Intestinal Permeability: Alcohol and non-steroidal anti-inflammatory drugs, or NSAIDs, are harmful agents which can disrupt the balance of the digestive system, ultimately affecting the gastroduodenal mucosal and damaging the epithelial barrier along the gastrointestinal tract, or GI tract, increasing intestinal permeability. Moreover, it’s not uncommon for patients to have been exposed to the two substances at the same time. It is therefore important to know how simultaneous use can affect intestinal barrier function and acquiring that knowledge was the goal of several research studies.
What is the effect of alcohol and NSAIDs in intestinal barrier function?
Changes in intestinal permeability became more evident after Meddings et al. introduced the sucrose permeability test in 1993 as a non-invasive measure for evaluating the extent of gastrointestinal tract damage induced by non-steroidal anti-inflammatory agents, or NSAIDs. Subsequently, several studies demonstrated that intestinal barrier dysfunction to sucrose is a reasonable marker for the presence of GI tract damage in NSAID users. Other researchers used sucrose permeability tests to assess damage to the gastroduodenal mucosa induced by oral corticosteroids, intense exercise, infection, atrophic gastritis, Crohn�s disease, celiac disease, coffee, smoking, or a combination of these damaging factors. Alcohol is another agent that affects intestinal barrier function. A few studies have also demonstrated that acute alcohol consumption increases intestinal permeability. The effects of chronic exposure to alcohol on intestinal permeability, however, are less well established than that of NSAID use on intestinal permeability.
Intestinal Permeability:�Intestinal Barrier Dysfunction from NSAIDs and Alcohol
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
The pathogenesis of NSAIDs is well investigated, but still not fully understood. The use of NSAIDs, or non-steroidal anti-inflammatory drugs, has been associated with the increased risk of developing gastrointestinal disease, or GI disease, as well as other digestive health side effects and issues. Considerable amounts of evidence have also demonstrated that, much like chronic alcohol consumption, constant use of NSAIDs can affect intestinal barrier function, which may cause significant GI tract, or gastrointestinal tract, damage, such as ulcers, perforation, hemorrhage and an exacerbation of inflammatory bowel disease, or IBD. It has been suggested that the effect of NSAIDs has separate phases.
First, NSAIDs are included into biological membranes because of their lipophilic properties. They interact with brush border phospholipids, causing direct damage to intestinal epithelium. NSAIDs also detach oxidative phosphorylation, which leads to mitochondrial dysfunction and, consequently, to a reduction in intracellular ATP. The decrease in ATP results in reduced intestinal epithelial barrier function, as the regulation of the intracellular actin-myosin complex is an ATP-dependent process. The regulation of membrane phospholipids and intracellular ATP levels are followed by leakage of intracellular calcium and increased production of free oxygen radicals. These processes will directly change intestinal permeability by affecting the contraction of the intracellular cytoskeleton and the integrity of the tight junction, or TJ, complex. This increased permeability then triggers the last phase of NSAID-induced enteropathy, which is the transportation of luminal compounds, such as bile acids, bacterial breakdown products, acid and pepsin, into the intestinal mucosa, triggering an immune response as well as inflammation. In addition to the phases mentioned above, NSAIDs can also induce mucosal damage by its prostaglandin-inhibiting properties. After absorption, NSAIDs inhibit cyclooxygenase-1 and -2, or COX-1 and -2. COX-1 inhibition leads to a decrease in mucosal blood flow, whereas inhibition of COX-2 has an effect on immune regulation.
Both acute and chronic use of non-steroidal anti-inflammatory drugs by healthy volunteers and patients demonstrated changes in intestinal barrier dysfunction and hypermotility, abnormal or excessive movement, specifically of the gastrointestinal tract. In vitro research studies utilizing MKN28, a gastric epithelial cell line has also demonstrated that aspirin-induced increase in permeability was characterized by a considerable decrease in the expression of claudin-7, but not claudins-3, -4, ZO-1 or occludin.
NSAID-induced gastrointestinal tract damage was initially found to be a consequence of cyclooxygenase inhibition and decreased prostaglandin synthesis; however, it is now evident that intestinal barrier dysfunction is a multi-stage process. Experimental and clinical research studies have demonstrated a contribution from neutrophils, microcirculatory disturbances, oxygen free radicals and bile acids in NSAID-induced GI tract damage. NSAIDs increase intestinal nitric oxide synthase expression, resulting in increased levels of NO, boosting intestinal permeability. NSAIDs may also detach mitochondrial oxidative phosphorylation, which impairs the mitochondrial energy generation required for TJ complex integrity, resulting in increased intestinal inflammation and permeability. Finally, a recent study demonstrated that aspirin induced an increase in gastric epithelial cell permeability which was mediated by activation of p38 MAPK and a decrease in claudin-7, and treatment where a p38 MAPK inhibitor attenuated this response.
Alcohol
Clinical and experimental research studies have revealed that constant alcohol consumption may often lead to increased intestinal permeability, inhibition of nutrient transportation, such as vitamins and minerals, and a decreased absorption of sodium and water. Research study evaluation results demonstrated the involvement of the byproduct of ethanol metabolism, acetaldehyde and nitric oxide, or NO, in alcohol-mediated intestinal barrier dysfunction. High levels of acetaldehyde were detected along the gastrointestinal tract, or GI tract, of rats following the administration of ethanol. Increased levels of acetaldehyde has also been closely associated with increased intestinal permeability and endotoxin translocation, according to the research studies. In addition, the incubation of Caco2 cells with acetaldehyde demonstrated increased monolayer permeability. The growth was associated with increased tyrosine phosphorylation of both ZO-1, E-cadherin and ?-catenin. Exposing Caco2 monolayers to ethanol also boosts inducible nitric oxide synthase expression, stimulating increased NO, or nitric oxide, production as well as increased monolayer permeability. NO-induced changes were associated with an increase in unstable, non-polymerized tubulin and extensive damage to the microtubule cytoskeleton.
Experimental and clinical research studies in rodents have also demonstrated that acute administration of alcohol can cause mucosal damage in the upper small intestine, such as villus ulceration, submucosal blebbing and hemorrhagic erosions as well as intestinal barrier dysfunction. It has been acknowledged that alcohol-induced intestinal permeability helps enhance translocation of endotoxins across various organs, resulting in tissue damage and inflammation. Intragastric application of endotoxins from alcohol administration in rodents provided considerably higher plasma endotoxin levels than animals fed endotoxin alone. Similar lesions have also been found in healthy volunteers and active alcoholics following acute alcohol consumption while plasma endotoxin levels in alcoholics were found to be 5 times greater than in healthy controls. While not entirely understood, evidence suggests that the mechanism inherent alcohol-induced intestinal barrier dysfunction is connected to the introduction of inflammatory cells and to the release of various mediators, including cytokines, reactive oxygen species, leukotrienes and histamine.
Maintenance of the intestinal barrier function is important for our health, and dysfunction may be a risk factor for a variety of disorders and diseases.�Information referenced from the National Center for Biotechnology Information (NCBI) and the National University of Health Sciences. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
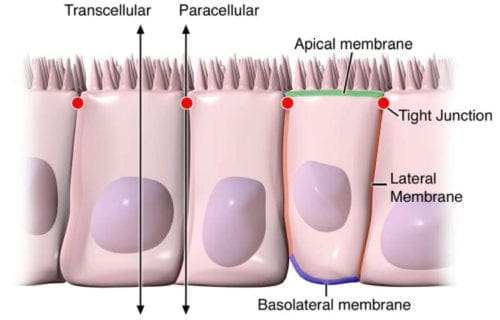
Digestive health can be attributed to the optimal function of the gastrointestinal tract. By way of instance, however, if disease affects the structure of the gut, understanding its anatomy and function, can help healthcare specialists conclude a diagnosis outcome. The intestinal epithelium is a single layer of cells found lining the intestinal lumen, which plays the role of carrying out two essential functions in the digestive system. Its first function is to act as a barrier to prevent the passage of harmful intraluminal entities, such as foreign antigens, microorganisms and their toxins. Its second function is to act as a selective filter, allowing the translocation of important dietary nutrients, electrolytes and water from the intestinal lumen to the blood stream. The intestinal epithelium distinguishes selective permeability through two main pathways: the transepithelial/transcellular and paracellular pathways, as seen on Figure 1.
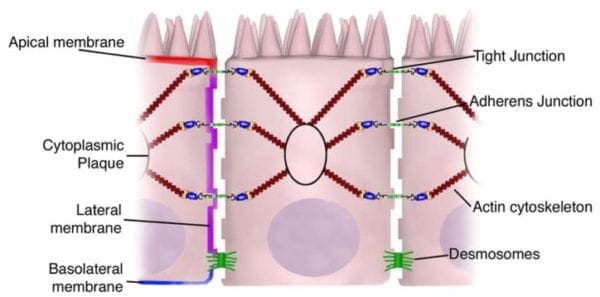
Transcellular permeability is generally related with the epithelial cells and is largely regulated by specific transporters in charge of also transferring amino acids, electrolytes, short chain fatty acids and sugars throughout the human body. Paracellular permeability is usually related to the transferring distance between epithelial cells and is greatly regulated by intercellular complexes found in the apical-lateral membrane junction and along the lateral membrane of the gastrointestinal tract, or GI tract. Interaction between the intestinal epithelial cells involves three components which can be identified at the ultrastructural level: desmosomes, adherens junctions, or AJs, and tight junctions, or TJs, as seen on Figure 2. The adhesive junctional complexes are made up of transmembrane proteins which connect adjacent cells to the actin cytoskeleton through cytoplasmic scaffolding proteins. The adherens junctions and desmosomes are believed to be more significant than the mechanical link of adjacent cells. The tight junctions, on the other hand, are the apical-most junctional complex, accountable for closing the intercellular space as well as regulating specific paracellular ionic solute transfer. The AJ and TJ complexes are also essential towards the regulation of cellular proliferation, polarization and distinction.
Structural Components of Junctional Complexes
Figure 1
Figure 2
Adherens Junctions (AJs)
The adherens junctions, also known as zonula adherens, are protein complexes located along the lateral membrane which happen in points of cell to cell contact, as seen on Figure 2. They’re shaped by interactions between transmembrane proteins, intracellular adaptor proteins and the cytoskeleton. The major AJs, or adherens junctions are formed by cadherin to catenin interactions. Epithelial (E)-cadherins, or calcium-dependent adhesion molecules, are Type-I single transmembrane spanning glycoproteins that contain an intracellular C-terminus and extracellular N-terminus. The extracellular domain creates homotypical interactions with the cadherins of neighboring cells to develop this cell to cell adhesion. The intracellular domain contains a catenin-binding domain that interacts with members of the armadillo repeat superfamily, ?-, ?- and p120-catenin. The catenins then connect the AJs into the cytoskeletal network through direct binding to the C-terminal domain of F-actin or indirectly through interactions with other adaptor proteins like afadin. Cadherin to catenin complexes are significant not only for connecting adjoining cells, but also for keeping cell polarity and for regulating epithelial migration and proliferation as well as the formation of additional adhesive complexes, such as desmosomes. In order to allow the link of adjoining cells, a decreased regulation of E-cadherin from the intestinal epithelium interrupts cell to cell adhesion which has been associated with affected intestinal epithelial proliferation and migration.
Nectin-afadin interactions create another significant AJ complex. Nectins, specificially nectin-1-4, are immunoglobulin-like proteins that withstand homophilic and heterophilic interactions with nectins on adjacent cells. Nectins can interact with the cytoskeleton through afadin, an F-actin binding protein, or rather preferably through interactions with other F- or ?-actin binding proteins including ponsin/SH3P12, vinculin and afadin dil domain-interacting proteins.
Tight Junctions (TJs)
The tight junctions are the apical-most adhesive junctional complexes in the epithelial cells of mammals which develop a continuous belt-like ring around epithelial cells at the boundary between the apical and lateral membrane regions of the gastrointestinal tract, according to Figure 2. Tight junctions, or TJs, are powerful, multi-protein complexes which serve as a selective/semipermeable paracellular barrier, that eases the passage of ions and solutes through the intercellular space, while also preventing the translocation of luminal antigens, microorganisms and their toxins. The progression of TJ biology began in the 1960’s with the development of electron microscopy. Evaluation and analysis of epithelial cells explained a series of apparent fusions, in which the space between adjacent epithelial cells had been eliminated. These so-called “kissing points” are morphologically different from AJs and desmosomes, where adjoining cell membranes stay approximately 15 to 20nm apart. Since the first observations, TJs have been found to include four families of transmembrane proteins: occludin, claudins, junctional adhesion molecules, or JAMs, and tricellulin.
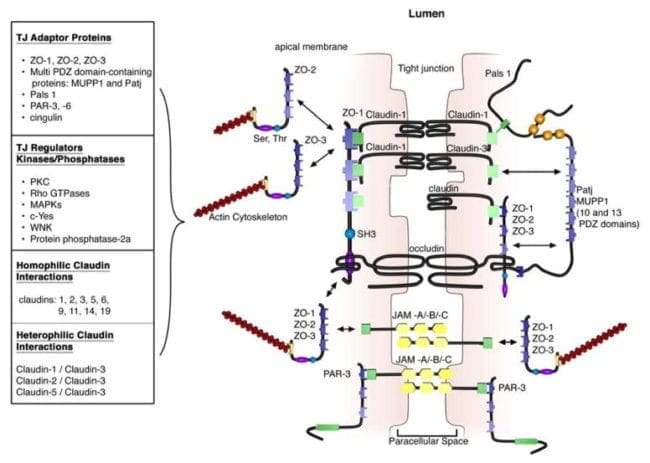
The extracellular domains of transmembrane TJ proteins in adjoining cells anastomose to shape the TJ isolate. These interactions involve those proteins found in the exact same membrane as well as those including proteins in adjacent cells. Additionally, TJ proteins may form homophilic interactions, with the exact same protein, or heterophilic interactions, between non-identical TJ proteins. Like the adherens junctions, the intracellular domains interact with different scaffolding proteins, adaptor proteins and signaling complexes to moderate cytoskeletal attachment, cell polarity, cell signaling and vesicle trafficking, as seen on Figure 3. The intracellular regions of AJs possess PDZ-binding domains, which gather and come in contact with PDZ domain containing proteins. The PDZ domain (Post synaptic density-95/Drosophila disk large/Zonula occludens-1 protein) is a common structural domain of about 80 to 90 amino acids which play the role of anchoring transmembrane proteins to the cytoskeleton. The intracellular domains may also interact with non-PDZ-binding domain including proteins like cingulin, which can interact with junctional membrane proteins, the actin cytoskeleton and signaling proteins. The complex network of intracellular protein interactions can also be known as the “cytoplasmic plaque”.
Figure 3
Tight Junction Formation in the Gastrointestinal Tract
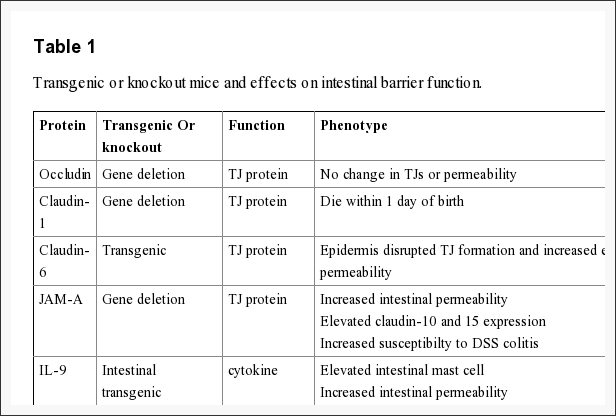
The intestinal epithelium shapes the largest and most essential barrier between our external and internal gastrointestinal tract environments. The barrier is preserved by the presence of AJs and TJs, such as cadherins, claudins, occludin and JAM proteins, which isolate groups of adjacent cells and maintains cytoskeletal anchorage, as seen on Figure 3. Expression of junctional proteins in the gut are highly regulated and dependent on both the small and/or large intestine, villus/crypt location and cell membrane specificity; apical, lateral or basolateral. The complex pattern of TJ expression from the gut is related to the particular functions of a distinct intestinal region and location. Expression of adherens junctions and tight junctions proteins can also be controlled by phosphorylation, according to Table 1. Phosphorylation can either promote TJ formation and barrier feature, or alternatively promote TJ protein redistribution and intricate destabilization.
Occludin
One of the first integral membrane proteins belonging specifically to the tight junctions to be recognized is the occludin. Occludin are predominantly found at TJs in the epithelial and endothelial cells but can also be located in astrocytes, neurons and dendritic cells. Occludin (60 to 82 kDa) is a tetraspanning integral membrane protein consisting of two extracellular loops, a short cytoplasmic N-terminus and a long cytoplasmic C-terminus. Analysis and evaluation of the function of these have demonstrated that the extracellular loops and transmembrane domains of occludin manage and maintain selective paracellular permeability. Intracellularly, the C-terminus interacts with the PDZ-domain containing protein ZO-1, which is required to connect occludin into the actin cytoskeleton, according to Figure 3.
Several occludin isoforms are characterized and believed to be the result of alternative mRNA splicing. Quite distinctly, many splice variants demonstrate altered subcellular distribution and interaction with other TJ molecules. Evaluation of these splice variants showed that the cytoplasmic C-terminal domain is funcamental for the intracellular exchange of occludin to the lateral cell membrane, which the fourth transmembrane domain name is important for targeting occludin into the TJ as well as for ZO-1 interactions.
The role of occludin is not fully outlined; nonetheless, data suggested another function for occludin from the regulation of paracellular permeability. The major allergen of the house dust mite, Der p 1, was determined to proteolyticly disrupt occludin altering this TJ complex and increasing paracellular permeability. In addition, hydrocortisone treatment of bovine retinal endothelial cells improved occludin expression two-fold and enhanced monolayer barrier properties. Though occludin is an important element of TJs, TJ formation and paracellular permeability barrier function are not dependent on occludin. Experimental investigations of occludin on mice demonstrated equivalent numbers and groups of TJs and corresponding paracellular ion passage as wild mice. Furthermore, epithelial transport and barrier function were normal in mice with occludin. Along with regulating paracellular permeability, there is evidence indicating occludin is included in cellular adhesion. Length of occludin at occludin and rat fibroblasts conferred cell to cell adhesion that has formally been interrupted by synthetic peptides associated to the first extracellular loop of occludin, underscoring the significance of the area of occludin in cell adhesion.
Evaluations indicated that occludin found along the TJ complex is regulated by phosphorylation. Several potential phosphorylation sites at tyrosine, serine, and threonine residues of occludin have been identified where the regulation of occludin phosphorylation is proposed to happen by kinases, for instance, non-receptor tyrosine kinase c-Yes and protein kinase C (PKC), and phosphatases including the serine/threonine protein phosphatase 2A, according to Figure 3. PKC?, a novel protein kinase predominantly expressed in the intestinal epithelium, was demonstrated to directly phosphorylate occludin in threonine residues (T403 and T404). Blockade of all PKC?-mediated occludin phosphorylation interrupted junctional distribution of occludin and ZO-1 and interrupted epithelial barrier function. The data suggest that occludin phosphorylation modulates occludin-ZO-1 interactions and the maintenance of intact TJ complexes and paracellular barrier function.
Claudins
Claudins are 20 to 27 kDa integral membrane proteins with four hydrophobic transmembrane domains, two extracellular loops and N- together with C-terminal cytoplasmic domains. The extracellular loops are crucial for homophilic and/or heterophilic TJ protein to protein interactions alongside the creation of ion-selective channels. The intracellular C-terminal domain is included in anchoring claudin into the cytoskeleton through connections with PDZ-binding domain names, such as ZO-1, -2 and -3, according to Figure 3. Presently, 24 distinct claudin family receptor members are identified in those who have a number of orthologues expressed in various species. They exhibit distinct cell, tissue and developmental stage-specific expression routines.
Claudin to claudin interactions between adjoining cells might be homophilic or heterophilic. Homophilic interactions have been shown for claudins 1, 2, 3, 5, 6, 9, 11, 14 and 19. On the reverse side, heterophilic interactions are more restricted and largely have been detected with claudin-3, which could interact with claudins-1, -2 and -5. Notably, there’s specificity in heterophilic trans-interactions. By way of instance, transfection of fibroblasts with claudins-1, -2 and -3 led to claudin-3 interactions with claudin-1 and -2; yet no interactions involving claudin-1 and -2 were detected. These discerning interactions are considered to describe the diversity in TJ formations and provide a molecular basis for tissue-specific heterogeneity of barrier function.
Recent study, together with claudin-deficient mice also give corroborative information supporting a role for claudins in the law of barrier function. Claudin-1 mice die within a day of birth due to significant transepidermal water loss. Furthermore, transgenic overexpression of both claudin-6 in skin disrupted tight junction formation and increased epithelial permeability. Experimental data indicates that claudins could have differential impacts on paracellular permeability. By way of instance, introduction of claudin-2 to MDCK I cells which state claudin-1 and -4 activates a decrease in transepithelial resistance, or TER; whereas transfection of claudin-3 had no effect indicating that claudin-2 markedly diminished claudin-1/claudin-4 based TJ strand regeneration. In support of the latest experimental evidence indicates that claudins can form measurements and charge-specific paracellular stations. Transfection of claudin-8 into MDCK II cells that lacks endogenous claudin-8 substantially reduced paracellular movement without impacting anion and uncharged solute movement. Experimental investigations suggest that the first extracellular loop of claudins play an essential role in deciding charge selectivity. Interchanging of the earliest or extracellular domains of claudin-4 on claudin-2 profoundly diminished the ion conductance of Na+ relative to Cl? 76. Additionally, substitution of a negatively-charged lysine into some positively charged aspartic acid (K65D) inside the loop of claudin-15 generated an increase in Na+ permeability, whereas mutation in exactly the same place of three positively charged amino acids into negatively charged aspartic acid, arginine and aspartic acid (E46K, D55R and E64K) altered the ion selectivity of claudin-15 in Na+ to Cl? channel. Pore size and density may also impact paracellular movement of non invasive and charged charged solutes.
Claudins also play an essential role in epithelial cell invasion and motility. Overexpression of claudins-3 and -4 in human ovarian epithelial cells, which lack the expression of these proteins, has been connected with enhanced epithelial cell survival and enhanced invasion and motility. Consistent with this observation, siRNA-mediated knockdown of the two claudins-3 and -4 in ovarian cancer cell lines diminished intrusion. The outcome of claudin-3 appear to get connected to altered matrix metalloprotease-2 activity, meaning claudin-induced invasion could possibly be regulated by metalloprotease proteins.
Similar to occludin, claudin localization to the TJ complex and its function are regulated by post-translational phosphorylation and through connections with PDZ-binding domains. The intracellular C-terminal domain of claudin possesses multiple regulatory sites, such as possible serine and theronine phosphorylation sites and PDZ-binding domain names. Phosphorylation of claudins-3 and -4 in prostate cancer cells is closely connected to the regulation of paracellular permeability. By way of instance, patients with pseudohypoaldosteronism type II (PHA II; or vitamin shunt syndrome) present with hyperkalemic metabolic acidosis, hypertension and dysregulated paracellular ion transport. The molecular basis is connected to some loss-of-function mutation from the serine-threonine kinases, WNK1 and WNK4, which regulate epithelial chloride cotransporters. This also contributes to an increase in the phosphorylation of both claudins-1-4 and an increase in paracellular permeability. A lot of signaling pathways are implicated in the phosphorylation of claudins like PKC, Rho GTPases, mitogen-activated protein kinases (MAPKs) and phosphatases. MAPK phosphorylation of claudin-1 is required for claudin-1-mediated barrier function. Furthermore, claudins-1, -2, -7, -8, -16 and -17 have putative PKC phosphorylation websites.
All claudins, except claudin-12, completing from the dipeptide arrangement YV, that’s been shown to interact with PDZ-binding domains comprise ZO-1, -2 and -3, multi-PDZ domain name and PALS1-associated TJ protein, according to Figure 3. Several of those scaffolding proteins contain several PDZ domains, which eases the introduction of dense localized protein complexes, also called “cytoplasmic plaques”. Also, the scaffolding proteins can interact with signaling molecules, such as heterodimeric GTP binding proteins (Rab13 and G?12), transcriptional factors and RNA-processing variables, to connect TJ complexes to the actin-cytoskeleton and modulate aspects of adrenal polarization, differentiation and barrier function.
Junctional Adhesion Molecules (JAMs)
Junctional adhesion molecules are integral membrane proteins which belong to the immunoglobulin superfamily and have two immunoglobulin folds, the VH- and C2-type, from the extracellular domain. JAMs are expressed by multiple cell types, including epithelial, endothelial and immune cells. They’re subdivided based on the expression of Type I or II PDZ-binding themes in the intracellular C-terminus, which implies that the two types interact with exceptional scaffolding and cytoplasmic proteins. JAM-A, -B and -C (or JAM1-3) have Type II binding subjects, while the atypical JAMs, such as JAM-4, coxsackie and adenovirus receptor (CAR) and endothelial selective adhesion molecule make up Type I PDZ-binding domains. Comparable to additional TJ proteins, these JAM-PDZ interactions provide anchorage to the actin cytoskeleton, according to Figure 3.
The extracellular region of JAMs adapting to multiple ligands through homophilic and heterophilic interactions, which can be proposed to regulate the mobile functions and paracellular permeability of JAMs. Homophilic JAM-A or -B interactions govern the creation of operational TJs and cell to cell border formation, while heterophilic JAM interactions play a role in leukocyte-endothelial cell adhesion.
Recent studies demonstrate the significance of JAM-A at the formation and assembly of TJs in intestinal epithelial cells. SiRNA downregulation of JAM-A at SK-C015 epithelial cells triggered an increase in permeability. Consistent with this, JAM-A mice had increased mucosal permeability as indicated by enhanced dextran flux and decreased TER. Nonetheless, these mice also had an increase in claudin-10 and -15 expression, which is believed to shape selective pores from the TJ complex, improving paracellular permeability. Interestingly, JAM-A mice have increased susceptibility to chemical-induced colitis. Dextran sodium sulfate administration to JAM-A mice induced more acute colonic injury as compared to WT control animals. These studies imply altered intestinal permeability for a susceptibility factor to autoimmune disorder.
The above information is evidence-based. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
A healthcare professional at a gastroenterology practice, such as a dietitian specializing in gastrointestinal diseases, will often care for a great deal of individuals who walk into their clinic reporting symptoms which haven’t yet been diagnosed to a specific digestive health issue. Because not many primary care physicians are in charge of diagnosing GI diseases nor are they properly aware of their wide array of symptoms, many people with gastrointestinal diseases will often go undiagnosed for years.
How can you talk to your doctor about your digestive issues?
A healthcare provider specializing in gastrointestinal diseases may look out for certain symptoms, as well as possible dietary triggers, to determine a digestive health issue. Simple lifestyle changes are generally the best treatment method to help improve GI diseases and its symptoms, however, being able to communicate accordingly with your doctor can help them diagnose your problem more accurately in order to begin treatment immediately. By following a few factors the patient can control, they can ensure their medical diagnostic procedure is fast, easy, and correct.
Arrive to your Appointment on Time
While careful planning and preparations can occasionally be sabotaged by events and situations that are out of our control, it’s essential for you to initially intend to reach your appointment on time. It’s recommended to arrive at least 15 minutes before your original appointment time, especially if you are a new patient as you will need to complete the necessary paperwork on your first visit. If you show up 15 minutes late for a 15 minute appointment, there is a great chance you’ll be hurried through your visit without ample time to go over your issues thoroughly with your doctor.
Bring Evaluation Results & Procedure Reports
It can’t be emphasized enough how common it is for patients to not know which previous diagnostic tests or even surgeries they’ve gone through for their specific disease and/or condition. If you show up to a healthcare professional’s appointment for further diagnosis and a second opinion regarding your symptoms without being aware of this information, your doctor may waste valuable time and money re-testing you for digestive health issues which may have already been ruled out by another healthcare specialist. Furthermore, without previous evaluation results and/or procedure reports, doctors can miss an obvious diagnosis based on your health history, or worse, they may perform yet another invasive procedure which you no longer needed.
If you have had an endoscopy or a colonoscopy, what were the signs? If you’ve had surgery somewhere on your gastrointestinal tract, which process was it? If you have experienced a breath test, what were they checking for and what were the results? If blood has been drawn lately, what was being checked and also what, if anything, has been discovered? Have you had any specialized tests that involved imaging of your gastrointestinal tract? These are all important questions you must know before visiting a doctor’s office.
Also, to get to a faster diagnosis, your best option is to bring copies of all relevant tests and reports you have undergone related to your digestive health issues. It may take some effort to collect these results from previous doctors or even hospitals, though medical practices offering online patient portals may make this procedure easier. If you can’t obtain the true exam results, then compiling a summarized “medical resume” may be the next best thing. Just type up a list of all of the test names or procedure reports you’ve had; who ran them (as well as where and when they were performed); and exactly what they discovered, based on those evaluations and procedures. Hand the sheet to your healthcare professional. Their office can then track down copies of any relevant results after you leave from your first appointment.
Describe your Symptoms in Detail
It can be quite embarrassing to describe your digestive symptoms to a healthcare professional and you might even feel unsure of whether you may actually have a digestive issue based on your “normal” collection of gut sounds, backed up stools and that occasional nausea you experience after eating a heavy meal. You may be tempted to use more conservative, generic phrases to describe your symptoms but healthcare specialists say you don’t have to be considerate. Your doctor has literally heard it all and it is as routine to them as speaking about the weather is to everyone else.
If you say that you “get sick to your stomach” when referring to having diarrhea, for instance, the healthcare professional may actually think you are referring to nausea. If you say “constipated” to refer to straining to have a daily bowel movement, your doctor may presume you mean you are unable to move your bowels more than once or twice per week. If you say you get a “stomachache” after eating, it could refer to sharp pain, cramps or dull pain and it doesn’t properly inform your doctor where the pain is located. Tell your doctor exactly what you mean, along with all of the extra descriptive details. What’s happening and where, what it looks like, what it smells like, what it feels like and how frequently it happens. Correctly describing your symptoms is key to a correct diagnosis.
Mention When your Symptoms Started
At times, telling your healthcare specialist when your symptoms all started can be the clue to your diagnosis. Did you notice your digestive health issues after you recovered from a bout of food poisoning in your holiday? Did things change for you in the bathroom after having your gallbladder removed? Did your digestive discomfort increase after switching to a brand new diet, such as a 30-day cleanse, Weight Watchers or a paleo-style diet? Do your symptoms coincide with starting or stopping a particular drug/medication or supplement? Have you experienced this digestive health issue since you were a child? Did your issue get better or worse during pregnancy? Putting your complaints in context will help your doctor perform a better medical diagnostic procedure.
Inform your Doctor of What you Have & Haven’t Tried
Doctors often learn just as much out of what hasn’t helped you feel better as they do from what has helped you feel better. If you have already tried a drug/medication, supplement, lifestyle changes, including diet modifications and physical activities, to address your gastrointestinal issues and it has not worked, make sure you incorporate this in your conversation with your healthcare specialist. It will help them narrow down the list of possibilities and help point to more likely gastrointestinal diseases and conditions.
Keep an Open Mind
Now that we all have access to the internet, we’ll often arrive to a doctor’s appointment with a preconceived notion about what we believe we may have. Because of this, many patients may attempt to steer the conversation toward this self-diagnosis and accidentally leave out important information that could shed light on the correct diagnosis. It is absolutely appropriate to share your own hypothesis about your digestive health issue with your healthcare provider and this can be particularly more important if you’ve got a family medical history which may accurately indicate your problem. But be sure to share all the details of your conclusion, and be open to the possibility that your doctor may see matters in a different light than all the other articles you may have read on the internet. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
In the month of October, approximately 50,000 people worldwide gathered in the World Congress of Gastroenterology to discuss different ways in which healthcare professionals could improve care for individuals with gastrointestinal, or GI, diseases, involving the gastrointestinal tract. While these attempts within the GI community are undeniably essential, it’s also fundamental that we teach the broader medical community concerning the growing challenge these gastrointestinal diseases present for the doctors.
How can you improve gastrointestinal diseases and its symptoms?
As many as 16 million individuals in the United States alone, suffer from irritable bowel syndrome, or IBS, with diarrhea, a gastrointestinal disease which mainly affects the bowel or colon and its symptoms are commonly characterized by abdominal pain and nausea. Constipation is the most common and uncomfortable gastrointestinal, or GI, issue, frequently reported by patients taking opioids. There are over 200 million opioid prescriptions written every year, each of which can lead to GI disease.
Inflammatory bowel diseases, such as ulcerative colitis and Crohn’s disease, usually involve severe nausea, abdominal pain, fatigue and weight loss. In 1999, there were 1.8 million cases of inflammatory bowel diseases, or IBD, among Americans. As of 2016, that number has substantially increased up to 3.1 million cases within the American population. When the liver is unable to efficiently eliminate toxins from the bloodstream, it can cause loss of brain function, a condition known as hepatic encephalopathy. The yearly inpatient incidence of hepatic encephalopathy increased from 20,918 from 2005 to 22,931 in 2009, making up approximately 0.33 percent of all hospitalizations from the United States.
The Significance of Proper Care for Gastrointestinal Diseases
Not only do gastrointestinal, or GI, diseases and their symptoms affect an overwhelmingly big part of our population, these have also become a burden on the federal health care system. In 2013, direct expenses of IBS, or irritable bowel syndrome, had ranged from $1,562 to $7,547 per individual, annually. The total national charges associated with HE, or hepatic encephalopathy, also increased from $4.6 billion in 2005 to $7.2 billion in 2009.
The logical question we should ask ourselves regarding the increasing cases of gastrointestinal diseases is: Are patients receiving the proper treatment they need? Let us take a closer look at IBS, as it’s one of the most frequent functional GI diseases. Research published in the American Journal of Gastroenterology in June 2017, demonstrated that there is a greater than 40 percent chance that people who visit a healthcare professional for symptoms of IBS may not receive a proper diagnosis, as it generally takes patients four years to be diagnosed with IBS. It’s no surprise that gastrointestinal healthcare specialists would appreciate it if primary care physicians and nurse practitioners would handle the most common cases. But that may not occur until the wider medical community becomes more comfortable with diagnosing gastrointestinal disorders.
Unfortunately for the population of IBS sufferers that go undiagnosed, many resort to searching the internet for the answers themselves, followed by one attempt after another of self-diagnosis and self-treatment for their specific gastrointestinal diseases. A survey by the Pew Internet & American Life Project found that 80 percent of internet users have searched for a health-related topic online, most frequently, for information about a specific disease or medical issue. A Google search for “IBS,” for example, yields approximately 50 million hits. Add direct-to-consumer advertisements into the mix, and the clutter of information may be overwhelming for patients and healthcare professionals alike. Much of the information readily available to anyone with an online connection is evidence-based, however, much is specious and unfounded. Evaluating the information in an effort to self-diagnose and self-treat may be dangerous. What we need is a strategy to help individuals and doctors cut through the clutter and make that information work for them in mutually positive ways.
Many healthcare professionals are pledging to invest multimillions to increase awareness of gastrointestinal diseases and their symptoms. Specialist groups are starting a national educational program at the primary care level which will require doctors to take an educational voyage deep within a high-definition, virtual lumen of the small intestine. Through the lens of a virtual reality tool, doctors peruse a swarm of microbiota and various bacteria drifting through the undulating, glistening layers of pinkish gut while a narrator explains how these life forms can potentially create a life of abdominal pain and discomfort. This immersive cartoon is part of a strategy to engage and educate the wider medical community on many leading theories about IBS, including the role gut microbiota can play in generating symptoms as well as that of other GI diseases.
Gastrointestinal healthcare specialists are already knowledgeable about the anatomy and function of the digestive system, however a lot of primary care physicians and the broader medical community may not be. By educating the wider medical community about these common digestive health issues, healthcare professionals can begin making a difference towards the overall treatment of gastrointestinal, or GI, diseases. If primary care physicians and nurse practitioners aren’t acutely conscious of the symptoms and possible etiologies that could point a GI� healthcare specialist to the proper treatment, their patient may continue to endure the uncomfortable symptoms for several years before finding an appropriate treatment therapy.
The greatest goal for us is to remove any obstacles which may come in between proper GI patient care, especially for the undiagnosed and untreated patient population. If healthcare professionals can diagnose patients earlier, those obstacles may soon disappear altogether. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The digestive system is largely in charge of providing the body with the essential nutrients needed for all the other systems of the body to function effectively. But, what happens when your digestive health is less than optimal and your overall wellness is affected? Gastrointestinal diseases can wreak havoc on the structure and function of the digestive system, altering its effectiveness when providing the body with essential nutrients, as well as that of other important processes in the human body.
What are Functional Gastrointestinal Diseases?
Functional gastrointestinal diseases are those in which the gastrointestinal tract, or GI tract, appear normal but may actually not be functioning properly. They are the most common issues which affect the gastrointestinal tract, including the colon and the rectum. Irritable bowel syndrome, or IBS, and constipation are two of the most commonly reported examples of functional GI diseases. Many factors may affect the gastrointestinal tract’s function, primarily when it involves its motility, or the ability to keep “things” moving, such as:
Eating an improper diet that is also low in fiber,
Not participating in enough physical activity or exercise,
Changes in your daily routine due to traveling,
Eating large quantities of dairy products,
Stress,
Resisting the urge to go to the bathroom,
Resisting the urge to go to the bathroom due to pain from hemorrhoids
Overdoing it on the use of laxatives, or stool softeners, which weaken bowel muscles,
Taking antacid medicines, which calcium or aluminum,
Using certain drugs and/or medications, especially antidepressants, iron pills, and strong pain medicines such as narcotics,
And pregnancy.
Irritable Bowel Syndrome, or IBS
Irritable bowel syndrome, also known as spastic colon, irritable colon, or nervous stomach, is a gastrointestinal disease in which the colon muscle contracts more frequently than in people without IBS. Certain foods, drugs and medications, and even emotional stress have been identified to be some of the most prevalent aspects which can trigger irritable bowel syndrome and its symptoms. Symptoms of irritable bowel syndrome, or IBS, include:
Abdominal pain and cramps,
Excessive gas,
Bloating,
Changes in bowel movement habits, such as harder, looser, or more urgent stools than normal,
And alternating constipation and diarrhea.
Treatment methods for irritable bowel syndrome, or IBS include:
Avoiding the consumption of caffeine or caffeinated products,
Adding more fiber intake to your diet,
Monitoring which foods trigger your IBS and taking action to avoid eating these foods,
Decreasing stress levels by learning different ways to cope with the stress,
And occasionally taking drugs and medications as prescribed by a healthcare professional.
Constipation
Constipation is a common gastrointestinal disease, described as the inability or struggle to have a regular bowel movement, or move stools, where they’re infrequent, about less than three times a week, or incomplete. Constipation is usually brought on by insufficient fiber in the diet, or due to a disruption in your normal diet or daily routine. Constipation can cause a person to strain during a bowel movement. It may create small, hard stools and can sometimes lead to anal issues, such as hemorrhoids and fissures. Constipation is seldom a sign of a more serious digestive health issue. People with constipation can treat the problem by:
Increasing fiber intake to your diet,
Engaging in regular physical activity or exercise,
And by going to the bathroom promptly when you feel the urge to go, as resisting the urge is believed to cause constipation.
If these treatment methods are not enough, laxatives can be used but only as a temporary alternative. Be aware that the overuse of laxatives can eventually worsen constipation symptoms. Always follow the advice of your healthcare professional or follow the directions on the laxative medicine, accordingly.
What are Structural Gastrointestinal Diseases?
Structural gastrointestinal diseases are those in which the bowels themselves look abnormal while also not functioning properly. Occasionally, the structural abnormality may need to be surgically removed to relieve the digestive health issue. Commonly reported examples of structural gastrointestinal diseases, include hemorrhoids, diverticular disease, colon polyps, colon cancer, and inflammatory bowel disease.
Anal Disorders
Hemorrhoids
Hemorrhoids can be characterized as the swollen blood vessels that line the anal opening. They are brought on by chronic, excessive pressure from straining during a bowel movement, persistent diarrhea or even pregnancy. There are two types of hemorrhoids: internal and external.
Internal Hemorrhoids
Internal hemorrhoids are blood vessels on the interior of the anal opening. When they fall down into the anus as a result of straining, they can become irritated and start to bleed. Ultimately, internal hemorrhoids can fall down enough to prolapse, or sink and/or stick, out from the anus.
Treatment methods for internal hemorrhoids include:
Improving bowel movement habits, such as avoiding constipation, not straining during bowel movements and going to the bathroom when you have the urge to go,
Having your doctor use elastic bands to remove the blood vessels,
And, having a healthcare professional surgically remove them. Surgical interventions are generally only utilized for patients with painfully large and persistent hemorrhoids.
External Hemorrhoids
External hemorrhoids are veins that lie just underneath the skin on the outside of the anus. Occasionally, after straining, the external hemorrhoidal veins can burst, forming a blood clot under the skin. This very painful condition is medically referred to as a pile.
Treatment methods for external hemorrhoids include removing the clot and vein under local anesthesia and/or removing the hemorrhoid itself.
Anal Fissures
Anal fissures are splits or cracks which occur in the lining of the anal opening. The most common cause of an anal fissure is the passing of very hard or watery stools. The crack in the anal lining exposes the muscles which control the passage of stool through the anus and out of the body. An anal fissure is considered to be one of the most painful gastrointestinal diseases, or disorders, because the vulnerable muscles can become irritated from exposure to feces, or stool, and/or air, and may lead to intense burning pain, bleeding, or spasm after bowel movements.
Initial treatment methods for anal fissures includes pain drugs/medications, the addition of dietary fiber to reduce the incidence of large, bulky stools, and sitz baths, where the individual sits in a few inches of warm water. If these treatments do not relieve the painful symptoms, surgery may be required to repair the sphincter muscle.
Perianal Abscesses
Perianal abscesses can occur when the tiny anal glands that open on the interior of the anus become obstructed, and the bacteria always present in these glands trigger an infection. When pus develops, it can create the perianal abscess.
Treatment involves draining the abscess, usually under local anesthesia by a qualified and experienced healthcare professional.
Anal Fistula
An anal fistula often follows drainage of an abscess and can be an unnatural tube-like passageway in the anal canal to a hole in the skin near the opening of the anus. Body wastes traveling through the anal canal are redirected through this tiny channel and out through the skin, causing itching and irritation. Anal fistulas also bring about drainage, pain, and bleeding. They rarely heal by themselves and usually require surgery to drain the abscess and “close off” the fistula.
Other Perianal Infections
Occasionally, the skin glands near the anus become infected and may need to be drained. Just behind the anus, abscesses can form that contain a little tuft of hair at the back of the pelvis, known as a pilonidal cyst. Sexually transmitted diseases which could affect the anus include anal warts, herpes, AIDS, chlamydia, and gonorrhea.
Diverticular Disease
Diverticulosis is the presence of small outpouchings, known as the diverticula, in the muscular wall of the large intestine which form in weakened areas of the gastrointestinal tract, or GI tract. They usually develop in the sigmoid colon, the high-pressure area of the lower large intestine. Diverticular disease is relatively common and can occur in approximately 10 percent of people over the age of 40 and in 50 percent of people over the age of 60 in Western cultures. It’s frequently caused by too little amounts of fiber in the diet. Diverticulosis rarely causes symptoms.
Complications of diverticular disease happen in about 10 percent of people with outpouchings. They include inflammation or infection (diverticulitis), bleeding, and obstruction. Treatment methods for diverticulitis includes antibiotics, increased fluids, along with a specialized diet. Surgical interventions are needed in about half of the patients who have complications to eliminate the involved segment of colon.
Colon Polyps and Cancer
About 130,000 Americans are diagnosed with colorectal cancer each year, making it the second most common type of cancer in the United States. Fortunately, with medical advances in early detection and treatment method therapies, colorectal cancer is one of the most curable forms of the disease. By utilizing a variety of screening tests, it is possible to prevent, detect, and treat the disease before symptoms begin to appear.
The Value of Screening
Virtually all colorectal cancers begin as polyps, benign, or non-cancerous, growths in the tissues lining the colon and rectum. Cancer develops when these polyps grow and abnormal cells develop and start to invade surrounding tissues. Removal of polyps can prevent the development of colorectal cancer. Almost all precancerous polyps may be removed painlessly using a flexible, lighted tube called a colonoscope. If not caught in the early stages, colorectal cancer can spread throughout your system. More advanced cancer requires more complex surgical procedures. Most early forms of colorectal cancer do not cause symptoms, making screening an essential part of its diagnosis. When symptoms do occur, the cancer might already be very advanced. Symptoms include, blood mixed in with the stool, a change in normal bowel movement habits, narrowing of the stool, abdominal pain, weight loss, or constant tiredness.
Most cases of colorectal cancer are detected in one of four ways:
By screening people at average risk for colorectal cancer beginning at age 50,
By screening people at higher risk for colorectal cancer, for example, those with a family history or a personal history of colon polyps or cancer,
By investigating the bowel in patients with symptoms,
And through a chance finding at a routine, doctor’s check-up.
Early detection is your best opportunity for a cure.
Colitis
There are several types of colitis, gastrointestinal diseases which can cause an inflammation of the gut. The different types of colitis include:
Infectious colitis,
Ulcerative colitis, where the cause is unknown,
Crohn’s disease, where the cause is unknown,
Ischemic colitis, caused when not enough blood is going to the colon,
And radiation colitis, caused after radiotherapy.
Colitis causes diarrhea, rectal bleeding, abdominal cramps, and urgency, or frequent and immediate need to empty the bowels. Treatment methods for colitis depend on the diagnosis, which is made after a colonoscopy and biopsy.
Can Gastrointestinal Diseases be Avoided?
Many gastrointestinal diseases, or GI diseases, can be prevented or their risk can reduced by managing and maintaining a healthy lifestyle, such as a proper nutrition, exercise, and hydration, among other lifestyle modifications, by practicing good bowel movement habits, and submitting to cancer screening. Colonoscopy is recommended for average risk patients at age 50. When you have a family history of colorectal cancer or polyps, colonoscopy may be recommended at a younger age. Normally, colonoscopy is recommended 10 years younger than the affected relative. For instance, if your brother has been diagnosed with colorectal cancer or polyps at age 45, you should begin screening at age 35. In case you have symptoms of colorectal cancer you should speak to your doctor right away. Common symptoms include:
A change in normal bowel movement habits,
Blood on or in the stool which is either bright or dark,
Unusual abdominal or gas pains,
Very narrow stool,
A feeling that the bowel has not emptied completely after passing stool,
Unexplained weight loss,
And fatigue.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Several hours after you’ve swallowed that delicious first bite from your breakfast meal, the process of digestion has already started helping you get the most essential nutrients from your food. Your gastrointestinal tract, around 30 feet of prime digestive real estate, has the important function of breaking down food to absorb carbohydrates, proteins and fats, as well as vitamins and minerals, necessary for you to survive. However, your digestive system may not always function seamlessly.
Is digestive health important for overall wellness?
In fact, approximately 60 percent of adults suffer from gastrointestinal diseases and often experience symptoms such as gas, bloating and constipation. While an occasional abdominal discomfort might appear normal to most people, it could signal the beginning of a much bigger digestive health issue and you may find that it can be quite a relief to know that you can take action to feel your best. Listed below are five digestion health tips everyone can put into practice to achieve optimal gut wellness.
Understanding the Gut’s Microbiome
One hundred trillion of your body’s greatest allies, bacteria found throughout various areas of the gastrointestinal tract, make up what’s referred to as the microbiome. Researchers believe that digestive health can provide an insight into the well-being of the entire human body and there’s evidence that both the type and amount of bacteria growing on your gut can affect other functions as well, from your immunity to even your mood. The good kinds of bacteria, commonly known as probiotics, also need to eat in order to survive and help control the growth of harmful bacteria in the gastrointestinal tract. Prebiotics are the essential “food” for probiotics. There’s been many discussions regarding those probiotics found in fermented foods such as yogurt, kefir and kimchi, but it should be understood how vital it is to nourish these probiotics with prebiotics. Some prebiotic foods include raw asparagus, cooked onions, bananas and kiwifruit, among others.
Understanding How to Maximize Digestion
When it comes to achieving optimal digestive health, fiber can promote that sought after, comfortable digestion. The best sources of fiber include plant foods. In addition to enjoying those deliciously, colorful fruits and vegetables, make sure to fill up on whole grain foods to get enough fiber. The 2015-20 Dietary Guidelines recommends making half your plate fruits and vegetables and half of all your grains, whole grains. The United Nations called 2016 the International Year of Pulses, yet another name for beans and lentils, which are also rich in fiber. Some foods have compounds known as proteases which help break down protein, easing digestion when eating a hearty meal with meat. For instance, pineapple has a protease called bromelain, kiwifruit contains actinidin and papaya has papain. Another essential that can help maximize digestion which many people overlook is the simple principle of slowing down when you’re eating to make digestion easier. Taking time to properly chew your food is one of the smartest tricks anyone can do in order to optimize digestion.
Understanding How to Get the Gut Back on Track
Many of you may well know that sensation when your digestion is thrown out of whack and “things” get backed up a little. Although you may not have constipation, one can experience bloating and discomfort. In order to get your gut back on its regular track, you should maximize three things: water, exercise, and fiber. When that alone isn’t enough, many men and women can turn to fiber supplements such as psyllium and other bulking agents. Preliminary evidence from a study in New Zealand demonstrated that eating two green kiwifruit a day eases constipation as effectively as fiber supplements. Kiwifruit is an excellent source of fiber, like many fruits, but research affirms that kiwifruit fibers have a higher capacity of holding water, helping in laxation in the colon. Research studies are now underway in Italy and Japan to add to the understanding of kiwifruit as a natural remedy for relieving constipation. It’s a pretty exciting notion that using whole foods over supplements can be all that’s needed to get your digestive health back on track.
Understanding FODMAPs
Irritable bowel syndrome is a gastrointestinal disease estimated to affect 1 in 10 people. In the last few years, those diagnosed with irritable bowel syndrome, or IBS, have found digestive relief following a low FODMAP eating strategy. Certain carbohydrate foods, many of which can be nourishing fruits, vegetables and beans, are saturated in FODMAPs, which stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols, and may not be absorbed by people with sensitive intestines. Subsequently, these can create gas and other uncomfortable symptoms in the colon when bacteria ferment them, triggering irritable bowel syndrome symptoms. To ease IBS symptoms, the FODMAP foods must be removed from the individual’s diet and then later reintroduced in tolerable amounts. Talk to your gastroenterologist or a registered dietitian specializing in the low FODMAP protocol in case you have IBS and are considering trying this diet to improve your digestive health.
Understanding the Link Between the Brain and the GI Tract
You may also have already heard that stress can ultimately affect your digestive health. When some people feel stressed and anxious, their gastrointestinal tract often goes into hyperdrive. Nevertheless, the link between the brain and the GI tract is more than just that. More than 60 percent of our immune cells call the digestive system home. The gut has its own nervous system as well, frequently referred to as “the second mind,” containing more than a million nerve cells. Additionally, around 95 percent of people with IBS also struggle with depression or other mood disorders.
The concept that the gut microbiome can influence mood has become one of the most interesting areas of research today. Studies have revealed that the gut synthesizes significant levels of serotonin, the neurotransmitter that helps calm and relax the body. Adequate vitamin C is required for the gut to turn tryptophan into serotonin.
Scientists are analyzing how modifications to our eating patterns may contribute to an improved and diverse microbial community. Those studying kiwifruit have supplied evidence that consuming two kiwifruit per day (200 mg per day of vitamin C) was associated with optimal blood levels of vitamin C to benefit immune function and well-being. One study demonstrated a 35 percent decrease in mood disbalances based on self-reported perception of an improved mood once the participants consumed kiwifruit. While many different foods, such as oranges and strawberries, can provide vitamin C, SunGold kiwifruit is a particularly rich source of the nutrient.
Now that you’ve understood how to manage and maintain your digestive health better, you can start to make lifestyle changes that can help you support it. The good news is these changes can be simple, delicious and beneficial to your overall wellness. Whether you begin to eat more slowly, build a balanced plate to get more fiber, be sure to consume probiotics and prebiotics, get sufficient water, exercise, or do a bit of each of the tips mentioned above, you’ll feel the difference with better digestive health. Keep your eyes open for further evidence of what creates a healthy gut microbiome, because we’re just digging into the knowledge base of beneficial bacteria. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
There’s something about gastrointestinal issues that makes them difficult to talk about in polite company, which unfortunately leaves many of us suffering one problem or another in silence. “What’s more, gastrointestinal, or GI, diseases are putting an increasing weight on Americans, causing an unprecedented number of clinical visits and hospitalizations than ever before”, stated Stephen Bickston, an American Gastroenterological Association professor of internal medicine at Virginia Commonwealth University.
What are the most prevalent gastrointestinal diseases?
Nevertheless, treatments for gastrointestinal diseases can be as simple as making informed lifestyle modifications or even taking over-the-counter drugs and medications. Peppermint oil and soluble fiber, for instance, has been used to help people with irritable bowel syndrome, or IBS, where a 2008 British Medical Journal study suggested that both of these natural remedies ought to be first-line treatment therapies for IBS. Here’s a rundown of the latest medical knowledge on five of the most common gastrointen.
Acid Reflux
Symptoms of acid reflux, such as heartburn, are among several of the most common digestive discomforts reported by the general population. In a Swedish study, approximately 6 percent of people reported suffering from acid reflux symptoms daily and 14 percent had them at least weekly. Such frequent symptoms may indicate the presence of gastroesophageal reflux disorder, or GERD. Aside from being painful, GERD, or gastroesophageal reflux disorder can damage the esophagus throughout the years or even lead to esophageal cancer.
“Heartburn typically involves a hot or burning sensation which rises up from the center of the abdomen area and to the chest under the breastbone or sternum”, states Michael Gold, a gastroenterologist at MedStar Washington Hospital Center in Washington, D.C. “It might also be accompanied by a sour taste in the mouth, or hypersalivation, in addition to discovering fluid or food out of your mouth, particularly at night time.” Pregnancy, several drugs and medications, as well as consuming alcohol or certain foods can cause heartburn. Children under the age of 12 and a few adults may have GERD without heartburn, instead experiencing asthma-like symptoms, difficulty swallowing, or a dry cough.
Treatment options for acid reflux include drugs and medications that reduce acid levels, like the proton pump inhibitors Aciphex, Nexium, Prevacid, Prilosec, and Protonix, along with the H2 blockers Axid, Pepcid, Tagamet, and Zantac. But taking these drugs and/or medications is not without risk. In 2008, a study found that a proton pump inhibitor can weaken the heart-protective impact of the blood thinner Plavix in patients taking the two drugs/medications together. In severe cases of gastroesophageal reflux disorder, surgeons can tighten a loose muscle found between the esophagus and the stomach, to inhibit the upwards flow of gastric acid. Laparoscopic surgery, which involves small incisions, has been proven to reduce scarring and shorten recovery time in comparison with open procedures.
Diverticulitis
By one estimate, about 3 in 5 Americans older than 70 years of age have the abnormal lumps called diverticula someplace in the wall of their intestinal tract. However, only 20 percent may experience a complication like diverticulitis, inflammation of a pouch, a tear, or an abscess.
Individuals with Crohn’s disease or ulcerative colitis, the two most prevalent inflammatory bowel diseases, complain of abdominal pain and diarrhea and may sometimes experience anemia, rectal bleeding, weight loss and other symptoms. “No definitive tests and evaluations exist for either disease and patients generally endure two primary misdiagnoses”, says R. Balfour Sartor, chief medical adviser to the Crohn’s & Colitis Foundation of America. “With Crohn’s”, he states, “appendicitis, irritable bowel syndrome, an ulcer, or an infection can be incorrectly diagnosed.”
In case diverticulitis does develop, symptoms are most likely to manifest through abdominal pain and potentially fever, however, antibiotics can treat the problem. In severe instances, a tear can result in an abscess, which might result in nausea, vomiting, fever, and intense abdominal tenderness which demands surgical repair. Some healthcare specialists consider that a diet too low in fiber could trigger the gastrointestinal disease, which develops growingly common with age and is most widespread in western societies.
Inflammatory Bowel Disease
Both disorders may emerge from a wayward immune system that leads the body to attack the gastrointestinal tract, or GI tract. Crohn’s disease involves ulcers that could seep deep into the tissue lining at any given section of the GI tract, leading to infection and thickening of the intestinal wall and blockages which may need surgery. Ulcerative colitis, by comparison, interrupts only the colon and rectum, where it also causes ulcers; colitis is characterized by bleeding and pus.
Treating either disease requires beating back, then constantly holding in check, the inappropriate inflammatory response. Both steps are accomplished by means of a combination of prescription anti-inflammatories, steroids and immunosuppressants. Crohn’s patients might also be given antibiotics or other specialized drugs and medications. The current debate stands as to whether Crohn’s disease sufferers benefit if given highly potent treatment therapies early in the course of the gastrointestinal disease instead of escalating potency with time from milder initial treatments, as is traditionally done, clarified Themos Dassopoulos, manager of inflammatory bowel diseases at Washington University at St. Louis. Surgery “cures” ulcerative disorders by simply taking away the colon but signifies that patients will need to wear a pouch, internally or externally, for waste. “Inflammatory bowel disease, or IBD, patients must take particular caution when using NSAIDs, such as aspirin, since these painkillers may cause additional gut inflammation in 10 to 20 percent of individuals, ” states Dassopoulos.
Constipation
The fact that Americans spend $725 million annually on laxatives indicates that trying to unclog the nation’s plumbing, so to speak, is a national pastime. But overuse of stimulant laxatives, which cause the intestines to contract rhythmically, can make the gut more reliant on these, requiring more of them and finally rendering the aid ineffective. First, a little bit of clarification on the frequency of your flushing: “There is no need to worry about having a daily bowel motion; anywhere between three times a day and three times per week is normal”, says Sandler.
“However, if you are having discomfort and can not make your bowels move, try out an over-the-counter remedy such as milk of magnesia’,’ he states. And should you have attempted laxatives or not, going a week without a bowel movement is a very good reason to see the doctor, ” says Sandler. Constipation, hard stools, and straining could result in hemorrhoids or an anal fissure. Constipation is best avoided through regular exercise and a diet high in fiber from whole grains, fruits, and vegetables. To elderly folks, that are inclined to become constipated more frequently: Be sure you’re hydrating properly and conscious of any drugs and medications which may be causing your bowel movements to be backed up.
Gallstones
Just a quarter of people with gallstones typically require treatment. That’s fortunate, because every year nearly 1 million Americans are diagnosed with these small pebbles, which are largely made of cholesterol and bile salts. Eliminating these typically requires removal of the gallbladder, one of the most frequent surgeries in the United States.
“Gallstones can get blamed for symptoms caused by other, more elusive culprits, such as irritable bowel syndrome”, states Robert Sandler, chief of the division of gastroenterology and hepatology together with the University of North Carolina School of Medicine. An ultrasound evaluation may pick them up while missing the real issue. “If you’re told you’ve got to have gallstones out however they aren’t bothering you, get a second opinion”, he advises. Removal may be mandatory when the stones instigate infection or inflammation of the gallbladder, pancreas, or liver. This can happen if a stone going out of the intestine becomes trapped, blocking the flow of bile, at the ducts between the liver and the small intestine.
The pain of a gallstone lodged at a duct normally comes on quickly at the right upper abdomen, between the shoulder blades, or beneath the right shoulder,� and also means a visit to the ER is necessary, as may fever, vomiting, nausea, or pain lasting more than five hours. Gallbladder removal may be accomplished laparoscopically and more recently has been completed with no external incision by going through your mouth or vagina. Obesity can also be a risk factor for gallstones, and it is theorized that they increase due to a lack of fiber and an excessive amount of fat from the western diet. Losing weight then regaining it also seems to set the stage for the common gastrointestinal disease. In a 2006 study of men, the more frequent the weight cycling and the bigger the amount of pounds fall and are regained, the larger the chances of developing gallstones. Women, in particular those people who are pregnant or using birth control pills, face an increased risk of developing gallstones as well.
We will continue to discuss the common issues affecting the gastrointestinal tract, or GI tract, including the colon as well as rectum and anal problems, in the following series of articles. The 5 common gastrointestinal diseases mentioned above can manifest pain and discomfort as well as a variety of other symptoms if left untreated. Be sure to seek proper medical attention. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine