Cauda equina syndrome/CES is a rare condition in which the nerves in the lower back are compressed. It can include sciatica as one of its symptoms. Individuals presenting with symptoms that could be CES are advised to see a healthcare provider as soon as possible, as delaying treatment can lead to permanent damage.
Cauda Equina Syndrome
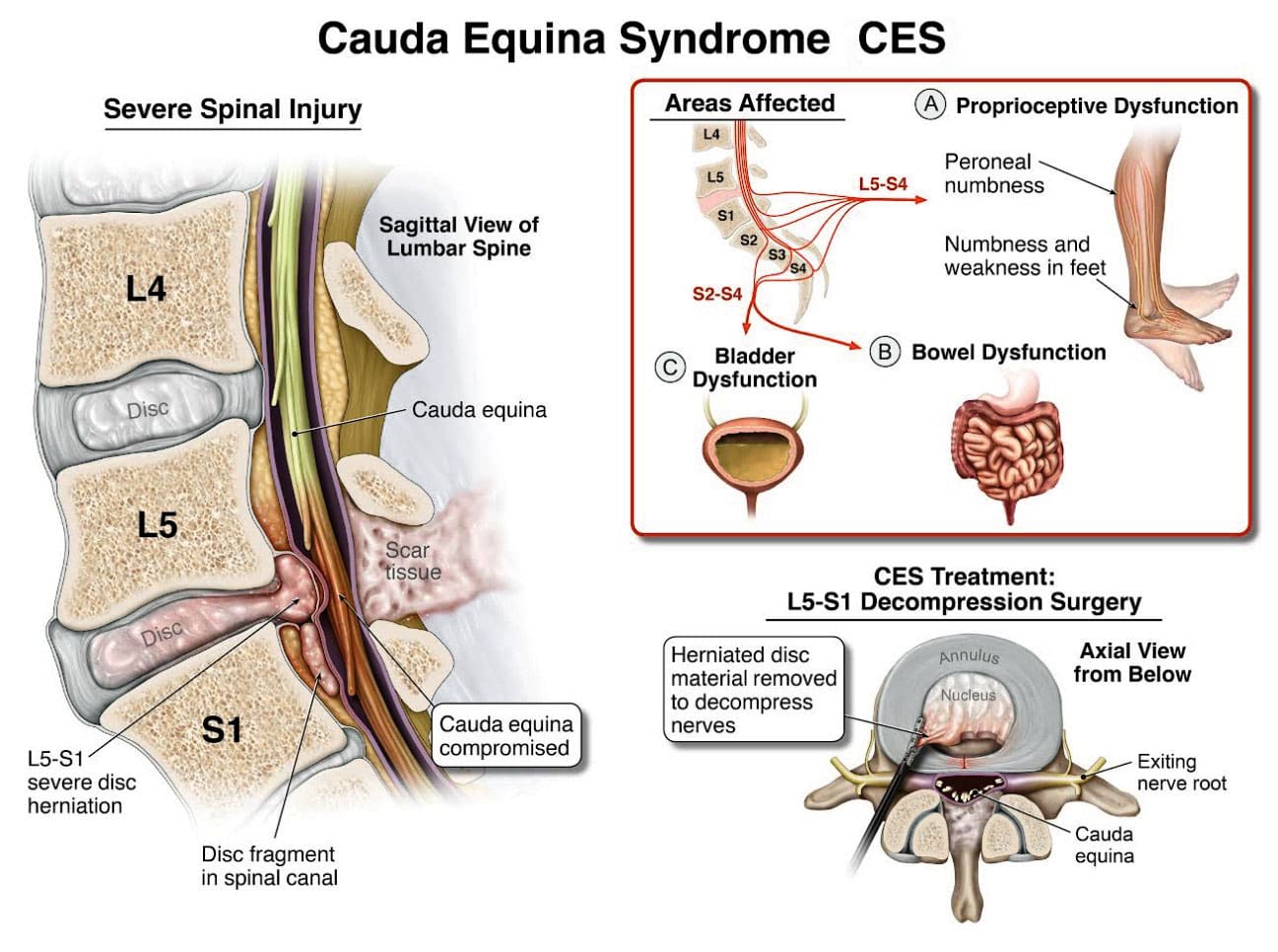
A cluster of nerve roots called the cauda equina, Latin for horse’s tail, sends and receives messages to the legs, bladder, and other body parts. Cauda equina syndrome is a rare condition in which nerve roots in the lower spinal cord are compressed. This compresses the nerves and disrupts motor and sensory function in the bladder and lower extremities. The most common cause is a ruptured or herniated disc in the lumbar area. This usually occurs when a severe disc herniation compresses the nerve bundle at the base of the spinal cord, causing significant neurological dysfunction like bladder/bowel issues and numbness in the saddle area. If found early, it is treated with surgery within 24 to 48 hours of symptom onset.
This is characterized by symptoms that include unusual urinary sensation, loss of desire to urinate, poor urinary stream, and having to strain to urinate. (Gardner A., Gardner E., & Morley T. 2011)
Pott’s paralysis is a neurological complication of tuberculosis (TB) of the spine.
TB is a bacterial infection that usually affects the lungs but can spread to the spine.
Iatrogenic Side Effects
Injuries or illnesses that result from medical or surgical treatment
Spinal Lesions or Malignant Tumors
A spinal lesion refers to any abnormal growth or damage within the spine.
It can include benign (noncancerous) and malignant (cancerous) tumors.
A malignant tumor is a cancerous growth within the spine; essentially, a malignant tumor is a type of spinal lesion with the potential to spread to other parts of the body.
Spinal Infection, Inflammation, Hemorrhage, or Fracture
A spinal infection refers to a bacterial, fungal, or viral infection that occurs within the bones of the spine (vertebrae) or the surrounding tissues, potentially causing pain, inflammation, and, in severe cases, neurological complications like weakness or paralysis;
Spinal inflammation is a general term for swelling or irritation within the spinal column.
Spinal hemorrhage” indicates bleeding within the spinal canal.
A spinal fracture refers to a break in one or more of the vertebrae in the spine.
Spinal Arteriovenous Malformations (AVMs)
A spinal arteriovenous malformation (AVM) is a rare condition in which the arteries and veins in the spinal cord tangle abnormally.
This can damage the spinal cord over time.
Complications from Lumbar Surgery
Lumbar surgery can have several complications, including infections, blood clots, nerve damage, and spinal fluid leaks.
Spinal Anesthesia
Spinal anesthesia is a regional anesthesia that blocks pain and sensation in the lower body.
It involves injecting a local anesthetic medication into the subarachnoid space surrounding the spinal cord.
The exact cause is not fully understood, but it can involve direct nerve root injury from the needle, inflammation caused by the anesthetic, or a spinal hematoma compressing the nerve roots.
Infection of the tissues (meninges) that cover the cauda equina and spinal cord.
An abscess pressing on the cauda equina.
Diagnosis
Diagnosis requires a medical history of symptoms, general health, activity level, and a physical exam to assess strength, reflexes, sensation, stability, alignment, and motion. (American Association of Neurological Surgeons, 2024) Testing includes:
X-ray or computerized tomography (CT) imaging is enhanced by the injection of contrast material into the cerebrospinal fluid spaces, which can show displacement of the spinal cord or spinal nerves.
Specialized Nerve Testing
This could be nerve conduction velocity tests and testing electrical activity in muscles or electromyography.
Treatment
The extent of urinary problems can determine treatment protocols. A CES diagnosis is usually followed by emergency surgery within 24 to 48 hours to relieve compression of the nerves. Moving quickly is essential to prevent permanent complications such as nerve damage, incontinence, or leg paralysis. (American Association of Neurological Surgeons, 2024)
Depending on the cause, corticosteroids also may be prescribed to reduce swelling.
Antibiotics may be needed if an infection is responsible for CES.
For situations in which a tumor is the cause, surgery to remove it may be necessary, followed by chemotherapy and/or radiation.
The outcome with CES-I during surgery is generally favorable.
Those whose CES has deteriorated to CES-R tend to have a less favorable prognosis.
Post Surgery Therapy
After surgery, CES can be challenging to deal with. If bladder function has been impaired, recovery of control can take time.
Frequent urinary infections are also a potential complication.
Loss of bladder or bowel control can be psychologically distressing, impacting social life, work, and relationships.
Sexual dysfunction can also occur, contributing to relationship difficulties or depression.
Therapy with a mental health professional may be recommended. When damage is permanent, it will be important to include family and friends in the adjustment to living with a chronic condition. Psychological counseling and/or a support group can be helpful. Other specialists who can help include: (American Academy of Orthopaedic Surgeons, 2024)
Occupational therapist
Physical therapist
Physiotherapist
Sex therapist
Social worker
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
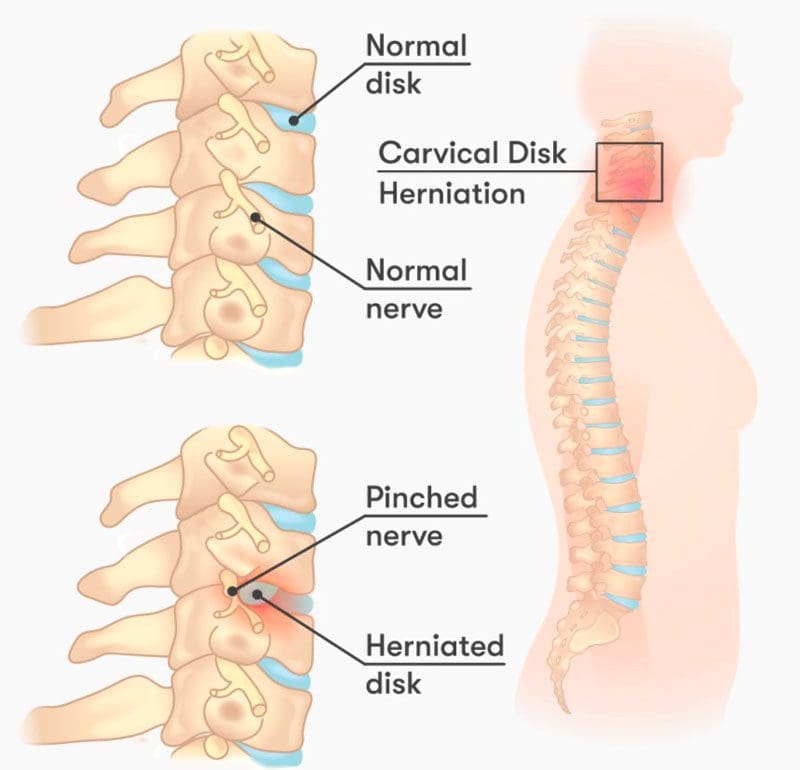
Disc Herniation
References
American Association of Neurological Surgeons. (2024). Cauda Equina Syndrome. https://www.aans.org/patients/conditions-treatments/cauda-equina-syndrome/
Gardner, A., Gardner, E., & Morley, T. (2011). Cauda equina syndrome: a review of the current clinical and medico-legal position. European Spine Journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 20(5), 690–697. https://doi.org/10.1007/s00586-010-1668-3
Fairbank, J., & Mallen, C. (2014). Cauda equina syndrome: implications for primary care. The British journal of general practice: the journal of the Royal College of General Practitioners, 64(619), 67–68. https://doi.org/10.3399/bjgp14X676988
American Academy of Orthopaedic Surgeons. (2024). Cauda equina syndrome. https://orthoinfo.aaos.org/en/diseases–conditions/cauda-equina-syndrome
Individuals suffering from a jammed finger: Can knowing the signs and symptoms of a finger that is not broken or dislocated allow for at-home treatment and when to see a healthcare provider?
Jammed Finger Injury
A jammed finger, also known as a sprained finger, is a common injury when the tip of a finger is forcefully pushed toward the hand, causing the joint to become compressed. This can cause pain and swelling in one or more fingers or finger joints and cause ligaments to stretch, sprain, or tear. (American Society for Surgery of the Hand. 2015) A jammed finger can often heal with icing, resting, and taping. This is often enough to allow it to heal in a week or two if no fractures or dislocations are present. (Carruthers, K. H. et al., 2016) While painful, it should be able to move. However, if the finger cannot wiggle, it may be broken or dislocated and require X-rays, as a broken finger or joint dislocation can take months to heal.
Treatment
Treatment consists of icing, testing, taping, resting, seeing a chiropractor or osteopath, and progressive regular use to regain strength and ability.
Ice
The first step is icing the injury and keeping it elevated.
Use an ice pack or a bag of frozen vegetables wrapped in a towel.
Ice the finger in 15-minute intervals.
Take the ice off and wait until the finger returns to its normal temperature before re-icing.
Do not ice a jammed finger for over three 15-minute intervals in one hour.
Try To Move The Affected Finger
If the jammed finger does not move easily or the pain gets worse when trying to move it, you need to see a healthcare provider and have an X-ray to check for a bone fracture or dislocation. (American Society for Surgery of the Hand. 2015)
Try to move the finger slightly after swelling, and the pain subsides.
If the injury is mild, the finger should move with little discomfort for a short time.
Tape and Rest
If the jammed finger is not broken or dislocated, it can be taped to the finger next to it to keep it from moving, known as buddy taping. (Won S. H. et al., 2014)
Medical-grade tape and gauze between the fingers should be used to prevent blisters and moisture while healing.
A healthcare provider may suggest a finger splint to keep the jammed finger lined up with the other fingers.
A splint can also help prevent a jammed finger from re-injury.
Resting and Healing
A jammed finger must be kept still to heal at first, but eventually, it needs to move and flex to build strength and flexibility.
Targeted physical therapy exercises can be helpful for recovery.
A primary care provider might be able to refer a physical therapist to ensure the finger has a healthy range of motion and circulation as it heals.
A chiropractor or osteopath can also provide recommendations for helping rehabilitate the finger, hand, and arm to normal function.
Easing The Finger Back to Normal
Depending on the extent of the injury, the finger and hand can be sore and swollen for a few days or weeks.
It can take some time to start feeling normal.
Once the healing process begins, individuals will want to return to using it normally.
Avoiding using a jammed finger will cause it to lose strength, which can, over time, further weaken it and increase the risk of re-injury.
If the pain and swelling persist, see a healthcare provider to get it checked for a possible fracture, dislocation, or other complication as soon as possible, as these injuries are harder to treat if the individual waits too long. (University of Utah Health, 2021)
At Injury Medical Chiropractic and Functional Medicine Clinic, we passionately focus on treating patients’ injuries and chronic pain syndromes and improving ability through flexibility, mobility, and agility programs tailored to the individual. Our providers use an integrated approach to create personalized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine protocols. Our goal is to relieve pain naturally by restoring health and function to the body. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective clinical treatments.
Treatment for Carpal Tunnel Syndrome
References
American Society for Surgery of the Hand. (2015). Jammed finger. https://www.assh.org/handcare/condition/jammed-finger
Carruthers, K. H., Skie, M., & Jain, M. (2016). Jam Injuries of the Finger: Diagnosis and Management of Injuries to the Interphalangeal Joints Across Multiple Sports and Levels of Experience. Sports health, 8(5), 469–478. https://doi.org/10.1177/1941738116658643
Won, S. H., Lee, S., Chung, C. Y., Lee, K. M., Sung, K. H., Kim, T. G., Choi, Y., Lee, S. H., Kwon, D. G., Ha, J. H., Lee, S. Y., & Park, M. S. (2014). Buddy taping: is it a safe method for treatment of finger and toe injuries?. Clinics in orthopedic surgery, 6(1), 26–31. https://doi.org/10.4055/cios.2014.6.1.26
University of Utah Health. (2021). University of Utah Health. Should I worry about a jammed finger? University of Utah Health. https://healthcare.utah.edu/the-scope/all/2021/03/should-i-worry-about-jammed-finger
Individuals experiencing shooting, aching pain in the lower extremities, and intermittent leg pain could be suffering from neurogenic claudication. Can knowing the symptoms help healthcare providers develop an effective treatment plan?
Neurogenic Claudication
Neurogenic claudication occurs when spinal nerves become compressed in the lumbar or lower spine, causing intermittent leg pain. Compressed nerves in the lumbar spine can cause leg pain and cramps. The pain usually worsens with specific movements or activities like sitting, standing, or bending backward. It is also known as pseudo-claudication when the space within the lumbar spine narrows. A condition known as lumbar spinal stenosis. However, neurogenic claudication is a syndrome or group of symptoms caused by a pinched spinal nerve, while spinal stenosis describes the narrowing of the spinal passages.
Symptoms
Neurogenic claudication symptoms can include:
Leg cramping.
Numbness, tingling, or burning sensations.
Leg fatigue and weakness.
A sensation of heaviness in the leg/s.
Sharp, shooting, or aching pain extending into the lower extremities, often in both legs.
There may also be pain in the lower back or buttocks.
Neurogenic claudication is different from other types of leg pain, as the pain alternates – ceasing and beginning randomly and worsens with specific movements or activities. Standing, walking, descending stairs, or flexing backward can trigger pain, while sitting, climbing stairs, or leaning forward tends to relieve pain. However, every case is different. Over time, neurogenic claudication can affect mobility as individuals try to avoid activities that cause pain, including exercise, lifting objects, and prolonged walking. In severe cases, neurogenic claudication can make sleeping difficult.
Neurogenic claudication and sciatica are not the same. Neurogenic claudication involves nerve compression in the central canal of the lumbar spine, causing pain in both legs. Sciatica involves compression of nerve roots exiting from the sides of the lumbar spine, causing pain in one leg. (Carlo Ammendolia, 2014)
Causes
With neurogenic claudication, compressed spinal nerves are the underlying cause of the leg pain. In many cases, lumber spinal stenosis – LSS is the cause of pinched nerve. There are two types of lumbar spinal stenosis.
Central stenosis is the main cause of neurogenic claudication. With this type, the central canal of the lumbar spine, which houses the spinal cord, narrows, causing pain in both legs.
Lumbar spinal stenosis can be acquired and develop later in life due to spine deterioration.
Congenital means the individual is born with the condition.
Both can lead to neurogenic claudication in different ways.
Foramen stenosis is another type of lumbar spinal stenosis that causes the narrowing of spaces on either side of the lumbar spine where nerve roots branch off the spinal cord. The associated pain is different in that it is either in the right or left leg.
The pain corresponds to the side of the spinal cord where the nerves are being pinched.
Acquired Lumbar Spinal Stenosis
Lumbar spinal stenosis is usually acquired due to the degeneration of the lumbar spine and tends to affect older adults. The causes of the narrowing can include:
Spinal trauma, such as from a vehicle collision, work, or sports injury.
Disc herniation.
Spinal osteoporosis – wear-and-tear arthritis.
Ankylosing spondylitis – a type of inflammatory arthritis that affects the spine.
Osteophytes – bone spurs.
Spinal tumors – non-cancerous and cancerous tumors.
Congenital Lumbar Spinal Stenosis
Congenital lumbar spinal stenosis means an individual is born with abnormalities of the spine that may not be apparent at birth. Because the space within the spinal canal is already narrow, the spinal cord is vulnerable to any changes as the individual ages. Even individuals with mild arthritis can experience symptoms of neurogenic claudication early on and develop symptoms in their 30s and 40s instead of their 60s and 70s.
Diagnosis
Diagnosis of neurogenic claudication is largely based on the individual’s medical history, physical examination, and imaging. The physical examination and review identify where the pain is presenting and when. The healthcare provider may ask:
Is there a history of lower back pain?
Is the pain in one leg or both?
Is the pain constant?
Does the pain come and go?
Does the pain get better or worse when standing or sitting?
Do movements or activities cause pain symptoms and sensations?
Are there any usual sensations while walking?
Treatment
Treatments can consist of physical therapy, spinal steroid injections, and pain meds. Surgery is a last resort when all other therapies are unable to provide effective relief.
Physical Therapy
A treatment plan will involve physical therapy that includes:
Daily stretching
Strengthening
Aerobic exercises
This will help improve and stabilize the lower back muscles and correct posture problems.
Occupational therapy will recommend activity modifications that cause pain symptoms.
This includes proper body mechanics, energy conservation, and recognizing pain signals.
Back braces or belts may also be recommended.
Spinal Steroid Injections
Healthcare providers may recommend epidural steroid injections.
This delivers a cortisone steroid to the outermost section of the spinal column or the epidural space.
Pain medications are used to treat intermittent neurogenic claudication. These include:
Over-the-counter analgesics like acetaminophen.
Nonsteroidal anti-inflammatory drugs or NSAIDs like ibuprofen or naproxen.
Prescription NSAIDs may be prescribed if needed.
NSAIDs are used with chronic neurogenic pain and should only be used when required.
The long-term use of NSAIDs can increase the risk of stomach ulcers, and the overuse of acetaminophen can lead to liver toxicity and liver failure.
Surgery
If conservative treatments are unable to provide effective relief and mobility and/or quality of life are affected, surgery known as a laminectomy may be recommended to decompress the lumbar spine. The procedure may be performed:
Laparoscopically – with small incisions, scopes, and surgical instrumentation.
Open surgery – with a scalpel and sutures.
During the procedure, facets of the vertebra are partially or completely removed.
To provide stability, the bones are sometimes fused with screws, plates, or rods.
Success rates for both are more or less the same.
Between 85% and 90% of individuals undergoing the surgery achieve long-lasting and/or permanent pain relief. (Xin-Long Ma et al., 2017)
Movement Medicine: Chiropractic Care
References
Ammendolia C. (2014). Degenerative lumbar spinal stenosis and its imposters: three case studies. The Journal of the Canadian Chiropractic Association, 58(3), 312–319.
Munakomi S, Foris LA, Varacallo M. (2024). Spinal Stenosis and Neurogenic Claudication. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430872/
Ma, X. L., Zhao, X. W., Ma, J. X., Li, F., Wang, Y., & Lu, B. (2017). Effectiveness of surgery versus conservative treatment for lumbar spinal stenosis: A system review and meta-analysis of randomized controlled trials. International journal of surgery (London, England), 44, 329–338. https://doi.org/10.1016/j.ijsu.2017.07.032
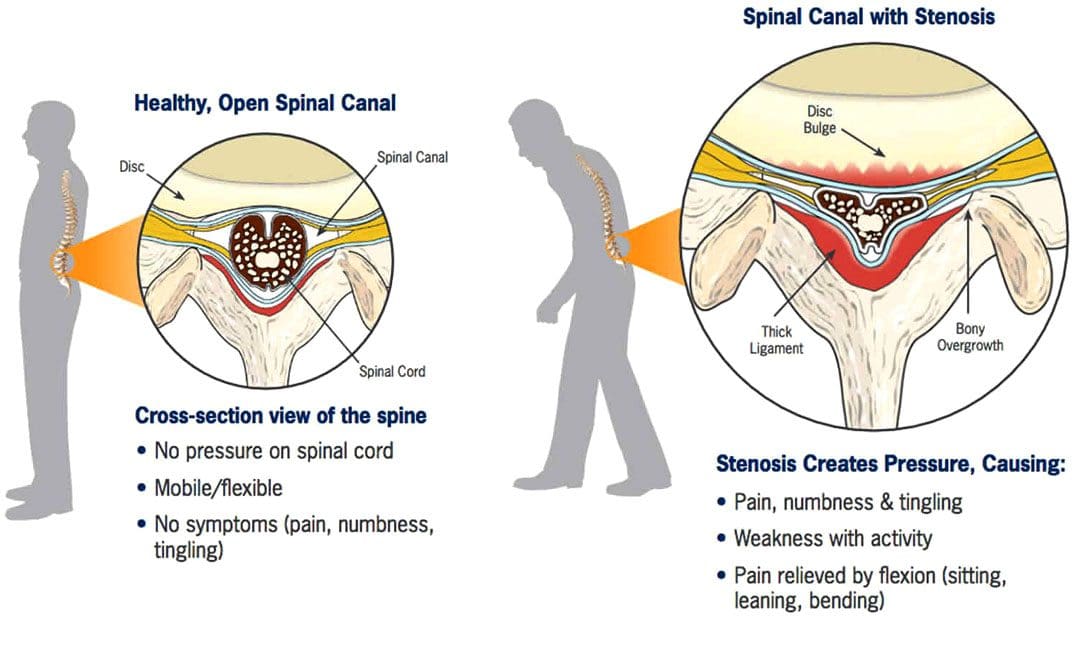
The discs between the spine’s vertebrae provide cushioning and shock absorption in the spine and the rest of the body. Degenerative changes to the discs are believed to be the start of spinal stenosis. When the discs lack sufficient hydration/water and disc height decreases over time, the cushioning and shock absorption becomes less and less effective. The vertebrae can then become compressed, causing friction. Degenerative spinal stenosis can also develop from excess scar tissue and bone spurs (growth that develops on the edge of a bone) that can form after injury or spinal surgery.
Assessment
A physician will make a diagnosis of spinal stenosis. The doctor will take an imaging scan of the spine to determine the exact location of the degeneration and to measure how narrow the openings have become. Pain, stiffness, limited mobility, and loss of range of motion are often present. If spinal stenosis has caused nerve compression, there may also be pain, numbness, tingling, or weakness in the buttocks (sciatica), thighs, and lower legs. A physical therapist will determine the degree by assessing the following:
Vertebrae mobility – how the spine bends and twists in different directions.
Ability to change positions.
The strength of the core, back, and hip muscles.
Balance
Posture
Gait pattern
Nerve compression to determine if there are any symptoms in the legs.
Milder cases usually do not involve nerve compression, as back stiffness is more common.
In more severe cases, there may be significant pain, limited mobility, and nerve compression, causing leg weakness.
The most common symptom of spinal stenosis is increased pain with backward bending or extension of the lumbar spine. This includes positions that extend the spine, such as standing, walking, and lying on the stomach. Symptoms usually improve when bending forward and when the spine is positioned more into a flexed or bent position, like when sitting and reclining. These body positions open up the spaces in the central spinal canal.
Surgery
Spinal stenosis is the most common reason for undergoing surgery in adults 65 and older. However, surgery is almost always performed as a last resort if pain, symptoms, and disability persist after trying conservative therapies, including chiropractic, non-surgical decompression, and physical therapy, for months or years. The severity of symptoms and current state of health will determine whether a doctor will recommend surgery. (Zhuomao Mo, et al., 2018). Conservative measures can be safer and just as effective. A systematic review or study based on all available primary research found that physical therapy and exercise resulted in similar outcomes to surgery for improving pain and disability. (Zhuomao Mo, et al., 2018). Except for severe cases, surgery is often not necessary.
Physical Therapy for Spinal Stenosis
The objective of physical therapy includes:
Decreasing pain and joint stiffness.
Relieving nerve compression.
Reducing tightness in the surrounding muscles.
Improving the range of motion.
Improving postural alignment.
Strengthening the core muscles.
Improving leg strength to help with balance and overall function.
Stretching of the back muscles, including those running vertically along the spine and those running diagonally from the pelvis to the lumbar spine, helps relieve muscle tightness and pain and can improve overall mobility and range of motion of the lumbar spine.
Stretching the hip muscles, including the hip flexors in the front, the piriformis in the back, and the hamstrings that run from the back of the hip down the leg to the knee, is also important as these muscles are attached to the pelvis, which directly connects to the spine.
Exercises for strengthening the abdominal core muscles, including the muscles in the trunk, pelvis, lower back, hips, and abdomen, help stabilize the spine and protect it from excessive movement and compressive forces.
With spinal stenosis, the core muscles often become weak and inactive and unable to do their job to support the spine. Core exercises often begin by activating the deep abdominal muscles while lying flat on the back with the knees bent.
Exercises will progress as the individual gains more strength and control as the spine stabilizes.
Spinal stenosis physical therapy will also involve balance training and glute exercises for strengthening the leg muscles.
Prevention
Working with a physical therapist can help prevent future problems by maintaining spinal mobility, keeping the individual active, and exercising to maintain strength and stability to provide a solid foundation to support the lower back and prevent symptoms from worsening.
Severe Spinal Stenosis Physical Therapy
Physical therapy usually involves performing stretches for the lower back, hips, and legs, mobility exercises, and core strengthening exercises to improve spinal support and decrease pain. Treatments like heat or electrical stimulation may also be used on a case-by-case basis if there is significant pain or tightness in the back muscles. However, there is not enough clinical evidence to support that there are additional benefits. (Luciana Gazzi Macedo, et al., 2013) The effectiveness of physical therapy is high because surgery alone cannot strengthen the muscles that stabilize the spine, increase the mobility or flexibility of the surrounding muscles, and improve postural alignment.
The Root Causes of Spinal Stenosis
References
Lurie, J., & Tomkins-Lane, C. (2016). Management of lumbar spinal stenosis. BMJ (Clinical research ed.), 352, h6234. https://doi.org/10.1136/bmj.h6234
Mo, Z., Zhang, R., Chang, M., & Tang, S. (2018). Exercise therapy versus surgery for lumbar spinal stenosis: A systematic review and meta-analysis. Pakistan journal of medical sciences, 34(4), 879–885. https://doi.org/10.12669/pjms.344.14349
Macedo, L. G., Hum, A., Kuleba, L., Mo, J., Truong, L., Yeung, M., & Battié, M. C. (2013). Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review. Physical therapy, 93(12), 1646–1660. https://doi.org/10.2522/ptj.20120379
A nerve becomes pinched/compressed when added pressure is placed on it by surrounding structures that can include muscles, bones, ligaments, tendons, or a combination. This injures and damages the nerve causing function problems and symptoms and sensations in that area or other parts of the body that are supplied by that nerve. Medical practitioners refer to this as nerve compression or entrapment. Although compressed nerves are more commonly associated with the neck, arms, hands, elbows, and lower back, any nerve in the body can experience irritation, spasms, inflammation, and compression. The causes and treatment of a compressed nerve in the knee.
Compressed Nerve In The Knee
There’s only one nerve that goes through the knee that has an increased risk of getting compressed. It’s a branch of the sciatic nerve called the peroneal nerve. The nerve goes around the outside of the knee before traveling down the outside of the lower leg. At the bottom of the knee, it lies between the bone and skin, making it vulnerable to irritation or compression by anything that can put pressure on the outside of the knee.
Causes
Traumatic injuries over time can lead to pressure on the nerve from inside the knee. Common causes of a compressed nerve in the knee include:
Frequently Crossing Legs
Compression by the opposite knee, while the legs are crossed is the most common cause.
Knee Brace
A too-tight or strong brace can compress the leg and nerve.
Thigh-High Compression Stockings
Designed to maintain pressure on the legs, if too tight these stockings can compress the nerve.
Squatting Posture For Long Periods
This position places pressure on the side of the knee.
Fractures
A fracture of the large lower leg bone/tibia or sometimes the small bone/fibula near the knee can entrap the nerve.
Lower Leg Cast
The portion of the cast around the knee can be tight and compress the nerve.
Tell the doctor if a cast or brace feels tight or is causing numbness or pain in the leg.
Knee-High Boots
The top of a boot can land right below the knee and be too tight pinching the nerve.
Knee Ligament Injury
The nerve can become compressed due to bleeding or inflammation from an injured ligament.
Knee Surgery Complications
This is rare, but the nerve can inadvertently get pinched during knee replacement surgery or an arthroscopic procedure.
Prolonged Bed Rest
When lying down the legs tend to rotate outward and the knees flex.
In this position, the mattress can place pressure on the nerve.
Tumors or Cysts
Tumors or cysts can develop right on top or next to a nerve irritating and compressing the area.
Abdominal or Gynecologic Surgery
The equipment used to keep the legs rotated outward and the knees flexed for gynecologic and abdominal surgeries can compress the nerve.
Symptoms
The peroneal nerve supplies sensation and movement to the outside of the lower leg and the top of the foot. When compressed, it becomes inflamed, which causes the symptoms of a compressed nerve. Usually, only the lining/myelin sheath around the nerve is what gets injured. However, when the nerve gets damaged, the symptoms are similar but more severe. Common symptoms include:
Weakness that limits the ability to lift the foot toward the leg aka dorsiflexion.
This causes dragging the foot when walking.
The ability to turn the foot outward and extend the big toe is also affected.
Symptoms can be felt on the outside of the lower leg and on the top of the foot and include:
Tingling or pins and needles sensations.
Numbness.
Loss of sensation.
Pain.
Burning.
For individuals that have had a pinched nerve for two or more weeks, the muscles supplied by the nerve can begin to waste away or atrophy.
Symptoms can be intermittent or continuous depending on the cause.
The other common cause is a pinched nerve in the lumbar/lower spine.
When this is the cause, sensations, and pain will present in the lower back or the back and outside of the thigh.
Diagnosis
A doctor will look at medical history and perform an examination to make a diagnosis, determine the cause, and lay out a personalized treatment plan. The nerve in the knee can be felt as it travels around the top of the tibia, so a doctor may tap on it. If there is shooting pain down the leg, a pinched nerve may be present. Tests a doctor may order can include:
Knee X-ray
Shows any bone fractures or abnormal masses.
Knee MRI
Can confirm the diagnosis
Shows masses within the nerve.
