Vibrant America is at the forefront of modern medicine and is a leader in autoimmune diagnostics. Vibrant America has the ability and technology to get high-quality, accurate test results down to the peptide level.
One of the many tests we utilize from Vibrant America at Injury Medical & Chiropractic Clinic is Food Sensitivity. With this test, we are able to analyze 96 of the most common foods that are consumed. This is important because food sensitivities can occur hours or days after the food is consumed. Many individuals who suffer from digestive orders, migraines, weight gain, and inflammation might not realize it is from food sensitivities.
Why test for Food Sensitivity?
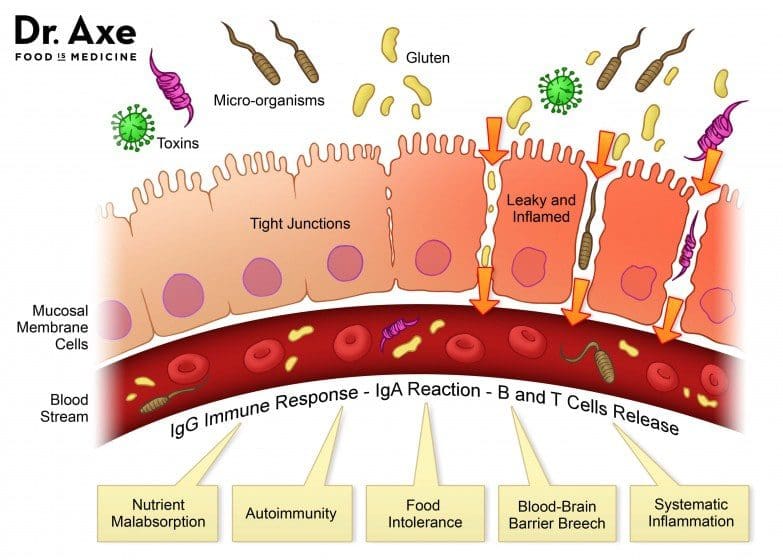
Not only do food sensitivities leave you with uncomfortable side effects days after ingestion, but they are damaging your gut. In a healthy gut, the intestinal lining will provide immunity to food antigens. The food we eat is not supposed to cross the intestinal barrier. However, in an unhealthy gut, the intestinal lining becomes damaged due to inflammation and an under abundance of healthy flora. This allows food particles to pass through into the bloodstream which then causes an IgG antibody response. This is commonly referred to as a “leaky gut”. This can result in further inflammation and can contribute to some diseases.
At Injury Medical, we want all of our patients to feel their best. On top of chiropractic care, we also offer functional medicine. When a patient mentions to us that they are having symptoms correlated to “leaky gut” such as abdominal pain, bloating, gas, skin itchiness, rashes like eczema, nausea, vomiting, joint pain, muscle stiffness, or feeling weak, we recommend running a food sensitivity panel.
How it works:
Once we sit down and have a detailed conversation, we send you to the labs with a “kit”. This “kit” provides the phlebotomist with everything they need in order to draw blood for the tests we order.
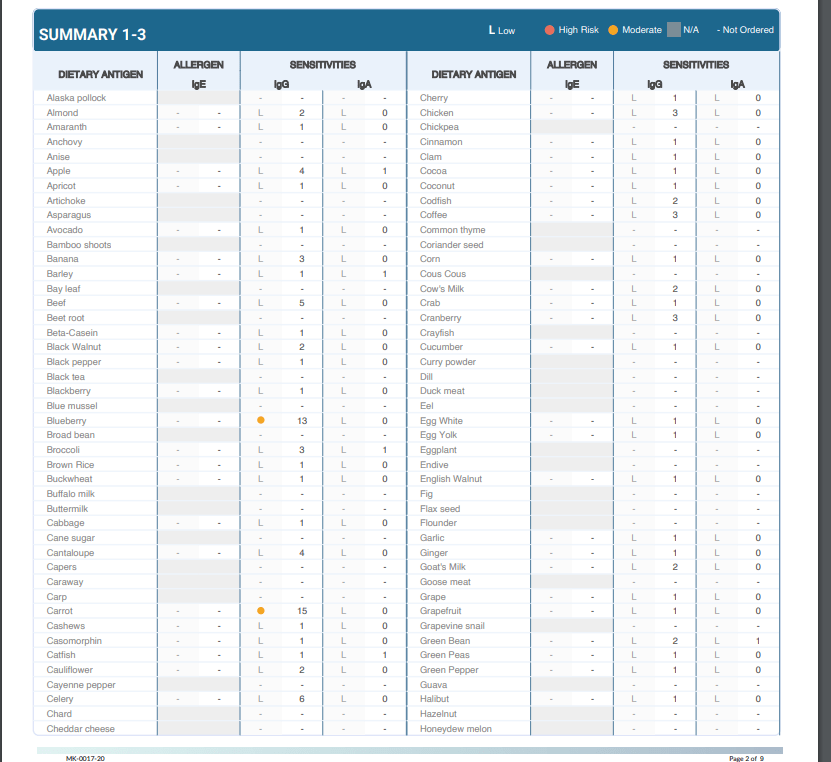
From here, the blood gets sent to Vibrant America. The blood is then examined all the way down to the peptide level. This allows a team of clinicians to discover the IgG and IgA antibody numbers in reaction to 96 foods (including dairy, meat, seafood, fruits, vegetables, grains, nuts, etc.).
Next, the results are sent back to us at Injury Medical Clinic. Dr. Jimenez and I ( Kenna Vaughn, Senior Health Coach), study these results to determine a proper treatment protocol. In addition to this, we have a team of clinicians that review each case with us, in order to fully understand what each result looks like and how to best approach it with the patient’s specific lifestyle.
Below is an example of how a patients test results would look:
Why this works
As mentioned above, food sensitivities have a delayed response. This testing works because it allows us to see what foods are responsible for the symptoms/reactions without the patient having to do an elimination diet.� With these results, the patient can start to make adjustments to their diet with our help in order to start feeling better and reducing their symptoms. The key to a healthy life is a healthy gut.
No one should have to live with uncomfortable symptoms or pain. If you or someone you know is experiencing these symptoms, come into Injury Medical Clinic where we can assess your needs and help you get on track to feeling better! – Kenna Vaughn, Senior Health Coach
Disclaimer: It is important to remember that food sensitivity testing and food allergy testing are not the same. Food allergies involve an IgE antibody and are an immediate reaction and can occur within minutes.
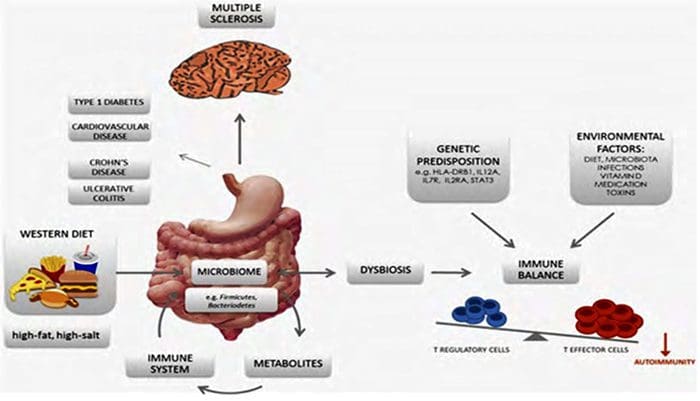
The phrase, �You are what you eat� implies that the way we are defines us as the food we all consumed. However, our gut tells us otherwise as the food we eat, may in fact be leading us to obesity. Our gut plays a role in our overall health, when we eat good food our gut is happy and when we eat bad food our gut will tell us by fighting off the bad food. A recent study showed us that the bacteria in our gut produce amyloid and lipopolysaccharides. These two microbiomes seem to show us that together, with proper dieting that these microbiomes can prevent Alzheimer�s Disease.
As the microbiomes and the bacteria that co-exist in our gut, there are the two most predominant groups that have also played a key role in our lifestyle: gram-positive Firmicutes and gram-negative Bacteroidetes- both play a huge role in obesity. Firmicutes are bad bacteria that lead us to obesity. When we eat processed food and sugars, our body starts to crave it more, thus leading us to be overweight.
Junk Food
When we eat junk food, all that sugar and fat are feeding the Firmicutes. Firmicutes thrive on sugar since our bodies need it and it can be both good or bad While Bacteroidetes are the good bacteria that leads us to a healthy gut. Bacteroidetes are in the stomach regions as well as the Firmicutes. These two predominant bacteria groups tell us that the food we eat can actually affect our bodies when we eat bad foods or good foods.
However, Dr. Kristen Senella mentioned that we all have a different balance of Firmicutes and Bacteroidetes since we are all different shapes and sizes. Depending on our health and food lifestyle, we can have either a low Firmicutes and a high Bacteroidetes or a high Firmicutes and a low Bacteroidetes. Plus, having either a high or low count of Firmicutes can lead to weight gain or weight loss; depending on which healthy lifestyle and exercise regime you are following.
Gram-Positive
Gram-positive bacteria will appear blue or violet, while gram-negative bacteria will appear red or pink under the microscope. When studying the gut and the bacteria groups that it is hosting, scientist use mice to study how their guts react to different diets they are put through so that way we, as humans, can take either pills to help our bodies maintain a healthy lifestyle or to read and do our own research. One group is fed in a healthy lifestyle and doesn�t experience diseases or ailments that we face. And the other group is fed with a bad lifestyle where they are prone to many of the diseases and fatigue as their life span is shortened very quickly. In order for us to actually maintain a healthy lifestyle and importantly feel good is to make sure our Firmicutes are not too dangerously low, but we can control it with probiotics.
Probiotics
Probiotics can vary from yogurt, fermented vegetables, kombucha, and miso. But there are certain companies that also reign supreme in the probiotic market. Activia yogurt and Yakult are two of the most well-known companies that use the live microorganisms to help us maintain a healthy lifestyle as well as keeping our gut�s microbiome in check. When we have some sort of probiotic foods in our system, we are preventing certain ailments and diseases going out of control. Like our cholesterol, blood pressure, being lactose intolerant, or recurring abdominal pains.
When we mix probiotics into our food when we are trying to maintain a healthy lifestyle, we can see a vast improvement in how we have more energy, we feel full that we don�t have to overeat or mindless snacking, and overall we feel good in our gut as we go through our daily routine. From 2007 to now, roughly 3.9 million Americans use probiotics to maintain a healthy gut, however, those probiotics are just a fraction of what the six types of foods that can help maintain a healthy gut microbiome to help support a healthy lifestyle.
Healthy Lifestyle
For instance, a good healthy lifestyle is eating your basic food groups; whether it be plant-based or omnivorous, as well as, exercising a couple of times out of the year. A bad healthy lifestyle is eating processed food and not exercising, which leads to obesity and cardiac arrest. Depending on the person and the efforts that they are willing to maintain a healthy lifestyle, they can achieve longevity by taking care of their gut first and foremost.
Family In Kitchen Making Morning Breakfast Together
Protein
Let�s start with protein. Protein can vary with lean meats like chicken and beef or plant-based like beans, legumes or tofu. Any of these types of protein can help our bodies by making us make our muscles grow, but also control the bacteria in our guts. Next up is fats. Fats can vary like good and bad bacteria. There are good fats like fish, nuts, olive oil, and avocado; as well as, bad fats like butter, lard, and fatty foods. Granted that we can overindulge on the trans fats as there are many fast-food chains, but we can moderate ourselves to not eat out at fast food joints all the time.
Yes, they are cheap and easy to access, however now and days, we as humans are now cooking more in our homes and meal prepping our meals to be healthier. Digestible and Non-Digestible Carbohydrates are mostly starch, sugars, and fibers. These two food groups can make our gut feel happy or upset depending on the food we consume. Sugars, starches, and fibers help our bodies by feeling full with the starches, the fibers help our bowel movements in case our gut feels bloated, and the sugars gives us microburst of energy for our fast-paced lives.
Fermented & Polyphenols
The last two food groups are fermented food and Polyphenols. Both of these food groups have amazing properties since we see them everywhere in the food market, hiding in plain sight. Fermented foods like yogurt and kimchi are a few examples of ways of keeping our guts happy and stopping many diseases. Polyphenols are antioxidant foods like dark chocolate, berries, dark greens, and certain fruits. These help our gut curb that sugar hunger and all in all taste really good.
All in all, our gut microbiomes are important to us and our overall health as we all try to maintain and achieve a healthy lifestyle. The phrase �we are what we eat� still implies to all of us, however, it is up to us to actually put in the work and constantly try out different foods to make sure that our gut is still functioning properly. No matter which diet you choose, pick one that will work with your body and your gut since we all are made differently. But our gut should be the first thing that we should listen to.
Many supermarkets have started offering their shoppers a choice in produce: organic or conventionally farmed. This can leave many wondering just what the difference is.
The truth is, both foods taste the same � or very close. Both have the same vitamins, minerals, and other nutrients, so what is the big difference?
It comes down to two major areas: safety and nutrition. That is what consumers need to understand when they are trying to make a decision on whether to purchase foods that have been conventionally farmed, or foods that are natural.
What Is �Organic�?
This is a misused word but the true meaning is that the term refers to how food is grown and processed. Organic farming is intended to encourage water and soil conservation as well as reduce pollution.
This type of farming does not use chemicals for controlling weeds, eliminating insects, or fertilizing. Most of the methods are completely natural. For instance, a farmer may use natural fertilizers to enrich the soil, strategically placed plants to control insects, and mulch or crop rotation to control weeds.
Organic Vs. Conventional Foods
Conventionally farmed products will often use chemicals for insect control and weed control. They often use some type of processing on their foods.
The fertilizer used in planting often has chemicals. The foods may even be genetically modified. Animals may be injected with steroids and hormones which can cause unpleasant or even harmful side effects.
These types of foods do not use any chemicals, they are not genetically modified, and they are not injected with antibiotics or steroids. The food has been very minimally processed � if at all.
There are no additives that don�t belong and could be potentially harmful. These foods are safer for human consumption and they are typically more nutritious.
How To Identify Organic Foods
In the United States, a food or product that is labeled as organic is required to be certified by the U.S. Department of Agriculture (USDA). The USDA has a certification program for natural growers and it has a set of very stringent standards that the product or food must meet.
There are some exemptions. For instance, a producer who does not sell more than $5,000 annually just in organic foods is not required to get the certification although they do have to adhere to the USDA�s stringent requirements for organic foods.
When a food carries the USDA Organic label, it means that it meets the requirements. While natural producers are not required to put the label on their products, many do.
The labeling varies, depending on the type of food. Single ingredient foods like eggs, vegetables, and fruits are considered to be 100 percent natural and are allowed to carry the USDA seal.
Foods that contain two or more ingredients, like breakfast cereal, are still allowed to use the USDA seal, but also must include the following information:
Organic � The product must be 95 percent organic or greater in order to be able to use this term
100 percent organic � The product must be completely organic or all of its ingredients must be natural
Made with organic ingredients � The product contains no less than 70 percent natural ingredients
If the product has less than 70 percent natural ingredients, they are not allowed to use the word �organic� anywhere on their product labels.
Health Benefits Of Natural Foods
The greatest health benefit of natural foods is what it does not provide. Organic growers do not use synthetic pesticides to protect their crops from disease, insects, and molds. This means that the food itself has never been touched by these chemicals.
Natural foods also do not have the food additives that conventional foods often do. They are free from artificial sweeteners, flavorings, and colorings as well as preservatives and monosodium glutamate. This means eating natural means that you aren�t putting those chemicals into your body. Plus, many people say that organic foods simply taste better.
If you have further questions or concerns about your particular diet, please ask us! Our Doctor of Chiropractic can help guide you toward a more healthy life, including the foods you consume.
Injury Medical Clinic: Accident Treatment & Recovery
Food:�Genes that determine illness are triggered by what we put into our bodies, literally what we eat. Our cells are literally created out of the foods we put into our bodies. Like most people do, we are likely eating nutrient-poor foods that create damaged dysfunctional cells. When we learn to eat foods that nourish the body, our cells repair themselves, and the new cells created will be optimal functioning cells.
Unhealthy foods create chronic inflammation, which is destructive to the body. Inflammation is normally the body�s healthy response to injury or infection. However, when inflammation becomes chronic, from constant assault on the gut by consuming the wrong foods, inflammation becomes the cause of destructive diseases, i.e. Lupus, Rheumatoid Arthritis, Colitis and other inflammatory diseases.
Disclosure
Terry Wahls, MD disclosed no relevant financial relationships with any commercial interest.
The two routes by which diet can influence our health:
(A) the metabolism of our cells and
(B) the population of our gut microbiota.
Paolo Riccio, and Rocco Rossano ASN Neuro
2015;7:1759091414568185
Copyright � by SAGE Publications Inc, or the American Society for Neurochemistry, unless otherwise noted.
Manuscript content on this site is licensed under Creative Commons Licenses.
1. Review of MS patient survival on a Swank low saturated fat diet. Nutrition. 2003 Feb;19(2):161-2. Review.
2. Effect of low saturated fat diet in early and late cases of multiple sclerosis. Lancet. 1990 Jul 7;336(8706):37-9.
3. Multiple sclerosis: twenty years on low fat diet. Arch Neurol. 1970 Nov;23(5):460-74
Low-Fat, Plant-Based Diet In Multiple Sclerosis: A Randomized
Controlled Trial
This was a randomized-controlled, assessor- blinded, one-year long study
1. Voitk AJ, Echave V, Feller JH, et, al: Experience with elemental diet in the treatment of inflammatory bowel disease. Is this primary therapy? Arch Surg, 1973;107: 329-333.
2. Tim LO, Odes HS, Duys PJ, et al. The use of an elemental diet in gastrointestinal diseases. S Afr Med J,1976;50: 1752-1756
3. Zoli G, Care? M, Parazza M et al, A randomized controlled study comparing elemental diet and steroid treatment in Crohn’s disease. Aliment
Pharmacol Ther. 1997 Aug;11(4):735-40.
4. Zachos M, Tondeur M, Griffiths AM. Enteral nutritional therapy for induction of remission in Crohn�s disease. Cochrane Database Syst Rev, 2007
January 24;(1)
5. Podas T, Nightingale JM, Oldham R, et al, Is rheumatoid arthritis a disease that starts in the intestine? A pilot study comparing an elemental diet with
oral prednisolone. Postgrad Med J. 2007 Feb;83(976):128-31
6. Podas T, Nightingale JM, Oldham R, et al, Is rheumatoid arthritis a disease that starts in the intestine? A pilot study comparing an elemental diet with
oral prednisolone. Postgrad Med J. 2007 Feb;83(976):128-31
Exclusion Diets
Eliminated specific protein sources � RA Sx ?
Raw vegan, vegan and gluten free vegan
Systematic review of 14 RCTs
Dietary benefits uncertain
Small studies with risk of bias
1. Kjeldsen-Kragh J, Haugen M, Borchgrevink CF, Laerum E, Eek M, Mowinkel P, Hovi K, F�rre O. Controlled trial of fasting and one-year vegetarian diet in rheumatoid arthritis. Lancet. 1991 Oct 12;338(8772):899-902.
2. Kjeldsen-Kragh J, Haugen M, Borchgrevink CF, F�rre Vegetarian diet for patients with rheumatoid arthritis–status: two years after introduction of the diet. Clin Rheumatol. 1994 Sep;13(3):475-82
3. McDougall J, Bruce B, Spiller G, et al, Effects of a very low-fat, vegan diet in subjects with rheumatoid arthritis. J Altern Complement Med. 2002 Feb;8(1):71-5
4. Hafstro?m I, Ringertz B, Spa?ngberg A, et. al, A vegan diet free of gluten improves the signs and symptoms of rheumatoid arthritis: the effects on arthritis correlate with a reduction in antibodies to food antigens. Rheumatology (Oxford). 2001 Oct;40(10):1175-9.
5. Hagen KB, Byfuglien MG, Falzon L, et, al. Dietary interventions for rheumatoid arthritis. Cochrane Database Syst Rev. 2009 Jan 21;(1):
6. Smedslund G, Byfuglien MG, Olsen SU, et. al, Effectiveness and safety of dietary interventions for rheumatoid arthritis: a systematic review of
randomized controlled trials. J Am Diet Assoc. 2010 May;110(5):727-35
Exclusion Diets
Atopic dermatitis improved n=20
UC � fewer symptoms n=18
Crohn�s food sensitivities identified in half n=42
Antibody cross-reactivity between myelin oligodendrocyte glycoprotein and the milk protein butyrophilin in MS – Inducing antibodies reacting with myelin oligodendrocyte glycoprotein (MOG) and Cerebellar peptides
Liquid cow milk (not cheese) and MS prevalence was highly correlated (rho = 0.836) across 27 countries and 29 populations.
�By eliminating lectins, which adversely influence both enterocyte and lymphocyte structure and function, it is proposed that the peripheral antigenic stimulus (both pathogenic and dietary) will be reduced and thereby result in a diminution of disease symptoms in certain patients with RA.�
1. Lindeberg, S., Jo?nsson, T., Granfeldt, Y. et al. Diabetologia (2007) 50: 1795. doi:10.1007/s00125-007-0716-y
2. O?sterdahl M, Kocturk T, Koochek A, Wa?ndell PE. Effects of a short-term intervention with a paleolithic diet in healthy volunteers. European Journal of
Clinical Nutrition. 2007;62(5):682�685. doi:10.1038/sj.ejcn.1602790.
3. Jo?nsson T, Granfeldt Y, Ahre?n B, et al. Beneficial effects of a Paleolithic diet on cardiovascular risk factors in type 2 diabetes: a randomized cross-over pilot study. Cardiovascular Diabetology. 2009;8:35. doi:10.1186/1475-2840-8-35.
4. Frassetto LA, Schloetter M, Mietus-Synder M, Morris RC, Sebastian A. Metabolic and physiologic improvements from consuming a paleolithic, hunter- gatherer type diet. European Journal of Clinical Nutrition. 2009;63(8):947�955. doi:10.1038/ejcn.2009.4.
5. Halberg N, Henriksen M, So?derhamn N, et. al, Effect of intermittent fasting and refeeding on insulin action in healthy men. J Appl Physiol (1985). 2005 Dec;99(6):2128-36.
6. Ryberg M, Sandberg S, Mellberg C, et al. A Palaeolithic-type diet causes strong tissue-specific effects on ectopic fat deposition in obese postmenopausal women. Journal of Internal Medicine. 2013;274(1):67�76. doi:10.1111/joim.12048.
7. Ruiz-Nu?n?ez B, Dijck-Brouwer DAJ, Muskiet FAJ. The relation of saturated fatty acids with low-grade inflammation and cardiovascular disease. The Journal of Nutritional Biochemistry. January 2016. doi:10.1016/j.jnutbio.2015.12.007.
8. Otten J, Stomby A, Waling M, et al. Benefits of a Paleolithic diet with and without supervised exercise on fat mass, insulin sensitivity, and glycemic control: A randomized controlled trial in individuals with type 2 diabetes. Diabetes/Metabolism Research and Reviews. January 2016. doi:10.1002/dmrr.2828.
9. Konijeti GG1, Kim N, Lewis JD, Groven S, Chandrasekaran A. Efficacy of the Autoimmune Protocol Diet for Inflammatory Bowel Disease. Inflamm Bowel Dis. 2017 Aug 29. doi: 10.1097/MIB.0000000000001221.
10. Spreadbury I. Comparison with ancestral diets suggests dense acellular carbohydrates promote an inflammatory microbiota, and may be the primary dietary cause of leptin resistance and obesity. Diabetes Metab Syndr Obes. 2012;5:175-89.
11. Eaton SB, Konner MJ, Cordain L. Diet-dependent acid load, Paleolithic nutrition, and evolutionary health promotion. Am J Clin Nutr. 2010;91:295-7. Andersson A, et al. Whole?grain foods do not affect insulin sensitivity or markers of lipid peroxidation and inflammation in healthy, moderately overweight subjects. J Nutr.2007 Jun;137(6):1401?7.
12. Tighe P, et al. Effect of increased consumption of whole ? grain foods on blood pressure and other cardiovascular risk markers in healthy middle?aged persons: a randomized controlled trial. Am J Clin Nutr. 2010 Oct;92(4):733?40.
13. Brownlee IA, et al. Markers of cardiovascular risk are not changed by increased whole?grain intake: the WHOLEheart study, a randomised, controlled dietary intervention. Br J Nutr. 2010 Jul;104(1):125?34.
14. Masters RC, et al. Whole and refined grain intakes are related to inflammatory protein concentrations in human plasma. J Nutr. 2010 Mar;140(3):587?94.
15. Katcher HI, et al. The effects of a whole grain-enriched hypocaloric diet on cardiovascular disease risk factors in men and women with metabolic syndrome. Am J Clin Nutr. 2008 Jan;87(1):79?90.
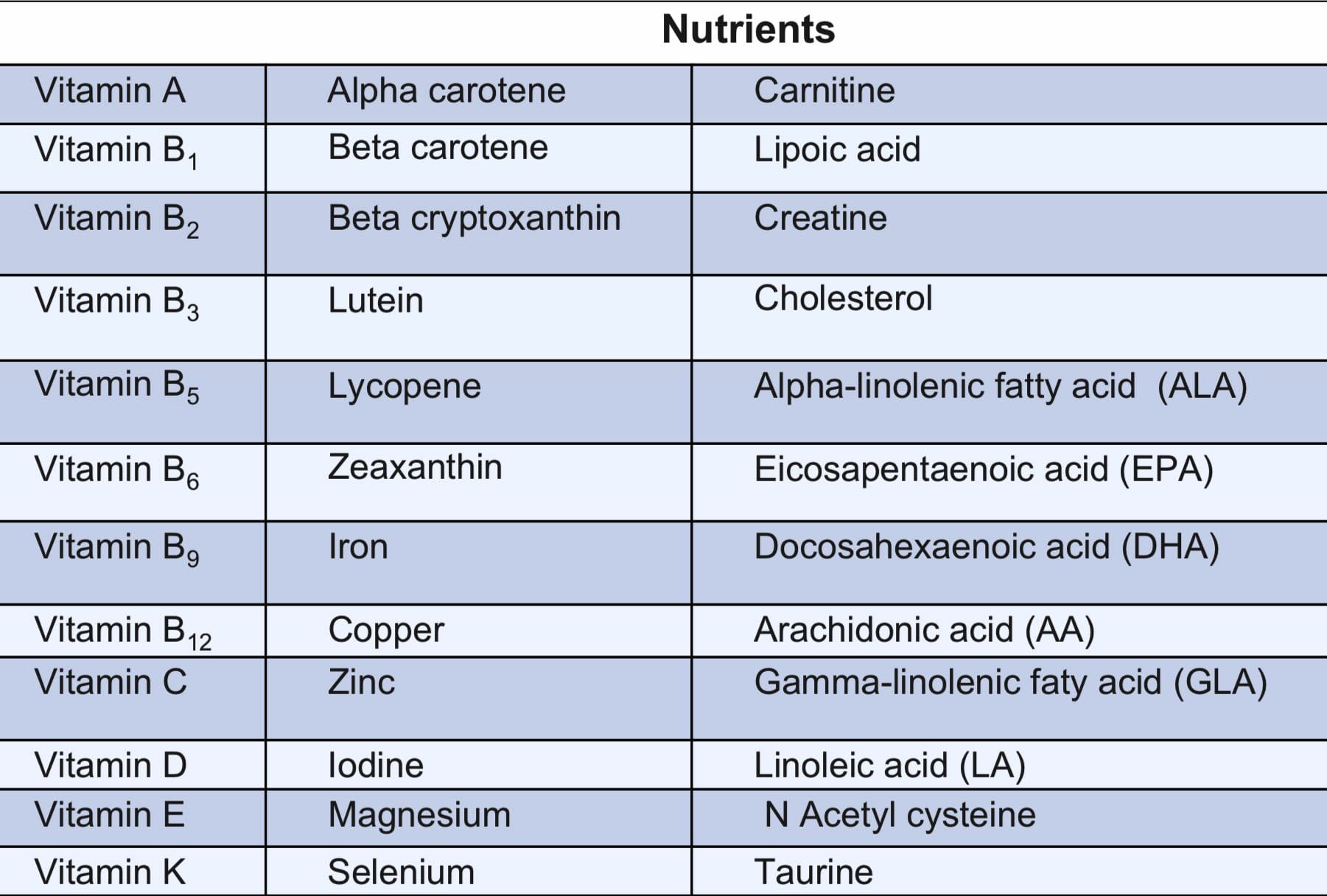
Nutrient Triage
Low micronutrient intake may accelerate the degenerative diseases of aging through allocation of scarce micronutrients by triage.
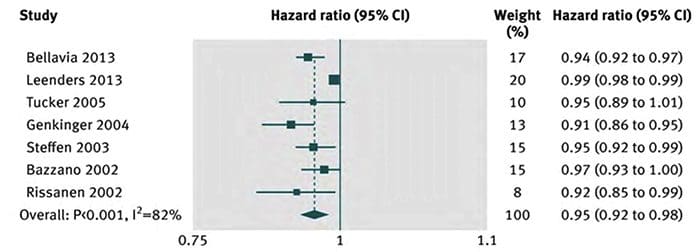
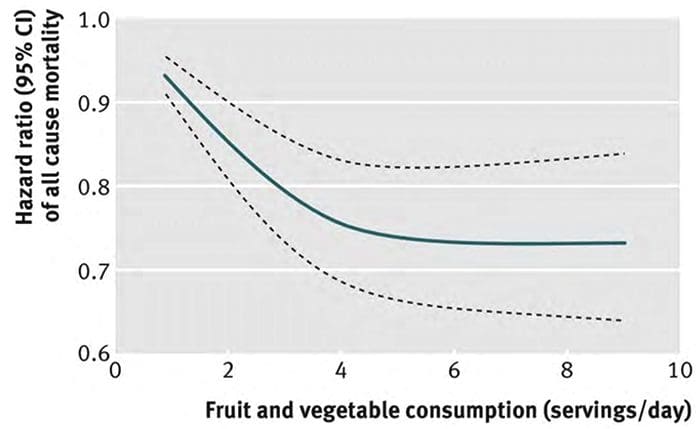
Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose response meta-analysis of prospective cohort studies.
16 studies – 833,234 participants
Risk Of All Cause Mortality Associated With Servings/Day Of Fruit & Vegetables
Dose-Response Relation Between Fruit & Vegetable Consumption & Risk Of All Cause Mortality
BMJ. 2014; 349: g4490.
1. Neuroprotective Effect of Brassica oleracea Sprouts Crude Juice in a Cellular Model of Alzheimer’s Disease. Med Cell Longev.2015;2015:781938
2. Learning and memory promoting effects of crude garlic extract. Indian J Exp Biol.2013 Dec;51(12):1094-100.
3. Enhancement of the neuroprotective activity of Hericium erinaceus mycelium co-cultivated with Allium sativum extract. Arch Physiol Biochem.2015 Feb;121(1):19-25.
4. Mori K, Obara Y, Hirota M, Azumi Y, Kinugasa S, Inatomi S, Nakahata N. Nerve growth factor-inducing activity of Hericium erinaceus in 1321N1 human astrocytoma cells. Biol Pharm Bull. 2008 Sep;31(9):1727-32.
5. Lee DH, Kim HW. Innate immunity induced by fungal ?-glucans via dectin-1 signaling pathway. Int J Med Mushrooms. 2014;16(1):1-16.
6. Akramiene D, Kondrotas A, Didziapetriene J, Kevelaitis E Effects of beta-glucans on the immune system. Medicina (Kaunas).2007;43(8):597-606.
7. Lai PL, Naidu M,Sabaratnam V,Wong K, DaviP, Kuppusamy UR, Abdullah N, Malek SN. Neurotrophic properties of the Lion’s mane medicinal mushroom, Hericium erinaceus (Higher Basidiomycetes) from Malaysia Int J Med Mushrooms.2013;15(6):539-54.
8. Phan CW, David P, Naidu M, Wong KH, Sabaratnam V. Therapeutic potential of culinary-medicinal mushrooms for the management of neurodegenerative diseases: diversity, metabolite, and mechanism. Crit Rev Biotechnol.2015;35(3):355-68.
9. Scientifica (Cairo).2016;2016:3109254.
10. Berry antioxidants: small fruits providing large benefits. J Sci Food Agric.2014 Mar 30;94(5):825-33
11. Dietary and plant polyphenols exert neuroprotective effects and improve cognitive function in cerebral ischemia. Recent Pat Food Nutr Ag. 2013 Aug;5(2):128-43.
12. The impact of fruit flavonoids on memory and cognition. Br J Nutr.2010 Oct;104 Suppl 3:S40-7. d
13. Grape juice, berries, and walnuts affect brain aging and behavior. J Nutr. 2009 Sep;139(9):1813S-7S.
14. Fruit polyphenolics and brain aging: nutritional interventions targeting age-related neuronal and behavioral deficits. Ann N Y Acad Sci.2002 Apr;959:128-32.
15. Reversing the deleterious effects of aging on neuronal communication and behavior: beneficial properties of fruit polyphenolic compounds. Am J Clin Nutr.2005 Jan;81(1 Suppl):313S-316S.
16. Krikorian R, Shidler MD, Nash TA, Kalt W, Vinqvist-Tymchuk MR, Shukitt-Hale B, Joseph JA. Blueberry supplementation improves memory in older adults. J Agric Food Chem.2010 Apr 14;58(7):3996-4000.
17. Funding for the studies was provided by the US Highbush Blueberry Council, the National Institute on Aging, and Wild Blueberries of North America. Dr. Krikorian has disclosed no relevant financial relationships.
18. Lobo GP Amengual J, Baus D, Shivdasani RA Genetics and diet regulate vitamin A production via the homeobox transcription factor ISX. J Biol Chem.2013 Mar 29;288(13):9017-27
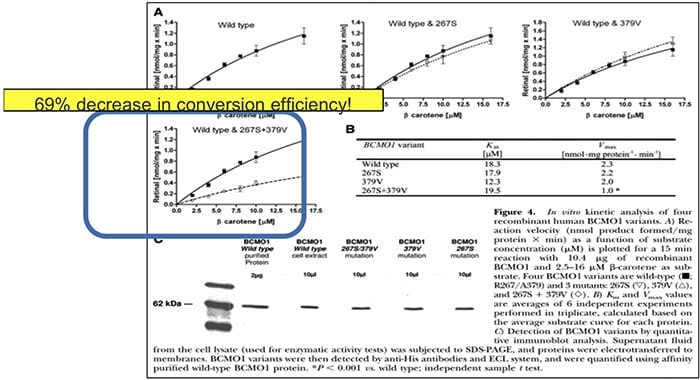
?-carotene Is Not Retinol (Vitamin A)
?-Carotene is converted to vitamin A in the intestine by the enzyme ?-carotene-15,15′- monoxygenase (BCMO1) to support vision, reproduction, immune function, and cell differentiation.
Considerable variability in BCMO1 exists and can effect individual vitamin A status
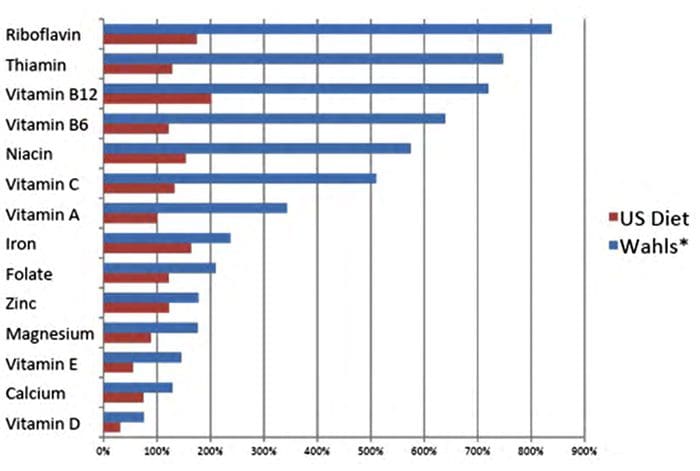
Nutritional Adequacy (%RDA) US Diet Vs. Study Diet
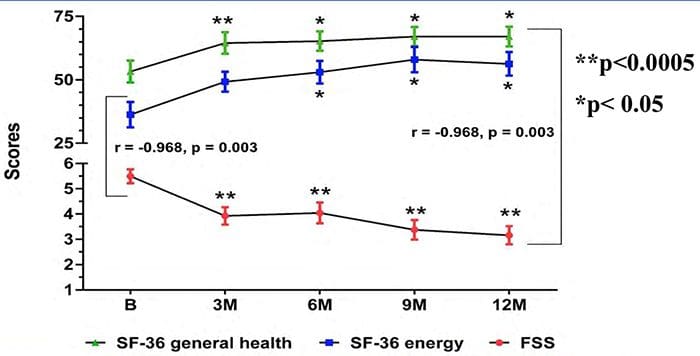
Multimodal Intervention Improves Quality Of Life
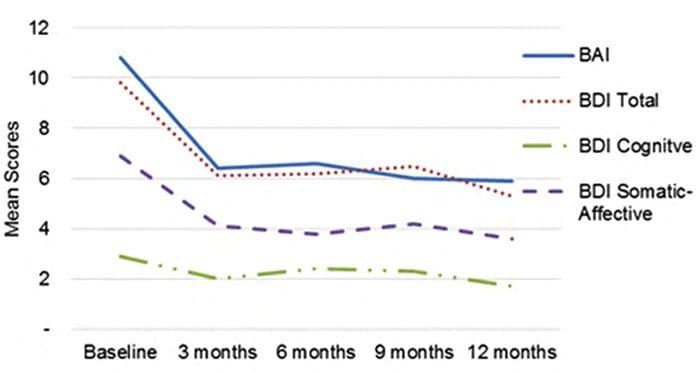
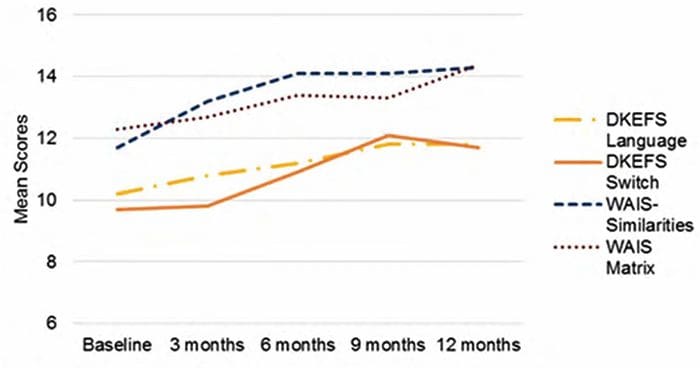
Mood & Cognition
In the setting of progressive MS Improved thinking ability and reduced anxiety and reduced depression
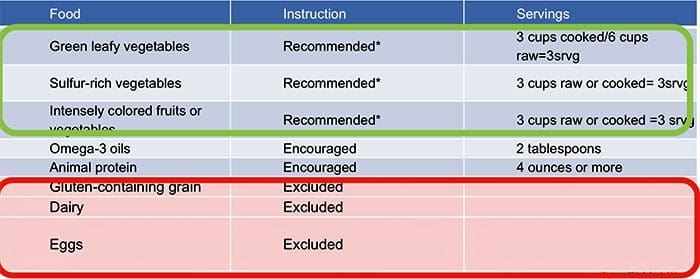
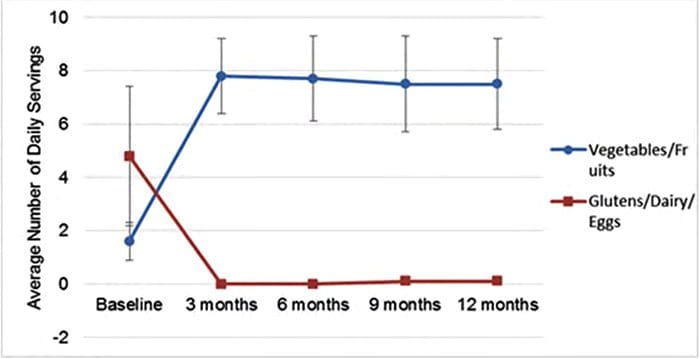
Average daily servings of the study diet recommended (vegetables/fruits) and excluded (gluten/dairy/eggs) foods p < 0.01 difference from baseline to 12 months
Average Scores On The Mood Measures At Each Study Visit
Average Scores On The DKEFS & WAIS Sub-Scales At Each Study Visit.
Relapsing Remitting MS
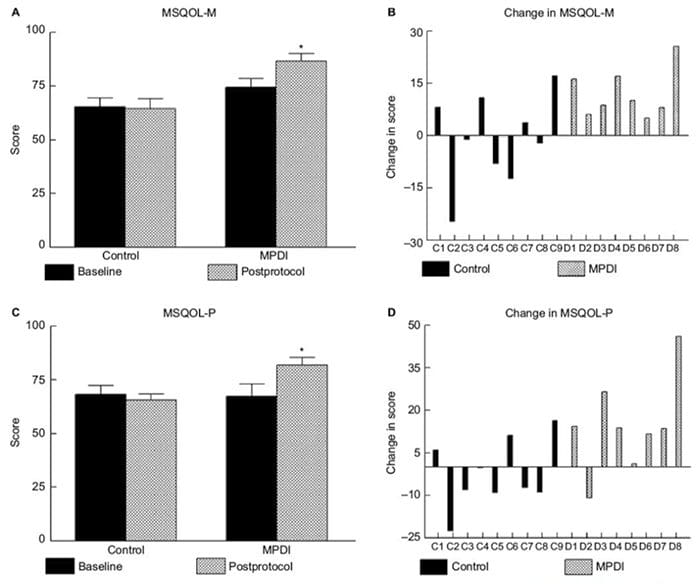
Reduce Fatigue
?Mental & Physical QoL 16% (> 5 points)
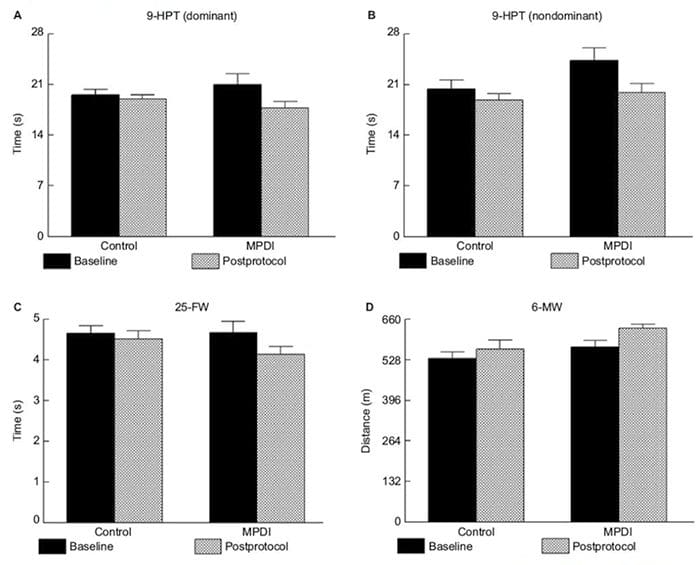
Improved Motor Function
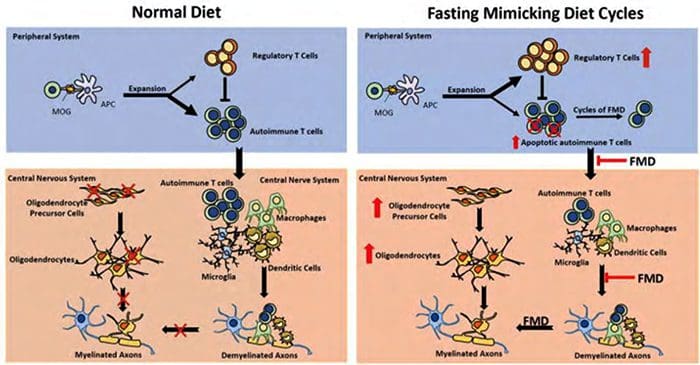
A Simplified Model Of FMD?Mediated Effects On Glucocorticoid, Immune Suppression & Oligodendrocyte Regeneration & Differentiation In MS
N=60 6 Month Human Clinical Trial
FMD 100 ml broth, 1 T flax oil tid, 200 � 350 Kcal, Plus enema as needed 7 days Mediterranean diet
Ketogenic(KD) 160gmfatm<100gPro,<50g CHO
Usual diet
Change at 3 month of (k) overall quality of life, (l) change in health, (m) physical health composite, and (n) mental health composite. The dotted line represents a threshold that is thought to be clinically important
The Two Routes By Which Diet Can Influence Our Health:
(A) the metabolism of our cells and
(B) the population of our gut microbiota.
Paolo Riccio, and Rocco Rossano ASN Neuro
2015;7:1759091414568185
Copyright � by SAGE Publications Inc, or the American Society for Neurochemistry, unless otherwise
noted. Manuscript content on this site is licensed under Creative Commons Licenses.
Gut Brain Immune Axis
Gut microbiota influence the brain and immune system balance
Diet influences the microbiome strongly
Exercise, sleep, stress level also important
Changes in the colon mucosa every early in the disease process
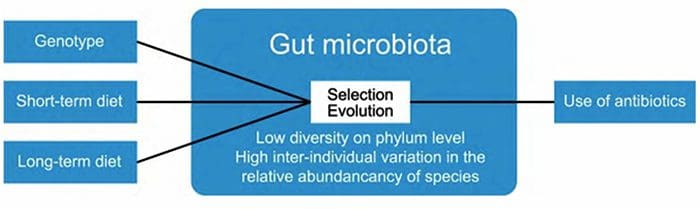
The composition of gut microbiota is influenced by multiple factors, such as diet and host genotype. Within the gut, ecological processes such as selection and evolution take place. The use of antibiotics reduces the numbers and diversity of gut microbiota.
Higher quality diet (food), stress reduction, movement � are relatively safe with large favorable benefits for all cause mortality
3 month trial of a grain free, dairy free, sugar free vegetable rich (or gluten free vegetarian) diet is relatively safe with potential for many favorable benefits
Dietary Approaches to Treating MS Related Fatigue RRMS & Fatigue Study funded by NMSS [email protected] Live within 500 Miles of Iowa City, Iowa [email protected]
The late nineties were an era of strong debate on the issue of genetically modified food and organisms in the UK. Controversy surrounded both the scientific and political aspects of GM, with government advisory bodies being accused of biased behavior and concerns being raised over the ethical issues of the science behind GM. At lunch, a bowl of good vegetable-based soup (home-made or Simply Organic�s naturally!) counts for another 1 or 2 portions and each one of our Pure & Pronto ready meals counts for a whopping 3 portions. Add a piece of fruit or two during the day and a salad or veg in the evening and you�re already at 6 or 7 portions of fruit and veg for the day � well above the 5.
At the same time there was substantial media coverage of scientific advances including cloning and the BSE crisis that fueled public concern into the governance of such issues. It was in this climate of debate, concern and contestation that the UK Government launched GM Nation, a national debate about the future of genetically modified crops and food in the UK.
Objectives: Genetically Modified Foods
The stated aims of the GM Nation debate were twofold: to promote an innovative, effective and deliberative program of debate on GM issues, framed by the public, against the background of the possible commercial production of GM crops in the UK and the options for possibly proceeding with this; and through the debate provide meaningful information to Government about the nature and spectrum of the public views, particularly at grass roots level, on the issue to inform decision-making.
We aim to develop business performance by ensuring the effectiveness and efficiency of people development relevant to our industry.
Eat your fruit and veg � you�re aiming for at least 5 portions a day but it�s not as hard as you might think. A glass of pure fruit juice and a handful of dried fruit added to your cereal at breakfast each count as 1 portion.
The focus of the debate was very much on empowering the public to lead the discussion and enabling wide participation, not just involving the usual suspects. The Agriculture and Environment Biotechnology Commission were clear in their recommendations for a wider public debate that it should not require a simple yes or no decision. Instead it stated it should “establish the nature and full spectrum of the public�s views on GM and the possible commercialization of GM crops, and any conditions it might want to impose on this”.
If you�re a journalist but you don�t like talking to pr people (even though ours are very nice), you can e-mail Chris or Gerry direct:
Is it time we faced up to the reality of GM in modern world?
The Government has given the go-ahead for the first growing trials of GM wheat. Farming Editor Peter Hall looks at the latest developments in this highly emotive topic.
The Question: Why So Much Disagreement?
There is so much disagreement about the benefits and risks of GM because there are so many different views surrounding it. Some focus on the benefits and view it as a natural development of existing plant breeding, while others say that such views do not take into account the genuine concerns of the public and that risks and benefits have not been scrutinized enough.
The debate was criticized for not having enough time or funding to give it the publicity it would need in order to reach a truly representative cross-section of the UK public, including at grass roots level. The lack of results from the scientific and economic studies meant that there was no new information available to feed into the debate. However feedback forms were generally positive about the debate and the chance to express views on such a controversial issue.
Details of Parliamentary and other events, including Labour Party Conference, the All Party Group on Advertising and the Debating Group.
Results:�Genetically Modified Foods
Those who had strong opposing views on GM and surrounding issues tended to agree with the outcomes and some did not pay too much attention to the process issues. However, independent evaluators tended to disregard the outcomes as not valid and focused on the process. The general view was therefore not a positive one. Taking these together, the Food Standards Agency outlined a precautionary, evidence-based approach, taking a case-by-case methodology for the future development of GM crops in the UK which was a component of all these different reports. They said that whilst there was no scientific case for a blanket approval of all the uses of GM, there was also no scientific case for a blanket ban on the use of genetic modification.
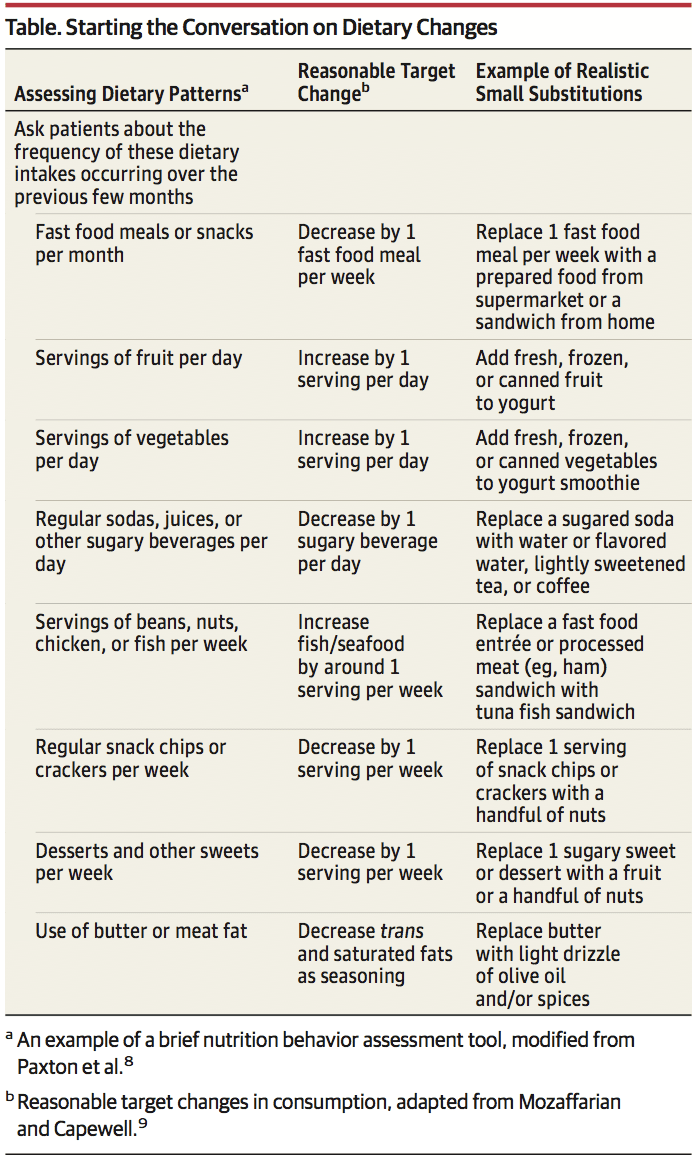
Wellness Chiropractor, Dr. Alexander Jimenez takes a look at discussing nutrition with patients in a clinical setting.
How Clinicians Can Do Better
Despite overwhelming evidence that relatively small dietary changes can significantly improve health, clinicians seldom discuss nutrition with their patients. Poor nutritional intake and nutrition-related health conditions, such as cardiovascular disease (CVD), diabetes, obesity, hypertension, and many cancers, are highly prevalent in the United States,1 yet only 12% of office visits include counseling about diet.2 Even among high- risk patients with CVD, diabetes, or hyperlipidemia, only 1 in 5 receive nutrition counseling.2 It is likely that many patients receive most of their nutrition information from other, and often unreliable, sources.
These data may reflect the minimal training, time, and reimbursement allocated to nutrition counseling (and preventive services in general) in clinical practice.3 Most physicians and other health care professionals receive limited education on nutrition in medical school (or other professional schools) or in postgraduate training. Just 25% of medical schools offer a dedicated nutrition course, a decline since the status of nutrition education in US medical schools was first assessed in 1985, and few medical schools achieve the 30 hours of nutrition education recommended by the National Academy of Sciences.4 As a result, physicians report inadequate nutrition knowledge and low self-efficacy for counseling patients about diet.3 In addition, time pressures, especially in primary care, limit opportunities to counsel on nutrition or address preventive issues beyond patients� acute complaints. Lack of time is frequently cited as the greatest barrier to counseling on nutrition and obesity.3
Moreover, nutrition and behavioral counseling have traditionally been non-reimbursed services. Few state Medicaid programs cover nutrition or obesity counseling, and before 2012, Medicare explicitly excluded coverage for obesity counseling; although now a reimbursed service for Medicare beneficiaries, just 1% of eligible Medicare beneficiaries receive this counseling.5 Dietitian counseling is also excluded by Medicare, unless patients have diabetes or renal disease. Although the Affordable Care Act mandates coverage for services graded A or B by the US Preventive Services Task Force, including nutrition counseling for patients with CVD risk factors and obesity counseling for patients with a body mass index of 30 or greater, existing private health insurance benefits are in- consistent, and the covered services are often unclear to both clinicians and patients, thereby limiting use.
Furthermore, health behavior change counseling is often frustrating given the current food environment, in which less nutritious foods tend to be less expensive, larger portioned, more easily accessible, and more heavily marketed than healthier options, making patient adherence 6 to nutrition advice challenging. Conflicting and confusing nutrition messages from popular books, blogs, and other media further complicate patient decision making.
Despite these unfavorable trends, there has been progress in this area. The evidence base supporting the benefits of nutrition intervention and behavioral counseling is expanding. Renewed focus on nutrition education in health care professional training is being driven by both student demand and the health care system. Although time pressures and reimbursement remain impediments, incentives and reimbursement options for nutrition and behavioral counseling are growing, and value-based care and health care team approaches hold promise to better align time demands and incentives for long-term care management. Initiatives to integrate clinical care and community resources offer opportunities to leverage resources that alleviate the clinician�s time commitment. There is evidence of some success; for instance, the amount of sugar-sweetened beverages consumed by individuals in the United States has declined substantially over the past 10 years.7
Clinicians can take the following reasonable steps to include nutrition counseling into the flow of daily practice:
1. Start the conversation. Several short, validated screen- ing questionnaires are available to quickly assess need for nutrition counseling, such as the Starting the Conversation tool8 (Table). This approach can be efficiently used prior to seeing the patient at an appointment, either delivered by medical assistants as part of vital sign assessment or as prescreening paperwork for patients to complete online or in the waiting room.
2. Structure the encounter.�Using methods such as the �5 A�s� (assess, advise, agree, assist, arrange), which has been adapted from tobacco counseling. Motivational interviewing, which has documented efficacy in numerous behavior change settings, is particularly helpful to engage patients who are not yet committed or are hesitant to consider behavioral change.
3. Focus on small steps. Changing lifelong nutrition behaviors can seem overwhelming, but even exceedingly small shifts can have an effect (Table). For example, increasing fruit intake by just 1 serving per day has the estimated potential to reduce cardiovascular mortality risk by 8%, the equivalent of 60 000 fewer deaths annually in the United States and 1.6 million deaths globally.9 Other examples include reducing intake of sugar-sweetened beverages, fast food meals, processed meats, and sweets, while increasing vegetables, legumes, nuts, and whole grains. Emphasize to patients that every food choice is an opportunity to accrue benefits, and even small ones add up. Small substitutions still allow for �treats,� such as replacing potato chips and cheese dip with tortilla chips and salsa, the latter lowering trans fats and saturated fat and increasing whole grain and vegetable intake (Table).
4. Use available resources. Numerous extracurricular resources are readily available for clinicians. The Nutrition in Medicine program offers online, evidence-based nutrition education and tutorials for clinicians and an online, core nutrition curriculum for medical students. The Dietary Guidelines for Americans offers evidence- based and freely available nutrition guidance, tutorials, and tools for clinicians and patients alike. A companion website, Choose My Plate, offers nutrition and counseling advice for clinicians and handy resources for patients, including recently added videos with useful examples of small substitutions that patients will appreciate.
5. Do not do it all at once. Expecting to create long-term behavioral change during a single episode of care is a recipe for frustration and failure, for both the patient and clinician. Empowering and sup- porting patients is an ongoing process, not a 1-time curative event. Use a few minutes at the close of a patient visit to identify opportunities for future counseling, offer to serve as a resource, and be- gin a discussion and support that can be reinforced over time. Take solace in knowing that small initial steps can quickly improve health; for example, reducing trans fats at a single meal (eg, replacing baked goods with fruit or nuts or fried foods with non-fried alternatives) promptly improves endothelial function.10
6. Do not do it all alone.�The primary care physician need not be the sole clinician who provides nutrition counseling. Proactive use of physician extenders (eg, physician assistants, nurses, medical assistants, and health coaches) and referrals can alleviate much of the burden for the busy clinician. Receptionists can distribute assessment and screening questionnaires for patients to complete in the waiting room; medical assistants can document behavioral change progress while assessing vital signs; administrative staff can identify and con- tact patients who are overdue for interaction. Large practices may benefit from including nutrition or health coaches on staff. Referring to clinical specialists and community-based support programs can significantly extend the clinician�s reach.7 In addition to registered dietitians, numerous clinical and community resources are available and often covered by insurance plans. Board-certified obesity medicine specialists, certified diabetes educators, and physician nutrition specialists are available as referrals in many areas. Diabetes Prevention Program group counseling sessions are now covered by Medicare and available throughout communities, such as in many YMCA sites, and electronically.
Summary
Although there is no conclusive evidence that these steps will improve diet and health outcomes for patients, there is virtually no harm in counseling and the potential gains, especially at the population level, are substantial. Nutrition and health behavior change must become a core competency for virtually all physicians and any other health professionals working with patients who have or are at risk for nutrition-related chronic disease.
A Healthier You
Scott Kahan, MD, MPH Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; and George Washington University School of Medicine, Washington, DC.
JoAnn E. Manson, MD, DrPH Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts; and Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, Massachusetts.
ARTICLE INFORMATION
Published Online: September 7, 2017. doi:10.1001/jama.2017.10434 Conflict of Interest Disclosures: All authors have
completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported.
REFERENCES
1. Ward BW, Schiller JS, Goodman RA. Multiple chronic conditions among US adults: a 2012 update. Prev Chronic Dis. 2014;11:E62.
2. Office of Disease Prevention and Health Promotion. Healthy People 2020. https://www.healthypeople.gov/2020/data-search/Search-the-Data#srch=nutrition. Accessed January 23, 2017.
3. Kolasa KM, Rickett K. Barriers to providing nutrition counseling cited by physicians. Nutr Clin Pract. 2010;25(5):502-509.
4. Adams KM, Kohlmeier M, Zeisel SH. Nutrition education in U.S. medical schools: latest update of a national survey. Acad Med. 2010;85(9):1537-1542.
5. Batsis JA, Bynum JPW. Uptake of the Centers for Medicare and Medicaid obesity benefit: 2012-2013. Obesity (Silver Spring). 2016;24(9):1983-1988.
6. Kahan S, Cheskin LJ. Obesity and eating behaviors and behavior change. In: Kahan S, Gielen AC, Fagan PJ, Green LW, eds. Health Behavior Change in Populations. Baltimore, MD: Johns Hopkins University Press; 2014:chap 13.
7. Rehm CD, Pe�alvo JL, Afshin A, Mozaffarian D. Dietary intake among US adults, 1999-2012.JAMA. 2016;315(23):2542-2553.
8. Paxton AE, Strycker LA, Toobert DJ, Ammerman AS, Glasgow RE. Starting the conversation performance of a brief dietary assessment and intervention tool for health professionals. Am J Prev Med. 2011;40(1):67-71.
9. Mozaffarian D, Capewell S. United Nations� dietary policies to prevent cardiovascular disease. BMJ. 2011;343:d5747.
10. Williams MJA, Sutherland WHF, McCormick MP, de Jong SA, Walker RJ, Wilkins GT. Impaired endothelial function following a meal rich in used cooking fat.J Am Coll Cardiol. 1999;33(4):1050-1055
El Paso, TX. Chiropractor Dr. Alex Jimenez takes a look at the Mediterranean diet.
I eat a wide variety of delicious foods every day including pasta dishes, curries, cheese and chocolate. I also drink red wine most days. Yet I’m in the best shape of my life and I’ve never felt healthier.
What’s my secret? Actually it’s not a secret at all. You’ve no doubt heard many good things about the Mediterranean diet. You probably also know that Asian diets, such as the Japanese diet, are also extremely healthy. All I did was combine the best parts of these traditional and highly appetising diets into one ‘MediterrAsian’ diet — so I literally get the best of both worlds.
I didn’t come up with this concept alone. In fact it was an extraordinary set of circumstances that led me to follow a MediterrAsian way of eating in the first place.
My parents are both medical doctors, so I’ve always had a natural interest in health and healthy living. But it wasn’t until I was introduced to authentic Asian cuisine by my Chinese-Malaysian sister-in-law in my late teens that I discovered that healthy food and delicious food could be one in the same. This was a revelation to me, and I’ve been hooked on Asian food ever since.
Then, in my early twenties, I met and fell in love with Ric. Like me, Ric was very interested in health and healthy living. That was mainly because he’d lost his own health following a near-fatal motorcycle accident six years earlier. After lots of struggle and pain, he only fully regained his health by adopting a Mediterranean diet. When we met, I introduced Ric to Asian cooking and he introduced me to Mediterranean cooking. We ended up bonding over pad Thai and paella!
We also discovered there were so many benefits to eating a combined diet of Mediterranean and Asian foods. One of the biggest benefits was for our taste buds! So many of the world’s most mouth-watering foods originate from Mediterranean and Asian regions, including pasta, pizza, risotto, sushi, curries, and stir-fries. So we never felt deprived. And the health benefits were also extraordinary. From getting us in the best shape of our lives to improving our cholesterol and blood pressure, and giving us bucket loads of energy.
What Exactly Makes MediterrAsian Eating So Health Giving?
Actually, we’ve discovered there are a number of important reasons. Unlike modern Western diets that are full of highly processed foods, traditional Mediterranean and Asian diets are based on a foundation of minimally processed plant foods. These vegetables, fruits, grains and beans are bulky and filling but are generally low to moderate in calories. Fish and shellfish, which are also traditional Mediterranean and Asian staples, are also quite low in calories and are a good source of hunger-suppressing protein. So, these foods fill us up long before they fill us out. They also more than counter-balance the higher calorie foods we do eat, such as olive oil, nuts and cheese. This means we end up feeling comfortably full after a meal, without consuming more calories than our bodies need.
Traditional Mediterranean and Asian foods are also overflowing with health-promoting compounds including dietary fibre (which also happens to be one of nature�s best appetite suppressants), omega-3 fatty acids, phytochemicals and antioxidants.
But there’s another big reason why combining Mediterranean and Asian eating practices make so much sense. And it comes down to how the foods in these traditional diets affect our genes.
Scientific research in recent years has found that many foods common in Mediterranean and Asian diets (such as olive oil, red wine, turmeric, green tea, dark chocolate and soyfoods) are rich in natural plant compounds that activate a type of gene in the body called sirtuins. Studies have found that sirtuins play a fundamental role in extending cellular life and the repair of DNA. They also inhibit fat storage and increase fat metabolism.
That’s why a diet rich in sirtuin-activating foods, or “sirtfoods,” is being recommended by a growing number of health experts. In fact, Adele credits much of her dramatic weight loss with following a diet rich in sirtfoods.
So if you want to get healthy and in shape, reduce your risk of chronic disease and live longer — all while enjoying a wide range of delicious foods — we highly recommend you give a MediterrAsian way of eating a go.
Call Today!
— Trudy Thelander is co-author of the acclaimed cookbook, The MediterrAsian Way, and co-creator of the newly-released mobile cooking app, The MediterrAsian Table.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine






 Nat Rev Rheumatol. 2017 Jun;13(6):348-358.
Nat Rev Rheumatol. 2017 Jun;13(6):348-358.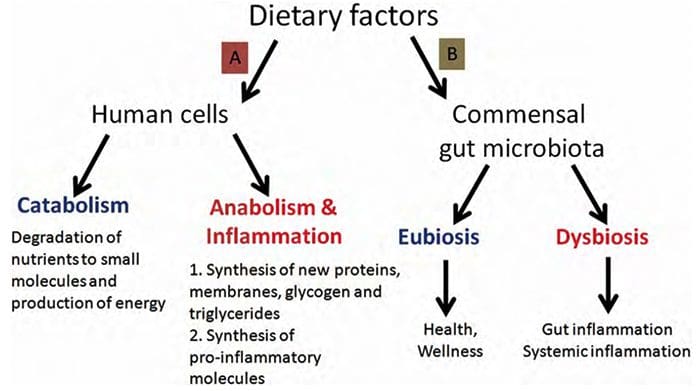 Paolo Riccio, and Rocco Rossano ASN Neuro
Paolo Riccio, and Rocco Rossano ASN Neuro
 BMJ. 2014; 349: g4490.
BMJ. 2014; 349: g4490.



 Reduce Fatigue
Reduce Fatigue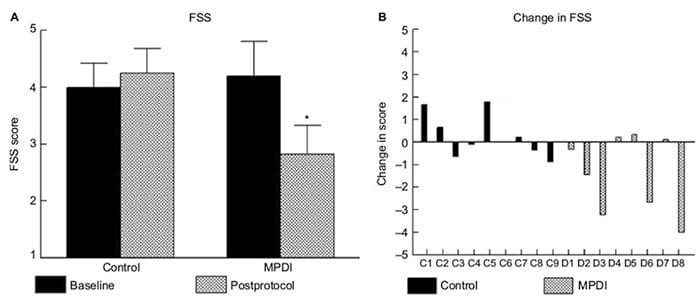

 The composition of gut microbiota is influenced by multiple factors, such as diet and host genotype. Within the gut, ecological processes such as selection and evolution take place. The use of antibiotics reduces the numbers and diversity of gut microbiota.
The composition of gut microbiota is influenced by multiple factors, such as diet and host genotype. Within the gut, ecological processes such as selection and evolution take place. The use of antibiotics reduces the numbers and diversity of gut microbiota.

 The late nineties were an era of strong debate on the issue of genetically modified food and organisms in the UK. Controversy surrounded both the scientific and political aspects of GM, with government advisory bodies being accused of biased behavior and concerns being raised over the ethical issues of the science behind GM. At lunch, a bowl of good vegetable-based soup (home-made or Simply Organic�s naturally!) counts for another 1 or 2 portions and each one of our Pure & Pronto ready meals counts for a whopping 3 portions. Add a piece of fruit or two during the day and a salad or veg in the evening and you�re already at 6 or 7 portions of fruit and veg for the day � well above the 5.
The late nineties were an era of strong debate on the issue of genetically modified food and organisms in the UK. Controversy surrounded both the scientific and political aspects of GM, with government advisory bodies being accused of biased behavior and concerns being raised over the ethical issues of the science behind GM. At lunch, a bowl of good vegetable-based soup (home-made or Simply Organic�s naturally!) counts for another 1 or 2 portions and each one of our Pure & Pronto ready meals counts for a whopping 3 portions. Add a piece of fruit or two during the day and a salad or veg in the evening and you�re already at 6 or 7 portions of fruit and veg for the day � well above the 5. The stated aims of the GM Nation debate were twofold: to promote an innovative, effective and deliberative program of debate on GM issues, framed by the public, against the background of the possible commercial production of GM crops in the UK and the options for possibly proceeding with this; and through the debate provide meaningful information to Government about the nature and spectrum of the public views, particularly at grass roots level, on the issue to inform decision-making.
The stated aims of the GM Nation debate were twofold: to promote an innovative, effective and deliberative program of debate on GM issues, framed by the public, against the background of the possible commercial production of GM crops in the UK and the options for possibly proceeding with this; and through the debate provide meaningful information to Government about the nature and spectrum of the public views, particularly at grass roots level, on the issue to inform decision-making.