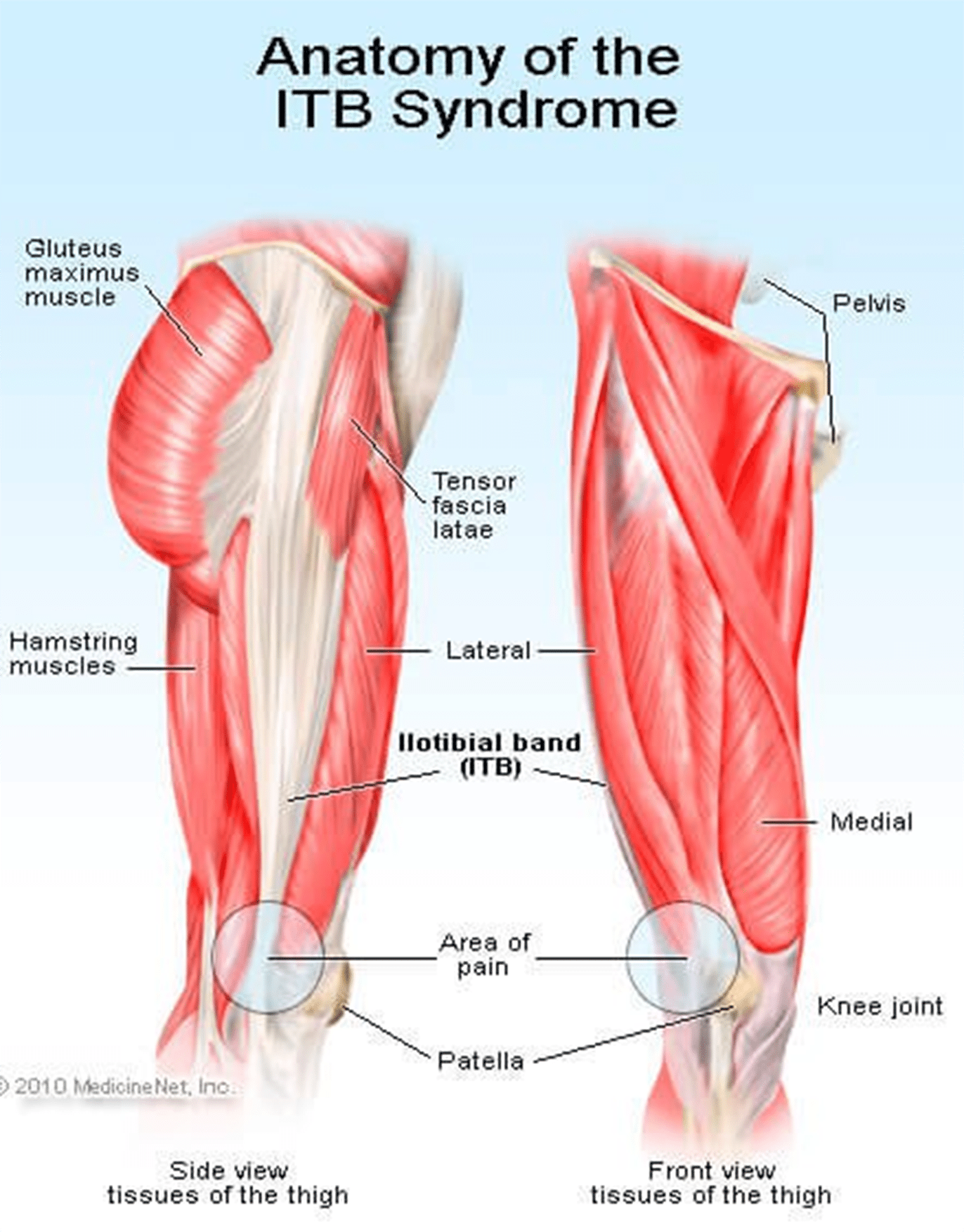
The Iliotibial Band, or fasciae latae, is the outer casing of muscle that extends along the outer thigh, from the top of the hip to the outside of the knee. IT Iliotibial band syndrome occurs when that casing becomes thickened. It is flexed or tight when you stand; it is what keeps your let straight, allowing the larger thigh muscle to rest.
There are two primary muscles that are involved in iliotibial band syndrome, the buttock muscle, or gluteus maximus, and the tensor fasciae latae muscles. Sometimes Iliotibial Band Syndrome is referred to Tensor Fasciae Latae Syndrome and the two terms can be used interchangeably.
IT Iliotibial Band Syndrome Defined
As the iliotibial band thickens it pulls in the area where it connects to the knee. This results in knee pain due to the application of too much pressure on the bursa. The bursa then becomes swollen, inflamed, and painful. During activity, such as running on an incline, the glutes are heavily involved.
The other end of the iliotibial band is inserted at the glutes so as the band tightens from this activity, it can trigger iliotibial band syndrome pain. Repeated activity further aggravates it, as does running on tight indoor tracks or uneven roads as well as having collapsed arches or running it inferior or worn out running shoes.
Symptoms Of Iliotibial Band Syndrome
There are several symptoms that can be used to diagnose iliotibial band syndrome. Lateral knee pain (pain on the outside of the knee) is a primary symptom and often used as a key diagnostic tool. Few conditions involve lateral knee pain. Other symptoms include:
Pain that worsens after running, particularly after running on an incline, climbing stairs, or climbing hills
There may not be any pain until you do something that aggravates it like climbing a hill.
The pain may not begin until you are mid-way through a run.
The pain can be intense and debilitating.
It can accompany a snapping hip, which occurs when the muscles that cross the outer hip may click or snap while running or walking.
The pain may be present along the lateral thigh without incorporating the knee, but it is only in very rare instances that it is concentrated on the gluteal or hip muscles.
Iliotibial band syndrome is often attributed to over training. This can mean suddenly increasing hill repeats or doubling your mileage.
Treatments For IT Iliotibial Band Syndrome
If your iliotibial band syndrome is caused by a problem with pelvic function, relieving the pain from the condition can be difficult. Stretching is not likely to bring relief � and if it does it won�t last long. If the pain from iliotibial band syndrome lasts for more than two weeks even if you are only stretching, your regular exercise routine, and ice and you don�t see much improvement, a chiropractor can help.
Even if the pain is located in the knee, the problem could originate in the pelvis. A chiropractor can assess your condition, check to see that your pelvis is functioning properly. If it isn�t, spinal adjustments and other chiropractic treatments can bring the body back into alignment and make the pelvis more functional.
Chiropractic Clinic Extra: Sport Injury Treatments
El Paso, TX. Chiropractor, Dr. Jimenez takes a look at top running shoes that are great for knee pain and Iliotibial (IT) Band Syndrome.
Running Shoes: Knee pain is one of the common problems with most active people. It could get worse for those who love running, especially the athletes. A majority of them suffer from knee pains each year. This pain hinders you from enjoying your daily sports activities and might even become worse with time if not treated correctly. There are causes and cures for such pains that this article is going to look at, but the main focus is on the best shoes for knee pain, also referred to as Iliotibial (IT) Band Syndrome.
This can happen due to various causes like overtraining, running many hills, and wrong running form, among others. These injuries are very frustrating as they can take up to months to go away. This is the reason different companies have designed shoes that will offer you support for any knee problem.
What Goes Wrong
The iliotibial band (ITB) is usually a structure whose job is to provide leg stability whenever you take a step. It works with the hip muscles in a thigh’s outward movement and also helps counter the movements within the knee joint. This band starts in the hip and ends just under the knee joint.
Repeated use of the ITB leads to stress, causing knee pain. You will also notice clicking sensations from the joint as ITB snaps across it. This pain is always experienced when the heel comes into contact with the ground; running slowly or downhill tends to make the symptoms worse.
ITBS will usually start as tightness while running but continues to a point where the pain is severe and unbearable. Although ITB continues to tighten when overstressed or injured from training, this is not the main problem. What causes the injury is how the ITB functions and the weakness around it.
The ITB is generally a weak structure and any weakness around it will lead to injury. Most runners have weak core muscles due to the fact that they don’t do strength training or have never been in any sports with side-to-side movement.
Signs Of IT Band Syndrome
If you are a runner, you will be able to distinguish ITBS by:
A swelling
A cracking feeling when stretching the knee
A feeling of burning, stinging and aching on the outer side of the knee that might migrate to the thigh. You will notice these discomforts especially, on your second half of the run.
Bending the knee at 45 degrees causes severe external knee pain
Criteria You Should Follow When Selecting The Best Running Shoes for ITBS
?There are various things that you should always consider when buying running shoes. Since most runners experience knee pain, it is wise to look for shoes that will help alleviate this pain without slowing them down. Below are some of the features to look out for in running shoes:
Stability/ Support
Since it is common to have knee pains due to lack of motion control and lack of stability, it is good to choose shoes that will offer you the support you need while running. If your running shoes don’t have any stability, you will end up stressing out your knee, which will result in pain and discomfort while running.
Fit
If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If your foot cannot move freely and the toes are restricted from spreading, it could lead to painful issues in your feet, legs, and knees.
Motion control footwear is not the whole solution; you need to ensure your feet can still function naturally as they are supposed to.
Comfort
No one wants to wear uncomfortable shoes! Each of these selected best shoes come with upper and underfoot comforts to ensure you get to enjoy your run.
Most of these shoes are made with DNA technology, Gel cushioning, and REVlite midsole for ultimate comfort.
Durability
Your running shoes should run their course without falling apart as this will cause you pain in the long-run. If they promise to offer you support, they should do just that and not start peeling off and tearing when you are on the run.
The ??below 5 shoes have passed the durability test to ensure they give you maximum performance.
Breathability
Although this has nothing to do with knees, it is paramount that your running shoes have enough breathing space to avoid accumulating excess moisture, which might bring discomfort and other feet related problems.
There is no magical cure for knee pain and you should always know the root cause. This way, you will be able to come up with the best solution of minimizing or even eliminating the pain entirely. Although there are various causes of knee pain, this article is focusing on ITB syndrome which happens to be one of the causes.
Reviews Of The Top 5 Shoes
These shoes have been selected with the runner’s welfare in mind. They will help deal with the ITBS, which is a problem for most of them. Since one way of dealing with this condition is getting good running shoes, here is a review of such products.
Asics Gel Kayano 23
This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
PROS
?Gel cushioning will act as a shock absorber for more comfort
?Has superb breathability feature
?Is ideal for overpronation and knee pain
?The outsole’s traction will offer the intended support on various surfaces
CONS
?It is a bit pricey
New Balance 890v5
It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
PROS
?It comes with one of a kind breathability and fit due to its great FantomFit design
?Its smooth upper construction will ensure no irritation occurs
?The REVlite midsole will give you much needed cushioning
CONS
?It has a narrow toe box and might not fit a person with a wide foot
?Puma Faas 600 V3
Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
PROS
?Great breathability
?Comes at a reasonable price
?It’s lacing system and fit offers you a secure and comfortable run
?It is designed to fit perfectly
CONS
?There have been reported concerns about the outsole’s durability
New Balance 1080v7
This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
PROS
?Very durable
?Enough breathability for long runs
?Good amount of cushioning and support from the Fresh Foam midsole
?It fits like a sock giving you a confident use
CONS
?The upper design is not seamless
?Can be stiff
Saucony Hurricane 16
This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
PROS
?Superb stability
?Lightweight rubber offers protection and cushioning
?Great ground contact
?Reflective parts allow you to have a safe run
?Comes with Sauc-Fit Technology that enhances its comfortability
CONS
?It is a bit narrow
?Limited colors to choose from
?Might be heavy for fast runners
If you are a long-distance runner, it is good to know that your shoes cushioning will wear out quite easily and you might be tempted to continue using them since they look good on the outside. This is a big mistake. The following will help you prevent any more ITBS recurrences:
Replace running shoes frequently to avoid wearing those with worn out inner cushioning
Always give your shoes time to rest so that the cushioning can get restored; it would be wise to have two pairs of running shoes.
Although shoes can offer you relief from ITBS, it is better to look out for other ways of helping you cope with or eliminate the pain entirely. Also, know what triggers the problem and avoid it at all costs.
These shoes have been tried and tested and found to offer support and help in managing the iliotibial band syndrome. Asics takes the lead on these best shoes. It comes with gel cushioning that will offer you the best shock absorption and maximum comfort as seen above. Its sole is also made to help you tackle any terrain and you can be assured that your knees will thank you later. The only drawback is the price, which is on the upper-side. However, always remember that cheap is expensive.
If you are an active person or an athlete suffering from ITBS, go ahead and get yourself a pair of these shoes as per your preference and choice.
Hey there, I’m Zoey, founder and the main editor of The Babble Out. I know nobody’s life is smooth as they wish, and it�s the same with mine. I had some terrible news a few years ago and running was the way I got through these issues. This has given me enough motivation to create this blog, so that I can give you a helping hand for as many daily problems as I can. If you are curious why “babble out” is the? name of the blog, then check the “About” page and find out more about me.
Chiropractor, Dr. Alexander Jimenez looks at the way this common injury shows itself.
Introduction
Iliotibial band syndrome (ITBS) between the knee is frequently diagnosed in sport injury clinics. ITBS presents having an incidence rate of around 22% in most lower extremity running-related injuries (1) also has been said to be the second most common complaint amongst distance runners (2). ITBS has been given the expression ‘runner’s knee’.
Trainers like endurance runners who perform flexion and extension combined with loading are subjected to this illness. ITBS presents during the first two or three miles in running with no mechanism of injury, which can make identifying the cause more interesting. With plenty of factors having been considered within the literature, changes are often purported to be a cause of ITBS. But some biomechanical factors have been researched and have been found to have little or no effect in the start of ITBS. Therefore this text’s point would be to examine the biomechanical changes which may induce an individual to the beginning of ITBS. The research published reviewed is largely based on a current systematic review that was published in Physical Therapy in Sport in 2014 (3).
Anatomy & Function
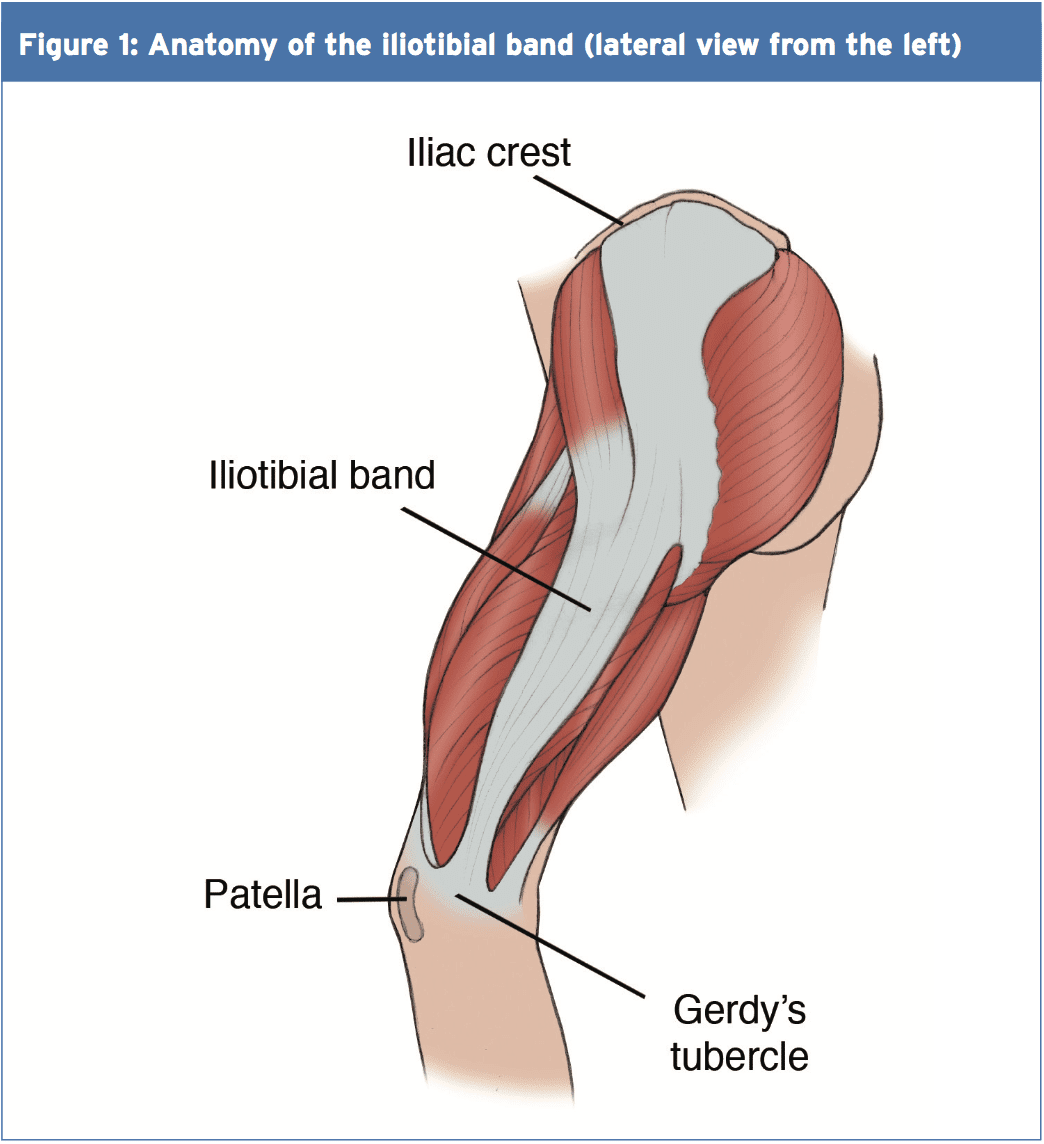
The iliotibial band (ITB) encapsulates the tensor fascia latae (TFL) presenting with both deep and superficial fibre attachments at the pelvis (4). In addition to attaching to the TFL, approximately three-quarters of the gluteus maximus tendon also conjoins with the ITB (4). The ITB courses along the lateral aspect of the hip and passes the greater trochanter. The ITB maintains an attachment on the posterior ridge of the femur whilst attaching itself to the fascia. The ITB has a fixed attachment at the lateral femoral condyle where it then divides into three segments with the first being the lateral patella (3). The remaining two segments cross the knee joint to insert at the head of fibula and most distally at the infrapatellar tubercle also known as Gerdy’s tubercle on the tibia (3). Figure 1 illustrates the location of the ITB.
The ITB passively functions to resist hip adduction, hip internal rotation and internal rotation of the knee in accordance with its attachments at the pelvis, femur and tibia(3). The gluteus maximus functions, through its attachment, to increase stability through the hip and knee complex by increasing the tension of the ITB(4). It is possible to see, based on its attachments at both the knee and hip, how changes could bring about the onset of ITBS.
Studies have proposed that as the knee flexes and extends the ITB ‘slides or flicks’ over the lateral femoral condyle of the knee causing an irritation beneath. This notion was debated by Falvey and colleagues (5), who stated that it was highly unlikely that the ITB would flick or slide over the bone during knee flexion due to it not being a loose structure. But the authors did agree that the impact of compression on the richly innervated fat pad was pain’s cause but by strain of the ITB where pain presents crossing the lateral femoral condyle. Strain rate and strain magnitude were measured in a prospective study involving female runners (6). The results indicated that frequency of strain of the ITB at the lateral femoral condyle was greater that the strain magnitude. This implies that a runner might have the ability to run for a short period but then incur lateral knee pain because of the strain to the ITB.
MRI scans have ascertained the knee flexion angle of 30� elicited the greatest compression of the ITB at the point of heel strike, whereas others have said that maximal compression occurs between 20-30�(2,6). A knee flexion angle at the point of heel strike has been found to be significantly different with 20.6� in ITBS patients compared to 15.3� in the control(7). Downhill running produces a greater knee flexion angle at the point of heel strike eliciting a larger strain load to the ITB and therefore this is often a main precursor to ITBS (6). Although an elevated knee flexion angle at the point of heel strike has been considered to contribute to ITBS, it is essential to examine the lower extremity from the frontal and transverse planes too and not solely from the sagittal plane (2).
Rearfoot Eversion
It’s possible to envisage how rear foot eversion could contribute to ITBS causing internal rotation of the tibia resulting at the distal attachment in greater strain of the ITB. In contrast Ferber and colleagues (2) indicated that there was no significant difference in the peak eversion angle of the female subjects, who were previously diagnosed with ITBS but were now symptom free, compared to controls. In a similar study non-significant differences were found between the currently symptomatic ITBS patients and controls for rear foot eversion (8).
Louw & Deary(3) found that ITBS patients sometimes demonstrated decreased eversion angles, accompanied by decreased internal rotation of the knee, at the point of heel strike. Ferber and colleagues (2) noted an increased inversion moment in the ITBS group which was suggested to control and limit the eversion moment. By comparison, currently symptomatic ITBS patients demonstrated a substantial difference compared to a control group with twice the rear foot motion during running (9).
Knee Internal Rotation
Peak internal rotation angle of the knee was found to be significantly greater in the ITBS patients when compared with controls at the point of heel strike (2). This research was supported by other studies who also found a significant effect for increased internal rotation of the knee following a run of moderate intensity to physical exhaustion(7). With excessive rotation comes compression due to increased strain of the ITB at the attachment.
An explanation of increased internal rotation of the knee was attributed to excessive external rotation of the femur perhaps due to shortening of the piriformis, gemellus inferior and superior and the obutrator externus (8). The authors added that excessive rotation at the hip might result from muscular activity of the rotators that were hip being the medius, minimus and the tensor fascia latae. These studies(2,7) were retrospective in design in that they tested healthy runners with a history of ITB pain, whereas(8) was a prospective study of patients with ITBS at the point of testing.
Hip Adduction Angle & Hip Abductor Strength
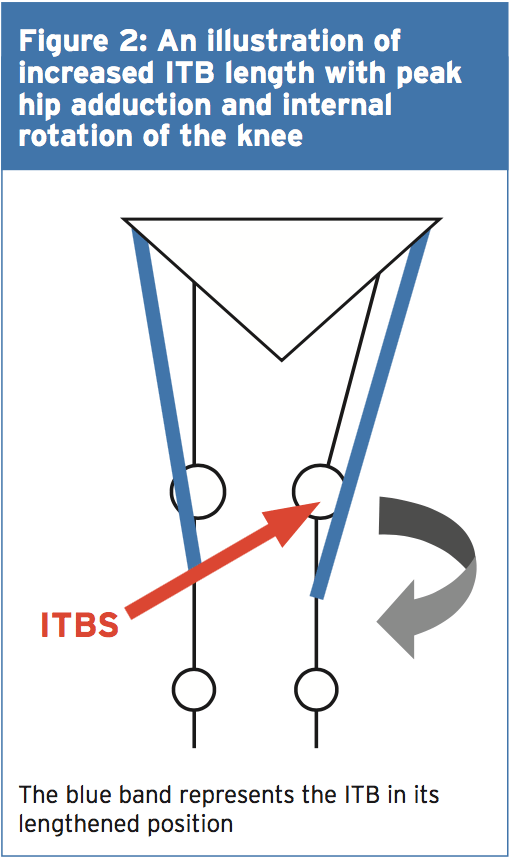
The hip adduction angle during the stance phase has been suggested to be greater. Ferber and colleagues(2) found that the peak hip adduction angle was significantly greater in the ITBS cohort and stated that with 95% confidence. Increased angle results in increased stress to the ITB and consequently increased compression at the lateral femoral condyle when combined with increased internal rotation of the tibia.
Figure 2 illustrates, when peak hip adduction and internal rotation combine, how this may result in increased the compression of the ITB at the lateral femoral condyle. Louw and Deary(3), however, stated that it remained inconclusive whether the peak hip adduction angle was a substantial element. Additional research is therefore required to support Ferber and colleagues'(2) initial findings as this study was a retrospective study carried out on healthy female runners with a history of ITBS.
Hip Abductor Strength
It’s been proposed that an increased peak hip adduction angle may coincide with hip abductor activity involving the gluteus medius in this group. During the stance phase of gait the gluteus medius functions to keep stability. Research has indicated that during stance the adduction forces can exceed three times an individual’s body weight(3). What’s more, it was stated that these forces were beyond the metabolic capacity of the gluteus medius to main pelvic stability during the stance phase using just this muscle alone(3).
Louw and Deary (3) were not able to identify a heightened hip abductor moment in the ITBS patients with increased peak hip adductor angles and suggested that it was more of an issue of timing as opposed to the size of the hip abductors. Louw and Deary (3) stated that the research is yet to examine trunk and pelvic movements in ITBS patients and it is plausible to suggest that biomechanical changes from higher up the kinetic chain has the potential to be a contributing element in ITBS etiology.
A research study of 24 (14 female, 10 male) patients with ITBS undertook a six-week rehabilitation programme to increase the strength of the hip abductors(10). Following six weeks of hip abductor strengthening to running 22 patients reported being pain-free and had returned. The female patients reported an average hip abductor torque increase of 34.9% and the male patients found 51.4% increase. However this study used a hand held dynamometer to measure isometric strength and therefore Fedricson (10) findings should be viewed with caution.
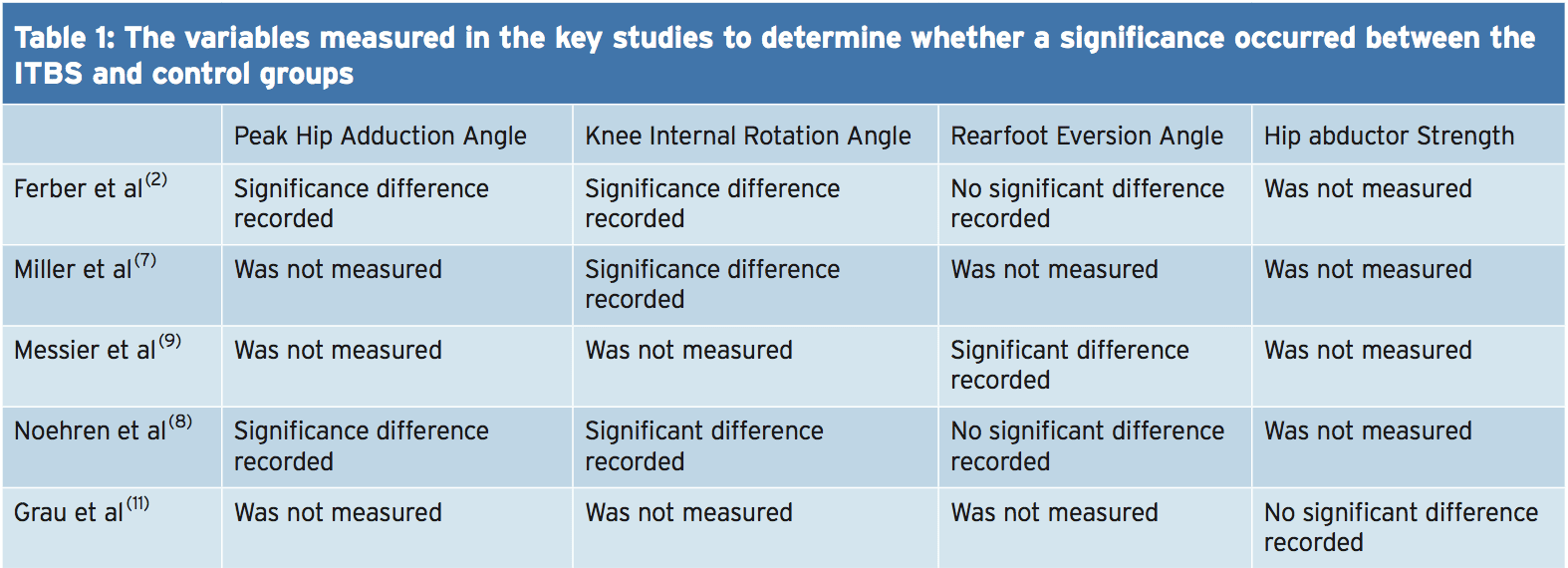
A more recent study assessed the hip abductor strength of currently symptomatic patients with healthy controls in a fixed position(11). The results indicated that no substantial differences occurred for static and dynamic hip abductor strength between the groups. Further research should look into the EMG and strength of the hip abductors in the role of managing ITBS. Table 1 shows of significance in the some of the variables of the studies used in this text.
Rehabilitation programs, following periods of immobilization and during, should include gluteal exercises to provide stability to the leg that is involved. If active exercises for the gluteal muscles are provided in a manner that is secure and effective then this can influence the period of transition from non weight. It’s prudent based on the research provided to date to develop function although research is lacking in terms of quality and volume as to the biomechanical influences on the etiology of ITBS. This guarantees that once load bearing commences that the leg that is involved has the stability and control that is active to keep the beginning of load of the ITB.
Summary
The recent review published by Louw and Deary(3) indicates that much of the research published within the literature depending on the etiology of ITBS is inconclusive. The level of research is relatively low and is based on retrospective trials. The research does indicate that knee biomechanics and abnormal hip is involved in the occurrence of ITBS. The authors ascertain that muscle strength is involved as is foot biomechanics that are abnormal. It is recommended that future research should measure kinematic movements of the hip and knee during downhill running as this is a complaint of ITBS onset.
References
1.Clini J of Sports Med, May 2006,16, (3), 261-268
2.J of Sports Phys Therap, Feb, 2010, 40, 2, 52-58.
3.Phys Therap in Sport, 2014, 15, 64 e75.
4.Surgic and Radiologic Anatomy (Dec) 2004; 26, (6), 433 – 446
5.Scand J of Med & Sci in Sports, Aug 2010, 20 (4), 580-587.
6.Clini Biomech, 2008, 23, 1018-1025.
7.Gait Posture. 2007 Sep, 26 (3), 407-13
8.Clini Biomech, Nov 2007, 22 (9), 951-956.
9.Med Sci in Sport & Ex, 1995, 27, 951-960.
10.Clini J of Sports Med, 2000, 10:169�175.
11. Int J of Sports Med, Jul, 2008, 29 (7), 579-583.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Symptoms Of Iliotibial Band Syndrome
Symptoms Of Iliotibial Band Syndrome
 Signs Of IT Band Syndrome
Signs Of IT Band Syndrome If you are a runner, you will be able to distinguish ITBS by:
If you are a runner, you will be able to distinguish ITBS by: If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted. This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible. It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice. Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed. This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains. This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.