Shows details of fractures or other problems in the bones.
Electromyogram – EMG
Tests electrical activity in the muscles.
Nerve Conduction Test
Tests the signal speed of the nerve.
Treatment
Treatment is aimed at reducing pain and improving mobility.
Over-the-Counter Pain Medication
OTC medication can reduce inflammation and improve symptoms short term.
Ice and Heat
Applying either heat or ice for 15 to 20 minutes at a time can provide relief from the symptoms.
An ice pack can make symptoms worse if it adds more pressure on the nerve.
Chiropractic and Physical Therapy
Chiropractic and physical therapy can release the compressed nerve, realign the structures, strengthen the muscles, and provide gait training.
Orthotic Boot
If walking gait is affected because the foot cannot bend, an orthotic boot can help.
This is a support that maintains the foot in a neutral position to walk normally.
Corticosteroid Injection
A corticosteroid injection can reduce inflammation and relieve pressure on the nerve.
Surgery
The nerve can suffer permanent damage if it has been pinched for a long time.
If that happens, surgery cannot repair the damage.
A doctor can perform surgery to correct a fracture, tumor, or other invasive problem causing a compressed nerve.
If conservative treatment doesn’t work, a peroneal nerve decompression procedure can be done to remove the pressure.
If surgery is needed, symptoms can disappear immediately, but it takes around four months to recover and rehabilitate.
Injury Rehabilitation
References
Krych, Aaron J et al. “Is peroneal nerve injury associated with worse function after knee dislocation?.” Clinical orthopedics and related research vol. 472,9 (2014): 2630-6. doi:10.1007/s11999-014-3542-9
Lezak B, Massel DH, Varacallo M. Peroneal Nerve Injury. [Updated 2022 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549859/
Soltani Mohammadi, Sussan, et al. “Comparing the squatting position and traditional sitting position for ease of spinal needle placement: a randomized clinical trial.” Anesthesiology and pain medicine vol. 4,2 e13969. 5 Apr. 2014, doi:10.5812/aapm.13969
Stanitski, C L. “Rehabilitation following knee injury.” Clinics in sports medicine vol. 4,3 (1985): 495-511.
Xu, Lin, et al. Zhongguo gu Shang = China Journal of Orthopedics and Traumatology vol. 33,11 (2020): 1071-5. doi:10.12200/j.issn.1003-0034.2020.11.017
Yacub, Jennifer N et al. “Nerve injury in patients after hip and knee arthroplasties and knee arthroscopy.” American Journal of physical medicine & Rehabilitation vol. 88,8 (2009): 635-41; quiz 642-4, 691. doi:10.1097/PHM.0b013e3181ae0c9d
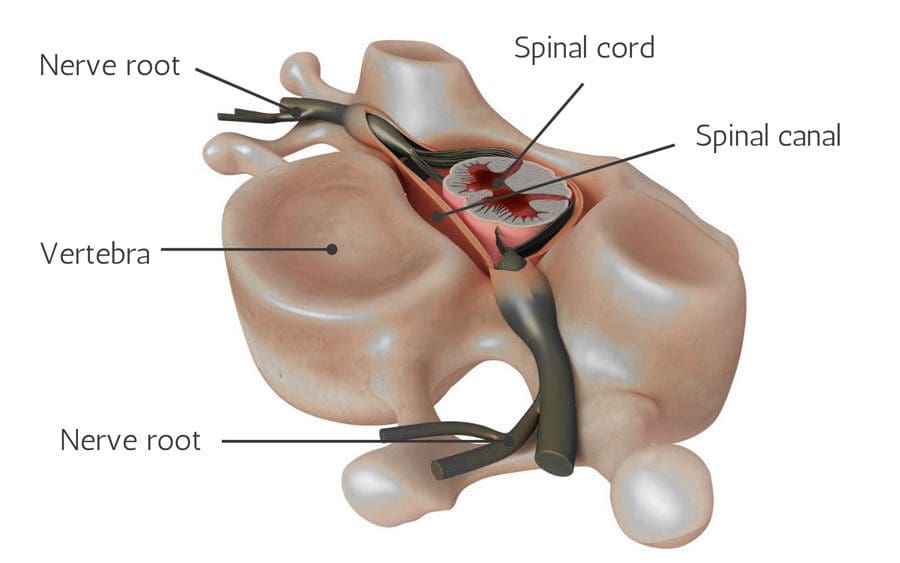
Spinal nerves send motor, sensory, and autonomic signals between the central nervous system and the body and are part of the peripheral nervous system. They are essential for carrying information that controls body movements and sensations to the brain. When a nerve gets injured, compressed, or damaged, it can cause discomfort, increased sensitivity, numbness, muscle weakness, and pain.
Damaged Nerve Roots
Nerve root pain is often caused by other underlying conditions that have caused compression or damage to the nerve root. Causes of nerve root pain can include:
Spinal nerves impacted by injuries or infection can lose their ability to control the body areas, lose their functional capacity, lose sensation, and die.
Spinal Imaging
Nerve damage can be diagnosed on a neurological exam and correlated with MRI and X-ray imaging. Conditions that MRI can identify include herniated discs, spinal cord compression or fracture, arthritic development, tumors, or cysts pressing on a nerve.
MRI images are obtained with a magnetic field and radio waves.
MRI shows spine images from the side/sagittal view and cross-sectional/axial views.
This allows the chiropractic doctor to see the vertebrae and discs and identify abnormalities.
The spinal cord is a gray area in the middle surrounded by the spinal fluid, which appears white.
Little white channels on either side of the spinal cord are where the nerve roots branch off.
X-rays can show the alignment of the bones along the spine and determine any narrowing or damage to the discs.
It is important to be evaluated and diagnosed for signs and symptoms of nerve injury as soon as possible, as nerve damage accelerates and worsens.
Function Restoration
Sometimes, the symptoms improve by themselves and do not require treatment. Nonetheless, physicians begin with conservative, non-surgical approaches to treat nerve root pain. Chiropractic and physical massage therapy involves specific movements, stretches, and exercises to keep the affected muscles and joints active,prevent stiffness and help restore function and feeling. Treatment can include:
Therapeutic massage
Manual adjustment/resistance treatment
Trigger point therapy
Instrument-assisted soft tissue therapy
Decompression
Traction
Joint stretching
Electrical stimulation
Ultrasound
Specialized exercise
Activity modification
Anti-inflammatory diet
Nerve Chiropractor
References
Liu, Yan, and Huan Wang. “Peripheral nerve injury-induced changes in the spinal cord and strategies to counteract/enhance the changes to promote nerve regeneration.” Neural regeneration research vol. 15,2 (2020): 189-198. doi:10.4103/1673-5374.265540
Menorca, Ron M G, et al. “Nerve physiology: mechanisms of injury and recovery.” Hand clinics vol. 29,3 (2013): 317-30. doi:10.1016/j.hcl.2013.04.002
Shehab, Safa Al-Deen Saudi. “Fifth lumbar spinal nerve injury causes neurochemical changes in corresponding and adjacent spinal segments: a possible mechanism underlying neuropathic pain.” Journal of chemical neuroanatomy vol. 55 (2014): 38-50. doi:10.1016/j.jchemneu.2013.12.002
Stoll, G, and H W Müller. “Nerve injury, axonal degeneration, and neural regeneration: basic insights.” Brain pathology (Zurich, Switzerland) vol. 9,2 (1999): 313-25. doi:10.1111/j.1750-3639.1999.tb00229.x
Ye, Xuan, et al. “Nerve fascicle transfer using a part of the C-7 nerve for spinal accessory nerve injury.” Journal of neurosurgery. Spine vol. 28,5 (2018): 555-561. doi:10.3171/2017.8.SPINE17582
A pinched nerve may not feel like it is healing. This is because of the soreness, aches, discomfort, and tingling feelings/sensations around the affected area. This could be the neck, shoulder, arm, hands, back, legs, and feet. However, when the achiness and tingling move around and shift, it is a sign of the pinched nerve healing.
Amount of Time For Pinched Nerve Healing
Waiting for the nerve to heal is not a recommended treatment option, as most pinched nerves do not fully recover on their own. A pinched nerve usually takes around six weeks to heal with proper treatment. The longer the nerve stays pinched, the more likely there will be permanent damage. To keep the pinched nerve from returning and getting worse, individuals are recommended to incorporate a pre-habilitation plan that involves continuing rehabilitation exercises to strengthen and keep the muscles, ligaments, and nerves loose, and adjusting posture, work, exercise, and diet habits to prevent re-injuring the nerve or cause new injury/s.
Common Nerve Sites
Nerves run throughout the body, so it’s possible to experience a pinched nerve anywhere. The most common pinched nerve sites occur at joints where there is constant movement. These areas include:
Neck
Shoulders
Lower Back
Arms
Hands
Feet
Healing Signs
Individuals often believe that their pinched nerve is getting worse because of soreness, aches and pains, and weird sensations. When the pain stays in one area, that could be a sign that the nerve has not been fully stretched/released and/or that there is still compression taking place. Treatment and healing include feeling the symptoms but in a different way. The symptoms will move up, down, or around depending on where the pinched nerve is. Treatment takes the nerve/s and stretches/elongates them, but the pinch created a nerve crimp, crease, fold that wants to return to the pinched position. This is why continued treatment and stretching are recommended, as a spasm, trauma, or some awkward movement can cause the nerve to re-fold to the pinched position or cause a whole new pinch.
Chiropractic Release
Chiropractic treats pinched/compressed nerves with several therapeutic modalities. These include:
Body Adjustments
Flexion-distraction
Therapeutic massage
Traction
Inversion
Laser therapy
Ultrasound
Combined, these methods can help heal pinched nerves and keep them from recurring.
Body Composition
Skeletal Muscle
Skeletal muscle is a major muscle group. These muscles are attached to the bone by the tendons. Skeletal muscles incorporate nerves, blood vessels, and connective tissue to operate as a unit. Each skeletal muscle consists of cells that come together that form bundles of skeletal muscle fibers.
Strength training stimulates the muscle fibers. When combined with proper nutrition causes hypertrophy/muscle growth.
Muscles contract and shorten to pull bones and joints, allowing body movement.
The nervous system signals the nerves in the muscle/s and triggers these contractions.
Skeletal muscle helps the body:
Maintain posture
Generate body heat
Stability to the bones and joints
References
Bowley, Michael P, and Christopher T Doughty. “Entrapment Neuropathies of the Lower Extremity.” The Medical clinics of North America vol. 103,2 (2019): 371-382. doi:10.1016/j.mcna.2018.10.013
Campbell, W. “Diagnosis and management of common compression and entrapment neuropathies.” Neurologic clinics vol. 15,3 (1997): 549-67. doi:10.1016/s0733-8619(05)70333-9
England, J D. “Entrapment neuropathies.” Current opinion in neurology vol. 12,5 (1999): 597-602. doi:10.1097/00019052-199910000-00014
Kane, Patrick M et al. “Double Crush Syndrome.” The Journal of the American Academy of Orthopaedic Surgeons vol. 23,9 (2015): 558-62. doi:10.5435/JAAOS-D-14-00176
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine