An improper diet and nutrition can often lead to a variety of health issues, such as cardiovascular disease and hypertension. Additionally, other food-related risk factors can include, high blood pressure, or BP, obesity and type 2 diabetes. Saturated and trans fats, for example, can increase cholesterol in the blood. It’s this build-up of fatty deposits in the coronary arteries, which can lead to cardiovascular disease, hypertension and even heart attacks.
Which vitamins and minerals can improve cardiovascular disease and hypertension?
A healthy balance of vitamins and minerals can help manage and maintain heart health. According to research studies, the right intake of potassium, magnesium, calcium and zinc can substantially improve cardiovascular disease and hypertension. A proper diet and nutrition can have similar effects as taking cardiovascular disease and hypertension drugs and medications, but through a much more natural approach.
Potassium
The average U.S. dietary intake of potassium (K+) is 45 mmol/d with a potassium to sodium (K+/Na+) ratio of less than 1:2. The suggested intake of K+ is 4700 mg/d (120 mmol) with a K+/Na+ ratio of about 4-5 to 1. Several clinical and observational trials have demonstrated a substantial decrease in BP with greater K+ intake in hypertensive patients. The normal blood pressure reduction with a K+ supplementation of 60 to 120 mmol/d is 4.4/2.5 mmHg in hypertensive patients but may be as far as 8/4.1 mmHg with 120 mmol/d (4700 mg). In hypertensive patients, the linear dose response relationship is 1.0 mmHg reduction in systolic blood pressure, or SBP, and 0.52 mmHg decrease in diastolic blood pressure, or DBP, that a 0.6 g/d growth in dietary fiber intake. The solution can involve race (black > white), sodium, magnesium and calcium intake. Those on a higher sodium intake have a greater decrease in BP. Alteration of this K+/Na+ ratio is very important to the two polyunsaturated and outcomes. High potassium intake reduces the prevalence of cardiovascular disease independent of their BP reduction. Furthermore, If the serum potassium is less than 4.0 meq/dL, there is a higher risk of CVD mortality, ventricular tachycardia, and ventricular fibrillation. Red blood cell potassium is a sign of overall body stores and CVD risk in comparison to the serum potassium. Gu et al discovered that potassium supplementation in 60 mmol of KCl Daily for 12 wk significantly reduced SBP -5.0 mmHg (range -2.13 into -7.88 mmHg) (p < 0.001) in 150 Chinese men and women aged 35 to 64 decades.
Insulin raises natriuresis, modulates sensitivity, vasodilates, reduces the sensitivity to catecholamines and Angiotensin II, raises nitric oxide ATPase and DNA synthesis in the vascular smooth muscle cells and decreases sympathetic nervous system activity. In addition, potassium increases bradykinin and prostate kallikrein, decreases NADPH oxidase, which reduces oxidative stress and inflammation, improves insulin sensitivity, reduces ADMA, reduces intracellular sodium and reduces production of TGF-?.Each 1000 mg increase in potassium intake per day reduces all cause mortality by approximately 20 percent. Potassium intake of 4.7 g/d is estimated to decrease CVA by 8 percent to 15 percent and MI by 6 percent to 11 percent. Numerous SNP’s, such as nuclear receptor subfamily 3 group C, angiotensin IItype receptor and hydroxysteroid 11 beta dehydrogenase (HSD11B1 and B2) determine an individual’s reaction to dietary potassium intake towards their overall health and wellness.
Each 1000 mg drop in sodium intake daily will reduce all cause mortality. A recent study indicated a dose related response to CVA. There has been a RRR of CVA of 23 percent at 1.5-1.99 gram, 27% at 2.0-2.49 g, 29 percent at 2.5-3 g and 32 percent more than 3 g/d of potassium urinary excretion. The recommended daily dietary intake for individuals with hypertension is 4.7 to 5.0 g of potassium and less than 1500 milligrams of sodium. Potassium used out of supplementation should be decreased with care in patients with renal impairment or those ARB, DRI and serum aldosterone receptor antagonists.
Magnesium
A high dietary intake of magnesium of at least 500-1000 mg/d reduces BP in the majority of the reported observational epidemiologic and clinical trials, but the outcomes are much less consistent than those seen with K + and Na +. There’s an inverse relationship between BP and dietary magnesium intake. A report on 60 essential hypertensive subjects given magnesium supplements showed a substantial decrease in blood pressure in an eight week interval reported by 24 h ambulatory BP, office and home BP. The maximum decrease in clinical trials has been 5.6/2.8 mmHg but some studies have shown no change in BP. The blend of high potassium and low sodium intake with increased magnesium intake had.
Magnesium also raises the effectiveness of all anti-hypertensive drugs and medications, according to research studies. Magnesium competes with Na+ for binding sites on vascular smooth muscle and also functions as a direct vasodilator, . Magnesium increases prostaglandin E (PGE), modulates intracellular sodium, potassium, calcium and pH, increases nitric oxide, improves adrenal function, reduces oxLDL, reduces HS-CRP, TBxA2, A-II, and norepinephrine. Magnesium also enhances insulin resistance, glucose and MS, binds at a necessary cooperative manner with potassium, causing EDV and BP reduction, reduces CVD and cardiac arrhythmias, reduces carotid IMT, reduces cholesterol, reduces cytokine production, inhibits nuclear factor Kb, reduces oxidative stress and inhibits platelet aggregation to reduce thrombosis. Magnesium is an essential co-factor because of its delta-6-desaturase enzyme that for conversion of linoleic acid (LA) to gamma linolenic acid (GLA) required for synthesis of this vasodilator and platelet inhibitor PGE1.
A meta-analysis of all 241378 patients utilizing 6477 strokes showed a reverse relationship of dietary magnesium to the incidence of stroke. For each 100 milligrams of magnesium intake, stroke diminished. The mechanism comprise inhibition of induced glutamate release, NMDA receptor blockade, CCB actions reduction in vasodilation and ATP depletion of the arteries. A meta-analysis showed discounts mmHg in 22 trials of 1173 patients. Intracellular level of calcium (RBC) is more indicative of overall body shops and should be quantified along with serum and urinary magnesium. Magnesium might be supplemented in doses of 500. Magnesium formulations may improve absorption and reduce the incidence of diarrhea. Adding taurine in 1000 increases the ramifications of magnesium. Magnesium supplements should be avoided or used with caution in individuals with renal insufficiency.
Calcium
Population studies reveal a link between hypertension and calcium, but clinical trials that handled calcium supplements have shown consequences on blood pressure. The heterogeneous responses to calcium supplementation have been clarified through research studies. This is really the “ionic hypothesis” of hypertension, cardiovascular disease and associated cognitive, cognitive and functional disorders. Calcium supplementation is not recommended at this time as an effective method to decrease blood pressure due to insufficient research studies on its use.
Zinc
Low serum zinc levels in observational research and hypertension correlate as well as CHD, type II DM, hyperlipidemia, elevated lipoprotein that a [Lp(a)], increased 2 h post-prandial plasma glucose levels and insulin resistance. Zinc is hauled to vascular and cardiac muscle and cells by metallothionein. Deficiencies of metallothionein with intramuscular zinc deficiencies can lead to cardiomyocyte oxidative stress , mitochondrial dysfunction, dysfunction and apoptosis with cardiac remodeling hypertension, cardiovascular disease, heart failure, or fibrosis. Intracellular calcium increases oxidative.
Bergomi et al assessed Zinc (Zn++) status in 60 hypertensive subjects compared to 60 normotensive control subjects. A reverse correlation of serum Zn++ and BP has been observed. The BP was inversely associated with a Zn++ dependent enzyme lysyl oxidase activity. Zn++ inhibits gene expression and transcription through NF-?Band activated protein-1 and is now a significant co-factor for SOD. These impacts plus those on insulin resistance and SNS consequences, membrane ion exchange, RAAS might account for Zn++ antihypertensive effects. Intake needs to be 50 mg/d.
Individuals with cardiovascular disease and hypertension can benefit from the proper diet and nutrition. Essential vitamins and minerals found in a balanced, healthy nutrition, such as potassium, magnesium, calcium and zing, among others, can help improve heart health. Deficiencies in these and a diet full of saturated and trans fats can increase the prevalence of cardiovascular disease. While diagnosis and drugs/medications can be prescribed to treat cardiovascular disease and hypertension, a balanced diet and nutrition can have similar effects.� The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Cardiovascular disease and hypertension can often occur due to a variety of factors, however, an improper diet and nutrition has been appointed to be one of the most prevalent causes behind the onset of cardiovascular disease and hypertension. While an improper diet and nutrition can lead to these issues, a balanced, healthy diet and nutrition can help prevent cardiovascular disease and hypertension, even treat the existing conditions.
What’s the best dietary and nutritional approach to treat cardiovascular disease and hypertension?
Many of the substances in food, particularly in nutraceutical supplements, antioxidants, vitamins or nutritional supplements, function in a manner that is similar to a category of drugs and medications to improve cardiovascular disease and hypertension. The effect is synergistic when used in combination with other nutritional supplements even though the drug might not be less than the potency of the compounds. These natural compounds have been outlined to the significant antihypertensive drug classes, such as diuretics, beta blockers, central alpha agonists, direct vasodilators, calcium channel blockers (CCB’s), angiotensin converting enzyme inhibitors (ACEI’s), angiotensin receptor blockers (ARB’s) and direct renin inhibitors (DRI).
Dietary Approaches to Stop Hypertension
The Dietary Approaches to Stop Hypertension (DASH) Iand II diets conclusively demonstrated significant reductions in BP in borderline and stageIhypertensive patients. Back in DASH I, untreated hypertensive subjects with SBP < 160 mmHg and DBP 80-95 mmHg were placed on one of three diets for 4 weeks, controled diet, vegetable and fruit diet (F + V) and combined diet, which added F + V and low fat milk. Sodium restriction was added by DASH II in every group. The control diet consisted of sodium at 3 g/d, potassium, calcium and magnesium in 25% of the US average, macronutrients at US average of 4 portions every day, a sodium/potassium ratio of 1.7 and fiber at 9 g/d. The F + V diet raised the potassium, calcium and magnesium to 75 percent, macronutrients compared to the US average, a sodium potassium ratio of 0.7, 31 gram of fiber and 8.5 portions of vegetables and fruits per day. The joint diet was similar to the F + V diet but additional fat milk. At 2 wk the BP was decreased by 10.7/5.2 mmHg from the hypertensive patients in DASHIand 11.5/6.8 mmHg from the hypertensive patients in DASH II. These reductions persisted provided that the patients were on the diet. The DASH diet increases plasma renin activity (PRA) and serum aldosterone levels in response to this BP reductions) The increase in PRA was 37 ng/mL every day. There has been an associated of reaction with the polymorphism of beta 2 adrenergic receptor. The A allele of G46A had blunted PRA and a higher BP reduction and aldosterone. The arachidonic acid (AA) genotype had the best response along with the GG genotype had no response. Adding an ARB, DRI or ACEI improved BP reaction due to blockade of the increase in PRA to the DASH diet at the GG group. A very low sodium DASH diet reduces oxidative stress (urine F2-isoprostanes), enhances vascular function (enhancement indicator) and lowers BP in salt sensitive areas. In addition, plasma nitrite increased and pulse wave velocity decreased on the DASH diet at week two.
Sodium (Na+) Loss and Hypertension
The average sodium intake in the US is 5000 mg/d with some regions of the nation consuming 15000-20000 mg/d. On the other hand, the minimal requirement for sodium is most likely roughly 500 mg/d. Epidemiologic, observational and controlled clinical trials reveal that an increased sodium intake is associated with increased risk for proteinuria, renal insufficiency, CVD LVH, CHD, MI and of the SNS as well as BP. A decrease in sodium intake in hypertensive patients the salt sensitive patients, will significantly lower BP by 4-6/2-3 mmHg that’s proportional to the level of sodium restriction and might stop or delay hypertension in high risk patients and decrease CV events.
Salt sensitivity (? 10% increase in MAP with salt loading) occurs in about 51 percent of hypertensive patients and is a vital variable in determining the cardiovascular, cerebrovascular, renal and BP responses to dietary salt intake. Cardiovascular events are prevalent in the salt patients than ones, independent of BP. An increased sodium intake has a direct positive correlation with BP and the risk of CHD and CVA. The risk is independent of BP to get CVA with a relative risk of 1.04 to 1.25 in the lowest to the highest quartile. In addition, patients may convert into a BP routine with increases in nocturnal BP as the sodium intake increases.
Increased sodium intake has a direct impact on endothelial cells. Sodium promotes cutaneous lymphangiogenesis, increases endothelial cell stiffness, reduces dimensions, surface area, volume, cytoskeleton, deformability and pliability, reduces eNOS and NO generation, raises asymmetric dimethyl arginine (ADMA), oxidative stress and TGF-?. Every one of these vascular responses are increased in the presence of aldosterone. These modifications occur independent of BP and may be partially counteract by potassium. The endothelial cells act as vascular salt sensors. Endothelial cells are targets for aldosterone which activate epithelial sodium channels (ENaCs) and also have a negative effects on discharge of NO and on endothelial function. The mechanical stimulation of the cell plasma membrane along with the submembranous actin network (endothelial glcyocalyx) (“shell”) serve as a “firewall” to protect the endothelial cells and are regulated by serum sodium, potassium and aldosterone within the physiological selection. Changes in shear-stress-dependent activity of the endothelial NO synthase located in the caveolae regulate the viscosity in this “shell”. High plasma sodium gelates the casing of the cell, whereas the casing is fluidized by high fructose. These communications between intracellular enzymes and extracellular ions happen in the plasma membrane barrier, whereas 90 percent of the cell mass remains uninvolved in such changes. Blockade of the ENaC using spironolactone (100%) or amiloride (84%) minimizes or prevent many of these vascular endothelial responses and boost NO. Nitric oxide release follows not vice versa and nanomechanics and decreases vascular endothelial cell stiffness which enhances circulation conducive vasodilation that is dependent. In the presence of HS-CRP that was increased and vascular inflammation, the effects of aldosterone on the ENaC is enhanced further raising vascular stiffness and BP. High sodium intake also abolishes the AT2R-mediated vasodilation immediately with complete abolition of endothelial vasodilation (EDV) within 30 d. Thus, it is now clear that high dietary sodium has adverse effects on the circulatory system, BP and CVD by changing the endothelial glycocalyx, which is a negatively charged biopolymer that lines the blood vessels and also serves as a protective barrier against sodium over-load, increased sodium permeability and sodium-induced TOD. Certain SNP’s of salt inducible kinaseIwhich alter Na+/K+ ATPase, determine LVH and sodium caused hypertension.
The sodium intake every day in patients must be between 1500. BP reduction improves in people on patients which are on treatment and the decrease in BP is additive with limitation of refined carbohydrates. Reducing sodium consumption may reduce damage to the brain, heart, kidney and vasculature through mechanisms dependent on the BP reduction that is little as well as those independent of the BP. A balance of sodium with nutrients, particularly calcium, magnesium and potassium is important, not just in reducing and controlling BP, but also in decreasing cerebrovascular and cardiovascular events. An increase in the sodium to potassium ratio is associated with risk of all-cause mortality and CVD. The Yanomamo Indians consume and excrete only 1 meq of sodium from 24 h and consume and excrete 152 meq of potassium in 24 h. BP doesn’t rise with age and is related to elevated PRA, although the Na + to K + percentage is 1/152. Currently 50 the BP in the Yanomamo is 100-108/64-69 mmHg.
In conclusion,�Cardiovascular disease and hypertension can often occur due to a variety of factors, however, an improper diet and nutrition has been appointed to be one of the most prevalent causes behind the onset of cardiovascular disease and hypertension. According to the above research studies, an imbalance in the intake of sodium can lead to cardiovascular disease and hypertension.� The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Cardiovascular disease,�also called heart disease, involves numerous issues,�including diseased vessels, structural problems, and blood clots. High blood pressure, or hypertension, occurs when your blood pressure increases to unhealthy levels. Your blood pressure measurement takes into account how quickly blood is passing through your veins and the amount of resistance the blood meets while it’s pumping.
What are the leading causes of cardiovascular disease and hypertension?
Oxidative stress, inflammation and autoimmune dysfunction initiate and propagate hypertension and cardiovascular disease.�In a series of research studies correlated to cardiovascular disease and hypertension, Dr. Mark C. Houston, MD, discussed the role that oxidative stress, inflammation and autoimmune dysfunction plays in relation to treatment of hypertension and cardiovascular disease.
Oxidative Stress
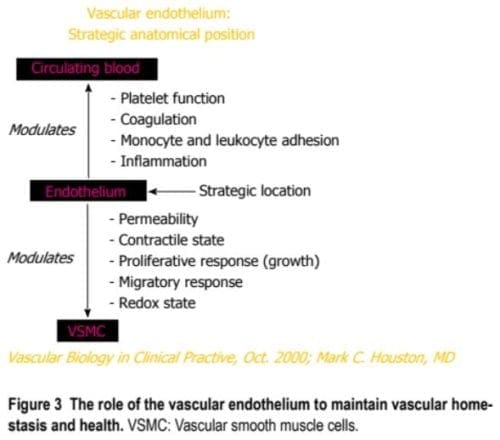
Oxidative stress, with an imbalance between the defense mechanisms and RNS as well as ROS, contributes to the etiology of hypertension in humans and animals. Radical oxygen species and RNS are generated by numerous mobile sources, such as nicotinamide adenine dinucleotide phosphate hydrase (NADPH) oxidase, mitochondria, xanthine oxidase, uncoupled endothelium-derived nitric oxide (NO) synthase (U-eNOS), cyclo-oxygenase and lipo-oxygenase. Superoxide anion is your predominant ROS species produced with these tissues, which inhibits NO and also leads to downstream production of additional ROS (As seen in Figure 3).
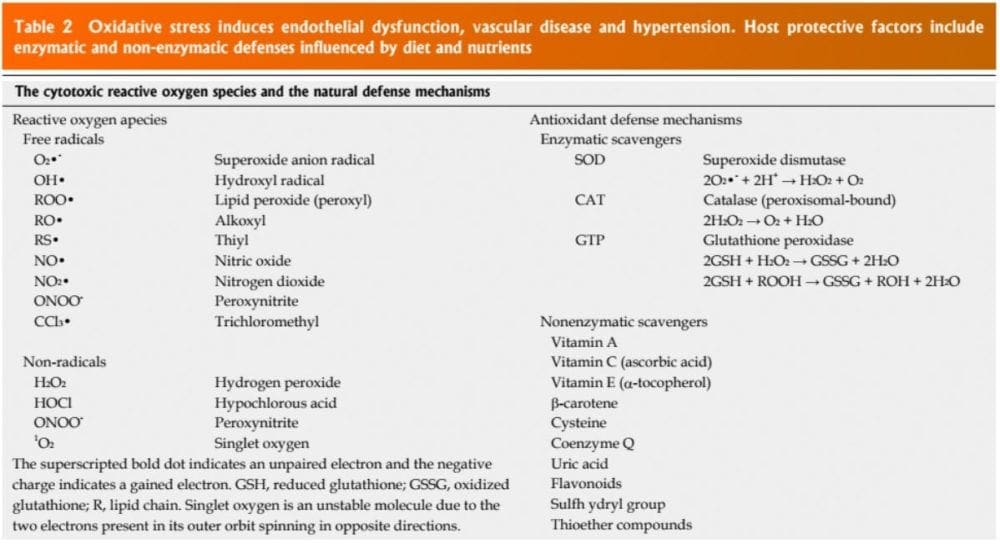
Patients have impaired an oxidative stress reaction to several stimuli, an elevated plasma oxidative stress and exogenous and endogenous antioxidant defense mechanisms. Hypertensive subjects also have lower plasma ferric reducing ability of plasma vitamin C levels and increased plasma 8-isoprostanes, which correlate with both diastolic and systolic BP. Different single-nucleotide polymorphisms (SNP’s) in genes that codify for antioxidant enzymes are directly linked to hypertension. These include NADPH oxidase, xanthine oxidase, superoxide dismutase 3 (SOD 3), catalase, glutathione peroxidase 1 (GPx 1) and thioredoxin. Antioxidant deficiency and excess free radical production have been implicated in human hypertension in several epidemiologic, observational and interventional studies (Table 2).
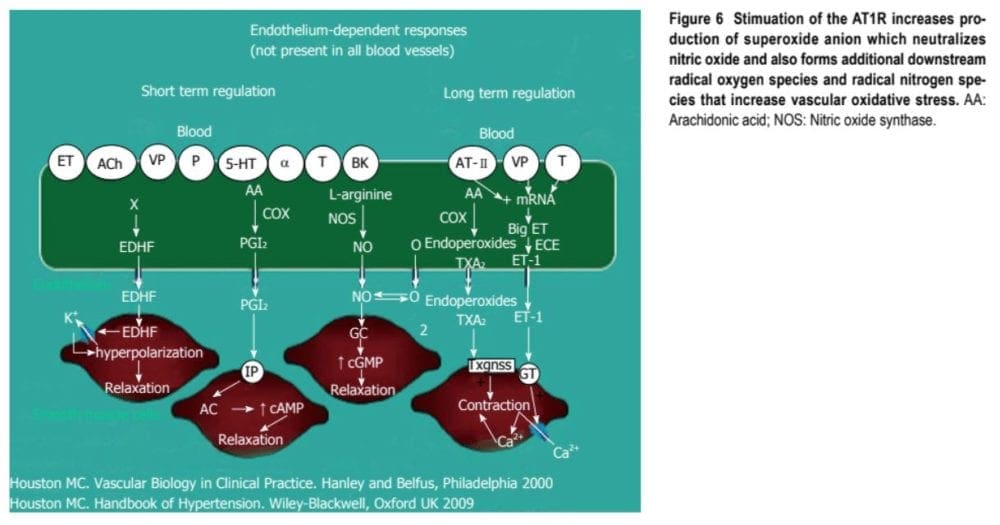
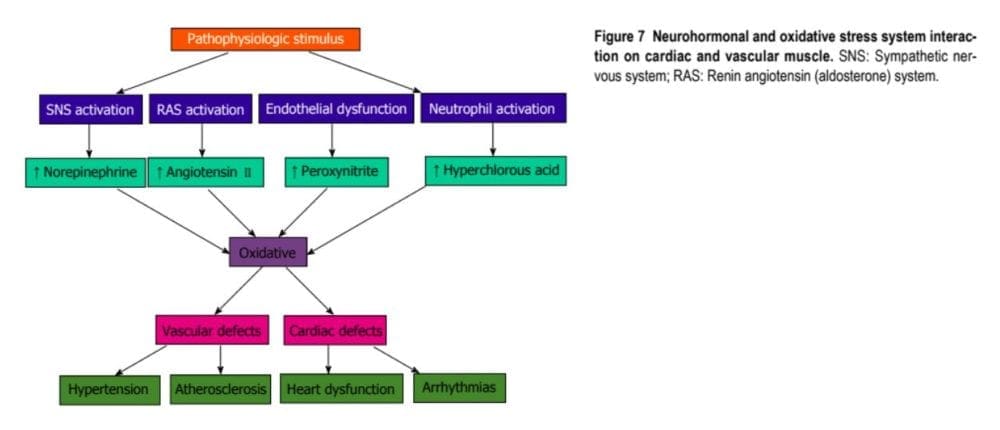
Radical oxygen species directly damage endothelial cells, degrade NO, influence eicosanoid metabolism, oxidize LDL, lipids, proteins, proteins, DNA and natural molecules, boost catecholamines, harm the genetic machinery, affect gene expression and transcription factors. The interrelations of systems, oxidative stress and cardiovascular disease are shown in Figures 6 and 7. The increased oxidative stress, inflammation and autoimmune vascular dysfunction in human hypertension results in a combination of an response to ROS and RNS increased generation of ROS and RNS and a decreased antioxidant reserve. Increased oxidative stress from the rostral ventrolateral medulla (RVLM) enhances glutamatergic excitatory inputs and attenuates GABA-ergic inhibitory inputs into the RVLM which contributes to increased sympathetic nervous system (SNS) activity from the paraventricular nucleus. Activation of this AT1R in the RVLM raises NADPH oxidase and increases oxidative stress and superoxide anion, increases SNS outflow causing an imbalance of SNS/PNS action with elevation of BP, increased heartbeat and alterations in heart rate variability and heart rate recovery time, which can be obstructed by AT1R blockers.
Inflammation
The link between hypertension and inflammation was suggested in both longitudinal and cross-sectional studies. Raised in high sensitivity C-reactive protein (HS-CRP) and other inflammatory cytokines such as interleukin-1B, (IL-1B), IL-6, tumor necrosis alpha (TNF-?) and chronic leukocytosis occur in hypertension and hypertensive-related TOD, such as increased carotid IMT. HS-CRP predicts CV events. Elevated HS-CRP is risk factor and a risk marker for hypertension and CVD. Increases in HS-CRP of over 3 ?g/mL can increase BP in only a couple of days that is directly proportional to the increase in HS-CRP. ENOS and nitric oxide are inhibited by HS-CRP. HS-CRP, down-regulates the AT2R, that counterbalances AT1R. Angiotensin II (A-II) upregulates many of those cytokines, notably IL-6, CAMs and chemokines by activating nuclear factor Kappa B (NF-?B) resulting in vasoconstriction. These events, as well as the increases in endothelin-1 and oxidative stress, elevate BP.
Autoimmune Dysfunction
Innate and adaptive immune responses are associated with hypertension and hypertension-induced CVD through at least three mechanisms: central nervous system stimulation cytokine generation and renal impairment. This includes salt-sensitive hypertension with dysregulation of both CD4+ and CD8+ lymphocytes increased inflammation because of T cell imbalance and chronic leukocytosis with increased neutrophils and lymphocytes that are decreased. Leukocytosis, especially neutrophils and decreased lymphocyte count raise BP in Blacks by. Macrophages and invade the wall, trigger TLRs, various subtypes govern BP and cause autoimmune vascular damage. Angiotensin II activates immune cells (T cells, macrophages and dendritic cells) and promotes cell infiltration into target organs. CD4+ T lymphocytes express AT1R and PPAR gamma receptors, and release TNF-?, interferon and interleukins inside the vascular wall when triggered (Figure 5). May play a role in the genesis of hypertension brought on by Angiotensin II. Patients have higher TLR 4 mRNA in monocytes in comparison to normal. Intensive decrease in BP to systolic BP (SBP) less than 130 mmHg vs SBP to just 140 mmHg reduces the TLR 4 longer. A-II activates the TLR expression resulting in inflammation and activation of the innate immune system. When TLR 4 is triggered there is downstream macrophage activation, increase metalloproteinase 9, migration, vascular remodeling, collagen accumulation in LVH the gut and cardiac fibrosis. The autonomic nervous system is essential in either increasing or decreasing inflammation and immune dysfunction. Efferent cholinergic pathways through the nerve innervate the spleen, nicotine acetylcholine receptor subunits and cytokine producing immune cells to BP and affect vasoconstriction. Nearby CNS inflammation or ischemia may mediate vascular hypertension and inflammation.
Aldosterone is correlated with increased adaptive immunity and autoimmune responses with CD4+ T cell activation and Th 17 polarization with improved IL 17, TGF-? and TNF-? which modulate over 30 inflammatory genes. Serum aldosterone is also an independent risk factor for CVD and CHD via non-hemodynamic effects as well as through increased BP. Blockade of receptors in brain, the heart, blood vessels and immune cells reduces CV danger even with the persistence of hypertension.
In conclusion, cardiovascular disease and hypertension have been associated with numerous issues, however, oxidative stress, inflammation and autoimmune dysfunction have been regarded as the most prevalent causes behind cardiovascular disease and hypertension.�Oxidative stress, defined as a disturbance in the balance between the production of reactive oxygen species (free radicals) and antioxidant defenses, inflammation and autoimmune dysfunction, occurs�when the body’s immune system attacks and destroys healthy body tissue by mistake. Cardiovascular disease and hypertension is an indication of cardiovascular issues which should be addressed by a healthcare professional.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine