Not getting enough fiber in one’s diet can lead to fiber deficiency. Fiber helps support gut and microbiome health. Individuals not getting enough fiber may experience irregular bowel movements, constipation, blood sugar fluctuations, not feeling full/satisfied after eating, or rising cholesterol levels. About 100 trillion microorganisms in the gut are integral to maintaining a healthy immune system. Fiber is the food these microorganisms eat that helps them to do their job. Without the proper amount, the immune system’s health may also be compromised.
Fiber and Gut Health
Fiber and gut health benefits include regulating the body’s sugars, helping to keep hunger and blood sugar in check, helping to maintain a healthy weight, its ability to prevent or relieve constipation, reduce the risk of diabetes, heart disease, and certain types of cancer.
Dietary fiber, or roughage, is the part of plant foods the body can’t digest or absorb.
It passes through the stomach, small intestine, and colon and out of the body.
It is found mainly in fruits, vegetables, whole grains, and legumes.
Soluble and insoluble forms are important to overall health.
Types
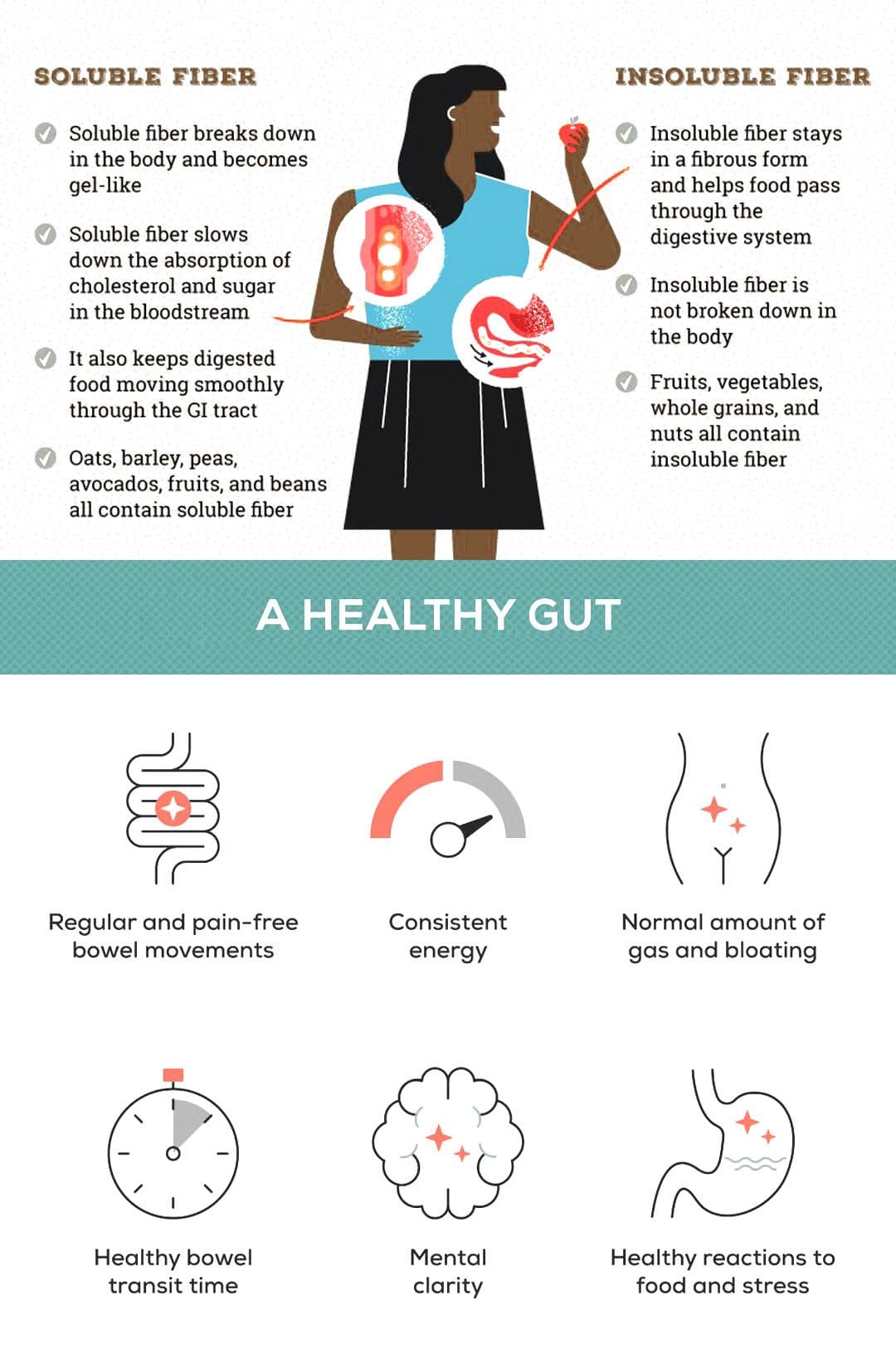
Soluble Fiber
This type dissolves in water to form a gel-like substance.
It can help lower blood cholesterol and glucose levels.
It is found in oats, peas, beans, apples, citrus fruits, carrots, and barley.
Insoluble Fiber
This type of fiber promotes the movement of material through the digestive system.
It increases stool bulk, benefiting individuals who struggle with constipation or irregular stools.
Whole-wheat flour, wheat bran, nuts, beans, and vegetables, such as cauliflower, green beans, and potatoes, are good sources.
Benefits
Healthy Bowel Movements
Dietary fiber increases stool weight and thickness and makes it soft.
Fiber helps to solidify the stool by absorbing water and adding bulk.
A thicker stool is easier to pass, decreasing the potential for constipation and other problems.
Maintains Bowel Health
A high-fiber diet can lower the risk of developing hemorrhoids and small pouches in the colon/diverticular disease.
Studies have also found that a high-fiber diet can help lower the risk of colorectal cancer.
Some fiber gets fermented in the colon.
Researchers are looking at how this can help prevent diseases of the colon.
Lowers Cholesterol
Soluble fiber found in beans, oats, flaxseed, and oat bran can help lower blood cholesterol levels by lowering low-density lipoprotein or unhealthy cholesterol levels.
Studies also have shown that high-fiber foods can help reduce blood pressure and inflammation.
Regulates Blood Sugar Levels
In individuals with diabetes, fiber, particularly soluble fiber, can slow the absorption of sugar and improve blood sugar levels.
A healthy nutrition plan that includes insoluble fiber can help reduce the risk of developing type 2 diabetes.
Helps Achieve Healthy Weight
High-fiber foods can be more filling than low-fiber foods, helping individuals eat less and stay satisfied.
High-fiber foods can also take longer to eat and are less energy dense, meaning they have fewer calories.
Getting More Fiber
Ideas for adding more fiber to meals and snacks:
Fiber to Start The Day
Choose a high-fiber breakfast cereal with five or more grams of fiber per serving.
Choose cereals with whole grain, bran, or fiber in the name.
Add a few tablespoons of unprocessed wheat bran to the cereal.
Add Whole Grains
Try to make at least half of the grains eaten whole grains.
Look for bread that lists whole wheat, whole-wheat flour, or another whole grain as the first ingredient, with at least 2 grams of dietary fiber per serving.
Experiment with whole-wheat pasta, brown rice, wild rice, barley, and bulgur wheat.
Baked Foods
Substitute whole-grain flour for half or all white flour when baking.
Add crushed bran cereal, unprocessed wheat bran, or uncooked oatmeal to muffins, cakes, and cookies.
Legumes
Beans, peas, and lentils are recommended sources.
Add kidney beans to soups or salads.
Make nachos with refried black beans, fresh vegetables, whole-wheat tortilla chips, and healthy salsa.
Fruit and Vegetables
Fruits and vegetables are rich in fiber and vitamins and minerals.
Try to eat a favorite fruit daily.
Healthy Snacks
Fresh fruits, raw vegetables, low-fat popcorn, and whole-grain crackers are healthy choices.
Try for a handful of nuts or dried fruits; however, be aware that nuts and dried fruits can be high in calories.
Moderation
High-fiber foods are beneficial for the body’s health.
Adding too much fiber can promote intestinal gas, abdominal bloating, and cramping.
Increase fiber gradually over a few weeks.
This allows the natural bacteria in the digestive system to make adjustments.
Maintain hydration, as fiber works best when it absorbs water.
Individuals not sure how to incorporate more fiber can consult a nutritionist and health coach to help begin the process.
Gut Dysfunction
References
Anderson, James W et al. “Health benefits of dietary fiber.” Nutrition Reviews vol. 67,4 (2009): 188-205. doi:10.1111/j.1753-4887.2009.00189.x
Cronin, Peter, et al. “Dietary Fiber Modulates the Gut Microbiota.” Nutrients vol. 13,5 1655. 13 May. 2021, doi:10.3390/nu13051655
Fuller, Stacey, et al. “New Horizons for the Study of Dietary Fiber and Health: A Review.” Plant foods for human nutrition (Dordrecht, Netherlands) vol. 71,1 (2016): 1-12. doi:10.1007/s11130-016-0529-6
Gill, Samantha K et al. “Dietary fiber in gastrointestinal health and disease.” Nature reviews. Gastroenterology & hepatology vol. 18,2 (2021): 101-116. doi:10.1038/s41575-020-00375-4
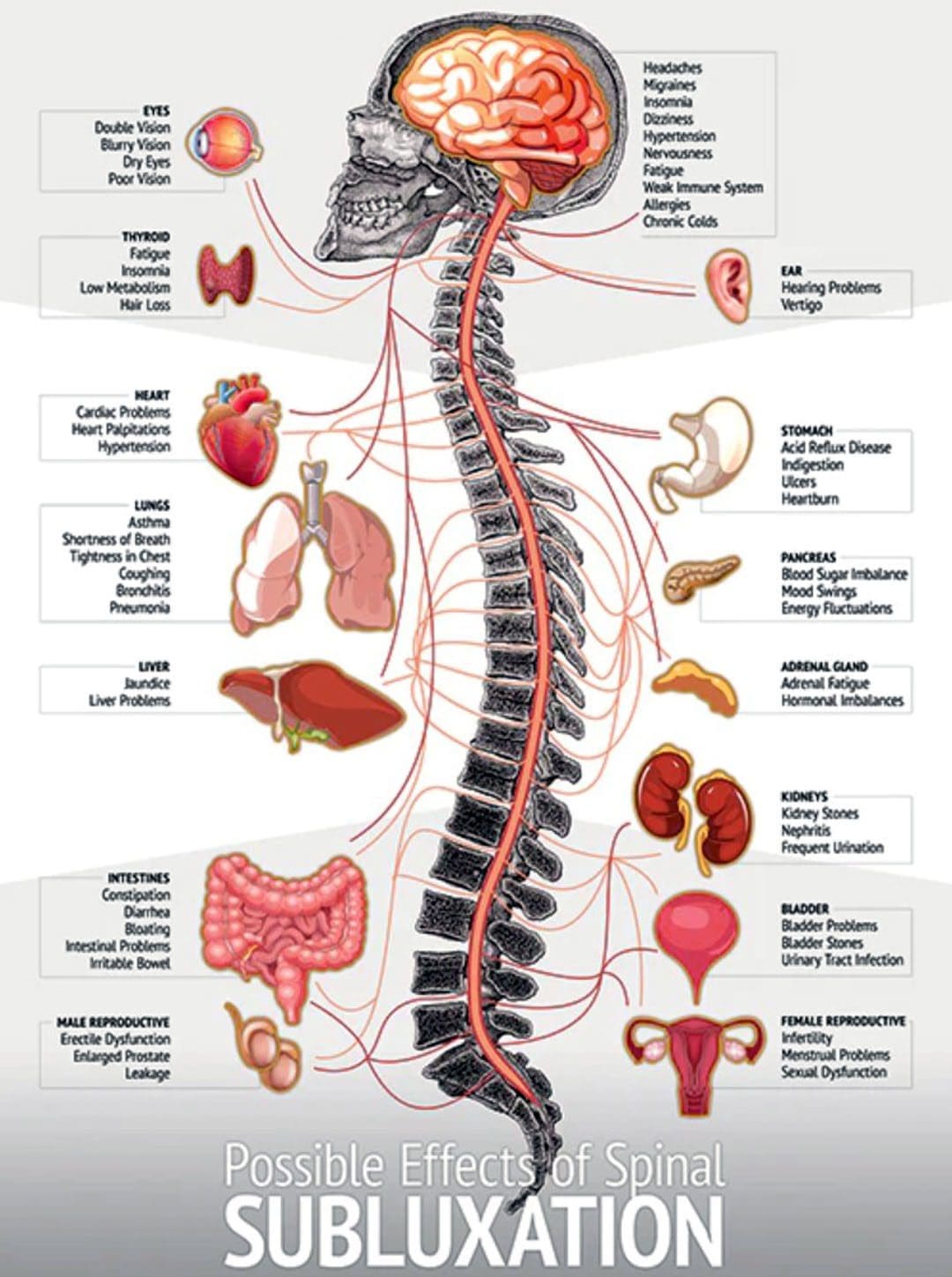
Body misalignment can cause various symptoms to be experienced, ranging from headaches, neck and back pain, sore feet, discomfort in the joints, muscles, or nerves, and digestive problems. Improperly aligned vertebrae can press against nerves, pinching or compressing them, causing the nerve signals of the digestive system, including those in the stomach and intestines, to misfire or fail to transmit at the appropriate moment. This can cause the organs to malfunction, resulting in heartburn, gas, constipation, cramping, diarrhea, and other symptoms. Chiropractic realignment adjustments are an effective treatment option for frequent stomachaches, reflux, constipation, and other gastrointestinal conditions.
Body Misalignment Digestive Problems
There are over a million nerve cells within the digestive system. A collection of nerves branch out from the lower part of the spinal cord and travels to the stomach and intestines. Nerve transmission plays an essential role in the following:
Digestion.
Movement of food through the gastrointestinal system.
Absorption of nutrients and minerals.
Removal of waste products.
Misalignments of the vertebrae are known as subluxations. Pressure on nerve roots caused by misalignment can interfere with the function of the bowel and other organs, which can lead to gastrointestinal issues. Muscle tension in the abdomen can also contribute to digestive problems, whether because of stress or sitting for long hours daily.
Misalignment Symptoms
When the body is out of alignment, symptoms of discomfort begin to appear. The most common include:
Fatigue.
Stiff neck.
Sore shoulders.
Chronic headaches.
Sore muscles.
Pain throughout the back.
Joint pain throughout the body.
Chronic aches.
Tight hips.
Difficulty walking.
Tingling, pins and needles, and numbness nerve sensations – sciatica.
Constantly getting sick.
Healthy Gut
A balanced healthy gut will have less difficulty processing food and eliminating waste, leading to reduced and eventually alleviated symptoms. The following show healthy gut function:
Regular, consistent energy levels.
Increased mental clarity.
Regular and healthy bowel movements.
No pain or discomfort symptoms.
A normal amount of gas and bloating.
Healthy stress levels.
Chiropractic
Chiropractic care will realign the body to its proper form, improving gastrointestinal issues. The chiropractic team will use various tools and techniques to guide and correct any subluxations, relax the muscles, and increase nerve and blood circulation.
Healthy Diet and Chiropractic
References
Ernst, Edzard. “Chiropractic treatment for gastrointestinal problems: a systematic review of clinical trials.” Canadian Journal of Gastroenterology = Journal canadien de Gastroenterologie vol. 25,1 (2011): 39-40. doi:10.1155/2011/910469
Hills, Ronald D Jr, et al. “Gut Microbiome: Profound Implications for Diet and Disease.” Nutrients vol. 11,7 1613. 16 Jul. 2019, doi:10.3390/nu11071613
Hornbuckle, William E., et al. “Gastrointestinal Function.” Clinical Biochemistry of Domestic Animals (2008): 413–457. doi:10.1016/B978-0-12-370491-7.00014-3
Leeming, Emily R et al. “Effect of Diet on the Gut Microbiota: Rethinking Intervention Duration.” Nutrients vol. 11,12 2862. 22 Nov. 2019, doi:10.3390/nu11122862
Li, Yuanyuan, et al. “The Role of Microbiome in Insomnia, Circadian Disturbance, and Depression.” Frontiers in psychiatry vol. 9 669. 5 Dec. 2018, doi:10.3389/fpsyt.2018.00669
Redwood, Daniel. “Chiropractic and visceral disorders.” Journal of Alternative and complementary medicine (New York, N.Y.) vol. 13,5 (2007): 479-80. doi:10.1089/acm.2007.7146
Valdes, Ana M et al. “Role of the gut microbiota in nutrition and health.” BMJ (Clinical research ed.) vol. 361 k2179. 13 Jun. 2018, doi:10.1136/bmj.k2179
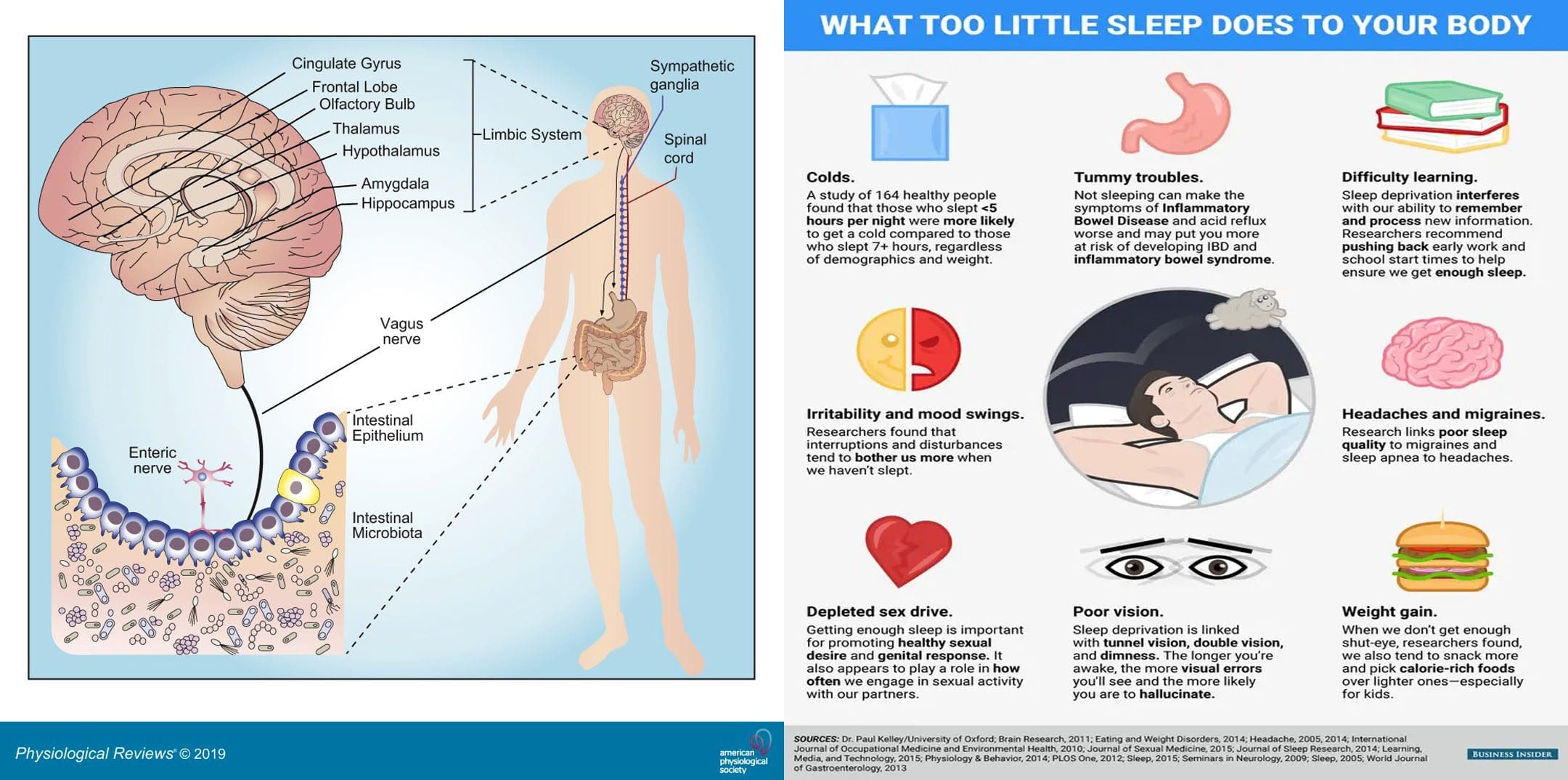
Viruses, bacteria, fungi, and protozoa are the microorganisms that naturally live in the digestive tract. Sleep affects gut health and vice versa. A healthy gut microbiota consists of all kinds of microorganisms that produce thousands of compounds and coexist harmoniously. A healthy diet and lifestyle are the biggest factors influencing bacteria variety, and maintaining a varied diet preserves microbiota diversity. Everybody’s gut microbiome is different; the more diverse the gut microbiome, the healthier sleep will be. The Injury Medical Chiropractic and Functional Medicine Clinic Team can develop a personalized nutritional plan to improve gut health and sleep patterns.
Sleep Affects Gut Health
Not having a diverse gut microbiome has been linked to autoimmune diseases, Parkinson’s disease, and mental health issues like anxiety and depression. Not getting healthy sleep is associated with many diseases and disorders, including:
Gastrointestinal disorders
Infections
Diabetes
Cardiovascular disease
Neurological disorders
Anxiety
Depression
Cancer
Changes in sleep patterns influence the central nervous system and the immune system, which affect different organ systems. For example, studies have shown some gastrointestinal disorders, like irritable bowel syndrome – IBS could be associated with increased REM sleep or the fourth part of the sleep cycle when vivid dreaming occurs. In Crohn’s disease or ulcerative colitis, long-term immune response activation can result in poor sleep, insufficient quality sleep, or other sleep problems. The deepest stages of sleep are when the brain and gut communicate to repair the body, restore nutrients, and remove and release toxins.
Sleep Cycle
During sleep, the immune system produces proteins called cytokines that perform functions during the inflammatory response, either by increasing or blocking inflammation, depending on the body’s needs. Cytokines help promote sleep, fight infection, or stop inflammation in chronic inflammatory diseases like Crohn’s disease or ulcerative colitis.
Insufficient sleep significantly alters cytokine production, and infection-fighting cells decrease in numbers when sleep deprived, making it harder for the body to fight infections and lessening protection. This increases the inflammatory response and keeps the immune system on.
Chronic or long-term immune response activation can result in sleep disturbances or disorders.
Some disorders include small intestinal bacterial overgrowth and inflammation caused by microbiome abnormalities or dysbiosis.
The gut barrier function begins to malfunction, leading to bacteria and pathogens leaking into blood circulation/leaky gut, triggering immune responses.
Ways to Improve Sleep
One of the main ways to improve sleep quality and gut microbiome health is to practice healthy sleep hygiene. According to the National Sleep Foundation, individuals should:
Nap Smart
Naps can be a great way to refresh the mind and body and replenish energy levels during the day.
The bright lights from phones and screens can make it difficult to fall asleep fully.
Use an alarm clock with a soft night light and keep the bedroom tech-free.
Create Sleep Routine
Take a warm shower, read a book, or do light stretches.
Create a wind-down routine to relax before bed to signal the body that it’s time for sleep.
Avoid Caffeine and Alcohol Before Bed
These substances make it harder for the mind and body to fall or stay asleep.
Food As Medicine
References
Chabé, Magali et al. “Gut Protozoa: Friends or Foes of the Human Gut Microbiota?.” Trends in parasitology vol. 33,12 (2017): 925-934. doi:10.1016/j.pt.2017.08.005
Deng, Feilong, et al. “The gut microbiome of healthy long-living people.” Aging vol. 11,2 (2019): 289-290. doi:10.18632/aging.101771
Gut Bacteria Research: Physicians’ Committee for Responsible Medicine. (2019). “Gut Bacteria: Optimize Gut Health With a Plant-Based Diet,”
Ianiro, Gianluca, et al. “How the gut parasitome affects human health.” Therapeutic advances in gastroenterology vol. 15 17562848221091524. 30 Apr. 2022, doi:10.1177/17562848221091524
Lozupone, Catherine A et al. “Diversity, stability and resilience of the human gut microbiota.” Nature vol. 489,7415 (2012): 220-30. doi:10.1038/nature11550
Sleep and Gut Microbiome Study: PLoS One. (2019). “Gut microbiome diversity is associated with sleep physiology in humans.
Sleep Hygiene Information: National Sleep Foundation. (2019). “Sleep Hygiene.”
Vaishnavi, C. “Translocation of gut flora and its role in sepsis.” Indian journal of medical microbiology vol. 31,4 (2013): 334-42. doi:10.4103/0255-0857.118870
Digestive disorders affect millions of individuals and cover a variety of diseases ranging from mild to severe. These conditions involve the digestive tract, also known as the gastrointestinal or GI tract. The digestive disorders of heartburn, acid reflux, and gastroesophageal reflux disease/GERD are related and have similar symptoms but are different. Accurately diagnosing digestive disorders involves a thorough medical history, imaging and lab tests, and physical examination to develop the proper treatment plan.
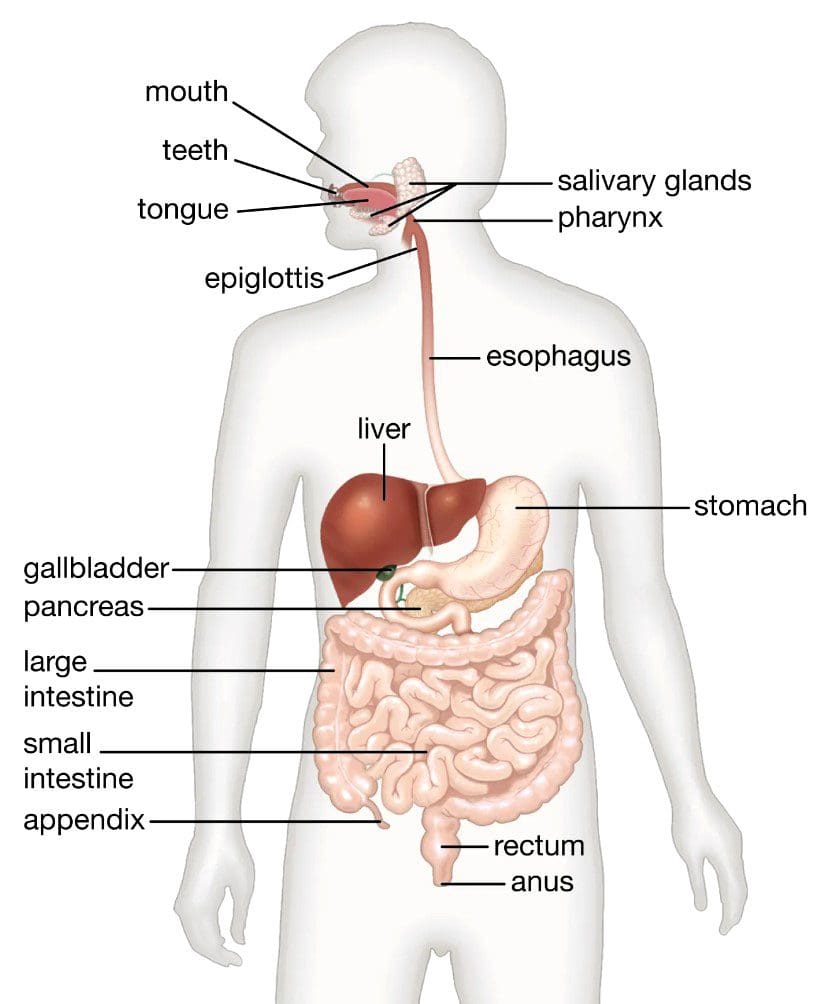
Digestive Disorders
The gastrointestinal tract includes the esophagus, liver, gallbladder, stomach, pancreas, and large and small intestines.
Heartburn
Heartburn has nothing to do with the heart but describes a burning sensation in the chest. Individuals experience heartburn when stomach acid flows back into the esophagus. Occasional heartburn after eating spicy foods or foods an individual is not used to is common and is no cause for alarm. Most can manage the discomfort symptoms with lifestyle adjustments and over-the-counter medications. Chronic heartburn that interferes with daily/nightly routines could indicate a more serious condition requiring medical care. Symptoms include:
The burning discomfort sensations in the stomach and chest regions are usually worse after eating a meal, bending down, at night, and when lying down.
A bitter or acidic taste.
Acid Reflux
The esophagus comprises mainly smooth muscle that extends from the throat down through the chest cavity and past the abdomen, where it connects with the stomach. When swallowing, the esophagus opens and squeezes food down to the bottom, where a valve (lower esophageal sphincter LES) separates it from the stomach. The valve is normally closed. When swallowing, it opens so that food can pass through and then closes up. Acid reflux is a disorder that causes the valve to open when it’s not supposed to. This allows stomach contents like acid, digestive juices, enzymes, and food to flow backward from the stomach into the esophagus, causing heartburn symptoms. This usually happens when the lower esophageal sphincter is under added pressure, weakened, or malfunctioning. Symptoms can be caused by:
Overeating.
Eating spicy or acidic foods that can trigger symptoms.
Eating right before going to bed.
Medications.
Over alcohol consumption.
Exercising after eating.
Pregnancy.
Smoking.
Acid reflux and heartburn affect everyone, but most can handle the discomfort by taking antacids and avoiding the foods that brought it on. Occasional acid reflux can be treated with over-the-counter medication, including:
Acid reflux can potentially progress to gastroesophageal reflux disease, a more serious form of acid reflux that lasts longer. GERD is frequent heartburn that happens two or more times a week. Other signs and symptoms can include:
Some individuals with digestive disorders may need more extensive diagnostic evaluations, including GI endoscopy, laboratory tests, and imaging.
Chiropractic Treatment
Body misalignments, unhealthy posture, and restrictive positions can contribute to digestive disorders that put pressure on the stomach and chest, triggering symptoms. A chiropractor can realign the body and take the stress off the joints and spine, relieving the pressure on the nerves. They can also strengthen the muscles through adjustments that help alleviate pressure on the stomach. A chiropractor designs a treatment plan that suits the individual’s needs, including stretches and exercises, nutrition, and health coaching to achieve and manage a healthy weight.
Chiropractic Precision
References
Carvalho de Miranda Chaves, Renata, et al. “Respiratory physiotherapy can increase lower esophageal sphincter pressure in GERD patients.” Respiratory medicine vol. 106,12 (2012): 1794-9. doi:10.1016/j.rmed.2012.08.023
Harding, Susan M. “Acid reflux and asthma.” Current opinion in pulmonary medicine vol. 9,1 (2003): 42-5. doi:10.1097/00063198-200301000-00007
Kahrilas, Peter J. “Regurgitation in patients with gastroesophageal reflux disease.” Gastroenterology & hepatology vol. 9,1 (2013): 37-9.
Pope, C E 2nd. “Acid-reflux disorders.” The New England journal of medicine vol. 331,10 (1994): 656-60. doi:10.1056/NEJM199409083311007
Dr. Jimenez, D.C., presents how chronic metabolic connections like inflammation and insulin resistance are causing a chain reaction in the body in this 2-part series. Many factors often play a role in our health and wellness. In today’s presentation, we will continue on how these chronic metabolic diseases affect the vital organs and organ systems. It can lead to overlapping risk factors associated with pain-like symptoms in the muscles, joints, and vital organs. Part 1 examined how overlapping risk profiles like insulin resistance and inflammation affect the body and cause muscle and joints pain-like symptoms. We mention our patients to certified medical providers that provide available therapy treatments for individuals suffering from chronic conditions associated with metabolic connections. We encourage each patient when it is appropriate by referring them to associated medical providers based on their diagnosis or needs. We understand and accept that education is a marvelous way when asking our providers’ crucial questions at the patient’s request and acknowledgment. Dr. Alex Jimenez, D.C., uses this information as an educational service. Disclaimer
How The Liver Associated With Metabolic Diseases
So we can look to the liver to find earlier cues of cardiovascular risk. How can we do that? Well, let’s understand some liver biochemistry. So in a healthy liver cell hepatocyte, when you have increased insulin being secreted because there was a meal that required glucose to be absorbed, what you expect if the insulin receptor works is that the glucose would go in. Then the glucose would get oxidized and turned into energy. But here’s the problem. When the hepatocyte has insulin receptors that don’t work, you’ve got that insulin on the outside, and the glucose never made it in. But what also happens on the inside of the hepatocyte is it was assumed that the glucose was going to get in. So what it does is it turns off fatty acid oxidation, thinking, “Guys, we don’t need to burn our fatty acids. We’ve got some glucose coming in.”
So when the glucose is not there, and you’re not burning off fatty acids, very common for people to feel fatigued because nothing is burning for energy. But here is the secondary sequela; where are all those fatty acids going, right? Well, the liver may try to repackage them as triglycerides. Sometimes, they stay in the hepatocyte or get shifted out of the liver into the bloodstream as VLDL or very low-density lipoprotein. You might see it as a high triglyceride shift in a standard lipid panel. So, when all of us are talking about getting a triglyceride level to around 70 as your 8+ goal, when I start seeing triglycerides rising, we wait until they’re 150, even though that’s the cutoff for our labs. When we see it at 150, we know they are shunting triglycerides out of the liver.
So that will happen many times before we find impaired fasting glucose. So look at your triglycerides, fasting triglycerides, as an emerging or early biomarker of insulin dysfunction. So this is another diagram that says that if the triglycerides are being created because the fatty acids are being oxidized, they can stay in the liver. Then that makes steatosis or the fatty liver, or they can be pushed out, and they turn into lipoproteins. We’re going to talk about that in just a second. The body is like, “What are we going to do with these fatty acids?” We can’t try to shove them into places because nobody wants them. To that point, the liver is like, “I don’t want them, but I will keep some with me.” Or the liver would have these fatty acids transported and stuck to the blood vessel walls.
And then the blood vessels and arteries are like, “Well, I don’t want them; I’ll put them underneath my endothelium.” And so that’s how you get atherogenesis. The muscles are like, “I don’t want them, but I’ll take some.” That’s how you get the fatty streaks in your muscles. So when the liver is getting bogged down with steatosis, inflammation occurs in the body and produces this feed-forward cycle inside the hepatocyte, damaging the liver. You’re getting cellular death; you’re getting fibrosis, which is just an extension of what happens when we don’t address the core issues for fatty liver: inflammation and insulin resistance. So, we look for subtle rises in AST, ALT, and GGT; remember that it is a liver-based enzyme.
Hormone Enzymes & Inflammation
GGT enzymes in the liver are smoke detectors and tell us how much oxidative stress is going on. Will we look at HSCRP and APOB to see the output of this liver? Is it starting to dump excess fatty acids through VLDL, APOB, or triglycerides? And how it picks that is just genetics, honestly. So I look for liver markers to tell me what’s going on in the liver as a sign of what’s happening everywhere. Because that might be the genetic weak spot of the person, some people are genetically vulnerable just in terms of their lipid profiles. To that point, we can look for something called metabolic dyslipidemia. You know this as high triglycerides and low HDL. You can specifically look for a ratio; an optimal balance is three and lower. It starts going from three to five and then five to eight, like eight is almost pathognomonic of insulin resistance. You’re just reaching becoming more and more insulin resistant.
As the number increases for that trig over HDL ratio, that is a simple, easy way to screen for insulin resistance. Now some people look 3.0 on this but still have insulin resistance. So there are other tests you do. This is a way to find those who show insulin resistance through lipids. And remember, everybody is different. Women with PCOS could have amazing lipids but could express an increase or decrease of hormones associated with insulin, estrogen, and inflammation. So look for something other than one test or ratio to indicate whether they’ve got it. You’re looking to see what could be the place where we will find the clue.
So let’s use the word healthy. A healthy person has VLDL that looks to be a healthy normal size in their bodies, and they have normal LDL and HDL. But now look at what happens when you get insulin resistance. These VLDL ls start to pump up with triglycerides. That’s why they’re fattening up. It’s lipotoxicity. So if you start looking at the VLDL three numbers in a lipoprotein profile, you’ll see that that number is creeping up, and there are more of them, and their size is bigger. Now with LDL, what happens is that the cholesterol amount within the top and the bottom is the same. If I pop all these water balloons, it’s the same amount of LDL cholesterol. However, that amount of LDL cholesterol in insulin resistance is repackaged in small dense LDL.
How Does Functional Medicine Play Its Part?
Now we understand that there may be some of you who cannot or do not have access to this testing, or your patients cannot afford it, and that’s why we answered the questions and looked for other clues of insulin resistance and treat the root cause that is affecting the body. Look for signs of inflammation and other overlapping profiles of insulin resistance. The particle number is higher when they’re insulin resistance. So cholesterol is the same, whereas the particle number is more elevated, and small dense LDL is more atherogenic. Treat it because whether or not you have access to knowing the LDL particle, there should be something in your head that says, “Man, even though this person’s LDL cholesterol looks good, they have tons of inflammation and insulin resistance; I can’t be sure that they don’t have higher particle number.” You might assume that they do this just to be safe.
The other thing that happens in insulin resistance is that the HDL or the healthy cholesterol tends to become small. So that’s not very good because the efflux capacity of HDL is lessened when it’s smaller. So we like the larger HDL, if you will. Access to these tests would give you a solid indication of what’s going on with your patient from a cardiometabolic perspective.
When it comes to these tests, it is important to utilize them to determine the patient’s timeline when they have inflammation or insulin resistance in their bodies, affecting their quality of life. However, many people would often express that these tests are expensive and would go with the gold standard of testing for affordability and be able to decide if it is worth it to better their health and wellness.
Look For Cardiometabolic Risk Patterns
So when it comes to cardiometabolic risk factor patterns, we look at the insulin aspect and how it correlates with mitochondrial dysfunction associated with insulin resistance and inflammation. A research article mentions how two mitochondrial dysfunctions can affect the body. Okay, let’s talk about the first issue, which is the quantity issue. One could be endotoxins that we encounter in our environment, or two; it can be genetically passed along from generation to generation. So the two types could indicate that you don’t have enough mitochondria. So that’s a quantity issue. The other problem is it’s a quality issue. You got plenty of them; they don’t work well, so they don’t have high output or at least normal results. Now how does this play out in the body? So out in the periphery, your muscles, adipocytes, and liver, you have mitochondria in those cells, and it’s their job to energize that lock and jiggle. So if your mitochondria are in the right number, you’ve got plenty to energize the insulin cascade lock and jiggle.
Interesting, right? So here it is in summary, if you don’t have enough mitochondria, which is the problem in the periphery, you get insulin resistance because the lock and jiggle aren’t working well. But if you do not have the mitochondria working well in the pancreas, especially in the beta cell, you don’t secrete insulin. So you still get hyperglycemia; you don’t have high insulin state. When this happens, we know your brain should be hurting, but hopefully, it will come together slowly.
Another article mentions that it connects mitochondrial dysfunction with type two diabetes, and poor maternal nutrition can prime it. This one talks about how fatty liver is associated with lipotoxicity, right? That’s that increased fatty acid, and oxidative stress, which, remember, is the byproduct of inflammation. ATP depletion and mitochondrial dysfunction. When this happens, it can affect the liver, which then turns into the fatty liver, and can also be associated with gut dysfunction, which leads to chronic inflammation, elevated insulin resistance, mitochondrial dysfunction, and many more. These chronic metabolic diseases are connected, and there are ways to reduce these symptoms from affecting the body.
Conclusion
When having a conversation with their doctors, many patients know that the same drivers affect a whole host of other phenotypes, all commonly rooted in inflammation, insulin, and toxicity. So when many people realize these factors are the root cause, doctors will work with many associated medical providers to develop personalized functional treatment plans. So remember, you always have to use the timeline and the matrix to kind of help you know where do you start with this patient, and for some people, it might be you’re just going to tweak a little bit of lifestyle because all they’re working on is changing their body count. So it’s one of the blessings of functional medicine that we were able to turn off the inflammation in the gut, which helps reduce the toxic impact burdening the liver. It also allows the individual to find out what works or doesn’t work with their bodies and take these small steps to improve their health.
We hope you have fresh eyes about inflammation, insulin, and toxicity and how it is at the root of so many conditions that your patients are facing. And how through very simple and effective lifestyle and nutraceutical interventions, you can change that signaling and change the course of their symptoms today and the risks they have tomorrow.
Dr. Alex Jimenez, D.C., presents how metabolic connections are causing a chain reaction to major chronic diseases in this 2-part series. Many factors often play a role in our health and wellness. It can lead to overlapping risk factors associated with pain-like symptoms in the muscles, joints, and vital organs. Part 2 will continue the presentation on metabolic connections with major chronic diseases. We mention our patients to certified medical providers that provide available therapy treatments for individuals suffering from chronic conditions associated with metabolic connections. We encourage each patient when it is appropriate by referring them to associated medical providers based on their diagnosis or needs. We understand and accept that education is a marvelous way when asking our providers’ crucial questions at the patient’s request and acknowledgment. Dr. Jimenez, D.C., makes use of this information as an educational service. Disclaimer
How Inflammation Affects The Body
Dr. Alex Jimenez, D.C., presents: So here you have a lean set of adipocytes on the left, and then as they start to plump up with more cellular weight, you can see those macrophages, the green boogies come around looking, saying, “Hey, what’s going on here? It doesn’t look right.” So they are investigating, and this causes local cell death; it’s just a part of the inflammatory cascade. So there is also another mechanism happening here. Those adipocytes are not just getting plumper by accident; it’s often related to a calorie surfette. So this nutrient overload damages the endoplasmic reticulum, leading to more inflammation. What these cells and the adipocytes are trying to do is protect themselves from glucose and lipo toxicity.
And the whole cell, the adipocyte cell, is creating these caps that are trying to say, “Please stop, we can’t take any more glucose, we can’t take any more lipids.” It’s a protection mechanism known as insulin resistance. It’s not just some random thing happening. It is the body’s way of trying to prevent glucose and lipotoxicity. Now that the inflammation alarm is occurring more than just in the adipocytes, it’s getting systemic. Other tissues and organs are starting to feel the same burden of the calorie surfette, causing inflammation and cell death. So glucose and lipotoxicity look like fatty liver when dealing with the liver. And you can also have it just like fatty liver progresses to cirrhosis with hepatocyte death. The same mechanism that’s happening in muscle cells. So our skeletal muscle cells specifically see cell death after inflammation and see fatty deposition.
The best way to think about it is, for example, the cows raised for food consumption and how they have marbled. So that’s the fatty deposition. And in humans, you can think about how people become sarcopenic as they become more and more insulin resistant. It’s the same phenomenon when body tissue tries to protect itself from glucolipotoxicity, causing a local inflammatory response. It becomes an endocrine response when it starts targeting other tissues in the periphery, whether the liver, muscle, bone, or brain; it’s just whatever is happening; they’re in the visceral adipocytes that can occur in other tissues. So that’s your paracrine effect. And then it can go viral, if you will.
Inflammation Associated With Insulin Resistance
Dr. Alex Jimenez, D.C., presents: You’re getting this local and systemic pro-inflammatory response coupled with insulin resistance, returning to this protection mechanism against glucose and lipotoxicity. Here you see how the blood vessels in our arteries get caught in the loop of fatty deposition and cell death. So you’ll see leaky blood vessels and fatty deposits, and you’ll see damage and pro-atherogenesis. Now, this is something we explained in AFMCP for the cardiometabolic module. And that is the physiology behind the insulin receptor. This is known as the lock and jiggle technique. So you have to have insulin lock into the insulin receptor up at the top., which is known as the lock.
And then there’s a phosphorylation cascade called the jiggle that then creates this cascade that ultimately causes the glucose-4 channels to open up the glucose-4 receptors to go into the cell so that it can be then the glucose, which is then utilized for energy production by the mitochondria. Of course, insulin resistance is where that receptor isn’t sticky or as responsive. And so not only do you fail to get glucose into the cell for energy production, but you are also rendering a hyper insulin state in the periphery. So you get hyperinsulinemia as well as hyperglycemia in this mechanism. So what can we do about that? Well, many nutrients have been shown to improve the lock and jiggle things that can improve the glucose-4 transporters coming up towards the periphery.
Anti-Inflammatory Supplements Reduce Inflammation
Dr. Alex Jimenez, D.C., presents: You see these listed here: vanadium, chromium, cinnamon alpha lipoic acid, biotin, and another relatively new player, berberine. Berberine is a botanical that can dampen all primary pro-inflammatory signals. So what precedes these comorbidities often and it’s insulin dysfunction. Well, what precedes insulin dysfunction many times? Inflammation or toxicity. So if berberine is helping the primary inflammation issue, it will address the downstream insulin resistance and all the comorbidities that can happen. So consider berberine as your option. So again, this shows you that if you can reduce inflammation up here at the top, you can minimize many cascade effects downstream. Berberine specifically seems to act in the microbiome layer. It modulates the gut microbiota. It may create some immune tolerance, therefore not rendering as much inflammation.
So consider berberine as one of the tools you can use to support insulin dysfunction and insulin resistance-related comorbidities. Berberine seems to increase insulin receptor expression, so the lock and jiggle work more effectively and improve the cascade with the glucose-4 transporters. That’s one mechanism by which you can start to find the root cause of many of the conditions we discussed when you see paracrine and endocrine glucose toxicity, lipotoxicity organ damage. Now another mechanism for you to consider is leveraging NF kappa B. So the goal is to keep NF kappa B grounded because as long as they don’t translocate, a host of inflammation signals do not get triggered.
So our goal is to keep NF kappa B grounded. How can we do that? Well, we can use NF kappa B inhibitors. So in this presentation of treatment options for any comorbidities related to insulin dysfunction, there are many ways to reduce these overlapping conditions affecting our bodies. So you can directly affect insulin resistance through anti-inflammatory supplements or indirectly help insulin resistance or insulin dysfunction by leveraging things against inflammation. Cause if you remember, insulin dysfunction is what then causes all those comorbidities. But what causes insulin dysfunction is generally inflammation or toxins. So our goal is to address pro-inflammatory things. Because if we can address pro-inflammatory things and nip the insulin dysfunction in the bud, we can prevent all the downstream organ damage or organ dysfunction.
Reducing Inflammation In The Body
Dr. Alex Jimenez, D.C., presents: Let’s move on to the next section that you can leverage or reduce the inflammation and insulin soup damage if you will, that the genes bathe in the body. This is the one you’ll often hear in our presentation, and that’s because, actually, in functional medicine, we help fix the gut. That’s usually where you need to go. And this is the pathophysiology for why we do that in cardiometabolic medicine. So if you have that poor or sad diet, that modern western diet with bad fats, it will directly damage your microbiome. That change in the microbiome can render increased intestinal permeability. And now lipopolysaccharides can translocate or leak into the bloodstream. To that point, the immune system says, “Oh no way, buddy. You’re not supposed to be in here.” You’ve got these endotoxins in there, and now there is a local and systemic inflammatory response that inflammation will drive the insulin dysfunction, which will cause the metabolic disorders that come after that.
Whatever the person’s genetically prone to, it gets clicked on epigenetically. So remember, if you can quell the inflammation in the microbiome, meaning create this tolerant and strong microbiome, you can reduce the inflammatory tone of the entire body. And when you reduce that, it’s been shown that it sets the insulin sensitivity. So the lower the inflammation, the higher the insulin sensitivity related to the microbiome. So surprise, it’s been shown that probiotics are associated with improved insulin sensitivity. So the right probiotics will create immune tolerance. Microbiome strength and modulation occur with probiotics. And so insulin sensitivity is preserved or regained based on where you are. So please consider that as another indirect mechanism or treatment option for leveraging cardiometabolic health for patients.
Probiotics
Dr. Alex Jimenez, D.C., presents: So when it comes to probiotics, we will use them in someone who might also concurrently have irritable bowel syndrome or food allergies. We might pick probiotics over NF kappa B inhibitors if they also have insulin resistance issues. But if they have many neurocognitive problems, we might start with the NF kappa B. So, that’s the way you can decide which ones to pick. Now, remember, when talking with patients, it is important to discuss how their eating habits are causing inflammation in their bodies. It is also important to note that it’s not just a quality conversation; it’s a quantity conversation and an immune conversation.
This reminds you that when you fix the gut by feeding it well and reducing its inflammatory tone, you get a host of other preventative benefits; you stop or at least reduce the strength of the dysfunction. And you can see that, ultimately can reduce the overlapping risk of obesity, diabetes, and metabolic syndrome. We are trying to drive home that metabolic endotoxemia, or just managing the microbiome, is a powerful tool to help your insulin-resistant or cardiometabolic patients. So much data tells us that we cannot just make the conversation about eating right and exercising.
It’s so much beyond that. So the more we can improve the gut microbiota, we can change inflammation signals through proper diet, exercise, stress management, sleep, all the other things we’ve been talking about, and fixing the gums and the teeth. The less the inflammation, the less the insulin dysfunction and, therefore, the less all those downstream disease effects. So what we want to make sure you know is to go to the gut and make sure that the gut microbiome is happy and tolerant. It’s one of the most potent ways to influence a healthy cardiometabolic phenotype. And aside, although it was a bigger thing a decade ago, non-caloric artificial sweeteners do as they might be non-caloric. And so people may be tricked into thinking it’s zero sugar.
But here’s the problem. These artificial sweeteners can interfere with healthy microbiome compositions and induce more type two phenotypes. So, even though you think you’re getting the benefit with no calories, you’re going to increase your risk for diabetes more through its effect on the gut microbiome. All right, We’ve made it through objective one. Hopefully, you’ve learned that insulin, inflammation, adipokines, and all the other things that happen in the endocrine response affect many organs. So let’s now start to look at emerging risk markers. Okay, we’ve talked a bit about TMAO. Again, that’s still a relevant concept here with gut and insulin resistance. So we want to make sure that you look at TMAO not as the end all be all but as another emerging biomarker that could give you a clue about microbiome health in general.
Looking For The Inflammatory Markers
Dr. Alex Jimenez, D.C., presents: We look at elevated TMAO to help the patient recognize that they have changed their eating habits. Most of the time, we help patients reduce unhealthy animal proteins and increase their plant-based nutrients. It’s generally how many doctors use it in standard medical practice. Alright, now another emerging biomarker, okay, and it sounds funny to call it emerging because it seems so obvious, and that is insulin. Our standard of care is centralized around glucose, fasting glucose, to our postprandial glucose A1C as a measure of glucose. We are glucose so centric and need insulin as an emerging biomarker if we try to be preventative and proactive.
And as you remember, we talked yesterday that fasting insulin in the bottom of the first quartile of your reference range for fasting insulin might be where you want to go. And for us in the US, that tends to be between five and seven as a unit. So notice that this is the pathophysiology of type two diabetes. So type two diabetes can happen from insulin resistance; it can also occur from mitochondrial problems. So pathophysiology of type two diabetes could be because your pancreas is not secreting enough insulin. So again, this is that little 20% that we talk about the majority of the people who are getting type two diabetes; it’s from insulin resistance, as we would suspect, from a hyper insulin problem. But there is this group of people who have damaged mitochondria, and they are not outputting insulin.
So their blood sugar rises, and they get type two diabetes. Okay, then the question is, if there is a problem with pancreatic beta cells, why is there a problem? Is the glucose going up because the muscles have insulin resistance, so they cannot capture and bring in glucose? So is it the liver that’s hepatic insulin resistant that cannot take in glucose for energy? Why is this glucose running around in the bloodstream? That’s what this is paraphrasing. So contributing role, you have to look at the adipocytes; you have to look for visceral adiposity. You must see if this person is just a big belly fat inflammatory-like catalyst. What can we do to reduce that? Is the inflammation coming from the microbiome?
Conclusion
Dr. Alex Jimenez, D.C., presents: Even the kidney can play a role in this, right? Like perhaps the kidney has increased glucose reabsorption. Why? Could it be because of an oxidative stress hit to the kidney, or could it be in the HPA axis, the hypothalamus pituitary adrenal axis where you’re getting this cortisol response and this sympathetic nervous system response that’s generating inflammation and driving the blood insulin and blood sugar disturbances? In Part 2, we will talk here about the liver. It’s a common player for many people, even if they don’t have fulminant fatty liver disease; it’s generally a subtle and common player for people with cardiometabolic dysfunction. So remember, we’ve got the visceral adiposity causing inflammation and insulin resistance with atherogenesis, and the liver is like this innocent bystander caught up in the drama. It’s happening before sometimes the atherogenesis starts.
Winter is when most children and adults are prone to catching colds, the flu, etc. The excitement of the holiday season can also take a toll on the body’s neuromusculoskeletal system, leaving the individual more susceptible to illness. Digestive issues such as bloating, cramping, and constipation are also common. Certain supplements can help maintain body, gut, and brain holiday health. Here are a few recommended supplements to take during the holidays.
Holiday Health
To help fill in the gaps from the holiday foods and increase energy, holiday health supplements to consider adding include:
Probiotics
Probiotics are healthy bacteria and microbes that populate the gut or microbiome.
They help digest nutrients, support proper digestion and elimination, and manage appetite and mood.
A quality probiotic supplement supports healthy digestion and immune health.
It can help reduce diarrhea, constipation, gas, and bloating while protecting the immune system against pathogens.
For the most benefits, it is recommended to take a supplement with a high CFU count, diverse probiotic strains, and a delivery method that ensures the probiotics will survive once consumed.
The body produces melatonin naturally, especially at night, since this promotes sleep.
Melatonin is a hormone that helps regulate the body’s circadian rhythm, which makes you feel tired or alert at the right times of the day.
Taking melatonin can help decrease jet lag symptoms.
Consider taking melatonin to help promote healthy sleep.
However, it’s usually only recommended for short-term use, so consult your doctor.
Vitamin D
During the winter, when less sunlight is available, low vitamin D levels are very common among adults.
The body naturally makes vitamin D when the skin is exposed to the sun’s UV light rays; however, most spend nearly all their time indoors once the weather becomes cold.
Vitamin D is responsible for hundreds of reactions related to brain function, hormone production, and immune defenses.
A vitamin D supplement can help maintain healthy levels, which is important for maintaining a strong immune system, cardiovascular and bone health, and mood.
Magnesium
Magnesium is a mineral and electrolyte providing cardiovascular and bone support, improved sleep, healthy muscle and nerve function, and healthy digestion.
A magnesium supplement can help with aches and pains, restlessness, headaches, and constipation.
Vitamin C
Vitamin C intake protects against colds and other illnesses.
It supports healthy immune defenses, healthy nervous system function, antioxidant activity, neuron function, and skin health.
A vitamin C supplement combined with probiotics further helps support healthy gastrointestinal function and absorption.
Chiropractic For Digestive Health
Chiropractic care supports the healthy functioning of the nervous system.
The vagus nerve extends from the brain stem and innervates digestive system organs.
Sympathetic nerves in the thoracic and lumbar regions and the parasympathetic nerves near the sacrum also support digestion.
Decompressing the spine and correcting posture allow room for the muscles to contract, open up the spine to circulate fluids throughout the body, and expand and properly circulate food and waste.
Ernst, Edzard. “Chiropractic treatment for gastrointestinal problems: a systematic review of clinical trials.” Canadian journal of gastroenterology = Journal canadien de gastroenterology vol. 25,1 (2011): 39-40. doi:10.1155/2011/910469
Govender, Mershen et al. “A review of the advancements in probiotic delivery: Conventional vs. non-conventional formulations for intestinal flora supplementation.” AAPS PharmSciTech vol. 15,1 (2014): 29-43. doi:10.1208/s12249-013-0027-1
Leboeuf-Yde, Charlotte, et al. “Self-reported nonmusculoskeletal responses to chiropractic intervention: a multination survey.” Journal of manipulative and physiological therapeutics vol. 28,5 (2005): 294-302; discussion 365-6. doi:10.1016/j.jmpt.2005.04.010
Peterson, Caroline. “A case study of chiropractic management of pregnancy-related heartburn with postulated fetal epigenome implications.” Explore (New York, N.Y.) vol. 8,5 (2012): 304-8. doi:10.1016/j.explore.2012.06.001
Qu, Liuxin, et al. “Irritable bowel syndrome treated by traditional Chinese spinal orthopedic manipulation.” Journal of traditional Chinese medicine = Chung i tsa chih ying wen pan vol. 32,4 (2012): 565-70. doi:10.1016/s0254-6272(13)60072-2
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Fiber and Gut Health
Fiber and Gut Health